Embed Size (px)
Citation preview

1
Update re Pandemic Influenza and Precautions
Infection Prevention & ControlOccupational Health Hygiene
D. Moralejo PhD, RN; Marion Yetman MN, RN, CIC; Paula March BN, RN et al.
Fall, 2009

2
Overview
• The need for this review• Brief background
– How infections occur, breaking the chain– Routine Practices and Additional Precautions
• Seasonal flu and Pandemic (H1N1) 2009– The viruses and disease– Prevention: Clean, Cover, Contain, Choose to be
vaccinated– Management of illness– What to teach others
• Other issues

3
The Need for This Review

4
The story as it unfolded…
• April 26: 6 cases in Canada: 4 NS and 2 BC • June 11: WHO increases the pandemic alert
level to phase 6
• March 18: first cases in Mexico • April 2 – 60% of La Gloria, Mexico affected• April 17 – 2 cases identified in California• April 23 – Mexico confirms 1000 ill; 40
deaths; 20 H1N1
Edgar #14Y
La Gloria Mexico
• June 11: First lab confirmed cases in NL• Aug 1: > 10,000 cases in Canada• Aug 22: 1441 hospitalizations, 71 deaths
Increased and sustained transmission
H1N1
Pandemic (H1N1) 2009

5
Preventing a Repeat of 1918!
1918 was a bad year
We can be better prepared!
What about 2009?
Stuff of novels Just another influenza seasonStuff of novels Just another influenza season

6
The Need for This Review
• To be better prepared:– Reinforce good practices– Educate so better decisions are made
• And reassure HCWs, patients and others
• Learning objectives:– Reinforced breaking Chain of Infection– Reinforced RPAP– Understanding of Seasonal and Pandemic
Influenza

7
Background:Chain of Infection
• Agent – Bacteria – C. difficile, MRSA– Virus – influenza, norovirus
• Transmission– Contact- norovirus, MRSA…– Droplet – Influenza, RSV,
Pertussis, meningococcus…– Airborne – TB, VZV, Measles
• Susceptible host – No antibody– Reduced WBC or normal
defences
Infectious agent > DefencesInfectious agent > Defences

8
Breaking the Chainof Infection: IP&C
• Eliminate agent – Antibiotics or antivirals– Cleaning/disinfection– Remove reservoir
• Stop transmission– Hand hygiene– Protect portals of entry– Reduce carriage on hands and
clothes– Distance/isolation– Contain infectious source
• Reduce host susceptibility– Vaccinate– Improve defences e.g., stop
smoking, nutrition, control diabetes
Applicable for all infections!Applicable for all infections!
Break any link!
PPE

9
E.g., Chain of Infection: Influenza
• Agent – Seasonal influenza
virus
• Transmission– Droplet
(cough/sneeze)– Contact with
environment/objects contaminated with respiratory secretions

10From the School of Photographic Arts and Sciences, Rochester Institute of Technology TransmissionFrom the School of Photographic Arts and
Sciences, Rochester Institute of Technology
Droplet
Contact

11
Chain of Infection: Influenza
• Agent – Influenza virus
• Transmission– Droplet (cough/sneeze)– Contact with
environment/objects contaminated with respiratory secretions
• Susceptible host – No antibody– Reduced WBC or normal
defences, e.g., age, underlying conditions
Exposure to droplet ≠ transmission ≠ infection!Exposure to droplet ≠ transmission ≠ infection!

The Chain of Infection!One person
can spread the virus to
multiple others

13
Susceptible host – No antibody– Reduced WBC or normal
defences
Susceptible host – No antibody– Reduced WBC or normal
defences
Agent Influenza virus
Agent Influenza virus
Transmission– Droplet (cough/sneeze)– Contact with
environment/objects contaminated with respiratory secretions
Transmission– Droplet (cough/sneeze)– Contact with
environment/objects contaminated with respiratory secretions
Eliminate Agent – Clean environment– Antiviral drugs
Eliminate Agent – Clean environment– Antiviral drugs
+
+
Influenza: Breaking the Chain
Susceptible host – Vaccinate– Strengthen defences
Susceptible host – Vaccinate– Strengthen defences
Transmission–Droplet: Mask and
Eye Protection–Contact
•Hand Hygiene•Gloves, [Gown]•Distance
Transmission–Droplet: Mask and
Eye Protection–Contact
•Hand Hygiene•Gloves, [Gown]•Distance
Routine Practices and
Additional Precautions

