Embed Size (px)
Citation preview

1
Recreational Drug Use and Sexual Functioning

2
Nicotine
• (Complex impact on hormones & neurotransmitters.)• Short term = interferes with erection
– Decreases blood flow to penis– Increases venous outflow from penis
• Long term use destroys penile tissues = erectile dysfunction• Passive smoking can have similar impact

3
Alcohol• (Diffuse affects on neurotransmitter processes)
• (Affects hippocampus)
Males
• Self-report
• Increased latency to orgasm (reduced likelihood of premature ejaculation)
• Increased likelihood of erectile failure
• Alcoholic males: erectile dysfunction (59%); anorgasmic dysfunction (48%); at least one sexual dysfunction (84%) (Mandell et al., 1983)
• Laboratory Studies
• Inhibits erection (dose dependent)
• Increased latency to ejaculation (dose dependent)

4
Farkas & Rosen, 1976

5
Malatesta, Pollack, Wilbanks, & Adams, 1979

6
Alcohol: Females• Self-report:
– No change in sexual functioning when intoxicated– Moderate alcohol use (2 per week – 2 per day) associated with
lowest rates of sexual dysfunction– Alcoholic females report decrease in sex drive and difficulty
achieving orgasm/anorgasmia • Laboratory Studies:
– Decreased arousal (Wilson & Lawson, 1976)

7Wilson & Lawson, 1975

8
Alcohol: Females• Self-report:
– No change in sexual functioning when intoxicated– Moderate alcohol use (2 per week – 2 per day) associated with
lowest rates of sexual dysfunction– Alcoholic females report decrease in sex drive and difficulty
achieving orgasm/anorgasmia • Laboratory Studies:
– Decreased arousal (Wilson & Lawson, 1976)– Longer latency to orgasm (Malatesta et al, 1982)– Decreased intensity of orgasm (Malatesta et al, 1982)– Increased subjective arousal and orgasm pleasure (Malatesta et al,
1982)
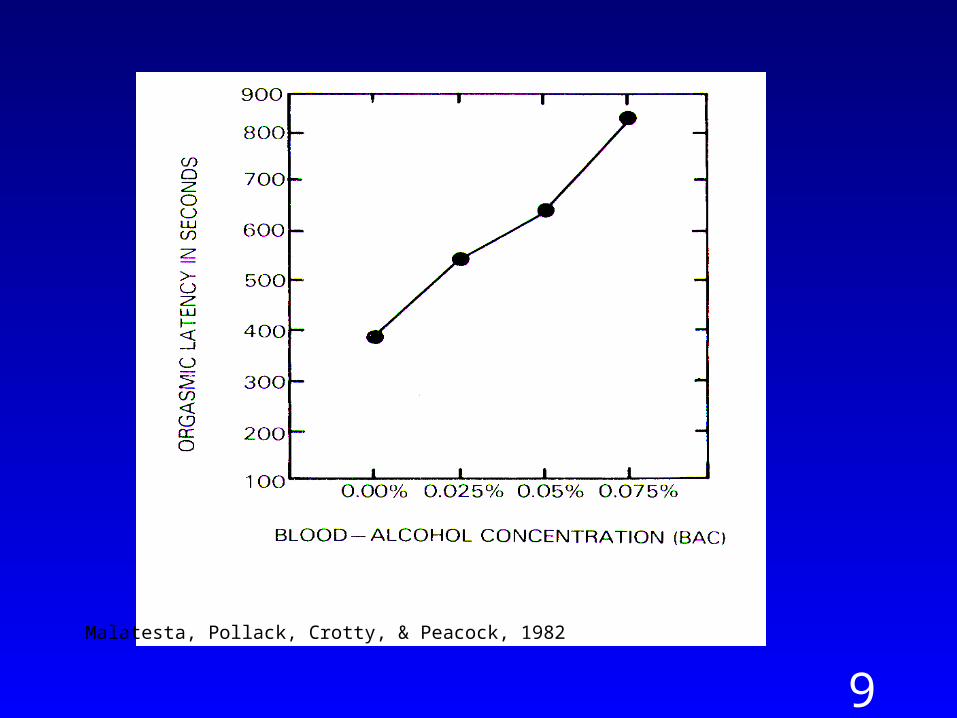
9
Malatesta, Pollack, Crotty, & Peacock, 1982

