Embed Size (px)
Citation preview

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Research report
Zinc supplementation augments efficacy of imipramine in treatmentresistant patients: A double blind, placebo-controlled study
Marcin Siwek a, Dominika Dudek a, Ian A. Paul e, Magdalena Sowa-Kućmad, Andrzej Zięba a,Piotr Popik c,d, Andrzej Pilc c,d, Gabriel Nowak b,d,⁎a Department of Psychiatry, Collegium Medicum, Jagiellonian University, Kraków, Polandb Chair of Pharmacobiology, Collegium Medicum, Jagiellonian University, Kraków, Polandc Faculty of Public Health, Collegium Medicum, Jagiellonian University, Kraków, Polandd Institute of Pharmacology, Polish Academy of Sciences, Kraków, Polande Department of Psychiatry and Human Behavior, University of Mississippi Medical Center, Jackson, MS, USA
a r t i c l e i n f o a b s t r a c t
Article history:Received 22 June 2008Received in revised form 18 February 2009Accepted 18 February 2009Available online 10 March 2009
Background: One of the main problems in the therapy of depression is the limited efficacy ofantidepressants and the limited utility of augmentation strategies. Zinc, a non competitiveNMDA receptor antagonist exhibits preclinical antidepressant efficacy. Moreover, a preliminaryclinical report suggests augmentation of antidepressant therapy by zinc in depression.Methods: A placebo-controlled, double blind study of zinc supplementation in imipraminetherapy was conducted in sixty, 18–55-year old, unipolar depressed patients fulfilling the DSM-IV criteria for major depressionwithout psychotic symptoms. After a one week washout period,patients were randomized into two groups treated with imipramine (~140 mg/day) andreceiving once daily either placebo (n=30) or zinc supplementation (n=30, 25mgZn/day) for12 weeks.Results: No significant differences in CGI, BDI, HADRS and MADRS scores were demonstratedbetween zinc-supplemented and placebo-supplemented antidepressant treatment non-resistant patients. However, zinc supplementation significantly reduced depression scoresand facilitated the treatment outcome in antidepressant treatment resistant patients.Conclusion: Zinc supplementation augments the efficacy and speed of onset of therapeuticresponse to imipramine treatment, particularly in patients previously nonresponsive toantidepressant pharmacotherapies.These data suggest the participation of disturbed zinc/glutamatergic transmission in thepathophysiology of drug resistance.
© 2009 Elsevier B.V. All rights reserved.
Keywords:Unipolar depressionImipramine treatmentZincPlaceboSupplementation
1. Introduction
One of the main problems in the therapy of depression isthe limited efficacy of antidepressants and the problematicusefulness of augmentation strategies (Nemeroff, 2007;Nierenberg et al., 2008; Carvalho et al., 2007). Only about50% of treated patients reach remission criteria (Warden et
al., 2007; Kirsh et al., 2008). In addition, the dosage requiredto achieve remission often results in multiple unwantedeffects. These data clearly argue the need for novel anti-depressant therapies and/or augmentation strategies.
Recent studies suggest, that disturbances of glutamatergictransmission (especially NMDA receptor hyperactivation) areinvolved in the pathogenesis of mood disorders (Sanacoraet al., 2004a,b). Considerable evidence has accumulated overthe past 20 years indicating that direct and indirect NMDAreceptor antagonists exhibit antidepressant-like effects inpreclinical animal paradigms sensitive to antidepressants andin models of depression in rodents. Of particular note are the
Journal of Affective Disorders 118 (2009) 187–195
⁎ Corresponding author. Institute of Pharmacology, Polish Academy ofSciences, Smętna 12, PL 31-343 Kraków, Poland. Tel.: +48 12 6623 215;fax: +48 12 6374 500.
E-mail address: [email protected] (G. Nowak).
0165-0327/$ – see front matter © 2009 Elsevier B.V. All rights reserved.doi:10.1016/j.jad.2009.02.014
Contents lists available at ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r.com/ locate / j ad

Author's personal copy
recent reports that NMDA receptor antagonists also displayclinical efficacy (Berman et al., 2000; Prescorn et al., 2008;Zarate et al., 2006). Similarly, there are clinical reportssuggesting augmentation of antidepressant therapy by nonspecific NMDA receptor antagonists (e.g. amantadine, rilu-zole) in refractory depression (Dziedzicka-Wasylewska et al.,2002; Sanacora et al., 2004a,b).
Zinc is an important modulator of glutamatergic transmis-sion. The main activity of zinc in the glutamatergic system isan attenuation of NMDA receptor function—directly or viamodulation of AMPA receptors and metabotropic glutamatereceptors (Szewczyk et al., 2008; Nowak et al., 2005).Preclinical studies have demonstrated the antidepressant—like effects of zinc administration in animal tests/models ofdepression. Thus, zinc is active in preclinical antidepressantscreening paradigms such as the forced swim test and tailsuspension test in rodents (Kroczka et al., 2000; Kroczka et al.,2001; Nowak et al., 2003c; Rosa et al., 2003; Franco et al.,2007). Moreover, zinc has antidepressant-like properties, inanimal models of depression such as olfactory bulbectomy,chronic unpredictable stress and chronic mild stress in rats(Nowak et al., 2003c; Cieslik et al., 2007; Sowa-Kućma et al.,2008). Recent data has also revealed that zinc enhances theefficacy/potency of citalopram or imipramine in preclinicalparadigms sensitive to antidepressants. Thus, subeffectivedoses of zinc administered in combination with subeffectivedoses of antidepressants resulted in antidepressant-likeeffects in the forced swim test, tail suspension test andchronic unpredictable stress model (Cieslik et al., 2007; Cuchaet al., 2008; Rosa et al., 2003; Szewczyk et al., 2002, 2009).
Conversely, in rodents, chronic antidepressant (imipramine,citalopram) treatment slightly increases the zinc level in thehippocampus and decreases it in the cortex, cerebellum andbasal forebrain, although the calculation of the hippocampus/other brain regions zinc concentration ratio demonstrated asignificantly higher level of zinc in hippocampus after treat-ment of both drugs (Nowak and Schlegel-Zawadzka, 1999).Chronic electroconvulsive shock (ECS) also induced a robust(32%) increase in zinc concentration in hippocampus and small(11–15%) increases in other brain regions (Nowak and Schlegel-Zawadzka, 1999). Chronic ECS was also reported to increasehippocampal mossy fiber sprouting, which was demonstratedhistochemically by the zinc–selenium method (Vaidya et al.,1999; Lamont et al., 2001). This method actually determinesconcentrations of synaptic zinc, so this (Vaidya et al., 1999) andthe other reports (Lamont et al., 2001) indicate an increase inhippocampal zinc synaptic concentration induced by ECS.Recently, we have also demonstrated an increase in hippo-campal synaptic zinc concentration after chronic zinc treatment(Szewczyk et al., 2006). Complementing these data are clinicalinvestigations that have indicated an alteration of blood zinclevel as a potential marker of depression (Maes et al., 1994,1997, 1999; McLoughlin and Hodge, 1990; Nowak et al., 1999).
