Embed Size (px)
Citation preview
8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 1/14
1
Cardiovascular drugs
Antihypertensive Drugs
Hypertension is a persistent elevation of arterial blood pressure (over 90/140 mm.Hg.), it is the most common
cardiovascular disease and the major factor of many diseases such as coronary artery disease, heart failure, stroke and
renal failure. Hemodynamically, blood pressure is a function of the amount of blood pumped by the heart and the ease
with which the blood flows through the peripheral vasculature.
Drug therapy in hypertension management must be for every individual and adjusted on co-existing risk factors
such as:
1- Degree of blood pressure elevation.
2- Severity of the disease.
3- The presence of underlying other cardiovascular risk factor.
4- Response to the therapy
5- Tolerance to drug induced side effects.
Large % of patients use a combination of 2 drugs at low doses with different mechanism of action, so a
synergestic blood pressure lowering occur with minimal side effects.
Hypertensive-state in human can be created by:
1- Diseases affecting the components of the central and peripheral nervous system that regulate the blood pressure.
2- Diseases of the kidney.
3- Diseases of peripheral vascular network that affect blood volume.
4- Abnormalities of the hormonal systems:
i- Tumors of the adrenal medulla that causes release of large amounts of catecholamines create hypertensive-state
known as pheochromocytoma.
ii- An excessive secretion of aldosterone by the adrenal cortex, often because of adenomas, also produces
hypertensive disorders.
iii- Enhanced adrenergic activity is recognized as a peripheral contributor to essential hypertension.
Antihypertensive agents are classified into:-
Classification of antihypertensive drugs:
1-Sympatholytics:
y Centrally acting drugs.
y Ganglionic blocker drugs.

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 2/14
2
y Adrenergic neuron blocking agents.
y ± Adrenergic blockers.
y ± Adrenergic blockers.
y Mixed , adrenergic blockers.
2- Vasodilators:
y Arterial.
y Arterial and venous.
3- Calcium channel blockers.
4-Angiotensin converting enzyme inhibitors.
5-Angiotensin receptor blockers.
I- Adrenergic system inhibitors
Drugs that reduce blood pressure by depressing the activity of the sympathetic nervous system have been used as
effective agents in the treatment of hypertension. This can be accomplished by several ways:-
a) Depleting the store of neurotransmitters:-
Rauwolfia Alkaloids (Reserpine)
Reserpine replaces or depletes catecholamines and serotonin from central and peripheral neurons, by inhibiting
the active transport of ATP-Mg2+-dependent uptake mechanism responsible for sequestering NE and dopamine into the
neuronal granules and the depleted catecholamines are metabolized by MAO causing reduction of amine content. This
leads to presence of a minimal amount of neurotransmitter, so adrenergic transmission is inhibited and the sympathetic
tone is decreased leading to vasodilatation.
It is effective orally and parenterally for the treatment of hypertension.
b ) Reducing the number of impulses traveling in the sympathetic nerves.
Guanethidine and related compounds:
Guanethidinemonosulfate ( Ismelin ):-
[2-(Hexahydro-1(2H)-azocinyl) ethyl] guanidine N
HN NH
NH2

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 3/14
3
Guanethidine has been classified as an adrenergic blocking agent because it can prevent the release of
norepinephrine from post ganglionic neurons in response to adrenergic stimulation. Guanethidine and other compounds
have other action on the catecholamine metabolism and cause significant depletion of these amines in the adrenergic
neurons. They do not interfere with the release of epinephrine from the adrenal medulla.
c- Selective 1-antagonists.
Selective 1-antagonists are effective antihypertensive agents. They act through:
y Production of peripheral vasodilatation by inhibiting post synaptic 1 receptors in vascular smooth muscle, so
results in blocking the vasoconstricting effect on the smooth muscle
y It does not interfere with the activation of 2-receptors on the adrenergic neurons which when activated inhibit
further release of norepinephrine.
Doxazosin ( Cardura )
Prazocin ( M inipr ess )
Terazocin ( Hyt r ine )
N
N N
N
H3CO
H3CO
NH2
O
O
O
Doxazosin: 1-(4-Amino-6,7-dimethoxy-2-quinazoliny)-4-(1,4-benzodioxan-2-ylcarbonyl)piperazine
N
N N
NO
H3CO
H3CO
NH2
O
N
N N
NO
H3CO
H3CO
NH2
O
Prazosin Terazosin
Therapeutic applications includes:
1- They are effective for the initial management of hypertension.
2- They possess a characteristic ³ first dose´ effect which means the occurrence of orthostatic hypotension that
frequently occurs with the first few doses. This side effect can be minimized by taking first few doses at bedtime.

