Embed Size (px)
Citation preview
0 | P a g e
Water, Sanitation and HygieneNeeds Assessment
Laghman , Nangarhar, and Kunar Province
April 2019
1 | P a g e
ABBREVIATIONS
BPHS Basic Package of Health Services
EPHS Essential Package of Hospital Services
DG District Governor
DoPH Directorate of Public Health
DoRR Directorate of Refugees and Returnees
EPHS Essential Packages of Health Services
FGD Focus Group Discussion
HF Health Facility
HP Hygiene Promoter
IOM International Organization for Migration
IDP Internally Displaced People
IEC Information Education and Communication
INGO International Non-Government Organization
IMC International Medical Corps
KAP Knowledge Attitude Practice
KIIs Key Informants Interviews
M&E Monitoring and Evaluation
MoPH Ministry of Public Health
MRRD Ministry of Rural Rehabilitation and Development
NGO Non-Governmental Organization
OFDA Office for Foreign Disaster Assistance
UNHCR United Nations High Commissioner for Refugees
UNOCHA United Nation Office for Coordination of Humanitarian Assistance
WASH Water, Sanitation and Hygiene
2 | P a g e
Table of Contents
Major findings of the Assessment are: .................................................................................................51. Assessment Objective .................................................................................................................92. Training of Enumerators: ............................................................. Error! Bookmark not defined.3. Coordination: ..............................................................................................................................94. Ethical Consideration: ...............................................................................................................105. Gender Mainstreaming.............................................................................................................106. Questionnaires and Assessment Tools: ....................................................................................107. Methodology Adapted..............................................................................................................108. Survey Limitations:....................................................................................................................109. Challenges faced in data collection: .........................................................................................1110. Surveyors Teams: ......................................................................... Error! Bookmark not defined.VI -Data Collection Methods:................................................................................................................111 Desk Review / Secondary Data Review:....................................................................................112 Key Stakeholders Meeting: .......................................................................................................113 Community Influential Meeting:...............................................................................................114 Needs Assessment :..........................................................................................................................11Daily Debriefing:....................................................................................................................................12Data Analysis and Reporting: ................................................................................................................13V: Stakeholder Analysis.........................................................................................................................13VII: MAIN FINDINGS ..............................................................................................................................17General Observation:............................................................................................................................17Potable Water: ......................................................................................................................................17Sanitation and Hygiene:........................................................................................................................17Hygiene Promotion ...............................................................................................................................18Environmental Health: ..........................................................................................................................19DATA TRINGULLATION:.........................................................................................................................19BENIFICIARIES TO BE TARGETED:..........................................................................................................20RECOMMENDATIONS: ..........................................................................................................................20Water Supply Infrastructure: ................................................................................................................20Sanitation Infrastructure:......................................................................................................................20Hygiene Promotion: ..............................................................................................................................20Environmental Health: ..........................................................................................................................21Detailed Beneficiaries Data:..................................................................................................................22
3 | P a g e
I. Need Assessment Summary and JustificationsAfghanistan continues to face immense humanitarian, environmental, social and political challenges.Continuous armed conflict, insecurity and recurrent disasters have resulted in large scale of internaldisplacements with in Afghanistan. As of December 31, 2018, IOM ’s Displacement Tracking System(DTS) has recorded a total of 95,970 people as being displaced in the 3 Eastern provinces ofNangarhar, Kunar and Laghman. The overall WASH infarastructure coverage remains cahllanging forthe newly displaced and hosting communities in terms of quanitity and quality. The eastern provinces,especially Nangarhar is among the provinces that houses the majority of the returnees, remains thehighest for the WASH needs for the returnees. Lack of improved sanitation coverage and are at thehighest risk of disease outbreaks including Acute Watery Diarrhea (AWD). Moreover, the conflict,drought and poverty is affecting the capacities of the communities to maintain necessary basic WASHinfrastructure in the targeted hard-to-reach areas. The current spill of drought, resulting from lowrainfall and snowpack melt in 2017 and 2018, has worsened the water availability in 2018 and part of2019.
As per the Humanitarian Needs Overview (HNO) 2019, the water supply and sanitation in Afghanistanis one of the worst in the world with almost 60% of Afghans have limited to none access to improvedsanitation and over 36% still using unprotected water sources. The continued returnees from Pakistanand Iran has added pressure on the already overwhelmed and dilapidated WASH infrastructure andhas stretched the available local resources posing extreme health risks to an already vulnerablecommunities and overwhelmed health system. Moreover, Poor and unsafe WASH practices adoptedamong the displaced populations has resulted in increased open defecation hence diarrheas amongchildren.
Based on WASH cluster data, the families of both documented and undocumented returnees,especially those coming from Pakistan, face a higher risk of poor access to improved WASHinfrastructure, with more than 60% of the returnees living in informal settlements with limited or noservices. Kabul, Kandahar and Nangarhar are the provinces with the highest gaps in WASH needs forthe returnees. IOM and UNHCR estimate that over 163,000 undocumented and 60,000 documentedrefugees will return from Iran and Pakistan in 2019 and a significant percentage of these People willbe in need of WASH assistance.
Based on past trends, an estimated 150,000 people will be affected by sudden onset natural disasters(e.g. floods and avalanches) with the potential to damage and destroy assets and livelihoods,generating additional needs. Communities living in insecure and remote and hard to reach districtsthat repeatedly suffer from the impacts of disasters and conflict are often not adequately assisted byhumanitarian actors. Those communities hosting considerable numbers of IDPs/returnees will suffersevere shortages of basic services unless additional assistance is provided. Conflict, drought andpoverty is affecting the capacities of the communities to maintain necessary basic WASHinfrastructure in the targeted hard-to-reach areas.
The eastern provinces, especially Nangarhar is among the provinces that houses the majority of thereturnees, remains the highest for the WASH needs for the returnees. Lack of improved sanitationcoverage and are at the highest risk of disease outbreaks including Acute Watery Diarrhea (AWD).
On 22 April 2019, an intra-NSAG conflict in the Zawa area of Khogyani and Wadisar in Sherzad districtled to large scale conflict based displacement. As of 30 April 2019, reportedly 56,329 people (8,047families) have been displaced from both the districts. The people have mainly been displaced fromthe Khogyani district (Haider Baba Kalai, Chakaw, Star Kalai, Kadalai, Shekh Neka, Chenargai,Khadarkhil, Asman Kalai, Soor Ragha, Tawda Chena, Bagicha) and Sherzad district (Wadisar, StaraTormai, Chapari, Markikhil, Bulelkhil, Leshakai, Kodikhil, Totoo, Gandomak and Ashfan). According to

4 | P a g e
the initial information, 63% (5,073 families) of the displaced people have moved to Surkhrod district,followed by Behsud (1,145 families), while 981 families have settled within the Khogyani district(Chamtala settlement and district center). A number of people have moved to Jalalabad city, Kama,Rodat district.
As per the nature of the movement due to conflict the IDPs left in a hurry used whatever transportmeans available and were unable to carry their belongings. The IDPs are currently face, lack ofclothing, shelter, hygiene materials and cooking materials. However, these districts have receivedsubstantial displacement from within Nangarhar as well as from neighboring Kunar and Laghmanprovinces in recent past, 70-80 % of the returnees from Pakistan have also settled in these districts.There is pressure buiding on the existing and overstretched available local housing market, withhouses and shelters getting scarce, and rental prices sprang higher.
Three health facilities (Zawa, Mamakhil and Belal Ahmadkhil) in the conflict areas remains nonfunctional, according to the health cluster. There were 4 schools (Miagan, Sekandari, and Zawa Boysand Girls schools) already closed before this conflict in the district, which already had a negativeimpact on the education and health service access for some displaced people. With pressure on theexisting water resources (wells), there is a need to reinforce the WASH service provision in the targtedvillages and districts hosting the IDPs, as the increased population is putting strain on the currentresources. On the afternoon of March 23, 2019, combatants affiliated with Islamic State Khorasan(ISK) launched simultaneous attacks on Taliban positions in Digal, Korangal and Manar villages ofChapadara district, resulting in heavy fighting that has displaced over 21,000 people (3,112 families)within Kunar and Nangarhar provinces. This includes over half of the population of Chapadara districtwho have fled the area. Other people in affected areas may be unable to leave due to restrictions onmovement, checkpoints or the challenges in moving over mountainous and remote areas. Displacedpeople have mostly relocated to nearby safe villages from the Taliban controlled areas; closer to thedistrict center and the Dara E Pech areas controlled by the Government or to the Provincial capital ofAsadabad. While numbers cannot be determined accurately, several civilian casualties and injurieshave been reported.
Location:
Nangarhar:
Nangarhar has 22 districts, including Spinghar district Achin (Batikot, Chaparhar, Haska Mina, Khewa,Khogyani, Sherzad, Pachiraga, Hisarak, Koot, Nazyan, Spingghar, Ghanikhel, Goshta, Momand Dara,Lalpora, Bihsud, Sorkh Roud, Dara-i-Noor, Door Baba, Rodat and Kama). The city of Jalalabad servesas the capital of the province, which is among one of the 5 major cities of Afghanistan and is highlypopulated town. Total population of Nangarhar province is estimated to be around 1,635,873.
Following districts have been selected and covered by the assessment: Rodat, Batikot, Behsud,Mohmandara, Goshta.
Kunar:
Kunar is a mountainous province of the country bordered with Nuristan province in north, south withNangarhar province, west with Laghman province and also bordered with Pakistan in itseast. Currently, Kunar has 15 administrative units, including Asadabad the provincial capital , KhasKunar, Noorgul, Sawkai, Narang, Sarkano, Marawara, Shegal, Dangal, Asmar, Ghazi Abad, Nari,Watapur, Manogai and Chapa Dara districts. Kunar Province (Chawki, Khas Kunar, Shegal and Chapa

5 | P a g e
Dara Districts). Total population of the province is estimated 48,211. The assessment mainly covered3 following district of Kunar Province (Shegal, Sakaney and Khas Kunar Districts).
Laghman:
Laghman is among the eastern provinces of the country. Nangarhar is located to the south andsoutheast of Laghman, Kunar to its northeast, Nuristan to its north, Panjshir to its northwest and Kabuland Kapisa provinces to its west. Laghman province has six administrative units including the capital;Mehtar Lam. Alishing, Alingar, Dawlat Shah, Qargayi and Bad Pukh are the districts. Total populationof the province is estimated around 476537. The assessment has covered the following districts of theprovince: Laghman Province (Mehterlam the capital city and Qargayi Districts)
Major findings of the Assessment:
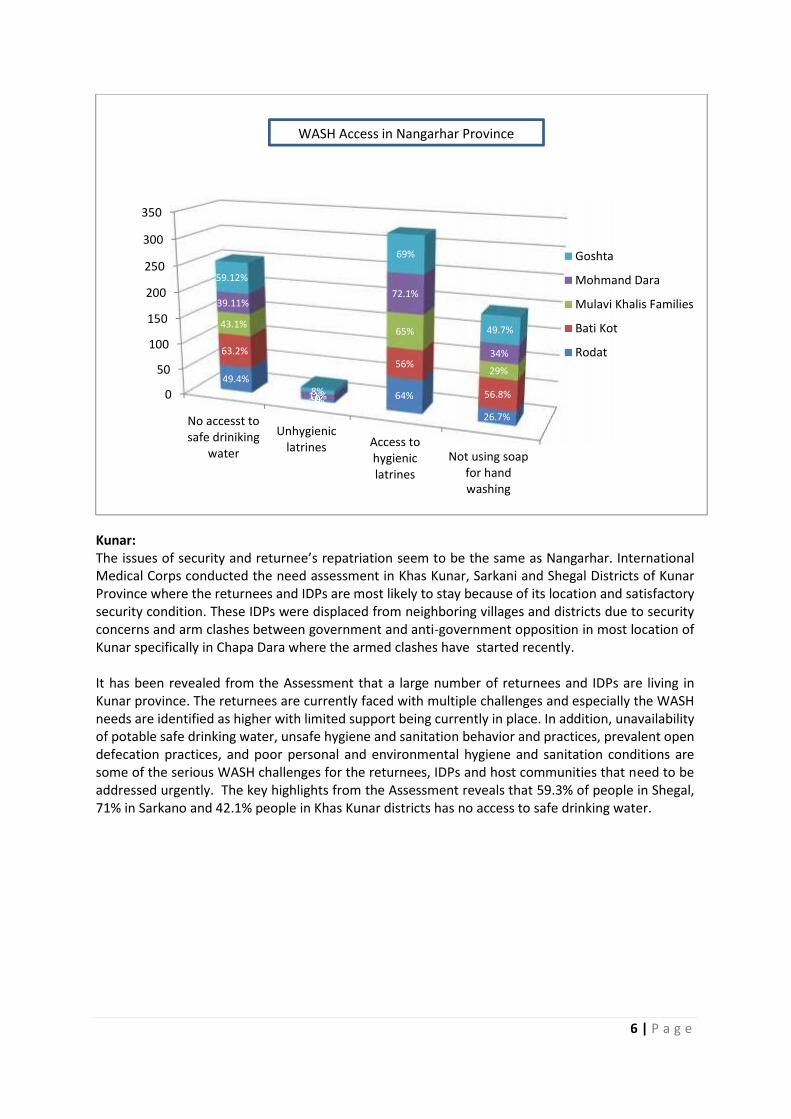
Nangarhar:
Safe Drinking water: The 49.4% of people in Rodat, 63.2% in Bati Kot, 43.1% people in Mulavi KhalisFamilies, 39.11% people in Mohmand Dara district, 59.12% people in Goshta, 39% people inMehterlam, 44.12% people in Qargayi, 59.7% in Khas Kunar, 55.3% people in Sarkani and 44.5% peoplein Shegal district have no access to safe potable drinking water and use the unprotected water sources.
