Embed Size (px)
Citation preview
Early versus delayed laparoscopic cholecystectomy for acute
cholecystitis (Review)
Gurusamy KS, Samraj K
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2009, Issue 1
http://www.thecochranelibrary.com
Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
11DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 1 Bile duct injury. . 25
Analysis 1.2. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 2 Bile leak requiring
ERCP. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Analysis 1.3. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 3 Intra-abdominal
collections requiring percutaneous drainage. . . . . . . . . . . . . . . . . . . . . . . . 27
Analysis 1.4. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 4 Superficial infection. 28
Analysis 1.5. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 5 Deep infection. . 29
Analysis 1.6. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 6 Conversion to open
cholecystectomy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Analysis 2.1. Comparison 2 Early versus delayed LC (number of people operated), Outcome 1 Bile duct Injury. . . 31
Analysis 2.2. Comparison 2 Early versus delayed LC (number of people operated), Outcome 2 Bile leak requiring ERCP. 32
Analysis 2.3. Comparison 2 Early versus delayed LC (number of people operated), Outcome 3 Intra-abdominal collections
requiring percutaneous drainage. . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Analysis 2.4. Comparison 2 Early versus delayed LC (number of people operated), Outcome 4 Superficial infection. . 34
Analysis 2.5. Comparison 2 Early versus delayed LC (number of people operated), Outcome 5 Deep infection. . . 35
Analysis 2.6. Comparison 2 Early versus delayed LC (number of people operated), Outcome 6 Conversion to open
cholecystectomy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Analysis 3.1. Comparison 3 Early versus delayed LC - risk difference, Outcome 1 Bile duct injury. . . . . . . . 37
Analysis 3.2. Comparison 3 Early versus delayed LC - risk difference, Outcome 2 Bile leak requiring ERCP. . . . 38
Analysis 3.3. Comparison 3 Early versus delayed LC - risk difference, Outcome 3 Intra-abdominal collections requiring
percutaneous drainage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Analysis 3.4. Comparison 3 Early versus delayed LC - risk difference, Outcome 4 Superficial infection. . . . . . 40
Analysis 3.5. Comparison 3 Early versus delayed LC - risk difference, Outcome 5 Deep infection. . . . . . . . 41
Analysis 3.6. Comparison 3 Early versus delayed LC - risk difference, Outcome 6 Conversion to open cholecystectomy. 42
Analysis 4.1. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 1 Bile duct injury. . . . . . 43
Analysis 4.2. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 2 Bile leak requiring ERCP. . . 43
Analysis 4.3. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 3 Intra-abdominal collections requiring
percutaneous drainage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Analysis 4.4. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 4 Superficial infection. . . . . 45
Analysis 4.5. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 5 Deep infection. . . . . . . 45
Analysis 4.6. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 6 Conversion to open cholecystectomy. 46
Analysis 5.1. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 1 Bile duct injury. . 46
iEarly versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.2. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 2 Bile leak requiring
ERCP. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Analysis 5.3. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 3 Intra-abdominal
collections requiring percutaneous drainage. . . . . . . . . . . . . . . . . . . . . . . . 47
Analysis 5.4. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 4 Superficial infection. 48
Analysis 5.5. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 5 Deep infection. . 48
Analysis 5.6. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 6 Conversion to open
cholecystectomy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Analysis 6.1. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC,
Outcome 1 Bile duct injury. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Analysis 6.2. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC,
Outcome 2 Bile leak requiring ERCP. . . . . . . . . . . . . . . . . . . . . . . . . . 50
Analysis 6.3. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC,
Outcome 3 Intra-abdominal collections requiring percutaneous drainage. . . . . . . . . . . . . . 50
Analysis 6.4. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC,
Outcome 4 Superficial infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Analysis 6.5. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC,
Outcome 5 Deep infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Analysis 6.6. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC,
Outcome 6 Conversion to open cholecystectomy. . . . . . . . . . . . . . . . . . . . . . 52
Analysis 7.1. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies),
Outcome 1 Bile duct injury. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Analysis 7.2. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies),
Outcome 2 Bile leak requiring ERCP. . . . . . . . . . . . . . . . . . . . . . . . . . 53
Analysis 7.3. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies),
Outcome 3 Intra-abdominal collections requiring percutaneous drainage. . . . . . . . . . . . . . 53
Analysis 7.4. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies),
Outcome 4 Superficial Infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Analysis 7.5. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies),
Outcome 5 Deep infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Analysis 7.6. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies),
Outcome 6 Conversion to open cholecystectomy. . . . . . . . . . . . . . . . . . . . . . 55
55ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
59APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
60FEEDBACK . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
63DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
63INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiEarly versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Early versus delayed laparoscopic cholecystectomy for acutecholecystitis
Kurinchi Selvan Gurusamy1, Kumarakrishnan Samraj2
1University Department of Surgery, Royal Free Hospital and University College School of Medicine, London, UK. 2Department of
General Surgery, John Radcliffe Hospital, Oxford, UK
Contact address: Kurinchi Selvan Gurusamy, University Department of Surgery, Royal Free Hospital and University College School of
Medicine, 9th Floor, Royal Free Hospital, Pond Street, London, NW3 2QG, UK. [email protected].
Editorial group: Cochrane Hepato-Biliary Group.
Publication status and date: Edited (no change to conclusions), published in Issue 1, 2009.
Review content assessed as up-to-date: 9 August 2006.
Citation: Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Cochrane Database ofSystematic Reviews 2006, Issue 4. Art. No.: CD005440. DOI: 10.1002/14651858.CD005440.pub2.
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Gallstones are present in about 10% to 15% of the adult western population. Between 1% and 4% become symptomatic in a year.
Cholecystectomy for symptomatic gallstones is mainly performed after the acute cholecystitis episode settles because of the fear of
higher morbidity and conversion from laparoscopic cholecystectomy to open cholecystectomy during acute cholecystitis.
Objectives
The aim was to compare the early laparoscopic cholecystectomy (less than seven days of onset of symptoms) versus delayed laparoscopic
cholecystectomy (more than six weeks after index admission) with regards to benefits and harms.
Search methods
We searched The Cochrane Hepato-Biliary Group Controlled Trials Register, the Cochrane Central Register of Controlled Trials (CENTRAL)
in The Cochrane Library, MEDLINE, EMBASE, and Science Citation Index Expanded until November 2005.
Selection criteria
We considered for inclusion all randomised clinical trials comparing early versus delayed laparoscopic cholecystectomy for acute
cholecystitis.
Data collection and analysis
We collected the data on the characteristics of the trial, methodological quality of the trials, mortality, morbidity, conversion rate,
operating time, and hospital stay from each trial. We analysed the data with both the fixed-effect and the random-effects models using
RevMan Analysis. For each outcome we calculated the odds ratio (OR) with 95% confidence intervals (CI) based on intention-to-treat
analysis.
Main results
We included five trials with 451 patients randomised: 223 to the early group and 228 to the delayed group. Surgery was performed
on 222 patients in the early group and on 216 patients in the delayed group. There was no mortality in any of the trials. Four of the
five trials were of high methodological quality. There was no statistically significant difference between the two groups for any of the
1Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

outcomes including bile duct injury (OR 0.63, 95% CI 0.15 to 2.70) and conversion to open cholecystectomy (OR 0.84, 95% CI 0.53
to 1.34). Various other analyses including ’available case analysis’, risk difference, statistical methods to overcome the ’zero-event trials’
showed no statistically significant difference between the two groups in any of the outcomes measured. A total of 40 patients (17.5%)
from the delayed group had to undergo emergency laparoscopic cholecystectomy due to non-resolving or recurrent cholecystitis; 18
(45%) of these had to undergo conversion to open procedure. The total hospital stay was about four days shorter in the early group
compared with the delayed group.
Authors’ conclusions
Early laparoscopic cholecystectomy during acute cholecystitis seems safe and shortens the total hospital stay. The majority of the
outcomes occurred rarely; hence, the confidence intervals are wide. Therefore, further randomised trials on the issue are needed.
P L A I N L A N G U A G E S U M M A R Y
Early laparoscopic cholecystectomy during acute cholecystitis is safe and shortens the total hospital stay
Cholecystectomy for symptomatic gallstones is mainly performed after an acute cholecystitis episode settles. The main reason is the
fear of higher morbidity and conversion from laparoscopic cholecystectomy to open cholecystectomy during acute cholecystitis. This
systematic review of five randomised trials shows that there is no significant difference in the complication rate or the conversion rate
in regard to the time when the laparoscopic cholecystectomy is performed during acute cholecystitis versus performed 6 to 12 weeks
after the symptoms settle. No mortality was reported in any of the trials. Early laparoscopic cholecystectomy during acute cholecystitis
appears to be safe and shortens the total hospital stay.
B A C K G R O U N D
About 10% to 15% of the adult western population have gall-
stones (Janzon 1985; Jørgensen 1987; NIH 1992; Muhrbeck
1995; Halldestam 2004). Between 1% and 4% become symp-
tomatic in a year (NIH 1992; Halldestam 2004). More than half
a million cholecystectomies are performed per year in the United
States alone (NIH 1992). Regional differences exist in the chole-
cystectomy rates (Mjäland 1998). Laparoscopic cholecystectomy,
which was introduced in 1987, is now the preferred method of
cholecystectomy (NIH 1992; Fullarton 1994; Bakken 2004).
There is a considerable controversy regarding the timing of laparo-
scopic cholecystectomy in acute cholecystitis. While early open
cholecystectomy has no increased morbidity or mortality over de-
layed open cholecystectomy (Papi 2004) and delayed cholecystec-
tomy increases the risks of further gallstone related complications
(Lawrentschuk 2003; Papi 2004), there are concerns about higher
morbidity rates in laparoscopic cholecystectomy performed as an
emergency procedure (Cuschieri 1991; Wilson 1991; Kum 1996)
and about the higher conversion rate to open procedure during
the acute phase (Cheema 2003; Livingston 2004). While one of
the main reasons for conversion in early laparoscopic cholecystec-
tomy is inflammation obscuring the view of Calot’s triangle (Peng
2005), the main reason for conversion in the delayed group is fi-
brotic adhesions (Lo 1998; Peng 2005). Severe inflammation is
also one of the important reasons for bile duct injury (Richardson
1996). There are also reports that the hospital stay is longer in
early performed cholecystectomy (Lo 1996).
Only about 30% of the laparoscopic cholecystectomies in the
United States are performed during acute cholecystitis (Livingston
2004). Only 20% of surgeons in the United Kingdom perform
laparoscopic cholecystectomy during acute cholecystitis (Senapati
2003). We have not been able to identify any Cochrane review
comparing early and delayed laparoscopic cholecystectomy in pa-
tients with acute cholecystitis. We identified three previous meta-
analyses related to the topic. Two of these (Papi 2004; Shikata
2005) included both open and laparoscopic cholecystectomy for
comparison. The first (Papi 2004) included only two trials. The
second meta-analysis included three trials. Both these meta-anal-
yses (Papi 2004; Shikata 2005) included a trial by Chandler et
al (Chandler 2000) that in fact examined two different surgical
strategies for early treatment. The most recent meta-analysis by
Lau et al (Lau 2006) also included three studies. One of these was
the study by Serralta et al (Serralta 2003) in which the allocation
was by surgeon’s experience and hence is not a randomised trial
at all. However, all three meta-analyses found no significant dif-
ference in the morbidity between early and delayed laparoscopic
cholecystectomy in patients with acute cholecystitis.
2Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

O B J E C T I V E S
To assess the benefits and harms of early laparoscopic cholecys-
tectomy compared with delayed laparoscopic cholecystectomy in
patients with acute cholecystitis. The following null hypothesis
was tested: there is no difference in outcome between early and
delayed laparoscopic cholecystectomy in acute cholecystitis.
M E T H O D S
Criteria for considering studies for this review
Types of studies
We included all randomised clinical trials, which compare early
versus delayed laparoscopic cholecystectomy in acute cholecystitis
(irrespective of language, blinding, or publication status).
Quasi-randomised trials (where the method of allocating partici-
pants to a treatment are not strictly random, for example, date of
birth, hospital record number, alternation) were not included.
Types of participants
Patients with acute cholecystitis who are about to undergo laparo-
scopic cholecystectomy.
Types of interventions
We included only trials comparing early versus delayed laparo-
scopic cholecystectomy (irrespective of the size and the number
of ports or abdominal lift or open or closed method of induc-
tion of pneumoperitoneum). Early laparoscopic cholecystectomy
is defined as laparoscopic cholecystectomy performed within seven
days of onset of symptoms. Delayed laparoscopic cholecystectomy
is defined as laparoscopic cholecystectomy, which was intended to
be performed after six weeks of index admission.
Types of outcome measures
Primary outcomes
1. Morbidity.
i) Complications (pancreatitis, recurrent episodes of
cholecystitis, obstructive jaundice).
ii) Surgery related morbidity (bile duct injury, bile leak,
reoperation rate, infection, bleeding).
2. Conversion to open cholecystectomy.
3. Mortality.
Secondary outcomes
1. Hospital stay.
2. Operating time.
Other outcome measures mentioned by individual trials were
recorded for each trial. The data of the above outcome measures
were extracted. In addition, the data on language of publication
and inclusion and exclusion criteria for each study were extracted.
Search methods for identification of studies
See: Hepato-Biliary Group strategy (Gluud 2006).
We searched The Cochrane Hepato-Biliary Group Controlled TrialsRegister, the Cochrane Central Register of Controlled Trials (CEN-TRAL) in The Cochrane Library, MEDLINE, EMBASE, and Sci-ence Citation Index Expanded. We have given the search strategies
and the time span of the searches in Appendix 1.
We did not apply any language or publication status restrictions.
Both of us, independently of each other, identified the trials for
inclusion. We resolved any differences in opinion through discus-
sion.
References of the identified trials were also searched for identifying
further trials.
Data collection and analysis
We assessed the methodological quality of the trials independently,
without masking of the trial names. We sought any unclear or
missing information by contacting the authors of the individual
trials. We resolved any differences by discussion.
Assessment of methodological quality
We followed the instructions given in the Cochrane Reviewer’s
Handbook (Higgins 2005).
Due to the risk of overestimation of intervention effects in ran-
domised trials with unclear or inadequate methodological quality
(Schulz 1995; Moher 1998; Kjaergard 2001), we looked at the
influence of methodological quality of the trials on the trial results
by evaluating the reported randomisation and follow-up proce-
dures in each trial. We assessed generation of allocation sequence,
allocation concealment, and follow-up.
Generation of the allocation sequence
• Adequate, if the allocation sequence was generated by a
computer or random number table. Drawing of lots, tossing of a
coin, shuffling of cards, or throwing dice was considered as
adequate if a person who was not otherwise involved in the
recruitment of participants performed the procedure.
• Unclear, if the trial was described as randomised, but the
method used for the allocation sequence generation was not
described.
• Inadequate, if a system involving dates, names, or
admittance numbers were used for the allocation of patients.
3Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

These studies are known as quasi-randomised and were excluded
from the review.
Allocation concealment
• Adequate, if the allocation of patients involved a central
independent unit, on-site locked computer, or sealed envelopes.
• Unclear, if the trial was described as randomised, but the
method used to conceal the allocation was not described.
• Inadequate, if the allocation sequence was known to the
investigators who assigned participants or if the study was quasi-
randomised.
Follow-up
• Adequate, if the numbers and reasons for dropouts and
withdrawals in all intervention groups were described or if it was
specified that there were no dropouts or withdrawals.
• Unclear, if the report gave the impression that there had
been no dropouts or withdrawals, but this was not specifically
stated.
• Inadequate, if the number or reasons for dropouts and
withdrawals were not described.
Blinding was not assessed since we expected that there were no
double-blind trials. However, we registered if trials used blinded
assessment of outcomes. There were no trials which used blinded
assessment of outcomes.
Statistical methods
We performed the meta-analyses according to the recommenda-
tions of The Cochrane Collaboration (Higgins 2005).
We used the software package RevMan Analyses 1.0 (RevMan
2003) provided by The Cochrane Collaboration for analysis. For
dichotomous variables, we calculated the odds ratio with 95% con-
fidence interval. We used the random-effects model (DerSimonian
1986) and the fixed-effect model (DeMets 1987).
We performed subgroup analyses depending on the methodologi-
cal quality of the trials in order to compare the intervention effect
in trials with adequate methodological quality to that of trials with
unclear or inadequate methodological quality. We also performed
sub-group analyses to determine whether trials, which included
only patients with less than four days of symptoms were different
to those, which included patients with symptoms for seven days.
We also performed subgroup analysis to determine whether the
results varied with surgical experience.
We explored the heterogeneity using the chi-squared test with sig-
nificance set at P value 0.10 and measured the quantity of hetero-
geneity using I2 (Higgins 2002).
We performed all the analyses based on the intention-to-treat prin-
ciple (Newell 1992). We also performed the available case analy-
sis (Higgins 2005) to check whether the results changed. We also
performed a sensitivity analysis with and without empirical con-
tinuity correction factors as suggested by Sweeting et al (Sweeting
2004) for ’zero-event trials’. We performed this using StatsDirect
2.4. We also calculated the risk difference between the interven-
tion groups in order to take into account the ’zero-event trials’
using RevMan 2003.
We used a funnel plot to explore publication bias and other bias
(Egger 1997; Macaskill 2001). We used asymmetry in funnel plot
of study size against treatment effect to identify bias. We also
performed linear regression approach described by Egger et al (
Egger 1997) to determine the funnel plot asymmetry. We used
StatsDirect 2.4 for this purpose.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
We identified a total of 4886 references through the electronic
searches of The Cochrane Hepato-Biliary Group Controlled Tri-als Register and the Cochrane Central Register of Controlled Trials(CENTRAL) in The Cochrane Library (n = 742), MEDLINE (n =
1263), EMBASE (n = 1627), and Science Citation Index Expanded(n = 1254). We excluded 754 duplicates and 4104 clearly irrele-
vant references through reading abstracts. Twenty-eight references
were retrieved for further assessment. No references were identi-
fied through scanning reference lists of the identified randomised
trials. Of the 28 references, we excluded three because of the rea-
sons listed under the table ’Characteristics of excluded studies’ and
18 because they were clearly irrelevant. In total, seven publications
describing five randomised trials fulfilled the inclusion criteria.
