Embed Size (px)
Citation preview

http://www.aaos.org/icl65/videos/11
SYMPOSIUM
Reverse Shoulder Arthroplasty for Trauma: When, Where, and How
Benjamin W. Szeriip, DO Brent J. Morris, MD
T. Bradley Edwards, MD
AbstractReverse shoulder arthroplasty has become increasingly popular fo r the treatment o f com
p le x shoulder injuries, including p ro x im a l humerus fractures and fixed glenohumeral
dislocation, in the elderly population. The early to midterm results o f reverse shoulder
arthroplasty fo r the treatment o f p rox im a l humerus fractures are promising compared
with the results o f unconstrained humeral head replacement, and patients may have more
predictable improvement with less dependence on bone healing and rehabilitation. However,
long-term follow-up is needed, and surgeons m ust be fam ilia r with various complications
that are specific to reverse shoulder arthroplasty. To achieve optimal pa tien t outcomes
fo r the management o f traumatic shoulder injuries, surgeons m ust have a comprehensive
understanding o f the current im plant options, indications, and surgical techniques fo r reverse shoulder arthroplasty.
Instr Course Lect 2016;65:171-180.
Reverse shoulder arthroplasty was initially developed for the treatment of arthritis in a rotator cuff-deficient shoulder.1 The nonanatomic prosthesis used for reverse shoulder arthroplasty improved function and decreased pain.2
The indications for reverse shoulder arthroplasty continue to expand as it is used to treat a broad spectrum of shoulder pathologies that may not be adequately addressed by anatomic shoulder arthroplasty. These shoulder
pathologies include traumatic injuries, such as fixed glenohumeral dislocations and proximal humerus fractures, which may potentially require prosthetic replacement.
Proximal humerus fractures are the third most common fracture in patients older than 65 years.3 The incidence of proximal humerus fractures is expected to substantially increase over the next 20 years as the growth rate of this patient population increases.4 Although many proximal humerus fractures can be treated nonsurgically with satisfactory results, displaced or comminuted proximal humerus fractures are often treated surgically. Definitive management may be challenging because of the lack of consensus on appropriate surgical treatment as well as the technical demands that are required to achieve an optimal functional outcome.5
The three primary surgical options for the treatment of proximal humerus fractures are open reduction and internal fixation (ORIF), hemiarthroplasty, and reverse shoulder arthroplasty.
Dr. M orris or an immediatefamily member serves as a p a id consultant to or is an employee ofTomier. Dr. Edwards or an
immediatefamily member has received royaltiesfrom Tomier, O rthoHelix, and Shoulder Options; is a member o f a speakers'
bureau or has made p a id presentations on behalf ofTom ier; serves as a p a id consultant to or is an employee o f Kinamed
and Tomier; has received research or institutional supportfrom Tomier; has received non income support (such as equipment
or services), commercially derived honoraria, or other non-research-related funding (such as p a id travel) fro m Tomier; and
serves as a board member, owner, officer, or committee member o f the Am erican Shoulder and E lbow Surgeons. Neither
Dr. Sqerlip nor any immediate fam ily member has received anything o f value from or has stock or stock options held in a
commercial company or institution related directly or indirectly to the subject o f this chapter.
