Embed Size (px)
Citation preview
I-~F,,,,,---I~ FT I i < . , ~ ~ e N w c . 15
I yd /"i- ? ""
FE ~ ' , f J F t r j C c r]Ok, t ,,.J * . ~ [ j . - <
~ 0 . i + L C A N I B w
" 9" . , t J t , ',.- :; <I , , , $d A ,.;* . i i ; H 4 i
* * * " -v ?P-".I"...- -..- - 2..
.b--. *=, -
SEMINAR ON THE PREVENTION OF
MAJOR CARDIOVASCULAR DISEASES
TEHERAN. 1 0 - 18 DECEMBER 1972
WORLD HEALTH ORGANIZATION EASTERN MEDITERRANEAN REGION
ALEXANDRIA
WORLD HEALTH ORGANIZATION Regional Office for the Eastern Mediterranean
EM/~ard.Vasc ./5 E?:\~/PRV.W. CARD. VSC . D I S / ~ ~ EMRO 8202 (0142)
May 1973
ON TKE SEMINAR ON THE PRFVENTION OF MAJOR CARDIOVASCULAR DISEASES
Teheran, 10 - 16 D c c e m b e r 1972
The views expressed i n t h i s Report do not necessa r i ly r e f l e c t the o f f i c i a l policy of t h e World Hea.lth 0rganiza. t ion.
This document ha,s been prepa,red by t h e WE0 Regional Of f i ce f o r t h e &s te rn Mediterranean f o r Governments of Member S t a t e s i n t h e Region and f o r those who p a r t i c i p a t e d i n t h e Seminar. A l i m i t e d nurnber of copies is a.va.ilable on request f o r persons o f f i c i a . 1 1 ~ o r p ro fess iona l ly coficcrned w i t h the P r e v e n t i u r l US Ma.jora Ca.rdlova,scula.r Disea,seS.

Participants and Observers who attended the Seminar on the Prevention of Major Cardiovascular Diseases
Held in Teheran from 10 - 16 December 1972

WHO Em0
T A m OF CONTENTS
W ~ a r d . Vasc ./5 Efrl/PRV. I'4J . CARD ,VSC , D I S / ~ ~ page i
I1 RHEUMATIC FEVER
1. Background 2. Current a c t i v i t i e s i n the Region 3. Guidelines f o r control
3.1 Prevention 3.2 Treatment and management
4. Recommendations
111 HYPERTENSION
1. Background 2. Si tuat ion i n the Region 3 . Guidelines f o r control
3.1 Diagnosis 3.2 Management and therapy 3.3 Control of hypertension i n communltles
4. Recommendations
IV ISCHAEMIC HEART DISEASE
1. Background
1.1 Prevalence 1.2 Etiology 1.3 Epidemiology 1.4 Clinical features
2. The s i tua t ion i n the Region 3. Treatment and Rehabili tation
3.1 Emergency care 3.2 Coronary care un i t s (CLV) 3.3 Rehabili tation and secondary prevention 7.4 Medical versus surgical treatment
4. Prevention 5. Recommendations
5.1 Intensive care 5.2 Rehabili tation 5.3 Prevention
Page
1
EM/~ard .Vzsc ./5 EM/pRV,MJ. CARD. vsc . D I S / ~ ~ page ii
V CONCLUSIONS AND RECOMMETUTIONS
WHO m o
Page
25
A N N M I AGENDA
ANNM I1 LIST O F PARTICIPANTS
ANNEX 111 CARDIOVASCULAR DISEASES I N COUNTRIES OF THE REGION
ANNM IV RHEUMATIC FEVER AND RHEUMATIC HEART DISEASES: EPIDENIOLOGY, P F W E N T I O N , TREATMENT AND REHABILXTATION
ANNEX V THE CONTROL O F R H E m U T I C FEVER AND RHEUlY!lTIC HEAm DISEASE - AN OUTLINE O F WHO A C T I V I T I E S
ANNEX V I HYPERTENSION I N GENERAL
ANIEX VII CONTROL OF HYPE-SION IN POPULATIONS
fINNM VIII PR0BZ;EMS OF I S W d I C HEART D I S W E : EPIDFJIIOLOGY
A N N M I X INTENSIVE CORONARY CAEiE UNITS - OUTLINE
ANNEXX TREATMENT AND H X A B I L I T A T I O N O F ISCWIEMIC HEART DISEASE - PRESENT TRENDS
ANNEXXI CONTROL O F RISK FACTORS O F ISCHAEMIC HEXRT DISEASE
ANNEX X I 1 PFBIENTTON O F ISCHAl3MIC HEART DISEASE
ANNEX X I 1 1 APPROACHES TO THE COMMUNITY CONTROL O F ISCHAEMIC HEART DISEASE - TI.IEoRY P r n PRACTICE
ANNEX XIV ORGANIZATION OF CPYRDIOVASCULAR SERVICES I N GENERAL HOSPITALS
ANNEX XV PROEE&MS ELND CHAILLENGES I N REHABILITATION O F PATIEXTS W I T H ACUTE MYOCARDIAL INFARCTION
WHO m o
I INTRODUCTION
The first seminar organized by the World Health Organization i n the Eastern Mediterranean on the prevention of major cardiovascular diseases was held i n Teheran from 10-16 December 1972, a t the inv i ta t ion of the Government of Iran, who provided excellent f a c i l i t i e s f o r the meeting.
The seminar was inaugurated by H.E. D r M. ~hah&ol i , Ministry of Health, Iran. In h i s welcoming address, D r Shahgholi expressed his conviction t h a t the seminar would be an e f fec t ive way of increasing knowledge on prevention, treatment and rehabi l i ta t ion of major cardio- vascular diseases. A l W ~ u u @ i Lf1ar.e had Leeti a rapid developlent of this knowledge during the l a s t decade, he queried the impact on mortal i ty o r morbidity from hear t diseases. He s t a t ed t h a t some congenital hear t diseases mainly those due t o in t rau ter ine infections, could be prevented, but t h i s type of disease const i tuted a minor percentage of a l l hear t disease. Infect ious hear t diseases ca l led f o r ear ly eradication of the infect ing agent. The incidence of rheumatic fever and rheumatic hear t disease, which cons t i tu tes the major proportion of inl'ectious hear t disease, was declining. The cause of thLs decline, however, was not c l e a r and needed f'urther epidemiologic exploration t o es tab l i sh t o what extent this regression is due t o an t ib io t i c s o r t o improvement of l i v ing conditions and b e t t e r hygiene.
The epidemiology of chronic hear t diseases i n adul ts was even more important, and a mul t i fac tor ia l approach involving the dietary, soc ia l , physical, psychological a s wel l a s hereditary ro les should be considered. Only a f t e r sound and thorough epidemiological s tud ies i n d i f f e r en t par t s of the world would i t become known to what extent hear t disease could be combatted. This ca l led f o r in te rna t iona l co-ordination and collaboration f o r well designed experimental planning, supplementing the ex is t ing basic studies.
D r Shahgholi reminded part ic ipants of the f a c t t h a t medicine i n general had a dual nature unique t o i t s very being and application. It was an exact science, since it is a body of systematic knowledge acquired thrmgh precise experimentation i n man and laboratory animals. And yet, it was no l e s s a soc ia l science, because it must be applied t o a sensitive unpredictable being, man, Hence, c l in ic ians should look towards the basic sciences a s well a s towards society i n acquiring and applying new f a c t s on treatment and prevention.
Dr A. H. Taba, Regional Mrec tor f o r the Eastern Mediterranean, a l so welcomed the participants. He outlined the scope of the meeting, a s re la ted t o the overal l a c t i v i t i e s of WHO i n the f i e l d of cardiovascular diseases. The seminar was pa r t of WO's cardiovascular programme which
WHO ETJIRO EM/~ard .Vast ./5 EM/PRV. MJ' . CARD. VSC . D I s / ~ ~ Page 2
i s based on an assessment of the present and i t t u r e in te rna t iona l public heal th importance of cardiovascul-ar diseases. The aim of t h i s programme was t o promote and a s s i s t prevention and control of major cardiovascular diseases i n the community,
The prominence of cardiovascular diseases among the main causes of death was well known. I n many indus t r ia l ized countries these diseases a r e responsible f o r more than 50 per cent of a l l causes of death of which a t l e a s t 10 t o 15 per cent could have been avoided. Furthermore, with adequate measures, morbidity from cardiovascular diseases could have been considerably reduced. These deaths were not necessarily re la ted t o aging of the population because ischaemic hear t dlsease struck r~ow rr1or.e and [more or ten a t people who a re a t the height of t h e l r careers.
Many countries of the Eastern Mediteyranean Region were sh i f t i ng from pastoral l i f e t o a high speed indus t r i a l age with a l l the dangers of the r i s ing t i de of cardiovascular diseases.
While some cardiovascular diseases such a s hypertension, cerebrovascular disease and those caused by primary diseases of the lungs were ubiquitous, rheumatic fcver and cardiopathies of infect ious or ig in were predominant i n some areas, mainly among the l e s s privileged groups of people, while ischaemic heart disease of atherosclerotic or ig in was a t the moment a disease of affluence.
Thus p r i o r i t i c s i n the WHO programme i n cardiovascular diseases varied from region t o region and often from country t o country. The basic common principles were t o apply available measures a t the l eve l of the community and t o stimulate and co-ordinate research i n t o etiology and prevention.
He s ta ted t h a t a number of countries i n the Region were par t ic ipa t ing i n t . h ~ WHO pmgrarnrne 7 n r r ~ r i i i nvasci~lar diseases, be it the p i l o t study on prevention of rheumatic fever and rheumatic heart disease, o r the control of a r t e r i a l hypertension i n the community i n order t o reduce the most severe complications - stroke and cardiac fa i lure . There was growing i n t e r e s t i n providing proper treatment and rehabi l i ta t ion f o r a l l who were s t r icken with ischaemic hear t disease; and a l so i n taking care of those who were i n danger o f developing this condition. There were a l so good opportunities t o invest igate deeply i n a number of areas of t h i s Region the prognostic importance of fac tors known i n other, and par t icu lar ly i n industr ia l ized, areas t o be associated with an increased r i sk of severe atherosclerosis and of ischaemic hear t disease.
He f e l t t h a t i t was timely coincidence tha t t h i s meeting closed the year 1972 which was marked by WHO'S campaign t o prevent hear t diseases, with the slogan: "Your hear t i s your health".

WHO m o
The meeting, which was ass i s ted by a number of WHO advisers was attended by th i r ty- three part ic ipants from eighteen countries (Annex 11). The Internat ional Society of Cardiology and several national soc ie t ies of cardiology also sent representatives.
Dr M, Nadimi, Director, Department f o r Control of Heart Diseases, I ran, was elected a s Chairman; D r A. H, Akhtar, Associate ISnysician (Pakistan), D r A. A. El-Sherif, Professor of Cardiolo@;y, Cairo University (Egypt), and D r V. Kalbian, Spec ia l i s t Physician and Cardiologist, Nicosia (Cyprus), were elected Vice-Chairmen. D r M. H. Gabir, Cardiologist, Khartoum Hospital (Sudan), was nominated a s Rapporteur.
The provisional agenda was adopted and i t was agreed that each session would be guided by a d i f fe ren t moderator.
Summaries of da i ly sessions were provided and the general conclusions and recommendations were agreed upon a t the closing session.
I1 RHEUMATIC rnWR
1. Background
Rheumatic fever i s a complication of streptococcal pharyngitis which can occur i n a l l ethnic groups throughout the world, Although the pathogenesis i s still unproved, there is a strong correlat ion botween acute rheumatic fever and the severi ty of streptococcal pharyngitis, c l in ica l ly , epidemiologically and immunologically. The ubiquity of streptococcal s t r a in s , t h e i r var iat ion i n virulence, and t h e i r qua l i ta t ive differences, par t icu lar ly between "skin" and "throat" s t r a in s , have made the study of streptococcal epidemiology complex.
Rheumatic fever is, however, a preventable disease as has been ~110~11
by i t s v i r t u a l disappearance i n some communities. The disease and i ts major complication, rheumatic hcart disease, continues t o be a problem i n any par t of the world where crowding, la rge families, and low socio- economic conditions (increasing urbanization, rapid indus t r ia l iza t ion and changing ways of l i f e ) a re most s t r ik ing . Effective control, however, requires an intimate understanding of i t s complex epidemiology, i ts diagnosis and its natural h i s tory , Control of rheumatic fever a l so requires thorough co-operation of rheumatic subjects and t h e i r families, of a l l involved hea l th workers, and can be most e f fec t ive when well planned action is undertaken at the community lcvcl.
2. Current a c t i v i t i e s i n the Region
The meeting agreed t h a t rheumatic fever and rheumatic hear t disease continue t o be a problem i n a l l countries par t ic ipat ing. I n several countries it appeared t o be the predominant cardiovascular disease, e,g. Algeria, Egypt, I r an , Morocco atrd Turlisia. Many participants reported the absence of several of the more s t r i k ing manifestations of rheumatic

E l / ~ a r d . Vasc ./5 EPI/PRV.P~J. CARD. VSC . D I S / ~ ~ page 1! ,
WHO Em0
CLv,r, and emphasized thc uredoninant c l i n i c 3 1 p i r t u r ~ n F p o l y a r t h r i t i s , 2nd c a r d i t i s , manifested p r inc ipa l ly bjr v a l m l a r l c s ions . The Jones c r i t o r i c wcre discussed and i t was pointed ou t t h ~ t sonc of t h e major : ~ , , ? n i f ~ s t a t i o n s c f subcut,-.n.-ous ncdulcs a d e r y t h c i l ? ~ marginaturn werL L*-"rckr scen. Chorea, h~ izvor . , tras not infrcqucnt ly n c t ~ d i n Egypt, I r a n ,-.nd sonc o ther countr ies .
T~.L usef'ulness cf AS0 t i t r c s and othcr s t reptococcal ant ibodies vrns er~pi-icsizcd vihen thesi! srcrc rl~tcrmincct e a r l y i n t h ~ rheumatic a t t ack , s ~ c h a s during p c l y a r t h r i t i s . VOlt t l t h ~ ~ ~ S L Z S L i s ddt~et,~?CZ l a t c r i n t l lL nttack, c s wi th t h ~ cnsat of chore,' o r t h e de tec t ion of low grada c ? . r ~ i t i s , thc titr,s of antibociics may a l r ~ a d y h a v ~ dtcrcnscd and t h c r t t f o r ~ n:z:r b~ misleadingly low. Thi: u s t of s e r i a l dctcrr.1inations of AS0 titris during fcllow-up of w t i c n t s was cmphasizcd a s a maans ?or detecting ~7~1bs~qucnt r tcurrenccs o r f a i l u r e s of prophylaxis.
Four p i l o t p ro jec t s f o r tha con t ro l of rheumatic fever and rheumatic h L a r t disease arc n p ~ r n t i n g i n thc Region. Thr~, ol thca arc directly co-opcrating wi th t h t Cardiovascular Diseases Unit oC WHO, Gcnevz,
( 2 ) Egypt: Four compl~mentnry programmes a r c underway.
( i ) Surveys of schocl ch i ld ren aged 6-12 y t c r s i n the Qunlyub a rea and s tudcn t s en te r ing the Univtrs i iy .
(ii) Epidemiology cr s t reptococcal infections, p a r t i c u l a r l y wi th regard t o streptococcal serotypcs. Also, surveys of s t reptococcal pyodcrmc. with rrigard t o ~ f t u r c s t u d i c s of acutd glomeruloncphrit is ,
( i i i ) Reg is t ra t ion oi and long-term prophylaxis f o r rheumatic subjects.
( i v ) Rehabi l i ta t ion of p a t i e n t s aged 18-25 years wi th rheumatic h e a r t disease. This includes vocational guidance, placcrnent, follow-up and s p e c i a l education.
A programme i s und~rway which i s based on iJHO @idel incs and i s conducted i n co-opcrc?.tion wi th the CVD Unit i n Geneva.. Thc P r c g r m m c C ~ n t r t , ~ u r l s l s l s of a c n r . ~ l o l o g i s t , h l s iocglStrarS, nUrSe, sec re ta ry 2nd thc school h e a l t h o f l i c c r . This tcan aims t d provide thc e n t i r e i s l a n d wi th e p ~ v ~ n t i o n programmu.
(c ) Irnn
'Iho programmes are undersuny:
( i ) The School of Public Health of the University of Teheran several years agn ~ s t ~ h l i s h e d , w i t h the support of the WHO Streptococcal Laboratory, e deta i lcd survey of streptococcal infections, rheumatic fever and rheumatic heart disease i n some communities i n Teheran. Currently, t h i s group has expanded . t h e i r a c t i v i t i e s t o s tudies of the probelm i n nearly 14 000 worlters and t h e i r families i n a suburban community.
( i i ) Thc Ministry of Healtn of I ran selected 10 per cent of school children i n a d i s t r i c t of Teheran f o r a de ta i led analysis of the prevalence of rheumatic hear t disease i n re la t ion t o socio-economic standards, I n preliminary analysis there appeared t o be 7.8 cases of rheumatic fcver and rheumatic heart disease per 1 000 children 6-15 years of age. An analysis of the d is t r ibu t ion of cases so f a r showed no predominance i n the lower income group.
3. Guidelines f o r control
3.1 Prevention
Prevention of rheumatic fever includes prophylactic measures f o r f i r s t a t tacks (primary prevention) and f o r recurrences (secondary prevention); it i s a complex task. The best programmes f o r rapid and routine diagnosis of sore throats by throa t cul tures have of ten been mounted i n c o m n i t i e a i n w h i c h rheumatic fcvcr doc& not occm t o bc a prominent problem. The streptococc 1 s t r a i n s i n such places have become B attenuated, and the disease sporadic . Contrariwise, only the poorest medical care and no surveillance of respiratory infect ions a re available t o some of the most severely affected groups. The global nature of streptococcal pharyngitis and the seemingly i r reducible human reservoir of pharyngeal ca r r i e r s of virulent s t ra ins , however, make it incumbent upon g.& communities t o l i m i t the exposure and the spread or ch is disease by scrupulous adherence t o the pr inciples of rheumatic fever prevention, It is the duty, therefor i ,, of every community, whether o r not it has a serious streptococcal disease problem, t o assess i t s own programme f o r rheumatic fever prevention and t o decidc how t o meet the recommended standards f o r such programmes.
An up-to-date advice available t o a l l physicians and heal th workers concerning how rheumatic fever prevention may best be implemented i n communities, can be round i n the report of a WHO Expert committee2 and that of the US ItlLer-Sucittty Conmission f o r IIeart Disease ~esources3,
1stollerman, G. H., Siegal, A.C., Johnson, E.E. (1965) Variable epidemiology of streptococcal disease and the changing pat tern of rheumatic fever. Mod. Conc. Cardiovasc, Dis. 2, 45.
Qld. Hlth. Org. Techn. Rep. Ser., (1966),
3FUleumatic Fever and rheumatic heart disease study group: Report of the Inter-Society Commission f o r Heart Disease &sources: prevention of rheumatic fever and rheumatic hear t disease. (May, 1970) Circulation, 5, A-1-15.

~ ~ / ~ a r d .Vase ./5 EM/PRV.MJ'. CARD.VSC.DIS/~~ page 6
WHO EMRO
The most uFgent task . t o be tackled immediately, i s an appropr ia te programme of secondary prevention. Howcvcr, prirnery prcvcntion mcamrcc should a l s o be considered a s an important p r i o r i t y t a sk .
3.1.1 Secondary prevention -., (prevention of recurrent rheumatic a t t a c k s )
Although ac t ions ziming a t preventing recur ren t rheumatic a t t a c k s a r e c l e a r , it was considered usef'ul t o o u t l i n e the s t eps f o r t h e i r implementation i n d i f f e r e n t environmental and c u l t u r a l s e t t i n g s .
( i ) Establishment 02 a rheumatic f c v e r r e g i s t r y : There is a need t o c n t a b l i ~ h a r c f ~ i c t r y ?or rhcurnatio h e a r t d isoase and rheumatic fever, a t o o l f o r co l l ec t ing- anc! processing information about t h e community o r programmes erea , on persons e l i g i b l e f o r prophylaxis and t h e ca re they receive. An ou t l ine of such an information system i s given i n WHO Programme of Rheumatic Fever Prevention (Reference: WHO Programme on Rheumatic Fevcr Prevention Report of a Consultat ion he ld i n Cairo, 19- 22 February- 1972, ~ ~ ~ / 7 2 . 2 ) ; t h e scheme may be adapted t o l o c a l s i t u a t i o n s ana needs.
( i i ) Provision o l prophylactic d . g z : The most e f f i c i e n t regimen f o r continuous p r o p h y l ~ x i s aga ins t g r m p A streptococci i s a monthly i n t r a - muscular i n j e c t i o n of 1.2 mi l l ion u n i t s of bcnzathine p e n i c i l l i n . The disadvantages and discomfort of t h i s have t o be weighed aga ins t the ind iv idue l p a t i e n t ' s s u s c e p t i b i l i t y t o rccurrences. Those wi th rheumatic h e a r t d isease , recent rheumatic fever , and exposure t o an environment i n which t h e incidence of s t reptococcal i n f e c t i o n is frequent deserve t h c most e f f e c t i v e protect ion. A s a second choice, prophylaxis may be administered o r a l l y with e i t h e r 1 gm of su l fad iaz ine d a i l y i n a s i n g l e dose or 200 000 un!ts of p e n i c i l l i n given twice d a i l y on an empty stomach.
The d u ~ t i o n of continuous prophylaxis cannot be f i x e d unequivocally f o r a l l pa t i cn t s , alt'nough the s a f e s t genera l i za t ion is that i t be continued i n d e f i n i t e l y . Those under the age of eighteen years should certainly receive a continuous prophylactic regimen. A minimum period of f i v e years i s recommendecl f o r p a t i c n t s who develop rheumetic fever without c a r d i t i s over t h e age of eighteen.
The decis ion t o continue prophylaxis beyond t h i s period should t a k s i n t o account a number of var iables . Pa t i en t s wi th rheumatic h e a r t d isease a r e more suscept ible t o reac t iva t ion o f rheumatic fever i f they con t rac t a s t reptococcal in fec t ion . Moreover, p a t i c n t s who have had c a r d i t i s i n a previous a t h c k a r e much more l i k e l y t o s u f f e r c a r d i t i s again i n a subsequent a t t ack . Climato, age, occupation, household s i t u a t i o n , cardiac s t a t u s , and l eng th of time s ince t h e previous a t t a c k a r e a l l s i g n i f i c a n t va r iab les which inf luence the r i s k of recurrences.
WHO EMRO
The decline i n recurrence r a t e s with increasing age i s due to: (a) decreased r . 3 ~ ~ of streptococcal Infection, ana (D) decrease i n t he r a t e of rheumatic react ivat ion following streptococcal infect ion i n older rheumatic subjects. Despite this decreased ra te , however, the r i sk of rheumatic recurrence i n adul ts remains r e l a t i ve ly high when the streptococccl disease encountered is severe o r epidemic.
( i i i ) Establishment of follow-up programmes t o ensure pa t ien t f i d e l i t y t o the prophylactic regimen and doctors ' consistency. The follow-up should be devoted most vigorously t o those a t highest r i sk f o r recurrences - namely those with recent rheumatic fever (ht thin f ive years), and with exposure t o conditions of highest streptuuuucal a s e a s e prevalence.
( iv ) Making avai lable t o the community medical consultations, c l in ics , and laboratory f a c i l i t i e s f o r rheumatic pat ients .
(v) Undertaking case-finding izctions i n order t o ident i fy previously un- diagnosed cases of rheumatic hear t disease, needing secondary prevention. m e goal snoula be t o cover by continuous prophylaxis a l l cases of rheumatic fever and rheumatic hear t disease i n the community.
(v i ) Mounting a continuing programme of physician and community education on the needs of the rheumatic fever pat ient .
3.1.2 Primary prevention
( i ) Reliable, inexpensive and e f f i c i e n t throat cul ture services must be providedl. For a pa t ien t with an acute sore throat , it must be known simply i f the cul ture i s posi t ive f o r hemolytic streptococci. I f not , , the trouble and expense of an t ib io t i c s can be spared.
( i i ) Treatment of st.rept.orncca1 pharyngitis must be adequate to eradicate the organism. It i s still d i f f i c u l t t o convince the profession t h a t a s ingle in jec t ion of 0.6 t o 1.2 million un i t s of benzathine pen ic i l l i n G intramuscularly is optimal treatment. The a l te rna t ive of ten days of o r a l pen ic i l l i n G (200 000 - 9 0 000 un i t s b,i.d.) i s dependent upon -2 unpredictable pat ient f i d e l i t y . ( i i i ) Medical students, physicians, nurses and other professionals should be taught streptococcal microbiology adequately i n a c l i n i c a l context by departments of medicine, paediatr ics and community medicine.
bannemaker, L. W. (1970) Differences between streptococcal infect ions of the throat and of the skin. New England J . Med. 3, 23 & 78
2~ornmittee on Prevention of Rheumatic Fever and Bacter ial Endocarditis: Prevention of rheumatic fever. (1965) Circulation 2, 948

m/card*vasc ./5 EM/PRv.MJ .CARD. VSC . D I S / ~ ~ Page 8
WHO EMRO
( i v ) School-orJen.t_ed programmes, p a r t i c u l a r l y i n overcrowded schools i n high-r isk areas , provide exce l l en t oppor tuni t ies f o r ch i ld ren wi th symptomatic ph2ryngit is t o be examined and t o have a t h r o a t c u l t u r e made by ava i l ab le t r a i n e d personnel - t r a i n e d volunteers, school nurses o r o t h e r paid h e a l t h workers.
(v ) Community s u r v e i l l a n c e f o r s t reptococcal i n f e c t i o n s i s helpf'ul i n i d e n t i f y i n g suspect cases of pharyngi t is , t o determine when asymptomatic con tac t s should have t h r o e t c u l t u r e s made, o r even t o determine when mass prophylaxis wi th p e n i c i l l i n should be given.
(vi) Once a primary prevention programme i s developed i n t h e community, the public should be informed through a l l ava i l ab le communications media.
3.103 Establishment of community con t ro l programmes
P i l o t , model programmes should be i n s t i t u t e d i n l i m i t e d areas . Some s p e c i f i c fea tu res nre given b e l o w :
(i) The rheumatic fevcr/rheumatic h e a r t d i sease con t ro l programme should pr imari ly concentrcte on school-age chi ldren, a s these a r e a t h ighes t r i s k , and a s they a l s o represent a r e l a t i v e l y manageable, cap t ive population group. However, p a r t i c u l a r l y i f zt tendancc a t primary (elementary) schools i s not complete, ch i ld ren s taying away from the schools must also be oarod for ,
( i i ) Working rela-tionships could be es tab l i shed between t h e rheumatic f e v e r con t ro l prop;rme and t h e e x i s t i n g school h e a l t h se rv ices o r family h e a l t h Services, a s we l l a s wi th both the paed ia t r i c and medied departments of t h e adjacent hosp i ta l .
(iii) A bactcriulugicsl . an6 serological laboratory should be made ava i l ab le f o r cu l tu r ing and poss ibly grouping of s t reptococci , and f o r a n t i - s t r e p t o l y s i n 0 determination and o ther se ro log ica l t e s t s .
( i v ) Establishment of a programme f o r secondary prevention is, pragmati- ca l ly , the f i r s t advisable s t ep , and should be followed by primary prophylac- t i c a c t i v i t i e s . De te i l s of a community con t ro l programme (mainly secondary prevention) a r c given i n t h e WHO Programme on Rheumatic Fever Prevention - Report of a Consultatlion held i n Cairo, 19-22 February 1972 ( ~ ~ ~ / 7 2 . 2 ) . An important aspect i n primary prevention i s monitoring of poss ible impending streptoooocttl cpidcmics i n cei-tail1 c losea pOpUlatlOnS, such a s i n s t i t u t i o n s , and wide-scale prompt p e n i c i l l i n prophylnxis , i f appropriate, (so-called "mass prophylaxis" treatment of the e n t i r e l o c a l population. A s i n g l e i n j e c t i o n of 1.2 mi l l ion u n i t s of benzathene p e n i c i l l i n ) .
3.2 Treatment and management
There i s no s p e c i r i c cure f o r rheumatic fever . Good supportive therapy however, can reduce the s e v e r i t y of the scquelae of the disease and i t s morta l i ty .

WHO EMRO
3.2.1 Ant ib io t i c thcrapx
Af te r rhcumntic f e v e r i s f i r s t diagnosed, a course of p e n i c i l l i n should be given t o e l iminate group A s t rep tococc i , This is advisable even i f bacter io logic examination y i e l d s t h m a t c u l t u r e s negative f o r s t reptococci , s ince the organisms may be present i n a r e a s inaccess ib le t o swabs. It is preferable t o adminis ter p e n i c i l l i n pa ren te ra l ly . An e f f e c t i v e course is e i t h e r a s i n g l e i n j e c t i o n of 1.2 mi l l ion u n i t s of benzathine p e n i c i l l i n intramuscularly o r 600 000 u n i t s of procaine p e n i c i l l i n intramuscularly d a i l y f o r t a n days. Attempts t o reduce u l t imate h e a r t dmagc by a d m i n i s t ~ r i n g p e n i c i l l i n e a r l y i n the acute rheumatic a t t z c k i n l a r a e r doses have not been successfUl t o date . A f t e r completion of thc therapeut ic course of p e n i c i l l i n , continuous p ro tec t ion from re in fec t ion w i t h streptococci should be provided by i n s t i t u t i n g onc of the prophylactic regimens described.
3.2.2 Anti-inflammatory therapx
Both cor t icns t .c rn i d s 2nd s n l i cylat t s arc of considerable value i n a l l e v i a t i n g t h e symptoms of rheumatic fever , i n con t r ibu t ing t o t h e comfort of the pa t i en t s , and i n combating anorexia and anaemia. I n severe rheumatic c a r d i t i s a ssoc ia ted wi th h e a r t f a i l u r e , such non- s p e c i f i c anti-inflammatory e f f e c t s may, occasionally, tilt the balance i n favour of su rv iva l of a c r i t i c a l l y ill pa t ien t . Cor t icostcroids are more potent than s a l i c y l a t e s i n suppressing acute exudative inflammation, aild surne p a t i e n t s in whom s a l i c y l a t e a f a i l t o con t ro l thc d i s c a ~ u rospond quickly t o r e l a t i v e l y l a r g e doses of cor t i cos te ro ids . Whether o r not in tens ive c o r t i c o s t c r o i d therapy i n s t i t u t e d e a r l y i n t h e f i r s t rheumatic a t t a c k can reduce t h e degree of u l t imate cardiac s c a r r i n g is a point which is s t i l l somewhat a t i s s u e i n p a t i e n t s wi th r e l a t i v e l y mild cardiac involvement. Where c a r d i t i s i s more severe, a l l c a r e f i l l y con t ro l l ed s t u d i e s f a i l t o reveal any c l t r r r s u p e r i o r i t y of c o r t i c o s t e r o i d s over a s p i r i n i n t c m s of moalfying thc dura l lou US Llw auu tc : cliseast: ur res idua l h e a r t dcmage a f t e r f i v e years of follow-up. However, t h e r e i s s t i l l considerable v a r i a t i o n i n the recommendations concerning t h e use o f these agents.
The durat ion of treatment should be guided by t h e cxpected course of t h e disease and by the s e v e r i t y of the rheumatic process i n t h e ind iv idua l cnsc. Because most rheumatic z t t a c k s l a s t s i x weeks, treatment should b~ continuous a t l e a s t f o r t h i s period, wi th doses tapered during t h e l a s t two wteks. Should c l i n i c a l symptoms re lapse (rebound phenomenon), an acirlitioncl four t o six w e e k s of treatment io adviacd. I n otubborn a t t acks , such courses may have t o be repeated severa l times. Weekly t e s t s f o r C-reactive p ro te in i n the blood and f o r t h e erythrocyte sedimentation r a t e a r e a a e f u l i n following t h e hezl ing p r o c ~ s s , p a r t i c u l a r l y when t r e a t - ment wi th c o r t i c o s t e r o i d s o r s a l i c y l a t t s i s gradually withdrawn. With adequate suppressive: doses, t h e C - r ~ n c t i v e p ro te in should disappear from the blood, and the crythrocytc sedimentation r a t e should decrcnsc.
EM/Card.Vasc ,/5 EM/PRV. IW . CARD, VSC . ~ f S / l 7 page 10
WHO mo
Rwppearancc of C-rccctive p ro te in 2nd :n increase i n t h e ESR upon withdrawal of treatment ind ica t .~ . c0nt . i n l ~ c d rheumatic a c t i v i t y u n l ~ o c o ther cauaes of inflammation a r e prcsont.
Pa t i en t s who have rheumatic fevdr without evidence of c a r d i t i s r a r e l y have rheumatic h e a r t d isease when ex~mined t e n years l a t e r . They require no in tens ive e f f o r t t o prevent cardiac sequelae by prolonged bed r e s t o r prolonged r e s t r i c t i o n of physical a c t i v i t y . I f c a r d i t i s was a f e a t u r e of t h ~ a t t a c k g but murmurs have disappeared, fill a c t i v i t y may be resumed a f t e r s i x riloilths of observation have confirmed t h e continued absence of h e a r t disense. I n p a t i a n t s wi th res idua l cardiac murmurs, the dynamics of t h e l e s i o n and s i z e of t h e heart. u s i i x l l y detenninc f i ~ t ~ ~ r e r e s t r i c t i o n s of a c t i v i t y ,
3.2 .3 Rehabi l i t a t ion
School-age chi ldren should not be l e f t without teaching, if confined t o r e s t o r reduccd a c t i v i t y f o r a proplonged period, Hospi ta ls deal ing w i t h suoh p a t i e n t s should cmploy teachers w h o w i l l take car= uf Lhu curlLir~ulrlg education of t h c s i c k chi ldren. I f no f u r t h e r schooling is envisaged, teenage p a t i e n t s wi th valvular h e a r t d isease should be h a b i l i t a t e d f o r ga in fu l l i f e : they should be offered the opportunity t o l e a r n an occupation which would s u i t t h e i r physical handicap, due t o the permanent damage of t h e i r hea r t . However, o f t e n the handicap may be but of minor degree.
Special aLLerltlon should be paid t o t h e vocational counsell ing of a l l young p a t i e n t s wi th rheumntic h e a r t d isease , even wi th s l i g h t organic changes.
I n young people already engaged i n 2n occupation involving hcavy physical a c t i v i t y , measures f o r vocational r e h a b i l i t a t i o n (qual i fying them f o r a l i g h t e r job) may become necessary.
4. Hecommendations
( i ) Discussion 0.i" the ongoing programmes and experience from o t h e r coun t r i es has resu l t ed i n 2. general d e s i r e f o r t h e systematic establishment of rheumatic fever prevention programmes i n every country.
( i i ) Because no s p e c i a l f a c i l i t i e s c r e required, a secondary rheumatic f e v e r prophylaxis p r o g r m e should a t l c a s t be i n i t i a t e d i n every country a s a p i l o t p r o g r m e . The p r inc ip les of such programmes should follow
1 the WHO protocol on rheumatic fever prevention . Schools a r e p a r t i c u l a r l y aygropr la te places' Tor such prograrmcs.
'WHO Programme on Rhdurnatic Fever Prevention: Report of a Consultat ion he ld i n Cairo, 19-22 February 1972, WHO I n t . doc. ~VD/72.2
WHO EMRO EM/~ard , ~ a s c ./5 EM/PRv. w . CARD. VSC . ~ 1 S / 1 7 page 11
g i i ) Populations i n which crowded Living condLtions predispose t o rheumatic f e v e r should be sought a s the most appropr ia te s i t e s i n which t o mount programmes.
( i v ) Regis ters f o r secondary rheumatic fever prevention programmes should o f f e r the b e s t oppor tuni t ies t o develop r e h a b i l i t a t i o n and vocational guidance a s p a r t o f t h e programme.
(v) Once a s t rong p i l o t pmgnmme has been established, it should be expanded t o include a s much of t h e population o f a country a s is necessary and fens3 h l ~ , nssi gni ng prri nr i t.i es t,o areas of g r e a t e s t r i s k .
1. Background
A r t e r i a l hypertension i s the commonest c i r c u l a t o r y d i sorder a l l ovcr thc world. Approximately 10 pcr o c n t of adults - both males and females - have casua l blood pressure values a t o r above (160/95) m/Hg. The condi t ion is infrequent only i n some pr imit ive t r i b e s and i n populations l i v i n g on high a l t i t u d e plateaus. By f a r t h e g r e a t e s t proportion of sub jec t s a r e those wi th so-cal led e s s e n t i a l hypertension, followed by r e n a l parenchymal and r e n a l vascular d isease . Hypertension caused by hormone- producing tumours i s r e l a t i v e l y ra re . I n some a reas , such a s those s t r i c k e n wl th schlstosomiasis (S. t laerr~a~ublur~~), hyperter ls iun secondilly t o pyelonephr i t i s i s common.
Since t h e e a r l y 1 9 5 0 ~ ~ drugs which lower e lcvated blood pressure have appeared, which have changed t h e prognosis of sub jcc t s wi th high blood pressure s i g n i f i c a n t l y . Pa t i en t s wi th some forms of malignant hypertension now can be maintained i n s a t i s f a c t o r y h e a l t h f o r ycars , Continued t r e a t - mcnt wi th hypotensive drugs have proved t h a t some rnajor complications ot' hypertension, e.g. s t roke, hypertensive h e a r t f a i l u r e and hypertensive r e n a l d isease can be avoided t o a considerable cxtcnt . It has not y e t been proved, howcver, whether, o r t o what extent , such treatment w i l l reduce the incidence of ischaemic h e a r t d isease , of which hypertension i s one of t h e main predisposing fac to rs .
Ef fec t ive treatment, unfortunately, so f a r has bccn given only t o a f r a c t i o n of hypertensive subjects , a s many have no symptoms compelling them t o see t h e doctor. Even i f drug treatment i s given, it is often not a m i n i s t e r e a continuously over a long period of time, as 1 L bfluuld be. The exce l l en t p o s s i b i l i t i e s f o r reducing s e r i o u s colnplications of hyper- tens ion on the one hand, and t h e lack of app l ica t ion of t h i s treatment t o n l l who need it, require measures f o r de tec t ion o f a l l hypertensive sub jec t s a t t h e e a r l y phasc of t h e discase , and i n s t i t u t i o n of appropr ia te long-term treatment. Control programmes the re fore have bcen i n i t i a t e d by WHO on a p i l o t b a s i s i n f i f t e e n communities i n various p a r t s of the world covering a t o t a l of approximately 750 000 people. These may demons t r a t e wi thin f i v e years how h e a l t h a u t h o r i t i e s may expand t h e de tec t ion
EN/~ard . ~ a s c ./5 EN/PRV , M J . CARD .VSC . D I S / ~ ~ page 12
WHO EMRO
and con t ro l of hypertensive sub jec t s t o e n t i r e populations, and organlze nation-wide se rv ices i n diagnosis and ca re , Such measures may prolong a c t i v e and s a t i s f a c t o r y l i f e f o r count less sub jec t s wi th high blood pressure. Simultaneously, of course, the general publ ic should be made aware of these programmes and t h e i r a c t i v e pa r t i c ipa t ion , e s s e n t i a l f o r i ts success, should be secured.
While it i s imperative t o t r e a t a l l sub jec t s wi th es tab l i shed hyper- tens ion, even i f asymptomatic, f 'urther research i s needed on t h e n a t u r a l h i s t o r y and prognosis of sub jec t s wi th mild o r i n t e r m i t t e n t e leva t ion uf blvod pressure and un the etiology and pathogenesis uf e s s e n t i a l hyper- tension. Research should a l s o c l a r i f y t h e r e l a t i o n s h i p of hypertension t o ischaemic h e a r t d isease .
2. S i t u a t i o n i n t h e R e g 1 2
L i t t l e i n f o m a t i o n is a v ~ 5 l a b l e on t h e prevalence of hypertension and the incidence of i t s complications i n t h e coun t r i es of t h e Region. I n Egypt, a study was made of a group of 11 000 c l i n i c a l l y h e a l t h male labourers aged 11-40: i n 1 2 per cent of t h i s population group e levated blood pressure was Tound ( ~ l s h e r i f ) . I n another Egyptian study of a general population group hypertension was found i n 10.5 per cent . No population-based s tud ies were made i n o ther coun t r i es of t h e Region t o determine the prevalence of high blood pressure. Hospital data, under- standably, under-rate i t s s ignif icance.
I n severa l places hypertensive h e a r t f a i l u r e seems t o occur r a t h e r frequently; i t may be, i n f a c t , t h e second commonest cause of h o s p i t a l admissions among the cardiovascular d i seases . Stroke i s probably t h e commonest complication of hypertension i n coun t r i es of t h e Region, a s elsewhere. I n the majority of cases, horuever, stroke patients are not hosp i ta l i zed ; therefore h o s p i t a l da ta should not be considered a r e l i a b l e i n d i c a t o r of t h e frequency of s t roke i n t h e Region. !here may be severa l reasons f o r t h e presumed low r a t e of h o s p i t a l i z a t i o n f o r s t roke: the a t t i t u d e of t h e public which mc;. be due t o t h e f a c t t h a t t h e condit ion usua l ly occurs i n the o lder age group; some scepticism may p r e v a i l a s t o the benef i t s t o be gained from h o s p i t a l treatment; t r a d i t i o n may a l s o be a f a c t o r i n severa l areas .
Renal f a i l u r e associa ted wi th high blood pressure is frequent ly observed. The d i f f e r e n t i a t i o n of rena l involvement i n hypertension from hypertension due t o primary r e n a l d isease is of ten d i f f i c u l t . A s mentioned, i n a reas in fes ted wi th schistosoma haematobium, severe hyper- tens ion i s o f t e n observed a s a consequence of pyelonephr i t i s due t o schistosorniasis. I n Egypt, f o r example, i n schistosoma-ridden areas , the r a t i o of e s s e n t i a l t o rena l hypertension i s 2:1, while i n schistosoma- f r e e a reas t h e r a t i o i s approximately t h e same a s i n o t h e r p a r t s of t h e world,

WHO m o EN/~ard.~asc ./5 EM/PRv,NJ. CARD. VSC .DIS/17 page 13
Renal tuberculosis was reported t o be a re la t ive ly frequent cause of hypertenslon I n cer ta ln places (e.g. Pakistan); based on hospi tal s t a t i s t i c s , up t o 7 per cent of hypertension might be a t t r i bu ted t o renal tuberculosis.
I n general, however, w i t h these two exceptions, there do not seem t o be any other epidemiological pecu l i a r i t i e s of a r t e r i a l hypertension i n the Region, and the same principles fo r i t s control should be applied a s elsewhere.
3. Guidelines f o r control
3.1 Diagnosis
I f high blood pressure has been found i n a subject, e f f o r t s should be made t o determine i t s etiology. The diagnostic work-up i s discussed i n d e t a i l i n Annex VI. I n practice, however, the constraints of rea l - l i f e s i tua t ions do not allow f o r the application of a l l sophisticated ciiagnostic prweaures, and an estimate of the additional. benefi ts resu l t ing from an exhaustive diagnostic schedule seems t o plead f o r simple diagnostic procedures, a s outlined i n the WHO protocol f o r the c o m n i t y control of hypertension1 unless there is c l i n i c a l suspicion of a specif ic (renal, endocrine o r other) cause. I n common medical practice, i n approximately 99 per cent of a r t e r i a l hypertension, no cause, o r no surgical ly curable cause, i s found and therefore one must r e ly on medical treatment which has accomplished tremendous advances i n the course of recent years.
3.2 Management and therapy
The d i e t should be low i n sodium, poor i n 3ipids and sometimes r e s t r i c t ed i n carbohydrates. The pa t ien t should s top smoking, absorbing l iquorice o r taking contranept j ve p5.ll.s. Analgesic mixtures with a high phenacetin content should be avoided also.
The pat ient should lead a healthy l i f e avoiding violent physical exertion, espeoially a f t e r meals, but should take up a moderately act ive sport. Diving and bathing i n cold water a re not advised,
Drug therapy varies according t o d i f f e r en t authori t ies . I n the past few years, several drugs have been shown t o be par t icu lar ly efficacious.
One may s t a r t by using chlorothiazide (250-500 m) with potassium s a l t s . I n addition spironolac tones may be confined f o r more e f fec t ive sal idiureses . I f this treatment is insuf f ic ien t , it a t l e a s t renders more eff icacious other antihypertensive drugs which can be added next. Thus, can be added 250-500 mg of alpha-methyldopa, o r 10-20 mg guanethidine, 10-20 mg of
lCommunity Control of Stmke and Hypertension - Report of a WHO meeting, Giiteborg, 29 November - 3 December 1971 (Int . doc. W/72.1)
EM/~ard .~asc ./5 . EM/PRV.MJ. CARD. VSC. D I S / ~ ~ page 14
hydralazine, 1-2 mg of re-srpin, 75-150 mg of c lon id in o r sometimes merely a beta-blocking agent (profanolol , 10-20 mg) i f t h e p a t i e n t does not s u f f e r from bronchial. asthma ( o r cardiac conduction defec t s ) . These d m g s may a l s o be combined.
Sometimes i n the presence of spontaneous o r sa l id iure t ic- induced hyperuricemia, uricosui>ic agents a r e added. I n the presence of hyper- cholesterolaemia, hypolipernic &rugs may be used.
L i fe for the p a t i e n t becomes complicated when drugs a r e given i n high doses, o r i f too many drugs a r e associated. The p a t i e n t g e t s depressed and t i r e d , and impotence and gynecomastia may increase h i s discomfort.
I n s p i t e of &&ese inconveniences, t h e l i f e expectancy of a sub jec t su f fe r ing from hypertension tends t o appro::imate more and more t o t h a t of an ind iv idua l wi th normal blood pressure.
I n 1960, v i r t u a l l y a l l p a t i e n t s d ied wi thin f i v e years following the onset of malignant hypertension. 'Nowadays, a f t e r f i v e years, 55 per cent of such p a t i e n t s a r c s t i l l a l i v e . This change i n prognosis i s an encouraging ?orecast f o r t h e fu tu re success of ant ihyper tensive therapy except f o r t h n r e l a t i v s l y high incidenct! of coronary accidents (although of ten minor) i n p a t i e n t s whose a r t e r i a l hypertension has been gradually normalized.
3.3 Control of hypertension i n coinmunities
There a r e severa l reasons which c a l l f o r hypertensive con t ro l programmes a t t h e l e v e l of vrhole cor;&nnities. Thc prevalence of hypertension i s very high; i t s complications may be severe; though adequate therapy is e f f e c t i v e , population-based s tud ies i n severa l p a r t s of t h e world show t h a t very o f t e n hypertcnsion i s not recognized i n time, even i f t r e a t e d therapy i s usua l ly ne i the r cons i s ten t nor adequate.
The approach t o t h e community con t ro l of hypertension s t a r t s wi th an assessment of t h e epidemiological s i t u a t i o n i n a community. This may be b e s t achieved by a preparatory p i l o t inves t iga t ion of t h e prevalence of hypertension i n a sampl, of t h e population t o be screened f o r high blood pressure, and by an a n ~ l y s i s of ava i lnb lc da ta on morbidity and mor ta l i ty f ~ o m t h e complications of hypertension. Ir no general h e a l t h s t a t i s t i c s are available, hospital atatistius rliay ?.JC used. Such a p r e p l l u t assess-
*merit can be done wi th a r e l a t i v e l y low investment of ensrgy, time and money.
Based on t h e da ta from t h e i n i t i a l assessment i n the community, a programme f o r the con t ro l of hypertension i n a community should be es tab l i shed on a p i l o t bas i s , i n order t o ga in p r a c t i c a l experience i n t h e area . -If successful , 'the p l l o t programme should serve a s a model f o r more extensive con t ro l progranmcs i n the community.
WHO EMRO
DetaLls 09 a programtile f o r t h 3 community con t ro i 0.f b - p e r t a s i m a r e gfven l n the Gijteborg yr.olucoll and Annex KCI. The maln obgectives a r e i d e n t i f i c a t i o n of hypertensive subjects, regu la r and long-term treetment, and systematic long-term follow-up of t h e subjects . The over211 aim i s prevention of complicntions .
Th2 methods include: screening f o r e levated blood pressure; r e g i s t r a t i o n oi those found t o be hypertcnsivc; establishment of a hypertension c l i n i c t o provide a h igh l e v e l of medical ca re and t o n c t a s a spec ia l i zed cen t re o f fe r ing i t s se rv ices and diagnost ic f a c i l i t i e s t o t h c p r a c t i t i o n e r s i n t h e a rea w i l l i n g t o ask f o r con- s u l t a t l o n ; educational activities dlrecLcd at lie pt~yslclarls arid ottler* h e a l t h workers i n the community; ancl h e a l t h education of t h e general population and ol" hypertensive p a t i e n t s and t n e i r famil ies .
However, t h e methods should be adjus ted t o t h e l o c a l s i t u a t i o n , including t h e soc io -cu l tu ra l p a t t e r n and h e a l t h ca re system i n t h e area . Experience wi th community con t ro l programmes f o r hypertension i s s t i l l l imi ted a t present . The p i l o t progr~mmes should the re fore be considered a l s o a s research p ro jec t s which should y i e l d s p e c i f i c information on how t o manage hypertension i n an e n t i r e population.
( i ) The con t ro l of a r t e r i a l h y ~ e r t e n s i o n c a l l s f o r community-wide act: on.
( i i ) A step-wise approach t o t h e con t ro l of hypertension is recommended.
( i i i ) A s a f i r s t s t ep , p i l o t commrity con t ro l progrz lmes should be establ ished.
( i v ) Those should bo prooedod by a l imi tod preparatory study of tho provs- lence of hypertension i n t h e community and the incidence of i t s complica- t ions .
(v) I n medical teaching centres , hypcrtension c l i n i c s should bc mad^ avai lable .
( v i ) The con t ro l programmes should include i d e n t i f i c a t i o n of hyper- tens ives , thdi? yeg i s t ra t ion , treatment and long-term a c t i v e follow-up, a s we l l a s education of a l l t h e physicians i n t h e a rea and h c a l t .h ~ d 1 1 r n t . i nn n f t . h ~ pat3 c,nt . s , t .h~>i r fami 1 i es a n d n f *,he g~nernl public.
( v i i ) Thc p i l o t programmes should y i e l d experience on which extension o f t h e con t ro l progranmes could be besed.
( v i i i ) Af te r such programmes have been es tabl ished, t h e problem should bu r ~ - a s a c s s c d and rcsourccs f o r d o a l i n ~ with it should bu c~cplorcd and developed. - ~ ~ o m m u n i t y Control. of Stroke and Hypertension -- Report 02 a WHO Meeting,
Gteborg , 29 November - 3 December 1971 ( k t . doc. CVD/72.1)

EM/~ard.Vasc ./5 EM/PRV. NJ . CARD. VSC . DIS/17 page 16
WHO EMRO
I V ISCHAEDlIC HEART DISEASE
1. Background
There a r e severa l reazons f o r t h e increas ing a t t e n t i o n paid t o ischaemic h e a r t d isease . It i s a world-wide disease which has now reached enonnous proportions, s t r i k i n g more and more a t younger subjects , and causing g r e a t l o s s i n human l i f e and i n economic product ivi ty . A s i t i s assumed t o be associa ted with the present a f f l u e n t mode of l i v i n g , a f h r t h e r increase i s expected which could r e s u l t i n t h e g r e a t e s t epidemic mankind has faced, un less we a r e ab le t o reverse t h e t r end by concentrated research i n t o i t s et io logy, pathogenesis, cure and prevention.
1.2 Etiology
A myocardial i n f a r c t i o n is usua l ly caused by occlusion of one o r more coronary a r t e r i e s , mainly by a th romb~~s , However, i n some ins tances , no thrombus i s found desp i te evidence of damage t o t h e myocardium. There a r e reasons t o focus not only on the thrombus and the coronary a the rosc le ros i s but a l s o on o ther mechanisms of myocardial damage such a s metabolic d i s - turbances producing conduction defec t s which r e s u l t i n ischaemia. The re la t ionsh ip between coronary a the rosc le ros i s and ischaemic h e a r t d i sease ' has been s tudied i n severa l autopsy s e r i e s . It has been found t h a t those who died f r v m myoca~dia l infarction had, in a l l age groups and in both sexes, a h igher degree of coronary a the rosc le ros i s than those dying from any o t h e r cause.
1.3 Epidemiology
Many s i x d i e s conducted &x-ing the pas t twenty-five years have demonstra- t e d assoc ia t ions between c e r t a i n biochemical, physiological ana environmental f a c t o r s and t h e development of ischaemic h e a r t d isease . S t a t i s t i c a l a ssoc ia t ion of ischaemic h e a r t d i sease wi th these r i s k f a c t o r s has l e d t o specula t ions concerning t:ieLr e t i o l o g i c a l importance.
Such important f a c t o r s a s high blood pressure, increased semm choles te ro l and smoking can, however, expla in only a p a r t of t h e pathogenesis and o ther va r iab les musJi be important t o t h e e t io logy. It i s important, f o r erample, t o study psycho-social f ac to rs , p z t t e r n s of behaviour and the pathogenesis of premature aging. The r e l a t i v e l y low incidence of coronary a r t e r y a l sease I n women during the child-bezring age, drld Wle d ~ a ~ i ~ a L i e accele~-atiull of a the rosc le ros i s by such d i seases a s d iabe tes and c e r t a i n f a m i l i a l forms of hyperlipidaemia, suggest important metabolic f a c t o r s which requ i re in tense inves t iga t ion .
Great d i f fe rences i n ischaemic h e a r t d i sease mor ta l i ty r a t e s between count r i es of t h e same c u l t u r a l and economic l e v e l a r e w e l l recognized. For

WHO m o EM/~ard .Vase ./5 EM/PRV.W. CARD .VSC . D I S / ~ ~ page 17
example i n males i n the age group 45 - 54 the death r a t e s from ischaemic hear t disease f o r 1969 were f o r Sweden 126.0, Norway 1 1.5, Scotland 329.2 and Flnlancl 427. j per 100 000 population respectively.q Such differences a r e intr iguing and challenging. Fur-themlore, within one country differences among various populations may a lso be s t r iking. I n fac t , the correlat ion of a given r i sk f ac to r with ischaemic hear t disease may vary i n d i f fe ren t countries.
1.4 Clinical features
( i ) Sudden death. One of the most dramatic and frightening features of acute myocardial in farc t ion I S sudden and unexpected death i n VigOrOU$, apparently healthy individuals often a t the peak of t h e i r careers. ,Possi- b i l i t i e s of salvaging such individuals by treatment i n coronary care un i t s and of preventing such events by open hear t coronary by-pass surgery, have focused great i n t e r e s t upon highly specif ic but expensive methods f o r diagnosis and treatment. Whereas such intensive treatment centres have created much i n t e r e s t i n the problem and have improved considerably the care of pat ients with acute myocardial infarct ion, they have not ye t dea l t with the f a r more important and general problem of the recognition and treatment of subcl inical coronary atherosclerosis i n a huge segment of some populations (e.g. i n some studies a s high a s one-third of the population of men i n the s ix th decade of l i f e ) . The major achievement of the coronary care un i t s has been t o t r e a t o r prevent ventr icular f i b r i l l a t i o n o r other serious arrhythmias i n acute ischaemi c. heart, d i spaso (ar11t.e myocaxulir,l in farc t ion) , the most important causes of sudden death.
( i i ) Other aspects of myocardial infarct ion. Myocardial in farc t ion of ten remains unrecognized f o r several reasons. The symptoms of pain may be atyp%cal., misinterpreted o r absent. Prognosis i n these pa t ien ts i s no be t t e r than i n those with typ ica l and properly diagnosed chest pain. Further- more, in o l d c r oubjecta progressive deter iorat ion o f t l ~ e hear t from asympto- matic infarct ions leads t o cardiac f a i l u r e andoftcn ends i n sudden death. These features of myocardial in farc t ion make it d i f f i c u l t t o ident i fy a l l pa t ien ts with coronary a r te ry disease i n i t s ear ly stages and complicate the problem of prevention. The widespread and insidious development of coronary atherosclerosis, well before the c l a s s i ca l and overt myocardial in farc t ion becomes apparent, demands preventive approaches which can head off o r modify the disease i n i t s ear ly phase. A l l e f f o r t s must be made therefore t o seek clues t o the pathogenesis of the disease i n a l l populations whether the incidence i s high or low.
l ~ e j f a r , Z: Prevention of Ischaemic Heart Disease i n the l i g h t of mortality and morbidity data. Paper presented a t Skandia Symposium on ear ly phases of cardiovascular disease, Stockholm, 19-21 September, 1972.