10
Marijuana
• (THC (active ingredient) – THC receptors rich in the hippocampus)• lowers testosterone (mixed evidence)• Enhances sexual enjoyment in both men and women (83% and 81%
respectively)• Does not affect erection, lubrication, or orgasm.• Increases relaxation, sociability, touch, and comfort.• high doses = sedation and impaired sexual performance.• In animals, decreases sexual activity – general decrease in physical
activity.

11
Amphetamines “speed”
• (Enhanced release and block reuptake of norepinephrine, and at higher doses, dopamine.)
• Can cause vasoconstriction of genital tissue
• Sexual Performance:
– Increased libido (increased energy)
– Erectile failure; prolonged erection (up to 18 hours!)
– Anorgasmia; multiple orgasms
• Long term use: loss of interest in sex

12
MDMA “Ecstasy”
• (Similar to amphetamines, stimulates SNS)
• Purported effects:
– increased energy
– increased endurance
– feelings of euphoria
– increased sociability
– feelings of intimacy
– altered visual perception
– enhanced libido

13
MDMA “Ecstasy”
• Sexual functioning
– Subjective ratings: 20 men, 15 women (Zemishlany et al., 2001)
• Desire: moderately to profoundly increased
• Erection: impaired in 40%
• Orgasm: delayed but more intense
• Satisfaction: moderately to profoundly increased
– Laboratory studies?

14
MDMA “Ecstasy”
• Acute side effects/adverse effects (Smith, Larive & Romanelli, 2002):
– agitation, anxiety, tachycardia, hypertension
– arrhythmias, hyperthermia
• Chronic adverse effects:
– Toxicity to serotonin system
• cardiovascular system
• CNS serotonin
• Overlap between recreational and fatal dose (Kalant, 2001)

15
Crystal Methamphetamine“Crank,” “Crystal,” “Speed”
• (Increased release of dopamine, adrenaline)
• Purported effects:
– sense of exhilaration
– sharpening of focus
– sense of sexual liberation
• Sexual Functioning
– constricts blood vessels
– erectile dysfunction
• Risks: similar to amphetamines, risk greater

16

17
Physiology of penile erection
Sexual stimulation Nitrix oxide synthesized in nerveand vascular tissue of penis
Nitrix oxide activates guanylate cyclaseGTP cGMP
cGMP relaxes smooth muscles of corpus cavernosum/penile arterioles
Vasocongestion of penile tissues
18
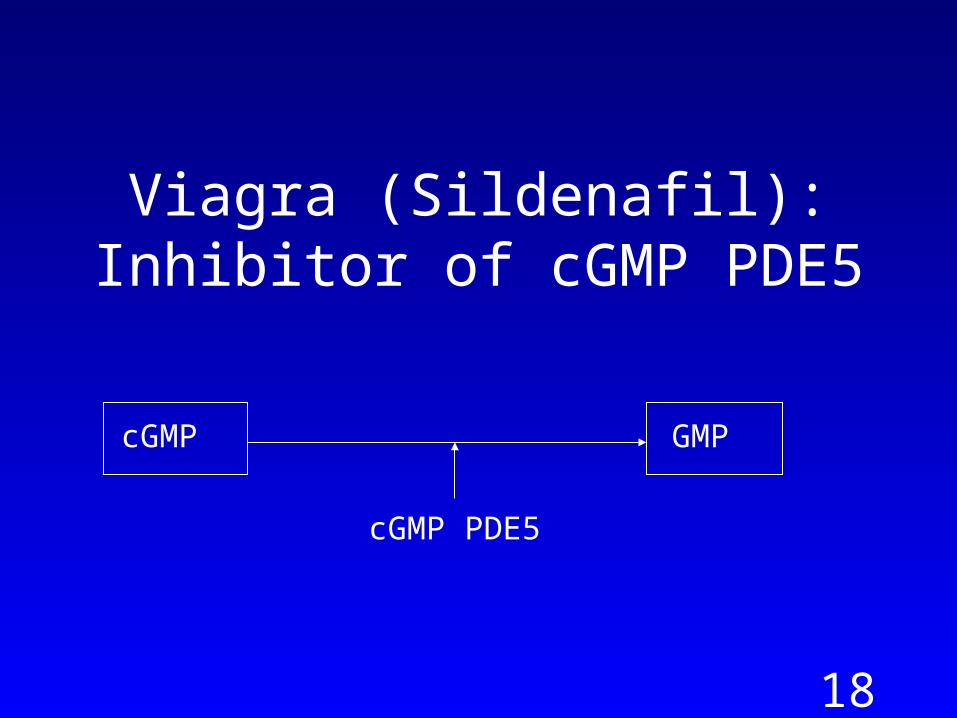
Viagra (Sildenafil): Inhibitor of cGMP PDE5
cGMP GMP
cGMP PDE5

