Embed Size (px)
DESCRIPTION
גידולים ציסטיים בלבלב
Citation preview

Anatomy

Anatomy
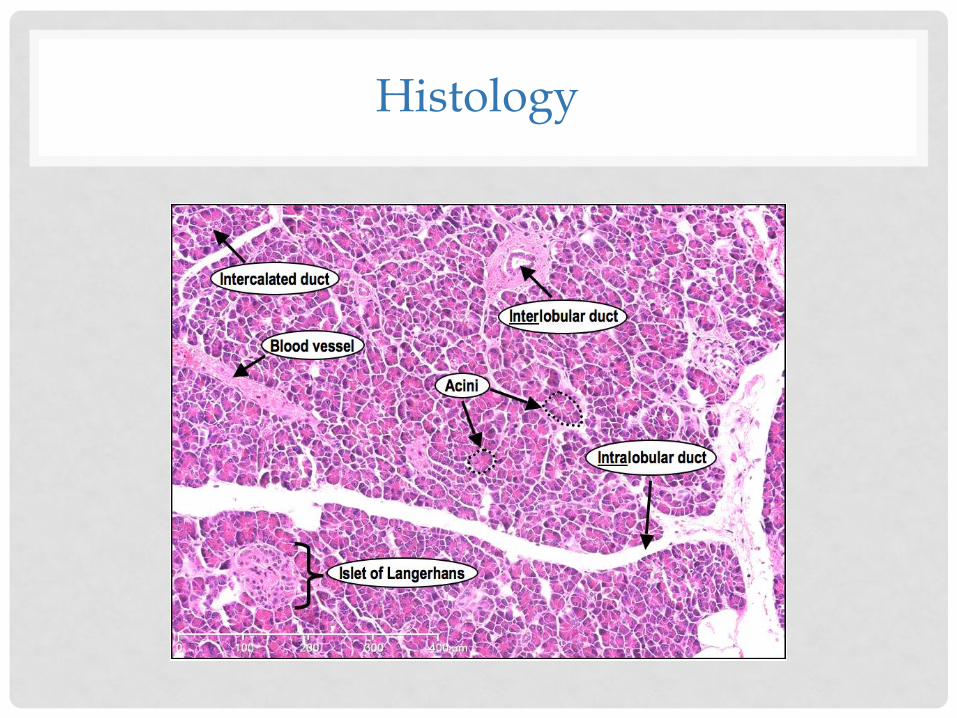
Histology
Introduction
• Pancreatic cysts are sac-like pockets of fluid on or
within your pancreas
• Most pancreatic cysts aren't cancerous, and don't
cause symptoms.
• Pancreatic cysts may be detected in over 2% of
patients who undergo abdominal imaging for
unrelated reasons.

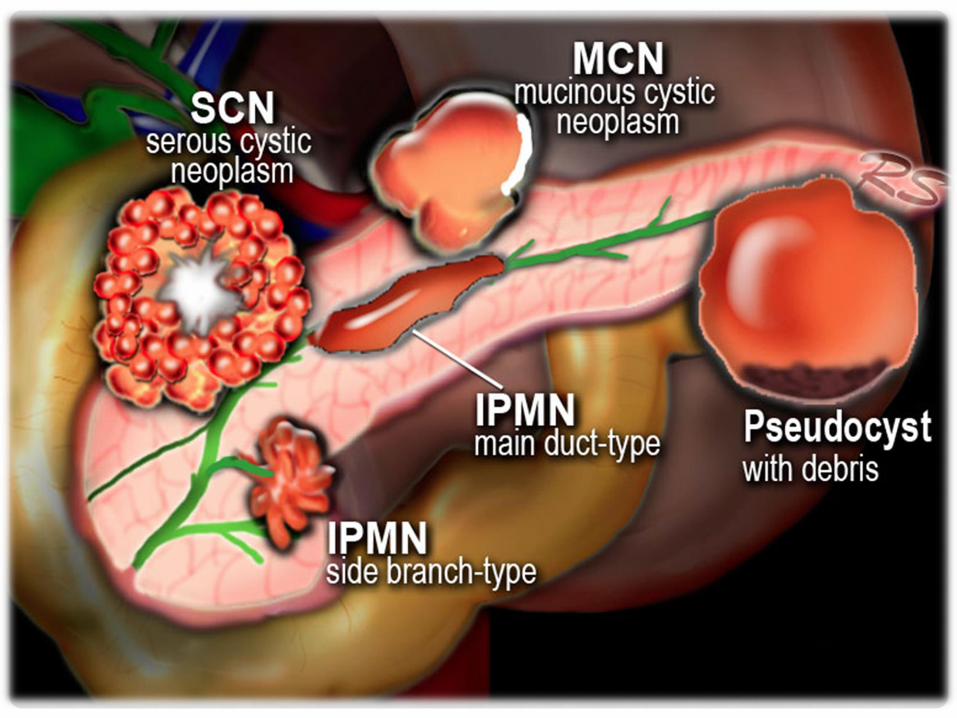
CLASSIFICATION
Pancreatic cysts
Pseudocysts Non-neoplastic
True cysts Retention cysts
Mucinous non-neoplastic cysts
Lymphoepithelial cysts
Pancreatic cystic neoplasms
Serous cystic tumors
Mucinous cystic neoplasms (MCNs)
Intraductal papillary mucinous neoplasms (IPMNs)
Solid pseudopapillary
neoplasms (SPNs)

