Embed Size (px)
Citation preview

1
Clinical
Therapy Guide
Not for external distribution - Reference tool only

2
NURSING PROCESS
Risk Factors for Geriatric Syndromes 1
TESTS AND MEASURES
Short Physical Performance BatteryGait Speed5X Sit to StandBerg Balance ScaleDGIUnilateral Stance (Eyes Open)360° TurnFunctional ReachBarthel IndexTUG Mean Arterial Pressure
22333334444
OBSERVATIONAL ANALYSIS
Sit-to-Stand AnalysisStand-to-Sit AnalysisStanding Postural Control AnalysisGait AnalysisComplex Gait AnalysisActivity Analysis
566789
TABLE OF CONTENTS
OT/PT ASSESSMENT
OT Assessment – Medical Necessity andHomebound StatusOT Assessment – Impairments and PrognosisOT Assessment – Activity Limitations and Contextual Factors PT Assessment – Medical Necessity andHomebound StatusPT Assessment – Impairments and PrognosisPT Assessment – Activity Limitations and Contextual FactorsImprovements in Task PerformanceOngoing Deficits in Task Performance
1112
13
1516
171920

3
OT/PT INTERVENTION
Older Adult Strength Training RecommendationsGait TrainingCue TrainingmCIMTTraining Amplitude in Voice and MovementTraining Posture Vertical (A/P) Changes Related to Foot OrthosesOT Treatment IdeasPT Treatment IdeasGo-to TasksOther Treatment Ideas
21222223232425262728
SLP SPECIFIC
SLP Assessment – Impairments and PrognosisSLP Assessment – Activity Limitations and Contextual FactorsMotor with SwallowBolus ModificationSLP Language and Cognition Treatment IdeasSLP Swallow and Voice Treatment Ideas
29
3133343537
TABLE OF CONTENTS
Collaborative Construct TeamLisa Archibong, Project ManagerJennifer Ellis, PT, DPT, MSLaurie Otis, PT, MBA, MHAPatty Scheets, PT, DPT, NCSChris Stadler, Manager of Education
Thank you to each Subject MatterExpert for invaluable contributions
SELECTED REFERENCES
A – FF – MM – W
383940
CARDIOVASCULAR SCREENING AND GUIDELINES
Vital Sign Response GuidelinesDyspnea ScaleBorg Rating of Perceived Exertion (RPE)
414243
1
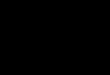
RISK FACTORS FOR GERIATRIC SYNDROMES FALLS FX DECLINE INCONTINENCE DELIRIUM DIZZINESS
• Older age• Two or more
falls in one year• Decreased
strength, balance, ambulation
• Psychotropic meds
• >4 total meds• Impaired depth
perception• Orthostasis• Foot problems• Depression
• Older age• H/o falls• Functional
impairment• Cognitive
impairment • Hospitalization• Stroke or MI• Depression• Vision
impairment• DM• Limited mobility
• Older age• High BMI• Constipation• UTI/urinary
retention• Antihistamines• Narcotic
analgesics• Diuretics• Impaired
mobility• Environmental
hazards• Cognitive
impairment• Restrictive
clothing
• Older age• Cognitive
impairment• Psychotropic
meds• Severe illness• Dehydration• Functional
impairment• Alcohol abuse• Infection• Metabolic
derangement• Sleep
deprivation• Visual
impairment• Hearing
impairment
• Depression• Cataracts• Impaired
balance or ambulation
• Orthostasis (20% decrease in MAP)
• DM• H/o MI• Three or
more meds
SYNDROME IDENTIFICATION

2
SHORT PHYSICAL PERFORMANCE BATTERYCLASSIFICATION
MCID = 1 – 2 points≤ 10 = increased risk of mobility disability
0 – 3 Severe limitations 7 – 9 Mild limitations
4 – 6 Moderate limitations 10 – 12 Minimal limitations
GAIT SPEED
Gait Speed Normal 3.3 ft/s (range 2.5 – 3.3)
Risk for Fx Decline 2.3 – 3.3 ft/s
Risk for Hospitalization <2 ft/s
Categories Household <1.3 ft/s
Limited Community 1.3 – 2.6 ft/s
Full Community >2.6 ft/s
MCID Older Adults 0.33 ft/s
Stroke 0.48 ft/s (acute); 0.45 – 0.75 ft/s (sub-acute)
PD 0.57 ft/s
TESTS AND MEASURES
3
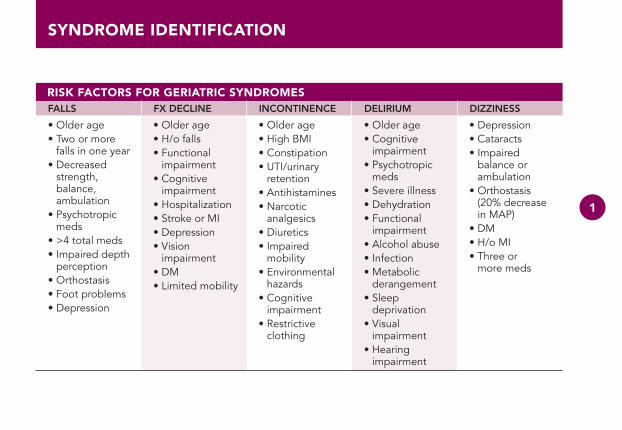
5X SIT TO STANDAGE NORMS
Normal = 10 sFall risk = >14 – 15 sMCID for vestibular patients = 2.3 s
60 – 69 yr = ≤ 11.4 s70 – 79 yr = ≤ 12.6 s80 – 89 yr = ≤ 14.8 s
BERG BALANCE SCALE
MCID = 3.3 – 5.9 points in elderly patients7 – 8 points in stroke patients5 points in Parkinson’s patients
DGI
Fall risk = ≤ 19 MCID = 3 – 9 points (higher with lower baseline score)
UNILATERAL STANCE (EYES OPEN)AGE NORMS
60 – 69 yr = 27.0 s70 – 79 yr = 17.2 s80 – 89 yr = 8.5 s
360° TURN
Normal = Full circle without loss of balance in <3.8 s
TESTS AND MEASURES