© 2016 AAOS Instructional Course Lectures, Volume 65 171

Shoulder and Elbow
Although each procedure may have different indications, tuberosity position and healing are critical for ORIF and hemiarthroplasty. Although results of reverse shoulder arthroplasty for the treatment of proximal humerus fractures are improved if union is achieved, union is not the sole director of outcome. ORIF of complex humerus fractures in the elderly population is challenging and may result in an increased incidence of rotator cuff pathology and osteoporotic bone. Failure rates for patients older than 60 years who are treated with ORIF range from 13% to 20%.640 Even with the use of locking plates to provide a fixed angle construct for ORIF, the rate of secondary screw cutout has been as high as 57%.n’12
The use of hemiarthroplasty for the treatment of displaced three- and four-part proximal humerus fractures, as first described by Neer in 1953,13 may provide some pain relief, but has shown inconsistent results for range of motion, recovery of shoulder function, and tuberosity healing.14'21 Although Grammont has used reverse shoulder arthroplasty for the treatment of proximal humerus fractures since the late 1980s,22 the procedure was not introduced in the United States until 2004. The prosthesis for reverse shoulder arthroplasty has an increased deltoid lever arm and places less biomechanical stress on the healing tuberosities, which may deliver more consistent functional results. Several studies have reported the short-term results of reverse shoulder arthroplasty for the treatment proximal humerus fractures.23 27
Older patients who have a fixed glenohumeral dislocation present several challenges, including soft-tissue contracture, glenohumeral arthritis, and bone deficiency in both the humeral
head and the glenoid. In a study of 11 patients with fixed anterior shoulder dislocations who were treated with anatomic total shoulder arthroplasty, Matsoukis et al28 reported seven complications in five patients, including four patients (36%) with anterior instability of the shoulder. Older patients who have fixed posterior dislocations are at a decreased risk for recurrent instability. In a study of 32 patients with fixed posterior shoulder dislocations who were treated with anatomic total shoulder arthroplasty, Wooten et al29 reported three patients with recurrence (9%) in the early postoperative period; however, 13 patients had unsatisfactory outcomes according to a modified Neer rating system, and 9 patients underwent revision surgery for various reasons. The outcomes from these studies suggest that anatomic total shoulder arthroplasty for fixed dislocation is difficult and can lead to complications, and the overall satisfaction rate for patients who undergo anatomic total shoulder arthroplasty for fixed dislocation is inferior compared with that of patients who undergo the same procedure for primary osteoarthritis.
IndicationsTraditionally, the indications for hemiarthroplasty in the management of proximal humerus fractures are four- part fractures, three-part fractures in older patients who have osteoporotic bone, fracture-dislocations, headsplitting fractures, and fractures that involve more than 40% of the articular surface.30'32 These fracture patterns are at an increased risk for complications with traditional ORIF because of the tenuous fixation of fracture fragments in osteoporotic bone and the high rates of osteonecrosis. Hertel et al33 reported
that the most relevant predictors of humeral head ischemia were the length of dorsomedial metaphyseal extension, the integrity of the medial hinge, and the basic fracture pattern. The authors reported that proximal humerus fractures with metaphyseal head extension less than 8 mm, a medial hinge disruption greater than 2 mm, and an anatomic neck fracture pattern had a positive predictive value of 97% for humeral head ischemia. This may explain why valgus-impacted four-part fractures are relatively unlikely to result in osteonecrosis and may be amenable to non- surgical treatment.
Reverse shoulder arthroplasty for proximal humerus fractures is typically reserved for older patients with severe osteopenia or comminution who would otherwise be indicated for a hemiarthroplasty (Figure 1). Patients with preexisting rotator cuff pathology who sustain proximal humerus fractures that require surgical treatment also are candidates for reverse shoulder arthroplasty rather than hemiarthroplasty. The contraindications for reverse shoulder arthroplasty for proximal humerus fractures are similar to those for conventional shoulder arthroplasty. Active infection is an absolute contraindication, and poor overall health is a relative contraindication. Although there is no absolute minimum age for reverse shoulder arthroplasty, ORIF should be attempted whenever possible for a physiologically young patient, even with a comminuted fracture. Both hemiarthroplasty and reverse shoulder arthroplasty should be approached with caution if the patient is unable to participate in a rehabilitation program to facilitate an optimal outcome. Deltoid insufficiency that results from permanent axillary nerve
172 © 2016 AAOS Instructional Course Lectures, Volume 65

Reverse Shoulder Arthroplasty for Trauma: When, Where, and How Chapter 11
Figure 1 A, AP radiograph demonstrates a four-part proximal humerus fracture-dislocation with osteopenia. B, Coronal CT scan demonstrates an anatomic neck fracture-dislocation.
palsy is a contraindication specific to reverse shoulder arthroplasty; however, this contraindication does not apply to transient or subclinical axillary nerve palsy, which can occur in patients who have proximal humerus fractures.