~ i i / ~ a l - d .Vase ./5 EPI/PRV. iW . CAFD.-iC. D I s / ~ ~ page 18
WHO EMRO
2. The situ.?:Lion i n t h e Region
Ischaenic hear-L disease i s on the r i s e i n t h e countr ies of t h e Region according TO repor t s by various pa r t i c ipan t s . Atheroscleros is seems t o be co-nmca and the same r i s k Pacto's seem t o be present i n t h i s R ~ g i o n a s i n otiiei- areas . Some of zhcse f a c t o r s reported arc : obesi ty , high f a t d i e t , s-oking, d iabetes , rncntal s t r e s s , e t c .
A survey 5u.urln; the seminar showL3 t h a t h a l f of the countr ies had e coronary cays u n i t ba t only th ree coun t r i es had more than three .
Nyocarcllal infarction p a t i e n t s a r e very o r ten hosp i ta l i zed i n t h e Rcgion. This s i t u a t i o n w a s most evident i n Turkey, Cyprus, Lebcnon and Syria. On thc. o the r hctnd, q -ocard ia l i n f a r c t i o n seems t o be zulnost unknown i n h o s p i t a l s i n Ethiopia and Y,. ~mcn.
3. Treatment and Rehabi l i ta t ion
3.1 Emergency care
Excelli-.nz ~ e s u l t s i n tkLe treatment of p a t i e n t s i n coronary care u n i t s have arouscd the i n t e r e s t of t h e public a s we l l a s of h e a l t h workers. A number of s tud ies , however, including WHO co-operative inves t iga t ions i n t o the community aspects of acute myocardial i n f a r c t i o n (~nnei : XTTT p , i i ) , c o n i i ~ ~ c d t h a t more than 50 per c e n t o f p a t . i ~ n t . s d y i n g with acute i n f a r c t i o n never reached hosp i ta l . The e a r l y emergency care f o r p a t i e n t s wi th a c u t i i n f a r c t i o n outs ide the h o s p i t a l immedLately c?fter t h e a t t a c k has occurred i s thcrcfort . css tn 'c inl i f mol3tality i s t o bc reduced. Tpaiiicd personnel and s - e c i a l equipfi~ci~t s:iould bc: ava i l cb lc throughout t h c community, and a l l se rv ices need t o be organizsd so as t o reach evert. p c t i e n t wi th t h e s h o r t c s t poss ible delay.
. A review 02 1x7 p a t i e n t s t ranspor ted t o the Royal Mclboulnr. Hospit2l. i n a mobile COiqonaT ca re u n i t during a ten-month period r tvealed t h a t one - t h i r d had nradyarrhytimia, one-third an errhythmia associated tr?lt'fl
ven t r i cu la r irri t z b i l i t y , while thc r e m i n d e r had no rhythm disturbance . A s first a i d treatment i n t h e management of bradyarrhythmia, tht-
use of a t ropine , given a s an intramuscular i n j e c t i o n using an automatic t i s s u e spray i cv icc ( t h e doses were 1 o r 2 mgm) was compared wixh tha-c of an intravecous i n j e c t i o n of the 0.3 rag21 (Dr Sloman) . Bcth fomis ol' thr?rapy w e r e shorm tc increase the heart rato. Tho most suitable mod0 of dcliirery, however, i s a s y e t unproven. The value of intramuscu1c.r l idocaine (200 msx, 10 per cent so lu t ion) administered by a u x i l i a r y s t n f l ' was a l s o d i s c u s s d . It appears, howcv~r , t h a t an intravenous bolus 02 1 per ccnt l idoca ine i n a dose of 1 mgm per kgm body weight followed 5:. a c o n t i n u o ~ s inrus ion (2 mgm/~g b.w./per minute) reaains tho truatmcnt of choice.

WHO m o
Experience showed t h a t mobilc and t ranspor table r e s u s c i t a t i o n equipment shuulil be ilelivu~.ad L u l l e slLe or accldent (home, occupation place c tc . ) f o r i n i t i a l treatment (outs ide t h e ambulance) so t h a t t h e p a t i e n t could be s t a b i l i z e d before bcing t ranspor ted t o the h o s p i t a l . The cormon experience of delayed admission t o emergen- cy ca re was emphnsizcd and it ~sls rccommcnded t h a t h o s p i t a l s should s t reamline sdmission procedures t o f n c i l i t s t c . access t o t h e coronary ca re u n i t .
3.2 Coronary ca re u n i t s (%x) Thc main j u s t i f i c a t i o n for the estnblinlment of CCUs waa tlre
immediate, e f f i c i e n t treatment of primary v e n t r i c u l a r f i b r i l l a t i o n and o ther se r ious premonitoqr arrhythmias and conduction defects . The u n i t s a r e c o s t l y and must be considered i n ind iv idua l countries i n t h e l i g h t of t h e p a t t e r n of cardiovascular d i seases and o r budgetary p r i o r i t i e s .
'I'l~e o y t i ~ n u l caLmc: ctvallable I n CCUs can a l s o be o f fe red I n general medical se rv ices us ing s i m i l a r t r anspor tab le equipment which allows t h e continuous monitoring o f cardiovascular f inc t ion . However, where coronary ca re u n i t s a r e a l ready s e t up, one should t r y t o avoid dupl i - ca t ion and t o make t h e b e s t use of ava i lab le resources. I n u n i v e r s i t y teaching h o s p i t a l s , it i s worthwhile t o e s t c b l i s h CCUs. Apart from providing exce l l en t up-to-date care , they should be t h e focus f o r research i n t o the problems of t h e n a t u r a l h i s to ry , e t i o l o a , patho- genesis and treatment of acute myocardial i n f a r c t i o n and serve a l s o a s cen t res f o r t r a i n i n g of s t a f f , Thc concept of t o t a l p a t i e n t ca re must be emphasized i n a l l t r a i n i n g progrnmmcs. While it i s economi- c a l i n some sriinll h o s p i t a l s f o r p a t i e n t s wi th myocardial i n f a r c t i o n t o be nursed alongside with o t h e r seriously ill s u r g i c a l p a t i e n t s , t h i s must be regarded a s a poor expedient.
Appropriately t r a i n e d nurses should be encouraged t o perform diagnost ic and therapeutic procedures previously handled by physicians. It had been t h c expcricnce of many ccn t res t h a t such t r a i n e d nursing s t a f f can provide more rapid diagnosis and treatment on t h e spo t i n the CCU than can be provided by physicians who have t o be c a l l e d t o the ccu ,
I n a country, o r i n a l a r g e arcn of a country, wi th one major teaching h o s p i t a l and a CCU, t h e use of telcphonc transmission of t h e ECG from small in tens ive ca re u n i t s o r cardiac monitoring u n i t s can enable immediate profess ional advice t o be given. The system a l s o has a s i g n i f i c e n t educational element f o r t h e s t a f f i n t h e small u n i t s . A small personalized ECG t r a n s m i t t e r wns demonstrated and it was noted t h a t the scme type of device can bc used f o r t e s t i n g implanted pacemakers thyou.& t h e telephone t r ~ ~ n s m i s s i o n system.

WHO ENRO
The remcrkable achievements i n 'chc treatment of p a t i e n t s wi th aautc myoonrdiel inParat ion i n the CCU has lcd, among o ther things, t o t h e develop~ient o r more precise physiologic monitoring, c .g. t h e f l o a t i n g balloon c a t h e t e r technique which enables cardiac pressure and blood flows t o bc mc?.surcd a t t h c bedside o l p a t i e n t s wi th acute myo- c a r d i a l i n f a r c t i o n . Tie tschnique i s sa fc , quick, r e l i a b l e and may be of value i n assessing changes i n cardiac f inc t ion , and i n providing oppor tun i t i e s f o r pacing. However, i n s p i t e of considerable e f f o r t , l i t t l e progress has been achieved i n t h e management o f cardiogenic shock, and of severe h e a r t f a i l u r e , and these complications remain major challenges.
3.3 Rehabi l i t a t ion and secondary prevention
These a r c t h e indispensable complements of acu te s t age surveillance and medical treatment. Rehab i l i t a t ion may be defined a s t h e "sum of a c t i v i t i e s required t o ensure handicapped cardiac p a t i e n t s t h e b e s t poss ible physical , mental and s o c i a l condit ions so t h a t they may, by their own c f f o r t a , rcsumc aa normal n plccc aa pooaiblc i n thc l i f c of the community". (WHO, 1969).
This impl ies t h s t r e h a b i l i t a t i o n measures should be ea r ly , continuous and take i n t o considerat ion nll aspec t s of a p a t i e n t ' s needs, physiologi- c a l , psychological and s o c i a l .
From the onset oi' the drlsease, progr~esslve rnublllzallurl sl~uuld be i n s t i t u t e d under medical supervision, and a t t h e same time t h e psycholo- g i s t and the s o c i a l a s s i s t a n t should endeavour t o solve the p a t i e n t ' s problems, and inf luencc t h e fami ly ' s and t h e employers' a t t i t u d e .
Gradual mobilization should (except i f complications a r i s e ) enable t h e p a t i e n t t o leave t h e h o s p i t a l wi thin th ree weeks a t most and t o continue a t home, o r i n a convalescent home, a programme of gradual r e - education.
The majori ty of p a t i e n t s w i l l benef i t afterwards by n period of more in tens ive re-education. Subsequently, maintenance treatment may be i n s t i t u t e d , on a permanent bes i s , i f possible.
Systematic psychological inves t iga t ion i s s t i l l a sub jec t o f d iscuss ion i n regard t o t h e methods t o be used; but t h e contact of t h e psychologist wi th the p a t i e n t and h i s family produces t h e b e s t r e s u l t s . Soclo-economlc bencr i t s a r e obvious ana tne re tu rn t o worn Is more frequent i n r e h a b i l i t a t e d p a t i e n t s than i n con t ro l subjects . This dynamic a t t i t u d e towards myocardial i n f a r c t i o n s w i t h a favourable cl inical . course i s sometimes d i f f i c u l t t o apply i n view of t h e p a t i e n t ' s anxiety, h i s 2 ~ a r of t h e a t tending doctors, and t h e s o c i a l organization.

EN/~ard .~asc ./j
EM/PRv,IW. CARD. VSC . D I s / ~ ~ page 23-
On thc o t h e r hatlit, somi2 probl :ms hnvc not been ~ l u c i d a t e d so f a r ; these a r e t h e o p t i n a l durzt ion anc? i n t e n s i t y of pliysical re-educztion programmes, the nccd r'or s t rdctUre1 z c t l b i t y , rncl long-tern11 a a t a on morbidity end r,.orti?.li~g.
Altogether t h c benef i t r of e a r l y m(~Siliz?.tion t o avoid muscular catabolism, thromboembolic mp1ication.- and I n r a i s i n g t h - morale of t h e p a t i e n t and rcaseui-in& l l s re--ntivir; , f a r ol~tweigh t h e poss ible disadvantages of such mnnegtmznt rlf pat i e n t s v ~ i t l i acute myocardi-1 i n f a r c t i o n .
I n p a t i e n t s who hava recovered fiWV a c u t ~ myocardial. i n f a r c t i o n 1% has becom custonnry t o c>c)nLraol ~lrlil L r t i ~ L 11~pe;'1'~~'ilbi~11,'~~ilbiutl, hypc~- l ip . idz~- mia, obesi ty o r physiccl i r s c t i ~ i t y ~ ~ r - d smoking. One has t o be renindcdz however, th2.t resul--,s of secondary prevention t r i a l s have been l a r g e l j negative i n t h s t they havc rLot resu l t ed i n marked reduction ol" deaths o r of new i n l n r c t i o n s , Sov'e e p i 3 e ~ i o l o g i c a l s t u d i e s ind ica ted t h a t t h e prognostiz value of tint> mcljo, fie': f ac to rs , including e levated serum cholesterol, bucomes ; f l~ch lowcy cL"ter t h e accident has occurred. A poss ible explanation i s t h a t the ~ a t l e n t s nlready heve, by d e f i n i t i o n , myocardial dcrxgc 0," v z q i i n ~ degrec and t h i s overr ides t h e weight or" f a c t o r s re levant bccorc t h e rir;t c l i n i c a l manifestat ions of t h ~ disease .
3.4 Medical v e ~ s u s s u r g i c a l .trzatmeni
The ~ r i n c i p l e s have been ou t l ined i n the document presented by Professor H, Denolin c n t i t l e d Ircatmcnt end Rehab i l i t a t ion o f Ischacmic Heart Disease, Present Trend, (Anncx X), and f u r t h e r views werc expressed by the p a r t i c i p z n t s .
Apart firom n!.troglgcenin c vi t rol -as nc:l beta adrenergic blockers, the value of o t h e r so-ccl.1t.d ~ O r o i l Z i ~ va.:od:Llators i s not es tabl ished, Thc va r i ab i l i t y i n rssponso of pationku with 3ne;itl.a t o different ~3n1~;s was emphasizecl andmzi- be relnteci t o cuLtu;-21 p a t t e r n s o r ind iv idua l r eac t ions t o sxpressing pa:;, , C! inicn.!. cxpe~ienct , a l s o i n d i c a t e s t h a t hypotensive d-rugs i n pzticni;; :r?-t.11 zng3nn and r c i s e d blood pressure do not p r e c i p i t a t e ischaemia or- ac:l.-:;> myoc;lrdicl infarc t ior l .
Discussion on s u r g i c a l t r e n L lent or ischnemic h e a r t diseasc, aiming t o r e l i e v e t h ~ isckL2,e.?ia wi th venous g r n f t s ("coronary by-pass") showed t h e t tlic over211 mor te l i ty v z r i c s between 1-10 pcr cant , and it i s obviously 2li:h~~ I n thosc: wi th szverc damage of t h e heapt. Althou[$i symptomtic qii:>jc r t i vc i rlprnvi.,~c.nt. o r cu?-s, thi long-term r e s u l t s a r c not y e t we l l known. Hcncs, i t i s plcmaturc t o judge tlne e f fec t iveness of t h e coronary g r l f t operation befox con t ro l l ed s t u d i e s a r e c a r r i e d out. Angina on e i f o r t rkritli n noimal c o r o n u y angiogram was not considered a s an ind ica t ion f o r operat ive treatment.

EM/Card.Vasc ./5 B$'PRV. W . CARD ,VSC . DIS/17 page 22
WHO am0
Ccronamj angiogrnphy has 3 d e f i n i t e place when opcm t i v e treatment i s contemplated. This method needs t o be supplemented by vcntr iculo- graphy and by o ther methods which assess nyocarcEf~31 funct ion before aaking 2 dec i s icn f o r t h c operative 2.pprozch.
Smoking, obesi ty , hypertensicn, hypcr l ip idaemi~~ and physical i n a c t i v i t y V I ~ P C s t r c s s x l a s major r i s k k c t o r s t h z t a r c monnble t o control .
Diabetcs inell i tus, which i s a major r i s k f a c t o r , was discussed. wi th regard t o i - ~ s vcscular complications. Thcse are , u n f o r t u n a t ~ l y , not prevcnteci by thc con t ro l of d iabe tes mel l i tus . The vasculcr chzng~s and t h e c a r b o h y d r c t ~ metabolic de fec t may be considered a s two para1121 gene t ica l ly :J~tzrniincd disorders .
Sincc th - c t io logy of ischaemic h c e r t d isease appears t o be multi- i"actoria1, thr collti*nl o f a1 1 knnwn ~ h n o r n n l i t i r , . s appears advisnblo . This przgmatic approach howevcr, docs not rcvdal which i'actoT i s more inpor tan t i n 2 given sub jec t o r a populction.
Diet i s r2l~ldas1,ntal t o 211 p r e v ~ n t i v c mcasurcs, Unt i l r t c L n t l y it had btvn acccptcci t h a t reduction o l t o t n l calorie in take, s o as t o balance energy requirements, and r e d u c ~ i o n of f a t intake, p a r t i c u l a r l y nnimcl aatur2tcd fa t , 511ould be sur"Cicicnt , Huwevtr, d i f ~ C L . C I I L Lypds of d is turbances of l i p i d mctabolisn, cxprcsscd, among o ther th ings , by thc prcdomin-nce o: c e r t a i n groups o i c i r c u l a t i n g l ipopro te ins , r t q u i r e m o r ~ spec i f i c ciict2ry indasures, su; ,slernented, ii necc' ;d, by cntilipaer.!ic drugs. I n n trcry schematic way, onc may r1:commend a d i e t wi th low f 2 t content i n groups I, 112 and IIb. I n sub jec t s wi th l i p o p r o t ~ i n typos 11, I V and V, onz has t o limit, prcfcr,?.bly, carbchydratas.
With rcgai?!. t o 2.ntilipaemic drugs, i t sczms t h c t r e s i n s inf luencing 2bsorption oP i~.t Iron the i n t e s t i n e , such as cholestrynminc, :ze preferable i n sub jec t s ~ 5 t h type I1 l i p o p r o t e i n pa t t e rn , and c l o f i b r z tc end n i c o t i n i c x i 3 mong types 111, I V and V; c l o f i b r a t e a l s o i n type IIb. I n thd r a r e type I, d i e t nlcnc i s s u l M c i e n t .
Antilipccmic i m g s a r e h i n d developeJ f a s t d r than proper c l i n i c s 1 evaluation can So m z d ~ of t h e i r thernpcutic o f l i cacy , to lerance and t o x i c i t y over l c n ~ pcriods of time. Study of a small number of sub jec t s fur a f e w w ~ ~ 1 . s w i l l cbci~ionstrate thc: blood l l p i d rcduclng e r f c c t . Ufi
t h e o ther hcnc?, ncquiring proof a s t o ~ . ~ h e t l l c ~ thcg w i l l eventually rcducc -chc i n c i d ~ n c c of ischaemic h e m t disczsu i n populations i s n pains- taking, complicated, tine-consuming and o f ten f r u s t r a t i n g study f o r severa l yecrs . I n ;his sense one Lizs t o regard present population t r i a l s a s p ionoer in ,~ vrork pnving the way Tor fu tu re preventive a c t i o n c a v ~ r i i ? ~ t h e t o t a l conmuni ty.

WHO EMRO
The evolution 02 a the rosc le ros i s from childhood and t h e cumulation of predisposing f a c t o r s wi th age suggest t h a t prevcntivc measures should i d e a l l y s t a r t i n childhood. They should bc o r ien ted pr imari ly towards proper n u t r i t i o n cnd towards c rea t ing optimrl condit ions f o r t h t physical and mental development of every c h i l d an?. adolescent. Before coming t o t h i s point , we must however f i r s t of n l l l e a r n f a r more about t h c e t io logy of a the rosc le ros i s , as wel l a s about the mechanisms leading t o acutc ischaemic h e a r t d isease and sudden death. The f irst requirenicnt f o r prevention i s the re fore more in tens ive research i n t o the metabolic processes involved i n atherogenesis.
For h igh r i s k subjects , or-e needs b e t t e r and simpler mcthods of diagnosing coronzry a the rosc le ros i s and l n t e n t ischaemic h e a r t d isease . Coronary angiography o r t h e mecsurement of cardiac funct ion during maximal o r sub-maximal workloads a re not y e t s u i t a b l c methods f o r screening l a r g e population groups. The3 are , of course, very u s e f i l t o o l s f o r d i f f e r e n t i a l diagnosis of sub jec t s wi th evidence of r i s k o f d isease , before deciding on morc radica, treatment than d i e t and drugs.
A s genercl advice, it becomes morc and more important t o put every e f f o r t i n t o increas ing t h e pkysical 2nd mental f i t n e s s of youth. Increased aerobic worlring captc i ty , ~ v i t h lower h e a r t r a t e and blood pressure c t t h e given workloac, a s compared wi th u n f i t persons, can place them a t a highex- l e v e l of heal th . This may be an important source t o draw upon lator during a d u l t l i f e , bc it i n connc~don with cging, o r on t h e occasion of a. cnrdiovascuiar accident. It i s much morc d i f f i c u l t t o a l t e r 1 i f e . h a b i t s o r a d u l t s than t o continue those which have become a p a r t of d a i l y rout ine s ince childhood. One may go so f a r a s t o s t a t e t h a t medicine today pays n veqr heavy t a x f o r neglected education i n t h e family and a t school. Again, t h i s i s connected wi th ignorance on how t o measure andhow t o promote optimal heal th .
Epidemiological, c l i n i c a l and experimental research over t h e p a s t twenty years has brought about, recognition of the s i t u a t i o n and has changed our a t t i t u d c s . Ischaemic h c a r t d isease i s no longer an inev i - t a b l e consequence of aging; it can be wel l t r e a t e d and in tens ive research i s going on i n a l l cont inents on how t o decrease i t s frequency.
We need now more in tens ive inves t iga t ions on t h e b e s t preventive measures ad jus tcd Tor age i n persons w i t h high r i s k . We need s t u d i e s on the optimal development o fhez l thypersons from childhood, wi th s t r e s s on health rathcr tlmn on disease. We ncod alao inves t iga t ions 011 t l x adapta t ion of man t o man's c i v i l i z a t i o n .
I n order t o motivate ind iv idua l s t o a c t i v e l y s t o p smoking, change d i e t , o r take p i l l s , it i s necessary t o mike them aware of t h e presence of a h e a l t h problem. This is a very d i f f i c u l t task . Besides t h e psycho- l o g i c a l inf luences t h a t might f o l l o ~ i e f f i c i e n t treatment, drugs have s i d e

EM/Card.Vaoc ./5 EM/PRV .MJ . CARD .VSC . D I S / ~ ~ page 24
WHO EMXO
e f fec t s . This could a l s o be s a i d of changing d i e t and cessa t ion of smoking (e.g. weight increase and mental d is turbance) .
The motivction of changing r i s k f a c t o r s can be increased by h e a l t h education i n thc form of t a l k s , various audiovisual a ids , information booklets and group discussions. One way of g e t t i n g feedback i s t o supply d e t a i l s on t h e change i n r i s k f a c t o r s brought about by treatment. Blood pressures can be measured by t h e sub jec t s themselves, cho les te ro l values can be revealed rout inely , and t h e blood concentration of carbon monoxide has been shown t o r e f l e c t inha la t ion of tobacco smoke.
5. Recommendations
5.1 In tens ive ca re
( i ) CCUs should be es tab l i shed i n major u n i v e r s i t y and government h o s p i t a l s i n t h e Rcgion, t o s e t an example f o r the most appropr ia te treatment of p a t i e n t s wi th acu te myocairlial i n f a r c t i o n , f o r t r a l n i n g of personnel and l o r research inves t iga t ions .
( i i ) I n o r d m t o reduce e a r l y mor ta l i ty before hosp i ta l i za t ion , t h e poss ible r o l e of mobile in tens ive care u n i t s should be inves t iga ted i n places where CCUs e;:ist.
( i i i ) WHO should arrange a r e g i o n d t r a i n i n g programme t o i n i t i a t e t h e concepts of coronanj ca re management i n t h e Rcgion. This should encompass a l l concerned wi th cardiovascular d iseases , i .e. physicians, nurses, technicians. The t r a i n i n g of nurses i s espec ia l ly important. A regional t r a i n i n g c e n t r ~ should be es tab l i shed and serve the coun t r i es t o devclop t h e i r own t r a i n i n g programme. An in tens ive four-week course combined wi th i n - s e r v i c t t r a i n i n g of about s i x months durat ion has proved i t s value 1/2.
5.2 Rehab i l i t a t ion
While up-to-date treatment of p a t i e n t s wi th acute myocardial in fa rc - t i o n i s usua l ly provided, e a r l y r e h a b i l i t a t i o n is of ten not considered, The advantage of e a r l y mobilization of the p a t i e n t f a r outweighs t h e poss ible harmlZll e f f e c t . It i s the re fore recommended t o organize regional t r a i n i n g courses i n r e h a b i l i t a t i o n of p a t i e n t s wi th cai~diovascular d i seases i n general , and, recovery from acute myocardial i n f a r c t i o n i n p a r t i c u l a r . ' I l ~ e t r a i n i n g courses should include p r i n c i p l e s of psycho- l o g i c a l and ghy-sic31 training, ass~ssment n f working capacity, and e w l u a t i o n of s o c i a l and vocational mensures.
5.3 Prevention
Heal thier l i f e h a b i t s , con t ro l of outstanding r i s k f a c t o r s and.of underlying condit ions (diabetes , hypertension, e t c . ) a r e p a r t of t h e
-- u u l i a n , D.G., Oliver, M.F. (1970) Manual of Coronary Care Units, WHO Regional Office f o r Europe, EURO 5020(2) .
ROCO OM system developed by D r Melizer and Miss Pinnss f o r the US Public Health Service.
:~llnazcment cf 2 c t i c n . i ~ VLQO have recovered from ncuti: myocardial i n f a r c - t ion . R e w l a r fcllor!-up i s necessary t~ cxhiuve this. The un lTic r s i ty ccntrcs i n the atig-isn shculd be encouraged t o spread t h i s knowledge of sccondc?.ry provzntion i n t r a i n i n g coui7ses f o r physicians and nurses, F a c i l i t i e s p r c v i d d Sy na t iane l a~ l . thor i t i c s could be enhanced (exchnng;: o.? ideas bo%i.r;i;n coun t r i es of s i m i l a r c u l t u r a l background) . 'dHO should a s s i s t 0r.g-nizctioc of such t r a i n i n g f o r which a fund of teaching n c t e r i a l i s cv?.il?-%la.
Althcush L ~ L c t i o l o a ~f a thorosclLyosis and of ischaernic h c m t ' i sbasu hcs not bcca fUll:r c l a r i f i s d , t h c present evidence po in t s c le? r -
l : r t o tbc tn2t2,-: LOr n3?;lGn7dlCi,: Inicmlntlon ,-[LO. crivicc to tlic publ ic . 215s ri12tLs p a r i i c ~ l - r l y tc d i e t , wi th m:)d,ration i n c a l o r i c in takc re lcvant lo physical n c t i v i t y , and i n pa r t i cu l - r rkduction 02 t h e propcr- ion of f a t i~ t h e C E L L . It r i l ~ t c s to tlie e l iminat ion of cigarette smoking from youth, and -.rnphasizes t h e inpor tanct of b ~ t t e r pliysicnl f i t n e s s l o r liL?l th.
Collcction o f 22-ucational mntcr iz ls , and txchange o f such inyomat ion i n t h e Region snoulJ be facilitated by WHO. Countries a r c encouragid t o i n t ~ n s i f y t h c i r t P i o T t t o increase -the knowl~dge of tha public on how t o prcnot i be t tuF h ~ z l t h .
A s i n o t l ? ~ r ? a r t s o f the world, cardiovasculnr d i seases represent n rfl2 jo r public he-ltli p r o b l ~ n i n the R ~ g i o n . Howcvcr, from preliminary' r epor t s it i s ? p p z r ~ n k t t h n t t h e r ~ i s p e n t i l ivc r s i ty among ' i i e c o u n t r i ~ s i n the r e l a t i v t ir?portance of ca rc l i cv~scu lnr cLi.seascs t o o the r d iseases , 2nd t h a t t h c r c a r t vz r ia t ions i n the r e l ~ . t i v b frociu~ncy of czcll k ind o i cardiovascular discaso. It i s of mz j o r ir,iportancc the rc f ore t h a t cf f o r t o b~ roc.cl; -60 oSi;nin r c l i a b l o data cn tlid occurrence o f ca r i iovnsc l l~ r J-
J i seases i n t h c coun t r i es of the R ~ g i o n and on tna burdens t h z t they inpbsc.
The coun-crics of t h e a rea , wi th t h e clssistance o f PfiIO, should emplo:~ the dxperience of c t h c r regions which hcva a l ready published user"u1 rccomrnendations f o r t h e insthods by which i n f o m a t i o n may be o b t a i n c ~ l ~ L I
t l i t m3gnitudL arS. ncturc of t h e problca.
An efPcct ivL wc;. t o b tg in would bL, a s ~ l s e w h e r e , t o focus on xis sting progranlaes i c countr ies of t h e R ~ g i o n which izavci been usei'ul nlrendy i n rLxvt -n l i n g ::h(- prc!)lt.ms requiring a t t e n t i o n of ~ h y s i c i a n s and h e a l t h 2 u t h o r i t i L s . D ~ r i n g the c o u r s ~ 03 the serninar c number of such pro,;rmia~s hcvc demonstr?.tcd t h ~ i r p o t m t i a l t o produce valuable infomct ion.
Therc i s a ncui t o mobilize and un i fy wi thin t h e c o u n t r i ~ s of the Rcgicn thosi? rrorl~ers srhosc e f f o r t s h n v ~ be& iiost committed t a i z r d the
EM/Card.Vasc ./5 EM/PRV.W. CAW). VSC . D I S / ~ ~ page 26
WHO EMRO
s o l u t i o n of thcse problems. It is recommended t h a t each country promote such e f f o r t s by forming a na.tiona1 committee f o r t h e prevention of major cardiovascular d iseases . Such committees might include:
( a ) Univers i t i e s and teaching c l i n i c s deal ing wi th research and se rv ice programmes i n cardiov?.scular d iseases .
(b) Health p r o f ~ s s i o n n l s whose a c t i v i t i e s a r e concerned wi th cardio- vascular d iseases , cog . ca rd io log i s t s , paed ia t r i c ians , surgeons, nurses and a l l i e d h e a l t h workers.
(c ) Health a u t h o r i t i e s of l o c a l and. na t iona l governments.
(d) National s o c i e t i e s of cardiology, and o t h e r re levan t profess ional organizations.
( e ) Voluntary h e a l t h organizat ions , public s p i r i t e d c i t i z e n s , inclus t r ia l and commercial en te rpr i ses .
It is recommcnclcd t h a t i n c lose co-opcration wi th na t iona l h e a l t h a u t h o r i t i e s such committees be es tab l i shed i n 1973 and fd-nt WHO be informed about t h e i r existence and plans.
The count r i es o f the Region should explore immediately t h e sources of read i ly ava i l ab le information (even i f thcy a r e of l o c a l character) w h i c h m a y rovonl information on tho ooourrcnco of c a r d i o v a ~ c u l a r diacnaco. These could include h o s p i t a l morbidity and. mor ta l i ty s t a t i s t i c s , information from spec ie l i zed cen t res end programmes, such a s coronary ca re u n i t s , rs fercnce l abora to r ies , c t c .
The resources t o d e a l wi th t h e problcms of t h e Region should be assessed wi th regercl t o t h e i r qua l i ty , p o t e n t i a l f o r expansion, and ns ins txwnurlts i u r d~vulupir lg br'uadcr' progrummes f o r the con t ro l of cardlo- vascular d iseases . Cardiological and. paed ia t r i c wards and services, coronary ce re u n i t s , hypertensive c l i n i c s , myocardial i n f a r c t i o n d i s - pensaries, IYnewnatic fever prevention programmes, school h e a l t h services , and s i m i l a r rcsourccs should bc reviewed and plans be made f o r t h e i r optimum u t i l i z a t i o n before attempting t o e s t a b l i s h new a c t i v i t i e s .
Though exce l l en t cen t res a r e i n operation i n a number o f coun t r i es o f t h e Region, it i s f c l t t h a t t h e i r a c t i v i t i e s should be expanded and i n t e n s i f i e d i n ordzr t o cover g r e a t e r numbers of pa t i en t s . These progmmrnca ahould c o m m e the r o l e of "ccntrcs of excellencc", empl~as i t i ng t r a i n i n g i n cdd i t ion t o model medical ca re and research.
For thc next l i v e years, t h e primary t a r g e t should be the e s t a b l i s h - ment o f e f f e c t i v e rheumatic fever prevcntion programmes i n a l l coun t r i es i n t h e Region.

WHO m o EM/~ard .Vasc ./5 EM/'PRv. w . CARD. VSC . ~ 1 S / 1 7 p2ge 3
It is a l s o urgent t c develcp facilities and cen t res f o r adequate clingnosia, and cnrc 02 ca~diovnscular cmci-gcncics such aa acutc m y o - c a r d i a l i n f a r c t i o n and stroite, a s rvcll a s ?or r e h a b i l i t a t i o n of p a t i e n t s .
The r o l e of hypertension shoulrl bc xcognized and p u b l i c i z ~ d a s a p o t e n t i a l l y prcvcntablc cause of s t roke, cardiac and rena l f a i l u r e , and a s a se r ious complication i l ? pa t j e n t s with a therosc le ros i s . The cur ren t e f f e c t i v e trectment i o r low-.;oin,.- ~Loocl brLssurc therefore c a l l s a t l e a s t f o r t h e devclopmcnJc of p i l o i pTcgr?Jhncs Ln t h e Rc-gion t o a t t a c k t h i s a spec t of prevention of czrdiovascular c iscases .
Rcfl .dct ing n tzorld-wide r ;~c.nC, inan?owir is short in a11 health professions. This shorts:? i s accentcated by the emergence of cardiovascular d i scascs a s a major hecLth problem i n t h e Region. Thcre- fore , na t ionc l ,?uthorit i t .s should ns6rzn n very high p r i o r i t y t o t r a in ing . Systematic t r a i n i n g programmes a r e iu;o~'cly needed a t a l l l e v e l s , such a s a u x i l i a r y personnel, nurses f o r i cxns ivc : ca re u n i t s , f i e l d nurses, l abora to ry technicians, czrdiologis ts , c~.rcliovc?.scular d i sease cpidemio- l u g i s t s , etc. V a l - i u ~ ~ s fvixls uf t ~ - c t L i l i ~ ~ g s11uuld be ubed buch t r a i n i n g i n spec ia l i zed i n s z i t u t e s &road, v i s i t i n g consul tants , exchange fellowships, e tc . Specic l a t t c c t i o n should be paid t o t h e develop- ment of t r a i n i n g cen t res wi th in t h ~ 3egion i t s e l f , us ing regional resources and t h e advnntzges oi' t h c -.bsence of language b a r r i e r s wherever poss ible . Exchange t r a i n i ig i s rcc ommendcd on na t iona l , b i l a t e r a l , and m u l t i l a t c m l l e v e l s . I n cases -vlzerc spec ia l i zed teams a r c e s s e n t i a l (e.g. CGU) t h ~ t r a l n l n g 01 t h e t e a l 2s a Vrhole should be considered.
WHO should assume the respons ib i l i ty for co-ordinating and promoting such t r a i n i n g a c t i v i t i e s an6. consider t h c establishment of regional cen t res t o be en t rus ted wi th the de ; rdop~e i i t of these a c t i v i t i e s .
A s improved measures h v e be con^ ava i l ab le f o r t h e con t ro l of cardio- vascular d iseases , t h e gancral p~b1i.c rnlrst be w e l l informed i n o rder t o p a r t i c i p a t e i n , anct supFort, ~ h e s c e f f o r t s .
WHO i s i n v i t e d t o a s s i s t and t o cctc?lyzc contact between various =search cen t res which have olrcr?dy bcc-n recognized i n t h c Region. Periodic inTomat ion on achicvcn~en-ts and progress i n the f i e l d should be c o l l a t e d and disscminntc;d bg WHO, Apart from e x i s t i n g WHO publ icat ions (World Health, Chronicle, BJI-lctin, Press Releases, e t c .) , it i s recommended t o publish from time t o t i n e 2 L u l l ~ t i n on Cardicvascular Diseases i n the Middle East on achicv~ments and progress i n t h e coun t r i es of t h e Region.
The mul t ip le t a sks irnposad by cardiovascular (and o ther chronic) d i seases i n t h e Region prescnt increased r c s p o n s i b i l i t i c s f o r WHO.
The organizat ion i s a l s o i n v i t e d t o expand i t s a c t i v i t i e s and t o increese i t s potcnt i31 i n the f i e l d of chronic d i seases i n t h e Eastern Medi tcr ranean Region.
E P . I / c ~ ~ ~ .Vcsc ./5 BJI/PRV.MJ. C U D .VSC . D I S / ~ ~ page 28
WHO EMRO
Final ly , i n view of t h e increas ing importance 02 cardiovascul,?r diskases, it ia rccouncnd~d t h a t znc tho r confcrencc s h n i ~ l d hr plann~; within t h c nc-;;t thrc , years . A t t h i s meeting a l l rnajor c a r d i c v ~ ? s c u l ~ . r d isecses i n t h i coun t r i es of t h e RL-gion shculd be tliscussed. Ifi
ackliticn t o rheumatic P L V G ~ , hypertension and ischaemic h e a r t d iscasc , h e a r t d i seases resulting frcm pulmonary cliscascs, congenital rnalformatic,n.; cn3 S ~ P C ~ J a l s c dcscrv, a t t en t ion . Pcr t i c ipa tns should r a p r c s ~ n t s ~ v e i ~ l Ciisciplines involvad i n the f i g h t aga ins t c2rdiovascul2r d i s a s ~ s - card io log i s t s , paecii2b t r i c ians , opiclerniolcgists, bac t c r i o l c g i s t s , an2 ~ ~ g a n i z e r s of public 1 1 ~ ~ 1 t h act ion. It would therefore be zpproprin.t, t h a t sevcra l pa r t i c ipnn ts be d i l cga ted b;: x,ch government.
Further~lo'e, more frequent mectings of various kincls shoulJ. b~ ccnvcncd, pnr t i cu ln r ly i n connexion wi th p i l o t s t u d i c s undi.rtaken i n ' c ! ~ Region.
WHO EMRO EM/Card.~asc ./5 EM/PKV .MJ .CARD .VsC. DI S/17 Annex I
A N N M I
AGENDA
Opening Session
Election of Seminar Officers (Chairman, Vice-chairman and ~appor teu r )
Problems of Ischaemic Heart Disease
a. Epidemiology of ischaemic heart disease
(i) General problem ( i i ) Ischaemic heart disease i n the Region: country reports
on size or" the problem prevalence, natural history, incidence.
b . Treatment and rehabil i ta t ion
(i) Present trends ( i i ) Situation i n the Region: this should include services
available f o r acute care, surgical treatment, rehabil i ta t ion, registers , e t c .
c. Prevention
( i ) Present s ta tus (individual and corrnnunities) ( i i ) Discussion: this would include early diagnosis, mass
screening, control of predisposing factors , heal th education
Acute Rheumatic Fever - prevention and treatment. Rheumatic Heart Disease
Hypertension i n general and i ts relat ions with ischaemic heart disease
Field v i s i t s
mar' report and Recommendations

WHO EMRO
BAHRAIN
CYPRUS
EGYPT
~M/Card .Vast ./5 EM/~RV. MJ .CARD. VSC .DI 8/17 Annex I1 page i
ANNEX I1
LIST OF PARTICIPANTS
Dr Mohamed Feghoul Professor (agr8g6) University Hospital Centre of
Algiers Service of Cardiovascular Diseases Algiers
D r Akbar Mohsen Mohamed He ad Department 02 Paediatr ics Ministry of Health Bahrain
D r V a ~ h b Kalbian Specia l i s t Physician and
Cardiologist In t e rna l Medicine Section Ministry of Health Nicosia
Dr Abdel Aziz E l - m r i f Professor of Cardiology Cairo University Cairo - D r A l i Abd E l Magid Ramzy Lecturer of Cardiology Ain Shams University Cairo - D r Mohanaed ~ a ' ad El-Din Salama Cardiologist Minia General Hospital El-Minia
D r Abdel Emam Abdel Meguid Senior Registrar I n s t l t u t e of c;arctlotnoraclc Surgery Embaba .. Cairo
I%M/card.~asc ./5 EM/PRv .MJ .CARD .VSC .DI s/17 Annex I1 page ii
ETHIOPIA
WHO EMRO
U r Fikre Wolde Georgis He ad Department of Intelrnal Medicine
of Menelik I1 Hospit a1 Addis Ababa --
DT Mulouchehr Nadimi Director Department f o r Control of Heart
Diseases MiniStr?,T of HealLl Teheran
D r Mehdi Mahdavi Director Division fo r Paediatric Cardiology Fir0uzga.r Medic a1 Centre Teheran Medic a1 School Teheran -- D r Reza A m i r i Gharagozlu Associate Professor Faculty of Public Health University of Teheran Teheran
D r Daneshpajouh Rssearch Associate of t he
Faculty of Public Health University of Teheran Teheran
-Dz Ahmad Mostashar Associate Professor University of Teheran Teherm
D r Ihsan Al-Bahrani Cardiologisk Medical City Teaching Hospital Raghdad
D r Nie' amat Fadhi1 El-Sahar Cardiologist Y arm0u.k Hospi t a1 Baghdad

WHO EMRO
JORDAN
LEBANON
LIBYA
~ M / C a d . ~ a s c ./5 EM/PRV . M J .CARD .VSC . D I S / ~ ~ An:lex I1 page iii
Dr Isam Ibrahirn H i g a z i * Director Amman Civi l Hospital Amman - D r Zakaria Parid Ijaoud Cardiologist Chief of In terna l Medicine
Department Ministry of Health A m m a n - D r Abdul Mohsin Abdul Razzak Al-Yusu; Head Cardiac Department Ministry of Public Health Kuwait
D r Abdul Razzak Al-Yusuf .Assistant Under-Secretary f o r
Technical Affairs Ministry of Public Health Kuwait
D r George Ei~drys '' Consultant Cardiologist Ministry of Public Health Kuwait
D r Edouard Stephan Chief Medical OTficer Baabda Hospital Baabda
D r Riad Tabbarah Professor of Medicine Chief, Department of In terna l
Medicine Beirut
D r A l i YousseP Misherghi ~ l r e ~ t ~ r - ~ e n e r a l Central Hospital In terna l Diseases Department and
Chairman oL" the Medical Board Tripoli
*did no t attend

EM/card .V=C ./5 EM/PRV .MJ .CARD .VSC .DIS/17 Annex I1 page i v
MOROCCO
SAUDI ARABIA
WHO EMRO
D r Belkacem Bellouchl Chief Service of Cardiovascular Diseases - - -
Al-Ghassani Hospital Fez - Dr Abdul Hafeez Akhtar Associate Physician Central Government Hospital Rawalpindi
D r Abdul K a r i m Abbassi Assistant Professor Liaquat Medical College Hyderabad
D r S.M. Malik Assoclate Physlclan Central Government Polyclinic Islamabad
D r Allah Bux Khan Physician Sandeman Civi l Hospital Quetta
D r Soliman Abdel Kader+ Pathologist Director of Health Affairs Jeddah
D r E l Nur Abdel Mageed Cardiologist E l Shaab Hospital Khartoum
D r Mohd Hassan Gabir Cardiologist Khartoum Hospital Khartoum
D r Ghazi Ketabi Soubhi He ad Department of Cardiology Damascus Hospital Damascus
- *did not attend

WHO EMRO
YEMEN
EM/Card.~asc ./5 EM/PRV .MJ .CARD .VSC .DIS/~~ Annex I1 P a 9 v
Professor Ben Ismail Mohamed Senior Lecturer (agrdgd) Tunis Faculty of Medlcine Chief, Service of Cardiology Ernest Conseil Hospital Tunis - D r Orhan Balkan Chief Clinician Degartment of Cardiovascular
Diseases Numune Hospital mars D r A l i Mahdi E l Ansi Cardiologist Ministry of Health ~ a n a ' a
OBrnVERS FROM HOST COUNTRY
D r Ghassem Shafi-Zadeh Associate Professor D e p s t n ~ e n t of C a - d i ac D i sewc Pahlavi Medical Centre Teheran Medical School Teheran
D r Behrouz Khadivi Associate Professor and Supervisor
of Training Department i n ln ternal Medicine
Faculty of Medicine Meshed University Meshed
D r M .A. Naghshineh Associate Professor Cardiovascular Diseases Faculty of Medicine University of Tabr io Tabri z -

EM/Card. Vas c . /5 EN/F'RV.MJ. CARD .VSC .DIS/17 Annex I1 pa@;e v i
WHO EMRO
OBSEFIVERS FROM HOST COUNTRY (cont 'd)
D r Morteza Amidi Associate Professor and Cardiologist Faculty of Medicine Pahlavi University Shiraz
D r A l i ~awab* Vice-Dean Faculty of Medicine University of Isf ahan Is f ahan
D r Manouchehr Ram-Ara Associate Professor of Cardiology Faculty of Medicine National University of Iran Teheran
D r Mohammed Kamkar Associate Professor Faculty of Medicine Jundi Shahpour University Ahwaz
D r Geni Parandeh Cardiologist National Iranian O i l Co. Hospital Health Department and Health Division Teheran

EMRO EM/~ard. Vasc ./5 ~ / P R V . M J . CARD.VSC. D I S / ~ ~ Annex I1 page v i l
REPREXEXTATIVES FROM OTHER UNITED NATIONS BODIES
M r N. Sha!.lon Eesident Representative United Nations Development Progr'amme Teherrn --
M r Nasri M. Rashed United Nations Information Centre Teheran
RE PRESEITAT IVES FROM OTHER ORGANIZATIONS
D r A. Sorour The Egyptian Society of Cardiology Cairo - EGYPT
D r Ahrnad Mostashar Iranian Society of Cardiology Teheran - -- -RAN
Pi~wI'assur. H. D e r l o l i r l The Intcrnatj .ma1 Society of Cardio! ~ 5 ) ~ Geneva SbJITZERLAND
Zi8j/Card.Vasc EN/PRV .r41J .CAN) .VSC .DIS/17 Annex I1 page v i i i
N-IQ SECRETARIAT
D r T. S t rasser
D r G . Ti bblin
Director
Cliief, Cardio- vascular Diseases Unit
Regional I~dviser on Organization of t.ledical Care - Secretary of the Seminar
Medical Officer Cardlovascular U n l t
VJHO Consultant
D r G .H. Stollerman Temporary Adviser
Proressor P. Milliez Temporary Adviser
Professor H. Denolin Temporary Adviser
D2 G . Slorilan Temporary Adviser
D r A.H. Sorour
bk J . Simon
Temporary Adviser
Public Information Officer
WHO EPilRO
Regiolial Office io? Lie Eastern PiIediter2ax1csul
Regional Off ice fop ;i a
Eastern Mediterranean
Physician-in-Chie;, Fac11it;r oi Medicine, Universi-hy 02 G'dteborg, Sweden
Proiessor and Chairman, University of Tennessee, Department of Medicine, USA
Proi'essor of Medical C15:.4c Hospital Broussais - Par is 14th - Prance
Cnief, Department o i Cardiolo&y, Hospital Saint P ie r re - Brussels; Belgium
Cardiac Department, Royal P.lelbourne Hospital, V i c t ~ ~ i a - Austral ia
Processor, Vice-Chancellor, Cairo University, Cairo, E,y:2t
Regional OPTice f o r the Eastern Mediterranean
WHO EMRO
WHO SCRETAFUA!T (conttd)
Conference Service
Miss C .L. Cartoudis Conference Officer
Miss F. Genevrier Translator
Mrs I. Sakov In t e rp re t e r
Mrs E. Berger In t e rp re t e r
Mrs M. Saad In t e rp re t e r
M r P. Lambert In t e rp re t e r
M r s E. Rizkallah Secretary
Mrs I. Farid Secretary
EM/c ard .Vasc ./5 EM/PRv. CARD .VSC .DI s/17 Annex 11 page i x
Regional Office f o r the Eastern Mediterranean
Geneva, Switzerland
Geneva, Switzerland
Geneva, Swltzerland
Alexandria, Egypt
Geneva, Swltzerland
Regional Office f o r the Eastern Mediterranean
Regional Office f o r the Eastern Mediterranean

FN/~ard .Vasc ./5 EM/PRV .MJ. CARD .VSC r D I S / ~ ~ Annex 111 page 3.
ANNEX I11
CARDIOVASCULAR DISEASES I N COUNTRLES OF 17IE REGION
1. Algeria
No comprehensive nat ional data on the occurrence of cardiovascular diseases a r e available, but data from the Algiers University Hospital may be considered a s f a i r l y representative, a s t h i s hospi tal admits pat ients from the whole country. Rheumatic hear t disease is the leading cardiovascular disease, It occurs a t a young age, involves usually more than one valve, and a t t a i n s ear ly stage I11 and I V of NYHA c lass i f ica t ion . Recurrences a r e frequent, mostly due t o inadequate treatment of the f i r s t a t tack and t o the absence of prophy- l ax i s . Congenital hear t disease i s found i n 0.8 per cent of the population. Ischaemic hear t disease i s r e l a t ive ly rare, but seems t o be on the increase i n recent years. Hypertension accounts f o r 4.3 per cent of pat ients hospitalized f o r cardiovascular discnses , This number, however, undervalues the t rue significance of the disease, a s i t includes only the most severe cases.
2. Bahrain
The population of the s t a t e of Bahrain is 216 000. The government hospi tals provldc health care t o the ent i re population. About 90 per cent of t h i s population is admitted t o the government hospi tals .
The data col lected from the hospi ta l r eg i s t e r s of admissions during 1971 rcvealed the following: t o t a l admissions t o the medical wards, both sexes, wore 2 197; there were 225 cases of Ischaemic Heart Disease (10 per cent ) ; ninety-five cases were diagnosed as oercbrova~cular diseases (cerebr7al luemorrhagc + thrombosis), for ty- three cases out of the above two categories were diabet ics; for ty-s ix cases were diagnosed a s hypertensive hear t disease. Adding t o the above admissions those admitted t o the p e d i a t r i c wards, the t o t a l figure was 3 368. Only thir ty-nine cases were diagnosed a s rheumatic heart disease and nineteen cases of de f in i t e rheumatic fever.
Unti l now there a re no programmes f o r prevention and control of the major cardiovascular diseases.
Ischaemic hear t disease seems t o be ever on the increase. No accurate s t a t i s t i c s a r e available, but judging from the admissions t o the Department o f In te rna l Medicine a t Nicosia General Hospital, there seems to be a very rapid increase i n cases of ischaemic hear t diseese and myocardial in farc t ion (MI) .
EM/~ard .Vase ./5 EM/PFW.KJ .CARD.VSC.DIS/~~ Annex I11 page ii
WHO EMRO
The t r u e incidence of rheumatic f e v e r (FU?) i n Cyprus i s not known, because no morbidity s t a t i s t i c s a r e kept-RF i s not a n o t i f i a b l e disease . The information cvni lable i s es t imates based on s t a t i s t i c s of small s e l e c t e d groups admitted t o Governm~nt Hospitals , but c e r t a i n l y RF i n t h e form of a saquzl t o chronic rheumatic h e a r t d isease (RHD) i s n problem i n Cyprus.
Again judging from t h e records of Nicosia General Hospital , t h e admission of new cases of RF seems t o have been a r e l a t i v c l y ronstnnt f i g u r e over the l n s t t e n years (1960 - 1970). There were around f o r t y t o f i f t y annual admissions to the pecd ia t r i c department and t e n t o f i f t e e n i n thc Department of I n t e r n a l Medicine.
A l l cases of chronic RHD a r c followed up a t the above c l i n i c s and the re i s an appreciable dec l ine i n readmissions t o t h e h o s p i t a l of those cases o f ch rnn i r RHD who a t tond rcgulcrrly f o r treatment and follow-up. This i s due t o t h e dcorease of recurrencGs of acute RF and a l s o a decrease of cardiac complications due t o t h e i r prompt t r e a t - ment a s outpat ients .
The problem t o be faced now i s how t o reduce f i r s t a t t a c k s of RF and how t o dcnl wi'th o r pick up s u b c l i n i c a l a t t a c k s t h a t present a f t c r many yeam ac chronic mID.
During 1971, a THO Rheumatic Fever Control Programme was es tab l i shed which might r e s u l t i n the accumulation of some r e l i a b l e f i g u r e s and data .
For hypertension, no r e l i a b l e f i g u r e s a r e ava i l ab le e i t h e r , Hospi ta l records i n d i c a t e t h a t chronic rena l d isease i s t h e commonest cause next t o e s s e n t i a l hypertension. No epidemiological s t u d i e s have been done,
I n November 1971 a two-bedded coronary ca re u n i t was es tab l i shed i n Nicosia General Hospital , which serves a population of 120 000. The f i r s t yea r ' s c.xperiencc has shown t h a t two beds a r e t o t a i l y inadequate and probably s i x w i l l bc a. more reasonable number.
4. Egypt
Heart d isease i s common i n Egypt.
Rheumatic h e a r t d i sease i s still t h e commonest d i so rder amongst t h e lower s o c i a l c l a s s e s of the population but hypertension end coronary h e a r t d i seases t o p the list amongst the upper and the i n t e l l e c t u a l c l a s s e s of t h e population.
WHO m o m/carcl.vasc ./5 EM/PRV.MJ. CARD. VSC , DIS/l7 Annex I11 page iii
Rheumatic fever is get t ing l e s s acute and many cases may be label led a s "chronic ,?ctiveU which crcates diagnostic d i f f i c u l t i e s . Established rheumatic hear t disease occurs i n younger age groups and cases of t i g h t mi t ra l s tenosis below the ngc of f i f t e e n account f o r 2.5 per cent of the t o t a l miCral s tenosis cases.
Coronary hecrt disease a f f ec t s younger age groups of both sexes. Hypertension i s reported t o occur amongst 12 per cent of healthy males above the age of clcvcn years, and i n 10.5 per cent of a random sample of both sexes. The ro l e of urinary schistosomiasls i n the dcvslopment of hypertension ~mongst agr icu l tura l workers has been established.
Chronic constr ic t ive pc r i ca rd i t i s of a tuberculous nature seems t o be on tha increase due t o the adoption of anti-tuberculous agents during the zcute phase.
Pulmonary schistosomiasis cons t i tu tes a quarter of cases of chronic cor pulmonale; emphysema and chronic pulmonary f ib ros i s account f o r the - majority of thc res t .
Cardiovasculrr syphi l i s i s no longer exis tent . Cardiomyopathies a re being recognized and const i tute 2.5 per cent of cases of cardiac h o s p i t a l acimissions r e c e n t l y . Endnmyornrdinl fj hrosi s @xi st.s but. i s evidently rarc; alcoholic cardiomyopathies are , f o r obvious reasons, a lso rarc .
A type of congestive cardiomyopathy with generalized cardiac enlargement, s t r i a l f i b r i l l a t i o n and moderate elevation of i ntracardiac pressure was reported amongst pat ients with l i v e r c i r rhos i s of non- ochiotooomial origin.
5. Ethiopia
Despite the remarkable progross made i n the control of infect ious disease i n Ethiopia during the l a s t tvrcnty-five years, infect ious disease is s t i l l n major problem, and so l i t t l e has been done i n the f i e l d of carcliov~scular diseases. I n general, one can say t h a t cardio- vascular d i ss rse i s not a major problem a t present i n this country.
Rheumatic heart cliscaso is tho most common form of c a r d i a c d i s e a s o c l i n i ca l ly dingnos~cl by physicians working i n Ethiopia. The various manifestations of rheumatic hear t disease i n t h i s country had been well documented by Vukotic and l a t e r by Parry and Gordon, I n t h e i r s tudies they have shown tha t c l a s s i ca l rheumatic f c v w i s not common. Chorea, and nodules arc. not scen and t h a t ery'chemia marginatum i s rare . It was a l so of i n t c r c s t t h a t most of t h e i r pa t ien ts suffcrod from v,?lvular damage w h i l e still children.

