Embed Size (px)
Citation preview

Nutrition Tools
TOOL A
241
Tool A: Nutrition Questionnaire for Infants
The nutrition questionnaire for infants (see pocket atthe back of the guide) is a tool for parents to completebefore meeting with a health professional. Thequestionnaire provides a useful starting point foridentifying areas of nutrition concern and the need foradditional screening.
When reviewing the responses to the questionnaire,use the interpretive notes to identify areas of concern anddetermine follow-up questions or actions. The notes arelisted by their corresponding questions on thequestionnaire.
1. Feeding is crucial for the development of ahealthy relationship between parents and theirinfant. A parent’s responsiveness to an infant’scues of hunger and satiation and the closephysical contact during feeding facilitate healthysocial and emotional development.
2. Signs of hunger include hand-to-mouth activity,rooting, pre-cry facial grimaces, fussing sounds,and crying. Signs of fullness are turning the headaway from the nipple, showing interest in thingsother than eating, and closing the mouth.
3. Infants should be fed breastmilk or iron-fortifiedinfant formula, even in infant cereal. If infantsare weaned from breastmilk before 12 months,they should be fed iron-fortified infant formularather than cow’s milk. Cow’s milk, goat’s milk,and soy milk are not recommended during thefirst 12 months of life, and reduced-fat (2percent), low-fat (1 percent), and fat-free (skim)milk are not recommended during the first 2years of life.
4. Developmental readiness for eating differenttextures of food and the acquisition of self-feeding skills are important in establishingrealistic feeding goals for infants.
5. By 4 to 6 months, infants need more nutrientsthan can be supplied by breastmilk or infantformula alone; they should gradually beintroduced to solid foods when they aredevelopmentally ready. After the infant hasaccepted iron-fortified infant cereal, then pureedor soft fruits, vegetables, and meats can beoffered. Only one new food should be introducedat a time; parents should wait 7 or more days tosee how the infant tolerates the food.
Between 6 and 12 months, infants masterchewing, swallowing, and manipulation of fingerfoods. They begin to use cups and utensils, andwhile they are experimenting with new tastes andtextures, their sensory and perceptualdevelopment are stimulated.
6. A reasonable amount of juice is 4 to 6 oz per daywhen the infant is developmentally ready (6months or older). Juice should be served in a cup,not a bottle. It should be offered in smallamounts (more than 8 to 10 oz per day isexcessive) because too much juice may reduce theinfant’s appetite for other foods and increases therisk of loose stools and diarrhea.
7. Infants permitted to suck on a bottle of any fluidthat contains carbohydrates, including juice andmilk, for prolonged periods are at risk fordeveloping early childhood caries (baby bottletooth decay). Infants should not be put to bed atnight or at naptime with a bottle or allowedunlimited access to a bottle (i.e., permitting theinfant to carry a bottle around whenever hewants).
8. Honey should not be added to food, water, orformula that is fed to infants because it can be asource of spores that cause botulism poisoning in

242
TOOL
A
infants. Processed foods containing honey shouldnot be given.
9. Starting at 6 months, infants receiving breastmilkor infant formula prepared with water needfluoride supplementation if the water is severelydeficient in fluoride. To assess fluoride levels, askabout all sources of water used by the family,including municipal, well, commercially bottled,and home system–processed water. In addition,find out whether any ready-to-feed infantformula used is manufactured with water that haslittle or no fluoride. Refer an infant who is notgetting enough fluoride to a dentist or primarycare health professional for follow-up.
10–11. If inadequate cooking or food-storage facilitiesadversely affect a family’s nutrient intake, referthe family to social services. If a family does nothave adequate resources to obtain food, referthem to food assistance and nutrition programssuch as WIC and the Food Stamp Program, or to acommunity food shelf or pantry. (See Tool K:Federal Food Assistance and Nutrition Programs.)
12. Respond to parents’ questions and concerns.

Tool B: Nutrition Questionnaire for Children
243
TOOL B
The nutrition questionnaire for children (see pocketat the back of the guide) is a tool for parents to completebefore meeting with a health professional. The question-naire provides a useful starting point for identifying areasof nutrition concern and the need for additionalscreening.
When reviewing the responses to the questionnaire,use the interpretive notes to identify areas of concern anddetermine follow-up questions or actions. The notes arelisted by their corresponding questions on thequestionnaire.
1. Children grow more slowly from ages 1 to 5 thanin infancy. Their appetites can change from dayto day, depending on how fast they are growingand how active they are. As long as they areenergetic and growing, they are probably gettingenough of the nutrients they need. Youngchildren often eat small portions. They should beoffered small servings and be allowed to ask formore.
Irregular eating and frequently missing meals canresult in a low intake of calories (energy) andnutrients. Busy schedules and inadequateresources for obtaining food may cause a child tomiss meals.
2. Encourage parents to eat meals together as afamily. If children see their parents and otheradults enjoying meals together and eating avariety of foods, they will want to do the same.Explain that being a role model is the bestteacher.
3. During mealtimes, a relaxed atmosphere shouldbe maintained and children should not berushed. Well-balanced meals and snacks shouldbe offered in a pleasant environment. Whenchildren are stubborn about eating, it is oftentheir way of learning to be independent. Fighting
over food may make them even more stubborn.Encourage parents to get rid of distractions such astelevision during meals.
4. Meals and snacks for children need to be plannedand offered at scheduled times throughout the dayand should consist of a variety of healthy foods.Children should not be pressured or rewarded toeat certain foods.
5. Children 2 to 3 years old need the variety andsame number of servings as older children butmay need small portions—about 2/3 of a serving.By the time children are 4 years old, they eatportions similar to those eaten by older familymembers: 1 slice of bread; 1 cup of raw vegetables;1 medium-size piece of fruit; 1 cup of milk oryogurt; 2 to 3 oz of cooked lean meat, poultry, orfish.
Grains. Children need 6 to 11 servings per day.Grain products provide vitamins, minerals,complex carbohydrates, and dietary fiber, whichare important for good health.
Vegetables. Children need 3 to 5 servings per day.Vegetables provide vitamins, minerals, and dietaryfiber. Children need to eat dark-green leafy anddeep-yellow vegetables often.
Fruits. Children need 2 to 4 servings per day. Fruitsprovide vitamins, minerals, and dietary fiber.Many juice beverages are not 100 percent juice.Parents need to check the ingredients to make surethat they purchase juice without added sugar suchas corn syrup, and canned fruits with little or noadded sugar.
Milk and other dairy products. Children need 2 to 3servings per day. Milk, yogurt, cheese, and otherdairy products supply calcium for building andmaintaining strong bones and teeth and

TOOL
B
244
protecting bones from osteoporosis. Children 1 to2 years old need whole milk. Older children candrink reduced-fat (2 percent), low-fat (1 percent),or fat-free (skim) milk.
Meat and meat alternatives. Children need 2 to 3servings per day. Meat and meat alternativesinclude both animal and plant sources of protein,iron, and other important nutrients. Two to 3 ozof cooked lean meat, poultry, or fish equal 1serving from this group. One egg or 1/2 cup ofcooked dry beans counts as 1 oz of lean meat; 2tablespoons of peanut butter count as 1 oz ofmeat.
Fats and sweets. This group includes butter,margarine, mayonnaise, vegetable oil, gravy, saladdressing, cake/cupcakes, pie, cookies, chips,doughnuts, and candy. There is no recommendedserving because consumption of fats and sweetsshould be limited.
6. For children under age 3, foods that may causechoking need to be avoided (e.g., hard candy,mini-marshmallows, popcorn, pretzels, chips,spoonfuls of peanut butter, nuts, seeds, largechunks of meat, hot dogs, raw carrots, raisins andother dried fruits, whole grapes).
Young children, 3-year-olds especially, are at riskfor choking on food and remain at risk until theycan chew and swallow better at about age 5.Precautions to prevent choking include
• Staying with children while they are eating.
• Having children sit while eating because eatingwhile walking or running can cause choking.
• Keeping things calm at eating time becausebecoming overexcited while eating can causechoking.
For children between ages 3 and 5, foods thatmay cause choking can be modified to makethem safer (e.g., by cutting hot dogs in quarterslengthwise and then into small pieces, cuttingwhole grapes in half lengthwise, chopping nutsfinely, chopping raw carrots finely or into thin
strips, spreading peanut butter thinly on crackersor bread).
7. Juice should be offered in small amounts becausetoo much juice may reduce a child’s appetite formeals. Parents should limit sugary drinks such asfruit punch, soft drinks, and artificially sweetenedbeverages. If allowed to consume sweets inunlimited amounts, children are likely to fill upon these rather than eat healthy foods.
8. Children permitted to suck on a bottle of any fluidthat contains carbohydrates, including juice andmilk, for prolonged periods are at risk fordeveloping early childhood caries (baby bottletooth decay). Children should not be put to bed atnight or naptime with a bottle or allowedunlimited access to a bottle (i.e., permitting thechild to carry a bottle around whenever she wants).
9. Children need fluoride supplementation if thewater is severely deficient in fluoride. To assessfluoride levels, ask about all sources of water usedby the family, including municipal, well, commer-cially bottled, and home system–processed water.Refer a child who is not getting enough fluoride toa dentist or primary care health professional forfollow-up.
10–11. If inadequate cooking or food-storage facilitiesadversely affect a family’s nutrient intake, referthe family to social services. If a family does nothave adequate resources to obtain food, referthem to food assistance and nutrition programssuch as WIC and the Food Stamp Program, or to acommunity food shelf or pantry. (See Tool K:Federal Food Assistance and Nutrition Programs.)
12. The Surgeon General’s report on physical activityand health states that everyone should participatein a moderate amount of physical activity (e.g., 15minutes of running, 30 minutes of brisk walking,45 minutes of playing volleyball) on most, if notall, days of the week. Longer or more vigorousphysical activity will yield greater health benefits.The benefits of physical activity include givingchildren a feeling of accomplishment, reducing