4
FUNCTIONAL REACHAGE NORMS
≤ 6 inches = limited balance10+ inches = adequate balanceUnwilling = fall risk 8x >normal<6” = fall risk 4x >normal6 – 10” = fall risk 2x >normal≥ 10” = low fall risk
41 – 69 yr: 15” men; 14” women70 – 87 yr: 13” men; 10.5” women
BARTHEL INDEX
MCID = 1.85 0 – 40 = associated with placement in long-term care or death> 6 0 = likely to be in homes and community, have more social
interaction and higher life satisfaction
TUG AGE NORMS
>14 s = high fall risk>30 s = predicts need for amb device
and assist with ADLs
60 – 69 yr = 8.1 s70 – 79 yr = 9.2 s80 – 89 yr = 11.3 s
MEAN ARTERIAL PRESSURE
MAP = 2(DP) + SP 3
20% drop in MAP indicates orthostatic hypotension
TESTS AND MEASURES

5
SIT-TO-STAND ANALYSISOVERALL INITIATION EXECUTION TERMINATION
• Unable to assume normal starting posi-tion; stiffness
• Absent preparatory movements
• Unable to modify movement strategy with cues/practice
• Increased base of support
• Insufficient force production
• Decreased weight bearing• Shifts center of mass to
one side• Shifts COM to one side or
back; resists correction• Medial hip rotation/hip
adduction• Extends knees before hips
in first half• Insufficient anterior transla-
tion of tibia over foot• Pushes on thighs to extend
trunk• Valgus of knee• Varus of knee• Excessive pronation of foot• Supination of foot
• Posterior sway• Steps• Shifts COM to
one side• Shifts COM to one
side or back; resists correction
• Increased lumbar extension
• Inadequate hip extension
• Inadequate knee extension
new section
OBSERVATIONAL ANALYSIS
6
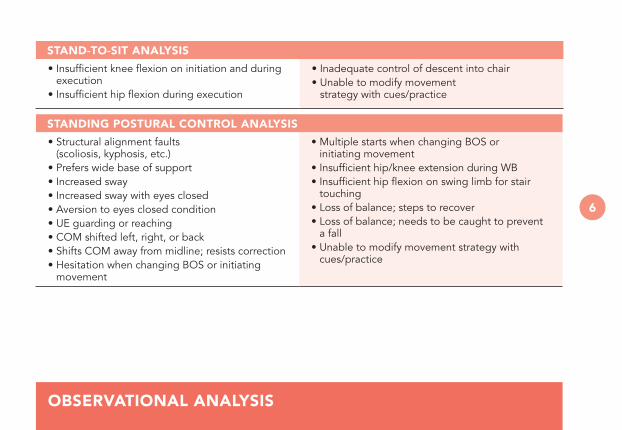
STAND-TO-SIT ANALYSIS
• Insufficient knee flexion on initiation and during execution
• Insufficient hip flexion during execution
• Inadequate control of descent into chair• Unable to modify movement
strategy with cues/practice
STANDING POSTURAL CONTROL ANALYSIS
• Structural alignment faults (scoliosis, kyphosis, etc.)
• Prefers wide base of support• Increased sway• Increased sway with eyes closed• Aversion to eyes closed condition• UE guarding or reaching• COM shifted left, right, or back • Shifts COM away from midline; resists correction • Hesitation when changing BOS or initiating
movement
• Multiple starts when changing BOS or initiating movement
• Insufficient hip/knee extension during WB• Insufficient hip flexion on swing limb for stair
touching • Loss of balance; steps to recover• Loss of balance; needs to be caught to prevent
a fall• Unable to modify movement strategy with
cues/practice
OBSERVATIONAL ANALYSIS
7
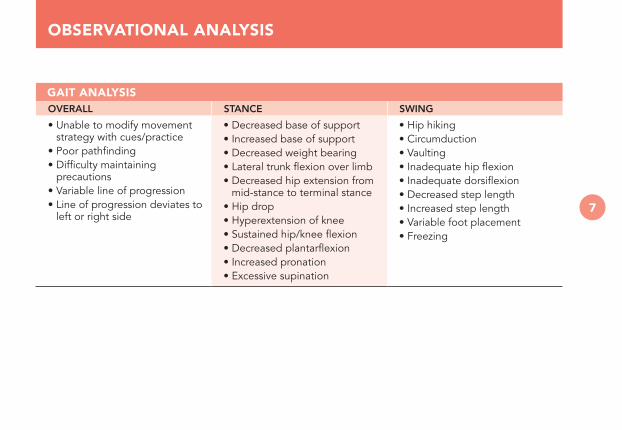
GAIT ANALYSISOVERALL STANCE SWING
• Unable to modify movement strategy with cues/practice
• Poor pathfinding• Difficulty maintaining
precautions• Variable line of progression• Line of progression deviates to
left or right side
• Decreased base of support• Increased base of support• Decreased weight bearing• Lateral trunk flexion over limb• Decreased hip extension from
mid-stance to terminal stance• Hip drop• Hyperextension of knee• Sustained hip/knee flexion• Decreased plantarflexion • Increased pronation• Excessive supination
• Hip hiking• Circumduction• Vaulting• Inadequate hip flexion• Inadequate dorsiflexion• Decreased step length• Increased step length• Variable foot placement• Freezing
OBSERVATIONAL ANALYSIS

8
COMPLEX GAIT ANALYSIS
• Deviation in line of progression with head turning• Hesitates or takes extra steps when changing
direction• Poor control of posterior momentum when stepping
backward• Hesitates before stepping over obstacles• Poor adjustment in step length to step
over obstacles
• Difficulty clearing second limb when stepping over obstacles
• Insufficient hip/knee extension when stepping over obstacles
• Guarded movement/fear avoidance behavior• Unable to modify movement strategy with
cues/practice
OBSERVATIONAL ANALYSIS

9
ACTIVITY ANALYSIS
• All required actions and performance skills present
MOTOR SKILL DEFICITS
• Weakness• Abnormal movement synergy• Delayed initiation• Bradykinesia• Hypermetria• Tremor
• Stiffness• Poor balance• Apraxia• Impaired fine motor• Requires frequent rests
SENSORY – PERCEPTUAL SKILL DEFICITS
• Impaired body positioning for task• Impaired visual identification of objects/
environment
• Impaired tactile location of objects/environment• Impaired spatial orientation of objects
COGNITIVE SKILL DEFICITS
• Attention to task limited to ____________________• Impaired selection of objects appropriate for task• Impaired sequencing of task components• Impaired organization of task components given
allotted time• Seeks excessive assistance• Seeks insufficient assistance
• Task perseveration• Impaired prioritization of attention, increasing
risk of adverse events• Impaired adaptability to changing task or
environmental demands• Diminished performance with a secondary
cognitive task
OBSERVATIONAL ANALYSIS