Sanitation: 5% people in Rodat, 0% in Bati Kot, 0% people in Mulavi Khalis Families, 11% people inMohmand Dara district, 8% people in Goshta, 0% people in Mehterlam, 15% people in Qargayi, 23%in Khas Kunar, 45.2% people in Sarkani and 51.6% people in Shegal district have no access to hygieniclatrines and open defectaion was observed by the assessment team as common exterta disposalpractices.
Hygiene promotion: Overall the education level revealed to be lower among these communities.More than 71% families reported that they didn’t receive Hygiene Kits and those who have receivedit while they have been settled in returnees camp acknowledge that they received the hygiene kits.Open defecation practice has been noticed as one of the very common phenomena particularly amongreturnees and IDPs who live with the host communities inside the villages. Hygiene promotionactivities are carried out only in planned settlements and the rest areas (mostly scattered) were leftout.
Hand washing practice: The hand washing practices reported, to be in a very poor condition. Theassessment shows that 42.1% of people in Rodat, 39.12% in Bati Kot, 29.9% people in Mulavi KhalisFamilies, 42.4% people in Mohmand Dara district, 16% people in Goshta, 13% people in Mehterlam,43.79% people in Qargayi, 55.3% in Khas Kunar, 41.1% people in Sarkani and 46.7% people in Shegaldistrict were reported as not using soaps as safe hand washing practice at the critical times. Similarly,during the assessment the teams visited randomly few schools in every district and none of them werefound to having hand washing facilities as well as the knowledge identified limited about safe handwashing practices and majority of them were not washing their hand during critical times.
6 | P a g e
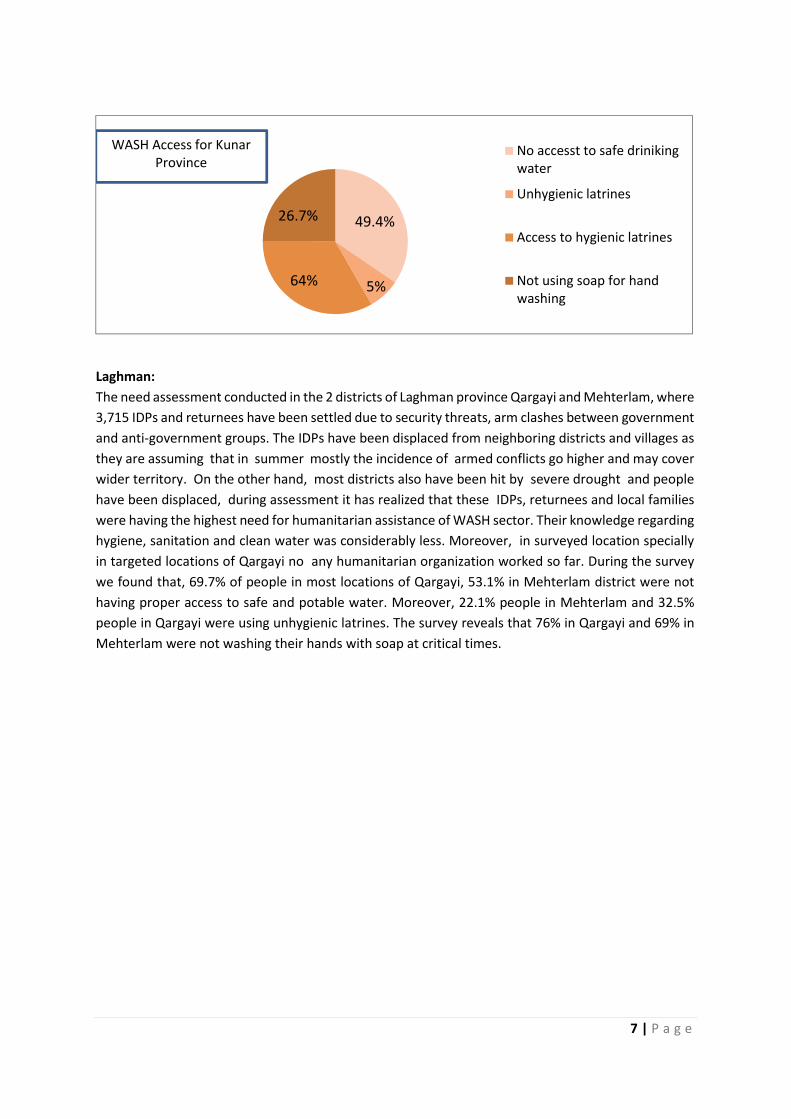
Kunar:The issues of security and returnee’s repatriation seem to be the same as Nangarhar. InternationalMedical Corps conducted the need assessment in Khas Kunar, Sarkani and Shegal Districts of KunarProvince where the returnees and IDPs are most likely to stay because of its location and satisfactorysecurity condition. These IDPs were displaced from neighboring villages and districts due to securityconcerns and arm clashes between government and anti-government opposition in most location ofKunar specifically in Chapa Dara where the armed clashes have started recently.
It has been revealed from the Assessment that a large number of returnees and IDPs are living inKunar province. The returnees are currently faced with multiple challenges and especially the WASHneeds are identified as higher with limited support being currently in place. In addition, unavailabilityof potable safe drinking water, unsafe hygiene and sanitation behavior and practices, prevalent opendefecation practices, and poor personal and environmental hygiene and sanitation conditions aresome of the serious WASH challenges for the returnees, IDPs and host communities that need to beaddressed urgently. The key highlights from the Assessment reveals that 59.3% of people in Shegal,71% in Sarkano and 42.1% people in Khas Kunar districts has no access to safe drinking water.
0
50
100
150
200
250
300
350
No accesst tosafe driniking
water
Unhygieniclatrines Access to
hygieniclatrines
Not using soapfor handwashing
49.4%
5% 64%
26.7%
63.2%
0
56%
56.8%
43.1%
0
65%
29%
39.11%
11%
72.1%
34%
59.12%
8%
69%
49.7%
Goshta
Mohmand Dara
Mulavi Khalis Families
Bati Kot
Rodat
WASH Access in Nangarhar Province
7 | P a g e
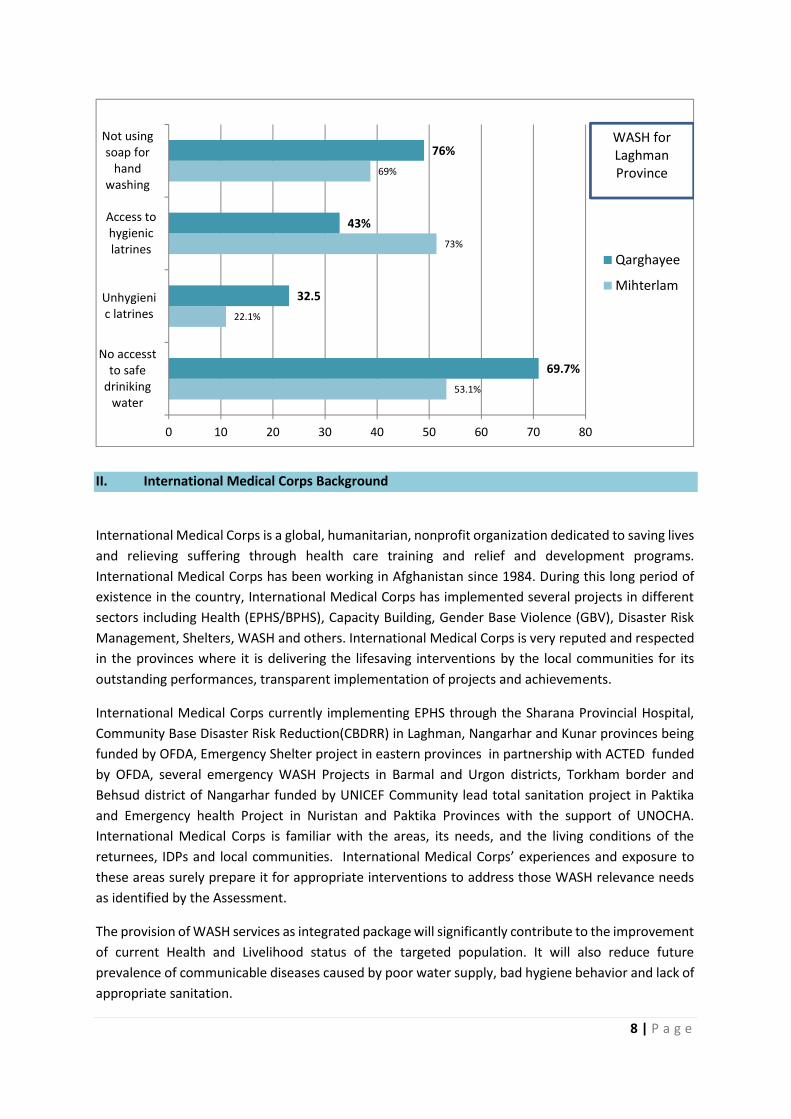
Laghman:The need assessment conducted in the 2 districts of Laghman province Qargayi and Mehterlam, where3,715 IDPs and returnees have been settled due to security threats, arm clashes between governmentand anti-government groups. The IDPs have been displaced from neighboring districts and villages asthey are assuming that in summer mostly the incidence of armed conflicts go higher and may coverwider territory. On the other hand, most districts also have been hit by severe drought and peoplehave been displaced, during assessment it has realized that these IDPs, returnees and local familieswere having the highest need for humanitarian assistance of WASH sector. Their knowledge regardinghygiene, sanitation and clean water was considerably less. Moreover, in surveyed location speciallyin targeted locations of Qargayi no any humanitarian organization worked so far. During the surveywe found that, 69.7% of people in most locations of Qargayi, 53.1% in Mehterlam district were nothaving proper access to safe and potable water. Moreover, 22.1% people in Mehterlam and 32.5%people in Qargayi were using unhygienic latrines. The survey reveals that 76% in Qargayi and 69% inMehterlam were not washing their hands with soap at critical times.
49.4%
5%64%
26.7%
No accesst to safe drinikingwater
Unhygienic latrines
Access to hygienic latrines
Not using soap for handwashing
WASH Access for KunarProvince
8 | P a g e
II. International Medical Corps Background
International Medical Corps is a global, humanitarian, nonprofit organization dedicated to saving livesand relieving suffering through health care training and relief and development programs.International Medical Corps has been working in Afghanistan since 1984. During this long period ofexistence in the country, International Medical Corps has implemented several projects in differentsectors including Health (EPHS/BPHS), Capacity Building, Gender Base Violence (GBV), Disaster RiskManagement, Shelters, WASH and others. International Medical Corps is very reputed and respectedin the provinces where it is delivering the lifesaving interventions by the local communities for itsoutstanding performances, transparent implementation of projects and achievements.
