Embed Size (px)
Citation preview

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 1/26
1
HEALTH WORKERS’OPERATIONS MANUAL
_______________________________________________________________
I N T E G R A T E D D I S E A S E S U R V E I L L A N C E
M I N I S T R Y O F H E A L T H A N D F A M I L Y W E L F A R E

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 2/26
2
INDEX
Sl. No Topic Pagenumber
Abbreviations 31.0 Introduction 4
1.1 What is surveillance? ……………………………......................... 41.2 Why surveillance? ………………………………......................... 4
2.0 Integrated Disease Surveillance Project 52.1 Syndromes under surveillance ……………………………........... 52.2 Types of surveillance under IDSP ………………......................... 62.3 Which are the reporting units? ……………………………........... 7
3.0 Data Collection .................................. 74.0 Flow of Information ........................... 85.0 Laboratory Confirmation ............... 9
5.1 Biosafety ……..………………………............................................ 106.0 Outbreak Response .......................... 107.0 Inter-sectoral Collaboration ............. 108.0 Conclusion ..................,...................... 10
Annexure I: Syndromes Under Surveillance ........ 12I. Syndrome of Fever …………………………………………………. 12
II. Syndrome of Cough (with or without fever) ...……………………. 16III. Syndrome of Watery Diarrhoea ...…………………………………. 18IV. Syndrome of Jaundice ……………………………………………… 22V. Syndrome of Unusual Events Causing Death or Hospitalization 25
Glossary of terms 27

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 3/26
3
ABBREVIATIONS
AFP Acute Flaccid Paralysis ARI Acute Respiratory InfectionBDO Block Development Officer CDC Centers for Disease Control and Prevention
CEO Chief Education Officer CFR Case Fatality RatioCHC Community Health Center DH District HospitalDSU District Surveillance UnitESI Employee State InsuranceIDSP Integrated Disease Surveillance ProjectIEC Information Education CommunicationJE Japanese EncephalitisMO Medical Officer MP Malarial ParasiteNGO Non Governmental OrganizationOPD Out Patients DepartmentORI Outbreak response immunizationORS Oral Rehydration SaltsORT Oral Rehydration TherapyOT OrthotoludinePHC Primary Health Center RRT Rapid Response TeamRT Radical TreatmentSPP Sentinel Private Practitioner TB Tuberculosis
This manual is intended for the use of the most peripheral workers in the healthsystem, both in the Government and Private sector. It should help them identifycases, alert the higher authorities and take action within the limits of their capacity.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 4/26
4
1.0 Introduction
1.1 What is surveillance?Surveillance is collecting data on disease conditions so that necessary action can betaken. Action may be in the form of improvement of services when gaps areidentified or outbreak response when an outbreak is detected. The key output of a
good surveillance system is the early detection of outbreaks. The six main steps insurveillance are:
• Detection and notification of health event;
• Collection of data;
• Investigation and confirmation (Epidemiological, clinical, laboratory);
• Analysis and interpretation of data;
• Response – a link to public health program specially actions for preventionand control; and
• Feed back and dissemination of results.
1.2 Why surveillance?
Surveillance is an important component of public health measures. Surveillancehelps the health services keep a close watch on health events occurring in thecommunity and detect outbreaks that may be occurring so that corrective action canbe taken immediately. By preventing outbreaks, the credibility of the health servicesis greatly improved.
2.0 Integrated Disease Surveillance Project
Integrated Disease Surveillance Project (IDSP) is a decentralized, state basedsurveillance programme in the country. It is intended to detect early warning signalsof impending outbreaks and help initiate an effective response in a timely manner. It
is also expected to provide essential data to monitor progress of on-going diseasecontrol programmes and help allocate health resources more efficiently.
All outbreaks cannot be predicted or prevented. However, precautionary measurescan be taken within the existing health infrastructure and service delivery to reducerisks of outbreaks and to minimize the scale of the outbreak if it occurs. Theeffectiveness with which national programs are implemented and monitored, thealertness for identification of early warning signals and the capacity for initiatingrecommended specific interventions in a timely manner are important to achieve theabove objectives.
The course of an epidemic is dependent on how early the outbreak is identified and
how effectively specific control measures are applied. The epidemiological impact of the outbreak control measures can be expected to be significant only if thesemeasures are applied in time. Scarce resources are often wasted in undertakingsuch measures after the outbreak has already peaked and the outcome of suchmeasures in limiting the spread of the outbreak, and in reducing the number of casesand deaths, is negligible.
When outbreaks occur or when the risk of such outbreaks his high, the co-operationof other government departments, non-governmental agencies and the community

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 5/26
5
often becomes necessary. Such help will be more forthcoming if mechanisms for interactions have been developed before the onset of an outbreak.