All the five were completed trials and could provide data for the
analyses (Lai 1998; Lo 1998; Davila 1999; Johansson 2003; Kolla
2004). Details of the trials are shown in the table ’Characteristics
of included studies’.
Participants
A total of 451 participants with acute cholecystitis were ran-
domised in the five trials. The number of participants in each trial
ranged from 40 to 145. We were not able to extract relevant data
on the percentage of sex of the participants from one trial (Davila
1999). The percentage of females was 57.3% in the remaining
trials. The mean age was 57 years.
Experimental intervention
Early laparoscopic cholecystectomy was conducted within seven
days of onset of symptoms in all trials. The timing is described in
the ’Characteristics of included studies’ table.
4Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Control intervention
Delayed laparoscopic cholecystectomy was conducted at least six
weeks after the onset of symptoms in all trials. The timing is
described in the ’Characteristics of included studies’ table.
Concomitant intervention
The way the common bile duct stones were dealt with in each
study is given in Table 1.
Outcome measures
The primary outcome measures reported by all the included trials
were the complications and conversion rate in each group. The
complications reported were bile duct injury, bile leak, infection,
and conversion in all the trials. Two trials (Lo 1998; Johansson
2003) reported recurrent cholecystitis, and one trial (Lo 1998)
reported cholangitis during the waiting time for delayed laparo-
scopic cholecystectomy.
The other outcome measures reported by the trials were operating
time (all the included trials), hospital stay (all the included trials),
quality of life (Johansson 2003), and pain (Lo 1998; Kolla 2004)
in each of the two groups.
Risk of bias in included studies
Four out of the five trials (80%) had adequate generation of the
allocation sequence, adequate allocation concealment, and ade-
quate follow-up and were of high methodological quality compo-
nents (Lai 1998; Lo 1998; Johansson 2003; Kolla 2004). These
same four trials performed analyses following the intention-to-
treat principle. Two trials (40%) reported on sample-size calcula-
tions (Lai 1998; Lo 1998).
Information is not available for one study (Davila 1999) regarding
the methodological quality components, intention-to-treat prin-
ciple, and sample size calculation, in spite of attempts to contact
the authors of the study.
Effects of interventions
Five trials including 451 patients were included for this review:
223 patients were randomised to the early group and 228 patients
to the delayed group. Two hundred twenty-two patients in early
group and 216 patients in delayed group underwent surgery.
Bile duct injury
There was no statistically significant difference between the two
groups for this most feared complication (OR 0.63, 95% CI 0.15
to 2.70). There was no change in the results by adopting the
random-effects model, available case analysis, calculating the risk
difference, or by using empirical correction factors for zero-event
trials described in the section ’zero-event trials’. The bile duct
injury rate was 0.5% in the early group versus 1.4% in the delayed
group (Table 2).
Bile leak requiring endoscopic retrograde
cholangiopancreatography
Bile leak requiring endoscopic retrograde cholangiopancreatogra-
phy was higher in the early group (3.2%) than the delayed group
(0%). However, this was only statistically significant using the
fixed-effect model (OR 5.78, CI 1.00 to 33.3), but not in the ran-
dom-effects model, available case analysis, calculating risk differ-
ence, or by using empirical correction factors for zero-event trials.
Intra-abdominal collections requiring drainage
There was no statistically significant difference between the two
groups regarding intra-abdominal collections requiring drainage
using the fixed-effect model (OR 1.86, 95% CI 0.56 to 6.18),
random-effects model, available case analysis, or by calculating the
risk difference.
Superficial infections
There was no statistically significant difference between the two
groups regarding superficial infections using the fixed-effect model
(OR 1.39, 95% CI 0.56 to 3.44), random-effects model, available
case analysis, or by calculating the risk difference.
Deep infections
There was no statistically significant difference between the two
groups regarding deep infections using the fixed-effect model (OR
0.43, 95% CI 0.09 to 1.98), random-effects model, available case
analysis, calculating the risk difference, or by using empirical cor-
rection factors for zero-event trials.
Conversion to open cholecystectomy
There was no statistically significant difference between the two
groups regarding conversion to open cholecystectomy (OR 0.84,
95% CI 0.53 to 1.34). There was no change in the results by
adopting the random-effects model, available case analysis, or by
calculating the risk difference. The conversion rate was 20.3% in
the early group and 23.6% in the delayed group (Table 2).
The results of the meta-analysis are summarized in Table 3.
The heterogeneity was explored by the chi-squared test and I2
(Higgins 2002). There was no heterogeneity among the trials as
denoted by the chi-squared values and I2 in Table 4.
5Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Mortality
There was no mortality in any of the trials.
Subgroup and sensitivity analysis
A sensitivity analysis including only trials with high methodolog-
ical quality (ie, low risk of bias) did not change the results of any
outcome apart from the fixed-effect model analysis of bile duct
leaks, which now became insignificant.
A subgroup analysis of trials which included only patients with less
than four days of onset of symptoms and those which also included
patients with more than four days of onset of symptoms in the
early group was performed. There was no statistically significant
difference between the early group and delayed group in any of the
outcome measures in spite of the change in duration of symptoms
(Table 5).
A subgroup analysis of trials in which the experience of the sur-
geons was a minimum of 25 to 50 laparoscopic cholecystectomies
was performed. There was no statistically significant difference be-
tween the early group and delayed group in any of the outcome
measures in spite of the moderate prior surgical experience of the
surgeons (Table 5).
Zero-event trials
We also performed a sensitivity analysis with and without empir-
ical continuity correction factors as suggested by Sweeting et al
(Sweeting 2004) for ’zero-event trials’. There was no statistically
significant difference in any of the outcomes (Table 3).
We also determined the risk difference to take into account the
’zero-event trials’. There was no statistically significant difference
in any of the outcomes (Table 3).
Funnel plots
Funnel plots did not reveal any bias for any of the outcomes mea-
sured. However, there were too few trials to perform the Egger’s
test for exploration of bias (Figure 1; Figure 2; Figure 3; Figure 4;
Figure 5; Figure 6).
Figure 1. Funnel plot - Bile duct injury
6Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 2. Funnel plot - Bile leak requiring ERCP
7Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 3. Funnel plot - Intra-abdominal collections requiring drainage
8Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 4. Funnel Plot - Superficial Infection
9Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 5. Funnel Plot - Deep Infection
10Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 6. Funnel plot - Conversions
Other outcome measures
We also recorded other outcome measures, which were not
amenable to meta-analysis because of the heterogenous ways of
reporting and also because only the delayed group was exposed to
the risk.
Non-resolving cholecystitis or recurrent cholecystitis
17.5% of the people belonging to the delayed group had either
non-resolution of symptoms or recurrence of symptoms before
their planned operation and had to undergo emergency laparo-
scopic cholecystectomy (Table 6). The proportion with conver-
sion to open cholecystectomy is 45% in this group (Table 2).
Other gallstone-related morbidity
Two patients in the delayed group developed cholangitis during
the waiting time. There were no reports of pancreatitis during the
waiting time.
Operating time and hospital stay
In all trials but one (Johansson 2003), the operating times were
longer for early compared with the delayed group (Table 7). How-
ever, the total hospital stay was about four days shorter for the
early compared with the delayed group in all the trials (Table 7).
In the trials of high methodological quality, this was 4.5 days on
average.
D I S C U S S I O N
In this systematic review we have found that there are no signif-
icant differences in the complication rate or the conversion rate
whether the laparoscopic cholecystectomy is performed during
acute cholecystitis or performed 6 to 12 weeks after the symp-
toms settle. However, early laparoscopic cholecystectomy has the
advantage of decreased hospital stay and these patients do not run
the risk of non-solved symptoms or risk of emergency operation.
The latter leads to a high proportion of patients undergoing open
cholecystectomy.
Before the advent of laparoscopic cholecystectomy, early open
cholecystectomy was preferable over delayed open cholecystec-
tomy for acute cholecystitis (Papi 2004). However, about 20%
11Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

of surgeons in United Kingdom prefer to perform laparoscopic
cholecystectomy during the phase of acute cholecystitis (Senapati
2003). About 30% of patients in USA are operated upon during
the phase of acute cholecystitis (Livingston 2004). The main rea-
sons for performing a delayed laparoscopic cholecystectomy are
because of the fear of increased morbidity rates (Cuschieri 1991;
Wilson 1991; Kum 1996) and conversion rates (Cheema 2003;
Livingston 2004).
Bile duct injury is one of the most feared complications during la-
paroscopic cholecystectomy. Bile duct injury can sometimes even
be fatal because of sepsis (Sicklick 2005). The corrective surgery
for bile duct injury also carries mortality and morbidity (Schmidt
2005; Sicklick 2005). The quality of life of these patients after
corrective surgery can be poor even after three years of surgery
(Moore 2004). Cholecystitis has been considered as a risk factor
for bile duct injury (Nuzzo 2005; Richardson 1996). However, we
found that the bile duct injury rate was lower in the early group
(0.5%) than in the delayed group (1.4%). However, this differ-
ence is not statistically significant and the numbers are too small
to detect any pattern. Although no bile duct injury in the delayed
group occurred in the cross-over group (no information available
from one study - Davila 1999), one possible reason for this con-
tradictory evidence between the observational studies and the ran-
domised studies is that the patients with repeated episodes of acute
cholecystitis (because of following a policy of delayed laparoscopic
cholecystectomy) may be classified under ’cholecystitis’ in the ob-
servational studies, while such cases would not be included under
the early group, if a strict ’intention-to-treat’ analysis was applied.
Bile leak is a complication in about 1% of laparoscopic cholecys-
tectomies (Buanes 1996; Barkun 1997). Common bile duct in-
juries can be a cause for bile leak (Buanes 1996). However, the
majority of these are due to cystic stump leaks (Barkun 1997; De
Palma 2002; Kaffes 2005). Obstruction to the bile duct is found
in nearly one third of the patients (Barkun 1997; De Palma 2002).
The majority of the bile leaks (not due to major bile duct injury) are
managed successfully by endoscopic retrograde cholangiopancre-
atography and endoscopic sphincterotomy with or without stent
(De Palma 2002; Kaffes 2005). However, endoscopic retrograde
cholangiopancreatography is not without risks and can have com-
plications such as mortality, pancreatitis, haemorrhage, and perfo-
ration (Christensen 2004). However, recently, contrast enhanced
MRCP cholangiography is being considered for the diagnosis of
the site of the leaks (Aduna 2005). However, after diagnosis, many
of these patients would require endoscopic intervention depend-
ing upon the nature of the leak. Hence, bile leak is a significant and
important complication. In this review, we found an increase in
the risk of bile leak in early laparoscopic cholecystectomy (3.2%)
compared to delayed laparoscopic cholecystectomy (0%). How-
ever, this was not statistically significant difference in the random-
effects model, which had to be adopted because of the presence of
statistical heterogeneity. The majority of the bile leaks occurred in
the early group in one trial (Johansson 2003).
Laparoscopic cholecystectomy during acute cholecystitis has been
found to have a higher conversion rate than elective cholecystec-
tomy. However, none of the trials included showed a statistically
significant difference in the conversion rates. In fact, the over-
all conversion rate was higher in the delayed intervention group
(23.6%) as compared with the early intervention group (20.3%).
This difference is not statistically significant.
While there are reports of increased conversion rate if the surgery is
delayed for more than 48 to 96 hours after the onset of symptoms
(Eldar 1997; Madan 2002; Liguori 2003; Peng 2005), other stud-
ies do not confirm this (Knight 2004). In our review, we found
two trials, which included only patients with less than four days of
onset of symptoms. Three trials included patients with less than
seven days of onset of symptoms. A subgroup analysis showed no
significant difference in the conversion rate or complication rate
in the early group (whether less than four days of onset of symp-
toms or less than seven days of onset of symptoms) compared with
delayed laparoscopic cholecystectomy, thereby proving the safety
of laparoscopic cholecystectomy up to seven days after onset of
symptoms. This provides adequate time for investigating the pa-
tient and dealing with common bile duct stones (depending upon
the individual surgeon’s strategy), before performing operation in
the next available operating list. Again, the reason for the con-
tradictory results between observational studies and randomised
trials may be due to not adopting the ’intention-to-treat’ analysis.
One would expect the infection proportion to be higher in the
early group than the delayed group because of the presence of in-
flammation. However, we found no statistically significant differ-
ence in the superficial infection rate (5% versus 3.7%) or deep
infection rate (1% versus 2.3%) between the early and delayed
group. Neither was there any statistically significant difference in
the rate of abdominal collections requiring percutaneous drainage
between the two operations (2.7% versus 1.4%).
One of the other issues is the management of common bile duct
stones. Pre-operative endoscopic sphincterotomy is one of the op-
tions available for the management of common bile duct stones
(Lo 1998). This may cause delay in surgery. However, where ex-
pertise is available, laparoscopic exploration of the common bile
duct can be performed successfully in the majority of the patients
(Snow 1999; Thompson 2002; Rojas-Ortega 2003; Hemli 2004).
Per-operative endoscopic sphincterotomy (Cox 1995; Enochsson
2004; Saccomani 2005) and post-operative endoscopic sphinc-
terotomy (Rhodes 1998; Nathanson 2005; Saccomani 2005) are
the other options available for the management of common bile
duct stones. Of the five trials included in this review, two trials
(Lai 1998; Kolla 2004) did not include patients with common
bile duct stones; in two trials (Davila 1999; Johansson 2003) the
stones were dealt with in the same operation, and in one trial (Lo
1998) pre-operative endoscopic sphincterotomy was performed in
12Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

the presence of common bile duct stones. This is summarized in
Table 1. One patient in each group in one of the trials (Johansson
2003) was converted to open cholecystectomy with open common
bile duct exploration due to large common bile duct stone (per-
sonal communication). Two patients from the early group in the
same trial underwent post-operative ERCP for removal of com-
mon bile duct stones (personal communication). Thus manage-
ment of common bile duct stones remains an issue in early laparo-
scopic cholecystectomy.
Another main issue is the experience of the surgeon (Johansson
2003). The surgeries were performed by surgeons who had a min-
imum experience of 25 laparoscopic cholecystectomies in one of
the trials (Johansson 2003) and in another trial (Lai 1998), the
surgeries had a minimum experience of 50 laparoscopic cholecys-
tectomies. The surgical experience in the different trials is sum-
marized in Table 1. The subgroup analysis of these trials did not
reveal significant difference in the outcomes between early and
delayed cholecystectomy. The techniques had to be modified and
gallbladder decompression had to be performed more often in the
early group than in the delayed group (Lai 1998; Lo 1998; Kolla
2004).
Operating time was less in early than in delayed group in one trial
(Johansson 2003). In the rest of the trials, early cholecystectomy
took an average of 10 minutes to 30 minutes longer than delayed
cholecystectomy (Lai 1998; Lo 1998; Davila 1999; Kolla 2004).
However, this increase in operating time and hence the costs are
more than compensated for by the duration of hospital stay, which
was 1.1 to 6 days longer (on an average) in the delayed group than
in the early group (Lai 1998; Lo 1998; Davila 1999; Johansson
2003; Kolla 2004).
Another important issue is gallstone-related morbidity during the
waiting period. The most important one is the non-resolution of
the current episode of cholecystitis or recurrence of cholecystitis.
Forty patients (17.5%) in the delayed group underwent emergency
surgery during the waiting period. Laparoscopic cholecystectomy
performed in such patients carries a higher conversion rate (45%
conversion rate) than those who undergo surgery in the acute
cholecystitis or those who are symptom-free during the interval
period (Table 2). Although, there were not many gallstone-related
morbidity events in the trials included in the meta-analysis, the
surgeries in the delayed group were actually performed within 12
weeks in all the trials. However, the actual reality may be different
and patients may have to wait for much longer than 12 weeks (
Glasgow 2000; Lawrentschuk 2003) and develop complications of
gallstones including pancreatitis, cholangitis, choledocholithiasis,
and recurrent attacks of cholecystitis while waiting for surgery
(Rutledge 2000; Lawrentschuk 2003; Vetrhus 2003).
While the trials reviewed here have performed delayed surgery
between 6 weeks and 12 weeks after the acute episode, another
strategy reported is of performing surgery after a short course of
antibiotics (Chandler 2000; Dimov 2005). This may provide time
to deal with common bile duct stones, where facilities are limited.
Because of the existing practice of performing delayed laparoscopic
cholecystectomy, it is possible that many patients are treated with
antibiotics and investigated by the primary care physician before
being electively referred to the surgeon for laparoscopic cholecys-
tectomy. However, by following a policy of urgent referral of these
patients to the surgeon (and urgent investigations to confirm the
diagnosis, as opposed to elective referral and elective investiga-
tions), it is quite possible that some patients having only biliary
colic and no associated inflammation are identified. Studies have
shown that laparoscopic cholecystectomy done for biliary colic has
a lower conversion rate and morbidity rate than that performed
after an attack of cholecystitis (Glasgow 2000; Peng 2005). Thus,
such patients may indirectly benefit if surgeons follow a policy of
early laparoscopic cholecystectomy.
A U T H O R S ’ C O N C L U S I O N SImplications for practice
1. Early laparoscopic cholecystectomy during acute
cholecystitis appears to be safe and shortens the total hospital
stay. However, the confidence intervals are wide for many of the
outcomes measured and hence significant benefits (lower
conversion and bile duct injury rates) and harms (higher risk of
bile leak requiring ERCP and abdominal collections requiring
percutaneous drainage) may be overlooked.