International Medical Corps currently implementing EPHS through the Sharana Provincial Hospital,Community Base Disaster Risk Reduction(CBDRR) in Laghman, Nangarhar and Kunar provinces beingfunded by OFDA, Emergency Shelter project in eastern provinces in partnership with ACTED fundedby OFDA, several emergency WASH Projects in Barmal and Urgon districts, Torkham border andBehsud district of Nangarhar funded by UNICEF Community lead total sanitation project in Paktikaand Emergency health Project in Nuristan and Paktika Provinces with the support of UNOCHA.International Medical Corps is familiar with the areas, its needs, and the living conditions of thereturnees, IDPs and local communities. International Medical Corps’ experiences and exposure tothese areas surely prepare it for appropriate interventions to address those WASH relevance needsas identified by the Assessment.
The provision of WASH services as integrated package will significantly contribute to the improvementof current Health and Livelihood status of the targeted population. It will also reduce futureprevalence of communicable diseases caused by poor water supply, bad hygiene behavior and lack ofappropriate sanitation.
53.1%
22.1%
73%
69%
69.7%
32.5
43%
76%
0 10 20 30 40 50 60 70 80
No accesstto safe
drinikingwater
Unhygienic latrines
Access tohygieniclatrines
Not usingsoap for
handwashing
Qarghayee
Mihterlam
WASH forLaghmanProvince
9 | P a g e
III. Assessment Description:
1. Assessment ObjectiveTo have an in-depth knowledge on current WASH service provision and the gaps for Afghan returnees,IDPs and local communities particularly who have returned back to Afghanistan in the past 18 months.The Assessment result will invariably guide International Medical Corps to provide short and medium-term WASH supports to these impoverished communities.
International Medical Corps’ main objective for this Assessment was to identify the critical gaps andneeds of the returnees and IDPs, and to prioritize future short and medium term emergency WASH.However, in the process, we have also identified the emergency Shelter needs in our targeted areas,which is being analyzed and reported separately for future interventions
International Medical Corps conducted need assessment and the final report to designed contextuallyappropriate, innovative and effective program to promote WASH and Health through the followingprimary tasks.
a. Complete a desk review;
b. Conduct a series of meetings with key stakeholders;
c. Train the surveyors of International Medical Corps on how to conduct the assessment, using thepre-constructed assessment tool, in the relevant geographic areas;
d. Analyze the primary and secondary data being collected;
e. Assessment report including recommendations.
International Medical Corps’ main objective for this Assessment was to identify the critical gaps andneeds of the returnees and IDPs, and to prioritize future short and medium term emergency WASH.However, in the process, we have also identified the emergency Shelter needs in our targeted areas,which is being analyzed and reported separately for future interventions.
Furthermore, based on the meeting held with community health workers and health servicesproviders as well as with Education department workers (School Teachers and Headmasters) insidethe community, gaps and needs of these important sectors also has been identified and concluded inthe assessment report’s relevant sections.
2. Coordination:International Medical Corps believes in coordination and always struggles to establish goodcoordination with all key stakeholders at all levels. During the Assessment, International MedicalCorps met with key stakeholder such as DoPH, DoRR, DGs, BPHs and EPHS implementer NGOs, MRRD,MoPH and other WASH related actors in the targeted areas. International Medical Corps informedthem about the Assessment and its purpose and sought their coordination during the assessmentand about the expected future project.
3. Training of Enumerators:For necessary data collection, International Medical Corps used the WASH cluster assessment toolsand conducted a one-day training session for the staff in the field. The training session on these toolswas facilitated by M&E officer, WASH Coordinators and project manager of WASH OFDA project. Theone day training in each province included practical works, a complete briefing session on needassessment particularly on conducting KII and FGD.
10 | P a g e
4. Ethical Consideration:The Survey teams took all ethical consideration into account and explained the purpose of theassessment to the target population. The teams were also given proper training on data collectionbefore conducting the field visit. The beneficiaries were informed prior to the field visit. After gettingtheir verbal consent of the beneficiaries, the survey teams visited their houses and filled thequestionnaire through conducting FGDs and KIIs.
5. Gender MainstreamingInternational Medical Corps always try to reach to the underserved and most vulnerable populationof the affected communities. It maintained gender balance in the Assessment as well as in the servicesprovision. International Medical Corps has strictly considered this point in the Assessment and hastaken below steps:
The assessment has been conducted by the local male and female surveyors. FGDs and KIIs both has been planned and conducted with all communities including male, female,
youth and disabled. Schools and HFs has been included in the assessment to find out the current status of WASH and
other hygienic aspects.
6. Questionnaires and Assessment Tools:International Medical Corps adapted the Afghanistan WASH cluster assessment tools as the principledata collection tool for the assessment. The tools and questionnaire have been shared withInternational Medical Corps WASH Advisor for the review and update. The WASH Advisor at the HQreviewed the tools and for enrichment of data and assessment helpful comments and instruction hasbeen added to the assessment process and into the questionnaires.
MethodologyInternational Medical Corps opted for qualitative and quantitative methods to triangulate thecollected information through Key Informants Interviews (KIIs) and Focus Group Discussion (FGDs)methodologies and this is how the primary data has been collected from the field. Moreover, adetailed desk review was conducted to collect the secondary information through relevantassessments reports, IOM weekly and monthly updates, and reports, UNOCHA, UNHCR and otherresources.
Beside KIIs and FGDs, the teams were also trained on how to collect data during direct observation.It is worth mentioning here that there were multiple challenges limited the data collection processsuch as security, gender consideration, women’s participation or availability and others. However,fortunately, the team managed to reach out to all the groups which are the most vulnerable such aswomen, children and disabled.
Survey Limitations:International Medical Corps always utilize the best efforts to reach out to the un-covered areas interms of all services. Fact remains that most of the un-covered areas have been left unserved due toinsecurity in those areas. In Nangarhar province, in some areas of the 6 districts, the security situationwas not satisfactory and had negatively affected the Assessment. International Medical Corps hashowever, tried to maintain the gender and mainstreaming issues although it was hard to find womensurveyors for the Assessment. Women’s interest and participation in common activities, educationlevel among women, and family restriction among them mostly effect the activities where womenparticipation is a must .
11 | P a g e
Challenges faced in data collection:Un-availability of professional staff, low education level, women’s lower interest and participation inFGDs and KIIs, security and limited access to the most vulnerable areas were noticed as key challengesfaced by the surveyor during the data collection process.
VI -Data Collection Methods:1 Desk Review / Secondary Data Review:The Assessment team conducted a detailed desk review of all the available key documents, surveyreports, journals issued by DoRR, MRRD and UN agencies pertaining to respective districts of theprovince prior to holding the Assessment. The desk review provided the team with basic knowledgeof the current humanitarian situation, and plight of IDPs, returnees, school and hospitals.
2 Key Stakeholders Meeting:
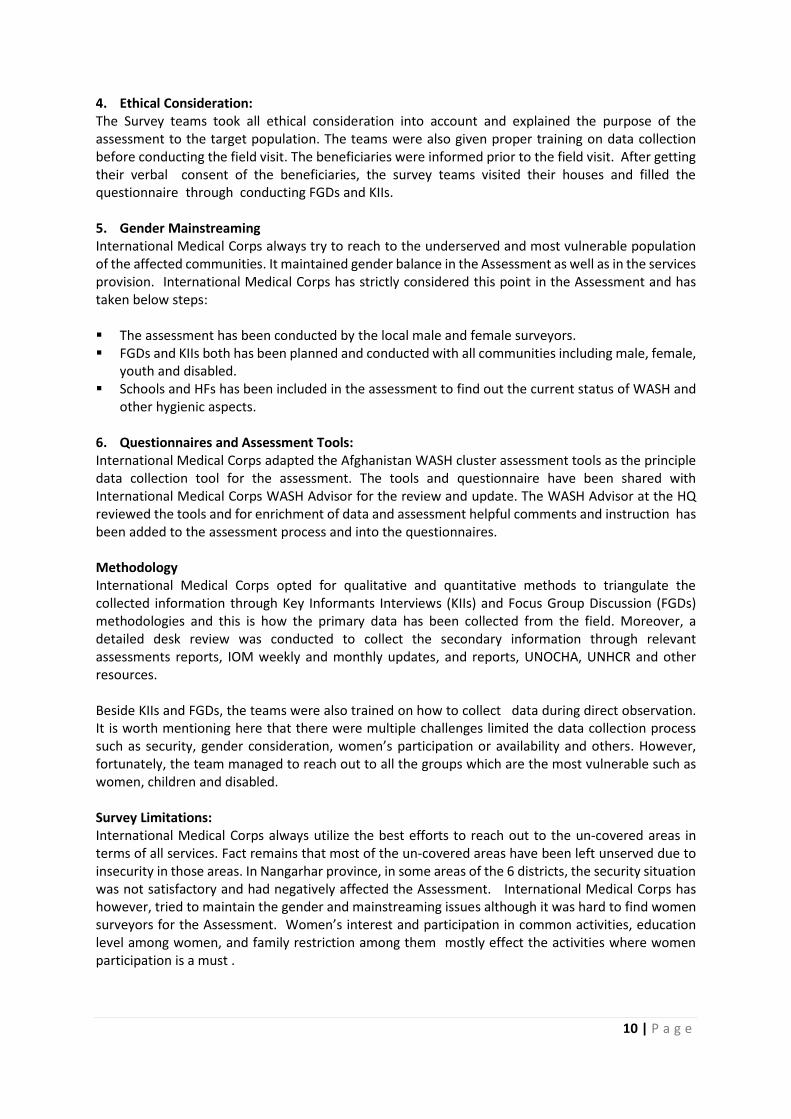
A proposed list of key stakeholders and main questions to be asked were shared with the team forreview and comments for finalization. A totalof 4 organizations/offices (8 persons) wereinterviewed mainly on gaps of services andcapacities in relation to WASH, Health andShelters. The key stakeholders includedrepresentatives of directorate of returneesand refugees (DoRR), Districts Governors(DGs), Representative of provincial Healthsector and representative of implementingNGOs for Basic Packages of Health Services.
3 Community Influential Meeting:The Assessment included, and was planned to have, a quick meeting with community influential whowere well aware about the geographical locations of returnees and IDPs, as well as about the currentsituation of the districts, security concerns, and local and community behaviors and believes.