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 4/14
4
Side effects:
1- Most common side effects id due to 1 blocking effect, this includes dizziness, orthostatic hypotension, nasa
congestion, headache and reflux tachycardia.
2- Fluid retension is a problem that can be solved by using diuretics.
d) Centrally acting adrenergic drugs (Selective 2-agonist)
The use of 1 blockers that directly affect the peripheral component of the sympathetic nervous system represents an
important approach to the treatment of hypertension.
A second approach to modify sympathetic influence on the cardiovascular system is through inhibition or reduction
of the CNS control of blood pressure. Several widely used medications act by stimulating 2-receptors which reduce the
sympathetic outflow to the cardiovascular system and produce a hypotension effect.
Mechanism of action:
1- They block sympathetic activity by binding and activating 2 receptors, which reduces sympathetic outflow to
the heart, so as a result decreases cardiac output by decreasing the heart rate and contractility.
2- The reduced sympathetic output to the vessels decreases sympathetic vascular tone, which causes vasodilatation
and reduces systemic vascular resistance which in turn decreases arterial pressure.
i. Clonidine Hydrochloride ( Cat a pr es ), Guanabenz ( Wytensin ), Guanfacine ( Tenex ).
N
HN
NH
Cl
Cl
H
Clonidine: [(2,6-Dichlorophenyl)imino]imidazolidine HCl
.HCl
Cl
Cl
N
HN NH2
Cl
Cl
HN NH2
NH O NH
Guanabenz Guanfacine

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 5/14
5
Uses:
They are used in the management of mild to moderate hypertension. They are used in combination with other
hypotensives and diuretics so decrease dose needed and hence adverse effect while maintaining blood pressure
control.
Metabolism:
They are metabolized by glucuronide and sulphate conjugates, in addition guanafacine has additional mercapturic
conjugates.
ii. Methyldopate Hydrochloride (Aldomet ester Hydrochloride)
L--3-(3,4-Dihydroxyphenyl)-2-methylalanine ethyl ester Hydrochloride
HO
HO
H2
C C
NH2
CH3
COOC2H5
.HCl
Methyldopate hydrochloride
Mechanism of action:
The parent compound -methyldopa was found to be an inhibitor of dopa decarboxylase (L-amino acid decarboxylase, an
enzyme involved in the biosynthesis of NE and epinephrine) and the compound found to be an effective antihypertensiveagent. Detailed studies, however, showed that its hypertension effect not be explained by the inhibition of dopa
decarboxylase in the peripheral nerves, but it was found also that -methylnorepinephrinedisplaces NE in nerve terminals
and act as a false transmitter.
OH
OH
H2C C COOH
NH2
CH3
L-amino acid
decarboxyase
OH
OH
H2C C H
NH2
CH3
OH
OH
CH C HNH2
CH3
Dopamine
FHydroxylase
HO
Methyldopa E-Methyldopamine E-Methylnorepinephrine
Methyldopate, suitable for oral use, is a Zwitterion and is not suitable enough for parentral use. Masking the
carboxylic acid group solved this problem by formation ethyl ester, leaving the amine free to form water-soluble
hydrochloride salt.
8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 6/14
6
Side effects:
Postural hypotension, sodium and water retension. If a diuretic is used concurrently, tolerance to the
antihypertensive effect of the drug during prolonged used can result.
II-Drugs Acting Directly on Smooth muscle (Vasodilators)
Definition: They are drugs that relax the smooth muscles in the blood vessels, causing the vessels to dilate.
*Dilatation of arterial vessels leads to a reduction in systemic vascular resistance, causing a fall in arterial blood
pressure and hence decrease after load on the left ventricle. It also cause a decrease in oxygen demand so improve th
oxygen supply/demand ratio.
*Dilatation of venous vessels decreases venous blood pressure, so reduce the preload on the heart , decreasecardiac output and edema formation.
These drugs have the ability to reduce arterial smooth muscle tone without interference with the autonomic
enervation. They have also the property of increasing sympathetic reflux activity, causing an increase in heart rate and
cardiac output as well as stimulating renin release from the kidney, which results in increased sodium retention and
expansion of plasma volume. As a result, it is common to co-administer saluretics and -adrenergic blocking agents with
these agents.
Drawbacks of vasodilators:
1- They can lead to mediated reflux stimulation of the heart that leads to increase heart rate.
2- They may cause orthostatic tension on standing.
3- They can lead to renal retension of water and sodium causing increase blood volume and cardiac output.
Members of Directly-Acting Vasodilators:
Hydralazine Hydrochloride (Apresoline)
1-Hydrazinophthalazine monohydrochlorideN
N
HN NH2 .HCl
Hydr l zi Hydr l ride

