Embed Size (px)
Citation preview

Knee Osteoarthritis:A Physical Therapist’s Perspective
Ed Mulligan, PT, DPT, OCS, SCS, ATC
Associate ProfessorD t t f Ph i l ThDepartment of Physical TherapyDallas, TX

Knee OA – What it is …
PathophysiologyMechanical biochemical and cellular processes related to progressive– Mechanical, biochemical and cellular processes related to progressive deterioration of cartilage and resulting in the formation of osteophytes
Onset– Primary idiopathic
Age dependent with symptoms rare prior to 5th decade– Secondary to joint instability
Etiology– Exact cause is unknown but several factors such as
heredity trauma and obesity seem to be relatedheredity, trauma and obesity seem to be related

Impact
Most common condition affecting synovial joints worldwide affecting over 20 million Americansaffecting over 20 million Americans
Predicted to have the largest increase in new patients of any disease in the US by 2020– Constitutes 30‐40% of knee pathology
Affects approximately 10% of adults over 5580% have radiographic evidence by 75– 80% have radiographic evidence by 75
US Bureau of Labor Statistics and US National Center for Health Statistics report medical and job related expenses to be between $3‐13 billion/year
Hallmark Signs and Symptoms
Diffuse joint pain that increases with ti itactivity
Increased stiffness with inactivity
Mild to moderate joint effusion and joint line tenderness
Antalgic Gait Pattern

Altman Criteria for Knee OA
Traditional Format Knee pain and radiographic
Classification Tree Knee pain and Knee pain and radiographic
osteophytes and at least 1 of the following 3 items: – Age > 50 years
Knee pain and radiographic osteophytes or
Knee pain and age > 40 yrsAge 50 years – Morning stiffness < 30 min– Crepitus on motion
Knee pain and age > 40 yrs Morning stiffness < 30 min Crepitus on motion
SN 89% SP 88% LR 7 4 LR 13 SN = 89%; SP = 88%; + LR = 7.4; - LR = .13 indicating moderate shift in probability
American College of Rheumatology (1995) based on Altman RD, et al, Arthritis Rheum 29:1039‐1049, 1986

Normal vs. Arthritic
decreased joint space and presence of osteophytesof osteophytes

Kellgren-Lawrence Grading Scale
Based on 4 features joint space narrowing osteophytesp y subchondral sclerosis subchondral cysts subchondral cysts

Kellgren-Lawrence Grading Scale
Grade IDoubtful narrowing of joint space and possible osteophytic lipping– Doubtful narrowing of joint space and possible osteophytic lipping
Grade II– Definite osteophytes and narrowing of joint space
Grade III– Moderate multiple osteophytes, definite narrowing of joint space,
some sclerosis, and possible deformity of bone contour, p y
Grade IV– Large osteophytes, marked narrowing of joint space, sever
sclerosis and definite deformity of bone contoursclerosis, and definite deformity of bone contour

Kellgren-Lawrence Grading Scale
lipping
narrowing
progressionp gScleroisContour changes
I IVIIIII

Co-morbidities of Patients with Knee OA
Approximately 80% of these patients have at least one additional musculoskeletal (MSK) and one non MSK coadditional musculoskeletal (MSK) and one non‐MSK co‐morbidity
Most common non‐MSK co‐morbidities– Cardiovascular (8x more likely)– Endocrine (5x more likely)
l– Gastrointestinal– Respiratory
Chan KW, et al, Hong Kong Med J, 2009

How it’s managed
Pharmacological Treatment Physical Therapy1 S l
Surgical Intervention1. Symptom control2. Psychosocial 3. Education4. Unloadingg5. Mobility6. Flexibility7. Strength

Oral NSAIDs including Cox-2 inhibitors Opioids
adapted from Porcheret, M. et al. 4 step approach in managing knee pain in older adults. Rheumatology 2007 Clinical Practice Guideline Recommendations
Co b to s
Topical NSAIDs
Op o ds
OTC
Capsaicin
Supports and Braces
Education, Advice, Information Access
St gth i g E i *
OTC NSAIDs
Supports and Braces
Wedged or
TENSDietary
G-CSStrengthening Exercise*Flexibility/ROM Exercise
Low Impact Aerobic Fitness Training*Weight Loss* (if applicable)
IA Cortico-steorid
injections
Wedged or shock
absorbing shoes or
Walking Aids
Weight Loss (if applicable)ThermotherapyAcetaminophen
injectionsinsoles
Acupuncture
IA HyaluronanManual Therapy
Assistive DevicesSurgical Surgical ReferralReferral
Taping
* Most beneficial interventions in combination as recommended by the Ottawa Panel for Evidence Based Practice Guidelines

OA rehabilitation guidelines
Minimize pain and inflammationOTC NSAID /A t i h OTC NSAIDs/Acetaminophen
NSAIDs/COX‐2 Inhibitors Topical NSAIDs/Capsiacin Glucosamine‐Chondroitin Sulfate Corticosteroid IA Injections Viscosupplementation – Hyaluronic Acid Injections Viscosupplementation Hyaluronic Acid Injections
Physical Therapy Modalities

Physical Agents-Modalities
ThermotherapyBoth men and women demonstrated improvement in– Both men and women demonstrated improvement in function but women more likely to experience clinically meaningful improvement in pain and symptoms
Denegar CR Physiother Theory Pract 2012Denegar CR, Physiother Theory Pract, 2012
TENS– Effective at decreasing resting and activity pain (but has
hi h l b t)high placebo component)Vance CG, et al, Phys Ther, 2012

