Embed Size (px)
Citation preview



WP/2008/DHP/04 English only Report series number: RS/2009/GE/76(FIJ)
REPORT
WORKSHOP ON THE FIRST INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESS COMPUTERIZED TRAINING (ICATT)
IN THE PACIFIC
Convened by:
WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR THE WESTERN PACIFIC
and
FIJI SCHOOL OF MEDICINE
Suva, Fiji
17–21 August 2009
Not for sale
Printed and distributed by:
World Health Organization Regional Office for the Western Pacific
Manila, Philippines
April 2010

NOTE
The views expressed in this report are those of the participants in the Workshop on the First Integrated Management of Childhood Illness Computerized Training (ICATT) in the Pacific and do not necessarily reflect the policies of the World Health Organization.
This report has been prepared by the World Health Organization Regional Office for the Western Pacific for the governments of Pacific island countries and for those who participated in the Workshop on the First Integrated Management of Childhood Illness Computerized Training (ICATT) in the Pacific, which was held in Fiji from 17 to 21 August 2009.

CONTENTS
Page
SUMMARY
1. INTRODUCTION................................................................................................................. 1
1.1 Background................................................................................................................... 1 1.2 Objectives ..................................................................................................................... 2 1.3 Participants......................................................................................................2
2. PROCEEDINGS ................................................................................................................... 2
2.1 Opening session............................................................................................................ 2 2.2 Introduction to the training ........................................................................................... 2 2.3 Installation and use of ICATT ...................................................................................... 3
3. CONCLUSIONS .................................................................................................................. 4
ANNEXES: ANNEX 1 - LIST OF PARTICIPANTS, TEMPORARY ADVISER, FACILITATORS AND SECRETARIAT
ANNEX 2 - COURSE SCHEDULE
ANNEX 3 - INTRODUCTION TO ICATT
ANNEX 4 - ICATT IN THE PACIFIC – PRESENTATION OF OBJECTIVES AND PROGRAMME SCHEDULE
ANNEX 5 - INSTRUCTIONS FOR THE USE OF ICATT
ANNEX 6 - REVIEW OF FIJI TRAINING MATERIALS FOR ICATT
ANNEX 7 - ICATT EARLY IMPLEMENTATION STEPS
ANNEX 8 - COUNTRY PLANS
ANNEX 9 - EVALUATION
ANNEX 10 - SCHEDULE FOR IMCI CLINICAL PRACTICE
Keywords:
Child health services / Disease management / Delivery of health care, Integrated / Teaching / Pacific islands

SUMMARY
The Integrated Management of Childhood Illness (IMCI) strategy was introduced in the Pacific in 2001. Fiji, Kiribati, Solomon Islands and Vanuatu were the first countries targeted for implementation. Fiji completed the initial adaptation of the generic 11-day course in 2001, after which training of health workers at the district level began. Kiribati, Solomon Islands and Vanuatu likewise completed their adaptations of IMCI clinical guidelines and conducted their first national courses between 2002 and 2004. IMCI was introduced and adapted in the Federated States of Micronesia in 2003.
In Fiji, IMCI was incorporated into the curricula of the Fiji School of Medicine and Fiji School of Nursing at an early stage, which provided undergraduate training to a wide range of students from all over the Pacific. The University of Papua New Guinea is in the process of introducing IMCI; however, it has had difficulty fully incorporating IMCI into its medical curriculum. The nursing schools in Papua New Guinea have been quite successful in incorporating IMCI, but the pace has been rather slow. In-service training across the Pacific has been expanded; however, many logistical difficulties were experienced, including keeping the materials continually updated.
In 2008, the Pacific was introduced to the IMCI Computerized Adaptation and Training Tool (ICATT) through the country participation of Fiji, Papua New Guinea and Solomon Islands in the Workshop on Integrated Management of Childhood Illness Computerized Adaptation and Training Tool. ICATT is an innovative computerized software application developed by WHO in collaboration with Novartis Foundation. It allows for easy adaptation of the most updated generic guidelines into national IMCI guidelines. Being computer-based, it has the potential to significantly increase training coverage in both in-service and pre-service settings. The ICATT training set includes: the contents of the 11-day course with the latest updates on assessment and treatment; new and improved audio-visual segments targeted to teach clinical signs and procedures such as counselling techniques; and a library of technical resources. The training set includes interactive exercises with immediate feedback to trainees.
Almost immediately after the ICATT orientation workshop, the Fiji School of Medicine updated the IMCI guidelines using ICATT and incorporated them into the curriculum. With the successful experience of using ICATT in the school, the WHO Regional Office for the Western Pacific and WHO Representative Office for the South Pacific, in close collaboration with Fiji School of Medicine, conducted the IMCI Computerized Training for selected Pacific island countries from 17 to 21 August 2009 at the Fiji School of Medicine, Suva, Fiji. The training was attended by 20 participants from eight countries (Fiji, Kiribati, the Federated States of Micronesia, Papua New Guinea, Samoa, Solomon Islands, Tonga and Vanuatu), representatives of the United Nations Children's Fund (UNICEF) from the Pacific and country offices, WHO resource persons, and an observer from the WHO Collaborating Centre in Australia, the Centre for International Child Health (CICH).
The overarching aim of the five-day workshop was to introduce and train participants in the use of the ICATT training set. At the same time, the training agenda was assessed for feasible adoption in other Pacific island countries. Throughout the training, participants provided valuable inputs, and efforts were made to facilitate the migration from traditional paper-based training to computerized training. Towards the end of the training, countries identified key steps for scaling up IMCI and ICATT implementation.

1. INTRODUCTION
1.1 Background
The Integrated Management of Childhood Illness (IMCI) strategy was introduced in the Pacific in 2001. Fiji, Kiribati, Solomon Islands and Vanuatu were the first countries targeted for implementation. Fiji completed IMCI adaptation in 2001, after which training of health workers at the district level began in 2002. Solomon Islands and Vanuatu completed their adaptations of IMCI clinical guidelines and conducted their first national courses. Kiribati explored further ways of introducing IMCI and two new countries. The Federated States of Micronesia and the Marshall Islands also proceeded to adapt IMCI. Over the next few years, from 2003 onwards, the generic 11-day model course was adapted to align with country needs. The modules are continually being refined. Several countries have had ‘roll-out’ programmes for in-service training. Expansion of the strategy has been challenged by many factors, including the logistical difficulty of having nurses released from their daily routine to attend the training workshops. Another constraint has been the dearth of clinical opportunities for participants to learn and recognize the signs required to satisfactorily complete the training. Furthermore, the knowledge and practice of IMCI may deteriorate over time if there is no mechanism for updating or refreshing the skills.
Experience with IMCI and pre-service training has been variable throughout the Pacific. Inclusion of the IMCI strategy into the Fiji School of Medicine curriculum was relatively easy because of the problem-based learning nature of the course. The Fiji School of Nursing followed suit shortly afterwards. However, some of the students do not like the training methodology, which includes a lot of reading. The University of Papua New Guinea has tried to introduce IMCI but has had difficulty incorporating it into the medical curriculum. The nursing schools in Papua New Guinea have been more successful in incorporating IMCI, but the pace has been rather slow.
In 2008, the Pacific was introduced to the IMCI Computerized Adaptation and Training Tool (ICATT) through the country participation of Fiji, Papua New Guinea and Solomon Islands in the Workshop on Integrated Management of Childhood Illness Computerized Adaptation and Training Tool, which was held in Seoul, Republic of Korea in June 2008. Almost immediately after the ICATT orientation workshop, the Fiji School of Medicine updated the IMCI guidelines using ICATT and incorporated them into the medical curriculum. Student feedback indicated that this computerized package was very easy to use, was interesting and gave clear guidelines on assessment, treatment and management. The audio-visual material reinforced the clinical skills taught and prepared them to recognize these signs when they saw patients in their clinical practice.
With the successful experience of using ICATT in the Fiji School of Medicine, a five-day workshop on IMCI Computerized Training was organized by the School in collaboration with Fiji Ministry of Health, WHO Representative Office for the South Pacific and WHO Regional Office at the Fiji School of Medicine, Suva from 17 to 21 August 2009. The training served to consolidate partnerships for ICATT implementation in the Pacific, as discussed during the 2008 ICATT workshop in Seoul.

