Embed Size (px)
DESCRIPTION
Cell Wall Synthesis Inhibitors
Citation preview

Cell wall synthesis inhibitors
Giuseppe A BottaDileep K. Rohra
POD Block, Semester 32014-15

Learning Objectives• Classify the cell wall synthesis inhibitors.• Discuss the structure-activity relationship of b lactam
antibiotics.• Revisit the physiology of cell wall synthesis and
explain the mechanism of action of b lactam antibiotics and vancomycin.
• Describe the mechanisms of drug resistance against b lactam antibiotics.
• Discuss the role of b lactamase inhibitors in combination with b lactam antibiotics.
• Describe the clinical uses and adverse effects of b lactam antibiotics and vancomycin.

Classification of Antibiotics• Cell wall synthesis inhibitors:• b-lactam drugs (Penicillins, Cephalosporins,
Carbapenems, Monobactams), Vancomycin• Protein synthesis inhibitors:
• Aminoglycosides, Chloramphenicol, Tetracyclines, Macrolides, Clindamycin, Linezolid
• Nucleic acid synthesis inhibitors:• Fluoroquinolones
• Antimetabolites:• Sulfonamides, Trimethoprim

Cell wall synthesis inhibitors: Classification

β-Lactam Antibiotics
• Penicillins• Cephalosporins • Carbapenems• Monobactams

C NH CH CH C
O
O C N CH
CH3
CH3COOH
S
Penicillin: Structure
Thiozolidineb-lactam
Cell Wall synthesis• Cell walls of bacteria are essential for their
normal growth & development.• Peptidoglycan is a heteropolymeric
component of the cell wall that provides rigid mechanical stability by virtue of its highly cross-linked latticework structure.
• The peptidoglycan is composed of glycan chains, which are linear strands of two alternating amino sugars (N-acetylglucosamine and N-acetylmuramic acid) that are cross-linked by peptide chains. (NAG-NAM).

Bacterial cell wall synthesis


b lactams: Mechanism of action• It is this last step in peptidoglycan
synthesis that is inhibited by the b lactam antibiotics.
• Beta lactams bind at the active site of the transpeptidase enzyme (PBPs) that cross-link the peptidoglycan strands.
• Beta lactams irreversibly inhibit the enzyme transpeptidase by reacting with a serine residue.

b lactams: Mechanism of action
• Eventually, the growth of the bacterial cell wall is inhibited.
• In the presence of b lactams, autolysins are also released causing the lysis of the bacteria.

Inhibitory effects of b lactams on bacterial cell
wall

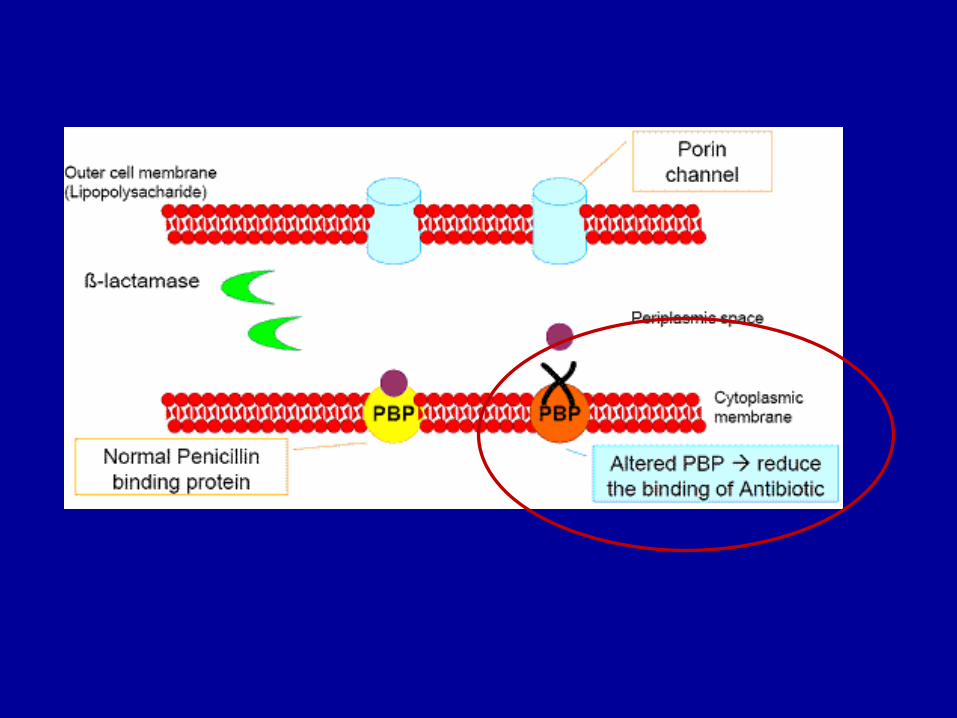
Mechanisms of bacterial resistance to penicillins
Resistance to penicillins & other b lactams is due to one of four general mechanisms:• Inactivation of the antibiotic by b
lactamase• Modification of target PBPs• Impaired penetration of drug to target
PBPs

