Embed Size (px)
Citation preview

11
`
PUBLIC -PRIVATE PUBLIC -PRIVATE PARTNERSHIP FOR PARTNERSHIP FOR
HEALTH CARE HEALTH CARE DEVELOPMENTDEVELOPMENT
fi!LH fiajdfjss ixjO—kh i|yd rdcH fi!LH fiajdfjss ixjO—kh i|yd rdcH yd fm!oa.,sl wxYhka fldgialrejka yd fm!oa.,sl wxYhka fldgialrejka
ùuùubyby
Dr A.K.S.B.DE AlwisDr A.K.S.B.DE Alwis
Dr Luxman EdirisingheDr Luxman Edirisinghe

22
Private & public mix Private & public mix (partnership)(partnership)
Government Government hospitalhospital rcfha rcfha frday,frday,
Contracting Contracting out by out by governmentgovernment .sj.sjsiqus.; siqus.; fiajd ,nd .ekSugfiajd ,nd .ekSug
Paying wards Paying wards of governmentof government f.jk jdgsgqf.jk jdgsgq
Private Private hospitalshospitals mqoa.,sl frday,amqoa.,sl frday,a
Public rdcH Private mqoa.,sl
Funding uq,H iemhqu
Public rdcH
Private mqoa.,sl
ProductionProduction ksIamdokhksIamdokh

33
Aims of the partnershipAims of the partnership iyfhda.S;djfha wruqKiyfhda.S;djfha wruqK
1.1. Promote inter and intra-sectoral coordination and Promote inter and intra-sectoral coordination and cooperation for health developmentcooperation for health development.. fi!LH ixjrAOkh i|fi!LH ixjrAOkh i|yd jsjsO fCIa;% w;r iusnkaOSlrKh jrAOkh lsrSuyd jsjsO fCIa;% w;r iusnkaOSlrKh jrAOkh lsrSu
2. 2. Mobilize more resourcesMobilize more resources. . jevsmqr iusm;a jevsmqr iusm;a fhdod .ekSugfhdod .ekSug
3. 3. Reduce the service gapsReduce the service gaps. . fiajd ysoeia wju lsrSugfiajd ysoeia wju lsrSug
4. 4. Promote participation of community and other Promote participation of community and other stakeholdersstakeholders m%cd iyNd.S;ajh jevs lsrSugm%cd iyNd.S;ajh jevs lsrSug
5. 5. Ensure the equity and qualityEnsure the equity and quality. . .=Kd;aul;djh yd .=Kd;aul;djh yd idOdrk;ajh jevslsrSugidOdrk;ajh jevslsrSug
6. 6. Reduce wastage of resourcesReduce wastage of resources. . iusm;a kdia;sh iusm;a kdia;sh jevslsrSugjevslsrSug

44
There are many references to partnershipsThere are many references to partnershipsTo ensure the delivery of comprehensive health service, which reduce the
disease burden and promote health it is proposed -Rationalized health network,(that include allopathic & indigenous as well as public & private services mrsmQrAK fi!LH fiajdjla u.ska frda. ;;ajhlg uqyqK §ug mj;akd l%ufjsoh Yla;su;a lsrSu
Strengthened public-private partnerships to enhance efficient health service delivery. fi!LH fiajd iemhSu ldrAAhlaIu lsrSu i|yd rdcH-fm!oa.,sl fiajd w;r iyfhda.S;dj kxjd,Su
To empower communities towards more active participation in maintaining their health it is proposed to achieve fi!LH kxjd,Su i|yd m%cd iyNd.S;ajh iy;sl lsrSu
Improved participation of civil society and non governmental organizations
in promoting behavioral and life style changes cSjk rgdjka yd mqoa.,sl yeiSrSus rgdjka hym;a lrjSu i|yd isjs,a iudch iy rdcH fkdjk ixjsOdk iyNd.S lrjSu
To strengthen stewardship and management function of the health
system. fi!LH fiajd l<uKdlrk l%shdldrlus jevs oshqKq lsrSu
Strengthened coordination and partnerships with other sectors
(Strategic framework for health development in Sri Lanka,2004-2005\April 2003)

