Embed Size (px)
Citation preview

..Cytogentic & Molecular Risk Cytogentic & Molecular Risk Stratification based management Stratification based management
of Pediatric AML in 2015of Pediatric AML in 2015
Brijesh Arora,Brijesh Arora,
Professor, Division of Pediatric Oncology, Professor, Division of Pediatric Oncology, Tata Memorial Hospital, MumbaiTata Memorial Hospital, Mumbai
SynopsisSynopsis
.Molecular Pathogenesis.Molecular Pathogenesis Genomic abnormalities in Pediatric AMLGenomic abnormalities in Pediatric AML Role of MRDRole of MRD Current risk stratification & Current risk stratification &
recommendationsrecommendations Approach to TreatmentApproach to Treatment

COG
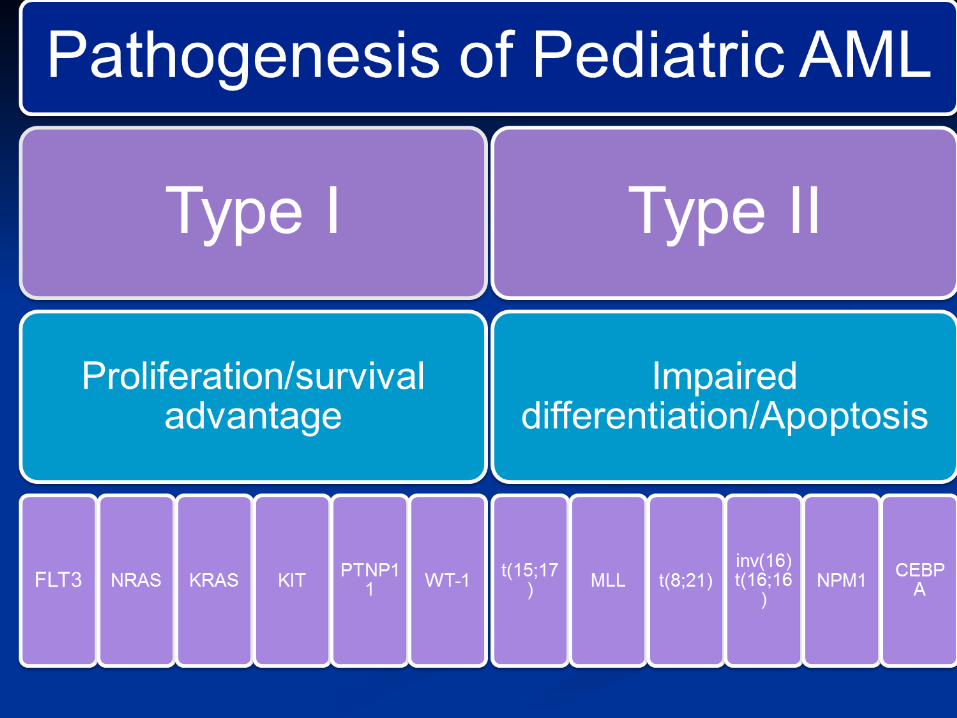

Genomic subtypes in Genomic subtypes in Pediatric AMLPediatric AML

Integrative analysis( Type I & Integrative analysis( Type I & II abnormalities)II abnormalities)

Genetics in Pediatric AML: Proven factorsGenetics in Pediatric AML: Proven factors

Pediatric AML: Probable Pediatric AML: Probable factorsfactors

Pediatric AML: Unproven factorsPediatric AML: Unproven factors

Cytogentic & Molecular factors Cytogentic & Molecular factors used to classify good riskused to classify good risk
Factor St Jude 08 MRC 15/17 COG 1031 BFM2012
t(8;21), inv(16)
YES Yes YES YES
t(1;11) No No No YES
NPM/ BICEBPA
No Yes Yes YES

Cytogentic & Molecular factors Cytogentic & Molecular factors for defining high riskfor defining high risk
Factor St Jude 08 MRC 15/17 COG 1031 BFM2012
FAB M0, M6 & M7without t(1:12)
YES No No No
Secondary AML YES Yes Yes Yes
-5, -7, del (5q), complex ktype
YES Yes Yes Yes
t(4;11),t(5;11) t(6;11),t(10;11),t(9;22)
No Yes No Yest(7;12),12p
t(6;9), t(8;16),t(16;21)
Yes No No Yes
abn (3q),inv3,t(3:3), -17,Abn 17p
No Yes No No
FLT3-ITD YES ( MRD+) Yes Yes YES