Physical Agents-Modalities
Shortwave DiathermyEffective at decreasing pain as evaluated by high quality trials− Effective at decreasing pain as evaluated by high quality trials
Laufer Y, Osteoathiritis Cartilage, 2012 (Systematic Review)– Diathermy induced hyperthermia beneficial at decreasing pain, self‐report function, and TUG time in RCT
Giombini A, et al, Knee Surg Sport Traumatol Arthrosc, 2011
Cold Laser− Immediate analgesic effect on pain VASg p
Stiglic‐Rogoznica N, et al, Coll Antropol, 2011− Effective in decreasing pain and improving function when combined with exercise therapy
Alfredo PP et al Clin Rehabil 2012Alfredo PP, et al, Clin Rehabil, 2012

OTC Topical Analgesic VarietiesOTC Topical Analgesic Varietiesapplied 3-4 times/day for maximum of 7 days
Counterirritants Salicylates CapsaicinCounterirritantscontains ingredients likementhol and camphor that mask pain by pro‐
Salicylatescontain methyl ortrolamine salicylate that reduce pain by
Capsaicinderived from hot
peppers and reducesthe amount of p y p
ducing a warming or cooling sensation
inhibiting the releaseof prostaglandins
neurotransmitter P
less effective than topical NSAIDs and should only be used as adjunct toless effective than topical NSAIDs and should only be used as adjunct to other interventionsAltman RD, Drugs, 2011

Importance of Psychological Influence
Two variables were significantly associated with treatment response after adjustment for covariates (age sex BMI x-ray severity)response after adjustment for covariates (age, sex, BMI, x-ray severity)
– Self‐report instability• To what degree does buckling, giving g g, g gway, or shift of the knee affect your level of ADL? (KOS ADL question)
Fear Avoidance Behavior– Fear Avoidance Behavior• Physical activity scale score
Fitzgerald GK, et al, Arthritis Care Res, 2012g , , ,

OA rehabilitation guidelines
Patient EducationADL difi ti ADL modifications
Weight Control
Decrease in impact activities Decrease in impact activities Encouragement of adherence
Long‐term HEP and maintenance of active lifestyle i t d ith b tt tassociated with better outcomes
Pisters MF, et al, Arthritis Care Res, 2010
Weight Bearing Assistance Recommendations

Assistive Devices
Cane use can to unload between 10‐30% of body weight when used properly– Correct height
handle level with proximal wrist crease
– Correct placement on uninvolved (or worst) side

Obesity Risk Factor
Overweight (> 30 BMI) women 4x risk for OA Overweight (> 30 BMI) men 5x risk for OA
Weight loss Weight loss– Women with 11 lb loss (approx 2 BMI) had OA risk decrease by 50%
– Men who went from >30 BMI to 26‐29.9 range decreased risk by 21% (women by 33%)
Felson, J Rheumatol, 1995

Weight Reduction Effect on Function
Function– WOMAC score (disease specific outcome measure) improved by 9% for eachimproved by 9% for each % of body fat reduced 28% improvement in function with a 10% reduction in weight
F l J Rh t l 1995Felson, J Rheumatol, 1995

OA rehabilitation guidelines
Alter Applied Forces Orthotic therapy and insoles Footwear Recommendations OA Bracing

Foot Orthoses
Orthotic therapy and insolesvs.
– Pronated feet are more likely in patients with medial compartment OAReilly K, et al, Physiotherapy, 2009
– Medial‐wedge (posted) orthotic insoles decreased pain, altered the tibiofemoral angle, and improved function in patient with valgus induced knee OARodrigues PT, et al, Arthritis Rheum, 2008g , , ,
– Laterally wedged orthoses were of benefit in patients with medial compartment OA in regards to pain during a 6‐min walk test, stiffness, and function (based on the WOMAC outcome tool)and function (based on the WOMAC outcome tool)
Barrios JA, et al, Knee, 2008