EM/Card .Vase ./5 EN/PRV.MJ. CARD.VSC.DIS/L~ Annex I11 page i v
WHO mmo
Hypertension i s a very common d i sorder a f f e c t i n g young a s wc l l a s o lde r Ethiopians. The e t io logy i s s t i l l obscure though we s s c associa- t e d rena l d isecse i n good number of our pa t i en t s .
The well-known assoc ia t ion of hypertension wi th Ischaemic h c a r t d isease is not commonly seen i n t h i s country.
Ischaemic h e a r t d isease is very rr?.rL among Ethiopians. Among 983 cardiac cases s tudied by Vukotic and Parry i n 1968 not a s i n g l e case of myocardial infarctionhas been reported. It i s only recen t ly t h a t authent ic cases of m y o c a r d i a l i n f a r ~ o n w i t h o u t being complication o f d iabe tes e tc . were reported from m a o r h o s p i t a l s i n Addis Ababa.
Pa t i en t s w i t h cardiovascular diseases are f r e ~ u e n t . 1 ~ socn in Tran and a r e responsible f o r about 1 2 p e r c e n t of deaths of pa t i en t s . A survey of about 500 000 p a t i e n t s i n d i f f e r e n t p a r t s of t h e country i n d i c a t e s t h a t rheumatic fever and rheumatic h e a r t d isease a r e the most common type of h e a r t ciiserse (30-45 per cent, of cardiac p a t i e n t s and 3 per cen t of t o t a l paed ia t r i c patients) . Ischaemic h e a r t clisezse (IHD), a r t e r i a l hypertension, and congeni ta l h e a r t d i seases a r c among the l c s s f requent typos. IHD is m o ~ t l y ocen among the hi& and mid s u c i u - economic groups, and includes 7-15 per cent of cardiac pa t i en t s .
I n a school survzy i n Tchcran, congenital h e a r t d isease was found t o have a prevalence r a t e of 3.8 per 1 000.
About 2.5 t o 8 per cent of p a t i e n t s wi th cardiovascular d i seeses have hacl a r t e r i a l hypcrtcnslon .
The c a r r i e r r a t e of haemolytic s t rep tococc i i n I r a n i s about 7.4 t o 13.2 per cent.
About sixty-seven CCU beds are cs tnb l i shed i n I ran , covering about 7 mi l l ion people.
7. I r a q
I n I raq , rheumatic haart disease usud Lu be Lhe leading carcllac ai lment u n t i l few ycars ago when it was noticed t h a t ischaemic h e a r t d isease was taking t h e lead, and t h e s i t u a t i o n i s becoming s i m i l a r t o t h a t which is seen i n t h e Western countries.
The reason f o r this change i s m u l t i f a c t o r i a l , but the most important f a c t o r i s the rapid change of t h e I r a q i soc ie ty from a poor backward a g r i c u l t u r a l soc le ty t o a r e t h e r sopi i is t ica ted i n d u s t r i a l one wi th 3 r i s e i n t h e standard of l i v i n g , b e t t e r incomes and more worries.

WHO EMRO EM/~ard .Vasc ./5 EM/PRV . W . CARD. VSC . DIS/17 Annex I11 page v
Rheumatic h e a r t d isease on t h e o ther hand i s decl in ing i n incidence i n the l a s t few years, the reasons being improvement i n t h e standard of l i v i n g , b e t t e r housing condit ions, b e t t e r medical services , e a r l y diagnosis of rheumatic fever and e a r l y treatment, a s we l l a s b e t t e r prophylactic measures.
Hypertensive h e a r t d isease is s t i l l a b ig problem, but lagging behind ischaemic and rheumatic h e a r t d isease , wi th more o r l e s s t h e same e t i o l o - gical. f a c t o r s a p a r t from one important point - the h igh i na jdence of renal hypertension i n young pa t i en t s . This is a t t r i b u t e d p a r t l y t o poorly t r e a t e d schistosomiasis and ur inary t r a c t i n f e c t i o n s i n ch i ld ren and young a d u l t s which l eads t o chronic phelonephr i t i s and hypertension i n e a r l y a d u l t l i f e and even i n chi ldren, e spec ia l ly i n r u r a l areas .
Cor p l m o n a l c seems t o be t h e same a s elsewhere i n the world and - smokjng h a h j t s , w h i c h a re a p o t o n t i a t i n 8 faotor, accm t o be an i m p o r t a n t one i n I r a q a s very young people and adolescents smoke heavi ly , e spec ia l ly i n v i l l a g e s and r u m l d i s t r i c t s of t h e country.
Concerning treatment and prevention of h e a r t d isease , spec ia l i zed c l i n i c s i n c e n t r a l and teaching h o s p i t a l s f o r h e a r t d iseases , coronary Care u n i t s i n teaching and general h o s p i t a l s , and dingnost ic cen t res equipped f o r cardiac ca ltle Ler-izatlon and anglocardiography were es tabl ished, Country-pride h e a l t h education i s us ing radio and television programmes.
8. I s r a e l
The most prevalent problem i n cardiovascular d i seases i n I s r a c l i s ischaemic h e a r t d isease , though, rheumatic h e a r t d isease is an important cause of morbidity i n c e r t a i n groups of t h e population, trllcl'c i t is believed t o be r e l a t e d t o socio-economic fac to rs , e spec ia l ly overcrowding.
The incidence of hypertension is about the same a s i n o t h e r coun t r i es wi th no s i g n i f i c a n t d i f fe rences i n incidence o r s e v e r i t y between t h c &iff e r e n t e thn ic groups.
From c l i n i c a l experience and e p i d ~ m i o l o g i c a l inves t iga t ion it may be deduced t h a t IHD i s a s common i n I s r a e l and a s f a t a l a s among t h e various populations i n Western and Northern &rope and USA. Any c o n t r a s t r e s u l t s mainly f r o m the ~-airiarkably l o w frequency i n l e s s suscep t ib ie groups such a s Yemenite Jews and Arab Bedouins.
Rehab i l i t a t ion of cardiac p a t i e n t s is being done i n a number of s p e c i a l i n s t i t u t e s . A s p e c i a l procedure of r e h a b i l i t a t i o n of post- i n f a r c t p a t i e n t s c o n s i s t s of combined occupational therapy, k i n e s i therapy and physical t r a i n i n g i n a day-hospital type arrangement.
EM/~ard. Vasc ,/5 EM/PRV,MJ , CARD .VS c , DIS/17 Annex I11 page v i
WHO Elmo
& the end of August 1972, five cur-urlury uclr.t! u11iL.s were I n operat ion i n t h e country. Pa t i en t s s t a y i n these u n i t s on average f o r 3-5 days, i f they have no p a r t i c u l n r complications, There a r e regu la r t r a i n i n g a c t i v i t i e s , courses 2nd seminars i n the coronary ca rc u n i t s .
9. Jordan
An ana lys i s of f i f t y - f o u r p a t i e n t s admitted f o r myocardial i n f a r c t i o n t o the biggest medical centre i n the country shows t h a t ischaemic h e a r t d isease occurs i n younger a s we l l a s i n o lder age groups, and t h a t it i s hy no means rare. JAypertansion, d i n b o t o s , and smolting w c r c found i n a g r e a t number of thesc pa t i en t s , and a s t r e s s f b l l i f e may have contr ibuted t o the developmznt of thc disease . Nut r i t ion does not seem t o play a major r o l e i n the diseasc i n Jordan.
10. Kuwait
Ttlcra are fuur ni i~, jur . cardic~c dlseases i n Kuwait, n~mely , coronary a r t e r y diseasc , hypertensive h e z r t d isease , rheumatic h e a r t d isease and congenital h e a r t disensu. I n add i t ion t h e r e i s the complex group lnmped toget'ner as myopathies, and becoming l e s s common the incicenco of pe r ica rd in l h c a r t d iszase .
I n general , it i s not poss ible t o give a c t u a l s t a t i s t i c s of t h e incidence of thc vcrious types of h e a r t d isease i n Kuwait. From t h e record of t h e cardiac c l i n i c about 1 2 0 0 cases of rheumatic h e a r t d isease giving an incidence of 1 .6/1 000 3nd 1 000 cases of congeni ta l h e a r t d i scase giving c?n incident;: of l.j/l 000 hzve been dccumentcd. This i s d e f i n i t e l y an undertst imation of t h e a c t u a l incidence, e spec ia l ly of rheumatic h e a r t d isease 1 1 h ~ r e l a r g e numbers a r c s t i l l not being r c f e r r e d t o the cardiac c l i n i c from t h e mediccl c l i n i c .
Primary prevention of rheumatic h e a r t disease is not p rac t i sed but prophylaxis of recurrence of rheumatic fever i n suspected o r confirmecl cases of rheumatic h e a r t d isease i s widely prxct ised. Long-acting p e n i c i l l i n i s usua l ly t h e drug of choice and surpr i s ing ly the incidence of drop-out i s very low, This is probably because t h e r c are no r u r a l a reas wi th d i s tance problems and t h e c l i n i c s a r c wi th in easy reach uf t h e general population.
Coronary a r t e r y disease i s becoming a major problem i n Kuwait, a f f e c t i n g the male population a t t h e most productive period of t h e i r l i v e s .
The in t roduct ion of coronary ca rc u n i t s has d e f i n i t e l y proved t o be u s e f u l but it only touchcs t h e t i p of t h e iceberg a s t h e majori ty of Jca ths from acute myocarclinl i n f a r c t i o n occur s u suddenly t h a t no s t a t i c or mobile coronary u n i t ccn a t present prevent it. I n Kuwait semi cnmnnry care i n a general medical ward has reduced morta l i ty . The mor ta l i ty p a t t e r n resembles t h a t of a coronary care u n i t where e a r l y deaths were reduced.

WHO rn EM/~ard. . ~ a s c ./5 EM/PRV.W . CARD .VSC . DIS/17 Annex I11 page v i i
Hypertension is a major prcblem i n t h e country and 2 survey of t h e disease h a s not been made.
11. Lebanon
Hospi ta l s t a t i s t i c s cannot g ive r e p ~ s c n t a t i v e da ta on t h e nccuracy of cardiovascular d i seases i n Lebanon, a s t h e number of h o s p i t a l beds i s l imi ted , and p a t i e n t s 2re se lected. There is, however, an impression t h a t rheumatic fever i s i n regression. R t 7 g a r d i n g ischacmio hcart d isease , a t t e n t i o n should bo paid t o ciiabctcs, which seems t o be increas ing, and t o f a m i l i a r hypercholes terola~mia, o f t e n observed i n consanguinous marriages.
Obstructive cnrdiomyopathy i s a l s o observed i n Lebanon, p a r t i c u l a r l y a s a he red i ta ry condit ion.
12. Libyan Arab Republic
Libyc is a l a r g e country wi th a population of over two mil l ions . An o i l pro~lucing ccuntry; y c t prosper i ty from o i l production and urbaniza- t i o n i n Libya a r e of l a t c advent and t h c i r impact has y e t t o be assessed i n terms of hea l th , hygiene, morbidity and morta l i ty .
Though no s t a t i s t i c a l da ta f o r cnrc.liovascular d i seases a r c ava i l ab le , b e t t e r recording and repor t ing systems havc been introduced a s t h e bas i s c f sound e f f i c i e n t s t a t i s t i c a l se rv iccs i n a l l f i c l d s .
A Cardiac Department w i l l . be cs tab l i shcd f o r the f i r s t time i n Libya wi th in 1973. It seems apparent, from cases seen i n t h e Medical Deprrtmcnt, U l u t Llbya nas i t s Cuc share of cardiovasculnr d i seases and these cliscases follow the pa t t e rn of developing a s w e l l a s developed nations.
Data co l l ec ted from the Department of Medicine, T r i p o l i Centra l Hospital cover t h e t o t a l number o f carcliovascular cases admitted over a period of s i x months from Apr i l 1972 - November 1972. There were 414 cardiovascular cascs ou t of a t o t a l of 2 030 medical admissions.
The d i s t r i b u t i o n according t o cliagnostic groups was as follows: ischaamic h e a r t d isease (including acute myocardial i n f a r c t i o n ) - 31 per ocnts rheumatic hoar t dibeuse (botn compensated and decompensated valvular l e s i o n s ) - 35.5 per cent ; hypertension - 20.3 Per cent ; pulmonale - 10.6 pe r cent ; congeni ta l h e a r t d isease - 1 p e r cent; miscellaneous - 1.6 pcr cent.
Ischaemic h e a r t d isease i s c l e a r l y the lending h e a r t d isease among males wi th a r i s i n g incidence over t h e age of f o r t y , whereas rheumatic h e a r t d isease takes the leading r o l e among females.

EN/Card .Vast ./5 EM/pRV.rllT .CARD.VSC.DIS/~~ Annex I11 page v i i i
WHO EFBO
Rheumatic h c a r t d isease i s c lose ly fcl lowing the pa t t e rn a s observed i n most of the developing countr ies ; high incidence, lower age group, more severe type of i l l n e s s and 2 high proportion of mul t ip lc valvular l e s ions with high mor ta l i ty r a t e .
It w i l l be of considerable i n t e r e s t t o compare these f indings with those a f t e r t e n years when newer housing schemes, public h e a l t h measures and h e a l t h c2.r~ programmes have been f u l l y implemented.
Hypertension shows a much higher incidence among females and some of it can bc explained by t h e g r e e t e r occurrunce of pyelonephr i t i s among them.
There is a l s o considurablc morbidity cluc t o chronic b ronch i t i s , emphysema and resp i rz to ry disorders . This has l e d t o a f a i r proportion of cop pulmonale.
13. Morocco
Admissions t o the Cardiology Department of thc: Hospi ta l Centre i n Fez comprised i n a two-year period (October 1970 - October 1972) 5 348 cadiac p a t i ~ n t s , amounting t o 12 per cent of a l l h o s p i t a l admissions during t h a t pcrioc?. Thc d i s t r i b u t i o n according t o diagnost ic groups shows the dominnt,inz significancz of rheumatia h c a r t diacaae. 61 per cen t o f c11 admissions f o r cariiiovascular d s c a s e s were f o r rheumatic h e a r t d isease , 9 per cent f o r ischaemic h e a r t d isease , 3 per cent f o r congenital. h e a r t d isease , n n J 27 per cent f o r various o t h e r cardiovas- c u l a r J iseases . The p a t i e n t s ' ages range? from two t c seventy-nine years, but 60 per cee t of a l l p a t i e n t s were below t h e age o f twenty years.
Accordingly, i n Morocco the same types of c a ~ i o v a s c u l a r d isease may be found a s elsewhere, but the carcliovascular pathology has some p a r t i c u l a r aspects . Though ischacmic h e a r t d isease i s on t h e increase , it s t i l l does not represent a major problem. Congenital malformations, though not more prevalent than elsewhere, a r e a problem because the re a r e no adcqucte diagnost ic and surg ica l facilities i n the country. However, con t ro l of rheumatic fever and rhsumatic h e a r t d isezsc should be t h e main t ask f o r carc l ic logis ts i n Morocco, and establishment of rheumatic f e v e r c o n t r ~ l programmcs mer i t s p r i o r i t y .
14. Pakistan
Although the evidence of an upward t rend i n ischaemic h e a r t >'isease i n developed coun t r i es i s overwhelming, the re i s a paucity of da ta pe r ta in - i n g t o thc prev,?,lcnce of ischacmic henr t d isease i n developing countr ies . V i t a l s t a t i s t i c s which can form an important source f o r epidemiological rosearch, are uni'urtunalely riot propcrly maintalned.
WHO m o EM/~ard .Vase ./5 ~/PRV.MJ.CARD.VSC.DIS/~~ Annex 111 page i x
To stu&j t h t prevalence of a ~discasc i n thc country, t h e main re l iance is on the stucly of h o s p i t a l admission and discharge. I n t h e f i e l d of ischaemic h e a r t d isease , some liclp has been made a v a i l a b l e from the autopsy repor t s of medico-legal cases 2nd a coupl? of epidemiological surveys have a l s o been c a r r i 4 out , These s t u d i e s show t h a t t h e U s e a s e has been increas ing rapidly anJ t h a t thc disease process, a s evidenced by autopsy repor t s stcr~s a s cnr ly a s t h e s ~ c o n d decade of Life.
The pcrccntage of ischacmic h e a r t disensc amongst t h e carcliac aJmissions i n h o s ~ i t a l i n various b i g c i t i e s va r ies from 15 t,o 20 per cen t but i n Karzchi it i s butvrcen 35 t o 40 per ccn t which i s more than reported from any c t h c r cen t re i n t h e sub-continent. This could form an idezl placc f o r carrying out rcsearch on the determinaticn of t h e e t io logy of t h ~ d i sease , The population of I b r a c h i was 300 000 i n 1947 and i s over 2 000 000 a t present .
&sides t h e ischacmic heart. ?i S P O S Q , hypa~tonsion and rheumatic h e a r t d isease form the bulk of the p a t i e n t s aclmitted i n t h e ca rd iac w n ~ d s .
I n a study ~f two admissions i n t h c Central Government ' H ~ s p i t a l , Rawalpiniii, hypertension was found t o account f o r 40 per cen t cf cases, rheumatic henr t c:isc.nsc f o r 25 per cent , ancl ischaomic h e a r t cliscoso f o r 21 per cent .
15. Sudan
The pa t te rn o f cardiovascular d i seases i n the Sudan may bc summed up a s follows:
Rheumatic h e a r t d i sease is t h e connonest carcliovascular clisease i n thc Sudan an11 ii c11cim.u lcr.lzed by:
( a ) t h e avercg,: onset i s e a r l y ancl t h a t of s j m p t o ~ ~ s a s w e l l a s of t o t a l incapac i t a t ion arc e a r l i e r than i n Europc and the USA;
(b) t h e main symptoms a r c clyspnoea anc: CHT while b ronch i t i s , h n e n ~ p t y s i s , chorea and cutaneous l e s i o c s a r e ra re ;
( c ) the d i s e x c severcly damages t h e myocardium and l e a d s to :
( 2 ) CHB is commoner than atrial f iLril laLLon and occurs l n s inus rhythm an2 a t z l r l i e r age below f o r t y yecrs ;
( i i ) FuLmom.ry ocdema i s r a r e even i n young pregnant women;
( i i i ) C H ~ r a t h e r than pulmonary oedema i s t h e main complication of rhemlatic h e a r t d isease i n pregnancy.

EM/~ard ,Vasc ./5 EM/PRV.MT. CARD r VSC . ~ 1 S / 1 7 Annex I11 page x
Hypertension is a common discas2 and i s an important f a c t o r i n the high incidence of s t rokes and l e s s commonly ischaemic h e a r t clisease. Hypertension i n t h t young is mainly seconJary t o chronic pyelonephr i t i s on top o f rena l c c l c u l i which a r e common duo t o dehydration i n a dry ho t country .
Hypertension and cerebrovasculnr Giseases a r e equal ly common i n thc low and high income groups, while d iake tes rnel l i tus and ischaemic h c a r t d isease are common i n t h e high income group. DM is t h e main r i s k f a c t o r i n ischaemic: heill-L Gist'aSe I n t h e Sudan.
Blood pressure and serum cho les te ro l a r e low and do not r i s e wi th age i n t h e pr imit ivc t r i b e , t h e Maban, which l e a d s an a c t i v e l i f e and l i v e s on a v i r t u a l l y h t - f r e e d i e t .
Cardiomyopnthy: i t is n ~ t e d t h a t EMF, previously reported a s r a r e I n t n e Sudan, i s incrensingly diagnosed.
Cor pulmonale i s ra re , and e v ~ n extremely ra re , i n cases of sch i s to - s o m i a a .
16. Syr ia
Ischaemic h e a r t d isease i s becoming a major cause of death i n middle-agud people i n Syria, i n males more than i n females. However, no s t a t i s t i c a l ch ta a r e avzi lablo a t present which woulc2 allow camparison wi th o ther countr ies . The majori ty of p a t i e n t s is seen and t rcn t~c ' . by general. p r a c t i t i o n e r s , and a smal ler number only i s soen by i n t e r n i s t s o r ca rd io log i s t s . Most of t h c p a t i e n t s a r c t r e a t e d i n p r i v a t e c l i n i c s o r a t homc. Tht. pr iva te h o s p i t 2 . l ~ do no t have t h ~ f a c i l i t i e s tu auceyL o r t r e a t such p a t i e n t s and t h e government h o s p i t a l s dc not have enough beds t o care f o r them.
Besides, these h o s p i t a l s do not have any follow-up c l i n i c s f o r cardiac p a t i e n t s an2 this makes any study d i f f i c u l t . There i s an impression that the re i s an increase i n the inciilence of t h i s d lseasc cmong tho general population i n t h e l a s t t e n years , s p e c i a l l y i n t h c age group 40-50, i n men r a t h e r than women, mort i n the c i t i e s than i n v i l l ages . The high income group i s more a f fec ted thcn t h ~ low. Nevertheless, t h e age-group 30-40 i s not protccteci, which i s no t silrprisinp; bocauso of ipcrcased migration from v i l l a g e s t o c i t i e s where pcople have t o l i v e under g r e a t e r s t r e s s than before. I n add i t ion the re is a high incidence of d iabe tcs m e l l i t u s and hypertension.
Health eclucation i s eml~hasizing the adverse e f f e c t s of f a u l t y d i e t , c i g a r e t t e smoking 2nd s t r e s s , a s w e l l a s t h e importance of e a r l y treatment o f hyp~r t ens ion and diabetes.

WHO EMRO EM/card .vast ./5 EM/PRV.W. CARD .VSC. DIS/17 Annex 111 page x i
Rheumatic heart Slsease is wiclespread among young ch i ld ren and youths; most of these cases a r e cliagnoscd e i t h e r i n l a t e childhood o r adolescence. About h a l f of the cascs nre diagnosed a f t c r tho appearance of complicating symptoms, and t h e o ther h a l f a r e diagnosed e i t h e r during an episode of rheumatic a c t i v i t y c r during a medical check-up on en te r ing school o r applying f o r an employment. A small number of cases only a r e diagnosed enr ly before the appcarancz of symptoms. A high incidence of rheumatic h e a r t d isease i s seen among t h e low socio-economic l e v e l such a s Pa les t in ian re f igees .
Ilypertensiun i s widespread among mldclle-aged people. Most of t h e cascs a r e t r e a t e d i n p r i v a t e c l i n i c s and a r e discovered e i t h e r casua l ly o r a f t e r t h c appearance c f complications. Cases wi th secondary hyper- tens ion which could benef i t from s u r g i c a l treatment, a r e ~liagnosed l a t e a t a time when treatment is of no benef i t . Lack of t echn ica l f a c i l i t i e s may be one of tho reasons f c r t h i s . CCUs a n . ICUs do not e x i s t a t t h e present time, but the re is a plan t o e s t a b l i s h them i n tho major h o s p i t a l s i n the near m t u r e .
17. Tunisia
A s nc general hcn l th s t a t i s t i c s a r e ava i l ab le , t h e i a t a from Hzpi ta l Ernest Conseil a r e reviewed. This h o s p i t a l admits p a t i e n t s from a l l p a r t s of the country, rcgarGless of t h c i r socio-economic cnndj+.inn. 1 ' . l l ages above twa years n r s represented.
I n the Dcpartmcnt of Cardiovascular Diseases, 1 3 4 9 p a t i e n t s wcrc h o s p i t a l i z e 3 between June 1970 and June 1972. Rheumatic h e a r t d i sease i s by f a r the l i~ost important condit ion, comprising 45 per cen t of a l l p a t i e n t s haspi ta l izef i f o r cardiovascular cliscases. Congenital h ~ a r t -lisease ranks scconrl, w i t h 15 per cent. Pat icn t s hoopitaliacd f u r a r t e r i a l h y p c r t e n s i o n mads 7.3 per ccnt cf t h e admissions, and 8.5 per cent of t h e p a t i e n t s were acmitted f o r ischaemic h e a r t J iscnsc .
Rheumatic h e a r t d isease i s a 3x21 scourgc i n t h e country; i t a t t a c k s a11 s t r a t a of pcpulntion, but p a r t i c u l a r l y t h e socio-economically poor population group who f c r want u f means o r information see t h e physician only when valvular h e a r t d isease i s f u l l y es tabl ished, and. do not follow up treatment and prophylaxis when t h e a c t i v e phase h a s ceased. I n t h e whole country the re a r e c!ispensaries where long-acting p e n i c i l l i n i s given f r e e t o a l l ini l igcnts on a simplc medical ~ r ~ s r r i p t i o n : nevertholoss p a t i e n t s very o f tcn discontinue the prophylactic regimen.
Ischaemic h e c r t d isease i s much lsss common, but i s on t h e increase . The same predisposing f a c t o r s wcrc obscrvcd a s elsewherc and it occurs mostly i n a p a r t i c u l a r s o c i a l category. No preventive a c t i o n has been
EM/~arcl.Vasc ./5 EM/PRV.MJ . CARD. VSC , ~ 1 S / 1 7 Annex 111 page x i i
i n s t i t u t e d f o r ischaemic h e a r t d isezse . Coronary p a t i e n t s a r c t r e a t e d i n cord io log ica l *'.ep?.rtmcnts, bu t t h c r e i s no i n t e n s i v e coronary ca re u n i t o r cardiac r c h a b i l i t a t i c n u n i t i n the country.
18. Turkey
The pathogenesis of cardiovascular 3 s e a s c s i n Turkey does not d i f f e r much f ron t h a t i n European coun t r i e s . The s i t u a t i o n of cardio- vascular d i seases t h e r e may bc sumrn?,rizcJ cn t h e b a s i s of t h e frjllowing d a t a , taken from thc rrl.cur.Js of tho iinkara Nurxiusu H o o p i t a l w h i c h i s one of t h e b u s i e s t postgraeuatc h o s p i t a l s of the country.
The t o t a l number of p a t i e n t s ~ ? J m i t t c d to t h e genera l warcls during the l a s t deczdc i s 54 562, 9 273 cf whom nrc czrdiac cases , o r 16.8 per cent .
Thc p ropor t ion with chronic ~-tiewiliiLic c a r d l t l s , Ischaemlc h e a r t d iscnsc and e s s e n t i n l hypertension t o t h c t o t a l number o f car2.iac cases i s 50, 35 and. 15 per cen t respect ively .
Ischaemic h e a r t \Usease accounts f o r 6.1 p e r cent of genera l mcclical cases, c s s e n t i z l hypcrtcnsion f o r 2.1 p c r cent , and chronic rhcumetic c a r d i t i s f o r 7 pur cent .

WHO m o EM/~arrl .Vasc ./5 EM/PRV.MJ . CARD, VSC . DIS/17 11nnex IV page i
Gene H. S t o l l c m m , M.D.* WHO Temporary rdvi s e r
I n temperatc c l imates :
The c l e c r e s t relationship of group ;L s t rep tocccca l i n f e c t i o n t o rheumatic fevcr is ioun?. i n s t u d i e s of "closetl" populations (such a s m i l i t a r y r e c r u i t s ) sub jec t t o epiLlernic s t reptococcal sore t h r o z t i n temperate c l imates (11). Several f irm concepts have emerged i n these s t u d i e s which may be summarizer! b r i e f l y :
1. When one s e l e c t s p a t i e n t s vrho art: ill with frank, emclative s t reptococcal phz.ryngitis duc t o c e r t a i n common prevalent pharyngeal s t r a i n s of v i r u l e n t group f~ s t rcptococci , rheumatic fever follows zt n f a i r l y predic table a t t a c k r a t e (approximately 3 per cen t ) rc-gardless of t h e aga, racc, o r e thn ic group s tud ied and re;~nrc'ilcss of t h c year o r season i n which t h c stuctv was m~cle.
2, The major va r iab les which a r e r c l a t c d t o t h i s a t t a c k r a t e i n such s t u d i e s a re :
( a ) Thc magnitude of the immune response t o t h e antecedent s t reptococcal in fec t ion , and
(b) the cluration of convalescent ca r r i age cf the organism.
Weak AS0 responses may be associatec! wi th acute rhewnatic fever a t t a c k r c t c s o f ~ o n s i ~ l c r a b l y l e s s than 1 per ccnt , whereas s t rong responses rnzy pror7ucc r a t e s we l l i n excdss of 5 per ccnt.
3 . Rheumatic fever can be preventc.1 following such i n f e c t i o n s by treatment wi th a n t i b i o t i c s which promptly and thoroughly e rad ica te t h e streptococcus from t h e pharynx.
Streptococcal i n f e c t i o n s a r e spread by in t imate , person-to-person, a i rborne contact . Streptococci recovered frcm dus t on f loors , b lankets and c lo th ing a r e of very low i n f e c t i v i t y . Close, in t imate l i v i n g con- :litions, however, represent t h e most dangerous s e t t i n g f o r transmission
*Pmfcssar and Chairman, k p a r t m e n t of hkdicino, Universi ty o f Tennoss~o; Physician-in-Chief, Ci ty of Memphis Hospital .

EM/~ard .vase ./5 EM/PRV.W. CARD. vsc . DIS/L~ Annex I V page ii
WHO mo
of pharyngit is , p a r t i c u l a r l g when extremes of seasons promote crowded indoor l i v i n g condi t ions (5) . Under such condit ions, t h e explosive spread of a s i n g l e group A s t reptococcal serotype i s most impressive.
Sporadic Streptococcal d isease and rheumatic fever among school ch i ld ren ---- ---..-- i n l a r g e c i t i e s of tenpe;-zJC_~-z~c~
When one attempts t o d5r"it:e more p rec i se ly t h e threshold of s t reptococcal pharyngi t is required t o produce rheumatic fever and tu rns t o t h e study ol" cn6em-i~ s t reptococcal d isease -in school chi ldren, thc complexity of t h e problern 3f dcr ining a s t reptococcal i n f e c t i o n becomes very g rea t . Studies made I n Chicago school chi ldren, f o r example (14), showed t h a t sore t h r o a t s associa ted wi th pos i t ive cu l tu res f o r group A s t rep tococc i r e s u l t e d i n rheumatic f e v c r a t t a c k r a t e s t h a t var ied g r e a t l y according t o the c l i n i c a l , bacter io logic and immunologic c r i t e r i a of s t reptococcal diseasc. Thus, more than 800 untreated p a t i c n t s who had a pos i t ive t h r o z t c u l t u r c for Zmup A struptococci but who haiL u r ~ l y mild c l i n i c a l manifcsi;ations, such a s non-exudative pharyngit is , d i d not . develop rheumatic fever although 40 per cent of these had de tec tab le s t reptococcal immune responses, The i n i t i a l o r acute phase s t rcp tococca l antibody titses i n these p a t i c n t s werc o f ten r e l a t i v e l y high (c lose t o 300 A S 0 u n i t s , f o r oxample) s ~ g g e s t i n g frequent, small, an t igen ic s t imul i , but t h e rnagnitudc of the cn t igen ic boost of each i n f e c t i o n was on t h e average rc . ln t ivc ly vroak. :%rthermore, uf Ltic s t reptococcal s t r a i n s i s o l a t e d only 40 per cent were typable f o r known M p ro te in serotypes, and o t h e r s t u d i e s of these s t r a i n s showed them t o havc l e s s v i rulence p roper t i e s than epidemic s t r a i n s (18).
Such observations drew a t t e n t i o n t o severa l p o s s i b i l i t i e s concern- i n g s t reptococcal pharyngi t is and rheumatic fever . First, t h a t a mi lder form of st l-eplucoccal Infection, c l i n i c a l l y and epidemiologically, might have much l e s s p o t e n t i a l f o r p~oduc ing rheumatic fever. Second, t h e d e f i n i t i o n of a s i g n i f i c a n t s t reptococcal i n f e c t i o n is very d i f f i c u l t i n a population of ch i ld ren i n rrhcm pharyngeal ca r r i age of s t rep tococc i i s r e l a t i v e l y high, i n r;:hon repeated mild s t reptococcal i n f e c t i o n s a r e frequent, but i n whom v"_r,:.1 i c f e c t i o n i s by f a r the most frequent cause of upper resp i ra to ry syr.lptoms, Iricluding sore th roa t . Although an increase i n s t rep tacocca l ant ihodics between acute and convalescent phase se ra i s usua1l:r cn acceptab1.e c r i t e r i o n of s t rep tococca l pharyngi- tis, some s t u d i e s have ;sointcd out t h e problem of excluding recent procoding s-t;rcptococcczl i l l n v s s as CL cause f o r a l a t e - r i s i n g t i t r e . m e n such i n f e c t i o n s a r c associa ted wi th prolonged pharyngeal cotlvales- cent ca r r i age of s t reptococci , i n t e r c u r r e n t v i r a l upper resp i ra to ry i n f e c t i o n s may secm t o be s t rcptococcal i n charac te r when t h r o a t c u l t u r e s a r e made (7)
EP/I/C~ rd .Va sc . /5 EM/PRV.W, CARD. VSC . D I S / ~ ~ Annox I V pagc iii
Stre2tococcal d isccs? i,n a z l l u ~ n t c o m c ~ n i t i c s i n the temper-t,: zo:l;s
The v i r tu21 disappcarznce of a c u t ~ rhcunntic fever nnong ~ e 1 z t l v e l . y a f f l u e n t populations of North America and Europz, and os~cci3 , l l .y i n a i t i e s wi th few, i f m y , slums 2nd with optima1 housing condi-Lions, i s cn?: of the d i - i ~ ~ ~ i ~ t i ~ cvcnts of rcccnt nLclical h i s to ry . Yet strcptococc;,l ~11:;ryngitis i n thu school-age ch i ld ren of such communitir;s con t i~ lucs t o 52 relatively common, and assays of s t reptococcal antibody t i t r a e s continruc. t c show m d e r z t a l y h i & t i t p e s i n thcse populations. Altlloush m ~ c h crcxiiit l i ~ s Leerl given L u Uiu ycri~r'uus c?i.sperlsirle;; of a:lLitiiuLics Lv cccuu;li .CL!L. t'nis change, GIG most casual survey of tho ths rapcu t ic regimen proscribi . , l by many physicians would reveal , i n t h i s author s e x p e r i ~ n c c ~ the us2 ~f f c r l e s s thnn the optimal courscs o l penicillin required t o prevent rheumatic a t t acks , a t l e a s t from epidemic-type s t reptococcal pharyngi t ls .
Is thcn the clicngc i n i n c i d c n c ~ of rheumatic fevLr i n such modii^iL I ~pidcmiologic s o t t i n g s a mat ter of a quan t i t a t ive change i n t h ~ v i r u l c n c ~ of rheur;ato&.nic or,:anisms o r i s t h c r ~ , pc-rha;ss, a l s o a c p J i t 2 t i v L chzn~a- i n t h ~ prevalent s t r a i n s of pharyngcz.1 ~ t ~ t p t o c c c c i i n such cul tures? 'fie l z t t e r q u ~ s t i o n r n i s z s zn o ld i s s u c (19, 12) . Arc thc rc strcptccbcc-1- st12zins t h a t cr i ncn-rh~umotogenic? I? so, u n L r what cpi3zmiclcgic candi t ions a r c thcy prevalent?
Rh,umatogenic and n u p h r i t c g d c s t r ~ p t o c o c c i : "Skin s t r c p t c c o c c ~ "
The epicl~mioloby of s t ~ p t o c o c c a l i n f c c t i o n s i n w a r n c l i m z t ~ s has b ~ c o r n ~ of g rea tu r i n t ~ r t s t i n recent t i n c s Secausc of thu incrczsin, mareness of t h ~ frcqucncy of s t r c p t ~ coccal s k i n i n f o c ' l c n s (22). It i s now c l e a r t n ~ t thc common type of skin s o m which r e s u l t s f r c n ~cccnc'.~li.:. i n f L c t i o n abrr~sions , fnsc.ct b i t c s and other- types of skin trnumn, anL which i s a s s c c i a t ~ d wi th poverty nni! u n h y ~ i z n i c l i v i n g condit ions i s 2 sti-cptococcal in fec t ion . Staphylococci ovLrgrow t h s c m s t e * i surf?.cd oQ sbch l e s i c n s 2nd. have, i n t h c p ~ s t , confuscd t h ~ e t io logy of t h i s kinci cE pyodema ( 3 ) . Purthermorc, a s epidemic s trcptococcnl pilaryngit is hns ccrnc under S e t t c r con t ro l , upidemics of acutc g1one:ulonephritis obscrvdd i n recent yecrs havc been found primarily i n p o ~ u l a t i c n s i n whlch pjroilu~~i: is prcvzlont i n chi lcrcn. Thus, fhc c n r c i b l stu&ics - c t h c Indian r ~ s l i r v a t i o n s cr Dliizn~scta - Red Lakc and Cczss L~kc. (20) iri Tyinld?b~l (9) , i n southcrn USA ( 2 , 1) , and i n I s r - e l ( lo ) , hcvc iden t9f ied so-cnl lLd "new" s e r o t y ~ e s of ~ t ~ e p t o c o c c i which secm t o havL 2 s r c d i l c c t i o n f o r skin r ~ s i i i e n c c . Moreover, thc t r a n s ~ ~ ~ i s s l o n of such organisms seems ti-. b t from skin t o t h r o z t , r z t h e r than via--vcrsa (22), and t h r o a t carr ingc of so-called "skin s t r a i n s " i s a commcn fcnturo o f populations i n whlch
The rennrkcble fea tu re of streptococcal pyoddrma an4 i t s complica- t in; acu te g lormmloncphr i t i s i s tno complctc a b s ~ n c ~ of 7.cusc rhcurnatic f c v i r following such in fcc t ions , 3 ; s p i t ~ t h e Prcqucnt concomitant t h r o a t

c z r r i a , ~ cf tndss i,r;ar_isrns. Fur~ ;hc i~?ore , f rcm stu~!it.s of i )ha~~n; ; i t i s i n t h ~ s , po lml l t i CS, it a p p ~ ~ r s tH althou&i i s o l a t i o n o l thcse "skin' s trzi ins Prc:~ thd th rc - t i s common, t h ~ s t rc&tococca l immune response i s considc-rabl-y liss v L ~ c r o i ~ s tnan th2.t observe?. fallovring phnrynpdzl iLlf ,c t ions with tfic k t , c t t r - s t u 2 i ~ l " t h r c z t s t r a l n s " (1 ) .
Such clbs,:rT,~.tii::is havc lc.2 t i ; tho concept t h a t acute glomerulonc- ;:hritis r c q ~ ~ i i ~ e s en aritdccdcnt inf'-- ,cbt lon by n s t r a i n of s t rcp tccocc i C' sfi3t has ncplir i to~enLc p o t c n t i s l , thc i n f x t i c n may bc e i t h e r of t h e s k i n cr of thc t l i r -ca t , ~ P - C it C L O G S n ~ t cc"uoc rhcuinstic f e v ~ r . W e hsvc: t i r~nc- l such str-".ins "nc a-rheu.m-ztc~~enic" (19) . Convcrscly, t h c v ~ c l l - r~co:;nize.l i;i?x','nzczl s,rct.ypcs which have cr~use,ll most c~ idern ics c f rheumatic f ~ v c r ( 2 . ~ . typcs 1, 5, 6, 19, 24, e t c . ) have not ca1~sc.l #-. -uti: u ~ l c m ~ - ~ ~ l l e n ~ ~ ! l i - i t i s an-: .-':c nct ap lxar t o cause common strcptccocc,-.l pyoilcrma .
;I f b ~ - t l i ~ r - .?ib b i u c LILLI b~twoen V f i ~ two typcs cS 1nSectlons 1s tnc l i f f d r s n c ~ i n tl:b i i m n e rospcnse. S t r ~ p t o c o c c a l pyoC~rmc, wi th o r ~britnout ac-tb ~,loin,;-vllcnci-hritis, prv-!ucts r ~ l l t i v e l y f t e b l e fiSO nni: ?.nti-?J,"~DEtsc titre:;,. w h ~ r ~ a s t h b response 3f nnti-DPJiisa B an:! a n t i - h y - l ~ r o n i ~ l a s c i s v i ;orcvs (22) ,
I n view of thc f~rego in , ; r?iscussion, those who nttemlst stur.li;.s ci' ncutc rheu.nctic f?v;rq i n warn clirnatcs harbouring pcpulations prone t c py-icma must b t isr~l:~-rccl. t c i n t e r y r c t phar;~n&dal ca r r i age of s t rep to - cocci cn:l ;,SO rtsi3rinsc.s wi th ?.waren~ss of t h i x h i x t u r e rf thc: strc;:ta-- cocczl s t r a i n s which may be present. I r i thi. southern USA, seesonnl v c r i a t i a n t l c n o n s t r ~ t ~ s s t r i k i n z l y -;hc : l i ssocic t ion 0: the ti{:, c!iscascs .- x u t k g1omdrulcnc;)hritis p r ~ v z l c n t i e sumncr znC- ccute rheu.rnctic ~ ' L V L T
i n l a t e f a l l cln.l winter (3 ; -x rc 1 ) . I n t r o ~ i c z l climntc:.c,, iicwnvc.r, such seascnal clistiriction i s n c t grsscnt , a t l c c s t not. t o t h e same J=eg:.rcc, an:! bcth ~;isc?,scs may bo supcrirnpcsc;,l thrcu&cut thi: yccr.
YTarinti~ns of ~;:ilcrnic>;ic s c t t i n z s i n tlic t r o p i c s which ~r;c?isposc -1,: zcutc rhev.mntic f ~ z
B e c ~ u s c t h L r L i s littib firm L v i d ~ n c e t o suppc:*t zn ~ f f c c t of cl imate ;,dr sb bn Yni: p a t h o ~ c n c s i s bi' ncu-t, rh~urnatic. fcvdr, onL shoul ' c,nsic:er t l i ~ rc ld oT c1imr.t~ a s but wether var iab le which c?*n z f f ~ c t the condit ions 2rornotinl; thc rapi:. s~rec, ' ! of pharyngcal s ~ r e p t r e o ~ c i of rhcunato;~~i ic poccnt ia l . I f this t h L s i s i s valicl,, w: shoulc: DL aS1, t o i n t t r p r t t i n c i s t o i t h e vz r iz t ions observc:~ i n t h e p r ~ v a l c n c ~ of r h ~ u m a t i c I ' L V L ~ r h ~ m a t i c i iecrt c l i s e a s ~ i n various p a r t s of the trorl!. P~r the rmcrc , t o ' 2 t t tiler- i s no p n r t i c u l a r r 2 . c ~ o r L thn ic drou14 thac i s s i t h c r m o r ~ o r l t ss s ~ s c e ~ t i b L e td s t rcptococcnl p h a r y n ~ i t i s o r t o ~ i t h ( ~ ~ c f i t s nbn-sup;~urztivc s ~ q u e l s , ~ n l thc r c l ~ uf 4cneLic f a c t o r s i n t h ~ c!cv;lc;~ment 0: 5 P t h e s t comc1icatfc;ns i s 2 l i m i t c I Gns (16)-
WHO m o EM/Card.Vasc ,/5 EM/PRV. w . C ~ R D . vsc . D I S / ~ ~ Annex I V pago v
Because thc most consistent praeillsposlng cpiclemiologic rrrctors f o r rheumatic fever appcar t o bc crowdtd l i v i n g c ~ n d i t i o n s , c l o s ~ person-to- pcrson contact ,andinadequate trcatmcnt and prevention of s t rep tococca l in fec t ions , z survey of thc pruvalcncc of acute rheumatic fevur and rheumatic h e a r t J i seasc i n c e r t a i n t r o p i c a l populations shculd c l e a r l y r e f l c c t tho e f f c c t of t h e s t f ac to rs . mhc Wcrld Health Organization Regional Officc f o r the Western Pac i f i c hcld 2 seminar i n Manila i n 1968 on the p r e v ~ n t i o n ~ n d con t ro l of cardiovascular d iscasc duo t o i n f e c t i o n s (2,) a t which t h ~ sub jec t oi' rheumatic hearst d isezse i n "be region received p a r t i c u l a r a t t en t ion .
The seminar emphzsized the remarkable v a r i a t i o n i n cu l tu rcs , e thn ic groups and gcogmphical f e a t u r e s of thL region. Regardless of such var iables , rheumatic fever and rheumatic h e a r t d isease was i d c n t i - f i e d a s a m~Qor problem only i n a reas whcre crcwding, l a r g e famil ies , low socio-economic condit ions, increas ing urbanization, r ap id i n d u s t r i a - l i z a t i o n , and changing ways of l i f c w ~ r c most s t r i k i n g .
The impltmontation of preventive measures f o r f i r s t a t t a c k s (primary prevention) and recurrences (secondary prevention) of rheumatic fever i s more complex than the simple f a c t s of prevention suggest. The b e s t programmes f o r rapid and rout ine J iagnosis of sore t h r o a t s by t h r o a t c u l t u r e s havc o f ten bccn mountcd i n ccrnmunities i n which rheuma- t i c f ever .lots not sicm t o be a problem st a l l . Thc s t reptococcal s t r a i n s i n such places have become at tenuatdd, and the tdiseasc. spora-Sic ( 1 C o n t m r i w i s ~ , only t h e poorest medico1 cclre and surveillance: of resp i ra to ry i n f c c t i o n s z r e ava i l ab le t o some c f thc most scvcrely a f fec ted groups. Tht global nature of s t reptococcal pharyngi t is and t h e seemingly irrcclucible human r e s e r v o i r of pharyngeal c a r r i c r s of v i m l e n t s t r a i n s , howcver, makc it incumbent upon communities t o l i m i t t h e exposure and. thz spread of t h i s d isease by scrupulous adherence t o t h e p r inc ip les of rheumat ic - fcv~r preventirjn. It is t h e duty, therefore , c f every community, whether o r nbt i t has a se r ious streptococcal-disansc problem, t c a s s e s s i ts own programme f o r rheumatic-fcver prevention and t o deci:.~ how t o meet t h e recornrnendcd standards f o r such programmes.
The most knowledgeable aclvicc ava i l ab le t c a l l physicians and h e a l t h workers i n a11 commnitics, here and nbmad, concerning how rheumatic fever prevention may b e s t be implemented can be found i n the recent r epor t o f t h e Inter-Socie ty Commission f o r Heart Disease Resources, e s tab l i shed j o i n t l y by t h e L~merican Heart Association and t h e US Public Health Service's Re~;ionnl Meclical Prcgrmmcs, which appointed a study group of rheumatic fever and rheumatic h c c r t d isease t o h e l p t o f u l f i l the Commission's purposc of "dcvoloping guiclclines f u r t h e avaluat iun
FN/card .Vast ./5 ESVI/PRV. M J . CARD. VS c . D I S / ~ ~ Annex I V page v i
WHO EMRO
of medical f a c i l i t i e s an2 se rv ices i n the prevention, diagnosis, t r e a t - ment, and r e h a b i l i t a t i o n of p a t i e n t s wi th c?mliovnscular disease" (13). The rhewntltic f L v c r study grcup's r epor t i s both nn e legant b luepr in t f o r a c t i o n by the com~mnity and a p ~ r c c p t i v ~ compenclium c f tht. s p e c i f i c problems t h a t must be overcome if z programme i s t o bc e f fec t ive . An o u t l i n e of t h c mnjcr p r inc ip les a r e cnumcratc,: a s follows:
Primary prevention
1. The community should i d e n t i f y t h c profess ional gmup tha t c a n serve a s a committee on strcptococcc?l clisease - rheumatic h e a r t clisease and should fix r c s p o n s i b i l i t y f o r the prevention programmes upon an agency w i t h t h ~ bcs t p o t e n t i a l f o r the job - usua l ly thc l o c n l h e a l t h clepartment . 2. The community should be ab le t o es-timatc t h o s i z e of i t s problem by rearlily availnblo scuroos o f data (suoh as hospi ta l iliachargca, h e a l t h recorJs , and survcys) . 3. Reliable, incxponsive ancl e f f i c i e n t t h r o a t c u l t u r e se rv ices must be provided (21). For a p a t i e n t wi th acute sore t h r o r t , wc need t o know simply, "is the c u l t u r e pos i t ive f o r hemolytic s t reptococci?" I f not, the t rouble ane cxpense c f a n t i b i o t i c s can be sparcd.
4. Treatment of s t reptococcal phs ryng i t i s must be adequate t o e rad ica te thc organism. It i s s t i l l d i f f i c u l t t o convince t h e profession t h a t a s i n g l e i n j e c t i o n of 0.6 t o 1.2 mi l l ion u n i t s of benzathine p e n i c i l l i n G intramuscularly i s optimal treatment. The a l t e r n a t i v e of t e n days of o r a l p e n i c i l l i n -000 - 250 000 u n i t s b. i .d. ) or , f o r p e n i c i l l i n - a l l e r g i c pdrsons, of erythromycin ( .5 Gm. b.i .d. ) i s dependent upon unpredictable p a t i e n t f i G c l i t y (2).
5. Medical s t ~ d c n t s , physicians, nurses and o ther professionaLs should be taught s t reptococcal microbiology aJequately i n a c l i n i c a l context by departments of medicine, paed ia t r i c s c7.ncl community medicine.
6. Once a primary prevention programme i s developed i n t h e community, t h e l eaders should present t h e i r case d i r e c t l y t o t h e public throu* a l l ava i l ab le c o m n i c a t i o n s media.
7. Schuol-ur- ier l LcC, programmss, particularly I n overcrcjw l e a schools i n t h e cen t re c i t y ~ n c ! those i n o ther h igh-r isk areas , providc exce l l en t opportunities f o r ch i ld ren wi tn symptomatic pharyngi t is t c be examined and t o have a t h r o a t c u l t u r e made by any ava i l ab le t r a ined personnel - e i t h e r t r a i n e d volunteers o r school nurses o r o the r paid public h e a l t h workers.

WHO EM30 EM/~ard .Vase ./5 EM/PRv. IV . CARD .VSC . D I S / ~ ~ i'innex I V page v i i
8. Community su rve i l l ance f o r s t reptococcal i n f e c t i o n s i s very help- fbl t o s e t t h e appropr!.nte index of suspicion f c r deal ing wi th p a t i e n t s wi th pharyngi t is , t o d e t ~ r m i n i when a symptomatic contact should have t h r o a t c u l t u r e s m a h , o r ever: t o determine wher mass prophylaxis wi th p e n i c i l l i n shou l l be giverl,
Secondary prevention (prevention of recurrent rheumatic a t t a c k s 1
1. Es tab l i sh a rheumztic fever r e g i s t r y .
2. Provldc p r o p h y l a c t ~ c drugs: 'lbc most e f f i c i e n t regimen f o r continuous prophylaxis agains t group 1; s t reptococci is a monthly i n t r a - muscular i n j c c t i o n c f 1.2 mi l l ion u n i t s of benza;hine p e n i c i l l i n . The clisadvantages anZ discomfcr% of this regimen havz t o bc weighed aga ins t t h e ind iv idua l p a t i ~ n t ' s s u s c ~ 2 t i b i l i t y t o rccurrenccs. Those wi th rheumatic h e a r t Lise?.se, reccn; rheumatic fcvcr, znd exposure t o an environment i n which thc inciJcncc of s t reptococcai i n f e c t i o n is f requ tn t d e s e r v ~ the mcst c f f c c t i v c protect ion. P.S a s ~ c o n d choice, prophylaxis may be ac?ninistc.rcd c r a l l y wi th o i t h e r 1 a m of su l fad iaz ine d a i l y i n n s in& rlosc o r 200 000 u n i t s of p e n i c i l l i n given t w i c ~ d a i l y on an empty stomach. The duration of continuous prophylaxis cannot be f ixed a r b i t r a r i l y f o r a11 p a t i e n t s , although t h e s a f e s t genera l i za t ion is t h a t i t be continue6 indef in i t e ly . Certainly, those under the age of eighteen gesi-s should receive a 5ontinuous pmphylnctic regimen. A miniinum period of f i v e years i s recommended f o r p a t i e n t s who develop rheumatic fever without c a r t l i t i s ovcr age of eighteen. The decis ion t o continue prophyl'ucis beyoili t h i s period should take i n to account a number of v:riablcs. Pa t i en t s wi th rheumatic h e a r t d isease a r e more suscep t ib le t 3 reac t iva t ion of rheumatic fever i f they con- t r a c t a s t reptococcal in fec t ion . Moreover, p a t i e n t s who have had . carditis i n a previous a t tack aro much morc l i l r c ly t o s u f f e r ca~-c l i t i s again i n a subsequent a t t ack . Climate, aga, occupation, hcusehold s i t u a t i o n , car?-iac s t a t u s , and length of time s ince t h e previous a t t a c k a r e a l l s i g n i f i c a n t va r iab les which influence t h e r i s k of recurrence. The dec l ine i n recurrence r a t e s with inc reas ing age is due to : ( a ) decrenscc r a t e of s t reptococcal in fec t ion , and (b) decrease i n the r a t e o f rheur~nt ic r3cc t iva t ion following streptococcal. i n f e c t i o n i n o lder rheumatic s u b g ~ c t s . Despite t h i s decreased r a t e , however, t h e r i s k of rheumatic recurrence i n aclults remains relatively high when the s t reptococcal d isease encountered i s sever€ o r epidemic.
3 . Estab l i sh follow-up prograrilmcs t o ensure p a t i e n t f i d e l i t y t o t h e prophylactic regimens. The follow-up should be devoted most vigorously t o those a t h ighes t r i s k f o r recurrences - namely, those wi th rheumatic h e a r t diseaso, wi th recent rheumatic fever (within f i v e years) , and wi th exposure t o condi t ions of h ighes t streptococcal-disease prevalencc.

