Embed Size (px)
DESCRIPTION
nnn
Citation preview

THE RESULT OF TREATING CHILDREN’S ACUTE LYMPHOBLASTIC LEUKEMIA (ALL) IN DR. SARDJITO HOSPITAL WITH WK-ALL
PROTOCOL, 1999-2002
Mulatsih S, Sumadiono, Sutaryo, Purwanto
Division of Childhood Hematology-Oncology, Faculty of Medicine, Gadjah Mada University, Yogyakarta, Indonesia
Abstract.Background. After1994 the Indonesian Pediatric Oncology Working Group started using high and intermediate-dose methotrexate for pediatric ALL. However, the numbers of dropouts were high because of financial constraints. In 1999, the Wijaya Kusuma (WK-ALL) protocol was developed as an intended cost-effective treatment.Objectives. To evaluate and to investigate the Overall Survival (OS), Disease Free Survival (DFS) of our ALL patients.Material and Method. Between January 1st 1999 to December 31st 2002, 113 children younger than 15 y, with newly diagnosed ALL in Dr. Sardjito Hospital, Yogyakarta were retrospectively analyzed. Until December 31st 2004, patients were treated with WK-ALL protocol.Results. Of the 113 patients who started on the WK-ALL protocol, 15 (13%) dropped out and 14 (12%) died during induction, and 6 (5%) did not achieve complete remission. Of the 78 (69%) who achieved complete remission, 29 (37%) relapsed, whereas 17 (59%) in the bone marrow. Overall, 26/113 patients (23%) dropped out from therapy, more than a half (58%) in induction. Of the remaining 87 patients, 25 (29%) died from complication: 14 (16%) in induction, 11 (13%) after induction. Septicemia was considered the causes of death in 11 (44%). Six years overall OS, DFS, are 62/87 (71%), 27/87 (31%) respectively. Conclusion. Drop out (23%) still a major reason of failure, and probably non-compliance is also a big problem. Almost one third of patients were lost through complications. Septicemia is a major cause of death. Relapse at 37% is reasonable for a basic protocol, and non-compliance may be part of the background. Currently, 27 patients (31%) survive Disease-free, after median follow-up of almost 3 years.
Abstrak.Latar belakang. Sejak tahun 1994, Unit Kelompok Kerja Hematologi Onkologi Anak IDAI telah menerapkan pemberian methotrexat dosis tinggi dan menengah untuk anak-anak penderita ALL. Namun didapatkan angka drop-out yang tinggi terkait masalah biaya. Sejak tahun 1999, dengan pertimbangan efektivitas dan biaya dikembangkan protocol WKRL.Tujuan. Meneliti dan mengevaluasi penderita yang hidup (overall survival) dan penderita yang bebas dari penyakit (disease free survival) dari seluruh penderita ALL yang kami rawat.Bahan dan cara kerja. Penelitian retrospektif. Data penderita ALL anak baru di RS Dr. Sardjito Yogyakarta mulai 1 Januari 1999 hingga 31 Desember 2002 dianalisis. Terdapat 113 anak berumur < 15 tahun yang mendapatkan terapi dengan protocol WKRL.Hasil. 113 penderita baru ALL menjalani terapi dengan protokol WKRL. 15 (13%) drop out dan 14 (12%) meninggal saat fase induksi, 6 (5%) tidak mencapai remisi komplit. Dari 78 (69%) yang mencapai remisi komplit, 29 (37%) mengalami relaps, di mana 17 (59%) dibuktikan dengan aspirasi sumsum tulang. Secara keseluruhan, 26 dari 113 penderita (23%) yang drop out dari terapi, lebih dari separoh (58%) saat fase induksi. Sisanya 87 penderita, 25 (29%) meninggal oleh karena komplikasi: 14 (16%) saat induksi, 11 (13%) setelah induksi. Septicemia menjadi penyebab kematian pada 11 (44%) penderita. Selama 6 tahun penelitian, penderita yang hidup secara keseluruhan adalah 62/87 (71%), dan 27/87 (31%) dinyatakan bebas penyakit.Kesimpulan. Drop out masih merupakan alasan kegagalan terapi yang utama (23%), yang kemungkinan akibat faktor ketidak-patuhan. Hampir 1/3 penderita meninggal akibat komplikasi. Septicemia merupakn penyebab kematian yang utama. Angka relaps sebesar 37% masih bisa diterima untuk terapi dasar, hal ini kemungkinan besar oleh karena faktor ketidak-patuhan. Dalam kurun hampir 3 tahun follow-up didapatkan 27 (31%) penderita yang terbebas dari penyakit.