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 7/14
7
Synthesis:
Hydralazine action appear to be centered on the relaxation of the smooth muscle of the vascular walls especiallyof the arteries with a decrease in the peripheral resistance to blood flow, which is an important consideration in patient
with renal insufficiency.
The mechanism of action is proposed that hydralazine interferes with Ca2+ entry and Ca2+ release from
intracellular stores. It has also been reported that hydralazine causes activation of guanylatecyclase, resulting in
increasinglevels of c-GMP. All of these biochemical events can cause vasodilatation. The diastolic blood pressure usually
is decreased more than diastolic one.
Side effects:
1-Its reduction in blood pressure and peripheral resistance causes a reflex response which is accompanied by
increase in the heart rate, cardiac output and plasma rennin activity. These effects limits its effectiveness.
2-It also causes sodium and water retension with expansion of blood volume which could develop tolerance to its
hypertensive effect during prolonged therapy. So co-administration of a diuretic improves the therapeutic outcome.
Therapeutic applications:
1- It is used in the management of moderate to severe hypertension. It is generally used for patients who fails torespond to any hypertensive regimen.
2- Parenteral hydralazine is used for management of severe hypertension when the drug can not be taken orally
or blood pressure must be lowered immediately.
Metabolism:
It is metabolized by NH2 acetylation or OH of the phenyl ring followed by N- or O- glucuronide conjugation.
NH2NH2
N
NH
O
N
N
OH
POCl3
N
N
Cl
N
N
HN NH2
.HCl NH2NH2
O
O
OH

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 8/14
8
Sodium Nitroprusside (Nipride)
Sodium nitroferricyanide, disodium pentacyanonitrosyle
ferate Na2[Fe(CN)NO].
Sodium Nitroprusside is one of the most potent blood pressure lowering drugs. Its use is limited to hypertensive
emergencies because of its short duration of action. The drug differs from other vasodilators in that vasodilatation occurs
in both venous and arterial vascular vessels.
Its therapeutic solution must be protected from light to avoid degradation which can also be catalyzed by trace
metals such as iron and copper. This leads to release of cyanide so any change in color is a sign for degradation.
Mechanism of action:
1- Its hypotensive effect is due to the formation of nitric oxide (NO) in situ that binds to protein receptors in the
cell wall which finally leads to activation of guanylylcyclase that elevates the cellular levels of cGMP.
2- It also inhibits the aggregation of platelets so keeps inappropriate clotting from interfering with blood flow.
3- It is inactive drug till it is metabolized to its active form, NO, which activates guanylatecyclase leading to
increase level of cGMP formation. This action triggers vasodilation of both arterioles and veins.
4- NO also activates K + channel which leads to hyperpolarization and relaxation.
Therapeutic application:
*IV infusion is used in hypertensive crises and emergencies and is useful when other drugs have failed.
*It may be used in management of acute conjestive heart failure.
*Its use is augmented by concomitant use of other hypotensive agents and is not blocked by adrenergic blockers.
Metabolism:
Sodium Nitroprusside is metabolized by the liver to its active metabolite, nitric acid and to cyanide which is
rapidly converted to thiocyanate by the action of sulfurtransferase. Because thiocyanate is excreted by the kidneys, patient
with impaired renal function may suffer from thiocyanate toxicity as it is neurotoxic and inhibits both uptake and binding
of iodine producing symptoms of hypothyrodism.
Side effects of directly-acting vasodilators:
1-They cause sodium and water retention so require co-administration of diuretics.
2-They cause reflux tachycardia so co-administrated with -blockers.
Fe
CN
CNNC
CN
CN
ON
-2
.2H2ONa2
Sodium Nitroprusside