~ b l / ~ ? r d .Vmc ./5 EI~/PRV. M;T . CARD. vsc . D I S / ~ ~ i~nnex I V ' C [* L.A2u v i i i
4. FiIokz avcilcblc: t~ t h e community mcdic--.l ccnsu l t a t ions , c l i n i c s , 2nd laborato%j f c c i l i t i e s f o r rhzurnntic pn t i cn t s .
i. Mount 2 ccntiiiuln,: p r o g r m i e G.L physician 2nd community education ~ G T t h t n~cJ .s c f tha 1-heuinatic fevei7 i x t i ~ n t .
There i s no s p c z i f i c cur2 Tor rheumatic fever , 2nd nc known measures chmgc thc c o u r s ~ o i i h c a t t a c k . G o d su~1:ortivc thorapy, however, c r n r ~ 2 . u . c ~ th, mor tz l i ty ~ n d rnorbi3.it:i a f t h c disease.
A f t L r rheumatic f ~ v t r i s f i r s t ?.ingnose:l, 2 cours t c f p e n i c i l l i n szcul : bc given t,: d i m i n a t e &rail> ;. s t rcp tococc i . This i s ni2vis_?blc ~i;cn if b a c t ~ r i r ~ l c sic cx~liii n;r t i n n y i c l ~ i s thr'oat culturvs noi;ativi. f o r s t r ep tococc i , s incb t h o organisms nay bc l ~ r e s e n t i n a r e a s i n a c c t s s i b l e t o swabs. It is pre le rab lc t c a h i i n i s t t r p e n i c i l l i n pnrentcra l ly . .in c f f e c t i v c C O J i q S L i s e i t h c r a s in& i n j ~ c t i o n o f 1.2 m i l l i o n u n i t s ~f bonzathine p e n i c i l l i n in t ramuscul?~r ly o r 600 000 u n i t s of procaine p , n i c i l l i n intr?vrmi~sculcrly l a i l g f o r t ~ n Says. L ~ t t ~ m p t s t o reduce u l t im? tc i lcnrt :zrnagt by a ~ h i n i s t e r i n s p e n i c i l l i n ca.rlg i n the acu te ,h,u:,:ctic cttr.ck i n l n i - z ~ r J ~ s c s !~c..v~ . l uL bec i~ succcssfUl t o J 2 - t ~ . ' ~ l t ~ r c o ~ i ~ p l c t i s n of t h ~ thc ra&ut ic cdursi. cr" y d n i c i l l i n , continuous - ~ r ~ t ~ c t i o n YPcin r ~ i n r " c c t i c n wi th sti3cptococci should b~ p rov i i :~ : by i n s t i t u t i n ; ~ n - of ti?, : , rophy l~c t i c regimens 2 ~ s c r i S t ~ l I n t e r .
Both c o r l ; l c c s t e r a , l s anci s a l i c y l a t c s a r e of censiderablc v a . 1 ~ ~ i n c , , n t r c l l i n ~ the tcixic manif c s t a t i o n s cf rhtumatic f t v c r , i n con t r ibu t ing LL -Sic ccmfort ,i t h c p a t i > n t , an1 i n combatin; anor txin , anaemia, and c c n a t i t u t i o n n l s p ~ t c ~ ~ s . I n s ~ v c ~ c r h e u ~ ~ ~ c t i c c a r d i t i s associntecl wi th h L z r t f a i l u r e , such n o n s p ~ c i f i c cnti-inflz-mrn-tory cff ~ c t s may re2.uce ~ 1 1 ~ bLlr.!en ~il;on t h ~ labourini; h e z r t . Occ,?.sionally, they may tilt tht: n?lzncc i n f ? " v ~ u * ~ -,.C s ~ r v i v s l s f a c r i t i c a l l y ill p a t i e n t . Curticos- c L r v i J s a r c m o r ~ pL)tcat than s e l i c y l ~ . t c s i? supprassint; acute e x u d a t i v ~ iLi21ammation, an: s o r i ~ p a t i e n t s i n W ~ G I , I s a l i c y l a t e s f a i l t c con t ro l the 3. - ~ s c c s c rts$on_l quickly tl, r ~ l n t i v c l y lz.rsL ~ l o s ~ s of c o r t i c o s t c r o i d s .
T r.Jncth~r , ur i ~ t i i i t ~ i l s i v e cc , r . l lcostcr I(; therapy lns t l tu tec l e a r l y i n t h e f i r s t r h s m r t i c z?;t?ck ccn reduct t h ~ Jct.ree of ultimate cardiac s c ~ r r i n g is 2 :,olnt vilifch i s s t i l l some~~hc?t a t i s s u e i n p a t i e n t s wi th - ~ l s t i v e l y m i l . ? cnrc:izc invclvement. bi'hlhcr~ c a r d i t i s i s mere severe, ~11 c a r e f u l l y ccntrcllc,: s t u J i L s f c i l t~ rcvez l any c l ~ a r s u p e r i o r i t y .f c , r t icos tdroids over a s p i r i n i n t ~ m n s o r moclifying t h e Ju ra t ion cP tnd ?curt 3 i s t n s ~ c ~ - rds idua l he - r t 'crnag~ ~ f t c r f i v e yea r s of follow- u;. HoweTJ~r, tnLrL IS s t i l l c o n s i l ~ r c b l d varicrtion i n t h e recomen2la- t i o n s concernin; t h c USL cf thdso n:;~nts.

Most ?.uth:.i-itizs now usc s a l i c y l a t c s r a t h e r than c c ~ t i c o s t c r c i ~ 2 ~ s t o trep-t ch i ld rcn wi th rh~;.umatic i"cvdr but wi th nc, evidenci. cf c a r J i t l s , s incz t h e progncsis f o r rccovcry without pemcnent s t i m a s i n sdch C?+SCS
i s z r c a t c r tl.:cn 95 psi-. ccnt . If s i z n s 2nd symptoms Zrc not si!equatcly su~:;~rcssed by salicglc".tc-s, ccr t icostcrc ic ls c r c substitutc:l. Pa t i en t s wi th m i l L i c c r d i t i s zri: probably :<ivcn oorticcstl-.roirls i n mcst i n s t a n c i s , -.lthou:$ it i s i r sluch c:!ses t h c t tlier;, i s t h c .;1-cztest 2isagrccmen-t zbout t h e i r velu:. Pa t i cn t s wi th sevcru c a n l i t i s c ro usua l ly t r e a t e l promptly wi th c ~ r t i c c s t e r o i ~ l s , ix t r t i cu la r lg i f h e a r t f a i l u r c i s ~viLIent, i n which ccoc p c ~ i n t ~ r c . 1 :looca sf mcrcur ia l &iurc"cics ?,re i;iren nz.1
sC:lt i n t ~ ~ k ~ i s restrict;:.
Nc n r b i t i - z q ~ scheCulc of doses of c o r t i c o s t z r o i d s o r s a l i c y l n t c s i s recor.mendc2, s l thcugh they shoul" be a?.equntc t c nchiavc prompt sjmptr~matic i n ~ r c v c m ~ i i t . Salicy12tes arc: 11.silally ~ i v e n a s zcc- tylsa l i - c y l i c aci.?. i n I- t c t c l i!aily close i n i t i a l l y of 2.15 J pcr kg ( 1 g r a i n per yvurid) i . ~ " bi,i':~ v i ~ L : $ t , UiJ ti: a naxlrnun dal ly dos,: of 1-0 :;. c o r m - cos';ari;iGs rr- usuall j i s t a r t e l? i n iLoscs comparable f o r Jif f e r c n t nna- l(,,ucs t c tinct of 1 0 ti, 15 rn, of 9 r ~ i n i s o n e cvcry s i x hours. 21c
i s ~ a s i : nnJ I?;. t h L Stv~rTtg of tilt r h c m a t i c llroccss i n t h c inti ivi2ual c-sc. Becmsc s o s i rheulnntic =rtta.cl:s lasr , s i x wet!rs, treatrilcnt shoul,: bc: continuous 2t 1v.s t f o r this ;ieriuJ, wi th Jcses tnperec! ,lurin: t h L l z s t twz w,eks. S ~ c u l r ? c l i n i c 2 1 symptcns re laps- (relsuunJ phenornercn) , ?n ~ . J Z i t i o n ~ . l f o i ~ r ~ tc s i x vroelis of trcctr:dnt i s ~?..Lvis,.-~. I n stcbborn c t t -cks , such cuxrs,s qizy hzvc t o Sc rcljtZ.t,J s c v L r a l t i n e s . Weckly ttsts f o r C - r c x t i v e ;;rotein i n the blc,oi'. nri' f o r the e q t h r c c y t L sb '.irn,ntati9n r a t , <-.r~ U S C I ~ ~ i n follovrin, t h ~ heal ing p r o c ~ s s , p n r t i - c u l a r l y when cre:.tn~n t wi th c c ~ r t i c o s t ~ i - o i L . s o r snlic:rlctLs i s t;ra-luclly ~rriti;:!r~;n. W i t r , =rxLquat, su~r j rcss ivd , l o s ~ s , t h e C-rcactivc p ro t t i i i shcul! J i s > p ~ ~ n r f ~ o n thc b l c o - , n n l tinL ~ r y t h r o c y t t st-irnent#ction r z t i shaul i ;-cr~?sc-. Rc2?pcc..m.ncc o i C-rcnctive g r o t ~ i n an 1 r?n i n c r t a s c i n thc. ESIr u,mn w i t h d r 2 ~ 2 1 uf trcatmcnt i n d i c a t e contirmc,: r h e ~ n a t i c ,ct ivit j- un less c t h c r causcs of infl~.mmction a r c prcsent.
Course anl p~osncsLs c l ncutc: rhewiiatic c a d i t i s
Propcr rchc.5ilit:tion s f p a t i e n t s rccovcring from riicumctic fever rheumatic c?.r:li t is requires intim:itc k n ~ & l e ? . ~ c cf' tho "nctural
l i i s tc~ry" ~f t h e i s c a s c . mi. S c s t Z.T~cilnbli: information cjf t h e ilvclu- t i c n of rh2u:natic h e z r t 2fsezsc has been o'ut?.inerl f x m recent long-term fc.llcw-up s t u i c ' s o f m t i e n t s h ~ v i n g c n t i s . t r c p t c c ~ c c c 1 prophylxiis i n whcm the fe- turcs o f thi. acute rhmr,l;;tic a t t a c k wcrc: c a r e f i l l y docmion- t e l nntl annlyzc '. by st~nc?arclize,:l c r i t c r i z (4, 1 5 ) .
% ~ s c s2d2it-s clcmonstrztc: th- t p c t i ~ n t s whc have rhcurnntic fever :citi?out cvitlcnc;: of c?.ilclitis ( a t ltl-zst 50 :,or ciint i n m o s t s c r i t J s ) rnrcl;.

EM/Card .Vasc ./5 EM/PRV.MJ.C~;RD.VSC.DIS/~~ Annex I V page x
WHO EMRO
have rheumatic h e c r t c!iscase when examine< f i v e years l a t e r . Obvious- l y , therefore , p a t i e n t s without s i g n i f i c a n t c a ~ l i a c murmurs requ i re no in tens ive e f f o r t t o prevent ca re iac sequelno by prolonged beclrest o r prolonged r e s t r i c t i o n of physical a c t i v i t y .
I n addi t ion, these s t u d i e s show t h a t c c r t a i n manifes ta t ions which have been consic?crei! by some t o kc: i n ~ l i c a t i v c of "carcXtis" (such a s prolongation of the P-R i n t e r v a l 2nd T wave changes i n the e l e c t r o - cardiogram; arrhythmiasis; anc? s l i g h t o r equivocal evidence o f t t c c t ~ y ~ i t l r : erilt2rgement '' ) may havc a benign p r o ~ n o s i s . Unless these manifes ta t ions a r e associa ted wi th s i g n i f i c a n t murnmrs they cause l i t t l e h a m . Moreover, the prognosis cliff o r s markcdly wi th t h e Cegrec of cardiac involvcment, a s r e f l e c t e d by t h e i n t e n s i t y and t h e kind of h e a r t murmurs anci by t h e presence of congestive h e a r t f a i l u r e . Thus, i n one study (4) of p a t i e n t s having "probable v a l v u l i t i s " (a J i agnos i s based upGn t h e presence of 3 louc!, a p i c a l s y s t o l i c blowing murmur ra-l iat ing t o t h e LuiLla) approximately 25 pLr ccnt haJ rheumatic h e a r t d isease f i v e years l a t e r . O f those who had "unmistakable v a l v u l i t i s " (manifesteC by a d i a s t o l i c m u m r , e i t h e r m i t r n l o r a o r t i c ) , 67 per c e n t hacl rheumztic h e a r t d isease f i v e years l a t e r . Similar ly , i n t h e "cooperative study'' (6) t h e incidcncc: of rlwumatic h e a r t d isease f i v e years a f t e r t h e acute a t t a c k was clirectly r e l a t e d t o the s e v e r i t y of acute rheumatic cnr l? i t i s . a s f o l l o w s : 4 pe r cen t in p a t i e n t s with no c a r d i t i s d u r i n ~ the acute a t t acks ; 18 p e r cent i n those wi th s o f t organic a p i c a l s y s t o l i c murmurs only; 32 per cent i n those wi th louder organic a p i c a l s y s t o l i c mumurs; 52 p t r ccn t i n those wi th d i a s t o l i c murmurs; and 70 p ~ r cent i n those wi th c o w o s t i v e h e a r t f a i l u r e of p e r i c a r d i t i s .
R e g u l a t i o n n f physical activity
Knowle2gc of the f ec tu rcs of acute rhewnatic f e v t r which i n f luencc t h e prognosis f o r t h e dcvelopment o f cardiac st igmata i s t h e most u s e f i l guiclc t o thc, amount of physical a c t i v i t y which may be permitted t h e p a t i e n t during thc a t t a c k anc! during conval~scence. I n thc absence of c a n l i t i s , s t r i c t bedres t i s unnecessary a f t e r t h e f i r s t few weeks of the d i seass i f the ncute manifes ta t ions ( p o l y a r t h r i t i s , fever, chorea) are suppressed o r hcvc abnted. Such p a t i e n t s may be permitted seJcntary a c t i v i t i e s u n t i l suppressive anti-rheumatic therapy i s terminated. Relapses, if any. usua l ly occur w i t h i n two t~seks of Lisoontinuing tho t reatment o r occasionally a s l a t e a s f o u r wseks afterward. Sydenham's chorea may appeczr s t i l l l a t e r . I n general , i f no re lapse i s eviclcnt one month a f t c r discontinuing therapy, o r two months a t the very most, t h e a t t a c k may bc considered t o have enclcd. We have never observeil spontaneous reac t iva t ion of acute rheumatic f t v e r a f t e r t h i s period of time un less new s t r ~ ~ t o c o c c a l i n f e c t i o n has intervened (15).

WHO m o EM/card.Vasc ./5 EM/PRV.W. CARD.VSC.DIS/~~ Annex IV page x i
Therefore, t h e p a t i e n t without card!itis may resume f 'u l l a c t i v i t y two months a f t e r t h e a t t a c k has ended. I f c a r d i t i s was a f e a t u r e of t h e a t t ack , but murmurs have disappeared, fill a c t l v i t y may be resumed a f t e r s i x months of observation have confirmed t h e continued absence o f h e a r t disease. I n ~ a t i e n t s wi th res idua l carcliac murmurs, t h e dynamics of t h e l e s i o n and s i z e of t h e h e a r t usua l ly deternine f'uture r e s t r i c t i o n s of a c t i v i t y .
CONCLUSIONS
Htleumatic fever i s a cornpiicetion of streptococcal pharyngi t is which can occur i n a l l races and ethnic groups throughout the world. Although t h e pathogenesis i s s t i l l unprovec, the re i s a s t rong cor re la - t i o n between acute rheumatic f e v e r and t h e s e v e r i t y of s t rep tococca l phazyngit is , c l i n i c a l l y , epiclemiologicc?.lly, and immunolo~;ically. The ubiqui ty o f s t rcp tocccca l s t r a i n s , t h e i r v a r i a t i o n i n vi rulence, anci t h e i r q u n l i t e t i v e d i f fe rences , p a r t i c u l a r l y between "skin" and " throat" s t r a i n s , have mndo t h e study of s t reptococcnl cpidemiolo~~y complex. It i s now apparent, however, t h a t pyodcrma-producing s t r ~ p t o c o c c i of nephritogenic p o t e n t i a l do not cause rheumatic fcver.
SWCCU~FZ OF f~S0 TITRES I N FILIPINOS~
1 Data e x t r a c t c c from repor t of Limson, c t a 1 (8).
' Mcan T i t e r I
u/ml $4 > 200u
7 2
40
24
I --
Live. Rise u/ml
303
167
-
I Acute rheumatic 419
Convalescent s t r c d 229
Controls i 110 I
L
$ Pts. wi th r i s c c f > 200u
65
32
- I

9 1 / / ~ c r :.Vase ,/5. 2K/PRV.$U. CLRD,VSC. ~ 1 S / 1 7 ,,nncx IV ; X ~ C xi i
Bisnc, ii.L., Fsx-cc, I .L., Wcll, E.P., Moocly, ivI.3. an? S t c l l c m a n , G.H, : Contrcs-Ling i-;;ideniolcg of acutc: rheumatic fi;.vc.r and ncutc 2; lomer~lsne:~h~qi t is : Naturr of thc 3nt~?cx:cnt s t reptococcal i n f ec t ion . G r England J !+le(j.. 283 : 561, 1970.
C o m i t t s ~ G n PTo-~int ion c-,f fii?eu:nctic E'cvi-r and B z . c t ~ r i a 1 EnclocnrCLitis: P r ~ . v i n t t z n cf 1'!1c~m~tic f ,-vc.F. Cirau1ation 31 ~948, 1965. ---- Dillcin, K.C., Jr. : P;.ollcmn n e p h r i t i s . :Inn. Rev. Fle-l. 18:207, 1967
F c i n s t ~ i n , L ~ . R . , cn2~ c t h e r s : L~ c , n t r c l l ~ , i s tudy c,f t h r e e methods of prophyl?<;:is 2;P"inst s t r ap tccccca l i n f c c t i c n i n n pcpulation of rhcurnatic chi1Crcn. I T . R c s ~ l t s (IT' t n c iirst t h r c ~ yecrs ~f the. stuj.y, incluclics i:~thc:?s f c r e v a l u ~ t i n ~ thd nnintenance of c r a l pr~i;hyl2::is. NCW Enrland J . J!slcc:::, 260 : 697, 1959
Frcnlc, P.F., Stollermnn, G.E., an.! LvIilli-r, L.F.: Protcct icn sf n m i l i t a r y gc.pulction from ~hcu:natic fcver. J . A .M.;L. 19J:775, 1965.
Ilca: PIC t i - ~ ~ t r n ~ n t ,i acutc rheumatic f2vcr i n children: C C L > L T Z ~ ~ V L c l i n i c c l t r i c l L? IxCTH, Cortisond, and I ispi r in . C i r c u l a t i c n U:347, 1955.
Kajlnn, E.L., Tclp, F.H. Dudcling, B.ii.: Diczncsis oi streptococcal h i ML'fcrcntiat iJn si c?cti-\rL i n f c c t i c n frcm the. c a r r i ~ r s t n t e i n zh;. s y n i ~ t ~ m a t i c chilcl. J . I n f c c t . D i s . 123:490, 1971.
Limscn, B.M., Martieres, F.M. an2 Bravc, E,L.: h c t ~ r i c l o g i c an2 inxui lu lu , f l: l:v!i,g~~'i~ L.?- V L s tc2y ~r Flllljlnc. rneurnatlc sub3 cc t s , non- r h ~ u m a t i c s u b j ~ c Ls wjth group i-i s t r ~ p t o c o c c c l i n f e c t i o n s at12 hczl thy c z c t r c l s u . b j ~ c t s . J . ~i chc Phi l ippine Me?. i ,ssociation 40~988 , 1954,
Po t te r , i=. iT , , ::nl c thers : C h ~ r a c t ~ r i s t i c s c f bcta hen~c ly t i c s t r c p t o c ~ c c l ,zsscci?ti:. with ncute g l ~ r n t r u l o n c p h r i t i s i n TrinicIa.1, J. h b . & Clin. iki!. 7 1 ~ 1 2 6 , 196G.
Rabino~ri tz , S.B., fck, I., Davids, I!..l., and Rnbinowi tz, li: Qr'i-apLci-Cic strtptococcal z n t i b ~ i ' . i ~ s i r l ~ ~ ~ J L L I I I L L ~ i~~pilr'lti~. J. In fcc t . D i s . 124:488, 1971.
%mmelltcmg, C.H., Dcnny, F.W., ,?.nil WnnnzmcLker, L.W. : Stuilics c.n c;l-?i,lcrnii:li,;y c,? rheumatic fovcr i n i'irnc,'. Scrviccs, i n Thcmcs, L. ( c l) : R ~ c u ~ n a t i c f cvcr ( ~ i n n c c p o l i s : Univcrsity c.f Minnescjta Prcss, 1352) .

WHO EMRO F,M/c~~J .Vzsc ./5 EN/PRv. M J , C~IRD, VSC . D I S / ~ ~ i~nnex IV pngc x i i i
12. Pafimcllcamp, C.H., Jr., ?.n:;, Wcnvzr, 2.S. : Acute ~ ~ l o r n c m l o n e p h r i t i s : Significnneu of v-.riztj.cns i n inci:;,ncc of d i sease . J. Cline Invkst . 32:>G5, 1952.
1 . R%eumetic fcvii? anG r h e u n ~ t i c he:~-rt :isensc: s t d L y group: Rcport of t h c I i l ter-socicq; Ccfiu!lission ?or !I:;z.Yt Disease Resources: p r c v e e t i ~ n ci' ~Lieumatic fiivc? cn.1 rhc~urnntic h e a r t c l i s ~ a s e . Circulnt- <l::.-1-15, Mag, 1970.
14. S i s z u l , ;. .C., Jz?lnsiin, E.B., L:L..~. S L ( , l l ~ ~ i . r i ~ ~ : i l , G.H. : CcntroLLcd s tu , l ios jf s.Lrrctooccccal 12h.?r:::i:;itis i n n pacd ia t r i c yo;:ulation. I. P = c t c ~ s r e l ~ , t c 2 tz t h c a t t c c k r z t c ,? rheumatic fever. Now England J . x, 265 : 559, 1961.
15. Stt 1 l ~ r m r . n ~ G.H., >.nc? c t h e r s : i ic la t icnshig ~f iinrnunt response t.. grculj a*A S t r t ; ~ t o c o c c i t c t h c c c u r s ~ c f acute, chronic an2 recui"rcnt rhcurnntic PLvL~. irL?. J. Ned. 2O:l6jJ 1956.
16. S t c l l c m n n , G.H.: Thc e p i L a r n i o 1 0 ~ ~ ,JL^ primary r?n? scconc?nry rhiumctic i zvLr , i n Ulir, J .W. (LLI) : The s t r e p t a c o c ~ u s , r h e u a l t i c f e v e r p.12 ~ l c i x c m l e n e p h r i t i s (3zlt imore : bJilliams & WiUcins CG . , 1964) .
17. S t d l e n n a n , C.H., SiL:;<l, II .C, , Joiinson, E.E. : Variable c p i d o m i ~ l c i y c;f streptocc.ccn1 c l i s ~ z s c an:.! t h s changing pn t t c rn o f rhcunat ic rc~:c;.?, Mcd. Conc . CarLllovasc . Dis. 34:&5, 1965.
19. Top, F.li., Jr., ~ n 2 c thc r s : I\I nnti;;cns mlonc; group iL strLptococ~:f i s ~ l s t Pr.crn sk in l e s ions . J. &y . MeL. 126:667, 1967.
20. Wann;:ind<~r, L.:I. : i , meYnc2 for s u l t u r i n ~ bvta hcinolytic s t r ~ p t c ; c o : c i frc;m t!i~ t h ~ c 2 t . Circulc~t ion, 32 : 1054, 1965.
21. Ihrsnnanakcr, L.N. : D i f f c r ~ n c ~ s bct~vedn s t r ~ i ) t o c u c c d i n f c c t i o n s L 3 t h e t h r o a t nni! of the skin . NLW En[;lcnd J . Mtd. 282: 23 & 78, 1970.
22. Uc r1 1 Hr ,o1 t.l? Or,-~niz-tticn Wcsttrn P x i f i c Scminar Discusses Prevention ?,a,. C o n t r ~ l of C a r J i o v ~ . s c u l ~ r Disc-czses by G.H. Stol lcmcrl . ~ u l l . ~ n t ' 1. ~ o c , ~f Car ' i c l cu lo:$, 1963.

WHO mo EM/~ard.~asc ./5 Dl/PRV . M J . CARD .VSC . DIS/17 Anne:: V page i
THE CONTROL OF RHETJbiATIC FEVER AND RHEUMATIC HEART DISEASE .@J OUTLINE OF WHO ACTIVITIES
D r T. Strasser cnd D r J . Rotta Medical Officer, Cardio- C?a.-ef, ITdO Internat ional vascular Diseases Unit, Reference Centre f o r Streptococcus WHO Headquarters, Genev~~ Typing, I n s t i t u t e of Epidemiology Srvi tzerland and Microbiology, Prague,
Czechoslovakia
THE EXTENT OF THE PROl3LEIY TODAY
I n a number of a f f luent countries the incidence 02 rheumatic fever has considerzbly decreased during the las t decades. I n some countries, f o r instance, cases of f l o r i d rheumatic fever a r e hardly seen any more. A s a resu l t , a tendency t o minimize the public heal th importance of rheumatic fever has appeared, on the assumption tha t the disease may subside o r even vanish spontaneously a s the standard of l iv ing of mankind increases.
However, even i n soc ie t ies with a high average income there may remain lslurlds o.C poverty where, morg o Lhela erldernlc diseuses , i: rela Lively lli& r a t e of occurrence of rheumatic fever ma pers i s t , rendering the "eradication of rheumatic fever an un fu l f i l l ed hopett.% ( I t may be in te res t ing t o mention thc t a smnll streptococcal epidemic with cases of rheumatic fever occurred i n Geneva i n 1971.)2/ Moreover, rheumatic heart disease may not be preceded by a c l i n i ca l ly apparent a t tcck of rheumatic fever. I n many countries a great number of comrnissurotomies a r e performed each year, indicat ing t h a t rheumatic hear t disease remains an important problem even where the incidence 02 acute rheumatic fever is insignif icant . But above a l l , the major par t of mankind i s s t i l l f a r from t h s t l eve l of welfare a t which a decline of rheumatic fever could be expected solely by improving l iv ing condLtions. I n rheumatic fever, a s i n any disease, the c i r c l e poverty-disease-poverty should be attacked f r o m both sides. The question i s only what should be the l eve l of pr ior i ty of rheumatic fever control among the many heal th problems i n view of the l imitat ions of resources i n any society.
There is no generally val id answer t o t h i s d i f f i c u l t question, because i t depends on an undeSined number of t'actors re la ted t o m e texture of neal th and soc ia l conditions i n a given area. Nevertheless, a number of, ,considera- t ions should be taken in to account concerning rheumatic iever i t s e l f . Mortali- t y data, with some reservations due t o inherent uncertaint ies , show the in te - res t ing f a c t t ha t i n 1968, i n the age group 15 - 24, rheumetic fever with

EM/~ard.Vasc ./5 EM/PRV.MJ. CARD .VSC . DIS/l7 Annex V page ii
WHO EMRO
rheumatic h e a r t d isease - a disease of youth - was the leading cause of death (accidents excluded) i n s i x countr ies , and was a t "Le second o r t h i r d place i n a fu r the r four countr ies a able 1). Most of these t e n countr ies a r e n e i t h e r a t a low nor a t a high l e v e l of aZTluence. It could be assumed t h a t a s i m i l a r pa t t e rn of mor ta l i ty w i l l emerge i n developing countries, when t h e i r present leading h e e l t h problems a r e overcome. Endeavours i n developing countr ies t o con t ro l rheumatic fever and h e a r t d isease thus might be an investment i n t o the fu tu re .
Rheumatic fever and rheumatic h e a r t d isease a r c preventable by t r e a t i n g t h e s ~ r e p t o c o c c a l i n f e c t i o n s adequately, a s s t a t e d i n severa l WHO documents.& Prevention of re lapses i s r e l e t i v c l y casy and cheap, i t c o s t s probably severa l hundred times l e s s than e.g. t h e s u r g i c a l treatment of a p a t i e n t with m i t r a l s t enos i s cr a o r t i c incompetence. Pa t i en t s wi th rheumatic h e a r t d isease may l i v e a s i n v a l i d s f o r s s v e r a l decades, and socie ty cannot d isregard the humane nor the economic aspect o f i n v a l i d i t y .
Data on the magnitude 02 t h e problem a r e becoming ava i l ab le i n an increas ing number of countr ies . A t a recent WHO consul t a t i o n p' t h e s i t u a t i o n i n some count r i es of t h e Mediterranean was reviewed. According t o the repor t s given a t this consul ta t ion, Algeria has a s i g n i f i c a n t rheumatic fever problem, and it seems t o be on the increase . I n a p i l o t study of an a rea wi th a general population o f 45 000 inhab i tan t s ( a l l ages) , threc per thousand of t h c t o t a l inhab i tan t s so~tght medical care f o r rheumetic fever and rheumatic h e a r t d isease from Jun? 1970 t o June 1971. Eighty per cent of these were ch i ld ren under s ix tean years of age. More than 470 000 school ch i ld ren undenvent sys temat ical h ~ a l c h examinations: near ly 7 000 ch i ld ren (1,S per thousand) were found t o have rheumatic h e a r t d isease . I n Cyprus, the importance of rheumatic Lover can be judged from h o s p i t a l admissions. These seem t o be r e l a t i v t l y common over t h e past Len years: f o r t y t o s lx ty - f f ve new cases per year art: adr111 LLed L u Nicosia General Hospital , serving a general population o r 150 000 inhab i tan t s . Most of these p a t i e n t s a r e chi ldren. I n Egypt, i n a f i e l d study on school ch i ld ren 6-12 years old, a prevalence r a t e of LO pcr thousand of d e f i n i t e rheumatic h e a r t d isease cases was found. Group A s -~rcptococcus i n f e c t i o n s werc found t o havc a high incidence - approximately j O per cen t of school chi ldren per year. I n - IFan, on the 70 000 general population of Abadan, an i n o i d ~ n c c r a t e of 1 per thousand was reported i n 1971. A group of school chi ldren i n a socio-economically underprivileged a rea oi' Tcheran was found t o havc a rheumatic h e a r t d isease prevalence r a t e o i 22 pcr thousand, and a 1-heumatic fevtzr annual incidence r a t e of 4 per thousand. In a population of 40 000 s o c i a l l y insured Teheran workmen and t h e i r iernil ics, a prevalence r a t e of 2.5 per thousand was observed. Hospital s t s t i s ' i i c s i n I r a n show t h a t 30-60 p e r cent of a l l ca rd io log ica l admissions nre due t o rheumatic ievar . I n Morocco, the f indings of A. Tazi and c o l l c n ~ w e s i n d i c a t c a
WHO EMRO ~ M / ~ a r d .Vasc ./5 EM/PIIV .MJ .CARD ,VSC .DIS/17 Annex V p,age iii
rheumatic hear t disease prc;~~lc?nec i2a'cc of 9,85 par t housad i n school children. Up t o 4,5 per cerit of 32.1 h o s p i t e l i ~ c d pa;tients are admitted f o r rheumatic fevar. kin or,?;mlzed coi'.&rol p?"ogi3wame seems highly desirable. I n the &dm, 14 855 cases of :-heume';.ic fever and i*ematic hear t disease - were admitted t e hospi.t&l. i n LSTO. As t.hc - to ta l population amounts t o about 14 million, OX: per ' ~ ; I o u s ~ ~ ~ inhabi t s r t s was admitted t o hospi tal f o r rheumatic hear t disecse. R l . n i 7 ~ c ? nlmber of these were children; 45 per cent were below 23 years ~ f ' age, The nuinber of t'nose not hospi tal ized i s unknown.
Data from otner places ;u~h ns H~'r;7adns, C o l u n b i a , E th iop ia , Polynccia, India , Jameica, l \ !~ngo~~ia, Nigerl;:, pelu, Senecal, show t h a t rheumatic fever mid rheumatic W o r t disease prestent a yr obl -rn nnyvhere on the globe.
Fortunately, d1. germ;; frcm g:'cl:i-' t i ~i,u.e~t,ococcl are sens i t ive t o penici 1 1 in. Unfortuna-ioly, th ~ x - c u ~ ? c o n s i s t s of L!. gi'eaL number of immunologically different, t>pea, a d t ? e ~ e i s nc sa t i s fac tory cross-immunity b other types a f t e r i n f e s t i c r ~ wi-& on? type. Ther8ef ore, no immunization t o rhematric fever i s pr,?.nticz,bl.c a5 r~re.sent, pad prevention has t o rely on the bacter ici2al ef-'ec'i, of perl?'cil!.in ( o r on other a l t i b i o t i c s , i f t he subject i s a l l e rg i c t o pen ic i l l i n ) .
Streptococci are ubicjultol~s end, prs?cticdLL.Lg, c m o t be eradicated. The idea l way of prevention i s ear ly pen ic i l l i n treatment of any group A streptococcal infect ion. TI? prac t ice l ctif f i c u l v j l i e s i .a. i n ident i fying a l l streptococcal infectionr;. Tr:ough. th-. bacter ioiopical diagnosis is simple :'and' r e l a t i ve iy inexpensLve, thb incidence of th roa t and skin infect ions which inFght bc ? . ~ 2 -i;o sf:r.~ptococerl i a fec t ion i s so great t h a t a bacter iological di.hgngsis could hcr5l.j; hc est?.blished i n a l l cases, especial ly i f la,borakor~.cs 3 . x ?~~?r?e:- 'r,!i:+ s.tinain of other important work. Besides, nxly pa t ien ts with m i m r s t reptocwc,d infect ions do not reach the physician. :In acute Vlroat infeckion m z y be due t o motk~er cause, e.g, a virus, and streptoezccus may ~'iill be present, i f the subject i s a ca r r i e r . Rheumatic ?'eiroi. a s oPt.3:. GGLL;.? without being preceded by a c l in i ca l ly manifest stre2tocs ccz.? 3.n:'ec-Lion. Furthermore, rheumatic fever m a y produce i n sone psrtien-ks or17 r.li.2.d o r a typical symptoms. About a third of pa t ien ts l~it 'rl hear-t disecse have never had an at tack of rheumatic fever. If a l l Y ~ i s i s t A c n in to account, together with the fortunate f a c t t h a t r b ~ ...-_?t, i c feve? develops cnly i,n c small percentage of (uutreaLed) sLYept.ococcaL infections, i ;; may be real ized t h a t several thousands of cases of group 12 strep-tooocc al in f ecti.ons should be t rea ted ea r ly and e f f i c i en t ly i n order t o prcvcn-t n single case of rheumatic hear t disease.g/ This c lear ly shorrs the rnzgnit?ide of the task, i f primary

EM/Card.~asc ./5 EM/PRV,PIT, CARD, VSC , D I S / ~ ~ Annex V page i v
WHO mo
prophylaxis i n en t i r e populations i s aimed a t . Nevertheless, much can be done for primary prophylaxis, c.g. i n co l l cc t iv i t i c s o r P m i l i c ~ , par t icu ler ly i f outbreaks of streptococcal infect ions a re announcing an impending epidemic, o r a t the time of any increasing exposure t o streptococci.
I f a person has contracted rheumatic fever, it is essent ia l t o prevent development o r deter iorat ion of rheumatic hear t disease by administering pen ic i l l i n a t regular i n t e rva l s f o r a long time. Details a re given i n the recommendations of WHO y. There i s no doubt t ha t regular pen ic i l l i n prophylaxis of recurrences considerably improves thc prognosis of rheumatic f'cvcr, yct i n many cams prophylaotio treatment i s given irregularly o r i s not given a t a l l , and organized community action has remained limited. The cruc ia l problem i n t h i s f i e l d i s how t o extend prophylaxis t o a l l those who need it. WHO has therefore developed a programme of rheumatic fever and rheumatic heart disease prevention i n communities.
WHO CONTROL PROGRAMMES
WHOs s a c t i v i t i e s s t a r t ed with the Expert Committee ' s recommendations f o r the prevention of rheumatic fever and rheumatic hear t disease&?/ Theg were taken up by the F i f th World Congress of Cardiology (New Delhi, 1966)10/ wherz the necessity of establ ishing model centres of prevention was outlined a t a symposium on rheumatic fever. This was followed by a WHO Seminar i n the Wektern Pacific Region i n 1968,11/ where the epidemiology and control of rheumatic fever i n the region was discussed. I n 1970, WHO issued a proposal f o r the epidemiological study and control of strzptococcal infect ions and t h ~ i r sequelae, rheumatic fever and g l o m e r u l a n c p h r i t i s . ~ The protocol* was tes ted and reviewed i n February 1972, a t a meeting i n ~ s i r o u and the Agenda of the Regional Seminar on Cardiovascular Diseases (Annex I) includes also the control of rheumatic fever and rheumatic hea r t diseases.
WHO'S current approach t o the community control or rheumatic fever i s t o es tab l i sh p i l o t programmes i n various countries and environments which, i f succcss~"u1, should serve a s a model i n the respective area. The main objectives of the programme are: ( a ) surveillance of known cases of
hear t disease and rheumatic fever i n a communi-ky, and regular pen ic i l l i n prophylaxis i n order t o prevent relapses and deter iorat ion of the hear t disease, and (b) studying the incidence and prevalence of the disease, and i t s na tu rz lh i s to ry , a s compared t o other areas. Other
*A l imited number of copies of the operating protocol a r e available on request from CVD U!l.it, WHO, Geneva.

EM/C ayrd .Vase . /5 EM/PRv . M J .CARD .VSC .D1S/l7 :raex TJ page v
important sub jec t s tc he studied are the c o s t nf prophylaxis programmes; pat ients ' rosponse including the czuses of missed appointments, drop-outs, and e f f ec t s of migrat.j.on in to ~ n d o11.t of th .e study area; promotion of primary prevention or pl~nu??,tic fever; bacter iological and sero-immunological research i n group A streptococcus epfdemjology; promotion of t ra in ing of physicians and other heal th t9?o??-i~:rs.
Pat ients known t o have had rheu~natic fever and pat ients with rheumatic hear t disease are regis tered ,md followed up. !̂ Jn infom.ation system i s b u i l t up i n order t o include 2 i l kliosrr- cases i n a comrnu.nity. This involves g a t h e r i n g r7at.a f m m -:.he h q s ~ i t n l s , t h ~ school hea1t.h s e r v i c e ( i f any) ,?nd the physicians i n fhc area. Eesides, systamatic screening of high r i s k groups, mostly school-age children, i s carr ied out i n order t o include h i ther to undetected cases. Good w~i-king relat ionships arc established between a l l fac tors involved i n - ~ l c prograinme. 17, scheme of these relat ionships is given i n Lmex 11. He2lt:l v i s i t o r s m e an e s sen t i a l par t of the programme, as they are sent t o a l l those registered patiencs who do not appear f o r the prophylactic treatment i n due tirro. It shoul?. be str:ssed that ~vherever t h i s su i t s the hea l th care system, the intentfon i s t o bring the pat ients , a t regular in te rva ls , t o t h e i r t r ea t in2 pnysj_cicws, snd not t o take them away from t h e i r doctors.
Circumstances may i-equire t h a t the protocol be sldapted t o specif ic s i tua t ions . The organizational design of the programme may d i f f e r , i n de t a i l s , from place l;o place. The principles, however, should be conserved i n any s i tuat ion. Defined communities or population groups should be covered as cornpl-et,elj as possible ad, f o r the sake of comparability, the da ta should be recorded i n ~r--jcus places !r~ 7. mif form way.
Studies and control programmes of rheumatic fever woye s t a r t ed according t o the WHO design i n several areas of the world. [ , p i lo t project, i n i t i a t e d i n Barbados i n 1970, has demons'nated t h a t good coverage of the population and sa t i s fac tory pat ient response t o an organized preventive programme of rheumatic fever yelapses inay be obtained i n a r e l a t i ve ly unsophisticated population .?/
,', similar programme i n Egypt includes a l l school-age children of the Qualyub area, near Cairo. Q u a l ~ p b Hospital, the r u r a l heal th services and the school heal th service i n t h . 3 study area a re co-operating with the Rhewn8t:tic Fever Project Centrc i n Cairo. Bacteriological and c l i n i c a l examinations are mado on a population of 10 000 school children annually.
b o t h e r programme i n Tigeria covers several thousands of school-age children i n the Lagos metropolitan area. I n I r an the prop;ramme i s conducted i n Teheran, by the School of Public Health i n co-operation with

EM/Card . ~ a s c ./5 EM/PRV . M J . CARD - VSC . D I S/17 Annex V p&e v i
WHO EMRO
the soci a1 insurance medical service; the study area has a population of 100 000 made up of 26 000 social ly insured workers and t h e i r families. A programme on the same l i nes has been prepared t o include a population of s imilar s ize i n the c i t y of Abadan. I n Senegal, the Cardiolo,gy Department and two other departments of the Medical School i n Dakar and the school heal th services are co--operating i n preparing a p i l o t p r o g r m e of the same kind f o r school children. Another such programme i s being organized i n Ulan Bator, Mongolia.
A t the 1972 consultation on Rheumatic Fever Control i n C a i r o , there were part ic ipants from Algeria, Cyprus, Egypt, Iran, Morocco and the Sudan. Lively i n t e r e s t was shown i n a l l these countries and preparations were s t a r t ed f o r extending the WHO rheumatic fever control programme t o new areas . It was a l so agreed t o launch a co-operative study on the val idat ion of the diagnostic c r i t e r i a f o r rheumatic fever, co--0rdinated by WHO and based on the Rheumatic Fever Project Laboratory i n Cairo and the WHO Internat ional Reference Centre f o r Streptococcus Typing in Prsy;uue.
THE RHrmMATIC FEVER CRITERIA STUDY
The diagnosis of rheumatic lever i s a straightforward one i n typ ica l cases of the disease. However, very o l ten the symptomatology of rheumatic fever is far from being typical . The sens i t i v i ty and spec i f ic i ty of the criteria at prc~cn t used fo r the d ia (y1us l s or rheumatic fever i s not known. The pat tern of the disease may have undergone some changes duping the l a s t decades, and it might show some diPTerences according t o various geographical regions Recent advances i n laboratory assessment of the organism' s react ion t o streptococcal infect ion may f a c i l i t a t e an attempt t o val idate the diagnostic c r i t e r i a f o r rlieumatic fever . I n suspect cases, when a decision must be taken as t o whether o r not prophylactic treatment should be instituted, the va l id i ty or" diagnostic c r i t e r i a becomes highly relevant. The WHO study therefore aims a t val idat ion of the current ly used c r i t e r i a f o r the diagnosis of rheumatic fever .
A s ignir icant number of cases with both c l in i ca l ly c l ea r and suspect rheumafic fever w i l l be analyzed, Cl in ica l symptoms and signs are confronted with laboratory findings, and pa t ien ts a re followed up. Event- ual ly , it w i l l be assessed with what probabili ty various combinations of c l i n i c a l and immunological findings can be a t t r ibu ted t o rhew,atic fever ,
D o t h cases u.C ffrst ana of suDsequent a t tacks of acute rheumatic fever and cases of act ive rheumatic heart disease a re studied, whether t he diagnosis i s established def in i te ly , o r whether it is equivocal. "Definitet' cases are those complying with Joncst modified c r i t e r i a . Guidelines f o r considering a pat ient t o have " equivocali' acutd rheumatic i'ever or act ive
WHO EMRO ~M/Card .Vase ./5 EM/PRV .MJ .CARD .VSC .DIS/L? imcx v page v i i
rheumatic heart disease are the presence of ,any one of tho major c r i t e r i a ; o r combination of any minor c r i t e r ion with ar thralgia; o r established - rheumatic heart disease being the opinion of the p h y s i c i z highly suspicious of n recurrent episode of rheumati c ac t iv i ty .
The d i a g n o ~ t i c procedures include a de ta i led c l i n i c a l work-up and a se r i e s of laboratory inves t igaeons , including grouping and typing of t he streptococcus, i f present. Serological t e s t s , such as ADPNase, ADNase B, cross-reactive heart antigen and ACHO antibody assays are Included. W pat ien ts a re followed up and careful ly observed as t o whether Rheumatic Heart Disease w i l l develop o r de te r iora te after a spell of "oquivocdU rl~eumatlc fever.
THE WHO INTERNCiTIONPL RE-CE GENTRE FOR STIBPTOCOCCUS TYPING
Bacteriological and serological procedures ,we of basic importance f o r the diagnosis of streptococcal infect ions and t h e i r sequelae and f o r s e t t i ng up a prophylc&.s progrcunme of streptococcal irlfectlons I n rheumatic individuals o r i n la rger population groups. I n order t o ensure r e l i a b i l i t y of laboratory r e su l t s and comparability of findings obtained i n various pa r t s of the world, standard laboratory procedures and reference biological materials ,are t o be uscd. The recognition of such a need l ed WHO t o the decision t o es tab l i sh the WHO Internat ional Reference Centre f o r Streptococcus TJ ping. The Centre was created a t the I n s t i t u b of Hygiene and Epidemiology i n Praguc i n 1966.
I n t he past f i v e years, the Centre has maintained a col lect ion of reference s t r a in s f o r the preparation of grouping and typing sera, and f o r the production of ex t race l lu la r streptococcal products. A t o t a l of 8 176 ampoules were made and 1 0 4 7 lyophilized s t r a in s meeting 114 requests were sent abroad. Sera f o r group A t o U of haemolytic streptococci, precipitation sera for the m a j u r i l y of types 1 t o 61 f o r group f~ s t r a in s ( a n t i M se ra) , %glutination typing sera f o r group A s t r a i n s ( an t i T sera) , and group B typing sera a r e currently used by the Centre i n research, and may be supplied t o other laboratories, on request, as reference sera. I n past years, t he Centre has met a considerable number of requests fo r grouping and typing sera, and ident i f ied by both agglutination and prec ip i ta t ion techniques several hundreds of streptococcus s t r a i n s sent from other laborator ies .
A large part of the cen t r e ' s work i s concerned with the determination of an t i s t rep to lys in 0 tltres i n human se re or iginat ing from various D R P ~ . ~
of t.he world. The aeicrluglcal surveys provided valuable information on the occurrence of streptococcal infect ion among the population of the t rop ica l and subtropical zones. The se ra were col lected by study teams within WHO a c t i v i t i e s re la t ing t o various hea l th problens i n several developing

EM/C ard . Vasc ./5 EM/PRV . M J .CARD .VSC . D I S / ~ ~ Annex V page v i i i
WHO EMRO
countries. I n general, the population sampled can be considered "average" with respect t o streptococcal infections, since no e f f o r t was made t o include o r exclude individuzls who migh-t have been suffer ing from streptococcal in fec t ion a t the time of scrilaling. The col lect ions of s e ra were sent t o Prague and were stored a t the WHO Regional Reference Serum Bank. Anti- s t rep to lys in 0 was determined by a. modification of t he photometric method of Liao.
A t o t a l of 4 000 s c ~ a were examined, collected i n various surveys, from Algeria, Burma, Kenya, M~ilgolia, Nigeria, Pakistan, Thailand and Togo. Table 11 shows the percentage of se ra with an t i s t rep to lys in t i t r e s above 199 units i n these countries. While the tes ted sera from some countries covered a wide age range, only school-age chi ldren 's se ra were t i t r a t e d from c ther countries, it :, - ,.:.:n ~ p p a r e n t t ha t , s imilar ly t o the temperate zone, the age group of 6-14 years i s a t t he grea tes t r i s k from streptococcctl infect ion i n the t ropics a d subtropics.
I n the temperate ZOjIe of the Northern Hemisphere elevated titres m e usual ly found i n 5 - 20 per cent of healthy individuals, The higher per- centage i n most of the t rop ica l and subtropical countries investigated c a l l s f o r fur ther comparative bacter iological and epidemiological invest igat ions i n order t o assess the r e a l significance of these serological findings.
The centre's r e s~mch programme is fucussed on mLcrobiological, biochemical and immunologic,d~pects of streptococcal infect ions and t h e i r sequelae, with spcci,d reference t o the ro le of s t r e ~ t o c o c c a l c e l l u l a r a d ex t race l lu lc r products i n the pathogenesis ( c e l l w a l l mucopeptide, M protein, erythrogenic toxin, s t r e p b l y s i n 0) , t o t he virulence of streptococci and immun:ty i n streptococcal infect ions. Furthermore, the research programme includes the study of the submicroscopic s-tructure of hacmolytic streplucoccl ~ 3 d t n e l r L forms and of various problems of t he epidemiology of strcptococc a1 infect ions , rheumatic fever and acute gl~merulonephri t~is . The Cent,re endeavours t o co-ordinate the work of nat ional streptococcus reference laborator ies and t o a s s i s t WHO in the co-ordination of nat ional 'and internat ional s tud ies of the control of streptococc,d infect ions 2nd t h e i r sequelae. It i s ready t o supply, on reguest, reference s t re~tococcu; str,ains. These s t r a i n s are representative cul tures of t h e indiv-d~lai gl.oups and types, su i tab le f o r the production of grouping and typing sera. Moreover, p referen t ia l s t r a i n s f o r the preparation of different e : : t r ~ c , e l l u l ~ streptococoal products are available. The Centre o w cupply -bo ii:tur*us ted laborator ies grouping and typing se ra i n small quantitZcs as reference material . The Centre i s also ready t o t e s t grouping and typing se ra prepared i n nat ional streptococcus reference laborator ies or p i l o t centres, i f requested. F a c i l i t i e s a re available f o r grouping and typing . f l imited numbers of streptococci, and aid may be

WHO m o EM/C ard . V a s c . /5 EM/PTIV .MJ .CARD .VSC . DI ~ / 1 7 i',nncx V page i x
provided i'or the a s s 3 of zntis.LYeptoiysii~ 0 t i t z a t i o n or , i f necessary, of an alternaze an%lbodjr, Lf' sera c.rjm'$i.i.eCL !:'or resesu'ch are t o be analyzed.
The control $roG-;:.!nms:; c--:. sarr5..;.C cu-c according t o the same basic design, and ~ q i f o ~ n detbu. z?-'; 2~,'!.!.ecl.i'zd. [this r.al.1. callow a pa ra l l e l t o be drawn betweer, tke p~c ;g : :~~ ; i ; i cs .iri vw-i.oua ?a r t s cf the world. It is also expected. t o ob-La2.r~ c~spa~;'r,ict 5a.t.n a2 t h s prevalence and incidence of rheumatic fever ax'. ~hei:r,lc~tj c: hear% disease i n t he vcrious study areas. AS there 1s a gre2,t clve-oa,.l.-- .. -, 7.2.:- ,L-,:<c,~A- .t??n t h ~ areas w2lere the s tudles will be conducted, comparsblc cln;L~. ~-'?.lo?li.,! 'c e valu.&le, pat icular ly because no population-based d a t : ~ on tkis occizr?-clo? of rheuiat ic fever and rheumatic hear t disecse are 2.veilr.ble frsr; t ~ o p l c d and subtrcpical countries.
The rheuma'tic 2eve-r; cri%e-,:j. v,dld-.?.ton st.~d!y i s conceived la rge ly , . on the basis of 5 nJ: ?xic;tlo::c!. c --.T-: .?:-.h_.-lr,:.-. ?,or ~ W C , Ileasons, A consider-
able number of c,-.cos :.~-i-t;? :,(:>; i~:;. - --;:-,~ ..t?-:.cs fever a re needed, and i f they are col lected fiq?ri; SAVE>;~LZI - .. i.?:-i,";, -i.>..r r:tudy may be completed sooner. Furthermore, a grea.t .a:r,bc?r of scp:~-;.si;ic;~ted laboratory assays w i l l be done. By divis icn of I.a,bour, some of the centres r.vil.1 make cer ta in
4-7 analyses centrd- ly. ~hxs.. tne lnhora-tory workload w i l l diminish and comparal;ill.:_- of the resul-6s w i l l bs ?;ncreaseci.
Central compu-ker da'ca-processing by WHO i s foreseen, both f o r the community control 2nd c:?.%eria valridat,ion stuc'~, basgd on the use of uniform record forrco j.2 t5.c 7.-arIi.31.~~ c.;-.cpext:.;.= centres. I ts advantage i s an ident ica l t yea t l~sn t af 'ch-. dzta coming from various centres, hence eas i e r comparison 02 the r e s - ~ . l - t ~ , ?not!ier advantage is t h a t cen t ra l data processing i s eczjnomicel, Tt nlso providesthe opportunity f o r timely spot t i% o f m c - t h ~ d o l . s ~ i c ; c ~ do? rcicncics, c .a. incomplctc or erroneous recordings. Such ir-?o:r,?~,-tio~ i s fed back t o the centre immediatel.y , and the ixthzd.olo~ic~.!. f a-~.Lt c m be corrected.
The 1nternatio;ln~. E.eferencc Ccat-tre prcrnotes the "common langu'age" between streptoconca7. la5orxLories i ; ~ various par t s of t he world. For instance, the Centre ozrrS.cl r:ut a co-ope-;.at.ive evaluation of streptococcus T-typing with thc pp.rticipattion of f i f teei l nat ional streptococcus reference laborator ies . Tlne par t i tips-ts u.nanimously s ta ted t h a t t h i s type of co-operating was -:c:eful, 5~1-k t.11~ sf,ur7tjr made it obvious t h a t T-typing r e q u i r e s f u r t h e r ,zi;tonkion. tc. tcchilicd d e t a i l s be fo re world-wide results can be compared 7with cert~i11t.y.
EM/Card, Vas c . /5 EM/P~v.oar. CARD.VSC.DIS/L~ Annex V Page x
WHO Ern0
In another evaluation study, eleven national reference laborator ies par t ic ipated i n a s s e s s h g the baci t racin t e s t as a screening method f o r iden1;ifyii;g grloup A streptococci. This study revealed t n a t the baci t racin test can on u u account replace the serological ident i f ica t ion of Group A s-treptococci which alone gives 1-eliab1.e resu l t s .
Internat ional co-operation i s not always an easy task. It may require somei;irnes considerable e f f o r t from the part ic ipants e.g. t o drop a laboratory method -Lo adopt another, or '"u comply with some standards. Co~nmunications nay be sl.ower than desired. In te rcu l tura l differences may cause some d i f f i c u l t i e s i n the in te rpre ta t ion of questionnaires. However, these Lnconveiiiences a2e runply compensated by the advantages of a co-operative project.
Streptococci are complicated, fascinat ing micro-organisms. Rheumatic fever i s a complicated, i n sany respects s t i l l mysterious, response of the human body t o streptococcal i i~ fec t ion . It i s t o be hoped t h a t internationa? co-operation w i l l contribute t o a be t t e r understanding of the germ and the disease, arid ~ l ? d ; eventua.i-I-,. the des'red l eve l of control w i l l be achieved.

WHO EMRO EM/Card.~asc ./5 EM/PRv. MJ . CARD .VSC. DIS/~~ Annex v Page xi
Markowitz, M. : Eradication of Rheumatic Fever : an unfulfilled hope. Circulation 5 : 1077, 1970. Hazeghi, P., Humbert, J.R., Svejnarova, M. et Piguet, J.D. : Les infections B streptocoques E?-hdmolytiques du grape A chez l'enfant : Mdd. et Hyg. 2 : 308-312, 1972
Prevention of Rheumatic Fever : Second report of Expert Committee on rheumatic diseases : Wld Hlth Org., Tech. Rep. Ser. 195T9 126. - Prevention of Rheumatic Fever : Report of a WHO Expert Committee; Wld Hlth Org., Tech. Rep. Ser., 1966, - 342.
Streptococcal and Staphylococcal Infections : Report of a WHO Expert Committee; Wld Hlth Ora., Tech. Rep. Ser.. 1968, 2. Epidemiological. Study and Control of Stleptococcal Infections, Rheumatic Fever and Glomerulonephritis : Proposal for an International Co-operative Study; WHO, Geneva, 1971. WHO int. doc. CVD/70,5.
WHO Programme on Rheumatic Fever Prevention : Report of a Consultation held in Cairo, 1.9-22 February 1972. WHO int . doc. CVD/72.2
Strasser, T. : I1 controllo della febbre reumatica : rassegna internazionale : C1. Terap. 15 Ottobre 1971, 59, Fasc. 1, 15-28
Hassel, T.A. Renwick, Sonia, Stuart, K.L. : Rheumatic Fever and Rheumatic Heart Disease in Barbados : Detection and Proahylaxis; Brit. Med. J., in press.
Fifth World Congress of Cardiology, New Delhi, Oct. 30 - Nov. 5, 1966. Symposia - Acta Cardiologica, Brussels. First Regional Seminar on the Prevention and Control of Cardiovascular Diseases due to Infections, particularly Rheumatic Heart Diseases; Manila, Philippines, 5 - 12 November 1968. WHO Regional Office for the Western Pacific. Internal Document. WPR/103/68.