1

Keywords: Acute lymphoblastic Leukemia-WK-ALL protocol-Survival
INTRODUCTION
The outlook for children with ALL has improved dramatically. However, up to now, Indonesia has not yet had a national protocol for acute lymphoblastic leukemia (ALL). Starting in 1998, when we have national workshop meeting for Indonesian pediatric oncologist in Yogyakarta, Indonesia, The Wijaya Kusuma (WK) ALL protocol was borne. This description was taken for the economical constraints. Since 1999, we have WK ALL-protocol study. This protocol was developed in order to improve the cure and survival rates of childhood ALL with still consider the cost effectiveness of the regimen. In our study, all children with newly diagnosed acute lymphoblastic leukemia (ALL) were classified into two subgroups according to age, white blood cell (WBC), organomegaly, and risk group.
PATIENTS AND METHODS
Patients.
Between January 1999 and December 2002, 113 children with ALL L1 and L2
who below 15 years of age, and have no treatment previously with corticosteroid or
chemotherapy started on WK-ALL protocol. Diagnosis and therapy was centralized to the
Department of pediatric, DR. Sardjito Hospital, Yogyakarta. Informed consent was
obtained according the inform consent form Hospital Medical Record.
The diagnosis was established by analyzing bone marrow aspirates, including
standard morphology according to the French-American-British (FAB) classification
(Bennett et al, 1985). Percentage of blasts cell at least 25%.
The criteria of high risk group were less than 1 year or more than 10 years old;
white blood cell count (WBC) more than 50,000/ul; present of mediastinal mass
according the chest x ray, present of CNS (Central Nervous System) leukemia cells.
Beside that, if the blast in peripheral blood still more than 1000/ul after one week with
dexamethazone, must be include to the high-risk group. CNS involvement was diagnosis
2
if more than 5 leucocytes/ill were identified in the cerebrospinal fluid (CSF) in
combination with detectable leukemia cells in the cytospin and/ or with occurrence of
neurological symptoms (e.g. cranial nerve palsy).
Complete remission (CR) was defined as a normocellular bone marrow (BM) with
less than 5%. BM aspiration was done at 42 days induction or after complete treatment,
no blasts cells in peripheral blood, no CNS leukemia, and no infiltration of leukemia cells
in others organ. Partial remission (PR) was defined as a normocellular BM with blasts
cell 5 to 20% in 200 nuclear cells.
Relapse was defined as presenting blast cells more than 20% in 200 nuclear cells
in BM, and/or presenting of blats cells in peripheral blood, and/or presenting of blast cells
in CSF slide at least twice with interval 24 hours or more, and/or present of leukemia cell
infiltration in others organ.
Treatment Protocol
The treatment outline of WK-ALL protocol is shown in Figure 1. One-induction
courses were followed by consolidation, re-induction, and maintenance courses. For the
standard risk group, without re-induction. The chemotherapy for induction consist
dexamethazone orally 6 mg/m2, Vinvristine 1.5 mg/m2 (maximum dose was 2 mg) iv, at
day 7, 14, 21, 28 and 35 (diluted with normal saline or aquadest until 10 ml, bolus slowly
duration 5-10 minutes); Daunorubicine (just for high risk group) 30 mg/m2 4-h infusion;
L-Asparagines (L-Asp) 6,000 u/m2 4-h infusion; Intrathecal methotrexate was given on
the first day, 14, and 42 at age-adjusted doses: below 1 year, 6 mg; 1 year old, 8 mg; 2
year old 10 mg; 3 years and older, 12 mg. Leucopenia and/ or thrombocytopenia was not
indication to reduce the dose of chemotherapy in this course. If allergic reaction was
found with L-Asp (produce fro E-coli), the treatment can continue with Erwina Caratova
with the same doses, or antihistamine can be use for allergic reaction.
