Embed Size (px)
Citation preview

ANTI-GBM DISEASE-From Discovery to Cure:
50 years of Progress
Richard J. Glassock, MD, MACPGeffen School of Medicine at UCLA
2nd Annual Renal Conference-Brugge, 2018March 16, 2018

THE DESCRIPTION OF ANTI-GBM DISEASE IN ANTI-GBM DISEASE IN
HUMANS

DESCRIPTION OF ANTI-GBM DISEASE IN HUMANS
(J Exp Med, 1967)

ANTI-GBM DISEASE IN HUMANS(Lerner, Glassock and Dixon, J. Exp Med,1967)
� 250 sera from 50 intact and 25 bilaterally nephrectomized patients (47 had GN; 6 with Crescentic GN- 2 had pulmonary haemorrhage)
� GBM solubilized by collagenase used as target � GBM solubilized by collagenase used as target antigen. Antibody tested by Ouchterlony double-diffusion in gel and by indirect IF using normal human kidney
� Eluates of IgG from diseased kidney prepared by 0.02M Citrate buffer
� Passive transfer of eluted antibody (IgG) into uni-nephrectomized squirrel monkeys

ANTI-GBM DISEASE IN HUMANS(Lerner, Glassock, Dixon, 1967)
� 2 of 23 nephrectomized and 0 of 47 intact patients with GN had precipitating antibody to collagenase GBM digests
� Eluates of 13 kidneys (2 with pulmonary haemorrhage) were studied. 2 patients (both with crescentic GN and linear IgG/C3 studied. 2 patients (both with crescentic GN and linear IgG/C3 deposition, one with pulmonary haemorrhage) had IgG in eluates reactive with GBM collagenase antigen in vitro
� Passive administration of eluted IgG with anti-GBM activity from 2 cases produced acute GN in uni-nephrectomised squirrel monkeys.
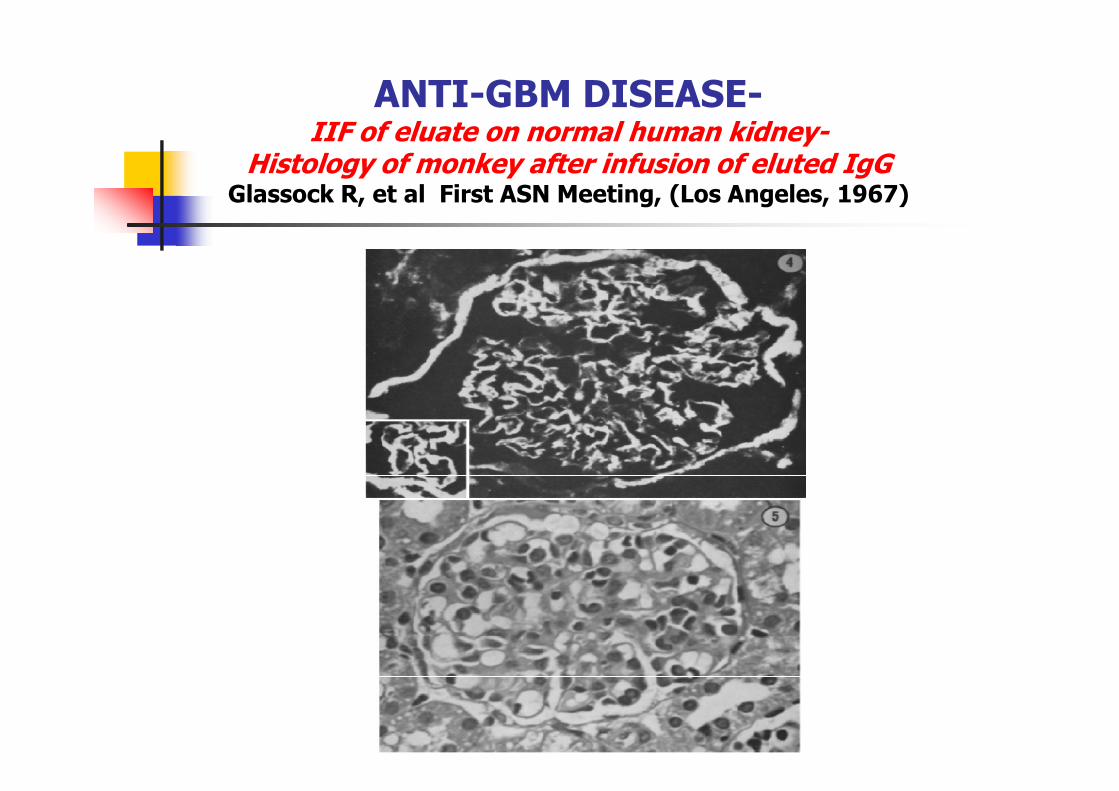
ANTI-GBM DISEASE-IIF of eluate on normal human kidney-
Histology of monkey after infusion of eluted IgGGlassock R, et al First ASN Meeting, (Los Angeles, 1967)