55
Health care Priority areas of the GovernmentHealth care Priority areas of the Government rdcH fi!LH ixrÌKfha m%uqL;djhka rdcH fi!LH ixrÌKfha m%uqL;djhka
EExpand access to curative health care services through hospitals and other xpand access to curative health care services through hospitals and other providers at the district level to move their services more accessible in poor and providers at the district level to move their services more accessible in poor and rural areas.rural areas.wvq jrm%ido,dNS ÿIalr m%foaYj, ck;dj i|yd fi!LH fiajdjka flfrys m%fõYhka wvq jrm%ido,dNS ÿIalr m%foaYj, ck;dj i|yd fi!LH fiajdjka flfrys m%fõYhka osia;s%la uÜgñka mq,q,a lsrSuosia;s%la uÜgñka mq,q,a lsrSu
EExpand the services to meet the needs of specific groups such as elderly, victims xpand the services to meet the needs of specific groups such as elderly, victims of war, displaced people, and specific health problems such as occupational health, of war, displaced people, and specific health problems such as occupational health, mental health, estate health etc…mental health, estate health etc… jhia.;jQjka, hqO mSä;hska iy wj;eka jQjka jhia.;jQjka, hqO mSä;hska iy wj;eka jQjka jeks úfYaIs; lKavdhï j, fi!LH wjYH;djka iy jD;a;Sh fi!LH, udkisl fi!LH iy j;= jeks úfYaIs; lKavdhï j, fi!LH wjYH;djka iy jD;a;Sh fi!LH, udkisl fi!LH iy j;= ck;djf.a fi!LH jeks úfYaIs; .eg,q ksrdlrKh lsrSu i|yd fi!LH fiajdjka mq,q,a ck;djf.a fi!LH jeks úfYaIs; .eg,q ksrdlrKh lsrSu i|yd fi!LH fiajdjka mq,q,a lsrSu lsrSu
DDevelopment of health promotion programs with specific emphasis on outreach evelopment of health promotion programs with specific emphasis on outreach through the schedule.through the schedule. fi!LH m%jrAOkh i|yd ÿria: jevigyka ilia lsrSu fi!LH m%jrAOkh i|yd ÿria: jevigyka ilia lsrSu
HHealth care financial options and partnershipsealth care financial options and partnerships
fi!LH ixrÌKfha uQ,Huh úl,amhka iy odhl;ajhkafi!LH ixrÌKfha uQ,Huh úl,amhka iy odhl;ajhka
HHuman Resource Developmentuman Resource Development. . udkj iïm;a ixjO—Khudkj iïm;a ixjO—Kh

66
Policy Issue: m%;sm;a;suh .eg,qj
Strengthening of public - private partnership in development of health care delivery system in NWP of Sri Lanka. jhT m<df;a fi!LH ;;ajh kxjd,Su i|yd rdcH yd mqoa.,sl wxY j,
iyfhda.S;djh Yla;su;a lsrSu
Policy Vision : Harmonious Public Private- partnership contributing to highest possible level of health for the people of NWP jhT m<df;a ck;djg b;du;au by, ugsgfus fi!LH fiajdjla ,nd §u i|yd rdcH iy mqoa.,sl wxY j, ukd odhlFjh iy;sl lsrSu
Policy Mission : To strengthen public -private- partnership in health care delivery fi!LH fiajdj i|yd rdcH iy mqoa.,sl wxY j, iyfhda.S;dj ,n§u
Policy Goal : To ensure the private sector participation in health care provision in NWP. jhT m<df;a fi!LH fiajdj iemhSfus§ mqoa.,sl wxYfha odhlFjh ,nd .ekSu

77

88
– Internal factorsInternal factors
• • Health care provision in essentially needs multi-sectoral collaboration. Health care provision in essentially needs multi-sectoral collaboration. fi!LH fiajd iemhSu i|yd w;HjYH f,ig jsjsO fCI;% j, odhlFjh u; mokus jSufi!LH fiajd iemhSu i|yd w;HjYH f,ig jsjsO fCI;% j, odhlFjh u; mokus jSu
• • To reduce rising cost in health care provision. To reduce rising cost in health care provision. jevsjk fi!LH fiajd jshou md<kh lsrSujevsjk fi!LH fiajd jshou md<kh lsrSu
• • To ensure the quality assurance in health care provision. To ensure the quality assurance in health care provision. fiajd iemhSfus .=Kd;aul ;;ajh wdrlaId lsrSug wjYH jSufiajd iemhSfus .=Kd;aul ;;ajh wdrlaId lsrSug wjYH jSu
• • To ensure accessibility in health care provision. To ensure accessibility in health care provision. fi!LH fiajdj ,nd.ekSug we;s yelshdj iy;sl lsrSufi!LH fiajdj ,nd.ekSug we;s yelshdj iy;sl lsrSu
• • To ensure the cost effectiveness of health strategies. To ensure the cost effectiveness of health strategies. fi!LH Wmdh udrA. j, M,odhs;djh iqrlaIs; lsrSu i|yd fi!LH Wmdh udrA. j, M,odhs;djh iqrlaIs; lsrSu i|yd
• • To ensure stakeholder participation in health policy implementation. To ensure stakeholder participation in health policy implementation. fi!LH m%;sm;a;s l%shd;aul lsrSfuS§ jsjsO mdrAYjlrejkaf.a iyNd.SFjh iy;sl fi!LH m%;sm;a;s l%shd;aul lsrSfuS§ jsjsO mdrAYjlrejkaf.a iyNd.SFjh iy;sl
lsrSug wjYH jSu lsrSug wjYH jSu
• • To resource sharing for better service delivery. To resource sharing for better service delivery. hym;a fiajdjka iemhSu i|yd iusm;a ksis whqrska fhdod .ekSug wjYH jSuhym;a fiajdjka iemhSu i|yd iusm;a ksis whqrska fhdod .ekSug wjYH jSu
• • To achieve national health objectives. To achieve national health objectives. cd;sl fi!LH wruqK lrd ,.d jSugcd;sl fi!LH wruqK lrd ,.d jSug