Footwear Recommendations
Cushioned midsole Running Shoes
Sturdy heel counter
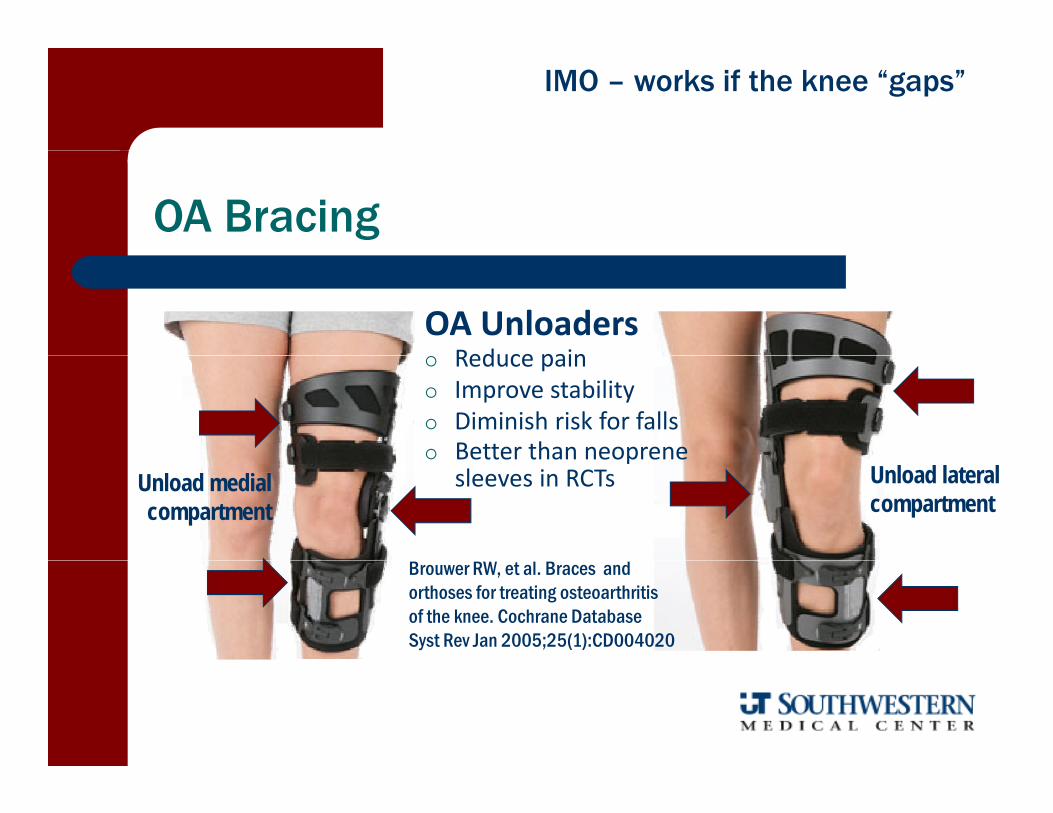
IMO – works if the knee “gaps”
OA Bracing
OA UnloadersReduce pain Reduce pain
Improve stability Diminish risk for falls Better than neoprene
Unload lateral compartment
Better than neoprene sleeves in RCTsUnload medial
compartment
Brouwer RW, et al. Braces and orthoses for treating osteoarthritis of the knee. Cochrane Database Syst Rev Jan 2005;25(1):CD004020

OA rehabilitation guidelines
Improve mobility through manual therapy for h i lthe entire lower quarter Restore normal osteo and arthrokinematic motion at
k d hi j i tknee and hip joints Especially knee extension and hip rotation
ROM No knee supports or bolsters

Need to look proximal and distal to the Knee
Lower Extremity is a kinetic change that is influenced by forces and factors from above and below
Concurrent arthritic change in hip is commonG i l i b d b Gait alterations may be caused by or the result of knee pain

OA h bilit ti id liOA rehabilitation guidelines
Hip Rehabilitation Critical
Significant improvement inSignificant improvement in knee pain and ROM followinghip mobilization interventionp
Cliborne AV, J Ortho Sports Phys Ther 2004
P-A glide Caudal glide
J Ortho Sports Phys Ther, 2004
P-A glide in FABER A-P glide

D l t f Cli i l P di ti R l f b fit Development of a Clinical Prediction Rule for benefit of Hip Mobilization to Treat Knee OsteoarthritisValidation and Impact Analysis to come
1. Hip or Groin Paini hi h i2. Anterior Thigh Pain
3. Passive knee flexion < 122°4 Passive hip int rotation < 17°4. Passive hip int. rotation < 175. Pain with hip distraction
1 positive variable had a + LR of 5 1 with a 92% chance of treatment1 positive variable had a + LR of 5.1 with a 92% chance of treatmentsuccess at 48‐hour follow‐up; 2 positive variables increased + LR to12. 9 and success to 97%Currier LL, et al, Phys Ther, 2007

Manual Therapy
Joint mobilization Soft tissue massage “Hands on” resistive and stretching exercise

Mobilization for pain reduction
MWM (mobilization with movement) and distraction techniques were effective at significantlytechniques were effective at significantly reducing pain levels
Pollard H, J Can Chiropr Assoc, 2008
A/P mobilizations provided significant A/P mobilizations provided significant improvement in pain pressure thresholds
Moss P, Man Ther, 2007
Manual mobilization showed a moderate effect Manual mobilization showed a moderate effect size on pain compared to small effect sizes for strength or exercise therapy alone
Jansen NJ et al J Physiother 2011Jansen NJ, et al, J Physiother, 2011

OA rehabilitation guidelines
Enhance LE flexibility ‐ Hip, knee, and calf

OA rehabilitation guidelines
Improve muscular strength and endurance Particularly the quadriceps and gluteals! Particularly the quadriceps and gluteals!
Quad strength associated with pain levels (but not radiographic severity) Quad strength associated with pain levels (but not radiographic severity)Ruhdorfer et al, Arthritis Care Res, 2014
Hip abductor strengthening did not reduce knee joint loading but did improve function and reduce pain in a group with medial knee OAimprove function and reduce pain in a group with medial knee OA

Does Physical Therapy Work?(more specifically manual and exercise therapy)
Deyle GD, et al. Effectiveness of Manual Physical Therapy and Exercise in Osteoarthritis of the Knee: A Randomized Controlled Trial Ann Intern Med 2000;Osteoarthritis of the Knee: A Randomized Controlled Trial. Ann Intern Med 2000; 132(3):173‐181
Double‐blind RCT with 83 patients with knee OAManual therapy + exercise group (entire LQ)– Manual therapy + exercise group (entire LQ)
– Placebo ultrasound group Treatment group received manual therapy to knee and other
i l iregions, plus exercise Both groups received 8 sessions over 4 weeks Outcome assessed by distance walked in 6 minutes and WOMAC
functional outcome measure