10
COMMUNICATION AND SOCIAL SKILL DEFICITS
• Delayed response• Impaired use of gestures
• Lack of response to visual cues
EMOTIONAL REGULATION SKILL DEFICITS
• Lack of persistence with task completion• Frustration with efforts
• Anxious• Anger with efforts
OBSERVATIONAL ANALYSIS

11
OT ASSESSMENT – MEDICAL NECESSITY AND HOMEBOUND STATUSPatient requires skilled intervention due to new deficits related to recent events including:
• Hospitalization and related functional decline• Recent or progressive decline in mobility• Increased dependence on caregiver for ADLs
and mobility• Recent c/o dizziness, unsteadiness, and/or pain• Fall
• Change in mental status• S/p fracture • Exacerbation of chronic condition
affecting function• New problem in health condition
Patient requires care in the home because:
• Unable to transfer without assistance• Unable to walk community distances• Unable to negotiate stairs without assistance• Symptoms at rest _________________• Symptoms when away from home• Requires rest every ________ minutes• Excessive fatigue when away from home
• Unable to toilet self in community• Pain with extended sitting, standing or walking• Unable to maintain attention with distractions • Unable to problem solve in community situations• Unable to manage behaviors in
community situations
OT/PT ASSESSMENT

12
OT ASSESSMENT – IMPAIRMENTS AND PROGNOSISPatient's primary impairments identified on clinical examination which contribute to decline in function:
SENSORY-PERCEPTUAL
• Impaired spatial/object organization• Perceptual deficits• Visual field loss• Other visual deficits• Disregard/neglect• Impaired tactile sensation
• Impaired two-point discrimination or proprioception• Pain• Impaired sensory selection, weighting, and
integration needed for balance• Decreased balance confidence
MOTOR
• Joint pain/stiffness• Impaired postural reactions• Weakness/muscle fatigue• Delayed postural responses• Hypertonicity/non-fractionated movement/
impaired tone
• Slowness of movement• Dyskinesia/dystonia• Hypermetria• Apraxia• Slow/imprecise object manipulation
FUNCTIONAL CAPACITY
• Impaired activity tolerance • Impaired respiratory capacity
continued on next page
OT/PT ASSESSMENT

13
OT ASSESSMENT – IMPAIRMENTS AND PROGNOSISCOGNITIVE
• Impaired sequencing • Impaired organization• Impaired judgment/safety• Impaired problem solving/adaptability
• Impaired attention to task• Instability with secondary tasks• Impaired memory• Delayed initiation
EMOTIONAL/BEHAVIORAL
• Lack of response to cues• Lack of interest/depression• Anxiety
• Anger• Frustration
Prognosis for improvement in impairments that contribute to decline in function:
• Good (75 – 100% improvement) • Fair (30 – 75% improvement) • Poor (0 – 30% improvement)
OT ASSESSMENT – ACTIVITY LIMITATIONS AND CONTEXTUAL FACTORSPatient’s impairments are believed to contribute to the following activity limitations and participation restrictions:
• Inability to perform tasks with sufficient consistency, flexibility, and/or efficiency
• Decreased independence with ADLs• Decreased independence with IADLs• Inability to tolerate continuous activity
• Inability to manipulate objects• Impaired safety awareness• Inability to plan for future events• Inability to manage medications
OT/PT ASSESSMENT

14
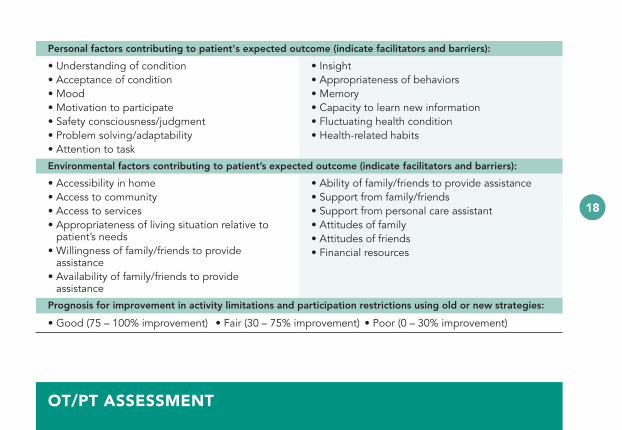
Personal factors contributing to patient’s expected outcome (indicate facilitators and barriers):
• Understanding of condition• Acceptance of condition• Mood• Motivation to participate• Safety consciousness/judgment• Problem solving/adaptability• Attention to task
• Insight• Appropriateness of behaviors• Memory• Capacity to learn new information• Fluctuating health condition• Health-related habits
Environmental factors contributing to patient’s expected outcome (indicate facilitators and barriers):
• Accessibility in home• Access to community• Access to services• Appropriateness of living situation relative to
patient’s needs • Willingness of family/friends to provide assistance• Availability of family/friends to provide assistance
• Ability of family/friends to provide assistance• Support from family/friends• Support from personal care assistant• Attitudes of family• Attitudes of friends• Financial resources
Prognosis for improvement in activity limitations and participation restrictions using old or new strategies:
• Good (75 – 100% improvement) • Fair (30 – 75% improvement) • Poor (0 – 30% improvement)
OT/PT ASSESSMENT

15
PT ASSESSMENT – MEDICAL NECESSITY AND HOMEBOUND STATUSPatient requires skilled intervention due to new deficits related to recent events including:
• Hospitalization and related functional decline• Recent or progressive decline in mobility• Increased dependence on caregiver for ADLs
and mobility• Fall• Recent c/o dizziness, unsteadiness, and/or pain
• Change in mental status• S/p fracture • Exacerbation of chronic condition affecting
function• New problem in health condition
Patient requires care in the home because:
• Unable to transfer without assistance• Unable to walk community distances• Unable to negotiate stairs without assistance• Symptoms at rest _________________• Symptoms when away from home• Requires rest every ________ minutes• Excessive fatigue when away from home
• Unable to toilet self in community• Pain with extended sitting, standing, or walking• Unable to maintain attention with distractions • Unable to problem solve in community situations• Unable to manage behaviors in community
situations
OT/PT ASSESSMENT