245
the risk of certain diseases (e.g., diabetes mellitus,hypertension) if they continue to be active duringadulthood, and promoting mental health. Helpthe inactive child identify enjoyable activities andincorporate them into a daily routine.
13. Children who spend too much time watchingtelevision and videotapes or playing computergames are likely to have a sedentary lifestyle,which can lead to overweight. These sedentaryactivities should be limited to 1 to 2 hours per day.
14. Respond to parents’ questions and concerns.
TOOL B

246
Tool C: Nutrition Questionnaire for AdolescentsTO
OL C
The nutrition questionnaire for adolescents (seepocket at the back of the guide) is a tool for adolescentsor parents to complete before meeting with a healthprofessional. The questionnaire provides a useful startingpoint for identifying areas of nutrition concern and theneed for additional screening.
When reviewing the responses to the questionnaire,use the interpretive notes to identify areas of concern anddetermine follow-up questions or actions. The notes arelisted by their corresponding questions on thequestionnaire.
Eating Behaviors1–2. Irregular eating and frequently missing meals can
result in a low intake of calories (energy) andnutrients. Busy schedules and inadequateresources for obtaining food may cause anadolescent to miss meals. If the adolescent isoverweight, reinforce the importance of eatingthree meals per day instead of frequent snacks.
3. Adolescents who are on their own for mostmeals—perhaps because of a busy schedule—maynot have healthy eating behaviors. Remindadolescents and parents that family meals ensureoptimal nutrition and encourage communication.Explain to parents that family meals give themthe opportunity to model healthy eatingbehaviors.
4. Shopping for and preparing food give adolescentsthe opportunity to learn about healthy foodchoices. Make sure the adolescent is familiar withthe basic rules of food safety.
5. Consumption of convenience and fast foods iscommon among Americans. Frequentconsumption increases fat, caloric, and sodiumintake and reduces the intake of certain vitaminsand minerals. Suggest that adolescents reduce the
consumption of these foods, and offer suggestionsfor making healthier food choices.
6. If the adolescent is on a special diet, ask, “Whatkind of diet are you on?” This will provide anopportunity to evaluate the adolescent’s dietarymanagement of conditions such as diabetesmellitus.
7. Because the term “vegetarian” is often usedloosely, ask adolescents who follow a vegetariandiet which foods they eat. Further assessment isrecommended.
8. Excessive or poor appetite and weight gain or lossmay indicate depression or other emotional stress,which should be assessed. Because excessiveappetite may also indicate binge eating orovereating, an adolescent who reports excessiveappetite needs further assessment to rule out aneating disorder.
9. Soft drinks, fruit-flavored drinks, coffee, and teacontain few essential nutrients and may displacehealthier beverages (e.g., milk, which providescalcium, protein, and vitamins; orange juice,which is an important source of vitamin C andfolate).
Food Choices10. Grains. Grains supply complex carbohydrates
(which are important sources of energy), protein,and minerals; they also tend to be low in fat.Whole grains are a good source of dietary fiber.Six to 11 servings of grains per day arerecommended.
Vegetables. Vegetables provide vitamins, such as Aand C, and minerals, such as calcium and iron.Most are low in fat and high in dietary fiber.Green leafy vegetables are good sources of folate.

TOOL C
247
Three to 5 servings of vegetables per day arerecommended.
Fruits. Fruits are important sources of vitaminsand fiber and are low in fat. Citrus fruits andjuices, strawberries, and cantaloupe are goodsources of vitamin C and folate. Two to 4 servingsof fruits per day are recommended.
Milk and other dairy products. Milk, yogurt, andcheese are good sources of calcium and provideprotein, vitamins, and minerals. Three or moreservings per day of milk and other dairy productsare recommended. Encourage the adolescent toconsume reduced-fat (2 percent), low-fat (1percent), or fat-free (skim) milk and other lower-fat dairy products. Adequate calcium intakeduring adolescence is essential for peak bone-mass development. If the recommended calciumintake cannot be met by diet, a supplement maybe warranted. Of the various forms of calcium,calcium carbonate contains the highestproportion (40 percent) of elemental calcium byweight.
Meat and meat alternatives. Red meat, poultry, fish,eggs, and dried beans provide protein, iron, zinc,and many other minerals and vitamins. Adequateprotein intake is essential for growth anddevelopment. Two to 3 servings of meat or meatalternatives per day are recommended. Cold cuts,bacon, sausage, and fried meats are high in fatand calories; therefore, their consumption shouldbe limited.
Fats and sweets. This group includes butter,margarine, mayonnaise, vegetable oil, gravy, saladdressing, cake/cupcakes, pie, cookies, chips,doughnuts, and candy. There is no recommendedserving because consumption of fats and sweetsshould be limited.
Food Resources11–12. If inadequate cooking or food-storage facilities
adversely affect a family’s nutrient intake, referthe family to social services. If a family does not
have adequate resources to obtain food, refer thefamily to food assistance and nutrition programssuch as the Food Stamp Program, a communityfood shelf or pantry, or a free or reduced-priceschool meal program. (See Tool K: Federal FoodAssistance and Nutrition Programs.)
Weight and Body Image13. Some adolescents may be dissatisfied with their
weight and use unhealthy means to alter it. If theadolescent expresses a concern about weight,follow up with questions such as “Do you feelyou are underweight?” “Do you feel you areoverweight?” “Are you doing anything to changeyour weight?”
14. If the adolescent is dieting, determine thefrequency, duration, and methods of weight loss.Chronic food restriction and inadequate energyintake may cause poor growth, delayed sexualdevelopment, menstrual irregularities, poorconcentration, irritability, sleep difficulties, andconstipation. Frequent dieting may be associatedwith binge eating. Purging (e.g., self-inducedvomiting, laxative use) may be associated withother risk behaviors (e.g., substance use, suicideattempts).
15. Self-induced vomiting and/or the use of laxatives,diuretics, or diet pills are warning signs of eatingdisorders. Adolescents who engage in thesebehaviors need further assessment.
Physical Activity16. The Surgeon General’s report on physical activity
and health states that everyone should participatein a moderate amount of physical activity (e.g.,15 minutes of running, 30 minutes of briskwalking, 45 minutes of playing volleyball) onmost, if not all, days of the week. Longer or morevigorous physical activity will yield greater healthbenefits. The benefits of physical activity includegiving adolescents a feeling of accomplishment,reducing the risk of certain diseases (e.g., diabetes