PSEUDOCYST
• The capsule of a pseudocyst is composed of collagen
and granulation tissue and it is not lined by epithelium
• History of pancreatitis or abdominal trauma
• Cysts develop in 4-6 weeks - usually decrease in size over
time - sometimes enlarge or become infected.
• Found in any part of the pancreas or anywhere within
the abdomen and sometimes even in the chest.


PSEUDOCYST - TREATMENT
• Approximately half of all pseudocysts resolve spontaneously
• Indications for treatment include:
• infection
• large size: > 4-6 cm
• gastric outlet obstruction
• biliary obstruction
• growth on serial scanning
• Treatment options include:
• open surgical debridement, or cystenterostomy with a Roux-en-Y
jejunal loop
• endoscopic drainage into the stomach (or duodenum)
• percutaneous drainage


Serous Cystic Neoplasm
• Benign tumor, but large tumors have a tendency to increase in size and cause symptoms.
• Lobulated surface
• Can arise anywhere in the pancreas
• No communication between cysts and pancreatic duct.
• Most commonly diagnosed in women over the age 60 years
• Malignant transformation into serous cystadenocarcinoma is exceedingly rare

Mucinous Cystic Neoplasms
• Occur exclusively in women and are most
commonly discovered after the age of 40 years
• Macrocystic with thick wall septations and
peripheral calcifications (25%)
• Typically arise in the pancreatic tail or body
• Most are symptomatic, presenting with nondescript
abdominal pain