- 2 -
1.2 Objectives
At the end of the workshop, the participants will have:
(1) used the IMCI Computerized Adaptation and Training Tool to acquire updated knowledge in standard case management of childhood illness through the
(2) demonstrated skills transfer through use of advanced technology combined with supervised clinical practice; and
(3) assessed the feasibility of expanding ICATT application in pre-service and in-service settings in the Pacific.
1.3 Participants
The training was attended by 20 participants from eight countries (Fiji, Kiribati, Federated States of Micronesia, Papua New Guinea, Samoa, Solomon Islands, Tonga and Vanuatu); representatives of the United Nations Children's Fund (UNICEF) from the Pacific and country offices, WHO resource persons, and an observer from the WHO Collaborating Centre in Australia, the Centre for International Child Health (CICH).
Most of the country participants were key IMCI facilitators, except for Samoa and Tonga, which were represented by paediatricians sent to further study IMCI adoption. Since one of the objectives was to assess the feasibility of using ICATT to complement the current IMCI strategy, it seemed prudent to invite countries to send participants who were trained in IMCI.
A list of participants is in Annex 1, and the agenda is in Annex 2.
2. PROCEEDINGS
2.1 Opening session
The opening session began with words of welcome by the course convenor, Dr Elizabeth Rodgers, Associate Professor. An address was then delivered by the Director of Family Health, Dr Josaia Samuela of the Ministry of Health of Fiji. He described the implementation of IMCI in Fiji and some of the challenges faced. Dr Marianna Trias, WHO Regional Adviser in Child and Adolescent Health, then delivered a message on behalf of the WHO Regional Director, Dr Shin Young-soo. He emphasized the importance of the training, this being the first of its kind in the Western Pacific Region. The training was then formally opened by the Dean of the Fiji School of Medicine, Professor Ian Rouse.
2.2 Introduction to the training
A presentation to introduce the computerized IMCI training tool was delivered by Dr Emmalita Mañalac, WHO Medical Officer, who gave an overview of IMCI and ICATT (Annex 3). The objectives of the training, together with the programme schedule, were then presented to the participants by Dr Rodgers (Annex 4).
- 3 -
2.3 Installation and use of ICATT
Most of the participants arrived in Fiji the evening before the workshop. While some had had the opportunity to install and use the ICATT programme before their arrival, many had difficulty using it without support. A lot of time was spent on the installation of the training set and attention was drawn to potential programme conflicts and how to overcome them. Guidelines on how to install and use the ICATT training set is shown in Annex 5. Eventually, all of the participants were able to install and use the training set.
The session consisted of two components:
(1) completion of the ICATT programme; and
(2) clinical practice component.
All participants were asked to complete both components and to provide feedback to help develop a model course using the IMCI computerized training set. Following the completion of these tasks, candidates held discussions on what would be feasible in their own settings and developed future plans for implementation in their home countries. An overview of the proceedings is further expounded below.
2.3.1 Work on the computers
Some technical difficulties encountered were associated with saving and transferring personal profiles. Many participants lost the tracking profile and had to restart a number of times. Participants who had personal laptops did not have this difficulty as their profiles were saved on their document folders. Time was perhaps the biggest constraint. Participants spent many evenings and long hours in the computer lab completing the training set. On average, it took at least three full working days to complete the training set from start to finish.
Some technical or technological inconsistencies were noted in parts of the training materials. These were recorded and collated for future revision of the training set (Annex 6). Some of the inconsistencies were found in the generic set and some in the adapted Fiji version. For example, participants spent a lot of time trying to achieve "green" bars in the test (80% correct responses) but consistently received "red" bars instead. It was unclear whether the constant "red" scores were due to a technical problem or a point that was missed.
The first day was devoted to finishing the module "Assess and classify the sick child age module on two months up to five years" in order to be prepared for the clinical session scheduled for the following morning. Many participants stayed at the computer laboratory until the institution closed (21:30 hours) or worked on their personal laptops till late at night.
2.3.2 Clinical practice sessions
Clinical practice sessions were held in three locations: Valelevu Health Centre, Makoi Health Centre and Colonial War Memorial Hospital. The sessions began with a demonstration of the assessment and classification of a sick child, followed by clinical practice by the participants. As all the participants were either IMCI facilitators or paediatricians, no difficulty was encountered. The number of patients seen over three days was small but sufficient. The types of pathology were wide and varied, providing a good opportunity for participants to refresh their skills. In-patients, including young infants and newborns in the maternity unit, were also seen to demonstrate clinical signs.

- 4 -
2.3.3 Feedback on programme
Question-and-answer sessions were formally conducted on the first day, but the use of the training set provided great opportunity for interaction. Toward the end of the training, participants were assisting each other not only with technical challenges but also with problems in the training set. Several fruitful discussions were held among the participants on the content of the modules. This interaction allowed different levels of health care personnel to share their expertise. This was an added bonus to the training. Formal feedback on the improvements needed is presented as a working document in Annex 6.
2.3.4 Country plans
One of the objectives of the training was to assess the feasibility of using the ICATT training set in the Pacific and how this might be achieved if found useful. A presentation on Early Implementation Steps was given as a guide to this session (Annex 7). Furthermore, staff from the WHO Regional Office presented technical updates on community IMCI, referral care, programme management and new monitoring and evaluation tools to facilitate the development of the country plans in the overall context of child health and survival. Participants were unanimous in accepting the relevance of community IMCI at the same time when facility-leased trainings are enhanced through ICATT. The individual country plans were very realistic and are collated in Annex 8.
2.3.5 Evaluation
A generic evaluation form for participants was used to evaluate the use of the ICATT training set. The responses were variable depending on the computer literacy level of the participants. Most found this method of teaching very useful, but there were many hitches in the technicalities of the programme. The collated responses are found in Annex 9.
3. CONCLUSIONS
(1) This was the first IMCI computerized training workshop in the Western Pacific Region. All participants except one had no experience with or knowledge of this computerized programme until the planning for this training. Therefore, this workshop was a very good opportunity to introduce the ICATT programme and to test the five-day training agenda in the Pacific. While there were some technical and technological challenges during the workshop, these were overcome with assistance. The agenda was rather fluid and flexible and allowed participants to work at their pace.
(2) The assembly of more than 20 IMCI facilitators provided an opportunity for feedback and further improvement of the chart booklet and ICATT training set. The feedback also pointed out where and how the IMCI computerized programme could be used more effectively. Some additional time may be needed to complete the training set. In general, ICATT was regarded by all countries as an option for further improvement of IMCI training in both in-service and pre-service settings. Various approaches for in-service training were considered. In places where the environment is not favourable for ICATT-based training (i.e. poor logistical support, no electricity, low level of computer literacy), the conventional 11-day course could still be conducted.