Shoulder arthroplasty may be required for older patients who have chronic (fixed) shoulder dislocations or in the presence of a humeral defect that involves more than 40% of the articular surface.28,29 For anatomic arthroplasty, if stability in posterior dislocations is not restored with humeral head replacement alone, then posterior capsular plication may be necessary. Augmentation o f the glenoid with bone graft may be necessary in anterior dislocations if the humeral head is unstable or if the glenoid deficiency is extensive. The options for glenoid bone graft include an autograft from the native humeral head, iliac crest autograft, coracoid transfer, or a distal tibia allograft. Given the poor outcomes and high rate o f complications with anatom ic shoulder arthroplasty, the authors o f this chapter have found reverse shoulder arthroplasty to be a valuable alternative to anatomic shoulder
arthroplasty for the treatment of fixed dislocation in the older patient. O ne o f the authors of this chapter (T.B.E.) performed reverse shoulder arthroplasty in 21 older patients who had fixed shoulder dislocation (20 anterior and 1 posterior).34 Only two complications (recurrent dislocation and infection) in one patient were reported at a minimum 2-year follow-up, and active elevation improved from 20° preoperatively to 100° postoperatively.34
Influence of Tuberosity Healing on Outcomes for Fracture PatientsAlthough reverse shoulder arthroplasty for the treatment of proximal humerus fractures is less contingent on a functional rotator cuff or the healing of the tuberosities24 for active forward elevation than hemiarthroplasty for the treatment o f proximal humerus fractures, it is critical that the correct position and stable fixation o f the greater tuberosity is achieved during humeral hemiarthroplasty to attain active range of motion and optimal clinical outcome.15,17,18,20'35 Boileau et al15 reported that the major
risk factors for poor outcomes after hemiarthroplasty for the treatment of proximal hum erus fractures were female sex, age older than 75 years, incorrect prosthetic height or version, and poor initial positioning of the greater tuberosity. The authors reported that the failure to restore the greater tuberosity within 10 mm below or 5 mm above the apex of the humeral head was correlated with superior migration of the humeral prosthesis, shoulder stiffness, and low patient satisfaction.15 This may explain the bimodal distribution of outcomes reported after hem iarthroplasty and why pain relief is more predictable than mobility.14 Correct position and healing of the greater tuberosity is crucial to restore external rotation, regardless of w hether hem iarthroplasty or reverse shoulder arthroplasty is used. Com pared w ith hemiarthroplasty, reverse shoulder arthroplasty has the theoretical biomechanical advantage of direct compression on the glenosphere during shoulder elevation, which potentially decreases the torque placed on the tuberosities and promotes healing.36
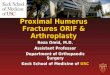
Fracture-Specific ImplantsAlthough reverse shoulder arthroplasty has rapidly gained acceptance as a treatment option for complex proximal humerus fractures, tuberosity healing is still an im portant factor to achieve optimal results; therefore, humeral im plants have been specifically designed to address this clinical need. Humeral implant features include a low-profile metaphysis for positioning of the greater tuberosity, a proximal hydroxyapatite coating, and a window into the metaphysis for additional bone graft that may facilitate union between the tuberosity fragments22 (Figure 2). T he diaphyseal portion of the humeral implant is
© 2016 AAOS Instructional Course Lectures, Volume 65 173

Shoulder and Elbow
Figure 2 Photograph of a fracture-specific humeral stem for reverse shoulder arthroplasty. (Courtesy of Tornier, Bloomington, MN.)
smooth for cementation, which allows the surgeon to gain the appropriate humeral height and provides rotational stability if there is metaphyseal bone loss.
Reverse Shoulder Arthroplasty Versus HemiarthroplastySeveral studies have recently compared reverse shoulder arthroplasty for the treatm ent o f proximal humerus fractures w ith hem iarthroplasty for the treatm ent of proximal hum erus fractures.23'27'37'38 Namdari et al39 performed a systematic review that compared the outcomes o f reverse shoulder arth ro plasty for the treatm ent o f proximal humerus fractures with those o f hemiarthroplasty with the use o f a fracture- specific stem for the treatm ent o f proximal humerus fractures. Shoulder outcome scores and mobility measurements were similar between the two groups; however, the overall complication rate for the reverse shoulder arthroplasty group was 19.4% compared with
5.6% for the hemiarthroplasty group. The revision surgery rates did not differ between the two groups, which suggest that clinical complications were treated nonsurgically. In a systematic review that compared the outcomes of reverse shoulder arthroplasty for the treatment of older adults who had proximal humerus fractures with those of hemiarthroplasty for the treatment of older adults who had proximal humerus fractures, Mata-Fink et al40 reported improved forward flexion and functional outcome scores for the reverse shoulder arthroplasty group compared with those for the hemiarthroplasty group; however, the complication rates were not appreciably higher for the reverse shoulder arthroplasty group. Gal- linet et al37 retrospectively compared 40 patients with three- or four-part proximal humerus fractures who were treated with reverse shoulder arth ro plasty or hemiarthroplasty. Tuberosity fixation was not routinely performed in the reverse shoulder arthroplasty group. The reverse shoulder arth ro plasty group had higher postoperative Constant assessment scores and better forward flexion and abduction than the hemiarthroplasty group; however, bo th internal and external rotation measurements were decreased in the reverse shoulder arthroplasty group, which emphasizes the im portance of tuberosity healing for the restoration of external rotation. Furthermore, it is difficult to accurately compare the overall performance of reverse shoulder arthroplasty with hemiarthroplasty with respect to the treatm ent o f proximal humerus fractures if tuberosity fixation was not attempted for reverse shoulder arthroplasty.25,37'41,42 A lthough recent results o f reverse shoulder arthroplasty for the treatment proximal humerus
fractures are promising,23'27’37,43 future studies are necessary to determ ine if reverse shoulder arthroplasty leads to improved functional outcomes and better tuberosity healing compared with hemiarthroplasty. Furtherm ore, more studies are necessary to determ ine if the outcomes and tuberosity healing of hemiarthroplasty versus reverse shoulder arthroplasty are influenced by surgeon technique and experience.