The frequency of the occurrence of epidemics is an indication of the inadequacy of the surveillance system and preparedness to identify and control outbreaks in atimely manner.
The Integrated Disease Surveillance system will be operational all over the countryand will help the health services to improve the alertness of the health services topotential outbreaks. The main components in this surveillance system would be: 1)surveillance of diseases; capacity building of health staff at various levels;strengthening of laboratories; provision of computers at the District Surveillance Unitto enable rapid transmission of surveillance data; and partnership with private healthsector. There are many surveillance systems currently in the country. Efforts will bemade under IDSP to converge surveillance under various national disease programsin to a single surveillance system under IDSP.
2.1 Syndromes under Surveillance:
The paramedical health staff will undertake disease surveillance based on broadcategories of clinical presentation. The following clinical syndromes will be under surveillance in IDSP:
1. Fever i. Less than seven days duration without any localizing signsii. With Rashiii. With altered sensorium or convulsionsiv. Bleeding from skin or mucus membranev. Fever more than seven days with or without localizing signs
2. Cough more than three weeks duration3. Acute Flaccid Paralysis4. Diarrhoea5. Jaundice6. Unusual Events causing death or hospitalization
These syndromes are intended to pick up all priority diseases listed under regular surveillance at the level of the community under IDSP.
1. Fever with or without localising signs Malaria, Typhoid, JapaneseEncephalitis, Dengue, Measles
2. Cough more than 3 weeks Tuberculosis
3. Acute Flaccid Paralysis Polio
4. Diarrhoea Cholera
5. Jaundice Hepatitis, Leptospirosis
6. Unusual events causing death Plague, emerging diseases, Viralor hospitalization outbreaks

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 6/26
6
2.2 Types of surveillance under IDSP:
Depending on the level of expertise of the health staff, disease surveillance under IDSP will be of the following three categories.
Syndromic: Diagnosis made on the basis of history and clinical pattern by
paramedical personnel and/or members of the community.Presumptive: Diagnosis made on typical history and clinical examination by medical
officers.Confirmed: Clinical diagnosis confirmed by an appropriate laboratory test.
Syndromic surveillance is defined as the surveillance of diseases based on thepresenting symptom/s (and not the disease attributable to the syndrome). Under IDSP, the Health Workers, Village Volunteers and Non-formal Practitioners willconduct syndromic surveillance. The cases identified through the presentingsymptoms are classified as ‘suspect cases’ of a certain disease condition. For e.g. acase of fever with rash will be classified under the syndrome ‘fever with rash’ and notas measles. The medical diagnosis of a condition, based on presenting symptoms
and clinical signs will be conducted only at the level of Medical Officers (such asthose at Primary, Community Health Centers, Dispensaries and Hospitals) or qualified medical practitioners.
Symptoms, signs and syndromeSymptom is complaint perceived by the patient or identified by the examiner (e.g.
fever, loose motions, headache, vomiting, cough etc.)
Signs are findings on examination of patients e.g. skin rash, yellow discoloration(jaundice).
Syndrome is group of symptoms and/or signs attributable to particular disease
condition (e.g. fever with skin rash indicative of measles).

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 7/26
7
2.3 Which are the reporting units?
A reporting unit is one that generates the data and feeds it into the surveillancesystem. The Health Workers are the most peripheral workers at the subcentres andare the primary reporting units in the surveillance system. Village volunteers from thePanchayat, local private practitioners (including practitioners of Indian Systems of Medicine) and non-formal health providers may be incorporated as reporting units for
syndromic surveillance, after proper training.
Reporting units for disease surveillancePublic health sector Private health sector
Rural Sub-centers, PHCs, CHCs, DistrictHospitals
Sentinel Privatepractitioners (SPPs) andSentinel hospitals.
UrbanUrban Hospitals, ESI / Railway /Medical college hospitals
Sentinel Private nursinghomes, sentinelhospitals, Medicalcolleges, Private and
NGO laboratories
3.0 Data collection
The health workers are the most important personnel for syndromic surveillance. Thereporting units are the sub-centers of PHC and urban health centers. The peripheralhealth workers will be provided a register in which they will note down the syndromesthat are under surveillance as and when they come to know of this during their routine visits to the village and urban wards. The register will contain the verifiableinformation which can be counter-checked by the supervisory staff under IDSP atPHC/CHC and District levels. The health worker would be expected to record the
number of these syndromes seen by her/him each week and report it to the nextlevel on a weekly basis.
Every Monday, this information will be translated into a summary sheet (form S) andgiven to the Medical officer in charge of the PHC / Urban Health Center. This will beimmediately forwarded to the District Surveillance Officer. The reports from theUrban Health Center will be forwarded to the Municipal Health Officer. The MunicipalHealth Officer will then forward the reports to the District Surveillance Officer.