14
Background: Routine Practices
System of practices to prevent and control transmission of microorganisms • To protect patients, HCWs and others • Used by all health care workers, for all patients, all
the time, in all health care settings Assumes all blood, body fluids, secretions,
excretions, drainage, tissues of all patients are potentially infective
Behaviors determined by assessment of risk of encountering the above during the patient interaction, not by diagnosis

15
Point of Care Risk Assessment
• New term, new emphasis, not new concept!
Prior to each patient Interaction, assess patient and interaction
Is there potential for exposure to secretions via coughing or sneezingor to other blood/body fluids, mucous membranes, non-intact skin or contaminated objects?
Is there potential for exposure to secretions via coughing or sneezingor to other blood/body fluids, mucous membranes, non-intact skin or contaminated objects?
What other risks for transmission are there?What other risks for transmission are there?
What PPE do I need?What PPE do I need?
What other actions are required?What other actions are required?
What is the need for hand hygiene?What is the need for hand hygiene? Is ABHR/a sink available?Is ABHR/a sink available?

16
Hand Hygiene PPE Respiratory hygiene/ cough etiquette Patient placement/ accommodation Patient flow/activity Cleaning/disinfection
of patient equipment
Hand Hygiene PPE Respiratory hygiene/ cough etiquette Patient placement/ accommodation Patient flow/activity Cleaning/disinfection
of patient equipment
Cleaning of environment
Handling of waste, linen and dishes
Management of visitors Aseptic technique Sharps safety
Cleaning of environment
Handling of waste, linen and dishes
Management of visitors Aseptic technique Sharps safety
RP Helpful for Influenza
17
RP vs AP
Routine Practices:• Disrupt chain of infection for influenza• Assume everyone carries something so use
interventions if possibility of being exposed
But with a known or highly suspect infection, probability of exposure is high so definitely need to use interventions!
Additional = Transmission-based Precautions “Pre-packaged” based on mode of transmission and
interruption of transmission Contact, Droplet, Droplet/Contact, Airborne, (Airborne/Contact)

AP for Seasonal Influenza
Seasonal Pandemic
Droplet Precautions•Mask/eye protection within 2 metres of pt
Contact Precautions•Gloves for contact with pt or environment•Gown if likely to be soiled with resp. secretions
Hand hygiene
Other
18
√ √
√ √
√ √N95 for selected AGMP

19
Eye Protection

20

21
Overview
• The need for this review• Brief background
– How infections occur, breaking the chain– Routine Practices and Additional Precautions
• Seasonal flu and Pandemic (H1N1) 2009– The viruses and disease– Prevention: Clean, Cover, Contain, Choose to be
vaccinated– Management of illness– What to teach others
• Other issues

