Embed Size (px)
Citation preview

177Lu-Dotatate Significantly Improves Progression-Free Survival in Patients with Midgut Neuroendocrine Tumours: Results of the Phase III NETTER-1 Trial
Jonathan Strosberg1, Edward Wolin2, Beth Chasen3, Matthew Kulke4, David Bushnell5, Martyn Caplin6, Richard P. Baum7, Erik Mittra8, Timothy Hobday9, Andrew Hendifar10, Kjell Oberg11, Maribel Lopera Sierra12, Philippe Ruszniewski13, Dik Kwekkeboom14 on behalf of the NETTER-1 study group
1 Moffitt Cancer Center, Tampa, FL 33612, USA;2 Markey Cancer Center, University of Kentucky, Lexington, KY 40536-0093, USA;3 University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA;4 Dana-Farber Cancer Institute, Boston, MA 02215, USA;5 University of Iowa, Iowa City, IA 52242, USA;6 Royal Free Hospital, London, United Kingdom;7 Zentralklinik, Bad Berka, Germany;8 Stanford University Medical Center, Stanford, CA 94305, USA;9 Mayo Clinic College of Medicine, Rochester, MN 55905, USA;10 Cedars Sinai Medical Center, Los Angeles, CA 90048, USA;11 University Hospital, Uppsala University, Uppsala, Sweden;12 Advanced Accelerator Applications, New York, NY 10118, USA;13 Hopital Beaujon, Clichy, France;14 Erasmus Medical Center, Rotterdam, Netherlands
1Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna

Introduction
• Neuro Endocrine Tumors, also known as NETs, are a group of tumors originating in the neuroendocrine cells of many different organs. NETs can remain clinically silent for years delaying the diagnosis in a large number of patients. These cancers are rare but they are the second most common type of gastrointestinal malignancy and their incidence is increasing.
• The estimated incidence of NETs for the combined populations of the United States and the European Union is approximately 47,3001.
• NETs are classified as orphan diseases by European and U.S. regulatory authorities.
• From 1973 to 2004, incidence of NETs has grown by almost 500% (from 1,09/100,000 to 5,25/100,000 respectively).2
• There are limited therapeutic options for patients with advanced midgut neuroendocrine tumours (20-45% of NETs) progressing on first-line somatostatin analogue therapy.
• Thousands of patients have been treated with 177Lu-Dotatate peptide receptor radionuclide therapy (PRRT) with promising results.
2Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
1. Lawrence B, et al. 2011, 2. JC Yao et al. 2008 - see abstract on 1st page. 2. Yao et al: One hundred years after « carcinoid »: epidemiology of and prognostic factors for NET in 35,825 cases in the US. J. Clinical Oncology 26:3063-3072

1.Yao et al: One hundred years after « carcinoid »: epidemiology of and prognostic factors for NET in 35,825 cases in the US. J. Clinical Oncology 26:3063-3072; 2. SEER: National Cancer Institute’s Surveillance, Epidemiology, and End Results
Incidence of NETs vs all malignant neoplasms from 1973 to 20042.
• From 1973 to 2004, incidence of NETs has grown by almost 500% (from 1,09/100,000 to 5,25/100,000 respectively)1
NET EpidemiologyA growing population of patients