TechniqueSurgical A pproachSimilar to standard shoulder arthroplasty, the patient should be positioned in the modified beach-chair position. Care must be taken to position the patient sufficiently near the edge of the table to allow for full extension of the surgical arm for humeral preparation. The two prim ary surgical approaches for reverse shoulder arthroplasty are the standard deltopectoral approach and the anterosuperior approach. Each approach has certain benefits and limitations. The anterosuperior approach uses a deltoid split, which improves access to the greater tuberosity; however, the approach requires deltoid detachment and may result in dehiscence. In addition, extensibility is limited during humeral shaft exposure if humeral shaft com m inution is present. The authors o f this chapter prefer to use the deltopectoral approach because it provides reliable access to the fracture fragments and uncompromised glenoid exposure after tuberosity mobilization.
An incision is begun at the tip of the coracoid process and is extended distal- ly, approximating the deltopectoral interval. The cephalic vein, which is used as a guide to identify the deltopectoral interval, is retracted laterally with the deltoid. The pectoralis major tendon is
174 © 2016 A AOS Instructional Course Lectures, Volume 65

Reverse Shoulder Arthroplasty for Trauma: When, Where, and How Chapter 11
Figure 3 Illustration of a height gauge, which is used to reproduce humeral height. Electrocautery is used to make a mark at the lateral fin of the stem, which will serve as a landmark for retroversion of the final implant. Double- loaded sutures are placed in the diaphysis to serve as a vertical support. (Courtesy ofTornier, Bloomington, MN.)
then identified, and the superior 1 cm may be incised to enhance exposure.
Technique for Fracture CasesThe long head of the biceps tendon is used to identify the greater and lesser tuberosity fragments, which are mobilized with the use of a Cobb elevator. After the lesser tuberosity is identified with its subscapularis attachment, the subscapularis tendon is tagged with two stay sutures to gain control of the fracture fragment. The sutures are placed at the tendon-bone interface and not through the bone. The head fragment is exposed, removed, and preserved for later bone grafting. The greater tuberosity is then gently mobilized with a Lahey clamp, and a double-loaded free needle is used to pass two nonabsorbable sutures through the bone-tendon interface of the greater tuberosity, one superiorly through the infraspinatus tendon and one inferiorly through the teres minor tendon. Any tendon attachment to both the greater and lesser tuberosities, including the supraspinatus, is preserved. After control of the greater and lesser tuberosity fracture fragments is attained, the biceps tendon is tenoto- mized and, later, tenodesed to the pec- toralis major tendon.
Attention is then turned to glenoid exposure and preparation. Anterior and posterior glenoid retractors are placed to retract the lesser and greater tuberosity fragments, respectively. A Hohmann retractor is then placed inferiorly on the glenoid to retract the humeral shaft inferiorly. A capsular release is performed to optimize glenoid exposure, and the long head of the triceps is released from the glenoid to avoid a traction osteophyte that can occur with reverse shoulder arthroplasty. After adequate glenoid exposure has been attained, the
remaining labrum and the stump of the long head of biceps are removed. The glenoid is then prepared and instrumented in a standard fashion.