99
Evidence from international health agenciesEvidence from international health agenciescd;Hka;r fi!LH ixjsOdk j,ska ,efnk idÌscd;Hka;r fi!LH ixjsOdk j,ska ,efnk idÌs
WHO policy direction focuses on six priority WHO policy direction focuses on six priority areas, areas,
f,dal fi!LH ixúOdkfha ih jeoEreï m%uqL;djhkaf,dal fi!LH ixúOdkfha ih jeoEreï m%uqL;djhkaHealth sector reform & health system development.Health sector reform & health system development.
fi!LH m%;sixialrKh iy ixjO_khfi!LH m%;sixialrKh iy ixjO_kh
Communicable diseases control.Communicable diseases control.
fndajk frda. md,khfndajk frda. md,kh
Promoting healthy life styles & reducing environmental risk factors, Promoting healthy life styles & reducing environmental risk factors,
fi!LH iïmkak cSjk rgd m%jO_kh iy mdrsirsl wjOdku wju lsrSufi!LH iïmkak cSjk rgd m%jO_kh iy mdrsirsl wjOdku wju lsrSu
Integrating health services to enhance efficiency & effectiveness. Integrating health services to enhance efficiency & effectiveness.
ldrAhÌu;djh iy M,odhs;djh jeä lsrSu i|yd fi!LH fiajdjka wka;rA.%yKh ldrAhÌu;djh iy M,odhs;djh jeä lsrSu i|yd fi!LH fiajdjka wka;rA.%yKh lsrsulsrsu
Emergency preparedness & response.Emergency preparedness & response.
yosis wjia:djka i|yd iQodkïùu iy m%;spdr oelaùuyosis wjia:djka i|yd iQodkïùu iy m%;spdr oelaùu
Partnership & coordination.Partnership & coordination. iyfhda.S;djh iy iïnkaO;djhiyfhda.S;djh iy iïnkaO;djh

1010
Financial Evidence uQ,Huh idOl
Cost of Health: fi!LH fiajdfõ nerlï
In 1994 World Bank assured that basic package for health should be US$ 13 per person (WB,1994). The Sri Lankan government has been spending around US$ 10 (Annual Health Bulletine,2000).
If Sri Lanka wants to subsidize the health system, the
following new challenges should be addressed Y%S ,xld rch fi!LH iqNidOkh iemhSfïoS uqyqKoshhq;= kj wNsfhda.
1. Increasing elderly populations jeäjk jeäysá ck.yKh
2. NCD fnda fkdjk frda.
3. HIV/AIDS tps whs jS tavsia
4. Unfinished work in communicable diseases & malnutrition ksu fkdjQ fndajk frda. iy ukaofmdaIKh ms<sn| lghq;=
5. Dengue fvx.= frda.h
1991 § uQ,sl fi!LH fiajdjla iemhSu i|yd rgla jsiska wju jYfhka we fvd,rA 15la tla mqoa.,hl= i|yd jirlg jeh l, hq;= nj m%ldY lrk ,§ tfy;a tu ld,fha§ Y%S ,xldj ta i|yd jeh lrkq ,enqfjs we fvd,rA 10ls ^cd;sl fi!LH m%ldYh 2005&

1111
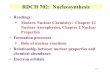
Estimatied Growth of Health Expenditure by govenrnment of Sri Lanka -1996-2015
0
50
100
150
2001996
1998
2000
2002
2004
2006
2008
2010
2012
2014
Year
Bil
lio
ns o
f R
s.
Low GDP Growth
Madium GDP Growth
High GDP Growth
This shows that public expenditure for health could rise from about 20 Billion Rupees in 2003 to between 70 & 173 billion Rupees in 2015.
ta wkqj 2003È ns,shk 20la jq rdcH jshou 2015§ ns,shk 70-173 olajd jkq we;
Source: Sri Lanka Health Financing Scenarios, 2000 to 2015
Y%S ,xldfjs rdcH wxYfha fi!LH i|yd jshou 1996-2015

1212
Total Government Expenditures by Function, 1997
42%
21%
11%
4%
20%
0%0%2%
In-patient care
Ambulatory care
Services of rehabilitative care
Ancillary services to medicalcare
Medical goods dispensed toout-patients
Preventive and Public healthservices
Health programmeadministration and insurance
Capital formation
Source: National health Accounts-2002

1313
Total Government Expenditures by Function, 1997
42%
21%
11%
4%
20%
0%0%2%
In-patient care
Ambulatory care
Services of rehabilitative care
Ancillary services to medicalcare
Medical goods dispensed toout-patients
Preventive and Public healthservices
Health programmeadministration and insurance
Capital formation
fkajdisl frda.S fiajd
idhksl
mqkre;a:dmk fiajd
wdOdrl fiajd
T!IO yd iemhSus ^ndysr frda.S&
frda. ksjdrK yd m%cd fi!LH fiajd
fi!LH mrsmd,khl<uKdlrKh
iuia: rdcH fi!LH jshous 1997
cd;sl fi!LH uq,H m%ldYh 2002

1414
Total Non-Government Expenditures by Function, 1997
31%
9%47%
10%
0%
1%2%
In-patient care
Ambulatory care
Services of rehabilitativecare
Ancillary services tomedical care
Medical goods dispensedto out-patients
Preventive and Publichealth services
Health programmeadministration andinsurance
Source: National health Accounts-2002