16
PT ASSESSMENT – IMPAIRMENTS AND PROGNOSISPatient’s primary movement system impairments identified on clinical examination which contribute to decline in function:
MUSCULOSKELETAL
• Skeletal muscle weakness/fatigue• Structural alignment faults• Joint pain/stiffness
• Neuropathic pain• Other pain
NEUROMUSCULAR
• Impaired postural responses and reactions• Impaired sensory selection, weighting, and
integration needed for balance• Decreased sensation• Impaired vertical orientation• Impaired vertical orientation with resistance
to correction• Decreased balance confidence/fear avoidance
strategies
• Dizziness• Hypertonicity/non-fractionated movement• Hypokinesia/Bradykinesia• Dyskinesia/dystonia• Hypermetria• Impaired motor planning• Instability with secondary tasks
continued on next page
OT/PT ASSESSMENT

17
PT ASSESSMENT – IMPAIRMENTS AND PROGNOSISCARDIOPULMONARY
• Poor gas exchange at rest or with activity per O2 SAT monitoring
• Labored breathing at rest or with activity• Irregular heart rhythm with activity
• Cardiovascular inefficiency with extended recovery period after activity
• Pulmonary inefficiency with extended recovery period after activity
• Abnormal vital sign response with activity
Prognosis for improvement in impairments that contribute to decline in function:
• Good (75 – 100% improvement) • Fair (30 – 75% improvement) • Poor (0 – 30% improvement)
PT ASSESSMENT – ACTIVITY LIMITATIONS AND CONTEXTUAL FACTORSPatient's impairments are believed to contribute to the following activity limitations/participation restrictions:
• Inability to perform tasks with sufficient consistency, flexibility and/or efficiency
• Decreased independence with mobility• Inability to tolerate continuous activity• Instability in sitting• Instability in standing
• Instability with walking• Impaired safety awareness• Pain during functional activity or at rest• Risk for falls• Risk for functional decline
continued from previous page
OT/PT ASSESSMENT
18
Personal factors contributing to patient's expected outcome (indicate facilitators and barriers):
• Understanding of condition• Acceptance of condition• Mood• Motivation to participate• Safety consciousness/judgment• Problem solving/adaptability• Attention to task
• Insight• Appropriateness of behaviors• Memory• Capacity to learn new information• Fluctuating health condition• Health-related habits
Environmental factors contributing to patient’s expected outcome (indicate facilitators and barriers):
• Accessibility in home• Access to community• Access to services• Appropriateness of living situation relative to
patient’s needs• Willingness of family/friends to provide
assistance• Availability of family/friends to provide
assistance
• Ability of family/friends to provide assistance• Support from family/friends• Support from personal care assistant• Attitudes of family• Attitudes of friends• Financial resources
Prognosis for improvement in activity limitations and participation restrictions using old or new strategies:
• Good (75 – 100% improvement) • Fair (30 – 75% improvement) • Poor (0 – 30% improvement)
OT/PT ASSESSMENT

19
IMPROVEMENTS IN TASK PERFORMANCECONSISTENCY because
• Larger/faster associated postural adjustments• Larger/faster corrective postural responses• Larger/faster protective postural responses• Patient is getting stronger
• Maintaining attention to primary task• Allowing more time for movement preparation
and planning• Able to report intrinsic feedback
FLEXIBILITY because
• Rapid access to best movement strategy• Able to change strategy relative to situational
demands
• Able to shift attention from one aspect of task performance to another
• Able to maintain primary task performance during performance of a secondary task
EFFICIENCY because
• Improved vital sign response during activity• Decreased energy expenditure associated with
fear or instability
• Decreased co-contraction in order to complete task or activity
• Improved speed of movement
OT/PT ASSESSMENT

20
ONGOING DEFICITS IN TASK PERFORMANCECONSISTENCY because
• Fluctuating medical condition limits opportunity for repeated practice
• Lack of intrinsic feedback to guide movement performance
• Performance within a session improving but needs more practice for learning
• Deficits in movement timing which are changing but still insufficient for all tasks
• Deficits in movement timing which are not changing with practice
• Deficits in movement amplitude which are changing but still insufficient for all tasks
• Deficits in movement amplitude which are not changing
• Weakness which is improving but will require ongoing resistance training
• Weakness which is not changing• Deficits in placement of attentional resources• Agitation which limits opportunity for repeated
practice
FLEXIBILITY because
• Fluctuating medical condition limits opportunity for repeated practice
• Lack of intrinsic feedback to guide movement performance
• Inability to develop effective strategy without extrinsic feedback
• Fear or anxiety with new activities• Agitation which limits opportunity for practice
EFFICIENCY because
• Fluctuating medical condition limits opportunity for extended practice
• Primary medical condition limits opportunity for extended practice
• Poor prognosis for improvement in impairments
OT/PT ASSESSMENT

21
OLDER ADULT STRENGTH TRAINING RECOMMENDATIONS
Stroke: likely to progress from 60 to 80% 1 – RM more slowly; 3 sessions/week; 12 weeksPD: generally follow guidelines for older adultsMS: 60% 1 – RM; 1 – 3 sets initially, then 3 – 4; 2 – 3 days/week; 10 – 12 weeks
• 60% 1 – RM• 15 reps @ RPE
of 12 – 13 (Borg)
• 80% 1 – RM• 10 reps @ RPE
of 15 – 17 (Borg)
• 1 – 3 sets• 2 – 3 days/week• 6 – 8 weeks
Minimal Intensity
Sets/RepsTarget Intensity
OT/PT INTERVENTION