Deyle G, et al, Ann Intern Med, 2000
Manual Therapy +
WOMAC Score Walking Distance
Placebo UltrasoundManual Therapy Exercise
Pl b Ult d
Distance
Manual Therapy + Exercise
Placebo Ultrasound
Combination of manual therapy and supervised exercise yields functional benefits for patients with knee OA and may delay or prevent the need for
surgical interventionAverage distance walked in 6 minutes at baseline, 4 wks, and 8 wks. Among patients who completed the study, those in the treatment group had a greater average improvement in distance walked compared with placebo recipients by week 8
Average WOMAC scores at baseline, 4 wks, and 8 wks.Lower scores indicate perceived improvement in pain, stiffness, and function. Among patients who completed the t d th i th t t t h d t
surgical intervention
distance walked compared with placebo recipients by week 8 (P = 0.001).
study, those in the treatment group had a greater average improvement in WOMAC scores compared with placebo recipients by week 8 (P < 0.001).
Outcomes
Improved function as evidenced by WOMAC and 6‐minute walk test
alsoalso, Likelihood of needing a TKA or injection at 1 year was
– 5% in the manual therapy + exercise group– 20% in the ultrasound placebo control group
– NNT ≈ 7 For every seventh patient treated with MT/TE at least one patient avoided a TKR or injection at one year

What was the therapeutic intervention?
InterventionIntervention FocusFocus
Stretching Calf Hamstrings QuadsStretching Calf, Hamstrings, Quads
ROM Exercise AROM, Manual Therapy, Stationary Bike
Strengthening Quad Isometrics, Terminal Extensions, Leg Press, Mini Squats Step UpsMini‐Squats, Step Ups
In a separate study there was minimal outcome difference between high and low‐resistance training though both interventions were significantly better than no treatmentJan MH, et al, Phys Ther, 2008

One more study …
RCT looking at 8‐week WB exercise NWB iprogram vs. NWB exercise program vs.
control– Equally significant gains in function, muscleEqually significant gains in function, muscle torque, and walking speed in both exercise groupsWB i h d t i t– WB exercise had an even greater impact on knee repositioning ability (proprioception)
Jan MH et al Arch Phys Med Rehabil 2009Jan MH, et al, Arch Phys Med Rehabil, 2009

Arthroscopic Surgery (L d D b id ) Arthroscopic Surgery (Lavage and Debridement) vs.
Physical Therapy and Usual Medical Care
RCT at a 2 year follow‐up– No significant difference in function (WOMAC)– No significant difference in quality of life (SF‐36)
Kirkley A, et al, N Engl J Med, 2008

Aquatic Therapy
Some short‐term benefit in regards to function but no sig‐ifi diff h d l d b d i inificant difference when compared to land‐based training– Generally does not show as much gait or muscle strength
improvement or carryover as land‐based exercise– May have fewer adverse effects and less pain than land‐based
therapy and serve as a satisfactory alternative for those with convenient access
Harmer AR, Arthritis Rheum, 2009Silva LE, Phys Ther, 2008
Lund H, et al, J Rehabil Med, 2008Cochrane Database Sys Rev, 2007
Foley A, et al, Ann Rheum Dis, 2003
Further Endorsements for Exercise Therapy
“Exercise should be a core treatment for people with OA irrespective of age pain severity or disability andOA, irrespective of age, pain, severity, or disability and include both local strengthening and general aerobic fitness components.”
2008 Clinical Practice Guidelines of the National Institute for Health and
Clinical Excellence (NICE) for Osteoarthritis
A di t t l i f RCT L d b d According to a meta‐analysis of RCTs ‐ Land‐based exercise therapy has at least a short‐term benefit in regards to pain and physical disability
l h lFransen M, et al, J Rheumatol, 2009

“Won’t exercise further “wear out” an already damaged joint?”
NOEvidence shows that regular low‐impact exercise in osteo‐arthritic joints does not accelerate the disease process
Kovar PA, et al, Ann Intern Med, 1992Lane NE J Rheumatol 1995Lane NE, J Rheumatol, 1995

Is supervision necessary?
Improvement in Function (WOMAC), Pain, and Stiffness in subjects who had supervised clinical exercise and manual therapy vs. a HEP
First 4 weeks appear to make a substantial difference
o ad supe sed c ca e e c se a d a ua e apy s a
HEP Supervised PT
Even at the 8 week follow‐up the MT and Ex group had significantly more improve‐ment in WOMAC (52% vs. 26%)
Deyle GD, et al. Phys Ther, 2005

Comparison of Interventions from Deyle studies in 2000 and 2005
Placebo
MT
HEP

Intervention Recommendations
Systematic review and Meta‐analysis from 17 international organizations
St l R d d C ti l U t d NOTStrongly Recommended
Recommended Cautiously Recommended
Unsupported NOT Recommended
• Therapeutic Exer• E.Stim/TENS
• WBing Assist• Taping
Ultrasound • Laser• Magnets
Electro‐accupuncture
• Equipment(braces/insoles/shoe wear)
• Education• Manual TherapyW i ht L
• Thermotherapy • Accupuncture• MassageTherapy
• Weight Loss• Hydrotherapy
Larmer PJ, Arch Phys Med Rehab, 2014

How to evaluate the patient’s status
NPRSi l i i l– Numerical Pain Rating Scale
GROCGlobal Rating of Change Patient Satisfaction– Global Rating of Change – Patient Satisfaction
Outcome Tools– LEFSLEFS– WOMAC– KOOS

Surgical Indications
Failure of all conservative measures to alleviate the patient’s pain p pcomplaint that has become disabling and affecting the patient’s quality of life
Roentgenographic evidence that correlates with the clinical presentation
Correction of significant varus/valgus deformity
Findings that correlate with a clear Findings that correlate with a clear clinical impression of knee arthritis.