ANTI-GBM DISEASE IN HUMANS: The Case of G.L.
Witebsky’s Postulates for Auto-Immunity Fulfilled
� 29 year old male with rapidly progressive crescentic GN and ESRD. Bilateral nephrectomy performed pre-allo-transplantation(living related donor- sibling). Linear IgG deposition.
� IgG (radiolabeled) obtained from serum (post-nephrectomy; pre-transplant)� IgG (radiolabeled) obtained from serum (post-nephrectomy; pre-transplant)
bound specifically to monkey kidney in-vivo
� Pre-implantation transplant biopsy negative for IgG and C3; post-implantation biopsy (at 75 minutes) positive for linear IgG and C3
� Injection of 500mg of IgG from serum (containing about 1mg of anti-
GBM antibody) produced acute GN with proteinuria/hematuria in 2
uni-nephrectomized squirrel monkeys. Linear deposition of IgG and C3 shown

ANTI-GBM DISEASE IN HUMANS-HUMANS-
POST-1967

Important Developments in 1970’s-1980’s
� Description of a sensitive and specific immunoassay (RIA) for anti-GBM antibodies using collagenase solubilized GBM antigen GBM antigen (Wilson CB and Dixon, FJ, KI, 1973)
� Description of antibody-independent, T-cell dependent actively induced anti-GBM disease in bursectomized chickens (Bolton WK,
et al JCI, 1984, 1988)

Anti-GBM Disease: Pathogenesis – Circa 1980
(simplified version)
Auto-antibody to GBM auto-antigens (“trigger” +
genetic susceptibility)
Anti-GBM antibodies bind to Anti-GBM antibodies bind to
GBM auto-antigens in situ
Complement activated (solid phase)
Leucocyte/ROS mediated injury
Focal gaps/discontinuities in GBM
Fibrinogen in Bowman’s Space; Crescents Develop
ANTI-GBM DISEASE IN HUMANS-1980-2018
� The molecular nature of the GBM antigen (COLIVa3-NC1 domain) and the responsible epitopes defined; genetic predisposition to disease (HLA-based) delineated
� Roles of complement, neutrophils, monocytes and T-cells elucidatedelucidated
� Accurate, sensitive and reliable (ELISA) assays for circulating anti-GBM antibodies developed using recombinant antigens
� Clinical description of the essential features, spectrum and natural history of anti-GBM disease described
� Non-IgG and monoclonal antibody forms of anti-GBM described; Dual ANCA + Anti-GBM antibody disease delineated
� Secondary forms of anti-GBM antibody disease described
� Effective treatments for anti-GBM disease (immunosuppression plus plasma exchange) discovered and applied

MODERN CLASSIFICATION OF ANTI-GBM DISEASE- I
� “PRIMARY”� With Nephritis and Pulmonary hemorrhage (“Goodpasture’s disease”)
With Nephritis but without Pulmonary hemorrhage� With Nephritis but without Pulmonary hemorrhage
� With Nephritis and Combined with ANCA-associated vasculitis (with or without pulmonary hemorrhage)
� Without nephritis but with pulmonary hemorrhage (“IPH”)

MODERN CLASSIFICATION OF ANTI-GBM DISEASE- II
� SECONDARY
� Monotypic antibody and B-Cell neoplasia (IgA1-kappa directed to alpha1/2 chains of Collagen Type IV)
� Lung cancer (IgA anti-GBM)� Lung cancer (IgA anti-GBM)
� Post-shock wave lithotripsy; post urinary tract obstruction
� Influenza A2 infection (?)
� Insecticides, hydrocarbons, rapeseed oils (?)
� Anti-lymphocyte Globulin (horse) contaminated with anti-GBM
� Alemtuzumab therapy of Multiple Sclerosis (?co-incidental-HLA)
� Anti-TNF alpha therapy of Rheumatoid Arthritis
� In association with Celiac Disease, Ulcerative Colitis, Bacterial Endocarditis (Staphylococcal)
� IgG4 related disease