22
Influenza Viruses
• Families: A, B, and C– Multiple strains
• Variants for humans, birds, pigs…– Animal/bird strains do not
usually infect humans
• 2 spike proteins on its surface: H and N– 16 different
haemagglutinins – 9 different neuraminidases
Eg: A/Brisbane/10/2007 (H1N1)Eg: A/Brisbane/59/2007 (H3N1)
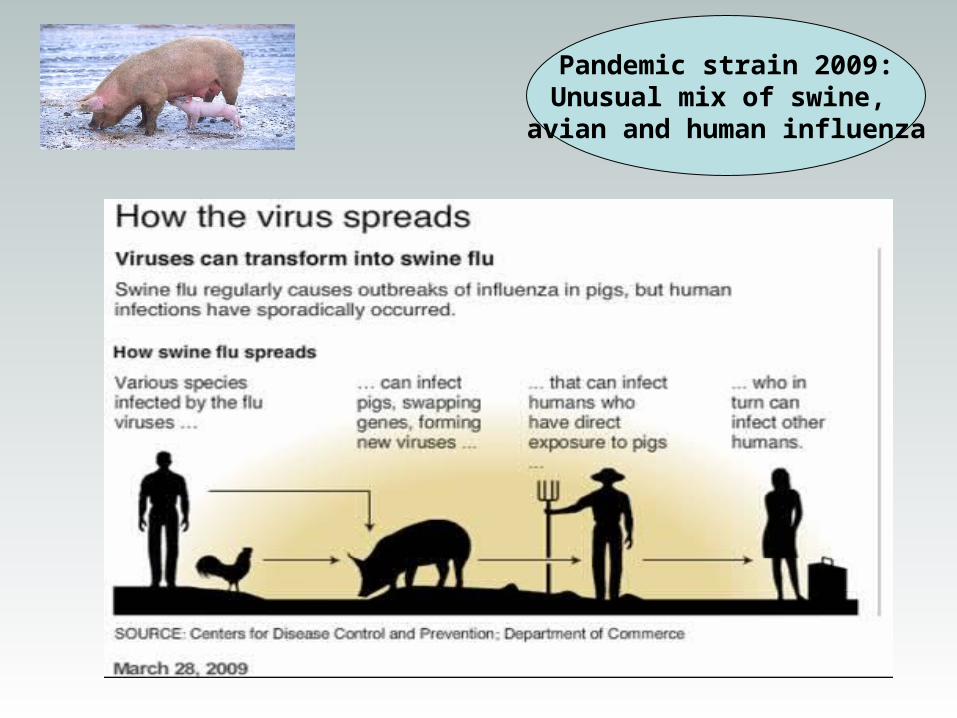
Pandemic strain 2009:Unusual mix of swine,
avian and human influenza

24
S&S of Seasonal Flu• Fever > 38º
– May not be prominent in elderly• Cough• Sudden onset • 1 of: Fatigue, sore throat, headache,
muscle & joint pain
• Flu is a respiratory infection!– But children <5 years may have GI
symptoms--diarrhea and vomiting • Range: mild to severe illness

25
A Word About Influenza-Like Illness (ILI)
Multiple viruses cause similar S&S!
Clinical dx based on what is circulating--need to test to know what causative agent is

26
Why Worry About Seasonal Influenza?
• Up to 10-25% of population ill in season• Per year, in Canada, flu or its
complications causes:– Average of 4000 deaths [6000-8000*]– 20,000 hospitalizations [30,000-40,000*]– Most severe in very old and very young
Note: most influenza deaths and cases are not recorded!
*in more severe seasons

27
Seasonal and H1N1: Similarities
Seasonal Pandemic (H1N1) 2009
S&S Similar Similar*
Transmission Droplet/Contact Droplet/Contact
Incubation 2 days 7 days
Period of communicability
5 days 7 days
Where spread 1° Community 1° Community
* But younger people affected, also certain populations: aboriginal, obese persons & pregnant women--ARDS in severely ill

• Novel virus – NO immunity– Except >60 years
• Two or three times a century• Two waves
– Several months apart– Each lasts 2 or 3 months
• 35 % or more affected– Healthy adults
• Vaccine not available for up to 6 months after novel virus identified
• Anti-virals – may be in short supply
• Novel virus – NO immunity– Except >60 years
• Two or three times a century• Two waves
– Several months apart– Each lasts 2 or 3 months
• 35 % or more affected– Healthy adults
• Vaccine not available for up to 6 months after novel virus identified
• Anti-virals – may be in short supply
Seasonal InfluenzaSeasonal Influenza Pandemic InfluenzaPandemic Influenza• Some immunity from prior
exposure to similar viruses
• Happens every year
• Usually from Jan – April & stops
• 10-25% of pop affected• Very young and old
• Vaccine available pre-season which offers protection
• Anti-virals available
• Some immunity from prior exposure to similar viruses
• Happens every year
• Usually from Jan – April & stops
• 10-25% of pop affected• Very young and old
• Vaccine available pre-season which offers protection
• Anti-virals available
Seasonal and Pandemic: Differences

