Embed Size (px)
Citation preview

Opioid Withdrawal in Critically Ill Adults
A Retrospective Study to Identify at Risk Patients
Primary Investigator: Raymond Melika, PharmD, RPh
Supervisor:
Lisa Burry, BScPharm, PharmD, FCCP, FCCM
Collaborators:
Alexandra Cheung, BSc, BScPharm, PharmD, RPh
Jennifer Korman, BScPharm, ACPR, RPh
May Musing, BScPharm, RPh
1

Acknowledgements
I would like to acknowledge the truly tireless hard work of Andrew Wyllie, Christinne Duclos, Winnie Seto and Virginia Fernandes; a team which, without, I could not have overcome the obstacles presented by this study.
2

TABLE OF CONTENTS
1: Abbreviations...............................................................................................................................4
2: Abstract........................................................................................................................................5
3: Background..................................................................................................................................7
4: Methods.......................................................................................................................................9
4.1: Design...................................................................................................................................9
4.2: Patients..................................................................................................................................9
4.3: Procedures...........................................................................................................................10
4.4: Statistical Analysis..............................................................................................................11
5: Results.......................................................................................................................................11
5.1: Population...........................................................................................................................12
5.2: Outcomes............................................................................................................................12
6: Discussion..................................................................................................................................13
7: Conclusion.................................................................................................................................17
8: References.................................................................................................................................19
9: Figures.......................................................................................................................................23
9.1: Figure 1: Study Flowchart..................................................................................................23
9.2: Figure 2: Schematic of Patient Chart Assessment..............................................................24
9.3: Figure 3: Symptom Documentation Frequency..................................................................25
9.4: Figure 4: Daily Clonidine, Dexmedetomidine, and Propranolol Administration...............26
9.5: Figure 5: Daily Acetaminophen, NSAID, and Antipsychotic Administration...................27
9.6: Figure 6: Daily Benzodiazepine and Propofol Administration...........................................28
10: Tables.......................................................................................................................................29
10.1: Table 1: Baseline Patient Demographics..........................................................................29
10.2: Table 2: Daily Opioid Dose Changes...............................................................................30
10.3: Table 3: Symptom Documentation Frequency on Each Day............................................31
11: Appendix.................................................................................................................................32
11.1: Protocol for the Collection of Data...................................................................................32
11.2: Comparison of Opioid Withdrawal Assessments.............................................................34
11.3: Opioid and Benzodiazepine Dosing Equivalence.............................................................35
3

1: Abbreviations
COWS: Clinical Opiate Withdrawal Scale
CPOT: Critical Pain Observation Tool
DSM: Diagnostic and Statistical Manual of Mental Disorders
GCS: Glasgow Coma Scale
ICU: Intensive Care Unit
IOWS: Iatrogenic Opioid Withdrawal Syndrome
LOS: Length of Stay
NRS: Numerical Rating Scale
OBWS: Opioid and Benzodiazepine Withdrawal Score
PTSD: Post-Traumatic Stress Disorder
SAS: Riker Sedation-Agitation Scale
SOS: Sophia Observation and Withdrawal Symptoms Scale
WAT-1: Withdrawal Assessment Tool – Version 1
4

2: Abstract
Background: The incidence of opioid withdrawal and associated symptoms in critically ill adults has
not been adequately studied. The lack of dedicated scales for the detection of iatrogenic opioid
withdrawal syndrome (IOWS) in critically ill adults represents a gap in the literature.
Objectives: To 1) determine the feasibility of identifying patients at risk of IOWS for a future study
evaluating IOWS in critically ill adults 2) determine the frequency of documentation of potential
signs and symptoms of IOWS; 3) determine patterns of opioid doses used in critically ill adults.
Methods: A retrospective chart review of critically ill adults (aged ≥ 18 years) who received
regularly administered opioids for at least 72 hours in the ICU. Patient charts were reviewed for
documentation of signs and symptoms of opioid withdrawal using a checklist of 17 symptoms
developed from a review of the literature. Feasibility was defined as the ability to include 20 subjects
in 1 year.
Results: One thousand, one hundred and eighteen subjects were screened between December 2016
and December 2017. Twenty-eight subjects were included. The median age was 65 years. Male sex
comprised 61% of subjects. The most common reason for exclusion was not receiving scheduled
opioids in ICU for ≥ 72 hours (91.7%.) The most commonly documented symptom was a ≥ 15%
variance in respiratory rate (92.5% frequency of documentation). Documentation of the absence of
symptoms was rare (< 1%). The symptoms least commonly documented were piloerection and
lacrimation (0% frequency of documentation, respectively). Median daily opioid dose changes were
+ 13%, - 5%, -19% and -22% on days 2, 3, 4 and 5, respectively. The most frequently used opioids
were IV Fentanyl, IV Hydromorphone, and Oral Hydromorphone, representing 70.1%, 42.5%, and
21.6% of patient days, respectively.
5

Conclusions: In identifying 28 patients at risk of IOWS, our findings demonstrate the feasibility
identifying patients at risk of IOWS for a future study evaluating IOWS in critically ill adults. Data
on the frequency of documentation of 17 symptoms suggest a wide range of documentation
frequency and may inform the choice of symptoms assessed in future studies of IOWS. Our data
identified 20% dose reductions beginning on day 4, which informs a standardized dose reduction to
be tested in an interventional study.
6