TOOL
C
248
mellitus, hypertension) if they continue to beactive during adulthood, and promoting mentalhealth. Help the inactive adolescent identifyenjoyable activities and incorporate them into adaily routine.
Some adolescents participate in a physical activitytoo frequently or intensely. Excessive physicalactivity may lead to fatigue, loss of appetite, ormenstrual irregularities; it may also be a sign ofan eating disorder.
Lifestyle17. Adolescents who spend too much time watching
television and videotapes or playing computergames are likely to have a sedentary lifestyle,which can lead to overweight. These sedentaryactivities should be limited to 1 to 2 hours perday.
18. If the adolescent uses vitamin, mineral, herbal, orother dietary supplements, ask about the kind,dosage, length of use, and reason for use.Encourage the adolescent to eat healthy foodsinstead of using supplements to obtain nutrients.If the adolescent is interested in vitaminsupplements, emphasize the importance of usinglow-dose supplements and the need to avoid highdoses (particularly of vitamins A and D), whichcan be toxic.
Adolescents who participate in physical activitiesin which strength is a critical factor (e.g., football,weightlifting) may consume a high-protein dietor take protein supplements to increase strengthand muscle mass. However, increased proteinintake does not affect muscle size.
Adolescents who use protein supplements shouldbe asked about anabolic steroid use. Someadolescents take anabolic steroids to enhancetheir strength, muscle size, and endurance.Steroid use can cause side effects, including acne,deepening of the voice, and hair recession.
19. Unhealthy behaviors occur in clusters inadolescents. For example, adolescents who smoke
are more likely to have unhealthy eatingbehaviors and low levels of physical activity.Adolescents who smoke cigarettes to lose weightneed counseling on both smoking and healthyweight management. Cigarette smoking alsoincreases the need for vitamin C.
20. If the adolescent admits to using alcohol or streetdrugs, screen for substance use and refer for coun-seling and treatment.
Some adolescents take anabolic steroids toenhance their strength, muscle size, andendurance. Steroid use can cause side effects,including acne, deepening of the voice, and hairrecession. Emphasize the dangers of steroid use toadolescents who participate in strenuous physicalactivity to build muscle or who participate insports in which strength is a critical factor (e.g.,football, weightlifting).
249
TOOL D
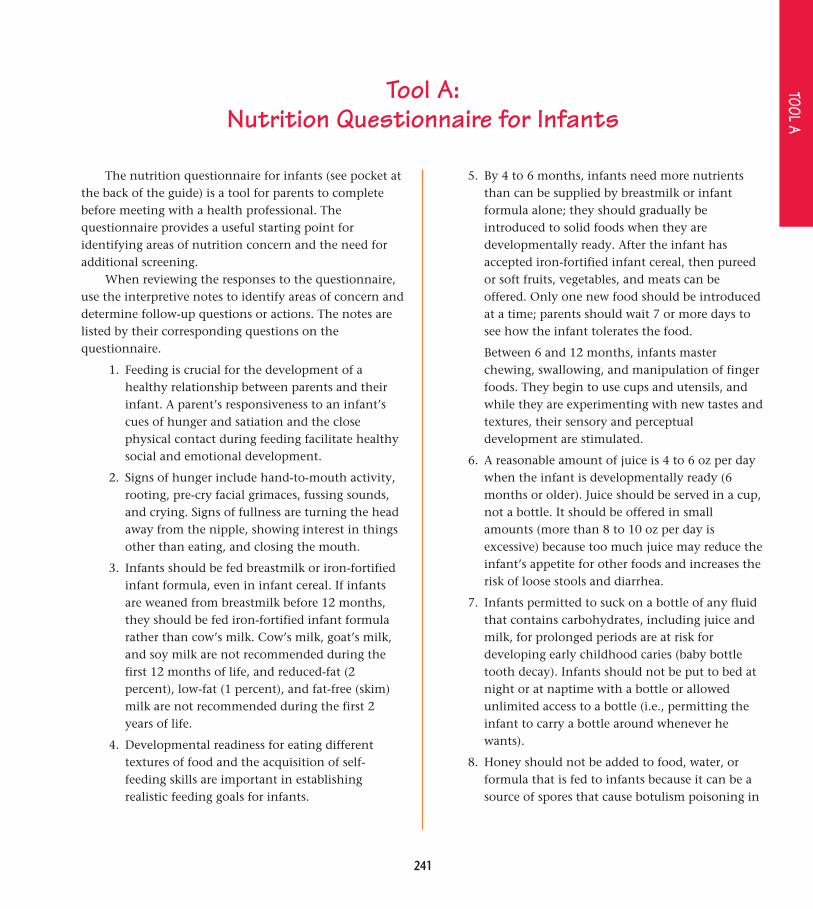
Tool D: Key Indicators of Nutrition Risk for Children and Adolescents
Consumes fewer than 2 servings offruits per day.
Consumes fewer than 3 servings ofvegetables per day.
Consumes fewer than 6 servings ofbread, cereal, rice, pasta, or othergrains per day.
For children younger than 9 years,consumes fewer than 2 servings ofdairy products per day.
For children 9 years and older andadolescents, consumes fewer than 3servings of dairy products per day.
Fruits and vegetables provide dietaryfiber, vitamins (such as A and C), andminerals. Low intake of fruits andvegetables is associated with anincreased risk of many types of cancer.In females of childbearing age, lowintake of folic acid is associated withincreased risk of giving birth to aninfant with neural tube defects.
Grain products provide complexcarbohydrates, dietary fiber, vitamins,and minerals. Low intake of dietaryfiber is associated with constipationand increased risk of colon cancer.
Dairy products are a good source ofprotein, vitamins, and calcium andother minerals. Low intake of dairyproducts may reduce peak bone massand increase the risk of osteoporosis.
Assess the child/adolescent who isconsuming less than 1 serving offruit per day.
Assess the child/adolescent who isconsuming fewer than 2 servings ofvegetables per day.
Assess the child/adolescent who isconsuming fewer than 3 servings ofbread, cereal, pasta, rice, or othergrains per day.
Assess the child/adolescent who hasrecent history of constipation.
Assess the child (younger than 9years) who is consuming less than 1serving of dairy products per day.
Assess the child (9 years and older)or adolescent who is consumingfewer than 2 servings of dairyproducts per day.
Assess the child/adolescent who hasa milk allergy or is lactose intolerant.
Assess the child/adolescent who isconsuming more than 2 soft drinksper day.
Indicators of Nutrition Risk Criteria for Further Screeningand Assessment
Relevance
Food Choices

TOOL
D
250
Consumes fewer than 2 servings ofmeat or meat alternatives (e.g.,beans, eggs, nuts, seeds) per day.
For children 5 years and older,consumes excessive amount of fat.
Exhibits poor appetite.
Consumes food from fast-foodrestaurants 3 or more times perweek.
Protein-rich foods (e.g., meats, beans,dairy products) are good sources of Bvitamins, iron, and zinc. Low intake ofprotein-rich foods may impair growthand increase the risk of iron-deficiencyanemia and of delayed growth andsexual maturation. Low intake of meator meat alternatives may indicateinadequate availability of these foodsat home. Special attention should bepaid to children and adolescents whofollow a vegetarian diet.
Excessive intake of dietary fatcontributes to the risk of cardio-vascular disease and obesity and isassociated with some cancers.
A poor appetite may bedevelopmentally appropriate for youngchildren, but in older children it mayindicate depression or other emotionalstress or chronic disease.
Excessive consumption of conveniencefoods and foods from fast-foodrestaurants is associated with high fat,calorie, and sodium intake, as well aslow intake of certain vitamins andminerals.
Assess the child/adolescent who isconsuming less than 1 serving ofmeat or meat alternatives per day.
Assess the child/adolescent who hasa family history of prematurecardiovascular disease.
Assess the child/adolescent who hasa body mass index (BMI) equal to orgreater than the 85th percentile.
Assess the child/adolescent if BMI isless than the 15th percentile or ifweight loss has occurred.
Assess if irregular menses oramenorrhea has occurred for 3months or more.
Assess for organic and psychiatricdisease.
Assess the child/adolescent who isoverweight/obese or who hasdiabetes mellitus, hyperlipidemia, orother conditions requiring reductionin dietary fat.
Indicators of Nutrition Risk Criteria for Further Screeningand Assessment
Relevance
Food Choices (cont.)
Eating Behaviors

TOOL D
251
Indicators of Nutrition Risk
Skips breakfast, lunch, ordinner/supper 3 or more times perweek.
Has food jags—eats one particularfood only.
Has inadequate financial resources tobuy food, insufficient access to food,or lack of access to cooking facilities.
Practices unhealthy behaviors (e.g.,chronic dieting, vomiting, and usinglaxatives, diuretics, or diet pills tolose weight).
Is excessively concerned about bodysize or shape.
Meal skipping is associated with a lowintake of energy and essential nutrientsand, if it is a regular practice, couldcompromise growth and sexualdevelopment. Repeatedly skippingmeals decreases the nutritionaladequacy of the diet.
Food jags, which limit the variety offood consumed, decrease thenutritional adequacy of the diet.
Poverty can result in hunger andcompromised food quality andnutrition status. Inadequate dietaryintake interferes with learning.
Chronic dieting is associated with manyhealth concerns (e.g., fatigue, impairedgrowth and sexual maturation,irritability, poor concentration, impulseto binge) and can lead to eatingdisorders. Frequent dieting incombination with purging is associatedwith health-compromising behaviors(e.g., substance use, suicidal behaviors).Purging is associated with seriousmedical complications.
Eating disorders are associated withsignificant health and psychosocialmorbidity. Eighty-five percent of all casesof eating disorders begin duringadolescence. The earlier adolescents aretreated, the better their long-termprognosis.
Assess the child/adolescent to ensurethat meal skipping is not due toinadequate food resources orunhealthy weight-loss practices.
Assess the child’s/adolescent’sdietary intake over several days.
Assess the child/adolescent who isfrom a family with low income, ishomeless, or is a runaway. (See ToolK: Federal Food Assistance andNutrition Programs.)
Assess the child/adolescent foreating disorders.
Assess for organic and psychiatricdisease.
Assess the child/adolescent fordistorted body image anddysfunctional eating behaviors,especially if child/adolescent wantsto lose weight but BMI is less thanthe 85th percentile.
Criteria for Further Screeningand Assessment
Relevance
Weight and Body Image
Eating Behaviors (cont.)
Food Resources

TOOL
D
252
Indicators of Nutrition Risk Criteria for Further Screeningand Assessment
Relevance
Exhibits significant weight change inpast 6 months.
Has BMI less than the 5th percentile.
Has BMI greater than the 95thpercentile.
Is physically inactive: participates inphysical activity fewer than 5 daysper week.
Significant weight change during the past6 months may indicate stress, depression,organic disease, or an eating disorder.
Thinness may indicate an eatingdisorder or poor nutrition.
Obesity is associated with elevatedcholesterol levels and elevated bloodpressure. Obesity is an independent riskfactor for cardiovascular disease and type2 diabetes mellitus. Overweight childrenand adolescents are more likely to beoverweight adults and are at increasedrisk for health problems as adults.
Lack of physical activity is associatedwith overweight, fatigue, and poormuscle tone in the short term, and agreater risk of cardiovascular disease inthe long term. Regular physical activityreduces the risk of cardiovasculardisease, hypertension, colon cancer,and type 2 diabetes mellitus. Weight-bearing physical activity is essential fornormal skeletal development duringchildhood. Regular physical activity isnecessary for maintaining normalmuscle strength, joint structure, andjoint function; contributes topsychological health and well-being;and facilitates weight reduction andweight maintenance throughout life.
Assess the child/adolescent todetermine the cause of weight loss orweight gain (e.g., limited or too muchaccess to food, poor appetite, mealskipping, eating disorder).
Assess the child/adolescent foreating disorders.
Assess for organic or psychiatricdisease.
Assess for inadequate food resources.
Assess the child/adolescent who isoverweight or at risk for becomingoverweight (e.g., on the basis ofpresent weight, weight gainpatterns, family weight history).
Assess how much time thechild/adolescent spends watchingtelevision/videotapes and playingcomputer games.
Assess the child’s/adolescent’sdefinition of physical activity.
Physical Activity
Weight and Body Image (cont.)
Growth

