Embed Size (px)
Citation preview

PART III
MANAGEMENT OFDISEASE RISK ANDWITH DIABETES
Downlo
CORONARY HEARTDISEASE IN PATIENTS
12 Effect of Lifestyle Interventions onCoronary Heart Disease Risk in Patients
with DiabetesBarry A. Franklin, Wendy M. Miller, and Tracy R. JuliaoWEIGHT MANAGEMENT ANDENERGY BALANCE, 140Dietary Intake and CardiometabolicRisk, 142
Smoking Cessation, 142
EXERCISE AND PHYSICAL ACTIVITYIN THE PREVENTION ANDTREATMENT OF TYPE 2 DIABETESMELLITUS, 143Walking: “Exercise Is Medicine” forPatients with Diabetes, 144
aded for Aman Shah (a.shah.1@elsevFor personal use only. N
Cardioprotective Effects of RegularExercise, 144
PHYSICAL ACTIVITY, EXERCISEPROGRAMMING, ANDPRESCRIPTION, 144Type of Exercise, 144The Structured Exercise
Session: Special Considerationsfor Exercisers withDiabetes, 148
ier.com) at Elsevier - Demonstration Account from ClinicalKeyo other uses without permission. Copyright ©2017. Elsevier Inc
PSYCHOSOCIAL INTERVENTIONSTO SUPPORT LIFESTYLECHANGE, 148Readiness for Change, 148Motivational Interviewing, 150Evidenced-Based Mind-Body
Therapies, 152
SUMMARY, 152
REFERENCES, 153
In the United States, the prevalence of high cholesterol,hypertension, and cigarette smoking together with age-adjusted cardiovascular deaths has declined over the lastseveral decades.1 On the other hand, the prevalence ofdiabetes has risen steadily, largely because of an epidemicof obesity and adiposity and our increasingly inactivelifestyle (see also Chapters 1 and 5).2 These trends will likelymitigate further reductions in cardiovascular mortality andeven reverse the decline in cardiovascular disease (CVD)incidence.3
Using 2010 as the baseline, the estimated direct andindirect costs of CVD are expected to triple by the year2030, making this a critical medical and societal issue.4,5
These sobering projections and other recent data6,7 suggestthat effective preventive strategies are needed if we areto limit the growing burden of CVD (see also Chapters 5and 6). The current reactive-based health care model, inwhich patients are seen when they become ill, typically dur-ing outpatient visits or hospitalizations, often fails to proac-tively improve health, because so many health outcomesare explained by individual behaviors and the lifestylechoices people make on a daily basis.6,8
Unfortunately, many patients as well as individuals in themedical community continue to rely on costly coronary
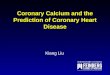
revascularization procedures and/or cardioprotective medi-cations as a first-line strategy to stabilize or favorably modifyestablished risk factors and the course of coronary heartdisease (CHD). However, these therapies do not addressthe root of the problem, that is, the most proximal risk factorsfor CHD, including poor dietary practices, physical inactivity,and cigarette smoking, as shown in Figure 12-1.3 Unhealthylifestyle habits strongly influence not only conventional riskfactors (e.g., blood pressure, lipid and lipoprotein levels,glucose-insulin homeostasis) but also novel or emerging riskfactors such as endothelial function, inflammation (e.g.,C-reactive protein), thrombosis and coagulation, arrhythmias,and other disease modulators (e.g., psychosocial stressors),3
even among users of lipid-lowering and antihypertensivemedications.9 Collectively, these data suggest it is time tochange our emphasis from disease management to diseaseprevention, focusing on the foundational causes of CVD byreengineering prevention into the U.S. health care system.7
This chapter emphasizes the role of lifestyle interventionsin the prevention and treatment of CVD in patients withdiabetes, with specific reference to weight managementand energy balance, dietary intake and cardiometabolicrisk, smoking cessation, exercise and physical activity,cardiorespiratory fitness, and research-based psychosocial
139.com by Elsevier on December 21, 2017.. All rights reserved.

Death
Early vascular disease
Inflammation
Coronarydisease
Abnormalheart
rhythms
Heartfailure Stroke
Diabetes Psychosocialstressors
Airpollution
Obesity Highcholesterol Hypertension
Poor dietary habits
Diseaseprogression
Clinicalendpoints
Establishedand novelrisk factors
Lifestylerisk factors
Physical inactivity Smoking
Cognitivedecline
FIGURE 12-1 Unhealthy lifestyle habits lead to coronary risk factors, the progression of cardiovascular disease, and ultimately adverse outcomes or clinical endpoints. Thus thefirst-line strategy to prevent coronary heart disease (or recurrent cardiac events) is to favorably modify poor lifestyle habits or practices, including suboptimal dietary habits, physicalinactivity, and cigarette smoking. (Modified from Mozaffarian D and colleagues.3)
140
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
interventions (e.g., readiness for changes, motivationalinterviewing, counseling strategies) to support cardioprotec-tive lifestyle change in this at-risk patient subset (see alsoChapter 5).
WEIGHT MANAGEMENT AND ENERGYBALANCE
Obesity is an independent risk factor for hypertension, dys-lipidemia, and CVD, increasing the risk of cardiovascularevents and mortality in patients with type 2 diabetes.10–12
Distribution of body fat also plays a role in cardiometabolicrisk; individuals with central adiposity, as evidenced byincreased waist measurement or “apple” body shape, havehigher risk.13 Elevated waist circumference is defined asgreater than 100 cm (40 inches) for North American menand greater than 88 cm (35 inches) for North Americanwomen.14 The proposed Diabetes Federation cut pointsfor other geographical areas and countries are somewhatlower.15 Most individuals with type 2 diabetes are overweightor obese and/or have an elevated waist circumference.Therefore weight reduction is commonly indicated forpatients with type 2 diabetes.
Increased waist measurement is a surrogate marker forvisceral adiposity, which is fat tissue within the peritonealcavity surrounding the intra-abdominal organs. Visceraladiposity is metabolically active, secreting a number ofcytokine-like factors, referred to as adipokines. Adipokinespromote inflammation and a prothrombotic state and areassociated with development of atherogenic dyslipidemia(hypertriglyceridemia, low high-density lipoprotein [HDL]cholesterol [HDL-C] level, and an elevated subfraction ofsmall, dense low-density lipoprotein [LDL] cholesterol[LDL-C] level), insulin resistance, dysglycemia and elevatedblood pressure.16 Inflammation, as measured by serum level
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
of high-sensitivity C-reactive protein, is also associated withtype 2 diabetes and CVD.17 Modest weight reduction of 5%total body weight in individuals with type 2 diabetes is asso-ciated with decreased visceral adiposity and improvementin serum lipid concentrations, insulin action, and fastingblood glucose, as well as reductions in blood pressure,serum markers of inflammation, and the need for diabetesmedication(s).18 In some patients, substantial weight losscan lead to clinical resolution of type 2 diabetes (see alsoChapters 2, 9, and 10).19
Weight loss occurs when energy intake is lower thanenergy expenditure. An energy deficit of 500 to1000 kcal/day (3500 to 7000 kcal/wk) usually results in aweight loss of 1 to 2 lb/wk. Rate of weight loss can vary, how-ever, depending on genetic factors, age, fidgeting, amount oflean body mass, and habitual physical activity. Older indi-viduals tend to lose weight more slowly than younger per-sons because metabolic rate declines by approximately2% each decade.20 A higher lean body mass is associatedwith greater energy expenditure and therefore a higher rateof weight loss. Most overweight or obese adults will loseweight if they comply with a diet of 1000 to 1200 kcal/dayfor women or 1200 to 1600 kcal/day formen.14 An alternativeapproach to determining prescribed calorie content is basedon current total body weight and is divided into five weightcategories (Table 12-1).21
Investigators have attempted to define the dietary macro-nutrient composition that is optimal for weight reduction,improvement in cardiometabolic risk factors, and long-termweight maintenance in overweight and obese individuals, aswell as patients with type 2 diabetes (see also Chapter 5).Overall, it appears that lower-carbohydrate diets (<40% oftotal calories) may result in greater short-term weight loss,improvement in hypertriglyceridemia, and possibly improve-ment in insulin resistance and glycosylated hemoglobin, butdegree of weight loss and improvement in cardiometabolic
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

TABLE 12-1 Determining Prescribed Calorie ContentPRESCRIBED CALORIECONTENT (KCAL/DAY)
CURRENT TOTAL BODYWEIGHT (POUNDS)
1000–1200 150–199
1200–1500 200–249
1500–1800 250–299
1800–2000 300–349
2000 300 or higher
141
12EffectofLifestyle
Interven
tionsonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
risk factors is similar to that seen with low-fat or high-proteindiets at 1 to 2 years.22 Of note, however, is that many partic-ipants have difficulty maintaining the macronutrient compo-sition of their assigned diet after 6 to 12 months, so the trueimpact of differingmacronutrient composition dietary intakein the long term is not known. It is likely that the optimalmac-ronutrient composition varies for different individuals withregard to long-term compliance. Therefore, dietary guidanceshould be individualized to the patient’s lifestyle, prefer-ences, and culture. According to the American DiabetesAssociation (ADA) 2013 Position Statement,23 the mix of car-bohydrate, protein, and fat may be adjusted to meet the met-abolic goals and individual preferences of the person withdiabetes.The ADA, the Obesity Society, and the American Society for
Nutrition recommend a 500- to 1000-kcal/day deficit through adiet that meets guidelines for reducing risk of comorbiditieswith obesity.18 Specifically, these organizations recommendthat the dietary macronutrient content and nutritional qualitybe based on guidelines from the ADA,24 the American HeartAssociation (AHA),25 and the National Cholesterol EducationProgram—Adult Treatment Panel (Box 12-1).26 These areevidence-based dietary interventions that have been shownto improve selected cardiovascular risk factors, includinghypertension and LDL-cholesterol level, and therefore areappropriate for patients with type 2 diabetes. According tothe 2013 ADA Position Statement,23 individuals who have pre-diabetes or diabetes should receive individualized medicalnutritional therapy (MNT) as needed to achieve treatmentgoals, preferably provided by a registered dietitian familiarwith the components of diabetes MNT. The ADA statementrecognizes that for weight loss, low-carbohydrate, low-fat,calorie-restricted, or Mediterranean diets may be effective in
BOX 12-1 Dietary Guidelines Associated withCardiovascular Risk Reduction
Eat a variety of fruits, vegetables, whole grains, legumes, and low-fator nonfat dairy products.
Choose lean meats and poultry without skin, and prepare them withoutadded saturated and trans fat.Consume two or more servings of fish per week (with the exception ofcommercially fried fish fillets).Limit saturated fat to less than 7% of total calories.Minimize intake of trans fat by greatly limiting foods containing partiallyhydrogenated vegetable oil.Limit dietary cholesterol intake to less than 200 mg/day.Consume 20 to 30 g of fiber daily.Greatly limit foods and beverages with added sugars.Choose and prepare foods with little or no salt. Limit sodium intake to2300 mg/day or less, according to ADA guidelines (or less than1500 mg/day per AHA guidelines).Limit alcohol intake to � two drinks per day for men and � one drink perday for women.
Data from the ADA,24 the AHA,25 and the National Cholesterol Education ProgramExpert Panel.26
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
the short term (up to 2 years). However, for patients onlow-carbohydrate diets, it is recommended to monitor lipidprofiles, renal function, and protein intake (for those withnephropathy) and adjust hypoglycemic pharmacotherapyas needed.
Prepackaged meal replacements in the form of liquidshakes, bars, and entrees are a useful tool to simplify aprescribed diet and minimize errors with portion controland high-caloric-density food choices. Meal replacementdiets can enhance weight loss, improve cardiovascular riskfactors, and have shown durable weight loss for periods of 4to 5 years.27–32 A meal replacement weight loss diet typicallyconsists of replacing two food meals and two snacks withfour approximately 110- to 200-kcal shakes or bars, plusone food meal consisting of lean protein, low-starch vegeta-bles, a fruit serving, and a starch serving. Total daily caloricintake often ranges from 900 to 1300 kcal/day. For weightmaintenance, individuals typically have two food mealsand replace a third meal and one to two snacks per day witha shakes and/or bars. In a study of 119 patients with type2 diabetes, use of prepackaged meal replacements, com-pared with calorie-equivalent usual-care diet, resulted ingreater weight loss (�3.0 � 5.4 kg versus �1.0 � 3.8 kg),improved glycemic control with lower hemoglobin A1c(HbA1c) levels, improved quality of life, and better compli-ance with dietary recommendations after 1 year.27 Anotherstudy found that the use of liquid meal replacementsfor 12 weeks in patients with type 2 diabetes resulted insignificantly greater weight losses and reductions in fastingblood sugar compared with a conventional diet with thesame calorie goal.33
With the prescription of ameal replacement diet, caremustbe taken to lower or discontinuemedications that can lead tosignificant hypoglycemia, such as sulfonylureas, insulin secre-tagogues, and insulin. Required medication adjustments arebased on the patient’s current glycemic control, the pre-scribed dietary carbohydrate content, and the anticipatedrate of weight loss based on calorie deficit. Patients shouldmonitor blood glucose on a scheduled basis, and assessmentfor further medication adjustments should be completeddaily to weekly for the first 3 to 4 weeks on the diet and thenat intervals of 2 to 4 weeks during weight loss.
Recently, the Look AHEAD (Action for Health in Diabetes)study34 examined whether cardiovascular morbidity andmortality in persons with type 2 diabetes were reducedthrough an intensive lifestyle intervention aimed at achiev-ing and maintaining at least a 10% loss of body weight over4 years. This large randomized controlled trial of 5145 partic-ipants included moderate-intensity exercise with a goal of200 min/wk, a healthy diet that included portion-controlledfoods, and behavior modification, versus a usual-care con-trol group (diabetes support and education). The primaryoutcome was a composite of death from cardiovascularcauses, or hospitalization for angina pectoris for up to13.5 years. One-year results showed an average 8.6% weightloss, significant reduction of glycosylated hemoglobin, andreduction in several cardiovascular risk factors in the inter-vention group. Other important health benefits includedimprovement in obstructive sleep apnea, reduction indiabetes medications, maintenance of physical mobility,and improvement in quality of life. However, despite thesenumerous health improvements, the intensive lifestyleintervention did not reduce the rate of cardiovascular eventsand the trial was halted early.
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