3: Background
Critically ill patients often require analgesia with opioids to manage the pain associated
with procedures and the use of supportive care devices. Beyond patient comfort, analgesia-first
strategies (as opposed to sedation-first) are increasingly important in the prevention of negative
patient outcomes, including PTSD, agitation and delirium.1,2 Canadian literature indicates that
opioids are prescribed to greater than 90% of ICU patients.3 Furthermore, the total days of opioid
exposure represents 90% of ICU patient-days.3
Prolonged opioid exposure results in tolerance, which manifests clinically as an increased
need for opioid dose or opioid frequency to achieve therapeutic effects, as well as physiological
dependence.4 Once patients become tolerant to opioids and physiologic dependence is exhibited,
Iatrogenic Opioid Withdrawal Syndrome (IOWS) can be precipitated with either abrupt
discontinuation of therapy or active reversal with opioid receptor antagonists or partial
agonists.5,6
IOWS symptoms in both non-critically ill adults and critically ill pediatric patients have
been described in the literature to include central nervous system hyperirritability, autonomic
system dysregulation, gastrointestinal dysfunction and motor abnormalities.7,8,9,10,11
Several scales have been validated to assess the severity of IOWS in children and non-
critically ill adults, including CINA8, SOWS9, SOWS-Gossops10 and COWS11. The Diagnostic
and Statistical Manual of Mental Disorders, 5th edition (DSM V) indicates that 3 or more of the
following symptoms must be present to diagnose opioid withdrawal syndrome: dysphoric mood,
nausea or vomiting, muscle aches, lacrimation or rhinorrhea, pupillary dilation, piloerection, or
sweating, diarrhea, yawning, fever, insomnia.6 These symptoms have not, however, been
7

integrated into a validated tool for assessment of IOWS in the adult ICU. Given the ubiquity of
therapeutic and pathological sedation and paralysis in the ICU, the reliance on subjective patient-
reported symptoms in these scales limits the utility of these tools in the ICU.
In critically ill children two tools have been specifically developed and validated to
assess opioid withdrawal: WAT-112 and SOS scale.13 These assessment tools cannot be
generalized to the adult population, given anticipated differences in manifestations of withdrawal
between children and adults such as inconsolable crying and startle to touch (Appendix 11.2). A
recent assessment of the applicability of the WAT-1 in critically ill adults found a specificity of
0.7, and a sensitivity of only 0.5.14 Despite the association between IOWS in pediatric ICU
patients and adverse clinical outcomes (e.g. prolonged ICU length of stay [LOS]12 and duration
of mechanical ventilation15) the risk factors for, and incidence of, IOWS in the adult critically ill
population have not been well described.
Despite the presence of dedicated scales in both the pediatric ICU population and the
non-critically ill adult population, the lack of dedicated scales for the detection of IOWS in
critically ill adults is a gap in the literature. We conducted a literature review to identify
symptoms used in the assessment of opioid withdrawal in the pediatric ICU (SOS13, WAT-112)
and adult non-ICU population (DSM-V6, and COWS11). We identified 17 symptoms (Appendix
11.2). Our objectives of this study are to 1) determine the feasibility of identifying patients at risk
of IOWS for a future study evaluating IOWS in critically ill adults 2) determine the frequency of
documentation of potential signs and symptoms of IOWS; 3) determine patterns of opioid doses
used in critically ill adults.
8

4: Methods
4.1: Design
We conducted a retrospective chart review in the medical-surgical ICU of Mount Sinai
Hospital, Sinai Health System. Patient enrollment occurred between December 2016 and
December 2017. The study protocol was reviewed and approved by the Research Ethics Board of
the hospital (MSH REB #18-0038-C).
4.2: Patients
Patients were included if they were admitted to the ICU, aged at least 18 years old, and
received scheduled opioids for at least 72 hours in the ICU. We used 72 hours as the cut-off due
to a previous study describing IOWS after as little as three days of exposure.2 We also included
patients ordered “as-needed” doses who received more than half of the daily permitted doses. A
convenience benchmark “half of the daily permitted doses” was used, following a previous
study2, and in order to capture a larger sample size.
We excluded the following patients: self-reported exposure to opioids in the 90 days prior
to admission (determined from outpatient medication list); receiving opioids in the ICU
administered exclusively spinally; severe brain injury (defined as GCS of 8 or less on admission
to the ICU); palliative on ICU admission; admission to the ICU with substance overdose or acute
alcohol withdrawal syndrome.
Given the sample sizes used in studies for the development of withdrawal scales in the
pediatric ICU such as OBWS16 (n=15), SOS13 (n=79), and WAT-112 (n=83), and considering a
study by Perrault et al.17 which included 54 adult patients from two ICUs over an enrollment
9