TOOL D
253
Indicators of Nutrition Risk Criteria for Further Screeningand Assessment
Relevance
Participates in excessive physicalactivity.
Has chronic diseases or conditions.
Has hyperlipidemia.
Has iron-deficiency anemia.
Intense physical activity nearly everyday, sometimes more than once a day,can be unhealthy and associated withmenstrual irregularity, excessive weightloss, and malnutrition.
Medical conditions (e.g., diabetesmellitus, spina bifida, renal disease,hypertension, pregnancy, HIV/AIDS)have significant nutritionalimplications.
Hyperlipidemia is a major cause ofatherosclerosis and cardiovasculardisease in adults.
Iron deficiency causes developmentaldelays and behavioral disturbances.Another consequence is increased leadabsorption. Childhood lead poisoningcauses neurological and developmentaldeficits.
Assess the child/adolescent foreating disorders.
Assess child’s/adolescent’s compliancewith therapeutic dietary recom-mendations.
Refer to dietitian if appropriate.
Refer child/adolescent to a dietitianfor cardiovascular screening andassessment.
Screen children whose families havelow incomes, are migrant, or arerecently arrived refugees.
Screen male children/adolescentswho have low iron intake, a historyof iron-deficiency anemia, limitedaccess to food because of poverty orneglect, or special health care needs.
Screen nonpregnant adolescentsevery 5 to 10 years or annually ifthey have a history of iron-deficiencyanemia, low iron intake, or extensivemenstrual or other blood loss.
Physical Activity (cont.)
Medical Conditions
TOOL
D
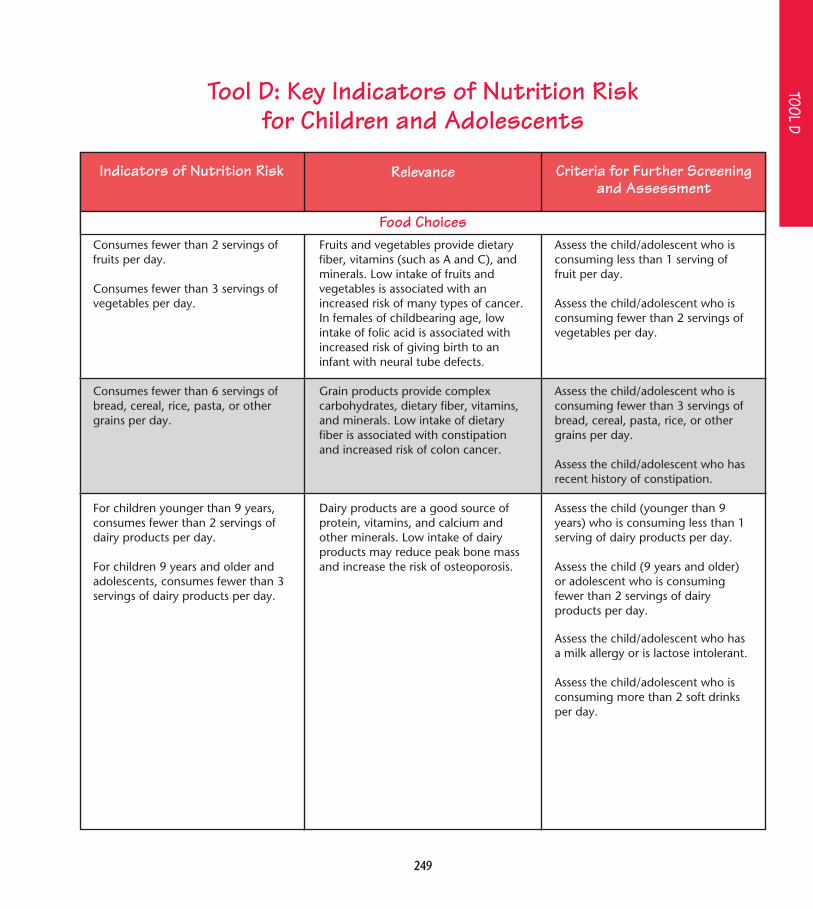
254
Indicators of Nutrition Risk Criteria for Further Screeningand Assessment
Relevance
Has dental caries.
Is pregnant.
Is taking prescription medication.
Engages in heavy alcohol, tobacco,and other drug use.
Uses dietary supplements.
Food affects the health of the mouth aswell as overall health. Calcium andvitamin D are vital for strong bonesand teeth, and vitamin C is necessaryfor healthy gums. Eating habits have adirect impact on oral health. Frequentconsumption of carbohydrate-richfoods (e.g., candy, soda) that stay inthe mouth longer may cause dentalcaries. Fluoride in water used fordrinking and cooking as well as intoothpaste reduces the prevalence ofdental caries.
Pregnancy increases the need for mostnutrients.
Many medications interact withnutrients and can compromisenutrition status.
Alcohol, tobacco, and other drug usecan adversely affect nutrient intake andnutrition status.
Dietary supplements (e.g., vitamin andmineral preparations) can be healthyadditions to a diet, especially forpregnant and lactating women and forpeople with a history of iron-deficiencyanemia; however, frequent use or highdoses can have serious side effects.Adolescents who use supplements to“bulk up” may be tempted toexperiment with anabolic steroids.
Assess the child’s/adolescent’sconsumption of snacks andbeverages that contain sugar, andassess snacking patterns.
Assess the child’s/adolescent’s accessto fluoride (e.g., fluoridated water,fluoride tablets).
Refer the adolescent to a dietitian forfurther screening, assessment, andcounseling.
Assess potential interactions ofprescription drugs (e.g., asthmamedications, antibiotics) withnutrients.
Assess the child/adolescent furtherfor alcohol, tobacco, and other druguse.
Assess the child/adolescent for thetype of supplements used anddosages.
Assess the adolescent for use ofanabolic steroids and megadoses ofother supplements.
Medical Conditions (cont.)
Lifestyle

Tool E: Screening for Elevated Blood Lead Levels
255
In 1997, the Centers for Disease Control andPrevention (CDC) updated its lead screening guidelinesand published revised guidance to help state and localpublic health authorities determine which children are atrisk for elevated blood lead levels and are most likely tobenefit from lead screening.1 The American Academy ofPediatrics (AAP) supports these revised guidelines. Thefollowing information has been compiled from CDC andAAP guidelines.1,2 Federal Medicaid policy requires thatall eligible children be screened for lead poisoning asdescribed below under Universal Screening, because theyare at high risk for lead poisoning.
Screening RecommendationsTo prevent lead poisoning, lead screening should
begin at 9 to 12 months of age and be considered again atapproximately 24 months of age. Health professionalsshould follow the local or state health departmentrecommendations for universal or targeted screening.2
Universal ScreeningUniversal screening will be recommended in
communities in which the risk of lead exposure iswidespread. A universal screening recommendation mayread as follows:1(p85)
Using a blood lead test, screen all children at ages 1and 2, and all children 36–72 months of age whohave not been previously screened.
Targeted ScreeningTargeted screening will be recommended in
communities in which the risk of lead exposure is not widespread or is confined to specific geographicareas or to certain subpopulations. Health professionalsshould determine whether each child is at risk and screen when necessary. A sample targeted screeningrecommendation follows:1(p85)
Using a blood lead test, screen children at ages 1 and2, and all children 36–72 months of age who havenot been previously screened, if they meet one of thefollowing health department criteria:
• Child resides in a geographic area (e.g., a specifiedzip code) in which ≥ 27 percent of housing wasbuilt before 1950
• Child receives services from public assistanceprograms such as Medicaid or WIC
• Child’s parent or guardian answers “yes” or “don’tknow” to any of the three questions in the basicpersonal-risk questionnaire
A Basic Personal-Risk Questionnaire for
Lead Exposure in Children1. Does your child live in or regularly visit a house
or child-care facility that was built before 1950?
2. Does your child live in or regularly visit a houseor child-care facility built before 1978 that isbeing or has recently been renovated orremodeled (within the last 6 months)?
3. Does your child have a sibling or playmate whohas or did have lead poisoning?
Source: Reproduced with permission from AAP.2 Copyright © 1998American Academy of Pediatrics. See also CDC.1(p62)
History of Possible Lead ExposureHealth professionals should periodically assess
infants and children between 6 months and 6 years of agefor a history of possible lead exposure, using the basicpersonal-risk questionnaire here and any additionalcommunity-specific questions recommended by the stateor local health department. Blood lead testing should alsobe considered in abused or neglected children and inchildren who have conditions associated with increasedlead exposure.2
TOOL E
Due to copyright permissions restrictions, this text is not
available on the Web. Please see printversion of the nutrition guide, or visit
http://www.aap.org/policy/re9815.html.

Due to copyright permissions restrictions, this table is not
available on the Web. Please see print version of the nutrition guide, or visit http://www.aap.org/policy/re9815.html.
256
Anticipatory GuidanceHealth professionals should provide anticipatory
guidance on lead exposure to parents of all infants andyoung children, including information on risk factors and specific prevention strategies (Table 23).2 CDCrecommends providing anticipatory guidance at prenatalvisits, when the infant is 3 to 6 months of age, and againat 12 months of age; parental guidance at these timesmight prevent some lead exposure and the resultingincrease in blood lead levels that often occurs during achild’s second year of life. When children are 1 to 2 yearsold, parental guidance should be provided at healthsupervision visits and when the personal-riskquestionnaire is administered.1(p83)
References1. Centers for Disease Control and Prevention. 1997. Screening
Young Children for Lead Poisoning: Guidance for State and Local
Public Health Officials. Atlanta, GA: Centers for Disease
Control and Prevention. Also in Centers for Disease Control
and Prevention [Web site]. Cited May 14, 1999; available at
http://www.cdc.gov/nceh/programs/lead/guide/1997/
guide97.htm.
2. American Academy of Pediatrics. 1998. Screening for
elevated blood lead levels [policy statement no. RE9815].
Pediatrics 101(6):1072–1078. Also in American Academy of
Pediatrics [Web site]. Cited May 14, 1999; available at
http://www.aap.org/policy/re9815.html.
TOOL
E
Source: Adapted with permission from American Academy of Pediatrics.2 Copyright © 1998 American Academy of Pediatrics.
Table 23. Risk Factors and Prevention Strategies for Lead Exposure in Children