142
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
Dietary Intake and Cardiometabolic RiskThe ADA MNT goals include achieving and maintainingblood glucose levels in the normal range or as close to nor-mal as safely possible, a lipid and lipoprotein profile thatreduces the risk for CVD, and blood pressure levels in thenormal range or as close to normal as possible.24 In type 2diabetes, there is evidence that more intensive treatmentof glycemia, particularly in newly diagnosed diabetes, mayreduce long-term CVD events. The glycosylated hemoglobingoal according to ADA guidelines is below 7.0% but shouldbe individualized based on factors such as age and lifeexpectancy, comorbid conditions, and hypoglycemiaunawareness. MNT has been shown to reduce glycosylatedhemoglobin levels by 1% to 2% in type 2 diabetes, dependingon duration of diabetes.35,36 Lowering of LDL-C to a target ofless than 100 mg/dL has been shown to decrease cardiovas-cular risk in type 2 diabetes; and for high-risk individualswith overt CVD, an LDL-C goal of below 70 mg/dL is recom-mended.37 There is also evidence that lowering blood pres-sure to below 140 mm Hg systolic and below 80 mm Hgdiastolic in individuals with type 2 diabetes reducescardiovascular events.38,39 Accordingly, the ADA guidelinesrecommend a systolic blood pressure target of below140 mm Hg and a diastolic blood pressure target of below80 mm Hg.
Dietary carbohydrate intake is the major determinant ofpostprandial blood glucose levels, which in turn have a sig-nificant impact on overall diabetes control and glycosylatedhemoglobin level. Therefore the impact of carbohydrateintake on blood sugars with regard to carbohydrate amount,type, glycemic index, and glycemic load has been the focusof several investigations. Glycemic index is a measure thatcompares postprandial blood glucose responses to constantamounts of different carbohydrate-containing foods.40
Glycemic load is calculated by multiplying the glycemicindex of the food by the amount of carbohydrate. Fiber,lactose, fructose, and fat tend to lower glycemic index.Examples of carbohydrate foods with a lower glycemicindex include oats, barley, bulgur, lentils, apples, oranges,milk, and yogurt. High–glycemic index foods include itemssuch as white bread, most white rice, potato, pretzels, cornflakes, and extruded breakfast cereals. Ameta-analysis of theeffects of low–glycemic index diets on blood sugar controlfound a 0.4% reduction in glycosylated hemoglobin incomparison with high–glycemic index diets.41 In additionto the modest benefit of low–glycemic index diets on glyco-sylated hemoglobin, many low–glycemic index foods havehigher nutritional quality with regard to fiber, vitamins,and minerals. The ADA recommends a diet that includescarbohydrates from fruits, vegetables, whole grains, legumes,and low-fat milk, which are lower–glycemic index foods.
The total amount of carbohydrate in a meal also affectspostprandial glucose levels. The recommended dailyallowance for carbohydrate intake is 130 g/day, which isthe average minimum requirement.42 There are no largerandomized long-term trials that evaluate outcomes of low-carbohydrate diets specifically in individuals with diabetes.One small weight loss trial reported improvement in fastingglucose among a subset with diabetes after 1 year on a lower-carbohydrate diet (120 g/day) compared with a higher-carbohydrate diet (230 g/day), but no significant changein glycosylated hemoglobin.43 Because of lack of long-termdata on the safety of low-carbohydrate diets in patients withdiabetes as well as minimal evidence of benefit, it is
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
recommended that clinicians focus on the nutritional qual-ity of carbohydrates rather than the quantity of carbohy-drates. Therefore, counseling diabetic patients to consumemost or all of their carbohydrates from fruits, vegetables,whole grains, legumes, and low-fat milk is preferred.
Dietary strategies associated with reducing blood pressurein individuals with diabetes include the DASH (DietaryApproaches to Stop Hypertension) diet and moderation ofalcohol intake. The DASH diet is high in fruit and vegetables,moderate in low-fat dairy products, and low in animal pro-tein and includes a substantial intake of plant protein fromlegumes and nuts. This diet, which is promoted by theNational Heart, Lung and Blood Institute for the preventionand treatment of hypertension, substantially reduces bothsystolic and diastolic blood pressure.44 Additional sodiumrestriction in combination with DASH results in even greaterblood pressure lowering.45 The ADA recommends areduced-sodium diet (e.g., 2300 mg/day) for normotensiveand hypertensive individuals with diabetes. The DASH diethas also been shown to reduce LDL-C.46 A large prospectivecohort study from the Nurses’Health Study found that adher-ence to the DASH-style diet was associated with a lower riskof CHD and stroke among middle-aged women during24 years of follow-up.47
Chronic excessive alcohol intake is associated withincreased risk of hypertension,whereas light-to-moderate alco-hol intake is associated with reductions in blood pressure.38
Therefore it is recommended that adults with diabetes whochoose to drink alcohol should limit consumption to a mod-erate amount, defined as 1 drink or less per day for womenand 2 drinks or less per day for men, ideally with meals.
Findings from large trials on dietary fat intake andcardiovascular outcomes in individuals with diabetes arenot available. Because patients with diabetes have similarcardiovascular risk as those with preexisting CVD, the samedietary goals are recommended. These include limiting sat-urated fat intake to less than 7% of total calories, minimizingtrans fatty acids, and limiting cholesterol intake to less than200 mg daily. Saturated and trans fatty acids are the maindietary determinants of LDL-C, and reduction of dietaryintake of these fats has been shown to decrease plasma totalcholesterol and LDL-C. Dietary n-3 polyunsaturated fattyacids appear to have beneficial effects on plasma lipid con-centrations, lowering plasma triglycerides in individualswith hypertriglyceridemia and type 2 diabetes. Both fishand fish oil supplements contain n-3 polyunsaturated fattyacids, and consumption from either source may reduceadverse CVD outcomes.48 Other recent analyses, however,have reported no additional cardioprotective benefit fromomega-3 fatty acid supplementation.49,50 The ADA guide-lines recommend two or more servings of fish per week(with the exception of commercially fried fish filets).
Smoking CessationSmoking is an independent risk factor for all-cause mortalityin patients with diabetes, mainly because of CVD.51 There isalso a higher risk of stroke in diabetic patients who smokecompared with those who do not smoke.52 The Nurses’Health Study found there is a higher relative risk of CVDamong women who smoke a higher number of cigarettesper day as well as an increased relative risk based on pack-years.53 However, this study also found that quitting smokingfor 10 or more years virtually eliminated excess mortality risk.
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

143
12EffectofLifestyle
Interven
tionsonCoronary
Heart
Disease
Risk
inPatien
tswith
Smoking is associated with cardiovascular risk factorsincluding elevated serum total cholesterol and LDL-C levels,low serum HDL-C levels, and insulin resistance.54 In addition,smoking is associated with poorer glycemic control.55,56 Inpatients with type 1 diabetes, smokers have higher levels ofintracellular adhesion molecule-1, which is a marker ofendothelial dysfunction, compared with nonsmokers.57
Given the greatly increased cardiovascular risk associatedwith smoking in those with diabetes as well as the nearelimination of increased risk 10 years after quitting, smokingcessation is an important lifestyle change target for cardio-vascular risk reduction in individuals with diabetes. TheADA recommends including smoking cessation counselingand other forms of treatment as routine components ofdiabetes care.24 A number of large randomized controlledtrials demonstrate that even brief counseling on smokingcessation, including the use of quit dates, can be efficaciousand cost-effective. For the patient who is motivated to quit,pharmacologic therapy in addition to counseling is moreeffective than either treatment alone.58 There is alsoevidence that smoking cessation programs are cost-effectiveand successful in patients with diabetes. One proposedstrategy for clinicians managing smoking in diabetic patientsis the five As strategy59:1. Ask every patient about tobacco use.2. Advise the patient about the importance of smoking cessa-
tionateveryvisit, inabrief, clear, andunambiguousmanner.3. Assess the patient’s willingness to quit smoking within the
next 30 days.4. Assist the patient who is interested in quitting by offering
self-help material, setting a quit date, offering referral to alocal support group, and considering nicotine replace-ment therapy.
5. Arrange follow-up with those patients who are ready toquit, and give positive reinforcement during the first yearafter cessation.
Diab
etes
EXERCISE AND PHYSICAL ACTIVITY IN THEPREVENTION AND TREATMENT OF TYPE 2DIABETES MELLITUS
There is a pathophysiologic cascade by which physicalinactivity predisposes to a cluster of cardiometabolic diseases,including type 2 diabetes mellitus. With an increasingly inac-tive lifestyle, skeletalmuscle downregulates its capacity to con-vert nutritional substrates to adenosine triphosphate. Inactiveskeletal muscle’s impaired ability to oxidize glucose and fattyacids is presumably mediated by several mechanisms, includ-ing decreased mitochondrial concentration and oxidativeenzymes; a reduced ability to remove glucose from bloodbecause of fewer capillaries and diminished glucose trans-porter; and an attenuated capacity to hydrolyze blood triglyc-erides to free fatty acids, secondary to decreased lipoproteinlipase activity.60 Collectively, these metabolic perturbationsreduce the somatic capacity to burn fuel, resulting in hyperin-sulinemia, insulin resistance, and hypertriglyceridemia, andultimately increased cardiovascular risk. On the other hand,regular moderate-to-vigorous leisure-time physical activity,structured aerobic exercise, or both, can often reverse theseadverse sequelae. A significant increase in physical activityand daily energy expenditure also improves insulin actionin obesity, with or without a concomitant reduction in bodyweight and fat stores.61 This is an important (and often
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
overlooked) salutary effect, suggesting that physical activityis as efficacious in preventing insulin resistance as losing bodyweight.
Several recent randomized controlled trials in patients withtype 2 diabetes have investigated the effects of moderate-to-vigorous aerobic exercise and resistance training on cardiore-spiratory fitness, modifiable cardiovascular risk factors, andarterial stiffness, with specific reference to changes in bodyweight and fat stores.62–64 Compared with the control groupand/or counselingalone, supervisedexerciseproduced signif-icant improvements in cardiorespiratory fitness, upper andlower body strength, HbA1c, systolic and diastolic blood pres-sure, total serum cholesterol, HDL-C and LDL-C, body massindex (BMI), waist circumference, insulin resistance, inflam-mation (high-sensitivity C-reactive protein), leptin, and CHDrisk scores, independent of body weight losses. Structuredexercise durations exceeding 150 min/wk were associatedwith greater HbA1c declines than those of 150 min/wk or less(0.89% and 0.36% reductions, respectively).65 On the otherhand, large-artery elasticity, assessed by measuring pulsewave velocity, did not improve.62 A systematic review andmeta-analysis of the relevant literature from 1970 to 2009revealed that combined aerobic exercise and resistance train-ing, as well as aerobic exercise alone, were related to statisti-cally significant declines in HbA1c, triglyceride levels, waistcircumference, and systolic blood pressure among individ-uals with type 2 diabetes.66 In contrast, the meta-analysisfound little support for the benefits of resistance training aloneon cardiovascular risk factors, including changes in HbA1c orresting systolic blood pressure, in patients with diabetes.Others, however, have reported that resistance training aloneis associated with reductions in HbA1c as compared with acontrol group of patients with type 2 diabetes.65
Compared with overweight and obese individuals, thosewith a normal weight at the time of diabetes diagnosis havehigher mortality rates, even after adjustment for potentialconfounding variables.67 Because these data extend the“obesity paradox” to patients with diabetes, other potentialmodulators of survival, including body composition, fatdistribution, regular physical activity, and cardiorespiratoryfitness, beyond the measurement of BMI, may help themedical community clarify the relationships among obesity,morbidity, and mortality in adults with diabetes.68
Numerous investigations and systematic reviews haveexamined the relationships among habitual physicalactivity, cardiorespiratory fitness, diabetes, BMI, and mortal-ity. The risk for all-cause and/or cardiovascular mortality islower among overweight and obese individuals with goodaerobic fitness than in individuals with normal BMI andlow fitness.69,70 This finding has also been reported in a studyof African American and Caucasian veterans with diabetes,in whom the obesity paradox was observed along with anindependent association between poor exercise capacityand mortality within BMI categories.71 Others have reportedthat higher levels of cardiorespiratory fitness are associatedwith a substantial reduction in health risk for a given level ofvisceral and subcutaneous fat,72 and that increased physicalactivity and/or cardiorespiratory fitness is inversely associ-ated with all-cause and cardiovascular mortality in personswith diabetes.68,73–75 Collectively, these data and otherrecent reports76,77 strongly support the role of structuredexercise, regular moderate-to-vigorous physical activity, orboth, in interventions designed to prevent and treat type 2diabetes, regardless of the patient’s BMI.
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