period of eight months, we defined feasibility as the ability to include a convenience sample 20
subjects from one site in one year.
4.3: Procedures
Patients meeting the above-mentioned inclusion, and not meeting the exclusion criteria,
were then assessed against the 17 symptoms derived from a review of the literature (Appendix
11.2) to determine the frequency of the documentation of these symptoms in the population of
interest. Once patients were enrolled, demographic information was collected using a
standardized case report form in Microsoft Excel (Microsoft Office 365 [2016], Version 1810,
Build 11001.20108). Baseline data collected included: age, sex, height, weight, date of hospital
and ICU admission and discharge, reason for ICU admission, mechanical ventilation (% of
patients mechanically ventilated and duration of mechanical ventilation), alcohol abuse (defined
as ≥2 drinks per day and/or ≥14 drinks per week in men and ≥9 drinks per week for women2),
smoking history, illicit substance history (such as cocaine or non-medicinal marijuana use at the
time of admission), medical comorbidities, and ever use of physical restraints during ICU
admission. Given the uncertainty/ambiguity of risk factors for, and consequences of IOWS, these
data were collected due to their anticipated availability and ubiquity in similar studies and for
potential investigation in future studies.
Beginning on the first day on which each patient received regular opioids for at least 12
hours of the day [referred to as “Day 1”]) each patient’s archived ICU nursing record was
reviewed for documentation daily of the 17 signs and symptoms. Symptoms were scored as
present, absent, or not documented (Appendix 11.1). Daily assessment for symptom
documentation continued until the patient died, was transferred out of the ICU, or until 5 days of
assessment had been completed – whichever came first (Figure 2). A convenience period of 5
10

days was chosen. Other daily data collected from the daily ICU nursing records included
Numerical Rating Scale (NRS) pain scores, Critical Care Pain Observation Tool (CPOT) scores,
Riker Sedation-Agitation Scale (SAS) scores, and Intensive Care Delirium Screening Checklist
(ICDSC) scores.
Daily doses of opioids and benzodiazepines were also collected, both from patient
electronic medical records (e-MAR) as well as from the daily ICU nursing flowsheets. All doses
of opioids and benzodiazepines were converted to fentanyl and midazolam equivalents,
respectively18–20 (Appendix 11.3). Data on the use of co-analgesics (acetaminophen, non-steroidal
anti-inflammatory drugs; NSAIDs) and other sedatives (antipsychotics, propofol,
dexmedetomidine, clonidine, and propranolol) were also collected.
4.4: Statistical Analysis
Descriptive statistics were applied to the data. Median daily opioid doses were calculated
for each day, and the percentage change from one day to the next. Descriptive data are expressed
as absolute values and/or percentages. Continuous data are expressed as medians and ranges
except where otherwise specified. The frequency of documentation of a symptom is expressed as
the proportion of “present,” “absent” and “not documented” designations for each symptom
across the total number of patient days included in this study. Listwise deletion (a method in
which missing data are omitted from the analysis of the variable of interest21) was used for
missing data. Statistical analysis was performed by the primary investigator using Microsoft
Excel (Microsoft Office 365 [2016], Version 1810, Build 11001.20108).
5: Results
11

5.1: Population
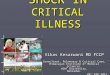
During the selected study period there were 1,018 patient admissions. After 30 patients
were included in this study, two patients were found to have been included in error. Thus, 28
patients met our predefined inclusion criteria and did not meet exclusion criteria (Figure 1). The
main reasons for exclusion were regular administration of opioids in the ICU for less than 72
hours (n = 933), self-reported exposure to opioids in the 90 days prior to admission (n = 26) and
severe brain injury on admission (n = 22). The eligibility of seven patients could not be
determined due to missing outpatient medication reconciliation data (n=4) and/or patient records
explicitly locked against access for research purposes (n=3).
Male sex represented 61% of the study population; the median age was 65 years (range
26 – 88) (Table 1). The majority of patients were admitted to the ICU for sepsis or hypoxia or
respiratory failure (53.4%, cumulatively). Mechanically ventilated patients represented 83.9% of
the study population. The median duration of mechanical ventilation was 7 days (range 1-112
days). Three patients had alcohol use disorder, and one patient had documented history of
intravenous cocaine use.
5.2: Outcomes
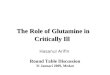
The symptoms most commonly documented as present were a ≥ 15% variance in
respiratory rate between peak and trough rate (92.5% frequency of documentation) and a ≥ 15%
variance pulse between peak and trough rate (88.1% frequency of documentation) (Figure 3).
While reasons may vary, documentation of the absence of symptoms was rare (< 1%).
Piloerection, muscle aches, and persistent yawning were never documented in the charts. The
frequency of documentation of symptoms ranged from 0% to 92.5% (Figure 9.3, Table 10.3).
12

Median changes in total daily opioid dose are represented in Table 2, illustrating a
roughly 20% decrease on days 4 and 5 of regular opioid administration. Median daily opioid
dose changes were + 13%, - 5%, -19% and -22% on days 2, 3, 4 and 5, respectively. The most
frequently used opioids were IV fentanyl, IV hydromorphone, and oral hydromorphone,
representing 70.1%, 42.5%, and 21.6% of patient days, respectively. The frequency of symptom
documentation on each respective day is presented in Table 3. No appreciable increase in the
frequency of symptom documentation was demonstrated following dose reductions.
Data on the use of dexmedetomidine, clonidine, and propranolol as well as
acetaminophen, NSAIDs, and antipsychotics are depicted in Figures 4 and 5, respectively. The
number of patients administered benzodiazepines and/or propofol on each day is presented in
Figure 6. The number of patients using either of these medications declines with each successive
day.
6: Discussion
This study’s inclusion of 28 patients met our pre-specified criteria for feasibility of
identifying patients at risk of IOWS. The main reason for study exclusion was not receiving
regular opioids in the ICU for at least 72 hours. This reflects similar findings in a previous
study.2 A more liberal inclusion of “as needed” opioids would increase the number of patients
included in the study, but may have captured a population at a lower risk for IOWS. Given a
potential association between higher doses of opioids, and incidence of IOWS22, future studies
may consider identifying patients at risk of IOWS not merely on the basis of frequency of
administration of the “as needed” doses, but also on the basis of cumulative daily dose.
13