4 Needs Assessment :
a) Key Informants Interviews (KIIs):The KIIs were conducted with community representatives and influential individuals of returnees,IDPs and host communities in various locations of the 10 districts (Goshta, Mohmand Dara, Rodat, BatiKotand and Behsud districts of Nangarhar, Mehterlam and Qargayi districts of Laghman provinceand Khas Kunar, Sarkani and Shegal districts of Kunar province). The questionnaires enabled the teamto collect both quantitative and qualitative information and data. The qualitative part of theassessment covered the type and magnitude of needs, challenges, access and quality of servicesavailable, while quantitative data included numbers and figures of IDPs, returnees and hostcommunities who have access to WASH (safe drinking water, hygienic latrines, and percentage offamilies using soap and practicing hand washing behaviour). Information collected from theAssessment will provide a broader picture that will inform us to design appropriate interventions forshort and medium term periods.(The details of Settlements covered by assessment are as follows):
12 12
3229
10
2
0
5
10
15
20
25
30
35
FGDs KII
Kunar
Nangarhar
Laghman
12 | P a g e
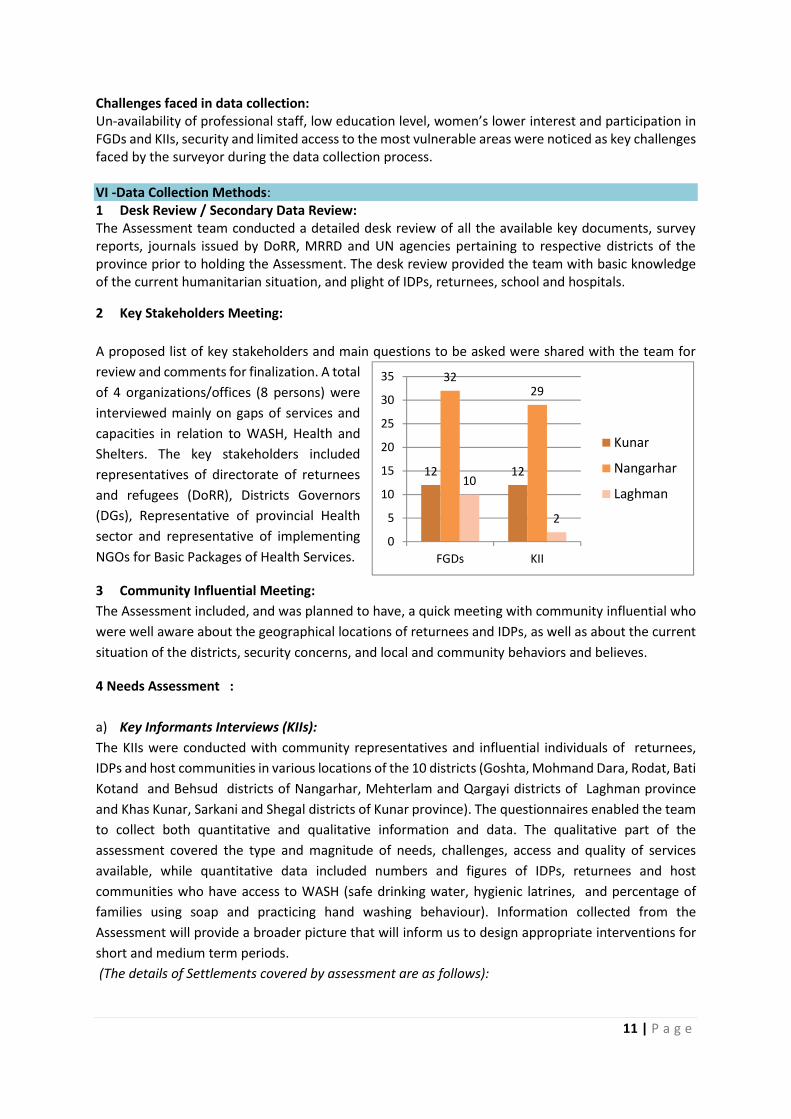
b) Focus Group Discussion (FGDs):
The FGDs were conducted with community elders, different local committee members, religiousleaders and influential community members considering gender and mainstreaming principles. FGDswere conducted with both male and female community members to collect broader informationabout WASH / Health and Shelters, personal hygiene issues in targeted areas. The sessions have beenconducted separately with females by female survey teams.
c) Direct Observations:Direct observation was a part of the survey and all groups were instructed to look around the areasthey visit and collect data and information. The teams were also instructed how to place the data intheir checklists or either to write the qualitative/quantitative information in separate papers andsubmit it to the survey supervisor. During the analysis, the data was properly analyzed and processedfrom direct observations as well and the information included in the report.
d) Daily Debriefing:Each day, after finishing field works, a daily debrief meeting was conducted with surveyors to discussall problems, challenges and constraints they faced in the field and in order to assure the validity ofcollected data. The meeting also discussed about next day’s plan and areas that were supposed to becovered by the teams.
District Province Villages / Sites # ofKIIs
#ofFGDs
Goshta
Nang
arha
r
Swro Ghoudi, Arkhy Dag, Khwezo, Aka BabaDaman, Mama Khail, Saifullah Jor, KhwezoDaman Dag,Khas goshta
8 8
Bati Kot Barikab, Qala e Awal, Barikab Ali Khail, BarikabMaktab Kaly, Barikab Raghah Kalay, Chahardi,Koz Kalay, Chahardi, Manz Kalay, Chahardi, LarKalay, Chahardi, Qala e Sar
8 7
Rodat Kuz Dag, Sachi Qala, Manz Kaly, Mirza Kaly, KozaQala , Roghani Loy Kaly, Roghani Manz Kaly
8 6
Mohmand Dara Hazar Nawo Hadizee, Gardi Ghous, Nawe Kaly,Gardi Ghous Kaly
4 4
Mulavi Khalis Families Site 1, Site 2, Site 3, Site 4 4 4
Khas Kunar
Kuna
r
Chandravi, Zargaran , Mangwal, Waly 4 4
Sarkani Dosaraka, Pashad, Tango, Sarkani Markaz 5 5
Shegal Mora Kaly, Shangar Shah, Morai kaly 3 3
Mehterlam
Lagh
man
Omerzaee, Katal Muskeen Abad, Deh Ziarat,Hajyaan Kaly
4 4
Qarghay Charbagh, Nawabad Qalatak Sulfa, Aziz khan kasreturnees camp, Aziz khan kas Farash ghani camp,Mandrawar, Suleiman Khel Nud Mara
6 6

13 | P a g e
e) Data Analysis and Reporting:Data collection, transcription and translation were planned to be completed each other day, and by28 March 2019 this process was completed by M&E department. For data analysis, a brief orientationof encoding procedures was provided by M&E department for the International Medical Corps teammembers in Jalalabad. The team developed a preliminary codes list for qualitative data analysis andfor qualitative data analysis the program Excel were used. Data for each code was summarized andexamined in any marked differences such as Sex, Age groups and Locations.
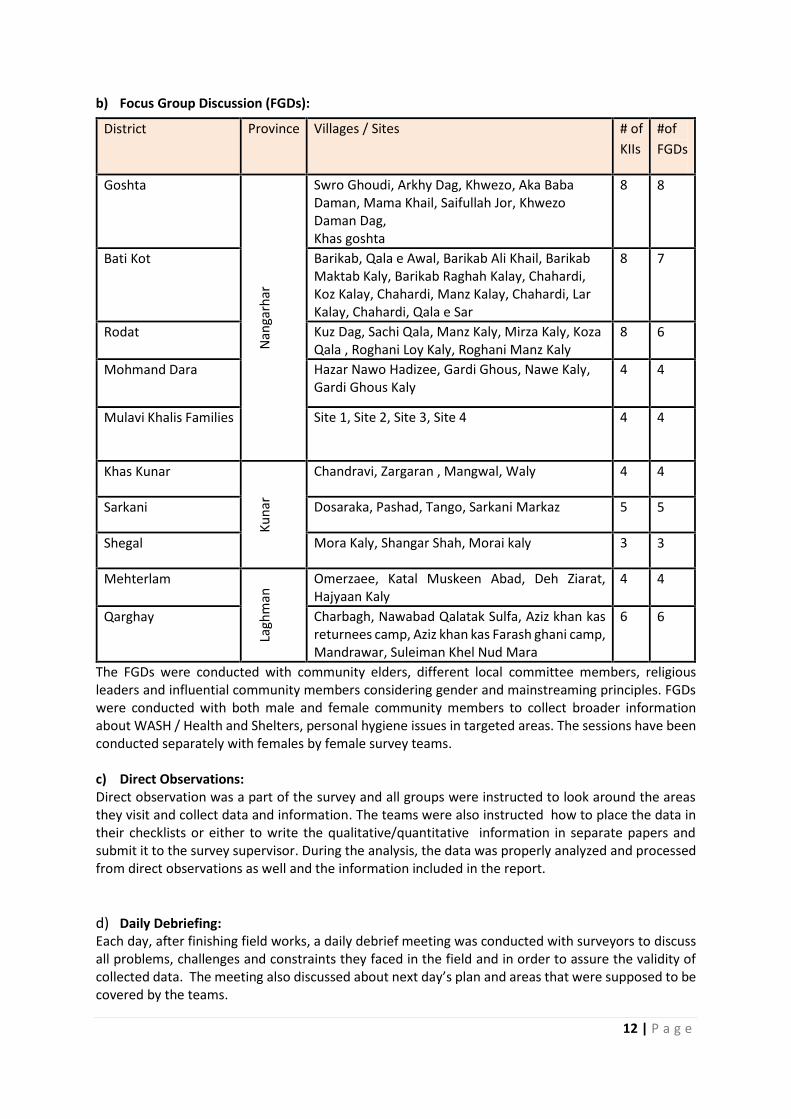
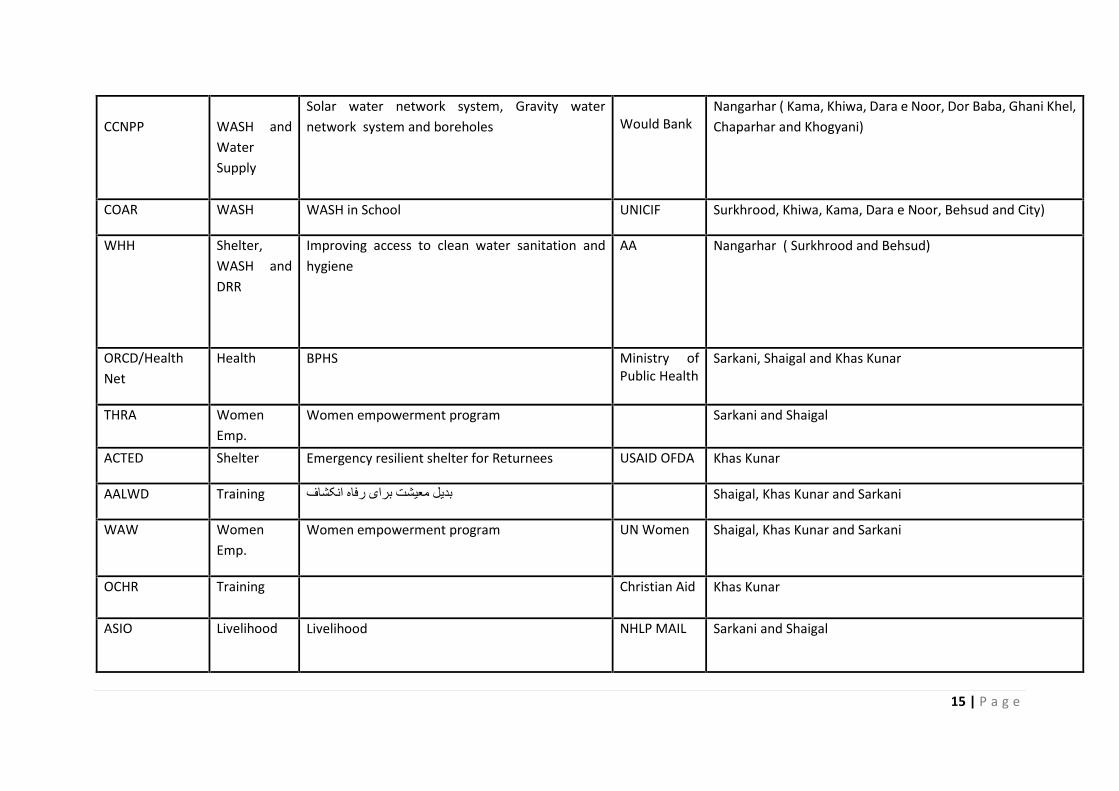
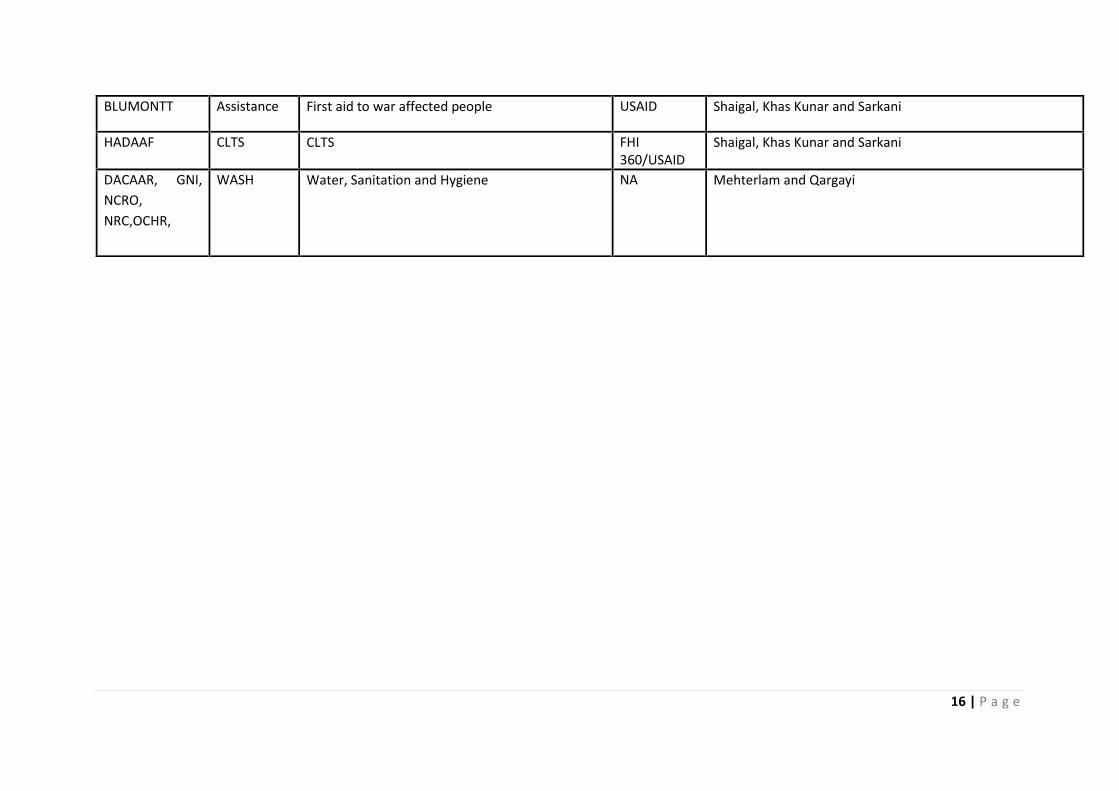
V: Stakeholder AnalysisInternational Medical Corps tried to avoid any duplication of activities and resource wasting andpromotes good coordination and cooperation with stakeholders. Therefore, a stakeholder analysiswas done by the team. Some key actors in the field were determined in all or some areas of thetargeted locations. Below Chart shows the key actors with their specific roles and interventions.