Solid Pseudopapillary Neoplasm
• Very uncommon neoplasm
• solid and cystic areas with hemorrhage on cut
sections
• seen in women 20-30 years
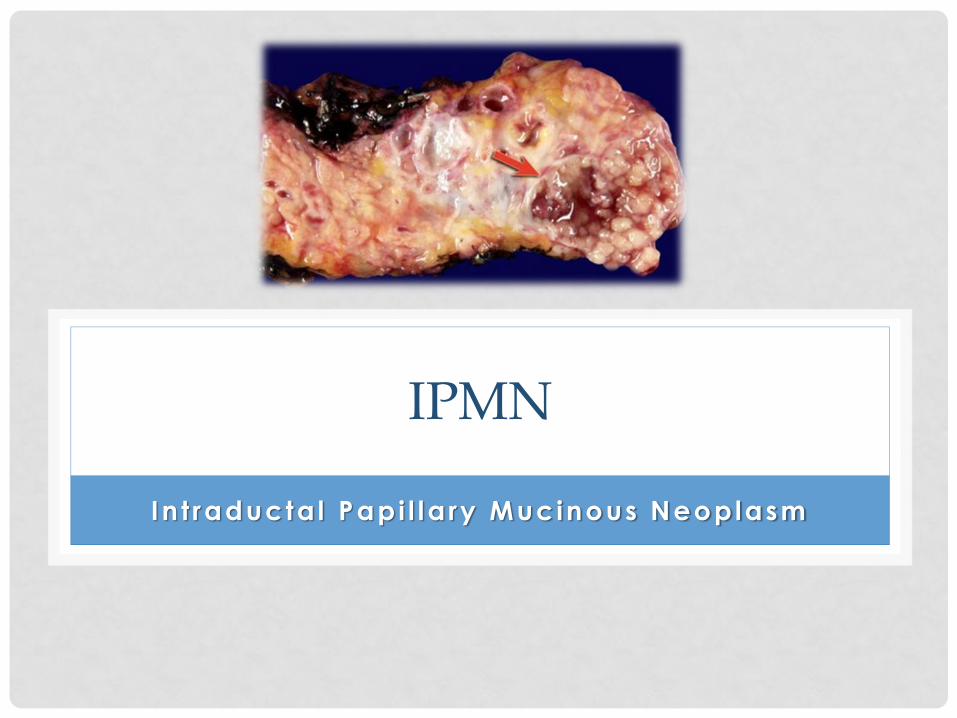
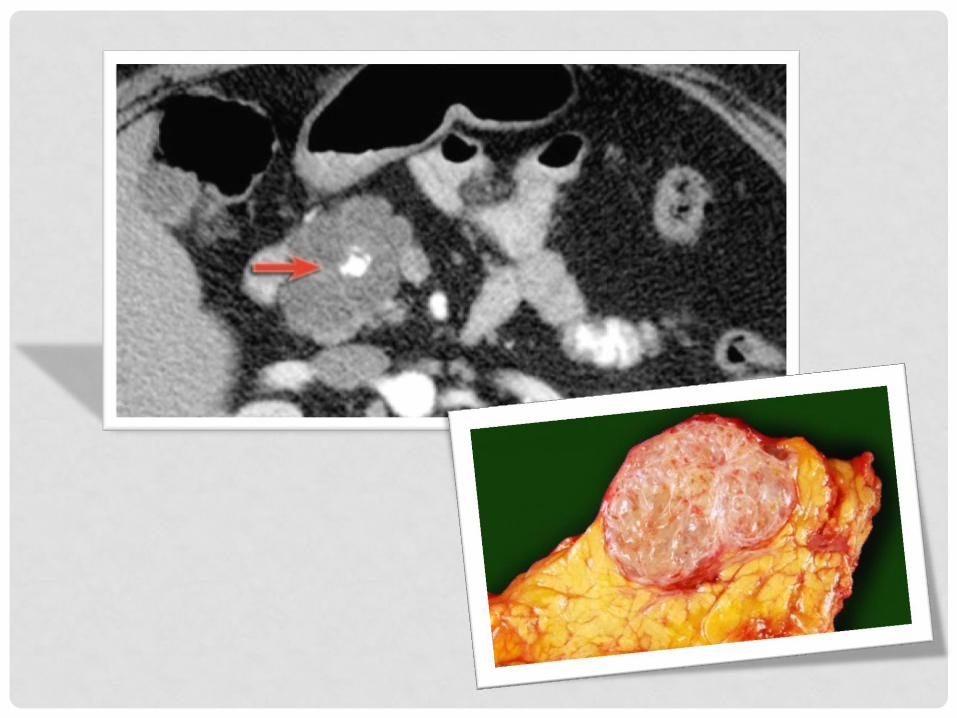
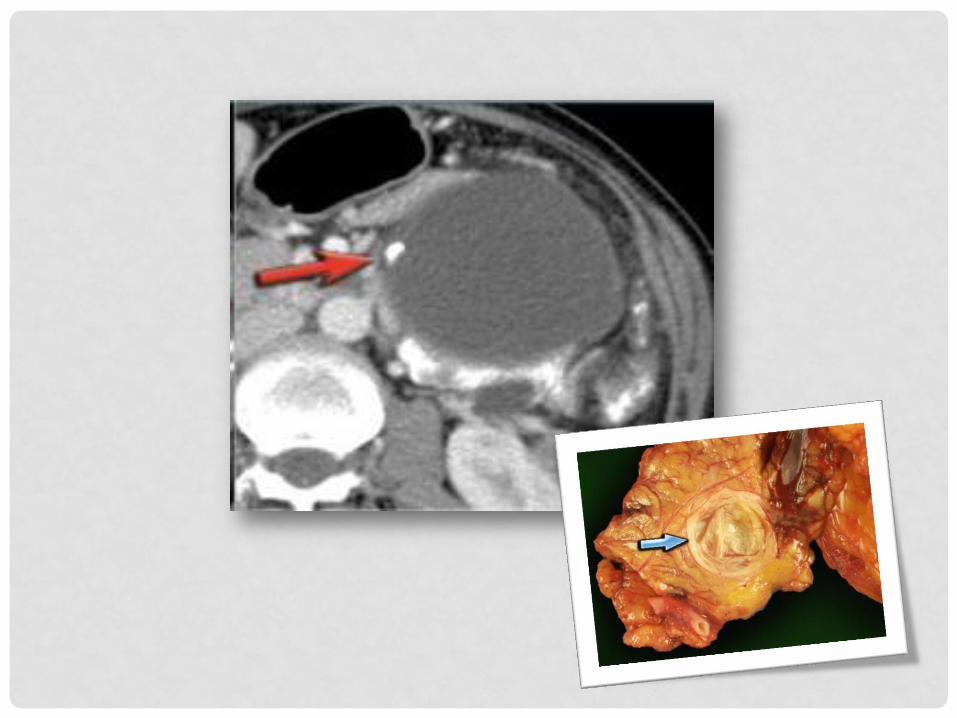
IPMN
In t raducta l Papi l la ry Mucinous Neoplasm
• Precancerous lesions with a well-described adenoma carcinoma sequence
• Grow within the pancreatic ducts
• May involve the main pancreatic duct, the branch ducts, or both.
• IPMNs composed of columnar tumor cells that make lots of mucin (thick fluid).
• The lesions show papillary proliferation, cyst formation, and varying degrees of cellular atypia