As noted above, there is much preclinical data to provide“proof of concept” that antagonists of the NMDA receptor canhave significant antidepressant efficacy. However, the dis-sociative effects of full antagonists such as ketamine limittheir introduction into general clinical practice. As a result,strategies which augment inhibition of the NMDA receptorwithout full antagonism may represent more viable clinicalapproaches. We recently reported in a preliminary clinical
study that zinc enhanced the efficacy of several antidepres-sants in patients withmajor depression (Nowak et al., 2003a).We now report that zinc augments the efficacy and speed ofonset of therapeutic response to imipramine treatment,particularly in patients previously nonresponsive to antide-pressant pharmacotherapies.
2. Methods
2.1. Patients and treatments
Patients admitted to the Department of PsychiatryCollegium Medicum Jagiellonian University or to AffectiveDisorder Outpatients (single center study, January 2005–April2006) and fulfilling the DSM-IV criteria for major depression,with a moderate or severe depressive episode withoutpsychotic symptoms (or drug or alcohol abuse/dependence)were accepted for the study. The patients were randomized1:1 by independent staff member into two groups: onereceiving placebo (group I, n=30) and second receiving zincsupplementation (group II, 25 mg Zn2+ once daily, ZincasForte, Farmapol, Poznan, Poland, n=30). Placebo was pre-pared by Farmapol (Poznan, Poland) as identical to the Zincastablets and consisted of all ingredients of Zincas besides zinchydroaspartate. All study researchers and subjects were blindto group allocation for the duration of the study. Both groupswere treated with imipramine (Polfarma, 100–200 mg oncedaily). All patients had a one week washout period withoutany pharmacotherapy.
2.2. Assessments
The Hamilton Depression Rating Scale (HDRS, 17 items)(Hamilton, 1960), Beck Depression Inventory (BDI) (Becket al., 1961), Clinical Global Impression (CGI) and Montgom-ery–Asberg Depression Rating Scale (MADRS) were used toassess efficacy of antidepressant therapy, and patients' statuswas evaluated before the treatment and 2, 6 and 12 weeksafter its commencement. A therapeutic response was definedas: “much” or “very much improved” in CGI scale plus at least50% reduction of MADRS (MADRS/CGI criteria) scores orHADRS scores (HADRS/CGI criteria). Remission was definedas: “very much improved” on the CGI scale plus scores onMADRS (MADRS/CGI criteria)≤10 or HADRS (HADRS/CGIcriteria)≤7 or BDI (BDI/CGI criteria)≤9. Staging of depressionbased on prior treatment response was made according to 6-grade treatment resistant criteria by Thase and Rush (1997).Scores were rated by well trained and experienced psychia-trists. Supplementation and assessment of the patients' statuswere performed according to a “double blind” procedure. Thestudy was approved by the Ethical Committee of CollegiumMedicum, Jagiellonian University, Kraków and the informedconsent was obtained from all participants. Trial Registry:Zinc supplementation of imipramine therapy; number:NTC00693680; URL: http://www.clinicaltrials.gov/.
2.3. Statistics
Assessments of depression were evaluated with GeneralLinear Model mixed design ANOVAwith the TEST NUMBER asrepeated factor, and TREATMENT and ANTIDEPRESSANT
188 M. Siwek et al. / Journal of Affective Disorders 118 (2009) 187–195

Author's personal copy
TREATMENT RESISTANCE as between factors, followed byDuncan's post-hoc test (Statistica 8 and SPSS 16). Depressionassessment data were distributed normally and the varianceswere homogenous; missing data were excluded from ana-lyses. Some of the data reported in tables did not meet criteriafor normal distribution, and thus they were assessed with theX2 test, Fisher's Exact Test, Mann Whitney U or Wilcoxontests, where appropriate. Data were deemed significant whenpb0.05.
3. Results
3.1. Patient characteristics
Group characteristics at the beginning of study arepresented in Table 1. The mean age (±SD) in the placebo-and zinc-treated groups was 45.7±6.1 and 46.2±5.8 years,respectively, and did not significantly differ (p=0.73, t-test).There were no significant differences in the male/female ratiobetween placebo (9/21) and zinc group (11/19) (X2 Test).Similarly, demographic parameters (education, employment,marital status, cigarette smoking, treatment site) were notsignificantly different between placebo and zinc groups(Table 1).
3.2. Exclusions
Some patients were excluded during the trial because ofunwanted side effects and need to alter therapeutic strategy(2 in placebo and 1 in zinc group) or due to compliance failure
(3 in placebo and 2 in zinc group). At the end of the study,groups consisted of 25 placebo-treated and 27 zinc-supple-mented patients (Table 2). The frequency of unwanted sideeffects was similar in both treatment groups (58.3%—Table 3).Only trial completers were included in the analysis of zinc andimipramine treatment effects.
3.3. Efficacy of treatment and supplementation
The mean of the final imipramine doses were similar inboth groups: 140.2±17.1 and 137.1±15.8 mg/day for placeboand zinc, respectively (p=0.47, Mann Whitney Test U).Themean±SD of the CGI-S and BDI in the beginning of therapywere 5.0±0.8 and 35.9±4.9, respectively, and did notsignificantly differ between placebo+imipramine and thezinc+imipramine groups. There were also no differencesbetween these groups assessed by HDRS and MAS score atbaseline (22.9±3.3 and 37.0±5.6, respectively).
The analysis of BDI scores (Fig. 1) revealed that treatmentwith imipramine and zinc resulted in lower scores than thetreatment with imipramine and placebo (main factor oftreatment). Moreover, antidepressant treatment non-resistantpatients showed lower scores than antidepressant treatmentresistant patients (main factor of treatment resistance). Allgroups demonstrated a gradual decrease in the scores over thetime of treatment (main factor of the test number). A significantinteraction between test number and antidepressant treatmentresistance suggest treatment resistance differently affected BDI
Table 1Demographic features of patients included in trial and comparison betweenindividual groups (χ2 and t-tests); (group Pl—imipramine and placebo-treatedpatients; group Zn—imipramine and zinc-treated patients; groups Pl+Zn—allpatients included in trial).
Group Pl+Zn(n=60)
Group Pl(n=30)
Group Zn(n=30)
GroupPl vs Zn
t-testAge 45.9±5.9 45.7±6.1 46.2±5.8 p=0.73
χ2 testSexFemale 40 (66.7%) 21 (70.0%) 19 (63.3%) p=0.58Male 20 (33.3%) 9 (30.0%) 11 (36.7%)
EducationElementary orprofessional
20 (33.3%) 9 (30.0%) 11 (36.7%) p=0.85
Secondary 29 (48.3%) 15 (50.0%) 14 (46.7%)Higher 11 (18.3%) 6 (20.0%) 5 (16.7%)
Employment statusEmployed 22 (36.7%) 14 (46.7%) 8 (26.7%) p=0.11Unemployed 38 (63.3%) 16 (53.3%) 22 (73.3%) p=0.54Annuitant 46 (76.7%) 22 (73.3%) 24 (80.0%)
Marital statusSingle 5 (8.3%) 3 (10.0%) 2 (6.7%) p=0.35Married 50 (83.3%) 26 (86.7%) 24 (80.0%)Separated/Divorced 5 (8.3%) 1 (3.3%) 4 (13.3%)
Cigarettes smokingNo 29 (48.3%) 16 (53.3%) 13 (43.3%) p=0.79Yes 31 (51.7%) 14 (46.7%) 17 (56.7%)
≤20 cigarettes/day 27 (46.7%) 13 (43.3%) 14 (46.7%)N20 cigarettes/day 4 (6.7%) 1 (3.3%) 3 (10%)
Place of therapy performed in recruitment dayOutpatient department 17 (28.3%) 10 (33.3%) 7 (23.3%) p=0.57Clinical department 43 (71.6%) 20 (66.7%) 23 (76.7%)
Table 2Number of patients in groups Pl and Zn in each measuring points (group Pl—imipramine and placebo-treated patients; group Zn—imipramine and zinc-treated patients).