29
Preventing influenza: 1918 versus 2009 public health messages

30
Shared Responsibility
• Screening protocols• Source Control
– Adequate space and plexiglass (separate ILI pts)
– Signs, ABHR– Accommodation
• Environmental control– Housekeeping
• Air exchanges• HCW Dx and Rx
– Antiviral drugs
• Vaccination programs
• Point of care risk assessment/ screening
• Hand hygiene• Droplet/Contact
Precautions• Teach/facilitate cough
etiquette
• Self screening• Vaccination
OrganizationalOrganizational HCW: Direct CareHCW: Direct Care
HCW: OtherHCW: Other

31
Contain
Cover
Clean
Simplifying the Messages
• Clean
• Cover
• Contain
Cho
ose
to b
e
vacc
inat
ed !
• Charge up your defences–Choose to be vaccinated!

32
1. Contain
Contain Spread/Illness– Screen for illness– Maintain distance
• Stay home if ill
Contain Spread/Illness– Screen for illness– Maintain distance
• Stay home if ill
Screening at entry:• Ambulance calls• ILI pts in clinics/ER• Signs directing pts to right
area, respiratory hygieneScreening inpatients,
visitors /companion: Screen for change: new ILI
Distance
• 2 metres between ILI pts
• Designated areas for ILI pts
• Plexiglass, curtains etc.
Permits timely application of Droplet/Contact Precautions and appropriate accommodation
Report to IP&C any patient with ILI symptoms!

33
Contain: More on Screening
• Screening criteria– Abrupt onset of:
• Fever (>380) or • New onset or worsening of existing cough; and• Any of the following: headache, sore throat, joint
pain, muscle pain or severe fatigue
• Screen patients, and don’t forget visitors and companions
• HCWs: Self-assessment prior to arriving in the workplace

New or worsening cough or
SOB?
ILI Screening
Fever or chills in past 24
hrs?
Yes
Yes
Initiate Droplet and Contact Precautions
and continue assessmentMaintain until diagnosis confirmed or ruled out
RPNo
Yes
Yes
No Fever or chills in past 24
hrs?
NoNoHeadache, sore throat
joint or muscle
pain, severe fatigue?
1 of:

35
Accommodation– Single room or cohort– Droplet-Contact Sign on
door– Confine patient to room
• Outside room – patient wears surgical mask
• Respiratory hygiene must be practiced
•Self isolate at home
In ER/Assessment Clinics–Partitions in triage areas–Post signs–Provide masks–Provide ABHR–Provide hand free garbage receptacles
–Remove magazines and toys from waiting areas
More about “Contain”

36
2. Cover
• Coughs – Everyone to use respiratory hygiene/ cough
etiquette: Self and teach patients/ others – Cover cough/sneeze with tissue or sleeve– Discard tissue– Hand hygiene after!– Need signs, ABHR, tissues, hands-free
garbage receptaclesDroplet Precautions!• Nose/mouth and eyes of HCWs
– Wear a surgical mask and eye protection!•Within 2 metres of coughing patient
• Patient to wear surgical mask outside room

37
Cover: Masks, not N95s?
• Surgical mask for Droplet Precautions• N95 respirator is used for aerosol-generating medical
procedures (AGMPs) if pt has TB or SARS or suspected novel influenza virus – E.g., endotracheal intubation, bronchoscopy,
respiratory/airway suctioning and resuscitation– List as per PHAC web site – Recommendations change as knowledge evolves– Use respirator as per fit test
Inappropriate and widespread use of N95 respirators
– Has negative health effects for HCW
– Will reduce supplies so not available when needed
Inappropriate and widespread use of N95 respirators
– Has negative health effects for HCW
– Will reduce supplies so not available when needed

38
More to Cover!
• HCW hands– Wear gloves when in direct contact
with patient or patient’s environment
• HCW clothes– Wear gown if anticipate clothes will come in
contact with respiratory secretions
Perform hand hygiene immediately after removal of PPE and immediately after exit from patient environment!
Perform hand hygiene immediately after removal of PPE and immediately after exit from patient environment!

