Embed Size (px)
Citation preview

1
PSU Professional Development Center
Welcomes You!
Carmen SchwisowProgram ManagerTwitter@PSU_HR
www.pdx.edu/professional-development/hrProfessional Development Center

Welcome! • Thank you• Healthcare Reform in PDX HR • How the HR Certificate at Portland State can help• Introduction of Panelists & Program

www.bullardlaw.com
Federal Health Care Reform Laws
The Patient Protection and Affordable Care Act and the companion Health Care and Education Reconciliation Act will affect employee health plans and other benefits
The new laws are phased in over many years Election results and legal challenges may lead to
changes

www.bullardlaw.com
Outstanding Issues
2012 Presidential election States – delay exchange funding? Decline Medicaid
expansion funds? Challenges to contraception mandate Creation of exchanges Guidance pending from IRS/DOL/HHS

www.bullardlaw.com
Provisions Effective in 2012
Four-page (double-sided) summary of benefits Plans must give 60 days’ advance notice of
changes to summaries Penalty for noncompliance – up to $1k per
person per day W-2 reporting on cost of coverage

Women’s Health Care Services
For plan years starting on or after 8/1/12, non-grandfathered plans must include – Well-woman visits Gestational diabetes screening Contraception (subject to exception for religious
employers) Nursing support and supplies Domestic violence screening and counseling
www.bullardlaw.com

www.bullardlaw.com
Provisions Effective in 2013
FSA contributions limited to $2,500 (indexed) Medicare hospital insurance tax increased from
1.45% to 2.35% on employee share for earned income over $200k ($250k if joint)
2.9% excise tax on medical device makers; may be passed on
Employers must give notice of health insurance exchange and premium credits, effective 3/1/13

Provisions Effective in 2014
Play-or-pay mandate for employers with at least 50 FTE employees
Waiting periods limited to 90 days Non-grandfathered plans must cover clinical
trials for cancer or similar conditions Wellness programs may offer up to 30%
reward (up from current 20%)
www.bullardlaw.com

www.bullardlaw.com
Caution!
Multiple bills make for confusion – be careful where you get your information
Guidance regularly being issued by Internal Revenue Service and U.S. Departments of Labor and Health & Human Services
This is general information, not legal advice
Confidential | Planar Systems10
Chiefly competitive reasons
Hard to attract and retain employees without health coverage
There would be a huge advantage to those employers offering health coverage in attracting the best candidates
Confidential | Planar Systems11
Chiefly competitive reasons
Hard to attract and retain employees without health coverage
There would be a huge advantage to those employers offering health coverage in attracting the best candidates

Confidential | Planar Systems12
Employers also continue health coverage
Employers feel moral obligation to provide health coverage Need access to care for employees to be productive Cannot image not offering health coverage in mature industries Wage increases traded for health coverage maintenance in past
Executives demand health coverage Do not want total cost of health coverage to be imputed income now
Cadillac plan results in some imputed income in 2018

Confidential | Planar Systems13
Health Care offered in the US Bureau of Labor Statistics 2009 National Compensation Survey
• Latest data published nationally
• 74% offered medical plan• 76% enroll
• 48% offered dental plan• 79% enroll
• 20% offered vision plan • 77% enroll
• Medical coverage offered to 88% FT ees• Medical coverage offered to 24% PT ees
• 58% PT ees enroll
Greater income, education, skills more likely to have coverage

Healthcare Changes
Challenges and Strategies from an HR Department Manager’s Perspective

Context for Employee Benefits
Financial context: While average wages and salaries have increased by 1-
3% per year recently, medical insurance has increased an average of 9-12%
Benefits constitute 40.2% of payroll costs*
HR Directors need to control costs for both the company and for employees
*US Chamber of Commerce 2004 data
Challenges
Actual and potential cost increases Example: coverage for adult dependents
Last minute changes (grrrrrrr!) Example: changing the FSA limits in the middle of open
enrollment
Administrative / system changes take time Example: we had to cover adult dependents, but carriers
computer systems wouldn’t allow enrollment
Uncertainty In this election year, healthcare reform is a political
football

Strategies
Partner with your benefits broker and insurance carriers for information
Stay nimble… change is pretty much inevitable
Work at balancing business needs with employee needs

1818
is an Independent Licensee of the Blue Cross and Blue Shield Association.
The Regence Group
Jim Walton, Director of New Sales
Regence BlueCross
BlueShield of Oregon
Jim Walton, Director of New Sales
Regence BlueCross
BlueShield of Oregon
Exchange 2.0Fall/Winter 2012 PSU HR Presentation
Exchange 2.0Fall/Winter 2012 PSU HR Presentation
Regence
Blu
eC
ross
Blu
eShie
ld o
f O
regon
is a
n Independent
Lice
nse
e o
f th
e B
lue C
ross
and B
lue S
hie
ld A
ssoci
ati
on
© 2012. The Regence Group, all rights reserved.