• 177Lu-DOTATATE belongs to an innovative drug category called PRRT (Peptide Receptor Radionuclide Therapy). PRRT involves the systemic administration of a specific radiopharmaceutical to deliver cytotoxic radiation to a tumor1
• 177Lu-DOTATATE is composed of a lutetium radionuclide chelated to a peptide1. Lutetium emits high energy electrons (therapy) and gamma rays (imaging).
• The peptide is designed to target somatostatin receptors1 which are overexpressed in approximately 80% of NETs.
1. Zaknun et al. Eur J Nucl Med Mol Imaging 2013, 40: 800-16; 2. Bergsma et al. Best Practice & Res Clin Gastroenterol 2012, 26: 867-81 3. Reubi et al. Eur J Nucl Med Mol Imaging 2003, 30: 781-93
The affinity for SSTRs and the specificity of binding ensures a high level of specificity in the delivery of radiation to the tumor
Structure of a radiopharmaceutical2
4
A brief presentation of 177Lu-DOTATATE
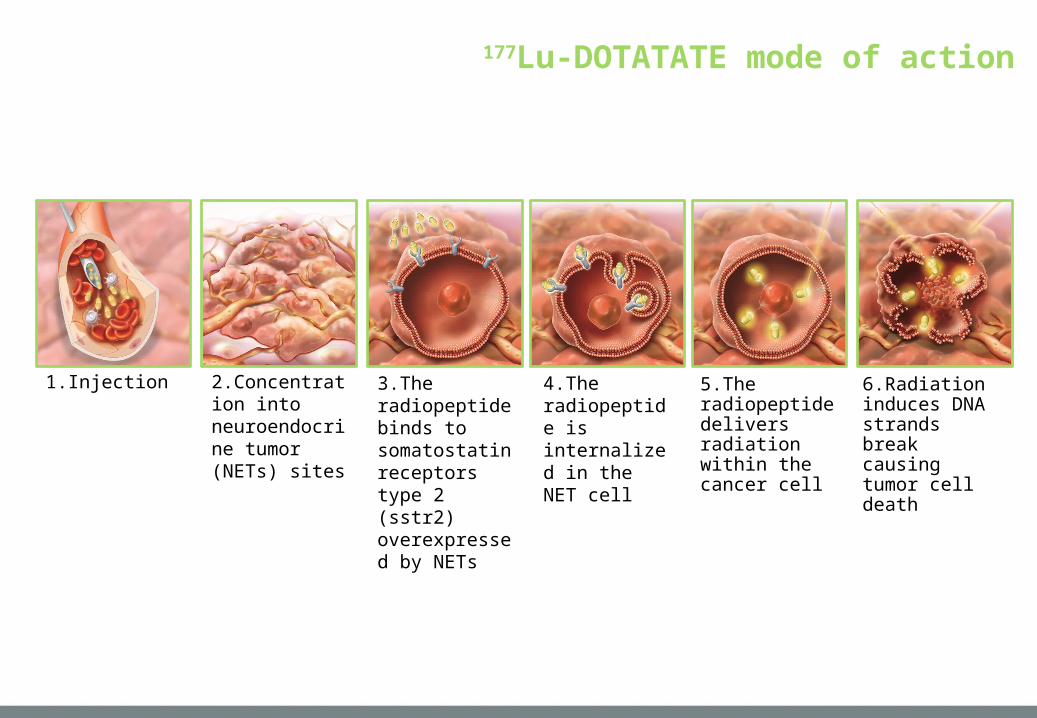
177Lu-DOTATATE mode of action
5.The radiopeptide delivers radiation within the cancer cell
6.Radiation induces DNA strands break causing tumor cell death
4.The radiopeptide is internalized in the NET cell
1.Injection 2.Concentration into neuroendocrine tumor (NETs) sites
3.The radiopeptide binds to somatostatin receptors type 2 (sstr2) overexpressed by NETs

Progression-Free Survival
6Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
Hazard Ratio [95% CI]0.209 [0.129 – 0.338]Risk reduction: 79.1p < 0.0001
N = 229 (ITT)Number of events: 90
• 177Lu-Dotatate: 23 • Oct 60 mg LAR: 67
All progressions centrally confirmed and independently reviewed for eligibility (SAP)
Octreotide LAR 60 mgMedian PFS: 8.4 months
177Lu-DotatateMedian PFS: Not reached

Tumour Response Rate(currently evaluable patients)
7Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
177Lu-Dotatate
(n=101)Octreotide LAR 60mg
(n=100)
Complete Response (n) 1 0
Partial Response (n) 18 3
Objective Response Rate (CI 95%)
19 (11-26) % 3 (0-6) % *
Progressive Disease (n, %) 5 (4%) 27 (24%)
Stable Disease (n, %) 77 (66%) 70 (62%)
*P<0.0004