Weeks of treatment
0 2 6 12
Group Pl 30 28 27 25Group Zn 30 29 27 27
Table 3Frequency of individual side effects observed during the trial in groups: Pl,ZnI, Pl+Zn and comparison between groups (χ2-test) (group Pl—imipramine and placebo-treated patients; group Zn—imipramine and zinc-treated patients; groups Pl+Zn—all patients included in trial).
GroupPl+Zn
Group Pl Group Zn GroupPl vs Znχ2 test
Patient excludedfrom trial by thereason of sideeffects
5 (8.3%) 3 (10.0%) 2 (6.7%) p=0.64
All side effects 35 (58.3%) 16 (53.33%) 19 (63.3%) p=0.43Dry mouth 30 (50%) 14 (46.7%) 16 (53.3%) p=0.61Dizziness/Orthostatichypotonia
19 (31.7%) 11 (36.7%) 8 (26.7%) p=0.41
Drowsiness 8 (13.3%) 5 (16.7%) 3 (10.0%) p=0.45Constipations 17 (28.3%) 7 (23.3%) 10 (33.3%) p=0.57Tachycardia 5 (8.3%) 3 (10.0%) 2 (6.7%) p=0.64Urinationdisturbances
3 (5.0%) 1 (3.3%) 2 (6.7%) p=0.55
Nausea 3 (5.0%) 2 (6.7%) 1 (3.3%) p=0.55Headache 3 (5.0%) 2 (6.7%) 1 (3.3%) p=0.55Visual disturbances 2 (3.3%) 1 (3.3%) 1 (3.3%) p=1.0
189M. Siwek et al. / Journal of Affective Disorders 118 (2009) 187–195

Author's personal copy
measure along with testing. The post-hoc analysis revealed thatall groups demonstrated significant improvement at week 2 ascompared with the baseline; however, the “antidepressanttreatment resistant group treated with imipramine andplacebo” did not demonstrate an improvement at week 6 ascompared with week 2 test, while other treatment groups did.In addition, at week 6, all groups showed significant reductionof scores as compared with “treatment resistant group treatedwith imipramine and placebo.” The difference between placeboand zinc supplementation in antidepressant treatment resistantgroups was seen also at week 12. These comparisons suggestlower BDI scores of imipramine and zinc treatment (ascompared with imipramine and placebo) in antidepressantresistant patients at weeks 6 and 12.
The analysis of CGI-S (Fig. 2) scores revealed that treatmentwith imipramine and zinc resulted in lower scores than thetreatment with imipramine and placebo (main factor oftreatment). All groups demonstrated a gradual decrease inthe scores over the time of treatment (main factor of the testnumber). In addition, the significant interactions between test
number and treatment as well as between test number andantidepressant treatment resistance suggested that thesefactors affected the CGI-S responses over the time of treatment.The post-hoc analysis revealed that all groups demonstratedsignificant improvement at week 2 as compared with thebaseline as well at week 12 as comparedwithweek 6, howeverthe “treatment resistant group treated with imipramine andplacebo” did not demonstrate an improvement at week 6 ascompared with week 2 test, while other treatment groups did.In addition, at weeks 6 and 12, all groups showed significantreduction of scores as compared with “treatment resistantgroup treated with imipramine and placebo.” These compar-isons suggest lower CGI-S scores of imipramine and zinctreatment as compared with imipramine and placebo inantidepressant resistant patients at weeks 6 and 12.
The analysis of HDRS scores (Fig. 3) revealed thattreatment with imipramine and zinc resulted in lower scoresthan the treatmentwith imipramine and placebo (main factorof treatment). All groups demonstrated a gradual decrease inthe scores over the time of treatment (main factor of the testnumber). In addition, the significant interactions between
Fig. 1. Effect of zinc supplementation on response to imipramine inantidepressants resistant and non-resistant patients measured by Beck Depres-sion Inventory (BDI). Data represent themean+SEM BDI scores of 9 treatmentresistant patients treated with imipramine+placebo, 16 treatment non-resistant patients treated with imipramine+placebo, 12 treatment resistantpatients treatedwith imipramine+zincand15 treatmentnon-resistantpatientstreated with imipramine+zinc. ANOVA demonstrated the following values:treatment: F(1,48)=6.05, Pb0.025, treatment resistance: F(1,48)=5.86,Pb0.025 and test number: F(3,144)=178, Pb0.001. The interaction betweentest number and treatment resistance was also significant: F(3,144)=3.57,Pb0.025. Post-hoc Duncan's test revealed that all groups demonstratedsignificant improvement at week 2 as compared with the baseline, howeverthe “antidepressant treatment resistant group treated with imipramine andplacebo” did not demonstrate an improvement at week 6 as compared withweek 2 test, while other treatment groups did (# symbol). At week 6, all groupsshowed significant reduction of scores as compared with “treatment resistantgroup treated with imipramine and placebo.” The difference between placeboand zinc supplementation in antidepressant treatment resistant groups wasseen also at week 12 (⁎ symbols). Analysis of covariance using Greenhouse–Geisser estimate revealed no interaction between test number and age, sex,education, smoking, length of disease, number of hospitalizations, final drugdose, and treatment resistance; only the test number×treatment interactionwas significant: F(2.467,96.195)=5.713, P=0.02.
Fig. 2. Effect of zinc supplementation in response to imipramine inantidepressants resistant and non-resistant patients measured by ClinicalGlobal Impression Scale (CGI). Data represent the mean+SEM CGI scores of 9treatment resistant patients treated with imipramine+placebo, 16 treatmentnon-resistant patients treated with imipramine+placebo, 12 treatmentresistantpatients treatedwith imipramine+zincand15 treatmentnon-resistantpatients treated with imipramine+zinc. ANOVA demonstrated the followingvalues: treatment: F(1,48)=7.56, Pb0.01 and test number: F(3,144)=143.55,Pb0.001. The following interactions were significant: test number×treatment:F(3,144)=3.13, Pb0.05 and test number×treatment resistance: F(3,144)=4.64, Pb0.01. Post-hoc Duncan's test revealed that all groups demonstratedsignificant improvement at week 2 as compared with the baseline as well atweek 12 as compared with week 6, however the “treatment resistant grouptreated with imipramine and placebo” did not demonstrate an improvement atweek 6 as compared with week 2 test, while other treatment groups did (#symbol). At weeks 6 and 12, all groups showed significant reduction of scores ascompared with “treatment resistant group treated with imipramine andplacebo” (⁎ symbols). Analysis of covariance using sphericity estimate revealedno interaction between test number and age, sex, education, smoking, length ofdisease, number of hospitalizations, final drug dose, and treatment resistance;however, the test number×treatment interaction: F(3,117)=6.07, P=0.01and test number× treatment resistance interaction: F(3,117)=4.205,P=0.007 were significant.