14 | P a g e
Organization Sectors Projects Donors District
InternationalMedical Corps
WASH-OFDA,WASHUNICIF,
Provision of Humanitarian WASH Assistance toAfghan Returnees, IDPs and Vulnerable LocalCommunities in Nangarhar and Kunar Provinces.
OFDA,UNICIF
Nangarhar ( Khiwa, Surkhrood, Pacher Wagram, Bati Kot,Rodat, Kot and Mohmandara)
ZOA WASH AFGR 2019 DRA Nangarhar ( Khogyani, Surkhrood and Kot)
NCRO WASH DRA- AFJR Pase 4 OXFOM Nangarhar ( Chaparhar, Khogyani, Behsud and Surkhrood)
UNHCR ReliefAssistanceto returneesand IDPs.
Provision of essential relief assistance to returneesmostly covering shelters and cash assistance.
UNHCR Nangarhar(all 22 districts of Nangarhar)and Kunar(in all 14districts of Kunar)
DACAAR WASHconstructionandEmergency
Emergency Response and Mechanism, WASHEmergency
. ECHO,DANIDA
Under ERM project DACAAR works in all 22 districts ofNangarhar Province and under Emergency WASH projectworks in Khiwa and Surkhrood districts.
AADA Health(BPHS)
Provision of primary/basic health services inNangarhar province.
MoPH andWorld Bank.
Nangarhar (in all 22 districts of Nangarhar)
15 | P a g e
CCNPP WASH andWaterSupply
Solar water network system, Gravity waternetwork system and boreholes Would Bank
Nangarhar ( Kama, Khiwa, Dara e Noor, Dor Baba, Ghani Khel,Chaparhar and Khogyani)
COAR WASH WASH in School UNICIF Surkhrood, Khiwa, Kama, Dara e Noor, Behsud and City)
WHH Shelter,WASH andDRR
Improving access to clean water sanitation andhygiene
AA Nangarhar ( Surkhrood and Behsud)
ORCD/HealthNet
Health BPHS Ministry ofPublic Health
Sarkani, Shaigal and Khas Kunar
THRA WomenEmp.
Women empowerment program Sarkani and Shaigal
ACTED Shelter Emergency resilient shelter for Returnees USAID OFDA Khas Kunar
AALWD Training بدیل معیشت برای رفاه انکشاف Shaigal, Khas Kunar and Sarkani
WAW WomenEmp.
Women empowerment program UN Women Shaigal, Khas Kunar and Sarkani
OCHR Training Christian Aid Khas Kunar
ASIO Livelihood Livelihood NHLP MAIL Sarkani and Shaigal
16 | P a g e
BLUMONTT Assistance First aid to war affected people USAID Shaigal, Khas Kunar and Sarkani
HADAAF CLTS CLTS FHI360/USAID
Shaigal, Khas Kunar and Sarkani
DACAAR, GNI,NCRO,NRC,OCHR,
WASH Water, Sanitation and Hygiene NA Mehterlam and Qargayi

17 | P a g e
VII: MAIN FINDINGSGeneral Observation:
The targeted 11 districts are close to the capital cities of Jalalabad, Mehterlam and Asadabad in eachof the province, as well as having easy access to other districts as well. Locally constructed marketsare available in each district. The capital cities Jalalabad of Nangarhar and Asadabad of Kunar havebigger markets and livelihood opportunities to some extent and the Assessment revealed that someof the affected population are working on daily wages in Jalalabad, Mehterlam and Asadabad withmonthly income of around 5,000 to 8,000 AFGs (USD 80-125).
Potable Water:Limited access to potable water considered the main problem of the households. The Assessmentrevealed that in 49.4% people in Rodat, 63.2% in Bati Kot, 43.1% people in Mulavi Khalis Families,39.11% people in Mohmand Dara district, 59.12% people in Goshta, 39% people in Mehterlam, 44.12%people in Qargayi, 59.7% in Khas Kunar, 55.3% people in Sarkani and 44.5% people in Shegal districthave no access to safe potable drinking water. However, some INGOs have already worked in someplanned returnee settlements like Shikhmisry, Chamtala but could not full-fill the needs of potablewater of majority of these people as most of these returnees also have been settled inside hostcommunities where the percentage of this indicators falls down significantly.
On the other hand, there are already exisiting boreholes reported to be not-functional due to lack ofgood maintenance systems in place. Based on the Assessment report, about 58% of these populationstated that they have to walk around 15-30 minutes to reach to the water points, while in some areas,particularly in Bati Kot, Goshta and Rodat of Nangarhar, this time is even more than an hour, andpeople are using water tankers to fulfil their needs for potable water. People frequently complainsabout lining up for at water points for long hours and 44% of them stated that they normally waitfor more than 30 minutes to collect water, while 37% of them are used to wait for 15 to 30 minutesat water collecting points.
Women are mostly doing the house-hold chores as their gender and socially routine assigned tasks,while water collecting responsibility is also being given to them in almost all areas. This indeed putextra burden on women and girls while they are exposed to risk of harassment. Also, the Assessmentrevealed that average need of water per person per day is around 20 litters, while the FGDsparticipants also pointed out that the average daily usage of water per person increases significantlyin hot weather during summer season.
Sanitation and Hygiene:Overall the poor condition of hygiene and sanitation revealed, one of the main causes of increasedwater borne diseases among these needy communities. The assessment revealed that most of thesepopulation have very limited or no information about safe hygiene and sanitation practices and on theother hand limited access to hygienic latrines and other sanitation facilities keep the population awayfrom safe hygiene practices. Although, in most mentioned locations, CLTS program has beenimplemented but the result were not satisfactory at the field level. In Rodat district, there are numberof families who constructed latrines for themselves and most of these latrines have been builtprivately by individuals. Point to note here that only those families who have built the latrines haveaccess to it. Assessment report revealed that there are hundreds of families that have 3-5 latrinesinside one house and also families were reported who used open defecation practices due to lack ofsimple vaults.
18 | P a g e
As per the Assessment, open defecation is commonly practiced among these communities. About 44%of the assessed families either were using unhygienic sanitation facilities or go for open deificationand 17% did not have any latrine at home. The male members of these families practiced opendefecation, while the female members used latrines at the neighbouring homes. Only 37% of thispopulation were using improved sanitation facilities.
The Assessment team identified the higher need for provision of safe and hygienic sanitation facilities(latrine) as the most urgent need of the returnees to avoid open defecation and, on the other hand,to control water born or communicable diseases among children and women.
Gender balance has been maintained zero in almost all the locations and none of these facilities wereseparately constructed for females. Access to flush and septic latrines reported below 2% in bothdistricts (less than 30% of families in above listed location of Nangarhar province). About 43% offamilies in mentioned location of Laghman province were using soaps during hand washing practicein most critical times, 10% of families received a hygiene kit during last one year in listed villages ofNangarhar province while less than 10% received it in Laghman and 0% in Kunar province. It is worthmentioning here that large numbers of these families have been newly arrived and settled in the areasand did not receive any assistance from any organization. Less than 20% people knew about how tokeep and prepare food safely in all districts and 80-90% of families have limited access to bathrooms.
Open defection practices were more common particularly among those returnees who are settledinside local communities and villages. During the assessment, the team identified that functioninglatrines and water sources were available in the schools and health facilities in the targeted areas. Thehealth facilities are having proper hand washing facilities, while handwashing facilities and practiceof handwashing reported as one of the urgent needs among schools.
Hygiene PromotionAccess to health facilities and hygiene promotion sessions revealed to be not satisfactory. Accordingto interviews with community health workers, the new returnees plus IDPs are an extra burden oncurrent health services and facilities. Returnees are either interested to stay inside the secured areasof these 11 districts (Khas Kunar, Sarkani, Shegal in Kunar, Bati Kot, Rodat, Mohmand Dara, MulaviKhalis Families, goshta in Nangarhar & Mehterlam and Qargayi districts in Laghman province) or inplanned camps such as (Shikhmisry and Chamtala in Nangarhar, Aziz khan kas in Laghman and KhasKunar camp in Khas Kunar), it is mentionable that in some planned camps the government and BPHSimplementing NGOs established fixed and mobile health facilities for them. However, those who havebeen settled inside the villages with host communities have no fixed or mobile health services andonly have hard access to those HFs and services which are designed only for a particular population ofhost communities and this puts an extra burden on them.
The Assessment reported that around 34 different types of HFs located in different location of thesedistricts with having around 311 technical staff including Medical Doctors, Nurses, Midwives andothers while 340 of them will be targeted in the project. Hygiene Promotion activities seemed to bein poor condition. None of the areas has taken these campaigns.
Over all knowledge regarding WASH, personal and environmental hygiene and hygiene promotionnoticed to be in a very lower level among the inhabitants of the camps, settlements, school andhospitals. Hand washing practice and other initial hygiene promotion activities were not practicing bythe majority of the population.
19 | P a g e
Environmental Health:Observations and qualitative data of the Assessment informed us that safe environmental hygienepractices among these communities is a major environmental health issue. Proper solid wastemanagement system is reported to be a common problem inside these communities and no properwaste collection system is in place. Families are mostly collecting their wastes individually and puttingit in an area which is called dumps.
Refuse pits, safe collection system or any other safe practice or system do not exist, thus, they needto be paid a special attention to prevent communicable and other infectious diseases in children andwomen. Moreover, none of these areas have any constructed canalization system for draining wastedwater, but still families have solved the issue individually for their houses and the spoiled water iseither washed or drained by rain water.