39
3. Clean
• Hands– ABHR or soap and water– Frequently! As per RP but especially…
• Before touching mucous membranes• After contact with respiratory secretions or environment
contaminated with secretions
• The environment– at least daily or more often, depending on extent of
contamination

40
Clean, Cover, Contain…Charge!
Charge up defences• Choose to be vaccinated• Strengthen normal
defences
• Seasonal flu vaccine• Pandemic flu vaccine• Pneumococcal
vaccine – If > age 65 or high risk
Strengthen normal defences:• Stop smoking• Stay hydrated, well-nourished• Control diabetes
4
Choose to beVaccinated!

41
• NL DOHCS provides vaccine for:– Infants >6 – 23 months– >65 years– Persons-medical conditions– Health care workers– Emergency responders– Care givers of high risk
individuals– Pregnant women
• NL DOHCS provides vaccine for:– Infants >6 – 23 months– >65 years– Persons-medical conditions– Health care workers– Emergency responders– Care givers of high risk
individuals– Pregnant women
• Three components–Two influenza type A–One type B
• Reconfigured annually–Decision of WHO based on
FluNet
• 2009-2010 Vaccine• A/Brisbane/59/2007(H1Ni)• A/Brisbane/10/2007(H3N2)• B Florida/4/2006-like virus
• Three components–Two influenza type A–One type B
• Reconfigured annually–Decision of WHO based on
FluNet
• 2009-2010 Vaccine• A/Brisbane/59/2007(H1Ni)• A/Brisbane/10/2007(H3N2)• B Florida/4/2006-like virus
Seasonal Influenza Vaccine
LTC > Acute
Only 10-60% of
HCWs get vaccinated

42
Pandemic Influenza Vaccine
• Production underway– Available in late fall 2009– Seasonal vaccine confers little or no protection
against novel virus
• Safety– Licensed vaccines held to high level of safety– Close monitoring and investigation of all adverse
events
• Priority for vaccine– Decision of national authorities
• Mass vaccination campaigns required!

43
Why Get Vaccinated?
Health care workers are at a higher risk of getting and transmitting the influenza virus because the nature of their work places them in close contact with a high risk group of patients
BUT…HCWs are also at risk of acquiring the influenza virus in the community—the same as everyone else!
E.g. in stores, on the bus, at hockey games…
Getting vaccinated protects the HCW, their families and their patients

44
Impact of Influenza Vaccine
• Pre-exposure immunization is the most efficient method to decrease “flu” outbreaks
• Experience with seasonal influenza vaccination– 70% - 90% effective in preventing illness in healthy adults– Prevents serious illness and death in all age groups– In older age group
• 50 – 60% effective at preventing hospitalizations• 80% effective at preventing deaths
– Preventing illness in HCWs prevents illness in patients!
• Both seasonal and pandemic strain vaccines will be available in Fall 2009

45
The flu shot doesn’t workThe flu shot doesn’t work
I never get sick so don’t need itI never get sick so don’t need it
Flu vaccine causes the fluFlu vaccine causes the flu
20% have few S&S but still pass the virus to others20% have few S&S but still pass the virus to others
+
Myths About the Flu Vaccine
70-90% effective when good match70-90% effective when good match
Contains dead virus – cannot cause fluContains dead virus – cannot cause flu
I’m pregnant and shouldn’t get the vaccineI’m pregnant and shouldn’t get the vaccine
Flu vaccine is safe during pregnancy and is recommended
Flu vaccine is safe during pregnancy and is recommended
Getting the vaccine weakens your immune systemGetting the vaccine weakens your immune system Vaccine prepares and
boosts your immune system against the virus
Vaccine prepares and boosts your immune system against the virus

46
HCWs Also Say They Don’t Get Vaccinated Because…
I don’t like needles!
It will give me a headache, sore arm, slight fever,
ache…
Benefits > Discomfort!
Acetaminophen reduces incidence
and severity of side effects!