- 5 -
(3) It was jointly agreed that the first step in scaling up IMCI implementation would be to review and finalize the national guidelines to include the latest updates. The Fiji IMCI algorithm could serve as a model for many countries in the Pacific once the necessary revisions are made, as per discussions during the training course. However, countries with a high prevalence for malaria (Papua New Guinea, Solomon Islands and Vanuatu) would need to update their algorithms according to the new methods for malaria diagnosis and treatment.

Participant List
Federated States of Micronesia
Dr Anamaria Akapito Yomai Paediatrician/MCH Physician PO box 82, Weno, Chuuk Federated State of Micronesia 6942 (691) 330 5809 [email protected] [email protected]
Fiji
Avinesh Kumar Staff Nurse Valelevu Health Centre Nasinu (679) 9317698 [email protected]
Dr Dennis G. Buenafe Senior Registrar ‐ Paeditrician Labasa Hospital PO Box 577 Labasa (679) 8811444 / (679) 9973515 [email protected]
Filomena Tawake Dokoni Tutor/Actg PHC Strand Coordinator Fiji School of Nursing Tamavua, Suva (679) 9683310 [email protected]
Sr Haemarie Taito Acting Head of School TISI Sangam School of Nursing PO Box 2047 Labasa (679) 8818691 ext: 201 (679) 7171226 [email protected]

Litia Ruban Senior Tutor – Sister Fiji School of Nursing Tamavua, Suva (679) 3321499 (wk) [email protected]
Pradeep Kuar Singh Special Clinic, CHOPD Childrens Outpatients Dept CWMH, Suva (679) 3600520 (679) 9416020 [email protected]
Kiribati
Dr Teatao Tiira Medical Officer Tungaru Central Hospital Nawerewere, Tarawa Kiribati (686) 28100 [email protected]
Mrs Tereba Abere Prinicipal Nursing Officer PO Box 268 NHMS, Nawerewere, Tarawa Kiribati (686) 28268/28874 [email protected]
Dr Turia Tekaai Registrar Paediatrician Tungaru Central Hospital Nawerewere, Tarawa Kiribati (686) 28100 [email protected]

Papua New Guinea
Dr Kenneth Gilchrist Oswyn Paeditrician Alotau General Hospital Milne Bay Province PNG (675) 6411200 (Hosp) (675) 6512160 (m) (Fax) 675 6410040
Dr Paulus Ripa Senior Lecturer‐Medical School School of Medicine & Health Sciences PO Box 5623, Boroko, PNG University of PNG (675) 311 2292 [email protected]
Samoa
Dr Farah Marumatakimanu Head of Paediatric Department National Health Services PO Box 3071, Apia, Samoa Apia, Samoa (685) 759 2029 (685) 21212 (Fax) 685 22905 [email protected]

Solomon Islands
Dr Divinal Ogaoga Medical Officer/ Child Health Ministry of Health PO Box 349 Solomon Islands (677) 7496343 [email protected]
Mr Mathias Tamou IMCI National Progam Officer Reproductive & Child Health Division MHMS, Honiara Solomon Islands (677) 28169 [email protected]
Mrs Versilyn Isom Facilitator/Head of School School of Nursing PO Box R113, SICHE, Honiara (677) 38428 Fax (677) 30390 [email protected]
Tonga
Dr Siaosi Aho Paediatrician Vaiola Hospital PO Box 1071, Nuku'alofa, Tonga Nukualofa, Tonga (676) 23200 (676) 7761026 [email protected]

Vanuatu
Ms Andorin Aki ENT Nurse Incharge ENT Clinic Vila Central Hospita PMB 013, Port Vila Vanuatu (678) 22100 ext: 33 [email protected] Mr John Tasserei Diabetes Coordinator Public Health Department Ministry of Health PMB 9009, Port Vila, Vanuatu (678) 22512 / (678) 5493558 [email protected]
Ms Marie Woleg IMCI Coordinator Directorrate of Health Department of Public Health Ministry of Health PMB 9009, Port Vila, Vanuatu (678)22512 [email protected]
UNICEF
Dr Ingrid Hilman Child Survival Specialist UNICEF Pacific (679) 9206722 [email protected] Tinai Iuta Health & Nutrition Field Officer UNICEF Office Teaoraereke, Tarawa Kiribati (686) 22904 ext: 113 [email protected]

WHO
Dr Amy Gray Paediatrician/Research Fellow Centre for Int'l Child Health Dept of Paediatrics / University of Melbourne Royal Childrens Hospital Parkville 3052, Australia (61) 439979108 [email protected]
Emmalita M. Manalac Medical Officer World Health Organisation ; WPRO PO Box 2932 United Nations Avenue; 1000 Manila, Philippines (63) 2528 9868 (Direct)/ (63) 2528 8001 (General) (Fax) (63) 526 0279 [email protected]
Dr Marianna V. Trias Regional Adviser Child and Adolescent Health World Health Organisation , Western Pacific Regional Office PO Box 2932 United Nations Avenue; 1000 Manila, Philippines (63) 2528 9868 (Direct)/ (63) 2528 8001 (General) (Fax) (63) 2521 1036 [email protected]
Wang Xiaojun EPZ Technical Officer World Health Organisation PO Box 113, Suva (679) 323 4113 [email protected]

Course Facilitators
Dr Lisi Tikoduadua Consultant ‐ Paediatrician Paedatric Department CWMH, Suva (679) 3313444 [email protected]
Dr Rigamoto Seforsa Taito Consultant ‐ Paediatrician Lautoka Hospital (679) 6660399 (679) 9935546 [email protected] [email protected]
Course Convenor
Dr Elizabeth Rodgers Associate Prof. Paediatrics Head of Department ‐ DMS Fiji School of Medicine Private Mail Bag Suva (679) 3233515 / (679) 9268659 [email protected]