Total Knee Arthroplasty
Surgical Factors– Prosthetic Design
Uni vs. Tri‐compartmentalMobile Bearing Rotary Platform Degree of Mechanical ConstraintIncisional Approach– Incisional Approach Traditional vs. minimally invasive
– Method of FixationMethod of Fixation Cemented vs. Cementless

Total Knee Arthroplasty
Key Rehabilitative Influences– Age, Overall medical status, and rehabilitation goalsJ i i i– Joint motion prior to surgery
– Pre‐operative muscle strength and enduranceand endurance
– Degree of axial alignment to be corrected

customizing the rehabilitation to the patient’s realistic expectation
Your Mother is making outstanding progress with her knee replacement progress with her knee replacement therapy

weight bearing status and progression
CementedWBAT D 1– WBAT Day 1
– Wean from assistive devices as tolerated
CementlessCementless– Analogous to fracture healing– TDWB first 2‐3 weeks– Week 4‐6: 25‐50% PWB– Week 7‐8: 50‐75% PWB
W k 9 FWB– Week 9: FWB

TKR precautions
• No kneeling or deep squatsi i i l d id• No pivoting on involved side
• No aggressive passive stretching• Maintain neutral hip rotation and maximal knee extension• Maintain neutral hip rotation and maximal knee extension
while in bed• Careful with heavy ankle weights while in sitting distractive
position• Continue avoidance of pivoting and deep knee bending for
first few monthsfirst few months

post-op modalities
TENS/Cryotherapy
Cryocuff (ice‐compression)
NMES to Quadriceps NMES to QuadricepsLevine M, et al, Orthopedics, 2013
Stevens‐Lapsley JE, et al, Phys Ther, 2012Stevens‐Lapsley JE, et al, Phys Ther, 2012
Walls RJ, et al, BMC Musculoskelet Disord, 2010 Meier W, et al, J Orthop Sports Phys Ther, 2008
Hydrotherapy if joint stiffnessy py j

post-op ROM
PHASE IE l i l t ti f CPM Early implementation of CPM– dosage is critical
20‐24 hours per day with at least /d d10‐15° increases in range/day expected
– dosage is not critical – JOSPT25:119‐27, 1997 P/AA/AROM – goal is 90 flexion by day 7
PHASE II Stretching program for all LE muscle groupsg p g g p Soft tissue massage prn

post-op ROM
The principal predictor of post‐op ROM is the pre‐op ROMRitt MA t l J B J i t S 85 A 1278 1385Ritter MA, et al. J Bone Joint Surg 85‐A:1278‐1385
Pre‐operative HEP results in quicker achievement of 90°fl i t d h t h it l tflexion post‐op and a shorter hospital stay
Matassi F et al, Knee Surg Sports Traumatol Arthrosc, 2014

TKR Phase I Strength Training
• Emphasis on Quadriceps– Isometrics with EMS augmentation – Straight Leg Raises – TKEs and Full Arc Quads
• Other Exercises– Hip PREs/Active ROM
H l Slid d A kl AROM– Heel Slides and Ankle AROM
• If cemented, begin CKC activities ‐ 1/4 squats during 2nd wk• Cycling if wound closed and ROM allowsCycling if wound closed and ROM allows

TKR Phase II Strength Training
• Continue PREs• Consider bicycling & swimming program• Consider bicycling & swimming program• Initiate closed kinetic chain activities

TKR Phase III Strength Training
• Maximize muscular strength and endurance based on SAID principle
• Consider walking program
• Initiate balance and proprioceptive training
• Functional Training
• Instruct in maintenance program

Points of Emphasis
Early restoration of motion 0 120 d– 0 – 120 degrees
– Knee flexion ROM at 1‐2 weeks correlates well (p<.0001) with flexion ROM at 7 weeks To achieve > 100° you should have > 80° by end of 2nd wk– To achieve > 100° you should have > 80° by end of 2nd wk
Ebert JR et al, Arch Phys Med Rehab, 2014
Weight Bearing to tolerance Day 1 Control Pain and Swelling Monitor for DVT Complications Effectiveness/Efficacy of CPM is controversial Effectiveness/Efficacy of CPM is controversial

What you’re going to get -happens pretty quickly!
Greatest improvement in f i i fifunction occurs in first 12 weeks
Slower improvement from Slower improvement from 3‐6 months
Little improvement after 6 months
Kennedy DM, et al, Phys Ther, 2008
Questions

Meniscal Injuries of the Knee
Edward P. Mulligan, PT, DPT, OCS, SCS, ATC
Associate ProfessorUT Southwestern School of Health ProfessionsDepartment of Physical TherapyDepartment of Physical TherapyDallas, TX


Meniscal Tears: MOI
Youthful: Acute Trauma Rotational and compressive forces with the
knee partially flexedmenisci are torn (usually longitudinal tears) when– menisci are torn (usually longitudinal tears) when they are caught, pinched, or impaled between the condyles
St i k f t f t t i Strong risk factor of acute tears in soccer, skiing, and rugby players or those who delay ACL reconstruction (for medial but not lateral)
Snoeker BM et al., J Orthop Sports Phys Ther, 2013Frizzerio A, et al, Muscles Tendons Ligaments, 2012