1515
Total Non-Government Expenditures by Function, 1997
31%
9%47%
10%
0%
1%2%
In-patient care
Ambulatory care
Services of rehabilitativecare
Ancillary services tomedical care
Medical goods dispensedto out-patients
Preventive and Publichealth services
Health programmeadministration andinsurance
fkajdisl frda.S fiajd
idhksl
mqkre;a:dmk fiajd
wdOdrl fiajd
T!IO yd iemhSus ^ndysr frda.S&
frda. ksjdrK yd m%cd fi!LH fiajd
fi!LH mrsmd,khl<uKdlrKh
iuia: rdcH fkdjk fi!LH jshous 1997
cd;sl fi!LH uq,H m%ldYh 2002

1616
24
Variation in Government Expenditures on health by Province
Western
Central Southern
North-Western
North Central
Uva
Sabaragamuwa
North Eastern
-30
-20
-10
0
10
20
30
40
50
60
Dev
iati
on
in G
ove
rnm
ent
Sp
end
ing
as
% o
f N
atio
nal
Ave
rag
e
Source: National health Accounts-2002
rdcH jshous j, m<d;a wkqj fjkialus

1717
Trends in Total Expenditure on Health, 1990-1999
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Rs. M
illio
n
Normal Constant 1997 prices
1999 – 1999 jir j, fi!LH wdfhdack

1818
rdPHrdPH fm!oa.,slfm!oa.,sl Pd;sl iuia:hPd;sl iuia:h
Pd;sl fi!LH jshouPd;sl fi!LH jshouFunding of national health Funding of national health expenditureexpenditure
50%50% 50%50% 3.4% of DGP-o< Pd;sl 3.4% of DGP-o< Pd;sl ksIamdokfha mqoa.,fhl= f,iksIamdokfha mqoa.,fhl= f,i
Pd;sl fi!LH jshoï Pd;sl fi!LH jshoï Wmfhda.s;djhWmfhda.s;djhUse of national health expenditureUse of national health expenditure
51%51% 49%49% 3.4% of DGP -3.4% of DGP -o< Pd;sl o< Pd;sl ksIamdokfha mqoa.,fhl= ksIamdokfha mqoa.,fhl= ioydioyd
frday,a fiajdjfrday,a fiajdj Hospital ServicesHospital Services
uq,H iemhquuq,H iemhqu
FundingFunding
87%87% 13%13% 1.4% of DGP-1.4% of DGP-o< Pd;sl o< Pd;sl ksIamdokfha mqoa.,fhl= ksIamdokfha mqoa.,fhl= ioydioyd
weoka ixLHdjweoka ixLHdj Bed availableBed available 96%96% 4%4% 3.0 per 1000 capita - 3.0 per 1000 capita - mqoa.,fhl= ioydmqoa.,fhl= ioyd
fkajdisl frda.skafkajdisl frda.ska Inpatient Inpatient admissionsadmissions
96%96% 4%4% 19.4 pre 100 capita -19.4 pre 100 capita -mqoa.,fhl= ioydmqoa.,fhl= ioyd
ndysr frda.s fiajdjndysr frda.s fiajdj
frdy,a fkdjk fiajdjfrdy,a fkdjk fiajdj 26%26% 74%74% 2.8% of DGP-2.8% of DGP-o< Pd;sl o< Pd;sl ksIamdokfha mqoa.,fhl= ksIamdokfha mqoa.,fhl= ioydioyd
frdy,a fkdjk fjk;a fiajdfrdy,a fkdjk fjk;a fiajd 27%27% 73%73%
Ndysr frda.s meusKsuNdysr frda.s meusKsu 48%48% 52%52% 3.9 per capita -3.9 per capita -mqoa.,fhl= ioydmqoa.,fhl= ioyd
Pd;sl fi!LH uq,H m%ldYh-2000National Health Accounts

1919
Total Expenditure on Health at Current Market Prices, 1990-99Total Expenditure on Health at Current Market Prices, 1990-99 19901990 19911991 19921992 19931993 19941994 19951995 19961996 19971997 19981998 19991999
Total public sources (Rs. Billion)Total public sources (Rs. Billion) 5.65.6 5.55.5 7.17.1 6.96.9 8.48.4 10.810.8 12.512.5 1414 17.717.7 19.219.2
Total private sources (Rs. Billion)Total private sources (Rs. Billion) 5.65.6 6.36.3 7.57.5 8.38.3 9.89.8 11.511.5 12.612.6 14.314.3 16.916.9 2020
Total national expenditures (Rs. Billion)Total national expenditures (Rs. Billion) 11.211.2 11.711.7 14.614.6 15.315.3 18.218.2 22.322.3 25.125.1 28.428.4 34.634.6 39.239.2
Source: National health Accounts-2002
Total Expenditure on Health at Current Market Prices, 1990-99
0
5
10
15
20
25
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Rs.
Bill
ion
Total public sources (Rs. Billion) Total private sources (Rs. Billion)
iuia: rdcH iy fm!oa.,sl fi!LH fiajdjka i|yd jshou 1990-99

2020
National Health Expenditures by Source as Share of GDP
1.7%1.7%1.6%1.6%1.6%1.4%1.4%1.7%
1.5%1.7%
1.7%
1.7%1.7%
1.8%
1.7%1.7% 1.6% 1.6%
1.6%1.9%
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
1990 1991 1992 1993 1994 1995 1996 1997 1998(Provisional)
1999(Provisional)
Total government Total private
%
Source: National health Accounts-2002
National Health Expenditures by Source as Share of GDP fi!LH jshou o< foaYSh ksYamdokfha m%;sY;hla f,i