FLT3-ITD:Allelic Ratio (AR)FLT3-ITD:Allelic Ratio (AR)

AML outcome: leukemia, Host AML outcome: leukemia, Host & Treatment& Treatment
MRD

Author Trial Group N MRD level %
Hazard ratio
95 % CI
P value
Multivariate
Sievers 2003 CCG 2941
& 2961
252 > 0.5 4.8 2.8-8.4 p <0.0001
independent
Langebrake 2006 AML BFM 98 150 > 0.1 2.0 1.0-4.39
p=0.05
not independent
Coustan-Smith 2003
Saint Judes
AML 02
46 > 0.1 3.79 p 0.037
independent
Results of MRD Studies in Paediatric AML

Impact OF MRD- COG studiesImpact OF MRD- COG studies

Probability of Relapse-free and Probability of Relapse-free and Overall Survival According to MRDOverall Survival According to MRD
94 children treated on MRC AML 12/DCOG ANLL 97 Independent of age, WCC, FLT3/ITD
V.H.J. van Velden et al, 2010

Risk Stratification in 2015Risk Stratification in 2015

COG 1031 risk stratificationCOG 1031 risk stratification
Low-Risk:Low-Risk: Inv(16), t(8;21), nucleophosmin (NPM)
mutations, or CEBPA mutations with any MRD status.
Standard-risk cytogenetics (defined by the absence of either low-risk or high-risk cytogenetic characteristics) with negative MRD at end of Induction I.

COG 1031 risk stratificationCOG 1031 risk stratification
High Risk:High Risk: High allelic ratio FLT3-ITD-positive with
any MRD status. Monosomy 7 with any MRD status. del(5q) with any MRD status. Standard-risk cytogenetics with positive
MRD at end of Induction I.

AML-BFM 2012AML-BFM 2012

St Jude AML-08 Risk groupsSt Jude AML-08 Risk groups

St Jude AML-08 Risk groupsSt Jude AML-08 Risk groups

Conventional Cytogentics & FISHConventional Cytogentics & FISH
CytogenticsCytogentics

Molecular Cytogentics:Molecular Cytogentics:
Impact on treatmentImpact on treatment

Induction Treatment ApproachInduction Treatment Approach
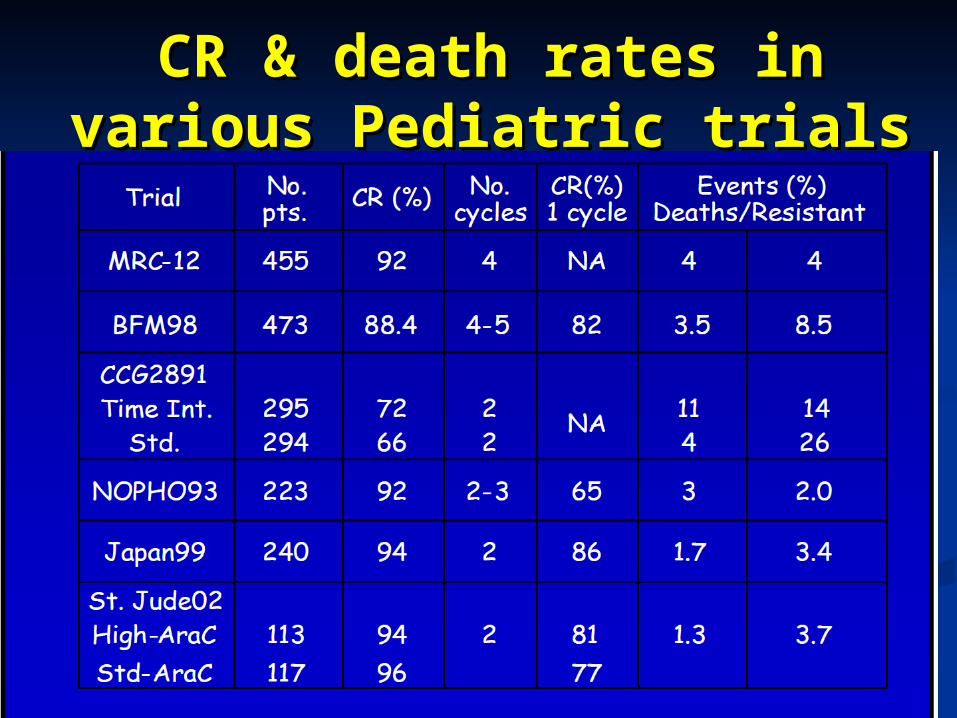
CR & death rates in various CR & death rates in various Pediatric trialsPediatric trials