190 M. Siwek et al. / Journal of Affective Disorders 118 (2009) 187–195

Author's personal copy
test number and treatment as well as between test numberand antidepressant treatment resistance suggested that thesefactors affected the HDRS responses over the time oftreatment. A significant interaction between treatment andantidepressant treatment resistance suggest zinc supplemen-tation differently affected HDRS measure in the treatmentresistant and non-resistant patients. Post-hoc Duncan's testrevealed that all groups demonstrated significant improve-ment at week 2 as compared with the baseline, however the“treatment resistant group treated with imipramine andplacebo” did not demonstrate an improvement at week 6 ascomparedwithweek 2 test, while other treatment groups did.Conversely, this group showed lower HDRS scores at week 12as compared with the week 6, while other groups did not. Inaddition, at weeks 6 and 12, all groups showed significantreduction of scores as compared with “treatment resistantgroup treated with imipramine and placebo”. The differencebetween placebo and zinc supplementation in antidepressanttreatment resistant groups was already seen at week 2. Thesecomparisons suggest lower HDRS scores of imipramine andzinc treatment as compared with imipramine and placebo inantidepressant resistant patients at weeks 2, 6 and 12.
The analysis of MADRS scores (Fig. 4) revealed thattreatment with imipramine and zinc resulted in lower scoresthan the treatment with imipramine and placebo (mainfactor of treatment). All groups demonstrated a gradualdecrease in the scores over the time of treatment (mainfactor of the test number). A significant interaction betweentest number and antidepressant treatment resistance sug-gest that treatment resistance differently affected MADRSmeasure along with testing. A significant interactionbetween treatment and antidepressant treatment resistancesuggest that zinc supplementation affected MADRS measurein treatment resistant and non-resistant patients. Post-hocanalysis revealed that all groups demonstrated significantimprovement at week 2 as compared with the baseline aswell as an improvement at week 6 as compared with week 2test. Except the group of resistant patients supplementedwith placebo, none of other groups showed reduced MARDSscores between week 12 and week 6. Moreover, at week 2test, the group “resistant to antidepressants and treated withimipramine and placebo” demonstrated significantly higherscore than the “resistant to antidepressants treated with
Fig. 3. Effect of zinc supplementation in response to imipramine inantidepressants resistant and non-resistant patients measured by HamiltonDepressionRating Scale (HDRS). Data represent themean+SEMHDRS cores of9 treatment resistant patients treatedwith imipramine+placebo,16 treatmentnon-resistant patients treated with imipramine+placebo, 12 treatmentresistant patients treated with imipramine+zinc and 15 treatment non-resistant patients treated with imipramine+zinc. ANOVA demonstrated thefollowing values: treatment: F(1,48)=6.40, Pb0.025; test number: F(3,144)=238.4, Pb0.001. Three interactions were also significant: treatment×treatmentresistance: F(1,48)=4.74, Pb0.05; test number×treatment: F(3,144)=3.30,Pb0.05 and test number×treatment resistance: F(3,144)=4.46, Pb0.01. Post-hoc Duncan's test revealed that all groups demonstrated significant improve-ment at week 2 as compared with the baseline, however the “treatmentresistant group treated with imipramine and placebo” did not demonstrate animprovement at week 6 as compared with week 2 test, while other treatmentgroups did (# symbol). At weeks 6 and 12, all groups showed significantreduction of scores as compared with “treatment resistant group treated withimipramine and placebo” (⁎ symbols). Analysis of covariance using Green-house–Geisser estimate revealed no interaction between test number and age,sex, education, smoking, length of disease, number of hospitalizations, finaldrug dose, and treatment resistance, however, the test number×treatmentinteraction was significant: F(2.344,91.425)=6.522, P=0.001.
Fig. 4. Effect of zinc supplementation on response to imipramine in antidepres-sants resistant and non-resistant patients measured by Montgomery–AsbergDepressionRatingScale (MADRS).Data represent themean+SEMMADRSscoresof 9 treatment resistantpatients treatedwith imipramine+placebo,16 treatmentnon-resistant patients treatedwith imipramine+placebo,12 treatment resistantpatients treatedwith imipramine+zinc and 15 treatment non-resistant patientstreated with imipramine+zinc. ANOVA demonstrated the following values:treatment: F(1,48)=8.41, Pb0.01; test number: F(3,144)=267.7, Pb0.001. Twointeractions were also significant: treatment×treatment resistance: F(1,48)=5.88, Pb0.025 as well as test number×treatment resistance: F(3,144)=3.73,Pb0.025. Post-hocDuncan's test revealed that all groupsdemonstrated significantimprovementatweek2as comparedwith thebaselineaswell as an improvementat week 6 as compared with week 2 test (# symbols). At week 2 test, the group“resistant to antidepressants and treated with imipramine and placebo”demonstrated significantly higher score than the “resistant to antidepressantstreated with imipramine and zinc.” At weeks 6 and 12, the group “resistant toantidepressants and treated with imipramine and placebo” demonstratedsignificantly higher scores than all other groups (⁎ symbols). Analysis ofcovariance using Greenhouse–Geisser estimate revealed no interaction betweentest number and age, sex, education, smoking, length of disease, number ofhospitalizations, final drug dose, and treatment resistance; the interaction of thetest number×treatment was significant: F(2.449,95.510)=3.361, P=0.03.
191M. Siwek et al. / Journal of Affective Disorders 118 (2009) 187–195
Author's personal copy
imipramine and zinc.” At weeks 6 and 12, the group“resistant to antidepressants and treated with imipramineand placebo” demonstrated significantly higher scores thanall other groups. These comparisons suggest lower MADRSscores of imipramine and zinc treatment as compared withimipramine and placebo in antidepressant resistant patientsat weeks 2, 6 and 12.