The second most common reason for exclusion was self-reported exposure to opioids in
the 90 days prior to admission. To reduce variability in the sample, patients were excluded if
their home medication list made mention of opioids. Future studies should aim to quantify opioid
exposure prior to hospitalization. This may require linking hospital data to external databases,
the use of provincial/state/federal medication administration records, or directly asking patients.
Documentation of IOWS symptoms was variable. Lacrimation, piloerection, muscle
aches, tremor, rhinorrhea and persistent yawning were rarely documented. The lack of
documentation of these symptoms may represent the ambiguity of their presentation, the
difficulty of their assessment, and may reflect a policy (whether formal or informal) to “chart by
exception”. If included in an opioid withdrawal checklist, these symptoms may increase nursing
workload. Missing data presented difficulty in the analysis of the results. Variable documentation
practices obscure the difference between the lack of documentation indicating absence of a
symptom or indicating a lack of assessment. Listwise deletion was used for missing symptom
data, but no sensitivity analysis was performed on the impact of this deletion. Future studies may
consider such an analysis.
Symptoms such as hallucination, nausea, vomiting, and diarrhea were difficult to
categorize in a retrospective review. While these symptoms were readily documented, the
subjective nature of certain symptoms makes documentation difficult in heavily sedated patients.
These may not be suitable for inclusion in an opioid withdrawal checklist.
The most readily documented symptoms are those with explicit documentation prompts
(such as check boxes, temperature recording boxes, etc.) on the standard daily nursing ICU
flowchart and which are not sensitive to level of sedation. Frequent daily documentation of SAS,
temperature, heart rate and respiratory rate allow for easy data collection. Though tachycardia
14

and tachypnea (as opposed to bradycardia and bradypnea) are the symptoms of interest in IOWS,
we did not assess for direction of variance in pulse and respiratory rate. We focussed our efforts
on determining whether these existed, before devoting focus to variance. Hallucination and
sleep-wake disturbance are components of the ICDSC score and are readily documented given
that the ICDSC checklist was completed by the nurse. Question 1 of the ICDSC checklist directs
nurses to not complete the ICDSC if the patient can only respond to intense repeated stimulation
or if the patient cannot respond to noxious stimulation. Thus, in heavily sedated or paralyzed
patients, the ICDSC checklist is not completed by a nurse, limiting its documentation frequency.
Since these symptoms are not frequently documented in heavily sedated or paralyzed patients,
their inclusion in an IOWS checklist would limit the utility of such a checklist to patients for
whom an ICDSC checklist assessment could be completed.
Decreases in total mean daily opioid dose were approximately 20% beginning on day 4 of
regular intermittent or continuous opioid administration. While there are no evidence-based
recommendations for opioid weaning in the adult ICU, this decrease is aligned with common
practices in the pediatric ICU.23 Using 72-hours as the of scheduled opioids as the cut-off for
inclusion into the study may have limited the ability to detect the emergence of IOWS as the
duration of opioid administration that predisposes a patient to IOWS is still unclear. Future
studies may benefit from investigation and validation of this 72-hour cut-off. While sedative
data was collected (such as benzodiazepine, and propofol), the small sample of patients using
these sedatives makes an analysis inappropriate. Future investigators may require a much larger
sample size in order to warrant an analysis.
A limitation of this study is its retrospective design, leading to uncertainty in categorizing
target symptoms into “present”, “absent” and “not documented”. The subjective nature of some
15

symptoms, variable nurse documentation practices, and potential for documentation error
decreases the internal validity of the study. In order to standardize the data collection process and
to support reproducibility of the results, stringent definitions were followed (Appendix 11.1) for
coding of symptoms. It is possible that categorizing these symptoms resulted in
oversimplification and may not accurately reflect the spectra of a patient’s clinical presentation.
Relying on a twice-daily prompt on the standard daily nursing ICU flowchart to reflect a
patient’s clinical presentation over a 24-hour period compromises accuracy. Nevertheless, while
this risks inaccurate documentation of symptom presentation, it reflects the nature of clinical
practice where an assessment is made as a snapshot and may not accurately reflect the
unobserved experiences of the patient.
Our data may be sensitive to the inclusion of patients receiving 72 hours of regular
opioids, and the use of half of scheduled as-needed doses as the threshold for “regular opioid.”
Future studies may consider sensitivity-testing the effect of these thresholds. In order to readily
assess exclusion criteria, patients were excluded if their home medication list made mention of
opioids. This may have limited the inclusion of patients who used opioids sparingly in the
outpatient setting, as opposed to chronic opioid use only. Future prospective studies may benefit
from quantifying the amount of opioid use prior to admission or using a sensitivity analysis to
assess the effect of excluding these patients. Data is also sensitive to nursing documentation
practices. For instance, sweating was assumed to be documented absent if “diaphoretic” was not
checked off, whether or not the nurse checked off the box for “skin dry.” Future studies may
consider a sensitivity analysis to determine the effect of this and other such assumptions
(Appendix 11.1).
16

