Embed Size (px)
Citation preview

ACLS 2010 Study Guide
1. BLS Primary Survey
• Be proficient with BLS: Check carotid pulses for less than 10 seconds.
At least 100 compressions per minute
2 breaths are given with 30 compressions for 2 minutes (5 cycles of 30:2)
Monitor “RDR” (Rate/ Depth/Recoil) during compressions
BLS primary survey continues during ALS secondary survey (ABCD)
If pulses are present with ineffective respirations, provide rescue breathing giving 1 breath every 5-6 seconds. Assess for bilateral chest rise and fall.
2. AED:
• Turn AED ON, Apply Pads, Analyzing (do not touch patient), Shock Advised, Charging (NOTE: Continue Compressions while charging), Clear and Shock
1|Page
ACLS 2010 Study Guide
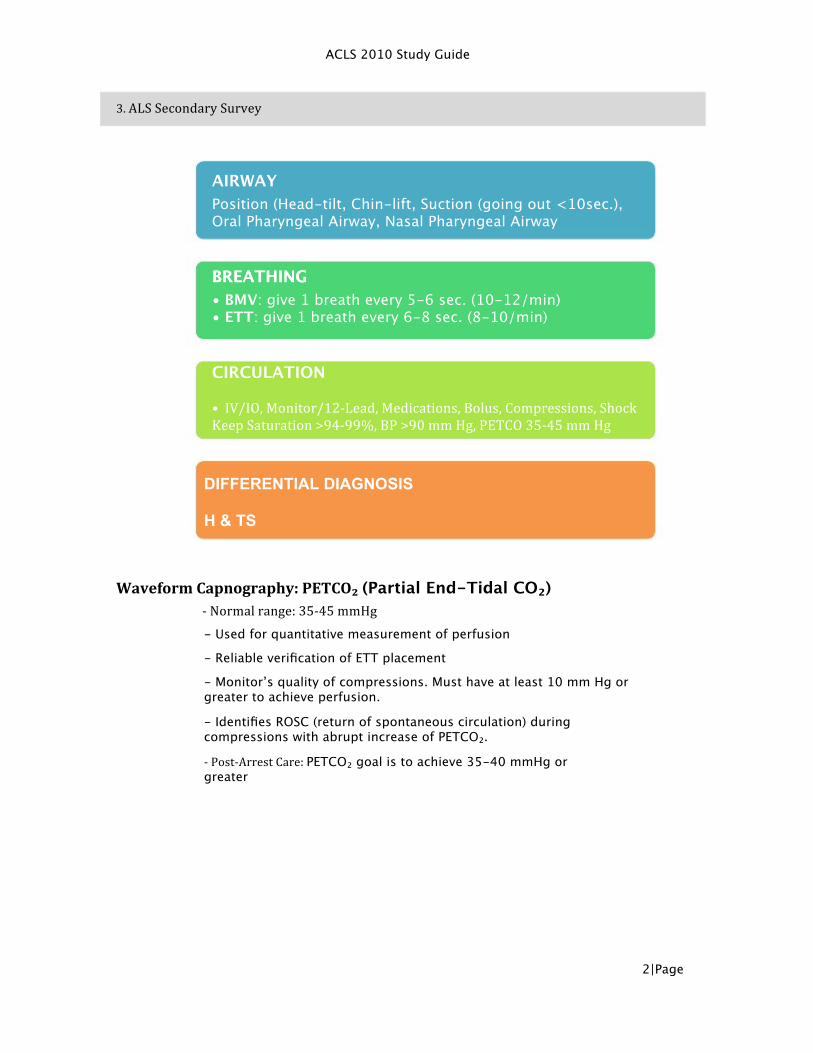
3. ALS Secondary Survey
AIRWAY Position (Head-tilt, Chin-lift, Suction (going out <10sec.), Oral Pharyngeal Airway, Nasal Pharyngeal Airway
BREATHING • BMV: give 1 breath every 5-6 sec. (10-12/min) • ETT: give 1 breath every 6-8 sec. (8-10/min)
CIRCULATION • IV/IO, Monitor/12-‐Lead, Medications, Bolus, Compressions, Shock Keep Saturation >94-‐99%, BP >90 mm Hg, PETCO 35-‐45 mm Hg