With the glenoid retractors removed, the arm is adducted and extended to deliver the diaphysis into the wound. The implant diameter is determined with the use of diaphyseal reamers, and a humeral trial is placed in 20° of retroversion. The ideal humeral height is determined by reducing the implant with the thinnest polyethylene insert available and applying axial traction to the arm. This may cause the humeral diaphysis to move distally on the stem and increase the overall height of the prosthesis that extends from the medial humeral calcar. The ideal amount of traction, or humeral length, is identified if good stability and no gaping between the glenosphere and polyethylene are
noted throughout range of motion. It is important that this part of the procedure be performed under full relaxation by anesthesia. A height gauge is then used to measure the determined humeral height on insertion of the final humeral component. The trial humeral component is removed, and 2-mm drill holes are placed on each side of the bicipital groove distal to the fracture. Two sutures are placed in these holes and used for vertical fixation of the tuberosities to the humeral shaft (Figure 3). A cement restrictor is placed, and the final humeral implant is cemented in place at the previously determined height and in 20° of retroversion. The authors of this chapter do not recommend uncemented implants because older patients with proximal humerus fracture may have metaphyseal bone deficiency, which can compromise humeral implant fixation.
© 2016 AAOS Instructional Course Lectures, Volume 65 175

Shoulder and Elbow
Figure 4 Illustrations dem onstrate tuberosity fixation. A, The arm is placed in neutral rotation. A clam p is used to gently pull the greater tuberosity anteriorly, which reduces the greater tuberosity to the prosthesis. Two horizontal cerclage sutures (one superio r and one inferior) are then tied to secure the greater tuberosity to the prosthesis. B, The two rem aining horizontal sutures, which had initia lly been passed through the posterior rotator cuff tendon and around the prosthetic neck, are then passed through the subscapularis tendon. One suture runs through the superior portion of the lesser tuberosity, and the other suture runs through the inferior portion of the lesser tuberosity. Both sutures are passed from inside to outside and are then tied. C, Final tightening of the double-loaded sutures that were previously p laced through the diaphysis creates a vertica l support. The shroud goes behind the infraspinatus tendon, in front of the subscapularis tendon, and is then tied. (Courtesy of Tornier, B loom ington, MN.)
Antibiotic-impregnated bone cement is used because it has been shown to prevent postoperative infection after primary reverse shoulder arthroplasty.44 After trialing is performed and stability is ensured throughout a full range of motion, the appropriate size polyethylene component is selected. There are two important steps before reduction with final implants. First, one limb of each of the four sutures through the greater tuberosity fragment has to be passed along the medial side of the implant for later tuberosity fixation. Second, if a fracture-specific implant is being used, then the bone graft should be placed in the metaphysis of the component.
After the final implant has been reduced, tuberosity fixation is performed, which is critical for restoration of active external rotation. The ideal construct for tuberosity management uses six sutures (four horizontal cerclage sutures and two vertical tension band sutures) that securely fix the tuberosities to one
another as well as the prosthesis and the diaphysis. This tuberosity management technique provides optimal inter- fragmentary stability and can be used for both hemiarthroplasty and reverse shoulder arthroplasty .45,46 One suture from the superior set of greater tuberosity sutures and one suture from the inferior set of greater tuberosity sutures are tied around the medial aspect of the implant to secure the greater tuberosity to the prosthesis (Figure 4, A). Next, the final sutures from the superior and inferior sets of greater tuberosity sutures that were previously passed around the medial side of the implant are now passed through the subscapularis tendon at the superior and inferior aspect of the lesser tuberosity. These sutures are tied to secure the lesser tuberosity to the implant and the greater tuberosity (Figure 4, B). The authors of this chapter prefer lesser tuberosity repair and healing because it can potentially improve implant stability and ultimate function; however, lesser tuberosity
repair in reverse shoulder arthroplasty for the treatment of proximal humerus fractures is somewhat controversial, and future studies are necessary to clarify this debate. Finally, the sutures that were previously placed through the drill holes in the humeral diaphysis are passed in a vertical cerclage fashion (one anteriorly based and the other posteriorly based) to secure the tuberosities to the diaphysis. The authors of this chapter prefer to use a Nice knot, which is a racking hitch knot, with the cerclage sutures to optimize tuberosity reduction .47 Additional bone graft may be placed in the area at which the diaphysis and tuberosities meet to promote healing (Figure 4, C).