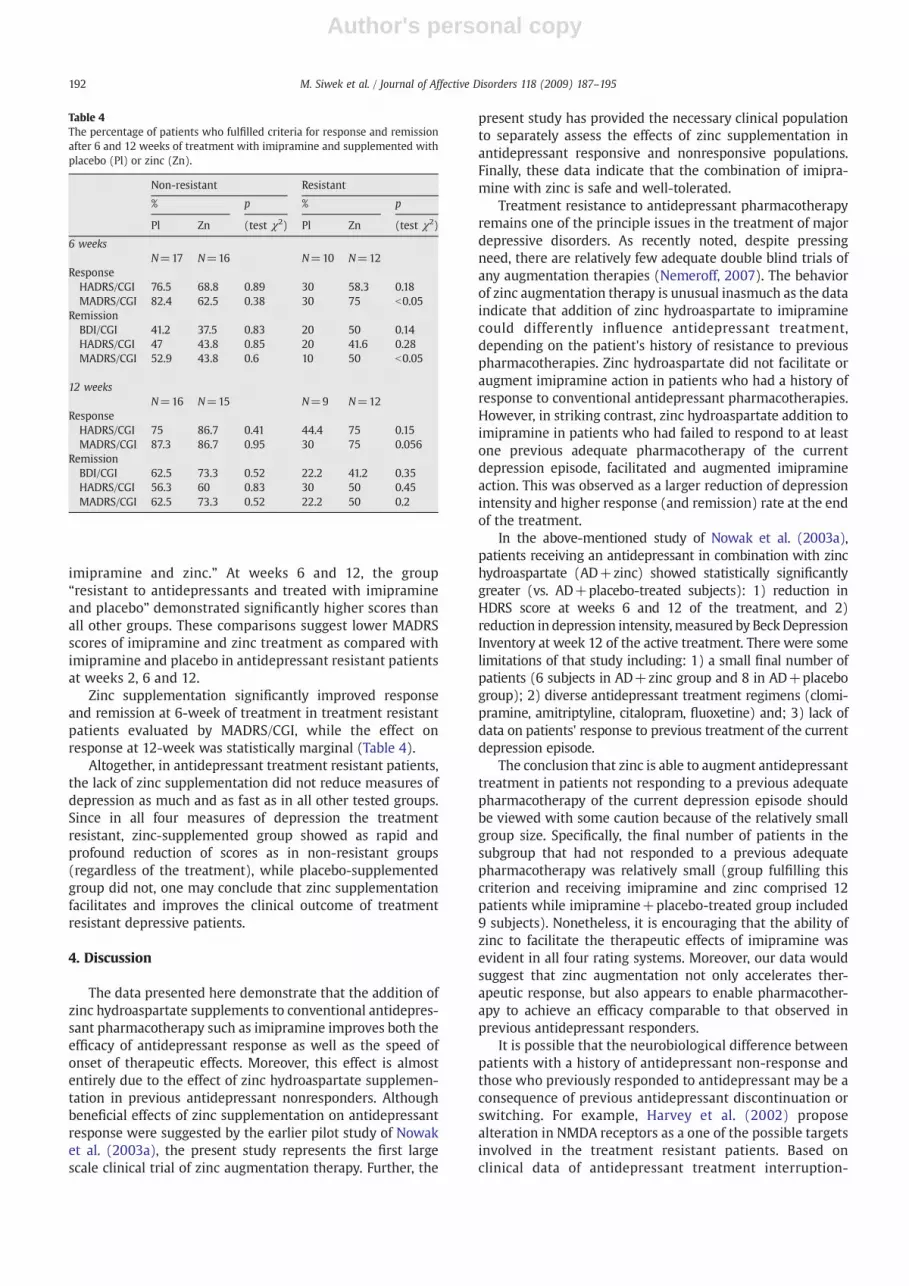
Zinc supplementation significantly improved responseand remission at 6-week of treatment in treatment resistantpatients evaluated by MADRS/CGI, while the effect onresponse at 12-week was statistically marginal (Table 4).
Altogether, in antidepressant treatment resistant patients,the lack of zinc supplementation did not reduce measures ofdepression as much and as fast as in all other tested groups.Since in all four measures of depression the treatmentresistant, zinc-supplemented group showed as rapid andprofound reduction of scores as in non-resistant groups(regardless of the treatment), while placebo-supplementedgroup did not, one may conclude that zinc supplementationfacilitates and improves the clinical outcome of treatmentresistant depressive patients.
4. Discussion
The data presented here demonstrate that the addition ofzinc hydroaspartate supplements to conventional antidepres-sant pharmacotherapy such as imipramine improves both theefficacy of antidepressant response as well as the speed ofonset of therapeutic effects. Moreover, this effect is almostentirely due to the effect of zinc hydroaspartate supplemen-tation in previous antidepressant nonresponders. Althoughbeneficial effects of zinc supplementation on antidepressantresponse were suggested by the earlier pilot study of Nowaket al. (2003a), the present study represents the first largescale clinical trial of zinc augmentation therapy. Further, the
present study has provided the necessary clinical populationto separately assess the effects of zinc supplementation inantidepressant responsive and nonresponsive populations.Finally, these data indicate that the combination of imipra-mine with zinc is safe and well-tolerated.
Treatment resistance to antidepressant pharmacotherapyremains one of the principle issues in the treatment of majordepressive disorders. As recently noted, despite pressingneed, there are relatively few adequate double blind trials ofany augmentation therapies (Nemeroff, 2007). The behaviorof zinc augmentation therapy is unusual inasmuch as the dataindicate that addition of zinc hydroaspartate to imipraminecould differently influence antidepressant treatment,depending on the patient's history of resistance to previouspharmacotherapies. Zinc hydroaspartate did not facilitate oraugment imipramine action in patients who had a history ofresponse to conventional antidepressant pharmacotherapies.However, in striking contrast, zinc hydroaspartate addition toimipramine in patients who had failed to respond to at leastone previous adequate pharmacotherapy of the currentdepression episode, facilitated and augmented imipramineaction. This was observed as a larger reduction of depressionintensity and higher response (and remission) rate at the endof the treatment.
In the above-mentioned study of Nowak et al. (2003a),patients receiving an antidepressant in combination with zinchydroaspartate (AD+zinc) showed statistically significantlygreater (vs. AD+placebo-treated subjects): 1) reduction inHDRS score at weeks 6 and 12 of the treatment, and 2)reduction in depression intensity,measured by BeckDepressionInventory at week 12 of the active treatment. There were somelimitations of that study including: 1) a small final number ofpatients (6 subjects in AD+zinc group and 8 in AD+placebogroup); 2) diverse antidepressant treatment regimens (clomi-pramine, amitriptyline, citalopram, fluoxetine) and; 3) lack ofdata on patients' response to previous treatment of the currentdepression episode.
The conclusion that zinc is able to augment antidepressanttreatment in patients not responding to a previous adequatepharmacotherapy of the current depression episode shouldbe viewed with some caution because of the relatively smallgroup size. Specifically, the final number of patients in thesubgroup that had not responded to a previous adequatepharmacotherapy was relatively small (group fulfilling thiscriterion and receiving imipramine and zinc comprised 12patients while imipramine+placebo-treated group included9 subjects). Nonetheless, it is encouraging that the ability ofzinc to facilitate the therapeutic effects of imipramine wasevident in all four rating systems. Moreover, our data wouldsuggest that zinc augmentation not only accelerates ther-apeutic response, but also appears to enable pharmacother-apy to achieve an efficacy comparable to that observed inprevious antidepressant responders.
It is possible that the neurobiological difference betweenpatients with a history of antidepressant non-response andthose who previously responded to antidepressant may be aconsequence of previous antidepressant discontinuation orswitching. For example, Harvey et al. (2002) proposealteration in NMDA receptors as a one of the possible targetsinvolved in the treatment resistant patients. Based onclinical data of antidepressant treatment interruption-
Table 4The percentage of patients who fulfilled criteria for response and remissionafter 6 and 12 weeks of treatment with imipramine and supplemented withplacebo (Pl) or zinc (Zn).