Meniscal Tears: MOI
Elderly: Degeneration Non‐specific trauma with slow, insidious onset
― menisci degenerate as they become less pliable and complex or radial tearing is generally irreparableradial tearing is generally irreparable
60% likelihood of degenerative tear after 60 Risk Factors (Snoeker, JOSPT, 2013)
― > 60― Male― Work‐related stair climbing squatting or kneeling requirementWork related stair climbing, squatting, or kneeling requirement

Meniscal Injury Predisposing Factors
Abnormal mechanical axes / l
discoid lateral i– genu varus/valgus
Congenital anomalies – Discoid menisci
meniscus
Discoid menisci Degenerative menisci Ligamentous laxity

Discoid Meniscus
• Broad, “pancake‐shaped” variant which is thicker 1‐5% incidence in normal knees, 2‐5% in symptomatic knees ~15% incidence in Japanese/Asians
M b i bil t l May be uni or bilateral Lateral >>> medial
• Widened lateral joint space• Cupping of the lateral tibial plateau• Flattening of the LF condyle• Calcification of the meniscus• Calcification of the meniscus

Meniscal Cysts
Represent 1‐10% of meniscal pathologiesi hl l d i h i l Highly correlated with meniscal tears
Most often occur in the lateral meniscus Directly connected to the meniscus Directly connected to the meniscus Symptoms include joint‐pain and palpable mass at or below
the joint line Can often be decompressed arthroscopically when
underlying meniscal lesion is treated

Meniscal Injury Clinical Features
History Trauma ‐ twisting injury Trauma twisting injury Degenerative ‐ no history of specific injury; often
in middle age Mechanical Symptoms Mechanical Symptoms
locking, catching, clicking, snapping, giving way Swelling and Pain
Physical Exam Physical Exam1. Joint line tenderness2. Effusion3 + McMurray's Apley's Squat Thessaly3. + McMurray s, Apley s, Squat, Thessaly4. Quad Shutdown or atrophy

Operative vs. Conservative Management
Small (< 3 cm), peripheral, vertical (< 1 cm), and/or stable tears that are not causing functional limitations maytears that are not causing functional limitations may respond to non‐surgical intervention, remain asymptomatic, or heal spontaneously
Bottom Line– All should have a course of non‐operative management prior
to surgeryto surgery – Exception: large tear with obvious mechanical symptoms– Surgery probably not indicated in those with severely
degenerative knees

Degenerative meniscal tears are like “wrinkles with aging”
Cannot solve with surgeryRisberg MA, editorial comment in Brit J Sport Med, 2014

Meniscal Tears in Degenerative Knees
Frequently co‐exist with osteoarthritisl di h fi d dd d l f Several studies have confirmed no added value of
arthroscopic debridement of degenerative joints– Studies excluded patients with large meniscal tearsStudies excluded patients with large meniscal tears – Likely no benefit of arthroscopy in patients without mechanical symptoms
Moseley et al, N Eng J Med, 2002Kirkley et al, N Eng J Med, 2008

A th i i t i i Arthroscopic menisectomies in patients with OA over 45
No difference in outcomes at 6‐12 months for those who had surgery vs a structured rehabilitation programhad surgery vs. a structured rehabilitation program
Limitations¾ f li ibl bj t d li d ll t– ¾ of eligible subjects declined enrollment
– 30% crossover between groups (most converted to surgery)(most converted to surgery)
Katz JN, et al, N Eng J Med, 2013
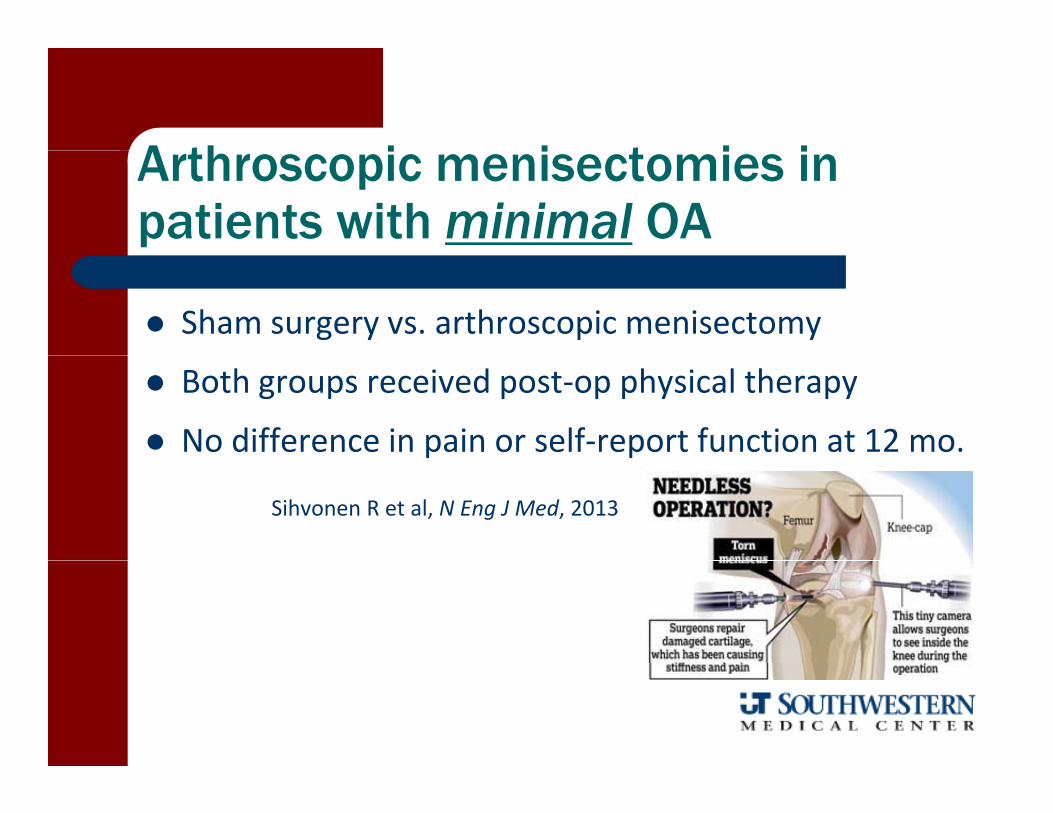
A th i i t i i Arthroscopic menisectomies in patients with minimal OA
Sham surgery vs. arthroscopic menisectomy
Both groups received post‐op physical therapy
No difference in pain or self‐report function at 12 mo.p p
Sihvonen R et al, N Eng J Med, 2013