DATDAT
ADEADE
MACEMACE MidACMidAC
Allo BMTAllo BMT
ABMTABMT
MRC AML 10
R1R1
ADEADE
DATDAT DONORDONOR
NO NO DONORDONOR
R2R2
NFTNFT

MRC AML 12
R1
ADE
MAE
V
RISK GROUPASSIGNED
ADE
V MACE
MidAC
CLASP MidAC
MidAC
CLASP MidAC
STANDARD + POOR
Allo BMT
CLASP AlloBMT
MAE
R2
R2
DONOR
NO DONOR
R2
GOOD
Mitoxantrone= Daunorubicin

MRC AML 15
Course 1Course 1+ LP+ LP
Course 2Course 2+ LP+ LP
Course 3Course 3 Course 4Course 4 Course 5Course 5
R
ADE 3+10+5
‘Good’, ‘Standard’ and‘Poor’ risk without a
donor in CR
ADE 3+8+5
FLAG-IDAFLAG-IDA
Risk group assessment
CRR
If no CR go to Relapse Protocol
‘Poor’ risk, but with aMatched donor and CR
Ara-C 3 g/m2
MACE
Ara-C 3 g/m2
MidAc
E Sibling/UD allogeneic BMT
R
No furthertreatment
Ara-C 1.5 g/m2
R = RandomiseE = Elect
Non-APL Patients (At a later date there may be a further randomisation for Mylotarg at Course 1 and 3)
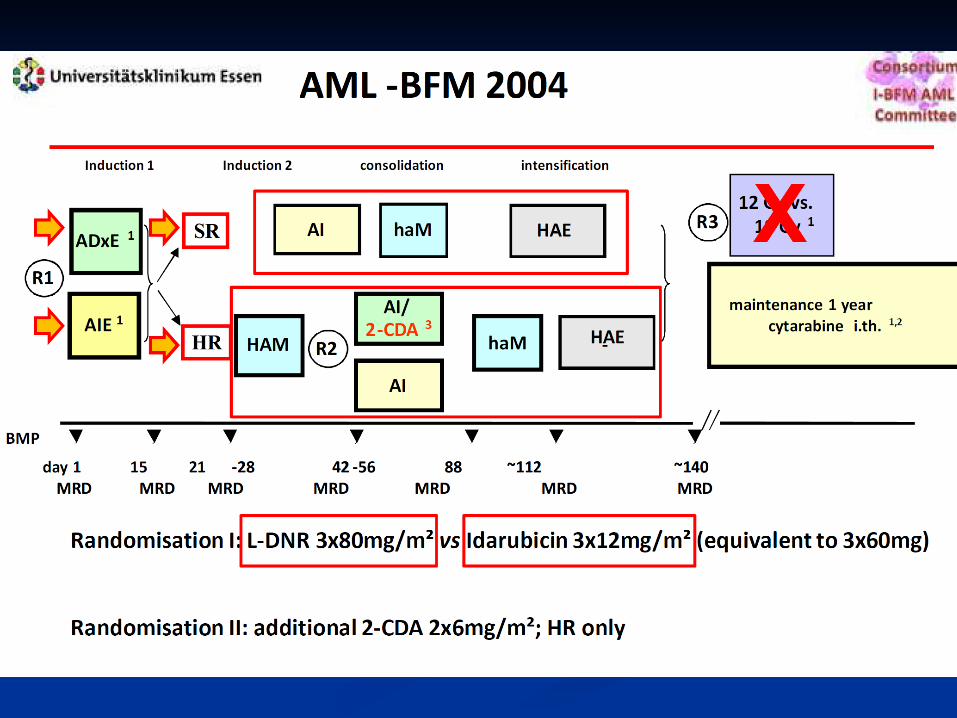

