Embed Size (px)
Citation preview

SYNAPTIC

NERVOUS SYSTEM
NERVOUS SYSTEM
CENTRAL NERVOUS SYSTEM PERIPHERAL NERVOUS SYSTEM
Brain Spinal Cord Autonomic nervous system
Somatic nervous system
Sympathetic nervous system
Parasympathetic nervous system

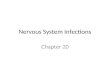
Acetylcholine (ACh): Synthesis and Breakdown
•Once released into the cleft, its rapidly broken down by the enzyme
acetylcholinesterase (AChE).
•Ch is transported back into the axon terminal and reused to make ACh.
•Made from
choline (Ch)
and acetyl
coenzyme
(acetyl CoA)
in the axon
terminal then
filled into
synaptic
vesicles.
•Synthesis
requires the
enzyme choline
acetyltransferase
(ChAT)

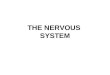
NEUROMUSCULAR JUNCTION ((( NMJ )))
• Transmission of neural impulse at the nerve terminal translated into skeletal muscle contraction at motor end plate

Junction between the
terminal of a motor neuron
and a muscle fiber.
One kind of synapse.
Also called myoneural
junction.
NEUROMUSCULAR JUNCTION


Acethylcholinesterase
• Synthesis in the muscle, under the end plate
• Secreted from the muscle but remains attached to it via thin stalk of collagen fastened to the basement membrane
• Destroy Ach that do not react immediately with receptor & that are released from binding sites.
• Ach is destroyed in < 1 ms after it is released.


INTRODUCTION
BRIEF HISTORY
PRINCIPLES OF
NEUROMUSCULAR
TRANSMISSION
MUSCLE RELAXANT
Ideal properties
Indications & Contraindication
Mechanism of action
Side effect

Before neuromuscular blocking introduce:
High concentration of inhalational anesthetic agent
Regional anesthesia
1942 curare (tubocurarine) introduce
Less anesthetic administered

What is a Muscle Relaxer?
• A muscle relaxer, also known as a muscle relaxant, is a drug which affects skeletal muscle function and decreases the muscle tone. It may be used to alleviate symptoms such as muscle spasms, pain.

Muscle Relaxer
block neuromuscular transmission
paralysis
presynaptically via the inhibition of acetylcholine
(ACh) synthesis or release .
postsynaptically at the acetylcholine receptor.
adjunct to anesthesia to induce paralysis

IDEAL PROPERTIES OF MUSCLE RELAXANT
Rapid onset (1 min)
To avoid hypoxia & aspiration of gastric content
Nondepolarizing
Predictable duration
Easily antagonized, fully reversed
No drug interaction
Non-toxic
Free of side effect eg. CVS, respiratory
Stable pharmacokinetic and pharmacodynamic in the present of renal or hepatic disease
No accumulation
Safe in pregnancy

Muscle Relaxers and the Nervous System
Muscle relaxers refer to two major therapeutic groups: neuromuscular blockers and spasmolytics

Neuromuscular Blockers Spasmolytics
Neuromuscular blockers act by interfering with transmission at the neuromuscular end plate and have no central nervous system activity. They are often used during surgical procedures and in intensive care and emergency medicine to cause temporary paralysis.
Spasmolytics, also known as "centrally acting" muscle relaxants, are used to alleviate musculoskeletal pain and spasms and to reduce spasticity in a variety of neurological conditions.
Two Therapeutic Muscle Relaxers

Neuromuscular Blockers
Most neuromuscular blockers function by blocking transmission at the end plate of the neuromuscular junction.
Normal end plate function can be blocked by two mechanisms :=
Non depolarizing agents, such as tubocurarine, block the agonist, acetylcholine, from binding to nicotinic receptors and activating them, thereby preventing depolarization.

Neuromuscular Blockers
• Alternatively, depolarizing agents, such as succinylcholine, are nicotinic receptor agonists which mimic Ach, block muscle contraction by depolarizing to such an extent that it desensitizes the receptor and it can no longer initiate an action potential and cause muscle contraction.

Neuromuscular Blockers
• Both of these classes of neuromuscular blocking drugs are structurally similar to acetylcholine, the endogenous ligand, in many cases containing two acetylcholine molecules linked end-to-end by a rigid carbon ring system, as in pancuronium (a nondepolarizing agent).

Spasmolytics
Spasmolytic agents generally work by either enhancing the level of inhibition, or reducing the level of excitation.
Inhibition is enhanced by mimicking or enhancing the actions of endogenous inhibitory substances, such as gamma-Aminobutyric acid (GABA).

Spasmolytics
GABA is the chief inhibitory neurotransmitter in the mammalian central nervous system. It plays a role in regulating neuronal excitability throughout the nervous system. In humans, GABA is also directly responsible for the regulation of muscle tone.
Spasmolytics are referred to as “centrally acting muscle relaxants” because they can be used to target specific regions of the body such as low back and neck.

Skeletal muscle relaxants
Classification
• ◙ Peripherally acting (Neuromuscular blockers).
• ◙ Centrally acting Sk. M. relaxants
• ► Baclofen -Diazepam
• ◙ Direct acting Sk. M. relaxants.
• ►Dantrolene

Peripherally acting
A) Presynaptic neuromuscular blockers
1) Inhibit Ach synthesis .
Triethylacholine -hemicholinium
2) Inhibit Ach release .
Mg, aminoglycosides, botulinum toxin,
B) Postsynaptic neuromuscular blockers
1) Competitive (non depolarizing blockers) .
2) Depolarizing blockers .