C NH CH CH C
O
O C N CH
CH3
CH3COOH
S
Site of penicillinase action
Penicillin: Structure
Thiozolidineb-lactam
• Natural penicillins:– Benzylpenicillin; Gm +ves, anaerobes &
selected Gm –ves• Penicillinase resistant penicillins:
– Flucloxacillin, Cloxacillin; penicillin-resistant staphylococci. Also active against streptococci
• Aminopenicillins (extended-spectrum):– Amoxycillin, Ampicillin; as for penicillin G
+ Gram –ve cocci, & Enterobacteriaceae.
Penicillins: Classification
• Carboxypenicillins:– Carbenicillin, ticarcillin; as for
aminopenicillins + Gm –ve rods resistant to ampicillin, including P. aeruginosa.
• Ureidopenicillins:– Piperacillin; similar to carboxypenicillins
Penicillins: Classification

Mechanisms of bacterial resistance to penicillins
Resistance to penicillins & other b lactams is due to one of three general mechanisms:• Inactivation of the antibiotic by b
lactamase• Modification of target PBPs• Impaired penetration of drug to target
PBPs• The presence of an efflux pump

β-Lactamase Inhibitors
• Clavulanic acid, Sulbactam, Tazobactam
• Weak, unimportant antibacterial activity
• Powerful irreversible inhibitor of b-lactamases - suicide substrate
β-lactam/Inhibitor combinations
• Ampicillin + Sulbactam = Unasyn• Amoxicillin + Clavulanic acic =
Augmentin• Piperacillin + Tazobactam = Zosyn

Penicillins: Clinical uses
• Bacterial meningitis:– Caused by N meningitidis, S pneumoniae;
Benzylpenicillin• Bone & joint infections:
– E.g with Staph aureus; Flucloxacillin• Skin & soft tissue infections:
– E.g with S pyogenes or Staph aureus; Flucloxacillin• Pharyngitis:
– S pyogenes; phenoxymethylpenicillin
Penicillins: Clinical uses• Otitis media:
– E.g. with S pyogenes or H influenzae; Amoxicillin
• Bronchitis:– Amoxicillin
• UTIs:– Amoxicillin
• Infections with P aeruginosa:– Ticarcillin, Pipercillin