Meniscal Surgical Options
Partial MenisectomyPartial Menisectomy Meniscal Repair M i l All ft Meniscal Allograft

Pro-Active Post-Arthroscopic Knee Rehab
BOTH the surgical procedure and subsequent clinical rehab influences the rate and extent of recovery ‐ Hughston, 1980the rate and extent of recovery Hughston, 1980
The earlier AROM is allowed, the earlier full ROM is achieved ‐Sherman, 1983
Patients need post‐operative PT to normalize motor control, muscular strength, and gait ‐ Durand, 1991 and 1993
Supervised rehab facilitates successful outcomes ‐ Supervised rehab facilitates successful outcomes ‐Moffett, 1994
Early AROM on bike significantly improves gait performance K li 2009performance – Kelin, 2009
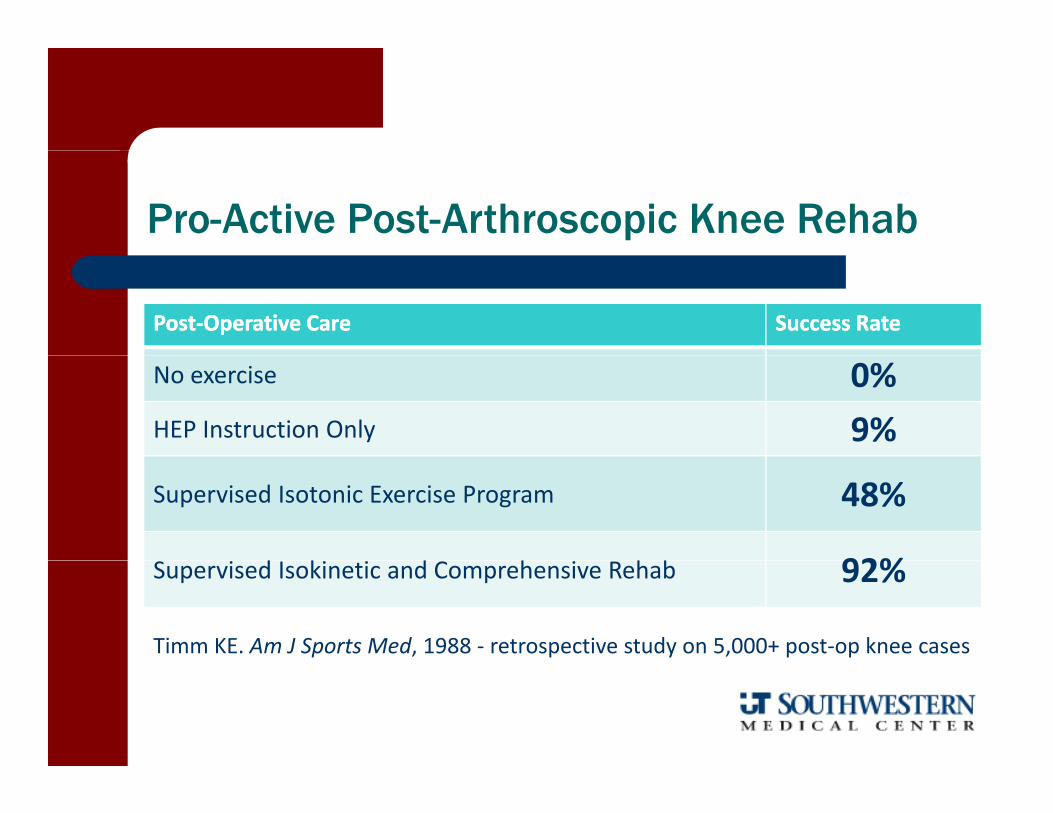
Pro-Active Post-Arthroscopic Knee Rehab
PostPost‐‐Operative CareOperative Care Success RateSuccess Rate
No exercise 0%HEP Instruction Only 9%
Supervised Isotonic Exercise Program 48%
d k d h h b 92%Supervised Isokinetic and Comprehensive Rehab 92%
Timm KE. Am J Sports Med, 1988 ‐ retrospective study on 5,000+ post‐op knee cases

Physical Therapy Effectiveness
PT group showed significantly better results than the control group in regards to patient satisfaction and functional outcomesregards to patient satisfaction and functional outcomes
Vervest et al, Knee Surg Sports Traumatol Arthrosc, 1999
Prospective RCT comparing post‐op medical exercise therapy vs. control showed significantly better outcomes in regards to pain and functionshowed significantly better outcomes in regards to pain and function (KOOS) at 3 month. At one year, exercise group had less anxiety/depression and better strength
Osteros et al, Knee Surg Sports Traumatol Arthrosc, 2014, g p ,
No differences between PT/HEP over 6 weeks and HEP alone in regards to self‐report outcomes, days return to work, gait kinematics, or hop/jump tests
Goodwin PC et al Phys Ther 83:520 535 2003Goodwin PC et al, Phys Ther 83:520‐535, 2003