Overall Survival (interim analysis)
8Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
N = 229 (ITT)Number of deaths: 35
• 177Lu-Dotatate: 13• Octreotide 60 mg LAR: 22
P < 0.0186
0.5

177Lu-Dotatate Safety - SAE
9Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
SAE (n)
Blood & lymphatic systemLymphocytopeniaThrombocytopeniaNeutropeniaPancytopeniaBicytopenia
731111
Renal & urinary disordersAcute kidney injuryRenal failure
321
Vascular disordersPortal hypertension
11

Summary and Conclusions
10Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
• In this first prospective randomized study in patients with progressive metastatic midgut NETs, 177Lu-Dotatate was superior to Octreotide 60 mg in terms of PFS (NR vs 8.4 months, p<0.0001) and ORR (19% vs 3%, p<0.0004)
• Interim analysis suggests increased overall survival (13 vs 22 deaths), to be confirmed by final analysis(
• Currently available safety data confirm the results of Phase I-II study, with favorable safety profile
• While few treatment options were up to now available, 177Lu-Dotatate appears as a major advance in this patient population

177Lu-Dotatate Significantly Improves Progression-Free Survival in Patients with Midgut Neuroendocrine Tumours:
Results of the Phase III NETTER-1 Trial
Back-up Slides
11Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna

Introduction
• There are limited therapeutic options for patients with advanced midgut neuroendocrine tumours (20-45% of NETs) progressing on first-line somatostatin analogue therapy.
• Thousands of patients have been treated with 177Lu-Dotatate peptide receptor radionuclide therapy (PRRT) with promising results.
12Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
Lutathera Phase I-II resultsDisease related survival in 310 patients according to treatement outcome.Ref: Kwekkeboom D.J et coll., J Clin Oncol, 2008, 26: 2124-2130.

Neuro Endocrine Tumors (NETs) Overview
NETs~47,300 patients/year in the US & EU1
~288,000 patients in US & EU2
GEP-NETs* (GI NET** + pNETs***)
~30,000 patients/year in the US & EU1
~175,000 patients in US & EU2
· Heterogeneous group of tumors originating from the cells of the endocrine (hormonal) and nervous systems
· They have different behavior depending on the site of origin
What are NETs? Current Treatment Paradigm
· Many patients do not have symptoms => incidental finding.
· When present, symptoms unspecific => delayed diagnosis
· Diagnosis is made with radiolabeled somatostatin analogs (SSA) such as Octreoscan
· There is a significant unmet medical need for patients with inoperable GEPNETs who are progressive under SSAs. Patients lack options for antiproliferative treatment.
· ~80% of NETs overexpress somatostatin receptors (particularly sstr2)· NETs are generally slow-growing tumors and
therefore prevalence is high compared to incidence
1. Lawrence B, et al. 2011 (table3 page8), 2. JC Yao et al. 2008 - see abstract on 1st page
* Gastroenteropancreatic NETs** Gastrointestinal NETs*** Pancreatic NETs
61% of NETs1

14Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
Aim
Design International, multicenter, randomized, comparator-controlled, parallel-group Phase III study conducted in 51 centers with 230 patients randomized
Evaluate the efficacy and safety of 177Lu-Dotatate plus Octreotide30 mg compared to Novartis Octreotide LAR 60mg (off-label use)1 in patients with inoperable, somatostatin receptor positive, midgut NET, progressive under Octreotide LAR 30mg (label use)
Baseline and
Randomization
n = 115
Dose 1
n = 115
Treatment and AssessmentsProgression free survival (Recist criteria) every 12 weeks
5 Years follow
up
Dose 2 Dose 3 Dose 4
NETTER -1 Study Objectives and Design
1. FDA and EMA recommendation
4 administrations of 7.4 GBq of LUTATHERA every 8 weeks + Octreotide30 mg
Octreotide LAR 60mg every 4 weeks

Participating Sites in 51 centers - 11 countries
15Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna

Study Endpoints
16Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
Primary objective
Compare Progression Free Survival (PFS) after treatment with 177Lu-Dotatate plus 30 mg octreotide LAR vs treatment with high dose (60 mg) octreotide LAR
Secondary objectives
▪Compare the Objective Response Rate between study arms
▪Compare the Overall Survival between study arms
▪Compare the Time to Progression between study arms
▪Evaluate the safety and tolerability of 177Lu-Dotatate
▪Evaluate the health related quality of life (QoL) as measured by the EORTC QLQ-G.I.NET21 questionnaire

177Lu-Dotatate Exposure
17Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
Patients who completed trt phase, N=102* Nb of Patients
Drug exposure, n (%)800 mCi400 – 800 mCi200 – 400 mCi200 mCiNo administration
81 (79%)5 (5%)9 (9%)3 (3%)4 (4%)
Number of administrations, n (%)43210
78 (76%)5 (5%)
11 (11%)4 (4%)4 (4%)
Dose modifying toxicity, n (%)All treated patients – N=111
No DMTDMT
105 (95%)6 (5%)
*14 pts still under treatment

Safety and Tolerability(Nb of patients (%), Safety Set; n=221)
18Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
177-Lu-Dotatate
(n=111)Octreotide LAR 60mg (n=110)
Any adverse event 106 (96%) 95 (86%)
Related to treatment 95 (86%) 34 (31%)
Serious adverse events 29 (26%) 26 (24%)
Related to treatment 10 (9%) 1 (1%)
Withdrawals due to adverse events 7 (6%) 10 (9%)
Related to treatment 5 (5%) 0 (0%)
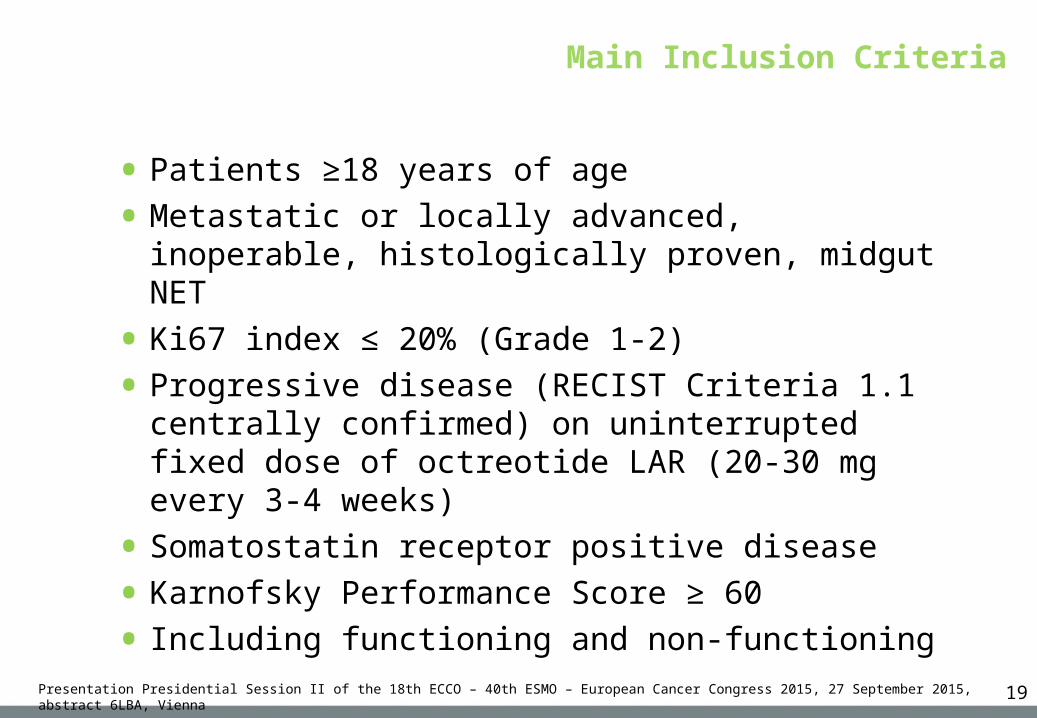
Main Inclusion Criteria
19Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
• Patients ≥18 years of age
• Metastatic or locally advanced, inoperable, histologically proven, midgut NET
• Ki67 index ≤ 20% (Grade 1-2)
• Progressive disease (RECIST Criteria 1.1 centrally confirmed) on uninterrupted fixed dose of octreotide LAR (20-30 mg every 3-4 weeks)
• Somatostatin receptor positive disease
• Karnofsky Performance Score ≥ 60
• Including functioning and non-functioning