CLASSIFICATION OF ANTI-GBM DISEASE- III
� DE NOVO POST-TRANSPLANTATION
� X-linked Alport Syndrome with truncating mutations of COLIVa5
� Autosomal mutations of COLIVa3/4 (?- rare)
� SUPER-IMPOSED ON ANOTHER GLOMERULAR DISEASE
� Membranous nephropathy
� Lupus Nephritis
� ANCA-associated Vasculitis (anti-MPO; Microscopic Polyangiitis)
� ATYPICAL ANTI-GBM DISEASE
ANTI-GBM DISEASE:Secondary to Monoclonal IgA1 kappa
(Fervenza F, et al, AJKD, 1999; Borza DB et al AJKD, 2005)
� Anti-GBM disease in a 54 year old man due to an IgA1-kappa monoclonal protein with anti-GBM reactivity to COLIV alpha ½
� Presented with crescentic GN and Pulmonary haemorrhage and responded to steroid, cyclophosphamide and PLEX
� Later progressed to ESRD and developed a recurrence following renal transplantation (IIF + for
anti-GBM; WB positive for anti alpha ½ antibody; no antibody to COLIVa3NC1 domain)

PULMONARY HEMORRHAGE AND PULMONARY HEMORRHAGE AND GLOMERULONEPHRITIS

ERNEST GOODPASTURE ANDANTI-GBM DISEASE:
A Confusing History of an Inaccurate Eponym
� Ernest Goodpasture (1919) described a single case of fatal pulmonary hemorrhage and nephritis in a 19 year old man (during the influenza pandemic)
Stanton and Tange (1958) first applied the eponym of � Stanton and Tange (1958) first applied the eponym of Goodpasture syndrome to cases of glomerulonephritis associated with pulmonary haemorrhage (aka Lung purpura with nephritis)
� Only a fraction of the cases of Stanton and Tange likely had anti-GBM disease and the case of Goodpasture (1919) had pulmonary vasculitis and a splenic vasculitic granuloma(Granulomatous Polyangiitis)

ERNEST WILLIAM GOODPASTURE, MD

“Doctor Goodpasture stated (in 1960) that the use of his name for the syndrome (of
pulmonary hemorrhage and pulmonary hemorrhage and glomerulonephritis) was inappropriate, in that
he was attempting to discern the cause of influenza rather than to establish any link
between lung and kidney disease”
(From Collins RD; Ernest William Goodpasture- scientist, scholar, gentleman.Hillsboro Press,2002)

Anti-GBM Disease:Definitions- 2018
� Goodpasture Syndrome= Glomerulonephritis with Pulmonary (Alveolar) Hemorrhage (of any cause)
� Anti-GBM Disease= Glomerulonephritis, with or without Pulmonary (Alveolar) Hemorrhage, due to anti-GBM auto-antibodies

The Serological Findings in 88 Patients with Pulmonary Hemorrhage and Nephritis
(Goodpasture Syndrome)(Niles JL, et al Arch Intern Med 1996; 156:194-198)
30%
55%
7%
8%
ANCA Only Anti-GBM Only
ANCA + Anti-GBM No ANCA or Anti-GBM

Pulmonary Hemorrhage and “Glomerulonephritis”
(Goodpasture Syndrome)
� About 15% will have anti-GBM disease (with or without ANCA; 55%+ will have ANCA only and 30% will have other diseases
� Pulmonary hemorrhage in anti-GBM is “bland” by broncho-alveolar lavage (like CHF or Mitral Stenosis); hemosiderin-laden alveolar lavage (like CHF or Mitral Stenosis); hemosiderin-laden macrophages are common but non-specific. kCO is elevated. Chest-Xray and CT show alveolar infiltrates (no cavitation), in a butterfly pattern.
� Lung biopsies show focal and irregular linear deposits of IgGalong alveolar BM (and may be negative if sample size is small)

Pulmonary HemorrhageChest X-Ray
(Courtesy of Fernando Fervenza)