In our study we noted variable documentation practices and were challenged to properly
interpret missing data. Patients who were sedated due to their condition or therapeutically
sedated could not express or be monitored for some symptoms, reducing the opportunity to
record symptoms such as nausea and hallucinations. These observations should direct future
researchers to isolate indicators of withdrawal which can be reliably collected – either through
prospective collection, or by mandatory documentation at regular intervals, and manifest
irrespective of the level of sedation of the patient. This will ensure that a complete and accurate
set of indicators be available for scoring. With their availability, the strength of association to
exposure to opioids can be determined and assessed for appropriateness in a tool for predicting
opioid withdrawal.
This study was also illuminating on documentation practices, interpretation of
documentation, and construction of clinical predictive tools. Specifically, in attempting to
isolate symptoms for a predictive tool, the study highlights the importance of consistent
documentation practices, impaired ability of the ICU patient to communicate symptoms, limited
ability of the staff to observe subjective patient experiences, and failing those, the limited ability
to determine the influence of confounding factors on the presence or absence of symptoms. The
use of a prospective design in future studies exploring IOWS may support more robust execution
of exclusion criteria, as well as standardized nursing documentation practices, and prompted
assessment of the symptoms of interest.
7: Conclusion
Our findings demonstrate the feasibility of identifying patients at risk of IOWS for a
future study assessing IOWS in critically ill adults. Data on the frequency of documentation of
17 symptoms suggest a wide variability of obtainability and frequency and may inform the
17

choice of symptoms assessed in future larger prospective studies of IOWS. Median daily opioid
dose changes were + 13%, - 5%, -19% and -22% on days 2, 3, 4 and 5, respectively. The most
frequently used opioids were IV fentanyl, IV hydromorphone, and oral hydromorphone, representing
70.1%, 42.5%, and 21.6% of patient days, respectively.
18

8: References
1. Barr J, Fraser GL, Puntillo K, Ely EW, Gélinas C, Dasta JF, et al. Clinical Practice
Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the
Intensive Care Unit: Crit Care Med. 2013 Jan;41(1):263–306.
2. Wang PP, Huang E, Feng X, Bray C-A, Perreault MM, Rico P, et al. Opioid-associated
iatrogenic withdrawal in critically ill adult patients: a multicenter prospective observational
study. Ann Intensive Care [Internet]. 2017 Dec [cited 2018 Oct 29];7(1). Available from:
https://annalsofintensivecare.springeropen.com/articles/10.1186/s13613-017-0310-5
3. Burry LD, Williamson DR, Perreault MM, Rose L, Cook DJ, Ferguson ND, et al.
Analgesic, sedative, antipsychotic, and neuromuscular blocker use in Canadian intensive
care units: a prospective, multicentre, observational study. Can J Anesth Can Anesth. 2014
Jul;61(7):619–30.
4. Masica AL, Girard TD, Wilkinson GR, Thomason JWW, Truman Pun B, Nair UB, et al.
Clinical sedation scores as indicators of sedative and analgesic drug exposure in intensive
care unit patients. Am J Geriatr Pharmacother. 2007 Sep;5(3):218–31.
5. Best KM, Boullata JI, Curley MAQ. Risk Factors Associated With Iatrogenic Opioid and
Benzodiazepine Withdrawal in Critically Ill Pediatric Patients: A Systematic Review and
Conceptual Model*. Pediatr Crit Care Med. 2015 Feb;16(2):175–83.
6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders
[Internet]. Fifth Edition. American Psychiatric Association; 2013 [cited 2018 Oct 29].
Available from: https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596
19

7. Tetrault JM, O’Connor PG. Substance Abuse and Withdrawal in the Critical Care Setting.
Crit Care Clin. 2008 Oct;24(4):767–88.
8. Peachey JE, Lei H. Assessment of Opioid Dependence with Naloxone. Addiction. 1988
Feb;83(2):193–201.
9. Bradley BP, Gossop M, Phillips GT, Legarda JJ. The Development of an Opiate
Withdrawal Scale (OWS). Addiction. 1987 Oct;82(10):1139–42.
10. Vernon MK, Reinders S, Mannix S, Gullo K, Gorodetzky CW, Clinch T. Psychometric
evaluation of the 10-item Short Opiate Withdrawal Scale-Gossop (SOWS-Gossop) in
patients undergoing opioid detoxification. Addict Behav. 2016 Sep;60:109–16.
11. Wesson DR, Ling W. The Clinical Opiate Withdrawal Scale (COWS). J Psychoactive
Drugs. 2003 Jun;35(2):253–9.
12. Franck LS, Harris SK, Soetenga DJ, Amling JK, Curley MAQ. The Withdrawal
Assessment Tool–1 (WAT–1): An assessment instrument for monitoring opioid and
benzodiazepine withdrawal symptoms in pediatric patients*: Pediatr Crit Care Med. 2008
Nov;9(6):573–80.
13. Ista E, van Dijk M, de Hoog M, Tibboel D, Duivenvoorden HJ. Construction of the Sophia
Observation withdrawal Symptoms-scale (SOS) for critically ill children. Intensive Care
Med. 2009 Jun;35(6):1075–81.
20