144
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
Walking: “Exercise is Medicine” for Patientswith DiabetesEpidemiologic studies and clinical trials have consistentlydemonstrated the survival benefits of regular exercise, espe-cially walking, in the prevention and treatment of type 2diabetes mellitus (see also Chapter 5). In epidemiologicstudies, brisk walking for at least 30 min/day has been asso-ciated with a 30% to 40% reduction in the risk of developingtype 2 diabetes in women.78 Two clinical trials demonstratedthat regular walking or other moderate exercise in conjunc-tion with dietary changes and modest weight losses resultedin a 58% reduction in the development of diabetes in over-weight patients with impaired fasting glucose, as comparedwith usual-care control groups.79,80 In the Diabetes Preven-tion Program, drug therapy with metformin reduced the riskby only 31%.
In a nationally representative sample (n¼2896) ofAmericanswith diabetes aged 18 years or older, regular walk-ing was associated with significant reductions in all-causeand cardiovascular mortality, up to 39% and 54% for walkingat least 2 hr/wk and 3 to 4 hr/wk, respectively.81 The inverseassociation held inmultivariable analyses after potential con-founding variables (e.g., risk factors, BMI, comorbid condi-tions) were controlled for. Walking at moderate-intensitylevels was associated with the greatest reduction in mortalityrates. The authors concluded that “1 death per year may bepreventable for every 61 people who could be persuaded towalk at least 2 hours [per] week.” These findings are consis-tent with previous studies conducted among younger andhealthier populations with diabetes. In the Nurses’ HealthStudy, in which baseline CVD and cancer patients were elim-inated, moderate and vigorous levels of physical activitywere associated with reduced rates of overall cardiovascularevents among diabetic women aged 30 to 55 years.82 Simi-larly, the Aerobics Center Longitudinal Study reported thatmen with type 2 diabetes who had a low fitness level andwere physically inactive had higher mortality rates duringfollow-up than did their counterparts who were active andfit.73 The clinical and public health implications of these dataare enormous, because the survival benefits of moderate- tovigorous-intensity exercise, often achieved by brisk walkingalone, may be even greater than those achieved by contem-porary pharmacologic therapies to manage diabetes.83
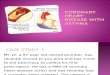
Cardioprotective Effects of Regular ExerciseTwo meta-analyses84,85 have now shown that regular exer-cise participation can decrease the overall risk of cardiovas-cular events by up to 50%, presumably from multiplemechanisms, including antiatherosclerotic, anti-ischemic,antiarrhythmic, antithrombotic, and psychological effects(Fig. 12-2). As noted earlier, aerobic exercise, with andwithout resistance training, has favorable effects on thediabetic patient’s cardiovascular risk factor profile, as wellas on coagulability, fibrinolysis, and coronary endothelialfunction. Because more than 40% of the risk reduction asso-ciated with exercise training cannot be explained bychanges in conventional risk factors, a cardioprotective“vascular conditioning” effect, including enhanced nitricoxide vasodilator function, improved vascular reactivity,altered vascular structure, or combinations thereof, has beenproposed.86 Decreased vulnerability to threatening arrhyth-mias and increased resistance to ventricular fibrillation havealso been postulated to reflect exercise-related adaptations
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
in autonomic control. As a result of endurance training, sym-pathetic drive at rest is reduced and vagal tone and heart ratevariability are increased. Moreover, ischemic precondition-ing before coronary occlusion, at least in animal models,can reduce subsequent infarct size and/or the potential formalignant ventricular arrhythmias.87,88
PHYSICAL ACTIVITY, EXERCISEPROGRAMMING, AND PRESCRIPTION
In many patients with type 2 diabetes, adequate glycemiccontrol can often be achieved by dietary changes, regularphysical activity, structured exercise, and weight reduction.The exercise program should generally follow contemporaryguidelines for the treatment of excessive body weight and fatstores,89 and other risk factors associated with this commonmetabolic condition (i.e., dyslipidemia, hypertension,inflammatory markers, fibrinolytic factors, waist circumfer-ence). Overall, individuals with type 2 diabetes have anincreased risk of morbidity and mortality from CVD ascompared with their age- and gender-matched counterpartswithout this comorbidity. Accordingly, a physical examina-tion and a careful preliminary cardiovascular assessment,including peak or symptom-limited exercise testing, withestimated or directly measured peak oxygen consumption( O2 peak), should be considered before beginning avigorous (�60% O2 reserve) exercise trainingprogram,where
_Vo2 reserve¼% intensity� _Vo2 peak� _Vo2 rest� �
+ _Vo2 rest
With this formula, O2 is generally expressed inmLO2/kg/min
or in metabolic equivalents (METs), where 1 MET¼3.5 mLO2/kg/min. Both the AHA90 and the American College ofSports Medicine (ACSM) guidelines for exercise testing andprescription91 recommend that peak or symptom-limitedexercise testing be considered before initiation of vigorousexercise training in individuals with known or suspectedCVD, including patients with diabetes mellitus.92Type of ExerciseAerobic (or endurance) exercise has been the most fre-quently studied mode of physical conditioning, and theresultant increases in cardiorespiratory fitness in patientswith type 2 diabetes have been consistently associated withimprovements in modifiable cardiovascular risk factors,independent of weight loss.64 The most effective exercisesfor the endurance phase use large muscle groups, are main-tained continuously, and are rhythmic in nature, such aswalking, jogging, elliptical training, stationary or outdoorcycling, swimming, rowing, stair climbing, and combinedarm-leg ergometry. Other exercise modalities commonlyused in structured exercise training programs for patientswith type 2 diabetes include calisthenics, particularly thoseinvolving sustained total-bodymovement, recreational activ-ities (e.g., golf, doubles tennis, pickleball), and resistancetraining.93 The last is a particularly important option,because traditional aerobic-conditioning regimens often failto accommodate participants who require improved musclestrength or endurance to perform occupational or leisure-time activities. Moreover, studies have now shown that mus-cular strength is inversely associated with all-causemortality,independent of cardiorespiratory fitness levels.94
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

Potential Cardioprotective Effects of Regular Physical Activity
Antiatherosclerotic
Improved lipids
Lower BPs
Reduced adiposity
Insulin sensitivity
Inflammation
Psychologic
Depression
Stress
Social support
Antithrombotic
Plateletadhesiveness
Fibrinolysis
Fibrinogen
Blood viscosity
Anti-ischemic
MyocardialO2 demand
Coronary flow
Endothelialdysfunction
EPCs and CACs
Nitric oxide
Antiarrhythmic
↑ Vagal tone
↓ Adrenergicactivity
↑ HR variability
FIGURE 12-2 A structured endurance exercise program, increased lifestyle physical activity, or both, sufficient to maintain and enhance cardiorespiratory fitness may providemultiple mechanisms to reduce nonfatal and fatal cardiovascular events in “at-risk” patients with diabetes. BP¼Blood pressure; CACs¼cultured angiogenic cells;EPCs¼endothelial progenitor cells; HR¼heart rate; O2¼oxygen; " ¼ increased; # ¼ decreased.
145
12EffectofLifestyle
Interven
tionsonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
Because of the high prevalence of underlying ischemicheart disease, and the heightened risk for exertion-relatedcardiovascular events and orthopedic injuries, adoption ofa moderate intensity (e.g., walking), rather than a vigorousphysical activity program (e.g., jogging, running) may bemore appropriate for diabetic patients, especially thosewho are middle-aged and older.83 Walking has severaladvantages over other forms of exercise during the initialphase of a physical conditioning program, including inher-ent neuromuscular limitations on the speed of walking(and therefore the rate of energy expenditure). Brisk walkingprograms can significantly increase aerobic capacity andreduce body weight and fat stores, particularly when thewalking duration exceeds 30 minutes.95 Additional advan-tages of a walking program include accessibility, social com-panionship, lack of special equipment (other than a pair ofwell-fitted athletic shoes), an easily tolerable exercise inten-sity, and fewer musculoskeletal and orthopedic problems ofthe legs, knees, and feet than with jogging or running. Walk-ing in water,96 with a backpack, or with a weighted vest97 areoptions for those who seek to progressively increase theexercise intensity and associated energy expenditure.
The Rule of 2 and 3 Miles per Hour (mph)Because most diabetic patients, many of whom are over-weight or obese, prefer to walk at moderate intensities, itis helpful to recognize that walking on level ground at 2and 3 mph approximates 2 and 3 METs, respectively. Forpatients who prefer the slower walking pace (2 mph;3.2 km/h), each 3.5% increase in treadmill grade addsapproximately 1 MET to the gross energy cost. Therefore,patients who desire to walk at a 2-mph pace, but require a4-MET workload for training, would be advised to add7.0% grade to this speed. For patients who can negotiatethe faster walking speed (3 mph; 4.8 km/h), each 2.5%increase in treadmill grade adds an additional 1 MET tothe gross energy expenditure. Accordingly, a workload of3 mph, 7.5% grade, would approximate an aerobic require-ment of 6 METs. Use of this practical rule can be helpful toclinicians in prescribing treadmill exercise workloads for
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
their diabetic patients, without the need for consultingtables, nomograms, or metabolic formulas or calculations.98
Resistance TrainingAlthough resistance exercise has generally been consideredto be less effective in preventing and treating type 2 diabetes,some reviews suggest that it provides independent andadditive benefits to an aerobic exercise program for virtuallythe entire cluster of associated cardiovascular risk factors.99
For example, numerous studies show that resistance trainingimproves insulin sensitivity, significantly decreases HbA1cand blood pressure in diabetic and hypertensive adults,respectively, and reducesbody fat stores andvisceral adiposetissue in bothmen andwomen. In addition, themaintenanceor enhancement of lean body mass from chronic resistancetraining is associated with a modest increase in basal meta-bolic rate, which over time may facilitate greater reductionsin bodyweight than can be achievedwith increased physicalactivity and/or structured exercise. Weight-training–inducedattenuation of the hemodynamic response to lifting standard-ized loads has also been reported, which may decrease car-diac demands during daily activities such as carryingpackages or lifting moderate to heavy objects.100 There arealso intriguing data to suggest that strength training canincrease endurance capacity without an accompanyingincrease in cardiorespiratory fitness.101
Although the traditional weight-training prescription hasinvolved performing each exercise three times (e.g., threesets of 10 to 15 repetitions per set), it appears that one setprovides similar improvements in muscular strength andendurance, at least for the novice exerciser.102
Consequently, single-set programs performed at least twotimes a week are recommended rather than multisetprograms, because they are highly effective, less time-consuming, and less likely to cause musculoskeletal injuryor soreness. Such regimens should include 8 to 10 differentexercises involving the trunk and upper and lower extremi-ties at loads that permit 8 to 15 repetitions per set. At least60 minutes of resistance training should be completed eachweek (e.g., two 30-minute sessions).
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