IMCI Computerized Training in the Pacific
17‐21 August, 2009
Course Schedule
Pre‐workshop Day 1 Day 2 Day 3 Day 4 Day 5 8am Registration Transportation to Training Sites 8.30 to 9.30 Opening 9.30 to 10.00 Morning Tea 10.00 to 1 pm Brief introduction
into ICATT and the rationale (WPRO); Objectives of the course and review of schedule (Course director)
Assess and Classify – Outpatients clinical section; Inpatient – for danger signs
Identify Treatment and Counselling Outpatients clinical session
Sick young infant – inpatient ( 2 hours) Full assessment to follow‐up of 2 months to 5 years – Outpatient clinical session;
Contd Group work on future plans for ICATT introduction Presentation of Country Plans
1pm to 2pm LUNCH 2pm to 3.00pm Assess and classify
the sick child ‐danger signs; cough
Q & A – clarify issues, feedback on activity
Q & A – clarify issues, feedback on activity
Q & A – clarifying remaining issues
Conclusions/ Recommendations Course Evaluation
3.00 to 3.30pm Afternoon Tea 3.30 to 5:00pm Continue assess and
classify diarrhoea, fever, ear problem
Identify treatment, counselling , follow‐up
Continue with unfinished business with computer work
Group work on future plans for
ICATT introduction
Closing ceremony
5:00 pm onwards
Day after arrival ‐ Work on ICATT
Training Set if not already completed.
Time for participants to review exercises (optional) facilitators meeting


Introduction to IMCI Computerized Adaptation and Training Tool (ICATT)
EMMALITA M. MAÑALAC MD MPHMedical Officer for Child Health
World Health OrganizationWestern Pacific Regional Office
Child and Adolescent Health Child and Adolescent Health
Mandate for IMCI …
WHO/UNICEF Regional Child Survival Strategy
Endorsed at the WHO Regional Committee meeting in September 2005
Child and Adolescent Health
WHO/UNICEF Regional Child Survival Strategy - Goal
To reduce inequities in child survival and achieve national targets for MDG4 by accelerating and sustaining actions to reduce childhood mortality
Child and Adolescent Health
Objectives
To improve access to and utilization of the essential package for child survival particularly in areas of greatest need;
To provide an enabling environment for child survival where political will, financial and human resources match the burden of disease
Child and Adolescent Health
Essential Package for Child Survival
Skilled attendance during pregnancy, delivery and immediate postpartumNewborn careBreastfeeding and complementary feeding
Micronutrient supplementationImmunization of mothers and childrenIMCIUse of insecticide treated nets in endemic areas
Child and Adolescent Health
IMCI Implementation in the Pacific
IMCI has been slowly expanding in the Pacific since it was introduced in the early 2000’sOf the 14 WPR countries implementing IMCI, seven are PICs at various stages of IMCI development

Child and Adolescent Health
IMCI Implementation in the Pacific
Fiji implements in all of its 4 administrative regions; the others in < 50% of districts;Difficult to maintain 60% training coverage of HW at 1st level care;Varied experience in financing of IMCI activities including training;Pre-service training has been started in Fiji and PNG.
Child and Adolescent Health
Barriers to Scaling up IMCI
High cost of trainingInavailability of facilitatorsQuick turnover of trained health workersLack of supportive supervisionSlow adaptation/dissemination of updated guidelines
Child and Adolescent Health
Global consultation on IMCI training approaches (2007)
Skills of trained health workers trained in an 11 day course vs 6 day course were comparable (Zambia)No significant difference in care given by doctors trained in 11 day course vs 8 days (Kosovo)Training by any format should focus on a measurable set of core competencies
Child and Adolescent Health
IMCI core competencies
General – how to use the IMCI chartKnow and recognize danger signsAssess/classify/treat/counsel on main symptomsCare of the young infantIdentify/treat/counsel on malnutrition and anemiaAssess need for immunization
Child and Adolescent Health
Experts meeting in Ethiopia (2008) – new options
Skills stationsCase booksClinical mentoringNew and improved audio visualsComputer based training (ICATT)
Child and Adolescent Health

Child and Adolescent Health
ICATT - definition
It is a computerized software application that allows easy adaptation of IMCI guidelines at country levelIt is also a training tool that can be used for individual or group learning
Child and Adolescent Health
ICATT key components
Chart booklet builder – permits easy adaptation and local update of WHO clinical guidelinesLibrary – includes reference and educational materials on IMCI and related child health issues developed by WHO and other international agenciesTraining set- that contains the generic training course that could be adapted to suit local needs
Child and Adolescent Health
ICATT “open” interface
It is intended for IMCI programme managers to allow for easy adaptation of generic IMCI guidelines into national/subnational guidelines;To update the library of documents and other resources;To design training programme
Child and Adolescent Health
ICATT “closed” interface
It is a training aid for individual or group learning; Can be used as a distance internet based course; on the job training; refresher course;Useful for both pre-service and in-service training
Child and Adolescent Health
ICATT based training
It will never completely eliminate human instructors and other forms of IMCI learning (modular based);Does not rely on computers alone, it has to be supported by clinical practice;
Child and Adolescent Health
Distinct advantages over traditional IMCI methods
ICATT is self pacing for slow or quick learners and reduces stress and even increases satisfaction;Expert knowledge is immediately available;Reduced cost for training

Child and Adolescent Health
ICATT implementation in Western Pacific Region
Workshop in Seoul ROK, 2008Fiji: adaptation of national guidelines & introduction in pre-service, 2008PHL: natl adaptation and first training September 2009CAM: Khmer version of ICATTLao ,MOG: early stages of adaptingVTN: soon on board
Child and Adolescent Health
ICATT is NOW in the Pacific!
This experience is a milestone in IMCI history in WPR and the world;Model for IMCI in-service training using an internet based method;Hopefully it will address the barriers to scaling up IMCI;Raise the bar in IMCI implementation in the Pacific!

IMCI Computerized Training in the Pacific
Objectives
Objectives of Workshop
• Use ICATT to acquire updated knowledge in standard case mge of childhood illness
• Demonstrate skills transfer through use of computer technology combined with supervised clinical practice
• Assess feasibility of expanding ICATT application in the pre‐service and in‐service settings.
Schedule
• 2 components to the completion of the course– Completion of the ICATT program
– Clinical practice
• Since nearly all are IMCI trained/facilitators –discussions on what would be feasible in your own countries.
• Future plans
Program
• installation and use of ICATT
• Completion of the modules – new updates and inclusions
• Clinical practice ‐ ?assess time needed to teach clinical skills for IMCI
• Discussions on activities to look at feasibility and transportability of ICATT to the countries.
Program Contd
• Look at possible plans for future using a ICATT course instead of the 11 day model course in situations where computers are available.

Instructions for the Use of ICATT
To install your ICATT package, open the folder – Fiji Training set final.
Click on the colourful icon – and you should get this.
Then install. If this does not happen, click on SETUP first – your computer may not have all the components to run the program. It should then install after following the on-screen instructions. If it still does NOT install, you may have Adobe Acrobat Reader 9 in your computer. Remove that program then try again (you can re-install Adobe Reader 9 again later

Once installed, on you computer desktop you will see something like this
Click on the jig-saw puzzle – Fiji IMCI training Course or something like that. You will get this.
Then click on new student profile - enter your details and click on save profile then click on start training.