4.0 Flow of information:
The health workers (and other peripheral reporting units such as the village volunteer
and non-formal provider) should register all patients seen by them (either at theSubcentre or during home visits) into their register for syndromic surveillance. On aweekly basis, this information has to be transferred onto the suspect case reportingformat (Form S). The health worker, village volunteer or other providers will submitform S to the PHC Medical Officer every Monday. If there are Sentinel PrivatePractitioners in his/her area who form a part of the reporting system, the HW shouldcollect the reports from them and submit it to the PHC (without delay in sending thesubcenter report to the PHC). The MO PHC will retain one copy of the form S and

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 8/26
8
forward the remaining copy to the District Surveillance Officer immediately onMonday or latest by Tuesday. The data from the periphery that will be provided tothe PHC will be used for action.
Other than patients coming to the subcenter, the HW may also hear about cases inthe community from key informants. The HW must verify these cases before
reporting.
Transmission of data
Once the data is collated, and entered into the reporting form, then the HW shouldensure that the form S reaches the PHC every Monday. This may be done either manually or by telephone where possible.If there are Sentinel Private Practitioners in a subcentre area, it is the responsibilityof the HW to collect the form S from them and forward them to the PHC. However, inthe process of collecting the forms from them, the HW should ensure that his/her forms do not get delayed in reaching the MO PHC.
Feedback
If the HW has referred patients for further investigation, she should find out from theMedical Officer at the PHC about the outcome of the referral. If the HW has receivedinformation about cases from key informants, she should share her diagnosis andaction with them.
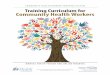
Weekly Information Flow under IDSP
Sub-Centres
P.H.C.s
C.H.C.s
Dist.Hosp.
Programme
Officers
Pvt. PractionersD.S.U.
P.H.LabOther Hospitals:ESI, Municipal
Rly., Army etc.
S.S.U.
C.S.U.
Nursing Homes
Private Labs.
Corporate
Hospitals
Med.Col.Private Hospitals

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 9/26
9
5.0 Laboratory confirmation
While the HW is expected to see and report cases, he/she is also required to sendspecimens of cases presenting certain symptoms to the laboratory for confirmation.The table below summarizes the types of samples to be sent to the laboratory aspart of routine surveillance activity and as a part of outbreak response.
Table 5.1: Action to be taken by the HW in the field
Syndrome Action
Only Fever Blood Smear for all patients
Acute Flaccid Paralysis
Inform PHC MO immediately to arrange for collection of stool samplesTwo samples of stools taken at interval of 24hours and transported to the MO PHC in reversecold chain
Loose watery stools withdehydration in an adult
Take sample of stools in a filter paper or in a
sterile bottle and send it by reverse cold chain tothe nearest District Laboratory (within two hours)or use Cary-Blair medium for transport of thesample
Fever with rashFever with alteredsensorium
Fever with bleeding
Fever more than 7 days
Cough for more than threeweeks
Unusual severe
syndromes
Referred to the MO PHC for specific lab action
5.1 Biosafety measures
The HW must follow precautionary measures while collecting samples from at theperiphery. This must be supervised by the MP PHC or the laboratory technician atthe PHCs.
Col lect ion
1. Blood samples – Use disposable syringe/needles2. Discard used needles into sharp boxes3. Decontaminate used syringes by immersing in 10% bleach; autoclaving and
then discarding. Recommended to use autodestruct syringes.4. In case of spills – wipe the surface with 10% bleach.
Transpor tat ion
1. Transportation boxes should be securely fastened. Keep absorbent cottoninside the carrier.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 10/26
10
2. If cold chain is required, ensure that there are ice packs. Loose wet ice shouldnot be used. Do not re-use the same cold chain box to transport vaccines.
6.0 Outbreak response
The role of the HW is not simply to collect and transmit data. She/he should also bealert to outbreaks so that they can be detected early and an effective response canbe taken. Thresholds for outbreaks are given in annexure I (page 11). Once adisease condition has crossed this threshold, the HW must take the appropriateaction which is specified in the annexure I (page 11). In the case of fever or AFP, theHW should also take the responsibility of collecting the appropriate sample. Presettrigger levels for diseases have been identified with specific responses for variouslevels of the health system. The trigger levels are dependent on theoutbreak/epidemic potential, case fatality rate of the disease and the prevalence of the problem in the community.
7.0 Inter-sectoral coordination
For an effective outbreak response it is important to involve members of thecommunity and members of non-health departments/sectors. Therefore, the healthworker as a part of the outbreak response will inform the Panchayat office and thelocally active NGOs regarding possible outbreaks in the community (if any).