Postsynaptic Neuromuscular
• Blockers Competitive NM blockers .
░ d-tubocurarine .
░ Gallamine .
░ Atracurium .
░ Pancuronium .
░ Vecuronium .
• Depolarizing NM blockers .
░ Succinylcholine (suxamethonium ) .

Uses of NMB blockers
♣control convulsion electroshock therapy in psychotic patient .
♣Relieve of tetanus and epileptic convulsion.
♣facilitate endoscopy
♣As adjuvant in general anesthesia to induce muscle relaxation
♣orthopedic surgery.

Competitive NM blockers
Mechanism of Action
• competitive antagonists: compete with Ach at the Nicotinic receptors of NMJ.
• No depolarization of postjunctionalmembrane.
• Cholinesterase inhibitors can reverse blockade (Neostigmine).

Pharmacokinetics
They are polar comp.
• inactive orally &taken parenterally.
• No cross placenta & CNS
• Metabolism depend upon kidney or liver
EXCEPT
• atracurium -mivacurium (cholinesterase).

Pharmacological actions :
1- Skeletal muscle relaxation.
2- CVS :-
▓ Hypotension (Histamine release) .
• d.Tubocurarine .
• Mivacurium .
• Atracurium .
▓ ↑ H.R Gallamine ● Pancuronium

Gallamine ( Flaxedil )
1-Less potent than curare ( 1/5 ).
2-Metabolized mainly by kidney 100% (((# in renal failure)))) .
3-Long duration of action.
4-Tachycardia due to :
♦ Atropine like action.

d –Tubocurarine
1-More potent than gallamine
2-Long duration of action ( 1 -2 hr. )
3-Eliminated by kidney 60% -liver 40%.
4-Histamine releaser :
►Bronchospasm .
►Hypotension .
5-Blocks autonomic ganglia (Hypotension) .

Atracurium
1- As potent as curare (1.5)
2-Has intermediate duration of action (30 min).
3-Eliminated by non enzymatic chemical
degradation in plasma ( Spontaneous
hydrolysis at body pH).
4-used in liver failure & kidney failure ( drug of choice ).
5-Liberate histamine ( Transient hypotension ).
6-No effect on muscarinic receptor nor ganglia .

Mivacurium
1- Chemically related to atracurium
2-Metabolized by pseudo cholinesterases.
3-Fast onset of action
4-Short duration of action (15 min).
5-Transient hypotension (histamine release).
6-Longer duration in patient with liver disease or genetic cholinesterase deficiency.

Pancuronium
1-More potent than curare ( 6 times ).
2-Excreted by the kidney ( 80 % ).
3-Long duration of action.
4-Tachycardia :
☻ Antimuscarinic action .

Vecuronium
1-More potent than tubocurarine ( 6 times ).
2-Metabolized mainly by liver.
3-Intermediate duration of action.
4-Has few side effects.
▒ No histamine release.
▒ No ganglion block.
▒ No antimuscarinic action.

Depolarizing Neuromuscular Blockers
☼☼Mechanism of Action
Phase I ( Depolarizing )
combine with nicotinic receptors →
depolarization of motor end plate →initial muscle twitching →Persistent depolarization →paralysis.
Phase I block is augmented not reversed by anticholinestrases.

Phase II ( Desensitization Block )
◙ Continuous exposure to succinylcholine → depolarization decreases and the membrane become repolarized, but the membrane cannot be depolarized by Ach as long as succinylcholine present→ desensitization of the membrane.
◙ This phase reversed by anticholinesterase.

Succinylcholine ( suxamethonium )
Pharmacological Actions :-
• 1. SK. muscle: fasciculation →spasticparalysis.
• 2. Hyperkalemia: Cardiac arrest.
• 3. Eye: ↑ intraocular pressure.
• 4.GIT: ↑intragastric pressure →regurgitation of gastric content to esophagus.
• 5. CVS: arrhythmia.

Pharmacokinetics
• Short onset of action ( 1 min. ).
• Short duration of action (5-10 min.).
• Destroyed by pseudocholinesterase .

Side Effects
1-Hyperkalemia.
2-CVS arrhythmia (Bradycardia, extrasystoland cardiac arrest ).
3-Malignant hyperthermia.
4-Succinylcholine apnea due to ?
♦liver disease (neonates –elderly).
♦Malnutrition .
♦ Organophosphorous poisoning.

Spasmolytics
• Baclofen:
☻ Centrally acting (GABA agonist –Sp. cord).
• Diazepam (Benzodiazepines):
☻Centrally acting (facilitate GABA action on Sp. Cord & CNS).
• Dantrolene:direct action on sk. muscles.

Uses of spasmolytics :
reduce muscle spasm in
1-Spinal cord injury .
2-Stroke .
3-Cerebral palsy .

Dantrolene
Mechanism of Action
1. It interferes with the release of calcium from its stores in sk. muscles (sarcoplasmic reticulum).
2. It inhibits excitation-contraction coupling in the muscle fiber.
☼Uses
Malignant Hyperthermia.
Spastic states.
IV, orally t ½ = 8 -9 hrs.

Malignant hyperthermia
► Inability to bind calcium by sarcoplasmic reticulum in some patients due to genetic defect .
► Sensitive to some drugs
• general anesthesia e.g. halothane
• neuromuscular blockers e.g. suxamethonium
► ↑ Ca release, intense muscle spasm, rise in Temp .