EM/Card.Vasc./5 EN/PRv.MJ. cARD.vSC.DIS/C~~ Annex V page x i i
WHO m o
THE RANK OF MORTALITY JXJE TO RHEUMA'IIC HEART DISEASE AND . RHRTMAlTC FEVER I N VARIOUS COUNTRIES, I N YOUNGER AGE GRCUPS
Data f o r 1968 (Source : World Health S t a t i s t i c s Annual, Geneva, 1971) ----- --
Bulgaria, How-Kong, lortugal, Rornarlla, Singapore, Yugoslavia
2. Hong-Kong Greece
3 . Portugal, Singapore I s r ae l , Mauritius, Poland
5. Bulgaria, Mauritius, Romania Philippines
6. spain -
7. - China (~a iwan) , Spain
8. New Zealand Ceylon, Mexico, New ~ e a l a h d
9. Ceylon, China (Taiwan) Chile
10. Dornini can Republic, Poland, . Australia, Austria, USA Yugoslavia
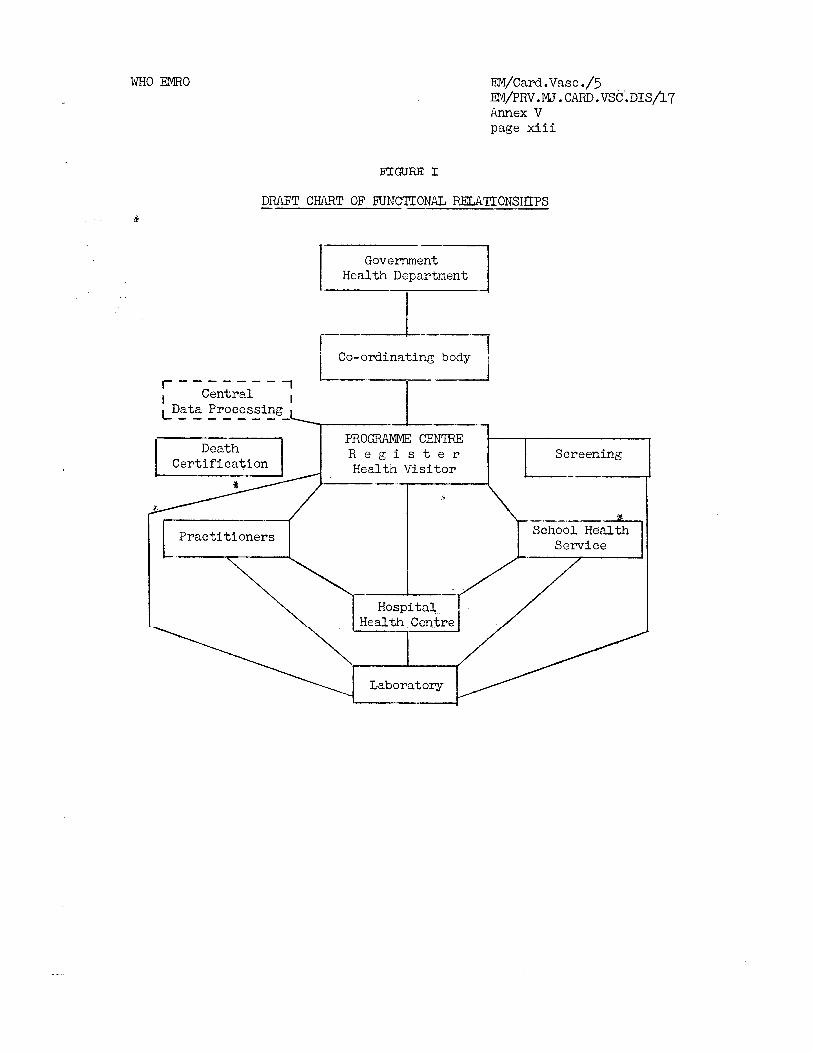
WHO EMRO EM/~ard .Vasc ./5 EM/PRV. M J . CARD. VSC. D I S / ~ ~ Annex V page x i i i
DRAFT CHART OF FUNC'I'IONAL RELATIONSHIPS -.
Government Health Department
-
I -2 I -----I I Co- ordinating body
I - - - - - - - - - I - , Central , ,-Data Processing - - - - - - - -
PROGRAMME CENTRE R e g i s t e r
Cer t i f ica t ion Health Vis i tor
School Health
Health Centre
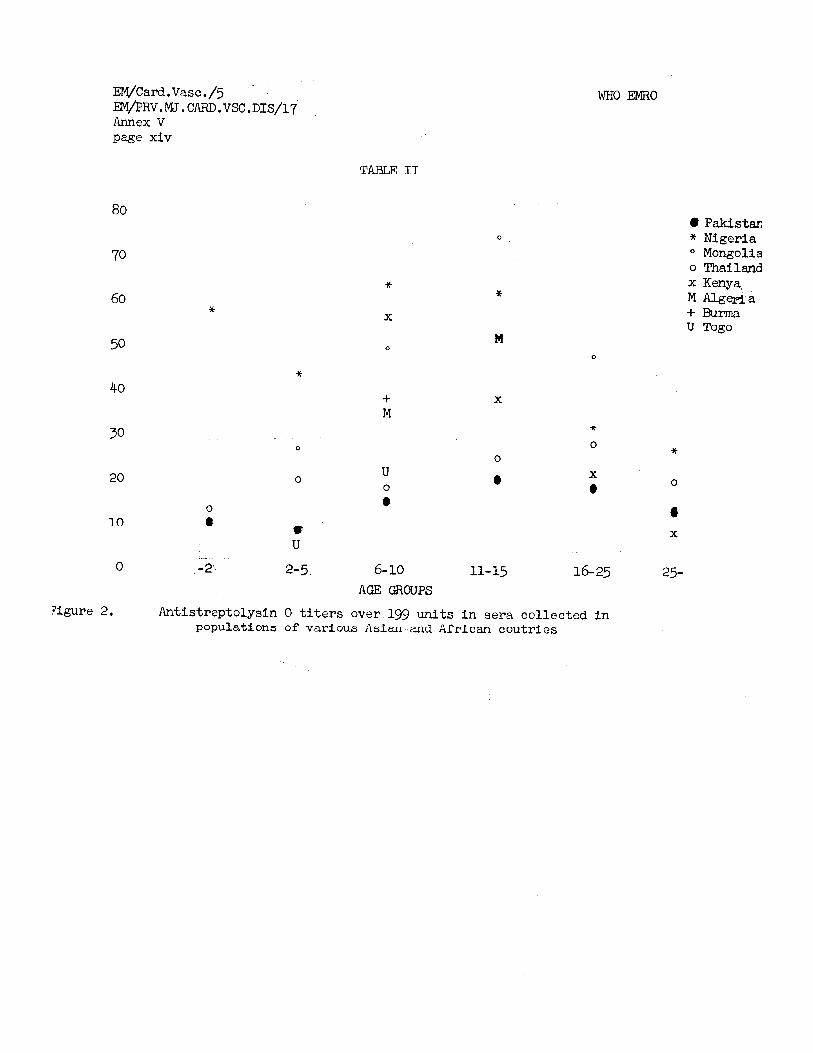
EM/Card.~asc./5 EM/PRv. M. CARD. VEX. DIS/17 Annex V page xiv
TABLE IT
u 0
e
6-10
AGE QiCKTPS
WHO EMRO
e Pakistan * Niger ia O Mongolia o Thailand x Kenya, M Algeria + Wlrma U Togo
Figure 2. Antistreptolysin 0 titers over 199 units in sera collected in populations of various A s i a and African coutries

WHO Elmo EM/Caril.~asc ./5 EN/PRV.W. CARD. VSC. ~ 1 S / 1 7 i~nnex VI page i
ANNEX VI
D r Paul Mill iez* WHO Temporary i ~ c l v i s ~ r
f ~ r t e r i a l hypertonsion unquestionabljr doserves t o a t t r a c t tho a t t e n t i o n of public a u t h o r i t i e s , phys ic ims and t h e population i n general , i n view of i t s very important r o l e i n t h e gcncsis of atheromatous carcliovascular d iseases .
It i s a known f a c t t h a t i n most c i v i l i z e d countr ies , mor ta l i ty from cancer reaches 18 per cent w h i l s t cardiovasculo-renal d i seases a r e responsible f o r 47 per cent of dcaths.
A r t e r i a l hypcr tens inn is m n s t f r i ~ q ~ l r n t . i n .subjects suffering from a therosc le ros i s . It cannot, however, be sa id , a t l e a s t f o r the time being, whether thc re is a rc la t ionsh lp between them. What can be a s s e r t e d wi th c e r t a i n t y i s that i n man the re is s i g n i f i c a n t a r t e r i a l hypertension i n 50 per cent of i n f a r c t i o n cases. I n women, the proportion reaches 76 per cent and what i s most remarkable is t h a t a r t e r i a l hypertension is discovcred more f requent ly i n coronary p a t i c n t s when t h e p a t i e n t is younger. Cases of 1i1yucurz2lal inf i i ; r -u t iu i l w i t l l u u t l-rypertension are obscrvod under forty ycara only i n 2 per ccnt of t h e pa t i cn t s .
A r t e r i a l hypcrtcnsion commonly appears between twenty-five and. t h i r t y years of agL. It may be a t f i r s t a border l ine a r t e r i a l hypcrtcnsion, l e s s f requent ly it i s a l a b i l e hypertension, i n which case i t is discovcred during systematic examination. Bcfore measuring the blooir pressure, the presence o f 2 2 a t h o l ~ g i c n l r i s e woulcl not be obvious except f c r a c e r t a l n degree of nervousness, o r sometimes a vascular ercthism. Such hypertension, although nc t grave, cven i f l a b i l e , i s of an obvious i n t e r e s t , a s t h e incidence of a r t e r i n l thrombosis is s i g n i f i c a n t l y h igher i n these cases than i n heal thy ~ x r s o n s .
The f a c t remains t h a t where the re is a r i s e i n blood pressure i ts func t iona l repercussion should be immediately invest igated: t h e p a t i e n t should be c a r e f u l l y questioned on the following points.
I n t h e encepnalc-retlnal system, a r t c r l a l hypertensloo rr1a.y Lc: manifested by ccphalec., o f t en t r u e hemicranic o r migraine, which a r e mistaken by thc physician o r t h e p a t i e n t a s s igns of a l i v e r inadequacy. The rhythm of t h e headache, i t s s e a t and. i n t e n s i t y , i t s gravat ive o r pulsa tory character , time of evolution, t h e method used t o soothe it must be s p ~ c i f i c i l . Occ ip i t a l sephaleas seem t o be a more gloomy prognosis than f r o n t a l cel2hal;as. Whether t h c p a t i a n t i s using an ta lg ics , including high doses of phcnacctin, should bc ascer ta ined.
+Professor o f Mc3ce l Cl inic , H8pital Broussais, Pa r i s 8e

EM/Card.~asc ./5 . EM/PRV.MJ . CIIRD.VSC.DISJ~~ Annex VI p a g ~ ii
WHO mo
Floating black spo t s (muscae v o l i t c n t c s ) - a point which need not be devclopccl a s i n t h e pas t it was adequately emphasized - a r e not a spec i f i c s ign of a r t e r i a l hypertension, a s t h ~ y may be observed i n shor t - s ighted persons and persons s u f f e r i n g from c o l i t i s although they a r e of ten contemporaneous wi th t h e onset of hypcrtansivo angiopathy.
It is a l s o important t h a t tho p c t i c n t mentions t h e presence of giddiness, a buzzing i n the e a r o r wheezing. k s t range phenomenon i s that MQnibre's Cisccsc (audi tory v e r t i z o ) i s o f t e n found a t t h c onsct of a r t e r i a l hypcrtcnsion and w i l l recur only many clecadcs afterwards.
Durinz thc cxminat ion, t h e p a t i e n t should bc asked whether he has e p i s t a x i s from t i n e t o time.
Conc~rnin;; thc pulmonary c i r c u l a t i o n or" the bloocl tlyspnea of c f f o r t should be c s ~ e r t n i n c ~ , which can e a s i l y be measured i n an urban cnviron- m e n t hy thc n ~ u n h ~ r o f flizhts of stail-s in thc r lwcl . l l ing. Thc pat ient should. a l s o bc asked whether when makin;; such an c f f o r t hc s u r f e r s from r e t r o - s t t r n a l , epigastric o r epi t rochlean pains. It should be kept i n mind t h a t very frequently an aerol2hzgy of e f f o r t i s a coronary equivalent o r a t l e a s t a s i s n of bad sub-diaphragmatic a r t e r i a l c i r c u l a t i o n .
The presence o r absencu of i n t e r m i t t e n t c laudicat ion of t h c lower limbs sbuulil bc i ~ l v t ; s t i ~ a t c d .
Impaire2 run?-l funct ion can be nsccr ta ined by one question only: i s t h c p a t i e n t obliged t o wake up dur inc the night t o u r ina te , whilst ha has no s i g n of ~nlargt : : pros ta te , nor fibroma nncl he i s not induccc! by s leeplessness t o re l i eve h i s bladAer i n order t o s l e e p again?
This quick examination is completecl by an assessment of t h e p a t i e n t ' s personal a n u a m i l y medical h i s t o r y .
I n h i s personal medical h i s t o r y the following po in t s should be invest igated:
- l a t e n ight enures is - unexplainec'. f ever i n childhood - repeated c y s t i t i s - acute rheumatic fcver - acute o r subacute glomerulopatny - tubulop~l thy - i s o l a t e d prote inur ia - nephrocolic a t t acks , o r - gout a t t c c k s which the p a t i e n t f o r g e t s when he t r i e s t o r e c a l l h i s
previous i l l n e s s e s .

EfI/Card .Vasc ./5 EM/PRV,MJ .cAR~>.vsc,DIS/~~ Annex VL page iii
A s f o r women, the h i s t o r y of pregnancies, t h e absence o r presencc of prote inur ia , of hypertension, of an excessive weight increase , u r i n a q in fec t ion during the pcriod of pregnencg, t'ne weights of the children a t b i r t h (an i n f a n t of l e s s than two and a hali ' k i l o s i s an almost p o s i t i v ~ i cd ica t ion t'nat angiopathy was already present a t t h e time of pregnancy, on the o thcr hand an i n f a n t whose weight exceeds four kilogramrnes musk always be considercd a s suspicious of an ignored d iabe tes ) should a l l be ascer ta ined.
For the 2a111ily h i s to ry , note should be taken without too ~ m c h ins i s t encd , of thc agz a t death of t h ~ parents, brothers and s i s t e r s , e spec ia l ly w h ~ n thz cause of t h s i r dcath i s associa ted with ce rebra l hemorrhage o r a myocardial i n f a r c t i o n . This i s an i t iportant f a c t o r and i t s predic t ive value should not bc overlooked.
Trlh~n t h i s qu i s t ionna i rc i s cndcd, the p a t i e n t ' s modi of l i f e , h i s i-~qbi t.s and bi.havinur should be inv2st igated. T ~ c tyge of work i n rrhich hc is engaged may a l s o play a pr~dominan-t r o l e .
The r o g l a r usc of l iquor ice , of contraceptive p i l l s , may be responsible l o r the onset o r t h e aggravation of an angiopathy.
An sxcessive consunlption of s a l t , and use of tobacco, play a l s o unqucationably an aggravatilli; rolc.
An accurate assessment of symptoms which may i n d i c a t e a su rg ica l ly curable e t io logy sho l~ ld always be nadc.
Thus, r i s e s a. blood pressure, very abundant sweating cornpullino" the p a t i e n t -to change h i s c lothing, Recklinghausen neurofibromatosis, d iabe tes without 2. rainily h i s t o r y suggcst a pheochromocytome.
Polydipsia, p e r s i s t a n t const ipct ion, pseudoparalysis, t e t ang ctucc!:s cculd i n d i c a t a n Conn cyndromc.
A lumbair traumatism, hematurias v r l t h c l o t s , nephrocolics without stone evacuation could mean t h a t a r e n d a r v t e r i a l l e s i o n i s prcsent; as could a suddcn onset of hypertension i n s person wi th normal blood pressure, suf f c r i n g from an a r t e r i t i s .
Repented urinary inTect iu : ls , cto l i v e VL' passivc r-vflux pain, polydipsia, nocturnal cnurcs is , suggest a raf lux, a d i scase of t h c s c r v i x vesicac.
An e v o l u t i v . ~ glomerulop~thy i s t o bc feared i n the presence of an o ld permanent prote inur ia .
A r t e r i a l hypai-tcnsion may a l s o appear during t h e progress o r thc decl ine of r e n c l tuberculos is .

~1/~ard.Vasc. / '5 . EIVI/PRV.PLJ .CAFXI.VSC.DI~S/~~ Annex VI page i v
When t h e questi0nir.g Is comple-tcd, the p a t i e n t i s exar~incd. Yh.<. zxamination must Sc c x h ~ ~ ~ s t i v e 2nd inc?.u.cLc the measurement of blood pressure i n both anas at. thc f.i.rsi; e ~ a n i r ~ c t l o n , i n a recurnbent posi t ion, then whilc standing an$. aftoziards c f t c r cti e f f o r t of t ~ n flex!.oiis of thc lower lirnSs.
I n the s u c ~ ~ s s i v ; cxa:ninekione, blood pressure should always be measured i i i th; ~ 3 1 ~ 213..
I n an add l t , a ~ I I ? E P L * F C :I<~;ICT than 1110-90 is always a pathologic; '.
s i g n whcn i t LQ y'cpyla--!-y Scilnd. T.lcr? i s r c c lea r -cu t l i m i t t o ihc pathological J f L 2 S S U r b anLl i t i~ a wel l known l a c t now thac the l i f o expectancy of a 9crson j s di rec t1 y pi>o?or:icncl. t c h i s blood p r e s s u r ~ l e v c l s . k man whosL p1c;surc i s 300-63 has rnorz chanccs t o livc: t o an o ld age than :: mail wkosc p-c.;;urz f-c 12~--80 who i n h i s t u r n w i l l l i v c longer than 2 inzn ;vi t h c? 140-90 p r ~ ~ s s u r c .
Tha c l i n i c a l cxamina5or ph2nlc! a l s o include palpat ion 02 t h c a r t e r i e s of t'r, h ~ k , ? li~nu;, i'ne LLPPCP liinbs an3 the ntck.
The epignstriu~nl 3rd tl1.c !l~mbar. foesa, the i l i a c fossa , t h e s i d c s , scarpa ' s t r i a n g l.c, the carotids ar?l tin, supra-c:!avicular cavuifl should be examined by auseu l ta~ i .on ,
Thc physician shou1.a he ab lL C-o cxnrain~ rapidly thc fundus ocu l i , and thcn p rasc r ibL ihL2 sxaninnticns r ~ q u l r ~ ? , Thcse vary according uo the nature of the c y ~ s ~ ~ h c trouk12s fmnd.
i n an jndird&dal -:vLthout iiilportant functi-onal d is turbances i t is not a!-ways c e r t a i n t h e t ap e l e c t i ~ o z a ~ d i o g ~ - ~ ~ m is necdtd, but i t i s ad7?isable, i l rhl l~ tfi!<lnrS 2'3 $ 3 ~ LII!IL I I L G ( - D ~ ~ ~ - Y , t,u ask f o r c, garrotliss kaliemia, a creatini,lernia. :. L) -ic~er?"La. n t o t a l cho les te ro l , t r i g l y c ~ - q l d c s , a t e s t f o ~ a l k m i n 2nd. cdg2i' iL: 24-'r,v1r urim:s, ~ h c VwM.I?I. r a t c , a d , i f possible, en hdd'.s coun , t-a;.
Very r i c h nat,ions :i::.vt: FJ;?. \,-en US syetc..natic urography. It .is considered thr.t it s i 7 3 ~ l j . 9~ carr_i.:.i? out i n thc fomi of a timed urograpil;. without compression, CLLL tb: mix of C ~ L I per mlinuto during the f i r s t f i vv minutes, ir . order t c l ':FP+. ~ 7 : t 7~ ?*Ciztd OP oxcrotion asyinmetry 2s tho i n v o l v ~ d kidney may c.ppricr srfla3: c? o r ;,ho.;i 2 delayed excret ion of tki: c o n t r a s t medluiil. I n svc.?; LL ccse ~~rotjl-aldly shcluld be complotcd by an urea r ins ing (30 LI!. 3-11 200 m7. of s e x m ) t o a s c e r t a i n ;rhethcr i n conf i rnat ion of tt:> Pirsi f.:lpression a "more accuratc p ic tu re" o f thu a f f e c t ~ d s ida is discovcr.cd: 3i1ll.c;l w3.th t h e dclnyed evacuation of thi: iodized substenzc.. 7he:;c ?xaini n:&-ti-ins 2re q u i t e .cdeql~ate un less .
a b n o m a l i t i c s PJC: detcr:t.erl.

WHO EMRO EM/Card.Vasc ./5 EM/PRv. NJ . CARD .VSC . ~ 1 S / 1 7 Annex V I page v
The de tec t ion of a high V.M.A. m y l e a d t o ca r ry ing ou t e i t h e r a r e g i t i n e t c s t o r a histamine t e s t , but c h i e f l y t o m n e d ~ g t h e vanylmandelic acid dose and p r a c t i s i n g anarteriography t o determine t h e s i t e o f t h c l e s ion .
A k a l i a n i a under J, r.Gq 5 (mi l l i cqu iva len t ) w h i l s t the ind iv idua l does not absorb l i q u o r i c e and is not subjcztcd t o s a l i d i u r e t i c s , should l e a d t o the determination o r t h e blood sodium and bicarbonates r a t c s , and t h e determination of the sodimi and potassium ri?.tes i n t h c ur ine; t h e presence of a natraemia and a l k a l i reserve a s s o c i a t ~ d wi th a k a l i u r i a over 40 mEq by l i t r c i n case of hypotaliaamia, nus t l e a d t o t h e determination of plasmatic aldostcrone r a t c o r c l s e the apprecia t ion of t h e 24-hour u r ina ry t c t ra -hydro-a ldos tc ron~ r a t e f o l l o v ~ ~ d by a systematic t es t of the a c t i o n of a s u f f i c i e n t dosc of spironolactone (an average of 300 mgr during th ree weeks), The rcvcr t ing of t h e pressure t c normal i n these condi t ions espec ia l ly when the b io log ica l examinations a r c pos i t ive , suggests a Conn syndrome.
I n t h e casc of a secretion asyrnrnctry shown by t h e timed I.V.U. ( intravenous urogrophy), ar tcr iography should be prescr ibed a s it may d i sc lose u n i l o t c r a l o r b i l a t e r a l l e s i o n s of t h e rena l a r t e r i e s o r confirm t h e presence of a u n i l a t e r a l parc;nchymctous c t t ack . I n the l a t t e r case it i s advisable t o complcte the inves t iga t ion by sc int igraphy w i t h mcrcury b ich lo r idc not only t o a p p r e c i a t i t h e value of t h e a f f e c t e d kidney but mni n l y t.o apprccinti? the q u a l i t y o f t h e suggosed hea l thy kidney.
A l l t h i s questioning and inves t iga t ions do not l e a d t o da tec t ion of s u r g i c a l l y curable ccuse of hypertension, excopt i n a vcry r c s t r i c t c d number of cases.
I n a h ighly spec ia l i zed French service , onc f i n d s out of 100 i n - patients one casc of phcochrom~cytoma, two cascc of Conn syndromo, one casc of l i q u o r i c e in tox ica t ion , four l e s i o n s of t h e rcna l a r t c r y , two of which a r c curable, thrci: cases of i n t e r s t i t i a l n e p h r i t i s ( rc f lux , l i t h i a s i s , tubercu los i s ) .
I n a nephrology u n i t , fo r ty - f ive cases of hypertsnsion suf fe red from glomerulopathy. Wl t it i s obvious t h a t this r igure i s inaccurate a s only individu?.ls su f fe r ing from high hypertension o r those whose symptoma- tology made a probable etiological diagnosis poss iblc a r e h o s p i t a l i z e d i n the spec ia l i zed services.
When nc czuse i s found o r when it is eventual ly not curable s u r g i c a l l y - 2nd this represents approximately 99 per cent of a r t e r i a l hypertension cases i n common medical p r a c t i c c - one must be s a t i s f i e d wi th medical treatment which has made tremendous advances i n t h e ccurse of recent years.

~ ~ / c a r d . ~ a s c . / 5 . EM/PRV.MJ. CARD .VSC . ~ 1 S / l 7 Annex VT page v i
The d i e t should be sodiurnlcss, poor i n l i p i d s and sometimes r e s t r i c t e d i n carbcl~ydzates The p a t i e n t should s t n p smokin~, absorbing l i q u o r i c e o r t-king c ~ n t r a c e p t i v r , p i l l s . A s far as possible , he should a l s o avoid t a k i n s a s p i - i ~ x i t h a high phenacetin content.
The p a t i e n t shoi:ld lcnd a heal thy l i f e avoiding v io len t physical exer t ion, e s p e ~ i 2 ~ l l y o f J ~ a r ncn l s , but shoule take up a moderately a c t i v e spor t . Diving and bath:.ng i n cold water a r e forbidden.
The e f f e c t s of G i ~ ~ g s a r e va r iab le but i n t h e course of these l a s t few years they hcve become p a r t i c u l a r l y eff icacious . Treatment s t a r t s by using s a l i d i u r 2 t i c s associa ted :vith potassium s a l t s o r spironolactones. I f the l a t t c r arc. i n s u f f i s i c n t , a s f requent ly occurs, f o r rej-glarizing t h e blood pressure, they a t l e a s t havc a mordantinf; e f f e c t which renders a l l o the r ant ihyper tensive drugs e f f i cac ious which a r e added t o sa l i c l iu re t i c s , spironolactones i n progressively increas ing doses and i n assoc ia t ion , as one o r t h e o ther of these drugs may a c t on d i f F c > r e n t p o i n t s of impact.
Thus, may bc given successively, afterwarcls a t t h e same time, two t o th ree t a b l c t s of Alpha-methvl.cpa, two t a b l e t s of manethidine , two t a b l c t s of hydralazinc, one o r two t a b l e t s of rcscrpin , one o r two t a b l e t s of clonidin and scmctimcs merely a beta-blocking agent i f tho p a t i c n t docs not s u f f e r from asthma o r i f he has no b d l e branch block.
Unfortunately i t is of ten necessary t c ?.ssociatc c thor drugs wi th those a l ready ind ica ted , Thus i n t h e presenoe of a spontaneous o r induced by s a l i d i u r e t i c s Izyperuricemie, a n t i - u r i c clrugs a r e ?dL!ec-l, a s f o r example i n t h e presence of h y p ~ r c h o l e s t e ~ o l e m i n , hypolipeniants a r c resor ted to .
L i f e f o r t ' r x p a t i e n t becomes complicated i f the assouia ted drugs a r e tuu n u n e r u u s . The nat:ent g e t s depresscC an? t i r e d , e spec ia l ly a s i n a b i l i t y and gynecomastia may incrcnse h i s 2Liscomfort.
The f a c t remains t h a t a t t h e present time, thanks t o modern therapies , t h e l i f e expectancy sf' an iaclivitJua1 s u f f e r i n g from hypertension tends t o approximate more and. more t o t h e l i f e expectancy of an ind iv idua l having a normal blood pressure ,
I n F'rance, it pias founrl t h a t i n 1960 a l l cases of deaths from malignant hypertension were 109 per c e ~ i t wi th in five years a t most following t h e onset of "malignancyu. IJowe,c?ays, aftur fi JL. yedrs, 35 per cent of cases a r e still a l i v e and this proportion of su rv iva l without funct ional d i so rders anC with a blood pressure nearer t o t h e normal than before, is an encouraging fo recas t f o r the f'uturc, except f o r the r e l a t i v e l y high frequency of coronary accidents , although of'ten minor, i n p a t i e n t s whose a r t e r i a l hypertension h a s been graclually regularized.

EM/~artl .Vz.sc ./5 E~VI/PRV.MJ. cm.vsc . D I S / / ~ ~ Annex V I page v i i
Tc conclu,lc, it i s r,ecessnp-- t t c nc",cztiously i n t h e cnse o f c r t c r i c l nypertensicn, ns unqu.estionably the re i s - (luring angiopathies associate_-
~ i t b hypcr tsns lsn - cn irngortznt psycliosomatic fac to r . Thc rcli . of the ~ S s e r v c r s an2 cbstrv,;,l ij a~sentia! . and the rlccl~s of apprec ia t i an 2 . r ~
only cmdc . It
various such a s
i s not kn~ivn zs y e t ~ c c u r a t e l y the wzight t c bc ascribe? t c tilt i 'uncticnal s l ~ n s . 'me trzlu:: 02 so-c211oA cb jcc t ivL symptoilis thL x,asurunon"i of t h e 5100-1 p r c s m r i cn-1 the cxaminatiun of
iht f i ~ n 71;s ocu l i nrt t l r t knowt?. The rclc or" ~nvironrncnt, cf psychc1oricc.l f a c t o r s , bcth or: th<, ;mrt c , f t h ~ physici2n an;: on t h e p a r t of h i s patients, cannot S c c a l c ~ l ? ~ t t 2 . .
Most ccrJiaii;ljr the: ilcuble-blinrl iildth~d a f f o r d s a rneans t o npprcciat , t h c a p p r ~ p r i n t ~ n e s s cf a t h ~ r a p j , but i n orf7.cr t o be v a l i d it shoulc: bd
bzsed on long c>~ra t ion c ~ p ~ r i m t n t a t i o n vrhcrc a l s o t h e secondary zncl t c r - t i c r j c f f e c t o of Z~IL mo?.ications choul?. bc ~ E E C E E O ~ .
It i s 2.s g - t iinp,>ssible t c know tEic conscqucnccs of i l i c t a t i c infrinc'e- ments, of thc r d ~ ~ o r s a l cf p a t i e n t s t o thoi' t s x i c h a b i t s , of t h ~ nc t ion cP nssociat~:! so-c-11~:. anodync n c l i c a t i o n s t o which thc p a t i e n t may r c s o r t :.ccr,r-l,ini; t o h i s idcz t h a t t h ~ ail",-hypcrtensivc therapy ap;3ears t o him l'o,voureble, unl"zvourz'olt: o r of no value.
2.t l e a s t f ~ r tnb t i ~ l t . being wor13.rli2.c s t u d i e s have put folwarcl scmc iirm ideas :
) The fcl lowing 2 . r ~ ncv c l c a r l y ~ s t ~ ~ b l i s h c ? ~ :
- Thi: e s s e n t i a l r o l e of t h c blooi? prcssure l e v ~ l s even physiological , G n t h e l i f e - span of ucch in;;ivi?~ual;
- t h e very l i ish frcquui.ncy of a r t e r i a l hypertension; - the usual. przsencc of a the rona tas i s i n ind iv idua l s su f fe r ing from
high blooi; pressuro aver long pcriods; - t i e unusuaL pcrcsntages of artc-1~n1 hypcrtension i n indivifiuals
suf f o r i n s frc;:~ ?.tlicrom~tosis :: - the fnvournblc 'ction of t h c various nnti-hypertensivc therapies
cn l i f e c:rpcctancy i n inclividucls suf f c r i n g f rotn high blood prcssurc, or! ti.12 Trequcncy of cercbra l anc! r e n a l complicaticns;
- the inefficacy df anti-hypcrtensivo t i e r a p i e s on t h e frequency of c0rcm"ir-y x c i d c n t s .
( 3 ) FurLhcr r e s ~ a r c l i i s needed on:
- the tru; i*zlationship between a r t ~ r l a l hyptr tension and a the rosc le ros i s ;
- t h e r o l e of Y ~ L 2rcp i n blood prcssure clue t o treatments on t h e devclopminc of scmc vzscular thrombosis;

U Y I / C Q ~ ~ .Vase ./5 EP/PRV.MJ .CARD ,VSC , D I S / ~ ~ Annex V I F v z ~ v i i i
- t h ~ preventive o r incueing ac t iun of c e r t a i n d i e t e t i c zn?. therapeut ic prescr ipt ions , of c ~ r t a i n in tox ica t i cns , oLn c e r t a i n n o k s cf l i f c : on ~ , r t c r i ? l i lypjrtcnsion 2s w L l l as on nth , rcm~tosls ;
- tht secc~.'-zlry br t e r t i a r y c f f ~ c t s ~f t h L th,rapcutic remecli~s a t our i i ispcsal cn t h e c~rbo!ly~ll~3ti;.l and u r i c m e t a b ~ l i s n , t h ~ renal function, tha cncbcrine glands and psychism;
- hirzcli ty i n e s s e n t i a l c r t c r i a l hypcr~tcnsion, - L k erTeuLs OC new :rugs.
( c ) It goes without scying t h n t thc C~ey wlicn t h e t h ~ r a p y of hypcr tensiar - whethcr sympt,,:,ie-~ic o r e t i o l o g i c - r e e l l y c x i s t s , t h c dcublc-'ulin:: s t a t i s t i c a l n~thc:' i r i l l nc longcr havd 2ny j u s t i f i c a t i o n a l t h o u a systcmntic res tc rch Ln p r e v c n t i ~ n cnC cpiCLmiologg rzmain v a l i d and c?..nnot b t c3~r'iec'. t h r ~ ~ g h s u ~ ~ c : s s f u l l y unless a l l c r t e r i a l hypertension s p e c i a l i s t s , ~?%, i '~ t~vcr mzy bt t h ~ i ~ S,isciplinc, thzi rs l t v c l and t h c i r cbuntryg with thL assistance ~f thc: g r e a t mcdicc-social a & i n i s t r ~ t i o n s , ?cciipt t c a a ~ r c t c 2 11arc. nnd f a s t long-tom1 scheme. I n t h i s S i ~ l . l , i n l y consc i~nc icusncss , p a t i t n c ~ L?.~L! ti111c s r i l l l e v 1 t o f r u i t f u l r c s u l t s . Tnis i s easy td w r i t , , d i f f i c u l t t o apply.

WHO m o ~ M / ~ a r d .~aso. /5 EM/PRv. MJ . CARD. VSC . DIs/17 Annex VII page i
ANNEX VII
CONTROL OF HYPERTENS1 ON IN POPULATIONS
Dr T. Strasser Medical Officer, Cardiovascular Diseases Unit, WHO/Headquarters
BLOOD PRESSURE IN POPUU'I'IONS
Arterial blood pressure is a well regulated haemodynamic variable. A oonsiderable number of fsotors are known to oontribute to itc regulation, some of them are still incompletely understood and there might be some more unknown factors.
Blood pressure is ceaselessly changing like many other dynamic variables of the living organism, and its assessment would be difficult, were we to use certain simplifications. These are based on the century-old principle of colllprabsirlg exter-r~jlly Lhe br-aulrLul ilrlery, though a new non-invasive technical approach is very much wanted. "~asual" blood pressure, in terms of systolic and diastolic values, measured with the classify individuals according to their arterial pressure. The perennial debate, whether there is a "true" dividing line between "normotension" and "hypertension" depends, of course, on the meaning we convey to these very terms m d on the use they are meant for. There is no aoubt that these tepms too, are simplifications - but, it should be admitted, very useful, almost indispensable ones.
If blood pressure is being measured in populations at large, adults are usually found having (cssual) values of 110-140 m/Hg systolic and 60-80 rnm/hg diastolic pressure. As well known, in many populations the values increase with age, in some they do not. However, in most populations a considerable number of individucls is to be found with blood pressure values being, at repeated measurements, definitely higher than the above mentioned range of "usual" pressures. Roughly, ten per cent of all the adults, both males and females, may have blood pressure values at or above, say, 60 and/or 95 rnm/Hg* in technically developed as well as developing countries.
HYPERTENSION IN POPuWI\TIONS
Although, usually, high blood pressure is a sign without symptoms, It is far from being an irrelevant sign. Even values slightly higher - +There is no sharp li& of demarcation between normotensive and hypertensive levels - i.e., it is not possible in the individual to give an absolute figure for the upper limit of normal blood pressure - for screening purposes in population groups certain values may be accepted, using "casualtT blood pressure recording: (1) below 140/90 mm/Hg - normal range; (2) 160/95 and above - hypertensive range. Report of an Expert Committee (1962) Arterial hypertension and ischaemic
heart disease, preventive aspect, GdHlth Orm. techn. Rep. Ser., a

EM/Gam.vasc ./5 EM/pRV. M J . CARD. VSC. DIS/17 h e x VII page ii
WHO m o
than the usual ones are, s t a t i s t i c a l l y , associated with higherthan usual mortality ra tes . The posi t ive correlat ion between blood pressure and general mortality is a continuous one, s t a r t i ng already a t the lower end. Blood pressure i s a graded charac te r i s t ic and the r i s k depends on the leve l of pEssure.
A t the upper end, natural ly the hazards of high blood pressure become even c l in i ca l ly obvious i n the form of i ts d i r e c t complicatbns: hyper- tensive hear t disease, hypertensive renal disease, r e t i n a l haemorrhage, and cerebral haemorrhage. However, even l e s s marked elevations do oontribute t o the development of a therosclerosis , and t o i t s main compljcations, ischaemlc hear t disease and ischaemic brain disease. Population based anatomical s tudies have shown impressive correlat ions between both degree and extent of coronary atherosclerosis and blood pressure previously observed. Several prospective epidemiological s tudies have demonstrated the importance of blood pressure as a r i s k fac tor of coronary heart disease, even i f only moderately above the usual values i n a population. I n a WHO epidemiological study, carried out on 7 700 persons i n seven c i t i e s (~iraycuna. Malm'd, Moscow, Prague, Riga, Ryazm md S a b ) , those i n the upper t h i rd of the frequency d is t r ibu t ion of blood pressure had a 25 per cent higher pre- valence of coronary heart disease than those i n the middle o r lower third.
Higher blood pressure thus def in i te ly seems t o be incompatible with "complete physical well-beingn, an essent ic l component of heal th l i k e the top of an iceberg, only i t s d i r e c t comglications are i m m ~ d i n t . ~ l y rlinically vis ib le . The epidemiological method, however, discloses i t s bulk, unveils i t s r e a l impact on the heal th of populations. I f both the frequency and the relevance of high blood pressure are takcn i n t o account, hypertension should be regarded a s a large-scale widely spread epidemic.
ADVANCES I N THE TREATVENT OF HYPERTENSION
The cause of hypertension i s usually not known, and therefore cannot be prevented. Even i f known, only exceptionally can hypertension be cured by t rea t ing the cause. Thus, treatment of hypertension means preventing i t s complications, and the most plausible way t o do so is by lowering the blood pressure i t s e l f . I n the past, hypertension treatment was v i r tua l ly ra re ly more than placebo-therapy. During the past two decades, however, several families of potent and r e l a t ive ly harmless hypotensive drugs have been developed. Long-term efficacious, systematic treatment of hypdr- tension has thus become possible, the more necessary i n order t o prevent the complications, Between 1961 and 1970 a number of s t u d i e s h n s d ~ m n n s l r a t e d the favourable long-term e f f ec t s of hypotensive treatment i n pat ients with more o r l e s s severely elevated blood pressure, the incidence r a t e of compli- cations anddeathbeing smaller i n the t rea ted than i n the control groups.
EM/Card .Vasc . /5 EM/PRV.MJ. CARD .VSC . D I S / ~ ~ Annex VII page iil
The most signiPiccult &vcst igat ion i n t h i s f i e l d is the well-known T'eterans Adninis-Lration Co-operative Study on Antihypertensive Agents; published i n 1967 m d 19'70. Mope lhan 5G0 male hypertensive pa t i en t s ( d i a s to l i c hloo53. pressures rruzging from 90 t o 129 r;lm/~g) were randomized i n t o a plscebs m d p n ac t ive therapy group. T-reatment w a s conducted a s 2 double b l ind tr i-al . Already af- ter .tvrentjr months of obsemn.cion there pras a s i gn i f i c an t clifference ir? tlie incidencz of complications between $122 two groups i;? +,he lipper pan$ of the d i a s t o l i c pressure range (115-129 nm/tI;). iiZter th ree moi-E yccrs of ohser-a t ion, it became miden t t h a t the prognosis of patients vrrlj;:~ ?.~~i.tia!. va!.ucs o? d i a s t o l i c presaure from 105 to 11)1 air;?,
considerably impPo-,res with trextment; the benef i t i n p r t i e n t s having i n i t i a l values of 90-1011 rnm/~g was i e s s c l e a r cut.
I n view oP the high p.evzlence of hypzrtension numerous members i n many popuLazlons should bc e l l g lb l e f o r trea%nent. Or1 l h e u ther 11a11~; some observationz show th? i i f a community is s u r v ~ y e d 3s a whole only e f r a c t i on of '.hose who need -brea.tment acccrding t o widely accepted standards, a r e indaed being ~ r e a t e d ; n s t i l l smaller p a r t receives systematical a~ld ef f icacioas keatment.
Community based daJ,a f?oa Baldwin County Georgia by J . A . Wilber and Wilber & Enrrow showed tht i n n random sample, 42 per cent of' hyper- t cn s i~ r e s were unaware of t h e i r condition. Only 30 per cent of t he knawn hypertensives were uwler treatment and only 17 per cent of t he known hypertensi-res weye v.ncler what uas ca l led "good contfrols' . Doctors l o s t t r a ck of 56 per Lent or' hypertensive, within th ree man% hs. Caldwell ~t cJ4 studied the dr s p o u t problem 112 an ti-h~rpe:~tensive treatment i n n :3ilat s h d y of s o c i a l and emotional f a c to r s influencing t he pa t i en t s ' a b i l i t y t o f o l l ~ w t ~ c a t m e n t . Only 13. per c a t of pa t i en t s first seen ,1113 t-eatec! f o r kvpercension I n !96i were Pr~und t o be on treatment a f t e r f i v e gears. By stxi-dylng i n p ~ t i e n t s hospi4,alized f o r emergency c o m p l i c ~ t i ons of hypertensic-I the cadses leading t o drop-nut, I t became evident thslC i n one-third or' these pa-tients ioiu inco,ne and h j ~ h cos t of treatment w a s a r e a l i s t i c r eacor , bc-: t%t 2)1 3cr ceat of "drop-outs" abandoned t reatm~n7; un advice ot tllei.r 2hysician thus clear! 7 demonstrating t he importance of' m information pYogrmlr,c! f o r ph,vsicims. me most important f a c t o r was, however, absence s f not ibat ion due t o l ack 22 health cJucation i n t he pa t i en t s and t h e i r f amil-ies ,
I n n comm~mi.l;y of a d i f f e r e n t socio-cul.tura1 s e t t i ng , Tibblin a l s o found a high preva:lenne of 1~ypertensPon. The r a t i o of t r e a t ed t o un- trea.Led pa t i en t s r!ss rat,hcr pony i? msn; approximately two-and-one-half

WHO EMRO
times more hypertensive men were without than with treatment. Half of those being treated had unsatisfactory blood pressure levels, in spite of Cru,: therapy. However the pattern was considerably more favourable in women.
These and other similar observations indicate that appropriate action is needed for the control of hypertension in populations.
The term (disease) 'scontrol" may give rise to some misunderstandings clnd needs, therefore, some comments. It is applied, in this context, in its widest sense, meaning comprehensive struggle against disease. It ~efers to cll zspects of heslth protection: prevention of a disease or of its com>lications, early diagnosis appropriate treatment, rehabilita- tion health educstion and includes also endeavours to obtain better hcwledge of a condition i.a. of its natural history and epidemiology. The Prench counterpart for "control of hypertensioni7 is "lutte contrc. I'hy~ertension" and the Russian term "barba prati hipertonicestoi boljeznig'.
"programme" mexiis a designed, organized action and a 7qcommunity progrme" aims at health protection and promotion of a large number of silhjerts in n community, caverinj all of i t s members in the i d e a l cas,.
Generally speaking, the ultimate goal of any control programme is, by definition the conquest of disease. However, this ideal goal is at the end of a very long road passing through several stagzs. First of all, before establishing a programme reliable informamn is needed on the state of the particular disease in the particular population or community, its rates of occurrence, natural h i s t o r y p r a c t i c e of h e a l t h care other features. Such information is necessary both in order to be able to build up the plan of a community control programme, and in order to have a baseline to which later changes possibly induced by the control Trogramme could be matched. It is understood that data on the structure of the population itself are needed and also on other diseases prevailins in the area.
Seconcl, experience dictates - and common sence as well - that any control programm? undergo a test on a limited scale and within a reasonzbly limited time before being extended t o a p o p ~ ~ l a t i o n a t large. Such pilot programmes may be analyzed on four levels. First of all, they are expectec: to show whether a particular control programme is feasible at all and if so, under what conditions and which adjustments to real-life situations. On the second level, the following question is to be answered: has the progrme, if shown to be feasible, any demonstrable health protective

WHO m o EM/Card.~asc ./5 EM/PRV.MJ. CARD.VSC.DIS/17 Annex VII page v
effect? Therefore, the changes a t t r ibu ted t o the programme should be compared t o changes occurring i n a s imilar community where no control programme was operating.
RESEARCH ASPECTS
A p i l o t control programme may well show t o be feas ib le and a l so efficacious, and yet a la rge sca le extension may not be jus t i f ied , i f i ts output does not outweight the input, a t a third- level analysis. The i n m t includes not only the f inanc ia l and material cost of a programme, but a l so energy and time invested and, above a l l , the hazards of the p r o g r m e such a s unwanted e f f ec t s of medication and possible psychological harm caused t o apparently well-off individuals. The output englobes a l l beneficial e f fec ts of the programme: e.g. prophylaxis of complicatibns, prolongation of f r u i t f u l l i f e , prevention of human suffering. Some of these items can be readi ly quantified (e.g. d i r e c t f inanc ia l cost) . Others are difficult to assess nr arp pvpn imponderable (e.~. ~ s ~ ~ h 0 1 0 f f i ~ a l harm, prevention of suffer ing) . Clearly, a comprehensive assessment of the t rue gain of a programme i s extremely d i f f i c u l t and can be done to-day only by rough approximation probably i n qua l i ta t ive ra ther than i n quanti- t a t i v e terms- but there should be no reason t o r e f r a in from such an essay.
Estimation of benefi t versus "costs" is not a spec i f ic fea ture of hypertension or any other control progrtunmc. It is a general principle i n srny human decision taking underlying t o constraints and therefore underlying t o the pr inciple of trade-off. Even i n t he f a r l e s s complicated s i tua t ion of deciding whether hypertensive treatment should be s t a r t ed i n an individual pat ient , thz physician is wcighing the pros and cons i n . the par t icu lar case taking i n t o consideration the inconveniences and possible hazards of therapy - there is no harmless medication - and the expected benefl ts t o the pat lent . This arlrtlysls of a given situation cannot be replaced by any overal l m l e : the reason why, i n the WHO study t o be discussed l a t e r , only therapeutic guidelines, but no de f in i t e instruc- t ions a re given concerning drug treatment i n hypertensive subjects.
There i s a l so a fourth l eve l of analysis: assessment of efficiency. Two drugs. o r two programmes, may require a s imilar input (cost, hazards) but y ie ld d i f f e r en t benefi ts . That giving b e t t e r r e su l t s is the more e f f i c i en t one. Obviously, efficiency of community control programme can be evaluated only i f two d i f fe ren t , ye t comparable programmes a r e operating side by aide, a condition which will hardly bc cnoountered at the t i m e bein@.
P i l o t programmes thus have seveml important objectives, s i tua ted a t various leve ls , and rea l iza t ion of a higher-level objective cannot be evaluated unless t he objective of the preceding l eve l has been attained.
E~/~ard. Vas c . /5 EM/PRV.MJ. CARD.VSC.DIS/~~ Annex VII page vi
WHO m o
A pilot hypertensicn control programme is thus more than a mere attempt to start hypertension control on a limited scale; it is a complex study which ideally should be evaluated on a series of consecutive levels. Nevertheless the basic goal of a pilot programme for the control of hypertension is naturally, tc demonstrate how hypertension could be controlled in populations at large. A pilot programme is both an opera- ting model and a major research undertaking.
THE NEED FOR IN'I!ERNAlTONAL CO-OPERATION
Accur~d lng ly , the control of hypertension in populations should be preceded by pilot programmes. WHO is striving to initiate a series of such pilot programmes within the frame of an internationally co-operative project.
There are several reasons in favour of international co-operation in this field.
Hypertension is a world-wide problem, prominently important in many countries, regardless of the level of technical development attained.
The pilot programmes are also ccmplex research projects, and methodo- logical assistance may facilitate their tasks. By proposing a common methodology, results from various centres mi&t be comparable.
On the other hand, there are considerable differences between the various socio-cultural settings in which mertension control programmes are to be established. International co-operation may give rise to an exchange of experience from these various settings..
Hypertension is n c h r o n i ~ , usually slowly progressing, condition, In order to arrive at an evaluation of the incidence of hypertensive complications, n long observation period would be needed. However, by increasing the number of observed subjects, the observation time could be held within practical, acceptable limits. Big numbers of observations can hardly be carried out by any one centre, while in a co-operative project, hodefully, many observations can be pooled within the time limits of a pilot grogranme.
WHO A C W m E S
Definitions and epidemiological aspects of hypertension were outlined in previous publications of WHO, in 1959, 1962 and 1963.
The need for programmed large-scale control of hypertension was first

EM/~ard. Vasc . /5 EM/PRV. M J . CARD. VSC. D I S / ~ ~ Annex VII page v i i
for,:~ulated by WHO a t a meeting on t h e Prevention, Treatment and Rehabi l i ta- t i o n of Cerebrovascular Diseases. Guidelines f o r such programmes were ~ u z l i n e d a t a meeting on t h e con t ro l cf s t roke and hypertension i n 1971. A t present, ;JHO is promoting an in te rna t iona l co-operative p ro jec t f o r t h e establishment of a network of p i l o t hypertension con t ro l programmes i n a number of conmunities. The bas i s of t h e p ro jec t was es tab l i shed a t ,z \KG meeting on t h e community control of s t r o k e and hypertension, held i n Gijteborg i n l a t e 1971.
A t t h e G'3teborg meeting, inves t iga to rs from f i f t e e n centres frorn f o u r cont inents ngreed on a common basic prucedure fon carrying out p i l o t community control pmgmmmes. Par t i c ipa t ing inves t iga to rs envisaged co- operation between programmes i n t h e Following places : Barbados; Leuven, ( ~ e l g i u m ) ; North Carelia, Finland; Lyons and Paris , France; Dublin, I re land; Tzl-Aviv, I s r a e l ; surroundings of Verona, I t a l y ; Fukuoka, J a ~ m : Ulan Bator, Manmlia; v i l l a g e s near I badan, Nigeria; GGteborg, Sureden; a r u r a l a rea near Ankara, Turkey; Boreham Wood, near London, UK; and thz Tushino d i s t r i c t of Yloscow, USSR. Some of t h e pr.ogrammes already s t a r t e d i n 1971, t3. g. i n Gijteborg, Fukuoka and Moscow. Others s t a r t ed- r ly i n 1972, e.g. i n Uons, Northern Caselia and Ulan Bator; ye t a t h e r s a r e i n prepcration.
The populcrtion groups involxr~d v n r y w i d e l y . Some of them are occupational groups (e. g. f ac to ry workers and employees), o the rs cover a defined general population o r one of i ts s t r a t a . Some of them a r e urban, :fithers are rurc?l population groups i n developed o r i n developing countr ies , Approximately 20 000 persons a r e comprised i n occupationrl gpoups, while t h e general populations include 30-100 000 inhab i tan t s of a defined area. On t h e whole, communities with a l toge ther some 750 000 members w i l l be covered by Li la pilcr t p ~ w g - ~ L I U I W S .
The first s t e p is a basel ine survey. This is t o e s t a b l i s h t h e present s i t u a t i o n concerning hypertension: i ts prevalence, t h e proportion of previously lanow versus unknown cases, t h e number of those who had received regu la r medical ca re a s compared t o those who d id not have appropr ia te care, and t h e reasons f o r it. I n smal ler groups (e.g. t h e sccupational groups) a l l members a r e being screened; i n l a r g e r population groups, a representa t ive sample of t h e cvmmunity is being screened a t t h e basel ine survey, t c a r r i v e a t a d e f i n i t i o n of t h e basel ine s i t s a t i o n . On thc w h o l c , appmxilnately 130 000 persons are envisqted t n he screened.
A basel ine suyvey w i l l be c a r r i e d out a l s o i n some refarence communities bf s i m i l a r c h a r a c t e r i s t i c s , w i t h m t being followed by any p a r t i c u l c r control programme. Refarcnce communities w i l l be l e f t t a cbpe wi th hypertension with t h e usual types of h e a l t h care. Af te r a period of f i v e years, a t t h e

~ ~ l / ~ a r d . Vasc . / 5 ~ ~ I / P R V . MJ. CARD. VSC. D I S / ~ ~ Annex VII page v i i i
WHO EMRO
end of t h e p i l o t stage, a terminal survey t o be c a r r i e d out i n both pragromme and reference communities shculd show t h e di f ferences , i f m y , according t n endpoints a s follo>:s:
'6,rbidity and mcr ta l i ty : Incidence and mdrta l i ty af complicaticns "f hypertension: s t roke, hypertensive h e a r t d isease with f a i l u r e , renal f ci l u r e due t d hypertensicn; incidence and morta l i ty ~f coronary hear t disease; prevalence of known hypertensive subjects with and without l e f t verLt r i c u l a r hypertrdph:f and argan ciaage: prevalence of ~lndingnosed hypertension; t o t a l morta l i ty .
Data r e l a t e d t o programme . )pe ra t idn and hea l th ca re de l ive ry : est imate of input t o h e a l t h care and its p a r t r e l a t e d t o hypertension, including complications, input t~ t h e hypertension prcgrnmma i t s e l f .
The sources o f morbidity and murtnl i t j . data w i l l tc: rcgular
mvrta l i ty s t a t i s t i c s ; h o s p i t a l s t a t i s t i c s ; s t roke and myocardial inf a r c t i o n r e g i s t r i e s ( i f ex i s t ing) ; terminal rescreening c f ancther sample ~f t h e p d p c l a t i ~ n .
I n view of t h e heterogeneity of t h e p c p u l a t i ~ n s and c o n d i t i - n s cf work, it nay not be poss ible t c ~ b t a i n a proper follow-up of t h e reference calai~lunity ill a l l yluc~s. 111 such Instances, the quest lon of fec lSibi l l ty sill be answered only, m d t h e q u z s t i ~ n of e f f i c a c i t y w i l l be l e f t dpen. But hopefully, 3. n.L7!~ber ;f co-aperating cen t res w i l l be able a l s a ts answer t h e question whether community c~n t rc .1 programmes, a s u t l i n e d i n t h i s p m j e c t , a m f e a s i b l e and use fu l a s well.
PRINCIPLES OF CONTROL PROGWMb'Z
Hypertension seems tc be so f requant m d so important a d i s c r d e r that, t h e general apprcach t o its contr-1 includes, a s i n any large-scale epidemic, appropriate ~-mnngemen+, of whola cor~munities, i n a d d i t i s n t r ? g iv ing adequata ~ e d i c s l care tc individuals . I n ~2rder t c do t h i s , t h e " f i r s t l i n e of a t tack" agains t d isease - t h e general public - and t h e second l i n e , the general pract ' i t ioners, should be nobi;ized, i n add i t ion t o c rea t ing gosd s3ec i a l i z e d sarvices . Theref ore, emphasis is on t h e management s f whble c o a m n i t i e s a s sacio-biological en-bities, though af course individual p a t i e n t s w i l l be t r e a t e d adequately, accvrding t o up-to-date standards of xedlcnl sclences. Concerted, slmult2neous ac t lon IS thus needed along t h r e e l i n e s : general h e a l t h e d u c a t i o n , ~ s i c i a n s l education and b e t t e r car? f o r hypertensives, including timely diagnosis and appropr ia te treatment.
An important f e a t u r e of t h e c o n t ~ 2 1 programme is a c t i v e f9llow-up 3f i d e n t i f i e d hypertensives. I f a hypertensive person does not appear for

WHO EMRO E ~ / ~ a r d . Vasc . /5 EM/PRV. M J . CARD. VSC. DIs/l7 Annex VII page i x
a periodic ex re-exmination, a hea l th v i s i t o r w i l l enquire f o r t he reasons of h i s absence. A more de ta i l ed annual re-examination ( reg i s te red on spec ia l forms) w i l l keep t he programme centre informed on t he course of each hypertensive subject t h a t has been i den t i f i ed i n t he s tudied population group.
The control programme is based primarily on ava i lab le resources. Basically, it is conceived a s a movement of i n t ans i f i c a t i on and extension of already ex i s t i ng current a c t i v i t i e s . The general p rac t i t ioners , whether prwlvaLe or' a~i~yluyed, s l w u l d beuuma associated wi th t h e programme t e rn , whenever possible. A hypertension c l i n i c , operated by t h e Programme Centre, is giving advice t a t h e co-operating physicians, i. e. doing spec ia l laboratory invest igat idns , i f necessary. Data handling and analysis, physicians ' infarmation programme and research a r e some of Cie o ther a c t i v i t i a s of t h e Programme Centre, co-operating wlth o ther centres and K O (Fig.1).
SOME OPEN QUESTIONS
An important quest isn w i l l f i n d no answer i n t h e present p ro jec t : it is r e l a t ed t o mild o r border l ine hypertension. Where is the l eve l below which it would be un ju s t i f i ed t o leave a perscln without a hypatensive intervent ion? Up t o now, t he only secure guidel ines a r e coming from the well-known US Veterans' Administration study. The present WHO p r , j e c t is not supposed t o give an answer t o t h i s questiun; it w i l l be reviewdd i n another WHO meeting i n 1972. For t he time being it is pointed out t h a t the decision, whether and what type of drug treatment shculd be i n s t i t u t e d is t he respons ib i l i ty of t he t r e a t i n g physician, who should take in to account not only t he blood pressure values, but t he pa t i en t a s a whole. Hnwever, error is esteemed t o be l e s s on t he ac t i ve than on t he conservative side, and ,widelines f o r therapy a re given ti the co- operating physicians .
There a re several methodological impediments t o the study. For instance, it w i l l be d i f f i c u l t t o avoid t'contaminationtt of a reference community by the programme i n an adjacent community. Contamination tends t o lower t he v i s i b l e e f f e c t s of a programme, and though i ts t r u e e f f e c t s may be sa t i s fac to ry , the d i f fe rences t o be observed may be l e s s than expected.
The communities t o be s tudied cover a very wide socio-cul tural range indeed. I n addi t ion t o t he common basic pricedures, accepted at the WHO meeting i n Wteborg, each centre is f r e e t o adopt approaches best su i t ed t o the l oca l conditfons.