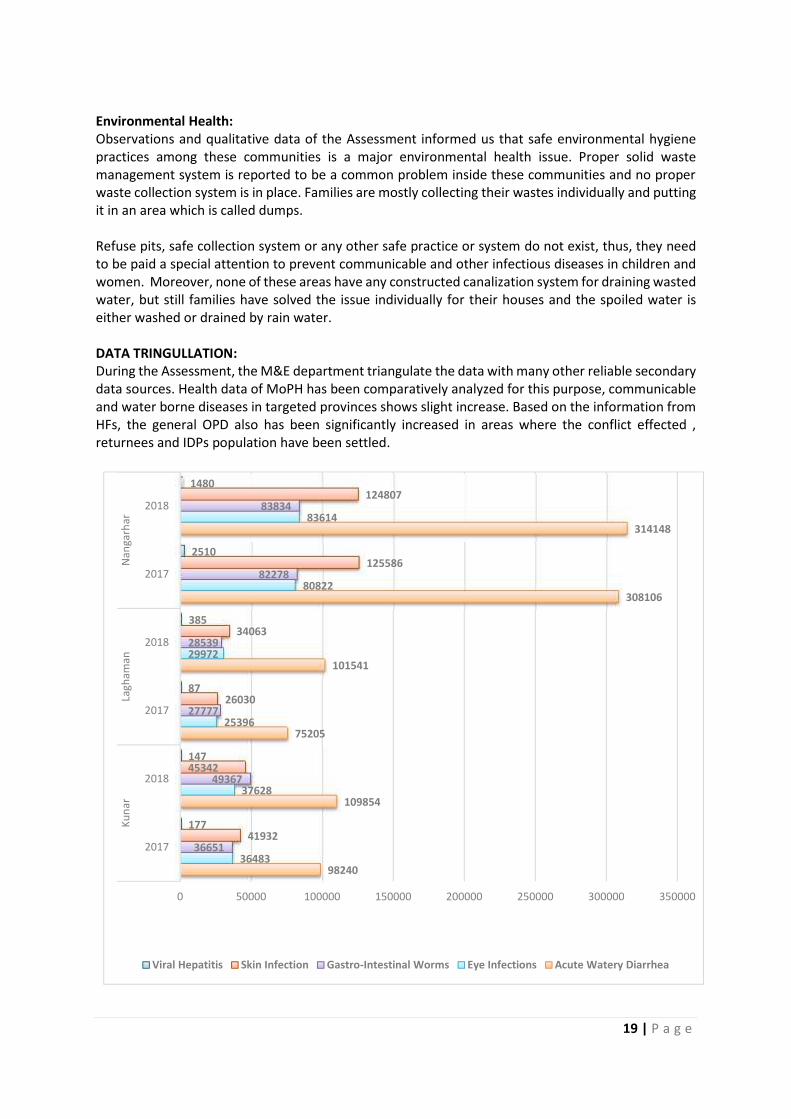
DATA TRINGULLATION:During the Assessment, the M&E department triangulate the data with many other reliable secondarydata sources. Health data of MoPH has been comparatively analyzed for this purpose, communicableand water borne diseases in targeted provinces shows slight increase. Based on the information fromHFs, the general OPD also has been significantly increased in areas where the conflict effected ,returnees and IDPs population have been settled.
HMIS Data of MoPH in three Provinces (Kunar, Laghman, Nangarhar)98240
109854
75205
101541
308106
314148
36483
37628
25396
29972
80822
83614
36651
49367
27777
28539
82278
83834
41932
45342
26030
34063
125586
124807
177
147
87
385
2510
1480
0 50000 100000 150000 200000 250000 300000 350000
2017
2018
2017
2018
2017
2018
Kuna
rLa
gham
anNa
ngar
har
Viral Hepatitis Skin Infection Gastro-Intestinal Worms Eye Infections Acute Watery Diarrhea
20 | P a g e
BENIFICIARIES TO BE TARGETED:Beneficiaries: Direct beneficiaries (returnees, IDPs and vulnerable local communities): 667,100individuals (95,300 families), 346,892 male and 320,208 female and plus 30 schools the targetedareas. Indirect beneficiaries (surrounding communities): 178,622 individuals (25,517 families).
RECOMMENDATIONS:
Water Supply Infrastructure:Improve access to sufficient quantity of safe drinking water by the returnees, IDPs and vulnerablelocal population.
Proposed activities: Development of new water sources (drilling of boreholes), equipped with hand pumps, for IDPs,
returnees and the local communities. Construction of water supply networks generated by solar systems. The Water Point sitting will be inclusive of consultative process and will consider the voices of
women, as per gender roles they are the primary beneficiary to fulfill the domestic and personalwater needs at household level thus, ensuring that they feel safe and comfortable to fetch thewater.
Ensure the maintenance and sustainability of hand pumps through trainings and tools distribution. Water quality analysis and disinfection of water systems to maintain the required FRC at all times.
Sanitation Infrastructure:Improve access to adequate and gender sensitive sanitation for the returnees, IDPs and vulnerable localpopulation.
Proposed activities: Construction of Ventilated Improved Pit (VIP) Latrines for eligible returnees and IDPs families. Distribution of latrine kits to the selected latrine beneficiaries. Installation of hand washing facilities in schools in the targeted areas. Construction of safe drinking water systems in targeted schools. Excreta management (vector breeding & awareness to the targeted families on proper disposal of
excreta).
Hygiene Promotion:Reduce the risks associated with unhygienic practices and conditions by the returnees, IDPs and localpopulation.
Proposed activities: Baseline and final KAP Survey to benchmark the interventions and to know the knowledge on
WASH. Hygiene promotion at household level through female IMC Hygiene Promoters (HPs). Training Community Hygiene Promoters (CHPs), and health and school staff on key health, hygiene
and sanitation topics. Distribution of Water Kits (jerry cans) to the selected households. Community meetings and awareness sessions in communal areas (mosques, public gatherings,
schools). Formation & capacity building of gender sensitive WASH committees in the targeted areas (19