Waveform Capnography: PETCO₂ (Partial End-Tidal CO₂) -‐ Normal range: 35-‐45 mmHg
- Used for quantitative measurement of perfusion - Reliable verification of ETT placement - Monitor’s quality of compressions. Must have at least 10 mm Hg or greater to achieve perfusion. - Identifies ROSC (return of spontaneous circulation) during compressions with abrupt increase of PETCO₂.
2|Page
BREATHING
DIFFERENTIAL DIAGNOSIS H & TS
-‐ Post-‐Arrest Care: PETCO₂ goal is to achieve 35-40 mmHg or greater
ACLS 2010 Study Guide
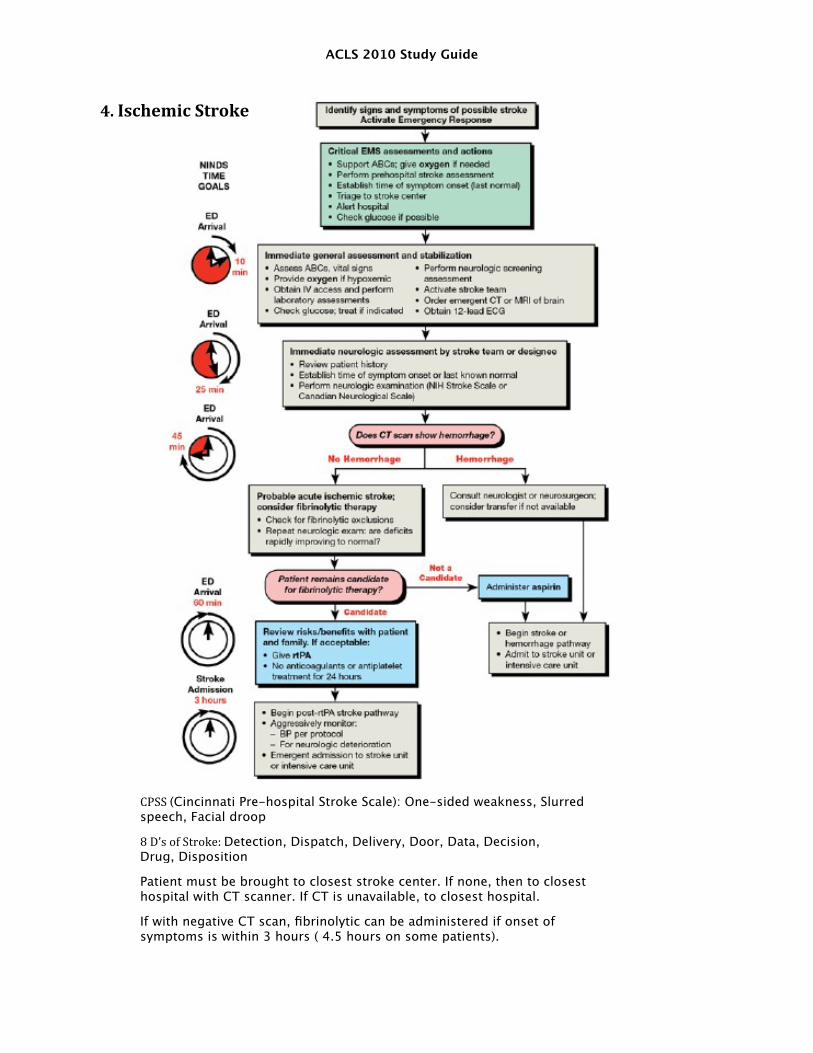
4. Ischemic Stroke
CPSS (Cincinnati Pre-hospital Stroke Scale): One-sided weakness, Slurred speech, Facial droop 8 D’s of Stroke: Detection, Dispatch, Delivery, Door, Data, Decision, Drug, Disposition Patient must be brought to closest stroke center. If none, then to closest hospital with CT scanner. If CT is unavailable, to closest hospital. If with negative CT scan, fibrinolytic can be administered if onset of symptoms is within 3 hours ( 4.5 hours on some patients).