Several courses of intensive post-remission chemotherapy combining non-cross
resistant agents, administered every week, 4 to 6 weeks. Randomized studies have been
conducted to compare the efficacy of different consolidation L-Asparagines and placebo
for ALL patients. Combination of L-Asparagines and Daunorubicine has been given as a
re-induction treatment for high-risk group. Consolidation consisted of combination 6-MP
3

50 mg/m2 orally; intrathecal MTX it at week 10, 11, and 12; L-Asp 6,000 u/m2 IV at
week 7, 8, and 9, 4-h infusion. Re-induction consisted intrathecal MTX at week 13 and
17; dexamethazone orally 6 mg/m2 3 doses since week 13 to 18; daunorubicine 30
mg/m2 4-h infusion at week 13, 15, and 17; L-Asp 6,000 u/m2 at week 13, 15, and 17.
Statistical analysis.
The STATISTICAL PACKAGE FOR THE SOCIAL SCIENCES (SPSS)
software was used in the statistical analysis. The probability of Overall Survival (OS),
Events Free Survival (EFS), and Disease-free Survival (DFS) were calculated using the
Kaplan-Meier method. In the analysis of OS, events included all patients who were
surviving since at diagnosis. EFS, events included induction failure (early death, death in
aplasia and resistant disease), death in remission, relapse disease. Children who did not
achieve remission were excluded from analysis of DFS (Mantel, 1966).
Figure 1. The Outline of WK-ALL-SR protocol
Figure 2. The Outline of WK-ALL-HR protocol
4
RESULTS
Patients Characteristic
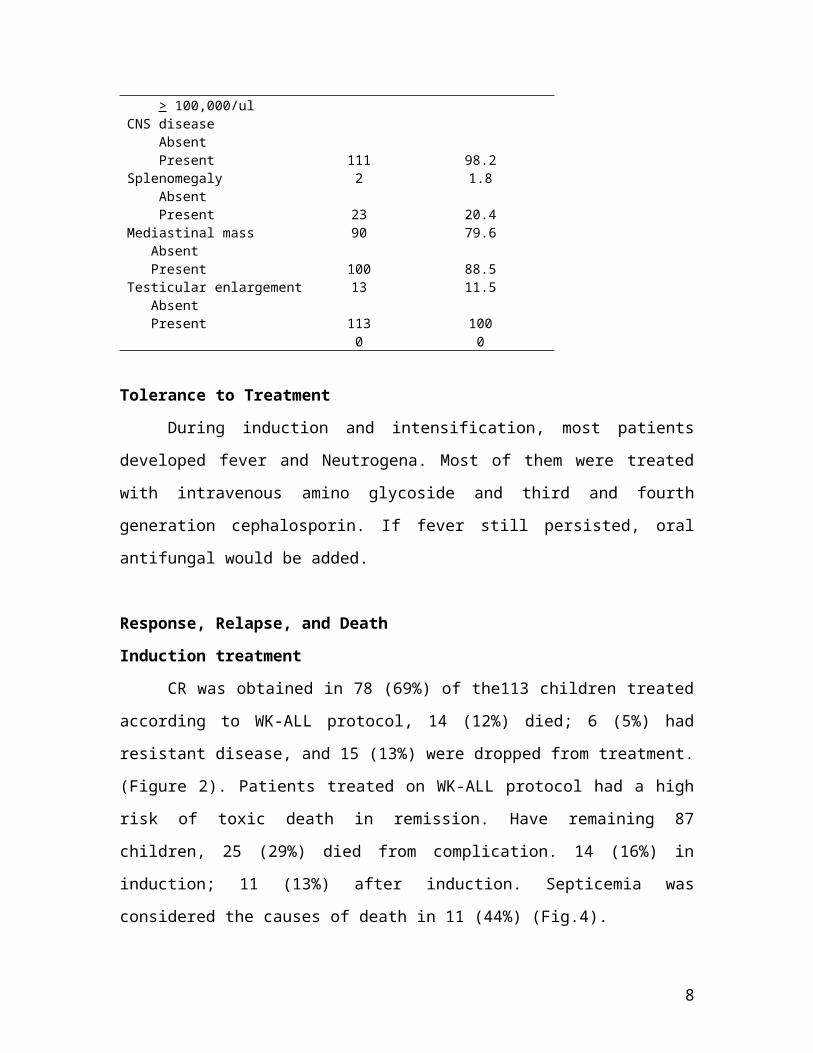
WK-ALL protocol study included a total 113 patients: the clinical characteristics
are presented in Table I. One patient (0.9%) was less than 1 year of age, 14 (12.4%) were
10 to 15-years old at diagnosis. Twenty-seven patients (23.9%) of the children had WBC
> 50,000/ul.