EM/~ard. ~ a s c . /5 EM/PRV. M. CARD. VSC. DIS/l7 Annzx V I I Page x
WHO EMRO
WHAT THE PROJECT IS EXPECTED TO G N E
Several p ~ i n t s of inportance should be made c l e a r by t h i s project . The survey done a t t he i n i t i a l s t age (baseline survey) should assess t he burden of hyper tens im on varicus pdpulations, and a l s o the t r u e d t u a t i o n concerning its ac tua l management, including inadequacies nnd t h e i r causes. The control programmes themselves should lead t o experience i n operating large-scale p ro jec t s f o r t he control of a common, and of ten symptomless condition. They should a l so show t h e best ways f o r operation i n various s?>c l o -cu l tu ra l settings . It should bccomc clear, whether therapeutic measures successful ly applied t o hospi ta l ized pa t i en t s can equally success- f u l l y be applied i n t he general p rac t ice a t large. Whether an organized programme has advantages over medical care a s administered i n t he respect ive areas i n the usual way is a basic question t o be answered by t he project . More ins igh t in to the na tu r a l h i s to ry of hypertension should a l so be gained.
A duratiun of five yaurs i s foreseen f o r t he project . It IS understood t h a t i f a p i l o t programme proves t o be successful , it should be continued as a model programme i n the respect ive area, and should eventually be expanded t o cover even l a r g e r populaticn groups. It should a l so be integrated with o ther con t ro l programmes f o r cardiovascular diseases i n t he area, e.g. s t roke and myocardial i n f a r c t i on programmes, the eventual object ive being a comprehensive programme f o r t he con t ro l of cardiovascular diseases, and a l so o the r chronic diseases i n e n t i r e populations.
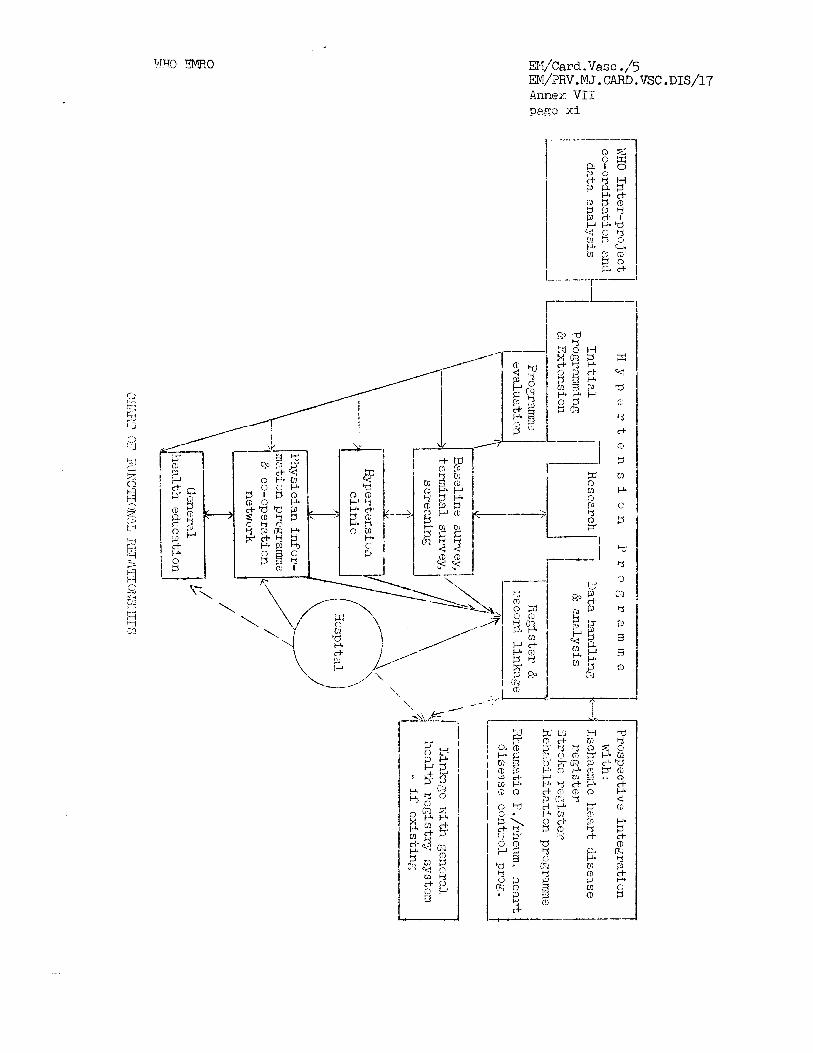
E ) ~ , ' ~ a r d . Vas c . ,I5 EM/'?RV. M J . CARD. VSC . Annex V I I p3gz xi
WHO EMRO EJv/Cafi-.Vasc./5 . EM/PRv.!JLT. C~~RD.VSC . D I S / ~ ~ Anne:: VIII page i
ANNM VIII
PROBLEMS OF ISCHliEMIC HEfiFlT DISUiSE EPIDEMIOLOGY
D r G. Tibblin* WHO Consultant
THE SIZE OF THE IHD PROEEGI
Thcre a m scvcra l rczsons Tor t h e inc reas ing n t ton t lon paid t o IHD. It i s a worlclwide diseasc . It hos now reachcJ onornous proportion causing g r e a t l o s s o f human l i P c 2nd reductions i n ccon~rnic productivity. Of t h e carcliovascular d i scases IHD is t h e most iinportant cause o f male Ceaths i n inclustrializcc! nnJ urbznizcd countr ies . Accorcling t o published WHO s t a t i s t i c s on mor ta l i ty i n t w ~ n t y - th rce coun t r i es i n 1964, t h i s form of the diseasc accounted on t h e average f o r 53 per cent of a l l deaths from cari l iovascular d iseases .
Data from twenty-nine coun t r i es show t h a t i n 1967 IID has been assigned a s a cause of dcath i n 25 per cen t of a l l m?.lcs 2nd 1 4 per cen t of a l l females aged 25-64 years, that i s a t thi hcight of t h e i r l i f e a c t i v i t i e s .
A myocardial i n f a r c t i o n has been consider td t o be caused by occlusion of one o r mort coronary a r t e r i e s , mainly by n thrombus. However, i n many ins tances , no thrombus i s found c l ~ s p i t c liiicroscopic cvidence of damage t o t h e myocardium. Kasan e t a 1 founl t h a t 25 per couL ur y a t i c n t s wit11 large frcsh rnyocarc!ictl in fn l -o t ion w o r e freo f r o m thrombctic o r o the r occlusion i n t h e major extra-rflyocnrc'.ial coronary a r t e r i e s . The poss ible explanation may be an i n i t i a t i n g thrombosis rcsolving before death o r l o c a l i n i t i a t i o n of a myocart'ial disturbance wi th ischaernic and necrosis sprea2ing c e n t r i f i g a l l y . Thcro a r c reasons for concentrating not only on t h e thrombus and the coronary a r t h e r i o s c l e r o s i s but a l s o on o t h e r mechanisms such a s rnctabolic disturbances i n myocardium operat ing throu& arrhythmia a n t spreading c e n t r i h ~ a l l y , The re la t ionsh ip between coronary a- thcroscleros is IHD has been s tud ied i n 211 autopsy-series by Sternby. He found t h a t persona who had died from IHD had i n all ago am?. sex Crnmll?s a higher de,-ree of coronary athei?osclerosis than those dying From any o t h e r cause. Thc difference i n gra?.c of coronary a t h e r o s c l e r o s i s i s more pronounccd i n t h e younger agc groups.
*Assistant Professor, Medical C l in ic I Sahlgren 's Hospitnl (Chief, Lars W w k o M.D.), Universi ty of Gateborg, Gijteburb, Sweden

w a r d .Vasc ./5 EM/PRv.MJ. CARD.VSC. D I S / ~ ~ finnex VIII page ii
WHO m o
RISK FACTORS
Mrmny s tudies conducted over the past twenty-five years have demonstrated associations botwcen cer ta in biochemical, l~hysiological and environmental fac tors end. the development of IHD. I n tab le I tht: most important r i sk fac tors a r c prescntcd.
Thc etiology of atk-srosclerosis and coronary thrombus i s unknown. Thc s t a t i s t i c a l association of IHD with the r i sk fac tors has l ed t o speculctions concerning these fac tors of e t io logica l importance i n the i 2 c v e l u p n e n l or thebe cur~c?i Liurls. Orie wcry ul: yr 'ovlr lg a b l u l o g l o a l re lat ionship i s t o t r e a t these conditions i n one group of subjects and leave another s imi la r group untreated. Such well-controlled s tudies a re underway i n England, Sweden and i n Finland. I f posi t ive r e su l t s can be achieved some of the e t io logica l mechanisms behind the disease could be elucidated.
Lincel ICeys has sa id t h a t important r i s k fac tors such as sys to l ic blood pressure, serum cholesterol and smoking can only explain a part of the etiology and concluded t h a t other variables besides those considered here must be important i n the etiology. Psycho-social factors , behaviour pat tern and premature aging were also suggested a s r i sk factors .
This i s a well-known sex ciifference i n IHD which secms t o be even more accentuated during the past years. The reason f o r these differences i n IHD-incidence i s not c lear . Blood l i p ids , blood prcssure do not d i f f e r between the sexes. On the othcr hand, smoking is more common amon:; men than women. Another manifestation of IHD - angina pector is is of the same magnitude i n the two se:ics. The sex-difference i n IHD need t o br? more e l ~ ~ c i d a t e d .
Great differences i n IHD-mortality r a t e s between countries of the same cul tura l and economic l eve l a r e wel l recognized. I n males i n the age group 45-54 the death r a t e s from IHD i n Sweden i s 126.0, Norway 191.5, Scotland 329,2 and Finland 427.3 per 100 000 population respeatively. The differences between these four countries a r e i n t r i ~ w i n g and a r e challenging.
CLINICW; COURSE
In most cases myocardial in farc t ion occurs suddcnly and dramatically by a violent a t tack of pain which spreads t o the whole of the thorax, often radiates along the arms and l a s t s f o r hours. Thesc pat ients a r e alarmed by the symptoms end look f o r medical assistance.
I n the c l i n i c a l course of UID there a r e two types which d i f f e r from t h i s c l i n i c a l picture and about which w e know considerably less : the s i l e n t myocardial in farc t ion and sudden IHD death.

E I ~ / c ~ ~ L .-V7us~ ./j B\I/EF.V. 1.15 . CL .iD. YSC . D I S / ~ ~ AIIKILX \TI1 p . 2 ~ iii
SILE3T FTfOCLiRD1A.L INFARCTION
,';ccort<inz t o data f ran -Lhc Praninghaai Study --.~oLI-i; !I.@ pir. c-nt of ell sub jec t s wi th "hear t a t t acks" were not hospitnlizo::.. Over211 m r v i v a l was no bcttc-;r than i n tllosc- wt th rccoc;nizd-'. s:ii:;;jJ~o~natic -inf'~.rc t i o n (Kannel et a 1 19'70) .
I n c: small study from our u n i t , only r i v e ou-c o r nlnc p a t i c n t s witJ;I scz's t o olil myocapdizl i n f a r c t i o n wcrz c l i t ~ i c c l l y r c ;co~n izc .?. Tnzc.si. 1x-1 t i e n t s n.r ,? ~ n t . .?.vr? r.;: n.P hcin- n hi211 risk :.;'r1oui, Por firth;;ra ;:o.;lplic:,tions o r su:idcn death. Oni: inp0rte.n.t prcblci:? i s t o let2c.L t h e s s p a t i k n t s i n livin:; stet;.
It has been r c p o r t ~ . : ~ t h a t t h e i n i w n l c l i n i c 2 1 iL~.~niL 'cs ta t ion or' IIiD has bt;t;n sudden dc;ct& in z~bout 20-25 per c e n t oi' ccs~:; and that
such zn aSmpt ending of l i f k occurs r,Iorc d f tdn i n th: malL with coronziT d i s ~ a s ~ than i n the rerflnlc. Knowlcfige i s l i m i t d concurning tllosc sui!.clcn IXD-daaths s i n c ~ t h c f i n a l episodi: i t s c l i ' i s o f t e n too brir;Z t o perrllit any cor~mnic&t ion wi th t h c p a t i a a t an2 c.n autopsy i s o f t ~ n lackin,<. I n an e n e l y s i s of a sm,zll s ~ r i e s ol casus, i t was found t h a t most IHD-cizzth was sudden a l s o i n thc l iospi tn l (Tibbl in 1972) . 'l'hc majoriVjr of sucP2;n 1HU had old iilyocnr~.:izl i n f a r c t i o n sca r s . and s i z n s of f r e s h los ion.
mi' c'wpaign t o c i e c r s a s ~ the mngnitudi of t'nz su;;.:?.in IHD-52ath.- pi-oblarn has rnnnjr f sco t s . hllany of the p a t i s n t s ha.i ;lisiJLcc: bh\: doctor '9cforc t h ~ a t t a c k without a d ~ q u a t ; cneasurcs nnvint :~LL!I taken. Bet-tcr i iuca t ion of t h e m e d i c ~ l profession is needccl. Too m2il:; < o c t o ~ s nsk only about c h e s t pain withoat poimittin;; t h ~ p-ticn'c Lo !;~.L.L h i s s t o w . E~s~$o&s of f a in tness , wczkness and p r o ~ l ~ s , : svcc-Ls a r c not al:vays view& sri th appropriat i : concern. B e t t e r cL~!caf,ioil of t h ~ , . ,
ijublic or? s i g n i f i c a n t ppernoni t o r y symptoms may be an irn:,~:~-Lant npprosch . mgoca~$ia l i n f a r c t i o n p a t i c n t s s t r ~ t ~ tha.6 t h ~ y h v c nad no ches t
.-.-;,I .. . A but had 2. pressure, ti;<htnoss, burning o r o thdr Ziscolnfort i n , . ZnL chos'i.
S c i c n t i f i c workcrs have two cornplcmcnta~r tasks : t o aclvisi. and c.pply i~mec l i a tc lifL-savin:; ~ ~ > ~ a t m c ; n t f o r p c t i ~ n t s wi th :.cutL myocardi.nl i n i a r c t i o n , and. t o prevent coronary a thc rosc lc ros i s an2 thi-ornbosis irom dbv-lcping a t a l l . I n recent yca r s spoctacular r o s u l t s 112vc bcen ,-.chiLv~c: i n the a c t i v e int ,nsivc care, rehabi1iti:tion an1 r;urvLil lanct oC p a t i ~ n t s wi th acu te myoc-rdfel i n f a r c t i o n . Taz piqLvbntion o f s~ rcndary thrnmbo-cmbolic c o ~ ~ ~ p l i c a t i o n s bJ- a n t i c o a r ~ ~ l a n t s 2nd attempts

EM/~ard .Vase ./5 m l / ~ ~ V . ?U . CARD. VSC . D I S117 i+nnex VIII pagc- i v
WHO ENRO
c ? t e a r l y mobilization of p a t i e n t s have been followed bjr encouraging r e s u l t s wi th t h e resusc i t a t ion of sub jcc t s wi th suddcn cardiac a r r e s t .
With t h e control of such vents and wi th more in tcns ive t r e a t - mcnt of cardiac f a i l u r d an2 cardiogcnic shock Hofvendahl lias shown an important reduction i n morta l i ty . I n s p i t e of 7.11 thcsc works t h e mor ta l i ty of IHD p a t i e n t s i s extremely hi*. lnilthin on2 ycar h a l f of them have died and only a t h i r d has t h e p o s s i b i l i t y t o go back t o work.
Thc! continuous survci l lanco of acute UID-patients has given encouraging r c s u l t s . It i s therefore poss ible t h a t s u r v c i l l a n c ~ of p a t i e n t s a f t e r t h e h o s p i t a l i z a t i o n period, including r c ~ a l a r check- ups and preventive measures d i r e c t c 2 towards complications and r i s k fac to rs , i s on2 way of improving the r e s u l t s . Preliminary r e s u l t s from Gijteborg, Sweden shows an important reduction i n mor ta l i ty and morbicli t y us lng specla1 myocarciial l n f a r c t l o n CU.~per~silr.i~a. (Wilhelmason
and Vcdin).
I n 1967, E f f l e r and Favaloro introduced the saphenous-vein by- pass v:Nch gained wid~sprcacl USL i n coronary revasculc?.lisation. The e::cellent primary r e s u l t s wi th t h i s relative-ly sirnplc technique - 2 P ~ C C L 0LO scphanous vein i s obliquely c u t i n t h t proximal cnd and i s nnastomoscd e n d - t o - s i d ~ t o a coronary a r t e r y , d i s t a l t o t h c a r t e r i o s c l e r o t i c changes, l e d t o widespread use i n m?ny cardio- s u r g i c a l c l i n i c s i n USA and Europc. I n t h e Unitkd S t c t c s alone i n 1971 26 000 operat ions wcrc performed and it i s ca lcu la ted t h a t i n 1972,35 000 operations w i l l bc dnnc at a c o s t oLn 750 mil l ion d o l l a r s .
It must bd important t h a t c a r d i o l o g i s t s and car,!iac surgeons co- operate i n w e l l - c o n t r o l l ~ d p r o s p ~ c t i v e s t u d i e s which allow them t o draw conclusions concerning the ind ica t ion f o r surgery i n IHD.
U p t o now the h e a r t surgeons havu few long-term follow-up s t u d i e s going on. They repor t h o s p i t a l tnortal.ity between 2-10 per cent. Without S~rawing any conclusion I would l i k e t o mention t h a t the r ~ o r t n l i t y among male p a t i ~ n t s a f t c r myocardial i n f a r c t i o n is i n the Coronaw rug Project 5.8 Dcr cent f o r a ~ o ~ I . o w - ~ A ~ I a f t , r eighteen months i n the age group 45-54 and 8.4 par cent i n t h t agc Group 55-64.
LONG-TEXP1 FOLLO1\1-UP STUDIES
Ths number of s t u d i e s of acute myocardial i n f a r c t i o n i n t h e acute phase i s grea t . On the o ther hand very little Is known about the long-tcrm course of thL disoaso.

WHO m o EM/~ard.Vasc ./5 EM/PRV. PlZJ . CARD. vsc . D I S / ~ ~ Annex VIII P a w v
One of the few s t u d i e s deal ing wi th this problem i s t h e Coronary D r u g Project . From t h i s study we knou t h a t i n f a r c t survivors can be i d c n t i f i e d a s having v a s t l y d i f f e r e n t r i s k of mor ta l i ty i n a given period. The usua l prirnary r i s k f a c t o r s such as cho les tc ro l , blood pressure and smoking a r e nmch l ~ s s important a f t e r myocardial i n f a r c t i o n than before. Using simple c l i n i c a l c l a s s i f i c a t i o n s of M I survivors it was poss ible t o discr iminate between p a t i e n t s w i t h a g-fold d i f fe rence i n r i s k of mor ta l i ty i . e . between p a t i e n t s wi th l e s s than 2 per cent mor ta l i ty r i s k versus over 16 p e r cen t r i s k ( i n eighteen months). The public h e a l t h impl icat ion is c lea r : 'chc high r i s k p a t i e n t s must be c a r e f i l l y followed and t r e a t e d and t h e low r i s k p a t i e n t s assured about t h e i r good prognosis. We need a l s o t o know more about prognosis i n order t o t r e a t t h e MI p a t i e n t s more accurate ly .
PREVENTION
THT) has been knnwn f n r n l o n g t i m e t o hr. r e l n t ~ d t.n ,z nurnhar of personel c h a r a c t e r i s t i c s and f a c t o r s i n t h e environment.
Several m u l t i f a c t o r i a l o r u n i f a c t o r i a l primary prevention t r i a l s a r e underway and t h e i r inventory i s being co l l ec ted by WHO i n co- operat ion wi th the Council on f i r t e r i o s c l e r o s i s and IHD of t h e I n t e r - na t iona l Socie ty of Cardiology.
I n most of them the main attempt has been t o inf luence t h e dis turbed l i p i d metabolism by an appropr ia te d i e t o r by drugs, a n t i - smoking devices and t o reducc e levated blood pressurae by drugs.
So f a r no f i n a l answer h a s been obtained.
RISK FACTORS FOR THE DEVELOPMENT OF IS-C HEUW DISEASE
1. Diet involving increased in take o f cho les te ro l end f n t .
2 , Elevat ion o f serum l i p i d l e v e l s (cho les te ro l ) .
3. Hypertension,
4. c i g a r e t t e SmOklng.
5. Diabetes m e l l i t u s and asymptomatic hyperglycaemia.
6. Obesity,
7. S e d c n t a r y l i v i n g .

EM/~arcl.Vnsc ./5 .
EM/PRv,KT. CARD.VSC.DIS/~I-/ Annex VIII page vi
WHO EMRO
8. Psycho-social factors .
9. Family h is tory ,
Fcjfnr has calculated t h a t i f a l l accidcnts o r respiratory diseases were "eliminated" hypothetically, expectation of l i f e a t b i r t h would be prolonged by l e s s than two years, control of a11 neoplasms would prolong expectation of l i f e by l e s s than three years. I n contrast t o t h i s , expected prolongation would amount from four t o f i f t e e n years i f a l l cardiovascular diseases were eliminated. 'Ibis shows the importance of IHD, which i s the most prevalent cardiovascular disease.
But the s i tua t ion i s not bright. There is only a crude picture of the etiolow of the disease. Present treatment of t h o d i s e a s ~ i s inef fec t ive with a very high mortality and up t o now it has not been possible t o prevent it.
REFERENCES
EM/~nrd..Vasc ./5 al/PRv. . CLFiD. VSC . D I S / ~ ~ Anne:: VIII pagj v i i
1. Blackburn, H. e t n l : Th,, n c t u r a l h i s t o r y c f myocardial i n f a r c t i o n i n thc Coronary D r u ~ Pro j uc t . Pr,ventivc Carcliology Llmqvist Sc itJiksel1, Stocl-&ol:n, 1972
2. Holvendd~l , S. : Influonce of troatrncnt i n a ccrcnary cc rc u n i t on prcgn~sis i n ecutc rnyocnri~ial i n f a r c t i o n . Pkcte Mid. Scand. Supyl. 519, 1971.
- , . lict:san, i k . , L ivs ic , '+.I?. , Stcrnby, N. And Vihcrt , Pi.11. : C o r ~ n a r y a r t e r y tnrornbosis and t h c ccu tc a t t a c k of coronary h c c r t d i seasc . Lancet 1199-1202, December, 1968.
Li. , 'r;,?..nn,l, W.D., McTJmarc, P.B., Feinlc ib , M. cnd Dawler, T.R.: The unrecognized myoczirdial i n f a r c t i o n . G o r i a t r i o s 25, 75-87, 1970-
5. Keys, h. : P red ic t ing coronary h e a r t d i seasc i n Prevsntivc Cardiology. klmqvist & Wiksell, Stockholla, 1972.
6. Sternby, N.H.: Atheroscleros is i n a def ined populction. Actn Pathologioa e L r 4 . i ~ ~ - u b i u l u g i c a Bcandinavicc . Suppl, 194, 1968,

WHO EM30 EM/card .Vast ./5 EN/PRV.W. CAFD.VSC.DIS/~~ Annex M. page i
ANNEX I X
LWmS1V.E CORONATPE CARE UNITS
D r G. Sloman* WHO Tcrnporaq Aclvi s o r
A l l p c t i ~ n t s i f i tn acutc i n f a r c t i o n may s ~ l f f c r a. l i f e threatLning arrhythmia. In'consivc coronery care should bc a v a i l a b l ~ f o r a l l p a t i c n t s vrh~ prcscnt t r i th a ctefinitc c r s u s p ~ c t c d i n f a r c t i o n .
- Gcncral rnLasurcs f o r thc r c l i ~ f of t h c pain, hypoxin and e a r l y rhythm d i s t u ~ b n n c cs .
- Mathnd af t m n s p c r t a t i o n , t o h o s p i t a l and treatment of crnergencics i n the emergency ambulance.
- Spcclal n o s p l t a l organlzat lcn i n tht ~murgtncy a rea f o r rapi3- t r a n s i t of ccut, i n f a r c t pa t i en t s .
The coronary cc rc a rea should have tho following c h a r a c t e r i s t i c s ;
1. Space t o acccmmcdate a l l in fa rc t s .
2. A p p r o p r i a t ~ c2lm q u i e t ntmospherc . 3. S t a f f t r a i n i n g should bc a t a high l e v s l f o r i ~ m e d i n t c emergency t rcn tncn t .
4. Continucus clectrocarx3ographi.c monitcring must be ava i lab lc .
5. Enlsrgency 3rug therapy ~ n d dmcrgcncy electrical thcrcpy should be st hrnci f o r ~ l c c t i v ~ and emergency usc.
- n s t e p clown ccrcnzly u n i t should be ava i lnb le f o r 13atient t r a n s f e r .
- Spzcif ic troa-tmc-nt of carcciac arrhythmias i n gatic-nts wi th ncutc i n f a r c t i o n , r t r i a l arrhythmias 7.ncl v e n t r i c u l a r arrhythmias o ther s i t e s of dcto;>ic a c t i v i t y ,
- Conduction d i s t u r b n n c ~ s . iirrhythmic trcatmcnt mag be clivicl~cl in tc> t h r c e categor ies :
1. E x p c c t ~ ~ n t drug thcrapy.
*C-rdiac Department, Royal Mclbournc Hospital , Vic to r ia , A u s t m l i a

E?d,/~ard .Vase ./5 EN/PRV. 14J . Ci:iI$D, VSC . DIS/'17 Annex IX
. " i:&Cc ii
S p ~ c l a L i>rc,blcms of heart block occurrins in patients with acute myocai~:liz.l In: ?:=c.tion,

.KM/Caild.Vasc ./5 F&I/PRV. r4J. CARD, VS C . DIS/17 Annex X page i
ANNEX X TRPAWLENT LAD R.E-lrZFJILITL4TION OF ISCHAEMIC
HEAFT DISEASli: - ?FGSENT TRENDS
Professor fl. Denolin* KiiQ T e r n b ~ ~ a l r y Adviser
It i s o b v i o u s l ~ not pcsslbl-e 9 2 a s h o r t docurnent t o review a l l t h e aspec t s of t h e treatmznt 02 t h e Ischaemic myocardic disease . Even i f we waive t h e problems of prlr2sr;l and secondary prevention and omit t h e Important chapter of -lh~ E : l r i , i l lsf ice ~ 1 x 3 trcetment of t'ne i n f a r c t i o n i n i t s acute s tage, the subjec.c remnlns r, v a s t one and only a few p a r t i - c u l a r points can be covered.: some sf these dea l wi th l a t e n t chronic coronary insuf f i c iency o r syvptor,:sf,ic (angor p e c t o r i s ) , t h e o thers a r e r e l a t e d t o t h e treatment o f t h e Fnfarc t e f t e r i t s acu te s tage.
AS t h e notion of an acci.lq.*te r ' - i r z n r + i ~ i s c l o s e l y l i*ed with therapy, some obser t~a t i cns u:f'l. 1.7 17.t f g r t h i n respect of t h e v a l i d i t y . of t h e means o f diagnos5-s cr! 111 p ? . - , t i ~ ~ ~ i a r exercise t e s t i n g .
1. Latent coronary ~ .nsuf -?.i.cIe)~:~r
1.1 Diagnosis of l a t e n t coronary insuf f i c i e n z
Before en te r ing i n t o i t s symptomatic s t age - angor o r i n f a r c t - coronary insufficiency nay pass through a l a t e n t period of va r iab le duration, during tflhich t h e electrocardiography of exercise t e s t i n g proved t o be an import. - t di?groet'.? technique.
It i s not intended here t o develop i n d e t a i l t h e methodology of the exercise Lest, v;Z.i_ch h?s been described i n a rim0 study (see: F'undamentals of exercise t ec t ing , WHO, Geneva, 1971).
Let u s rccz2.1 tht thr? method ( l e v e l of workload, duration, durat ion of recording? chef ce of e lect rocardiographic l eads - electrocardiograph-LC c r i t e - r i a ) should give a s u f f i c i e n t s e n s i b i l i t y and s p e c i f i c i t y .
The comparability ~ : 4 .h c ~ ~ o n a r o g r a p h y has enabled u s t o assess to-day more va l id ly t5e ~ d h 2 of exercise t e s t s . Master ' s t e s t and c h i c f l y the progressive r " ~ k -- url bicycle ergometers o r treadmills - a t t a i n a value clo?? t o t h z ua;:imum - with r e g i s t r a t i o n o f 3-4 leads including V4, 5, D2 and A-T;T wi th hor izon ta l o r descending ST depression of more than 1 mm a h i t t a d a; a s ign of coronary insuf f i c iency , g ive
-- ---- -- - "Chief, Cardiology Depar-tr0enJ;: ' ' 3 ; C,-.l L2Lnt-Pierre, Brussels , Belgium
EM/carcl .Vasc ./5 EM/PRV. l ' ~ . CARD. VSC . ~ 1 S / 1 7 Annex X page ii
WHO EMRO
val id r e s u l l s . I n the case of progresslve exerclse ConClucted t o a l e v e l c lose t o t h e maximum, i t i s noticed i n a middle-aged man, with normal r e s t i n g EGG, 8 t o 13 per cent of pos i t ive responses. A recent study by Cumming e t a 1 (1972) shows i n t e r e s t i n g information viz t h a t t h e frequency of ECG pos i t ive responses inc reases s t rong ly wi th age (4 t o 37 per cent from f o r t y t o s i x t y - f i v e years ) and pos i t ive responses a r e accompanied by a higher frequency of c e r t a i n r i s k fac to rs , a s we l l a s a gloomier prognosis. This prognostic value of the exercise t e s t ECG i n asymptomatic sub jec t s has been proved repeatedly.
1.2 Treatment of l a t e n t coronary insuf f i c iency
I n l a t e n t coronary insuf f i c iency - v i z asymptomatic - recorded only by electrocardiography i n exercise t e s t i n g - preventive measures which a r e d e a l t wi th f a r t h e r , a r e appl icable , v iz correct ion of t h e r i s k fac to rs , whatever they a re . A s f o r drugs, a p a r t from those modifying t h e l i p i d equil ibrium o r those cor rec t ing associa ted a f fec t ions , it appears t h a t so f a r no systematic treatment has proved e f f i c i e n t a t t h i s s t age of t h e disease .
Table I
C r i t e r i a f o r stopping exercise t e s t i n ~
1. Increas ing pain i n t h e chest , severe dyspnoea 2. Pa l lo r , profuse sweating, confusion 3. Sys to l i c blood pressure exceeding 250 rnmHg; pressure not
increas ing o r decreasing 4. Severe arrhythmia 5. Signs o f s i g n i f i c a n t coronary i n m ~ f f i c i e n c y 6 . Maximal cardiac h e a r t r a t e i n respect of age
2. Angina p e c t o r i s
2.1 Diagnosis
I f t h e questionnaire i s one of the e s s e n t i e l elements o f the diagnosis of angor ( l o c a l i s a t i o n and condi t ions of development of f e e l i n g of pain) i t should however, be borne i n mind t h a t the re a r e a c e r t a i n number of a typic angors, angors wi th normal r e s t i n g ECG o r inverse ly thoracic pain of d i f f i c u l t i n t e r p r e t a t i o n .
I n a l l these cases, t h e exercise t e s t wi th continuous diagnost ic i n t e r p r e t a t i o n of ECG during exercise and t h e recovcry s tage repre- sen t s a considerable contr ibut ion t o t h e accurate d iagnosis and prognosis, provided t h e h e a r t r a t e is ra i sed t o a f a i r l y high l e v e l t o l e t the pain o r the ECG sign^ of coronary insuf f i c ienoy appcar (ST segment depression of hor izon ta l o r descending type of a t l e a s t 2 mms). Table I i n d i c a t e s t h e c r i t e r i a f o r stopping exerc i se t e s t s .

WHO m o EM/Card.Vasc 4.5 E~~/PRV.MJ. CARD .vsC. DIS/17 Annex X page iii
2.2 Treatment of angina pec to r i s
I n angina pec to r i s - which i s t h e usua l warning of coronary insuf f i c izncg - a l l preventive measures a r e applica- b l e and l i a b l e tu b ~ i n g about an improvement of t h e condlhion, even i n t h e case of a confirmed angor.
Besides, t h e l i f e h a b i t s a r e f'undamental, and must be c l e a r l y ex~ln ine6 . - to t h e pa t i en t .
A t the monont o f t h e a t t ack , n i t rog lycer ine i s the drug ------- of choice; t h i s drug i s wel l to le ra ted , does not cause secondary s ide-effects l nor drug dependence; it remains i n t h e f o r e f r o n t of therapy provlded t h e p a t i e n t i s taught how t o use it cor rec t ly . Its mode of a c t i o n i s s t i l l disputed: d i l a t i o n of coronary a r t c r i c ~ o r m o r c l i l r e ly dimicishing ven t r i cu la r labouring# e i t h e r by reducing a r t e r i d res i s t ance o r by reducing t h e venous tonus and blood r e t l ~ r n .
A s a &s ic t reatment a long list of products have been proposed (see t a b l e below). We s h a l l d e a l wi th some of these. The d i f f i c u l t y of evaluat ing t h e i r e f f i cacy has o f ten been pointed out.
Some of t h e drugs used i n the treatment of angina p e c t o r i s
N i t r i t e s Papave r i n e Xanthines Khell ine (f'uronochrcme) Mono-amine--oxydase i n h i b i t o r s Segontin o r Hostcglnan ( prenylmine ) Amplivix (heneiadronc) I sop t ine (Veraponil) Persantine (Dipyr5-dornol-e ) In tensaine (~arbochromene) Ildamen (s t imulant c:' adrenerget ic beta-receptors) CLinium (Lidoflazine ) Cordarone ( Amiodarone ) Mta-blocking agents : Propranolol ( Indera l )
Oxprenolol (Tras icor) Alprenolol (Aptin) Prac t o l o l (Eraldin) Pindulol (Visken) S o t a l o l ........... e t c .
EM/~ard .Vast ./5 EM/PRV ,MT . CARD. VSC . DIS/17 Annex X page i v
WHO mo
Lurle-ac Liru rLt Lra te derlvatlves a r c sometimes recommended although t h e i r effectiveness remains questioned.
Another gmup of drugs proved more important: the beta- blocking agents, Propranolol f o r instance, one of the oldest known. These drugs aim a t diminishing the labouring- of the heart and thereby the oxygen requirements of the myocardium, by t h e i r act ion ch ief ly on the hear t rhythm but sometimes they a f f ec t other haemodynamic parameters - con t r ac t i l i t y f o r instance. However, the r e su l t s a re unquestionably favorable, but t h e i r contra-indicatiuus (asttma, braclycarclis, auriculo-ventricular block, hear t f a i l u re ) should be borne i n mind. The long l ist of drugs proposed fo r the treatment of angor, and the ever- increasing list of beta-blocking agents themselves, i s an adequate proof t h a t none of these drugs has a s ign i f icant act ion i n a great number of cases,
The problem of anti-coagulants w i l l be discussed l a t e r . I n principle, they a re not indicated i n s tab le angor, but may
.be a t the "pre-infarction syndrome" stage, t ha t i s t o say i n the case of sudden changes i n the coronary condition ( f i r s t a t tack o r sudden aggravation of s t ab l e angor).
-,.' We s h a l l not deal with the pmb7er-1 of the carotid s t h u l a - t ion which s t i l l requires f'urther investigations.
2.2.2 bronarography and angina pec t o r i s surgery
This subject is i n f u l l developmcnt and i s the subject of passionate discussions. Coronary surgery of fers unquestionably new possibilities. New techniques are required t u deLermine beforehand an accurate evaluation, from the morphological point of view, of coronary circulat ion.
Although cer ta in centres often resor t t o coronarography f o r an accurate evaluation of pat ients suffer i rg from atypic thoracic pains, we endeavour t o reserve t h i s technique t o pre- operative preparations. The l i s t of indications from my point of view, and a t the present time may be established a s follows:
a ) General indicat.3 onsr
- Stable, severe, incapacitating angor, which had no response t o a medical treatment; - s ~ b i n t r a n t angor not receding t o res t ;
- Prinzmetal angor; - ao r t i c valvulopathy with angor; - severe ventr icular arrhythmia after infarction.
WHO mo EM/~ard .vast ./5 EM/PRV. PU . CARD. VSC . D I s / ~ ~ , Annex X page v
b) Individual Indications:
- a typ ic thoraclc pains wi th normal ECG; - cardiomyopathy of undefined o r ig in ; - cardiogenic shock whsn i n f a r c t i o n decl ines .
The problclm o i thc t ~ c h n i q u e ms'c not bc discussed here.
Thc qucstion of iiacmodynamic measurcs t o be associa ted wi th coronarograph;. remains t o be determined. I f a global examina- t i o n O f WOCaPdic c o r ~ L r a u t i l i t y by ventriculo~raphy is d e s i r ~ h l e , the systematic assessment of t h e blood output, t h e t e l e d y a s t o l i c pressure of t h e l e f t v e n t r i c l e o r t h e determination of t h e c o n t r a c t i l i t y index remain doubtful o r a r e d i f f i c u l t t o i n t e r p r e t ,
The s u r g i c a l policy of our Department m y be summarized a s follows:
- aorto-coronary "jump" g r a f t i n presence of obs t ruc t ive l ca ions of a t l e a s t 70 per cent of the vcssc l light, provided t h a t the re i s no d i s t a l obst ruct ion exceeding 50 per cent of t h e light, the u t i l i z a b l t diameter o f thc vessel i s 5 1 m a t l e a s t and the v e n t r i c u l a r funct ion i s s a t i s f a c t o r y ( s a t i s f a c t o - r y global c o n t r a c t i l i t y and excessive increase of t h e t e l e d i a s t o l i c pressure, except v e n t r i c u l a r aneurysm);
- mammary implantation: i f "jump" g r a f t i s not feas ib le , provided t h e l e f t ven t r i cu la r f'unction i s w e l l preserved.
S ign i f i can t s t a t i s t i c a l s tud ies , over a s u f f i c i e n t long period, are still not svailable. Pos t -ope~a t ion mor ta l i ty appears t o be low i n wel l - t ra ined hands (for instance: Favaloro e t a 1 had a mor ta l i ty of 2.1 pe r cen t on 188 cases operated - from January t o March 1970) ; post-operation mor ta l i ty appears a l s o t o be small i n c e r t s i n s e r i e s ( f o r ins tance: Morris e t a 1 2.6 per cent mor ta l i ty on 480 cases f o l l o w ~ d up over a period of 6 t o 30 months). Most l i k e l y i n highly-cxperienced centres , the post-operztion mor ta l i ty must be from 3 t o 5 per cent . But t h e more o r l e s s delayed obst ruct ion of grar ts (may be 30 per cent a f t e r one secondary i n f a r c t i o n s a r e not exceptional and a u t h o r i z ~ d opin inns suggest caution, and rccomend l i m i t i n g t h i s surgery t o severe symptomatic condit ions o r severe function- a l d isorders .
The e f f e c t s of the operat ion on thc subject ive symptomato- logy a r e general ly f a i r l y spectacular , whi l s t tl?c benef i t from t h e myocardic funct ion point of view remains disputed.

EM/Card.Vasc ./5 EM/PRV.W . CARD.VSC . DIS/17 Annex X page vi
WHO EMRO
Br ie f ly , i t i s s L i l l d i f f i c u l t to-clay to determine p rec i se ly what i s t h e t r u e place of surgery i n t h e treatment of coronary insuff ic iency.
3 . Myocardic i n f a r c t i o n a f t e r t h e acute s t age
3.1 Complicated i n f a r c t i o n
The i n f a r c t e d p a t i e n t a f t e r h i s discharge from the coronary u n i t may progress favourably i n a g r e a t number of cases , However, m2ny complications of variouo gravity may disturb the uuurse of the disease :
- p e r i c a r d i t i e ( ~ r e s s l e r syndrom) - v e n t r i c u l a r aneurysm - rupture of t h e i n t e r v s n t r i c u l a r septum - rupture o f t h e p a p i l l a r y muscle - ar te r ia l ur pulrnorlsrry cmbollsm
These complications a r e mentioned f o r t h c purpose of showing t h e p o s s i b i l i t i e s of surgery i n some of these complications, viz.: p a r i e t a l aneurysm, o r septum rupture.
3.2 Non complicated i n f a r c t i o n
3.2.1 Medical treatment
Medical treatment w i l l be s i m i l a r t o t h a t of ' r e s idua l manifestat lons, not mentioned i n t h e previous payagraph: pain- f u l syndrome of shoulder, r e s idua l angor, s l i g h t cardiac decompensation, e tc .
I f tho p a t i e n t is asymptomatic the secondary preventivc measures should be applied. I n t h e absence of angor, "ant i - angina" o r "comnadi la tors" do not appear to bc J u s t i f i e d . The only o ld problem which has not so f a r bccn solved, i s t h e problem of anticoagulants. After some t h i r t y years, it is s t i l l impossible t o formulate a r u l e a s t o t h e use of these drugs. It i s probably r e a s o n a x e t o r e s o r t t o them i n acute i n f a r c t i o n o r i n t h e "pre-infarction" syndrome. This treatment would not be u s e f i l i n s t a b l e angor, and could be s t o m e d after a period of 6 t o 12 months a f t e r t h e i n f a r c t i o n a t t ack .
j .2.2 Rehabi l i t a t ion
Is t h e indispensable complement of' the regu la r su rve i l l ance and medical treatment. It may be defined a s the "sum of a c t i v i - t i e s required t o ensure the cardiac handicapp~d tho best po~aiblc
WHO EMRO EM/Card .Vasc ./5 EN/PRV. M J . CARD, V$C . DIS/~'-( Annex X page v i i
physical, mental and soc ia l conditions so tha t they may, by t h e i r own ef for t s , resume a s normal a place a s possible i n the l i f e of the communitytt (WHO, 1969).
This implies t ha t rehabi l i ta t ion measures should be early,continuous, and t&e in to consideration a l l the pa t i en t ' s aspects: physiological, psychological and social .
From the onset of the disease, a progressive mobilization should be i n s t i t u t e d under m e d i r d sl~pc.mrision, and a t the same time the psychologist and the soc ia l a s s i s t an t w i l l andeavour t o solve the pa t i en t ' s problem, and rule the fc;milys s and the employers a t t i tude .
The gradual. mobilization should (exccpt i f complications a r i s e ) enable the pa t ien t t o leave the hospi ta l within three weeks a t most and con.tinuc at home, or in s. convalesctjtice-hw111[:, . . a programme of gradual reeducation.
The majority of pa t ien ts w i l l afterwards benefit of a period of a morc intensive reeducation. After two months and a half o r three, an exercise t e s t s h a l l be carr ied out under the conditions of supervision mentioned abovc and the t e s t w i l l enable us to dzfine "the maimurn oxygen uptake a s l imited by the symptoms (V 02 max sL) s t a r t i ng from which time reeducation w i l l be conducted ( a t the r a t e of three 25-minute s i t t i n g s by week of intermit tent t ra in ing of 60 and 90 per cent of the maximum).
Subsequently, n maintenance treatment may be in s t i t u t ed , i f possible, on a permanent basis.
The physiological benefi t of t h i s rehabi l i ta t ion (intensive t ra in ing i n par t icu lar ) i s obvious: maximal increase of oxygen uptake, reduction of vent i la t ion, of heart ra te , of myocardia3- labouring, of the blood l a c t i c acid ra te , c t c . Mer ef fec t s may still be possible (Table),
Systematic psychological invest igat ion i s s t i l l the subject of discussions i n regard t o the methods t o be used; but the contact of the psychologist with the pat ient and h i s family produces the best r e su l t s , Socio-economic benefi ts a re obvious and the return t o work i s morc frequent i n rehabi l i ta ted pat ients than i n the control subjects. This dynamic a t t i t ude towards infarc t ions with a favourable c l i n i c a l development i s sometimes d i f f i c u l t t o apply i n view of the pa t i cn t ' s anxiety, the f ea r s of the attending doctors, the soc ia l organization.

El~l/~ard.Vasc./5 . . E!~/PRV.N. CARD .VSC . D I S / ~ ~ Annex X page v i i i
WHO EMRO
On the o ther hnncl, some problems havc not so f a r been e lucidated; these a re : the optimal durat ion and i n t e n s i t y of physical reeducation programmes, need of a s t ruc tu red a c t i v i t : ~ , long-term r e s u l t s on morbidity and n o r ~ a l i t y .
f i n a l l y , problems of work p h y s i o l o a ax-c t o be i n v c s t i - gated: t h e amount o r energy expended corresponding t o profess iu_. - a 1 a c t i v i t i e s , pal* of the naximal physical f i t n e s s t h a t m y be expended i n a wcrliinb day, e tc .
I S the d e t a i l of t h e programmes nay s t i l l bc questionec:, the physiological , psychological and s o c i a l b e n e f i t s of r e h ~ b f - l i t a t i o n - t h a t i s t o say t h e app l ica t ion oi' a s e t of r u l e s witi? the purpose of comforting the p a t i e n t an2 d i rec t ing him toward an a c t i v e l i f e - appear t o be d e f i n i t e l y a wel l -es tabl ished i 'a~b.
1. Ii-ilprovement o f maxirnuii? worliing capacity ( P V ~ , max. 1
S.L.
2. Rela t ive cos t of lovrer d a i l y a c t i v i t i e s
L
3. B e t t e r per iphereal adjustmen-'; ( AL ir )
4. Improvement of myocardial Pdnction (Qs 71, vh*) (Fa 2c fh) \
5. Obesity - Blood l i p i d s - Coagdlation
6. C o l l a t e r a l c i rcu la t ion .
7 . P.1odifications of adrenarget ic system.
EM/C ard .Vase -/5 El"I/PRV . M J .CARD .VSC . D I S / ~ ~ Annex X I page i
RISK FACTORS
Epiderniologlc a1 r e se mcl? 122s 5.d enitif Led om - of the a t t r i bu te s and circumsta;nces associated wi tli individuals ??ho develop IHD . These a t t r i bu te s arc ca l led r i s k i'actors z ~ d ar;: defined as detectable a t t r i - butes o r circumstances of an indi.uidua1 which ,we known t o be associated with an increased r i s k of developing over-L morbidity. Risk fac tors may be e t io logica l fac tors but e r s not necessari1.y so, o2ten they indicate individuals vrho ai>e a t spzcicl risk ~ i t h o u t actuaLly d e t e m m n g that r i sk .
To be of use a r i s k r^?.ctcr must be readAly detectable i n the individuals involved, i ~ d s t be sp$cZfically ~ s s o c i a t e d with a d is t ind iy increased r i sk of rr .~i~bidit :r ZI,~? : u s t pcrmit the poss ib i l i ty of an ef fec t ive ly e a r l i w l a t e r . - ~ n t i o n I 2 3 ZI v:~uld hcve been possible without knowing of it, i r n ~ r t c n t question ic c~hich diseases are worth con- s iderat ion i n respect of r islr f t z t c r s screening and r i s k f ac to r t r e a t - ment.
It i s gsnorallg -g-cced :21r'A t!ic d i s e s e s most su i tab le f o r inves t i - gating r i sk I"act@?s :flust bs rt-asonayiy comrr~on, ser ious and amenable t o
\ early intervenki-!, c-i-ion. THii i s corfi,nain F-nd serious but i s it amenable t o intervent ivc - ac'ciorl?
Unless the F L I ~ s ~ ~ ~ I C , ~ , ~ LCI 'LYS~ OC ha individual 's heal th can be improved, the i_Lentific,-;tion 02 hlga ~,isi,; inclividuals i s point less o r even harmful. lkeFe is I.l-L~,lt? cridcncc so f2.v t h a t intervention i n IHD i s successful. Tfi~ reason mzs be Lh?.t .t HD i s an example of the effects of post-reproductiva sen l le chc;?ges h35ch s e t biological limits to the duration of perf omancc and survivcl.
man^ i n ~ o r t e ~ ~ t r i s k fac tors f o r davel.opin~ IHD are impossible t o remove, e.g, age, scs , previous occEpation, heredity, but there are three fac tors which have bsen found t o predict LFD among middle-aged men i n many prospective populaticn s tudies 2nd i n which are possible t o i n t e r - vene. These are smolring, high blood pressure: and high blood l i p ids .
* Assistant professcr, Mec?icai Cl inlc I ~ a h l g r e n ' s Hospltal ( C h i e f , Lars Werkii M .D . ) University of G'dtebolpe, G'jtehorg, Sweden

EM/Card .Vasc ./5 EN/PRV.MJ .CARD .VSC . D I S / ~ ~ Annex X I
ii
WHO m o
STOPPING SMOKING
We do not know the e f fec ts on h2altkl when middle-aged men stop smoking. The .etiological ro l e of smoking i n r e l a t i on t o IHD is unlmown. Smoking can af fec t %he aLherosclerotic process i n the a r t e r i e s on the thrombotic mechaaisns. If it af fec ts the atherosclerot ic process it could be too Izte whet pat ients s top smoking a l t e r t h i r t y years of ex- posure. I f it Influences the thrombotic process, the benefi t might be more immediate.
Ind i rec t evidence of the benefi t of stopping smoking i s that excess IHD momality of curient c igare t te smokers great ly decreases a f t e r cessation, and a f t e r f i ve t o t en years it completely disappears,
Another indicat ion comes from e recent analysis of the ecperience of Br i t i sh doctors. During the l a s t f i f t e e n years, most Br i t i sh doctors who smoked c igare t tes have stopped. F i f teen years ago they had a re- ported IHD-mortality which was higher than t h a t of the United Kingdom population a s a whole. It is now below the nationdl leve l .
Erom these observations, it i s possible t o conclude t h a t the evidence is good enough t o j u s t i fy an abandonment of smoking i n order t o reduce the r i s k of developing IHD. To see the benefi ts and the cos ts we need controlLed trials.
PLAN OF ACTION
One way o f stopping smoking i s the method used i n G'dteborg, Sweden I n a preventive t p i c l we asked 10 000 middle-aged men t o change three r i s k factors , hyp?rt.ension, high cholest~erol and smoking and used 20 000 men as contrcls ,
Our anti-smoking programme has been based on a schene presented i n Table 1. The fi-st time we invi ted about Cody persons t o an infor- mative meeting at whic!i a lso individual infoimation on r e su l t s of the e a r l i e r examinations was given. A short t a l k on the heal th consequences of smoking and the smcking mechanisms introduced a discussion a f t e r which the part ic ipants were invi ted t o group meetings (seven t o ten men) with one week's i n t e rva l ?or fur ther information about the recommended ant i - smoking programme 2nd supply of chewing gum with nicotine. The meetings were conduceed by a doctor and one psychologist.
The r e su l t s were promising. Follow-up has shown that fo r ty per cent stopped smoking i n half a year.

WHO EMRO Ebl/Card , ~ a s c ./5 . EM/FBv. M J .CARD .VSC . DI S/17 Annex ](I p&e iii
It i s known t h a t general education, as well a s soc ia l and emotional factors , influence a pat ient ' s a b i l i t y t o adhere t o antihypertensive treatment. Thus, it has been found t h a t drop-outs from treatment have known about t h e i r disease Tor a shorter period, have l e s s education and a lower incoine than those who 2dhere t o treatment. A s i n a l l preventive measures, it i s necessary t o s t r e s s the necessity f o r hea l th education. Cne way i s t o use a special ly designed audiovisual programme including a tape-recorded talk and slides. I n the preventive trial i n G'dtebor~, such an approach has been used. After the information and when the systolXtic blood pressure a t a second v i s i t i s s t i l l 175 o r higher o r the d i a s to l i c blood pressure 115 o r higher, drug treatment i s in s t i t u t ed .
A follow-up a f t e r two years showed t h a t 20 per cent of the subjects were not i n need of dmz treatment, 20 per cent had s t i l l high blood pressure (5175/?115), 30 per cent had a moderate redUCtlOn of the blood pressure and 30 per cent were well regulated. I n G'dteborg, a systematic method f o r ca l l ing pa t ien ts t o follorr-up v i s i t s is used. In t h i s way pa t ien ts who might otherwise terminate treatment with adverse consequences can be callec! i n f o r a return appointment a t a time when preventive measures are s t i l l possible. A s f a r as possible each pat ient i s assigned always t o the same doctor. A s basal treatment s a l u r i t i e s on bet a-blocking agents are used.
DIAGI\IOSTIC WORK-UP AND THEADilENT IN THE KYPERTENSION CLINIC, Gt)TEBORG
The diagnostic work-up and treatment of hypertens .on i s a heavy burden which often requires a special c l i n i c separated from the screen- ing procedure. I n GZjteborg, the Hypei"Lension Clinic takes care of the screened hypertensives. The routine diagnostic work-up i n the c l i n i c i s presented i n Table 2.
The diagnostic work-up starts with a v i s i t t o a nurse. Blood pressure i n supine and i n standing positions i s recorded, blood samples and ECG are taken end appointments f o r chest X-ray and renography are given. A t the second v i s i t , the pa.tient i s examined by a t rained physician. This includes examination of the eyegrounds. A t this v i s i t tne physician decides about fur ther diagnostic examinations, i f necessary prescribes drugs and out l ines plans f o r fur ther manmement. If the blood pressure i s eas i ly controlled and there are no sigms of other severe i l l nes ses , he i s t o l d t o visit a nurse a t the c l i n i c lor blood pressure recordings every second inonth. He i s , however, seen by a doctor a t s i x o r twelve month in t e rva l . The blood pressure readings taken by the nurse i n the in t e rva l are continuously reviewed by the physician who decides on changes o r dosages and drugs.

