Embed Size (px)
Citation preview

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
Point‐of Care CD4 Testing• Bulk CD4 testing is done at accredited centralized National
Laboratories (NHLS SA) equipped to handle high volume sample throughput– TAT <24 hours
– Time delay from sampling to result‐in‐hand vary• Transport
• Reporting of results (electronic vs. manual)
• Patient return to clinics

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
Point‐of Care CD4 Testing• Decentralizing low volume CD4 testing to clinic level
– “same‐day‐results”
– “one‐stop” service of testing, counseling, initiation of therapy
– Get people onto therapy on 1st clinic visit if they qualify
– Not restricted to rural areas as urban clinics experience high % loss of patients
– POC systems

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
POC CD4 Technologies1. Rapid CD4 tests = laminar flow strips
BC ZyomyxTM
2. Low volume Fluorescent Cartridge Analyzers
PIMATM LabNowTM
3. Low volume Flow Cytometer Analyzers
FACSCountTM PointCareTM
ScreeningPositive/Negative answerCut-off 350cells/µlAccuracy questionable
Absolute CD4 count (no CD4%)Semi-Quantitative10-15 samples/instrument/dayBiohazard waste-disposalNo cold-chain
Absolute CD4 count and CD4%Quantitative20-40 samples/instrument/day“mini”-laboratory requiredCold chain required for some

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
(1) CD4 Test Strips
• Preliminary results with FirstSign strips– 1st generation done on plasma and serum
– 2nd generation done on whole blood
– Current cut‐off 250 cells/µl
– 95% false positive/negative results

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
(2) PIMATM
PHASE I: Laboratory evaluation
• Evaluated in the NHLS CD4 Reference Laboratory in Johannesburg
• 4 Pima Analyzers in parallel
• Testing done on whole blood drawn in EDTA tubes
• Manually pipetted 30µl of venous EDTA blood into cartridge capillary
• Results compared to reference CD4 method (PLG/CD4 by flow cytometry)
Closed cartridge systemFluorescent detection of CD4+ cells20min/day internal QC procedureSample analyses 20 minutes10 sample/instrument/8 hour day

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
Performance Comparison• In total 100 samples tested across 4 instruments
• Intra‐instrument variability negligible (50 samples run on 3 or 4 instruments in parallel) (1‐way ANOVA, p=0.95)
• Overall performance showed no significant difference in CD4 values (p>0.05)
• Error rate (NO READ) 1.3% across 4 instruments

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
Bias and Overall Agreement• Bland‐Altman analyses revealed a bias of ‐16±36 (95%LOA ‐88 to 55.2)
– At higher CD4 counts = bigger differences merely a function of the larger number
– %Similarity indicated tight reproducibility with overall agreement of 98% (slight under‐estimation of <2%) and precision of similarity (CV) of 4.6%
• Good correlation confirmed by linear regression analyses
Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
2 PIMA analyzers moved to HIV clinic in CM Hospital– Nursing staff trained to operate and use special finger prick lancet
– Dual testing of fingerprick/ capillary blood fill (CLINIC) versus EDTA venous blood pipette filled (LAB)
– PLG/CD4 reference method in the LAB
Preliminary data of 43 patients showed• Laboratory comparison good with %SIM CV<7% with outliers removed (differences not
significant)
• Finger prick derived data revealed 4 outliers with clinical impact and confirmed slight under‐estimation of absolute counts
• 13% NO READ in clinic = cartridge not filled correctly/closed properly (no results generated and patient already had left the clinic)
PIMATM PHASE IIClinic validation using finger prick derived capillary blood
Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
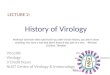
• Internal instrument QC • Manufacturer QC data confirmed reproducibility
(daily bead control) of system over time (CV<2%) in both laboratory and clinic analyzers
Control Cartridges
Pima 1
NPim
a 2 N
Pim
a 3 N
Pima 4
NPim
a 1L
Pima 2
LPim
a 3 L
Pima 4
L
0
500
1000
1500
Instrument PIMA 1 PIMA 2 PIMA 3 PIMA 4Low Bead ControlNumber of values 32 32 32 22Mean 152 220.9 150.1 148.595% CI of mean 151.3‐152.8 219.4‐222.4 149‐151.1 147.3‐149.8%CV 1.38 1.88 1.91 2.09High Bead ControlNumber of values 32 32 32 26Mean 994.6 828.4 960.6 988.595% CI of mean 998.8‐1000 825.2‐831.7 958.7‐962.5 985.4‐991.7%CV 1.60 1.09 0.55 0.72
Instrument and Control
Abso
lute
Bea
d C
ount

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
• External Quality Assessment– Retrospective AFREQAS EQA samples (n=10) showed system can process
stabilized blood products enabling external quality assessment on AFREQAS or equivalent EQAS
– Values between 1 to ‐2SDI with overall negative bias (NCS)
Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
(3) Low volume Flow Cytometers• FACSCount comparison to PLG/CD4
– Both in laboratory and clinic
– Data summarized on poster no P‐28• Good overall agreement
• %similarity 98% with CV of <5%
• PointCare comparison to PLG/CD4– Laboratory evaluation
– Data presented on poster no P‐28• Overall agreement not acceptable
• %similarity 122% with CV of >10%

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
Inter-instrument comparisonsPIMA™, PointCARE™, FACSCount™
Pima vs. PointCARE Pima vs. FACSCount™• Significant differences No significant differences• PCare vs. PLG or PIMA• Bias 125±137 (%sim of 122%, CV 18%) Bias 3.5±38 cells/µl; (%sim 98%, CV<5%)

Presented at the 4th INTEREST Workshop25-28 May 2010, Maputo Mozambique
SUMMARY• POC systems should be evaluated for purpose
• Choice of system depend on– Screening or monitoring
– Patient group (Adult vs. Pediatrics; #CD4 vs CD4%)
– Volume of samples/day
• Results within acceptable limit of error rate– Not adversely affect patient care
Acknowledgements
• RHRU, Hillbrow– Dr Regina Osih from RHRU for organizing clinic
– Prof Francois Venter
• Ms Dinah Ramasegane for operating the PIMA analyzer in clinic
• NHLS Johannesburg– Ms Sithembile Mojalefa for analyzing samples in the laboratory
– Professor Glencross, Stevens and Denise Lawrie, NHLS Johannesburg Hospital
• Alere for supply of PIMA and reagents.• Lynton Scorgie for supply of PointCARE