TOOL F
257
Tool F: Stages of Change— A Model for Nutrition Counseling
Precontemplation
Contemplation
Preparation
Action
Maintenance
Is unaware of problem andhasn’t thought about change.Has no intention of takingaction within the next 6months.
Intends to take action withinthe next 6 months.
Intends to take action withinthe next 30 days and hastaken some behavioral stepsin this direction.
Has changed overt behaviorfor less than 6 months.
Has changed overt behaviorfor more than 6 months.
Increase awareness of need forchange.Personalize information onrisks and benefits.
Increase motivation andconfidence to perform thenew behavior.
Initiate change.
Commit to change.
Reinforce commitment andcontinue changes/newbehaviors.
Create supportive climate forchange.Discuss personal aspects andhealth consequences of pooreating or sedentary behavior.Assess knowledge, attitudes,and beliefs.Build on existing knowledge.
Identify problematic behaviors.Prioritize behaviors to change.Discuss motivation.Identify barriers to change andpossible solutions.Suggest small, achievable stepsto make a change.
Assist in developing a concreteaction plan.Encourage initial small steps tochange.Discuss earlier attempts tochange and ways to succeed.Elicit support from family andfriends.
Reinforce decision.Reinforce self-confidence.Assist with self-monitoring,feedback, problem solving,social support, andreinforcement.Discuss relapse and copingstrategies.
Plan follow-up to supportchanges.Help prevent relapse.Assist in coping, reminding,finding alternatives, andavoiding slips/relapses.
Stage Description Goals Strategies
Source: Adapted from Glanz K, Rimer B. 1995. Theory at a Glance: A Guide for Health Promotion Practice. Bethesda, MD: National Institutes ofHealth, National Cancer Institute. Also adapted, with permission, from Sandoval WM, Heller KE, Wiese WH, Childs DA. 1994. Stages of change: Amodel for nutrition counseling. Topics in Clinical Nutrition 9:64–69. Copyright © 1994 Aspen Publishers, Inc.

TOOL
G
258
Tool G: Strategies for Promoting Healthy Eating Behaviors
Promote positive, nonjudgmental strategies to help thechild/adolescent adopt healthy eating behaviors.
Encourage the child’s/adolescent’s active participation inchanging eating behaviors.
Provide concrete learning situations.
Focus on the short-term benefits of healthy eatingbehaviors.
Understand and respect the child’s/adolescent’s culturaleating behaviors.
Use simple terminology.
Provide an office or clinic oriented to children/adolescents.
Communicate developmentally appropriate healthmessages.
Encourage health professionals and staff to become rolemodels for healthy eating behaviors.
Strategies Applications/QuestionsCommunication Factors
Reinforce positive aspects of the child’s/adolescent’s eatingbehaviors.
Help the child/adolescent identify barriers that make itdifficult to change eating behaviors, and develop a plan ofaction for adopting new behaviors.
Use charts, food models, and videotapes to reinforce verbalinformation and instructions.
Emphasize that healthy eating behaviors will make thechild/adolescent feel good and energized.
Help the child/adolescent integrate cultural eatingbehaviors with dietary recommendations.
Avoid using the term “diet” with the child/adolescentbecause it tends to be associated with weight loss and maybe confusing.
Use posters and materials written for children/adolescents.
Use posters and materials that highlight the importance ofhealthy eating behaviors.
Have health professionals and staff model healthy eatingbehaviors (e.g., by keeping a bowl of fruit at the frontdesk).
Environmental Factors

259
TOOL G
Identify the child’s/adolescent’s stage of behavior changeand readiness to change based on the Stages of Change—A Model for Nutrition Counseling (Tool F).
Facilitate behavior change with counseling strategiestailored to the child/adolescent based on the Stages ofChange model (Tool F).
Provide counseling for the child/adolescent who is in theearly stages of behavior change or who is unwilling tochange.
Provide task-oriented counseling for the child/adolescentwho is ready to change eating behaviors.
Identify and prioritize behavior changes to be made.
Set realistic, achievable goals that are supported by thechild’s/adolescent’s family and peers.
Identify and address barriers to behavior change; helpreduce barriers when possible.
Strategies Applications/QuestionsReadiness to Change
“Are you interested in changing your eating behaviors?”
“Are you thinking about changing your eating behaviors?”
“Are you ready to change your eating behaviors?”
“Are you in the process of changing your eating behaviors?”
“Are you trying to maintain changes in your eatingbehaviors?”
Provide a supportive environment, basic information, andassessment.
Prioritize behaviors to be changed, set goals, and identifybarriers to change.
Develop a plan that incorporates incremental steps formaking changes, support, and reinforcement.
Increase the child’s/adolescent’s awareness and knowledgeof eating behaviors.
Encourage the child/adolescent to make behavior changes ifnecessary.
Encourage a few small, concrete changes first, and build onthose.
Support and follow up with the child/adolescent who haschanged behavior.
Suggest changes that will have a measurable impact on thechild’s/adolescent’s most serious nutrition issues.
“What behavior will you change?” “What goal is realistic rightnow?”
“How and when will you change the behavior and who willhelp you?”
“What will make it hard for you to make this change?”“Money, friends, or family?” “How can you get around this?”
Action Plans

260
TOOL
G
Make sure that the behavior changes are compatible withthe child’s/adolescent’s lifestyle.
Establish incremental steps to help the child/adolescentchange eating behaviors.
Encourage the child/adolescent to commit to behaviorchanges with incentives or contracts.
Give the child/adolescent responsibility for changing andmonitoring eating behaviors.
Make sure that the child/adolescent has family and peersupport.
Offer feedback and reinforce successes.
Ask the child/adolescent about changes in eating behaviorsat every visit.
Emphasize to the child/adolescent the consumption offoods rather than nutrients.
Build on positive aspects of the child’s/adolescent’s eatingbehaviors.
Focus on “how to” instead of “why” information.
Provide counseling that integrates realistic behavior changeinto the child’s/adolescent’s lifestyle.
Strategies Applications/Questions
Don’t force the child/adolescent to conform to rigid eatingbehaviors. Keep in mind current behaviors and realistic goals.
For example, have the child/adolescent reduce fat consump-tion by changing the type of milk consumed, from reduced-fat (2 percent), to low-fat (1 percent), to fat-free (skim) milk.
Offer tangible non-food rewards to help the child/adolescentfocus on changing eating behaviors.
Stress the importance of planning how the child/adolescentwill make and track changes in eating behavior.
Make recordkeeping simple, and review the plan with thechild/adolescent.
Show the child/adolescent how to encourage parents andpeers to help.
Meet with parents to clarify goals and action plans;determine how they can help.
Regularly show interest to encourage continued behaviorchange.
“How are you doing in changing your eating behaviors?”
For example, say, “Consume more milk, cheese, andyogurt” rather than “Increase your calcium intake.”
“It’s great that you’re eating breakfast. Would you bewilling to try cereal, fruit, and toast instead of bacon anddoughnuts 4 days out of the week?”
Share behaviorally oriented information (e.g., what, howmuch, and when to eat and how to prepare food) ratherthan focusing on why the information is important.
“I understand that your friends eat lunch at fast-foodrestaurants. Would it help you to learn how to makehealthier food choices at these restaurants?”
General Strategies
Action Plans (cont.)

261
TOOL G
Strategies Applications/QuestionsGeneral Strategies (cont.)
Talk about how to choose foods in various settings such asfast-food and other restaurants, convenience stores,vending machines, and friends’ homes.
Practice problem solving and role-playing (e.g., having thechild/adolescent ask the food server to hold themayonnaise).
“Your food record indicates that after having pepperonipizza for lunch yesterday, you ate a lighter dinner. That’s agood way to balance your food intake throughout the day.”
“Be as accurate and honest as you can as you record yourfood intake. This record is a tool to help you reflect on youreating behaviors.”
“What eating behaviors are you planning to work on beforeyour next appointment?”
Discuss the definition of words that may cause confusion,such as “fat,” “calories,” “meal,” and “snack.”
Use food models or household cups and bowls to clarifyserving sizes.
Discuss how to make healthy food choices in a variety ofsettings.
Provide the child/adolescent with learning experiences andskills practice.
Introduce the concept of achieving balance and enjoying allfoods in moderation.
Make recordkeeping easy, and tell the child/adolescent thatyou do not expect spelling, handwriting, and eatingbehaviors to be perfect.
Make sure that the child/adolescent hears what you aresaying.
Make sure that you and the child/adolescent define termsthe same way to avoid confusion.
When assessing food intake, keep in mind that a child’s/adolescent’s portion size may not be the same as a standardserving size.

