Embed Size (px)
DESCRIPTION
tringtrungtrengtrong
Citation preview

G I N J A L G I N J A L & &
SALURAN KEMIHSALURAN KEMIH
Dr. T. Ibnu Alferraly, SpPADr. T. Ibnu Alferraly, SpPADepartemen Patologi Anatomi Departemen Patologi Anatomi
Fakultas Kedokteran – USU / UISUFakultas Kedokteran – USU / UISU20082008

Specific Function of KidneySpecific Function of Kidney
• Filtering Wastes From Blood Filtering Wastes From Blood PlasmaPlasma The kidneys filter blood plasma out of the The kidneys filter blood plasma out of the
bloodstream and remove its undesirable substances bloodstream and remove its undesirable substances to produce urine. to produce urine.
The kidneys filter about 180 quarts of blood plasma out of the The kidneys filter about 180 quarts of blood plasma out of the bloodstream each day. bloodstream each day.
About 99% of this blood plasma (minus most of the wastes) is About 99% of this blood plasma (minus most of the wastes) is reabsorbed by the kidneys to reduce urine production to about 1 to 2 reabsorbed by the kidneys to reduce urine production to about 1 to 2 quarts each day. quarts each day.
Without functioning kidneys, wastes accumulate in the blood causing a Without functioning kidneys, wastes accumulate in the blood causing a serious condition called "uremic poisoning" or "uremia."serious condition called "uremic poisoning" or "uremia."
Kidneys are also responsible for regulating the acidity of the blood by Kidneys are also responsible for regulating the acidity of the blood by excreting alkaline salts when necessary. excreting alkaline salts when necessary.



Kidneys :
• retroperitoneum ; 130 – 150 gr each• surface smooth, capsule (+), surrounded perinephric fat + Gerota’s fascia• anatomic unit : NEPHRON = glomerulus, proximal convulated tubule, loop of Henle, tubules• 1 kidneys = 1 million nephrons
Renal Functions
• Glomerular FiltrationGFR normal : 120 ml / min, measured by : the clearence of exo –genous inulin ( Inulin Clearance Test ) or endogenous creatinine( Creatinine Clearance )
• Tubular Reabsorption

Urine FormationUrine Formation
Glomerular filtrationGlomerular filtration Tubular reabsorptionTubular reabsorption Tubular secretionTubular secretion
Urinary excretion :Urinary excretion : glomerular filtration + tubular secretionglomerular filtration + tubular secretion
- tubular reabsorption- tubular reabsorption

The normal renal cortex contains glomeruli, other vessels, tubules and interstitium. When evaluating a renal specimen by light microscopy on an H&E stained section

In the glomerular diagram, The different colors indicate the various cell types that are of interest in assessing the pathologic changes that occur in a glomerulus (green = epithelial cells, yellow = endothelial cells, red = mesangial cells).
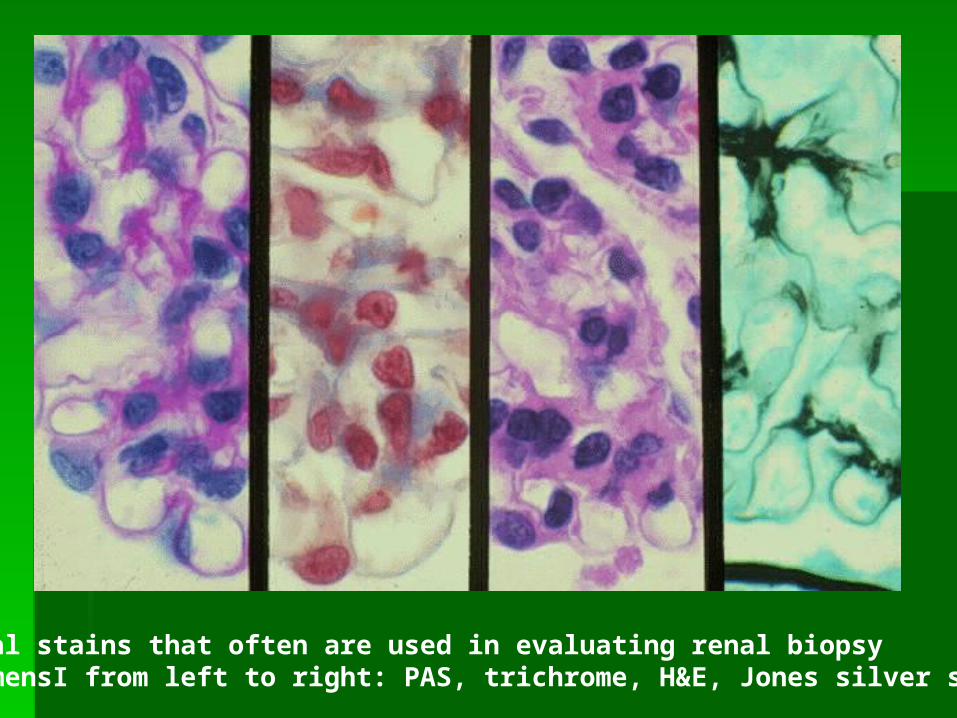
Special stains that often are used in evaluating renal biopsy specimensI from left to right: PAS, trichrome, H&E, Jones silver stains).