8.0 Conclusion
The HW is the eye and the ear and the most important personal of the HealthServices and plays a very crucial part in the early detection of outbreaks in the
community. If the HW works sincerely on surveillance, many outbreaks in thecommunity can be prevented which, will improve the credibility of his/her services.
Other than the HW’s own services, he/she should attempt to identify and buildrapport with key informants in each village who will inform him/her of the healthevents as and when they occur. These community based informants would improvethe alertness of the surveillance system and should stimulate the health services toidentify and respond immediately to potential outbreaks.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 11/26
11
Annexure I: Syndromes under surveillance
I. Syndrome of Fever
Diseases under Surveillance: Malaria/ Typhoid / Measles / Japanese Encephalitis(JE) / Dengue
I.a Why surveillance for fever?
Fever is the most common presenting symptom among patients at the periphery.The disease conditions of public health interest are Malaria, Typhoid, Measles, JEand Dengue. While the last two are not common, the HW needs to keep them under surveillance so that they are picked up early to identify impending outbreaks.
I.b Syndrome Definition
All new patients with fever should be classified as follows:
a) Fever less than seven days with:
Ø Rash and running nose or conjunctivitis (suspected Measles)Ø Altered sensorium (suspected JE)Ø Convulsions (suspected JE)Ø Bleeding from skin, mucus membrane, vomiting blood or passing
fresh blood through nose or ear or black motion (suspecteddengue)
Ø With none of the above (suspected malaria)
b) Fever more than seven days (suspected typhoid)
Trigger 1 : More than two cases with similar symptoms (as mentioned above) in
the village (1000 Population)Note: While there may be other accompanying symptoms e.g. fever withcough, fever with muscle pain, a patient is considered to be suffering fromfever, if his/her main symptom is that of fever.
I.c Recording information at reporting unit
Whenever the staff in the reporting unit sees a patient with fever, they should recordit in their register for syndromic surveillance. This includes simple details such asname, age, sex, address, the syndrome and date of onset. This would includepatients who come to the reporting unit or as seen during their field visits. Whileentering the diagnosis for fever, care must be taken to record it as one of the
following categories:• Only fever
• Fever with rash
• Fever with altered consciousness or convulsions
• Fever with bleeding
• Fever more than 7 daysThese registers for syndromic surveillance are the source of data from which theSyndromic Reporting Form (form S) will be filled by the HW on a weekly basis.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 12/26
12
I.d Analysis
The HWs should do a preliminary analysis of their data. If the threshold is crossed,then the HW should immediately take the necessary action.
Thresholds –
• Sudden/gradual increase in the number of cases of fever over thepast three weeks
• Two or more cases of fever with rash in one week
• Two or more cases of fever with altered consciousness or convulsions
• Two or more cases of fever with bleeding
• Two or more cases of fever more than seven days

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 13/26
13
I.f Detailed Surveillance Action:
Syndrome Trigger event (in a vil lage or urbanward for 1000 population approx)
Recommended Surveillance Actions Lab action
A) Fever less than 7days duration
a) Only fever 2 or more cases 1. Slides for MP2. Presumptive / RT for malaria
3. Inform MO PHC.4. IEC for community awareness*
Slides for MP
b) With rash 2 or more similar cases 1. Give vitamin A2. Give paracetamol.3. Check measles immunisation status
of cases4. Search for similar cases5. Refer the case to PHC6. Inform MO PHC7. Strengthen routine measles
immunization services, includingVitamin A
None
c) Alteredconsciousness or convulsions
2 or more similar cases 1. Collect slide for MP.2. Antipyretics3. Refer the case to CHC/District
Hospital4. Inform MO PHC5. Vector surveillance6. IEC for community awareness*
Slides for MP
*Regarding mosquito breeding sites, anti-larval measures and personal protection from mosquito bites (such as use of bed-nets)

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 14/26
14
d) Fever with bleeding 2 or more similar cases 1. Collect slide for MP.2. Paracetamol3. Refer the case to CHC/DH4. Inform MO PHC5. Vector surveillance6. IEC for community awareness
Slides for MP
Syndrome Trigger event (in a vil lage or urban
ward for 1000 population)
Recommended Surveillance Actions Lab action
B. Fever more than 7days
2 or more similar 1. Collect slide for MP.2. Give paracetamol.3. Give anti malarial treatment4. Inform MO PHC.
Once typhoid fever is confirmed1. Orthotoludine testing of drinking
water sources to check for residualchlorine level.
2. Collect water sample and send it toPHC for H2S testing and to districtlabs for MPN count.
3. Check TCL stock.4. Conduct appropriate chlorination of
all drinking water sources5. IEC - Train local person about water
Chlorination / Communityawareness about safe water andpersonal hygiene.