146
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
Lifestyle Physical ActivityDespite contemporary exercise guidelines and the much-heralded Surgeon General’s report,103 the traditional modelfor getting people to be more physically active (i.e., a regi-mented or structured exercise program) has been only mar-ginally effective. Randomized clinical trials have now shownthat a lifestyle approach to physical activity among previ-ously sedentary adults has similar effects on cardiorespira-tory fitness, body composition, and coronary risk factorsas a structured exercise program.104,105 These findings haveimportant implications for public health, suggesting an alter-native approach to sedentary people who, for one reason oranother, are not ready to integrate a formal exercise commit-ment into their daily schedule.106 The skyrocketing preva-lence of overweight and obesity and related sequelae(e.g., type 2 diabetes, metabolic syndrome) suggests theneed for “real world” interventions designed to circumventand attenuate barriers to achieving an adequate daily energyexpenditure.107 Accordingly, physicians and allied healthprofessionals should counsel patients to integrate multipleshort bouts of physical activity into their lives.108 Nonexer-cise activity thermogenesis—the spontaneous physical activ-ities of daily living (e.g., fidgeting while sitting, standingwhile reading, moving the lower extremities while workingat the computer)—represents another source of energyexpenditure for many people.109 Standing also elevates lipo-protein lipase, an enzyme that improves fat metabolismwhile reducing insulin resistance.110,111 Thus, energy expen-diture during nonexercise time may be as critical for preven-tative health as structured exercise time. Pedometers can behelpful in this regard, as can programs that use them (e.g.,America on the Move) to enhance awareness of physicalactivity by progressively increasing daily step totals. Accord-ing to one systematic review, pedometer users significantlyincreased their physical activity by an average of 2491 stepsper day more than their control counterparts.112 The Activity
2–3 ti
3–5 ti
Eve
• Make extra ste• Walk the dog• Take the stairs• Park your car f
• Golf• Bowling• Yardwork
Enjoy leisureactivities
• Watc• Play
gam
Sspa
• Long walks• Biking• Swimming
Aerobic activities
FIGURE 12-3 The Activity Pyramid, analogous to the U.S. Department of Agriculture (USDeducation for adoption of a progressively more active lifestyle. (Copyright ©1996 Park Nic
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
Pyramid (Fig. 12-3) has also been suggested as a model tocombat America’s increasingly hypokinetic environment.113
This schematic presents a tiered set of weekly goals to pro-mote improved cardiorespiratory fitness and health, build-ing on a base that emphasizes the importance ofaccumulating at least 30 minutes of moderate-intensity activ-ity on 5 or more days per week.
Intensity and DurationThere is some controversy regarding the most appropriateexercise intensity and duration that are needed to optimallyphysically condition patients with insulin resistance syn-drome.114 Different risk factors associatedwith this conditionmay respond more favorably to different exercise dosagesand intensities. For example, a randomized, controlled trialof previously inactive, overweight men and women withabnormal lipoprotein profiles compared the effectivenessof three different exercise regimens versus controls: high-amount, high-intensity exercise; low-amount, high-intensityexercise; and low-amount, moderate-intensity exercise.115
Although all exercise groups demonstrated improvedresponses on a variety of lipid and lipoprotein variables ascompared with the control group, the most beneficialchanges were noted in the high-amount, high-intensity exer-cise regimen. Because type 2 diabetes has been associatedwith increased body weight and fat stores, a sedentary life-style, and a low level of cardiorespiratory fitness, the initialexercise intensity should approximate at least 40% of theO2 or heart rate reserve or 55% of the maximal heart rate,at a rating of perceived exertion (6 to 20 category scale) of11 (fairly light) or higher, for a minimum accumulated dura-tion of 30 min/day.116,117 Over time, in the absence ofadverse signs and symptoms, the exercise intensity shouldbe gradually increased, generally corresponding to a ratingof perceived exertion up to 14 (somewhat hard to hard),to provide the stimulus to improve cardiorespiratory fitness
mes/wk
mes/wk
ryday
ps in your day
instead of the elevatorarther away and walk
h TV computeres
itringly
• Curl-ups• Push-ups• Weight lifting
Stretch/strengthen
• Tennis• Racquetball• Basketball
Recreational sports
A) Food Guide Pyramid, has been suggested as a model to facilitate public and patientollet Health-source Institute for Research and Education. Reprinted with permission).
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

147
12EffectofLifestyle
Interven
tionsonCoronary
Heart
Disea
and facilitate a progressive overload (i.e., attainment of goalenergy expenditure).The exercise intensity recommendation can be achieved
with a combination of moderate and vigorous physical activ-ity, which approximates 40% to 59% and 60% to 84% of O2 orheart rate reserve, respectively. The ACSM recommends thatmost adults engage in moderate-intensity exercise trainingfor at least 30 min/day on at least 5 days of the week for atotal of more than 150 min/wk, or vigorous exercise trainingfor at least 20 min/day on at least 3 days of the week for atotal of more than 75 min/wk, or a combination of moderateand vigorous-intensity exercise to achieve a total energyexpenditure of more than 500 to 1000 MET/min/wk.118 Whena combination is used, it has been suggested that thevigorous-intensity exercise time can be multiplied by 1.7to allow this to be added to the moderate-intensity time.116
For example, in 1 week a diabetic patient could exerciseon 3 days for 40 minutes at a moderate intensity andon another day for 20minutes at a vigorous intensity, approx-imating 154 minutes of moderate-intensity activity(120+[20 � 1.7]). Thus, this combination of moderateand vigorous exercise meets the minimum recommendedweekly moderate-intensity exercise dosage (�150 minutes).The 1.7 multiplication factor is derived from recommenda-tions that 150 minutes of moderate-intensity exercise isequivalent to approximately 90 minutes of vigorous physical
TABLE 12-2 Exercise Recommendations for Patients withTYPE OF EXERCISE* MAJOR GOALS AND OBJECT
Aerobic (large muscle activities)—forexample, walking, jogging, stationaryor outdoor cycling, swimming
Increase O2 peak; ADLs
Improve glycemic control and coronaryfactors
Decrease rate-pressure product duringsubmaximal exercise
Induce other cardioprotective benefits (enhanced nitric oxide vasodilator funimproved vascular reactivity, alteredstructure, increased resistance to ventachycardia and fibrillation)
Resistance training (multijoint exercises,large muscle groups, progressive)
Increase muscle strength and enduranc
Increase ability to perform leisure andoccupational activities and ADLs
Decrease the rate-pressure product at aresistance (e.g., during lifting or carryobjects)
Assist in the maintenance of basal metaby maintaining or increasing lean boover time
Flexibility and stretching (upper andlower body ROM activities)
Improve balance and agility
Decrease risk of musculoskeletal and orinjury
ADLs¼Activities of daily living; HR max¼maximal heart rate; HRR¼heart rate reserve; ROM*Aerobic exercise should be preceded by a warm-up (approximately 10 minutes) and follo
Stretching (5-10 minutes) may be incorporated before or after the endurance exercise pha†
O2 reserve formula¼ ( O2 peak � O2 rest) � 40%-84% intensity+ O2 rest, where{Approximates 70%-84% of one repetition maximum.
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
activity (a ratio of 1:1.7), and is compatible with a recentposition statement from the ACSM and ADA.119
FrequencyThe frequency of exercise is an important considerationwhen structured exercise and/or increased lifestyle physicalactivity are used to treat the abnormalities associated withtype 2 diabetes, especially insulin sensitivity and glucoseuse. Although even twice-weekly exercise sessions mayfavorably influence glycemic control, patients with type 2diabetes should exercise at least 3 days each week withno more than 2 consecutive days without training,117
because increases in insulin sensitivity decline markedlyby 48 hours after exercise.120 Nevertheless, more frequentexercise (i.e., at least 5 days/wk) may serve to maximizeboth the acute glucose-lowering effect and the effect oncardiovascular risk reduction.116
A summary of exercise prescription and physical activityguidelines for patients with type 2 diabetes mellitus isshown in Table 12-2, with specific reference to the type ofexercise, major goals and objectives, and the recommendedintensity, frequency, and duration. It should be emphasized,however, that if these recommended levels of exerciseare deemed by the patient to be unrealistic or excessive,the patient should be encouraged to achievemoremoderateexercise dosages or intensities, because the primary
Type 2 Diabetes MellitusIVES INTENSITY, FREQUENCY, DURATION
40%-84% O2R† or HRR; 55%-89% HR max; RPE 11-16 (6-
20 scale)
risk No more than 2 consecutive days without exercising; four to fivesessions per week (or more) may be needed to reduce bodyweight and fat stores
�150 min/wk or �90 min/wk for moderate-intensity or vigorous-intensity exercise, respectively; �20 min per session
e.g.,ction,vasculartricular
For moderate-intensity activity (�59% O2R or HRR and/or �69%HR max and/or RPE �13), multiple shorter periods of exercise(10- to 15-min exercise bouts) accumulated throughout the daymay elicit similar (or even greater) reductions in body weight andfat stores than a single bout of the same duration
Complement structured exercise with an increase in daily lifestyleactivities (walking breaks at work, gardening, householdactivities); move more, sit less
e 8-10 different exercises that work major muscle groups; weightloads gradually increased over time
�2 times/wk
ny givening
Moderate to vigorous intensity; one to four sets of 8-10 reps at aweight that cannot be lifted more than 8-10 times,{ or 12-15reps at a weight that cannot be lifted more than 12-15 times(for patients with known CHD), with 1- to 2-min rest periodsbetween sets
bolic ratedy mass
Static stretches: hold for 10-30 sec
thopedic 2-3 days/wk
¼ range of motion; RPE¼ rating of perceived exertion (6-20 scale); O2R¼ O2 reserve.wed by a cool-down (5-10 minutes) at a reduced exercise intensity (e.g., slow walking).se.O2 values are expressed in METs.
seRisk
inPatien
tswith
Diab
etes
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

148
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
beneficiaries are individuals with and without CVD who arein the least fit, least active subgroup (bottom 20%).121,122
The Structured Exercise Session: SpecialConsiderations for Exercisers with DiabetesStructured exercise training sessions should include a pre-liminary aerobic warm-up (approximately 10 minutes), aconditioning phase (�20 minutes of vigorous-intensity or�30 minutes of moderate-intensity exercise), a cool-down(5 to 10minutes), and ideally an optional recreational game.Stretching (5 to 10 minutes) may be incorporated before orafter the conditioning or endurance exercise phase. Thewarm-up facilitates the transition from rest to the condition-ing phase by stretching postural muscles and increasingblood flow. A gradual warm-up may also reduce the likeli-hood of exercise-induced ischemic responses, which canoccur with sudden strenuous exertion.123 A walking cool-down enhances venous return during recovery, decreasingthe possibility of hypotension and related sequelae, andameliorates the potential, deleterious effects of the post-exercise rise in plasma catecholamines.124 In addition, itfacilitates more rapid removal of lactic acid than stationaryrecovery.
For patients with diabetes with adequate blood glucosecontrol or those who are mildly hyperglycemic, regularphysical activity acutely decreases blood glucose levelsand, in some patients with diabetes treated with insulin,actually reduces insulin requirements. This is because ofthe insulin-like effect of aerobic exercise. However, physicalactivity can also result in a hypoglycemic state that is themost common problem experienced by exercising patientswith diabetes treated with insulin or, to a lesser extent, oralhypoglycemic drugs. Recommendations and precautionarymeasures to reduce the potential for exercise-related compli-cations in patients with diabetes are shown in Box 12-2.
BOX 12-2 Preventive Strategies for Exercisers with Di
Wear proper footwear and practice good foot hygiene. Patients with diabetes,especially those with impaired nerve conduction in their feet, should use cush-ioned shoes (gel or air soles) and avoid high-impact activities such as running orjumping. Such activities are more likely to traumatize the feet in patients withperipheral neuropathy and precipitate vitreous hemorrhage or tractional retinaldetachment in patients with active diabetic retinopathy.
Recognize that exercise in excessive heat or humidity may exacerbatethe risk of heat injury in patients with diabetes with autonomic neurop-athy. Associated abnormalities of the nervous system can alter cardio-vascular, skin blood flow, and sweating responses to exercise in hotand humid environments, increasing the risk of heat stroke. As a gen-eral guideline, patients with diabetes should curtail outdoor exercisewhen the temperature exceeds 90� F, when the relative humidityexceeds 60%, or both.Consider that diabetes increases the risk of cardiovascular events byapproximately threefold (or more in women) and is associated with ahigher prevalence of exertion-related myocardial ischemia, typically man-ifesting as angina pectoris and/or significant ST-segment depression,which can be highly arrhythmogenic. Beta blockers, in particular, mayattenuate the rate-pressure product and associated cardiac demands,camouflaging or preventing signs or symptoms of myocardial ischemia.Monitor blood glucose before, during, and after physical activitywhen starting an exercise program. Exercise at approximately the sametime each day; a good practice is to take advantage of the acuteglucose-lowering effect of physical activity by timing the session atapproximately 1 hour after a meal (to coincide with the peak postpran-dial rise in glucose).
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
PSYCHOSOCIAL INTERVENTIONS TO SUPPORTLIFESTYLE CHANGE
Psychosocial and counseling interventions that are recom-mended to support lifestyle change and reduce cardiovascu-lar risk in patients with diabetes include self-managementeducation, screening for traits that negatively affect healthbehaviors, skill training targeted toward improved self-monitoring and development of coping strategies,23
evidence-based mind-body therapies for stress reduction,125
assessing readiness for change,126 and motivational inter-viewing.127 The literature suggests varied results when life-style change interventions have been used in treatingpatients with diabetes and CVD,128,129 ranging from minimalto modest effects. Accordingly, the ADA recommends inter-ventions aimed at self-management and behavior change.23
Although the aforementioned interventions can assist inreducing health risk and mortality, this section focusesprimarily on interventions that can be incorporated intoday-to-day clinical practice with patients, including assess-ment of readiness for change, motivational interviewing,and evidence-based mind-body therapies for stress reduction.
Readiness for ChangeOne approach that can guide healthcare providers’ interven-tions with patients when personal choice and behavior arekey to determining outcomes is the transtheoretical model,originally proposed by Prochaska and DiClemente.130 Thismodel is often referred to as the health-related behaviorchange model.131 Health-related behavior change includesbehaviors that patients commonly engage in to maintainor improve their health. As Figure 12-4 demonstrates, thereare seven stages in the model. Although it is enticing to per-ceive the model as linear or circular, it is actually far morecomplex. It is possible for patients to move through variedbehavioral stages in a nonlinear fashion.131 Consequently,
abetes
Inject insulin in body areas where muscles are not actively recruited by exer-cise. For example, an inactive injection area like the abdomen should be usedbefore walking, jogging, or stationary or outdoor bicycling.The response to structured exercise and/or moderate-to-vigorous physicalactivity in the patient with diabetes taking insulin depends on a numberof variables, including the adequacy of control by exogenous insulin.Accordingly, diabetes must be under adequate control before the patientbegins an exercise program. A blood glucose concentration above300 mg/dL or above 240 mg/dL with urinary ketone bodies is considereda relative contraindication to exercise participation. In patients takinginsulin, consideration should be given to the ingestion of 20 to 30 g ofadditional carbohydrate before exercise when the preexercise blood glucoseis below 100 mg/dL.Exercising during the evening hours increases the risk of nocturnal hypogly-cemia, which may occur up to 4 to 6 hours after an exercise bout. To decreasethe likelihood of this response during the night (or day), the patient with dia-betes may need to reduce his or her insulin dose or increase carbohydrateintake before or after exercise.Recognize the signs and symptoms of hypoglycemia. These include heart pal-pitations, confusion, weakness, and visual disturbances. If hypoglycemia isleft untreated, it could lead to unconsciousness or convulsions. To reducethe likelihood of complications, patients with diabetes should always carrya form of fast-acting carbohydrate (e.g., juice, candy, glucose tablets), exer-cise with a partner, and wear a diabetes identification tag.Monitor for symptoms of hyperglycemia. These include excessive thirst; fre-quent urination; blurred vision; itchy, dry skin; and a fruity odor or breath.Hyperglycemia can lead to diabetic coma.
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