14. Chiu AW, Contreras S, Mehta S, Korman J, Perreault MM, Williamson DR, et al.
Iatrogenic Opioid Withdrawal in Critically Ill Patients: A Review of Assessment Tools and
Management. Ann Pharmacother. 2017 Dec;51(12):1099–111.
15. Ista E, van Dijk M, Gamel C, Tibboel D, de Hoog M. Withdrawal symptoms in critically ill
children after long-term administration of sedatives and/or analgesics: A first evaluation*:
Crit Care Med. 2008 Aug;36(8):2427–32.
16. Franck LS, Naughton I, Winter I. Opioid and benzodiazepine withdrawal symptoms in
paediatric intensive care patients. Intensive Crit Care Nurs. 2004;20:344-351. doi:10.1016/j.
iccn.2004.07.008.
17. Perreault M, Martone A, Sandu PR, et al. Withdrawal assessment in adult ICU patients:
validation of the WAT-1 scale. 37th International Symposium on Intensive Care and
Emergency Medicine. Crit Care. 2017;21(suppl 1):56, [abstract] P277.
18. Pereira, Jose, Otfinowski,Pamela, Hagen,Neil, Bruera,Aduardo, Summers, Nancy. Alberta
Hospice Palliative Care Resource Manual. In: 2nd ed. Division of Palliative Care,
University of Alberta; 2001. p. 20. Available from:
http://www.palliative.org/NewPC/_pdfs/education/ACB%20Hospice%20Palliative
%20Manual.pdf
19. Davies SJC. Clinical Handbook of Psychotropic Drugs, 19th Revised Edition Edited by
AdilVirani, Kalyna Z.Bezchlibnyk-Butler, J. JoelJeffries, Ric M.Procyshyn, Hogrefe
Publishing, Göttingen. Price £53.96, pp 362 + pp 50 printable PDF patient information
sheets. ISBN: Hum Psychopharmacol Clin Exp. 2012 Nov;27(6):632–632.
21

20. Barr J, Zomorodi K, Bertaccini EJ, Shafer SL, Geller E. A double-blind, randomized
comparison of i.v. lorazepam versus midazolam for sedation of ICU patients via a
pharmacologic model. Anesthesiology. 2001 Aug;95(2):286–98.
21. Allison PD. Missing data. Thousand Oaks, Calif: Sage Publications; 2002. 93 p. (Sage
university papers. Quantitative applications in the social sciences).
22. Wang PP, Huang E, Feng X, et al. Iatrogenic withdrawal syndrome due to opioids in
critically ill patients: a multicenter prospective observational study. Poster presented at:
Critical Care Canada Forum; Oct 30, 2016; Toronto, Canada.
23. Galinkin J, Koh JL, COMMITTEE ON DRUGS, SECTION ON ANESTHESIOLOGY
AND PAIN MEDICINE. Recognition and Management of Iatrogenically Induced Opioid
Dependence and Withdrawal in Children. Pediatrics. 2014 Jan;133(1):152–5.
22

9: Figures
9.1: Figure 1: Study Flowchart
23
Patient Charts
Reviewed (n = 28)
57 patients met exclusion criteria : Severe brain injury
(n = 22) Self-reported exposure to
opioids in the 90 days prior to admission (n = 26)
Deemed palliative on admission (n = 0)
Opioid dose exclusively through neuraxial administration (n = 1)
Substance overdose or alcohol withdrawal (n = 1)
Patients whose inclusion/exclusion criteria could not be ascertained due to locked charts(n = 3)
Patients whose inclusion/exclusion criteria could not be ascertained due to incomplete home medication list (n=4)
933 patient records did not meet inclusion criteria:
Patient did not receive regular opioid in ICU for ≥ 72 hours (n = 933)
Patient <18 YOA (n = 0)
Patient records screened between 12/01/2016 and 07/31/2017
(n = 1018)
AbbreviationsICU: Intensive Care UnitYOA: Years of Age

9.2: Figure 2: Schematic of Patient Chart Assessment
24

9.3: Figure 3: Symptom Documentation Frequency
≥ 15% va
rianc
e in p
eak an
d low
est pu
lse
≥ 15% va
rianc
e in p
eak an
d low
est re
spira
tory r
ate
Fever
(sing
le tem
perat
ure ≥ 38
.0 de
grees
Celsius
)
Sweating
Piloere
ction
Lacrim
ation
Rhinorr
hea
Persist
ent Y
awnin
g
Pupil D
ilatio
n
Muscle
Ach
es
Tremor
Anxiet
y/Agit
ation
/Rest
lessn
ess
Halluc
inatio
n
Sleep-W
ake D
isturb
ance
Nausea
Vomitin
g
Diarrhe
a0102030405060708090100
Symptom Documentation Frequency
Present Absent Not Documented
Symptom
Freq
uenc
y (%
)
25

9.4: Figure 4: Daily Clonidine, Dexmedetomidine, and Propranolol Administration
Day 1 Day 2 Day 3 Day 4 Day 50
0.5
1
1.5
2
2.5
3
3.5
ClonidineDexmedetomidinePropranolol
Num
ber o
f Pat
ient
s Rec
eivi
ng D
rug
26