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 9/14
9
3-They produce accumulation of cyanide which binds to haemoglobinproducing methemoglobinemia
4-It can bind to vitamin B6 and interfere with its distribution and metabolism.
III-Potassium channel agonists
Mechanism of action:
These drugs are called potassium channel opener. They activate ATP sensitive potassium channel in the vascular
smooth muscles (VSM) which lead to increase efflux of K + ion to the cells, in addition to decrease in the intracellular
calcium and reduce excitability of smooth muscles. The increased efflux of potassium from the cell results in
hyperpolarization of the membrane and hence decreased excitation.
With less calcium available to combine with protein so less phosphorylation of myosin light chains occurs leading
to relaxation and vasodilatation.
Diazoxide (Hyperstate IV)
Sodium 7-Chloro-3-methyl-2H-1,2,4-
benzothiadiazine1,1-dioxide
Diazoxide is a non diuretic hypotensive agent, it also has hyperglycemic activity. Although it is structurally
related to thiazide diuretics, it causes sodium and water retension with decrease in urinary output which can result inexpansion of plasma and extracellular fluid volume, edema and conjestive heart failure especially with prolonged
administration.
Mechanism of action:
It is suggested to act by
1-depleting an intracellular pool of Ca2+, inhibiting the release of Ca2.
2-It prolongs the opening of K
+
channel sustaining greater vasodilation on arterioles than in veins.
3-It causes increase in blood glucose level by inhibit insulin secretion, and increase hepatic release of glucose.
Therapeutic application:
1-IV drug is used in emergencies which need urgent decrease in diastolic pressure especially in adults with severe
hypertension, and with children with acute severe hypertension.
N
N
O
S
O
CH3
Na
Sodi iazoxide
Cl