Technical C onsiderations for Fixed D islocationThe same deltopectoral approach is used for fixed anterior dislocation; however, the humeral head and shaft may be retracted anteriorly when gaining access to the glenoid. The authors of
176 © 2016 AAOS Instructional Course Lectures, Volume 65

Reverse Shoulder Arthroplasty for Trauma: When, Where, and How Chapter 11
this chapter prefer to use an osteoto- mized humeral head if deficiency of the anterior glenoid is present (Figure 5). A short uncemented stem is implanted in a manner similar to that for reverse shoulder arthroplasty for cuff tear arthropathy. Tuberosity management or a fracture-specific stem are not necessary. Soft-tissue contracture may often occur with chronic fixed dislocations. Surgeons must be prepared to address contractures with a larger than normal humeral head cut and soft-tissue releases so that appropriate implant tension can be achieved and stable shoulder range of motion can be restored.
SummaryReverse shoulder arthroplasty for the management of complex shoulder pathologies, including comminuted proximal humerus fractures and chronic dislocations, has rapidly gained popularity. Reverse shoulder arthroplasty has a lower complication rate and better results than unconstrained arthroplasty for the treatment of fixed glenohumeral dislocations. Recent results of reverse shoulder arthroplasty for the treatment of fractures are promising and, when compared with results of hemiarthroplasty for the treatment of fractures, have shown improved functional outcomes for older patients who have poor bone quality; however, because long-term follow-up is needed, reverse shoulder arthroplasty for the treatment of proximal humerus fractures should be reserved for older patients with severe osteopenia or comminution who are not amenable to another treatment option. Regardless of whether hemiarthroplasty or reverse shoulder arthroplasty is used, correct positioning and healing of the tuberosities are crucial to obtain a good outcome. Surgeons
Figure 5 Intraoperative photographs of a patient who has a fixed anterior shoulder dislocation. A, Anterior bone deficiency of the glenoid is present. B, Glenoid architecture is restored with the use of an osteotomized humeral head.
must be familiar with various features that are specific to each implant and instrumentation system to restore optimal humeral length and version.
References1. Grammont PM, Baulot E: Delta
shoulder prosthesis for rotator cuff rupture. Orthopedics 1993;16(l):65-68.
2. Boulahia A, Edwards TB, Walch G, Baratta RV: Early results of a reverse design prosthesis in the treatment of arthritis of the shoulder in elderly patients with a large rotator cuff tear. Orthopedics 2002;25(2):129-133.
3. Baron JA, Karagas M, Barrett J, et al: Basic epidemiology of fractures of the upper and lower limb among Americans over 65 years of age. Epidemiology 1996;7(6):612-618.
4. Kannus P, Palvanen M, Niemi S, Parkkari J, Jarvinen M, Vuori I: Osteoporotic fractures of the proximal humerus in elderly Finnish persons: Sharp increase in 1970-1998 and alarming projections for the new millennium. Acta Orthop Scand 2000;71(5):465-470.
5. Petit CJ, Millett PJ, Endres NK, Dill- er D, Harris MB, Warner JJ: Management of proximal humeral fractures: Surgeons don’t agree./ Shoulder Elbow ■5»rg2010;19(3):446-451.
6. Hawkins RJ, Kiefer GN: Internal fixation techniques for proximal humeral fractures. Clin Orthop Relat Res 1987;223:77-85.
7. Lee CW, Shin SJ: Prognostic factors for unstable proximal humeral fractures treated with locking-plate fixation. J Shoulder Elbow Surg 2009;18(l):83-88.
8. Neer CS II: Displaced proximal humeral fractures: II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52(6):1090-1103.
9. Owsley KC, Gorczyca JT: Fracture displacement and screw cutout after open reduction and locked plate fixation of proximal humeral fractures [corrected]. J Bone Joint Surg Am 2008;90(2):233-240.
10. Zyto Ik, Ahrengart L, Sperber A, Tornkvist H: Treatment of displaced proximal humeral fractures in elderly patients./ Bone Joint Surg Br 1997;79(3):412-417.
11. Jost B, Spross C, Grehn H, Gerber C: Locking plate fixation of fractures of the proximal humerus: Analysis of complications, revision strategies and outcome. / Shoulder Elbow Surg 2013;22(4):542-549.
12. Ricchetti ET, Warrender WJ,Abboud JA: Use of locking plates in the treatment of proximal humerus fractures. J Shoulder Elbow Surg 2010; 19(2, suppl):66-75.
13. Neer CS, Brown TH Jr, McLaughlin HL: Fracture of the neck of the humerus with dislocationof the head fragment. A m J Surg 1953;85(3):252-258.