2121
Component of private Health Sector Component of private Health Sector fm!oa.,sl fi!LH fiajdfjs wx.hkafm!oa.,sl fi!LH fiajdfjs wx.hka
Private hospitals and nursing homes Private hospitals and nursing homes fm!oa.,sl frday,a iy ud;D ksjdifm!oa.,sl frday,a iy ud;D ksjdi
GPs full time (western & Indigenous medicine) GPs full time (western & Indigenous medicine) fm!oa.,sl ffjµ jD;a;sljka ^ngysr foaYSh&fm!oa.,sl ffjµ jD;a;sljka ^ngysr foaYSh&
Private practice of government health workers(MS, Dental Sur. Paramedics) Private practice of government health workers(MS, Dental Sur. Paramedics) rcfha fi!LH ldrH rcfha fi!LH ldrH uKav, j, mqoa.,sl fiajduKav, j, mqoa.,sl fiajd
Private pharmacies -5000 Private pharmacies -5000 fm!oa.,sl T!IO Yd,dfm!oa.,sl T!IO Yd,d
Private laboratories -450 Private laboratories -450 ridhkd.drridhkd.dr
Private ambulance services Private ambulance services .s,ka r: fiajd.s,ka r: fiajd
Contracting out of government services Contracting out of government services rdcH wxYh fj; ,nd fok .sjsiqus .; fiajdrdcH wxYh fj; ,nd fok .sjsiqus .; fiajd
Insurance companies. Insurance companies. rCIK wdh;krCIK wdh;k
Medical Manufactures /agents Medical Manufactures /agents ffjµ ksYamdok ksfhdacs;hka f,Iffjµ ksYamdok ksfhdacs;hka f,I
Traditional healers Traditional healers iusm%odhsl iqj lrkakkaiusm%odhsl iqj lrkakka
Quacks etc… Quacks etc… iqÿiqlus fkdue;s ffjµ ‘ffjµjreka’iqÿiqlus fkdue;s ffjµ ‘ffjµjreka’
^wOHCI-fm!oa.,sl ffjµ fiajd 2005&^wOHCI-fm!oa.,sl ffjµ fiajd 2005&

2222
Province Blood Banks CT/VS Scan MRI Units LithotriptorsWestern 6 6 2 0Southern 0 0 0 0Central 0 1 0 0NEP 0 1 0 0North Western 0 0 0 0Uva 0 0 0 0Sabaragamuwa 0 1 0 0Total 6 9 2 0
Facilities in Private sector Hospitals by Province in 2001
Source: CPCEH 2004
Contribution of Private Health Sector in Sri Lanka
fm!oa.,sl wxYfha odhl;ajh

2323
fm!oa.,sl frday,a - jhT m<d;

2424
Estimated Total Revenue of private hospitals1990-2001
0
500
1000
1500
2000
2500
3000
3500
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Year
Rs
. M
illi
on
Source: CPCEH 2004
fm!oa.,sl wxYfha frday,a j, wdodhu

2525
This shows that estimated private health expenditure to grow from 30 to 34 Billion Rupees in 2002 to between 98 & 291 billion Rupees in 2015.Source: CPCEH 2004
Estimated private health expenditure in Sri Lanka 1999-2015
0
100
200
300
400
Year
Bil
lio
ns o
f R
s.
Elasticity1.1
Elasticity 1.5
fm!oa.,sl wxYfha jshou
2002 § ns,shk 30-34 jk w;r 2015§ ns,shk 98-291 jkq we;

2626
1990 1992 1994 1996 1998 2000 2001Mean beds per reporting hospital 35 37 37 38 36 35 35Total reporting hospitals 44 48 54 57 60 63 64Total beds in reporting hospitals 1,537 1,774 1,969 2,189 2,147 2,187 2,236Total estimated beds 1,607 1,848 2,042 2,266 2,219 2,222 2,271Total estimated hospitals 46 50 56 59 62 64 65Source:Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
Number of beds in private hospitals, Estimates for 1990-2001
Number of Beds in Private Hospitals,
Estimates for 1990-2001
0
500
1,000
1,500
2,000
2,500
1990 1992 1994 1996 1998 2000 2001
Year
valu
e
Mean beds per reporting hospital
Total reporting hospitals
Total beds in reporting hospitals
Total estimated beds
Total estimated hospitals
7
Source: Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
fm!oa.,sl frday,a j, we|ka ixLHdj 1990 - 2001

2727
69%
9%
8%
7%
4% 2% 0%1%
Western
Central
NEP
NWP
Southern
NCP
Uva
Sabaragamuwa
Source: Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
Percentage distribution of private hospital beds by province, 2001
m,d;a wkqj mqoa.,sl frday,a we|ka m%;sY;h -2001

2828
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Year
Source: Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
Private sector admissions as a share of total admissions in the country
mqoa.,sl frday,a fkajdisl frda.Ska uq,q osjhsfka fkajdisl frda.Skaf.a m%;sY;hla f,i