Relapse
Maintenance
Contemplation
Determination
Termination
Precontemplation
Action
Determination � PreparationTermination � Exit
Synonyms
FIGURE 12-4 Stages of “readiness to change” model.
149
12EffectofLifestyle
Interven
tionsonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
it is important to understand the components of each of thestages and how to determine at which stage patients arefunctioning to most appropriately intervene.
Stages of the Transtheoretical ModelPrecontemplationPatients are not thinking about making a behavioral changeand likely do not even think that they have an unhealthy life-style and/or risk factors. The goal for healthcare providers atthis stage is to help patients recognize the need for lifestylechange(s) and move them into the contemplation stage.There are several barriers for patients in this stage, whichmay include lack of knowledge regarding their current statusor the risks for future health problems, a limited sense ofself-efficacy in relation to making positive lifestyle changes,or simply feeling content with their current weight, healthstatus, or lifestyle choices.126,130
ContemplationPatients are beginning to think about making a lifestylechange but are ambivalent; they remain unsure aboutwhether the inconvenience of changing longstandingbehaviors truly outweighs the potential risk of maintainingthe status quo. The goal for healthcare providers at this stageis to help patients explore the ambivalence they feel, help tosolidify their desire to make a change, and move them intothe preparation stage. In addition to the barriers that exist inthe precontemplation stage, which may persist, a sense ofindecisiveness may also be present. At this stage, patientsoften find it difficult to decide between continuing to engagein the same behaviors or making substantive changes thatwill ultimately lead to a healthier lifestyle.126,130
PreparationPatients have decided to change their behavior and are plan-ning to do so within the coming month. There are two goalsfor healthcare providers at this stage. The first is to helppatients move into the action stage. To achieve this, health-care providers need to help patients design an action planthat is reasonable for them. The second goal is to helppatients identify barriers tomaking lifestyle changes. Barriersat this stage often involve the decision-making process itself.Some patients find it challenging to remain committed tomaking a change because they are still actively engagedin their former behaviors. Others may feel overwhelmedby the behavioral options. Healthcare providers can helppatients explore these and decide which ones are most
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
appropriate for them. It is important to remind patients thatthe process of behavior change is dynamic and differentoptions can be subsequently chosen as replacementbehaviors or as complementary to the behaviors recentlyadopted.126,130
ActionDuring the action stage, patients have begun to make life-style changes toward meeting an identified goal. The objec-tives for healthcare providers are to help patients optimizetheir plans for success in the short and long terms and tohelp them maintain the changes to create habits. Thereare several barriers for patients in this stage, which mayinclude disillusionment with the process of change, a senseof failure, or a sense of overconfidence—the patient’s beliefthat change has occurred and that potential barriers can beeasily overcome. This can lead to unnerving experiences forpatients when an unexpected barrier arises and they do notknow how to handle it. The patient is in the action stageoften for at least 6 months, and sometimes longer. Behaviorchange is difficult, and patients may need to be remindedthat persistence regarding the target behavior is more impor-tant for long-term success than is perfection.126,130
MaintenanceNew behaviors have become well learned and newlyformed habits for patients. The goal for healthcare providersat this stage is to help ensure that patients’ newly formedbehaviors are stable and have become integrated into theirlifestyle. Barriers within the maintenance stage arise whenpatients have not reached their original goal or experiencemajor losses or stresses that can lead to resumption of previ-ous unhealthy habits or behaviors.126,130
RelapseSometimes patients resume previous unhealthy habits orbehaviors. Relapse does not occur only after patients failmaintenance, but can occur at any point during the changeprocess. The goals for healthcare providers when relapseoccurs is to identify the relapse, as well as possible triggersfor it, and then reframe the “slip” or “off-target behavior”as an opportunity to learn. Patients can use relapses to iden-tify barriers and formulate plans to address them in thefuture. Healthcare providers can help patients design amodified or improved plan of action in response to therelapse with the goal of overcoming the barrier and moving,once again, toward the original goal.126,130
ExitOnce maintenance of the new target behaviors is fullyestablished and stable, exit occurs. At this point in time,relapse is unlikely. Patients now find themselves in a stageof precontemplation regarding the previous unhealthy behav-iors. In other words, they cannot imagine wanting to go backto their former lifestyle and the unfavorable outcome(s) thatwere associated with their previous behaviors.126,130
Assessment of Stages of ChangeHow do healthcare providers determine the stage of changethat patients are in? Engaging in a dialogue with patients anddemonstrating a genuine interest in their perspective is thefirst step. Asking questions that are respectful, specific,and open-ended, without being judgmental, is critical.Taking time to listen to the responses carefully and thenasking follow-up questions to clarify key issues from the
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

TABLE 12-3 Stages of Readiness to Change, with Specific Reference to Patient Beliefs and Healthcare ProviderInteractionsSTAGE OFCHANGE PATIENT BELIEFS AND CHARACTERISTICS
HEALTHCARE PROVIDER INTERVENTION TECHNIQUESAND STRATEGIES
Precontemplation Not considering changeNot interested in hearing informationContent to maintain status quo
Validate lack of readiness for changeProvide informationPersonalize riskEncourage evaluation of current behaviorReassure that decision is the patient’s
Contemplation Ambivalent about changeNot considering change in near future
Validate lack of readiness for changeEncourage evaluation of pros and cons of current behaviorEncourage evaluation of pros and cons of behavior changeIdentify goals for behavior changeReassure that decision is the patient’s
Preparation Seriously considering changePossibly trying out some new behaviorsPlanning to make change within a month
Identify goals (small ones in service of larger outcome goal)Assess importance, confidence, and motivation for behavior changeAssist with identification of obstaclesAssist with problem-solving to address obstacles and challengesIdentify past skills and strengths that can be used and built on when change beginsIdentify social support network
Action Implementing new behavior(s)Practicing new behavior(s) for 6 months
Restructure goals as neededBolster self-efficacy; continue to build on skills and strengthsAssist with identifying and implementing strategies to combat obstaclesSupport exploration regarding lossProvide information to reiterate long-term benefits of behavior change
Maintenance Sustaining new behavior(s)Behavior(s) becoming habitsBehaviors have been consistent for more than
6 months
Reinforce internal rewardsPlan for possible relapseDevelop and implement coping strategies for triggers that can lead to off-target
behavior(s)Plan for support to maintain new behavior(s) as habit(s)
Relapse Resuming old behavior(s) Identify triggers for relapseDevelop and implement coping strategiesReassess importance, confidence, and motivation for behavior changeDiscuss pros and cons of relapse behavior(s)Discuss pros and cons of behavior change
Exit New behavior(s) now considered habit(s); natural partof daily life
Continue to support behaviors and coping strategies as neededUse success with behavior change as a strength to make other unrelated behavior
changes as needed
150
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
patients’ perspective helps develop a mutual understandingof the issue and the level of interest patients have regardingbehavior change.126,130 Table 12-3 provides an overview ofthe stages of change, typical patient beliefs or characteristicsat each stage, and methods of intervening, which healthcareproviders can use to support movement through the stagesand eventual behavior change.
Motivational InterviewingThe effectiveness of motivational interviewing as a therapeu-tic approach to address diabetes, cardiovascular health,and other clinically relevant lifestyle changes has yieldedvarying results, from strong evidence for to low levels of sus-tained behavior change.132,133 Nevertheless, there remainsenthusiasm for motivational interviewing within healthcareprovider–patient interactions in a variety of settings.134–137
Motivational interviewing is based on the notion that allbehavior is motivated, including the ambivalence that peo-ple experience when deciding whether to engage in a partic-ular behavior or not. It does not focus on the action of changeitself, but rather on the motivation to make change(s).138–140
This type of talk therapy was initially developed as a methodto treat patients with addictive behaviors and, once it wasshown to be effective, was expanded to address otherhealth-related behaviors.139,140 The underlying power of thistherapeutic approach is that patients talk themselves intochanging behavior, rather than having it suggested or
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
advised by others. Although motivational interviewing isnot a particularmethod of interactingwith patients, the spirit,principles, and skills it promotes offers healthcare providersa way of focusing on building rapport with patients and col-laborating with them to identify, examine, and reduce orresolve the ambivalence they may have in relation to behav-ior change through a variety of techniques.138–141
“Spirit” of Motivational InterviewingCollaborationToestablishapartnership, it is important todevelopagenuine,comfortableenvironment inwhichpatientsdonot feel judged.This approach requires more listening than talking, and restat-ingwhat thehealthcareproviderhears from thepatient, so thatthe patient feels that his or her perspective is valued. The ther-apeutic process is focused on developing a mutual under-standing, which may not always include agreement.127,131,140
EvocationDrawing out the patients’ beliefs and motivations regardingbehavior change is key to setting the stage for long-termchange. The role of healthcare providers is to draw outpatients’ motivations and skills for behavior change.127,131,140
AutonomyEmphasizing the right of patients to make their own deci-sions but also empowering them to maintain responsibilityfor implementing behavior change is critical, but sometimes
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