Pulmonary Hemorrhage and “Glomerulonephritis”
� Other non-anti-GBM, Non-ANCA causes� Lupus Nephritis (often with TMA and anti-PLa)
� HIVAN and TMA
� Opana (oxymorphone) Abuse syndrome with atypical HUS� Opana (oxymorphone) Abuse syndrome with atypical HUS
� IgA Vasculitis (HSP)
� Mixed (IgG/IgM)Essential Cryglobulinemia
� Legionella pneumonia (acute interstitial nephritis)
� Disseminated cryptococcosis (HIVAN)
� Collapsing FSGS
� Chemical injury and ATN
� “Uremic Pneumonitis”, pulmonary emboli, anti-coagulant overdosage, CHF
� Drug hypersensitity
Classical Anti-GBM Antibody Disease:
Defining Characteristics-2018
� Glomerulonephritis- most often of the necrotizing and crescentic variety, but focal and segmental GN and rarely membranous GN can occur. Ultra-Linear deposits of IgG (or IgA) along GBM and Alveolar BM (rarely choroid plexus). Granulomas are not seen, but giant-cells may form in Bowman’s space. C3 is deposited in a less-linear pattern; C1q deposits are less frequently observedless frequently observed
� Pulmonary (Alveolar) Hemorrhage- either overt or covert, of a “bland” non-inflammatory form is variably observed (30-60%)- often precipitated by a lung infection, cigarette smoking, cocaine inhalation, exposure to pulmonary toxins (e.g. volatile hydrocarbons)
� Circulating Auto-antibodies (IgG1,3 or 4 or IgA1) directed to conformational or quaternary epitopes on the non-collagenous (NC-1) domains of the alpha 3 (or 4 or 5) chains of type IV Collagen. Anti-neutrophil cytoplasmic auto-antibodies (typically anti-MPO can co-exist in 20-40%)

Anti-GBM Disease: Other Features
� Two age peaks -20-30 years (M>>F) with pulmonary hemorrhage; 50-70 years (F>M) without pulmonary hemorrhage-
� Iron-deficiency anemia - (low serum Fe, low MCV)- seen in covert or overt Pulmonary hemorrhage
� Elevated pulmonary diffusion tests (DLCO) – increased single breath CO uptake seen in overt or covert pulmonary hemorrhage (Hgb in alveoli)
� Systemic symptoms -usually mild- no fever, arthralgias, skin rash. TTP or atypical HUS co-existing is rare, except in IgA anti-GBM
� Seasonal distribution (Spring-Summer)- “Mini”-epidemics. General incidence=1-3 pmpy, varies by geography
� Blood pressure normal or only mildly elevated; nephrotic syndrome very uncommon
� Serum C3/C4, WBC, platelets normal

Spatial Clustering of Anti-GBM in Ireland
(Canney M, et al CJASN 2016; 11:1392-1399)



Anti-GBM Antibodies
� Typically IgG1 or IgG3-subclass (98%); rarely IgA1 (polyclonal or monoclonal) or IgG4 subclass
� Associated with co-existence of ANCA (10-40%)
� Can follow elevated ANCA (and SVV) by months or � Can follow elevated ANCA (and SVV) by months or years
� Usually abrupt onset of positive tests; self-limited
� Best commercial assays are ELISA using sheep, bovine or recombinant human NC-1 alpha3 chain of Type IV Collagen- 95%+ sensitive/95-99% specific. WB may be more sensitive, but not practical for routine use
� False negative ELISA in IgG4-disease or with anti-alpha1/2 (Ohlsson S, et al AJKD, 2014)
Combined Anti-GBM and ANCA+ Glomerulonephritis
� Tendency to occur in older subjects; females>males
� About 20-40% of Anti-GBM antibody + patients will also have pANCA+ (typically anti-MPO+ (87%); occasionally cANCA+ and anti-PR3+ (13%)anti-PR3+ (13%)
� Prognosis is worse than ANCA+ alone-closely resembles anti-GBM+ alone; but may respond to treatment better than pure anti-GBM (?)
� About 40-50% have concomitant Pulmonary Hemorrhage. Systemic symptoms (rashes, fever, ENT) more common than in anti-GBM only