Non-resistant Resistant
% p % p
Pl Zn (test χ2) Pl Zn (test χ2)
6 weeksN=17 N=16 N=10 N=12
ResponseHADRS/CGI 76.5 68.8 0.89 30 58.3 0.18MADRS/CGI 82.4 62.5 0.38 30 75 b0.05
RemissionBDI/CGI 41.2 37.5 0.83 20 50 0.14HADRS/CGI 47 43.8 0.85 20 41.6 0.28MADRS/CGI 52.9 43.8 0.6 10 50 b0.05
12 weeksN=16 N=15 N=9 N=12
ResponseHADRS/CGI 75 86.7 0.41 44.4 75 0.15MADRS/CGI 87.3 86.7 0.95 30 75 0.056
RemissionBDI/CGI 62.5 73.3 0.52 22.2 41.2 0.35HADRS/CGI 56.3 60 0.83 30 50 0.45MADRS/CGI 62.5 73.3 0.52 22.2 50 0.2
192 M. Siwek et al. / Journal of Affective Disorders 118 (2009) 187–195

Author's personal copy
induced stress exacerbation (Michaelson et al., 2000), theydemonstrated an imipramine-withdrawal-induced increasein the density of NMDA receptors in the rat hippocampus(Harvey et al., 2002). Moreover, since increased stress mayaccount in the treatment resistance phenomena, additionalevidence may be derived from our previous work demon-strating enhancement of glycine affinity to glycine/NMDAsite in the cortex induced by forced swim challenge in rats(Nowak et al., 1995). Brain extracellular (synaptic) zincconcentration rapidly increases following peripheral (i.p.)acute or chronic zinc administration to rats (Opoka et al.,2008, our unpublished data). Thus, zinc supplementationmay augment inhibition of pathologically hyper-activeNMDA receptors in non-responder patients. The demonstra-tion that the volume of the hippocampus of multipledepressive episodes patients is reduced compared withfirst depressive episode patients or controls (MacQueenet al., 2003), and whichmay by related to ongoing stress [e.g.(Bonne et al., 2008; Lee et al., 2002)] also points to neuronaldamage, perhaps driven by NMDA receptor hyperactivity.
Zinc functions as a reversible antagonist of the NMDAreceptor complex (Smart et al., 1994). Moreover, preclinicalstudies have indicated that zinc, like other antagonists of theionophore, glutamate, glycine and polyamine recognition sites ofthe NMDA receptor has antidepressant-like properties (Kroczkaet al., 2000, 2001; Nowak et al., 2003c; Rosa et al., 2003; Francoet al., 2007; Cieslik et al., 2007; Sowa-Kućma et al., 2008). Inaddition, there is evidence for the ability of zinc to augment theeffects of tricyclic antidepressants in preclinical studies in mice(Cieslik et al., 2007; Cucha et al., 2008; Rosa et al., 2003;Szewczyk et al., 2002, 2009) and rats (Cieslik et al., 2007).
However, since zinc can interact with serotonergic,nicotinic acetylcholinergic and AMPA receptors and caninhibit the glycogen synthase kinase-3 (GSK-3) (Cucha etal., 2008; Szewczyk et al., 2008, 2009) it is premature to assertthat the adjunctive benefits of zinc are entirely due to actionsat NMDA receptors.
There is also growing evidence that major depressivedisorders are associated with reduced serum levels of zinc(Maes et al., 1994, 1997, 1999; McLoughlin and Hodge, 1990;Nowak et al., 1999). Moreover, it has been reported that serumzinc levels are particularly low in treatment resistant majordepressives (Maes et al., 1997) and that serum zinc levelsnormalize with successful antidepressant treatment (Maeset al., 1997; Schlegel-Zawadzka et al., 2000). The relationshipbetween serum zinc level and its concentration in discretebrain structures has not been established. Central interactionsbetween zinc and antidepressant drugs have been analyzedonly in animalmodels (Nowak and Schlegel-Zawadzka,1999).Studies in rats have shown that augmentation of antidepres-sant efficacy of imipramine administered in combinationwithzinc hydroaspartate was accompanied by a drop in totalcontent of zinc and desipramine, an imipramine metabolite,in the brain (Wyska et al., 2004). Conversely, long-termimipramine or citalopram treatment in rats caused asignificant 10% increase in zinc level in the hippocampus aswell as a significant decrease in the forebrain, cortex andcerebellum (Nowak and Schlegel-Zawadzka,1999). Moreover,imipramine administered repeatedly significantly diminishedIC50 value of zinc to inhibit [3H]dizocilpine binding to theNMDA receptor ion channel in rat cortex, indicating the
sensitization of NMDA receptor to the inhibitory effects ofzinc (Szewczyk et al., 2001). Finally, while zinc concentrationsis not altered in brain samples from suicide victims, the IC50
value of zinc to inhibit [3H]dizocilpine binding is increased insuicidal hippocampus (Nowak et al., 2003b). Taken together,these data suggest that augmentation of antidepressant effectof imipramine in combination with zinc is attributable toredistribution of zinc (and possibly imipramine) in the centralnervous system and to pharmacodynamic interactionbetween imipramine and zinc occurring directly and/orindirectly at NMDA receptor, thereby influencing glutamater-gic neurotransmission.
Open label trials with the NMDA receptor modulatorsriluzole and lamotrigine indicate the antidepressant efficacyof reducing NMDA receptor activity in treatment resistantpatients (Zarate et al., 2005; McElroy et al., 2004). Moreover,two placebo-controlled clinical studies have demonstratedthe efficacy of the NMDA receptor antagonist, ketamine, torelieve symptoms ofmajor depressive disorder in a previouslytreatment resistant population (Berman et al., 2000; Zarate etal., 2006). However, the dissociative properties of availableNMDA receptor antagonists such as ketamine limit the utilityof this treatment, particularly in non-inpatient settings.Although, very recently, Preskorn et al., have publishedexciting data with an NMDA NR2B receptor antagonistwhich demonstrates antidepressant activity without disso-ciative effects (Prescorn et al., 2008).
Nonetheless, these data combined with results of thepresent study suggest a contribution of NMDA receptorcomplex to pathophysiology underlying treatment resistancein major depressive disorders. Further investigations on theuse of NMDA receptor modulators in patients respondingunsatisfactorily to previous therapies are clearly warranted.However, in view of zinc's ability to interact with both NMDAand AMPA receptors, it is of interest to note that antidepres-sant effects of some NMDA receptor antagonists may alsoinvolve the activation of AMPA receptors (Dybała et al., 2008;Maeng et al., 2008).
In summary, this placebo-controlled, randomized doubleblind study confirms our previous report of the benefit of zincsupplementation of antidepressant therapy. Notably, zincsupplementation has no influence on the efficacy of imipra-mine therapy in patients with a prior history of positiveresponse to conventional antidepressant therapy. In contrast,zinc supplementation can robustly enhance the effect ofimipramine in previous treatment nonresponders by increas-ing the efficacy of this conventional antidepressant.
Role of funding sourceThis study was supported by the Funds for Statutory Activity of Collegium
Medicum, Jagiellonian University Krakow and the Institute of Pharmacology,Polish Academy of Sciences, Kraków, Poland, but had no further role in studydesign, in the collection, analysis and interpretation of data, in writing of thereport and in the decision to submit the paper for publication.
Conflict of interestNo conflict declared.
Acknowledgement
The authors thank “Farmapol” Sp. z o.o., Poznań, Polandfor the generous gifts of Zincas and placebo.
193M. Siwek et al. / Journal of Affective Disorders 118 (2009) 187–195

Author's personal copy
References
Beck, A.T., Ward, C.H., Mendelson, M., Mock, J., Erbaugh, J., 1961. An inventoryfor measuring depression. Arch. Gen. Psychiatry 4, 561–571.