19
Oregon Exchange – Structure
•Public corporation- own entity• Similar to SAIF, or OHSU
•Governance:
• Citizen Board – 9 Members• Appointed by the Governor and were confirmed by the Senate-
September 23, 2011 • At least 2 consumer members, and no more than 2 members can
have ties to insurance or health care industry
• Board makes decisions, not recommendations

20
The Oregon Health Insurance Exchange Corporation
Mission Statement
Improving the health of all Oregonians by providing health coverage options, increasing access to information, and fostering quality and value in the health care system.
21
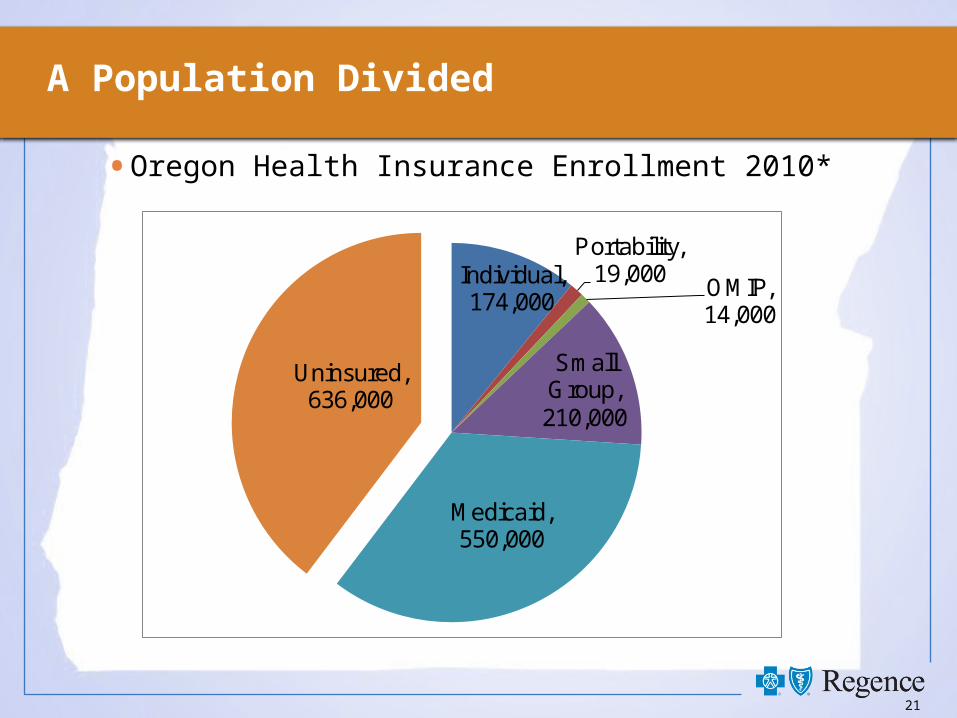
A Population Divided
• Oregon Health Insurance Enrollment 2010*
Individual, 174,000
Portability, 19,000
OMIP, 14,000
Small Group, 210,000
Medicaid, 550,000
Uninsured, 636,000

22
Individual Exchange: Tax Credits and Cost-Sharing Reductions
• Exchange and HHS determine if
individual is eligible for tax subsidy and cost share
subsidy
• Available only to individuals purchasing in Exchange• Sliding credit amount based on 133% - 400% Federal Poverty
Level (FPL)
• Not available to groups members in Exchange
• Cost Sharing Credit available up to 250% FPL• One third, one half or two thirds credit on out of pocket costs

