Embed Size (px)
Citation preview

1
KITSO AIDS Training Program
Lecture 2:
HIV Pathophysiology and Epidemiology
delivered byDr. Daniel J. Baxter, ACHAP

2
Learning Objectives
• Lifecycle of HIV-1.
• CD4 cell and host defense system.
• Natural history of HIV-1 disease.
• Immune responses to HIV-1 and mechanisms of immune evasion by HIV.

3
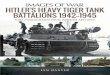
Worldwide Distribution of HIV-1 Viral Subtypes
Australia &New Zealand:
15,000
Source: WHO/UNAIDS (data as of December, 2000)
Caribbean:390,000
Eastern Europe &Central Asia:
700,000
Eastern Asia & thePacific: 640,000
Latin America:1.4 million
Northern Africa &Middle East:
400,000
Northern America:920,000
Southern & Southeastern
Asia:
7 million
Western Europe:540,000
Sub - Saharan Africa:
25.3 million:
B
B
C
BC
C,E
B

4
Viruses
• A virus is the simplest, most primitive life form on earth.
• A virus is unable to replicate (reproduce) on its own and must first infect a living cell in order to replicate.
• HIV is a retrovirus. A retrovirus is an RNA virus which uses DNA as an intermediary for its replication.

5
Human Immunodeficiency Virus

6
HIV-1 Particle

7
HIV Life Cycle

8
CD4
HIV Life Cycle
DNA
RNA
Reverse Transcriptase
RNA
HIVRNA
Protease
CD4 T -Lymphocyte
RNA
Proviral DNA
RNA
RNA
RNA
RNA
RNA

9
HIV Variability

10
HIV Variability
• HIV has enormous potential for change (mutations)
• The HIV copies in an infected person are not all identical but are rather like a swarm of closely related viruses.
• Reverse Transcriptase is a very error-prone enzyme.

11
Effects of HIV Mutations• Mostly of no consequence.
• Viral fitness increased or decreased.
• Viral infectivity/pathogenicity increased or decreased.
• Escape from immune control.
• ARV drug resistance.

12
Immunology

13
Host Defense System
Self versus Non-Self (antigen)
Innate Immunity
Adaptive Immunity
Plasma cells CD4 cells CD8 cells
B-Lymphocytes T-Lymphocytes-Skin, mucosa-Cells White blood cells Macrophages
-Complement
High Specificity/ Memory Cells

14
Helper Function of CD4 Cells
B Lymphocyte
T helper cell (CD4)Macrophage
Antibody secreting (plasma) cell
Infected cell
Cytotoxic T Lymphocyte (CD8)
Killed

15
White Blood Cell Distribution
Absolute/Total
cells/uL
Percent
Neutrophils 4000 55% WBC
Lymphocytes CD4
CD8
1000
500
30% Lymphocytes
Basophils Eosinophils
Monocytes

16
CD4 Counts in Botswana
• Uninfected: 750 cells/uL
(IQR: 560-900)
• Asymptomatic HIV-1 positive: 350 cells/uL (IQR: 268-574)
• Patients with AIDS: 121 cells/uL
(IQR: 50-250)

17
Surrogate Markers of HIV Disease
• CD4 is an indicator of the strength of the immune system.
• Viral Load is an indicator of the amount of viral replication.

18
Natural History of HIV Infection

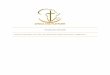
19
AIDS Clinical
Latency
Acute Retroviral Syndrome
Natural History of HIV-1 Infection
1-12 weeks 6-10 years 1-2 years
Vir
al L
oad
C
D4
cou
nt

20
Acute Retroviral Syndrome
1-12 weeks 8-10 years 1-2 years
Vir
al L
oad
CD
4 co
un
t

21
Acute Retroviral Syndrome
• Non-specific ‘flu-like’ symptoms;– Fever– Fatigue– Pharyngitis– Lymphadenopathy– Rash

22
Pathogenesis of Acute HIV-1 Infection
• Initial infection of CD4 cells and macrophages at site of exposure.
• Dissemination of infection to lymph nodes.
• Burst of viral replication results in intense viremia.
• Development of humoral immunity (HIV-specific antibodies).
• Development of cellular immunity (HIV-specific CD4 and CD8 cells).

23
Acute HIV-1 Infection
Viral load
CD4 cell count
0 3 6 12 weeks after HIV infection
HIV-antibodies
V
iral
Lo
ad
CD
4 co
un
t

24
Clinical Latency
1-12 weeks 6-10 years 1-2 years
Vir
al L
oad
C
D4
cou
nt

25
Clinical Latency
• At CD4 cell counts over 500 cells/uL many complications overlap with conditions found in uninfected populations (bacterial pneumonia, tuberculosis, minor skin conditions), but they may be more frequent.
• At CD4 counts between 200 and 500 cells/uL other conditions and opportunistic infections may begin to appear (Kaposi’s sarcoma, oral/genital candidiasis, herpes zoster, etc.).

26
Pathogenesis of Chronic HIV-1 Infection
• High turnover of CD4 cells.
– Continuous destruction and compensatory increased production of CD4 Lymphocytes.
• Viral load plateaus at viral set point.
• Non-specific, generalized, immune activation resulting in immune dysfunction.
• Viral reservoirs in resting infected cells.

27
Relative Control of HIV-1: Viral Set Points
Year 1
Vir
al lo
ad
Predictor for:- Disease progression- Risk of transmission

28
AIDS
1-12 weeks 6-10 years 1-2 years
Vir
al L
oad
C
D4
cou
nt

29

30
Immune Evasion by HIV

31
Inability to Eradicate HIV-1 Infection
• CD4 T cell decline
• CTL response inadequate
• Viral reservoir• Viral infection in sanctuaries (brain and genito-urinary
tract)• Viral persistence in lymphoid tissue• Latency – archiving in resting cells
• Mutational Potential of HIV-1• Escape of HIV from CD8 immune response and
neutralizing antibodies

32
Typical Progressor
Rapid Progressor
Vir
al l
oad
Vir
al l
oad
CD
4 co
un
tC
D4
cou
nt
Variability of Response to HIV Infection
Time
Time

33
Immune Response in Children
• Viral set point is higher in children.
• Disease progression similar to adults.
• 15-20% of children develop AIDS or die within 1 year.
• 10% survive for a prolonged period (5-6 years).

34
Immune Response in Children (2)
• Because the infant’s immune system is immature, disease progression is expressed as CD4%.
• CD4% is the percent of total lymphocytes that are CD4 cells.
– e.g., if total lymphocytes are 4000 cells per uL and 1000 of these cells are CD4 cells, the CD4% is 25%.

35
HIV Transmission and Prevention• Modes of Transmission
• Mucosa (genital/rectal)• Blood (transfusion, MTCT, needle stick injury)• Breast Feeding
• Prevention• Avoidance of infected mucosal secretions• Safe blood transfusion service• Post-exposure prophylaxis• Prevention of Mother-to-Child Transmission• Avoidance of breast feeding
• Universal precautions• Hand washing• Safe disposal of infected material

36
Summary• HIV life cycle involves transcription of viral RNA into
DNA and integration into human genome.
• Mutational potential of HIV-1 results in worldwide diversity (subtypes), viral escape from immune response and development of drug resistance.
• Viral replication persists throughout infection.
• Fundamental pathology is the inability of the host immune system to eradicate HIV infection, which results in progressive destruction of the immune system.