NATURAL HISTORY OF ANTI-GBM ANTIBODIES
� Usually abrupt onset, peaks at time of presentation
� Without treatment titers gradually decline and are typically negative in 6-9 months, rarely longer
� With adequate treatment (steroids, CYC, PLEX) titers decline rapidly and are typically negative in a few weeks to 2 months
� Relapses of antibody production are very un- common
� Anti-GBM antibody production in classical disease is usually self-limited

RATE OF DISAPPEARANCE OF ANTI-GBM ANTIBODY WITH AND WITHOUT PLEX THERAPY
(Savage COS, et al BMJ 1986; 292:301)

The Broad Spectrum of Anti-GBM Diseases
� Classic anti-GBM Disease; including Goodpasture Syndrome and combined anti-GBM + ANCA disease
� De Novo Anti-GBM disease post-transplant in patients with X-linked Alport Hereditary Nephritis (due to large deletion mutations linked Alport Hereditary Nephritis (due to large deletion mutations of α3COLIV)
� Anti-GBM disease associated with monoclonal B-cell neoplasia(typically IgA- kappa)
� Secondary Anti-GBM Disease- Post- shock wave lithotripsy; post-obstructive uropathy (rare), drugs, cancer, MS, RA, Lupus, Membranous Nephropathy
� “Atypical anti-GBM disease”- linear IgG on GBM but no circulating anti-GBM antibody

THE NATURE OF ANTI-GBM ANTIBODY AND THE NATIVE ANTIBODY AND THE NATIVE
GBM ANTIGEN

7S
NC1
CP1118229-2
3355
4444
55 33
NC1

NC-1 domain Type IV Collagen-Hexamer Structure
(from Hudson, 2002)

Disassociation of the Hexamer (sulfilimine bonds) Required for aGBM binding
(Hudson B, et al, 2012)

ANTI-GBM DISEASE: The Human Epitope
(Jia X-Y, et al PLoS One 2015: 0123277)
� A 13 mer linear (hydrophobic) sequence of the NC-1 domain of COLIV alpha 3 has been identified as the critical epitope for been identified as the critical epitope for induction of anti-GBM auto-antiboes
� The sequence is ISLWKGFSFIMFT
� The sequence is locate on alpha3 127-148 and sites on the alpha 3 -142, 143 and 145 provide the critical motif for auto-antibody production

Clinical Detection of Anti-GBM Antibodies
� Indirect immunofluorescence using normal human or primate kidney as substrate- 10-20% false negative; occasional false positive- positive in Classic anti-GBM, Alport post transplant and IgA monoclonal anti-alpha1/2
� ELISA or RIA using semi-purified Collagenase digest- 5-10% False � ELISA or RIA using semi-purified Collagenase digest- 5-10% False negative; rare false positive
� ELISA using sheep or recombinant NC-1 COLIV alpha 3- <5% false negative; rare false positive
� Western Blot with purified human GBM- false negative and false positive tests very uncommon
� Rarely anti-GBM antibody will be IgG4 subclass- undetectable in conventional ELISA assays- antibody directed to quaternary epitopes on intact hexamer. Anti-GBM anti-body in Alport syndrome directed to un-disassociated hexamer (alpha 4/alpha 5)

“Atypical anti-GBM Disease”(Nasr SH, et al Kidney Int 2016; 89:897-908)
� 20 patients with linear IgG/IgA or IgM GBM staining but without diffuse crescents and with negative anti-GBM antibody by ELISA or WB
� Average age 50 years; approximately equal male:female; no � Average age 50 years; approximately equal male:female; no pulmonary hemorrhage. Average Scr=2.1mg/dL. Nephrotic syndrome very common
� 50% had monoclonal deposits (7 kappa, 1 lambda)
� IgG4/IgG2 subclass dominated; none IgG3
� LM- Endo-capillary proliferative GN- 45%; MesPGN= 30%; MPGN-15%; FSGS- 10%. Superrimposed Focal crescents/ fibrinoid necrosis in 40% ; Superimposed TMA lesions in 40%3/20 developed ESRD in 1 year; stable or slow progression; 75% treated with IS