EPIDEMIOLOGY
• The true incidence of IPMN is not known.
• The typical age at presentation is in the fifth to
seventh decade
• male predominance in Japan and Korea
• female predominance in the United States and
Europe
• Associated with smoking
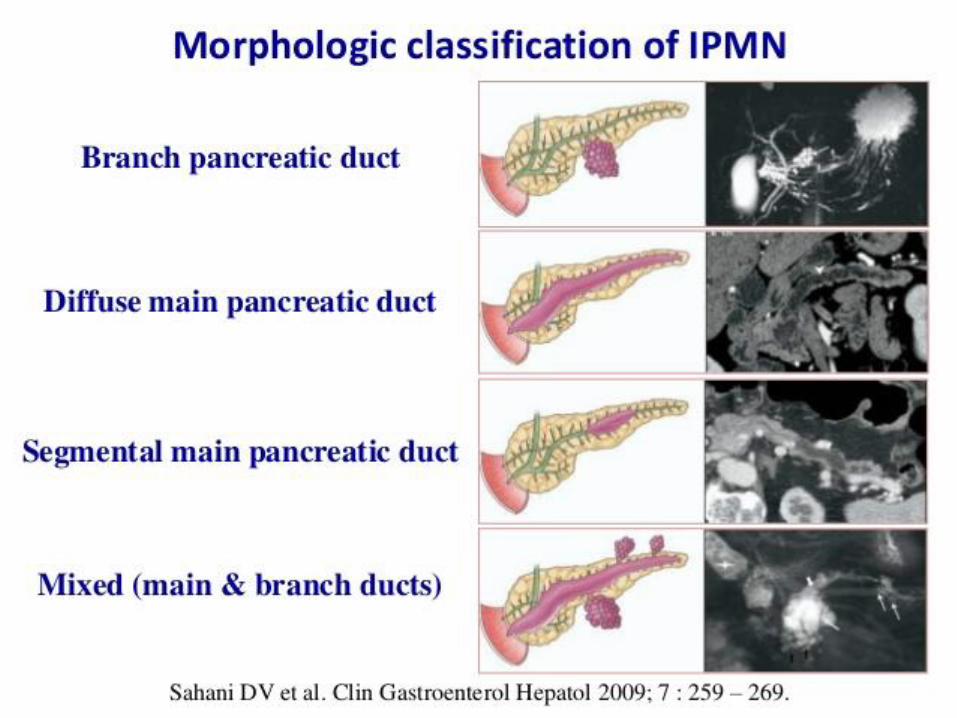
CLASSIFICATION

CLASSIFICATION
• MD-IPMNs-
• Involve the main pancreatic duct
• The majority arise within the head of the pancreas and
progress distally
• Histologically more aggressive than BD-IPMNs
• more likely to harbor a malignancy (70% in 10 years)
• BD-IPMNs-
• occur in younger patients
• arise in the uncinate process
• may also involve the tail of the pancreas.
• 20% malignancy within 10 years.

IPMN’s grading
low-grade dysplasia
(adenoma)
moderate dysplasia
(borderline)
High-grade dysplasia
(carcinoma in situ)
Invasive carcinoma

PATHOGENESIS
IPMN- COMMON MUTATIONS
• K-ras mutations:
• constitutively active MAP kinase signaling
• 50% of IPMN’s cases
• weakly associated with progression to malignancy
• CDKN2a inactivation
• SMAD4 inactivation
• ring finger protein 43 [RNF43] gene inactivation
• STK11
IPMN’s markers
• mRNAs:
• miR-21
• miR-221
• Serum antigens:
• carbohydrate antigen (CA) 19-9
• carcinoembryonic antigen (CEA)

ASSOCIATED DISEASES
• Diabetes
• Peutz-Jeghers syndrome
• familial adenomatous polyposis syndrome
• a family history of pancreatic ductal
adenocarcinoma

CLINICAL PRESENTATION
• Many patients have no symptoms
• Nausea
• Vomiting
• Abdominal pain
• Back pain
• Weight loss
• Anorexia
• Jaundice
• In most cases routine laboratory tests are normal!
DIFFERENTIAL DIAGNOSIS
• chronic obstructive pancreatitis
• mucinous cystic tumors of the pancreas
• pancreatic ductal adenocarcinoma

