Embed Size (px)
Citation preview

1
Speech Recognition & The Persistence of Narrative Documentation in the EHR Environment
Don FallatiVP-Senior Advisor

2
A Union of Speech Recognition Industry Leaders
A Union of Speech Recognition Industry Leaders

3
CPR
The Clinical Information Challenge:How Do We Automate Narrative?
CLINICALAUTOMATION
Clinical Information
Benefits:• Cost Savings/Efficiency
• Quality/Patient Safety
CPOE
Patient Documentation
Patient Documentation
Devices/Dept Systems
4
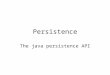
Voice: Fastest Information Entry Modality
“Speech Recognition’s record breaking accuracy
improvements make using speech recognition easier than
ever before.”
“Speech Recognition’s record breaking accuracy
improvements make using speech recognition easier than
ever before.”
Input Device Average Time
Mobile phone keypad 1:57
Mobile phone keypad
(T9 predictive text)
1:15
RIM Blackberry
(QWERTY keyboard)
0:57
RIM Blackberry 7100
(predictive text)
0:59
Desktop PC
(QWERTY keyboard)
0:22
Voice
(Mobile dictation)
0:12
Average text-entry time using various input mechanisms(expert users)
Text segment used:

5
Narrative Paradigm
• Medical reporting is capturing stories
• Narrative will persist for a long time and there will be a lot of it
• EMR documentation paradigm flawed
• Need to change the game
• Need Narrative-based structure

6
Persistence of Narrative
• Narrative will stay because:– Natural form of communication– Comfortable to create– Voice friendly– Provides nuance, detail,
context– Supports comprehensive
documentation– Not just habit
• Narrative remains.
• Transcription, as we know it today, may not.
Diagnoses are acute inferior wall MI and type II diabetes. Performed cardiac catheterization and a coronary angioplasty of the right coronary artery. Upon discharge patient prescribed Lopressor 25 mg. p.o. b.i.d. Also enteric-coated aspirin 325 mg. p.o. per day and Glyburide 2.5 mg. p.o. q AM. Dr. [RNAME] consulted on the case. HPI this is the first [RCLINIC] admission for a 67 year old white male who was transferred from [RCLINIC] for cardiac catheterization and possible intervention. He had been admitted to that facility on [RDATE] with a one to two week history of crescendo angina, described as chest pain and pressure with radiation to his arms which was occurring with activity and was becoming more frequent, and with easier onset of action. He had no previous cardiac history, myocardial infarction or congestive heart failure. He denied any dyspnea on exertion, PND, orthopnea, pedal edema, palpitations or syncope. Risk factors for coronary disease include a history of non insulin dependent diabetes, hypertension, family history. Cholesterol status was unknown. He had no history of tobacco abuse. Did not drink alcohol. Patient had a bilateral herniorrhaphy and is allergic to penicillin. Patient was already taking Glyburide and Lisinopril and aspirin. Exam info patient is a well developed man, no distress. Stable vital signs. No increased JVD. Lungs clear. Normal heart sounds without rub, murmur or gallop. Abdominal area soft without organomegaly, mass tenderness or bruits. GU deferred. No cyanosis, clubbing or edema. Good peripheral pulses. Neurological intact. EKG revealed a QS pattern in leads 2, 3 and F without other ST segment abnormalities. This gentleman had undergone a stress test at [RCLINIC] prior to his transfer which was markedly abnormal with ST segment elevation in the inferior leads, and for this reason it was felt that he would require catheterization. Subsequent laboratory studies revealed slightly elevated troponins, borderline elevated CK's and elevated MV's. The patient was transferred to the CCU and was continued on Heparin and Tridil. The following morning was taken to catheterization laboratory and underwent successful balloon angioplasty of his posterior descending artery.

7
Three Solutions taking aim at transcription
Outsource
EMRTranscriptionSpeech

8
Dictaphone Documentation Automation

9
Speech Recognition Editing Styles
Provider-drivenTranscription-assisted
Speech Recognition
with NLP

10
Integrating Speech Recognition Into Workflow Platforms
Workflow PlatformServer Based
Speech Recognition
EHR
Desktop Based Speech Recognition

11
State of Speech Recognition Today
• Over 1200 systems sold
• Covering broad range of medical specialties
• Inpatient and outpatient usage
• Large and small institutions
• Being applied to high percentage of daily volume

12
Gartner Healthcare Technology Hype Cycle
SR Transcription
SR Once and Done
13
Productivity Gains - Radiology
• 900 systems sold
• Elimination of hundreds of thousands of $ annual
transcription cost
• 24-48 hour turnaround times slashed to a few minutes