22
GAIT TRAININGCONTINUOUS STEPPING SPEED TRAINING
• Gait is a continuous task• More steps are better
• 10 sec bouts as fast as possible• Recover• Repeat• Increase baseline speed
CUE TRAINING
For speed • Visual cue: lines 20 – 24 inches apart; “Step on (or over) the lines.”• Auditory cue: 10% above baseline; “Match your movements to the beat.”
For amplitude • Visual cue: lines 20 – 24 inches apart• Auditory cue: 10% below baseline (especially for patients who freeze)
For freezing and turning
• Visual cue: lines 18 – 22 inches apart where likely to freeze; “Use the cue to remind you to take a bigger step to prevent freezing.”
• Auditory cue: baseline or 10% below; “Use the cue to maintain stepping movements.”• Stepping through strategy: keep stepping through the tricky spots, all directions• Approach doorway by aiming for the wall to the side of the door handle to allow
room for door to open
For dyskinesia • Visual cue: lines 20 – 24 inches apart; lines indicating step width for lateral deviations• Auditory cue: 10% above baseline
OT/PT INTERVENTION
22

23
mCIMT
• Constrain unaffected arm five hours/day, five days/week; two weeks
• Structured therapy; 1/2 hour sessions; three times/week
TRAINING AMPLITUDE IN VOICE AND MOVEMENT
High Effort “On a scale of 1 – 10, with 10 being a lot and 1 nothing at all, how much effort was that? Try to get as high on the effort scale as you can each time.”
Sensory Calibration
“How do your limbs feel? Do you hear how loud you can be? What you are feeling produces sound (or movement) that is normal. Repeat that feeling each time.”
Shape Quality Manual and verbal cues to improve quality of movement and sound each time. “Do what I do.”
Homework Incorporate therapy activities into functional activity. Do every day.
OT/PT INTERVENTION

24
TRAINING POSTURE VERTICAL (A/P)
Standing with the back against the wall
• Heels against wall; relax in position; use assistive device if needed• Increase amount of time standing without resisting• Produce active sway forward so that COM moves toward forward limits of stability• Practice walking and/or sit to stand after • Progress to wedge training with ankles in DF
Sit to Stand • Without UE support if possible, raise the surface height to accommodate for weakness during initiation
• If must use UE, do so only during initiation; then have the patient let go; push and let go• Provide a manual block to posterior translation of the tibia during execution• Provide assistance with anterior translation of the tibia relative to the foot • Provide encouragement and support related to fear of falling
Stand to Sit • Initiate by flexing the knees, keeping the COM over the BOS during the first half of execution
• Avoid teaching to initiate sitting down by reaching back for the chair • Avoid teaching to step back until the back of the knees touch the chair before sitting down• Use UE to compensate for weakness during the last half of execution
Ambulation with continuous stepping
• Emphasis on forward progression
Backward stepping
• Keep COM over BOS; don’t let COM get behind BOS
OT/PT INTERVENTION

25
CHANGES RELATED TO FOOT ORTHOSES TYPE OF SUPPORT EFFECT ON FOOT EFFECT ON ANKLE EFFECT ON KNEE
Medial Rearfoot eversion Calcaneal eversion Inversion moment
Eversion Tibial medial rotation moment
Valgus angle
Lateral Plantar strain Subtalar valgus Supination
Lateral instability Varus moment
Posterior Soft tissue strain DF excursion Flexion
➔➔
➔ ➔ ➔
➔
➔ ➔ ➔
➔
➔
➔
➔ ➔
OT/PT INTERVENTION

26
OT TREATMENT IDEAS• Remediation or compensation?• Is treatment harder than self-selected (intensity)? • What is the dosage of each treatment?
Self-Care Training • In standing • Speed training
Cognitive Training • Task complexity • Sequencing
Balance Training • Foam• Surface transitions• Trunk displacement• Secondary manual or cognitive task
• Head rotation and tilt• Eye exercises• VOR and VOR cancellation
UE Task Training • Containers and lids• Reach overhead and at ground level• Object manipulation• Unilateral and bilateral item transport
• Alternating item transport• mCIMT• Auditory cueing
Risk Factor Reduction • Improve lighting• Add visual contrast• Reduce visual stimulation and
distraction
• Organization
OT/PT INTERVENTION

27
PT TREATMENT IDEAS• Remediation or compensation?• Is treatment harder than self-selected (intensity)? • What is the dosage of each treatment?
Task Specific-training • Go-to tasks
Sit to/from Standing w/o UE Support
• Variable practice
Floor to/from Standing • With/without external support
UE Task Training • Reach, grasp, release • mCIMT
Stair Training • With/without railing• Step-to
• Step-through
Gait and Balance Training
• With/without device• Variable surface and surface
transitions• Foam, foam, foam, foam• Narrow BOS• Incline and verticality training• Secondary manual or cognitive task• Speed training – 10 sec bouts;
baseline speed
• Amplitude training• Cue training• Step up, over, and around• Backward stepping• Continuous stepping• Head turning and tilts• VOR and eye exercises
new section new color
➔
OT/PT INTERVENTION

28
GO-TO TASKS OTHER TREATMENT IDEAS
OT/PT INTERVENTION

29
SLP ASSESSMENT – IMPAIRMENTS AND PROGNOSIS Patient’s primary impairments identified on clinical examination which contribute to decline in function:
SENSORIMOTORSPEECH/LANGUAGE PRODUCTION DYSPHAGIA COGNITION
• Structural anomalies• Decreased ROM• Muscle weakness/
fatigue• Impaired coordination• Impaired sensation• Neglect• Delayed response
time or reflexes• Decreased respiratory
support
• Aphasia– Broca’s– Global– Wernicke’s– Anomic– Conduction– Transcortical motor/
sensory/mixed• Oral apraxia• Spastic/flaccid/ataxic
dysarthria • Velopharyngeal
insufficiency
• Oral/pharyngeal/esophageal dysphagia
• Impaired pharyngeal closure/laryngeal vestibule closure
• UES dysfunction• Impaired esophageal
motility• Poor dentition/oral
hygiene• Weak/imprecise
mastication• Ineffective bolus for-
mation/propulsion
• Decreased sustained/selective/divided/alternating attention
• Decreased imme-diate/short-term/long-term memory
• Impaired insight/ judgment
• Impaired problem solving
• Delayed processing/sequencing
• Decreased organiza-tion/planning
continued on next page
SLP SPECIFIC