DIAGNOSTIC TESTS
• pancreatic protocol CT scan
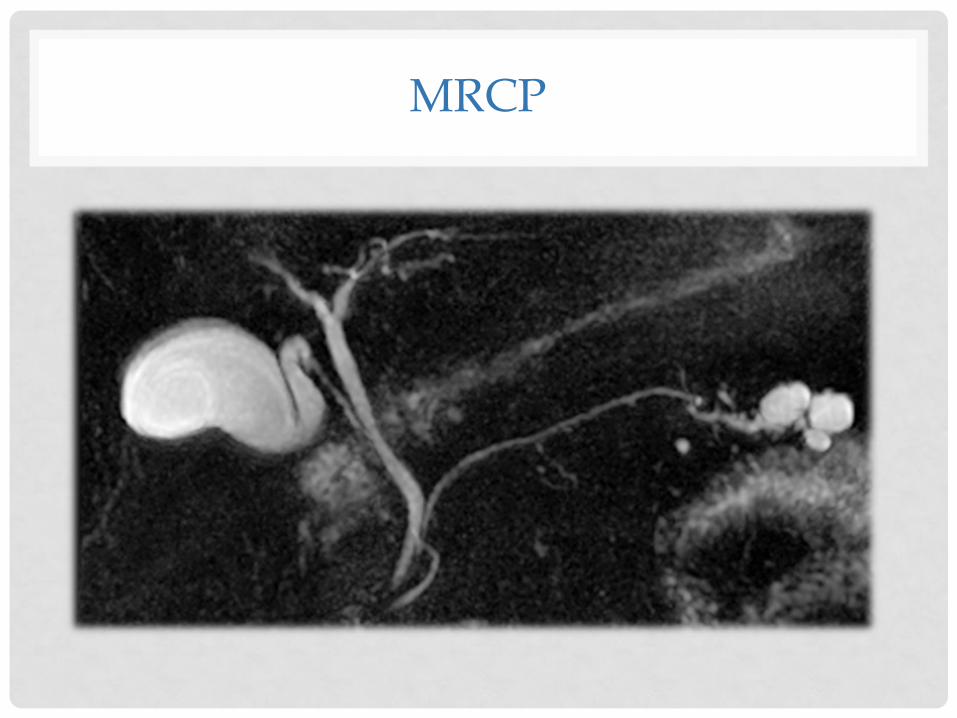
• magnetic resonance cholangiopancreatography
(MRCP)
• Endoscopic ultrasound
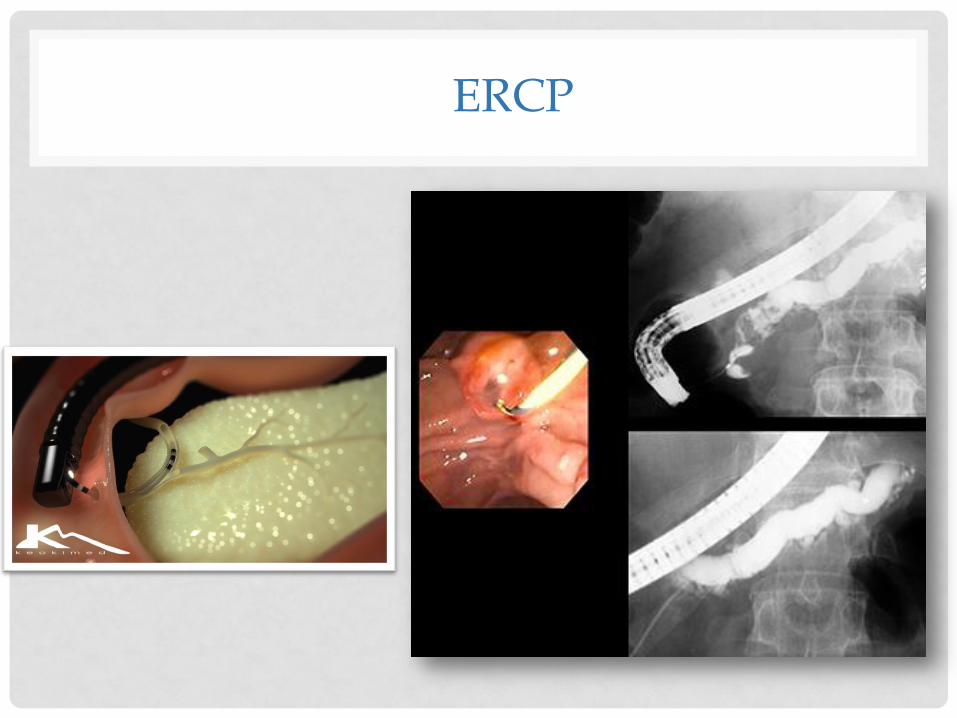
• endoscopic retrograde
cholangiopancreatography (ERCP)