El,;/Card .Yasc ./5 EM/PRv.MJ .CAFiD .VSC . D I S / ~ ~ Annex X I page i v
WHO EMRO
One of the mostimportant msasures i n prevention of IHD is reduotion of the serum l ip ids , j:ther bt7 die ta ry means o r by drugs.
DIET
Numerous experislenta!. s tvdies have demonstrated that the chole- s t e r o l l eve l c m be influenced by die-bay manipulation. Kinsch (1952) and Gmven (1952) firs% obnelved the cholesterol reducing effect of vegetable o i l s r i ch i n poly u n s a t ~ ~ r a t e d acids, especial ly l i n o l i c acid.
Control of saturated fe.t and cholesterol intake requires simulta- neous a t ten t ion t o meat, daily products, commercial baked goods, but ter , margarine and egg yolks. J. Stamler has pointed out t h a t it is not necessary t o "go on a d ie t" i n order t o protect one's heal th . Instead the sum shoulct be t o learn a new s e t of eat ing nabi t s .
Lean meats end poultry, f i s h and sea food, skim mill:, cottage cheese, beans, peas, fruits and vegetables a re d l recommended. StamLer also emphasizes t h a t it i s s matter of taking t o hear t the lessons impl ic i t i n t h e more natural eat ing habi t s such as those followed in Southern I t a l y , Greece, Dalmatia, China e t c .
DRUGS
Many drugs are a t t hc moment available f o r preventive treatment e .g. thyroid hormones, c lofcbrats , n ico t in ic acid and resins . These drugs a c t by differen5 mechenisms and on d i f fe ren t s i t e s of the organism,
When the p--rp=se i s t o rcduce blood l i p i d s i n healthy asymptomatic men c lof ibra te i s tk d ~ ~ g of choice. It reduces hypercholesterolaemia and hypertr igly~er; idae~ni~, i n the majority of cases. There are, so far, no s igni f icant toxic c f fec ts end it hes minimal s ide e f fec ts . It removes l i p i d accumulation f ~ o m t i ssues . It increases excretion of neut ra l s te ro ids i n the faeces. I n addition t o these e f f ec t s on Lipid metabo- l i s m , clofibra-tn lowers plasma fibrinogen, increases f ibr inolys is and decreases p l a t e l e t adhesiveness.
D I F F I C U L ~ S IN '~'m4n~rn~i' OF A S ~ M A T I C SUBJECTS
1. How are people t o be lncde aware of t h e i r heal th problems so t h a t treatment i s f ac i l i t z t ed?
I n conventiond medicine pzople who f e e l s i ck and wish t o be t r ea t ed are those who v i s i t a doctor. I n a preventive trial, most of the invited subjects feel well when they come for examination. They wish t o be reassured th2 t they awe he-dthy and want t o continue l i v ing a s ~ u a l .
WHO EMRO EM/C ard .Vasc ./5 WPRV .MJ . CABD .VSC .DIS/l7 Annex Xt page v
S u m have cuniplaints but these seldom have any obvious coimection with what we have designed as r i sk factors: high blood pressure, high cholesterol, o r tobacco smolring. I n o rde r t o motivate the par t ic ipants t o act ively s top smoking, change d i e t , o r take p i l l s , it i s necessary t o make them aware of the presence of a heal th problem. This is a very d i f f i c u l t task. We have t o break the medical law: "primum e s t non noncere" i n order t o make an attempt t o prevent a ser ious disease. Besides the psychological inlluences t h a t m i g h t follow e f f i c i e n t treatment, drugs have s ide e f fec ts . This could also be sa id of changing d i e t and cessation of smoking (e.g., weight increase and manta1 disturbances).
The e f f ec t of being aware of something being wrong has not been previously studied. We have found that untreated hypertensive sub- jec t s have very few symptoms, but t r ea t ed hypertensives have considera- bly more. This difference does not seem t o be due t o t he sever i ty of disease but ra ther t o o ther unrelated fac tors . One of our for th- cormng projects m t n i n tms s t u ~ y is t o evaluate the e f f ec t on a subject of being informed t h a t he i s a high-risk man.
2. How can r i sk fac tors be changed?
This problem is by no means solved. Treatment of i l l n e s s may have a prompt e f f ec t on the pa t ien t ' s perception of the disease process. W i t h treatment of r i sk fac tors the r i s k m a y decrease but the subject himself w i l l not not ice any par t icu lar change i n his condition. This absence of a na tura l feedback mechanism has t o be compensatedh some way i n order t o ensure the best co-operation f r o m the subject.
- The motivation- can be increased by heal th education i n the firm
of talks, various audiovisual aids, information booklets and group discussions. One way of get t ing feedback is t o supply d e t a i l s on the change i n r i s k f a c b s brought about by treatment. Blood pressures can be measured by the subjects themselves, cholesterol values can be revealed routinely, and the blood concentration of carbon monoxide shown as ref lec t ing the inhal ing of tobacco smoke.
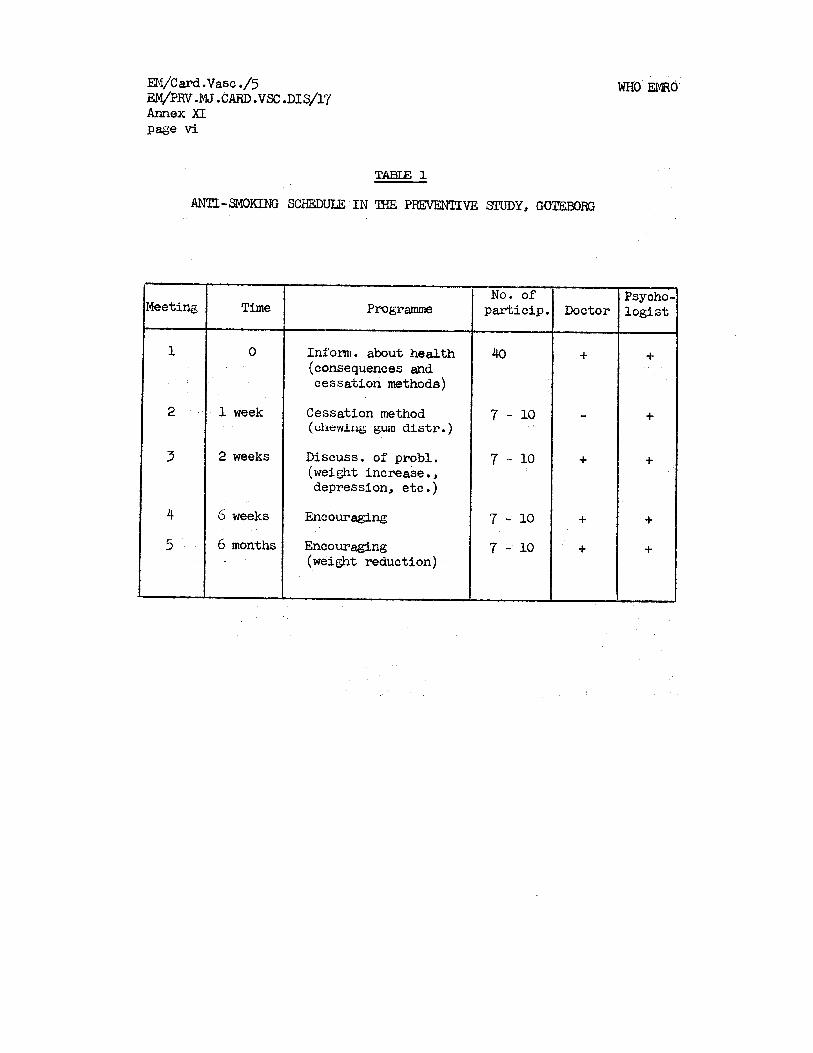
m/Card .Vasc ./5 iQ4/PRV. IUU .CARD .VSC .DI 8/17 Annex X I P a s vi
WHO EMRO
TABU2 1
AN'IZ-sp.IOK1:NG SCHEDULE I N THE PFEVENTIVE STUDY GOTE.EOFF.3
Meeting
1
2
3
4
5
Time
0
1 week
2 weeks
6 weeks
6 months
Programme
Inform. about health (consequences and cessation methoder)
Cessation method (chewing gum alstr.)
Discuss. of probl. (weight increase., depression, etc.)
Encouraging
Encouraging (weight reduction)
No. of particip.
40
7 - 10
7 .- 10
7 - 10 7 - 10
Doctor
+
-
+
+ +
Psycho- logis t
+
+
+
+
+
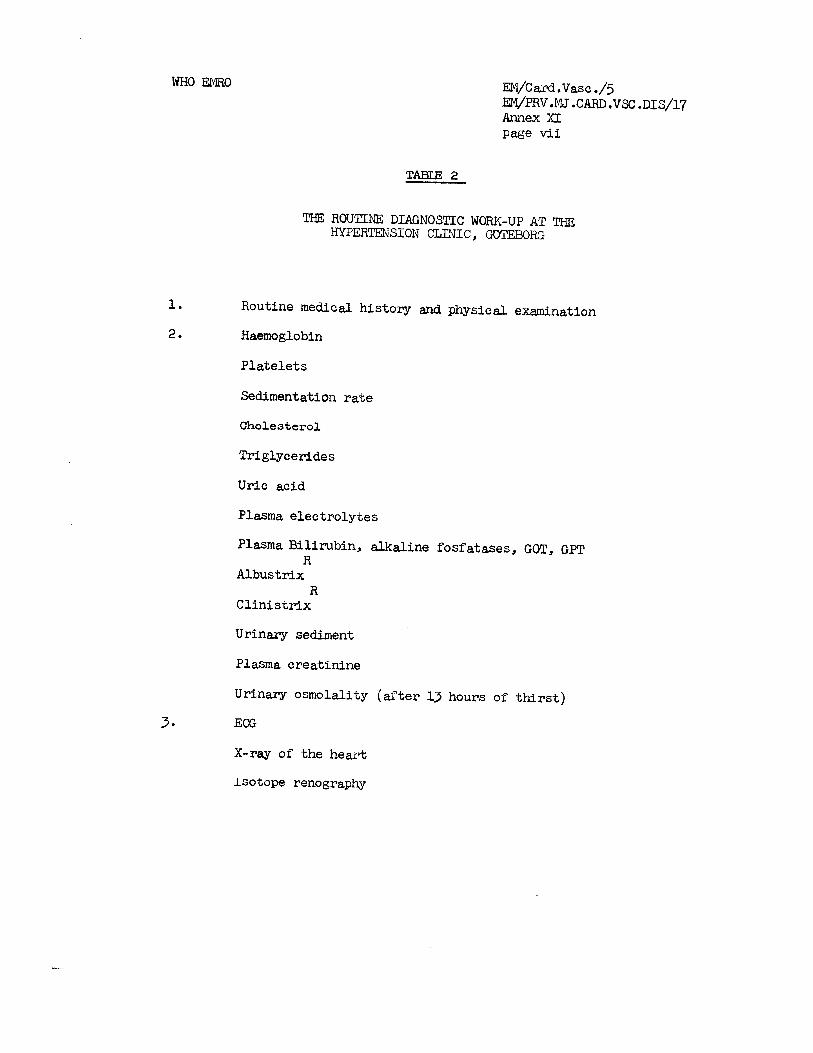
WHO EMRO EM/Card.~asc ./5 EM/PRV, M J .CARD .VX. D I S / ~ ~ Annex XI page v i i
TABLE 2
mE ROUTINE: DIAGNOSaC WORK-UP AT THE HYF'ERTENSION CLINIC, WTEBORG
1. Routine medical history and physical examination
2. Haemoglobin
Platelets
Sedimentation ra te
Cholesterol
Triglycerides
Uric acid
Plasma electrolytes
Plasma Bilirubin, alkaline fosfatases, GOT, GPT R
Albustrix R
Clinis t r ix
Urinary sediment
Plasma creatinine
Urinary osmolality (a f t e r 13 hours of t h i r s t )
3 ECG
X-ray of the heart
Isotope renography

WHO EMRO
ANNEX X I 1
EM/card. ~ a s c ,/5 .
ET'I/PRV. MT; CARD .VSC . D I S / ~ ~ Annex X I 1 Page i
PRFVENTION OF ISCHAEMIC HEART DISEASE
bgr
Z. Fe j fa r , M.D. Chief, Cardiovascular DLseases Unit, WHO/HQ, Geneva
INTRODUCTION
Prevention, i n a broad sense, comprises a corplex of a c t i v e measures aimed at preventing the onset of a disease in healthy o r i n high r i s k sub jec t s (primary prevention), o r i t s f u r t h e r advance i n diseased persons (secondary prevent ion) . Occlusive coronary a the rosc le ros i s with thrombosis i s t h e most frequent p r e c i p i t a t i n g cause i n acute ischaemic h e a r t d i sease which may s t r i k e without preceding c l a s s i c a l symptoms of pain. Treatment and r e h a b i l i t a t i o n of a l l p a t i e n t s suspected of having acute myocardial i n f a r c t i o n o r r r i t h s y m p t u m s uf i~rtntir~erlL acuLe Ischaernlc heareL dlsease Is now possible , and should be ava i l ab le f o r a l l who need it. Prevention of ischaernic h e a r t d isease however still requ i res long e f f o r t , p a r t i c u l a r l y t o impede t h e development of advanced a the rosc le ros i s and thrombosis.
There is a marlred con t ras t between t h e exce l l en t ca re o f i n d i v i d ~ l a l s p a r t i c i ~ l a r l y i n modern hospitals w i t h enormous technical f a c i l i t i e s , and lack o f adequate care f o r a l l i n need i n many communities. Preventive act ions , e.g. t h e con t ro l of coronary r i s k fac to rs , a r e a l s o more o r l e s s provided t o individuals , and ac t ions covering whole communities a r e l imi ted t o general hygiene measures. Mass preventive p r o g r m e s do no t e x i s t . The p o s s i b i l i t i e s of how t o prevent ischaemic h e a r t d isease a r e discussed on the b a s i s of mor ta l i ty data and epidemiological studies.
MORTALITY
Information on mor ta l i ty with a l l l i m i t a t i o n s i s very use fu l f o r planning t h e care and prevention programmes i n t h e community.
The knowledge on the time of death i n r e l a t i o n t o h i s to ry , c l i n i c a l s igns , type and speed of t h e de l ive ry of treat,ment i n t h e community may a s s i s t i n t h e evaluation and in planning care f o r acute cardiovascular emergencies. The WHO cooperative study which is underxay i n 20 communities i n 17 countr ies 1/2/ w i l l , by t h e end of 1972, accumulate d a t a from more than 13 000 p a t i e n t s with acute myocardial in fa rc t ion . Information i s co l l ec ted i n a uniform way with t h e at tempt t o cover a l l p a t i e n t s i n a defined population, a l i v e o r dead. This has been achieved i n a mmber of ways. P a t i e n t s a r e r e g i s t e r e d whenever the re is any suspicion t h a t acute myocardial i n f a r c t i o n might have occurred. Those who a r e seen a l ive , usua l ly have r e t r o s t e r n a l pain. However, i n order

lW/card. Vasc./5 EM/PRV. M J . CARD. VSC . DI ~ / 1 7 Annex X I 1 Page t i
t o cover a l l cases i n the community, death c e r t i f i c a t e s i n t h e a rea a r e regu la r ly checked, medical l e g a l a u t h o r i t i e s asked f o r information a s wel l a s general practit3oner.s and s o c i a l insurance. Screening f o r acute myocardial i n f a r c t i o n a l so , i s being done on p a t i e n t s hospi ta l ized f o r o the r causes.
The diagnosis of myocardial i n f a r c t i o n i s based on t h e h i s t o r y of t h e acute a t t a c k and on development of t y p i c a l changes of t h e e lec t ro - cardioaram. -
Preliminary published r e s u l t s from the Warsaw ( ~ y w i k 1972)~' and Helsinki r e g i s t e r s (Si l tanon 1972)~/snow a nigh f a t a l i t y r a t e . 37 per cent of p a t i e n t s i n Warsaw and 44 per cent i n Hels inki died within four weeks.
Prevention of t h e l e t h a l outcome i n acute ischaemic h e a r t d i sease is of ten a matter of minutes. More than 4@ of a l l cardiac deaths within 4 weeks occur i n l e s s than an hour and about three-quar ters during the f i r s t 24 hours, a s has been s oiin i n severa l comrnh"fity
57 r c l a t c d etud e (~ r rne t rong c t a l , 1372) Fulton c t a 1 1 6pg Kul ler e t a1 1966: 37 McNeilly and Pemberton 1968;8/ R o m m 2 ; 3 / Wikland 19711°/)*
Concerning prevent ior~ p a r t i c u l a r a t t e n t i o n should be given t o f indings t h a t a considerable percentage of p a t i e n t s who died within 6 hours from t h e onset of terminal symptoms, shorred c lear-cut necros i s of t h e myocardium. (Table l ) l l / . This can be explained i n two ways: e i t h e r the evolution of mvocardial nec ros i s i s f a s t e r than shown i n t h e experiments, o r t h e myocardial ischaemia s t a r t e d wel l before t h e appearance of c l i n i c a l symptoms. I f t h e l a t t e r case were t r u e , t h e p o s s i b i l i t i e s i n preventing sudden, unexpected death would considerably increase. The f e a s i b l e way seems t o be t o search f o r e a r l y symptoms ind ica t ing a f u t u r e catas t rophic event and f o r f i r s t a i d treatment ava i l ab le a t t h e moment of the h e a r t a t t ack . The first so lu t ion has usually been sought for from re t rospec t ive s t u d i s s . Approaches f o r evaluating, prospectively, symptoms such as unstable angina, non- s p e c i f i c chest pain, o the r non-specific symptoms such as t i r edness , and arrhythmias, have been proposed by a WHO working group i n 1971 f o r inves t iga t ing prospect ively p a t i e n t s who were once r e g i s t e r e d a s having acute myocardial i n f a r c t i o n . (WHO 1g71)12/ . SO f a r such s t u d i e s have been re t rospec t ive i n nature .
Close cor re la t ion has been found between t h e mor ta l i ty from ischaemic hear t d isease , and quan t i ty and composition o a j o r components i n t h e d i e t and t h e economic l e v e l i n t h e countr ies The o v e r a l l t r e n d i n q u a l i t a t i v e changes of nu tr.1 l i o r ~ YI L ~ I ~ C O I ~ D I I ~ ~ C l e v e l la ~ ~ I U W I I 111
information provided by ~ ~ 0 1 4 1 ; the consumption of t r e a t e d animal and vegetable f a t of p u r i f i e d sugars and of animal p ro te ins increased with t h e income of the countr ies , while the consumption of s tarched carbo- hydrates and vegetable p ro te ins goes do1m-i (Figure 1).
Information on the d i s t r i b u t i o n of myocardial l e s ions and on coronary a the rosc le ros i s i n the communities brought about o the r aspects r e l a t e d t o prevention. Figure 2 shows d i s t r i b u t i o n of a the rosc le ro t i c

WHO EMRO w a r d . vasc./5 EN/PRv. M J . CARD. VSC . D I S / ~ ~ Annex X I 1 page iii
lesivrls in the left anter ior de~cending coronary a r t e ry among 17 453 autopsy specimens co l l ec ted i n ~ a l m 8 , Prague, Ryazin, T a l l i n and Yalta. Regardless of the causes of death, f ib rous plaques, complicated l es ions and c a l c i f i c a t i o n a l l appeared a l ready i n adolescents, and were found i n around 8@' i n men 35 - 44 years of age. The frequency of complicated l es ions began t o r i s e i n t h e same age grou
45/ I n tvomen, a s i m i l a r evolution s t a r t e d about a
decade l a t e r . A high percentage of adu l t s , between 40 and 59 years of age,
were found a t autopsy t o have ischaemic h e a r t d isease . A marked s tenos i s o r occlusion of a branch of t h e coronary a r t e ry , f r e s h myocardfal i n f a r c t i o n o r myoczrdial sca r were t h e diagnost ic c r i t e r i z .
These autopsy d a t a co l l ec ted i n t h e communities c l e a r l y i n d i c a t e t h a t prevention of ischaemic hear t d isease should s t a r t i n e a r l y adulthood (20 - 30 years) and prevention of a the rosc le ros i s i n childhood.
Figure 3 shows t h e hypotl iet ical increase i n t h e expectation of l i f e a t 5 years, i f c e r t a i n important c l i n i c a l condit ions were eliminated. The estimated prolongation would be l e s s than 2 years i f one would con t ro l o r prevent r e s p i r a t o r y d i seases o r accidents, and f o r m a l i p a n t neoplasm t h e prolongation ;vould be l e s s than 3 years. I f however, a l l cardiovascular d i seases would be eliminated, t h e prolongation n f life expectancy r~ou ld he more than 3 y e m s with the mean value 8 years f o r males and 9 years f o r females. For h e m t d i seases ( i . e. mainly ischaemic h e a r t d isease) t h e average f o r both sexes would approach 5 years.
These es t imates i n d i c a t e very c l e a r l y t h a t preventive measures t o be undertaken a t t h e l e v e l of the community need t o be simultaneously accompanied by m adequate consideration of the whole complex of mediczl and s o c i a l a spec t s concerning t h e aging population. Without t h i s we might add years t o l i f e but no t t h e enjoyment o f l i v i n g f o r a considerable percentage of t h e population.
RISK FACTORS IN ISCHAFM-IC. -H'ZART DISEASE ---- -- -- --
Ischaemic hear t d isease has been known f o r years t o be r e l a t e d t o a number of personal c h a r a c t e r i s t i c s end f a c t o r s i n t h e environment. A formidable, though incomplete, l ist able 2) sho t~s t h e g r e a t v a r i e t y of f a c t o r s found t o be r e l a t e d t o a the rosc le ros i s and ischaemic h e a r t d isease . Some of them a r e widely accepted (age, e levated choles terol , hypertension and smoking), ot:?ers a re con t rovers ia l ( s t r a s s e r 197216/) .
The pred ic t ive value of these f a c t o r s v a r i e s considerably i n d i f f e r e n t environments. Multtple l o g i s t i c ana lys i s enables quan t i t a t ive assessment of t h e r i s k of ischaemic h e a r t d-isease. Similar l e v e l s of blood pressure, blood cho les te ro l and c i g a r e t t e smoking appear t o be associa ted with a lower incidence of ischaemic h e a r t d isease i n Europe than expected f r o m data in the USA ( ~ e p 197217/). A study of residents
w a r d . ~ a s c ./5 EM/PRV.MJ. CARD.VSC . D I S / ~ ~ Annex X I 1 Page i v
WHO EMRO
i r i r-ur.trl ar~d u~.Lau aree.s in Jr-pal, separat ing in the l a t t e r , t h e executives, ph; s i c i m s , c l e r i c a l and manual r~crkers , showed t h a t hypertension i n groups v i t h a low serum chol es ter01 l e v e l bras associated with ce rebra l stroiie. T:le incidence of ischaemic h e a r t d isease was positivel-cr co?relc?-ced with t h e l e v e l of blood cho les te ro l (Komachi -- e t a l l S ) --- Tilts confirms previous f indings t h a t Japanese l i ~ r i n g f o r m-AJ~ years i n Haicaii, a d suf fe r ing r e l a t i v e l y more from ischwmic l?-.%ct disec".se than from cerebra l stroke, have considerzbly higher blcod l i p i d l e v e l s (Kagan 197019/). Ten years ' incidence of ?cute myoenrdiai in fa rc t ion , including t h e f a t a l i t y rate, among J c p a ~ c c c mcn ~ ~ c d 35 - 64 years, was lower than among Hawaians (Bas3et-k 1970~": ) .
The evolution of a t l ieroscleros is and ischaemic h e a r t d isease , i n r e l a t i o n t o some e t i o l o g i c s l f ~ . c t o r s , i s shown schematically i n Figure 4-l3/ . The f u l l l i n e i n d i c e t e s evolution of n the rosc le ros i s i n epidemic areas , t h e do t ted l i n e shows gradual increase of f ibrous ~ l a a u e s i n a reas where ischaemic heaL-t d i sease i s r a r e . Prevalence of c l i n i c a l ischaemic h e a r t d iscasa begins t o r i s e about 1 0 years l a t e r than advanced l es ions i n t h e coronary vessels . The vascular l e s ions of t h e c e n t r a l nervous system (not i n graph) begin again about 10 years l a t e r than ischaemic h e a r t d isease .
Hypertension, d iabe tes a d gout may b6 considered schematically t o appear commonly 8.t the ege of about 40 years, the re fore i n t h e time when t h e process o r a the rosc le ros i s is f a i r l y advanced ,and when the re a r e a l r e ~ d y ischaemic l es ions i n t h e myocardium. That means t h a t a l l these f a c t o r s may advance t h e evolution o f a the rosc le ros i s , o r even provoke acute cardiovascular accident; however, they cannot be the primary cause even though hyperkns ion i n most population s t u d i e s i s an independent, impor.t3+r,t, pr.edj spo s ing " r i sk" f a c t o r , a s important as increesed blood l i pids.
The noxious e f f e c t of c i g x e t t e smoking i n t h e development of ischaemic h e a r t d isezse has been c l , ~ r i f i e d t o such ,?n ex ten t t h a t , 2 t t h e 24th World E e d t h I"-ssenlblg i n Geneve i n 1971, 3. s e r i e s of recommendations f o r inri ividusl and comrnunity2l/have been formulated.
A s for t h e r o l e of physical a c t i v i t y it is d l f f i c u l t t o a$$fpuch t h a t i s new t o t h e hypothesis cu t l ined by Morris e t a1 i n 1953= . We
-0
a r e s t i l l s t rugg l ing with the problem horr t o measure hab i tua l physical a c t i v i t y and most of our kno~liiedge i s r ined from t h e assessment of physical a c t i v i t y by exercise t c s t ~ ~ 3 / ~ ~ / ~ 5 / .
Apart from genet ic f a c t o r s , t h c beginning of a the rosc le ros i s i n childhood appezrs t o be r e l a t e d t o n u t r i t i o n , t o d i e t a r y h a b i t s and t o s o c i a l environment. To assess the mental f a c t o r s is d i f f i c u l t , because of t h e methodological problems i n measuring c h a r a c t e r i s t i c s of an individual i n h i s s o c i a l environiient, c h a r a c t e r i s t i c s of our c i v i l i z a t i o n , such a s overcrowding, over-motori zation, sedentary l i f e bekllnd Lhe w h e e l o f the c a r and i f r o n t of the t e lev i s ion , ever-
28/ increas ing l i f e speed ~ n d o thers .
WHO EMRO EN/card. ~ a s c . / 5 EM/PRV. MJ . CARD. VSC . DI ~ /17 Annex X I 1 P a g ~ v
The problem of n i ~ t r i t i o n and dic=t,srg habits is, of course, r e la ted , t o a l a rge extent , t o childhood, \<,i th the recogni t ion of t h e rn~~lnourished c h i l d from c a l o r i ~ overnu t r i t ion . An e levated l e v e l of cho les te ro l ?.nd other l i p i d s may, perhzps, be one of t h e b io log ica l parameters of t h i s .
Most l i p i d s i n plasma ? r e present a s l ipopro te ins and hyperlipidaemia near ly ~ lv rays mecans e lsvated concentration of some l ipoprote ins . The most p r a c t i c a l rray of d-etecting hyper l ip i - daemia is t o measure t h e concentration of cho les te ro l and t r i g l y - ce r ides i n the blood. It s l s o provides some, but n o t a l l , ~nformat ion on t h e type of hyperlipopro Lcir~aernf a. A number of s t u d i e s i n recen t years have revealed evidence t h a t c l z s s i f i c a t i o n of hyper l ipoprote in~emias i s needed f o r d i f f e r e n t i a l d iagnosis of t h e gene t ica l ly determined defec t s i n l i p i d metabolism, f o r d i f f e r e n t i a t i o n of hyperlipoproteinaemias accompanying common d i seases which promote a the rosc le ros i s , f o r r a t i o n s 1 t r e ~ t m e n t o f l i p i d d i s tu rbmce , and t o a s s i s t i n t h e discovery of t h e causes mc? mechanisms of hyperlipidaemia. A n i n t e r n a t i o n a l l y accepted simple c l a s s i f i c a t i o n should enhance knowledge on t h e d i s t c i b u t i o n of t h e disturbanc s i n l i p i d metabolism i n d i f f e r e n t e thn ic groups and
277 environments . Chzrac te r i s t i c s of plasma l ipopro te ins a r e assessed from concentration of serum cho les te ro l and t r i g l y c e r i d e , from t h e presence and/or absence of chylomicrons, abnormc,l p ro te ins and from estimation of Low dens i ty and very lov,l d e n s i t y 1j.poproteirls.
The dominant r o l e of n u t r i t i o n i n t h e progression of t h e a the rosc le ros i s process, and f o r t h e development of ischaemic h e a r t d isease , i s general ly ~ c c e p t e d . Thz chmges i n n u t r i t i o n i n r e l a t i o n t o mor ta l i ty and t o t h e n a t i o n a l income, have been a l ready mentioned (page 23).
A review of '(4 populatron s t u d i e s v?filcll were done a t d1fferenL times and of which methodology c ~ m o t be considered a s s t r i c t l y compar&ble, sho t~s t h a t c l a s s i c ~ l l ischaemic h e a r t d isease appears t o become frequent when the t o t a l c a l o r i e intaknkt. is g r e a t e r than 2 600/day, t o t a l f a t i n t d s e more than of a l l cn lo r ies , and da.ily animal f a t more than hnlf of t h e t o t a l f a t consumption ( F e j f a r and Mzsironi 1 9 7 0 ) ~ ~ / . Ischaemic h e m t discase incre2ses i n frequency with serum cho les te ro l l e v e l over 200 mg/dl (Figure 5). There i s a s i g n i f i c a n t c o r r e l a t i o n b e t v e ~ n blood cho les te ro l l e v u l s 2nd t o t a l consumption o f f a t (Figure 6), animal f a t o r sa tura tdd f a t , and nlso betwten thc t o t a l f a t consumption or. blood c ~ i o l t s l e r ~ u l arid t l ~ g l - e ~ of a t . l~e rosc l t roa ia at autopsy ( ~ a b l c 3 ) .
Thc r i s k of ischaemic h e a r t d isease i s increas ing with t h e number of prsdisposing fec to rs ; however only about 5% of t h e middle aged men i n one USA study have a l l th rcc major r i s k fac to rs , i . e . hypertension, hyper- cholesterolaemia and c i g a r e t t e smoking. Although near ly one-third o f them developed myocardial infa,rct ion within 10 years, this mounts only t o 104% of a11 in fa rc t ions . I n a prcdorninant, r n ~ jnrity of sub jec t s t h e r e was only one f i n 45%) o r two ( i n 3096) f a c t o r s present ; these two groups
w a r d . Vasc . /5 EM/PRV. M J . CARD. VSC . ~ 1 S / 1 7 Annex X I 1 P a g ~ v i
WHO EMRO
contributed t o f o u r - f i f t h s of a l l in fa rc t ions . Those with 2 and 3 r i s k f a c t o r s taken together would mount t o 35% and account f o r more than h a l f o f a l l infarctions.'g\ S i x i l a r da ta could be derived from other epidemiological s tud ies . Screening of a d u l t s f o r coronary r i s k f e c t o r s may thereyore i~ d i c a t e t h ~ s e groups of ind iv idua l s ~ h o a r e i n higher r i s k . 307
PIIEVENTIVE TRIALS
An inventory of m u l t i f e c t o r i ~ l o r u ~ ? i f a c t o r i a l primary prevention t r i a l s has been assembled by WHO i n cooperation with t h e Council on Ar te r iosc le ros i s and ischacmic h e a r t d isease of t h e I n t e r n a t i o n a l Socie ty o f Cardiology. I n most of them t h e main attempt is t o influence thc dis turbed l i p i d metzbolism by 333 ~ p p r o p r i a t e d i e t o r by drugs.
Encouraging r e s u l t s have been obts ined but no f i n a l answer so f . One of t h e reasons might be t h a t most t r i a l s , f o r p r a c t i c a l reasons, s t a r t i n middle-agsd men i n whom coronary a the rosc le ros i s has a l reaay been well dcveloped wllu tilay have scars in the myocardium - witnessing c l i n i c a l l y s i l e n t ischaernic a t t acks .
A s increased l evd l s of blood l i p i d s appear t o be t h c f i r s t biochemical a b n o r m ~ l i t y i n ~ . t h e r o s c l e r o s i s , a double-blind preventivc t r i a l designed t o investigz-te t h e e f f e c t of reducing blood cho les te ro l i n a d u l t s aged 30 - 59 y c m s without m'mifest ischaernic h e a r t d i sease has been sponsorad by WHO in Budapest, Erlinblrgti , Tnndon and prague31/.
Tha t r ie l s t a r t e d i n Edinburgh i n 1965 2nd was extended t o Prague and Budapest i n 1966 and 1967. 15 000 men have been r e c r u i t e d from blood-donors, population r e g i s t e r s nand o the r sources i n t h e t h r e e centres. On t h e b a s i s o f e preliminary detwmination of serum cho les te ro l l e v e l men i n t h e upper t h i r d of t h e d i s t r i b u t i o n curve of cho les te ro l values were assigned ct rmdom t o a t r e a t e d group taking 1.6 g of c l o f i b r a t e d a i l y o r t o a con t ro l group taking i d e n t i c a l capsules containing 300 - 500 mg of o l i v e o i l . A second con t ro l group chosen ?t rmdom from loi<?est t h i r d o f t h c cho les te ro l d i s t r i b u t i o n , a l s o receives the o l i v c o i l capsules. The study i s designed t o have a 9@ chance of detect ing, i n t h e t r e a t e d group, F+
reduction of one-third i n incidence of ischaernic hear t d i sease i f t h i s should occur. Subjects a r e exanined i n i t i e l l y , a t 6 monthly i n t e r v s l s f o r two years c?nd t h e r e a f t e r m n u ~ l l : ~ f o r t h e remainder of t h e f i v e y e w s f o r i ~ h i c h the study is designed. Data e r e s e n t t o London f o r processing and analys is . Blood samples are t e s t e d f o r adherence t o the drug. Incidence o f ischnemic h e a r t d i sease i s defined i n t e r m s of myocardial in fa rc t ion , sudden death and myocardial ischaernia. Suspected events a r e reviewed by an independent panel of s p e c i a l i s t s i n cardiology. Standardization of serum cho les te ro l est imations and ECG find-ings m e d i s c u s s ~ d . A l l sub jec t s have been admitted t o the t r ia l by 1971 .an& t h e i r c h a r a c t e r i s t i c s are known, but it i s too e a r l y t o r e p o r t anv r e s u l t s i n terms of in fa rc t ion , ischaernic o r death.

WHO EMRO EM/~ard. Vasc , /5 Ei"I/PRV. MJ. CARD.VSC .DIS/17 Annex XTI Page v i i
Since etiology of isohaeinio heart d iccnse appears t o be multi- f a c t o r i a l , t h e m u l t i f a c t o r i a l prevention approach is log ica l , though such s t u d i e s may become complex and it 4 s p a ~ t i c u l a r l g d i f f i c u l t t o d i f f e r e n t i a t e t h e more from t h e l a s s impo;?t?nt f a c t o r s .
Mul t l factor primary preventive t i - ia ls sponsored by WHO European Off i c e s t m t e d i l l London (W) ~71id E ~ ~ u s s e l s (Belgium), while t h e cen t res i n Warsaw (Poland.) md Rcme (Ttely) hope t o jo in t h e study l a t e r t h i s year, InvestLgators fyom these ceil tres met i n Warsaw a t an meeting from 25 - 30 ~ u n e 3 ~ / . A progress r e p o r t on a randomized study c a r r i e d out i n f a c t o r i e s has been presented, and the operat lng protocol l i n a l i z e d . Y'ne cen+re i n G8teborg ISiieden) is a l s o carrying out primars a ~ d s?condx?y preventive trials i n ischaemic h e a r t d isease on a pop l~ la t io r b a s i s . r i th a l l o c a t i o n of individuals i n t o zn in te rven t ion a n 2 c c n t r o l group.
Reduction of e levated blood pressure, blood c h o l e s t ~ r o l o r t r i g l y c e r i d e s , reduction of high ca1.ori.e in take, p a r t i c u l a r l y from fat. and l i m i t a t i o n o r stopping of cigarette smoking should decrease t h e problem of a the rosc le ros i s m d ischeemlc h e a r t d isezse , but these measures a r e f a r from mass prevention of t h e condit ion. This requ i res f u r t h e r research.
The recognized predisposing f a c t o r s of ischaemic h e a r t d isease accumulate with age and t h e r i s k of ischaemic hear t d isease increases with age and with t h e number of i rcdisgosing ?actors. H o w ~ ~ r e r the major i ty of sub jec t s who s u f f e r from ischaemic hear t d i sease may present one o r two r i s k f a c t o r s only.
Preventive measures concerning ischaemic h e a ~ t d i sease should i d e a l l y be applied t o t o t a l p ~ g u l ? ~ t i o n s , s t a r t i n g i n childhood, and be o r ien ted towards proper n u t r i t i o n and t o : ~ i ~ r d s c rea t ing an optimum environment f o r optimum physics1 sncl mental development and growth ol' t h e c h i l d and edolescent,. Such long-term s t u d i e s i n man do n o t e x i s t . Preventive s tud ies , r!;~l'ilf ac cor ia l o r un i f a c t o r i a l , ?.re a l l c z r r i e d ou t on adu l t s of middle age, msinljr men.
I n order t o promote such invest3-getioas9 a symposium on t h e metabolic aspects of ischaemic h e a r t d isease prevention ~ s s held i n Madrid from 2 - 4 October, i n cooperetion with the Cocncil on Ar te r iosc le ros i s and Ischaemic Heart Disease of t k 4 InAcernational Socie ty of Cardiology and t h e Medical Tribune. Ongoing s t u d i e s on prevention were c r i t i c a l l y reviewed. The major p a r t of the syrr.posj.um rvas however devoted t o discussion on investlga-tions on metnhnlir processes associated with t h e development of a the rosc le ros i s and ischaemic h e a r t d isease , with t h e o r ien ta t ion and emphasis how t o reverse o r i n h i b i t t h e d.eve1opmen-t of coronary a the rosc le ros i s and ischaeniic h e z r t d isease . These mlght include common metabolic pathways i n l i p i d s and carbohydrate metabolism; t h e r o l e of t r a c e minerals; t h e problem of adequate n u t r i t i o n f o r t h e optimum growth, physical aznd mental development of a chi ld ; de tec t ion c v l d care of ind iv idua l s a t risk from imminent myocardial infarction. Future cooperative inves t iga t ions were a l so proposed.
EM/card. Vasc . /5 EM/PRV. M J . CARD. VSC . DIS/17 Annex X I 1 Page v i i i
WHO EMRO
Research over the past 20 years, however, has n t l e a o t brought about recogni t ion of t h e s i t u a t i o n and changed e n t i r e l y our opinion. Ischaemic hear t d isease i s no longer an inev i tab le problem of aging: it can be rrell t r e a t e d 'and in tens ive resezxch goes on i n a l l cont inents on how t o decrease i ts frequency t o a minimum. ldhen t h i s w i l l apply a l s o t o research i n t o the biology of man rjld t o t h e evolution of t h e h e a l t h services , adequate t o new problems, b u i l t on a s o l i d s c i e n t i f i c b a s i s m d covering a l l members in t h e com- munity, lare ~ 1 1 3 1 1 be able t o conclude t h a t human c i v i l i z a t i o n is beginning t o be human.
SUMMARY
1. Morta l i ty from ischaemic h e a r t d i sease has been s t e a d i l y increasing, i n t h e p a s t 20 years, more i n younger men, although t h e mor ta l i ty r a t e s a r e dependent on age i n both sexes. Great d i f fe rences i n mor ta l i ty c ~ m be demonstrated between t h e countr ies a s wel l a s within t h e countr ies . Information on morbidity from i - sohaemio heart d iscnsc ie not i n t e r n a t i o n a l l y recorded. Nevertheless epidemiological and c l i n i c a l s t u d i e s more o r l e s s confirm mor ta l i ty data .
2. Analysis of t h e l i f e t?.bles shows t h a t cardiovascular d i seases are t h e main obs tac le f o r t h e prolongation of l i f e . It has been estimated t h a t hypothst ica l "elimination" of a l l accidents, r e s p i r a t o r y d i seases o r malignant neoplasms would prolong l i f e expectation by l e s s than 3 years. I n con t ras t t o t h i s , expected proloqgation would amount t o about 5 years i f a l l h e a r t d i seases were el iminated. The l o g i c a l conclusion t o be dralhm i s t h a t l a rge sca le preventive ac t ions must be simultaneously accompanied by appropr ia te a c t i v i t i e s f o r medical and s o c i a l care of aging populati ons.
3. Follow-up s t u d i e s of population groups have g r e a t l y contr ibuted i? overcoming t h e t r a d i t i o n a l concept t h a t age m d the male sex a r e p r i n c i p e l and unavoidnble r i s k s of coronary h e a r t d isease . They produced evidence t h e t a number o f c h a r a c t e r i s t i c s of the host and f a c t o r s i n our environment a r e operating, some o f them s ince b i r t h . They accumulate wFth age sad t h e i r combinations mag have en addi t ive e f f e c t . Some may fo recas t o r even provoke c l i n i c a l manifestat ions o f acute coronary h e a r t d isease . Others a r e associa ted with accelera ted progress of coronary a the rosc le ros i s . The l a t t e r beg im i n childhood and metabolic disturbance, manifested bv elevated blood l l p l d s mag be ccnslaered Its e a r l y b lo log lca l expression. The r e l a t i v e oreight of c e r t a i n r i s k f a c t o r s i n d i f f e r e n t s o c i e t i e s can be exemplified by a r t e r i s l hypertension, vrhich i s a l s o f requent i n populations 7.rhere coron?ry h e a r t d isease i s uncommon. The prcgnost ic importance a l so appears t o have a l t e r e d i n p a t i e n t s rho recovered from the f i r s t myoca~dia l in fa rc t ion .

WHO EMRO E;rf/~ard. vasc./5 EM/PRV. M J . CARD. VSC . D I S / ~ ~ Annex X I 1 Page i x
4. Although the etiology of atherosclerosis and of ischaemic h e a r t d isease has no t been f u l l y c l ~ r i f i e d , the present evidence po in t s c l e a r l y t n the need of nationwide informetion and advice t o t h e public. This r e l a t e s p a r t i c u l s r l y t o t h e d i e t , wZth moderation i n c a l o r i e in tdse re levan t t o physical a c t i v i t y , and i n p a r t i c u l a r reduction of the proportion of f s t i n t h e d i e t . It r e l a t e s t o the e l iminat ion of c l g n r e t t e smoking s ince youth, and emphasizes t h e importznce of b e t t e r physical f j t n e s s f o r heal th . It a l s o r e l a t e s t o t h e ca re of sub jec t s wi tn increased r i s k of Iscliaemic h e ~ r t d isease .
5. Early adulthood - t h i r d decade of l i f e - appe?.rs t h e des i rab le time f o r a d v x a t i n g mass ac t ions t o prevent ischaemic h e a r t d isease . Some of t h e f a c t o r s contr ibut ing t o t h e dev&lcpment of a the rosc le ros i s may be operat ing already from childhood, md f u t u r e inves t iga t ions need t o concentrste on t h e prevention of q, therosclerosis a t t h i s age.
6. Even i f a l l ava.ilable con t ro l measures were applied, cardiovascular d i seases i n a d u l t s would s t i l l remafn t h e most important problem i n t ec l~no log jca l ly advcmced communities. Further research is urgent ly needed t o c l a r i f y the e t io logy of a the rosc le ros i s and hypertension, t o provide f o r e a r l y diagnosis of ischaemic h e a r t d isease and t o introd-uce on a mass s c a l e scientifically proved prevention mecaures.
7. Mult i -d isc ipl inery approach i s obvious today. It requires , among others , the c o n c e n t r ~ t i o n of b r ~ i n s ,-ad of equipment i n l a r g e r i n s t i t u t i o n s , be it t h e h o s p i t a l s o r research i n c t i t u t c s m d i n t e r n a t i o n a l coopcretion. Phys ic i s t s s h ~ w e d the advantages of t h i s approach mmy years ago.
Exchange of i n f o m a t l o n from d l f f e r ~ n t cu l tu res , t r a d i t i o n s and socio-economic organizat ions assures rap id app l ica t ion of preventive measures. Division of work may speed up resecrch on e t in logy and prevention. This may be done by inves t iga t ing t h e importance of e t i o l o g i c a l f ~ c t o r s i n a reas with d i f f e r e n t incidence of the d-isease, o r by pooling s c i e n t i f i o information obtained i n s s imi la r way from suvtr?.l places. It goes without saying t h a t the viorldwide problem can be solved b e t t e r and f a s t e r by coordinated cooperation them i n i s o l a t i o n and individual ly . WHO, with access t o and cooperation of 135 member s t a t e s , can =IS is p1-epdrvC1 LU take up L l ~ t . ~ . e b p u ~ l b i b i l i L y fur ~ U C ~ I worldwide cooperation t o t h i s end.

EM/Card. ~ a s c . / 5 EM/PRv. M J . CARD. VSC . D I S / ~ ~ Annex X I 1 Page x
WHO EMRO
1. WHO Regional Office f o r Europe: Ischaemic Heart Disease Regis ters - Report of a Working Group, Copenhagen, 1968. E~O-5010 (1) (1969)
2. WHO Regional Office f o r Europe: Ischaeinic Heart Disease Regis ters - Report of t h e F i f t h Working Group, Copennagen, 1971. EURO-8201(5)
3. RYWIK, S.: The epidemiology of ischeemic hea r t d isease i n Polmd baaed on the results of tho studies conducted by the I n s t i t u t e of Cardiology i n Warsaw. Abstracts of papers of the Symposium on Epidemiology and Prevention of Coronary Heart Disease, Helsinki, 23 - 25 March 1972. The Scand. J. Clin. Lab. Invest . , 3., Suppl. 122, p. 12 (1972)
4. SILTANEN, P.: The Ischaemic Heart Disease Regis ter a s a Frame fo r Preventive Measures. Adv,mces i n Cardiologj , 1972 (in press)
5. ARMSTRONG, A., DUNCAN, B., OLIVER, M.F., JULIAN, D.G., DQNALD, K.W., FULTON, M . , Lutz, CJ. m d MORRISON, S.L. : Natural History of Acute Coron~sy Hezrt Attacks. A Cornrnunit!r Study. B r i t . Heart J., 3, NO. I., 67 - 80 (1972) -.
6. FULTON, M. , JULIAIT, D. G. , rtnd OLIVER, M. F. : Sudden Death and Myocardial Infsrotion. Ciroulation 33 and 42, Suppl. 4, 182 (1363)
7. KUL;LER, L., LILIENF'ELD, A., m d FISHER, R.: Epidemiological Study of Sudden and Unexpected Deaths due t o Ar te r iosc le ro t ic Heart Disease. Circulation, - 34, 1056 (1966)
8. McNEILLX, R.H. end PEfBERTON, J. : Duration g f Last Attack i n 998 Fa t a l Cases of Coronary Artery Disease cvld i t s Relation t o Possible Cardiac R e s u s o i t a L i u r ~ . Br'l L. Med. J., 2, 1 3 (1968)
9. ROMO, M. : Sudden Cororl~ry Death. Abstracts of papers of thz Sjmposium on Epidemiology and Prevention of Coronary Heart Disease, Helsinki, 23 - 25 March 1972. The Scmd.. J. Clin. Lab. Invest . , 29, Suppl. 122, p. 18 (1972) --
10. WIKLAND, B.: Medically Unattended Fa t a l Cases c f Ischaemic Heart Disease i n a Defined Population. Acta rned. scmd. 189, suppl. 524, 1971.
11. WHO Sc ie r l t i f i c Group on the Pathological Diagnosis of Acute Ischaernic Heart Disease. Wld. Hlth. Org. Techn. Rep. Ser. No. 441 (1970)
12. WHO Regional Office f o r Europe: The Prcdrornel Symptcms o f Myocardial In fa rc t ion and Sudden Death, Report of a. W~rking Group. EvRO-8204(3) (1971)
13. MASIRONI, R.: Dietary Fcctors and Coronary Heart Disease. Bull. Wld. Htlh. Ora. 32, 103-114 (1970)
WHO iNR0 m~r/card. Vzsc . /5 EM/PRv.MJ.cARD.vsc.DIs/~~ Annex XI1 Page x i
Provis ional Ind ica t ive World P l ~ n f o r Agricul tura l Development: A synthesis m d ana lys i s o f f a c t c r s relevcant t o wcrld, regional m d na t iona l a g r i c u l t u r a l development. Food m d Agriculture Organization of t h e United Nations, - 2, August 1969, ~ 6 9 / 4
The Work of' WHO i n 1971 - Annual Report of t h e Director- General. Off. Rec. No. 197, YHO, Geneva (1972)
STRASSER, T: Atherosclerosis and Coron8,rg Heart Disease: The Contribution of Epidemiology. WHO Chronicle 26, 7 - 11 ' 1972)
KEYS, A.: m a n t i t a t i v e Estimation of Risk. Abstracts of papers of the Symposium on Epidemiolog?~ and Prevention of Coronary Heart Disease, Helsinki, 23 - 25 March 1972. The Sce~ld. J. Clin. Lab. Invest . , 29, Suppl. 122, p. 17 - 18 (1972)
KCMACHI y Y 9 IIDA, M SHIMAMOTOg T. 9 CHIKAYAMA, Y y TAKAHASHI y H. y
KOKCSHT, M . , ~nr! TOMINAGA, S. : Geographic m d Occupational Comparisons of Risk F ~ c t c r s i n Cardiovascular Diseases i n Japan. Jap. Circula t . J . ( k g l . ~ d . ) , 35, No. 2, 189 - 207 (1971)
KAGAN, A. : The E p i d e d o g y of Coronary Heart Disease among Japanese Men Living i n Hiroshima m d Honolulu. From: Cardio- vascular Epidemiology i n t h e Pac i f i c , Raport of a WHO Meeting o f Inves t lga t lon i n lYelllngton9 New Zei: i la~d, 9 - 14 February 1370, WHO document CVD/70.6 (1970)
BASSETT, D.R.: Epidemiologic Studies of CErdiovascule.r Disease i n H ~ . w - i i . I n - Symposium on Epidsmiology of C a r d i o v a s c u l ~ r Diseases i n t h e Asim P a c i f i c Area, Chsirmzn: S i r Kempson Pladdox. 4 t h Asian-Pacific Congress of Cardiolog:r, I s r a e l , 1968; i n Cardiology, Current Topics and P m g r ~ s s , M. Fliakim and H.R. Neufeld - e d i t o r s , Academic Press, New ~ork/London, pp. 18 - 21 (1970)
Resolutions end Decisions - World Health Assembly, WHA 24.48: He.d& consequences of s m o a
Morris et 21 - C!ronary Hezrt Di-sc_ase_ end Physical Act ivi ty of Worlf, Lancet 2, 1053-1111, 1953
Assessment of Habitual Physicel A c t i v i t , ~ : Report of meeting of WHO -=- 2- temporary advisers, Prague, 1, 2 m d 6 August 1971. I n t e r n a l document OID/71.4
Lange Anderson e t 31, Fundamentals o - f E c i s e Testing, WHO, Geneva, 197 1
25. Exercise Tests i n Reletion t o Cardiovnscular Function, Wld. Hlth. Org. Techn. Rep. Ser. 1968, - - 388

EM/card. ~ a s c . / 5 EM/PRV. MJ . CARD. vsc . ~ 1 S / 1 7 Annex XI1 Page x i i
26. ISCflHO Meeting on Neural nnd Psychological Mechanisms of --- --'---
Cardiovascular Disease, 19 - 21 J u l y 1971 ( p F o ~ e e m - I1 Ponto, ~ilan-ess)
q. Beaumont e t al, 1970, Class i f i ca t ion of Hyperlipidaemia - --- - - .-- --- . --.- and Hyperlipoproteinaemias Bul l . Wld. Hlth. Org. 1970, 43,
915 --. .-- -- ---A
28. FEJFAR, 2. and MASIRONI, R. : Dietary Factors and Cardiovascular Disease - Epidemiological Studies i n Man. Proceedings of t h e 3rd In te rna t iona l Congress of Food Science and Technology, Washington D.C. 9 - 14 August 1970, p. 314-322 (1971)
29. Epstein, F.H., The value of screening examination on i d e n t i f i e d high r i s k ind iv idua l s i n coronary hear t d i sease prevention programmes - i n Cardiology, current top ic and progress, Symposia of the 4th Asian-Pacific Congress of Cardiology 1968,. Jerusalem end. T e l Aviv, I s r a e l . M. Ebrahim, and H.R. Neufeld - ed i to r s , Aoadcmic Press, N . Y . / ~ u n d o n 1970, pp. 92 - 95.
30. Bat? from the "pooling Project" i n the USA. Quoted from the Report of t h e Inter-Socie ty Commission f o r Heart Disea.se Resources: "Primary Preventton of Atherosclerot ic Disc‘-ses. " Circu la t ion 42 A 55 - A 95, 1970
31. HEADY, J . A . : Primary Prevention of Ischaemic Heart Disease - Cuuparatlve Trl ; l us ing Clof'ibrate. Design, Methods and Progress. WHO Bull . ( i n p ress ) (1972).

WHO ET/IRO card. vase ./5 ~ / P R V . M J . CARD. VSC . D I S / ~ ~ Annex X I 1 Psge x i i i
TABU3 1
PATHOLOGICAL FINDINGS I N SUDDEN DEATH
I N MEN AND W O N F S AG.ED 40-59 YEARS*
* Resul ts of WHO popula t~on- re la tea autopsy s t ud l e s I n Mam8, Prague 2, and Yalta.
$n t h i s study, sudden death was defined a s non-violent death occurring unexpectedly within 6 hours of t he onset of symptoms i n ,an apparently healtkgrperson o r i n a s ick person whose condition was s ta t ionary o r improving.
b IHD = Ischaemic herxt d i sease ( f r e sh myocardie.1 in fa rc t ion , o r scars , o r occlusions i n any coronary a r t e ry )
From : Wld. Htlh. Org. Techn. Rep. Ser., 1970, No. 441

EM/~ard. Vasc./5 EM/PRV. MJ . C-. vsc . D I S / ~ ~ Annex X I 1 '
Psge x iv
TARTX 2
FACTORS RELATEB -TO ATmOSCLEROSIS
AND ISCHAEMIC HEART DISEASE
Age and r ad ioac t i v i t y i n water Being e. B r i t i s h medical p r ac t i t i one r Blood group o ther than 0 Carbun ~l l su l f ide Carboxyhaemoglohin Cholesterol , e levated Chromium def ic iency Climate Coagulation disorders Diabetes, glucose tolerance ECG abnormalit ies Education Family h i s to ry , genetic f a c to r s Fc t in take, t o t a l Hsematocri t values Heart r a t e , r e s t i n g Heavy meals Hypertension Hypothyroidism, l a t e n t Income, l j ving standards Lipid f r ~ c t i o n s , serum l ipopro te ins Magnesium def ic iency Manganese def ic ienc:~ Nationel energy consumption Obesity, overweight Pectin consumption (p) Personal i ty type Physical a c t i v i t y (p) Polyunsaturated f a t t y acids {p) Respiratory impairment Saturated f a t s Sex Smoking S t r e s s Sugar in take Triglyceridaemia, elevated Uric ac id i n serum V~nadium def ic iency Water sof tness
p = pro tec t ive e f f e c t . - -_ . . . ___ _ _---
St rasse r , T.: WHO Chronicle (1972), -- 26, 7 - 11 .