151
12EffectofLifestyle
Interven
tionsonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
overwhelming. When multiple changes may be necessary toreach an identified health goal (e.g., control of diabetessigns and symptoms, weight loss), it often helps if patientsdetermine which behavior to focus on first.127,131,140
Principles of Motivational InterviewingExpress EmpathyIt is important to be able to express understanding in amanner that enables patients to feel heard and understood,in a nonjudgmental manner that reflects the viewpoints andexperiences of the patient.127,131,134,140,141
Support Self-EfficacyMotivational interviewing is a strengths-based approach thatoperates from the perspective that patients have withinthemselves the capability to change behaviors successfully.Healthcare providers support self-efficacy by focusing onprevious successes and highlighting skills and strengths thatpatients already possess. To this end, healthcare providerscan suggest skills and strengths that can be used or builton, as change is being considered, planned, and implemen-ted. In addition, allowing patients to set their own agenda forchange will support self-efficacy. For example, when consid-ering multiple lifestyle changes that might be necessary forsuccessful management of diabetes (e.g., self-monitoringof glucose levels, changing eating habits, increasing physicalactivity, reducing stress), allowing patients to determinewhich change to make first empowers them and increasesthe likelihood of the behavior change being sustained overtime.127,131,140–142
Roll with ResistanceResistance is not a part of the personality or character ofpatients. Instead, it is a manifestation of the process goingon between providers and patients, as well as the ambiva-lence that is felt or experienced by patients when they con-template making behavioral changes. When patients argueagainst, challenge, or discount information presented byproviders or interrupt and/or talk over providers, they arelikely demonstrating resistance to hearing or truly acceptingthe need for change. Resistance also presents itself in theform of denial, when patients deny they have lifestyle defi-cits, blame others for the problem, or minimize the potentialnegative impact of the habit at hand. Finally, resistance mayoccur when patients overtly ignore what providers say, donot respond, or sidetrack, discussing issues unrelated towhat providers have just articulated. Rather than engagingin a head-to-head confrontation, or meeting force with force,rolling with resistance involves use of techniques that allowthe scenario to dissipate. Some of the techniques that enablethis to occur are described later.127,131,140,141
Develop DiscrepancyWhen discussing change possibilities, helping to developdifferences among the beliefs of patients regarding theirhealth, current behaviors, and desired goal(s) may assistthem to move along the readiness to change continuum. Ifan agenda is set and self-efficacy is supported, discrepanciesamong patients’ understanding, beliefs, and goals oftencome to light. Essentially, motivation for change occurswhen individuals perceive a discrepancy between wherethey are and where they want to be. Once discrepanciesare identified and reflected back to patients, carefullycrafted questions can be asked to help the patients
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
understand the mismatch and empower them to movetoward behavior change.127,131,140,142
Interviewing Skills and StrategiesMotivational interviewing uses varied interviewing skills andstrategies that are taught as basic communication skills fordeveloping strong healthcare provider–patient relation-ships. The acronym OARS can cue healthcare providers toimplement the most commonly used skills and strategies,including open-ended questions, affirmations, reflections,and summaries.140
• Open-ended questions: Asking questions that cannot beanswered easily with a “yes/no” or limited response canlead to obtaining useful information from patients thatallows healthcare providers to develop a better under-standing of their concerns and perspectives. Open-endedquestions encourage patients to talk and provide personalviewpoints. These types of questions often begin withwhat, how, why, or could.131,140,141
• Affirmations: Statements that highlight patient strengthscan be a useful tool to support behavior change. Pointingout positive traits or characteristics to patients empowersthem to build on existing skills and strengths. Affirmationsmay include complimenting effort, acknowledging smallsuccesses, or stating appreciation.131,140,141
• Reflections: Reflective listening involves recognizing keywords or feelings expressed by patients and using themto paraphrase what was heard. The main ideas or conceptsreflected back to patients should represent their point ofview, not those of the healthcare provider. Reflective listen-ing accomplishes two goals: first, it enables providers toexpress empathy and demonstrate understanding ofpatients’ perspectives; second, healthcare providers canuse reflective listening to identity ambivalence regardingbehavior change and guide patients toward resolving theiruncertainty.131,140,141
• Summaries: Recapping what has occurred in healthcareprovider–patient interactions communicates interest andunderstanding and can lead to movement away fromprevious unhealthy behaviors.131,140,141
In addition to OARS, other skills are also useful within thecontext of motivational interviewing. Establishing structure,or setting an agenda for the visit, helps providers to focus onreadiness for change and appropriate behavior changeprocesses.127 The recommended structure is to ask a ques-tion that determines readiness for change, listen to patients’responses, and provide information that might help patientsmove along the change continuum. Once healthcare pro-viders have shared information with patients, they can thenask patients to share their understanding or interpretation ofthe information that was provided.131
Other important strategies when engaged in motivationalinterviewing include assessing the importance of the changebeing discussed, along with the confidence level of patientsin their ability to make the change, and finally attempting toincrease patients’ motivation for change.127,135 Readiness tochange is influenced by how important individuals perceivechange to be, as well as how confident they are that they canmake the change.
For healthcare providers, assessing importance andconfidence regarding a mutually agreeable change goalare necessary. For example, “On a scale of 1 to 10, with 10being the highest, how important is it for you to keep yourblood sugar level within the normal range each day?” In
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

TABLE 12-4 Stages of Readiness to Changewith SampleMotivational Interviewing Questions to FavorablyModifyPatient’s Behaviors (e.g., Weight Reduction)STAGE OFCHANGE PATIENT STATEMENT OR BELIEF HEALTHCARE PROVIDER INTERVENTION
Precontemplation I am comfortable at my current weight. I am worried about the effect that your weight is having on other healthfactors, and although you aren’t ready to discuss weight loss strategiestoday, I would like to discuss this issue the next time we meet, okay?
Contemplation I would like to lose weight, but I don’t know where to begin. What do you like least about your current habits? Which habit can yousee yourself changing first? How might you set things up in your life tobe able to do so?
Preparation I am going to buy a gym membership next month so that I can startexercising 3 days per week.
It sounds like you have decided that physical activity is the most importantthing to change right now. What can you do now to help ensure thatyou will be able to go to the gym 3 days per week like you stated youwant to do?
Action I have gotten all of the junk food out of the house so that I can focuson eating healthier foods without any temptations.
That’s wonderful. What are some other barriers that you find get in theway of making healthy eating choices on a consistent basis?
Maintenance I have been going to the gym 3-5 times weekly and am no longereating fast food. I have been able to sustain these behaviors for thepast 6 months.
It sounds like you have been able to maintain positive changes with youreating habits and physical activity for quite a long time. Do you worryabout particular triggers that might tempt you to engage in old,unhealthy behaviors? If so, have you thought about how to combat thetriggers if they arise?
Relapse Things got so busy at work that I started stopping for fast food on myway home from work and I have regained some of the weight I lostthis past year.
It sounds like you were able to identify the trigger that led you off target.What are some things you can do to balance work demands whilecontinuing to engage in the healthier new behaviors you have beenworking toward creating as habits that you would like to last for life?
Exit I have maintained my current weight for the past 2 years and I don’tsee myself ever going back to my old ways.
If you were giving someone else advice regarding how to maintainconsistent healthy choices, what would you tell him or her?
152
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
assessing the level of importance for making a change, it iscommon for resistance to arise. If a patient rates the level ofimportance below 7, it suggests that the healthcare providermay be moving too quickly in the approach.
Once an importance level has been established, it is alsopossible to use the rating to increase the patient’s motivationlevel to engage in change by asking him or her to elaborateon why he or she rated the importance at the particular levelthat was chosen. Whether the rating is higher or lower in therange, questions can be asked to solidify or shift the ratingupward. For example, “Although you indicated that youwant to pay closer attention to the fluctuation in your bloodsugar throughout the day, when I asked you to rate theimportance of monitoring your blood sugars daily, you ratedthe importance as 6. What would it take to increase theimportance level to a 7 or 8?”
Similar methods can be used to determine patients’ con-fidence level for making a behavioral change. Once again, aconfidence rating below 7 suggests the need to determinewhat would be necessary to increase the level of confidencethat change can be made successfully. Without a higherconfidence level, patients are likely to fail in their effort tochange behaviors.
Using Change Talk in Motivational InterviewingChange talk includes statements made by patients thatsuggest consideration of change, motivation for change, orcommitment to change. The acronym DARN CAT can helphealthcare providers to remember the different types ofstatements and their meanings. The first four types of changetalk, represented by DARN, reflect precommitment to change(desire, ability, reason, need). There may be conflict orambivalence noted between statement types, which are oftenpaired together with the connector word but. For example, “Iwant to [desire], but I can’t [ability]”.140,141 The last threetypes of change talk, represented byCAT, reflect commitmentto change (commitment, activation, taking steps).
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
In summary, motivational interviewing offers healthcareproviders a therapeutic approach to health-related behaviorchange issues that allows for increased mutual understand-ing regarding patients’ perceptions and experience, as wellas methods to increase importance, confidence, andmotiva-tion regarding making behavioral changes and developingan action plan to achieve long-term success.
Table 12-4 combines the transtheoretical model of stagesof change and motivational interviewing strategies to illus-trate how the two models can be used in conjunction witheach other.143 Weight loss goals are used as examples forinterventions for all stages.
Evidenced-Based Mind-Body TherapiesResearch demonstrates reduction in risk for both cardiovas-cular events and mortality when stress reduction techniquesare used by patients.125 Yet traditional medicine often fallsshort in offering integrative approaches for stress reduction.Healthcare providers can recommend options such asmeditation, yoga, mindfulness-based stress reduction, petownership, guided imagery, biofeedback, and tai chi, orcombinations thereof, all of which are associated with signif-icant reductions in stress and stress-related illnesses.125,142
Many of these methods can be taught by healthcareproviders, learned in settings identified by healthcare pro-viders, and offered to patients at risk, including those withdiabetes.
SUMMARY
The treatment of CVD has evolved from simple lifestylemodifications in the 1960s, largely focused on a “prudentdiet” and regular exercise, to an array of costly medicaland revascularization interventions that too often fail toaddress the underlying causes—poor dietary habits, physi-cal inactivity, and cigarette smoking. The INTERHEART
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