You will get this
Click on Introduction and complete that section
After this go to the section on “Care of young Child aged up to 2 months. See below.

After this then go to the “Care of child aged 2 months to 5 years” When you have completed all the modules, you can print a certificate if you have passed all the modules. You can stop at any time BUT when you have finished for that session, save your profile
And transfer profile to a flash drive by clicking on the transfer profile icon

You can now trasfer onto your flash drive. NOW delete the profile on the program AFTER you have ejected your flash disk. The next time you wish to start, insert you flash drive with your saved profile and Go through the same process but click on the “load a student profile from file” from the flash drive. When you finish and after you save your profile you do not transfer or delete file. Good Luck.

1
REVIEW OF FIJI TRAINING MATERIALS FOR ICATT 1. Sections needing review for corrections: Chart booklet OPV vaccinations do not line up with correct ages Computer sections: child 2 months to 5 years Part 1: Assess and classify Assess other problems: Practise section: exercise 6
- Malnutrition: The question asks to classify a “9 month old child weighing 7 kg”. On a girls chart; not low weight, on boys chart this child is low weight. Change the question to “9 month old girl…” IMCI chart included with exercise is a girl’s chart.
Sore throat: test section: the answers include acute viral pharyngitis which is not a classification in the chart booklet. Remove option. Skin problem: the IMCI charts attached to the section are for ear problem. Change to the correct charts. Do not include general data in exercises.; Part 2: Identify treatment Practise exercise:
- Exercise 2 and 5. Both children in the cases are more than one year old and will be treated and go home. In the case information neither has had OPV. But in the answers there is no indication that they need this vaccine. Has the OPV been missed from the case information OR is there a genuine reason why neither child should have OPV today? There is no information in the course reading to suggest a genuine reason for omitting OPV if the child is well enough to go home.
- Exercise 3: What is the treatment for dysentery: Booklet says cotrimoxazole. Answer says ciprofloxacin.
Part 3 Select and give oral drug Practise section: Exercise 6
- Jason, Jill and Joshua case studies: have wrong iron dose in answers, should be 10mL (not 2mL)
- Jill is to have treatment with mebendazole: 500mg once is not offered as an option in the exercise. The answer is 100mg bd 3 days which is not a dosing that is included in the booklet. Change the answer to mebendazole 500mg once.
“Teach the mother” to give the drug Practise section: Exercise 2
- Amoxycillin 3 times a day is the answer to how often the drug should be given. This does not correlate with the information in the doses in the booklet and is

2
different to the answer in Exercise 1 of the same section which says amoxicillin should be given 2 times a day. Make doses consistent in booklet and answers.
Communication skills Test section:
- Case 1: The child is only having food 3 times a day. The recommendation for a child of this age is to have food 5 times a day BUT the answer “Child should have more feeds in a day” is wrong. Is there a particular reason?
Computer sections: young infant to 2 months Part 2: Assess and classify Check immunisation Practise section: exercise 3
- For a 6 week old child who needs urgent referral: What immunizations are NEEDED today? The answer should be none OR change the question to “what immunizations is this child due to have? The next questions asks: should this child have immunizations today? The answer: no
Part 3: Identify treatment Practise section: Case study Henri
- Ampicillin dose: states that a 250mg vial is used (with no volume specified) and you cannot compare this with the dose schedule in the booklet which refers to a 500mg vial in a certain volume. Regardless, the answers seem wrong.
- In the same section the gentamicin dose is also wrong in the answers. Test section: Case study Sashie:
- Questions about antibiotic frequency and duration both ask about giving cotrimoxazole while this is not recommended in the age group and the first part of the case study identifies the correct treatment as flucloxacillin. Change questions about antibiotic frequency and duration to ask about flucloxacillin.

3
2. Sections needing review due to participants having difficulty with completion: Child 2 months to 5 years Part 1: Assess and classify Assess diarrhoea: test: Case 3 and 4
- Many candidates did not realize they have to include both classifications relevant to the patient, eg: some dehydration AND severe persistent diarrhoea, since to have severe persistent diarrhea the patient MUST have some dehydration. Either both answers should not be required OR the question should be changed to: Select ALL classifications that the patient satisfies.
Part 3: Treat the child “Give extra fluid for diarrhoea” Practise section: Exercise 2
- Amount of ORS: the answers given are different ranges to what appear in the chart booklet
Test section: - The answers assume that if a weight is given the amount of ORS should be
calculated but if it is not given then a number within the right range of fluid can be given. This assumes that everyone using the system is comfortable with calculation – in actual fact it may be safer for low level health workers to use a number in a range rather than make a calculation error. The answers should be changed to allow for any number in the appropriate range.
“Identify treatment for child” Test section: exercise: need for urgent referral
- This section is somewhat cumbersome to complete. Many candidates struggled to complete this section correctly even after reading the materials carefully. If people may be expected to complete computer training at home or before attending a course a section such as this would lead to frustrations. The problem seems to be that it requires very specific answers to pass the section but those answers aren’t necessarily what you would think after reading the information and completing the practice section. For example: the child with severe dehydration and severe malnutrition only receives the urgent treatment for dehydration before referral.

4
3. Issues regarding algorithms and adaptation Fever Malaria 1. Not all exercises specify malaria risk in order to allow participants to classify correctly. 2. The inclusion of malaria risk in the Fiji algorithm makes it unnecessarily complicated given that there is no risk of malaria unless a person has travelled to or is from a high risk country in the region. It was suggested that the only the no-risk portion of the algorithm could be used, at least if Fiji. To include children who have travelled to a malaria area, the algorithm could include something similar to the following: Any general sign OR Stiff neck OR ADD: If travel to malaria area in the last one month
Very severe febrile disease Usual treatment plus ADD: If recent travel give first dose of anti-malarial
The reasoning for this would be that since malaria is uncommon it may be best to treat or diagnose these children at a health facility familiar with the diagnosis and treatment. Another suggestion was that to include the same qualification “If travel to malaria area in the last one month” in the yellow section of the chart as well. The question was raised: If the Fiji algorithm is to be the starting point for a regional algorithm should there be a plan about what to include in countries with a risk of malaria?
- The high risk, low risk algorithm/a combination/something different? - Should there be some agreement about what is taught if students from these
countries come to Fiji to train?
Fever, possible bacterial infection Issues relating to the classification of fever also arose from the classification: “fever, possible bacterial infection”. In clinical sessions, course participants classified patients with impetigo or ear infection as “fever, bacterial cause unlikely” due to order of the algorithm. However although the classification of these children should have been different, the treatment they received was no different as it was addressed in other sections of the algorithm. Different solutions were proposed:
1. Moving the sore throat, ear and skin problems to before fever. Not preferred as fever would generally be a more important symptom to address first.
2. Ignoring this problem as the treatment for children would not be any different and any changes may make the algorithm more complicated.