Slides for MP
CONCLUSION
Remember that increasing cases of fever in the community could be the initial signs of an outbreak of malaria or dengue. So be alertto the trends. The main focus should be to pick up warning signals of outbreaks at an early stage before it spreads.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 15/26
15
II. Syndrome of Cough (with or without fever)
Diseases under Surveillance: Tuberculosis / Acute Respiratory Infections
II.a Why surveillance of cough?
Cough is a common symptom, especially among children. There are many causes of cough, ranging from the common upper respiratory tract infection to cancer of thelung. However, Tuberculosis and Acute Respiratory Infections among children are themajor public health problems. Thus the symptom of cough is divided into two broadcategories: 1) Short duration cough (less than three weeks); and, 2) Long durationcough (more than three weeks). Adults (more than or equal to five years) with coughfor more than three weeks should be suspected to be suffering from TB, while children(less than five years) with cough less than three weeks should be suspected to besuffering from ARI.
II.b Syndrome definition:
All new patients with cough as the main presenting symptom should be included.These Patients will be divided into two categories:
a) Short duration cough (Cough less than 3 weeks) - Suspect ARI (commonamong children less than five years)
b) Long duration cough (Cough of more than or equal to 3 weeks) - SuspectTuberculosisNote: While there may be other accompanying symptoms e.g. fever andbreathlessness, a patient is considered as one suffering from cough, if his/her main symptom is that of cough.
II.c Recording at Reporting Unit
Whenever the HW sees a patient with cough during the field visits or at the subcenter, he/she should record it in the register for syndromic surveillance. This shouldinclude simple details such as name, age, sex, address, syndrome and date of onset.While entering the diagnosis for cough, care must taken to record it as either shortduration cough or long duration cough (as mentioned above).These register for syndromic surveillance is the source of data from which theSyndromic Reporting Form S is filled by the HW on a weekly basis.
II.d Analysis and action
The HW should do a preliminary analysis of their data. If the threshold is crossed, thenshe should take the necessary action.
THRESHOLD(increase in number of cases during last 3 weeks) RESPONSE
Cough less than 3 weeks duration Alert the Medical Officer about apotential outbreak
Cough more than 3 weeks duration Refer the patient to the Medical officerfor further investigation.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 16/26
16
II.e ConclusionRemember that increasing cases of cough in the community may be the initial signs
of a measles outbreak or an outbreak of whooping cough. So be alert to trends. Alsotry and pick up suspect TB cases as early as possible before they transmit theinfection to others.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 17/26
17
III. Syndrome of Watery Diarrhoea
Diseases under surveillance – Acute Diarrhoeal Diseases, cholera
III.a Why surveillance for Diarrhoea?
Diarrhoea is one of the most common symptoms faced by health workers at the periphery. Ithas a high death rate, especially among children. While sporadic cases are not alarming fromthe public health point of view, there is a danger of diarrhoea attaining outbreak situation in ashort period of time, especially in areas where sanitation is poor. Thus it is important to keep astrict vigil on the cases of diarrhoea – to check whether they are increasing in number or whether there are deaths occurring due to diarrhoea in the community. Deaths due todiarrhoea and dehydration in adults (> 5 years) should alert the health workers about thepossibility of cholera and appropriate action should be taken as given below. Outbreaks of diarrhoea reflect poorly on the effectiveness of the health services. Preventing diarrhoealoutbreaks will improve the image of the health services and the health workers in theperiphery.
III.b Syndrome Definition
Syndrome of Acute Diarrhoeal Diseases:
Any new case of watery diarrhoea (passage of even one large profuse watery stoolsin the past 24 hours) with or without dehydration. The total duration of illness shouldbe less than 14 days.
Trigger : 1) More than 10 houses with at least one case of diarrhoea each in a village
or urban ward within a week; or 2) Single case of severe dehydration or death in apatient more than or equal to 5 years with diarrhoea; or 3) A single death due tosevere dehydration following diarrhoea.
III.c Reporting Details As the main aim of surveillance is to detect potential outbreak situations, and cases of cholera is one of them, all diarrhea cases would be divided into two categories –diarrhea with dehydration and diarrhoea without dehydration. They would be further divided into less than five years of age and equal to or more than five years of ageand by sex (male and female).Those cases of diarrhoea which last more than seven days should be labeled aschronic diarrhea (for surveillance purposes).Whenever the Health Worker sees a patient with diarrhea during field visit or at thesubcenter, they should record it in their register for syndromic surveillance. Thisshould include simple details such as name, age, sex, address, syndrome and date of onset. This would include patients who come to the reporting unit or as seen during
their field visits. While entering the diagnosis for diarrhea, care must taken to record itas one of the following categories.