30
SLP ASSESSMENT – IMPAIRMENTS AND PROGNOSIS Patient’s primary impairments identified on clinical examination which contribute to decline in function:
SENSORIMOTORSPEECH/LANGUAGE PRODUCTION DYSPHAGIA COGNITION
• Impaired intonation/pitch/rate of speech/volume
• Dysfluency• Impaired auditory/
reading comprehension• Impaired written
expression
• Impaired ant/post bolus transit
• Increased oral/ pharyngeal residue
• Impaired soft palate elevation and retraction
• Decreased executive function
• Agnosia• Impaired orientation
Prognosis for improvement in impairments that contribute to decline in function:
• Good (75 – 100% improvement) • Fair (30 – 75% improvement) • Poor (0 – 30% improvement)
continued from previous page
SLP SPECIFIC

31
SLP ASSESSMENT – ACTIVITY LIMITATIONS AND CONTEXTUAL FACTORSPatient’s new or worsened activity limitations and participation restrictions related to the impairments:
• Inability to perform tasks with sufficient consistency, flexibility and/or efficiency
• Safe swallowing/meals• Medication management• Calendar management• Financial management• Independent disease management• Respond in an emergency• Home safety• Express basic wants and needs• Verbalize plans/solutions• Understand spoken information• Comprehend basic information• Follow simple written instructions• Follow a map or directions
• Reading tasks (e.g., newspaper, medication labels)• Understand technical/complicated written material• Participate in simple conversation• Participate in complex conversation• Create routine lists/take simple messages• Compose reports/express complex ideas
in writing• Recall pertinent information• Perform routine tasks with/without reminders• Plan/execute new/unfamiliar tasks• Community activities• Understand and participate in abstract thinking• Divide or alternate attention between multiple
tasks
continued on next page
SLP SPECIFIC
32
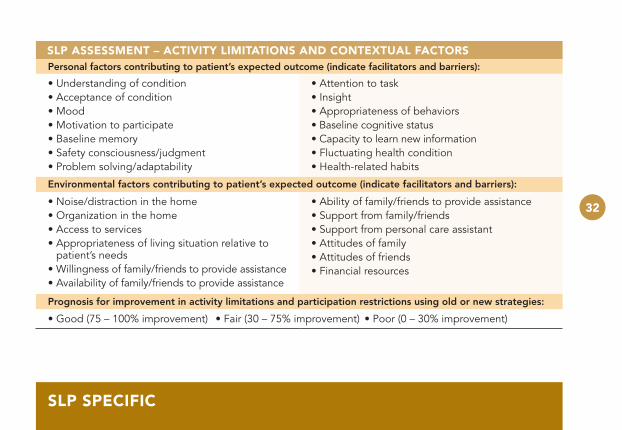
SLP ASSESSMENT – ACTIVITY LIMITATIONS AND CONTEXTUAL FACTORSPersonal factors contributing to patient’s expected outcome (indicate facilitators and barriers):
• Understanding of condition• Acceptance of condition• Mood• Motivation to participate• Baseline memory• Safety consciousness/judgment• Problem solving/adaptability
• Attention to task• Insight• Appropriateness of behaviors• Baseline cognitive status• Capacity to learn new information• Fluctuating health condition• Health-related habits
Environmental factors contributing to patient’s expected outcome (indicate facilitators and barriers):
• Noise/distraction in the home• Organization in the home• Access to services• Appropriateness of living situation relative to
patient’s needs• Willingness of family/friends to provide assistance• Availability of family/friends to provide assistance
• Ability of family/friends to provide assistance• Support from family/friends• Support from personal care assistant• Attitudes of family• Attitudes of friends• Financial resources
Prognosis for improvement in activity limitations and participation restrictions using old or new strategies:
• Good (75 – 100% improvement) • Fair (30 – 75% improvement) • Poor (0 – 30% improvement)
SLP SPECIFIC

33
MOTOR WITH SWALLOW
Supraglottic Super- supraglottic Effortful Mendelsohn
ManeuverMasako
Maneuver
Closes vocal cords before and during swallow
Closes airway entrance before and during swallow
Increases BOT retraction and propulsive forces
Facilitates pharyngeal clearance
BOT function
Timing and extent of laryngeal closure
Bolus swallow
Bolus swallow
Facilitates UES opening
Hold ant. por-tion of tongue between teeth and swallow
Bolus swallow
Hold breath; bear down; swallow; cough
Squeeze hard with tongue during swallow
Bolus swallow
Hold breath; swallow; cough to clear
Swallow; hold larynx elevated 3 – 5 sec; release
10 times/day for 5 min
SLP SPECIFIC

34
BOLUS MODIFICATION
CARBONATED• Carbonated water,
seltzer, soda water, ginger ale
BOLUS MODIFICATION
TEXTURE• Potato chips in puree• Crushed crackers in
mashed potatoes
EVERY 2 – 3 SWALLOWS• Rotate among different
bolus characteristics
SOUR• 1/2 lemon juice• 1/2 water
TEXTURE• Potato chips in puree• Crushed crackers in
mashed potatoes
CARBONATED• Carbonated water,
seltzer, soda water, ginger ale
EVERY 2-3 SWALLOWS• Rotate among different
bolus characteristics
BOLUS MODIFICATION
SLP SPECIFIC

35
SLP SPECIFIC
SLP LANGUAGE AND COGNITION TREATMENT IDEAS
• Remediation or compensation? • Is treatment harder than self-selected (intensity)?• What is the dosage of each treatment?
LANGUAGE/APHASIA
• Phonemic and semantic cueing• Phrase completions• Object, divergent/convergent naming• Picture descriptions
• Conversational speech• Synonyms/antonyms• Constraint-induced treatment
WRITTEN EXPRESSION
• Signature• Grocery lists and personal letters/cards
• Applications• Medical information
PRAGMATICS
ACC
AUDITORY COMPREHENSION
• Answering questions• Following increasingly complex directions
• Increasingly complex levels
continued on next page