5
Sore throat Representatives from other Pacific countries felt that their country algorithm would treat any child with an exudate as streptococcal sore throat, regardless of the presence of lymph nodes. This would have to be decided on a country to country basis. Skin problem 1. In the computer reading the question is “Does the child have pain related to the skin problem?’ In the booklet the question is “Does the child have pain from the skin problem?” These questions should be consistent, using whichever question is easier to understand. In the section on looking and feeling for a skin problem it was though that it might be better to write “Look for localised warm, painful swelling or redness”, rather than tender, to keep the terms consistent in this section. In the classify section the format should be kept the same with bullet points. For example the last box contains sentences but can be changed to “No signs OR insufficient signs for above classifications” 2. In the treatment section of the algorithm for abscess and impetigo it includes “refer to hospital”, but does not refer to the need for incision and drainage or suggest which conditions might need incision and drainage. This should be clarified? Malnutrition 1. Growth faltering is included for the purpose of classification in the algorithm. This should be determined from three consecutive visits and does not apply to acute visits.
- Should this be included in the algorithm to classify during the acute visit? - If not included for acute classification there should be reference to what
needs to done if detected so it is appropriately acted upon?
2. MUAC is discussed in the reading material but not used in the chart booklet. The purpose of training should be how to use the chart booklet. If MUAC is not going to be used this be included as additional reading, rather than core material? Some concerns raised regarding impact of including recommendations to dilute cow’s milk as an alternative feed. What is the potential impact? Ear infection: Inclusion of pain AND fever for diagnosis? Young infant Consider revising to include treatment of eyes given the prevalence of eye infections: eg tetracycline ointment post-partum and Vitamin A for mother.

ICATT – early implementation steps
Using ICATT at country level
Prerequisites for early ICATT country use
• IMCI strategy is adopted for use in a country• Strong national or sub national adaptation team• Clear decision on and experience with training needs
and approaches for IMCI clinical training• Strong leadership of a good training institution
Experience with training programmes for first level health workersGood links with first level clinics and front line health workersExperience in monitoring and evaluation of training outcomesInterest in use of innovative training approaches
Key ICATT early implementation steps (1)
1. Ensure availability of nationally adapted IMCI guidelines, whichreflect local priorities, realities and needs
2. Careful decision and agreement about most appropriate training approaches to be used:a. Group teaching vs. individual learning or combination of
bothb. Length of training and amount of learning materialsc. Balance between theoretical and clinical trainingd. Training schedule (uninterrupted course, several training
sessions or another approach) e. Role and functions of facilitatorsf. How monitoring and evaluation of training results will be
done
Key ICATT early implementation steps (2)
3. Review of materials included into ICATT – library, training set and identification of the local materials (reference document, illustrations, videos etc) which may be inserted into the tool
4. Ensuring availability of hard copies of national adapted IMCI clinical guidelines (chartbooklet) and clear structure of the training course, as well as electronic version of identified courses for inclusion into ICATT
5. Available expertise to work with OPEN interface of ICATTa. Making appropriate changes in IMCI bookletb. Updating/changing Library component of the toolc. Adaptation of the training materials included into ICATT according
to the local training needs and designd. Review of coherence of all changes made in the toole. Production of CLOSED version
Key ICATT early implementation steps (3)
6. Selection and training of the facilitators according to the training approach(s) chosen, including clinical component
7. Decision on ways and means of monitoring and evaluation of training performance and quality
8. Initial training of health care providers
9. Evaluation and summary of lessons learned, feedback on ICATT

Annex 8
1
Country Plans
Fiji Islands
IN‐SERVICE TRAINING – to begin January 2010
• Update IMCI Training Set and Modules
“Suggested to Modify IMCI Training set accordingly to the training level required
Make IMCI computerized Training Course to a 6‐day course
• adaptation suited for Fiji Islands
• Facilitator’s training – national level ‐ for 2010 in Suva. Participants from Central, Western, and Northern division
• “Update the present IMCI trained health personnel registration – to monitor, evaluate, and update them about ICATT.”
Plans for Implementation
• Participants to complete IMCI computerized training set on Assess and Classify prior to training
• Do a 6‐day Training o D1‐recap on Assess and Classify (go to the wall, drills, and role play) with participants and
proceed to clinical training.D1‐Identify Treatment o D2‐Treat the Child then go to Clinical training o D3‐ Recap up to Treat The child 2mos‐ 5years of age. Proceed to clinical practice and start
Counsel the Mother. o Day 4‐Recap of Counsel the Mother and may proceed to clinical practice. Start Follow‐up.
o Day 5‐Recap Follow up and Assess, classify, treat, counsel and follow‐up young infants and may proceed to clinical practice. Proceed to all clinical practice!
o Day 6‐Do clinical practice in NICU, children’s ward, and maternity unit! Evaluation and assessment of the program.
Planning
PRE‐ BASIC SERVICE TRAINING
• include ICATT in the curriculum of the following school:
• FSN, FSMed (already done) , TISI Sangam Nursing School • “Train more Nursing staff and tutors in the future!”

Annex 8
2
POST BASIC SERVICE TRAINING
• nurse practitioner – 20 participants september 2009
• post basic public health‐ >20 participants nov.2009
• midwifery
ICATT PLANNING‐ Fiji Islands August 2009
Activities When to start When to complete Budget Responsible Person
1.Correct and modify IMCI Training Set for FIJI adaptation now
before Jan.2010 FIJI IMCI committee
2.In‐Service Clinical Training‐ NP and PH Sept‐Nov 2009
End of Nov 2009 Dr. Lisi/Sr Ruban
3.Post‐Basic Service Training‐Midw/PH/NP Jan.2010 Nov.2010 Dr. Lisi/Sr Ruban Sr.Haemarie 4.Pre‐Service Training‐FSMed,FSN,SSN(LA) Jan.2010 Dec.2010 Dr.Rodgers/Sr.Filo/Sr.Hae5. In‐Service‐ National Facilitator's training (3 per Division)) Apr.2010 Ju 2010
FIJI IMCI com./WHO/Unicef
6.CIMCI ‐ Divisional level Sep.2010 Nov.2010 FIJI IMCI com./WHO/Unicef

Annex 8
3
Kiribati
Annual work plan 4th Quater 09 1st Quater 2010 Oct Nov Dec Jan Feb Mar Introduction to SMC Printing of updated IMCI chart modules/Training of IMCI facilitators Distribution of the new version IMCI chart booklet Update of all health workers on South Tarawa update health workers on the outer islands Training of remaining non IMCI nurses Use updated version and ICATT nation wide Systematic Monitoring /Evaluation of updated IMCI and ICATT
Yearly for the 5 years
Training of MA students Training of Doctors Intergrate the ICATT into the nursing curriculum
Kiribati will use the Fijian Version
we need funding assistance for the training
We will use the roll out training
5 days training will be applicable
For consultation, training and printing and equipment ask UNICEF/WHO for Funding
Training of Nurses on outer island ‐ Funding ‐KIRI‐EU, GOK
Evaluation ‐ TA for consultation ask from WHO and UNICEF