Berman, R.M., Cappiello, A., Anand, A., Oren, D.A., Heninger, G.R., Charney, D.S.,2000. Antidepressant effects of ketamine in depressed patients. Biol.Psychiatry 47, 351–354.
Bonne, O., Vythilingam, M., Inagaki, M.,Wood, S., Neumeister, A., Nugent, A.C.,Snow, J., Luckernbaugh, D.A., Bain, E.E., Drevets,W.C., Charney, D.S., 2008.Reduced posterior hippocampal volume in posttraumatic stress disorder.J. Clin. Psychiatry 69, 1087–1091.
Carvalho, A.F., Cavalcante, J.L., Castelo, M.S., Lima, M.C.O., 2007. Augmentationstrategies for treatment-resistant depression: a literature review. J. Clin.Pharm. Ther. 32, 415–428.
Cieslik, K., Klenk-Majewska, B., Danilczuk, Z., Wrobel, A., Lupina, T., 2007.Influence of zinc supplementation on imipramine effect in a chronicunpredictable stress (CUS) model in rats. Pharmacol. Rep. 59, 46–52.
Cucha, M.P., Machado, D.G., Bettino, L.E.B., Capra, J.C., Rodrigues, A.L.S., 2008.Interaction of zinc with antidepressants in the tail suspension test. Prog.Neuro-Psychopharmacol. Biol. Psychiatry 32, 1913–1920.
Dybała,M., Siwek,A., Poleszak, E., Pilc, A., Nowak,G., 2008. Lack of NMDA-AMPAinteraction in antidepressant-like effect of CGP 37849, an antagonist ofNMDA receptor, in the forced swim test. J. Neural Transm. 115, 1519–1520.
Dziedzicka-Wasylewska, M., Rogóż, Z., Solich, J., Dudek, D., Wrobel, A., Zieba, A.,2002. Effect of joint administration of imipramine and amantadine onbinding of [3H]7-OH-DPAT to dopamine D3 receptors in peripheral bloodlymphocytes of the patients with drug-resistant unipolar depression. Pol. J.Pharmacol. 54, 703–706.
Franco, J.L., Posser, T., Brocardo, P.S., Trevisan, R., Uliano-Silva, M., Gabilan, N.H.,Santos, A.R., Lleal, R.B., Rodrigues, A.L., Farina, M., Dafre, A.L., 2007.Involvement of glutathione, ERK1/2 phophorylation and BDNF expressionin the antidepressant-like effect of zinc. Behav. Brain Res. 188, 316–323.
Hamilton, M., 1960. A rating scale for depression. J. Neurol. Neurosurg.Psychiatry 23, 56–61.
Harvey, B.H., Jonker, L.P., Brand, L., Heenop, M., Stein, D.J., 2002. NMDAreceptor involvement in imipramine withdrawal-associated effects onswim stress, GABA levels and NMDA receptor binding in rat hippocam-pus. Life Sci. 71, 43–54.
Kirsh, I., Deacon, B.J., Huedo-Medina, T.B., Scoboria, A., Moore, T.J., Johnson, B.T.,2008. Initial severity and antidepressant benefits: a meta-analysis of datasubmitted to the Food and Drug Administration. Ploos. Med. 5, 260–268.
Kroczka, B., Zieba, A., Dudek, D., Pilc, A., Nowak, G., 2000. Zinc exhibits anantidepressant-like effect in the forced swimming test in mice. Pol. J.Pharmacol. 52, 403–406.
Kroczka, B., Branski, P., Pałucha, A., Pilc, A., Nowak, G., 2001. Antidepressant-likeproperties of zinc in rodent forced swim test. Brain Res. Bull. 55, 297–300.
Lamont, S.R., Paulls, A., Stewart, C.A., 2001. Repeated electroconvulsivestimulation, but not antidepressant drugs, induces mossy fibre sproutingin the rat hippocampus. Brain Res. 893, 53–58.
Lee, A.L., Ogle, W.O., Sapolsky, R.M., 2002. Stress and depression: possiblelinks to neuron death in the hippocampus. Bipolar Disord. 4, 117–128.
Maeng, S., Zarate, C.A., Du, J., Schlosser, R.J.,McCammon, J., Chen, G., Manjii, H.K.,2008. Cellular mechanisms underlying the antidepressant effects ofketamine: role of alpha-amino-3-hydroxy-5-methylisoxazole-4-propionicacid receptors. Biol. Psychiatry 63, 349–352.
Maes, M., D'Haese, P.C., Scharpe, S., D'Hondt, P.D., Cosyns, P., De Broe, M.E.,1994. Hipozincemia in depression. J. Affect. Disord. 31, 135–140.
Maes, M., Vandoolaeghe, E., Neels, H., Demedts, P., Wauters, A., Meltzer, H.Y.,Altamura, C., Desnyder, R., 1997. Lower serum zinc in major depression isa sensitive marker of treatment resistance and of the immune/inflammatory response in that illness. Biol. Psychiatry 42, 49–358.
Maes, M., De Vos, N., Demedts, P., Wauters, A., Neels, H., 1999. Lower serumzinc in major depression in relation tochanges in serum acute phaseproteins. J. Affect. Disord. 56, 189–194.
MacQueen, G.M., Campbell, S., McEwen, B.S., MacDonald, K., Amano, S., Joffe,R.T., Nahmias, C., Young, L.T., 2003. Course of illness, hippocampalfunction, and hippocampal volume in major depression. Proc. Natl. Acad.Sci. 100, 1387–1392.
McElroy, S.L., Zarate, C.A., Cookson, J., Suppes, T., Huffman, R.F., Greene, P.,Ascher, J., 2004. A 52-week, open-label continuation study of lamotriginein the treatment of bipolar depression. J. Clin. Psychiatry 65, 204–210.
McLoughlin, I.J., Hodge, J.S., 1990. Zinc in depressive disorder. Acta Psychiatr.Scand. 82, 451–453.
Michaelson, D., Amsterdam, J., Apter, J., Fava, M., Londborg, P., Tamura, R.,Pagh, L., 2000. Hormonal markers of stress response following interrup-tion of selective serotonin reuptake inhibitor treatment. Psychoneur-oendocrinology 25, 169–177.
Nemeroff, C.B., 2007. Prevalence and management of treatment-resistantdepression. J. Clin. Psychiatry 68, 17–25.
Nierenberg, A.A., Ostacher, M.J., Huffman, J.C., Ametrano, R.M., Fava, M., Perlis,R.H., 2008. A brief review of antidepressant efficacy, effectiveness,indications, and usage for major depressive disorder. J. Occup. Environ.Med. 50, 428–436.
Nowak, G., Schlegel-Zawadzka, M., 1999. Alterations in serum and brain traceelement levels after antidepressant treatment: part I. Zinc. Biol. TraceElem. Res. 67, 85–92.
Nowak, G., Redmond, A., McNamara, M., Paul, I.A., 1995. Swim stressincreases the potency of glycine at the N-methyl-D-aspartate receptorcomplex. J. Neurochem. 64, 925–927.
Nowak, G., Zięba, A., Dudek, D., Krośniak, M., Szymaczek, M., Schlegel-Zawadzka, M., 1999. Serum trace elements in animal models and humandepression. Part I. Zinc. Hum. Psychopharmacol. Clin. Exp. 14, 83–86.