CT SCAN
MRCP
ERCP
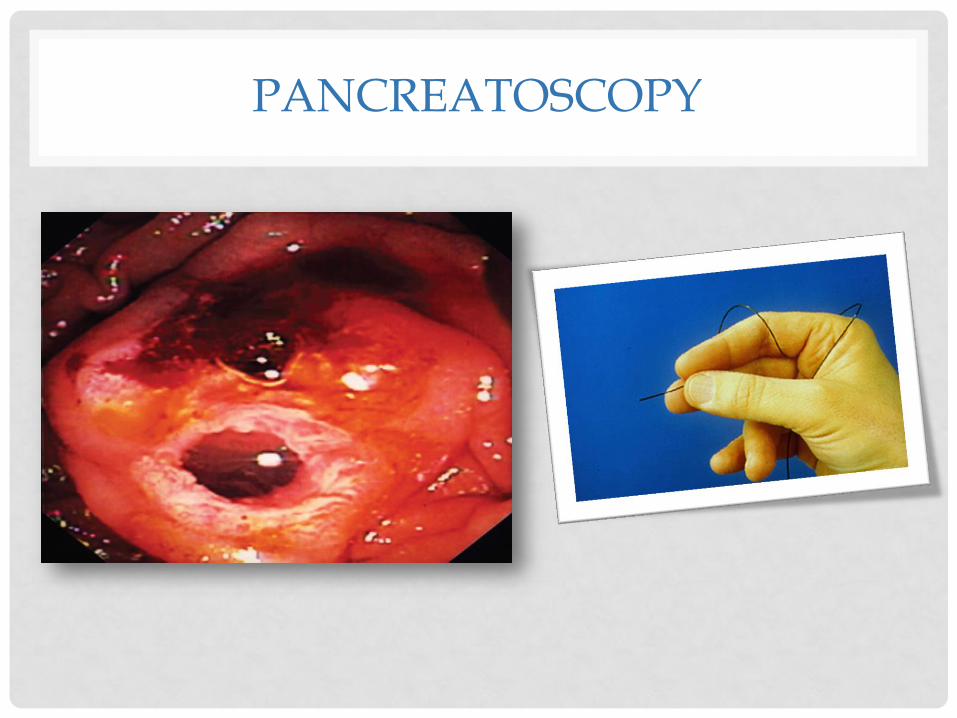
PANCREATOSCOPY

EUS

EUS-FNA
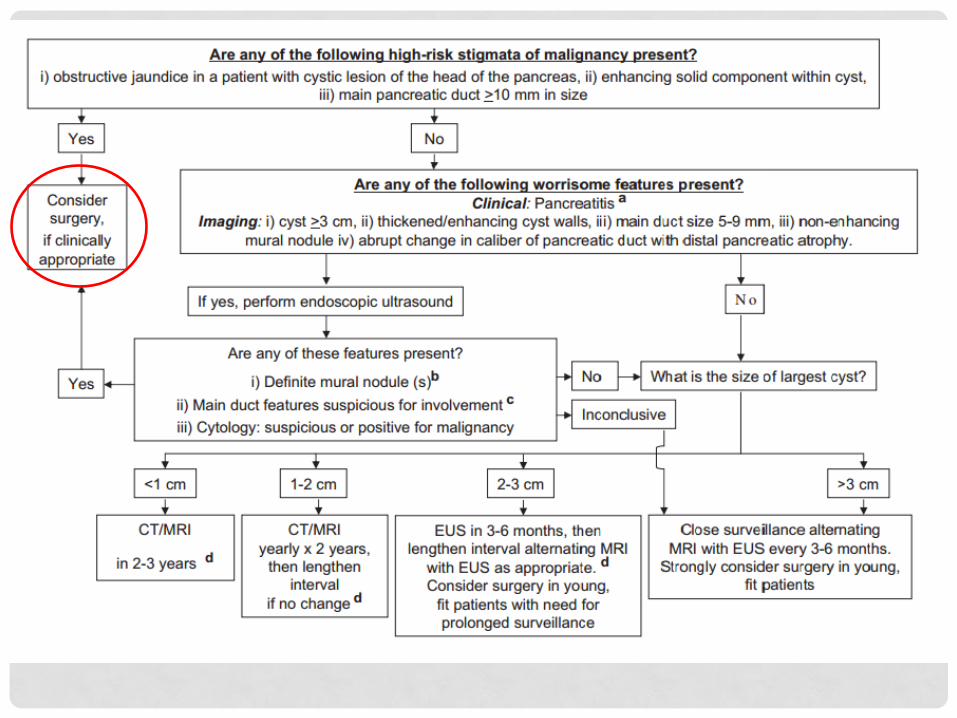
CONCERNING RADIOGRAPHIC FEATURES:
• solid components
• pancreatic ductal dilation ≥10 mm
• lymphadenopathy
• mural nodules
• synchronous
• increase in cyst size during follow-up