TABLE I. Patient Characteristics
Feature Total (n= 113) Percentage (%)
Sex Male FemaleAge at diagnosis < 1 years 1-9 years 10-15 yearsWBC < 10,000/ul > 10,000-50,000/ul > 50,000-100,000/ul > 100,000/ulCNS disease Absent PresentSplenomegaly Absent PresentMediastinal mass Absent PresentTesticular enlargement Absent Present
6251
19814
58281314
1112
2390
10013
1130
5545
0.986.712.4
51.324.811.512.4
98.21.8
20.479.6
88.511.5
1000
5
Tolerance to Treatment
During induction and intensification, most patients developed fever and
Neutrogena. Most of them were treated with intravenous amino glycoside and third and
fourth generation cephalosporin. If fever still persisted, oral antifungal would be added.
Response, Relapse, and Death
Induction treatment
CR was obtained in 78 (69%) of the113 children treated according to WK-ALL
protocol, 14 (12%) died; 6 (5%) had resistant disease, and 15 (13%) were dropped from
treatment. (Figure 2). Patients treated on WK-ALL protocol had a high risk of toxic death
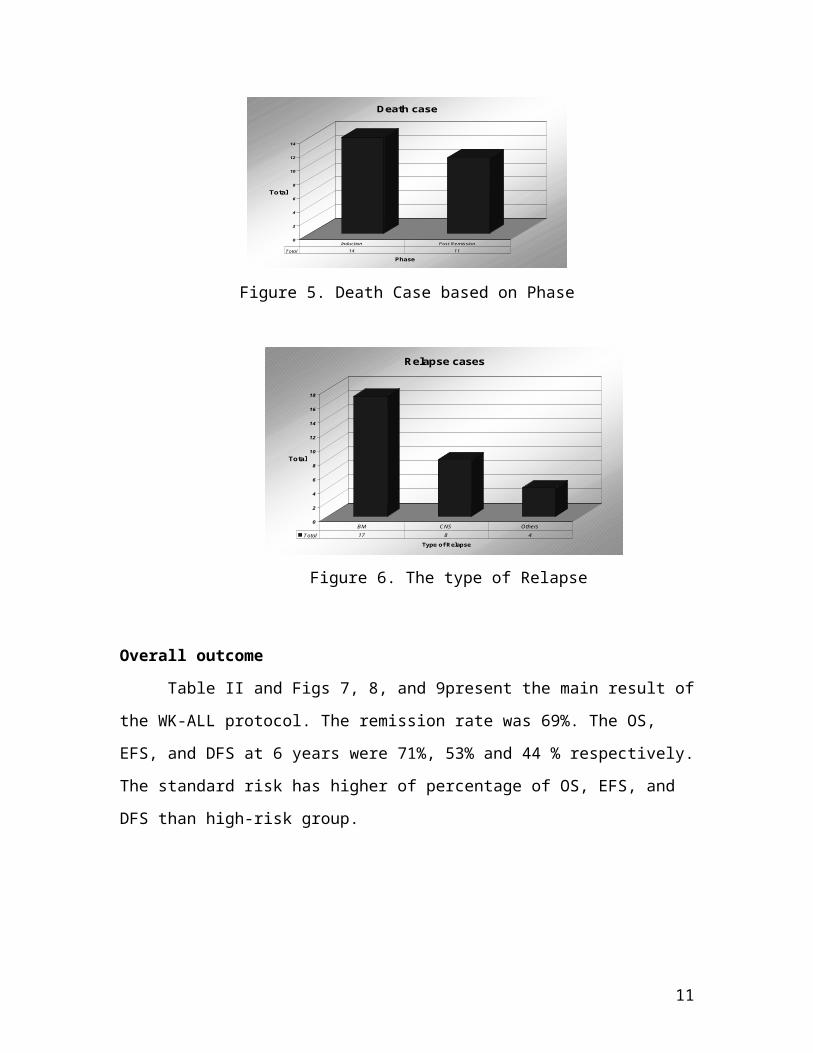
in remission. Have remaining 87 children, 25 (29%) died from complication. 14 (16%) in
induction; 11 (13%) after induction. Septicemia was considered the causes of death in 11
(44%) (Fig.4).