Diagram of a single glomerular capillary and illustrates the ultrastructural features that are assessed when evaluating renal biopsy specimens.

Electron micrograph that shows a portion of 1 capillary loop with adjacent mesangium

Much higher magnification electron micrograph. The urinary space and the foot processes are at the top.

Gejala Klinis Penyakit Ginjal :
• Sakit- Parenkhim ginjal : tanpa ujung saraf rasa sakit- Rasa sakit Ok :
> Meregangnya fascia ginjal > KOntraksi otot ureter : pd obstruksi ( urethral collic )
• Hematuria- Dengan / tanpa rasa sakit- Severe : urin merah, tkt rendah : tidak terlihat, tetqpi dengan mikr’kop pd sedimen urin eritrosit (+)- Penyebab :
> Penyakit Ginjal : glomerulonefritis, pyelonefritis, neoplasma, trauma, calculi, dll
> Penyakit2 pada kndung kemih, ureter, uretra : cystitis, uretri- tis, calculi, dll> Penyakit sistemik yg menyebabkan perdarahan saluran kemih : malignant hypertension, emboli sistemik pd endo – karditis, diathesis, terapi antokoagulan, Osler-Weber-Randu Diseade

Proteinuria
• Sangat bermanfaat utk screening peny ginjal• Bbrp individu : orthostatic / exercise proteinuria
Pyuria Adanya neutrofil pd urin
Sindroma nefrotik> 3,5 gr/d + hipoproteinemia + edema
Nefritis Akut ( Acute Nephritic Syndrome )oliguria ( < 700 ml/d ) + hematuria + proteinuria + hipertensi +
azotemia
Gagal Ginjal ( acute / chronic )
Hipertensi

Pemeriksaan :
• Fisik diagnostik• Radiologi
- foto abdomen polos- intravenous pyelography- ultrasonography- renal arteriography
• Pemeriksaan urin• Pemeriksaan darah• Biopsi ginjal

Kelainan Ginjal Kongenital
• Renal Agenesis ( unilateral or lateral )• Renal Hypoplasia : ginjal < 50 gr pd dewasa• Ectopic Kidney : dapat sebabkan obstruksi dan infeksi• Horshoe Kidney• Renal Dysgenesis ( Displasia Ginjal )
Kelainan Kistik Ginjal :
• Adult Policistic Disease• Infantile Polycistic Disease• Medullary Cystic Disease• Glomerulocystic Disease• Simple Renal Cysts• Dialysis Cystic Disease

Clinical Presentations of Glomerular Diseases
Clinical Manifestations of Glomerular Disease
•asymptomatic proteinuria •nephrotic syndrome (proteinuria, hypoproteinemia, hyperlipidemia, edema) •asymptomatic hematuria •glomerulonephritis (hematuria, proteinuria, hypertension, renal failure) •acute glomerulonephritis (neprhitis with short term renal failure) •crescentic glomerulonephritis (nephritis with rapidly progressive renal failure) •chronic glomerulonephritis (chronic progression of renal failure) •End Stage Renal Disease (irreversible renal failure)