2. Common bile duct stone is an important issue and the
management of acute cholecystitis may vary in the presence of
common bile duct stones, depending upon the preference of the
surgeon.
3. Early laparoscopic cholecystectomy should only be
performed by surgeons with adequate laparoscopic experience
and prior experience of operating during the acute cholecystitis.
Establishment of units specializing in this type of surgery may be
necessary to accomplish this.
Implications for research1. Further randomised clinical trials are needed to compare
the early versus delayed laparoscopic cholecystectomy.
2. Further randomised clinical trials are needed to compare
the laparoscopic cholecystectomy performed within four days of
onset of symptoms of acute cholecystitis and that performed
between four and seven days of onset of symptoms.
3. Further randomised clinical trials are needed to compare
the laparoscopic cholecystectomy performed immediately and
that performed after a short course of antibiotics.
4. More trials on surgical interventions for acute cholecystitis
need to adapt blinded assessments of outcome measures.
13Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

5. Trials need to be conducted and reported according to the
CONSORT Statement (www.consort-statement.org).
A C K N O W L E D G E M E N T S
Martyn Parker, first author of more than 15 Cochrane reviews,
who taught me how to write papers and who created my interest
in writing Cochrane reviews.
Dimitrinka Nikolova, Cochrane Hepato-Biliary Review Group
Co-ordinator, who provided guidance and made corrections.
Christian Gluud, Cochrane Hepato-Biliary Group, who provided
guidance.
Sarah Louise Klingenberg, Cochrane Hepato-Biliary Group, who
provided help with searching the databases.
Yan Gong, Cochrane Hepato-Biliary Group, who provided statis-
tical advice.
Abe Fingerhut, Cochrane Hepato-Biliary Group Editor, who pro-
vided advice.
Pepe Mullerat, Registrar Northampton General Hospital, who
helped with a Spanish translation.
Stoke Mandeville Hospital library, which obtained the full text
articles for many of the references cited in this review.
R E F E R E N C E S
References to studies included in this review
Davila 1999 {published data only}
Davila D, Manzanares C, Picho ML, Albors P, Cardenas
F, Fuster E, et al.Experience in the treatment (early vs.
delayed) of acute cholecystitis via laparoscopy. Cirugia
Espanola 1999;66(Suppl 1):233.
Johansson 2003 {published and unpublished data}
Johansson M, Thune A, Blomqvist A, Nelvin L, Lundell
L. Impact of choice of therapeutic strategy for acute
cholecystitis on patient’s health-related quality of life: results
of a randomized, controlled clinical trial. Digestive Surgery
2004;21(5-6):359–62.∗ Johansson M, Thune A, Blomqvist A, Nelvin L, Lundell
L. Management of acute cholecystitis in the laparoscopic
era: results of a prospective, randomized clinical trial.
Journal of Gastrointestinal Surgery 2003;7(5):642–5.
Johansson M, Thune A, Lundell L. A prospective
randomised trial comparing early versus delayed laparoscopic
cholecystectomy in the treatment of acute cholecystitis.
Gastroenterology 2002;123(1 Suppl):24.
Kolla 2004 {published and unpublished data}
Kolla SB, Aggarwal S, Kumar A, Kumar R, Chumber
S, Parshad R, et al.Early vs delayed laparoscopic
cholecystectomy for acute cholecystitis. Surgical Endoscopy
2004;18:1323–7.
Lai 1998 {published data only}
Lai PBS, Kwong KH, Leung KL. Randomized trial of
early versus delayed laparoscopic cholecystectomy for acute
cholecystitis. British Journal of Surgery 1998;85(6):764–7.
Lo 1998 {published data only}
Lo C, Liu C, Fan S, Lai ECS, Wong J. Prospective
randomized study of early versus delayed laparoscopic
cholecystectomy for acute cholecystitis. Annals of Surgery
1998;227(4):461–7.
References to studies excluded from this review
Chandler 2000 {published data only}
Chandler CF, Lane JS, Ferguson P, Thompson JE,
Ashley SW. Prospective evaluation of early versus delayed
laparoscopic cholecystectomy for treatment of acute
cholecystitis. American Surgeon 2000;66(9):896–900.
Dimov 2005 {published data only}
Dimov R, Strangev G, Kandilarov K, Marinov V, Argirov
D, Velkov B, et al.Prospective trial of early and delayed
laparoscopic cholecistectomy in patients presented with
acute cholecystitis. Bulgarian Medicine 2005;13(1):6–9.
Salman 2005 {published data only}
Salman B, Yuksel O, Irkorucu O, Akyurek N, Tezcaner
T, Dogan I, et al.Urgent laparoscopic cholecystectomy
is the best management for biliary colic. A prospective
randomized study of 75 cases. Digestive Surgery 2005;22(1-
2):95–9.
Additional references
Aduna 2005
Aduna M, Larena JA, Martin D, Martinez-Guerenu B,
Aguirre I, Astigarraga E. Bile duct leaks after laparoscopic
cholecystectomy: value of contrast-enhanced MRCP.
Abdominal Imaging 2005;30(4):480–7.
Bakken 2004
Bakken IJ, Skjeldestad FE, Mjåland O, Johnson E.
Cholecystectomy in Norway 1990-2002 [Kolecystektomi i
Norge i 1990–2002]. Tidsskrift for den Norske Laegeforening
2004;124(18):2376–8.
Barkun 1997
Barkun AN, Rezieg M, Mehta SN, Pavone E, Landry
S, Barkun JS, et al.Postcholecystectomy biliary leaks
in the laparoscopic era: risk factors, presentation, and
management. McGill Gallstone Treatment Group.
Gastrointestinal Endoscopy 1997;45(3):277–82.
14Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Buanes 1996
Buanes T, Waage A, Mjaland O, Solheim K. Bile leak
after cholecystectomy significance and treatment: results
from the National Norwegian Cholecystectomy Registry.
International Surgery 1996;81(3):276–9.
Cheema 2003
Cheema S, Brannigan AE, Johnson S, Delaney PV, Grace
PA. Timing of laparoscopic cholecystectomy in acute
cholecystitis. Irish Journal of Medical Science 2003;172(3):
128–31.
Christensen 2004
Christensen M, Matzen P, Schulze S, Rosenberg
J. Complications of ERCP: a prospective study.
Gastrointestinal Endoscopy 2004;60(5):721–31.
Cox 1995
Cox MR, Wilson TG, Toouli J. Peroperative endoscopic
sphincterotomy during laparoscopic cholecystectomy for
choledocholithiasis. British Journal of Surgery 1995;82(2):
257–9.
Cuschieri 1991
Cuschieri A, Dubois F, Mouiel J, Mouret P, Becker H,
Buess G, et al.The European experience with laparoscopic
cholecystectomy. American Journal of Surgery 1991;161(3):
385–7.
De Palma 2002
De Palma GD, Iuliano GP, Puzziello A, Manfredini S,
Masone S, Persico G. Biliary leaks after laparoscopic
cholecystectomy. Results of the endoscopic treatment.
Minerva Chirurgica 2002;57(2):123–7.
DeMets 1987
DeMets DL. Methods for combining randomized clinical
trials: strengths and limitations. Statistics in Medicine 1987;
6(3):341–50.
DerSimonian 1986
DerSimonian R, Laird N. Meta-analysis in clinical trials.
Controlled Clinical Trials 1986;7(3):177–88.
Egger 1997
Egger M, Davey SG, Schneider M, Minder C. Bias in meta-
analysis detected by a simple, graphical test. BMJ (Clinical
Research Ed.) 1997;315(7109):629–34.
Eldar 1997
Eldar S, Sabo E, Nash E, Abrahamson J, Matter I.
Laparoscopic cholecystectomy for acute cholecystitis:
prospective trial. World Journal of Surgery 1997;21(5):
540–5.
Enochsson 2004
Enochsson L, Lindberg B, Swahn F, Arnelo U. Intraoperative
endoscopic retrograde cholangiopancreatography
(ERCP) to remove common bile duct stones during
routine laparoscopic cholecystectomy does not prolong
hospitalization: a 2-year experience. Surgical Endoscopy
2004;18(3):367–71.
Fullarton 1994
Fullarton GM, Bell G. Prospective audit of the introduction
of laparoscopic cholecystectomy in the west of Scotland.
West of Scotland Laparoscopic Cholecystectomy Audit
Group. Gut 1994;35(8):1121–6.
Glasgow 2000
Glasgow RE, Cho M, Hutter MM, Mulvihill SJ. The
spectrum and cost of complicated gallstone disease in
California. Archives of Surgery 2000;135(9):1021-5;
discussion 1025-7.
Halldestam 2004
Halldestam I, Enell EL, Kullman E, Borch K. Development
of symptoms and complications in individuals with
asymptomatic gallstones. British Journal of Surgery 2004;91
(6):734–8.
Hemli 2004
Hemli JM, Arnot RS, Ashworth JJ, Curtin AM, Simon RA,
Townend DM. Feasibility of laparoscopic common bile
duct exploration in a rural centre. ANZ Journal of Surgery
2004;74(11):979–82.
Higgins 2002
Higgins JPT, Thompson SG. Quantifying heterogeneity in a
meta-analysis. Statistics in Medicine 2002;21(11):1539–58.
Higgins 2005
Higgins JPT, Green S, editors. Cochrane Handbook for
Systematic Reviews of Interventions 4.2.5 [updated May
2005]. The Cochrane Library. Chichester, UK: John Wiley
& sons, Ltd, 2005, issue 3.
Janzon 1985
Janzon L, Aspelin P, Eriksson S, Hildell J, Trell E, Ostberg H.
Ultrasonographic screening for gallstone disease in middle-
aged women. Detection rate, symptoms, and biochemical
features. Scandinavian Journal of Gastroenterology 1985;20
(6):706–10.
Jørgensen 1987
Jørgensen T. Prevalence of gallstones in a Danish population.
American Journal of Epidemiology 1987;126(5):912–21.
Kaffes 2005
Kaffes AJ, Hourigan L, De Luca N, Byth K, Williams SJ,
Bourke MJ. Impact of endoscopic intervention in 100
patients with suspected postcholecystectomy bile leak.
Gastrointestinal Endoscopy 2005;61(2):269–75.
Kjaergard 2001
Kjaergard LL, Villumsen J, Gluud C. Reported
methodologic quality and discrepancies between large and
small randomized trials in meta-analyses. Annals of InternalMedicine 2001;135(11):982–9.
Knight 2004
Knight JS, Mercer SJ, Somers SS, Walters AM, Sadek SA,
Toh SK. Timing of urgent laparoscopic cholecystectomy
does not influence conversion rate. British Journal of Surgery
2004;91(5):601–4.
Kum 1996
Kum CK, Eypasch E, Lefering R, Paul A, Neugebauer
E, Troidl H. Laparoscopic cholecystectomy for acute
cholecystitis: is it really safe?. World Journal of Surgery 1996;
20(1):43–8.
15Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lau 2006
Lau H, Lo CY, Patil NG, Yuen WK. Early versus delayed-
interval laparoscopic cholecystectomy for acute cholecystitis:
a metaanalysis. Surgical Endoscopy 2006;20(1):82–7.
Lawrentschuk 2003
Lawrentschuk N, Hewitt PM, Pritchard MG. Elective
laparoscopic cholecystectomy: implications of prolonged
waiting times for surgery. ANZ Journal of Surgery 2003;73
(11):890–3.
Liguori 2003
Liguori G, Bortul M, Castiglia D. The treatment of
laparoscopic cholecystectomy for acute cholecystitis [Il
trattamento della colecistite acuta in era laparoscopica].
Annali Italiani Di Chirurgia 2003;74(5):517–21.
Livingston 2004
Livingston EH, Rege RV. A nationwide study of conversion
from laparoscopic to open cholecystectomy. AmericanJournal of Surgery 2004;188(3):205–11.
Lo 1996
Lo CM, Liu CL, Lai EC, Fan ST, Wong J. Early versus
delayed laparoscopic cholecystectomy for treatment of acute
cholecystitis. Annals of Surgery 1996;223(1):37–42.
Macaskill 2001
Macaskill P, Walter SD, Irwig L. A comparison of methods
to detect publication bias in meta-analysis. Statistics in
Medicine 2001;20(4):641–54.
Madan 2002
Madan AK, Aliabadi-Wahle S, Tesi D, Flint LM, Steinberg
SM. How early is early laparoscopic treatment of acute
cholecystitis?. American Journal of Surgery 2002;183(3):
232–6.
Mjäland 1998
Mjäland O, Adamsen S, Hjelmquist B, Ovaska J, Buanes T.
Cholecystectomy rates, gallstone prevalence, and handling
of bile duct injuries in Scandinavia. A comparative audit.
Surgical Endoscopy 1998;12(12):1386–9.
Moher 1998
Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher
M, et al.Does quality of reports of randomised trials affect
estimates of intervention efficacy reported in meta-analyses?
. Lancet 1998;352(9128):609–13.
Moore 2004
Moore DE, Feurer ID, Holzman MD, Wudel LJ, Strickland
C, Gorden DL, et al.Long-term detrimental effect of bile
duct injury on health-related quality of life. Archives of
Surgery 2004;139(5):476–82.
Muhrbeck 1995
Muhrbeck O, Ahlberg J. Prevalence of gallstone disease
in a Swedish population. Scandinavian Journal ofGastroenterology 1995;30(11):1125–8.
Nathanson 2005
Nathanson LK, O’Rourke NA, Martin IJ, Fielding GA,
Cowen AE, Roberts RK, et al.Postoperative ERCP versus
laparoscopic choledochotomy for clearance of selected bile
duct calculi: a randomized trial. Annals of Surgery 2005;242
(2):188–92.
Newell 1992
Newell DJ. Intention-to-treat analysis: implications for
quantitative and qualitative research. International Journalof Epidemiology 1992;21(5):837–41.
NIH 1992
NIH. NIH consensus statement on gallstones and
laparoscopic cholecystectomy. http://consensus.nih.gov/
1992/1992GallstonesLaparoscopy090html.htm (accessed
10 August 2006).
Nuzzo 2005
Nuzzo G, Giuliante F, Giovannini I, Ardito F, D’Acapito
F, Vellone M, et al.Bile duct injury during laparoscopic
cholecystectomy: results of an Italian national survey on 56
591 cholecystectomies. Archives of Surgery 2005;140(10):
986–92.
Papi 2004
Papi C, Catarci M, Ambrosio D, Gili L, Koch M, Grassi
GB, et al.Timing of cholecystectomy for acute calculous
cholecystitis: a meta-analysis. American Journal of
Gastroenterology 2004;99(1):147–55.
Peng 2005
Peng WK, Sheikh Z, Nixon SJ, Paterson-Brown S. Role of
laparoscopic cholecystectomy in the early management of
acute gallbladder disease. British Journal of Surgery 2005;92:
586–91.
RevMan 2003
Copenhagen: The Nordic Cochrane Centre, The Cochrane
Collaboration. Review Manager (RevMan). Version 4.2 for
Windows. Copenhagen: The Nordic Cochrane Centre,
The Cochrane Collaboration, 2003.
Rhodes 1998
Rhodes M, Sussman L, Cohen L, Lewis MP. Randomised
trial of laparoscopic exploration of common bile duct versus
postoperative endoscopic retrograde cholangiography for
common bile duct stones. Lancet 1998;351(9097):159–61.
Richardson 1996
Richardson MC, Bell G, Fullarton GM. Incidence
and nature of bile duct injuries following laparoscopic
cholecystectomy: an audit of 5913 cases. British Journal ofSurgery 1996;83(10):1356–60.
Rojas-Ortega 2003
Rojas-Ortega S, Arizpe-Bravo D, Marin Lopez ER, Cesin-
Sanchez R, Roman GR, Gomez C. Transcystic common
bile duct exploration in the management of patients with
choledocholithiasis. Journal of Gastrointestinal Surgery 2003;
7(4):492–6.
Rutledge 2000
Rutledge D, Jones D, Rege R. Consequences of delay in
surgical treatment of biliary disease. American Journal ofSurgery 2000;180(6):466–9.
Saccomani 2005
Saccomani G, Durante V, Magnolia MR, Ghezzo
L, Lombezzi R, Esercizio L, et al.Combined
16Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

endoscopic treatment for cholelithiasis associated with
choledocholithiasis. Surgical Endoscopy 2005;19(7):910–4.
Schmidt 2005
Schmidt SC, Langrehr JM, Hintze RE, Neuhaus P. Long-
term results and risk factors influencing outcome of major
bile duct injuries following cholecystectomy. British Journalof Surgery 2005;92(1):76–82.
Schulz 1995
Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical
evidence of bias. Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials. JAMA 1995;273(5):408–12.
Senapati 2003
Senapati PS, Bhattarcharya D, Harinath G, Ammori
BJ. A survey of the timing and approach to the surgical
management of cholelithiasis in patients with acute biliary
pancreatitis and acute cholecystitis in the UK. Annals ofRoyal College of Surgeons of England 2003;85(5):306–12.
Serralta 2003
Serralta AS, Bueno JL, Planells MR, Rodero DR. Prospective
evaluation of emergency versus delayed laparoscopic
cholecystectomy for early cholecystitis. Surgical Laparoscopy,
Endoscopy & Percutaneous Techniques 2003;13(2):71–5.
Shikata 2005
Shikata S, Noguchi Y, Fukui T. Early versus delayed
cholecystectomy for acute cholecystitis: a meta-analysis of
randomized controlled trials. Surgery Today 2005;35(7):
553–60.
Sicklick 2005
Sicklick JK, Camp MS, Lillemoe KD, Melton GB, Yeo
CJ, Campbell KA, et al.Surgical management of bile duct
injuries sustained during laparoscopic cholecystectomy:
perioperative results in 200 patients. Annals of Surgery 2005;
241(5):786–95.
Snow 1999
Snow LL, Weinstein LS, Hannon JK, Lane DR.