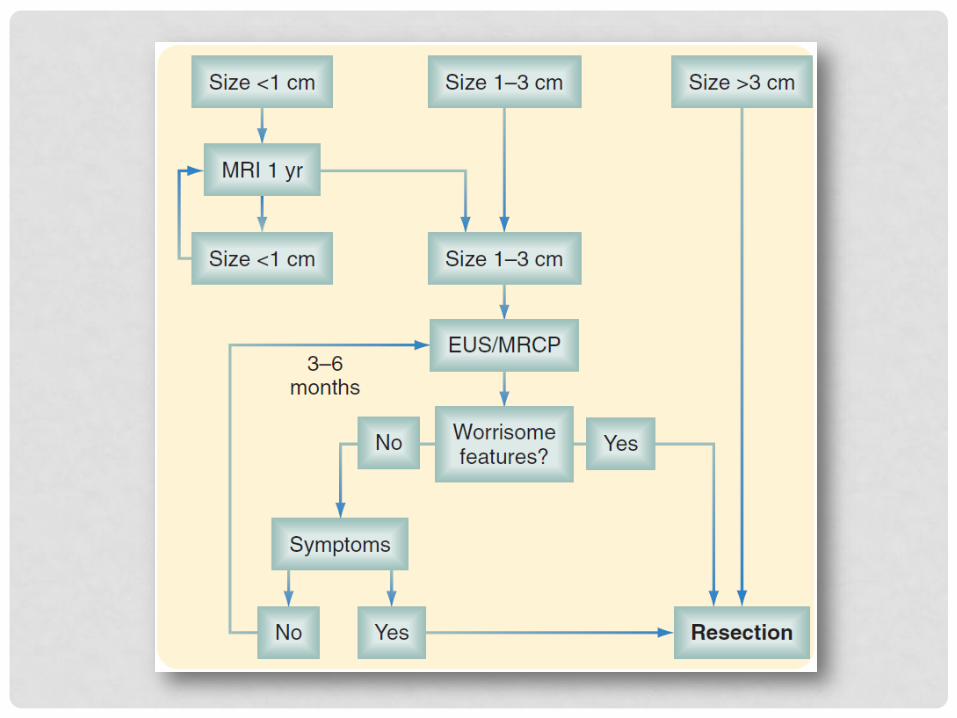
SURGERY

INDICATIONS
• MD-IPMN:
• Resection recommended for all patients who are
good surgical candidates
• The main duct is ≥10 mm in diameter
• . If the duct is 5 to 9 mm in diameter, additional
evaluation (EUS with fine-needle aspiration) ) is recommended
OPTIONAL OPERETIONS
• Pancreaticoduodenectomy
• Distal pancreatectomy
• Total pancreatectomy – rare!
• Segmental resection of the tumor
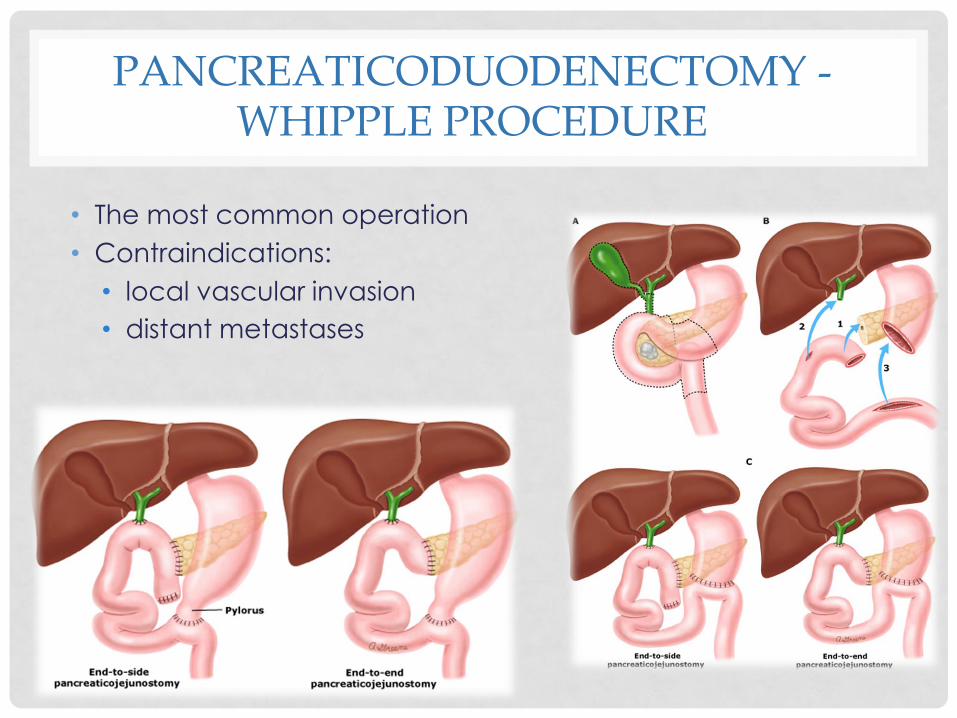
PANCREATICODUODENECTOMY - WHIPPLE PROCEDURE
• The most common operation
• Contraindications:
• local vascular invasion
• distant metastases
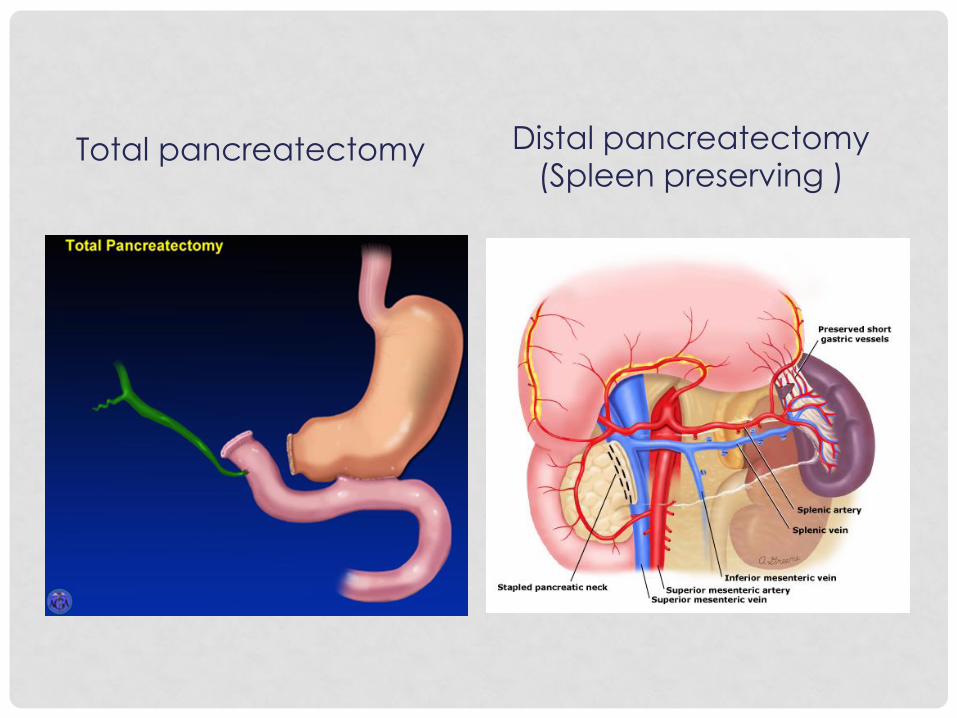
Total pancreatectomy Distal pancreatectomy (Spleen preserving )