Penyakit Yang Terutama Mengenai GlomerulusPenyakit Yang Terutama Mengenai Glomerulus
Glomerulonefritis proliferatifGlomerulonefritis proliferatif kelainan minimalkelainan minimal nefropati mebranosa (epimembranosa atau nefropati mebranosa (epimembranosa atau
ekstramembranosa).ekstramembranosa). glomerulosklerosis fokalglomerulosklerosis fokal glomerulonefritis menahun (khronik)glomerulonefritis menahun (khronik)
• Glomerulonephritis fokal yang mungkin berasal imunologik, tetapi bukan Glomerulonephritis fokal yang mungkin berasal imunologik, tetapi bukan oleh infeksi sistemik oleh infeksi sistemik
Kelainan itu secara klinik dibagi atas :Kelainan itu secara klinik dibagi atas :- glomerulonephritis fokal idiopatik,- glomerulonephritis fokal idiopatik,- hematuria recurrens- hematuria recurrens- kerusakan ginjal sebagai bagian penyakit komplex - kerusakan ginjal sebagai bagian penyakit komplex
imun imun sistemik seperti lupus erythematosus, periarteritis sistemik seperti lupus erythematosus, periarteritis nodosa, dan purpura Schonelein-Henoch nodosa, dan purpura Schonelein-Henoch
(purpura (purpura anafilaktoid). anafilaktoid).

PENYAKIT – PENYAKIT GLOMERULUS :
Glomerulonephritis acute. Etio : Streptococcus
VirusStaphylococcusPneumococcus
Patogenesis :* Biasanya didahului oleh infeksi ISPA, tonsi - litis, pharingitis, otitis, mastoiditis, infeksi kulit.* Kemudian timbul reaksi agab * Agab complex melekat ke glomerulus menim bulkan reaksi radang terutama pada membran basalis glomerulus* Glomerulus kehilangan foot processus
Klinis : - Edema pada muka & peri orbital- Edema bisa ke tangkai bawah- Malaise, demam- Mual muntah- Oliguria, proteinuria, hematuria- Hipertensi

Makroskopik :> Glomerulus hipertrofi dan hiperselular dan proliferasi> Sebukan sel-sel radang > Nekrosis fibrinoid dinding kapiler> Penebalan membrane basalis
Etiologi :* Sindroma neprotik primer ok. Glomerulopati* Sindroma neprotik secunder akibat :
- Penyakit-penyakit sistemik misalnya : DM. Amiloidosis,lupus, Hodgkin, dsb
- Gangguan sirkulasi darah trombosis vena renalis D.C- Keracunan : logam berat, obat-obatan, gigitan ular,
lebah- Infeksi/parasit : sipilis,malaria- Genetik, familial
Patogenesis :
Perubahan pada membrane basalis kapiler glomerulusPermeabilitas protein dan albumin bertambah.

N E F R O S I S
Merupakan kelainan ginjal degeneratif yang terutama mengenai tubulus :
I.Acute Tubular Necrosis:
A. Nefrosis toksik- Nefrosis kimiawi- Nefrosis cholemik- Nefrosis osmotic- Nefrosis vakuoler
B. Nefrosis hipoksik
II. Nefrosis kronik

P Y E LO N E F R I T I S
Radang ginjal yang mengenai parenchyma dan pelvis.
Infeksi dari : > Hematogen dari Tonsilitis Septikemi> Ascenden dari kandung kemih , dll> Limfatik
Faktor – faktor predisposisi :- Obstruksi air kemih- Kehamilan- Instrument- Penyakit Syaraf, paraphelia, poliomielitis- D.M - Daya tahan turun
Klinis : - Demam tinggi- Nyeri diatas ginjal- Leukositosis

H I D R O N E F R I T I S
Terjadinya dilatasi pelvis renalis dan calyces, serta atrofi progresif dan pembentukan kistik ginjal disertai pelebaran ureter.
Etiologi Hidroneprosis :1. Obstruksi :
Ureter : batu , tumorDinding ureter : strikturaPenekenan dari luar : tumor, prostat hipertropi, fibrosis
2.Kelainan neuromuskuler : Paraplegi, sclerosis multiple, tabes dorsalis
3.Kehamilan4.Idiopatik
Klinis :Nyeri pinggang Teraba tumor pada sudut costo vertebral.Payah ginjalPyelonephritis