9.5: Figure 5: Daily Acetaminophen, NSAID, and Antipsychotic Administration
Day 1 Day 2 Day 3 Day 4 Day 50
1
2
3
4
5
6
7
8
AcetaminophenNSAIDAntipsychotic
Num
ber o
f Pat
ient
s Rec
eivi
ng D
rug
27

9.6: Figure 6: Daily Benzodiazepine and Propofol Administration
Day 1 Day 2 Day 3 Day 4 Day 50
2
4
6
8
10
12
14
16
18
BenzodiazepinePropofol
Num
ber o
f Pat
ient
s Rec
eivi
ng D
rug
28

10: Tables
10.1: Table 1: Baseline Patient Demographics
29
AbbreviationsICU: Intensive Care UnitYOA: Years of AgeSCr: Serum CreatinineCOPD: Chronic Obstructive Pulmonary DiseaseCKD: Chronic Kidney Disease
Characteristic All subjects (n = 28)Male, n (%) 17 (60.7)Age (years), median (range) 65 (26 – 88)Weight (kg), median (range) 76 (58.2 – 117)Admitting Diagnosis, n (%)
Sepsis / Hypoxia / Respiratory Failure 15 (53.4)Post-Operative 6 (21.4)Other 7 (25.2)
SCr on ICU admission (mmol/L), median (range) 84.5 (33 – 597)Hospital Length of Stay (days), median (range) 22.5 (5 -371)ICU Length of Stay (days), median (range) 12 (3 – 112)Mechanically Ventilated, n (%) 25 (89.2)Duration of Mechanical Ventilation (days), median (%) 7 (1 – 112)Comorbidities, n (%)
Anxiety/Depression 6 (21.4)Epilepsy 1 (4.7)Asthma/COPD 4 (14.2)Heart Failure 4 (14.2)Hypertension 15 (53.6)Diabetes 4 (14.2)Liver Disease 1 (4.7)CKD 2 (9.5)
Ever-use of Physical Restraints, n (%) 15 (53.6)Ever-use of neuromuscular blockade during ICU stay, n (%) 15 (53.6)Admitted from, n (%)
Ward 10 (35.7)Surgery 5 (17.9)Transfer from another institution 7 (25.0)Outpatient 6 (21.4)

10.2: Table 2: Daily Opioid Dose Changes
30
Delta between days Raw Median Change in Total Daily Opioid Dose†
Adjusted* Median Change in Total Daily Opioid Dose
Days 1 and 2 + 12.5% + 12.7% *Days 2 and 3 - 2.5% - 4.7 % *Days 3 and 4 - 19.0 % - 19.0 %Days 4 and 5 - 21.9 % - 21.9 %
* Adjusted for missing opioid dose for one patient on one day within study period. Patient’s opioid dose on said date was omitted from calculation of median dose change from this interval.
† Change in Opioid doses calculated from change in daily fentanyl equivalents.

10.3: Table 3: Symptom Documentation Frequency on Each Day
Documentation Frequency (%)
Symptom Day 1 (28 patient-days)
Day 2 (27 patient-days)
Day 3 (28 patient-days)
Day 4 (28 patient-days)
Day 5 (23 patient-days)
≥ 15% variance in peak and lowest pulse 92.9 100 89.3 82.1 73.9
≥ 15% variance in peak and lowest respiratory rate 100 88.9 96.4 89.3 87.0
Fever (single temperature ≥ 38.0 degrees Celsius) 32.1 28.6 28.6 17.9 17.9
Sweating 3.6 7.1 14.2 3.6 7.1Piloerection 0 0 0 0 0Lacrimation 0 0 0 0 0Rhinorrhea 3.6 0 0 0 0
Persistent Yawning 0 3.7 0 0 0Pupil Dilation 0 3.7 3.6 0 0Muscle Aches 0 0 0 0 0
Tremor 3.6 0 0 0 0Anxiety/Agitation/
Restlessness 46.4 51.9 42.9 39.3 39.1
Hallucination 10.7 14.3 14.3 17.9 2.2Sleep-Wake Disturbance 57.1 70.4 53.6 46.4 56.5
Nausea 10.7 3.7 0 0 0Vomiting 3.6 0 3.6 0 0Diarrhea 7.2 0 0 3.6 8.7
31