Post-remission therapy
The outcome according to post-remission treatment is shown in Fig. 4. Of the 78
patients who achieved complete remission, 29 (37%) were relapse; 11(14%) died; and 11
(14%) dropped out from treatment (Figure 3). Of the 78 patients who achieved complete
remission, 29 patients (27%) relapsed. The relapses were predominantly located in the
bone marrow (59%). Eight patients (28%) suffered from CNS relapse, and 4 (13%) with
others relapsed (Fig.6). Most relapse occurred within the maintenance course.
Dropped out on WK-ALL protocol
Overall, 26/113 children (23%) dropped out from therapy, whereas 15 (58%) in
induction, and 11 (42%) after remission (Fig.5)
Table II. Main outcomes of WK-ALL
Standard Risk High Risk TotalN % N % N %
All patientsEarly deathResistant disease
6862
604333
4584
405767
113146
100
6

RemissionRelapseDeath in CRCCR 12/2004
OS at 6 yearsEFS at 6 yearsDFS at 6 years
5120727
65746477
774138
27748
35263623
613926
78271135
Overall715344
0
10
20
30
40
50
60
70
80
Total
Dropped out Died Persistant disease Remission
Response
Response of Induction Treatment
Figure 3. Response of Induction Treatment
0
5
10
15
20
25
30
Total
Relapse Died Dropped out
outcome
Post-remission therapy
Figure 4. Post-remission Therapy
7
0
2
4
6
8
10
12
14
Total
Phase
Death case
Total 14 11
Induction Post Remission
Figure 5. Death Case based on Phase
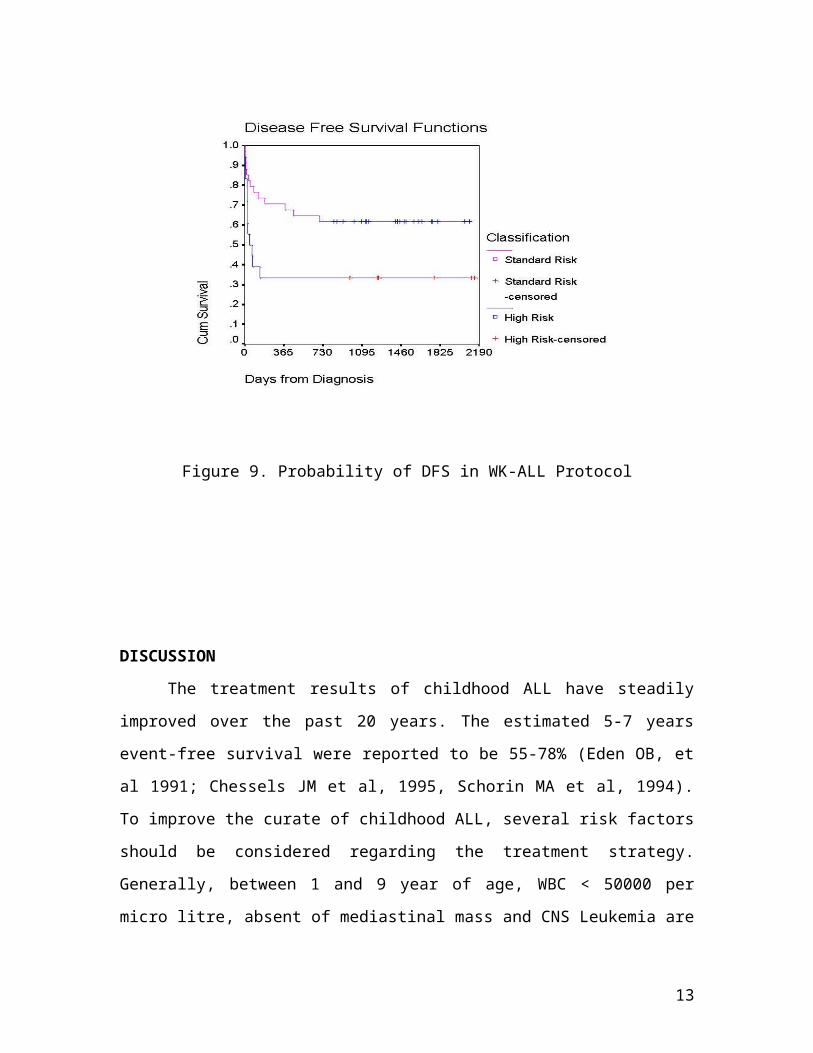
Overall outcome
Table II and Figs 7, 8, and 9present the main result of the WK-ALL protocol. The
remission rate was 69%. The OS, EFS, and DFS at 6 years were 71%, 53% and 44 %
respectively. The standard risk has higher of percentage of OS, EFS, and DFS than high-
risk group.
0
2
4
6
8
10
12
14
16
18
Total
Type of Relapse
Relapse cases
Total 17 8 4
BM CNS Others
Figure 6. The type of Relapse
8

Figure 7. Probability of Survival in WK-ALL protocol