2929
Estimated statistics for Private HospitalsYear 1990-2001 ('000')
0
500
1000
1500
2000
2500
3000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Year.
Total admissions ('000)
Total OP visits ('000)
Bed turnover rate
7
Source: Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001Total admissions ('000) 74 79 87 91 95 104 110 109 110 114 118 122Total OP visits ('000) 419 394 554 616 767 901 1274 1341 1605 1924 2406 2609Bed turnover rate 46 46 47 47 47 47 49 47 50 51 54 54
Estimated statistics for private hospitals, 1990-2001
Source:Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
fm!oa.,sl wxYfha fiajd iemhSu 1992 - 2001
fkajdisl
ndysr

3030
Total inpatient admissions by all hospitals, Estimates for 1990-2001
0
1,000
2,000
3,000
4,000
5,000
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Year
MOH admissions ('000)
Total private hospitaladmissions('000)
Co-operative and estateadmissions ('000) *
Source: Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001MOH admissions ('000) 2,533 2,629 3,024 3,174 3,204 2,949 3,339 3,454 3,791 3,825 4,015 4,091Total private hospital admissions('000) 74 79 87 91 95 104 110 109 110 114 118 122Co-operative and estate admissions ('000) * 20 20 20 20 20 20 20 20 20 20 20 20Total private sector share 3.60% 3.60% 3.40% 3.40% 3.50% 4.00% 3.70% 3.60% 3.30% 3.40% 3.30% 3.40%Source:Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004* Note: Data insufficient to estimate actual trend reliably.
Total inpatient admissions by all hospitals, Estimates for 1990-2001
iuia: fkajdisl frda.S ixLHdj – fm!oa.,sl wxYh 1990 - 2001
fkajdisl frda.Ska we;=,;a lsrSu

3131
Trends in outpatient visits at private hospitals, Estimates for 1990-2001
0
500
1000
1500
2000
2500
3000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
year
Total OP Visits-Colombo ('000)
Total OP Visits-out of colombo ('000)
Total OP visits('000)
Source:Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001Total OP Visits-Colombo ('000) 84 81 195 253 322 476 629 682 1,059 1,429 1,876 2,006Total OP Visits-out of colombo ('000) 336 313 359 363 446 426 645 660 546 495 530 603Total OP visits('000) 419 394 554 616 767 901 1,274 1,341 1,605 1,924 2,406 2,609Colombo share as a % total 20% 20% 35% 41% 42% 53% 49% 51% 66% 74% 78% 77%
Trends in outpatient visits at private hospitals, Estimates for 1990-2001
Source:Ministry of Health IPS-Private hospital survey 1998, CPCEH 2004
iuia: ndysr frda.S fiajdjka – fm!oa.,sl wxYh 1990 - 2001
mqoa.,sl wxYfha we;s ndysr frda.Ska

3232
Current situation in partnership
iyfhda.S;djfha jrA;udk ;;ajh1. No proper legal frame work ukd kS;suh mokula ke;
2. No coordination between two sectors wxY foflys iyiïnkaO;djhla fkdue;
1. Private sector institutions are not registered in health department mqoa.,sl fi!LH wdh;k rcfha ,shdmosxÑ lr fkdue;
2. No feedback mechanisms jsOsu;a ixksfjSok l%ufõohla fkdue;
3. No monitoring mechanisms wëÌK ms<sfj;la fkdue;
3. No participation in health planning & implementation
fi!LH ie,iqï lsrSfï iy l%shd;aul lsrSfï iyNd.S;ajhla fkdue;
4. No quality assurance mechanism for private sector
mqoa.,sl wxYfha ;;ajmd,k l%uhla fkdue;
5. No sharing of resources for the benefit to community
fmd\q iïm;a mrsyrK l%ufõohla fkdue;
6. Wastage and Duplication of works lghq;= oaú.=Kùfuka iïm;a wmf;a hdu

3333

3434
Possible causes for weak partnership\qrAj, iyfhda.S;djhg fya;=01. Lack of tradition in collaboration between two sectors.01. Lack of tradition in collaboration between two sectors.
tjeks iïm%odhla fkdmej;Sutjeks iïm%odhla fkdmej;Su 02. Objectives are differ 02. Objectives are differ tlu wruqKla fkd;sîutlu wruqKla fkd;sîu 03. The weak information 03. The weak information system. system. ÿrAj, ikaksfõokhÿrAj, ikaksfõokh04. Lack of capacity in public sector to manage and 04. Lack of capacity in public sector to manage and
regulate relationship with private sector. regulate relationship with private sector. mqoa.,sl wxYh iu. iïnkaO;d meje;aùfï oÌ;d mqoa.,sl wxYh iu. iïnkaO;d meje;aùfï oÌ;d rdcH wxYh fj; fkd;sîu rdcH wxYh fj; fkd;sîu 05. Political pressure. 05. Political pressure. foaYmd,k n,mEïfoaYmd,k n,mEï 06. Pressure from trade unions 06. Pressure from trade unions other stakeholders in other stakeholders in health. health. jD;a;Sh iñ;s we;=,q wfkl=;a mdY_jlrejkaf.a jD;a;Sh iñ;s we;=,q wfkl=;a mdY_jlrejkaf.a n,mEïn,mEï 07. Mistrust. 07. Mistrust. wúYajdih wúYajdih08. Weakly organized private sector in the country.08. Weakly organized private sector in the country. mqoa.,sl wxYh ;=, ukd ixúOdkh ùula fkd;sîumqoa.,sl wxYh ;=, ukd ixúOdkh ùula fkd;sîu