Makroskopis : - Kortex menipis dan atrofi- Ginjal membesar- Pelvis dan calyces melebar
Mikroskopis : - Dilatasi tubulus- Atrofi tubulus- Glomerulus atrofi & fibrosis
U R O L I T I A S I S
Adalah : pembentukan batu dalam saluran kemih dan penyakit yang berhubungan dengan adanya batu tersebut.
Faktor Predisposisi :> Konsentrasi kristaloid dalam urine> Lesi pada dinding tract.urinarius atau perubahan fisiokimiawi air kemih> Stasis urine

Misalnya : 1.Dehidrasi 2.Hiperkalsemia, hipercalciuria pada hiperparathyroid,
resopsi tulang, hipervitaminosis D, diet calcium meninggi, antasida. 3.Penyakit-penyakit gout 4.pH kurang dari 6 5.Defisiensi Vit. A 6.Infeksi kuman, parasit
Klinis :Ulserasi dan perdarahanColic ginjal / ureterPyelonephritis, cystitisHidronephrosisCarcinoma

Jenis2 Batu Sqaluran Kemih

Broad classificationBroad classification
Calcium containing stonesCalcium containing stones 75%75% RadiopaqueRadiopaque
Non calcium containing stonesNon calcium containing stones 25%25% RadiolucentRadiolucent Not cystine stones are radiopaque (sulphur)Not cystine stones are radiopaque (sulphur)


Age
Gender
Season/climate
Fluid Intake
Stress/diet
Occupation
Mobility
Metabolic disorders
Genetic disorders
Anatomical abnormality
Family history
Risk Factors for Calcium Stone-Formation

Occupation, Low Urine Volume and Urolithiasis
Occupation Percent of Male Stone-Formers
Urine Volume
(litre/day) Taxi-Drivers, Chauffeurs
5.6
1.42 0.27
Chefs, Kitchen-Workers
6.3
1.31 0.34

Urinary Risk Factors for Stone-Formation
• Low urine volume (<1L/24hrs)
• Alteration in urinary pH (<5.5,>7.5)
• Hypercalciuria (>4mg/kg/24hrs)
• Hyperoxaluria (45mg/24hrs)
• Hyperuricosuria (>600mg/24hrs)
• Hypocitraturia (<250mg/24hrs)
• Hypomagnesiuria (<50mg/24hrs)
T U M O R G I N J A LJinak : Adenoma
FibromaMyxoma ,dsb
1.Karsinoma sel ginjal1.Karsinoma sel ginjal (Renal Cell Ca : tumor Grawitz, hypernephroma, clear cell carcinoma)
berasal dari epitel tubulus
Makros : - Massa besar, berlobus-lobus- Massa kuning- Sebagian bercapsul- Tampak daerah nekrosis dan perdarahan
Mikros : - Kelompokan sel-sel besar- Sel dengan sitoplasma jernih- Clear cell
Ganas : KarsinomaTumor WilmsFibrosarcoma,dsb
2. Tumor Wilms. Tumor Wilms : ( Nephroblastoma, Carcinoma ) Biasanya mengenai anak-anak.
Makros : Tumor putih kelabu seperti otak, lemakMikros : - Glomelurus abortive
- Stroma spindle

Signs and Symptoms
HematuriaHematuria FeverFever Weight lossWeight loss ErythrocytosisErythrocytosis
Liver dysfunctionLiver dysfunction HypercalcemiaHypercalcemia Incidental finding of Incidental finding of
lytic lesions on lytic lesions on routine chest x-rayroutine chest x-ray

RCC ( Renal Cell Carcinoma )

In 2003 31,900 new cases In 2003 31,900 new cases RCC were expected in the RCC were expected in the U.S., with 11,900 deaths U.S., with 11,900 deaths attributable to RCCattributable to RCC
Classic triad: flank pain, Classic triad: flank pain, hematuria, palpable masshematuria, palpable mass
Paraneoplastic syndromes: Paraneoplastic syndromes: erythrocytosis, erythrocytosis, hypercalcemiahypercalcemia