Crescentic GN with “Linear” Deposits of IgG but “Negative”
anti-GBM Antibody Assay
� IgG4 or IgA anti-GBM antibody
� Monoclonal IgG or IgA antibody to COLIVa1/2
� Wrong substrate (Bovine GBM vs rHuCOLIValpha3NC
domain)
� End-stage disease with spontaneous decay of anti-GBM antibody
� Lab Error
� Insensitive assay
� Altered affinity of cationic IgG for GBM-- Concomitant DM or Vasculitis
� Anti-GBM antibody to non-Goodpasture epitopes (Alport Syndrome with de novo anti-GBM post transplant)

GENETIC GENETIC SUSCEPTIBILITY

ANTI-GBM DISEASE;Genetic Susceptibility
(Fisher, Pusey, Vaughan and Rees. Kidney Int, 1997)
� Susceptibility- HLADRB1*15, DRB1*04 alleles(same as for MS)
� Neutral- HLA-DRB1*03 alleles
� Protective- HLA-DRB1*07 alleles
� HLA-DR2 haplotype in 80% of patients

ETIOLOGYETIOLOGY

ANTI-GBM DISESASE:Etiology
� The etiology of anti-GBM disease is unknown although an environmental origin is suspected due to its uneven geographic distribution and the occurrence of “mini-epidemics”
� Auto-antigen complementarity (environmental peptides that are � Auto-antigen complementarity (environmental peptides that are the “anti-sense” of the auto-antigen) is involved in disease etiology. Such anti-sense peptides can induce disease in susceptible hosts and anti-idiotypic antibodies in diseased subjects are specific for the auto-antigen (alpha 3 peptide). Such anti-complementary antibodies are identified in humans with anti-GBM disease (see Reynolds J, et al J. Autoimmun 2015; 59:8-18)
� Environmental anti-sense (complementary) peptides to auto-antigens (COLIValpha3 N C-1 domain linear peptide epitope)-cause disease- hypothesis

THERAPY OF THERAPY OF ANTI-GBM DISEASE

PLASMA EXCHANGE IN ANTI-GBM DISEASE-
The Seminal Discovery(Lockwood CM, et al Lancet 1976; 1:711-715)
� 7 patients with anti-GBM disease (5 with Pulmonary hemorrhage) treated with intensive Plasma Exchange (centrifugal method; one plasma volume per day or every other day for up to 14 volume per day or every other day for up to 14 sessions; using fresh frozen plasma as replacement fluid)
� 3 non-oligo-anuric patients recovered ; 4 oligo-anuric patients did not recover despite lowered anti-GBM antibody levels. Pulmonary hemorrhagerapidly resolved in all 5 patients with this finding

Therapy of anti-GBM Disease(Hammersmith Triple Therapy Protocol- 2017-)
� Prednisolone� Methylprednisolone 500-1000mg IV X one dose, start 1mg/kg/d (maximum
60mg/d) of oral prednisolone. Taper oral prednisone weekly to zero by 4-6 months
� Cyclophosphamide� Cyclophosphamide� Oral cyclophosphamide (CYC) 2-3mg/kg/d - 1.5-2.0mg/kg/D if over 55 years;
50% of usual dose if renal function severely impaired. Monitor leukocyte counts weekly
� Discontinue at 3 months- no maintenance therapy required
� Azathioprine (or possibly MMF) may be used instead of CYC in those over 65 years
� Plasma Exchange� 60ml/kg (4L) daily for up to 14 days or until anti-GBM assay negative
� 5% Human Serum Albumin as replacement fluid unless high bleeding risk (e.g. post-renal biopsy)- then use Fresh Frozen Plasma

11--Year Outcome in Year Outcome in Treated AntiTreated Anti--GBM DiseaseGBM Disease
Patient Renalsurvival survival
mmol/L No. (%) (%)
Creat <500 19 100 95
Patient Renalsurvival survival
mmol/L No. (%) (%)
Creat <500 19 100 95
CP1112191-5
Creat <500 19 100 95
Creat >500 13 83 82
Dialysis 39 65 8
Total 71 77 53
Creat <500 19 100 95
Creat >500 13 83 82
Dialysis 39 65 8
Total 71 77 53
Levy et al: Ann Intern Med, 2001Levy et al: Ann Intern Med, 2001

OUTCOMES OF PATIENTS WITH COMBINED ANTI-GBM and ANCA-SVV*
(Levy J, et al Kidney Int 2004; 66:1535-1540-[*treated with P/CYC/PLEX])
Initial Serum Creatinine
# of subjects 1 year patient survival
1 year renal survival
<500µmol/L 7 100% 71%
>500µmol/L 1 100% 0%
Dialysis-dependent 17 35% 0%