ACLS 2010 Study Guide
4|Page

ACLS 2010 Study Guide
5. Acute Coronary Syndrome
5|Page

ACLS 2010 Study Guide
•
•
• •
Focus on STEMI (ST Elevation MI) pathway, verified on 2 contiguous leads on 12-Lead Memorize “MONA” doses and contraindications specially for Nitro and Morphine Know atypical signs of MI Know contraindications of Right Ventricular Infarction (RVI) or Inferior Infarct
6|Page

ACLS 2010 Study Guide
6. Invtravenous/Intraosseous
•
•
Preferred route of medication administration is via peripheral IV
After multiple attempts of IV insertion without success, IO is inserted.
Know IO insertion sites and be familiar with various IOs
All medications given through IV can be administered via IO.
Goals of IO: Insertion, Administration and Discontinuation (<24 hours)
•
•
•
7|Page

ACLS 2010 Study Guide
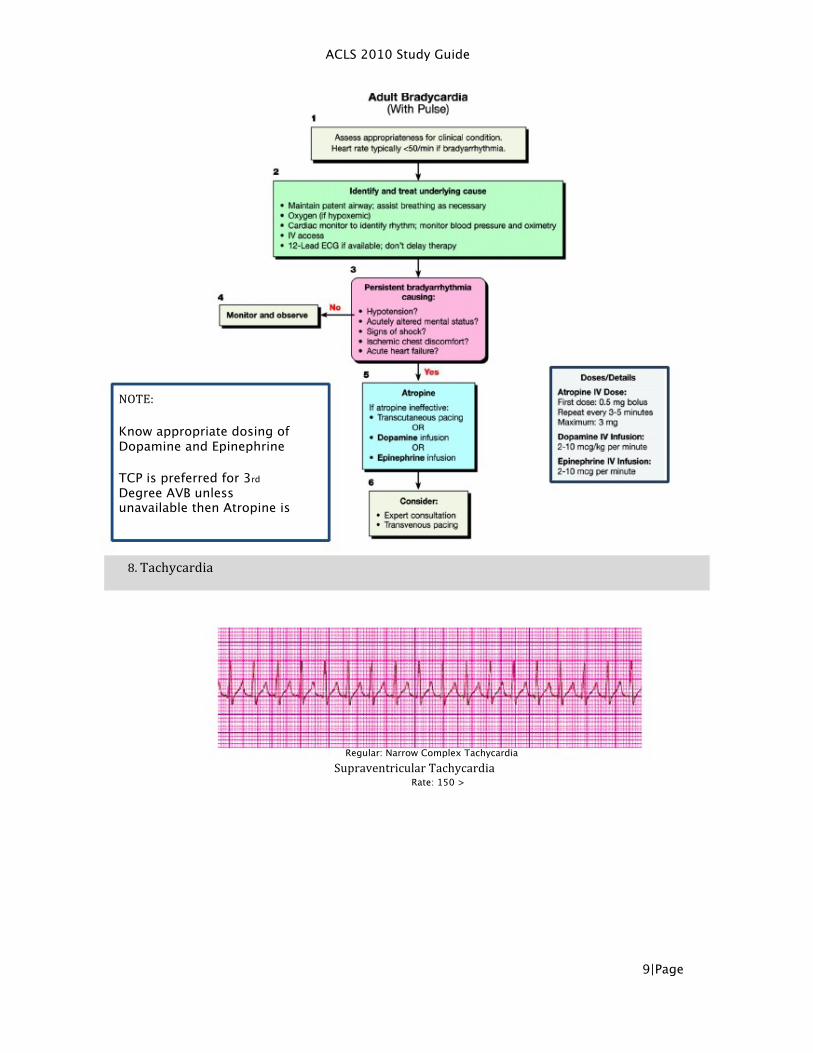
7. Bradycardia
Sinus Bradycardia
3rd Degree AV Block
8|Page
ACLS 2010 Study Guide
NOTE:
Know appropriate dosing of Dopamine and Epinephrine
TCP is preferred for 3rd Degree AVB unless unavailable then Atropine is
8. Tachycardia
Regular: Narrow Complex Tachycardia Supraventricular Tachycardia
Rate: 150 >
9|Page

ACLS 2010 Study Guide
Irregular: Narrow Complex Tachycardia Atrial Fibrillation
Regular: Monomorphic Wide Complex Tachycardia Ventricular Tachycardia
Irregular: Polymorphic Wide Complex Tachycardia
Torsade de Pointes
Synchronize
10 | P a g e
ACLS 2010 Study Guide
11 | P a g e