23
Exchange Premium Limits by Income
•Up to 133% FPL: 2.0% of income
•133-150% FPL: 3.0% - 4.0% of income
•150-200% FPL: 4.0% - 6.3% of income
•200-250% FPL: 6.3% -8.05% of income
•250-300% FPL: 8.05% - 9.5% of income
•300-400% FPL: Capped to 9.5% of income
24
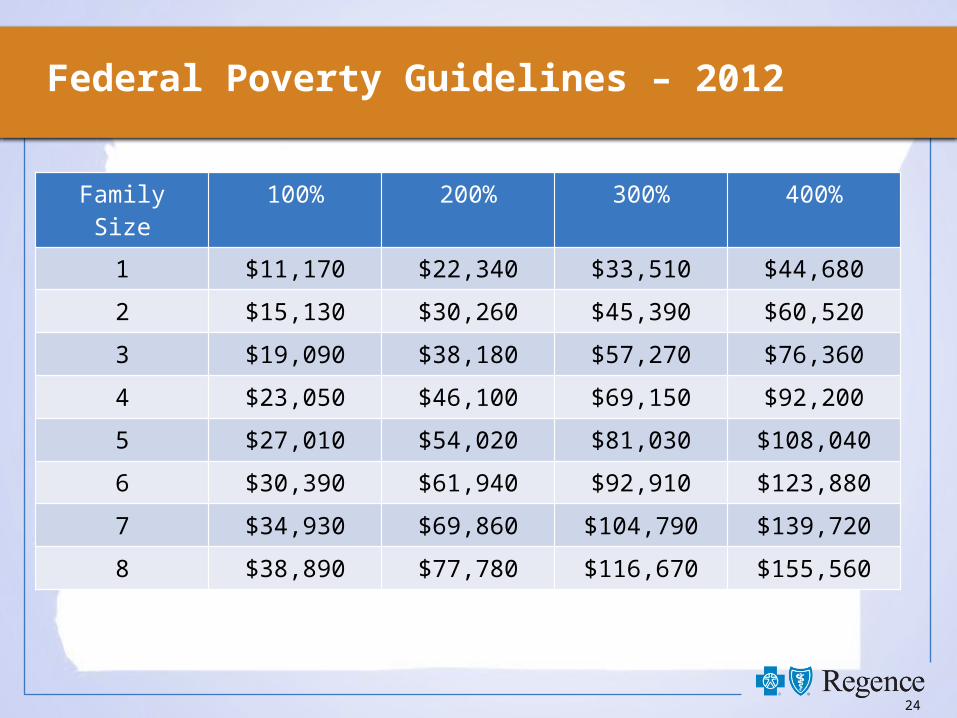
Federal Poverty Guidelines – 2012
Family Size 100% 200% 300% 400%
1 $11,170 $22,340 $33,510 $44,680
2 $15,130 $30,260 $45,390 $60,520
3 $19,090 $38,180 $57,270 $76,360
4 $23,050 $46,100 $69,150 $92,200
5 $27,010 $54,020 $81,030 $108,040
6 $30,390 $61,940 $92,910 $123,880
7 $34,930 $69,860 $104,790 $139,720
8 $38,890 $77,780 $116,670 $155,560

25
Individual Example
• Let’s do some math…Single Parent/Two Kids• $700 monthly premium. (2nd lowest Silver Plan)
• Annual income $38,180 (200% FPL)• Premium percentage is 6.0% of annual income, or $2,223.6 ($185
per month)• Advance credit is $700 (premium) – $185 (max allowed premium
percentage)= $515/month• ½ Cost Subsidy (deductibles, co pays, co-insurance, max out of
pocket)

26
Cost Sharing Subsidies
Cost Subsidy 0% 1/3 1/2 2/3
Federal Poverty Level 251%+ 201-250% 151-200% 133-150%
Actuarial Value - Possible Silver Plan Base - 70% 73% 87% 94%
Deductible - Individual $1,750 $1,750 $500 $50
Maximum out of Pocket - Individual $5,750 $4,000 $1,200 $600
Copay / Coinsuran
ce
Copay / Coinsuran
ce
Copay / Coinsuran
ce
Copay / Coinsuran
ce
Inpatient and Outpatient 30% 30% 30% 10%
Emergency Room 30% 30% 30% 10%
Preventive Visits and Services $0 $0 $0 $0
Office Visits - Primary Care $35 $35 $35 $10
Office Visits - Specialists $60 $60 $60 $25
Prescription Drug - Generic $10 $10 $10 $5
Prescription Drug - Preferred Brand 50% 50% 50% 30%Prescription Drug - Non-Preferred Brand 50% 50% 50% 50%

27
Individual Eligibility

Questions?





