villages).
21 | P a g e
Environmental Health:Ensure the collection and safe disposal of domestic waste in targeted areas in Nangarhar and KunarProvinces in collaboration with the relevant stake-holders.
Proposed activities: Design and implementation of the solid waste disposal programs in targeted areas. Ensure that household waste is disposed of into containers for regular collection - to be burned or
buried in specified disposal pits, being identified by the community. Organize six-monthly solid waste clean-up campaigns at village/school levels to encourage the
returnees, IDPs and schools to remove solid waste from the settlements/schools before itbecomes a health risk.
Distribution of IEC materials. Construction of garbage centers on community level.
22 | P a g e
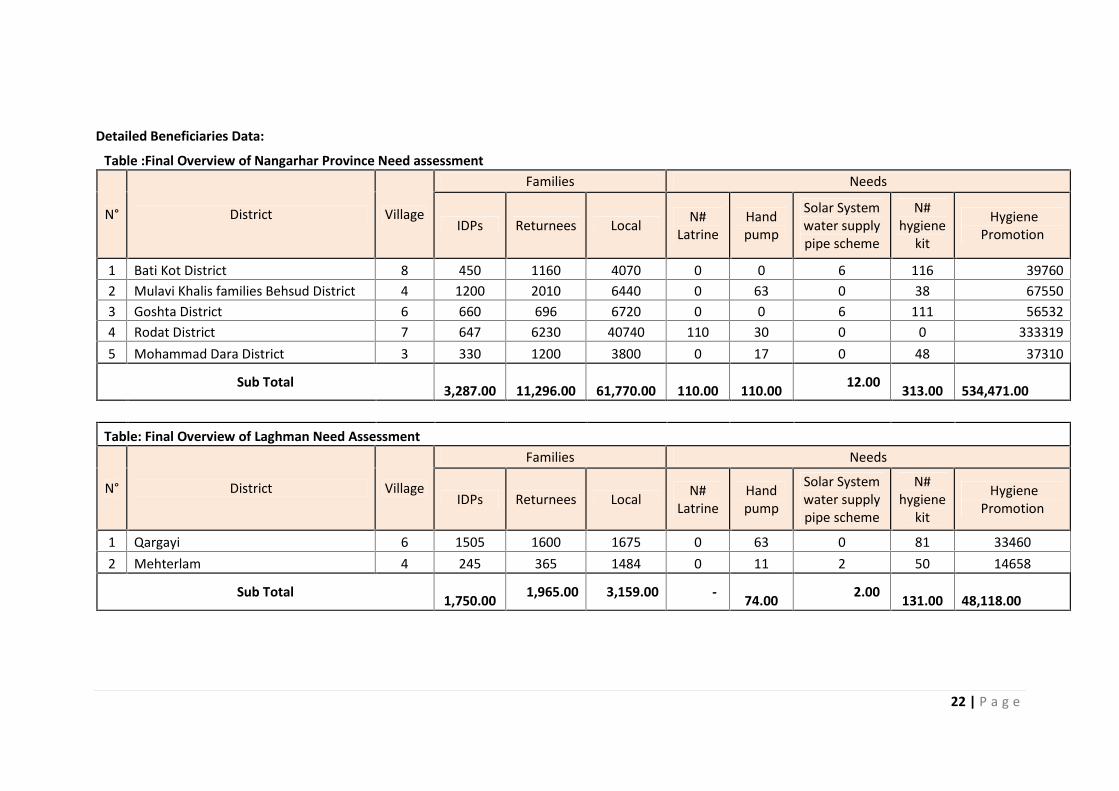
Detailed Beneficiaries Data:Table :Final Overview of Nangarhar Province Need assessment
N° District Village
Families Needs
IDPs Returnees Local N#Latrine
Handpump
Solar Systemwater supplypipe scheme
N#hygiene
kit
HygienePromotion
1 Bati Kot District 8 450 1160 4070 0 0 6 116 397602 Mulavi Khalis families Behsud District 4 1200 2010 6440 0 63 0 38 675503 Goshta District 6 660 696 6720 0 0 6 111 565324 Rodat District 7 647 6230 40740 110 30 0 0 3333195 Mohammad Dara District 3 330 1200 3800 0 17 0 48 37310
Sub Total 3,287.00 11,296.00 61,770.00 110.00 110.00 12.00 313.00 534,471.00
Table: Final Overview of Laghman Need Assessment
N° District Village
Families Needs
IDPs Returnees Local N#Latrine
Handpump
Solar Systemwater supplypipe scheme
N#hygiene
kit
HygienePromotion
1 Qargayi 6 1505 1600 1675 0 63 0 81 334602 Mehterlam 4 245 365 1484 0 11 2 50 14658
Sub Total 1,750.00 1,965.00 3,159.00 - 74.00 2.00 131.00 48,118.00
23 | P a g e
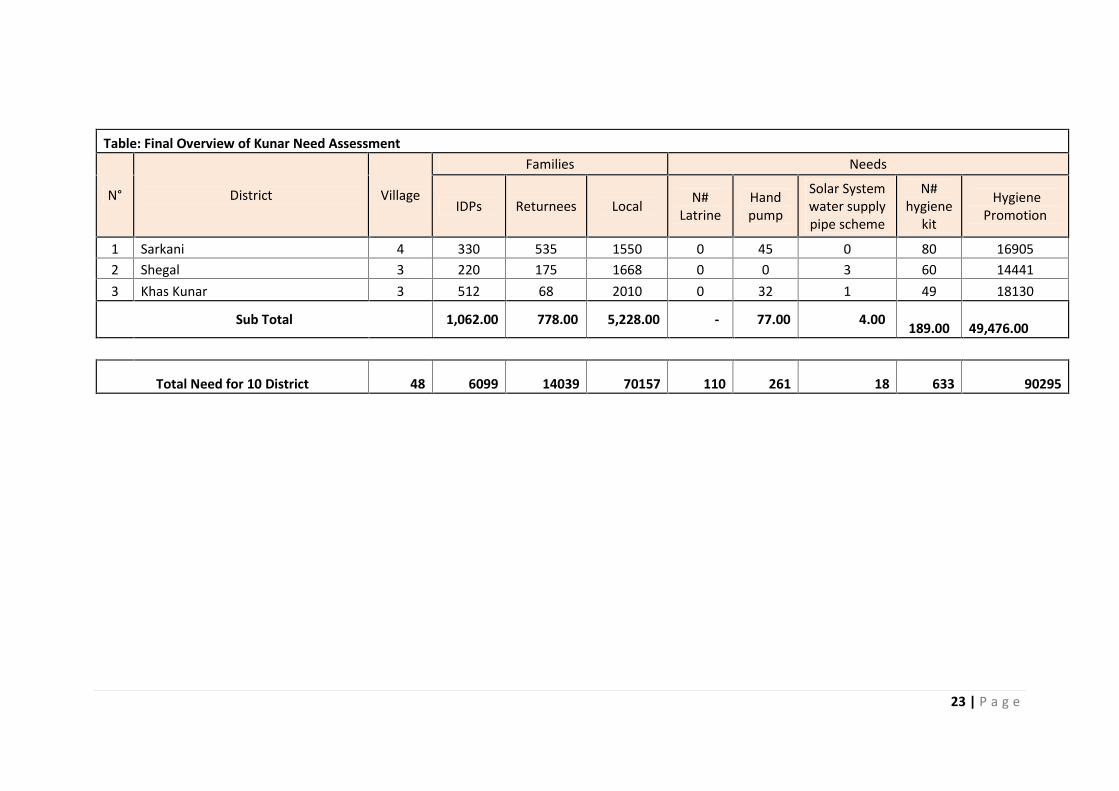
Table: Final Overview of Kunar Need Assessment
N° District Village
Families Needs
IDPs Returnees Local N#Latrine
Handpump
Solar Systemwater supplypipe scheme
N#hygiene
kit
HygienePromotion
1 Sarkani 4 330 535 1550 0 45 0 80 169052 Shegal 3 220 175 1668 0 0 3 60 144413 Khas Kunar 3 512 68 2010 0 32 1 49 18130
Sub Total 1,062.00 778.00 5,228.00 - 77.00 4.00 189.00 49,476.00
Total Need for 10 District 48 6099 14039 70157 110 261 18 633 90295
24 | P a g e
WASH Rapid Assessment Questionaire
25 | P a g e
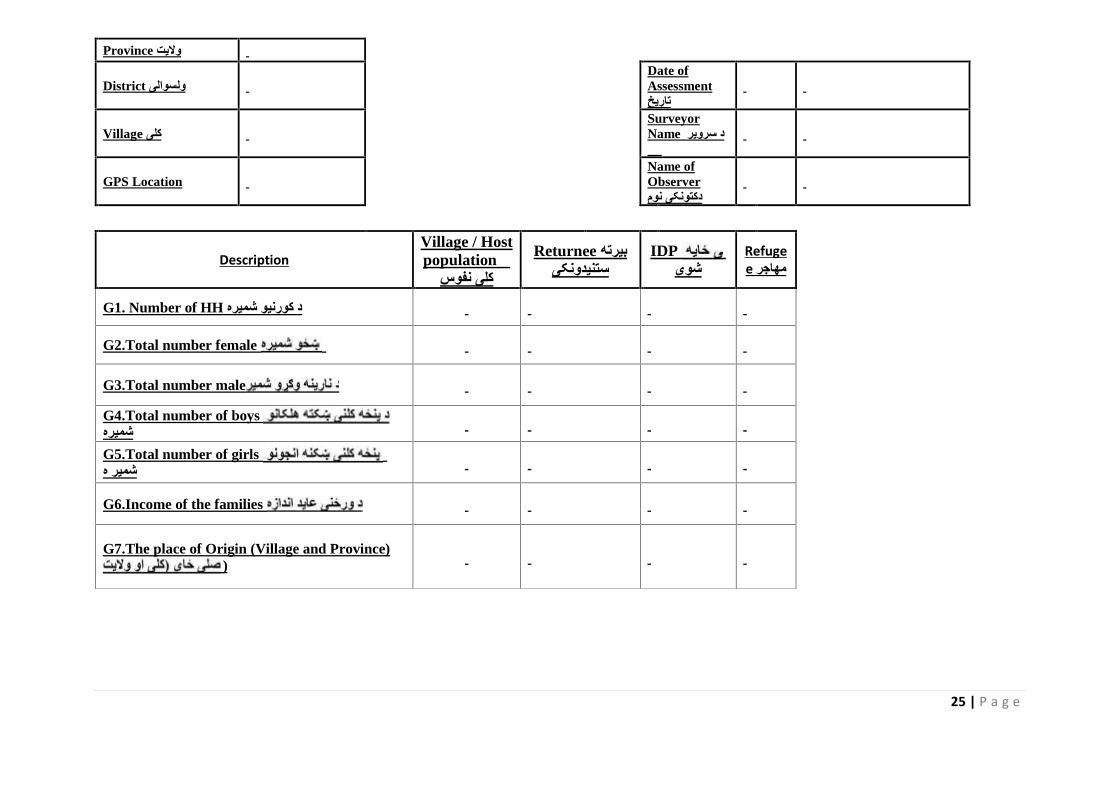
Province والیت
District ولسوالیDate ofAssessmentتاریخ
Village کلیSurveyorName د سرویر نوم
GPS LocationName ofObserverدکتونکی نوم
DescriptionVillage / Hostpopulation د
کلی نفوسReturnee بیرتھ
ستنیدونکیIDP
شویRefugee مھاجر
G1. Number of HH د کورنیو شمیره
G2.Total number female
G3.Total number male
G4.Total number of boysشمیرهG5.Total number of girlsشمیر ه
G6.Income of the families
G7.The place of Origin (Village and Province))
26 | P a g e
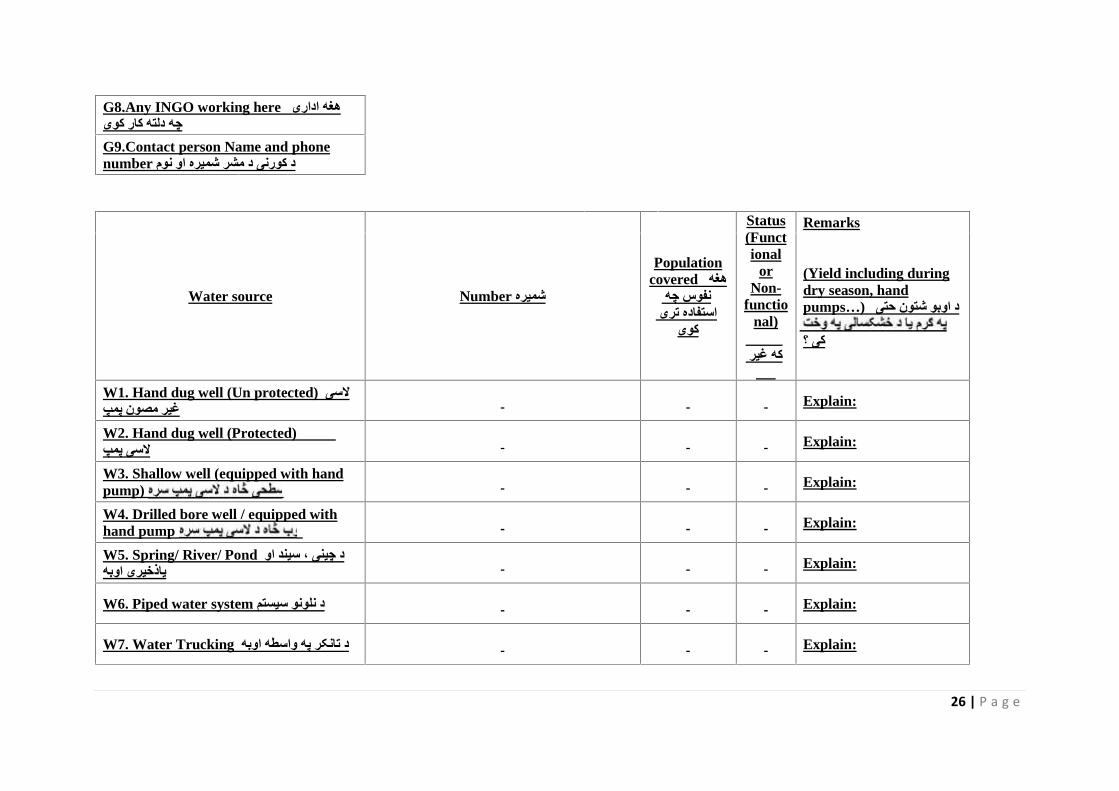
G8.Any INGO working here ھغھ اداری چھ دلتھ کار کویG9.Contact person Name and phonenumber د کورنی د مشر شمیره او نوم
Water source Number شمیره
Populationcovered ھغھ
نفوس چھ استفاده تری
کوی
Status(Functional
orNon-
functional)
فعال ده کھ غیر
فعال
Remarks
(Yield including duringdry season, handpumps…) د اوبو شتون حتی
کی ؟
W1. Hand dug well (Un protected) السی غیر مصون پمپ Explain:
W2. Hand dug well (Protected) مصون السی پمپ Explain:
W3. Shallow well (equipped with handpump) Explain:
W4. Drilled bore well / equipped withhand pump Explain:
W5. Spring/ River/ Pond د چینی ، سیند او یاذخیری اوبھ Explain:
W6. Piped water system د نلونو سیستم Explain:
W7. Water Trucking د تانکر پھ واسطھ اوبھ Explain:
27 | P a g e
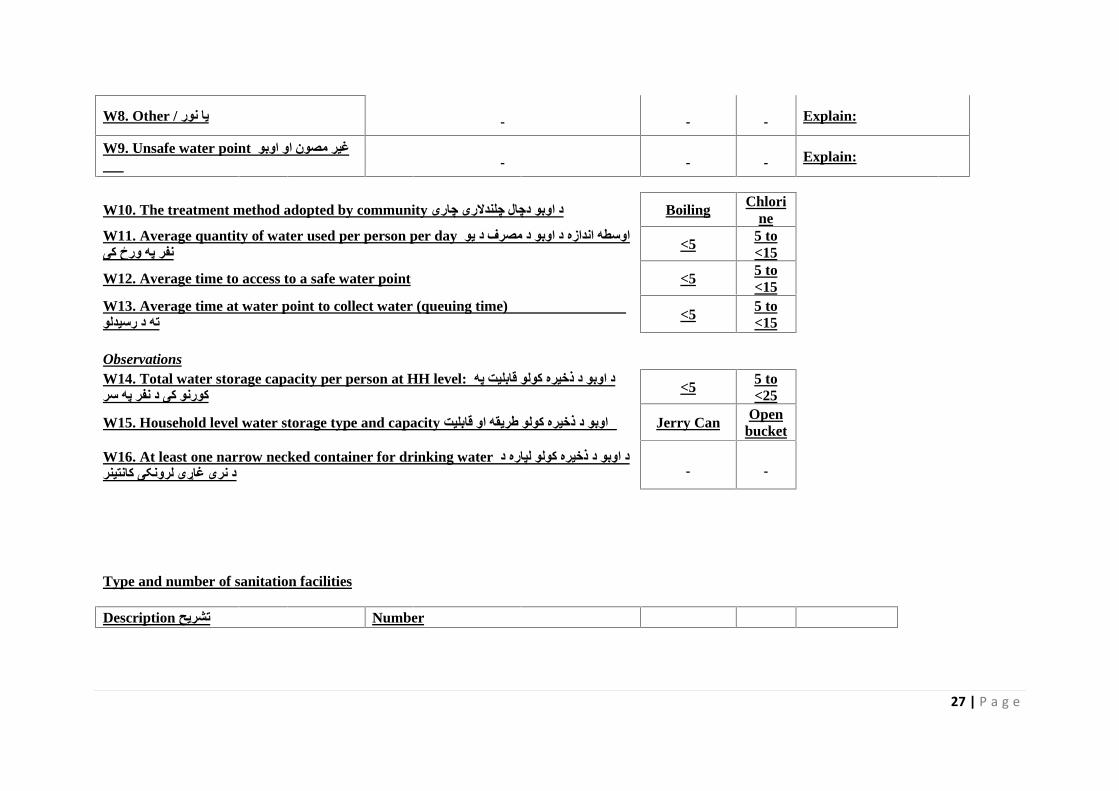
W8. Other / یا نور Explain:
W9. Unsafe water point غیر مصون او اوبو منبع Explain:
W10. The treatment method adopted by community د اوبو دچال چلندالری چاری Boiling Chlorine
W11. Average quantity of water used per person per day اوسطھ اندازه د اوبو د مصرف د یو نفر پھ ورځ کی <5 5 to
<15
W12. Average time to access to a safe water point <5 5 to<15
W13. Average time at water point to collect water (queuing time) اوسط وخت د اوبو منبع تھ د رسیدلو <5 5 to
<15
ObservationsW14. Total water storage capacity per person at HH level: د اوبو د ذخیره کولو قابلیت پھ کورنو کی د نفر پھ سر <5 5 to
<25
W15. Household level water storage type and capacity د اوبو د ذخیره کولو طریقھ او قابلیت Jerry Can Openbucket
W16. At least one narrow necked container for drinking water د اوبو د ذخیره کولو لپاره د د نری غاړی لرونکی کانتینر
Type and number of sanitation facilities
Description تشریح Number
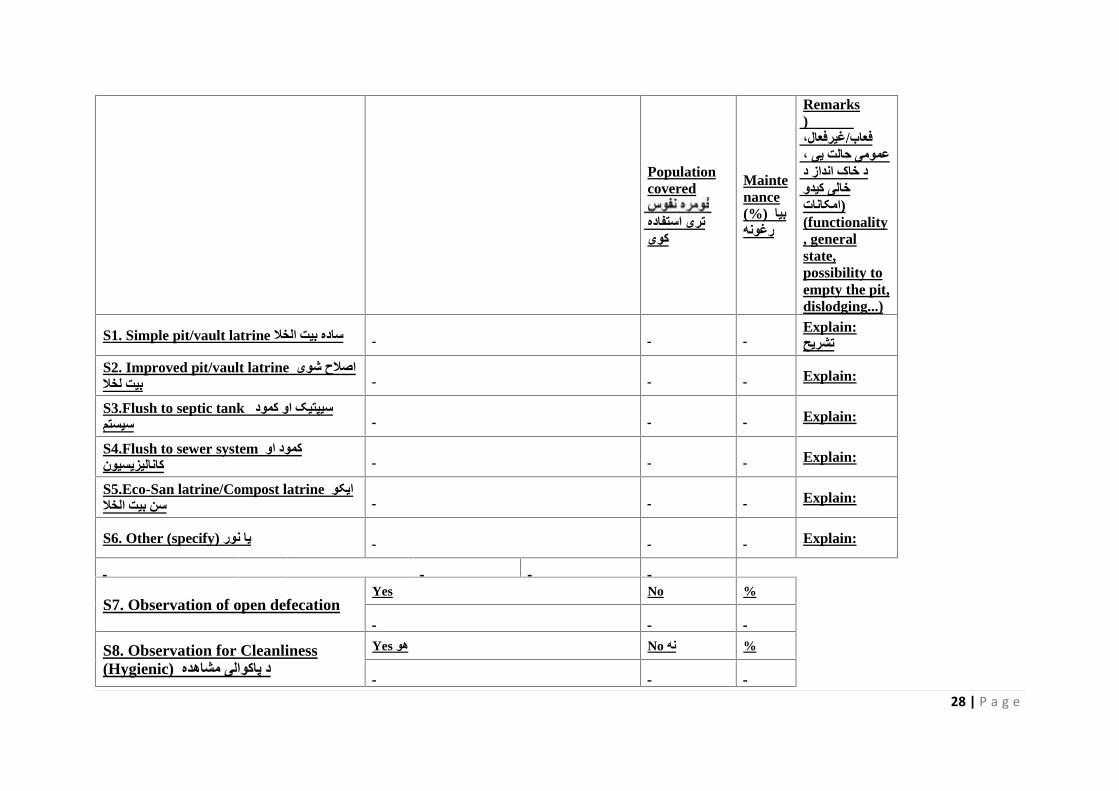
28 | P a g e
Populationcovered
تری استفاده کوی
Maintenance(%) بیا رغونھ
Remarksمالحظات (
فعاب/غیرفعال، عمومی حالت یی ، د خاک انداز د خالی کیدو (امکانات(functionality, generalstate,possibility toempty the pit,dislodging...)
S1. Simple pit/vault latrine ساده بیت الخال Explain:تشریح
S2. Improved pit/vault latrine اصالح شوی بیت لخال Explain:
S3.Flush to septic tank سیپتیک او کمود سیستم Explain:
S4.Flush to sewer system کمود او کانالیزیسیون Explain:
S5.Eco-San latrine/Compost latrine ایکو سن بیت الخال Explain:
S6. Other (specify) یا نور Explain:
S7. Observation of open defecationYes No %
S8. Observation for Cleanliness(Hygienic) د پاکوالی مشاھده
Yes ھو No نھ %
29 | P a g e
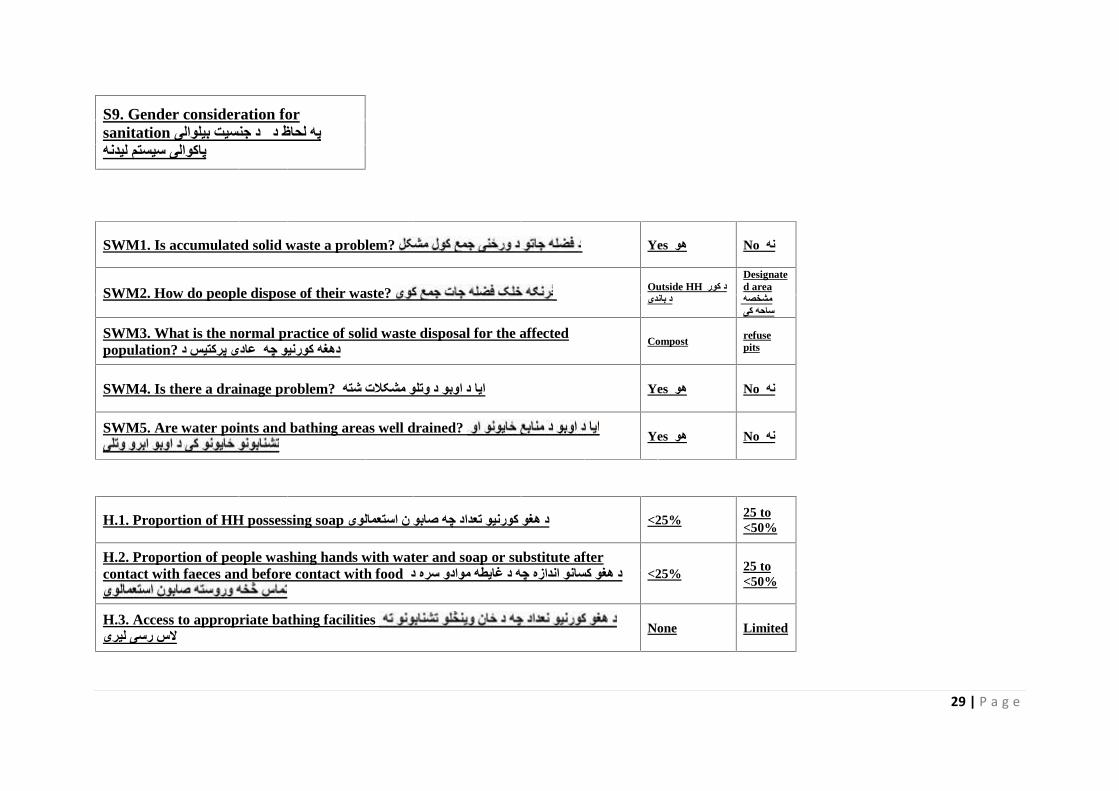
S9. Gender consideration forsanitation د جنسیت بیلوالی پھ لحاظ د پاکوالی سیستم لیدنھ
SWM1. Is accumulated solid waste a problem? Yes ھو No نھ
SWM2. How do people dispose of their waste? Outside HH د کور د باندی
Designated areaمشخصھ ساحھ کی
SWM3. What is the normal practice of solid waste disposal for the affectedpopulation? عادی پرکتیس د دھغھ کورنیو چھ Compost refuse
pits
SWM4. Is there a drainage problem? ایا د اوبو د وتلو مشکالت شتھ Yes ھو No نھ
SWM5. Are water points and bathing areas well drained? Yes ھو No نھ
H.1. Proportion of HH possessing soap د ھغو کورنیو تعداد چھ صابو ن استعمالوی <25% 25 to<50%
H.2. Proportion of people washing hands with water and soap or substitute aftercontact with faeces and before contact with food د ھغو کسانو اندازه چھ د غایطھ موادو سره د <25% 25 to
<50%
H.3. Access to appropriate bathing facilitiesالس رسی لیری None Limited
30 | P a g e
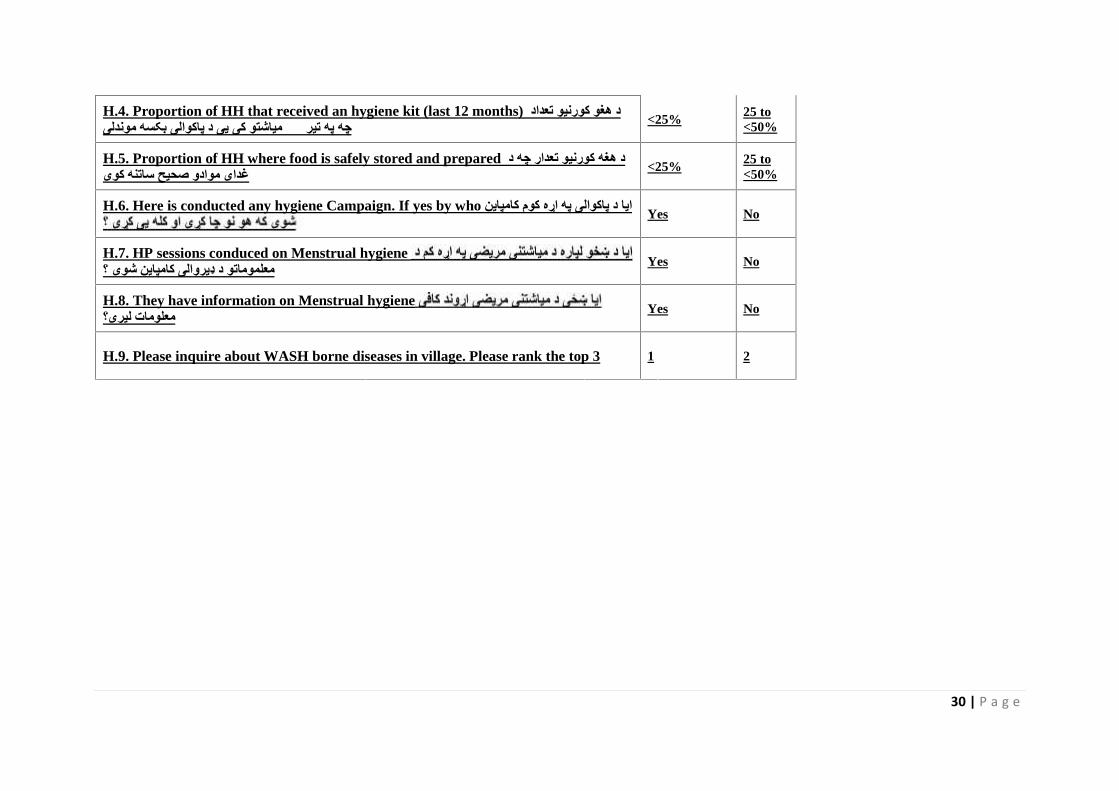
H.4. Proportion of HH that received an hygiene kit (last 12 months) د ھغو کورنیو تعداد میاشتو کی یی د پاکوالی بکسھ موندلی چھ پھ تیر ١٢ <25% 25 to
<50%
H.5. Proportion of HH where food is safely stored and prepared د ھغھ کورنیو تعدار چھ د غدای موادو صحیح ساتنھ کوی <25% 25 to
<50%
H.6. Here is conducted any hygiene Campaign. If yes by who ایا د پاکوالی پھ اړه کوم کامپاین Yes No
H.7. HP sessions conduced on Menstrual hygieneمعلموماتو د ډیروالی کامپاین شوی ؟ Yes No
H.8. They have information on Menstrual hygieneمعلومات لیری؟ Yes No
H.9. Please inquire about WASH borne diseases in village. Please rank the top 3 1 2





