14
Productivity GainsTranscription-Assisted SR
Name Overall Productivity
Top MTNumber of Dictators
Monthly SR Volume
SR % of Total Volume
Affinity Health Systems 54% 217% 105 17,600 35%
Advanced Healthcare30% 156% 101 8,000 75%
Brooks Memorial 43% 85% 32 392 62%
Reading Hospital 29% 388% 66 1,695 27%
Outagamie Health59% 361% 62 2,592 87%
Rush Foundation Hospital 40% 41% 18 343 15%
AthletiCo 41% 99% 300 8,000 78%
Regions 29% 68% 98 2,000 14%
Dean Medical Center43% 141% 350 12,900 22%

15
Self-Edit Non-Radiology Case Study
Self-Edit
Users Reports
Camino Healthcare
180 7,665

16
The Physician Adoption Challenge – User Interface

17
The Mobile Vision Any Device, on Any Network
MobilePhone
s
Telephones
Computers
Laptops
PDAs
The Physician Adoption Challenge – User Interface

18
The Physician Adoption Challenge – Time
• Breakthrough Dictaphone technology creates new time savings:– Reuse of previously dictated material
• Multiplier effect with other speech recognition features

19
Dictated Medical Report Clinical Data
Natural Language Processing
Natural Language ProcessingWhat does it do?
SectionalTagging

20
NAME: J ohn Doe LC#: 0992612 ADMISSION DATE: 09/ 14/ 02 DISCHARGE DATE: / / ATTENDI NG PHYSI CI AN: A. Physician, MD CHI EF COMPLAINT: Right ureteral calculus.> ASSOCI ATED DI AGNOSES:
1. History of nephrolithiasis. The patient is status post multiple lithotripsies in the past. 2. The patient is status post nephrolithotomy in 1978. 3. The patient with hypertension. 4. The patient with gout.
HI STORY OF PRESENT I LLNESS/ REASON FOR ADMISSION: The patient is a pleasant 75-year-old gentleman with a prior history of urolithiasis, status post left nephrolithotomy in 1978, and multiple lithotripsies, and now presents with 12-hours of right flank pain. He denies any associated diaphoresis, nausea, vomiting, fever, chills, chest pain, shortness of breath, change in bowel habits, or change in his urinary habits. He denies any recent passage of calculus, fragments in his urine, and denies hematuria, dysuria, frequency, or urgency. His flank pain is similar to his prior renal colic and does not radiate. I t is approximately 7 out of 10 in severity and comes and goes in waves. He has otherwise been in his usual state of health. He recently underwent an exercise tolerance test in July of 2002 which was within normal limits. This was initiated on review of a new right bundle-branch block on EKG.
PAST MEDI CAL HI STORY: 1. As above. 2. Hypertension. 3. Gout.
MEDI CATI ONS: Plendil 5 mg p.o. q.d.; Diovan 80 mg p.o. q.d.; indomethacin; and allopurinol p.r.n. ALLERGIES: PENI CI LLIN AND AMPI CI LLIN. FAMILY HI STORY: SOCIAL HISTORY: The patient denies any tobacco or ethanol use. REVI EW OF SYSTEMS: PHYSI CAL EXAMINATION: On exam he is afebrile with a temperature of 98.1, pulse is 83, blood
pressure 170/ 88. He is breathing at a rate of 16. He is in no apparent distress. He has no diaphoresis. HEENT: He is anicteric. NECK: He has no carotid bruits. CHEST: His lungs are clear. HEART: Regular. ABDOMEN: Soft, nondistended. He has mild right lateral abdominal pain; however, no guarding and no peritoneal signs. He has normal male genitalia with descended testes bilaterally. There are no inguinal hernias. RECTAL: Exam notes a 3+ smooth prostate. EXTREMI TI ES: Within normal limits. OTHER:
LAB DATA: EKG: CT SCAN: Noted an 8-mm right proximal ureteral calculus with hydroureter and hydronephrosis
and mild perinephric stranding. The left side also had a 5-mm renal calculus and a mild pull calix. There was no hydronephrosis or hydroureter on the left. DI AGNOSTI C: Significant for a creatinine of 2.1. His last prior creatinine was 1.3, checked in July. His white blood cell count was elevated to 17.8, and his hematocrit was 44.3. Urinalysis revealed a pH of 5.0 with red blood cells and white blood cells as well uric acid crystal within.
ASSESSMENT: The patient is a 75-year-old gentleman with a history of urolithiasis and hyperuricemia with an obstructing right ureteral calculus, elevated white count, intractable pain, and rising creatinine.
GOALS/ TREATMENT PLAN: The plan for the patient is to remain n.p.o., to have alkalinization of his urine with sodium bicarbonate and D-5-W and to go to operating room for ureteral stenting. He will be treated preoperatively and postoperatively with I V antibiotics and will be admitted to the hospital.
“Jump Start” Technology