19
Nitric Oxide & Penile/Clitoral Tumescence
Sexual stimulation Nitrix oxide synthesized in nerveand vascular tissue of penis/clitoris
Nitrix oxide activates guanylate cyclaseGTP cGMP
cGMP relaxes smooth muscles of corpus cavernosum and arterioles in penile/clitoral tissue
Vasocongestionof penile/clitoral tissues
20
Sextasy
• Combining Viagra with ecstasy, “hammerheading”
– headache, prolonged erection (priapism)
– high risk sexual behavior
– long-term heart damage
• Viagra with:
– crystal methamphetamine
– amyl nitrate
– any drug that produces erectile dysfunction
• Viagra and illegal recreational drugs (40%)

21
Amyl Nitrate “Poppers”
• Organic nitrate
– Short-acting vasodilator
– Increased blood flow to heart and brain
• Purported to make sexual organs feel “Herculean”

22
Cocaine
• Inhibits reuptake of dopamine• Potent vasoconstrictor• Increased sexual desire• Arousal:
– Men: • low doses – prolonged erection • high doses – erectile failure
– Women: reports of both increased and decreased subjective arousal
• Delayed or absent orgasm

23
Opioids: Heroin• Stimulate opiate receptors (enkephalins (body) and endorphins (brain))
– results in reduction in circulating testosterone
• Produce relaxation/sense of well being
• Analgesic affect – opiate receptors in female genital tract
• Few reports of acute use: lowers drive, delays orgasm
• Male Heroin addicts:
• loss of drive, erectile dysfunction, orgasmic dysfunction
• Withdrawal: increased morning erections, spontaneous ejaculation, slow return of sex drive, erectile and orgasmic dysfunction
• Female Heroin addicts:
• Decreased drive, increased drive, anorgasmia
• Withdrawal: loss of libido

24
Hallucinogens (LSD, PCP)
• Purported to be “ultimate sex drug.”
• Affects dopamine, serotonin, and with PCP, glutamate.
• Sexual pleasure enhanced (all pleasure enhanced – e.g., watching paint dry is equally pleasurable)
• Sexual Performance (animal studies):
– low doses:
• Males: premature ejaculation
• Females: normal receptivity
– Moderate to high doses – lack of physical coordination precludes any sexual activity.

25
Psychotropic Drug Use and Sexual Functioning

26
Antidepressants
• MAO inhibitors, SSRIs
• Impair all aspects of the sexual response cycle in men and women
• Serotonin 5-HT2 receptor implicated
– Nephazadone (serzone) SSRI and 5-HT2 antagonist – fewer sexual side effects
– Stimulation of the 5-HT2 receptor (peripherally) causes vasoconstriction

27
Antipsychotics
• Decreases dopamine activity
• Males
• Enhances erection
• Several reported cases of priapism
• Females
• Enhances vaginal lubrication?
• Delayed and inhibited orgasm

28
Anti-Parkinsonian drugs
• Increases dopamine activity• Sexual drive:
– Increases sex drive– Several cases of hypersexuality in men (<1%)– One reported case of hypersexuality in a woman
(levodopa/carbidopa)• Sexual arousal: L-dopa increases erection in men with erectile failure