153
12EffectofLifestyle
Interven
tionsonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
study examined the risk factors associated with first acutemyocardial infarction in 52 countries, including 15,152patients and 14,820 controls.144 Five risk factors (abnormallipids, smoking, hypertension, diabetes mellitus, abdominalobesity) accounted for approximately 80% of the populationattributable risk in men and women. Similarly, Khot and col-leagues145 and Greenland and colleagues146 examined datafrom 14 randomized clinical trials and three prospectivecohort studies and reported that more than 80% of patientswho developed CHD and 87% or more of patients who expe-rienced a fatal coronary event had antecedent exposure to atleast one of the four conventional cardiovascular risk factors(cigarette smoking, dyslipidemia, hypertension, diabetesmellitus). Collectively, these data and other recentreports147,148 suggest that a more rigorous focus on these riskfactors and the lifestyle behaviors that promote them hasgreat potential to reduce the burden of atheroscleroticCVD. Added benefits include a reduction in angina symp-toms, decreases in exercise-induced signs or symptoms ofmyocardial ischemia, fewer recurrent cardiac events, animproved quality of life, and diminished need for coronaryrevascularization.The issue is not information but methods, motivation, and
behavioral changes.149 Accordingly, patients with diabetesshould be directed toward comprehensive programsdesigned to change behavior and facilitate cardiovascularrisk reduction, with use of individually tailored interventionsto circumvent or attenuate barriers to participation andadherence. The challenge is yours!
References1. Thom T, Haase N, RosamondW, et al: Heart disease and stroke statistics—2006 update: a report
from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee,
Circulation 113(6):e85–e151, 2006.
2. Gregg EW, Cheng YJ, Cadwell BL, et al: Secular trends in cardiovascular disease risk factors
according to body mass index in US adults, JAMA 293(15):1868–1874, 2005.
3. Mozaffarian D, Wilson PW, Kannel WB: Beyond established and novel risk factors: lifestyle risk
factors for cardiovascular disease, Circulation 117(23):3031–3038, 2008.
4. Heidenreich PA, Trogdon JG, Khavjou OA, et al: Forecasting the future of cardiovascular disease
in the United States: a policy statement from the American Heart Association, Circulation 123
(8):933–944, 2011.
5. Weintraub WS, Daniels SR, Burke LE, et al: Value of primordial and primary prevention for car-
diovascular disease: a policy statement from the American Heart Association, Circulation 124
(8):967–990, 2011.
6. Asch DA, Muller RW, Volpp KG: Automated hovering in health care—watching over the
5000 hours, N Engl J Med 367(1):1–3, 2012.
7. Marvasti FF, Stafford RS: From sick care to health care—reengineering prevention into the U.S.
system, N Engl J Med 367(10):889–891, 2012.
8. Schroeder SA: Shattuck lecture. We can do better—improving the health of the American
people, N Engl J Med 357(12):1221–1228, 2007.
9. Chiuve SE, McCullough ML, Sacks FM, et al: Healthy lifestyle factors in the primary prevention of
coronary heart disease among men: benefits among users and nonusers of lipid-lowering and
antihypertensive medications, Circulation 114(2):160–167, 2006.
10. Krauss RM, Winston M, Fletcher BJ, et al: Obesity: impact on cardiovascular disease, Circulation98(14):1472–1476, 1998.
11. Wilson PW, D’Agostino RB, Sullivan L, et al: Overweight and obesity as determinants of cardio-
vascular risk: the Framingham experience, Arch Intern Med 162(16):1867–1872, 2002.
12. Lew EA, Garfinkel L: Variations inmortality by weight among 750,000men andwomen, J ChronicDis 32(8):563–576, 1979.
13. Balkau B, Deanfield JE, Després JP, et al: International Day for the Evaluation of Abdominal
Obesity (IDEA): a study of waist circumference, cardiovascular disease, and diabetes mellitus
in 168,000 primary care patients in 63 countries, Circulation 116(17):1942–1951, 2007.
14. National Heart, Lung and Blood Institute: Clinical guidelines on the identification, evaluation
and treatment of overweight and obesity in adults. The evidence report, NIH Publication No.
98-4083 Bethesda, MD, September 1998, National Institutes of Health.
15. Alberti KG, Zimmet P, Shaw J: Metabolic syndrome—a new world-wide definition. A consensus
statement from the International Diabetes Federation, Diabet Med 23(5):469–480, 2006.
16. Bray GA, Clearfield MB, Fintel DJ, et al: Overweight and obesity: the pathogenesis of
cardiometabolic risk, Clin Cornerstone 9(4):30–40, 2009, discussion 41–2.
17. Kaptoge S, Di Angelantonio E, Lowe G, et al, for the Emerging Risk Factors Collaboration:
C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an
individual participant meta-analysis, Lancet 375(9709):132–140, 2010.18. Klein S, Sheard NF, Pi-Sunyer X, et al: Weight management through lifestyle modification for the
prevention and management of type 2 diabetes: rationale and strategies: a statement of the
American Diabetes Association, the North American Association for the Study of Obesity,
and the American Society for Clinical Nutrition, Diabetes Care 27(8):2067–2073, 2004.
19. Janosz KE, Zalesin KC, Miller WM, et al: Impact of surgical and nonsurgical weight loss on dia-
betes resolution and cardiovascular risk reduction, Curr Diab Rep 9(3):223–228, 2009.
20. Goldstein DJ: Beneficial health effects of modest weight loss, Int J Obes Relat Metab Disord 16
(6):397–415, 1992.
21. Klein S, Wadden T, Sugerman HJ: AGA technical review on obesity, Gastroenterology123:882–932, 2002.
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
22. Sacks FM, Bray GA, Carey VJ, et al: Comparison of weight-loss diets with different compositions
of fat, protein, and carbohydrates, N Engl J Med 360(9):859–873, 2009.
23. American Diabetes Association: Standards of medical care in diabetes—2013, Diabetes Care 36(Suppl 1):S11–S66, 2013.
24. American Diabetes Association, Bantle JP, Wylie-Rosett J, Albright AL, et al: Nutrition
recommendations and interventions for diabetes: a position statement of the American Diabetes
Association, Diabetes Care 31(Suppl 1):S61–S78, 2008.
25. Krauss RM, Eckel RH, Howard B, et al: AHA dietary guidelines: revision 2000: A statement for
healthcare professionals from the Nutrition Committee of the American Heart Association,
Circulation 102(18):2284–2299, 2000.
26. Executive summary of the third report of the National Cholesterol Education Program (NCEP)
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults
(Adult treatment panel III), JAMA 285(19):2486–2497, 2001.
27. Metz JA, Stern JS, Kris-Etherton P, et al: A randomized trial of improved weight loss with a
prepared meal plan in overweight and obese patients: impact on cardiovascular risk reduction,
Arch Intern Med 160(14):2150–2158, 2000.
28. Haynes RB, Kris-Etherton P, McCarron DA, et al: Nutritionally complete prepared meal plan to
reduce cardiovascular risk factors: a randomized clinical trial, J Am Diet Assoc 99(9):1077–1083,1999.
29. Pi-Sunyer FX, Maggio CA, McCarron DA, et al: Multicenter randomized trial of a comprehensive
prepared meal program in type 2 diabetes, Diabetes Care 22(2):191–197, 1999.
30. Quinn Rothacker D: Five-year self-management of weight using meal replacements: comparison
with matched controls in rural Wisconsin, Nutrition 16(5):344–348, 2000.
31. Ditschuneit HH, Flechtner-Mors M, Johnson TD, et al: Metabolic and weight-loss effects of a long-
term dietary intervention in obese patients, Am J Clin Nutr 69(2):198–204, 1999.32. Flechtner-Mors M, Ditschuneit HH, Johnson TD, et al: Metabolic and weight loss effects of long-
term dietary intervention in obese patients: four-year results, Obes Res 8(5):399–402, 2000.33. Yip I, Go VL, DeShields S, et al: Liquid meal replacements and glycemic control in obese type 2
diabetes patients, Obes Res 9(Suppl 4):341S–347S, 2001.34. The Look AHEAD Research Group: Cardiovascular effects of intensive lifestyle intervention in
type 2 diabetes, N Engl J Med 369(2):145–154, 2013.
35. Pastors JG, Warshaw H, Daly A, et al: The evidence for the effectiveness of medical nutrition
therapy in diabetes management, Diabetes Care 25(3):608–613, 2002.
36. Pastors JG, Franz MJ, Warshaw H, et al: How effective is medical nutrition therapy in diabetes
care? J Am Diet Assoc 103(7):827–831, 2003.37. Smith SC Jr., Benjamin EJ, Bonow RO, et al: AHA/ACCF secondary prevention and risk reduction
therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update; a
guideline from the American Heart Association and American College of Cardiology
Foundation, Circulation 124(22):2458–2473, 2011.
38. Chobanian AV, Bakris GL, BlackHR, et al: The seventh report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report,
JAMA 289(19):2560–2572, 2003.
39. Adler AI, Stratton IM, Neil HA, et al: Association of systolic blood pressure with macrovascular
and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational
study, BMJ 321(7258):412–419, 2000.40. Jenkins DJ, Wolever TM, Taylor RH, et al: Glycemic index of foods: a physiological basis for
carbohydrate exchange, Am J Clin Nutr 34(3):362–366, 1981.41. Brand-Miller J, Hayne S, Petocz P, et al: Low-glycemic index diets in themanagement of diabetes: a
meta-analysis of randomized controlled trials, Diabetes Care 26(8):2261–2267, 2003.
42. Trumbo P, Schlicker S, Yates AA, et al: Food and Nutrition Board of the Institute of Medicine: The
National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids,
cholesterol, protein and amino acids, J Am Diet Assoc 102(11):1621–1630, 2002.43. Stern L, Iqbal N, Seshadri P, et al: The effects of low-carbohydrate versus conventional weight
loss diets in severely obese adults: one-year follow-up of a randomized trial, Ann Intern Med 140
(10):778–785, 2004.
44. Appel LJ, Moore TJ, Obarzanek E, et al: A clinical trial of the effects of dietary patterns on blood
pressure. DASH Collaborative Research Group, N Engl J Med 336(16):1117–1124, 1997.
45. Sacks FM, Svetkey LP, Vollmer WM, et al: Effects on blood pressure of reduced dietary sodium
and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative
Research Group, N Engl J Med 344(1):3–10, 2001.
46. Obarzanek E, Sacks FM, Vollmer WM, et al: Effects on blood lipids of a blood pressure-lowering
diet: the Dietary Approaches to Stop Hypertension (DASH) Trial, Am J Clin Nutr 74(1):80–89,2001.
47. Fung TT, Chiuve SE, McCullough ML, et al: Adherence to a DASH-style diet and risk of coronary
heart disease and stroke in women, Arch Intern Med 168(7):713–720, 2008.
48. Wang C, Harris WS, Chung M, et al: n-3 Fatty acids from fish or fish-oil supplements, but
not alpha-linolenic acid, benefit cardiovascular disease outcomes in primary- and secondary-
prevention studies: a systematic review, Am J Clin Nutr 84(1):5–17, 2006.49. Rizos EC, Ntzani EE, Bika E, et al: Association between omega-3 fatty acid supplementation and
risk of major cardiovascular disease events: a systematic review and meta-analysis, JAMA 308
(10):1024–1033, 2012.
50. Roncaglioni MC, Tombesi M, Avanzini F, et al, for the Risk and Prevention Study Collaborative
Group: N-3 fatty acids in patients with multiple cardiovascular risk factors, N Engl J Med 368
(19):1800–1808, 2013.
51. Moy CS, LaPorte RE, Dorman JS, et al: Insulin-dependent diabetes mellitus mortality. The risk of
cigarette smoking, Circulation 82(1):37–43, 1990.
52. Mulnier HE, SeamanHE, Raleigh VS, et al: Risk of stroke in people with type 2 diabetes in the UK:
a study using the General Practice Research Database, Diabetologia 49(12):2859–2865, 2006.
53. Al-Delaimy WK, Willett WC, Manson JE, et al: Smoking and mortality among women with type 2
diabetes: the Nurses’ Health Study cohort, Diabetes Care 24(12):2043–2048, 2001.
54. Facchini FS, Hollenbeck CB, Jeppesen J, et al: Insulin resistance and cigarette smoking, Lancet339(8802):1128–1130, 1992.
55. Lundman BM, Asplund K, Norberg A: Smoking and metabolic control in patients with
insulin-dependent diabetes mellitus, J Intern Med 227(2):101–106, 1990.
56. Hofer SE, Rosenbauer J, Grulich-Henn J, et al: DPV-Wiss Study Group: Smoking and metabolic
control in adolescents with type 1 diabetes, J Pediatr 154(1):20–23 e1, 2009.
57. Zoppini G, Targher G, Cacciatori V, et al: Chronic cigarette smoking is associated with increased
plasma circulating intercellular adhesion molecule 1 levels in young type 1 diabetic patients,
Diabetes Care 22(11):1871–1874, 1999.
58. Ranney L, Melvin C, Lux L, et al: Systematic review: smoking cessation intervention strategies for
adults and adults in special populations, Ann Intern Med 145(11):845–856, 2006.
59. Fiore MC, Jaen CR: A clinical blueprint to accelerate the elimination of tobacco use, JAMA 299
(17):2083–2085, 2008.
60. Chakravarthy MV, Booth FW: Hot topics: exercise, Philadelphia, 2003, Hanley and Belfus
(Elsevier).
61. Kelley DE, Goodpaster BH: Effects of physical activity on insulin action and glucose tolerance in
obesity, Med Sci Sports Exerc 31(11 Suppl):S619–S623, 1999.
62. Loimaala A, Groundstroem K, Rinne M, et al: Effect of long-term endurance and strength training
onmetabolic control and arterial elasticity in patients with type 2 diabetes mellitus, Am J Cardiol
103(7):972–977, 2009.
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