47
To Vaccinate or Not?
• If take it when offered– Have resistance before exposure
• If wait to take it when outbreak in work setting:– 14 days for antibodies to develop!– You may get sick and may not be able to work
• If refuse vaccine and rely on treatment or avoidance or other strategy:– You may get sick and may not be able to work

48
Duty of Care
Health care workers and health care systems have an ethical and moral duty to protect vulnerable patients from transmissible diseases
Yet HCW vaccination rates are low! What else
do we need to do to get
HCWs vaccinated?
• Vaccinate self
• Encourage others and facilitate access
• At minimum, do not discourage others!
Make mandatory? Declination forms?
More educationEasier access

49
Putting It All Together
• Contain– Screen– Distance
• Cover– Cough– Nose/mouth– Hands– Clothes
• Clean– Hands– Environment
Routine Practices• For all patients!
Additional Precautions• Droplet and Contact for ILI
• Choose to be vaccinated
Charge up defences
For now, same precautions for seasonal and pandemic strains

50
More on AP for Flu This Season
• Same precautions regardless of strain– But situation may change as virus or
pandemic evolves
• Risk assessment tools available to help identify risk given patient condition and interaction and PPE to use
Don’t self-contaminate when removing PPE!

51
Overview
• The need for this review• Brief background
– How infections occur, breaking the chain– Routine Practices and Additional Precautions
• Seasonal flu and H1N1– The viruses and disease– Prevention: Clean, Cover, Contain, Choose to be
vaccinated– Management of illness– What to teach others
• Other issues

52
Management of Illness
• Get lots of rest• Drink lots of fluids
– Feed a fever and feed a cold!
• OTCs and complementary medicine– No evidence of value for influenza
• Stay home until symptoms resolved and able to resume normal activities– Longer if cough not resolved
• Antiviral drugs not for everyone• For further info: see PHAC, NL and MUN websites

53
ILI in the Home
• Person with ILI should self isolate until symptoms resolved– Try to remain 2 metres from others– Dedicate room, bathroom, towels etc if possible– Enhance hand hygiene practices/general cleaning
practices– Do not need to have a NP swab done or see MD if mild
illness– Promote rest, fluids, pain relief etc…
• Others in the home or contact with ILI case:– Can go to work– Must self assess for ILI symptoms

54
Antiviral Drugs
• Tamiflu (oseltamivir) & Relenza (zanamivir)– Both effective against H1N1 Influenza A– Usual Adult Treatment
• Tamiflu – Adult - 75 mg BID x 5d (over 1 y)• Zanamivir – Adult – 10 mg Bid x 5 days (over 7)
• Treatment recommended for:– Severe cases & moderately severe cases with risks, as for
routine influenza– Pregnant women with ILI in 2nd or 3rd trimester or within 4
weeks post-partum
• Prophylaxis and treatment recommended for:– Outbreaks in closed facilities
Over use can lead to resistance!

55
Prevent flu in yourself! Clean & Choose
Prevent flu in others!Cover & Contain
Check yourself for ILI S&S
Clean,Cover, Contain, Choose to be
vaccinated
What to Teach Others

56
• Contain– Screen– Distance
• Cover– Cough– Nose/mouth– Hands– Clothes
• Clean– Hands– Environment
Routine Practices• For all patients!
Additional Precautions• Droplet and Contact for ILI
• Charge up defences– Vaccinate
For now, same precautions for seasonal and pandemic strains
Take Home Messages
Break the chain of infection!

57
Credits
Infection Prevention & ControlOccupational Health Hygiene
Narrated by: Dr. Donna Moralejo
Written by: Dr. Donna Moralejo, Marion Yetman and Paula March, in consultation with:•The Provincial Pandemic Infection Prevention & Control/Occupational Health Hygiene Action CommitteeEastern Health: Donna Ronayne & Ada FowlerCentral Health: Penny Ralph & Shelley WoolfreyWestern Health: Paula Price & Jackie YoungLabrador-Grenfell Health: Paula March & Lorraine Mitchell
Funding provided by:The Department of Health and Community Services, Newfoundland Labrador
Produced by: Distance Education and Learning Technologies© Dr. Donna Moralejo and Marion Yetman 2009

58
Thank you! Any Questions?





