BFM 2004BFM 2004

St Jude AML02- Dose of AraCSt Jude AML02- Dose of AraC

Antharcycline dose intensityAntharcycline dose intensity
High dose Daunorubicin not tested in view High dose Daunorubicin not tested in view of risk of cardiotoxicityof risk of cardiotoxicity

Current approachCurrent approach

Post Induction regimePost Induction regime

Number of coursesNumber of courses
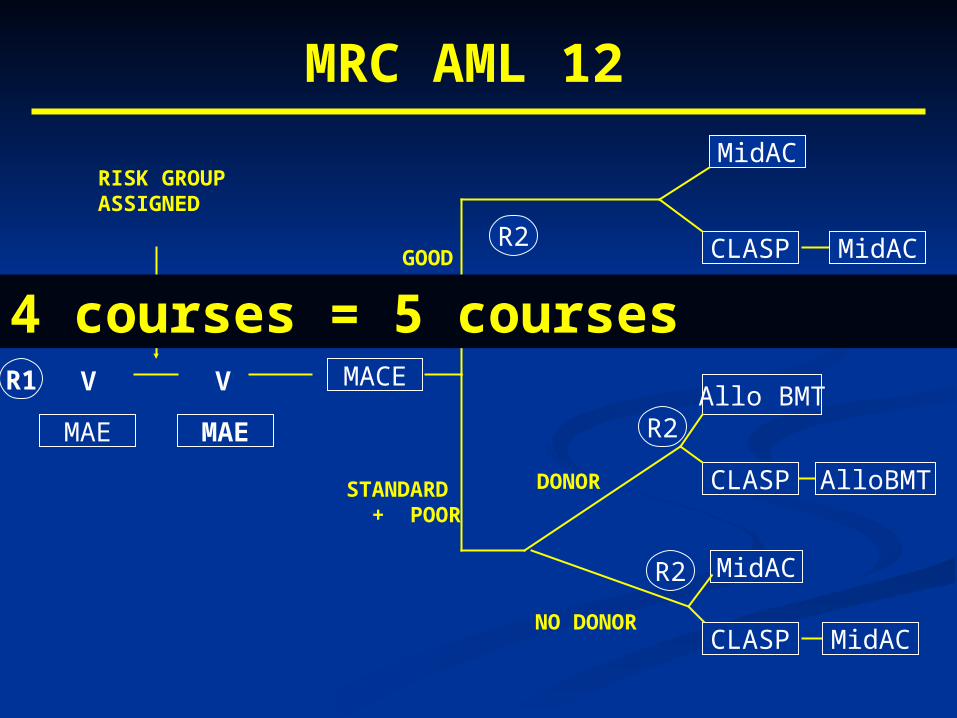
MRC AML 12
R1
ADE
MAE
V
RISK GROUPASSIGNED
ADE
V MACE
MidAC
CLASP MidAC
MidAC
CLASP MidAC
STANDARD + POOR
Allo BMT
CLASP AlloBMT
MAE
R2
R2
DONOR
NO DONOR
R2
GOOD
4 courses = 5 courses

MRC 15 Consolidation: MACE MRC 15 Consolidation: MACE v Ara-Cv Ara-C

CNS prophylaxisCNS prophylaxis

St Jude AML-02: Impact of TIT.St Jude AML-02: Impact of TIT.