Nowak, G., Siwek, M., Dudek, D., Zieba, A., Pilc, A., 2003a. Effect of zincsupplementation on antidepressant therapy in unipolar depression: apreliminary placebo-controlled study. Pol. J. Pharmacol. 55, 1143–1147.
Nowak, G., Szewczyk, B., Sadlik, K., Piekoszewski, W., Trela, F., Florek, E.,Pilc, A., 2003b. Reduced potency of zinc to interact with NMDAreceptors in hippocampal tissue of suicide victims. Pol. J. Pharmacol.55, 455–459.
Nowak, G., Szewczyk, B., Wieronska, J.M., Branski, P., Palucha, A., Pilc, A.,Sadlik, K., Piekoszewski, W., 2003c. Antidepressant-like effects of acuteand chronic treatment with zinc in forced swim test and olfactorybulbectomy model in rats. Brain Res. Bull. 61, 159–164.
Nowak, G., Szewczyk, B., Pilc, A., 2005. Zinc and depression. An update.Pharmacol. Rep. 57, 713–718.
Opoka,W., Sowa-Kućma,M., Kowalska,M., Baś, B., Gołembiowska, K., Nowak, G.,2008. Intraperitoneal zinc administration increases extracellular zinc in therat prefrontal cortex. J. Physiol. Pharmacol. 59, 477–487.
Prescorn, S.H., Baker, B., Kolluri, S., Menniti, F.S., Krams, M., Landen, J.W.,2008. An innovative design to establish proof of concept of theantidepressant effects of the NR2B subunit selective N-methyl-D-aspartate antagonist, CP-101,606, in patients with treatment-refractorymajor depressive disorder. J. Clin. Psychopharmacol. 28, 631–637.
Rosa, A.O., Lin, J., Calixto, J.B., Santos, A.R., Rodrigues, A.L., 2003. Involvementof NMDA receptors and L-arginine-nitric oxide pathway in the anti-depressant-like effects of zinc in mice. Behav. Brain Res. 144, 87–93.
Sanacora, G., Gueorguieva, R., Epperson, C.N.,Wu, Y.T., Appel, M., Rothman, D.L.,Krystal, J.H., Mason, G.F., 2004a. Subtype-specific alterations of gamma-aminobutyric acid and glutamate in patients with major depression. Arch.Gen. Psychiatry 6, 705–713.
Sanacora, G., Kendel, S.F., Fenton, L., Coric, V., Krystal, J.H., 2004b. Riluzoleaugmentation for treatment-resistant depression. Am. J. Psychiatry 161,2132.
Schlegel-Zawadzka, M., Zieba, A., Dudek, D., Krosniak, M., Szymaczek, M.,Nowak, G., 2000. Effect of depression and of antidepressant therapy onserum zinc levels—a preliminary clinical study. In: Roussel, A.M.,Anderson, R.A., Favrier, A.E. (Eds.), Trace Elements in Man and Animals,vol. 10. Kluwer Academic Plenum Press, New York, pp. 607–610.
Smart, T.G., Xie, X., Krishek, B.J., 1994. Modulation of inhibitory andexcitatory amino acid receptor ion channels by zinc. Prog. Neurobiol.42, 393–441.
Sowa-Kućma, M., Legutko, B., Szewczyk, B., Novak, K., Znojek, P., Poleszak, E.,Papp, M., Pilc, A., Nowak, G., 2008. Antidepressant-like activity of zinc:further behavioral and molecular evidence. J. Neural Transm. 115,1621–1628.
Szewczyk, B., Kata, R., Nowak, G., 2001. Rise in zinc affinity for the NMDAreceptor evoked by chronic imipramine is species-specific. Pol. J.Pharmacol. 53, 641–645.
Szewczyk, B., Branski, P., Wieronska, J.M., Palucha, A., Pilc, A., Nowak, G.,2002. Interaction of zinc with antidepressants in the forced swimmingtest in mice. Pol. J. Pharmacol. 54, 681–685.
Szewczyk, G., Sowa, M., Czupryn, A., Wieronska, J.M., Branski, P., Sadlik, K.,Opoka, W., Piekoszewski, W., Smialowska, M., Skangiel-Kramska, J., Pilc, A.,Nowak, G., 2006. Increase in synaptic hippocampal zinc concentrationfollowing chronic but not acute zinc treatment in rats. Brain Res. 1090,69–75.
Szewczyk, B., Poleszak, E., Sowa, M., Siwek, M., Dudek, D., Ryszewska-Pokraśniewicz, B., Radziwoń-Zaleska, M., Opoka, W., Czekaj, J., Pilc, A.,Nowak, G., 2008. Antidepressant activity of zinc andmagnesium in viewof current hypotheses of antidepressant action. Pharmacol. Rep. 60,588–599.
Szewczyk, B., Poleszak, E., Wlaz, P., Wróbel, A., Blicharska, E., Cichy, A.,Dybała, M., Siwek, A., Pomierny-Chamioło, L., Piotrowska, A., Brański, P.,Pilc, A., Nowak, G., 2009. The involvement of serotonergic system in theantidepressant effect of zinc in the forced swim test. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 33, 323–329.
Thase, M.E., Rush, A.J., 1997. When at first you don't succeed: sequentialstrategies for antidepressant nonresponders. J. Clin. Psychiatry 58 (Suppl13), 23–29.
194 M. Siwek et al. / Journal of Affective Disorders 118 (2009) 187–195

Author's personal copy
Vaidya, V.A., Siuciak, J.A., Du, F., Duman, R.S., 1999. Hippocampal mossy fibersprouting induced by chronic electroconvulsive seizures. Neuroscience89, 57–66.
Warden, D., Rush, A.J., Trivedi, M.H., Fva, M., Wisniewski, S.R., 2007. TheSTAR⁎D Project results: a comprehensive review of findings. Curr.Psychiatry Rep. 9, 449–459.
Wyska, E., Szymura-Oleksiak, J., Opoka, W., Baś, B., Niewiara, E., Pomierny, L.,Dybała, M., Nowak, G., 2004. Pharmacokinetic interaction after jointadministration of zinc and imipramine in forced swim test in mice. Pol. J.Pharmacol. 56, 479–484.
Zarate,C.A.,Quiroz, J.A., Singh, J.B., Denicoff, K.D., De Jesus, G., Luckenbaugh,D.A.,Charney, D.S., Manjii, H.K., 2005. An open-label trial of the glutamate-modulating agent riluzole in combinationwith lithium for the treatment ofbipolar depression. Biol. Psychiatry 57, 430–432.
Zarate, C.A., Singh, J.B., Carlson, P.J., Brutsche, N.E., Ameli, R., Luckenbaugh, D.A.,Charney, D.S., Manji, H.K., 2006. A randomized trial of an NMDA antagonistin treatment-resistant major depression. Arch. Gen. Psychiatry 63,856–864.
195M. Siwek et al. / Journal of Affective Disorders 118 (2009) 187–195








![Autoradiography of antidepressant binding sites in the human brain: localization using [3h]imipramine and [3h]paroxetine](https://img.dokumen.tips/doc/110x75/63141e703ed465f0570afe35/autoradiography-of-antidepressant-binding-sites-in-the-human-brain-localization.jpg)




