36
SLP SPECIFIC
SLP LANGUAGE AND COGNITION TREATMENT IDEAS
• Remediation or compensation? • Is treatment harder than self-selected (intensity)?• What is the dosage of each treatment?
READING COMPREHENSION
• Newspapers• Medication lists
• Medication schedules• Calendar
COGNITIVE SKILL DEVELOPMENT
• Daily journal/schedule• Calendar management• Digits forward/backward
• Recall tasks and strategies• Environmental adaptations
37
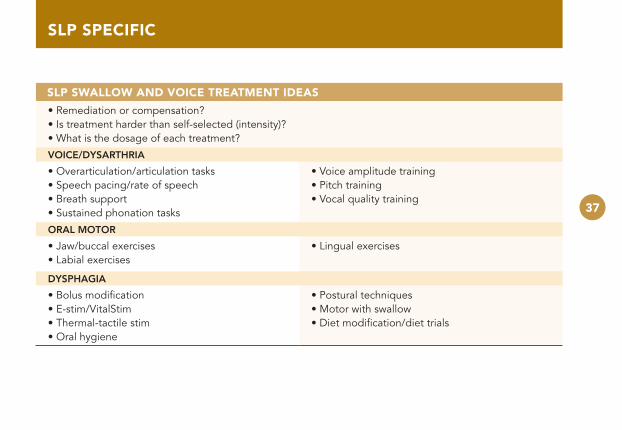
SLP SWALLOW AND VOICE TREATMENT IDEAS
• Remediation or compensation? • Is treatment harder than self-selected (intensity)?• What is the dosage of each treatment?
VOICE/DYSARTHRIA
• Overarticulation/articulation tasks• Speech pacing/rate of speech• Breath support• Sustained phonation tasks
• Voice amplitude training• Pitch training• Vocal quality training
ORAL MOTOR
• Jaw/buccal exercises• Labial exercises
• Lingual exercises
DYSPHAGIA
• Bolus modification• E-stim/VitalStim• Thermal-tactile stim• Oral hygiene
• Postural techniques• Motor with swallow• Diet modification/diet trials
SLP SPECIFIC

38
SELECTED REFERENCES
Selected ReferencesAvers D, Brown M. White paper: strength training for the older adult. Journal of Geriatric Physical Therapy. 2009;32(4):148-152.
Barbieri G, Gissot A-S, Perenonnou, D. Ageing of the postural vertical. Age. 2010;32:51-60.
Bastian AJ. Understanding sensorimotor adaptation and learning for rehabilitation. Current Opinion in Neurology. 2008;21:628–633.
Birkenmeier RL, Prager EM, Lang CE. Translating animal doses of task-specific training to people with chronic stroke in 1-hour therapy sessions: a proof-of-concept study. Neurorehabil Neural Repair. 2010;24(7):620-630.
Dean CM, Richards CL, Malouin F. Task-related circuit training improves performance of locomotor tasks in chronic stroke: a randomized, controlled pilot trial. Arch Phys Med Rehabil. 2000;81:409-17.
Dromerick AW , Lang CE, Birkenmeier RL, et al. Very early constraint-induced movement during stroke rehabilitation (VECTORS). Neurology®. 2009;73:195–201.
Ebersbach G, Ebersbach A, Edler D, et al. Comparing exercise in Parkinson’s disease - the Berlin LSVT BIG study. Movement Disorders. 2010;25(12):1902–1908.
Farley BG, Fox CM, Ramig LO, et al. Intensive amplitude-specific therapeutic approaches for Parkinson’s disease: toward a neuroplasticity-principled rehabilitation model. Topics in Geriatric Rehabilitation. 2008;24(2):99-114.
Farley BG, Koshland GF. Training BIG to move faster: the application of the speed–amplitude relation as a rehabilitation strategy for people with Parkinson’s disease. Exp Brain Res. 2005; 167(3):462-467.

39
SELECTED REFERENCES
Fried TR, Tinetti ME, Iannone L. Primary care clinicians’ experiences with treatment decision making for older persons with multiple conditions. Arch Intern Med. 2011;171(1):75-80.
Horn SD, DeJong G, Smout RJ, et al. Stroke rehabilitation patients, practice, and outcomes: is earlier and more aggres-sive therapy better? Arch Phys Med Rehabil. 2005;86(2):S101-14.
King LA, Horak FB. Delaying mobility disability in people with Parkinson disease using a sensorimotor agility exercise program. Phys Ther. 2009;89:384–393.
Kleim JA. III STEP: a basic scientist’s perspective. Physical Therapy. 2006;86(5):614-617.
Kleim JA, Jones TA, Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. Journal of Speech, Language, and Hearing Research. 2008;51:s225-s239.
Lang CE, MacDonald, JR, Gnip C. Counting repetitions: an observational study of outpatient therapy for people with hemiparesis post-stroke. JNPT. 2007;31:3-10.
Lang CE, MacDonald JR, Reisman DS, et al. Observation of amounts of movement practice provided during stroke rehabilitation. Arch Phys Med Rehabil. 2009;90:1692-8.
Manckoundia P, Mourey F, Perennou D, et al. Backward disequilibrium in elderly subjects. Clinical Interventions in Aging. 2008;3(4):667–672.
Matheron E, Dubost V, Mourey F, et al. Analysis of postural control in elderly subjects suffering from psychomotor disadaptation syndrome (PDS). Archives of Gerontology and Geriatrics. 2010;(51):e19–e23.
Morris ME. Locomotor training in people with Parkinson disease. Physical Therapy. 2006;86(10):1426-1435.

40
SELECTED REFERENCES
Morris ME, Martin CL, Schenkman ML. Striding out with Parkinson disease: evidence-based physical therapy for gait disorders. Physical Therapy. 2010;90(2):1-9.
Nieuwboer A. Cueing for freezing of gait in patients with Parkinson’s disease: a rehabilitation perspective. Movement Disorders. 2008;23(2):s475-s481.
Ozturk A, Simsek TT, Yumin ET, et al. The relationship between physical, functional capacity and quality of life (QoL) among elderly people with a chronic disease. Archives of Gerontology and Geriatrics. 2011;53:278–283.
Pak S, Patten C. Strengthening to promote functional recovery poststroke: an evidence-based review. Topics in Stroke Rehabilitation. 2008;15(3):177–199.
Sullivan KJ, Brown DA, Klassen T, et al. Effects of task-specific locomotor and strength training in adults who were ambulatory after stroke: results of the STEPS randomized clinical trial. Physical Therapy. 2007;87(12):1580-1602.
Thaut MH, Leins AK, Rice RR, et al. Rhythmic auditory stimulation improves gait more than NDT/Bobath training in near-ambulatory patients early poststroke: a single-blind, randomized trial. Neurorehabil Neural Repair. 2007;21:455-459.
Tilson JK, Settle SM, Sullivan KJ. Application of evidence-based practice strategies: current trends in walking recovery interventions poststroke. Topics in Stroke Rehabilitation. 2008;15(3):227–246.
Wolf SL, Winstein CJ, Miller JP, et al. Retention of upper limb function in stroke survivors who have received constraint-induced movement therapy: the EXCITE randomised trial. Lancet Neurol. 2008;7:33–40.
Wolf SL, Winstein CJ, Miller JP, et al. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke. JAMA. 2006;296:2095-2104.