3535
cont….Possible causes for weak partnershipcont….Possible causes for weak partnership
09. Strong public confidence on government health system 09. Strong public confidence on government health system (socio-cultural influences). (socio-cultural influences).
rdcH wxYh flfrys we;s oeäúYajdihrdcH wxYh flfrys we;s oeäúYajdih
10. Weaknesses of private sector in maintaining quality assurance10. Weaknesses of private sector in maintaining quality assurance mechanism and fulfilling social responsibilities as expected by mechanism and fulfilling social responsibilities as expected by the people the people ck;d wfmaÌdjkag wkqj fiajh ie,iSug mqoa.,sl wxYh wiu;a ck;d wfmaÌdjkag wkqj fiajh ie,iSug mqoa.,sl wxYh wiu;a
ùuùu 11. Dependency of private sector on public sector for human 11. Dependency of private sector on public sector for human resources resources mqoa.,sl wxYh rdcH wxYfha udkj iïm;a u;mqoa.,sl wxYh rdcH wxYfha udkj iïm;a u; hemSuhemSu 12. No legal framework for partnership 12. No legal framework for partnership kS;s iïmdok fkd;sîukS;s iïmdok fkd;sîu 13. Less public interest.13. Less public interest. ck;d Wkkaÿj wvq njck;d Wkkaÿj wvq nj 14. Unsuccessful out comes from partnerships in other sector 14. Unsuccessful out comes from partnerships in other sector fjk;a wxYj, rdcH-mqoa.,sl iúnkaO;djhka widrA:l ùufjk;a wxYj, rdcH-mqoa.,sl iúnkaO;djhka widrA:l ùu

3636
Outcome of weak partnership.Outcome of weak partnership. ÿrAj, iyfhda.S;djfha m%;sM,ÿrAj, iyfhda.S;djfha m%;sM,
01. 01. Uncoordinated activities.Uncoordinated activities.
wixúOdkd;aul l%shdldrlïwixúOdkd;aul l%shdldrlï
The health authorities have no information on private sector The health authorities have no information on private sector investments or activities and private sector, therefore not involved in investments or activities and private sector, therefore not involved in national health policy formulation and their contribution towards national health policy formulation and their contribution towards implementation of national health strategies are not significant.implementation of national health strategies are not significant.
02. Waste of resources from both sectors due to duplication or 02. Waste of resources from both sectors due to duplication or overlapping of investments. overlapping of investments.
iïm;a wmf;a hduiïm;a wmf;a hdu
03. Lack of sound quality- assurance mechanism in private sector.03. Lack of sound quality- assurance mechanism in private sector.
mqoa.,sl wxYfha ukd ;;aj md,khla fkd;sîumqoa.,sl wxYfha ukd ;;aj md,khla fkd;sîu
04.Increasing cost to the government in health care provision.04.Increasing cost to the government in health care provision.
rdcH wxYh wkjYH rdcH wxYh wkjYH úhoula oerSuúhoula oerSu
05. Reluctance from donor agencies 05. Reluctance from donor agencies
m%;smdok imhk wdh;k ukafoda;aidyS m%;smdok imhk wdh;k ukafoda;aidyS ùuùu

3737
Policy options in public-private partnershipPolicy options in public-private partnershipm%;sm;a;suh úl,amm%;sm;a;suh úl,am
1. A national policy should be developed to allow private and other non- 1. A national policy should be developed to allow private and other non- government sectors to actively participate and contribute in optimum government sectors to actively participate and contribute in optimum manner to achieve national health objectives in maximum cost manner to achieve national health objectives in maximum cost effective manner. effective manner. rcfha ueosy;aùfuka m%;sm;a;s ilia lsrSu’ rcfha ueosy;aùfuka m%;sm;a;s ilia lsrSu’
2. Policymakers should achieve this task with the participation and 2. Policymakers should achieve this task with the participation and consultation with all internal and external stakeholders of health. consultation with all internal and external stakeholders of health. ish,q ish,q odhl;ajhka iu. tl.;djhlg meñKSuodhl;ajhka iu. tl.;djhlg meñKSu
3. Formulation of guidelines and protocols for partnership, including 3. Formulation of guidelines and protocols for partnership, including modalities for monitoring. modalities for monitoring. fldgialrejka ùu ms<sn|j ish,q kS;s iy fldgialrejka ùu ms<sn|j ish,q kS;s iy Wmfoia iïmdokh lsrSuWmfoia iïmdokh lsrSu
4. Orientation of private and other non-government sectors on national 4. Orientation of private and other non-government sectors on national health policies and strategies. health policies and strategies. wfkl=;a rdcH fkdjk iy mqoa.,sl wxY wfkl=;a rdcH fkdjk iy mqoa.,sl wxY rcfha fi!LH m%;sm;a;s iy Wmdh udrA. ms<sn| oekqj;a lsrSurcfha fi!LH m%;sm;a;s iy Wmdh udrA. ms<sn| oekqj;a lsrSu
Development of consensus among all stakeholders on partnerships. Development of consensus among all stakeholders on partnerships. mdY_jlrejka w;r wfkHdkH wjfndaOhla we;s lsrSumdY_jlrejka w;r wfkHdkH wjfndaOhla we;s lsrSu
Cont..Cont..