ACLS 2010 Study Guide
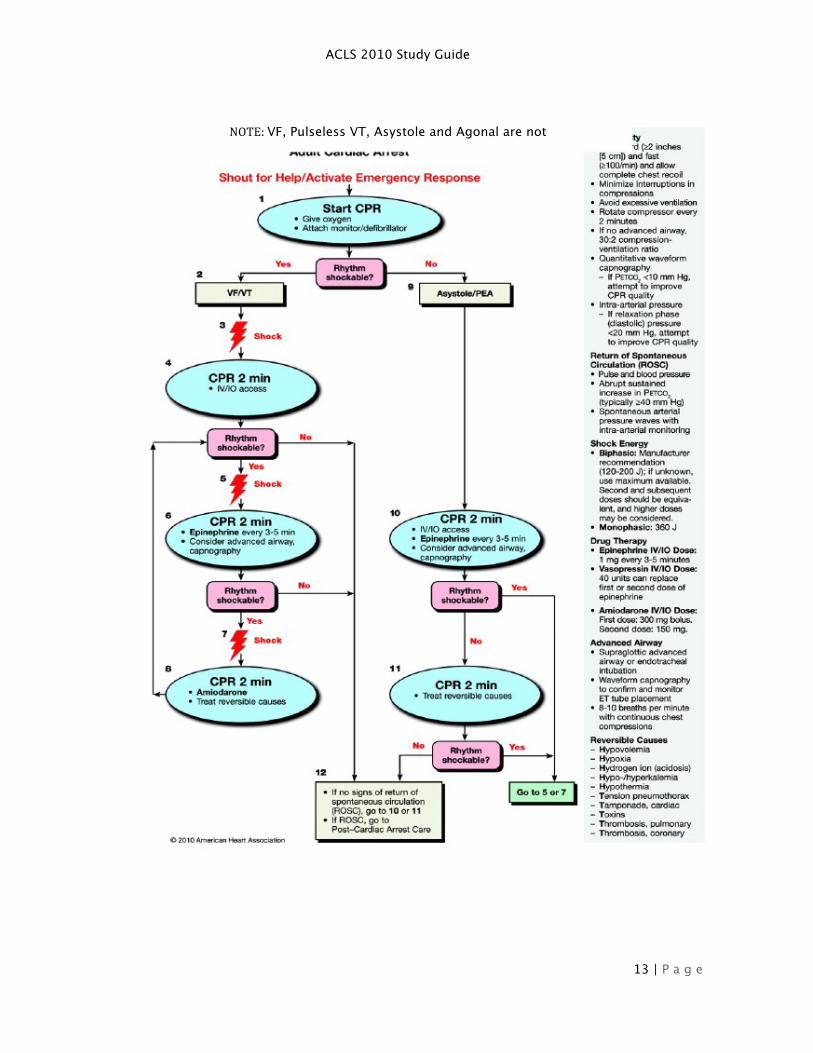
9. Pulseless Arrest
Ventricular Fibrillation
No Pulse Pulseless Ventricular Tachycardi a
Asystole
No Pulse
Pulseless Electrical Activity 12 | P a g e
ACLS 2010 Study Guide
NOTE: VF, Pulseless VT, Asystole and Agonal are not
13 | P a g e

ACLS 2010 Study Guide
10. Post-‐Resuscitation Care: ROSC
• • • • • • •
ROSC (Return of Spontaneous Circulation) Maintain O₂ Sat 94%>, titrate 10-12 breaths/min Consider advanced airway and maintain PETCO₂ 35-40 mm Hg> 1-2 L NS/LR bolus (at 4˚C to induce hypothermia if ALOC) Titrate vasopressors to keep BP 90 mm Hg> Identify and treat reversible causes 12-Lead ECG for possible PCI if STEMI or high suspicion of AMI
14 | P a g e

ACLS 2010 Study Guide
Consider hypothermia for 12-24 hours in ALOC for cerebral oxygenation and ventilation • Keep glucose slightly above normal to avoid hypoglycemia during hypothermia
•
11. Termination of Resuscitation Effort
•
•
•
•
•
•
•
•
DNAR (Do Not Attempt Resuscitation)
Decapitation
Presence of Rigor Mortis
Continued decompensation during resuscitative efforts
Inherent danger to team during resuscitation
Unwitnessed arrest
No defibrillation during BLS or ALS
MD ordered termination
15 | P a g e





