Figure 8. Probability of EFS in WK-ALL Protocol
9
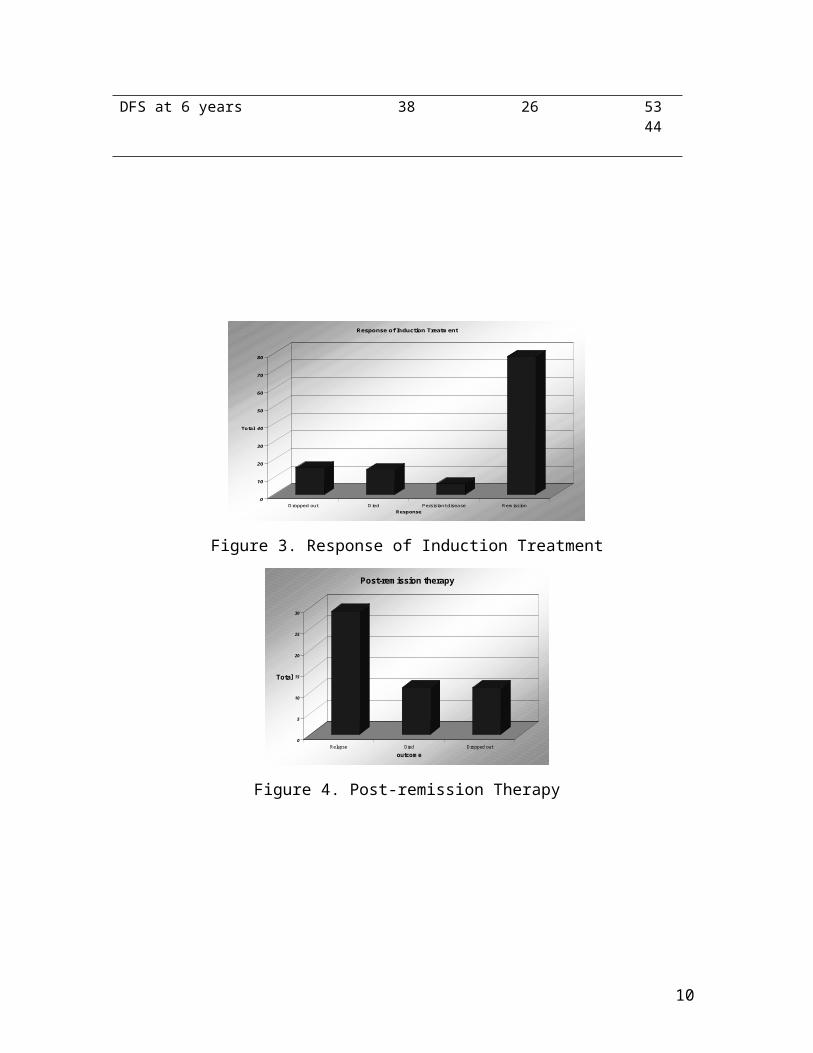
Figure 9. Probability of DFS in WK-ALL Protocol
DISCUSSION
The treatment results of childhood ALL have steadily improved over the past 20
years. The estimated 5-7 years event-free survival were reported to be 55-78% (Eden OB,
et al 1991; Chessels JM et al, 1995, Schorin MA et al, 1994). To improve the curate of
childhood ALL, several risk factors should be considered regarding the treatment
strategy. Generally, between 1 and 9 year of age, WBC < 50000 per micro litre, absent of
mediastinal mass and CNS Leukemia are used as criteria for low-risk ALL. Based on the
concept in the current study all the ALL children patients were classified in to two
subgroup according those criteria as a high risk and standard risk patients.
Our analysis suggests that the dropout still is major reason of failure, and probable
non-compliance in the remaining passions is also big problem. Overall, 26 from 113
patients (23% were dropped out from therapy due to many problem for instant the
10
financial reason, critical conditions of passions, persistence of the blood cells (more than
1000 UL after one week receive bethametason. Some of the patients develops septicemia,
so, the chemotherapy had not been given properly, eleven patients (42% were dropped
out after remission do to the relapse). Our result similar with previously study. In both
Taiwan CCG studies, protocol TCL-821 and TCL-842 reported that there were also high
dropped out rates (32% and 16.8%). The authors postulated that the inferior results were
due lack of financial support to the families, pessimistic attitudes of the families and
some medical personnel, high remission death rates, and possibly the questionable
compliance with maintenance therapy. (Kong Shing MM, et al. 1999).