Management of bile duct stones in 1572 patients undergoing
laparoscopic cholecystectomy. American Surgeon 1999;65
(6):530–47.
StatsDirect 2.4
StatsDirect Ltd. StatsDirect Statistical software Version
2.4.5. StatsDirect Ltd, 2005.
Sweeting 2004
Sweeting MJ, Sutton AJ, Lambert PC. What to add to
nothing? Use and avoidance of continuity corrections in
meta-analysis of sparse data. Statistics in Medicine 2004;23
(9):1351–75.
Thompson 2002
Thompson MH, Tranter SE. All-comers policy for
laparoscopic exploration of the common bile duct. BritishJournal of Surgery 2002;89(12):1608–12.
Vetrhus 2003
Vetrhus M, Soreide O, Nesvik I, Sondenaa K. Acute
cholecystitis: delayed surgery or observation. A randomized
clinical trial. Scandinavian Journal of Gastroenterology 2003;
38(9):985–90.
Wilson 1991
Wilson P, Leese T, Morgan WP, Kelly JF, Brigg JK. Elective
laparoscopic cholecystectomy for ’all-comers’. Lancet 1991;
338(8770):795–7.∗ Indicates the major publication for the study
17Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Davila 1999
Methods Randomised clinical trial
Generation of the allocation sequence: unclear.
Allocation concealment: unclear.
Follow-up: unclear.
Intention-to-treat analysis: unclear.
Sample size calculation: no.
Participants Country: Spain
Number randomised: 63.
Mean age: 56 years.
Females: not available.
Patients with acute cholecystitis.
Interventions Participants were randomly assigned to two groups.
Group 1: early laparoscopic cholecystectomy (n = 36).
Group 2: delayed laparoscopic cholecystectomy (n = 27).
Timing:
Early LC (less than 4 days of onset of symptoms).
Delayed LC (2 months after acute episode settles).
Peroperative cholangiogram: not mentioned.
Outcomes The main outcome measures were the complications and conversion in each group
The list of outcomes measured were bile duct injury, bile leak, infection, conversion, operating time, and
hospital stay
Notes Attempted to contact the author - no reply received.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
18Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Johansson 2003
Methods Randomised clinical trial
Generation of the allocation sequence: adequate. Computer generated randomisation list
Allocation concealment: adequate. Done by a third party after stratification for age and sex
Follow-up: adequate.
Intention-to-treat analysis: yes.
Sample size calculation: no.
Participants Country: Sweden
Number randomised: 145.
Mean age: 57 years.
Females: 87 (60%).
Patients with acute cholecystitis.
Exclusion criteria:
1. Symptoms more than 1 week.
2. Older than 90 years.
3. Bilirubin more than 3.5 mg/dl.
Interventions Participants were randomly assigned to two groups.
Group 1: early laparoscopic cholecystectomy (n = 74).
Group 2: delayed laparoscopic cholecystectomy (n = 71).
Timing:
Early LC (less than 7 days of onset of symptoms).
Delayed LC (6 to 8 weeks after symptoms settle).
Peroperative cholangiogram: yes.
Outcomes The main outcome measures were the complications and conversion in each group
The list of outcomes measured were recurrent cholecystitis, bile duct injury, bile leak, superficial Infection,
deep infection, conversion, operating time, hospital stay, and quality of life
Notes Information on allocation concealment and the way in which CBD stones were dealt with were obtained
on 16/8/2005 and 7/9/2005
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Kolla 2004
Methods Randomised clinical trial
Generation of the allocation sequence: adequate. Computer generated randomization list
Allocation concealment: adequate. Held by a third party.
Follow-up: adequate.
Intention-to-treat analysis: adequate.
Sample size calculation: no.
19Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kolla 2004 (Continued)
Participants Country: India
Number randomised: 40.
Mean age: 40 years.
Females: 32 (80%).
Patients with acute cholecystitis.
Exclusion criteria:
1. Symptoms more than 4 days.
2. Previous upper abdominal surgery.
3. Unfit for laparoscopic surgery.
4. CBD stones.
Interventions Participants were randomly assigned to two groups.
Group 1: early laparoscopic cholecystectomy (n = 20).
Group 2: delayed laparoscopic cholecystectomy (n = 20).
Timing:
Early LC (less than 24 hours of admission and less than 4 days of onset of symptoms)
Delayed LC (6 to 12 weeks after index admission).
Peroperative cholangiogram: no.
Outcomes The main outcome measures were the complications and conversion in each group
The list of outcomes measured were bile duct injury, bile leak, infection, conversion, operating time,
hospital stay, and pain
Notes Further information on follow-up was obtained on 27/9/2005.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Lai 1998
Methods Randomised clinical trial
Generation of the allocation sequence: adequate. Computer generated
Allocation concealment: adequate. Kept by a third party.
Follow-up: clear.
Intention-to-treat analysis: yes.
Sample size calculation: yes.
Participants Country: Hong Kong
Number randomised: 104.
Mean age: 56 years.
Females: 66 (63.5%).
Patients with acute cholecystitis.
Exclusion criteria:
1. Symptoms more than 1 week.
2. Previous upper abdominal surgery.
20Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lai 1998 (Continued)
3. Unfit for laparoscopic surgery.
4. CBD stones.
5. Acute cholangitis (co-existing).
6. Acute pancreatitis (co-existing).
Interventions Participants were randomly assigned to two groups.
Group 1: early laparoscopic cholecystectomy (n = 53).
Group 2: delayed laparoscopic cholecystectomy (n = 51).
Timing:
Early LC (less than 7 days of onset of symptoms).
Delayed LC (6 to 8 weeks after initial attack settles).
Peroperative cholangiogram: no.
Outcomes The main outcome measures were the complications and conversion in each group
The list of outcomes measured were bile duct injury, bile leak, infection, conversion, operating time, and
hospital stay
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Lo 1998
Methods Randomised clinical trial
Generation of the allocation sequence: adequate. Random number table
Allocation concealment: adequate. Sealed opaque envelopes.
Follow-up: adequate.
Intention-to-treat analysis: yes.
Sample size calculation: yes.
Participants Country: Hong Kong
Number randomised: 99.
Mean age: 58 years.
Females: 39 (38.4%).
Patients with acute cholecystitis.
Exclusion criteria:
1. Symptoms more than 1 week.
2. More than 3 days of admission.
3. Previous upper abdominal surgery.
4. Unfit for surgery.
5. Uncertainty about diagnosis.
6. Peritonitis.
7. Pregnancy.
21Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lo 1998 (Continued)
Interventions Participants were randomly assigned to two groups.
Group 1: early laparoscopic cholecystectomy (n = 49).
Group 2: delayed laparoscopic cholecystectomy (n = 50).
Timing:
Early LC (less than 3 days of admission and less than 7 days of onset of symptoms)
Delayed LC (8 to 12 weeks after initial attack settles).
Peroperative cholangiogram: no.
Outcomes The main outcome measures were the complications and conversion in each group
The list of outcomes measured were recurrent cholecystitis, cholangitis, bile duct injury, bile leak, infection,
conversion, operating time, hospital stay, and pain
Notes Further information on generation of random sequence was obtained on 20/8/2005, 29/11/2005, and 4/
12/2005
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
LC = laparoscopic cholecystectomy
CBD = common bile duct
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Chandler 2000 Early treatment patients underwent surgery as soon as operating schedule allowed. Delayed treatment patients
underwent operation after resolution of symptoms or within five days if symptoms failed to resolve. According to
the definitions used by us, both these groups fall in the early group
Dimov 2005 Early treatment patients underwent surgery up to 72 hours of onset of symptoms. Delayed treatment patients
underwent operation after five to seven days of medical treatment. Some of these patients may belong to the early
group according to the definitions used by us
Salman 2005 Compares early or delayed laparoscopic cholecystectomy in biliary colic
22Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Early versus delayed LC (number of people randomised)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Bile duct injury 5 451 Odds Ratio (M-H, Fixed, 95% CI) 0.63 [0.15, 2.70]
2 Bile leak requiring ERCP 5 451 Odds Ratio (M-H, Fixed, 95% CI) 5.78 [1.00, 33.29]
3 Intra-abdominal collections
requiring percutaneous
drainage
5 451 Odds Ratio (M-H, Fixed, 95% CI) 1.86 [0.56, 6.18]
4 Superficial infection 5 451 Odds Ratio (M-H, Fixed, 95% CI) 1.39 [0.56, 3.44]
5 Deep infection 5 451 Odds Ratio (M-H, Fixed, 95% CI) 0.43 [0.09, 1.98]
6 Conversion to open
cholecystectomy
5 451 Odds Ratio (M-H, Fixed, 95% CI) 0.84 [0.53, 1.34]
Comparison 2. Early versus delayed LC (number of people operated)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Bile duct Injury 5 438 Odds Ratio (M-H, Fixed, 95% CI) 0.61 [0.14, 2.62]
2 Bile leak requiring ERCP 5 438 Odds Ratio (M-H, Fixed, 95% CI) 5.55 [0.96, 31.94]
3 Intra-abdominal collections
requiring percutaneous
drainage
5 438 Odds Ratio (M-H, Fixed, 95% CI) 1.91 [0.62, 5.88]
4 Superficial infection 5 438 Odds Ratio (M-H, Fixed, 95% CI) 1.33 [0.54, 3.29]
5 Deep infection 5 438 Odds Ratio (M-H, Fixed, 95% CI) 0.41 [0.09, 1.88]
6 Conversion to open
cholecystectomy
5 438 Odds Ratio (M-H, Fixed, 95% CI) 0.79 [0.50, 1.25]
Comparison 3. Early versus delayed LC - risk difference
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Bile duct injury 5 451 Risk Difference (M-H, Fixed, 95% CI) -0.01 [-0.03, 0.02]
2 Bile leak requiring ERCP 5 451 Risk Difference (M-H, Fixed, 95% CI) 0.03 [0.00, 0.06]
3 Intra-abdominal collections
requiring percutaneous
drainage
5 451 Risk Difference (M-H, Fixed, 95% CI) 0.02 [-0.01, 0.05]
4 Superficial infection 5 451 Risk Difference (M-H, Fixed, 95% CI) 0.01 [-0.02, 0.05]
5 Deep infection 5 451 Risk Difference (M-H, Fixed, 95% CI) -0.01 [-0.04, 0.01]
23Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

6 Conversion to open
cholecystectomy
5 451 Risk Difference (M-H, Fixed, 95% CI) -0.03 [-0.10, 0.05]
Comparison 4. Early versus delayed LC (high-quality trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Bile duct injury 4 388 Odds Ratio (M-H, Fixed, 95% CI) 0.70 [0.14, 3.63]
2 Bile leak requiring ERCP 4 388 Odds Ratio (M-H, Fixed, 95% CI) 5.78 [1.00, 33.29]
3 Intra-abdominal collections
requiring percutaneous
drainage
4 388 Odds Ratio (M-H, Fixed, 95% CI) 2.34 [0.60, 9.19]
4 Superficial infection 4 388 Odds Ratio (M-H, Fixed, 95% CI) 1.24 [0.48, 3.23]
5 Deep infection 4 388 Odds Ratio (M-H, Fixed, 95% CI) 0.43 [0.09, 1.98]
6 Conversion to open
cholecystectomy
4 388 Odds Ratio (M-H, Fixed, 95% CI) 0.94 [0.58, 1.51]
Comparison 5. Early (< 4 days of onset of symptoms) versus delayed LC
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Bile duct injury 2 103 Odds Ratio (M-H, Fixed, 95% CI) 1.16 [0.15, 8.79]
2 Bile leak requiring ERCP 2 103 Odds Ratio (M-H, Fixed, 95% CI) 3.15 [0.12, 82.16]
3 Intra-abdominal collections
requiring percutaneous
drainage
2 103 Odds Ratio (M-H, Fixed, 95% CI) 1.77 [0.33, 9.53]
4 Superficial infection 2 103 Odds Ratio (M-H, Fixed, 95% CI) 1.12 [0.19, 6.60]
5 Deep infection 2 103 Odds Ratio (M-H, Fixed, 95% CI) Not estimable
6 Conversion to open
cholecystectomy
2 103 Odds Ratio (M-H, Fixed, 95% CI) 0.54 [0.18, 1.66]
Comparison 6. Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Bile duct injury 3 348 Odds Ratio (M-H, Fixed, 95% CI) 0.32 [0.03, 3.16]