How long should we see them?
Retrospective review to determine the number of visits to achieve the following minimal functional goalsachieve the following minimal functional goals– Full extension ROM = to uninvolved side– SLR without extensor lag– Normal gait pattern without assistive device– Pedal a stationary bike– Independent in HEPIndependent in HEP
Average of 4 visits over 9 days– Would be interesting to have a control group
( PT i t ti )(no PT intervention)

post-op meniscal rehab considerations
Proactive approach Protected arcs of motion Varus‐valgus stress Rotational torque OKC vs. CKC
i Time to Return– Excisions: 4‐6 weeksRepairs: 4 6 months– Repairs: 4‐6 months

post-op meniscal rehab considerations
Control post‐op pain/swelling FWB when gait normalizes ROM and strengthening to tolerance
Return to activity typically takes k3‐6 weeks

post-op meniscal REPAIR rehab considerations
General Considerations and Influences– Site of repair
Red vs. whiteC l i h l Complex vs. peripheral
– Associated pathologies– AgeAge – Athletic or ADL goals– Surgeon Philosophyg p y

Acutepost-op meniscal REPAIR rehab considerations
Immediate protected motion post‐op (0‐90°for 4 wks)for 4 wks)
Locked in full extension (drop lock) if early weight bearing; FWB at 4‐6 wks
– Radial or complete longitudinal tears may require more conservative ROM and weight‐conservative ROM and weightbearing
Neoprene compression sleeve to minimize swelling and provide supportswelling and provide support

Post-Acutepost-op meniscal REPAIR rehab considerations
Slow, gradual progressions based on objective statusobjective status– May progress more slowly with lateral repairs secondary to higher % of load transmission of weight distributiontransmission of weight distribution
No resistive flexion for 6‐8 weeks No squats, twisting, or “heel‐to‐butt”No squats, twisting, or heel to butt
stretching activities for 3‐6 months 4‐6 month restriction on return to athletics
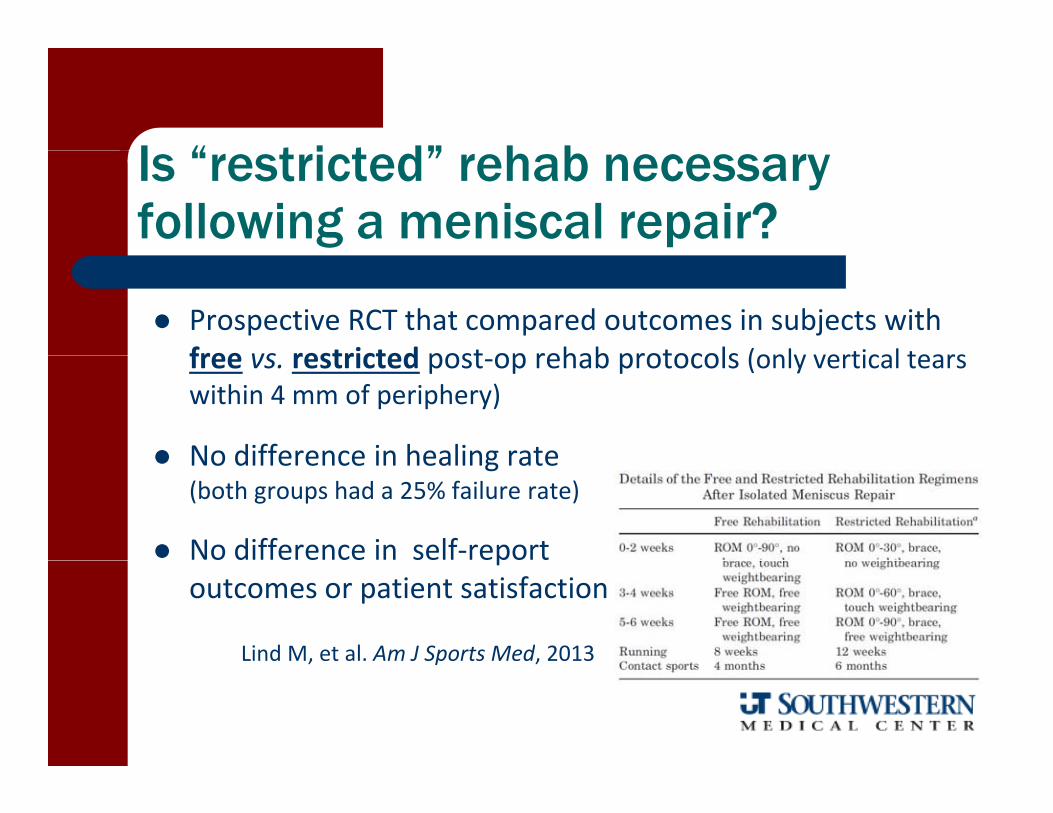
I “ t i t d” h b Is “restricted” rehab necessary following a meniscal repair?
Prospective RCT that compared outcomes in subjects with free vs restricted post op rehab protocols (only vertical tearsfree vs. restricted post‐op rehab protocols (only vertical tears within 4 mm of periphery)
No difference in healing rate No difference in healing rate (both groups had a 25% failure rate)
No difference in self‐report poutcomes or patient satisfaction
Lind M, et al. Am J Sports Med, 2013, p ,






