154
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
63. Balducci S, Zanuso S, Nicolucci A, et al: Effect of an intensive exercise intervention strategy on
modifiable cardiovascular risk factors in subjects with type 2 diabetes mellitus: a randomized
controlled trial: the Italian Diabetes and Exercise Study (EDES), Arch Intern Med 170
(20):1794–1803, 2010.
64. Balducci S, Zanuso S, Cardelli P, et al: Changes in physical fitness predict improvements in
modifiable cardiovascular risk factors independently of body weight loss in subjects with type
2 diabetes participating in the Italian Diabetes and Exercise Study (IDES), Diabetes Care 35
(6):1347–1354, 2012.
65. Umpierre D, Ribeiro PA, Kramer CK, et al: Physical activity advice only or structured exercise
training and association with HbA1c levels in type 2 diabetes: a systematic review and meta-
analysis, JAMA 305(17):1790–1799, 2011.
66. Chudyk A, Petrella RJ: Effects of exercise on cardiovascular risk factors in type 2 diabetes: a
meta-analysis, Diabetes Care 34(5):1228–1237, 2011.
67. CarnethonMR, De Chavez PJ, Biggs ML, et al: Association of weight status withmortality in adults
with incident diabetes, JAMA 308(6):581–590, 2012.
68. Florez H, Castillo-Florez S: Beyond the obesity paradox in diabetes: fitness, fatness, and
mortality, JAMA 308(6):619–620, 2012.
69. Wei M, Kampert JB, Barlow CE, et al: Relationship between low cardiorespiratory fitness and
mortality in normal-weight, overweight, and obese men, JAMA 282(16):1547–1553, 1999.
70. Fogelholm M: Physical activity, fitness and fatness: relations to mortality, morbidity and disease
risk factors. A systematic review, Obes Rev 11(3):202–221, 2010.
71. Kokkinos P, Myers J, Faselis C, et al: BMI-mortality paradox and fitness in African American and
Caucasian men with type 2 diabetes, Diabetes Care 35(5):1021–1027, 2012.
72. Lee S, Kuk JL, Katzmarzyk PT, et al: Cardiorespiratory fitness attenuates metabolic risk indepen-
dent of abdominal subcutaneous and visceral fat in men, Diabetes Care 28(4):895–901, 2005.
73. Wei M, Gibbons LW, Kampert JB, et al: Low cardiorespiratory fitness and physical inactivity as
predictors of mortality in men with type 2 diabetes, Ann Intern Med 132(8):605–611, 2000.
74. Church TS, LaMonte MJ, Barlow CE, et al: Cardiorespiratory fitness and body mass index as pre-
dictors of cardiovascular disease mortality among men with diabetes, Arch Intern Med 165
(18):2114–2120, 2005.
75. Sluik D, Buijsse B, Muckelbauer R, et al: Physical activity and mortality in individuals with
diabetes mellitus: a prospective study and meta-analysis, Arch Intern Med 172(17):1285–1295,
2012.
76. Lyerly GW, Sui X, Lavie CJ, et al: The association between cardiorespiratory fitness and risk of all-
cause mortality among women with impaired fasting glucose or undiagnosed diabetes mellitus,
Mayo Clin Proc 84(9):780–786, 2009.
77. Rejeski WJ, Ip EH, Bertoni AG, et al: Lifestyle change and mobility in obese adults with type 2
diabetes, N Engl J Med 366(13):1209–1217, 2012.
78. Hu FB, Sigal RJ, Rich-Edwards JW, et al: Walking compared with vigorous physical activity and
risk of type 2 diabetes in women: a prospective study, JAMA 282(15):1433–1439, 1999.
79. Tuomilehto J, Lindstr€om J, Eriksson JG, et al: Prevention of type 2 diabetes mellitus by changes
in lifestyle among subjects with impaired glucose tolerance, N Engl J Med 344(18):1343–1350,
2001.
80. Knowler WC, Barrett-Connor E, Fowler SE, et al: Reduction in the incidence of type 2 diabetes
with lifestyle intervention or metformin, N Engl J Med 346(6):393–403, 2002.
81. Gregg EW, Gerzoff RB, Caspersen CJ, et al: Relationship of walking to mortality among US adults
with diabetes, Arch Intern Med 163(12):1440–1447, 2003.
82. Hu FB, Stampfer MJ, Solomon C, et al: Physical activity and risk for cardiovascular events in
diabetic women, Ann Intern Med 134(2):96–105, 2001.
83. Hu FB, Manson JE: Walking: the best medicine for diabetes? Arch Intern Med 163(12):1397–1398,2003.
84. Powell KE, Thompson PD, Caspersen CJ, et al: Physical activity and the incidence of coronary
heart disease, Annu Rev Public Health 8:253–287, 1987.
85. Berlin JA, Colditz GA: A meta-analysis of physical activity in the prevention of coronary heart
disease, Am J Epidemiol 132(4):612–628, 1990.86. Green DJ, O’Driscoll G, Joyner MJ, et al: Exercise and cardiovascular risk reduction: time to
update the rationale for exercise? J Appl Physiol 105(2):766–768, 2008.87. Billman GE, Schwartz PJ, Stone HL: The effects of daily exercise on susceptibility to sudden
cardiac death, Circulation 69(6):1182–1189, 1984.
88. Hull SS Jr., Vanoli E, Adamson PB, et al: Exercise training confers anticipatory protection from
sudden death during acute myocardial ischemia, Circulation 89(2):548–552, 1994.
89. Donnelly JE, Blair SN, Jakicic JM, et al: Appropriate physical activity intervention strategies for
weight loss and prevention of weight regain for adults,Med Sci Sports Exerc 41(2):459–471, 2009.90. Fletcher GF, Ades PA, Kligfield P, et al: Exercise standards for testing and training: a scientific
statement from the American Heart Association, Circulation http://dx.doi.org/10.1161/CIR.
0b013e31829b5b44 2013 [Epub ahead of print].
91. American College of Sports Medicine: ACSM’s guidelines for exercise testing and prescription, ed8, Philadelphia, 2010, Wolters Kluwer/Lippincott Williams & Wilkins pp. 233–234.
92. Thompson PD, Franklin BA, Balady GJ, et al: Exercise and acute cardiovascular events: placing
the risks into perspective: a scientific statement from the AmericanHeart Association Council on
Nutrition, Physical Activity, and Metabolism; American Heart Association Council on Clinical
Cardiology; American College of Sports Medicine, Circulation 115(17):2358–2368, 2007.
93. Williams MA, Haskell WL, Ades PA, et al: Resistance exercise in individuals with and without
cardiovascular disease: 2007 update: a scientific statement from the AmericanHeart Association
Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism,
Circulation 116(5):572–584, 2007.
94. FitzGerald SJ, Barlow CE, Kampert JB, et al: Muscular fitness and all-cause mortality: prospective
observations, J Phys Act Health 1(1):7–18, 2004.
95. Pollock ML, Miller HS Jr., Janeway R, et al: Effects of walking on body composition and cardio-
vascular function of middle-aged man, J Appl Physiol 30(1):126–130, 1971.96. Evans BW, Cureton KJ, Purvis JW: Metabolic and circulatory responses to walking and jogging in
water, Res Q 49(4):442–449, 1978.
97. Shoenfeld Y, Keren G, Shimoni T, et al: Walking. A method for rapid improvement of physical
fitness, JAMA 243(20):2062–2063, 1980.
98. Franklin BA, Gordon NF, editors: Contemporary diagnosis and management in cardiovascular
exercise, Newtown, PA, 2009, Handbooks in Health Care Co.
99. Braith RW, Stewart KJ: Resistance exercise training: its role in the prevention of cardiovascular
disease, Circulation 113(22):2642–2650, 2006.
100. McCartney N, McKelvie RS, Martin J, et al: Weight-training-induced attenuation of the circulatory
response of older males to weight lifting, J Appl Physiol 74(3):1056–1060, 1993.101. Hickson RC, Rosenkoetter MA, Brown MM: Strength training effects on aerobic power and
short-term endurance, Med Sci Sports Exerc 12(5):336–339, 1980.102. Feigenbaum MS, Pollock ML: Strength training: rationale for current guidelines for adult fitness
programs, Phys Sportsmed 25(2):44–63, 1997.
103. United States Department of Health andHuman Services: Physical activity and health: a report of
the surgeon general, Atlanta, GA, 1996, US Department of Health and Human Services, Centers
for Disease Control and Prevention, National Center for Chronic Disease and Health Promotion.
104. Dunn AL, Marcus BH, Kampert JB, et al: Comparison of lifestyle and structured interventions to
increase physical activity and cardiorespiratory fitness: a randomized trial, JAMA 281
(4):327–334, Jan 27, 1999.
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
105. Andersen RE, Wadden TA, Bartlett SJ, et al: Effects of lifestyle activity vs structured aerobic exer-
cise in obese women: a randomized trial, JAMA 281(4):335–340, 1999.
106. Dunn AL, Andersen RE, Jakicic JM: Lifestyle physical activity interventions. History, short- and
long-term effects, and recommendations, Am J Prev Med 15(4):398–412, 1998.
107. Pratt M: Benefits of lifestyle activity vs structured exercise, JAMA 281(94):375–376, 1999.
108. Gordon NF, Kohl HW III, Blair SN: Life style exercise: a new strategy to promote physical activity
for adults, J Cardiopulm Rehabil 13(3):161–163, 1993.109. Levine JA: Nonexercise activity thermogenesis—liberating the life-force, J Intern Med 262
(3):273–287, 2007.
110. Bey L, Hamilton MT: Suppression of skeletal muscle lipoprotein lipase activity during physical
inactivity: a molecular reason to maintain daily low-intensity activity, J Physiol 551(Pt
2):673–682, 2003.
111. Levine JA, Lanningham-Foster LM, McCrady SK, et al: Interindividual variation in posture
allocation: possible role in human obesity, Science 307(5709):584–586, 2005.
112. BravataDM,Smith-SpanglerC, SundaramV,etal: Usingpedometers to increasephysical activity and
improve health: a systematic review, JAMA 298(19):2296–2304, 2007.
113. Leon AS, Norstrom J: Evidence of the role of physical activity and cardiorespiratory fitness in the
prevention of coronary heart disease, Quest 47(3):311–319, 1995.114. Shahid SK, Schneider SH: Effects of exercise on insulin resistance syndrome, Coron Artery Dis 11
(2):103–109, 2000.
115. Kraus WE, Houmard JA, Duscha BD, et al: Effects of the amount and intensity of exercise on
plasma lipoproteins, N Engl J Med 347(19):1483–1492, 2002.
116. Marwick TH, Hordern MD, Miller T, et al: Exercise training for type 2 diabetes mellitus: impact on
cardiovascular risk: a scientific statement from the American Heart Association, Circulation 119
(25):3244–3262, 2009.
117. Hordern MD, Dunstan DW, Prin JB, et al: Exercise prescription for patients with type 2 diabetes
and pre-diabetes: a position statement from Exercise and Sport Science Australia, J Sci Med Sport15(1):25–31, 2012.
118. Garber CE, Blissmer B, Deschenes MR, et al: American College of Sports Medicine position
stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory,
musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing
exercise, Med Sci Sports Exerc 43(7):1334–1359, 2011.119. Colberg SR, Albright AL, Blissmer BJ, et al: Exercise and type 2 diabetes: American College of
Sports Medicine and the American Diabetes Association: joint position statement. Exercise and
type 2 diabetes, Med Sci Sports Exerc 42(12):2282–2303, 2010.120. Borghouts LB, Keizer HA: Exercise and insulin sensitivity: a review, Int J Sports Med 21(1):1–12,
2000.
121. Blair SN, Kohl HW 3rd., Paffenbarger RS Jr., et al: Physical fitness and all-cause mortality. A pro-
spective study of healthy men and women, JAMA 262(17):2395–2401, 1989.
122. Martin BJ, Arena R, Haykowsky M, et al: Cardiovascular fitness and mortality after contemporary
cardiac rehabilitation, Mayo Clin Proc 88(5):455–463, 2013.123. Barnard RJ, MacAlpin R, Kattus AA, et al: Ischemic response to sudden strenuous exercise in
healthy men, Circulation 48(5):936–942, 1973.
124. Dimsdale JE, Hartley LH, Guiney T, et al: Postexercise peril. Plasma catecholamines and exer-
cise, JAMA 251(5):630–632, 1984.
125. Guarneri M, Mercado N, Suhar C: Integrative approaches for cardiovascular disease, Nutr ClinPract 24(6):701–708, 2009.
126. Salmela S, Poskiparta M, Kasila K, et al: Transtheoretical model-based dietary interventions in
primary care: a review of the evidence in diabetes, Health Educ Res 24(2):237–252, 2009.127. Van Nes M, Sawatzky JA: Improving cardiovascular health with motivational interviewing: a
nurse practitioner perspective, J Am Acad Nurse Pract 22(12):654–660, 2010.128. Angermayr L, Melchart D, Linde K: Multifactorial lifestyle interventions in the primary and
secondary prevention of cardiovascular disease and type 2 diabetesmellitus-a systematic review
of randomized controlled trials, Ann Behav Med 40(1):49–64, 2012.
129. Hardcastle S, Taylor A, Bailey M, et al: A randomised controlled trial on the effectiveness of a
primary health care based counselling intervention on physical activity, diet and CHD risk
factors, Patient Educ Couns 70(1):31–39, 2008.130. Prochaska JO, DiClemente CC: The transtheoretical approach: crossing traditional boundaries
of therapy, Homewood, IL, 1984, Dow Jones-Irwin.
131. Rollnick S, Mason P, Butler C: Health behavior change: a guide for practitioners, Edinburgh,
1999, Churchill Livingstone.
132. Armstrong MJ, Mottershead TA, Ronksley PE, et al: Motivational interviewing to improve weight
loss in overweight and/or obese patients: a systematic review and meta-analysis of randomized
controlled trials, Obes Rev 12(9):709–723, 2011.
133. Thompson DR, Chair SY, Chan SW, et al: Motivational interviewing: a useful approach to improv-
ing cardiovascular health? J Clin Nurs 20(9–10):1236–1244, 2011.134. Antiss T: Motivational interviewing in primary care, J Clin Psychol Med Settings 16(1):87–93, 2009.135. Greaves C, Sheppard K, Evans P: Motivational interviewing for lifestyle change, Diabetes Prim
Care 12(3):178–182, 2010.
136. Burke LE, Fair J: Promoting prevention: skill sets and attributes of health care providers who
deliver behavioral interventions, J Cardiovasc Nurs 18(4):256–266, 2003.137. Sonntag U,Wiesner J, Fahrenkrog S, et al: Motivational interviewing and shared decisionmaking
in primary care, Patient Educ Couns 87(1):62–66, 2012.138. Miller WR, Rollnick S: Motivational interviewing: preparing people for change, ed 2, New York,
2002, Guilford Press.
139. MillerWR, Rollnick S: Ten things that motivational interviewing is not, Behav Cogn Psychother 37(2):129–140, 2009.
140. Rollnick S, Miller WR, Butler CC: Motivational interviewing in health care: helping patients
change behavior, New York, 2008, The Guilford Press.
141. Levensky ER, Forcehimes A, O’DonohueWT, et al: Motivational interviewing: an evidence-based
approach to counseling helps patients follow treatment recommendations, Am J Nurs 107
(10):50–58, 2007.
142. Lorig K, Holman H, Sobel D, et al: Living a healthy life with chronic conditions: self-management
of heart disease, arthritis, diabetes, asthma, bronchitis, emphysema and others, ed 3, Boulder,
CO, 2006, Bull Publishing Company.
143. Steinberg M: Clinical perspectives on motivational interviewing in diabetes care, Diabetes Spec-trum 24(3):179–181, 2011.
144. Yusuf S, Hawken S, Ôunpuu S, et al: Effect of potentially modifiable risk factors associated with
myocardial infarction in 52 countries (the INTERHEART study): case-controlled study, Lancet364(9438):937–952, 2004.
145. Khot UN, Khot MB, Bajzer CT, et al: Prevalence of conventional risk factors in patients with
coronary heart disease, JAMA 290(7):898–904, 2003.
146. Greenland P, Knoll MD, Stamler J, et al: Major risk factors as antecedents of fatal and nonfatal
coronary heart disease events, JAMA 290(7):891–897, 2003.
147. Canto JG, Iskandrian AE: Major risk factors for cardiovascular disease: debunking the “only 50%”
myth, JAMA 290(7):947–949, 2003.
148. Kannel WB, Vasan RS: Adverse consequences of the 50% misconception, Am J Cardiol 103(3):426–427, 2009.
149. Franklin BA, Vanhecke TE: Counseling patients to make cardioprotective lifestyle changes: strat-
egies for success, Prev Cardiol 11(1):50–55, 2008.
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.