2 Bile leak requiring ERCP 3 348 Odds Ratio (M-H, Fixed, 95% CI) 7.03 [0.86, 57.69]
3 Intra-abdominal collections
requiring percutaneous
drainage
3 348 Odds Ratio (M-H, Fixed, 95% CI) 2.18 [0.48, 9.90]
4 Superficial infection 3 348 Odds Ratio (M-H, Fixed, 95% CI) 1.50 [0.52, 4.31]
24Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

5 Deep infection 3 348 Odds Ratio (M-H, Fixed, 95% CI) 0.99 [0.20, 5.00]
6 Conversion to open
cholecystectomy
3 348 Odds Ratio (M-H, Fixed, 95% CI) 0.93 [0.56, 1.54]
Comparison 7. Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Bile duct injury 2 249 Odds Ratio (M-H, Fixed, 95% CI) 0.32 [0.01, 7.87]
2 Bile leak requiring ERCP 2 249 Odds Ratio (M-H, Fixed, 95% CI) 7.03 [0.86, 57.69]
3 Intra-abdominal collections
requiring percutaneous
drainage
2 249 Odds Ratio (M-H, Fixed, 95% CI) 4.97 [0.57, 43.14]
4 Superficial Infection 2 249 Odds Ratio (M-H, Fixed, 95% CI) 1.47 [0.40, 5.35]
5 Deep infection 2 249 Odds Ratio (M-H, Fixed, 95% CI) 0.63 [0.10, 3.88]
6 Conversion to open
cholecystectomy
2 249 Odds Ratio (M-H, Fixed, 95% CI) 1.07 [0.61, 1.90]
Analysis 1.1. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 1 Bile duct
injury.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 1 Early versus delayed LC (number of people randomised)
Outcome: 1 Bile duct injury
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 1/36 0.43 [ 0.02, 10.98 ]
Johansson 2003 0/74 1/71 0.32 [ 0.01, 7.87 ]
Kolla 2004 1/20 0/20 3.15 [ 0.12, 82.16 ]
Lai 1998 0/53 0/51 0.0 [ 0.0, 0.0 ]
Lo 1998 0/49 1/50 0.33 [ 0.01, 8.38 ]
Total (95% CI) 223 228 0.63 [ 0.15, 2.70 ]
Total events: 1 (Early LC), 3 (Delayed LC)
Heterogeneity: Chi2 = 1.32, df = 3 (P = 0.72); I2 =0.0%
Test for overall effect: Z = 0.62 (P = 0.53)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
25Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 2 Bile leak
requiring ERCP.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 1 Early versus delayed LC (number of people randomised)
Outcome: 2 Bile leak requiring ERCP
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 0/36 0.0 [ 0.0, 0.0 ]
Johansson 2003 5/74 0/71 11.32 [ 0.61, 208.53 ]
Kolla 2004 1/20 0/20 3.15 [ 0.12, 82.16 ]
Lai 1998 1/53 0/51 2.94 [ 0.12, 73.92 ]
Lo 1998 0/49 0/50 0.0 [ 0.0, 0.0 ]
Total (95% CI) 223 228 5.78 [ 1.00, 33.29 ]
Total events: 7 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 0.51, df = 2 (P = 0.78); I2 =0.0%
Test for overall effect: Z = 1.96 (P = 0.050)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
26Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 3 Intra-
abdominal collections requiring percutaneous drainage.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 1 Early versus delayed LC (number of people randomised)
Outcome: 3 Intra-abdominal collections requiring percutaneous drainage
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 2/27 2/36 1.36 [ 0.18, 10.32 ]
Johansson 2003 2/74 0/71 4.93 [ 0.23, 104.53 ]
Kolla 2004 0/20 0/20 0.0 [ 0.0, 0.0 ]
Lai 1998 2/53 0/51 5.00 [ 0.23, 106.73 ]
Lo 1998 0/49 1/50 0.33 [ 0.01, 8.38 ]
Total (95% CI) 223 228 1.86 [ 0.56, 6.18 ]
Total events: 6 (Early LC), 3 (Delayed LC)
Heterogeneity: Chi2 = 1.98, df = 3 (P = 0.58); I2 =0.0%
Test for overall effect: Z = 1.01 (P = 0.31)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
27Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.4. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 4
Superficial infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 1 Early versus delayed LC (number of people randomised)
Outcome: 4 Superficial infection
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 1/27 0/36 5.1 % 4.13 [ 0.16, 105.45 ]
Johansson 2003 5/74 3/71 35.6 % 1.64 [ 0.38, 7.14 ]
Kolla 2004 1/20 2/20 23.7 % 0.47 [ 0.04, 5.69 ]
Lai 1998 1/53 1/51 12.5 % 0.96 [ 0.06, 15.79 ]
Lo 1998 3/49 2/50 23.2 % 1.57 [ 0.25, 9.80 ]
Total (95% CI) 223 228 100.0 % 1.39 [ 0.56, 3.44 ]
Total events: 11 (Early LC), 8 (Delayed LC)
Heterogeneity: Chi2 = 1.29, df = 4 (P = 0.86); I2 =0.0%
Test for overall effect: Z = 0.71 (P = 0.48)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
28Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.5. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 5 Deep
infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 1 Early versus delayed LC (number of people randomised)
Outcome: 5 Deep infection
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 0/36 0.0 [ 0.0, 0.0 ]
Johansson 2003 2/74 3/71 0.63 [ 0.10, 3.88 ]
Kolla 2004 0/20 0/20 0.0 [ 0.0, 0.0 ]
Lai 1998 0/53 0/51 0.0 [ 0.0, 0.0 ]
Lo 1998 0/49 2/50 0.20 [ 0.01, 4.19 ]
Total (95% CI) 223 228 0.43 [ 0.09, 1.98 ]
Total events: 2 (Early LC), 5 (Delayed LC)
Heterogeneity: Chi2 = 0.42, df = 1 (P = 0.52); I2 =0.0%
Test for overall effect: Z = 1.08 (P = 0.28)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
29Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.6. Comparison 1 Early versus delayed LC (number of people randomised), Outcome 6
Conversion to open cholecystectomy.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 1 Early versus delayed LC (number of people randomised)
Outcome: 6 Conversion to open cholecystectomy
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 1/27 6/36 12.5 % 0.19 [ 0.02, 1.70 ]
Johansson 2003 23/74 20/71 35.5 % 1.15 [ 0.56, 2.35 ]
Kolla 2004 5/20 5/20 9.5 % 1.00 [ 0.24, 4.18 ]
Lai 1998 11/53 11/51 22.4 % 0.95 [ 0.37, 2.44 ]
Lo 1998 5/49 9/50 20.2 % 0.52 [ 0.16, 1.67 ]
Total (95% CI) 223 228 100.0 % 0.84 [ 0.53, 1.34 ]
Total events: 45 (Early LC), 51 (Delayed LC)
Heterogeneity: Chi2 = 3.27, df = 4 (P = 0.51); I2 =0.0%
Test for overall effect: Z = 0.72 (P = 0.47)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
30Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.1. Comparison 2 Early versus delayed LC (number of people operated), Outcome 1 Bile duct
Injury.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 2 Early versus delayed LC (number of people operated)
Outcome: 1 Bile duct Injury
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 1/36 0.43 [ 0.02, 10.98 ]
Johansson 2003 0/74 1/69 0.31 [ 0.01, 7.65 ]
Kolla 2004 1/20 0/20 3.15 [ 0.12, 82.16 ]
Lai 1998 0/53 0/46 0.0 [ 0.0, 0.0 ]
Lo 1998 0/48 1/45 0.31 [ 0.01, 7.70 ]
Total (95% CI) 222 216 0.61 [ 0.14, 2.62 ]
Total events: 1 (Early LC), 3 (Delayed LC)
Heterogeneity: Chi2 = 1.37, df = 3 (P = 0.71); I2 =0.0%
Test for overall effect: Z = 0.66 (P = 0.51)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
31Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.2. Comparison 2 Early versus delayed LC (number of people operated), Outcome 2 Bile leak
requiring ERCP.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 2 Early versus delayed LC (number of people operated)
Outcome: 2 Bile leak requiring ERCP
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 0/36 0.0 [ 0.0, 0.0 ]
Johansson 2003 5/74 0/69 11.00 [ 0.60, 202.75 ]
Kolla 2004 1/20 0/20 3.15 [ 0.12, 82.16 ]
Lai 1998 1/53 0/46 2.66 [ 0.11, 66.83 ]
Lo 1998 0/48 0/45 0.0 [ 0.0, 0.0 ]
Total (95% CI) 222 216 5.55 [ 0.96, 31.94 ]
Total events: 7 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 0.53, df = 2 (P = 0.77); I2 =0.0%
Test for overall effect: Z = 1.92 (P = 0.055)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
32Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.3. Comparison 2 Early versus delayed LC (number of people operated), Outcome 3 Intra-
abdominal collections requiring percutaneous drainage.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 2 Early versus delayed LC (number of people operated)
Outcome: 3 Intra-abdominal collections requiring percutaneous drainage
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 2/27 2/36 34.6 % 1.36 [ 0.18, 10.32 ]
Johansson 2003 2/74 0/69 10.9 % 4.79 [ 0.23, 101.63 ]
Kolla 2004 1/20 0/20 10.1 % 3.15 [ 0.12, 82.16 ]
Lai 1998 2/53 0/46 11.1 % 4.51 [ 0.21, 96.49 ]
Lo 1998 0/48 1/45 33.3 % 0.31 [ 0.01, 7.70 ]
Total (95% CI) 222 216 100.0 % 1.91 [ 0.62, 5.88 ]
Total events: 7 (Early LC), 3 (Delayed LC)
Heterogeneity: Chi2 = 2.09, df = 4 (P = 0.72); I2 =0.0%
Test for overall effect: Z = 1.13 (P = 0.26)
0.001 0.01 0.1 1 10 100 1000
Favours Early LC Favours Delayed LC
33Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.4. Comparison 2 Early versus delayed LC (number of people operated), Outcome 4 Superficial
infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 2 Early versus delayed LC (number of people operated)
Outcome: 4 Superficial infection
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 1/27 0/36 5.0 % 4.13 [ 0.16, 105.45 ]
Johansson 2003 5/74 3/69 35.4 % 1.59 [ 0.37, 6.94 ]
Kolla 2004 1/20 2/20 23.2 % 0.47 [ 0.04, 5.69 ]
Lai 1998 1/53 1/46 12.8 % 0.87 [ 0.05, 14.24 ]
Lo 1998 3/48 2/45 23.6 % 1.43 [ 0.23, 9.00 ]
Total (95% CI) 222 216 100.0 % 1.33 [ 0.54, 3.29 ]
Total events: 11 (Early LC), 8 (Delayed LC)
Heterogeneity: Chi2 = 1.29, df = 4 (P = 0.86); I2 =0.0%
Test for overall effect: Z = 0.61 (P = 0.54)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
34Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.5. Comparison 2 Early versus delayed LC (number of people operated), Outcome 5 Deep
infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 2 Early versus delayed LC (number of people operated)
Outcome: 5 Deep infection
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 0/36 0.0 [ 0.0, 0.0 ]
Johansson 2003 2/74 3/69 0.61 [ 0.10, 3.77 ]
Kolla 2004 0/20 0/20 0.0 [ 0.0, 0.0 ]
Lai 1998 0/53 0/46 0.0 [ 0.0, 0.0 ]
Lo 1998 0/48 2/45 0.18 [ 0.01, 3.84 ]
Total (95% CI) 222 216 0.41 [ 0.09, 1.88 ]
Total events: 2 (Early LC), 5 (Delayed LC)
Heterogeneity: Chi2 = 0.46, df = 1 (P = 0.50); I2 =0.0%
Test for overall effect: Z = 1.14 (P = 0.25)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
35Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.6. Comparison 2 Early versus delayed LC (number of people operated), Outcome 6 Conversion
to open cholecystectomy.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 2 Early versus delayed LC (number of people operated)
Outcome: 6 Conversion to open cholecystectomy
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 1/27 6/36 12.2 % 0.19 [ 0.02, 1.70 ]
Johansson 2003 23/74 20/69 35.1 % 1.10 [ 0.54, 2.26 ]
Kolla 2004 5/20 5/20 9.2 % 1.00 [ 0.24, 4.18 ]
Lai 1998 11/53 11/46 23.0 % 0.83 [ 0.32, 2.15 ]
Lo 1998 5/48 9/45 20.5 % 0.47 [ 0.14, 1.51 ]
Total (95% CI) 222 216 100.0 % 0.79 [ 0.50, 1.25 ]
Total events: 45 (Early LC), 51 (Delayed LC)
Heterogeneity: Chi2 = 3.35, df = 4 (P = 0.50); I2 =0.0%
Test for overall effect: Z = 1.00 (P = 0.32)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
36Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.1. Comparison 3 Early versus delayed LC - risk difference, Outcome 1 Bile duct injury.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 3 Early versus delayed LC - risk difference
Outcome: 1 Bile duct injury
Study or subgroup Early LC Delayed LCRisk
Difference WeightRisk
Difference
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 1/36 13.7 % -0.03 [ -0.11, 0.05 ]
Johansson 2003 0/74 1/71 32.2 % -0.01 [ -0.05, 0.02 ]
Kolla 2004 1/20 0/20 8.9 % 0.05 [ -0.08, 0.18 ]
Lai 1998 0/53 0/51 23.1 % 0.0 [ -0.04, 0.04 ]
Lo 1998 0/49 1/50 22.0 % -0.02 [ -0.07, 0.03 ]
Total (95% CI) 223 228 100.0 % -0.01 [ -0.03, 0.02 ]
Total events: 1 (Early LC), 3 (Delayed LC)
Heterogeneity: Chi2 = 1.49, df = 4 (P = 0.83); I2 =0.0%
Test for overall effect: Z = 0.64 (P = 0.52)
-1 -0.5 0 0.5 1
Favours early LC Favours delayed LC
37Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Early versus delayed LC - risk difference, Outcome 2 Bile leak requiring ERCP.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 3 Early versus delayed LC - risk difference
Outcome: 2 Bile leak requiring ERCP
Study or subgroup Early LC Delayed LCRisk
Difference WeightRisk
Difference
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 0/36 13.7 % 0.0 [ -0.06, 0.06 ]
Johansson 2003 5/74 0/71 32.2 % 0.07 [ 0.01, 0.13 ]
Kolla 2004 1/20 0/20 8.9 % 0.05 [ -0.08, 0.18 ]
Lai 1998 1/53 0/51 23.1 % 0.02 [ -0.03, 0.07 ]
Lo 1998 0/49 0/50 22.0 % 0.0 [ -0.04, 0.04 ]
Total (95% CI) 223 228 100.0 % 0.03 [ 0.00, 0.06 ]
Total events: 7 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 5.01, df = 4 (P = 0.29); I2 =20%
Test for overall effect: Z = 2.06 (P = 0.040)
-0.5 -0.25 0 0.25 0.5
Favours early LC Favours delayed LC
38Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.3. Comparison 3 Early versus delayed LC - risk difference, Outcome 3 Intra-abdominal
collections requiring percutaneous drainage.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 3 Early versus delayed LC - risk difference
Outcome: 3 Intra-abdominal collections requiring percutaneous drainage
Study or subgroup Early LC Delayed LCRisk
Difference WeightRisk
Difference
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 2/27 2/36 13.7 % 0.02 [ -0.11, 0.14 ]
Johansson 2003 2/74 0/71 32.2 % 0.03 [ -0.02, 0.07 ]
Kolla 2004 1/20 0/20 8.9 % 0.05 [ -0.08, 0.18 ]
Lai 1998 2/53 0/51 23.1 % 0.04 [ -0.02, 0.10 ]
Lo 1998 0/49 1/50 22.0 % -0.02 [ -0.07, 0.03 ]
Total (95% CI) 223 228 100.0 % 0.02 [ -0.01, 0.05 ]
Total events: 7 (Early LC), 3 (Delayed LC)
Heterogeneity: Chi2 = 2.73, df = 4 (P = 0.60); I2 =0.0%
Test for overall effect: Z = 1.24 (P = 0.22)
-0.5 -0.25 0 0.25 0.5
Favours early LC Favours delayed LC
39Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.4. Comparison 3 Early versus delayed LC - risk difference, Outcome 4 Superficial infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 3 Early versus delayed LC - risk difference
Outcome: 4 Superficial infection
Study or subgroup Early LC Delayed LCRisk
Difference WeightRisk
Difference
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 1/27 0/36 13.7 % 0.04 [ -0.05, 0.13 ]
Johansson 2003 5/74 3/71 32.2 % 0.03 [ -0.05, 0.10 ]
Kolla 2004 1/20 2/20 8.9 % -0.05 [ -0.21, 0.11 ]
Lai 1998 1/53 1/51 23.1 % 0.00 [ -0.05, 0.05 ]
Lo 1998 3/49 2/50 22.0 % 0.02 [ -0.07, 0.11 ]
Total (95% CI) 223 228 100.0 % 0.01 [ -0.02, 0.05 ]
Total events: 11 (Early LC), 8 (Delayed LC)
Heterogeneity: Chi2 = 1.25, df = 4 (P = 0.87); I2 =0.0%
Test for overall effect: Z = 0.68 (P = 0.49)
-0.5 -0.25 0 0.25 0.5
Favours early LC Favours delayed LC
40Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.5. Comparison 3 Early versus delayed LC - risk difference, Outcome 5 Deep infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 3 Early versus delayed LC - risk difference
Outcome: 5 Deep infection
Study or subgroup Early LC Delayed LCRisk
Difference WeightRisk
Difference
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 0/36 13.7 % 0.0 [ -0.06, 0.06 ]
Johansson 2003 2/74 3/71 32.2 % -0.02 [ -0.07, 0.04 ]
Kolla 2004 0/20 0/20 8.9 % 0.0 [ -0.09, 0.09 ]
Lai 1998 0/53 0/51 23.1 % 0.0 [ -0.04, 0.04 ]
Lo 1998 0/49 2/50 22.0 % -0.04 [ -0.11, 0.03 ]
Total (95% CI) 223 228 100.0 % -0.01 [ -0.04, 0.01 ]
Total events: 2 (Early LC), 5 (Delayed LC)
Heterogeneity: Chi2 = 1.43, df = 4 (P = 0.84); I2 =0.0%
Test for overall effect: Z = 0.94 (P = 0.35)
-0.5 -0.25 0 0.25 0.5
Favours early LC Favours delayed LC
41Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
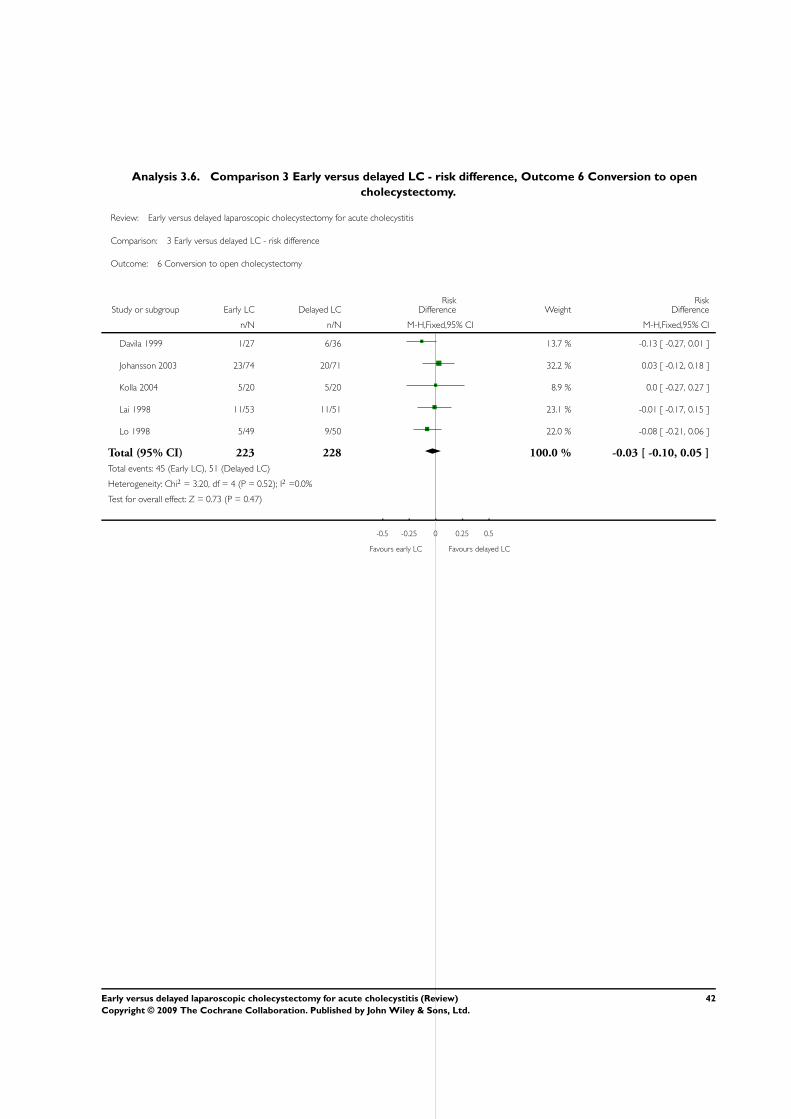
Analysis 3.6. Comparison 3 Early versus delayed LC - risk difference, Outcome 6 Conversion to open
cholecystectomy.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 3 Early versus delayed LC - risk difference
Outcome: 6 Conversion to open cholecystectomy
Study or subgroup Early LC Delayed LCRisk
Difference WeightRisk
Difference
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 1/27 6/36 13.7 % -0.13 [ -0.27, 0.01 ]
Johansson 2003 23/74 20/71 32.2 % 0.03 [ -0.12, 0.18 ]
Kolla 2004 5/20 5/20 8.9 % 0.0 [ -0.27, 0.27 ]
Lai 1998 11/53 11/51 23.1 % -0.01 [ -0.17, 0.15 ]
Lo 1998 5/49 9/50 22.0 % -0.08 [ -0.21, 0.06 ]
Total (95% CI) 223 228 100.0 % -0.03 [ -0.10, 0.05 ]
Total events: 45 (Early LC), 51 (Delayed LC)
Heterogeneity: Chi2 = 3.20, df = 4 (P = 0.52); I2 =0.0%
Test for overall effect: Z = 0.73 (P = 0.47)
-0.5 -0.25 0 0.25 0.5
Favours early LC Favours delayed LC
42Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
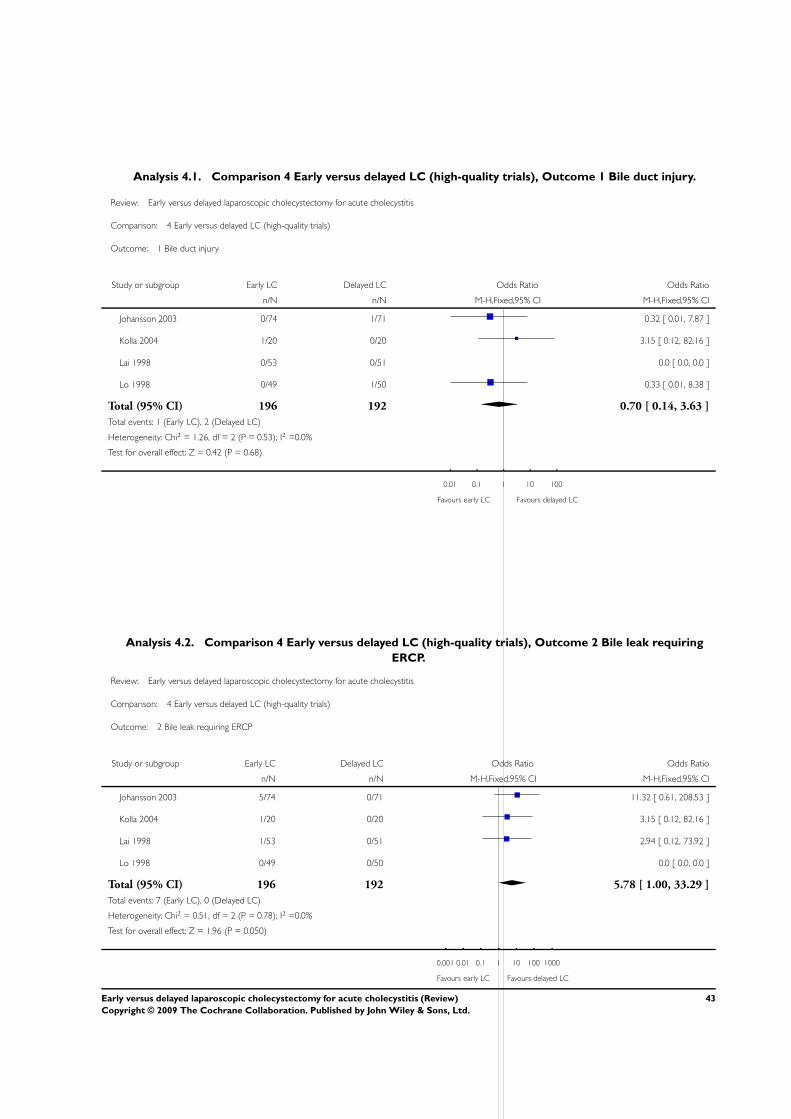
Analysis 4.1. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 1 Bile duct injury.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 4 Early versus delayed LC (high-quality trials)
Outcome: 1 Bile duct injury
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 0/74 1/71 0.32 [ 0.01, 7.87 ]
Kolla 2004 1/20 0/20 3.15 [ 0.12, 82.16 ]
Lai 1998 0/53 0/51 0.0 [ 0.0, 0.0 ]
Lo 1998 0/49 1/50 0.33 [ 0.01, 8.38 ]
Total (95% CI) 196 192 0.70 [ 0.14, 3.63 ]
Total events: 1 (Early LC), 2 (Delayed LC)
Heterogeneity: Chi2 = 1.26, df = 2 (P = 0.53); I2 =0.0%
Test for overall effect: Z = 0.42 (P = 0.68)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
Analysis 4.2. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 2 Bile leak requiring
ERCP.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 4 Early versus delayed LC (high-quality trials)
Outcome: 2 Bile leak requiring ERCP
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 5/74 0/71 11.32 [ 0.61, 208.53 ]
Kolla 2004 1/20 0/20 3.15 [ 0.12, 82.16 ]
Lai 1998 1/53 0/51 2.94 [ 0.12, 73.92 ]
Lo 1998 0/49 0/50 0.0 [ 0.0, 0.0 ]
Total (95% CI) 196 192 5.78 [ 1.00, 33.29 ]
Total events: 7 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 0.51, df = 2 (P = 0.78); I2 =0.0%
Test for overall effect: Z = 1.96 (P = 0.050)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
43Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.3. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 3 Intra-abdominal
collections requiring percutaneous drainage.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 4 Early versus delayed LC (high-quality trials)
Outcome: 3 Intra-abdominal collections requiring percutaneous drainage
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 2/74 0/71 16.9 % 4.93 [ 0.23, 104.53 ]
Kolla 2004 1/20 0/20 15.9 % 3.15 [ 0.12, 82.16 ]
Lai 1998 2/53 0/51 16.7 % 5.00 [ 0.23, 106.73 ]
Lo 1998 0/49 1/50 50.5 % 0.33 [ 0.01, 8.38 ]
Total (95% CI) 196 192 100.0 % 2.34 [ 0.60, 9.19 ]
Total events: 5 (Early LC), 1 (Delayed LC)
Heterogeneity: Chi2 = 1.90, df = 3 (P = 0.59); I2 =0.0%
Test for overall effect: Z = 1.22 (P = 0.22)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
44Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.4. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 4 Superficial infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 4 Early versus delayed LC (high-quality trials)
Outcome: 4 Superficial infection
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 5/74 3/71 37.5 % 1.64 [ 0.38, 7.14 ]
Kolla 2004 1/20 2/20 25.0 % 0.47 [ 0.04, 5.69 ]
Lai 1998 1/53 1/51 13.1 % 0.96 [ 0.06, 15.79 ]
Lo 1998 3/49 2/50 24.4 % 1.57 [ 0.25, 9.80 ]
Total (95% CI) 196 192 100.0 % 1.24 [ 0.48, 3.23 ]
Total events: 10 (Early LC), 8 (Delayed LC)
Heterogeneity: Chi2 = 0.81, df = 3 (P = 0.85); I2 =0.0%
Test for overall effect: Z = 0.45 (P = 0.66)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
Analysis 4.5. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 5 Deep infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 4 Early versus delayed LC (high-quality trials)
Outcome: 5 Deep infection
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 2/74 3/71 0.63 [ 0.10, 3.88 ]
Kolla 2004 0/20 0/20 0.0 [ 0.0, 0.0 ]
Lai 1998 0/53 0/51 0.0 [ 0.0, 0.0 ]
Lo 1998 0/49 2/50 0.20 [ 0.01, 4.19 ]
Total (95% CI) 196 192 0.43 [ 0.09, 1.98 ]
Total events: 2 (Early LC), 5 (Delayed LC)
Heterogeneity: Chi2 = 0.42, df = 1 (P = 0.52); I2 =0.0%
Test for overall effect: Z = 1.08 (P = 0.28)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
45Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.6. Comparison 4 Early versus delayed LC (high-quality trials), Outcome 6 Conversion to open
cholecystectomy.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 4 Early versus delayed LC (high-quality trials)
Outcome: 6 Conversion to open cholecystectomy
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 23/74 20/71 40.5 % 1.15 [ 0.56, 2.35 ]
Kolla 2004 5/20 5/20 10.8 % 1.00 [ 0.24, 4.18 ]
Lai 1998 11/53 11/51 25.6 % 0.95 [ 0.37, 2.44 ]
Lo 1998 5/49 9/50 23.1 % 0.52 [ 0.16, 1.67 ]
Total (95% CI) 196 192 100.0 % 0.94 [ 0.58, 1.51 ]
Total events: 44 (Early LC), 45 (Delayed LC)
Heterogeneity: Chi2 = 1.31, df = 3 (P = 0.73); I2 =0.0%
Test for overall effect: Z = 0.26 (P = 0.79)
0.1 0.2 0.5 1 2 5 10
Favours early LC Favours delayed LC
Analysis 5.1. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 1 Bile duct
injury.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 5 Early (< 4 days of onset of symptoms) versus delayed LC
Outcome: 1 Bile duct injury
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 1/36 73.2 % 0.43 [ 0.02, 10.98 ]
Kolla 2004 1/20 0/20 26.8 % 3.15 [ 0.12, 82.16 ]
Total (95% CI) 47 56 100.0 % 1.16 [ 0.15, 8.79 ]
Total events: 1 (Early LC), 1 (Delayed LC)
Heterogeneity: Chi2 = 0.72, df = 1 (P = 0.40); I2 =0.0%
Test for overall effect: Z = 0.14 (P = 0.89)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
46Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
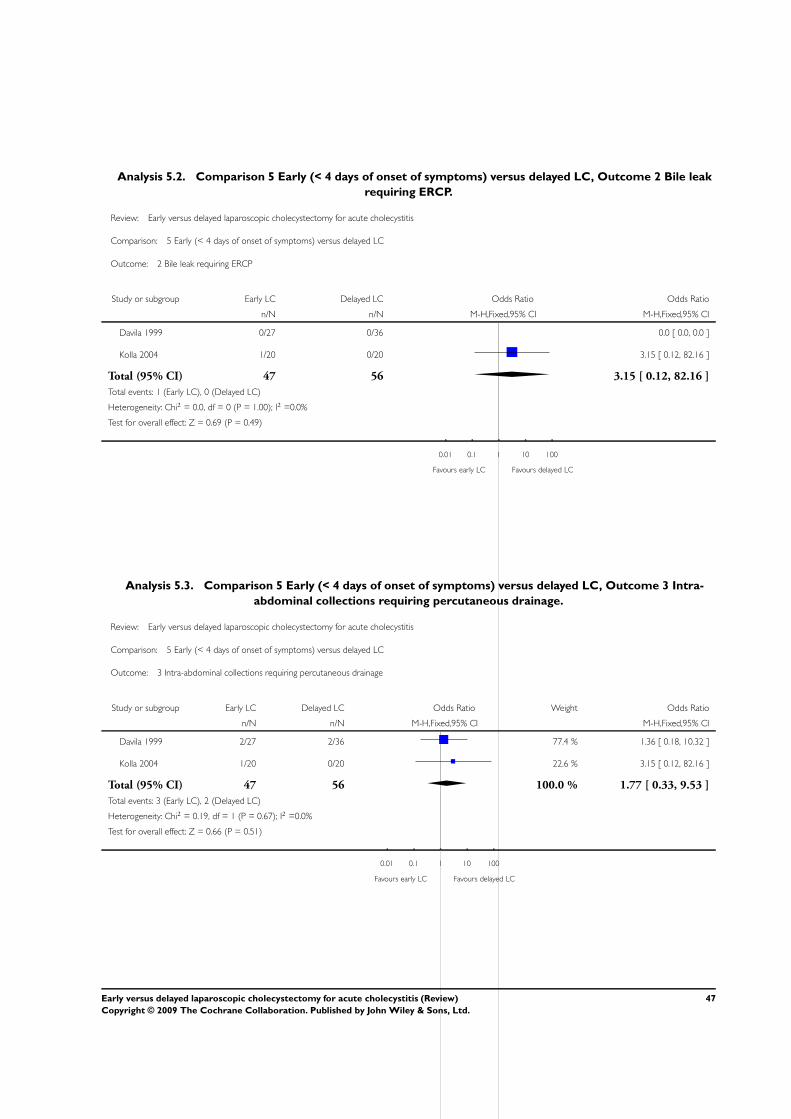
Analysis 5.2. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 2 Bile leak
requiring ERCP.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 5 Early (< 4 days of onset of symptoms) versus delayed LC
Outcome: 2 Bile leak requiring ERCP
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 0/36 0.0 [ 0.0, 0.0 ]
Kolla 2004 1/20 0/20 3.15 [ 0.12, 82.16 ]
Total (95% CI) 47 56 3.15 [ 0.12, 82.16 ]
Total events: 1 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 0.0, df = 0 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 0.69 (P = 0.49)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
Analysis 5.3. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 3 Intra-
abdominal collections requiring percutaneous drainage.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 5 Early (< 4 days of onset of symptoms) versus delayed LC
Outcome: 3 Intra-abdominal collections requiring percutaneous drainage
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 2/27 2/36 77.4 % 1.36 [ 0.18, 10.32 ]
Kolla 2004 1/20 0/20 22.6 % 3.15 [ 0.12, 82.16 ]
Total (95% CI) 47 56 100.0 % 1.77 [ 0.33, 9.53 ]
Total events: 3 (Early LC), 2 (Delayed LC)
Heterogeneity: Chi2 = 0.19, df = 1 (P = 0.67); I2 =0.0%
Test for overall effect: Z = 0.66 (P = 0.51)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
47Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.4. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 4 Superficial
infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 5 Early (< 4 days of onset of symptoms) versus delayed LC
Outcome: 4 Superficial infection
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 1/27 0/36 17.7 % 4.13 [ 0.16, 105.45 ]
Kolla 2004 1/20 2/20 82.3 % 0.47 [ 0.04, 5.69 ]
Total (95% CI) 47 56 100.0 % 1.12 [ 0.19, 6.60 ]
Total events: 2 (Early LC), 2 (Delayed LC)
Heterogeneity: Chi2 = 1.08, df = 1 (P = 0.30); I2 =8%