FOLLOW-UP AFTER SURGERY
• noninvasive IPMN – the risk of developing a recurrence in
the remaining pancreas is at least 5%. In such patients,
yearly follow-up with CT or MRCP has been suggested.
• For patients with invasive IPMN, studies suggest the risk of
recurrence is 25-50%, and it has been suggested that these patients undergo surveillance every six months.

FOLLOWING PATIENTS WHO DO NOT UNDERGO SURGERY:
• Lesions <10 mm: Evaluation every 12 months
• Lesions between 10 and 20 mm: Evaluation every
6 to 12 months
• Lesions >20 mm: Evaluation every 3 to 6 months
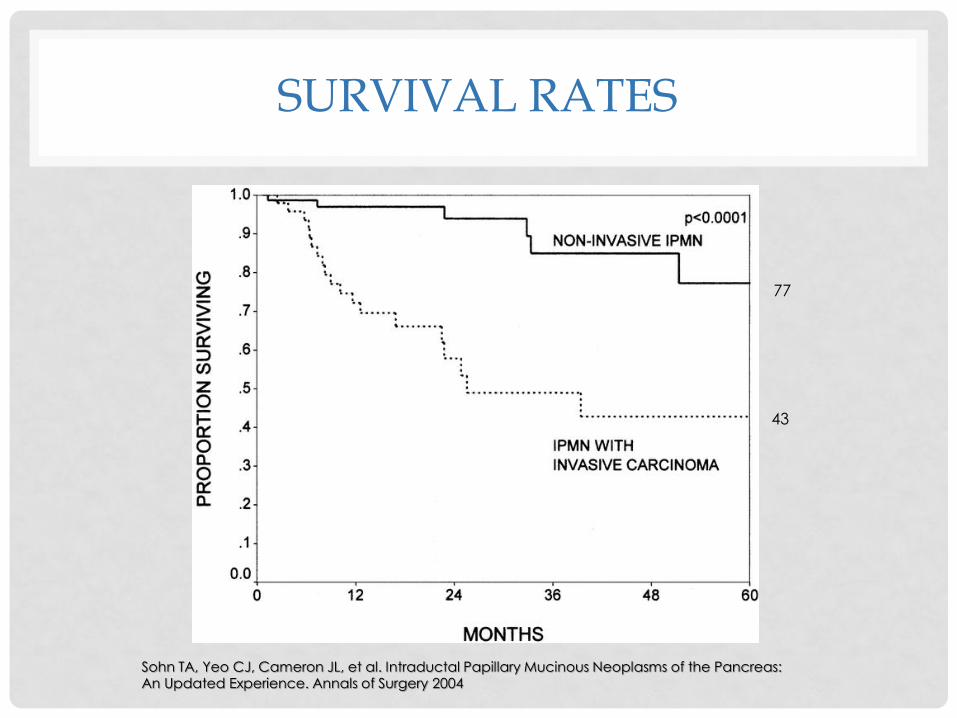
SURVIVAL RATES
Sohn TA, Yeo CJ, Cameron JL, et al. Intraductal Papillary Mucinous Neoplasms of the Pancreas: An Updated Experience. Annals of Surgery 2004
77
43

END THE





























