Embed Size (px)
Citation preview

1
VimoSEWA
SelfSelf--Employed WomenEmployed Women’’s s Association (SEWA)Association (SEWA)
Ms. Upasana Joshi
Ms. Rupal Jayaswal
15th Oct. ‘05

SEWAStrength in SolidarityStrength in SolidaritySome Experiences of SEWA Insurance
• Hospital tie-ups
• Renewal Campaign

SEWASEWASEWA is a trade union of women workers in the informal economy.

SEWA’s GoalsSEWA’s Goals
Full EmploymentFull Employment– work security– income security– food security and – social security
Self RelianceSelf Reliance

Insurance Membership - 2005
Women – 83514
Men – 34306
Children – 18,587
Total Insured – 136,407
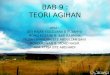
Current insurance packages offeredPolicy I Scheme II
Women Spouse Children
Family
Women Spouse Children
Family
Annual 100 70 100 250 225 175 100 480
Fix 2100 1500 - - 5000 4000 - -
Natural Death
5000 5000 - - 20000 20000 - -
Mediclaim 2000 2000 2000 - 6000 6000 2000 -
Asset 10000 20000
Accidental Death
40000 25000 65000 50000
Accidental Death -
Spouse
15000 15000
- Hospital tie-ups- Renewal Campaign
Two recent initiatives

OBJECTIVE ACTIVITIES
Direct members to Inpatient facilities of acceptable quality
Hospital tie-ups
1. Develop procedure for screening hospitals for inclusion;2. Select hospitals;3. Periodically re-evaluate hospitals based on performance.
Facilitate access tohospitalization byremoving financial barriers
1. Encourage use of public and trust hospitals;2. For members who use selected hospitals, pay 80% of claim within 48 to 72 hours of admission (balance at the time of discharge).
Make it easier to claim and receive benefits under the scheme
1. Annual house-to-house visits to remind members about hospitalization insurance, and educate about “PR”;2. Provide greater assistance in collecting and then submitting claims documentation.
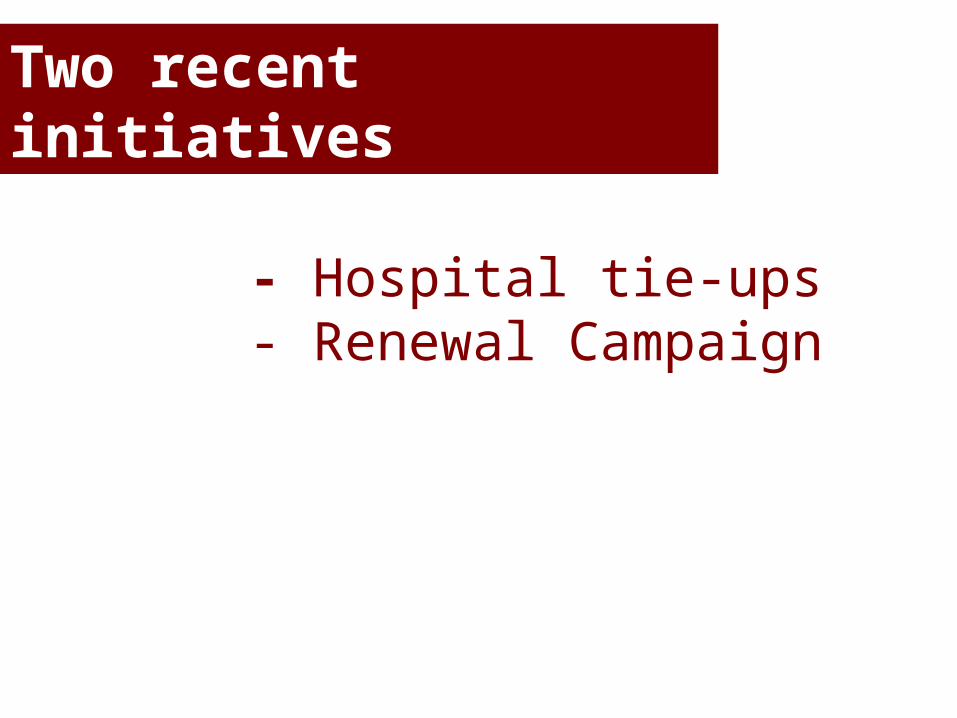
System design
1.Goes to hospitalInsuredSelected hospitals
2.Phone ca
ll
6.Receipts
& certif
icates
Local Vimo Rep.
Vimo SEWA Claims committee
4.Relays information, decision is made
3.Collects Info. On
Diagnosis,Length Of stay,
cost
5.Payment for bed,Doc.,
medicines, lab tests

Successes
• SEWA insurance members received better quality care service from selected hospitals
• 50% of claims came through cashless system
• Increased use of public and trust hospitals as against private hospitals
• Reduced the number of days of settlement of claim (80% in 48 hours)

• Availability of suitable public or trust hospitals
• Educating the members about cashless system
• Skilled human resource– Local representative
Challenges

SEWA’s Renewal Campaign
Objective
• Continued protection to Vimo SEWA members
• Achieve renewal rate – 70% - policy year 2006– Policy year 2004: renewal rate – 30% (YP)
– Policy year 2005: renewal rate – 42% (YP)
Reasons for non renewal
From Research
• Limited understanding of Insurance
• Lack of money at time of enrollment
• Limited contact between members and aagewans after enrollment

Reasons for non renewal
• Not enough focus and monitoring on renewals during enrollment campaign

Renewal Strategy – P.Y. 2006
• Limited to Ahmedabad city (30,000 insureds)
• Make individual contact with each member prior to enrollment campaign
• Distribution of insurance and health education material
• Visit each member during enrollment period for renewal
Implementation Process
1. Each aagewan was given user friendly member lists
2. Each aagewan was assigned manageable number of membership
3. Supportive supervision given to aagewans
4. Barcodes used for recording visits

Outcomes
1. Able to complete 82% of visits prior to enrollment period
2. Members felt good about the house-to-house visits
3. For the first time aagewans went systematically house-to-house to meet each insured member
4. There was increase in members’ understanding and information
Challenges
• Obtaining accurate addresses
• Labour and time intensive
• Monitoring of visits

Lessons Learnt
1. Supportive supervision is critical
2. Adequate human resources required for satisfactory completion of visits
– Aagewans– Supervisors
3. Individual house-to-house visits build trust