The second problem is toxic death, were as almost, one third of remaining patients
the lost though complication and septicemia is mayor cause of death. In our department
most of passions come from poor family while for the several period they did not get
funding from the government. In order to cover hospitalization cost, that was most
important reason for non-compliance. Treatment related mortality in London with
national multicentre study has been analyzed for induction and first remission (including
after intensification treatment). There was 2.3% induction death, whereas 84% of these
followed a bacterial and fungal infection. Thirty-seven infective remission deaths
occurred, which including caused by Pneumocystis carinii pneumonia (Wheeler K et al,
1996).
Relapse of leukemia (37%) was the main cause of treatment failure. As compared
with the MRC UKALL X study in Hong Kong we have a higher incidence of relapses
(24.6%) (Kong Shing at al, 1999).
Large part of the improvement in survival is clearly attributable to advances in
treatment methods, particularly, the increasing efficacy of combination chemotherapy.
How ever not a children benefited equally from this development (Styler C.A., 1999).
Our analysis, six-years overall OS, EFS, and DFS, are 62/87 (71%), 33/62 (53%), and
27/62 (44%) respectively. The patterns survival for children ALL in UK, which treated
with UKALL protocol show, that 5-year survival rate was 70% during 1980-84, while in
1990-94 the rate was 70% (Stiller CA, 1999). The Hong Kong study has better result on
overall survival and EFS (75% and 66%), respectively with more aggressive treatment
(Kong Shing, et al, 1999). In Japan, one of ALL study was done in 2001 with AL90
11

regimen, and the result of 5-years EFS was 67.4% (Ishii E, et al, 2001). The standard risk
group has a superior of 6-years Survival, EFS, and DFS to the high-risk group (77% vs.