BackgroundBackground Higher incidence in cigarette smokersHigher incidence in cigarette smokers
Associated with Von Hippel Lindau disease, which is caused Associated with Von Hippel Lindau disease, which is caused by mutations in chromosome 3by mutations in chromosome 3
Frequently invades renal veins or IVC leading to hematogenous Frequently invades renal veins or IVC leading to hematogenous disseminationdissemination
Prognosis Prognosis (Young, et al 2003)(Young, et al 2003) UCLA researchers described a staging system based on UCLA researchers described a staging system based on TNM stageTNM stage, , histologic histologic
gradegrade, and , and performance statusperformance status
This system predicts the clinical outcome and survival for patients who had surgical This system predicts the clinical outcome and survival for patients who had surgical resection of their kidney tumorresection of their kidney tumor
Patients are assigned to low-, intermediate-, and high-risk groups based on these 3 Patients are assigned to low-, intermediate-, and high-risk groups based on these 3 variables variables

PrognosisPrognosis
5 year survival ranges (UCLA):5 year survival ranges (UCLA):
Nonmetastatic / low-risk = 83.8%Nonmetastatic / low-risk = 83.8%
Nonmetastatic / high-risk = 44%Nonmetastatic / high-risk = 44%
Metastatic / high-risk = 0%Metastatic / high-risk = 0%

Prognosis Prognosis (Rathmell 2004)(Rathmell 2004)
Patients with clear cell RCC had a poorer prognosis Patients with clear cell RCC had a poorer prognosis than those with either papillary or sarcomatoid RCCthan those with either papillary or sarcomatoid RCC
5-year survival rates:5-year survival rates: 68.9% clear cell68.9% clear cell 87.4% papillary87.4% papillary 86.7% sarcomatoid86.7% sarcomatoid
Currently researchers are trying to identify Rx for each Currently researchers are trying to identify Rx for each specific subtype of RCC, since the underlying genetic specific subtype of RCC, since the underlying genetic changes are unique to each subtypechanges are unique to each subtype

StagingStaging TxTx Primary tumor cannot be assessed.Primary tumor cannot be assessed.
TCTC No evidence of primary tumor.No evidence of primary tumor.
T1T1 Tumor less than 7 cms in greatest dimension Tumor less than 7 cms in greatest dimension limited to limited to the kidney.the kidney.
T2T2 Tumor more than 7 cms in greatest dimension Tumor more than 7 cms in greatest dimension limited to limited to the kidney.the kidney.
T3T3 Tumor extends into major veins or invades Tumor extends into major veins or invades adrenal adrenal gland or perinephric tissue but not gland or perinephric tissue but not beyond Greota’s fascia.beyond Greota’s fascia.
Criteria for NephrectomyCriteria for Nephrectomy
> 75% tumor debulking possible> 75% tumor debulking possible
No CNS, liver, or bone metsNo CNS, liver, or bone mets
Adequate pulmonary and cardiac functionAdequate pulmonary and cardiac function
Good performance statusGood performance status
Biopsy with clear cell typeBiopsy with clear cell type

Wilm’sTumor

Wilm’sTumor


K A N D U N G K E M I HK A N D U N G K E M I H
Radang = Cystitis
Faktor Predisposisi : - Obstruksi air kemih- Trauma instrument- Pyelonephritis- Batu vesica urinaria- Cystocele- D.M- Septikhemia
Klinis :Pollakisuria, Dysuria, Nyeri supra pubis, Gejala sis- temik : demam,dsb
Tumor Jinak : PapillomaTumor Ganas : Karsinoma (terutama jenis transtitional)
Karsinoma Skuamous



Blader Neck Obstruction
O.K.Penyempitan muara uretha : * Hipertrofi prostate* Karsinoma* Fibrosis ok.cystitis chronica* Benda asing
Batu kandung kemih :- Primer- Sekunder
Faktor predisposisi :> Retensi urine> Infeksi bakteri> Benda asing> Vit. A defisensi
Neurogenic Bladder : Kandungan kemih yang kehilangan fungsinya akibat terputusnya persyarafan
Gejala : > Inkontinensia urine> Autonomic neurogenic bladder : keluarnya urine karena
kandung kemih telah penuh.