41
VITAL SIGN RESPONSE GUIDELINES
RESTING NORMAL HIGH VERY HIGH EMERGENCY
SBP 70 – 160 160 – 190 190 – 220 >220
DBP <90 90 – 110 110 – 120 >120
Heart Rate 60 – 90 90 – 110 110 – 125 >125
Heart Rhythm
Regular rhythm New arrhythmia with ≤ 6 skipped beats or irregular beats/min
New or different arrhythmia with >6 skipped or irregular beats/min
New or different arrhythmia with rapid rate
Therapist Response
Safe to begin exercise
Ask if taken medica-tion; avoid vigorous exercise; encourage compliance with medication; check at rest again next visit: report to MD if persists
Call MD; do not exercise; ensure plan for medical follow-up
Call MD; arrange for office visit or ER visit immedi-ately; return to bed; continue to monitor until patient under someone else’s care
CARDIOVASCULAR SCREENING AND GUIDELINES
41

42
How
short of breath are you? 0
Nothing at all
1 Very slightly
2 Slightly
3 M
oderately 4
Somew
hat severely 5
Severely 6 7
Very severely 8 9
Very, very severely 10 M
aximally
dy
SP
ne
a S
ca
le
44
Syndrome identification
Risk Factors for Geriatric Syndromes 1
teStS and meaSureS
Short Physical Performance Battery 2Gait Speed 25X Sit To Stand 3Berg Balance Scale 3DGI 3Unilateral Stance (Eyes Open) 3360° Turn 3Functional Reach 4Barthel Index 4Tug 4Mean Arterial Pressure 4
obServational analySiS
Sit to Stand Analysis 5Stand to Sit Analysis 6Standing Postural Control Analysis 6Gait Analysis 7Complex Gait Analysis 8Activity Analysis 9
ot/Pt aSSeSSment
OT Assessment – Medical Necessity and Homebound Status 11OT Assessment – Impairments and Prognosis 12OT Assessment – Impairments and Prognosis 13PT Assessment – Medical Necessity and Homebound status 15PT Assessment – Impairments and Prognosis 16PT Assessment – Impairments and Prognosis 17Improvements in Task Performance 19Ongoing Deficits in Task Performance 20
ot/Pt intervention
Older Adult Strength Training Recommendations 21Gait Training 22Cue Training 22mCIMT 23Training Amplitude In Voice And Movement 23Training Posture Vertical (A/P) 24Changes Related to Foot Orthoses 25OT Treatment Ideas 26PT Treatment Ideas 27Go-To Tasks 28
table of contentS
b
How
short of breath are you? 0
Nothing at all
1 Very slightly
2 Slightly
3 M
oderately 4
Somew
hat severely 5
Severely 6 7
Very severely 8 9
Very, very severely 10 M
aximally
dy
SP
ne
a S
ca
le
44
Syndrome identification
Risk Factors for Geriatric Syndromes 1
teStS and meaSureS
Short Physical Performance Battery 2Gait Speed 25X Sit To Stand 3Berg Balance Scale 3DGI 3Unilateral Stance (Eyes Open) 3360° Turn 3Functional Reach 4Barthel Index 4Tug 4Mean Arterial Pressure 4
obServational analySiS
Sit to Stand Analysis 5Stand to Sit Analysis 6Standing Postural Control Analysis 6Gait Analysis 7Complex Gait Analysis 8Activity Analysis 9
ot/Pt aSSeSSment
OT Assessment – Medical Necessity and Homebound Status 11OT Assessment – Impairments and Prognosis 12OT Assessment – Impairments and Prognosis 13PT Assessment – Medical Necessity and Homebound status 15PT Assessment – Impairments and Prognosis 16PT Assessment – Impairments and Prognosis 17Improvements in Task Performance 19Ongoing Deficits in Task Performance 20
ot/Pt intervention
Older Adult Strength Training Recommendations 21Gait Training 22Cue Training 22mCIMT 23Training Amplitude In Voice And Movement 23Training Posture Vertical (A/P) 24Changes Related to Foot Orthoses 25OT Treatment Ideas 26PT Treatment Ideas 27Go-To Tasks 28
table of contentS
b
42
DY
SP
NE
A S
CA
LE
4343
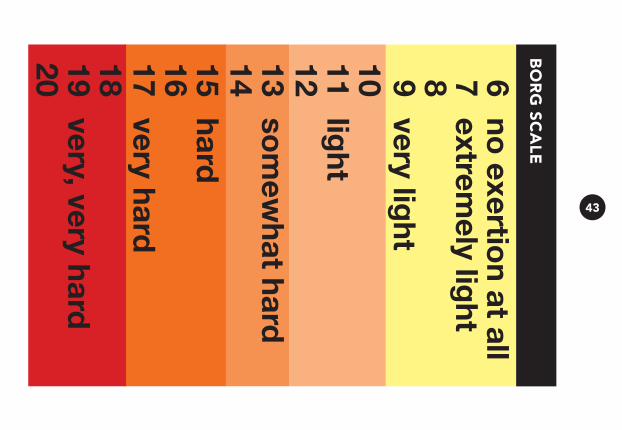
BO
RG
SC
ALE

44
NOTES

45
Not for external distribution - Reference tool only
We accept patients for care regardless of age, race, color, national origin, religion, sex, disability, being a qualified disabled veteran, being a qualified disabled veteran of the Vietnam era, or any other category protected by law, or decisions regarding advance directives. © 2017 Kindred Healthcare Operating, Inc. CSR 191459-01, EOE













![[Critica] Apple's Weakness](https://img.dokumen.tips/doc/110x75/54b2dc494a7959d10e8b456b/critica-apples-weakness.jpg)