© 2016 AAOS Instructional Course Lectures, Volume 65 177

Shoulder and Elbow
14. Antuna SA, SperlingJW, Cofield RH: Shoulder hemiarthroplasty for acute fractures of the proximal humerus: A minimum five-year follow-up. J Shoulder Elbow Surg 2008;17(2):202-209.
15. Boileau P, Krishnan SG, Tinsi L, Walch G, Coste JS, Mole D: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. / Shoulder Elbow 57og2002;ll(5):401-412.
16. Goldman RT, Koval KJ, Cuomo F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and four-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4(2):81-86.
17. Kralinger F, Schwaiger R, Wambach- er M, et al: Outcome after primary hemiarthroplasty for fracture of the head of the humerus: A retrospective multicentre study of 167 patients./ Bone Joint SurgBr 2004;86(2):217-219.
18. Mighell MA, Kolm GP, Collinge CA, Frankie MA: Outcomes of hemiarthroplasty for fractures of the proximal humerus. J Shoulder Elbow Surg 2003;12(6):569-577.
19. Prakash U, McGurty DW, Dent JA: Hemiarthroplasty for severe fractures of the proximal humerus. J Shoulder Elbow Surg 2002;ll(5):428-430.
20. Solberg BD, Moon CN, Franco DP, Paiement GD: Surgical treatment of three and four-part proximal humeral fractures. J Bone Joint Surg Am 2009;91(7):1689-1697.
21. Zyto K, Wallace WA, Frostick SP, Preston BJ: Outcome after hemiarthroplasty for three- and four-part fractures of the proximal humerus.J Shoulder Elbow Surg 1998;7(2):85-89.
22. Sirveaux F, Roche O, Mole D: Shoulder arthroplasty for acute proximal humerus fracture. Orthop Traumatol Surg Res 2010;96(6):683-694.
23. Boyle MJ, Youn SM, Frampton CM, Ball CM: Functional outcomes of reverse shoulder arthroplasty compared with hemiarthroplasty for acute proximal humeral fractures. J Shoulder Elbow Surg 2013;22(l):32-37.
24. Bufquin T, Hersan A, Hubert L, Massin P: Reverse shoulder
arthroplasty for the treatment of three- and four-part fractures of the proximal humerus in the elderly: A prospective review of 43 cases with a short-term follow-up. J Bone Joint Surg Br2007;89(4):516-520.
25. Cazeneuve JF, Cristofari DJ: Gram- mont reversed prosthesis for acute complex fracture of the proximal humerus in an elderly population with 5 to 12 years follow-up. Orthop 'Traumatol Surg Res 2014;100(l):93-97.
26. Gallinet D, Adam A, Gasse N,Rochet S, Obert L: Improvement in shoulder rotation in complex shoulder fractures treated by reverse shoulder arthroplasty. J Shoulder Elbow Surg 2013;22(l):38-44.
27. Garrlgues GE, Johnston PS, Pepe MD, Tucker BS, Ramsey ML,Austin LS: Hemiarthroplasty versus reverse total shoulder arthroplasty for acute proximal humerus fractures in elderly patients. Orthopedics 2012;35(5):e703-e708.
28. Matsoukis J, Tabib W, Guiffault P, et al: Primary unconstrained shoulder arthroplasty in patients with a fixed anterior glenohumeral dislocation. J Bone Joint Surg A m 2006;88(3):547-552.
29. Wooten C, Klika B, Schleck CD, Harmsen WS, SperlingJW, Cofield RH: Anatomic shoulder arthroplasty as treatment for locked posterior dislocation of the shoulder. J Bone Joint Surg Am 2014;96(3):el9.
30. Cadet ER, Ahmad CS: Hemiarthroplasty for three- and four-part proximal humerus fractures. ] A m Acad Orthop Surg 2012;20(l):17-27.
31. Nho SJ, Brophy RH, Barker JU, Cornell CN, MacGillivray JD: Innovations in the management of displaced proximal humerus fractures. J A m Acad Orthop J»rg2007;15(l):12-26.
32. VoosJE, Dines JS, Dines DM: Arthroplasty for fractures of the proximal part of the humerus. / Bone Joint Surg Am 2010;92(6):1560-1567.
33. Hertel R, Hempfing A, Stiehler M, Leunig M: Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus./ Shoulder Elbow Surg 2004;13(4):427-433.