Anti-GBM Disease:6 Country Study
(van Daalen EE, et al CJASN. 2018;13 63-72)
� 123 subjects with “linear” IgG on renal biopsy and/or positive serum anti-BM antibody with a clinical presentation “compatible” with anti-GBM diseaseGBM disease
� Serology available for 108/123:
� 49% aGBM only
� 32% aGBM + ANCA (85% anti-MPO)
� 6% ANCA only
� 13% negative for aGBM and ANCA

Anti-GBM Disease: 6 Country Study
(van Dallen, et al. 2018)
� Predictors of a favorable outcome (with treatment)
� High percentage of normal glomeruli
� Lower extent of interstitial cellular inflitrates
� Predictors of a failure to recover (with treatment)
� Dialysis-dependency
� 100% cellular crescents or >50% sclerotic glomeruli
� No effect on recovery or failure to recover (with treatment)
� Age, gender
� Lung involvement
� “Double Positivity”
� Serum Creatinine >5.7mg/dL (not on dialysis; p=0.07)

PREDICTORS OF RENAL AND PATIENT OUTCOMES IN ANTI-GBM DISEASE
(Alchi B, et al. NDT 2015; 30:814-821)
� Retrospective review of 43 patients with anti-GBM disease (34 anti-GBM only; 9 with anti-GBM + ANCA) over 20 years followed at 2 centers in UK
34 (81%) were on dialysis at presentation (late)- 32 (74%) were � 34 (81%) were on dialysis at presentation (late)- 32 (74%) were treated with steroids, CYC and PLEX
� Only Oligo-anuria at presentation was an independent predictor of dialysis dependency at 3 months and patient survival. Older age predicted poor survival but not dialysis dependency. A high percentage of crescents (>75%) added little to prognostication
� Renal biopsy may not be necessary in oligo-anuric patients with serologically proven anti-GBM disease

RELAPSES/RECURRENCES
� Relapses of anti-GBM disease are rare (<5%), once the anti-GBM level has decreased to undectable or very low levels.
� Recrudescence of pulmonary (alveolar) hemorrhage can occur if exposed to pulmonary toxins while anti-GBM levels are falling (e.g-return to smoking habits)
� Low risk (<<5%) of recurrence in renal transplants if anti-GBM levels undetectable or very low and > 6 months from onset (Nephrectomy not needed)

Predicting Outcome in Anti-GBM Disease with PLEX, CYC, Steroid Therapy-
Summary
� Favorable� Serum Creatinine
<5.7mg/dL
Non-oligo-anuric
� Unfavorable� Serum creatinine
>5.7mg/dL and dialysis dependent
� Non-oligo-anuric
� High % normal glomeruli
� Focal lesions only
� Low titer anti-GBM (?)
dependent
� Oligo-anuria
� 100% cellular crescents; advanced glomerulosclerosis/IFTA
� Few normal glomeruli
� High titer anti-GBM (?)

Anti-GBM Disease:Alternative Therapies-Not Usually
Recommended- Limited Data
� Rituximab/PLEX/Steroids –
� MMF/Steroids-
IV CYC/PLEX/steroids-� IV CYC/PLEX/steroids-
� CNI/Steroids-
� Galectin 3 inhibition, CXCR inhibition, IgG peptidase-experimental
� Immuno-adsorption with Fc binding columns-
(* see Syeda UA, et al Semin Arthritis Rheum January 2013; Shah Y, et al. QJM 105:195-197, 2012; ** see Biesenbach P, et al. PLoS One 2014; e103568 )

ANTI-GBM DISEASE-50 YEARS OF PROGRESS
� In approximately a half-century, anti-GBM disease has been transformed from an un-common medical curiosity to one of the best understood of the human auto-immune organ specific (kidney and lung) systemic diseases
� We understand its pathogenesis (but not its etiology), genetic susceptibility, molecular targets, antibody and cellular vectors, clinical and pathological behaviour, natural history, prognostic predictors and treatment.
� If recognized early and treated aggressively it can be “cured” in many instances





















![Crescentic IgA Nephropathy[1][1]](https://img.dokumen.tips/doc/110x75/55cf9903550346d0339b030a/crescentic-iga-nephropathy11.jpg)