61%; 41% vs. 39%; 30% vs.26%) respectively. The EUROCARE study mentioned about
Variation in survival of European children with ALL. During 1985-1989, the 5-year
survival rate from over 80 to 56% (with the exception of Estonia; 34%; various country,
90%; and European weighted was 72%. Survival was particularly favorable in (south)
Sweden, Finland, Germany and The Netherlands and rather unfavorable in Estonia
(Coebergh JW, 2001). However, the incidence of relapse was higher in standard risk to
that high-risk group (36% vs. 23%). The possibility reason for that problem was, in our
study, the criteria for classified just based on FAB (France American British) criteria,
without any better supporting examination such as immunophenotyping, karyotyping;
criteria for remission still a conventional, no minimal residual disease examination. Based
on this fact, we do not know whether the patients really include in standard risk or should
be high risk. If we looked the protocol it self, the high-risk group received more drug
(daunorubicine) and added the one phase re-induction. Those possibilities reason might
cause a higher relapse cases in standard risk group.
For high-risk ALL, the WK-ALL –HR protocol regimen including induction,
consolidation, re-induction and maintenance therapies did not improve patient outcome.
Failure to achieve remission in the high-risk group was 9%. The added once
daunorubicine 30 mg/m2, did not give better CR for HR group.
CONCLUSION
The survival of children with ALL living in developing countries is lower than
that of children in developed countries. The failure of treatment mostly due to the lack of
financial support to the families, pessimistic attitudes of the families and some medical
personnel, high remission death rates, and possibly the questionable compliance with
maintenance therapy.
REFERENCES
12
1. Chessels JM, Bailey C, Richards SM., 1995. Intensification of treatment and
survival in all children with lymphoblastic leukemia: Results of UK Medical
Research Council Trial UKALL X. Lancet; 345:143-8.
2. Coebergh JW., Pastore G., Gatta G., Corazziari I., Kamps W., 2001. Variation in
survival of European children with acute lymphoblastic leukemia, diagnosed in
1978-1992:the EUROCARE study. European Journal of Cancer 37: 687-94.
3. Eden OB, Lilleyman JS, Richard S.,1991. Results of medical Research Council
Childhood Leukemia Trial UKALL VII (report to the Medical Research Council
on behalf of the working party on leukemia in childhood). Br J Haematol; 78:187-
96
4. Ishii E, Eguchi H., Matsuzaki A., Koga H., Yanai F., et al. 2001. Outcome of
Acute Lymphoblastic Leukemia in Children with AL90 Regimen: Impact of
Response to Treatment and Sex Difference on Prognostic Factors. Medical and
Pediatric Oncology 37:10-19.
5. Schorin MA, Blattner S, and Gelber RD., 1994. Treatment of childhood ALL:
Results of Dana-Farber Cancer Institute/Children’s Hospital Acute Lymphoblastic
Leukemia Consortium Protocol 85-01. J Clin Oncol:12:740-7.
6. Shing MMK, Li CK., Chik KA., Lam TK., Lai HDH., et al. 1999. Outcomes and
Prognostic Factors of Chinese Children with Acute Lymphoblastic Leukemia in
Hong Kong: Preliminary Results. Medical and Pediatric Oncology 32:117-23.
7. Stiller CA., Eatock EM., 1999. Patterns of care and survival for children with
acute lymphoblastic leukemia diagnosed between 1980 and 1994. Arch Dis Child;
81:202-8.
13

8. Wheeler K, Chessells JM., Baiely CC., Richards SM., 1996. Treatment related
deaths during induction and in first remission in acute lymphoblastic leukemia:
MRC UKALL X. Archives of Disease in Childhood;74: 101-7.
14

15





























