Embed Size (px)
Citation preview

1
The Whole System of Unscheduled Care: causal mapping, flows and
improvement
Steve KendrickSteve [email protected]@scotland.gsi.gov.uk
Emergency Access Delivery Team Emergency Access Delivery Team Networking Event Networking Event
Beardmore Hotel. Dec 18Beardmore Hotel. Dec 18thth, 2008, 2008

2
I. A&E attendances: outcomes and the whole system

3
Outcomes: the target
Reduce A&E attendancesReduce A&E attendances or more preciselyor more precisely
Reduce ‘better treated elsewhere’ A&E Reduce ‘better treated elsewhere’ A&E attendancesattendances
or more generallyor more generally
Everyone treated Everyone treated in the appropriate place in the systemin the appropriate place in the system
at the appropriate level of the systemat the appropriate level of the system

4
Whole system/outcomes
• (BTE) A&E attendances as outcome of (BTE) A&E attendances as outcome of how whole system of unscheduled care how whole system of unscheduled care is working: to reduce them you need to is working: to reduce them you need to make the whole system work better.make the whole system work better.
• (BTE) A&E attendances as an indicator (BTE) A&E attendances as an indicator of how well the system is working: of how well the system is working: reflect degree of balance in systemreflect degree of balance in system

5
Useful ways of looking at the whole system of unscheduled care
Patient perspective Patient perspective Organisational system Organisational system Data system Data system Real systemReal system
But today want to focus onBut today want to focus on
a)a) A system of causes and effectsA system of causes and effects
b)b) As a system of patient flowsAs a system of patient flows

6
II. Unscheduled care as a system of causes and effects

7
a) Identify the various causal influences a) Identify the various causal influences which combine to produce the outcomewhich combine to produce the outcome
b) Identify the opportunities to intervene to b) Identify the opportunities to intervene to improve the outcome. improve the outcome.
Leads to Leads to driver diagramdriver diagram..
What do you need to do to achieve an outcome?

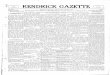
8
OutcomeChanges Drivers
Fewer‘bettertreated
elsewhere’A&E
attendances
e.g.
Morbidity
Patientknowledge/behaviour
Accessibilityof differentservices
Triagemethods
Integrationof system
e.g
Prevention
SocialMarketing
Improved access to alternatives
Improvedalgorithms/training
Sharing of data
Unscheduled care. Driver Diagram. Illustrative Only!Illustrative Only!

9
III. Unscheduled care as a system of patient flows

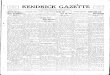
10
PublicA&E
Ambulance
NHS24
OOH
In hoursprimary care
“999
”
Self-referral
Flows into A&E. Orders of magnitudeOrders of magnitude!
1000attendances
8030
600
70
22040
250
800
600

11
IV. Relating flows to causes/drivers to improvement.

12
• Each of the flows is a result of decisions Each of the flows is a result of decisions made by particular agents at particular points made by particular agents at particular points in systemin system
• Many of the changes we need to make are Many of the changes we need to make are improvements in decision-making. Making improvements in decision-making. Making sure patients are in the right flows. sure patients are in the right flows.
• Plus services to support those improved Plus services to support those improved decisions.decisions.
How do we relate ‘flows’ to ‘causes/drivers’

13
The potential for improvement
• To a large extent defined by the number To a large extent defined by the number of patients who are in the wrong flowsof patients who are in the wrong flows
• End up being treated at too intensive a End up being treated at too intensive a level of the systemlevel of the system
• e.g. treated A&E when could have been e.g. treated A&E when could have been ‘better treated elsewhere’‘better treated elsewhere’

14
How do we assess this potential for improvement? (e.g. potential for reducing A&E attendances)
• Need a much more detailed picture of Need a much more detailed picture of patient characteristics in each of the patient characteristics in each of the flowsflows
• Which are the groups of patients with Which are the groups of patients with the greatest potential for diverting to a the greatest potential for diverting to a more appropriate flow/treatment point?more appropriate flow/treatment point?

15
V. Immediate priority: better understanding of who is attending A&E

16
Immediate priority
• Better understanding of the patients attending Better understanding of the patients attending A&EA&E
• Can we characterise A&E attenders in terms Can we characterise A&E attenders in terms of meaningful groups which e.g.of meaningful groups which e.g.– help us assess potential for alternative care?
• given current set-up• given better alternatives
– help us assess potential for prevention– help us assess the potential for improved services

17
Examples of the kind of patient groups it would be useful to identify and quantify
• Elderly fallsElderly falls• Minor illnesses who don’t need to be at A&EMinor illnesses who don’t need to be at A&E• Behavioural/psychological ‘chaotic lifestyle’Behavioural/psychological ‘chaotic lifestyle’• Alcohol relatedAlcohol related• Admissions from care homesAdmissions from care homes• Frail elderly in generalFrail elderly in general• Exacerbations of LTCs e.g. COPDExacerbations of LTCs e.g. COPD• ????????

18
Options for getting a better picture
• Existing electronic data: EDIS, Existing electronic data: EDIS, Manchester Triage dataManchester Triage data
• Digging into ‘the cards’. Get information Digging into ‘the cards’. Get information from A&E paper records.from A&E paper records.
• Detailed survey of A&E attendersDetailed survey of A&E attenders

19
Taking this forward• Each method will give us a different and Each method will give us a different and
useful perspectiveuseful perspective• Each NHS Board has different strengthsEach NHS Board has different strengths
Timing.Timing.• January. Each Board to develop a picture January. Each Board to develop a picture
using existing data: electronic, paper using existing data: electronic, paper records /cardsrecords /cards
• Next couple of months: develop and do more Next couple of months: develop and do more detailed survey of A&E attendersdetailed survey of A&E attenders

20
Unscheduled Care Information Network
• Mutual support and sharing of expertiseMutual support and sharing of expertise
• So far involves NHS Boards, NHS24, SAS, So far involves NHS Boards, NHS24, SAS, SG, ISD.SG, ISD.
• Need lead information person from each Need lead information person from each BoardBoard
• Aiming for meeting late JanuaryAiming for meeting late January


![no · PDF fileE. Kendrick Ma] 16-3 Round 4 Kendrick Gustilo E. Kendrick C. Lewis Kendrick Maj 16-4 ... Johnson South port puni Jayden Bowles Citrus Wrestlin Mason Wislon](https://img.dokumen.tips/doc/110x75/5a8ed0e57f8b9a4a268d68c8/no-kendrick-ma-16-3-round-4-kendrick-gustilo-e-kendrick-c-lewis-kendrick-maj.jpg)