Penicillins: Adverse effects• Hypersensitivity Reactions:
– Most common adverse effects noted with the penicillins.
– Manifestations of allergy to penicillins include maculopapular rash, urticarial rash, fever, bronchospasm, vasculitis, serum sickness, exfoliative dermatitis, Stevens-Johnson syndrome, & anaphylaxis
– The overall incidence of such reactions to the penicillins varies from 0.7% to 10% in different studies
• Rarely, bone marrow depression, granulocytopenia, & hepatitis
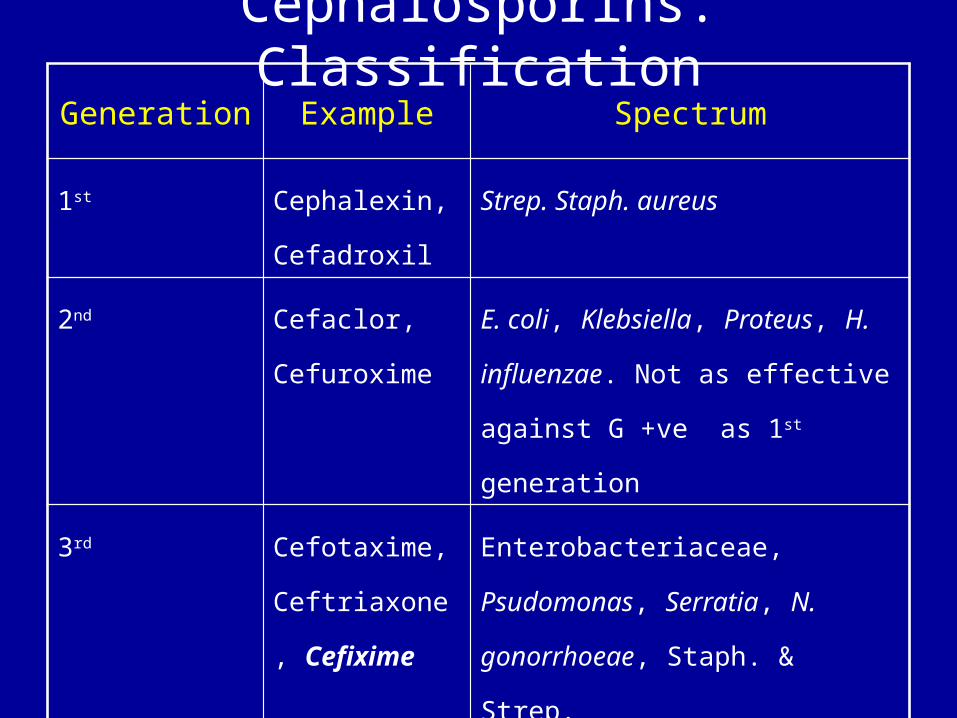
Cephalosporins: ClassificationGeneration Example Spectrum
1st Cephalexin, Cefadroxil
Strep. Staph. aureus
2nd Cefaclor, Cefuroxime
E. coli, Klebsiella, Proteus, H. influenzae. Not as effective against G +ve as 1st generation
3rd Cefotaxime, Ceftriaxone, Cefixime
Enterobacteriaceae, Psudomonas, Serratia, N. gonorrhoeae, Staph. & Strep.
4th Cefepime, Comparable to 3rd generation but more resistant to some b-lactamases & greater activity against Gm +ve

Carbapenems
• Imipenem• Meropenem

Imipenem• Imipenem is always co-
administered with Cilastin; an inhibitor of renal dehydropeptidase I - enzyme responsible for hydrolysis of imipenem. Does increase the duration of action of Imipenem.
• Active against most clinically important bacteria including anaerobes.
• Not destroyed by most b lactamases

• Administere only IV• Adverse effects (Relatively
infrequent):– Phlebitis or pain at site of injection– Nausea, Vomiting– Fits (usually with pre-existing CNS
disease)
Imipenem
Monobactams: Aztreonam• Primarily active against aerobic Gram-
negative organisms • Used in severe sepsis, often hospital
acquired, especially infections of the respiratory, urinary, biliary, gastrointestinal & female genital tracts.
• Has a narrow spectrum of activity & cannot be used alone unless the organism´s sensitivity to aztreonam is known.
• Adverse effects include Rashes

…but in 1983…

But in 2008…,

Mechanisms of bacterial resistance to penicillins
Resistance to penicillins & other b lactams is due to one of three general mechanisms:• Inactivation of the antibiotic by b
lactamase• Modification of target PBPs• Impaired penetration of drug to target
PBPs


• So what?
Vancomycin
• Vancomycin inhibits bacterial cell wall synthesis by inhibiting peptidoglycan polymerization at a step earlier than that inhibited by the b lactams.
• It is effective mainly against MRSA.
• Vancomycin is not absorbed from the gut, & is usually given as an intravenous infusion.
Vancomycin: Adverse effects
• Hearing loss• Venous thrombosis at infusion
site• “Red man” syndrome due to
cytokine/histamine release following rapid intravenous administration
• Hypersensitivity: rashes etc.• Nephrotoxicity





