Test for overall effect: Z = 0.13 (P = 0.90)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
Analysis 5.5. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 5 Deep
infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 5 Early (< 4 days of onset of symptoms) versus delayed LC
Outcome: 5 Deep infection
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 0/27 0/36 0.0 [ 0.0, 0.0 ]
Kolla 2004 0/20 0/20 0.0 [ 0.0, 0.0 ]
Total (95% CI) 47 56 0.0 [ 0.0, 0.0 ]
Total events: 0 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 0.0, df = 0 (P<0.00001); I2 =0.0%
Test for overall effect: Z = 0.0 (P < 0.00001)
0.1 0.2 0.5 1 2 5 10
Favours early LC Favours delayed LC
48Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
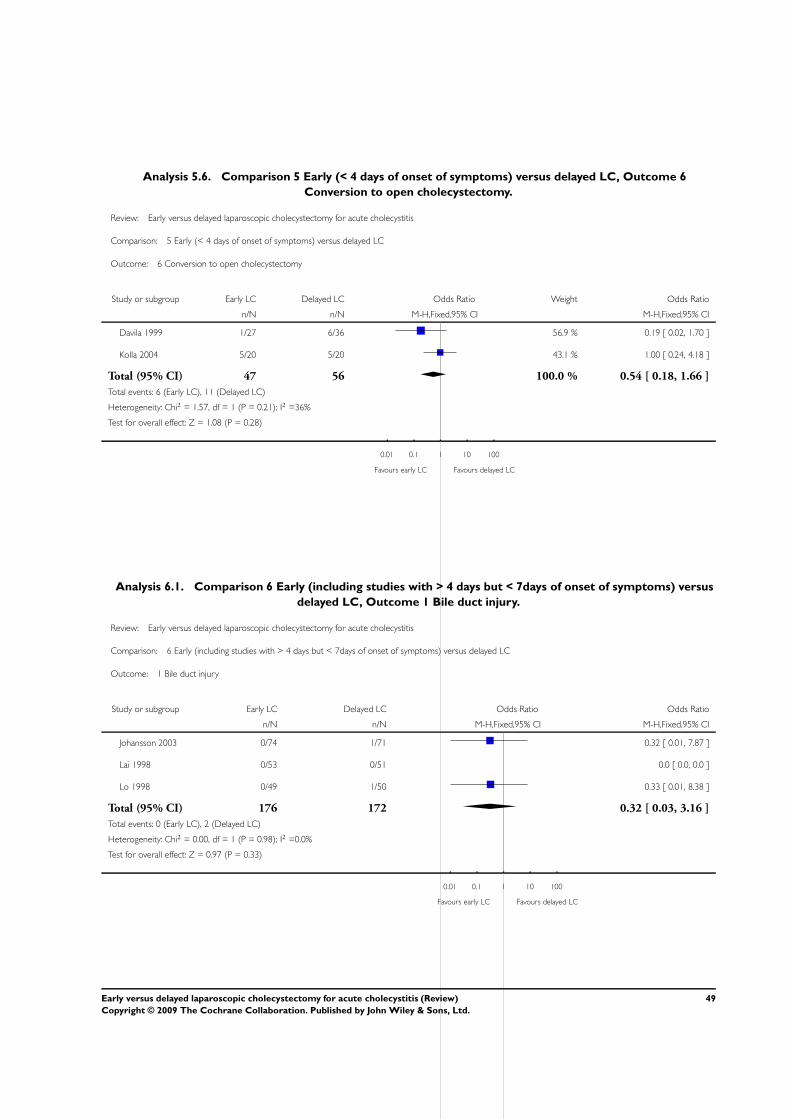
Analysis 5.6. Comparison 5 Early (< 4 days of onset of symptoms) versus delayed LC, Outcome 6
Conversion to open cholecystectomy.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 5 Early (< 4 days of onset of symptoms) versus delayed LC
Outcome: 6 Conversion to open cholecystectomy
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Davila 1999 1/27 6/36 56.9 % 0.19 [ 0.02, 1.70 ]
Kolla 2004 5/20 5/20 43.1 % 1.00 [ 0.24, 4.18 ]
Total (95% CI) 47 56 100.0 % 0.54 [ 0.18, 1.66 ]
Total events: 6 (Early LC), 11 (Delayed LC)
Heterogeneity: Chi2 = 1.57, df = 1 (P = 0.21); I2 =36%
Test for overall effect: Z = 1.08 (P = 0.28)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
Analysis 6.1. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus
delayed LC, Outcome 1 Bile duct injury.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC
Outcome: 1 Bile duct injury
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 0/74 1/71 0.32 [ 0.01, 7.87 ]
Lai 1998 0/53 0/51 0.0 [ 0.0, 0.0 ]
Lo 1998 0/49 1/50 0.33 [ 0.01, 8.38 ]
Total (95% CI) 176 172 0.32 [ 0.03, 3.16 ]
Total events: 0 (Early LC), 2 (Delayed LC)
Heterogeneity: Chi2 = 0.00, df = 1 (P = 0.98); I2 =0.0%
Test for overall effect: Z = 0.97 (P = 0.33)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
49Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
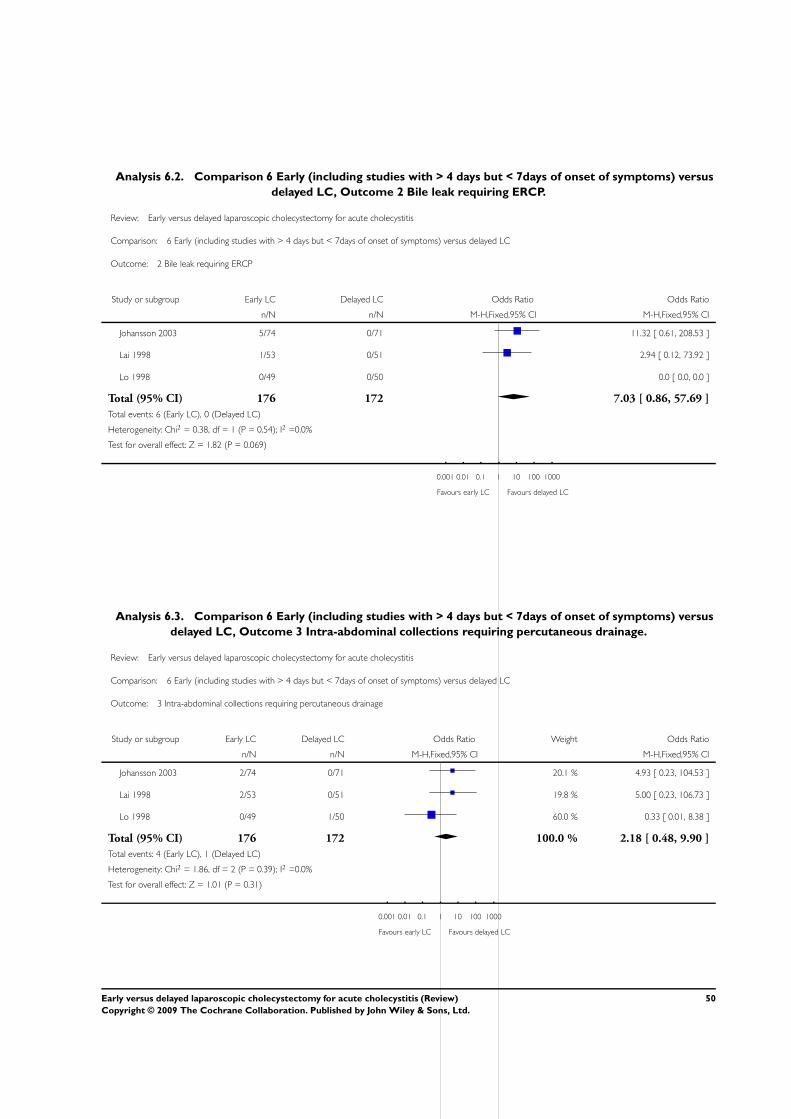
Analysis 6.2. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus
delayed LC, Outcome 2 Bile leak requiring ERCP.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC
Outcome: 2 Bile leak requiring ERCP
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 5/74 0/71 11.32 [ 0.61, 208.53 ]
Lai 1998 1/53 0/51 2.94 [ 0.12, 73.92 ]
Lo 1998 0/49 0/50 0.0 [ 0.0, 0.0 ]
Total (95% CI) 176 172 7.03 [ 0.86, 57.69 ]
Total events: 6 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 0.38, df = 1 (P = 0.54); I2 =0.0%
Test for overall effect: Z = 1.82 (P = 0.069)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
Analysis 6.3. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus
delayed LC, Outcome 3 Intra-abdominal collections requiring percutaneous drainage.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC
Outcome: 3 Intra-abdominal collections requiring percutaneous drainage
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 2/74 0/71 20.1 % 4.93 [ 0.23, 104.53 ]
Lai 1998 2/53 0/51 19.8 % 5.00 [ 0.23, 106.73 ]
Lo 1998 0/49 1/50 60.0 % 0.33 [ 0.01, 8.38 ]
Total (95% CI) 176 172 100.0 % 2.18 [ 0.48, 9.90 ]
Total events: 4 (Early LC), 1 (Delayed LC)
Heterogeneity: Chi2 = 1.86, df = 2 (P = 0.39); I2 =0.0%
Test for overall effect: Z = 1.01 (P = 0.31)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
50Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.4. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus
delayed LC, Outcome 4 Superficial infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC
Outcome: 4 Superficial infection
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 5/74 3/71 50.0 % 1.64 [ 0.38, 7.14 ]
Lai 1998 1/53 1/51 17.5 % 0.96 [ 0.06, 15.79 ]
Lo 1998 3/49 2/50 32.5 % 1.57 [ 0.25, 9.80 ]
Total (95% CI) 176 172 100.0 % 1.50 [ 0.52, 4.31 ]
Total events: 9 (Early LC), 6 (Delayed LC)
Heterogeneity: Chi2 = 0.11, df = 2 (P = 0.94); I2 =0.0%
Test for overall effect: Z = 0.75 (P = 0.45)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
Analysis 6.5. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus
delayed LC, Outcome 5 Deep infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC
Outcome: 5 Deep infection
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 2/74 0/71 4.93 [ 0.23, 104.53 ]
Lai 1998 0/53 0/51 0.0 [ 0.0, 0.0 ]
Lo 1998 0/49 2/50 0.20 [ 0.01, 4.19 ]
Total (95% CI) 176 172 0.99 [ 0.20, 5.00 ]
Total events: 2 (Early LC), 2 (Delayed LC)
Heterogeneity: Chi2 = 2.14, df = 1 (P = 0.14); I2 =53%
Test for overall effect: Z = 0.01 (P = 0.99)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
51Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
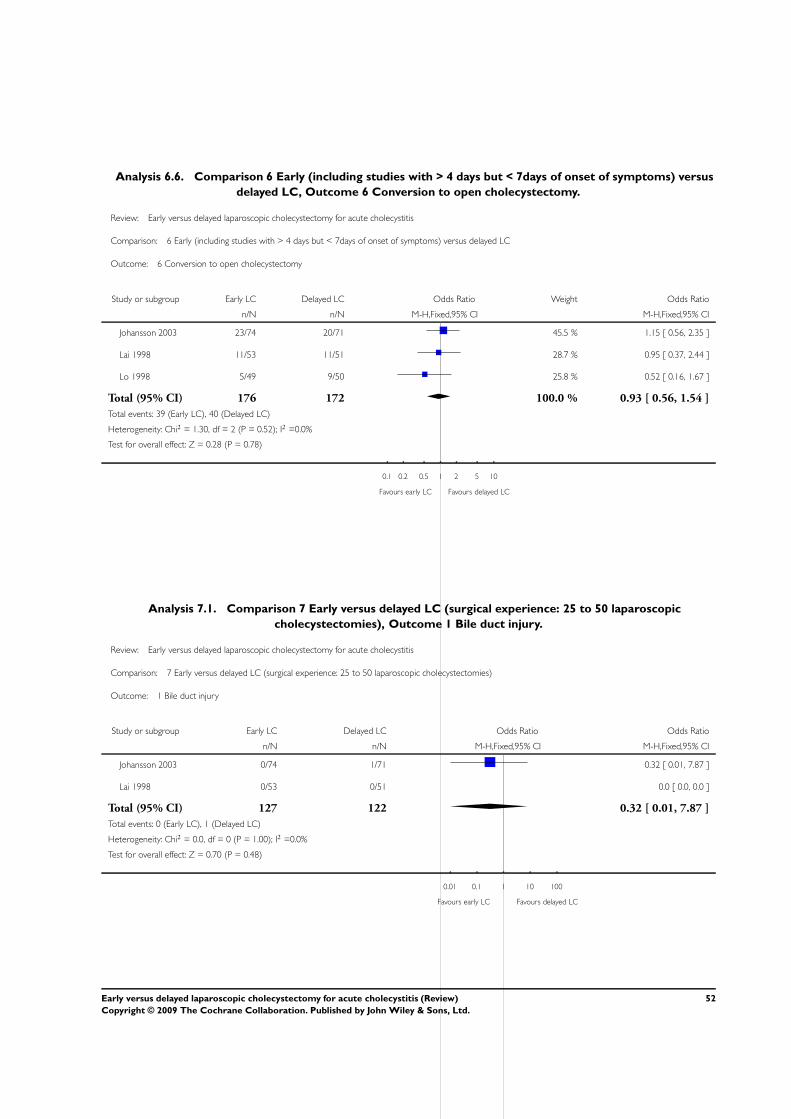
Analysis 6.6. Comparison 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus
delayed LC, Outcome 6 Conversion to open cholecystectomy.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 6 Early (including studies with > 4 days but < 7days of onset of symptoms) versus delayed LC
Outcome: 6 Conversion to open cholecystectomy
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 23/74 20/71 45.5 % 1.15 [ 0.56, 2.35 ]
Lai 1998 11/53 11/51 28.7 % 0.95 [ 0.37, 2.44 ]
Lo 1998 5/49 9/50 25.8 % 0.52 [ 0.16, 1.67 ]
Total (95% CI) 176 172 100.0 % 0.93 [ 0.56, 1.54 ]
Total events: 39 (Early LC), 40 (Delayed LC)
Heterogeneity: Chi2 = 1.30, df = 2 (P = 0.52); I2 =0.0%
Test for overall effect: Z = 0.28 (P = 0.78)
0.1 0.2 0.5 1 2 5 10
Favours early LC Favours delayed LC
Analysis 7.1. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic
cholecystectomies), Outcome 1 Bile duct injury.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies)
Outcome: 1 Bile duct injury
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 0/74 1/71 0.32 [ 0.01, 7.87 ]
Lai 1998 0/53 0/51 0.0 [ 0.0, 0.0 ]
Total (95% CI) 127 122 0.32 [ 0.01, 7.87 ]
Total events: 0 (Early LC), 1 (Delayed LC)
Heterogeneity: Chi2 = 0.0, df = 0 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 0.70 (P = 0.48)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
52Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
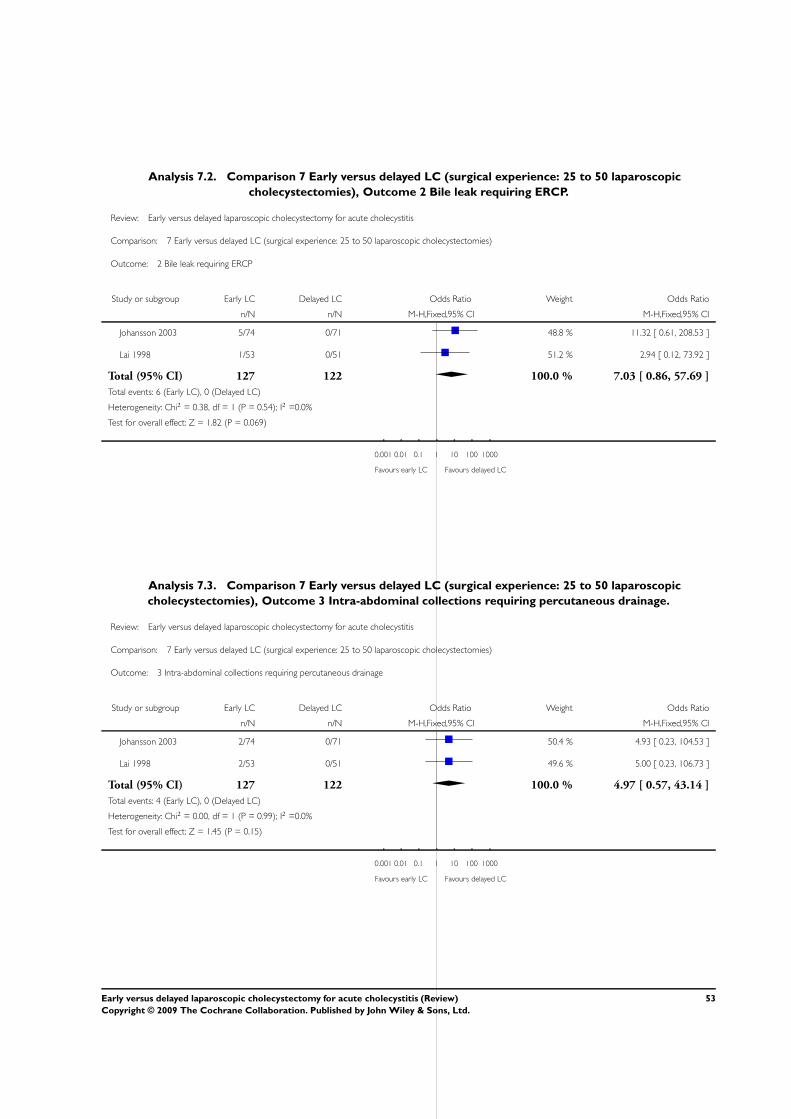
Analysis 7.2. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic
cholecystectomies), Outcome 2 Bile leak requiring ERCP.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies)
Outcome: 2 Bile leak requiring ERCP
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 5/74 0/71 48.8 % 11.32 [ 0.61, 208.53 ]
Lai 1998 1/53 0/51 51.2 % 2.94 [ 0.12, 73.92 ]
Total (95% CI) 127 122 100.0 % 7.03 [ 0.86, 57.69 ]
Total events: 6 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 0.38, df = 1 (P = 0.54); I2 =0.0%
Test for overall effect: Z = 1.82 (P = 0.069)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
Analysis 7.3. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic
cholecystectomies), Outcome 3 Intra-abdominal collections requiring percutaneous drainage.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies)
Outcome: 3 Intra-abdominal collections requiring percutaneous drainage
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 2/74 0/71 50.4 % 4.93 [ 0.23, 104.53 ]
Lai 1998 2/53 0/51 49.6 % 5.00 [ 0.23, 106.73 ]
Total (95% CI) 127 122 100.0 % 4.97 [ 0.57, 43.14 ]
Total events: 4 (Early LC), 0 (Delayed LC)
Heterogeneity: Chi2 = 0.00, df = 1 (P = 0.99); I2 =0.0%
Test for overall effect: Z = 1.45 (P = 0.15)
0.001 0.01 0.1 1 10 100 1000
Favours early LC Favours delayed LC
53Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.4. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic
cholecystectomies), Outcome 4 Superficial Infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies)
Outcome: 4 Superficial Infection
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 5/74 3/71 74.1 % 1.64 [ 0.38, 7.14 ]
Lai 1998 1/53 1/51 25.9 % 0.96 [ 0.06, 15.79 ]
Total (95% CI) 127 122 100.0 % 1.47 [ 0.40, 5.35 ]
Total events: 6 (Early LC), 4 (Delayed LC)
Heterogeneity: Chi2 = 0.11, df = 1 (P = 0.74); I2 =0.0%
Test for overall effect: Z = 0.58 (P = 0.56)
0.01 0.1 1 10 100
Favours early LC Favours delayed LC
Analysis 7.5. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic
cholecystectomies), Outcome 5 Deep infection.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies)
Outcome: 5 Deep infection
Study or subgroup Early LC Delayed LC Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 2/74 3/71 0.63 [ 0.10, 3.88 ]
Lai 1998 0/53 0/51 0.0 [ 0.0, 0.0 ]
Total (95% CI) 127 122 0.63 [ 0.10, 3.88 ]
Total events: 2 (Early LC), 3 (Delayed LC)
Heterogeneity: Chi2 = 0.0, df = 0 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 0.50 (P = 0.62)
0.1 0.2 0.5 1 2 5 10
Favours early LC Favours delayed LC
54Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.6. Comparison 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic
cholecystectomies), Outcome 6 Conversion to open cholecystectomy.
Review: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis
Comparison: 7 Early versus delayed LC (surgical experience: 25 to 50 laparoscopic cholecystectomies)
Outcome: 6 Conversion to open cholecystectomy
Study or subgroup Early LC Delayed LC Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Johansson 2003 23/74 20/71 61.3 % 1.15 [ 0.56, 2.35 ]
Lai 1998 11/53 11/51 38.7 % 0.95 [ 0.37, 2.44 ]
Total (95% CI) 127 122 100.0 % 1.07 [ 0.61, 1.90 ]
Total events: 34 (Early LC), 31 (Delayed LC)
Heterogeneity: Chi2 = 0.10, df = 1 (P = 0.75); I2 =0.0%
Test for overall effect: Z = 0.24 (P = 0.81)
0.2 0.5 1 2 5
Favours early LC Favours delayed LC
A D D I T I O N A L T A B L E S
Table 1. Common bile duct stones
Study Surgeon’s expe-
rience
Early group Delayed group Treatment Per-operative
cholangiogram
Notes
Davila 1999 Not given. 0 2 ’Resolved at the
same operation’ -
No further details
given.
Not mentioned.
Johansson 2003 Minimum 25 la-
paro-
scopic cholecys-
tectomies.
5 3 Laparoscopic
common bile duct
exploration.
Post-op ERCP.
Yes. One patient in
each group had
to be converted
to open common
bile duct explo-
ration because of
large common bile
duct stones
Kolla 2004 Surgical consul-
tant.
0 0 Not applicable. No. Co-existing
common bile duct
stones were exclu-
sion criteria.
55Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Common bile duct stones (Continued)
Lai 1998 Minimum 50 la-
paro-
scopic cholecys-
tectomies.
0 0 Not applicable. No. Co-existing
common bile duct
stones were exclu-
sion criteria.
Lo 1998 More
than 300 laparo-
scopic cholecys-
tectomies.
0 0 Preoperative selec-
tive ERCP.
No.
ERCP = endoscopic retrograde cholangio-pancreatography
Table 2. Conversion and bile duct injury rates (Based on people who underwent surgery)
Study Conversion-ELC Conversion -DLC Conversion-
crossover
Bile duct injury-
ELC
Bile duct injury-
DLC
Davila 1999 1/27 (3.7%) 6/36 (16.7%) 4/5 (80%) 0/27 (0%) 1/36 (2.8%)
Johansson 2003 23/74 (31.1%) 20/69 (29%) 10/18 (55.5%) 0/74 (0%) 1/69 (1.4%)
Kolla 2004 5/20 (25%) 5/20 (25%) Not applicable. 1/20 (5%) 0/20 (0%)
Lai 1998 11/53 (20.8%) 11/46 (23.9%) 2/8 (25%) 0/53 (0%) 0/46 (0%)
Lo 1998 5/48 (10.4%) 9/45 (20%) 2/9 (22.2%) 0/48 (0%) 1/45 (2.2%)
All studies 45/222 (20.3%) 51/216 (23.6%) 18/40 (45%) 1/222 (0.5%) 3/216 (1.4%)
ELC = early laparoscopic cholecystectomy
DLC = delayed laparoscopic cholecystectomy
Table 3. Odds ratio and risk difference (95% Confidence intervals)
Outcome Fixed,
ITT
Random,
ITT
Fixed/
available
case
Random/
available
case
Good
quality,
fixed
“Zero”,
Kt+Kc=1 (
Sweeting
2004)
“Zero”,
Kt+Kc=0.