Population Characteristics at Enrolment(ITT population, N=229)
20
177Lu-Dotatate
(n=116)Octreotide LAR 60mg
(n=113)
Gender, n (%)MaleFemale
53 (46%)63 (54%)
60 (53%)53 (47%)
Age (years), mean (SD) 63 (±9) 64 (±10)
BMI (Kg/sqm), mean (SD) 25 (±5) 26 (±7)
Primary tumour site, n (%)JejunumIleumAppendixRight colonOther
6 (5%)86 (74%)1 (1%)3 (3%)
20 (17%)
9 (8%)82 (73%)2 (2%)1 (1%)
19 (17%)
Site of metastasis, n (%)LiverLymph nodesBoneLungsOther
97 (84%)77 (66%)13 (11%)11 (10%)40 (35%)
94 (83%)65 (58%)12 (11%)5 (4%)
37 (33%)
Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna

Population Characteristics at Enrolment(ITT population, N=229)
21Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
177Lu-Dotatate
(n=116)Octreotide LAR 60mg
(n=113)
Ki67, n (%)ENETS G1/G2 76/40 (66/34%) 81/32 (72/28%)
SRS, Krenning scale, n (%)Grade 2Grade 3Grade 4
13 (11%)34 (29%)69 (60%)
14 (12%)32 (28%)67 (59%)
Chromogranin A (µg/L), mean (SD) 649 (420) 670 (422)
5-HIAA (mg/24h), mean (SD)* 100 (183) 77 (83)
*Only available in 98 patients
Main Exclusion Criteria
22Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
• Serum creatinine >150 µmol/L, or creatinine clearance <50 mL/min
• Hb concentration <5.0 mmol/L
• WBC <2x109/L , Platelets <75x109/L
• Treatment with >30 mg Octreotide LAR at 3-4 weeks intervals within 12 weeks prior to randomization
• Surgery, radioembolization, chemoembolization, chemotherapy and RF ablation within 12 weeks prior to randomization

Assumptions Primary End-Point PFS
23Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
▪ 177Lu-Dotatate: median PFS of 30 months(conservative vs data from Phase I/II)
▪ Octreotide LAR: median PFS of 14 months (PROMID study)
▪ Significance level 5% two-sided with 90% power
▪ Pre-defined accrual period: 18 months
▪ Follow-up period: 18 months (length of standard trt period)
▪ Sample size: 124 patients (62 per trt group)
▪ Number of events: 74 evaluable and centrally confirmed disease progression (RECIST criteria assessed every 12±1 weeks)
Assumptions Secondary End-Point OS
24Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
▪ 177Lu-Dotatate: median OS of 50 months(data from Phase I/II confirmed with published studies)
▪ Octreotide mg LAR: median OS of 32 months (RADIANT-2)
▪ Significance level 5% two-sided with 80% power
▪ Pre-defined accrual period: 18 months
▪ Follow-up period: 5 years
▪ Sample size: 230 patients (115 per trt group)
▪ Number of events: 158 confirmed events
▪ Interim analysis at the time of the PFS analysis: significance level adjusted to 0.0085% (p<0.000085)

Current Status – Statistical Analysis
25Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
▪ End of recruitment in Dec 2014
▪ Substudy still ongoing (not randomized population)
▪ DB cut-off date of July 24, 2015, with primary end-point analysis
▪ Submission of first results (PFS) at ESMO and NANETS
▪ Database complete lock on Sept 14, 2015
▪ Statistical analysis ongoing; main results on Sept 18, 2015
▪ Full Statistical Report expected end of October 2015
▪ Aligned with FDA/EMA expectations for demonstrating therapeutic benefit and acceptable safety profile to support approval.