3838
6. The areas of possible partnerships should be identified, both in central and 6. The areas of possible partnerships should be identified, both in central and peripheral level. peripheral level. fldgialrejka ùu wjYH wxY yÿkd .ekSufldgialrejka ùu wjYH wxY yÿkd .ekSu
7. Address to the barriers for partnership. 7. Address to the barriers for partnership. ndOl yÿkd .ekSundOl yÿkd .ekSu
8. Capacity building and sharing of information in both sectors initially and 8. Capacity building and sharing of information in both sectors initially and provision of necessary assistance to the private sector for its development provision of necessary assistance to the private sector for its development and participation. and participation. mqoa.,sl wxYfha iïm;a ixjO_kh i|yd iydh oSumqoa.,sl wxYfha iïm;a ixjO_kh i|yd iydh oSu
9. Formulation of coordinating committees in national and peripheral level. 9. Formulation of coordinating committees in national and peripheral level. cd;sl cd;sl iy m%dfoaYSh kshdul lñgq msysgqùuiy m%dfoaYSh kshdul lñgq msysgqùu
10.Formulation of legal frame works for partnerships.10.Formulation of legal frame works for partnerships. kS;s iïmdokh lsrSukS;s iïmdokh lsrSu11. Operational research to evaluate the existing and identified areas of 11. Operational research to evaluate the existing and identified areas of
partnership. partnership. ióÌK u.ska l%shdldrlï we.ehSuióÌK u.ska l%shdldrlï we.ehSu

3939
Areas where public- private sector partnerships Areas where public- private sector partnerships could be establishedcould be established
rdcH-mqoa.,sl iyfhda.S;djh we;s l<yels fldgiardcH-mqoa.,sl iyfhda.S;djh we;s l<yels fldgia
* Joint policy formulation bodies and coordinated implementation * Joint policy formulation bodies and coordinated implementation of national health strategies. of national health strategies. cd;sl fi!LH m%;sm;a;Ska l%shd;aul lsrSucd;sl fi!LH m%;sm;a;Ska l%shd;aul lsrSu* Supportive services, Cleaning\Transport\ Training\ Security * Supportive services, Cleaning\Transport\ Training\ Security Wmldrl fiajdjka ^msrsisÿ lsrSu/ m%jdykh/ mqyqKqj/ wdrÌl Wmldrl fiajdjka ^msrsisÿ lsrSu/ m%jdykh/ mqyqKqj/ wdrÌl
fiajd&fiajd&* Sharing of information * Sharing of information f;dr;=re fnodyod .ekSuf;dr;=re fnodyod .ekSu* Coordinated curative activities. * Coordinated curative activities. taldnoaO m%;sldr fiajdtaldnoaO m%;sldr fiajd* High tech laboratory & curative services * High tech laboratory & curative services wë;dlaIksl ridhkd.dr iy mwë;dlaIksl ridhkd.dr iy m
%;sldr fiajd%;sldr fiajd* Long-term care * Long-term care oS._ ld,Sk m%;sldroS._ ld,Sk m%;sldr* Community based care * Community based care m%cd fi!LH fiajdm%cd fi!LH fiajd* Rehabilitation * Rehabilitation mqkre;a:dmkhmqkre;a:dmkh* Coordinated investments. * Coordinated investments. taldnoaO wdfhdackhtaldnoaO wdfhdackh* Training of human resource for private sector.* Training of human resource for private sector.
mqoa.,sl wxYh i|yd udkj iïm;a ixjO_khmqoa.,sl wxYh i|yd udkj iïm;a ixjO_kh* Quality assurance mechanism * Quality assurance mechanism ;;ajmd,k l%ufõo;;ajmd,k l%ufõo

4040

4141
PossiblePossible stakeholder reactionstakeholder reactionwfmaÌs; m%;spdrwfmaÌs; m%;spdr
1. Possible antagonism by trade unions 1. Possible antagonism by trade unions
jD;Sh iñ;s úfrdaO;djD;Sh iñ;s úfrdaO;d
2. Political sensitivity2. Political sensitivityfoaYmd,k m%;spdr foaYmd,k m%;spdr
3. Cooperation or resistance by health care managers3. Cooperation or resistance by health care managersfi!LH l<ukdlrKfha m%;sfrdaOhkafi!LH l<ukdlrKfha m%;sfrdaOhka
4. Low Interest from private sector4. Low Interest from private sectormqoa.,sl wxYfha WodiSk njmqoa.,sl wxYfha WodiSk nj
5. Possible resistance of private sector5. Possible resistance of private sectormqoa.,sl wxYfha m%;sfrdaOhmqoa.,sl wxYfha m%;sfrdaOh
6.6. Support from donor agenciesSupport from donor agenciesm%;smdok imhkakkaf.a iyfhda.hm%;smdok imhkakkaf.a iyfhda.h
7.7. Resistance from the publicResistance from the public
uyck úfrdaO;duyck úfrdaO;d

4242
THANK YOU