Embed Size (px)
Citation preview

Osteoprosis Haya M. Al-Malaq, Msc
Lecturer Clinical Pharmacy Department
Haya_malak@[email protected]

Defenition
Osteoporosis is a skeletal disorder characterized by compromised bone strength predisposing individuals to an increased fracture risk.

Categories
postmenopausal osteoporosis, age related steoporosis secondary osteoporosis.

Pathophysiology
Refer to textbook

Clinical presentation
Many patients are unaware that they have osteoporosis and only present after fracture. Fractures can occur after bending, lifting, or falling, or independent of any activity.
The most common osteoporosis-related fractures involve the vertebrae, proximal femur, & wrist. 2/3 of patients with vertebral fractures are asymptomatic; the remainder present with moderate to severe back pain that radiates down a leg after a new vertebral fracture. The pain usually subsides significantly after 2 to 4 wks, but chronic, low-back pain may persist.
Multiple vertebral fractures decrease height & sometimes curve the spine with or without significant back pain.

Clinical presentation
Patients with a non vertebral fracture frequently present with severe pain, swelling, & reduced function & mobility at the fracture site.

Diagnosis
History Major risk factor (<127 lb in postmenopausal
women), history of osteoporotic fracture in a first-degree relative, and personal history of low-trauma fracture as an adult. age, high bone turnover, low BMI index (<19 kg/m2), RA, & glucocorticoid use.
Complete physical examination BMD of central hip & spine T score: Normal bone mass is a T-score greater
than –1, osteopenia is –1 to –2.4, & osteoporosis is at or below –2.5.
low trauma fracture

Desired outcome
The primary goal of osteoporosis management is prevention.
Optimizing skeletal development & peak bone mass accrual in childhood, adolescence, and early adulthood will reduce the future incidence of osteoporosis.
Once osteopenia or osteoporosis develops, the objective is to stabilize or improve bone mass and strength and prevent fractures.
Goals in patients who have already suffered osteoporotic fractures include reducing future falls and fractures, improving functional capacity, reducing pain and deformity, and improving quality of life.

Treatment

Non-Pharmacologicla
balanced diet with adequate intake of calcium & vitamin D or , calcium supplements.
caffeine increases calcium excretion, caffein intake should be limited to two servings per day.
Smoking cessation Weight-bearing aerobic and strengthening
exercises improving muscle strength, coordination, balance, & mobility.


Pharmacologic therapy

Antiresorptive
Drug Comments
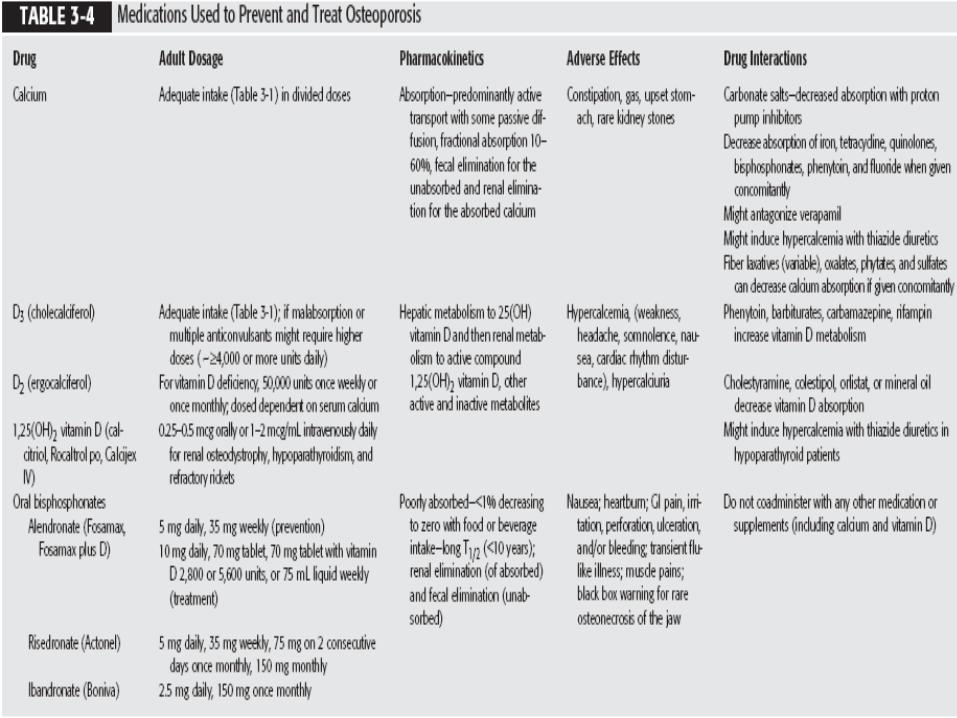
Calcium Intake should increase, with vit D, calcium carbonate is the best choice b/c it is high with Ca content, less expensive,Constipation is most common SE.
Vitamin D Maximize intestinal Ca absorption, intake should be 800-1000 u/d