Population Characteristics at Enrolment(ITT population, N=229)
26Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
177Lu-Dotatate
(n=116)Octreotide LAR 60mg
(n=113)
Synaptophysin, n (%)0% positive cells1-50% positive
cells> 50% positive
cellsNot evaluable
1 (0.9%)3 (2.6%)
111 (95.7%)1 (0.9%)
0 (0.0%)4 (3.5%)
108 (95.6%)1 (0.9%)
Overall tumour burden, n (%)LimitedModerateExtensive
99 (85.3%)13 (11.2%)4 (3.4%)
98 (86.7%)13 (11.5%)2 (1.8%)
Chromogranin A, n (%)0% positive cells1-50% positive
cells> 50% positive
cellsNot evaluable
2 (1.7%)5 (4.3%)
107 (92.2%)2 (1.7%)
1 (0.9%)5 (4.4%)
106 (93.8%)1 (0.9%)
Population Characteristics at Enrolment(ITT population, N=229)
27Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
177Lu-Dotatate
(n=116)
OctreotideLAR 60mg
(n=113)
Chromogranin A (µg/L), mean (SD)N=207 (Lutate: 101 - Octreotide: 106)
648.9 (419.6) 670.4 (421.6)
5-HIAA (mg/24h), mean (SD)N=98 (Lutate: 47 - Octreotide: 51)
100.1 (183.3) 76.9 (83.3)
Alkaline phosphatase (U/L), mean (SD)N=209 (Lutate: 111 - Octreotide: 98)
173.8 (269.1) 155.8 (170.5)

Prior Cancer Treatments at Enrolment(ITT population, N=229)
28
177Lu-Dotatate
(n=116)Octreotide LAR 60mg
(n=113)
Prior resection, n (%) 90 (78%) 93 (82%)
Prior ablation, n (%) 6 (5%) 11 (10%)
Chemo-embolization, n (%) 14 (12%) 11 (10%)
Time since last intervention, yrs (SD) 4.7 (±3.3) 5.7 (±3.6)
Type of previous treatmentRadiotherapyPRRTChemotherapyOther
7 (4%)1 (1%)
47 (27%)48 (28%)
8 (5%)0 (0%)
51 (30%)40 (24%)
Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna

Patient Disposition(ITT population, N=229)
29Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
177Lu-Dotatate
(n=116)Octreotide LAR 60mg (n=113)
Reason for end of treatment phasen (%)
Consent withdrawalBest subject interestAdverse eventDisease progression
9 (8%)10 (9%) 7 (6%)
19 (16%)
9 (8%)9 (8%)7 (6%)
58 (51%)

Population Characteristics at Enrolment(ITT population, N=229)
30Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
177Lu-Dotatate
(n=116)
Octreotide LAR 60mg
(n=113)
Statistical Significance
Time since first diagnosis (years) 5.13 5.93 NS (p=0.09)
Time since first disease progression (years) 2.73 2.93 NS (p=0.42)
Time since diagnosis of metastasis (years) 4.28 4.97 NS (p=0.30)

Treatment Time without Progression(at the cut-off date for analysis)
Treatment Time (months) 177Lu-Dotatate
(n=99)Octreotide LAR
60mg (n=55)
Mean 15.1 13.1
Maximum 32.2 33.6
Median 14.4 11.9
Minimum 1.6 1.7

Safety and Tolerability - All Grades(Safety Set; n=221)
Maximal Severity, number of episodes
177-Lu-Dotatate(n=111)
Octreotide LAR 60mg (n=110)
Grade 1 (mild) 938 494
Grade 2 (moderate) 370 178
Grade 3 (severe) 98 56
Grade 4 (threatening / disabling) 5 6
Grade 5 (death) 5 8
Missing 19 2