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 10/14
10
2-It is taken orally in management of hypoglycemia caused by hyperinsulinism with inoperable islet cell
adenoma, or carcinoma or extrahepatic malignancy in adults.
Minoxidil (Loniten)
2,4-Diamino-6-piperidinopyrimidine-3-oxide
Minoxidil has antihypertensive properties similar to those of hydralazine. It and its active metabolite causes direct
vasodilatation effect on VSM. It used in sever hypertension that is difficult to control with other agents. It is reported that
the drug has effect on androgenic alopecia. Its sodium and water retension can be reversed by the use of diuretic.
N
N NH2H2N
N
O
Mi i il(I active)
N
N NH2H2N
N
Mi i il lf ate (Active)
Sulf tr ansf er ase
SO3
Therapeutic application:
1- It is effective as arterial dilator so they are not the first line of treatment because of its side effect. It is only used
in emergencies
2- It is used with - blockers to avoid tachycardia and with diuretic to avoid water and salt retension.
3- It is used topically to stimulate regrowth of hair in patients suffering from androgenic alopecia.
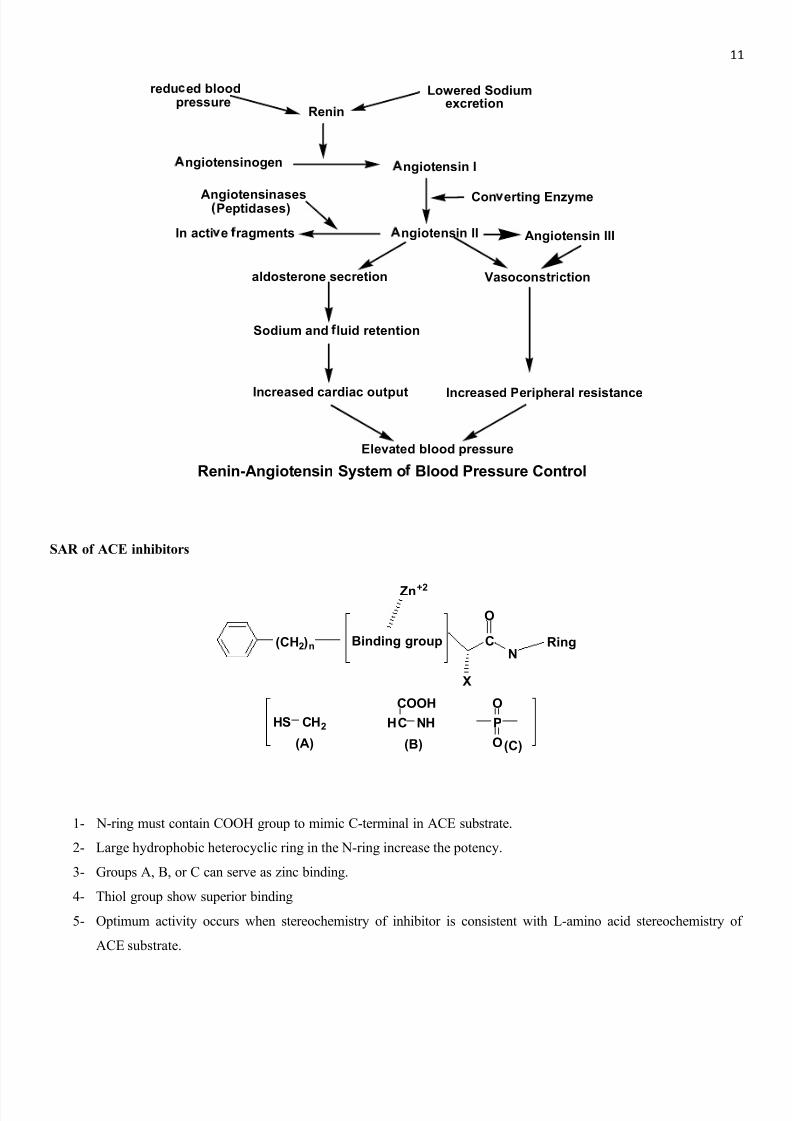
VI-Angiotensin Converting Enzyme Inhibitors (ACEI)
Renal hypertension is controlled by renin angiotensin systems, and the following scheme shows the role of
angiotensin converting enzyme in the formation of angiotensin II and initiation of aldosterone secretion from adrenal
cortex. Thus, drugs capable of inhibiting the action of the converting enzyme will lead to vasodilatation.
8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 11/14
11
r edu ed blood pr essur e
Renin
Lower ed Sodium excr etion
ngiotensinogen ngiotensin I
ngiotensin II
Con erting Enzyme
In acti e r agments
Angiotensinases Peptidases)
Vasoconstrictionaldosterone secr etion
Renin-Angiotensin System o Blood Pr essur e Control
Sodium and luid r etention
Incr eased Peripher al r esistanceIncr eased cardiac output
Elevated blood pr essur e
Angiotensin III
SAR of ACE inhibitors
(CH2)n Binding group
Zn+2
CN
Ring
X
O
HS CH2
(A)
HC NH
COOH
P
O
O(B) (C)
1- N-ring must contain COOH group to mimic C-terminal in ACE substrate.
2- Large hydrophobic heterocyclic ring in the N-ring increase the potency.
3- Groups A, B, or C can serve as zinc binding.
4- Thiol group show superior binding
5- Optimum activity occurs when stereochemistry of inhibitor is consistent with L-amino acid stereochemistry of
ACE substrate.