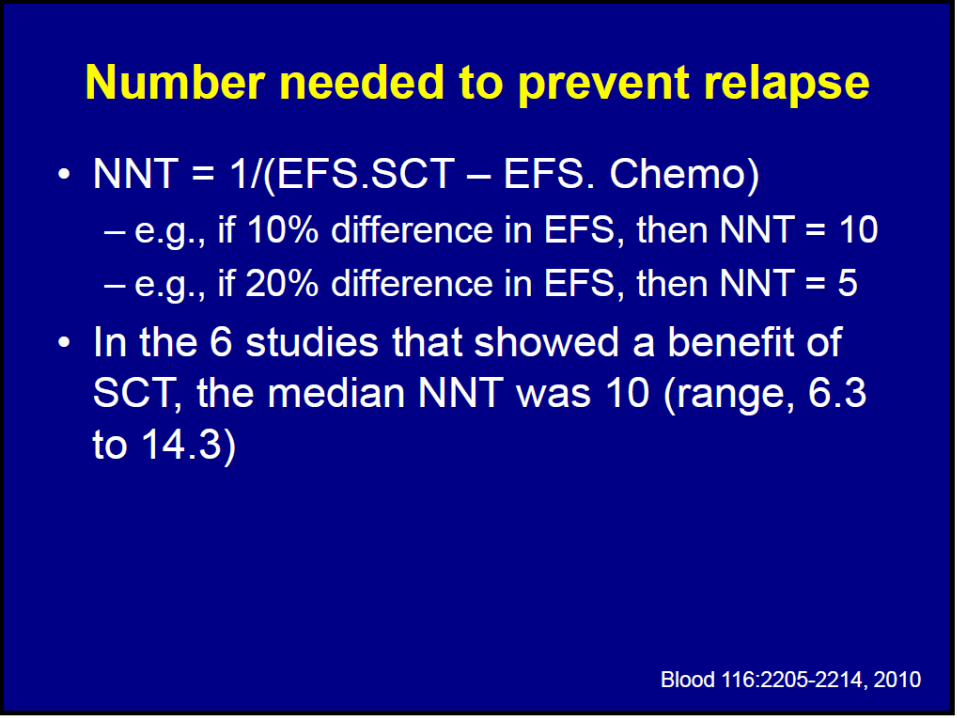
Role of SCT?Role of SCT?

AML-BFM 98Intent-to-treat Analysis
.56, SE=.04
Kein Spender (N=188, 77 events)
.58, SE=.09
HLA-id. Spender (N= 58, 20 events)
years
Log-Rank p = .16
P
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8
No donorHLA-id. donor
.43, SE=.04
Kein Spender (N=188, 104 events)
.47, SE=.07
HLA-id. Spender (N= 58, 32 events)
years
Log-Rank p = .52
P
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8
OS Event-free survival
No donorHLA-id. donor
HR= standard +poor

AML 10 & 12Survival from CR by Risk Group
SCT No SCT 2P Value
All patients 57% 65% 0.3
Standard 46% 61% 0.2
Poor 28% 47% 0.2
Standard Poor100
75
50
25
0 1 2 3 4 5
61 %
46% 47%
28%
0 1 2 3 4 5
100
75
2P = 0.2
4910
49240No Allograft
Allograft
No Allograft
Allograft
Years from CR Years from CR
2P = 0.2
2P = 0.2
50
25

BMT =480 Chemotherapy = 893
Outcome % % P value
Favorable-risk disease
Relapse 21 21 30 0.06
Disease-free survival 63 61 0.58
Overall survival 83 73 71 0.85
Intermediate-risk disease
Relapse 36 26 54 < 0.001
Disease-free survival 58 39 < 0.001
Overall survival 70 62 51 0.006
Poor-risk disease
Relapse 53 67 56 0.69
Disease-free survival 33 35 0.82
Overall survival 39 33 35 0.80
Nonclassifiable
Relapse 32 44 0.004
Disease-free survival 52 50 0.14
Overall survival 60 61 0.49
Risk Stratified Outcomes Comparing Matched Sibling BMT and Chemo Alone
MRC 15% COG 40% with no cytogeneticsHoran J, Journal of Clinical Oncology 2008, Vol 26, Issue 35


Role of MyelotargRole of Myelotarg


Role of TKIsRole of TKIs
Sorafinib- promising in FLT3-ITD mutated Sorafinib- promising in FLT3-ITD mutated AML and some benefit in Non-mutated AML and some benefit in Non-mutated populationpopulation


Heterogeneity within Heterogeneity within cytogenetic classes on GEPcytogenetic classes on GEP

Copy number Heatmap for Copy number Heatmap for Pediatric AML ( N-111)Pediatric AML ( N-111)

Frequency of CNA & MutationsFrequency of CNA & Mutations

Summary of AML PathogenesisSummary of AML Pathogenesis
Less than 2.0 copy number per case ( ALL Less than 2.0 copy number per case ( ALL 7/case)7/case)
Deletion= amplificationDeletion= amplification Recurrent focal lesion are rareRecurrent focal lesion are rare 30% with translocation had no CAN or 30% with translocation had no CAN or
point mutationpoint mutation














![[Brijesh]bioinformatics oppertunity](https://img.dokumen.tips/doc/110x75/577dac471a28ab223f8d9751/brijeshbioinformatics-oppertunity.jpg)