TOOL
H
262
Keep Everything Clean• Wash hands before preparing or eating food and
after doing anything that interrupts either activity.
• Wash fresh fruits and vegetables carefully beforecooking them or eating them raw.
• Wash dishes in a dishwasher or in hot soapy waterusing a clean dishcloth. Don’t use sponges—theyoften spread germs. Rinse and sanitize dishes and letthem air dry.
• Wash cutting boards thoroughly with hot soapywater between uses for different foods, especiallyafter using it to cut raw meat. Only use cuttingboards made of nonporous materials.
Prepare Foods Properly• Cook foods thoroughly, especially foods containing
meat, poultry, fish, or eggs. Cook hamburger until itis brown or gray on the inside. Cook chicken untiljuices are clear when a knife or fork is stuck into it.Cook fish until it is opaque and flakes easily with afork. Cook eggs until they are firm.
• Thaw frozen foods in the refrigerator or under coldrunning water—never on the counter or in a bowlof standing water.
• When serving foods, make sure hot foods stayabove 140ºF and cold foods stay below 40ºF.
Store Food Safely• Serve cooked foods stored in the refrigerator within
24 hours.
• Store raw foods underneath cooked and ready-to-eatfoods in the refrigerator.
• Store dry ingredients (rice, sugar) in nonporouscontainers with tight-fitting lids.
• Cover and refrigerate or freeze cooked foods if theywill not be eaten right away.
• Leftovers that are refrigerated or frozen should bereheated one time only.
• Reheat liquids (gravy, soup, sauce) by bringingthem to a boil. Reheat solid foods at 165ºF.
• Store cleaning products and medications away fromfood and out of children’s reach.
Source: Graves DE, Suitor CW, Holt KA, eds. 1997. Making FoodHealthy and Safe for Children: How to Meet the National Health andSafety Performance Standards—Guidelines for Out-of-Home Child CarePrograms. Arlington, VA: National Center for Education in Maternaland Child Health.
Tool H: Tips for Promoting Food Safety

TOOL I
263
Tool I: Tips for Fostering a Positive Body Image Among Children and Adolescents
Look in the mirror and focus on yourpositive features, not the negativeones.
Say something nice to your friendsabout how they look.
Think about your positive traits thatare not related to appearance.
Read magazines with a critical eye,and find out what photographersand computer graphic designers doto make models look the way theydo.
If you are overweight and want tolose weight, be realistic in yourexpectations and aim for gradualchange.
Realize that everyone has a uniquesize and shape.
If you have questions about yoursize or weight, ask a healthprofessional.
Demonstrate healthy eatingbehaviors, and avoid extreme eatingbehaviors.
Focus on non–appearance-relatedtraits when discussing yourself andothers.
Praise your child or adolescent foracademic and other successes.
Analyze media messages with yourchild or adolescent.
Demonstrate that you love your childor adolescent regardless of what heweighs.
If your child or adolescent isoverweight, don’t criticize herappearance—offer support instead.
Share with a health professional anyconcerns you have about your child’sor adolescent’s eating behaviors orbody image.
Child or Adolescent Parents Health Professional
Discuss changes that occur duringadolescence.
Assess weight concerns and bodyimage.
If a child or adolescent has adistorted body image, explorecauses and discuss potentialconsequences.
Discuss how the media negativelyaffects a child’s or adolescent’sbody image.
Discuss the normal variation inbody sizes and shapes amongchildren and adolescents.
Educate parents, physicaleducation instructors, and coachesabout realistic and healthy bodyweight.
Emphasize the positivecharacteristics (appearance- andnon–appearance-related) ofchildren and adolescents you see.
Take extra time with an overweightchild or adolescent to discusspsychosocial concerns and weightcontrol options.
Refer children, adolescents, andparents with weight control issuesto a dietitian.

TOOL
J
264
Tool J: Nutrition Resources
General nutrition resources are listed first, followedby resources for specific nutrition issues andconcerns.
General Nutrition ResourcesAmerican Academy of Family Physicians11400 Tomahawk Creek ParkwayLeawood, KS 66211-2672Tel: (913) 906-6000Fax: (913) 906-6075Web site: http://aafp.org
American Academy of Pediatrics141 Northwest Point BoulevardElk Grove Village, IL 60007-1098Tel: (847) 434-4000Fax: (847) 434-8000Web site: http://www.aap.org
American Cancer Society1599 Clifton Road, N.E.Atlanta, GA 30329-4251Tel: (404) 320-3333, (800) 227-2345Fax: (404) 329-7530Web site: http://www.cancer.org
American College of Obstetricians and Gynecologists409 12th Street, S.W.P.O. Box 96920Washington, DC 20090-6920Tel: (202) 638-5577Fax: (202) 484-5107Web site: http://www.acog.org
American Dietetic Association216 West Jackson Boulevard, Suite 800Chicago, IL 60606-6995Tel: (312) 899-0040, R.D. Referral (800) 877-1600, ext. 5000Fax: (312) 899-4757Web site: http://www.eatright.org
American Medical Association515 North State StreetChicago, IL 60610Tel: (312) 464-5000Fax: (312) 464-4184Web site: http://www.ama-assn.org
American Nurses Association600 Maryland Avenue, S.W., Suite 100 WestWashington, DC 20024-2571Tel: (202) 651-7000, (800) 274-4ANA (4262)Fax: (202) 651-7001Web site: http://www.ana.org
American Psychological Association750 First Street, N.E.Washington, DC 20002-4242Tel: (202) 336-5500, (800) 374-2721Fax: (202) 336-6069Web site: http://www.apa.org
American Public Health Association800 I Street, N.W.Washington, DC 20001-3710Tel: (202) 777-APHAFax: (202) 777-2534Web site: http://www.apha.org

TOOL J
265
American School Food Services Association700 South Washington Street, Suite 300Alexandria, VA 22314Tel: (703) 739-3900, (800) 877-8822Fax: (703) 739-3915Web site: http://www.asfsa.org
American School Health AssociationFood and Nutrition Council7263 State Route 43, P.O. Box 708Kent, OH 44240-0708Tel: (330) 678-1601Fax: (330) 678-4526Web site: http://www.ashaweb.org
Association of State and TerritorialPublic Health Nutrition Directors
P.O. Box 1001Johnston, PA 15901-1001Tel and fax: (814) 255-2829
Center for Science in the Public Interest1875 Connecticut Avenue, N.W., Suite 300Washington, DC 20009-5728Tel: (202) 332-9110Fax: (202) 265-4954Web site: http://www.cspinet.org
Consumer Information Center1800 F Street, N.W., Room G-142, (XC)Washington, DC 20405Tel: (202) 501-1794, (800) 688-9889Fax: (202) 501-4281Web site: http://www.pueblo.gsa.gov
Food and Nutrition BoardInstitute of Medicine2101 Constitution Avenue, N.W.Washington, DC 20418Tel: (202) 334-1732Fax: (202) 334-2316Web site: http://www4.nationalacademies.org/iom/
iomhome.nsf/Pages/Food+and+Nutrition+Board
Food Research and Action Center1875 Connecticut Avenue, N.W., Suite 540Washington, DC 20009Tel: (202) 986-2200Fax: (202) 986-2525Web site: http://www.frac.org
Health Resources and Services AdministrationInformation Center
2070 Chain Bridge Road, Suite 450Vienna, VA 22182-2536Tel: (703) 356-1964, (888) ASK-HRSAFax: (703) 821-2098Web site: http://www.ask.hrsa.org
International Food Information Council1100 Connecticut Avenue, N.W., Suite 430Washington, DC 20036Tel: (202) 296-6540Fax: (202) 296-6547Web site: http://www.ific.org
International Life Sciences Institute1 Thomas Circle, N.W., Ninth FloorWashington, DC 20005Tel: (202) 659-0074Fax: (202) 659-3859Web site: http://www.ilsi.org
National Association of Pediatric Nurse Practitioners1101 Kings Highway, North, Suite 206Cherry Hill, NJ 08034-1912Tel: (856) 667-1773, (877) 662-7627Fax: (856) 667-7187Web site: http://www.napnap.org
National Association of Social Workers750 First Street, N.E., Suite 700Washington, DC 20002Tel: (202) 408-8600, (800) 638-8799Fax: (202) 336-8331Web site: http://www.socialworkers.org

TOOL
J
266
National Center for Education in Maternal and Child Health
Georgetown University2000 15th Street, North, Suite 701Arlington, VA 22201-2617Tel: (703) 524-7802Fax: (703) 524-9335Web site: http://www.ncemch.org
National Center for Nutrition and DieteticsAmerican Dietetic Association216 West Jackson BoulevardChicago, IL 60606-6995Tel: (800) 366-1655Fax: (312) 899-1739Web site: http://www.eatright.org/ncnd.html
National Center for Youth Law405 14th Street, 15th FloorOakland, CA 94612-2701Tel: (510) 835-8098Fax: (510) 835-8099Web site: http://www.youthlaw.org
National Food Service Management InstituteP.O. Drawer 188University, MS 38677-0188Tel: (662) 915-7658, (800) 321-3054Fax: (800) 321-3061Web site: http://www.olemiss.edu/depts/nfsmi
National Healthy Mothers, Healthy Babies Coalition121 North Washington Street, Suite 300Alexandria, VA 22314Tel: (703) 836-6110Fax: (703) 836-3470Web site: http://www.hmhb.org
National PTA330 North Wabash Avenue, Suite 2100Chicago, IL 60611-3690Tel: (800) 307-4PTA (4782)Fax: (312) 670-6783Web site: http://www.pta.org
National School Boards Association1680 Duke StreetAlexandria, VA 22314Tel: (703) 838-6722Fax: (703) 683-7590Web site: http://www.nsba.org
National WIC Association2001 S Street, N.W., Suite 580Washington, DC 20009-3355Tel: (202) 232-5492Fax: (202) 387-5281Web site: http://www.nwica.org
Society for Nutrition Education9202 North Meridian StreetIndianapolis, IN 46260Tel: (317) 571-5618, (800) 235-6690Fax: (317) 571-5603Web site: http://www.sne.org
U.S. Department of Agriculture
Center for Nutrition Policy and Promotion3101 Park Center Drive, Room 1034Alexandria, VA 22302-1594Tel: (703) 305-7600Fax: (703) 305-3400Web site: http://www.usda.gov/cnpp
Cooperative State Research, Education, and ExtensionService
800 9th Street, S.W., Room 4413Washington, DC 20024Tel: (202) 720-4651Fax: (202) 690-0289Web site: http://www.reeusda.gov