34. Williams M, Stanley R, Cores Z, Edwards T, Elkousy H, Gartsman G: Reverse total shoulder arthroplasty as treatment for fixed anterior shoulder dislocation. Presented at the 10th International Congress on Surgery of the Shoulder. LaBahia Salvador, Brazil, September 16-20, 2007.
35. Loew M, Heitkemper S, Parsch D, Schneider S, Rickert M: Influence of the design of the prosthesis on the outcome after hemiarthroplasty of the shoulder in displaced fractures of the head of the humerus./ Bone Joint Surg Br2006;88(3):345-350.
36. Aaron D, Parsons BO, Sirveaux F, Flatow EL: Proximal humeral fractures: Prosthetic replacement. Instr Course Led 2013;62:155-162.
37. Gallinet D, Clappaz P, Garbuio P, Tropet Y, Obert L: Three or four parts complex proximal humerus fractures: Hemiarthroplasty versus reverse prosthesis. A comparative study of 40 cases. Orthop Traumatol Surg Res 2009;95(l):48-55.
38. Young SW, Segal BS, Turner PC,Poon PC: Comparison of functional outcomes of reverse shoulder arthroplasty versus hemiarthroplasty in the primary treatment of acute proximal humerus fracture. A N Z J Surg 2010;80(11):789-793.
39. Namdari S, Horneff JG, Baldwin K: Comparison of hemiarthroplasty and reverse arthroplasty for treatmentof proximal humeral fractures: A systematic review. J Bone Joint Surg Am 2013;95(18):1701-1708.
40. Mata-Fink A, Meinke M, Jones C,Kim B, Bell JE: Reverse shoulder arthroplasty for treatment of proximal humeral fractures in older adults: A systematic review. / Shoulder Elbow Surg 2013;22(12):1737-1748.
41. Cazeneuve JF, Cristofari DJ: Gram- mont reversed prosthesis for acute complex fracture of the proximal humerus in an elderly population with 5 to 12 years follow-up. Rev Chir Orthop Reparatrice Appar Mot 2006;92(6):543-548.
42. Klein M, Juschka M, Hinkenjann B, Scherger B, Ostermann PA: Treatment of comminuted fractures of the proximal humerus in elderly
178 © 2016 AAOS Instructional Course Lectures, Volume 65

Reverse Shoulder Arthroplasty for Trauma: When, Where, and How Chapter 11
patients with the Delta III reverse shoulder prosthesis. J Orthop Trauma 2008;22(10):698-704.
43. Lenarz C, Shishani Y, McCrum C, Nowinski RJ, Edwards TB, Gobezie R: Is reverse shoulder arthroplasty appropriate for the treatment of fractures in the older patient? Early observations. Clin Orthop RelatR.es 2011;469(12):3324-3331.
44. Nowinski RJ, Gillespie RJ, Shishani Y, Cohen B, Walch G, Gobezie R: Antibiotic-loaded bone cement reduces deep infection rates for primary reverse total shoulder arthroplasty:A retrospective, cohort study of
501 shoulders. J Shoulder Elbow Surg 2012;21(3):324-328.
45. Boileau P, Walch G, Krishnan SG: Tuberosity osteosynthesis and hemiarthroplasty for four-part fractures of the proximal humerus. Techniques in Shoulder and Elbow Surgery 2000;1(2):96-109.
46. Sirveaux F, Navez G, Roche O, Mole D, Williams MD: Reverse prosthesis for proximal humerus fracture: Technique and results. Techniques in Shoulder and Elbow Surgery 2008;9(l):15-22.
47. Boileau P, Rumian A: The doubled- suture Nice knot: A non-slipping and secure fixation of bone fragments
and soft tissues usable in open and arthroscopic surgery, in Boileau P, ed: Shoulder Concepts 2010: Arthroscopy and Arthroplasty. Montpellier, Frances, Sauramps Medical, 2010, pp 245-251.
Video ReferenceSzerlip BW, Morris BJ, Edwards TB: Video. Reverse Shoulder Arthroplasty for Trauma: When, Where, and How. Houston, TX, 2015.
©2016 AAOS Instructional Course Lectures, Volume 65 179

Copyright of Instructional Course Lectures is the property of Lippincott Williams & Wilkinsand its content may not be copied or emailed to multiple sites or posted to a listserv withoutthe copyright holder's express written permission. However, users may print, download, oremail articles for individual use.