BLADDER CANCERBLADDER CANCER
IncidenceIncidence
There are approximately 55,000 new cases of bladder, ureter and renal
pelvis cancers in the United States with approximately over 13,000
deaths each year.
EpidemiologEpidemiologyy
GenderGender Men have more incidence of bladder cancer than women and increased Men have more incidence of bladder cancer than women and increased
incidence in 7incidence in 7thth decade of life. decade of life.
RaceRace Cancers are more common in whites than blacks – 2:1.Cancers are more common in whites than blacks – 2:1.

Etiology and Risk FactorsEtiology and Risk Factors
Cigarette smokingCigarette smoking Analgesic abuseAnalgesic abuse
Analgesic compounds, especially Phenacetin, has been Analgesic compounds, especially Phenacetin, has been associated with increased risk of bladder cancerassociated with increased risk of bladder cancer
Chronic urinary inflammationChronic urinary inflammation Occupational exposuresOccupational exposures
Workers with organic chemicals, rubber, paint, and dye Workers with organic chemicals, rubber, paint, and dye industries have increased risks of urothelial cancers.industries have increased risks of urothelial cancers.
Balkan nephropathyBalkan nephropathy Increase of cancer with renal pelvis and ureters in patients in Increase of cancer with renal pelvis and ureters in patients in
Balkan nephropathy, unknown cause that results in Balkan nephropathy, unknown cause that results in progressive inflammation of the renal parenchymaprogressive inflammation of the renal parenchyma
Genetic factorsGenetic factors Families with higher risk of transitional cell carcinoma, no Families with higher risk of transitional cell carcinoma, no
genetic basis has been found as of yetgenetic basis has been found as of yet

Signs and SymptomsSigns and Symptoms
HematuriaHematuria Urinary voiding symptomsUrinary voiding symptoms Symptoms of advanced disease usually involve swelling in lower Symptoms of advanced disease usually involve swelling in lower
extremities secondary to a lymphatic obstructionextremities secondary to a lymphatic obstruction Pain and frank hematuriaPain and frank hematuria
Diagnostic Work-upDiagnostic Work-up
CT scanCT scan UltrasoundUltrasound Intravenous pyelogramIntravenous pyelogram Urine cytology from both ureters at time of cystoscopyUrine cytology from both ureters at time of cystoscopy Bone scanBone scan Chest x-rayChest x-ray

PathologyPathology
Transitional cell carcinoma constitutes 90-95% of Transitional cell carcinoma constitutes 90-95% of bladder, ureter and renal pelvis cancers.bladder, ureter and renal pelvis cancers.
Squamous cell carcinoma up to 7%Squamous cell carcinoma up to 7%
Adenocarcinoma, rare, less than 3%Adenocarcinoma, rare, less than 3% Adenocarcinoma in the bladder which arises from the dome is Adenocarcinoma in the bladder which arises from the dome is
felt to be urachal in origin.felt to be urachal in origin.
Carcinoma in situ 30% of newly diagnosed bladder Carcinoma in situ 30% of newly diagnosed bladder cancer with multiple sites of bladder involvementcancer with multiple sites of bladder involvement

TNM StagingTNM Staging
TXTX Definition – Primary tumor cannot be Definition – Primary tumor cannot be assessedassessed
T10T10 No evidence of primary tumorNo evidence of primary tumor
TATA Noninvasive papillary tumorNoninvasive papillary tumor
TisTis Carcinoma in situ flat tumorCarcinoma in situ flat tumor
T1 T1 Tumor in wedgeTumor in wedge Subepithelial connective tissueSubepithelial connective tissue
T2 T2 Tumor in wedge muscleTumor in wedge muscle T2a tumor in wedge, superficial T2a tumor in wedge, superficial muscle, inner halfmuscle, inner half T2a tumor in wedge, deepT2a tumor in wedge, deep
muscle, outer halfmuscle, outer half

Prognostic FactorPrognostic Factor
Lesions up to T1, especially TA, without carcinoma in situ have 95% survival Lesions up to T1, especially TA, without carcinoma in situ have 95% survival rate whereas those with high grade T1 lesion have a 10-year survival rate of rate whereas those with high grade T1 lesion have a 10-year survival rate of 50%.50%.
Muscle invasive carcinoma 5-year survival rates are 20-50%. With regional Muscle invasive carcinoma 5-year survival rates are 20-50%. With regional lymph node involvement 5-year survival rate is 0-20%.lymph node involvement 5-year survival rate is 0-20%.



