Annex 8
4
Papua New Guinea
Current Situation.
A. Resources.
• Standard Treatment Book for Children. 8th edition 2005. Being reviewed for 9th edition 2010.
• Child Health Record Books. Updated Vaccines, IMCI dangers signs, WFA.
• Two Flip charts. 1. 8 step check list Young Infant 0‐2m. 2. 10 step check list.
Paediatric Society of PNG.
• Involvement and support of : NDoH, W.H.O, Clinton Foundation, Provincial Govts, Churches, NGOs, Institutions.
• In‐services: Trainings done nationwide, supervision weak, system support‐ongoing problems,
• Pre‐service: Universities‐ aware, practiced; Colleges (HEO, School s of Nursing and Community Health Workers (Nurse Aids), 4‐5 graduates. Not reviewed
• CIMCI plans: some attempt, but not agreed upon for roll‐out.
B. Review being done. June‐Sept 2009.
1. Step pneumonia (2), Diarrhea (3), Fever (4), Weight (8), Feeding (9), Immunization (10), HIV (11). Young Infant: HIV (9), other steps
2. Pre‐referral drugs and doses. 3. Counseling. 4. Bind together, hard copy. 5. Video local adaptation; first step done, Further work? 6. Standard Treatment Book 9th edition. Recognizes IMCI. ?Sustenance.
C. ICAT T Adaptation.
• Update Flip chart (as above in reviews). ‐ Focus Group. Dr Oswyn (IMCI Focus person), Dr Rehlis (WHO), Dr Mokela (Chief Pediatrician), Dr Kiromat (National Facilitator), Dr Hwaiwhanje (Malaria), Dr Ripa (UPNG)
‐ Time frame: Up to December 2010.
• Review Final Draft Mid‐ year Meeting 2010 by Pediatric Society.
• ICAT adaptation. By first quarter 2010 ‐ Need for IT expert support (Contract with support from W.H.O PNG). ‐ Include other training aids and clinical training suggestion.

Annex 8
5
‐ Produce PNG version ICAT. ‐ Schedule: ? 5‐7 days.
• ICATT Training. By June 2010 ‐ TOT In‐service: Venue at Divine Word Univ. or UPNG.
D. Produce New IMCI Updated Version. For Health Workers in PNG. E. Re‐train on New IMCI updates.
‐ TOT Pre‐service School of Nursing and Nurse Aids (CHW), Divine Word University, UPNG, Pacific Adventist Univ., University of Goroka. Venue; Divine Word Univ.

Annex 8
6
Solomon Islands
Plan 2009/2010
Time Line Activity No Activity Resource Input Output Q1 Q2 Q3 Q4
1_2009 Child Health Committee endosrement Tea Edorsement ##
2_2009 Advocacy & Executive endorsment (ICATT) Tea Endorsement ##
3_2009
Review and update Module adaptation (10 day training material)
Tea ‐ 10 personsX$20X5 STC
Modules adapted
4_2009 Adaptation of ICATT (consider Fiji version)
Tea ‐ 10 personsX$20X5 STC ICATT adapted
5_2010 Printing 10 day training materials 6_2010 Printing ICATT materials
7_2010 Training ICATT (IMCI facilitators) Workshop cost 10 facilitators trained
8_2010 Training ICATT introduced to 2 SON Materials 100% student trained
9_2010 Evaluate ICATT training Workshop cost 10_2010 Strengthening of ICC Meeting cost
11_2010
Assess current community health activities by stakeholders (survey ‐ mapping)
Survey cost (contract)
12_2010
Stakeholders meeting on community IMCI
Meeting cost Stationary Venue
13_2010
Stakeholders plan on community IMCI
Meeting cost Stationary Venue
14_2010 Pilot community IMCI (2 sites)
15_2010
Capacity building in CH program planning and management ‐ module base
16_2010 M&E (to be further discussed)

Annex 8
7
Funding Sources ‐ SIG; UNICEF; WHO and other
Trination ‐ FSM, Samoa, Tonga
ICATT Country Introduction‐.
Rational or Justification
1. Tool to update knowledge in standard case management of childhood illnesses 2. Its more holistic and comprehensive 3. To replace ARI and CDD training 4. Strengthen pursuance of MDG4
Work Plan
1. Consultation process –Health Planning /Public Health –CMO/SPHN /senior doctor/nurse OPD/Head of school of nursing/Paediatricians/Obstetricians/GPs
2. Establish National ICATT Working group to coordinate ICATT [core team out of the above]‐need to appoint an ICATT coordinator. It may be a similar body already exists.
3. Adopt IMCI strategy‐link to existing Health Ministry strategic plan 4. Adapt Fiji version of ICATT to meet local requirements‐will be costly and time consuming 5. Initial implementation focus would be on in‐service training to improve skills of health workers. 6. Pre‐service IMCI training to be integrated to Nursing school/health assistant training/ medical
school curriculum at a later stage.
TOR National ICATT working group
1. Adapt ICATT to local requirements 2. Strike proper balance between theoretical and clinical training 3. Determine target trainees and number to train‐include selection criteria 4. Decide on merits of group vs individual learning‐likely peripheral training would be done as a
group 5. Agree on likely 5 days training duration rather than 11‐additional time may be needed to
enhance computer literacy 6. Assess current training/practices/stock availability/referral process
Adaptation – to include
1. Deleting Malaria section 2. Not using vitamin A and consider Zinc depending on availability of supply 3. Strep throat diagnosis –changed to exudates plus or minus lymph node enlargement 4. Acute ear infection classification– as is but to have ear pain + fever 5. Some parts of our trination‐ no oral meds for young infants

Annex 8
8
Resources
1. 1 or 2 external facilitator +/‐ facilitator training first 2. Computer lab or similar 3. Training materials/IT 4. Per diems/travelling expenses/accommodation etc 5. Monitoring and evaluation
In‐service trainees .‐ to consider
1. Health officers/ Public Health nurses/Outpatient doctors and nurses/district hospital doctors and nurses/ paediatric nurses /nurse midwives/GPs etc
Vanuatu
No Of
Activities
Activities to be implemented
Person
Responsible
Time Frame
1
• Adaptation Of IMCI Guidelines
. Malaria
. Diarrhoea
. Immunization • Review of logistic
WHO Consultant & Local IMCI Team. IMCI Coordinator
October 2009 Ongoing
2
• IMCI Refresher Training for Facilitators
IMCI Local Team
March 2010
3 4
• IMCI Training • Adaptation of VHW algomerithm
IMCI Local Team WHO Consultant & IMCI Local Team
April 2010 2010
5
• VHW Training
IMCI Facilitators
Ongoing
6
• Introduction to ICATT Trained ICATT Facilitators
August 2010

Annex 9
1
Participant evaluation questionnaire for IMCI course using ICATT
1. For each ICATT section or activity listed in the left column, tick ( ) the box which you think
best describes it.
20 Questionaires Very useful
Useful
Somewhat useful
Useless
Navigation in ICATT (Moving through ICATT) 75% 25%
How to use computer session 45 45 10
Introduction (Case management process, charts and recording forms)
65 25 10
Care of the sick child aged 2 months up to 5 years
Assess and classify 80 20
Identify treatment 70 30
Treat the child 75 25
Counsel the mother 70 30
Follow‐up 70 30
Care of young infant aged up to 2 months
Essential care 75 25
Assess and classify young infant 75 25
Identify treatment, treat and counsel 75 15 10
Follow‐up 75 15 10
ICATT READ sections 85 15
ICATT SEE sections 85 15
ICATT PRACTISE sections 80 20
ICATT TEST sections 90 10
Drills
Role plays
Outpatient sessions 60 35 5
Inpatient ward sessions 60 35 5