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 12/14
12
Captopril ( Ca poten ):-
1-[(2S)-3-Mercapto-2-methyl-1-oxopropionyl]L-proline
N SH
O
CH3
Captopril
COOH
Captopril inhibits the converting enzyme. The important binding points at the active site of ACE are shown in the
following diagram.
SHC C
H
CH3
C
O
N C O
O
Zn+ +XH
The use of captopril is associated with undesirable side effects such as rashes and loss of taste. The side effects
similarly, produced by mercapto-containing compounds.
Enalapril Maleate ( V a sotec ):
1-[ N[(S)-1-Carboxy-3-phenylpropyl]-L-alanyl]-L-proline 1-ethyl ester maleate
N
HN
COOHO
CH3C2H5O O
En l pril
HC
HC
COOH
COOH
Enalapril is a long acting ACEI and requires activation by hydrolysis of its ethyl esters to form diacidenalaprilate.
It is derived from captopril and is free from thiol group thus doesn¶t has the side effects of captopril.

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 13/14
13
V-Angiotensin II receptor antagonists
Angiotensin II receptor was the initial target for developing compounds which could inhibit the rennin-angiotensin
pathway. Efforts to develop Angiotensin II receptor antagonists began in the early 1970s and focused on the peptide based
analogs of the natural agonists.
The prototype compound which resulted from these studies was saralasin, an octapeptide in which the Asp 1 and
phe8 residues of angiotensin II were replaced with sarcosine and N-methyl glycine. These peptide analogs demonstrated
the ability to reduce the blood pressure; however, these compounds lacked the oral bioavailability and expressed
unwanted partial agonist activity. Efforts were made till 1955, approval of losartan, a nonpeptide angiotensin II receptor
antagonist.
Development of losartan
Losartan and a series of imidazole-5-acetic acid are developed as a nonpeptide angiotensin II receptor antagonist.
These compounds were relatively weak antagonists but they don¶t possess the unwanted agonist activity in the peptide
analogs.
N
NN
HNN
N
ClCH2OH
Losartan
Mechanism of action:
The angiotensin II receptor exists in at least two subtypes,
1- Type 1 (AT1): they are located in brain, neuronal, vascular, renal, hepatic, adrenal and myocardial tissues and
mediate the cardiovascular, renal, and CNS effects of angiotensin II. Losartan, Valsartan, irbesartan, and eprosartan
all show selectivity for this receptor subtype. They prevent and reverse all of the known effects of angiotensin II,
including rapid and slow pressor responses, stimulatory effects on the peripheral sympathetic nervous system, CNS
effects, release of catecholamines, secretion of aldosterone, direct and indirect renal effects, and all growth-
promoting effects.
2- Type 2 (AT2): the function of these receptors is not as well characterized; however, they have been proposed to
mediate a variety of growth, development, and differentiation processes.

8/8/2019 1 Anti Hypertensive Agents
http://slidepdf.com/reader/full/1-anti-hypertensive-agents 14/14
14
Structure activity relationships
All commercially available angiotensin II antagonists are analogs of the following general formula.
Acidic gr u
N
N
R
Acidic gr u COOH
HOOC
NHN
N
N
A B C
1- The acidic group is thought to mimic either the Tyr 4 phenol or the Asp1 carboxylate of angiotensin II. Groups capable
of such a role include the carboxylic acid (A), a phenyl tetrazole (B), or phenyl carboxylate (C).
2-
In the biphenyl series, the tetrazole and carboxylic groups must be in the ortho position for optimal activity (theterazole group is superior in terms of metabolic stability, lipophilicity, and bioavailability).
3- The n-butyl group of the model compounds provides hydrophobic binding and most likely mimics the side chain of
Ile5 of angiotensin II.
4- The imidazole ring or an isosteric equivalent is required to mimic the His6 side chain of angiotensin II.
5- Substitution with a variety of R groups including a carboxylic acid, methyl alcohol, an ether, or an alkyl chain is
required to mimic the Phe8 of angiotensin II. all of these groups are thought to interact with the AT1 receptor, some
through ionic or ion-dipole bonds and others through hydrophobic interactions.
V- Calcium Channel Blockers






















![Pharmacology of anti hypertensive agents[For BPT students]](https://img.dokumen.tips/doc/110x75/577dab8a1a28ab223f8c8fe7/pharmacology-of-anti-hypertensive-agentsfor-bpt-students.jpg)