TOOL J
267
Expanded Food and Nutrition Education Program800 9th Street, S.W., Room 4413Washington, DC 20024Tel: (202) 720-6079Fax: (202) 690-2469Web site: http://www.reeusda.gov/
f4hn/efnep/efnep.htm
Food and Nutrition Service3101 Park Center Drive, Room 528Alexandria, VA 22302-1500Tel: (703) 305-2281Fax: (703) 305-2312Web site: http://www.fns.usda.gov/fns
Office of Analysis, Nutrition and EvaluationRoom 1014Tel: (703) 305-2017Fax: (703) 305-2576
Supplemental Food Programs DivisionRoom 528Tel: (703) 305-2052Fax: (703) 305-2196
National Agricultural LibraryFood and Nutrition Information Center10301 Baltimore Avenue, Room 105Beltsville, MD 20705-2351Tel: (301) 504-5719Fax: (301) 504-6409Web site: http://www.nal.usda.gov/fnic
U.S. Department of Health and Human Services
Centers for Disease Control and Prevention1600 Clifton RoadAtlanta, GA 30333Tel: (404) 639-3534, (800) 311-3435Fax: (404) 639-6290Web site: http://www.cdc.gov
Food and Drug AdministrationCenter for Food Safety and Applied Nutrition5100 Paint Branch ParkwayCollege Park, MD 20740-3835Tel: (202) 436-2373Fax: (202) 436-2636Web site: http://www.cfsan.fda.gov
Food and Drug AdministrationOffice of Consumer Affairs5600 Fishers Lane, HFE-88, Room 16-85Rockville, MD 20857Tel: (301) 827-4422, (888) 463-6332Fax: (301) 443-9767Web site: http://www.fda.gov
Indian Health ServiceOffice of Clinical and Preventive Services801 Thompson Avenue, Room 331Rockville, MD 20852Tel: (301) 443-0576Fax: (301) 594-6135Web site: http://www.ihs.gov
Maternal and Child Health BureauHealth Resources and Services Administration5600 Fishers LaneParklawn Building, Room 18A-55Rockville, MD 20857Tel: (301) 443-2340Fax: (301) 443-4842Web site: http://www.mchb.hrsa.gov
National Center for Health StatisticsCenters for Disease Control and Prevention6525 Belcrest RoadPresidential Building, Room 1064Hyattsville, MD 20782Tel: (301) 458-4636Web site: http://www.cdc.gov/nchs

TOOL
J
268
National Institutes of HealthNational Institute of Child Health
and Human Development ClearinghouseP.O. Box 3006Rockville, MD 20847Tel: (800) 370-2943Fax: (301) 984-1473Web site: http://www.nichd.nih.gov
National Institutes of HealthNational Institute of Diabetes and Digestive
and Kidney DiseasesDivision of Nutrition Research Coordination6707 Democracy Plaza, Sixth Floor, MSC 7973Bethesda, MD 20892-0001Tel: (301) 594-8822Fax: (301) 480-3768Web site: http://www.niddk.nih.gov/federal/
dnrc.htm
Office of Disease Prevention and Health Promotion200 Independence Avenue, S.W.Hubert H. Humphrey Building, Room 738GWashington, DC 20201Tel: (202) 401-6295Fax: (202) 205-9478Web site: http://www.odphp.osophs.dhhs.gov
Nutrition Issues and ConcernsBreastfeeding
The Academy of Breastfeeding MedicineP.O. Box 81323San Diego, CA 92138Tel: (619) 295-0058, (877) 836-9947Fax: (619) 295-0056Web site: http://www.bfmed.org
Best Start Social Marketing4809 East Busch Boulevard, Suite 104Tampa, FL 33617Tel: (813) 971-2119, (800) 277-4975Fax: (813) 971-2280
International Lactation Consultant Association1500 Sunday Drive, Suite 102Raleigh, NC 27607Tel: (919) 787-5181Fax: (919) 787-4916Web site: http://www.ilca.org
La Leche League International1400 North Meacham RoadSchaumburg, IL 60173-4808Tel: (847) 519-7730Fax: (847) 519-0035Web site: http://www.lalecheleague.org
Children and Adolescentswith Special Health Care Needs
American Association of Mental Retardation444 North Capitol Street, N.W., Suite 846Washington, DC 20001-1512Tel: (202) 387-1968, (800) 424-3688Fax: (202) 387-2193Web site: http://www.aamr.org
Easter Seals230 West Monroe Street, Suite 1800Chicago, IL 60606Tel: (312) 726-6200, (800) 221-6827, TTY (312) 726-4258Fax: (312) 726-1494Web site: http://www.easter-seals.org
Family Voices3411 Candelaria N.E., Suite MAlbuquerque, NM 87107Tel: (505) 872-4774, (888) 835-5669Fax: (505) 872-4780Web site: http://www.familyvoices.org

TOOL J
269
March of Dimes1275 Mamaroneck AvenueWhite Plains, NY 10605Tel: (914) 428-7100, (888) MODIMES (663-4637)Fax: (914) 428-8203Web site: http://www.modimes.org
National Information Centerfor Children and Youth with Disabilities
P.O. Box 1492Washington, DC 20013-1492Tel: (202) 884-8200, (800) 695-0285Fax: (202) 884-8441Web site: http://www.nichcy.org
National Parent Network on Disabilities1130 17th Street, N.W., Suite 400Washington, DC 20036Tel: (202) 463-2299Fax: (202) 463-9405Web site: http://www.npnd.org
Diabetes Mellitus
American Diabetes Association1701 North Beauregard StreetAlexandria, VA 22311Tel: (703) 549-1500, (800) DIABETES (342-2383)Fax: (703) 549-6995Web site: http://www.diabetes.org
International Diabetes Center3800 Park Nicollet BoulevardMinneapolis, MN 55416-2699Tel: (888) 825-6315, (952) 993-3393Fax: (952) 993-1302Web site: http://www.idcdiabetes.org
Juvenile Diabetes Foundation International120 Wall Street, 19th FloorNew York, NY 10005-4001Tel: (212) 785-9500, (800) 533-2873Fax: (212) 785-9595Web site: http://www.jdf.org
National Diabetes Information Clearinghouse1 Information WayBethesda, MD 20892-3560Tel: (301) 654-3327, (800) 860-8747Fax: (301) 907-8906Web site: http://www.niddk.nih.gov/health/
diabetes/ndic.htm
Eating Disorders
National Eating Disorders Association603 Stewart Street, Suite 803Seattle, WA 98101Tel: (206) 382-3587; information and
referral: (800) 931-2237Fax: (206) 829-8501Web site: http://www.nationaleatingdisorders.org
National Association of Anorexia Nervosa and Associated Disorders
P.O. Box 7Highland Park, IL 60035Tel: (847) 831-3438Fax: (847) 433-4632Web site: http://www.anad.org
Food Allergy
American Academy of Allergy, Asthmaand Immunology
611 East Wells StreetMilwaukee, WI 53202Tel: (414) 272-6071, (800) 822-2762Fax: (414) 272-6070Web site: http://www.aaaai.org
Food Allergy Network and Anaphylaxis Network10400 Eaton Place, Suite 107Fairfax, VA 22030-2208Tel: (800) 929-4040Fax: (703) 691-2713Web site: http://www.foodallergy.org

TOOL
J
270
National Institute of Allergy and Infectious Diseases31 Center DriveBuilding 31, Room 7A-50, MSC 2520Bethesda, MD 20892-2520Tel: (301) 496-5717Fax: (301) 402-0120Web site: http://www.niaid.nih.gov
Human Immunodeficiency Virus
American Foundation for AIDS Research120 Wall Street, 13th FloorNew York, NY 10005-3902Tel: (212) 806-1600Fax: (212) 806-1601Web site: http://www.amfar.org
National Center for HIV, STD and TB PreventionCenters for Disease Control and Prevention1600 Clifton Road, N.E.Atlanta, GA 30333Tel: (404) 639-3311Fax: (404) 639-8600Web site: http://www.cdc.gov/nchstp/od/nchstp.html
National Pediatric and Family HIV Resource Center30 Bergen Street, ADMC No. 4Newark, NJ 07103Tel: (973) 972-0410, (800) 362-0071Fax: (973) 972-0399Web site: http://www.pedhivaids.org
Hyperlipidemia
American Heart Association7272 Greenville AvenueDallas, TX 75231Tel: (214) 373-6300, (800) 242-8721Fax: (214) 373-0268Web site: http://www.americanheart.org
Hypertension
American Society of Hypertension515 Madison Avenue, Suite 1212New York, NY 10022Tel: (212) 644-0650Fax: (212) 644-0658Web site: http://www.ash-us.org
Nutrition and Sports
American Alliance for Health, Physical Education,Recreation, and Dance
1900 Association DriveReston, VA 20191-1598Tel: (703) 476-3400, (800) 213-7193Fax: (703) 476-9527Web site: http://www.aahperd.org
American College of Sports Medicine401 West Michigan StreetIndianapolis, IN 46202-3233Tel: (317) 637-9200Fax: (317) 634-7817Web site: http://www.acsm.org
Disabled Sports USA451 Hungerford Drive, Suite 100Rockville, MD 20850Tel: (301) 217-0960Fax: (301) 217-0968Web site: www.dsusa.org
International Center for Sports Nutrition502 South 44th Street, Suite 3007Omaha, NE 68105Tel: (402) 559-5505Fax: (402) 559-7302