Annex 9
2. How did you find navigation in ICATT (Moving through ICATT)? Easy � Not easy �
If not easy, please explain why: 80% 20%
Software concerns, need more time, difficulty with saving profile, unclear instructions on
how to load
3. For each ICATT item listed in the left column, tick ( ) if you found easy or difficult to work through it
Easy Not
easy
If not easy, please specify why (Continue
below the table if not enough space)
ICATT Introduction 95% 5 %
ICATT READ sections 100
ICATT SEE sections 100
Exercises with videos 90 10 Poor quality of sound and video, had to
return to question repeatedly
Exercises with photographs 90 10 Answers not correlating
Exercises requiring typing numbers
90 10
Exercises requiring typing text 85 15 Need to simplify, try to beat the system
to get it right hence shift of focus from
learning material
Exercises requiring ticking answers
85 15
Entire ICATT 75 25

Annex 9
4. For each item listed in the left column, tick ( ) if you found easy or difficult to learn the content
Easy Not easy
If not easy, please specify which unit and why (Continue below the table if not enough space)
ICATT Introduction 90% 10%
Care of the sick child aged 2 months up to 5 years
Assess and classify 100
Identify treatment 100
Treat the child 85 15
Counsel the mother 100
Follow‐up 100
Care of young infant aged up to 2 months
Essential care 95 5
Assess and classify young infant 95 5
Identify treatment, treat and
counsel
95 5
Follow‐up 95 5
Entire course 95 5
Annex 9
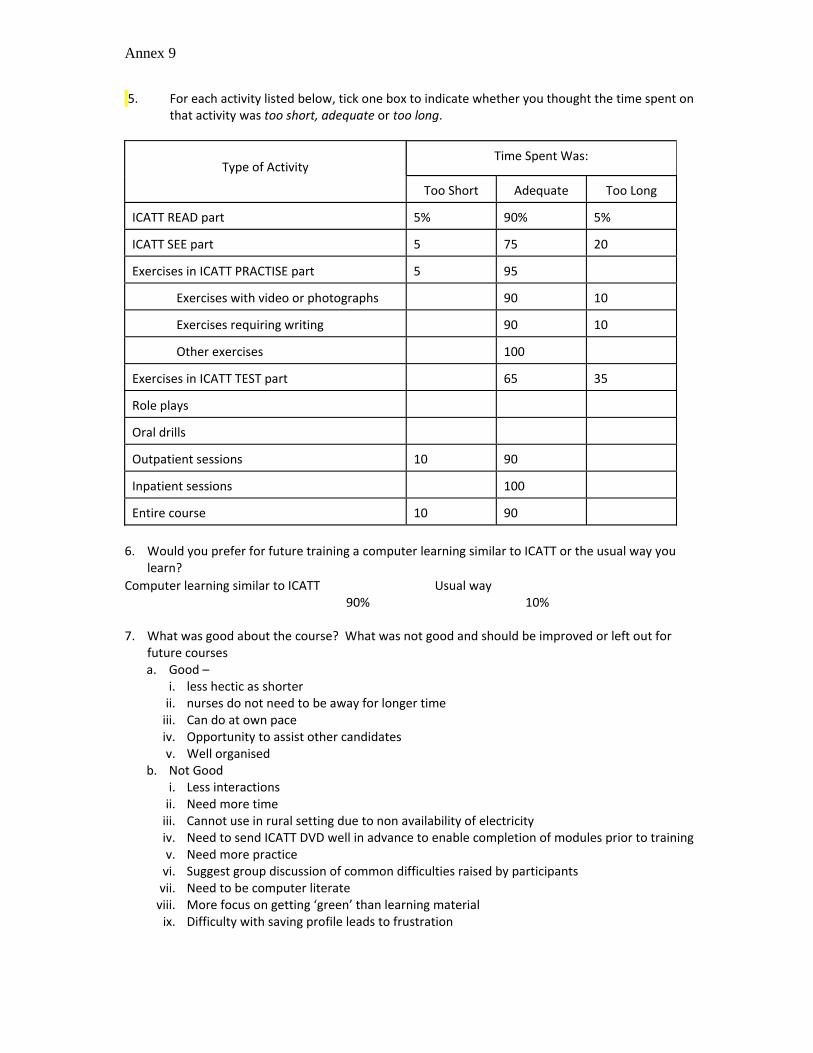
5. For each activity listed below, tick one box to indicate whether you thought the time spent on that activity was too short, adequate or too long.
Type of Activity Time Spent Was:
Too Short Adequate Too Long
ICATT READ part 5% 90% 5%
ICATT SEE part 5 75 20
Exercises in ICATT PRACTISE part 5 95
Exercises with video or photographs 90 10
Exercises requiring writing 90 10
Other exercises 100
Exercises in ICATT TEST part 65 35
Role plays
Oral drills
Outpatient sessions 10 90
Inpatient sessions 100
Entire course 10 90
6. Would you prefer for future training a computer learning similar to ICATT or the usual way you
learn? Computer learning similar to ICATT � Usual way � 90% 10% 7. What was good about the course? What was not good and should be improved or left out for
future courses a. Good –
i. less hectic as shorter ii. nurses do not need to be away for longer time iii. Can do at own pace iv. Opportunity to assist other candidates v. Well organised
b. Not Good i. Less interactions ii. Need more time iii. Cannot use in rural setting due to non availability of electricity iv. Need to send ICATT DVD well in advance to enable completion of modules prior to training v. Need more practice vi. Suggest group discussion of common difficulties raised by participants vii. Need to be computer literate viii. More focus on getting ‘green’ than learning material ix. Difficulty with saving profile leads to frustration

Annex 10
Tentative 6 day model IMCI Computerized Course using ICATT Training Set
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6
Opening & Welcome 10 min Introduction 20min. Assess & Classify revision of videos etc 2hrs.
OP work. A & E –complete 2.5 hrs
OP treat child, feeding assessment, counsel mother
OP – young infant Follow up
MORNING TEA OP –Demonstration Clinical Practice 2m up to 5years
Inpatient – 1hr Identify treatment & Treat the Child
Sick young infant Revision Video
Inpatient – young infant
LUNCH Diarrhoea –R/Videos Fever, Ear Problem Sore throat Skin problems
Role play‐ teaching mother to give oral drugs, WTR & WTRI Plan B & Plan A
Inpatient – BF Group discussion
Clarifications and round up
AFTERNOON TEA
The ICATT training set to be completed before the actual workshop First 2 Days to be dedicated to clarifying and queries and questions arising from the modules and to complete the exercises and tests.
Inpatient Chest indrawing wheeze
Feeding assessment & counsel mother Role play
Follow up Review
Closing.





