• Acute diarrhea with dehydration
• Acute diarrhea without dehydration
The register for syndromic surveillance is the source of data from which theSyndromic Reporting Form S is filled by the HW on a weekly basis.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 18/26
18
III.d AnalysisThe HWs should do a preliminary analysis of their data. If the threshold is crossed,then she/he should take the necessary action.
Thresholds –
• A single case of severe dehydration / death in a patient of more than or
equal to 5 years of age• More than 10 houses with at least one case of diarrhoea each in a village or
urban ward within a week.
III.e Response
Depending on the threshold, the HW should take the following action:THRESHOLD ACTION/RESPONSE
A single case of diarrhoea with severedehydration / death of a patient who ismore than 5 years old with diarrhea
More than 10 houses having at least
one case of diarrhea each in a villageor urban ward within a week.
Distribute ORS to the cases includingother vulnerable families
Refer cases with severe dehydration tothe nearest PHC
Search for more diarrhoea cases in thecommunity and prepare line listing of cases
Alert the MO PHC immediately.(Details of Action/Response – Refer toIII.g)
III.f ConclusionRemember that diarrhoea can spread very rapidly in a short time. Appearance of
diarrhoea cases should be is a warning signal of a potential outbreak.
III.g Annexure
i) Case management:
Rehydration therapy is the key treatment for diarrhoea. This is in the form of OralRehydration Therapy.Diarrhoea with dehydration
• 75 ml / kg of ORS in the first 4 hours.
• Reassess dehydration
• If same – continue for another 4 hours
• If rehydrated, ORS – 100 ml/kg/day• If worsened or increased – Refer to PHC/CHC.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 19/26
19
ii) Epidemiological investigationo Active search for all new cases in that area.o Line listing of cases.o Information to MO PHC / CHC
iii) Collection of lab specimens
o Collect stool specimens and send to PHC for Cholera isolationo Water samples for bacteriological analysis
iv) Prevention of further cases / deaths
o Provision of safe drinking water by disinfection of drinking water sourceso IEC to promote food and personal hygienic measureso Distribution of ORS packets to the vulnerable families.o Refers cases of dehydration to the PHCo Intimate the local practitioners about the probable outbreak
v) Safe drinking water: In an outbreak of cholera, providing safe drinking water is themost accepted method of control. This would include:
•
Immediate provision of safe drinking water - steps must be taken to provideproperly treated or other wise safe water to the community for all purposes(drinking and cooking).
• Chlorine tablets may be distributed to all households so that they maychlorinate their drinking water themselves.
• All water sources in the community should be chlorinated with bleachingpowder. Residual chlorine should be ensured before this water is used.
• Health education of the community to boil drinking water if feasible may beresorted to.
Provision of safe water is the responsibility of the department of water supply andshould be coordinated by the BDO / CEO / Collector. However, the health department
should be involved in this measure and should advise the water supply departmentabout the areas to be targeted.
vi) If diarrhoea outbreak occurs:
vi. a) Sanitary disposal of human waste: During an outbreak the community has to
be educated on the need for observing basic sanitary practices. These include
• IEC on food, personal and sanitary hygiene
• Use of sanitary toilets wherever possible
• Avoid defecation near water sources.
• Importance of washing of hands after defecating and before eating must be
emphasised.
vi. b) Food sanitation: Ensure proper hygiene and sanitatary precautions while
preparing and distributing food. Sale of food items must be strictly monitored and foodshould not be exposed to houseflies. The food must be freshly prepared and servedhot. Proper washing of hands by food handlers is essential for food safety. Discourageconsumption of cut fruits and raw vegetables like salads without thorough washingwith safe water.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 20/26
20
vi. c) Health Education: Health education is the most effective prophylactic measureand should be mainly directed at early reporting and prompt treatment, importance of safe water, hygienic food practices and personal hygiene.
vii) Stool Collection:
vii. a) Purpose:To confirm cases of cholera. So stools samples should be taken from adult patientswho have diarrhoea and severe dehydration. These should be transportedimmediately to the District laboratory for confirmation.
Vii. b) Procedure:
• Collection of specimens before the patient receives antibiotics
• In the event of an outbreak, collect from 5 – 10 patients.
• If stool is available, pour out /scoop specimen with spoon and fill upto the half thecontainer
• If stool is not available, introduce the swab well into the rectum (2 – 4 cms deep)and rotate by 90*. Ensure that it is moist and fecally stained.
• Put specimen / swab into the Cary-Blair transport medium which has beenpreviously cooled for one hour. This specimen then should be sent to the nearestlab as soon as possible. Vibrio cholera can be isolated from the media if transported and plated within 7 days. While cold chain is not necessary, it wouldbe advisable to store in a refrigerator and transport under reverse cold conditions.
• If C-B media is not available, then the specimen (or even filter paper soaked instool) can be placed in a sterile container and transported under reverse coldchain conditions (2* – 8* C). Ensure that the sample reaches the lab within 2hours.