21
NAME: J ohn Doe LC#: 111111 ADMISSION DATE: 09/ 14/ 02 DISCHARGE DATE: 09/ 16/ 02 ATTENDI NG PHYSI CI AN: A. Physician, MD PRI NCIPAL DI AGNOSIS: Right ureteral calculus. PRI NCIPAL PROCEDURES:
1. Cystoscopy. 2. Placement of right double J stent on 09/ 14/ 02.
HI STORY OF PRESENT I LLNESS: The patient is a pleasant 75-year-old gentleman with a prior history of ureterolithiasis, status post left nephrolithotomy in 1978 and multiple lithotripsies, who now presents with a 12 hour history of right flank pain. He denies any associated diagnoses, nausea, vomiting, fever, chills, or chest pain. He reports no change in bowel habits or change in his urinary habits. He denies any recent passage of a stone and denies hematuria, dysuria, frequency, or urgency. He reports that his flank pain is similar to his prior episodes of renal colic. He states that his pain is approximately 7 out of 10 in severity and comes and goes in waves. He has otherwise been in his usual state of health.
PAST MEDI CAL HI STORY: 1. As above. 2. Hypertension. 3. Gout.
MEDI CATI ONS ON ADMI SSI ON: Plendil 5 mg p.o. q.d.; Diovan 80 mg p.o. q.d.; I ndomethacin p.r.n.; allopurinol 0.625 mg p.o. q.d. p.r.n.
ALLERGIES: THE PATI ENT REPORTS ADVERSE REACTION TO PENI CILLI N AND AMPI CI LLI N. SOCIAL HISTORY: The patient denies any tobacco or ethanol use. PHYSI CAL EXAMINATION ON ADMISSION: The patient was afebrile and his vital signs were stable. In
general, he was alert, oriented, in no apparent distress. His head and neck exam was unremarkable. His lungs were clear to auscultation bilaterally and his heart had a regular rate. His abdomen was soft, nontender, nondistended. He had no evidence of peritoneal signs. He had normal male genitalia with descended testicles bilaterally. His extremities were warm and nontender. Rectal exam was significant for a 3+, smooth prostate.
HOSPI TAL COURSE: The patient was admitted and taken to the operating room, where he underwent a cystoscopy and double J stent placement. Postoperatively he was admitted to the floor. On postoperative day 1, he was continuing to have some mild discomfort in his right flank. He was otherwise tolerating a regular diet and ambulating without difficulty. Of note, he did have an elevated creatinine of 2.1 on admission. His creatinine had fallen to 1.8. On postoperative day 2, his pain had resolved and he was tolerating a regular diet. He was ambulating without difficulty. His pain was well controlled with p.o. pain medication. He was started on Polycitra in order to alkalinize his urine. He was discharged home with followup.
CONDI TI ON ON DISCHARGE: Stable. DISCHARGE DI SPOSITION: The patient will follow up with Dr. Michael Malone in the office as an
outpatient with a stone protocol CAT scan of his abdomen and pelvis. In addition, he will have a blood urea nitrogen and creatinine level drawn at the same time, prior to his visit.
DISCHARGE MEDI CATI ONS: Plendil 5 mg p.o. q.d.; Diovan 80 mg p.o. q.d.; I ndomethacin p.r.n.; allopurinol 0.625 mg p.o. q.d. p.r.n.; Polycitra 1 packet p.o. t.i.d. with meals; Bactrim DS 1 tab p.o. b.i.d. x 3 days; Tylenol No. 3 1-2 tabs p.o. q.4-6 h. p.r.n.; Colace 100 mg p.o. b.i.d. p.r.n.
from H&P Report
from Normals
“Jump Start” TechnologyDischarge Report Automation
from HIM Database

22
Report Completion by Shortcuts and Reuse
21%
48%
31%
>70%
>50%
<50%

23
“NaturalLanguage”
PatientRecord
Dictation
The Physician Adoption Challenge – Speech & the EMR
Data Quality & Re-usability
PhysicianUsability
High
Low High
Low
InstallCost &
Complexity
EMRwith
structureddata

24
Speech Can Address the Various Hospital/Clinic Scenarios
1. No EMR Interest or Intent
2. Actively Considering EMR
3. Implementing EMR –Concerned with Adoption
4. Deployed and Using

25
Speech Enable the EMR

26
Migrating the Physician
Traditional dictation
The “Natural Language”
Patient Record
Background MTSpeech Rec
SR & NLP structuredreport / data creation
Phys self-editSpeech Rec
Natural LanguageBridge to Clinical
Automation