Antiresorptive
Drug Comments
Estrogen Not FDA approved, short-term in patient with menapusal symptoms ,oral and transdermal estrogens at equivalent doses and continuousor cyclic HT regimens have similar BMD effects. Has many CI.
Testosteron Not FDA approved, should not be used alone, may reduce bone loss in patient with hypogondal symptoms , evaluate patient every 1-2m, then 3-6m.
Thiazide diuretics Thiazide diuretics increase urinary calcium reabsorption; should not be used alone, best in patient how require diuretic or with glucocorticiod use

Antiresorptive
Drug Comments
Bisphosphonates
Bisphosphonates bind to hydroxyapatite in bone and decrease resorption by inhibiting osteoclast adherence to bone surfaces. All bisphosphonatesbecome incorporated into bone, giving them long biologic half-lives of up to 10 years. provide the greatest BMD increases & fracture risk reductions. Fracture reductions are demonstrated as early as 6 m, with the greatest fracture reduction seen in pts with lower initial BMD and in those with the greatest BMD changes with therapy.
Antiresorptive
Drug Comments
Bisphosphonate BMD increases are dose dependent and greatest in the first 6 -12 m of therapy. Small increases continue over time at the lumbar spine but plateau after 2 to 5 years at the hip. After d/c, the increased BMD is sustained for a prolonged period that varies depending on the bisphosphonate used.Alendronate, risedronate, oral ibandronateare FDA approved for prevention & treatment of postmenopausal osteoporosis.IV ibandronate & zoledronic acid are indicated only for treatment of postmenopausal women. Risedronate & alendronate are also approved for male & glucocorticoid-induced osteoporosis.

AntiresorptiveDrug Comments
Bisphosphonate poorly absorbed (BA1-5%) Each oral tablet should be taken in the morning with at least 6 oz of plain tap water (not coffee, juice, mineral water, or milk) at least 30 minutes (60 minutes for oral ibandronate) before consuming any food, supplement, or medication. The patient should remain upright (sitting or standing) for at least 30 minutes after alendronate & risedronate & 1 h after ibandronate administration to prevent esophageal irritation & ulceration.Most patients prefer once-weekly or once-monthly administration over daily therapy. If a patient misses a weekly dose, it can be taken the next day. If more than 1 day has elapsed, that dose is skippeduntil the next scheduled ingestion. If a patient misses a monthly dose, it can be taken up to 7 days before the next scheduled dose.

Antiresorptive
Drug Comments
Bisphosphonate SE: GI, flu like symptoms. Osteonecrosis ofthe jaw occurs rarely; if it develops, oral chlorhexidine washes, systemic antibiotics, and systemic analgesics are used based on severity.

Antiresorptive
Drug Comments
Mixed Estrogen Agonists/Antagonists
Raloxifene is an estrogen agonist on bone but an antagonist on the breast & uterus. It is approved for prevention and treatment of postmenopausal osteoporosis. Less effective, less breast cancer risk, SE: hot flashes, bleeding, CI: thromboembolism.
Calcitonin is released from the thyroid gland when serum calcium is elevated. Salamon calcitonin is used b/c more potent & long lasting, indecated 5 years past menopause, 3rd line agent, can produce pain relief in vertebular fracture, intranasal dose 200 u/d

Anabolic therapy
Teriparatide recombinant product representing the first 34 amino acids in human parathyroid hormone. Teriparatide increases bone formation,the bone remodeling rate, and osteoblast number and activity. Both bone mass & architecture are improved.• Teriparatide is FDA approved for postmenopausal women & men whoare at high risk for fracture. Candidates for therapy include patients with a history of osteoporotic fracture, multiple risk factors for fracture, very low bone density (e.g., T-score <–3.5), or those who have failed or are intolerant of previous bisphosphonate therapy.

Anabolic therapy
Teriparatide The drug reduces fracture risk in postmenopausal women, but no fracture data are available in men. Lumbar spine BMD increases are higher than with any other osteoporosis therapy. Although wrist BMD is decreased, wrist fractures are not increased.• D/C of therapy results in a decrease in BMD, but some antifracture efficacy appears to be maintained. Sequential therapy with teriparatide followed by an antiresorptive agent (e.g., bisphosphonate) should be considered to maintain BMD gains.

Anabolic therapy
Teriparatide The dose is 20 mcg administered SC in the thigh or abdominal area. The initial dose should be given with the patient either lying or sitting, in case orthostatic hypotension occurs. Each prefilled 3-mL pen device delivers a 20-mcg dose each day for up to 28 days; the pen device should be kept refrigerated.• Transient hypercalcemia rarely occurs. A trough serum ca conc is recommended 1 m after initiation of therapy.• Teriparatide is CI in patients at baseline increased risk for osteosarcoma (e.g., Paget’s bone disease, unexplained alkaline phosphatase elevations, pediatric patients, young adults with open epiphyses, or patients with prior radiation therapy involving the skeleton).

Glucocorteciods-induced osteoprosis
Guidelines for managing corticosteroid-induced osteoporosis recommend measuring BMD at the beginning of chronic therapy (prednisone 5 mg or more daily or equivalent for at least 6 months) and follow up monitoring with DXA in 6 to 12 months. BMD should be measured in patients taking chronic therapy whose baseline values were not obtained.
All patients starting or receiving long-term systemic glucocorticoid therapy should receive at least 1,500 mg elemental calcium and 800 to 1,200 units of vitamin D daily and practice a bone-healthy lifestyle.