• Put the containers in separate polythene bags to prevent leakage and crosscontamination.
• Label the samples. The label should contain theo Patient’s nameo Unique ID number o Specimen type, date, time and place of collection.o Name/ initials of collector.
Send the samples to the nearest District Lab. In the urban areas, the samples need tobe sent to the nearest designated lab that may be a Private lab

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 21/26
21
IV. Syndrome of Jaundice
Diseases Under Surveillance: Acute Viral Hepatitis A, Viral Hepatitis E and
Leptospirosis.
IV.a) Why surveillance for jaundice?
Jaundice is not a common symptom in the village level, but it has the potential for developing into an outbreak situation. There are many causes of Jaundice of whichHepatitis A and E virus and Hepatitis B virus and Leptospirosis are the diseases thatare of public health importance and may occur as outbreaks. To differentiate this typeof jaundice from others of lesser public health importance, surveillance will focus onlyon jaundice of less than four weeks duration.
IV.b) Syndrome Definition
Clinical Description:
A case with an acute illness (less than 4 weeks) and with the following symptoms:
• jaundice, dark urine,
• anorexia, malaise, extreme fatigue and
• pain in the right upper abdomen.
Trigger: More than two cases of Jaundice in different houses irrespective of age in a
village/urban ward or approximately 1000 population.
IV.c) Reporting detailsWhenever the HW sees a patient with jaundice during the field visits or at thesubcenter, they should record it in their register for syndromic surveillance. Thisshould include simple details such as name, age, sex, address, syndrome and date of onset. While entering the diagnosis for jaundice, care must taken to record it as one of
the following categories.• Jaundice of less than 4 weeks
• Jaundice of more than 4 weeks.
The register for syndromic surveillance is the source of data from which theSyndromic Reporting Form S is filled by the HW on a weekly basis.
IV.d) Analysis
The HWs should do a preliminary analysis of their data. If the threshold is crossed,then he/she should take the necessary action.
Thresholds –
• If there are more than 2 cases of jaundice in a village or an urban ward(approximately 1000 population) within a week.
• A single case of death due to acute jaundice (jaundice of less than 4weeks)

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 22/26
22
IV.e) ResponseDepending on the threshold, the MPW should take the following action:
Threshold Response
More than 2 cases of Jaundice indifferent households irrespective of age
per thousand population in a village or ward
A single case of death due to acute jaundice (jaundice of less than 4weeks)
Alert Medical Officer, PHC about apotential outbreak
Active search for more cases in thecommunity. Line listing of these casesby name, age, sex, location andsymptoms
Active search for pregnant women with jaundice, who should be referredimmediately to the district level.
NOTE: If an outbreak of Hepatitis A or E occurs, take all action listed under diarrhoea
outbreak.
IV.f Conclusion
Remember that jaundice is an uncommon but important problem in the community.Most community members prefer to treat jaundice with traditional medicines, so theydo not usually approach the allopathic system for treatment. Thus a single case of jaundice should alert the MPW about potential cases in the community and sheshould make efforts to trace them. While a single case may be of no public healthsignificance, multiple cases may indicate problems due to contaminated water supply.
IV.g Annexure
i) Safe drinking water: In an outbreak of jaundice, and if Hepatitis A or E is
suspected, providing safe drinking water is the most accepted method of control. Thiswould include:
• Immediate provision of safe drinking water - steps must be taken to provideproperly treated or other wise safe water to the community for all purposes(drinking and cooking). Chlorine tablets may be distributed to all households sothat they may chlorinate their drinking water themselves.
• All water sources in the community should be chlorinated with bleaching powder.Residual chlorine should be ensured before this water is used.
• Health education of the community to boil drinking water if feasible may beresorted to.
Provision of safe water is the responsibility of the dept of water supply and should beco-ordinated by the BDO / CEO / Collector. However, the health department should beinvolved in this measure and should advise the water supply department about theareas to be targetted.
ii) Sanitary disposal of human waste: During an outbreak the community has to be
educated on the need for observing basic sanitary practices. These include
• Using of sanitary toilets wherever possible

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 23/26
23
• If they resort to open-air defecating then they must be instructed to ensure thatthey are not next to a water source, that they cover the faeces with mud mixed withslaked lime.
• The importance of washing of hands after defecating must be emphasized.