1
(Sweeting
2004)
“Zero”,
Kt+Kc=0.
01
(Sweeting
2004)
Risk
difference
Bile duct
injury
0.63 [0.15,
2.70]
0.61 [0.12,
3.07]
0.61 [0.14,
2.62]
0.59 [0.12,
2.98]
0.70 [0.14,
3.63]
1.47 [0.32,
6.70]
1.12 [0.09,
13.50]
1.02 [0.07,
15.91]
-0.01 [-0.
03, 0.02]
Bile leak
requiring
ERCP
5.78 [1.00,
33.29]
5.03 [0.83,
30.48]
5.55 [0.96,
31.94]
4.82 [0.80,
29.21]
5.78 [1.00,
33.29]
1.91 [0.57,
6.40]
17.3 [0.76,
391.37]
171.2 [0.
01,
0.03 [0.00,
0.06]
56Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 3. Odds ratio and risk difference (95% Confidence intervals) (Continued)
2494435.
29]
Intra-
abdominal
collections
requiring
drainage
1.86 [0.56,
6.18]
1.91 [0.55,
6.63]
1.91 [0.62,
5.88]
1.85 [0.53,
6.41]
2.34 [0.60,
9.19]
Not appli-
cable
Not appli-
cable
Not appli-
cable
0.02 [-0.
01, 0.05]
Superficial
infections
1.39 [0.56,
3.44]
1.38 [0.54,
3.52]
1.33 [0.54,
3.29]
1.32 [0.52,
3.37]
1.24 [0.48,
3.23]
Not appli-
cable
Not appli-
cable
Not appli-
cable
0.01 [-0.
02, 0.05]
Deep
infections
0.43 [0.09,
1.98]
0.46 [0.10,
2.22]
0.41 [0.09,
1.88]
0.44 [0.09,
2.12]
0.43 [0.09,
1.98]
0.78 [0.24,
2.62]
0.43 [0.09,
2.08]
0.39 [0.08,
2.02]
-0.01 [-0.
04, 0.01]
Conver-
sions
0.84 [0.53,
1.34]
0.87 [0.55,
1.4]
0.79 [0.5,
1.25]
0.82 [0.51,
1.31]
0.94 [0.58,
1.51]
Not appli-
cable
Not appli-
cable
Not appli-
cable
-0.03 [-0.
10, 0.05]
ITT = intention-to-treat analysis
ERCP = endoscopic retrograde cholangio-pancreatography
Table 4. Heterogeneity
Outcome Chi-square test Higgin’s I square
Bile duct injury 0.72 0%
Bile leak requiring ERCP 0.78 0%
Intra-abdominal collections requiring
drainage
0.58 0%
Superficial infections 0.86 0%
Deep infections 0.52 0%
Conversions 0.51 0%
ERCP = endoscopic retrograde cholangio-pancreatography
57Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 5. Subgroup analysis (Odds ratio - 95% Confidence intervals)
Outcome All studies ELC less than 4 days ELC (excluding column 3) Surgical experience 25 to
50 laparoscopic cholecys-
tectomy
Bile duct injury 0.63 [0.15, 2.70] 1.16 [0.15, 8.79] 0.32 [0.03, 3.16] 0.32 [0.01, 7.87]
Bile leak requiring ERCP 5.78 [1.00, 33.29] 3.15 [0.12, 82.16] 7.03 [0.86, 57.69] 7.03 [0.86, 57.69]
Intra-abdominal collec-
tions requiring drainage
1.86 [0.56, 6.18] 1.77 [0.33, 9.53] 2.18 [0.48, 9.90] 4.97 [0.57, 43.14]
Superficial Infections 1.39 [0.56, 3.44] 1.12 [0.19, 6.60] 1.50 [0.52, 4.31] 1.47 [0.40, 5.35]
Deep Infections 0.43 [0.09, 1.98] Not estimable 0.99 [0.20, 5.00] 0.63 [0.10, 3.88]
Conversions 0.84 [0.53, 1.34] 0.54 [0.18, 1.66] 0.93 [0.56, 1.54] 1.07 [0.61, 1.90]
ELC = early laparoscopic cholecystectomy
Table 6. Non-resolving or recurrent cholecystitis
Study Delayed laparoscopic
cholecystectomy
Emergency surgery in de-
layed group
Emergency surgery in de-
layed group (%)
Con-
version to open cholecys-
tecomy in the emergency
surgery in delayed group
Davila 1999 36 5 13.9% 4
Johansson 2003 71 18 25% 10
Kolla 2004 20 0 0% 0
Lai 1998 51 8 15.7% 2
Lo 1998 50 9 18% 2
Total 228 40 17.5% 18
Table 7. Operating time and hospital stay
Study Early-operating time Delay-operating time Early -hospital stay Delay-hospital stay
Minutes (Median) Minutes (Median) Days (Median) Days (Median)
Davila 1999 71 50 1.6 2.7
58Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
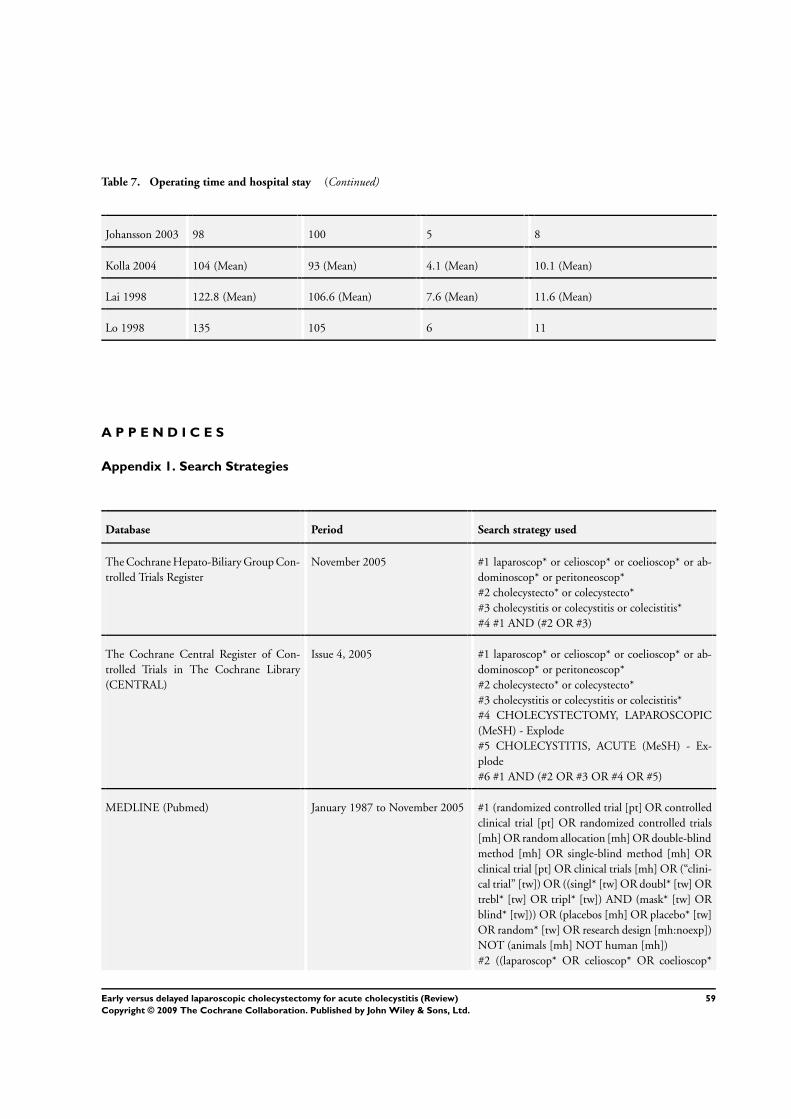
Table 7. Operating time and hospital stay (Continued)
Johansson 2003 98 100 5 8
Kolla 2004 104 (Mean) 93 (Mean) 4.1 (Mean) 10.1 (Mean)
Lai 1998 122.8 (Mean) 106.6 (Mean) 7.6 (Mean) 11.6 (Mean)
Lo 1998 135 105 6 11
A P P E N D I C E S
Appendix 1. Search Strategies
Database Period Search strategy used
The Cochrane Hepato-Biliary Group Con-
trolled Trials Register
November 2005 #1 laparoscop* or celioscop* or coelioscop* or ab-
dominoscop* or peritoneoscop*
#2 cholecystecto* or colecystecto*
#3 cholecystitis or colecystitis or colecistitis*
#4 #1 AND (#2 OR #3)
The Cochrane Central Register of Con-
trolled Trials in The Cochrane Library
(CENTRAL)
Issue 4, 2005 #1 laparoscop* or celioscop* or coelioscop* or ab-
dominoscop* or peritoneoscop*
#2 cholecystecto* or colecystecto*
#3 cholecystitis or colecystitis or colecistitis*
#4 CHOLECYSTECTOMY, LAPAROSCOPIC
(MeSH) - Explode
#5 CHOLECYSTITIS, ACUTE (MeSH) - Ex-
plode
#6 #1 AND (#2 OR #3 OR #4 OR #5)
MEDLINE (Pubmed) January 1987 to November 2005 #1 (randomized controlled trial [pt] OR controlled
clinical trial [pt] OR randomized controlled trials
[mh] OR random allocation [mh] OR double-blind
method [mh] OR single-blind method [mh] OR
clinical trial [pt] OR clinical trials [mh] OR (“clini-
cal trial” [tw]) OR ((singl* [tw] OR doubl* [tw] OR
trebl* [tw] OR tripl* [tw]) AND (mask* [tw] OR
blind* [tw])) OR (placebos [mh] OR placebo* [tw]
OR random* [tw] OR research design [mh:noexp])
NOT (animals [mh] NOT human [mh])
#2 ((laparoscop* OR celioscop* OR coelioscop*
59Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
OR abdominoscop* OR peritoneoscop*) AND
(cholecystecto* OR colecystecto*)) OR (cholecysti-
tis OR colecystitis OR colecistitis*) OR (CHOLE-
CYSTECTOMY LAPAROSCOPIC (MeSH) OR
CHOLECYSTITIS ACUTE (MeSH))
#3 #1 and #2
EMBASE (Dialog Datastar) January 1987 to November 2005 1.RANDOMIZED-CONTROLLED-TRIAL#.
DE.
2.RANDOMIZATION#.W..DE.
3.CONTROLLED-STUDY#.DE.
4.MULTICENTER-STUDY#.DE.
5.PHASE-3-CLINICAL-TRIAL#.DE.
6.PHASE-4-CLINICAL-TRIAL#.DE.
7.DOUBLE-BLIND-PROCEDURE#.DE.
8.SINGLE-BLIND-PROCEDURE#.DE.
9.1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8
10.RANDOM$ OR CROSSOVER$ OR CROSS-
OVER OR CROSS ADJ OVER OR FACTO-
RIAL$ OR PLACEBO$ OR VOLUNTEER$
11.(SINGLE OR DOUBLE OR TREBLE OR
TRIPLE) NEAR (BLIND OR MASK)
12.9 OR 10 OR 11
13.12 AND HUMAN=YES
14.laparoscop$ OR celioscop$ OR coelioscop$ OR
abdominoscop$ OR peritoneoscop$
15.cholecystect$ OR colecystect$
16.cholecystitis OR colecystitis OR colecistitis
17.CHOLECYSTECTOMY#.W..DE. AND LA-
PAROSCOPIC-SURGERY#.DE.
18.ACUTE-CHOLECYSTITIS#.DE.
19.14 AND 15
20.16 OR 17 OR 18 OR 19
21.13 AND 20
Science Citation Index Expanded ((http://
portal.isiknowledge.com/portal.cgi?
DestApp=WOS&Func=Frame)
January 1945 to December 2005 #1 TS=(laparoscop* or celioscop* or coelioscop* or
abdominoscop* or
peritoneoscop*)
#2 TS=(cholecystecto* or colecystecto*)
#3 TS=(cholecystitis or colecystitis or colecistitis*)
#4 #1 AND (#2 OR #3)
#5 TS=(random* OR blind* OR placebo* OR
meta-analysis)
#6 #4 AND #5
60Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

F E E D B A C K
Early versus delayed laparoscopic cholecystectomy
Summary
Date of Submission: 13-Feb-2007
Name: Groot Koerkamp
Email Address: [email protected]
Personal Description: Occupation resident general surgery, epidemiologist.
Feedback: The authors conclude that early laparoscopic cholecystectomy appears safe because no significant difference was found in
complication and conversion rate.
This is not a valid conclusion because the data is insufficiently powered to find such differences: the confidence intervals are very wide
and include over 6-fold differences in negative outcomes. If a 6-fold difference (lower border confidence interval of 0.15) is not unlikely
given the available evidence, you cannot conclude that you know that both strategies are equal: you don’t know! Absence of evidence
is not evidence of absence.
Submitter agrees with default conflict of interest statement:
I certify that I have no affiliations with or involvement in any organization or entity with a financial interest in the subject matter of
my feedback.
Reply
We thank Dr Groot Koerkamp for his comments.
The main reasons that delayed laparoscopic cholecystectomy has been preferred over early laparoscopic cholecystectomy is the fear of
increased bile duct injury risk and conversion to open cholecystectomy (although conversion is not considered a complication) during
early laparoscopic cholecystectomy. All the five trials included in our review reported the outcome ’bile duct injury’. The meta-analysis
showed an odds ratio of 0.63 (95% CI 0.15 to 2.70). Accordingly, there is no statistically significant difference. You are right that the
confidence interval is wide, ie, we cannot exclude that with the emergence of more data we could, one day, get evidence favouring one
strategy over the other.
In the Conclusions section, we have acknowledged the fact that the confidence intervals are wide and the benefits of early laparoscopic
cholecystectomy may have been overlooked indicating that the finding may be due to ’lack of evidence of effect’. However, with the
current evidence available, it appears that early laparoscopic cholecystectomy is at least as safe as delayed laparoscopic cholecystectomy.
We could not have made this conclusion if the bile duct injury rate was higher in early than delayed laparoscopic cholecystectomy
(whether statistically significant or not). At the same time, we could not have concluded that early laparoscopic cholecystectomy is safer
than delayed laparoscopic cholecystectomy as there is no statistical significance in the outcome. It may well be that early laparoscopic
cholecystectomy is better than delayed laparoscopic cholecystectomy with regards to reduced bile duct injury rate. However, until
further trials are available, it is not possible to come to this conclusion. In the interim, it is reasonable to conclude that early laparoscopic
cholecystectomy seems as safe as delayed laparoscopic cholecystectomy based on meta-analysis of five randomised clinical trials. If
expertise is available, there are other advantages in early laparoscopic cholecystectomy: decreased hospital stay and avoiding the exposure
of patients to the risks of gallstones during the waiting period.
We fully concert that absence of evidence is not evidence of absence of a difference between the two strategies. We may wish for more
data - but until they appear, we have to treat patients as continuously and evidence-based as possible.
Contributors
Kurinchi Gurusamy, primary author
14 February, 2007
London, UK
61Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Early versus delayed laparoscopic cholecystectomy
Summary
Date of Submission: 26-Jul-2007
Name: Stefan Sauerland
Email Address: [email protected]
Personal Description: Occupation surgical researcher and meta-analyst
Feedback: This Cochrane review is a well-written and very informative piece of work. However, I have noticed one obvious mistake in
the tables, which requires correction. In table 8, the length of hospital stay for the delayed group of the Kolla trial is stated to be 6.1
days. In truth, the correct figure is 10.1 days. Only the standard deviation was 6.1 days. Therefore, the author’s summarizing statement
that “hospital stay was about three days shorter in the early group” seems too sceptical. In fact, three of the four fully published trials
(Lai, Lo, and Kolla) have shown larger reductions in hospital stay (4, 5, and 6 days, respectively).
Submitter agrees with default conflict of interest statement:
I certify that I have no affiliations with or involvement in any organization or entity with a financial interest in the subject matter of
my feedback.
Reply
Thank you for your comments. This has now been corrected.
Contributors
Kurinchi Gurusamy, primary author
28 July, 2007
London, UK
W H A T ’ S N E W
Last assessed as up-to-date: 9 August 2006.
Date Event Description
20 October 2008 Amended Converted to new review format.
H I S T O R Y
Protocol first published: Issue 3, 2005
Review first published: Issue 4, 2006
62Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C O N T R I B U T I O N S O F A U T H O R S
K Gurusamy wrote the protocol, and is the lead author of the protocol and the review. He extracted data including the methodological
quality of the trials, performed the meta-analyses, and drafted the review.
K Samraj independently extracted data including the methodological quality of the trials and other data mentioned in the text.
D E C L A R A T I O N S O F I N T E R E S T
No potential conflict of interest.
I N D E X T E R M SMedical Subject Headings (MeSH)
Cholecystectomy, Laparoscopic [∗adverse effects]; Cholecystitis, Acute [∗surgery]; Randomized Controlled Trials as Topic; Time Factors
MeSH check words
Adult; Humans
63Early versus delayed laparoscopic cholecystectomy for acute cholecystitis (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
![Left Sided Laparoscopic Cholecystectomy: Case Report and ...open cholecystectomy - before laparoscopic era [2] and 1 case in 2008 [3] and about 50 cases of laparoscopic cholecystectomy](https://img.dokumen.tips/doc/110x75/5f6509906579645fd7227a11/left-sided-laparoscopic-cholecystectomy-case-report-and-open-cholecystectomy.jpg)