TOOL J
271
National Association for Health and Fitness401 West Michigan StreetIndianapolis, IN 46202-3233Tel: (317) 955-0957Fax: (317) 634-7817Web site: http://www.physicalfitness.org
National Association for Sport and Physical Education1900 Association DriveReston, VA 20191-1598Tel: (703) 476-3410, (800) 213-7193, ext. 410Fax: (703) 476-8316Web site: http://www.aahperd.org/naspe/template.cfm?
template=main.htm
National Recreation and Park Association22377 Belmont Ridge RoadAshburn, VA 20148-4501Tel: (703) 858-0784Fax: (703) 858-0794Web site: http://www.activeparks.org
National Sports Center for the DisabledP.O. Box 1290Winter Park, CO 80482Tel: (970) 726-1540, (303) 316-1540Fax: (970) 726-4112Web site: http://www.nscd.org
President’s Council on Physical Fitness and Sports200 Independence Avenue, S.W., Room 738-HWashington, DC 20201-0004Tel: (202) 690-9000Fax: (202) 690-5211Web site: http://www.fitness.gov
Special Olympics International1325 G Street, N.W., Suite 500Washington, DC 20005Tel: (202) 628-3630Fax: (202) 824-0200Web site: http://www.specialolympics.org
Obesity
American Obesity Association1250 24th Street, N.W., Suite 300Washington, DC 20037Tel: (202) 776-7711, (800) 98-OBESE (986-2373)Fax: (202) 776-7712Web site: http://www.obesity.org
Weight-Control Information Network1 WIN WayBethesda, MD 20892-3665Tel: (202) 828-1025, (877) 946-4627Fax: (202) 828-1028Web site: http://www.niddk.nih.gov/health/
nutrit/win.htm
Oral Health
American Academy of Pediatric Dentistry211 East Chicago Avenue, Suite 700Chicago, IL 60611-2663Tel: (312) 337-2169Fax: (312) 337-6329Web site: http://www.aapd.org
American Association of Public Health Dentistry1224 Centre West, Suite 400BSpringfield IL 62704Tel: (217) 391-0218Fax: (217) 793-0041Web Site: http://www.aaphd.org
American Dental Association211 East Chicago AvenueChicago, IL 60611-2678Tel: (312) 440-2500Fax: (312) 440-2800Web site: http://www.ada.org

272
American Dental Hygienists’ Association444 North Michigan Avenue, Suite 3400Chicago, IL 60611Tel: (312) 440-8900Fax: (312) 440-6780Web site: http://www.adha.org
Vegetarian Eating Practices
The Vegetarian Resource GroupP.O. Box 1463Baltimore, MD 21203Tel: (410) 366-8343Fax: (410) 366-8804Web site: http://www.vrg.org
TOOL
J

Due to copyright permissions restrictions, this tool is not
available on the Web. Please see print version of the nutrition guide.
273
TOOL K
Tool K: Federal Food Assistanceand Nutrition Programs
Source: Adapted, with permission, from Table 4-3 of Kaufman M. 1990. Nutrition in Public Health: A Handbook for Developing Programs andServices. Gaithersburg, MD: Aspen Publishers. Copyright © 1990 Aspen Publishers, Inc.

278
Tool L: Healthy People 2010Nutrition Objectives for Children and Adolescents
Healthy People 20101 provides a comprehensivehealth promotion and disease prevention agenda for thenation. The publication’s focus is on improving thehealth of individuals, communities, and the nation.
Healthy People 2010 includes 467 health objectives in 28focus areas. For each objective, there is a 2010 target. Theobjective, target, and baseline information for objectivespertaining to the nutritional status of children andadolescents are listed in Table 24 below.
TOOL
L
Table 24. Nutrition Objectives for Children and Adolescents
Objective Number
1-3
5-1
5-2
7-2h
10-5
Objective, Target, and Baseline
Increase the proportion of persons appropriately counseled about health behaviors.
Increase the proportion of persons with diabetes who receive formal diabeteseducation.
Target: 60 percent.
Baseline: 40 percent of persons with diabetes received formal diabetes education in1998 (age adjusted to the year 2000 standard population).
Prevent diabetes.
Target: 2.5 new cases per 1,000 persons per year.
Baseline: 3.1 new cases of diabetes per 1,000 persons (3-year average) in 1994–1996.
Increase the proportion of middle, junior high, and senior high schools that providecomprehensive school health education to prevent unhealthy dietary patterns.
Target: 95 percent.
Baseline: 84 percent in 1994.
Increase the proportion of consumers who follow key food safety practices.
Target: 79 percent.
Baseline: 72 percent of consumers followed key food safety practices in 1998.

279
TOOL L
16-19
16-19a
16-19b
16-19c
19-3
19-3a
19-3b
19-3c
19-4
19-5
Increase the proportion of mothers who breastfeed their babies.
In early postpartum period:
Target: 75 percent.
Baseline: 64 percent in 1998.
At 6 months:
Target: 50 percent.
Baseline: 29 percent in 1998.
At 1 year:
Target: 25 percent.
Baseline: 16 percent in 1998.
Reduce the proportion of children and adolescents who are overweight or obese.
Ages 6 to 11 years:
Target: 5 percent.
Baseline: 11 percent.
Ages 12 to 19 years:
Target: 5 percent.
Baseline: 10 percent.
Ages 6 to 19 years:
Target: 5 percent.
Baseline: 11 percent.
Reduce growth retardation among low-income children under age 5 years.
Target: 5 percent.
Baseline: 8 percent in 1997.
Increase the proportion of persons ages 2 years and older who consume at least twodaily servings of fruit.
Target: 75 percent.
Baseline: 28 percent in 1994–1996.
Objective Number
Objective, Target, and Baseline

280
TOOL
L
19-6
19-7
19-8
19-9
19-10
19-11
19-12
19-12a
Increase the proportion of persons ages 2 years and older who consume at least threedaily servings of vegetables, with at least one-third being dark green or deep yellowvegetables.
Target: 50 percent.
Baseline: 3 percent in 1994–1996.
Increase the proportion of persons ages 2 years and older who consume at least sixdaily servings of grain products with at least three being whole grains.
Target: 50 percent.
Baseline: 7 percent in 1994–1996.
Increase the proportion of persons ages 2 years and older who consume less than 10percent of calories from saturated fat.
Target: 75 percent.
Baseline: 36 percent in 1994–1996.
Increase the proportion of persons ages 2 years and older who consume no more than30 percent of calories from fat.
Target: 75 percent.
Baseline: 33 percent in 1994–1996.
Increase the proportion of persons ages 2 years and older who consume 2,400 mg orless of sodium daily.
Target: 65 percent.
Baseline: 21 percent in 1988–1994.
Increase the proportion of persons ages 2 years and older who meet dietaryrecommendations for calcium.
Target: 75 percent.
Baseline: 46 percent in 1988–1994.
Reduce iron deficiency among young children and females of childbearing age.
Children ages 1 to 2 years:
Target: 5 percent.
Baseline: 9 percent in 1988–1994.
Objective Number
Objective, Target, and Baseline

281
TOOL L
19-12b
19-12c
19-15
19-18
Children ages 3 to 4 years.
Target: 1 percent.
Baseline: 4 percent in 1988–1994.
Nonpregnant females ages 12 to 49 years.
Target: 7 percent.
Baseline: 11 percent in 1988–1994.
Increase the proportion of children and adolescents ages 6 to 19 years whose intake ofmeals and snacks at schools contributes proportionally to good overall dietary quality.
Increase food security among U.S. households and in so doing reduce hunger.
Target: 94 percent.
Baseline: 88 percent in 1995.
Objective Number
Objective, Target, and Baseline
Reference1. U.S. Department of Health and Human Services. 2000. Healthy People 2010: National Health Promotion and Disease
Prevention Objectives (2nd ed.). Washington, DC: U.S. Department of Health and Human Services.

282
The Centers for Disease Control and Prevention(CDC) pediatric growth charts included in the pocket ofthis guide are widely used as clinical and research tools toassess nutrition status and the general health and well-being of infants, children, and adolescents. The followinggender-specific growth charts are available:
■ Charts for infants, birth to 36 months, which provideweight-for-age, length-for-age, weight-for-length, andhead circumference-for-age percentiles
■ A chart for children, 2 to 6 years, which provideweight-for-stature percentiles
■ Charts for children and adolescents, 2 to 20 years,which provide weight-for-age, stature-for-age, andbody-mass-index (BMI)-for-age percentiles
The growth charts are available and can bedownloaded from the CDCs Web site: http://www.cdc.gov/growthcharts
The CDC growth charts include gender-specific BMI-for-age charts. BMI is calculated by dividing body weightin kilograms by height in meters squared(kg/m2). BMIcorrelates with an individual’s total body fat content orpercentage of body fat. BMI can be used to monitorchanges in body weight and to consistently assess risk ofunderweight and overweight in children and adolescents2 to 20 years.
The interpretation of BMI depends on the child’s oradolescent’s age. Established cut-off points should be usedto identify underweight and overweight children andadolescents. The following BMI-for-age percentile cutoffsmay indicate a health risk; in these cases, further medicalassessment (including diet, physical activity, andlaboratory measures) is recommended.
■ Underweight: BMI-for-age less than the 5th percentile
■ At risk for overweight: BMI-for-age greater than orequal to the 85th percentile but less than the 95thpercentile
■ Overweight: BMI-for-age greater than or equal to the95th percentile
Suggested ReadingHealth Resources and Services Administration, Maternal and
Child Health Bureau; Centers for Disease Control and
Prevention. 2002. Growth Charts Training. Available at
http://128.232.56/mchbgrowthcharts/module4/text/
mainmodules.htm.
TOOL
M Tool M: CDC Growth Charts
![[PPT]Kitchen Utensils and Equipment - Wikispacesbrennanfcs.wikispaces.com/file/view/Kitchen+Utensils+PPT... · Web viewKitchen Utensils and Equipment East High School Nutrition and](https://img.dokumen.tips/doc/110x75/5abe05ea7f8b9a7e418c6109/pptkitchen-utensils-and-equipment-utensilspptweb-viewkitchen-utensils-and.jpg)