• Washing of patient’s soiled linen and clothes should be done only after soakingthem in a solution of bleaching powder. Also washing should not be done with 10
m of a water source.
iii) Food sanitation: Steps should be taken to ensure proper hygiene and sanitationwhile preparing and distribution of food. Sale of food items must be strictly monitoredand food should not be exposed to houseflies. The food should be freshly preparedand served hot. Proper washing of hands by food handlers is essential for food safety.Sale of cut fruits and eating of raw vegetables like salads without thorough washingwith safe water should be discouraged.
iv) Health Education: Health education is the most effective prophylactic measure
and should be mainly directed at early reporting and prompt treatment, importance of safe water, hygienic food practices and personal hygiene.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 24/26
24
V. Syndrome of Unusual Events Causing Death or Hospitalization
V.a) Why surveillance of unusual syndromes?
While most common illnesses fit into the syndromic approach, the health workersshould be alert for uncommon events in the community also. Today is a period of bioterrorism and chemical warfare that pose a threat to the health of the community.So any unusual illness in the community causing either deaths or affecting largepopulations should be brought to the notice of higher authorities immediately.
V.b) Syndrome definition
Syndrome Description:
The sudden occurrence of unusual events, in a geographical region, causing death or hospitalization and which does not conform with the standard case/syndromedefinitions discussed earlier in the manual.
Some of the symptoms may be:
• Convulsions
•Alteration in consciousness
• Breathing Difficulty / Respiratory distress
• Bleeding
• Paralysis
Trigger: Two cases of death or hospitalisation due to an unusual symptom/s.
Examples given above.
V.c) Definitions
• Hospitalization and Death are self explanatory and do not require any specific
definition.
• Convulsion is defined for the syndrome as any patient admitted or diedfollowing involuntary muscular spasms with or without loss of consciousness.
• Altered Consciousness is defined as not able to recognize relatives and not
to be aware regarding time or place.
• Breathing Difficulty: When ever patients complain of severe breathlessness
associated with rapid respiration• Bleeding from skin, mucus membrane, vomiting blood or passing fresh blood
or black motion• Paralysis: Severe muscle weakness leading to difficulty in using any of the
limbs.
V.d) Reporting detailsWhenever the HW sees a patient with unusual syndromes during field visit or at thesubcenter, he/she should record it in the register for syndromic surveillance. Thisshould include simple details such as name, age, sex, address, syndrome and date of onset.
The register for syndromic surveillance is the source of data from which theSyndromic Reporting Form S is filled by the HW on a weekly basis.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 25/26
25
V.e) AnalysisThe HW should do a preliminary analysis of their data. If the threshold is crossed, thenhe/she should take the necessary action.
Thresholds –
• Two or more similar cases of unusual symptoms
Care should be taken to ensure as much as possible that it is a health event that isunusual. Some cases that may be confused as an unusual events are suicide,homicide, snake bites, unnoticed head injury etc.
V.f) Response
Depending on the threshold, the HW should take the following action:
Threshold Action
Two cases of death/hospitalization dueto unusual symptoms.
• Convulsions
• Alteration in consciousness
• Breathing Difficulty / Respiratory• Bleeding
• Paralysis
Refer the patients to the DistrictHospital immediately
Inform the MO of the PHC immediately
Active search for similar cases in thecommunity. If there are such cases,then line list them according to their age, sex, location, clinical details anddate of onset of symptoms and refer them to District Hospital.
V.g) Conclusion
Remember that unusual syndromes are the best way of picking up the presence of new agents in the community. This is the ultimate test of a surveillance system and all
levels of health workers should be alert to this. This also indicated effectivesurveillance in a given area.

7/28/2019 124545324 Health Workers Manual
http://slidepdf.com/reader/full/124545324-health-workers-manual 26/26
Glossary of terms
Non formal practitioner – This refers to the practitioners who are not medically
qualified but provide health care at the community level, especially in rural areas
Health Worker (M/F) – For consistency and convenience, all peripheral staff of the
health system such as Health Workers, Health Assistant, Health Supervisor, MultiPurpose Worker, Lady Health Visitor, Auxiliary Nurse Midwife, Anganwadi Workers,Village Volunteers, Non formal practitioners at the village level etc have been referredto as Health Worker (HW).
Trigger level – Under IDSP, a warning signal has been set under every disease to
identify a potential outbreak situation, which will serve as a trigger for action. Thiswarning signal is referred to as the trigger level. For e.g. a single case of measles is atrigger for a measles outbreak that should set into action, the control measures.
Outbreak/epidemic potential – It is the nature of diseases that are highly
communicable by virtue of their nature of transmission that makes them prone to
reach outbreak situations rapidly.
Key informants – These are members of the community that are knowledgeable
about the community, especially in rural areas, it’s composition, health problems etcand are capable of providing information to the HW regarding health events in thecommunity. Key informants could be panchayat members, school teachers or members of local NGOs, to list a few.
Threshold - Every disease needs a basic number of cases in order to sustain the
transmission to other vulnerables in the population. Also, when a disease reaches thisthreshold level, there is a risk of an outbreak of that disease.