11: Appendix
11.1: Protocol for the Collection of Data
Sign / Symptom How to collect
15% variance in RRDifference between highest and lowest number documented on the hourly chart. If ≥ 15%, mark “Present.” Otherwise, mark “Absent.” If no documentation, mark
“Not Documented.”
15% variance in HRDifference between highest and lowest number documented on the hourly chart. If ≥ 15%, mark “Present.” Otherwise, mark “Absent.” If no documentation, mark
“Not Documented.”
Fever Highest number documented on the hourly chart. If ≥ 38.0 degrees Celsius, mark “Present.” Otherwise, mark “Absent.”
Sweating
If sweating box is checked, mark “Present.” If the nursing notes state “sweating” and/or “diaphoretic” or variations thereof, mark “Present.”
If sweating is not checked and the nursing notes do not state “sweating” and/or “diaphoretic” or variations thereof, mark “Absent.”
Piloerection
If “piloerection” and/or “goosebumps” and/or “gooseflesh” are mentioned in the written notes, mark “Present.” If the absence is explicitly noted in the nursing
notes, mark “Absent.” If not mentioned in the nursing notes, mark “Not Documented.”
LacrimationIf the nursing notes state “lacrimation” and/or “tears” are, mark “Present.” If the absence is explicitly noted in the nursing notes, mark “Absent.” If not mentioned
in the nursing notes, mark “Not Documented.”
Rhinorrhea
If the nursing notes state “rhinorrhea” and/or “congestion” and/or “runny nose” and/or “nasal mucus” and/or “nasal secretions,” mark “Present.” If the absence is explicitly noted in the nursing notes, mark “Absent.” If it is not mentioned in the
nursing notes, mark “Not Documented.”
Persistent YawningIf the nursing notes state “yawning,” mark “Present.” If the absence is explicitly noted in the nursing notes, mark “Absent.” If it is not mentioned in the nursing
notes, mark “Not Documented.”
Pupil DilationIn the pupil measurement box, if any reading measures ≥ 4 mm, and the pupil is not reactive, mark “Present.” Otherwise, mark “Absent.” If no documentation is
made regarding pupil size, mark “Not Documented.”
Muscle AchesIf the nursing notes state “muscle aches” and/or “muscle pain”, mark “Present.” If the absence is explicitly noted in the nursing notes, mark “Absent.” If it is not
mentioned in the nursing notes, mark “Not Documented.”
Tremor
If the nursing notes state “tremor” and/or “shaking” and/or “trembling” and/or “twitching,” mark “Present.” If the absence is explicitly noted in the nursing notes, mark “Absent.” If it is not mentioned in the nursing notes, mark “Not
Documented.”Anxiety/Agitation/
Restlessness1) If there is a single SAS reading of 5 or greater, mark “Present.”
2) In the ICDSC score, if anxiety or agitation is circled, mark “Present.”
3) In the mental status exam box of the twice-daily shift assessment, if agitation is checked off or if the nurse writes (anywhere) the words “agitation” or
“anxiety” and/or “restlessness” and/or any variations of those specific verbs, mark “Present.”
32

In the absence of any of the above (and in the written nursing notes), mark “Absent.”
Hallucination
In the ICDSC score, so long as a single question is answered after the two preliminary questions (which dictate whether the scale should be completed or
not) the ICDSC box seal is considered broken.
In such a case, if hallucination is circled, mark “Present.” If hallucination is not circled (and the seal is broken), mark “Absent.”
If the nursing notes state “hallucination” mark hallucination as “present.”
If the ICDSC seal is not broken, and no mention is made in the written nursing notes, mark hallucination as “Not Documented.”
If the patient is neuromuscular blocked and/or sedated to SAS of 1 or 2 for greater than half the day, and there is no positive or negative documentation of
hallucination (as above), mark “Not Documented.”
Sleep-Wake Disturbance
In the ICDSC score, so long as a single question is answered after the two preliminary questions (which dictate whether the scale should be completed or
not) the ICDSC box seal is considered broken.
In such a case, if sleep-wake disturbance is circled, mark “Present.” If sleep-wake disturbance is not circled (and the seal is broken) mark “Absent.” If the
seal is not broken, mark “Not Documented.”
If the nursing notes state “insomnia” and/or “sleep-wake disturbance,” and/or “not sleeping” mark as “Present.”
Nausea
If nausea box is checked, mark “Present.”
If nausea is not checked, mark “Absent.” If the patient is administered any antiemetic medication, mark “Present.”
If the written nursing notes state “nausea,” mark as present.
If the patient is sedated to SAS of 1 or 2 for greater than half the day, and there is no positive or negative documentation of nausea (as above), mark “Not
Documented.”
Vomiting
If vomiting box is checked, mark “Present.” If vomiting is not checked, mark “Absent.”
If the written nursing notes state “vomiting” and/or “vomit,” mark “Present”.
Diarrhea
If diarrhea box is checked, mark “Present.” If diarrhea is not checked, mark “Absent.”
If the written nursing notes state “diarrhea” and/or stools described as “loose” and/or “watery” and/or “frequent,” mark “Present.”
33

11.2: Comparison of Opioid Withdrawal Assessments Used in Construction of 17-Item Checklist
Symptom SOS13 WAT-112 COWS11 DSM-V6
Restlessness x xAgitation x x
Fever x x xTremor x x x
Pupil Size x xSleep Disturbance x x
Startle to touch xSeizure x
Hallucination xGrimacing x
Inconsolable Crying x x
Time to gain calm xYawning x x x
Tachycardia x xTachypnea xLacrimation x xRhinorrhea x xSneezing xNausea x x x x
Vomiting x x x xDiarrhea x x x x
Piloerection x xSweating x x x x
Joint/bone/Muscle Aches x x
Uncoordinated Movement x x
Muscle Tone x x
34

11.3: Opioid and Benzodiazepine Dosing Equivalence
Opioid18 Morphine Hydromorphone FentanylOral 20 mg 4 mg N/AIV 10 mg 2 mg 0.1 mg
Benzodiazepine19,20 Midazolam Lorazepam Diazepam ClonazepamOral N/A 1 mg 5 mg 0.25 mgIV 2 mg 1 mg 5 mg 0.25 mg
35