WHO mo EM/~ard. Vasc./5 EM/PRv. M J . CARD. VSC . DIS/l7 Annex X I 1 Page xv
TABLE 3
SUMMARY OF SIGNIFICANT CORRELATIONS BEI'brEEN
D1ZTA.Y FACTORS AND CARDIOVASCULAR DISEASES
* Prevalence
46% 5-year incidence. F i r s t f igure r e f e r s t o $ deaths,
second f igure t o $ cases
From: Fejfar, Z. and M~sironi , R.: Dietary Factors and Cardio- vascular Diseases - E~idemiological Stud.ies i n Man. Proceedings of the 3rd Internat ional Congress of Food Science and Technology, Washington D.C., August 1970
I.A.P. = Internat ional Atherosclerosis Project.
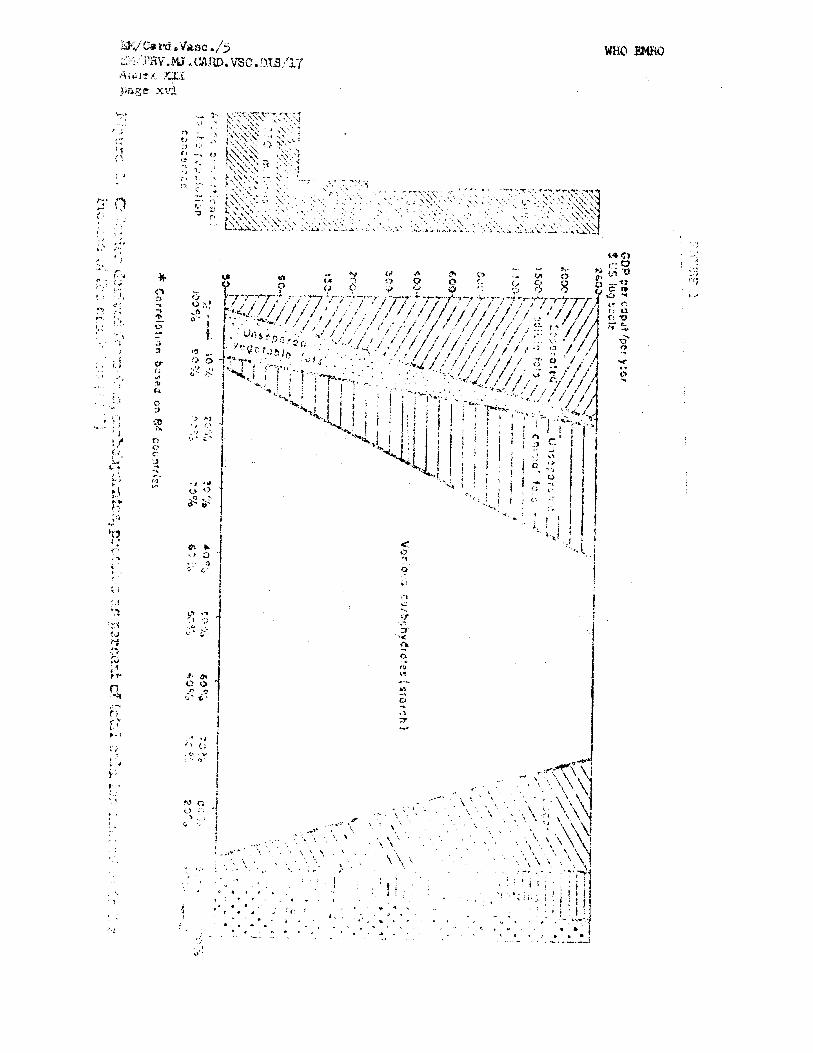


PROLCtNGATION OF LIFE iN YEARS, AT AGE 5. EXCLUDING WE CAUSES OF DEATH, 25 CQUNTRiES, 1967
ACCIDENTS Males Femalq
Mm\@m\- tlE/\RT DISEASES I I
I - , , , , , 1 2 s
0 1 2 3 4 5 6 7 8 9 1 0 Years
World Health ku, fkp, a. 430.439, 11172
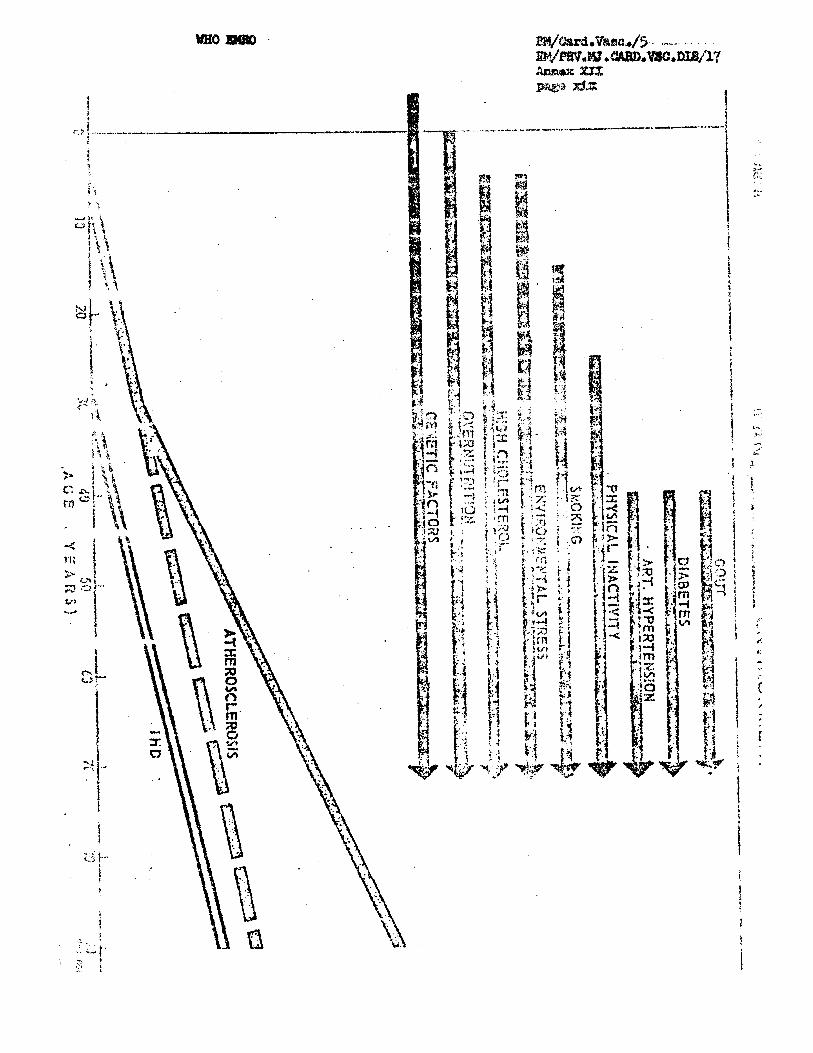

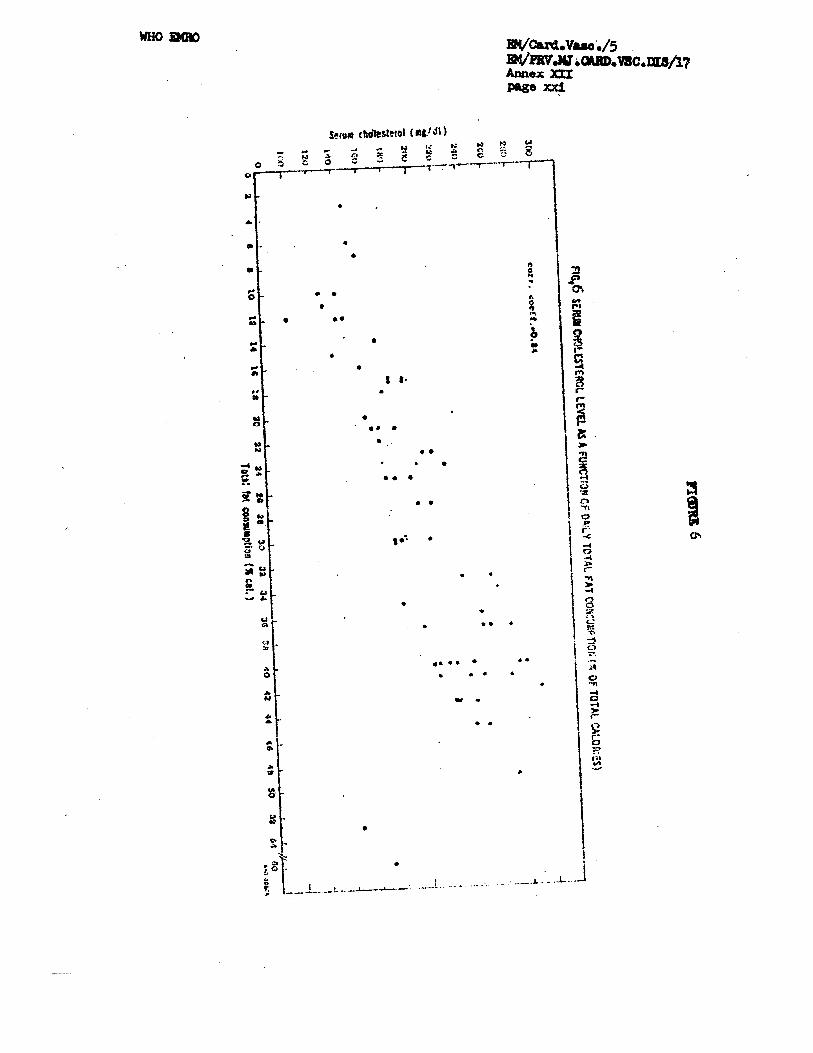

WHO m o EM/card .Vasc ,/5 EM/PRV.MJ .CARD.VSC.DIS/~~ knne:: XI11 page i
APPROACHES TO THE COMMUNITY CONTROL OF ISCHAEMlC HEART DISEASE - THEORY AND PRACTICE
Dr T. S t rasser Medical Officer, Cardiovascular Diseases Unit, FJHO/Headquarters
The control of a communicable disease is , i n theory, a simple task. It may suf f ice t o exterminate the gem, o r t o in te r rupt the chain of disease communication by k i l l i n g the vector, improving sani tat ion, immunization o r quarantine. Control of a mass deficiency disease ( s t i l l theore t ica l ly speaking) i s even simpler, a s shown by the example of the control of endemic goi te r ,
On the contrary, the control of ischaemic heart disease is over- whelmingly complex, even i n theory, Ischaemic hear t disease probably has a number of causes, and none of them is known. Neither e r e the pathogenetic mechanisms known, i n order t o allow intervention on the chain of events within the organism leading t o the disease. Furthermore, very of ten the disease i s diagnosed only when infarc t ion o r sudden death havc occurrcd - obviously too late. In fa rc t io rs arc vei-y often not even diagnosed: pathologists f ind many scars where no in fa rc t was found by the c l in ic ians (1). And, though i t may seem t o be a paradox, i n persons who died suddenly of ischaemic hear t disease, the pathologist cannot f ind an in fa rc t . How can, under such circumstances, control of a disease be aimed at?
It should be s ta ted a L orlce: r ~ u oorrryrellensivt: prugralmle for an e f f i c i e n t control of ischaemic hear t disease i s operating a s yet. But medicine seems t o be moving i n t h a t direct ion, and important advances i n per t inent research have been accomplished.
A possible "biographyw of an ischaemic hear t disease pat ient (Table 1 ) shows the various chapters i n the evolution of the disease; some of them l a s t f o r decades, others a r e measured i n minutes. In many cases, cer ta in chapters may be missing.
Little is known on gcnetic and prenatal influencca. Anatomical differences i n the coronary a r t e r i e s may ex i s t between some high and low incidence population groups i n the e a r l i e s t stages ( 2 ) a d the statement t ha t a r te r iosc le ros is may be a paediatric problem y3) has become a s o r t of slogan. Much population-based research i s needed, however, i n order t o a r r ive a t ;acts. On the other hand, the ear ly stages, the decades preceding c l i n i c a l disease were abundantly inves- t igated. his perlocl i s dominated by the concepts of ask factors ,
-
coronary proneness, and predic tab i l i ty of ischaemic hear t disease.

~M/Card.Vasc ./5 EM/PRV .MJ .CARD .VX .DIS/17 Annex XI11 page ii
WHO EMRO
The existefice of a prodromal s tage of the hear t a t tack with a variety of premonat ry symptcms has received a t ten t ion recently, "unstable angina "t47 being one of the manifestations. This stage m a y l a s t from some days t o a few weeks. The hear t a t tack i t s e l f occurs dramatically, withir- a fev min~ztes . This event - it may be the most important one i n t,he patie!itfs l iFe - has been well analyzed. The pa t ien t o r h i s fan i ly must, first of all, take a decision t o c a l l a doctor. Decision taking i s a complerc process i n i t s e l f (51, influenced by many factors . Much of rib& pre-hospital care can achieve depends on the decision t i m . The tica nf arrival 02 the doctor o r ambulance, t ransportat ion m d the speed of admission t o the coronary care unit may equally be of g r e ~ t impartance. M a n y pa t ien ts with ischaemic hea r t disease (70 per cent of those dying) never reach the hospi ta l and i ts coronary care u n ~ t ( 6 ~ 7 ) ~ An m d y s i s from Par i s showed a few years ago that the mean t i m s betwern onset of symptoms of myocardial t i o n and admission t o hospi tal ~zounted t o 23 hours 40 minutes tgfT- Only one o u t of a hundred cases of ird'arction reached the fiospltal I n l e s s than an hour!
Coronary care v--~Ats ?resent a major development i n the care of the acute stage of ischzrmic hear t disease. Reports are somewhat contru- versial : some authors found no change i n l a t e survival a f t e r coronary care (9310) , others reported outs tmding r e su l t s 9 . The l i t e r a l u r e on th l s t o p ~ c is very extensive; there i s no doubt concerning t h e immediate benefi ts of intensive coronary cae.
After t he attack, rehzbi l i ta t ion procedures should s t a r t a s soon a s possible (14). They d i f f e r wieely as regards the methods used; do the r e su l t s d i f f e r as well? Ths most successfu1 methods still have t o be determined (15 ) , Measurcs aimed a t diminishing the probability of re- infarct ion (seccnc;l=y prophylaxis) are essent ia l ly pa r t of the rehabi l i ta t ion proced~r-e; tl12f r t r ue value remains s t i l l t o be established with cer t i tude .
Most of the l i s t e d could be tackled and the control ofjschaemic hear t disease i n popul.,.-tions approached simultaneously, f r o m several direct ions, i n a systenztlcnl. way i f more knowledge were available. However, data should be b ~ s t d on populations, whole communities, not selected cases seen. b2 c z r t ~ i n physicims o r admitted t o hospi tals . A considerable number of such s t u s e s i s underway; preliminary r e su l t s from some are al.rea+j ava.ila3le.
I n an extensivd n3twork of tr~enty-two community-based reg is te rs , a WHO co-ordinated study ,161 has cnalyzed many features of acute ischaemic hear t disease, as it occurs i n populations. Data on al to- gether 8 912 pa t icn ts have been analyzed i n June 1972. Table 2 shows preliminary da ta on the incidence rate i n various poptllations and stresses once again the high r a t e s oi occurrence i n many of the C Q - O P ~ F ~ ~ ~ W centres*

WHO m o EM/~ard . ~ a s c ,/5 EI'~I/PFX.MJ.CARD.VSC .~1S/17 Annex XIII page iii
These figures should become the basis of planning the dimensions of control measures i n the respective communities. Figure 1 substantiates the ro le of the various time lapses before hospi tal admission. There is a grea t variety both i n the length and the s tructure of the onset-to- hospi tal delay. I n some places it may be eas i e r t o get t o a hospi tal (and t o be medically examined) by day than by night (Fig.2). Further da ta from the ischaemic heart disease r eg i s t e r study should a lso show whether, i n general, pat ients undergoing special rehabi l i ta t ion pro- cedures have a be t te r long-term prognosis p a n those who do not achieve such treatment. This question was discussed a t several WHO meetings, as well as the queationo of organiaing coronary care units and mobile coronary care units, t o speed up the delivery of qual if ied emergency care t o in fa rc t pat ients . A l l these measures belong, however, t o the "extinguisher" group, aiming a t l imit ing the severi ty of d isas te r , when it happens; s tudies are being conducted t o invest igate the methods and ef fec ts of interventions with the r i sk factors , i n to ta l communit e s before the manifestations of the disease. One of these s tudies h 7 j j done on 15 OW persons, co-orclmated by WHO, rn l l snow, whetner lowerlng the leve ls of serum cholesterol diminishes the hazards of developing ischaemic heart disease. This is a double blind t r i a l , and therefore no preliminary r e su l t s are available. "Multii'actor" studies, in te r - vening with smoking, hypertension, obesity, are also underway i n several places, e.g. London, Gtjteborg, B e l s , Ghent; t h e i r methodology has been discussed a t a WJ30 meeting r8f. Though methodological problems are d i f f i c u l t , a study of the protective e f f ec t of physical ac t iv i ty i s being planned i n the United States.
What could be done f o r t h e control of ischaemic heart disease? In theory, when present day assumptions are corroborated by fac ts , planned, designed action should be undertaken. It seems plausible t h a t while Ignoring the causes and mechanisms of ischaemic heart disease i n the early stages, t he "risk factors" should be attacked. Not all of them are l i ab le t o intervention. Though a correlat ion f i s c e m i c hear t disease with the l iv ing standard was demonstrated ? l g r a ? , it would be ra ther impracticable t o s t a r t preventing ischaemic hear t disease by lowering the standards of l iving. On the other hand, even the appa- ren t ly simplest changes, l i k e dropping the habit of c igare t te smoking o r changing the d i e t are wellknownto present i n pract ice tremendous d i f f i - cu l t ies , because they arepar t of firmly established soc ia l and behavioural patterns. There seems 'to be no easy w a y t o accomplish such changes; they reuuire long-term heal th education of en t i r e ~ o ~ y l a t i o n s , and also of the medical corps. I n this respect, much depends on how strong the evidence i s demonstrating the usefulness of such measures, and the involve- ment of the medical pro2ession may swing from a half-hearted support t o enthusiasm, i r " the current p i l o t programmes of intervention with r i s k fac tors turn out t o be convincingly useful.

EM& ard . Vasc ./5 EM/PRV.MJ .CARD .VSC .DIS/17 Annex XI11 page i v
WHO EMRO
I n the prodromal stage, probably much could be done f o r subjects who &ready had an infarc t ion and are experiencing the premonitory signs of a re- infarct ion (21). The ear ly care f o r t he acute coronary suspect has received great a t ten t ion recently (22), t he ways i n which an impending infarc t ion w i l l be mslaged depend considerably on the awareness of t he physicians and on co-operation from the public. The concept of pre- coronary care (7) has been put forward with an emphasis on se l f - r e f e r r a l of subjects who have been taught how t o recognize t h e i r own prodromal symptoms, linked with e f f i c i en t , specialized medical services, ambulatory t r i a g e and proposed Myocardial I n f a ~ c t i o n Detection Points (MIDI" s ) (22) have a de f ln l t e appeal f o r .certain cultures; it may have, however, a strong appeal t o neurotics i n some other cultures.
For instructed, selectedo highest r i s k pa t ien ts se l f -a id i n j ec t io s of l ignocain were suggested as a f i r s t - a i d prophylaxis of arrhythmias ?23 1 Mobile coronary c a r e units are great ly a question of l o g i s t i c s (24). Even the best equipped mobile u n i t s are helpless and useless i f they cannot reach a pa t ien t because of a t r a f f i c jam, and they are of l i t t l e use, i .a., i f a c i t y has no adequate telephone network so that a c a l l can be made by anybody immediately. Star t ing with recognizing t h e symptoms and taking the decision t o put through a c a l l , there is a whole chain of dramatic actions i n an attack. A mobile un i t is ju s t one l i n k , and the s t rength oL̂ the chain depends, qui te natural ly , on the we&sst l ink . A great majorlty of early sudden deaths by aou-t;e isohaemio hear t disease occurs prac t ica l ly instantaneously; mobile units- would add l i t t l e t o the care of such cases (23). - 1
The organization and &equate function of coronary care un i t s i s also t o a considerable extent a question oZ log i s t i c s . For operatio~nal reasons, one ten-bed uni 9 be of as much use t o a community as four units of five beds eaoh f208: Unit. should m e e t certain standards I n staff, -equipment and organization (27), and there should be ways of eva- luat ing t h e i r functions. Similarly, rehabi l i ta t ion procedures and pro- grammes should be evaluated regarding t h e i r effectiveness (151, in s p i t e of the f a c t t h a t very high economic e f f ec t s of rehabi l i ta t ion were com- puted (28).
A l l these measures f o r the control of ischaemic hear t disease need a systematical, planned, desi~med, approach: they ,need t o be formulated i n a programme. There seems t o be l i t t l e chance of achieving a notice- able i m p a c t an the disease unless, very muoh ac i n communicable diseases, t o t a l populations o r population groups are covered. Eehaviour , f o r example, i s i n a cer ta in sense a conununicable condition, and i f a pro- gramme i s t o include action against smolcing, fau l ty eat ing habi t s and physical inac t iv i ty , i t s h o u l d cover en t i r e population groups, l i k e mass vaccination. The same applies t o h e a education, f o r misbeliefs are also communicable. Operational measures, such as ~ r g a n i z a t i o n of coronary

WHO EMRO EM/~ard .Vase ./5 EM/PHv .MJ .CARD .VSC .DIS/17 Annex a11 page v
care and of an emergency system should be community based by desini t ion, and no evaluation i s possible unless population-based da t a on the disease and i t s trends are available; the ischmnic hear t disease r eg i s t e r s should thus continue t o give guidmcz t o CC~%:~I~. programmes.
Like any other coiitr,l. prcgrmir.s, ischaemic h z w t disease programmes should be placed i n t o tho riglit ca?taxt. They ars obviously not a s e l f -contained z i m . H*ypei-ti.~sicn is, fop example, an important r i s k f ac to r i n ischaemic heart disoczse. Thcua there is no evidence as ye t t ha t treatment of hyporternion rii.itig,?;tes the r i s k of ischaemic hear t disease, it Cerct;amly does low? the lncideice of complications of hy-rtension, such as s.troke, hypertersive heapt o r rena l disease. =ere are thus close connections ba'cv~een a kjpertension and an ischaemic hear t disease control progresne .. Similarly, anti-smoking propaganda i s - .. p& of an ischaemic hear t disezse prevention programme, but it i s pert inent a lso t o t h e prevention of cnronic bronchi t is and pulmonary hear t disease, and lung cancer as v:ell, It is important t o conceive an -ischaemic hear t disease cornmmity control programme as pa r t of a -i system of chronic disease control, i n which various programmes do not I
compete f o r funds, manpower 2nd the public, but a re promoting each other.
Such a system can be br l i l t up gr;?dualLy,by s t a r t i n g with one communityl control programme, and adding t o it. another and s t i l l another, aiming at a comprehensive approach to the control of non-communicable diseases ' i n populations.
There is, however, a long ney t o go. A t t he present, i n practice, (Table 3) the immediate approach t o the community control of ischaemic hea r t disease should, li-rst of al.1, ~ i r n a t rroliable and comprehensive inrormation on the disea.se and i t s przscnt mariagement i n the comunity. The ischaemic heart diaeaae r e g i a t w s aerve t h i s purpose. They give a good assessment of the s i t u ~ t i o n i n the cornunit> o r area which they cover. It is expected t h a t the r eg i s t e r s r.rill Iso be a useful t oo l f o r continuous evaluation of action mdert6k?n f o r the c o i ~ t r o l o? ischaemic hear t disease. These should take place sirfiul t sousl sly on several l eve ls . The "~xt inguisher" services should be male e f f i c i e n t , smoothly operztive and comprehensive f o r the whole community. Effofd shou1.d bc invested in to lay-medical education of high-risk parsons ;end ischaem3.c hear t disease pat ients , and t h e i r family members, Hwl th ~ d ~ : c ~ + , i o n of the general public should I
receive at tent ion, s t a r t i ng z t a?. ez.rly age. Education being fodunatelyi , a le0 a communicable condition, th:: CUzc,chcr~ should bc educated first, and good physickns should be good teachers, too.

EM/Card.vasc ./5 EM/FW. M J .CARD .VSC . D I S / ~ ~ Annex XI11 Page vi
WHO EMRO
T m 1
THE LIFE HISrORY OF AN ISCWlEMIC HEART DISEASE PATIENT
N.B. In persons dying suddenly some of the chaptei-s are n i i s s i n g .
Main Events
Prenatal influences
Incipient anatomical lesions.
Advancing lesions
Premonitory symptoms
Calling the doctor Transportation Admission
Monito rjxs Reanimation
Aehabi Li t a t i on
11 secondary" prevention
Chapter C
Heritage ,
Early stages
I
Latent CHD
Prodromal stage
Attack
'Acute stage
f
Convdesoenoe . Return t o society
Re-inf arction
Death
Duration
?
Decades
Years
Days
Minutes
DEW
Weeltc
Months-years

WHO m o EM/card.vasc ./5 EM/PRV.W.CARD.VSC .DIS/17 Annex XI11 page v i i
ACUm ISCHAEMIC HEART DISEASE: INCIDENCE RATE (PEFi 1 000 POPULATION)
PER ANNUMBY 23%. AGE 20-44 YEARS
Centre Male Female
G'dteborg
Prague
Budapest
Dublin
Helsinki
London
N i jmegen
Tampere
Warsaw
Lublin
Innsbmck
Kaunas
Boden
Sofia - -
Perth
Tel Aviv
Both sexes
0.8
0 97
1 .O
1.2
1.G
1.4
1 *3
1 .O
1 .O
0 -5
0.6
0.4
1.6
0.2
1,4
1 e 5
I
3.2
3.7
3 *5
4.2
5 -9
4.9
4.2
5 00
2 07
2.2
2.4
2 .O
5 -3
1.4
4 *7
4 *3
2.0
2.1
2.2
2.6
3 -5
3.2
2 07
2.8
1.8
1.3
1.5
1.1
3-4
o .8
3 -0
2.9

EM/c ard . as c . /5 W P R V .MJ .CARD .VSC .DI s/17 Annex XI11 page viii
WHO EMRO
T m 3 -- ACTION IN VARIOUS STATES OF ISCHAEMIC HEART DISEASE
Chapter
Heritage
Early stages
Latent CHD
Prodromal st age
Duration
I !
- - _ ?
Decades
Years
1 Attack
Acute stage
Convalescence
Return t o society
H e a 1 t
I Re-inf arction
Death
R e s e a r c h
I
h
E d u c a t i o n
Dws
Minutes
UWS
Weeks
Months-years
s e r v i c e s
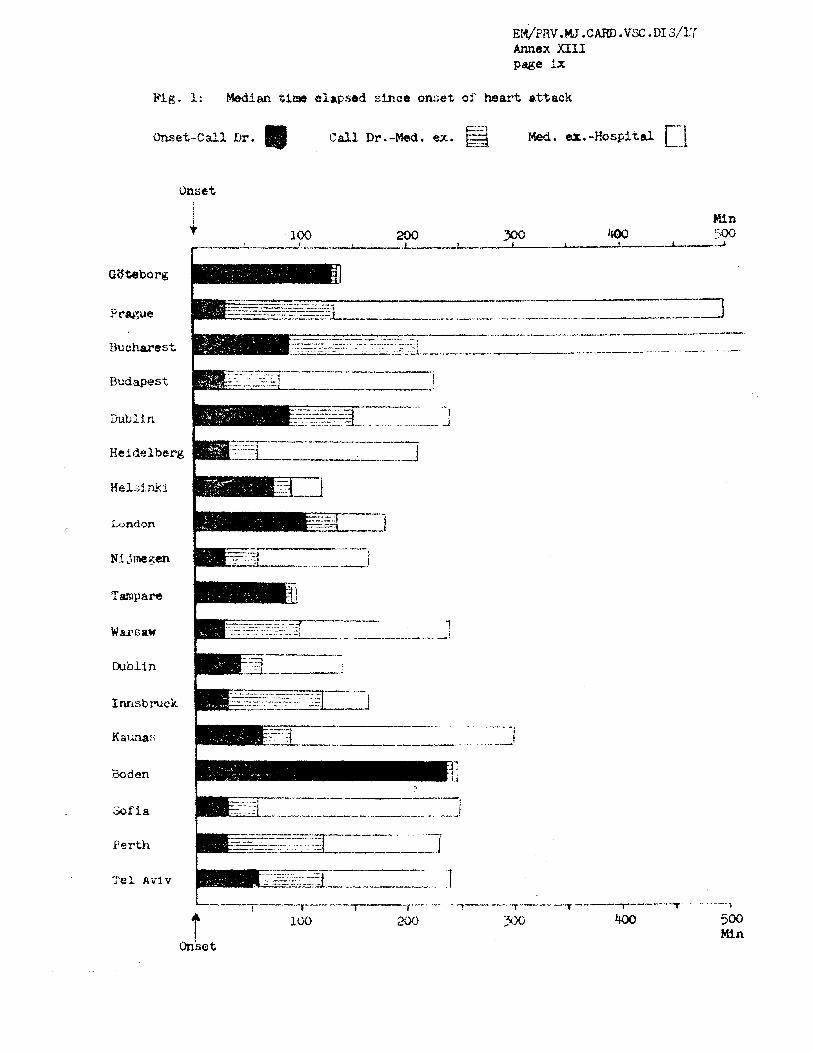
Fig, 2 : Metdim t i m e elapsed since onset of heart ettack
Onset
-------. -,-- .-
Prague - ,,--.--. .- .-- . ..--...-..--.---. -"-7 - . - . - -
Bucharest .- -~---
Budapest
fmblin
Heidelberg
Helslniii
L~ndon
Pli jm~gen
T m p m
r---1-.---- -.- -. -.-T ------ -.-.-,----.-- 1
t loo m 400 500 Min
Onset

-.* ---. -.-. = w r u w - . u a , . l J l i r / & ! -abb?
&wax =If page u MoaZm tiu elapsed s m s onsect of attack
f w s u r day night ----.-. . f
Sublin day night
WHO EMRO EM/~ard .Vasc ./5 EM/PIIV.MJ .CARD .VSC .D1S/17 Annex XI11 page xi
1. Edwards, J.E. The value and limitations of necropsy studies i n coronary artery disease. Prog. Cardiovasc. Res. 2: 309-323, 1971
2. Vlodaver, 2; K&, H; Neufeld, H. The coronary ar ter ies i n early l i f e i n three Lifferent ethnic groups. Circulation 2: 541, 1969
3. Epstein, F.H. International trends i n coronary heart disease epidemiology. Annals of Clin ica l Researah, 2, No.6, 293-299, 1971
4 Fulton, M. e t a l . Natural history of unstable angina. Lancet 1:860, 1972-- -
5. Goldstein, S. e t al. Fac$rs affecting decision t o seek medical -- help af ter acute myocardial infarction. Circulation 39/40 : S~PP~-3, P-93, 1969
6. .Lorn, B. e t al. Coronary and precoronary care. Am.J.Med. 46:705-724, 1969 -
7. Lown, B., Rubeman, W. The concept of precoronary care. Modern Concepts of Cardiovascular Disease, 2 ~ 9 7 , 1970
8. Bouvrain, Y; Puel, D. D Q l a i s d 'hospitalisation des infarctus r6cents. [email protected] 3:1969, 1971
9. Insacsson, S.O. -- e t - al. A review of 191 patients with myocardial infarction treated i n a Swedish coronary care unit. Acta Med. Scand. 185: 545-552, 1969
LO. Saslaw, M.S. Coronary Care Units: One hundred day evaluation. Angiology 23:372-376, 1972
11. Linko, E- e t a l . Intensive care of myocardial infarction. A two-year experience w i t h 329 patients. Acta Med. Scand. 187: 117, ~ 9 7 0
12. McNamee, B.T. -- e t a l . Long-term prognosis following ventricular f ib r i l l a t ion i n acute ischaemic heart disease. Brit .Med.J. 3: 204-X)6, 1970
13. Lemire, J. and Johnson, A. Is cardiac resuscitation worthwhile? New Engl . J. Med. - 286: 970, 1972
14. WHO Regional Office f o r Europe. A programme for the physical rehabilitation of patients w i t h acute myocardial infarction: Prep-d by a working group. Freiburg i m Breisg.au, 1968. Copenhagen, 1968

EM/C ard .Vasc ./5 EM/PRV .MJ .CARD .vsc . DI s,f17 Annex XCII page x i i
WHO EMRO
15. WHO Regional Off ice for Europe. Evaluation of rehabll l ta t lon programmes f o r pat ients with myocardial infarction; report of a working group, Bordeaux. Copenhagen, 1971
6 WHO Regional Office f o r Ekrope . Ischaemic heart disease ~ g i s t e r s ; report of the f i f t h working group, Copenhagen. Copenhagen, 1971
17. Heady, J.A. Primary prevention of ischaemic hear t disease: Co-operative trial using clofibrate . Bull .Wld.Hlth.Org. ( in press)
18. WHO Regional Office f o r Europe. Methodology of multifactor preventive t r i a l s i n ischaemic heart disease: report of a working group, Rome. Copenhagen, 1971
19. Brmfinner, P. Coronary heart disease and the l iv ing standard. Acta Med . Sc and. a: 523-527, 1967
2 Masironi, R. Dietary factors and coronary heart disease. Bull. Wld.Hlth.Org., - 42: 103-114, 1970
21. WHO Regional Office f o r Europe. The prodromal symptoms of myocardial infarct ion and sudden death: report of a working group, Copenhagen. Copenhagen, 1971
22. Early care f o r the acute coronary suspect. Bethesda Conference Report. Am.J,Cardiol. - 23:603-618, 1969
23. Bondurant, S. Problems of the prehospital phase of acute myocardial infarction. Arner. J .Cardiol. - 24: 612, 1969
24. WKO Regional Office f o r Europe. The role of mobile coronary care unitis: report of a working group, Moscow. Copenhagen, 1970
25. Wykland, B. Medically unattended f a t a l cases of ischaemic heart . ,
disease i n a defined population. Acta.Med. Scand., Supp1.524, 1971
26. Sady, L. e t a l . New epidemiological methods f o r coronary units. Circulation 39/40, suppl. 3, p.54, 1969
27. WHO Regional Offlce f o r Euro~e . The organization of oomnary care units; report of a preparatory meeting, Copenhagen. Copenhagen, 1959
28. Helander, E. Economic aspects of the ' rehabil i ta t ion of pat ients with cardiovascular diseases. Acta Cardiol . , suppl .XTV, 52, 1970

WHO EMRO EFI/card ,Vast ./5 F3l/PRV. iW . CkRD . vsc . D I S / ~ ~ Anne:: XIV page i
ANNE;: XIV ORGANIZATIOI\T OF CARDIOVASCULAR SERVICXS
IN CZ?!fERAL HOSPITALS
D r D. Verdugo Bininel is Regional Adviser on Orgailixation of Medical Care, WHO-EMR
I INTRODUCTION
The rate of change tha t hospi tals havc undcrgonc i n ~ C E E than 8 generation does not show sigcs o f dimi!{ishing. Most changes r e f l e c t technological and sc i en t i f i c advances a s wel l a s new cu l tu ra l and demographic trends.
The rapid increase i n medical science and technology makes it no longer possible f o r any physician e i t h e r t o master a l l new techniques o r t o cover a l l f 'ields or c i inxcal mealclne. m e lncreaslng coniplexlty of medicine has led t o a rapid development i n medical special izat ion and the concentration of many a c t i v i t i e s at/or near thc hospi tal .
There i s a l so a growing a>Jarencss among the public t h a t adequate heal th care const i tutes n basic human r igh t (7) and not a privilege, which has encouraged an increase i n the demand f o r such services. A t the same time there have been important demographic changes. There is a s h i f t i n the age d is t r ibu t ion of the population due t o two main factors: the steady decline of the b i r t h ra te , which has been d~amat i c i n developed countries and the trend of m o r t ~ l i t y during the l a s t one hundred years which has shown a marked reduction of mortality i n ear ly l i f e , considerable i n middlc l i f e and only moderate i n 3-ate l i f e . This means t h a t re la t ive ly more people wirvive i.nt.0 mi ddlc o r l a t e l i f e , ages where there is normally a higher prevalence of card iov~sculnr diseases.
New cul tura l trends? l i k e the r?se of modern t ransportat ion which leads t o sedentariness, prolonged excessive mental s t r a i n of modern l i f e i n overcrowded c i t i e s , fa t - r ich d i e t s , e tc . , a re a l l fac tors which play a par t i n the high r a t e s of morbfdlty and mortality from cardiovascular diseases. These fac tors can and should be controlled with adequate preventive programmes. Tmse Yacts make the organization of cardiovas- cu lar services an urgent nccd i n n?in general hospi ta l s ,
It i s necessary t o point out t ha t the degree t o which the c l i n i c a l work of the hospi tal i s departmentalized i s dete-mined ahlost en t i r e ly by the extent of special izat ion of the medical s t a f f . A s a minimum, however, a general hospi tal should comprise four basic departments that can cover prac t ica l ly a l l the spec ia l i t i es , t ha t is, gcncral mcdicine, gcncral surgery, gynaccology and obs te t r ics and pacdiatrics. I n the

EM/Card.Vasc ./5 EM/PRV.l'U. CARD.VSC.DIS/~~ Annex X I V page ii
WHO EMRO
szall hofipital this w i l l probably be the fl111 cxt.r?nt oi div i s ion i n t o c l i n i c a l departments, but a s t h e h o s p i t a l incrcasks in s i z c and the medical s t a f f becomes marc spec ia l i zed o ther dcpartments . i i i l l be added.
The span of cardiovascular s ~ r v i c e s i n general h o s p i t a l s ranges from tho onc extreme where a doctor interested i n cardiovascular d i seases puts as ide some beds f o r carcliovasculsr p a t i e n t s having a t h i s d isposal ECG equipment, t o t h e o ther uiklerc a complex, sophisticatccl? department i s developed with equipment f o r monitoi-ing pa t i en t s , cardiac ca the te r iza - t i o n , s p e c i a l coronary cnre u n i t s , e t c .
Succoss of any spec ia l i zed se rv ice depends more on thc effect iveness , s k i l l and experience o f Its doctors, nurses and a u x i l i a r y personnel and t h e i r work, than on i t s equipment.
2. ADMllJISTRATIVE ORGANIZATION OF A CARDIOVASCULAR SERVICE
2.1 ~ ~ a r l i z a t i o n uf EIospi tals
The organization of h o s p i t a l s and t h e i r administrative p a t t e r n s very i n d i f f e r e n t coun t r i es but t h e r c a r e some basic p r inc ip les t h a t apply t o most of them.
A h o s p i t a l cannot be thought of a s a s i n g l e i n s t i t u t i o n but a s a network of h o s p i t a l s i n given arens. A s a r e s u l t , u I-egiurral approach t o h o s p i t a l se rv ices has developed (10). Subject GO t h i s p r inc ip le Regional Boards o r Regional Directors a r e responsiblu f o r planning, co- ordinat ing and supervis ing regional group of h o s p i t a l s . A t t h e l c v e l of t h e ind iv idua l hospita!. the adminis t ra t ive s t r u c t u r e i s determined mainly by i t s s i z e . The funct ion of t h e Director of t h e h o s p i t a l i s t o direct, sugervise and co-ordinatc t h e work of t h e v2rious departments, 2nd t o a c t a s a c h ~ n n e l of information between the h o s p i t a l s t a f f and the rcgional au thor i ty .
2.2 Organization of Departments
Under the Di rec to r of t h e h o s p i t a l comes t h e heterogeneous group of Heads of Departments vrho a r e responsible t o t h e Director f o r t h e work i n t h e i r respect ive f i e l d . Ench incdical department hns a c e r t a i n degree of zutonomy 2nd i t i s organized according t o i t s particul2.r ixnct ion.
2.3 Organization of spec ia l i zed se rv ices
A s t h e s i z e of t h e mcdical s t a f f inc reases and t h e doctors become more spec ia l i zed o ther u n i t s , wi thin t h e department, sllould be developed. A Head of Service repor t ing d i r e c t l j t o t h e Head o f Department, from whom he receives delegated au thor i ty , should be i n charge of each u n i t . T h i s subdivision permits exercise of au thor i ty and con t ro l wi th more

WHO EMRO FN/~ard .Vase ./5 EM/PRv. i'4J . CARD .VSC. D I S / ~ ~ Annex XIV page iii
specialized competence. The number of doctors, nurses 2nd auxi l iary personnel within each of these specialized services w i l l depend on the s i ze and functions of the uni t .
l3ascd on these considerations i t is easy t o visual ize the organiza- t i ona l s t ructure of the hospi tal a s a pyramid where authority i s delega- ted f r o m top t o bottom becoming smaller a t each successive level .
A cardiovascular service cons t i tu tes one of these specialized uni t s , within the Department of In te rna l medicine. Its organizational s t ruc ture w i l l depend on i ts s i ze and the services provided.
3 . TECHNICAL ORGANIZATION OF A CARDIOVASCULAR SERVICE
The technical organization of a cardiovascular scrvice should always s t a r t with an objective study of the actual need and i t s ju s t i f i ca t ion i n terms of ava i l ab i l i t y oi" professional s k i l l s and supportive elements su f f i c i en t t o warrant the investment and support the decision to es tab l i sh the new f a c i l i t y .
In the technical or~;aniz@tion of a cardiovascular service an analysis w i l l be made of the following:
3.1 Nursing u n i t ; 3.2 Cardiac catheter izat ion and ~~ngiocardiography; 3.3 Coronary care uni t ; 3.4 Mobile coronary care uni t ; 3.5 Pacdiatric cardiovascular service; 3.6 Cardiovascular surgical u n i t ; 3.7 Exercise t e s t s un i t ; 5.8 RehaDilltatlon se rv loos fur C.V. p a t i e n t o ; 3.9 Out-patient department; 3.10 Home care programmes; and 3.11 Co-ordination and cardiovascular services.
3.1 Nursing Unit
The ward o r nursing u n i t f o r cardiovascular pat ients does not d i f f e r from any general ward. I n sp i t e of the variat ion i n design of wards, there a r c s t i l l many hospi ta l s i n countries of t h i s Rcgion whose wards Lire Wlc: t r a d i t i o n a l large r o o m a c c o m m o d a t i w twenty t n f n r t y pat ients , usually along each side with a spaco between the beds down the centre, being known a s the "~ igh t inga le" type of nursing uni t . This system f a c i l i t a t e s observation and nursing at tent ion, but has the draw-back, among others, of lack of privacy. This has l e d t o the construction of smaller wards, 4, 8 and LO beds, t ha t provide mom privacy and more f l e x i b i l i t y i n t h e i r use.
EM/~ard .Vast . /5 EM/PRV.NJ. CARD .mc. D I S / ~ ~ Annex XIV page i v
WHO EMRO
Any of these types of nursing un i t s mag perrom the mnctlons f o r a cardiovascular service, i f basic f a c i l i t i e s a r e avai lable (props, sockets f o r electrical equipment, e tc . ) .
Nevertheless the nursing u n i t s a r e not the most important considera- t ion i n the se t t i ng up of a cardiovascular service s incc Llicy do not d i f f e r from other wards. The most important elemcnts t o be considered a r e those re la ted t o special procedures i n the spec ia l i ty which a rc analyzed below,
(a ) Basis f o r t h i s u n i t
Cardiac catheterization and angiocardiography are inseparably wedded i n t h e modern diagnostic laboratory (2) sincc they are increasingly mutually complementary.
Cardiac roentgenology has becomc a t rue sub-speciality such a s roentgenology using special techniques l i k e cinefluorography with image-amplifier screen, venous angiocardiography, select ive angio- cardiography, e tc . A carvliovascular service nceds i t s own equipment f o r these procedures.
(b) Design
While space f o r radiology i n general h2s tcndcd t o increase during the past two decades, space requirements f o r any of the specialized s tudies a r e considerably above the average. An area of a t l e a s t 56 m2 (7x8 m) is suggested since the number of persons involved i n tho procedures can become consicl(~mh1c. There i s a l so the problem of the pa t i en t ' s bed ( ra ther than a s t re tcher ) , as well a s the number of pieces of equipment on wheels: s t e r i l e tmys , car t s , e tc .
Whenever possible the u n i t should be ins tn l lcd i n a room not f a r from the CCU i n view of the possiblc need Por resuscitator equipment during investigations, and the poss ib i l i ty of using the equipment f o r the inser t ion of pacemaking electrodes where there i s no portable X-ray machine with an image i n t e n s i f i e r f o r the CCU,
Ad~acent t o tkc cardiac catheter izst ion space, a working area o f a t l e a s t 12 rn2 fo r haemodynamic laboratory i s 2 must. A storage o r instrument room i n communication with the pr incipal room is desirable a s well a s cleaning f a c i l i t i e s f o r the maintenance of equipnent .

WHO EMRO EM/Cai?d .Vast ,/5 EM/PRV. 1.U . CARD. VSC . DIS/17 Annex XIV pagc v
( c ) Equipnent
The basic equipment of t h e u n i t is the examination t a b l e a t which t h e doctor works wi th t h e pa t i en t , thc X-ray generator and the X-ray tube. The components t o complement t h e equipment f o r the advanced examination procedures, a s i n ccrdiovascular radiology, a r e : image i n t e n s i f i e r s , cameras f o r c i n e f l ~ ~ o r o g r a p h y and 70 mrn fluorography, f ih chcttlgers , More soph is t i ca ted i n s t a l l a t i o n s will a l s o include t e l e v i s i o n chains and vidco-tape recoi-clers . Other necessary equipment are: high pressure i n j e c t o r s , devices f o r measuring, recoraing om3 dlsplaylng physlologlcnl Cia t3 Lr1cluLUru instruments for blood gas analyses. The t o t a l cq~~ipment of the u n i t should c o n s t i t u t e a f i l l y i n t e g r a t e d f l e x i b l e system based on compatible components. Thc system can be extcndod by adding more components t o provide f a c i l i t i e s f o r more complex examinations l i k e bi-plane examination techniques e t c .
S t a f f - An adequately t r a i n e d c a r d i o l o g i s t shoulc!. be i n charge of t h i s
u n i t . A nurse,an X-ray technic ian and a laboratory technic ian should i d e a l l y complement t h e s t a f f of this u n i t .
7 - 1 . 5 Coronarv Care U n i t (CCLJ)
, a Basis of t h i s u n i t
A study of the n a t u r a l h i s t o r y of p a t i o n t s wi th acute myocardial i n f a r c t i o n shows t h a t they a r e associa ted e a r l y i n t h e course of ill- ness wi th l i f e threatening arrhythmias which, iL̂ de-tected, a r e t r e a t a b l e . For theso p a t i e n t s there is a very high mor ta l i ty m t c on t h e f i r s t day of h o s p i t a l i z a t i o n and a decreasing mor ta l i ty r a t e on t h e subsequent drys. I f they can survive the f i r s t few days then t h e outlook i s reasonably good.
With reference t o the th ree p r inc ipa l complications which a r e t r e a t a b l e , t h e ranges of occurrence and mor ta l i ty reported i n various stuciies a r e (13) :
Occurrence $
Arrhythmias 13 t o 41 Cerdiogenic shock 11 t o 21 Congestive h e a r t f a i l u r e 16 t o 71
Morta l i ty $
It i s i n the a rea of arrhythmias t h a t t h e greatest hope f o r therapy l i e s a t the present time and i t i s on t h i s concept t h a t t h e coronary cam u n i t has evolved.

EM/Carcl .Vasc ./5 EM/PRV.MJ. CARD.VSC.DIS/~~ Annex XIV pago vi
(b) Design
From t h e point of view of workload a h o s p i t a l wi th 200 o r more beds and with morc: than 100 acute myocardial i n f a r c t i o n a h i s s i o n s pe r year may be j u s t i f i e d i n es tab l i sh ing c separate CCU u n i t , sub jec t t o adequate personnel and se rv ices .
For some small h o s p i t a l s i t may be advisable t o have a "Coronary- In tens ive ca re u n i t s ' under one s i n g l e u n i t . (14)
The rectangular rooms common t o most h o s p i t a l s a r e q u l t e s u i t a b l e f o r CCU allowing f o r reasonable reaal'aticn.
( i ) The CCU shculd be loca tad a s c losc a s poss ible t o the emergency admitt ing a rea and t o a medical o r c~~rc '~iovascu1ar ward t o f a c i l i t a t e rapid mobilization of appropr ia te personnel and equipment. It should a l s o be c lose t o t h i X-ray u n i t o f the cardiovascular service.
( i i ) The area around t h e p a t i e n t ' s bed should provide easy a c c e s s i b i l i t y and adequatt space f o r both rou t ine and emergency p a t i e n t ca re (around 1 2 t o 1 4 m2 ror each bed).
( i i i ) The c e n t r a l nursing stntinn 2 n d work nrcn should be loca ted so a s t o permit d i r e c t v i sua l observation o; a l l p a t i e n t s , (40 t o 55 m2 f o r t h i s a rea ) .
( i v ) The surroundings should be cheerful and t r a n q u i l (sound- proofed c e i l i n g s an? f l o o r coverings).
( v ) Emer-gency e l v c t l i c power sources must be provided. Satici- fac to ry provision should be made f o r adequate electrical c i r c u i t s wi th the necessary voltage f o r mounting and connecting equipment (adequate grounding ancl no e l s c t r i c in te r fe rence problems) .
( v i ) Provision should bc made f o r the following cdd i t iona l rooms adjacent t o tho CCU: physic ian 's consul-tation and s leeping room, lounge PO? nursing personnel, and z i m i l y wai t ing room. It is highly des i rab le t o have ava i l ab le ?, proc~clure room i n which mch tcchniqucc 2s pnccmakor o1oo t ro . l~ i n s o r t i o n and e l e c t r i c shock therapy can be applied.
( v i i ) A s f z r a s poss ible beds should be separated by p a r t i t i o n s t o prevent p a t i e n t s from being aware of the problems of t h e i r neighbours .
WHO EPmo ~ 4 / ~ a r d .Vasc ./5 EM/PRV .MJ . CARD .VSC . ~1S/17 Annex XIV page v i i
( v i i i ) Adequate a i r conditioning f o r the sake of pa t ien ts should be provided t o control temperature and humidity i n the presence of constant equipment operation.
(ix) Two-way intercoms a re highly desirable.
(c) Equipment
The essence of t he CCU is continuous electrocardiography and t rained observation f o r "aggressive management of cardiac arrkgrth- mias" ( 5 ) . The baslc equipment t o ensure sa t i s fac tory f'unction is:
( i ) Each bed must have a cardiac monitor with oscilloscope t o monitor the ECG. A simplified lead system w i t h adhesive chest electrodes leaves the limbs f r e e t o allow the pat ient t o move more f ree ly i n bed, diminishing the hazard of thrombosis (3). A pulse r a t e meter and alarm a re e s sen t i a l adjuncts t o the monitor. (For psychological reasons it is desirable t h a t monitoring should be kept out of immediate vision of the pa t ien ts ) .
( i i ) Each bed should be provided with i t s own oxygen out le t , suction equipment, overhead l i g h t , and intravenous stand.
(iii) Beds musk be of a type which permit the ragid apglication of resusci ta t ion techniques (8).
( i v ) Each bed should be provided with a bedboard t o give firm support of the thorax during cardiac compression.
(v) Each CCU should have a t l e a s t two e l e c t r i c de f ib r i l l a to r s , w h i c h ie thc moet important therapeutio tool in the unit (5).
(vi) The other two e l e c t r i c a l therapeutic tools i n l i fe- threatening arrhythmias a r e the "cardioverter" and the "e lec t r ic pacemakerst' ( a t l e a s t two "demand" type pacemakers with a good. supply of catheter pacemakers). The equipment and par t icu lar ly the s k i l l to use them should be available.
( v i i ) Equipment f o r endotracheal intubation and posi t ive pressure vent i la t ion should a l so be standard equipment i n CCU.
( v i i i ) A portable electrocardiograph which should be the sole property of the u n i t f o r recording da i ly standard electi-ocardiograms.
( i x ) A portable X-ray machine with an image i n t e n s i f i e r ( fo r the inser t ion of pacemaking electrodes).
EM/~ard .Vasc ./5 DI/PRV.W . CARD, VS c . D I s / ~ ~ Annex XLV page v i i i
WHO m o
(x) A resusci ta t ion ca r t , mobile c a r t stocked with accessible medicine and equipment.
(x i ) Miscellaneous : Stethoscopes, tourniquets, blood pressure cuff's, e tc .
(d) Additional equipment
(i ) Central monitoring consoles o r "slave" oscilloscopes mounted on a cent ra l panrr2 a t the nursing s t a t i on a re very useful (they must not replace "eyeball monitoring" which 2s by f a r thc most important). I f l e s s than four- pat ients a r e monitored these slave oscilloscopes a r e probably not necessary (5).
(ii) A mechanical chest compressor f o r cardiac massage (more e f fec t ive than the arms of the physician o r nurse and l e s s t i r i n g ) .
(e) Staf f
The s t a f f of the coronary care u n i t should include:
(i) Medical Mrec t o r . A card3 01 ogi st should be aggointed Unit Director with the responsibi l i ty of formulating a l l policy and carrying out overal l procedure within the uni t . He reports t o the Head of the Department through the chief of C.V. Service.
( i i ) Staff physicians. Physicians' coverage should be based on a 24-hour , 7-day week. They ahould be pr imar i ly rcoponoiblc t o the un i t , and immediately avai lable a t a l l times.
( i i i ) S ta f f nurses. A minimum of one special ly t ra ined graduate nurse s h o ~ ~ l d be on duty a t a l l times ( the idea l nurse/patient r a t e should be one nurse f o r every 1-1.5 ~ a t i e n t s ) , remembering t h a t the nurse i s the key f igure i n the CCU,
( i v ) Auxiliary nurses. Highly motivated, special ly t ra ined auxi l iary nurses can be of grea t value i n bedside pa t ien t care under the supervision of graduated nurses.
(v) Secretary. A non-medical person appointed a s u n i t secretary w i l l be responsible f o r keeping track of admissions, t ransfer , and discharges. She may be responsible f o r inventory of equipment, answering the telephone and placing c a l l s f o r the doctors and nurses i n the un i t .
EM/~ard.Vasc ./5 EM/PRV.MJ, CARD. vsc . ~1S/17 Annex X I 3 page i x
( f ) General recommendations
( i ) Standardization of equipment. A l l . e lectronic instruments should be purchased from the same company. This w i l l f a c i l i t a t e the subst i tut ion of one par t f o r another; the interchange of one instrument f o r another; and the education of the nurses and other s t a f f personnel. The company which provides equipment should a l so pmvide f o r servicing and repair .
( i i ) Electronic technician. An electronic technician with t ra in ing i n medical e lectronic instruments,who is readi ly available i s highly desirable i n a CCU. He I u s t look a f t e r the equipnent with n "preventive maintenance" approach.
( i i i ) Policy. Admission and discharge c r i t e r i a should be established a s well a s the specif ic resgonsibi l i ty and authori ty of a l l medical, nursing, auxi l ia ry and administrative personnel. It i s highly desirable t o promote the admission of pat ients a t the
- e a r l i e s t possible time (8).
( i v ) Training. A l l the CCU s ta f f should have part ic ipated i n formal t ra ining courses with par t icu lar a t t en t ioa t o electrocardiogra- phy and resusoi tat ion t c c h n i q u e ~ ~ For the continued efficiency of a CCU there should be regular meetings t o discuss the various medical and administrative problems within t h e u n i t a s well a s recent technological and s c i e n t i f i c advances re la ted t o the subject.
(v) Point t o s t ress . There i s a danger of s t a f f concentrating too much un Ule machines. The problem l i e s i n -the Sact t ha t they can become "equipment-orientedt' and i t i s necessary t o remember t h a t there i s a pat ient a t the end of a l l t h a t machinery. The equipment i s secondary: i t is very valuable and a l o t can be accomplished with it, but i t is a l so possible t o do a l o t without it.
3.4 Mobile Coronary Care U n i t (MCW
(a) B a s i s f o r this u n i t
The same principles a s applied t o CCU a re applied t o MCCU with more emphasis on the need t o avoid any delay i n the appl icat ion of intensive care since most of the deaths i n the f i r s t hours of acute myocardial infarct io n a r e due t o ventr icular f i b r i l l a t i o n which could be prevented i f proqdfly and I ~ ~ ! D C ~ ~ S T treated.

EM/~ard ,Vasc ./5 EPII/PRV.~.~~, CARD.VSC . D I S / ~ ~ Annex XIV Page x
WHO m o
Experiences i n many countries have demonstrated the f e a s i b i l i t y of integrat ing MCCU services within the exis t ing systems of medical care organizations, par t icu lar ly hospi tals . With MCCU, coronary pat ients can be put under intensive care quicker than by any other means. Therefore, the pr incipal objective of the MCCU i s t o de l iver sk i l l ed medical care t o the coronary pat ient a t the place of the at tack a t the e a r l i e s t possible moment.
(b) Design
Ambulances i n general use a r e su i tab le i'or IvlCLU. 'lbe only requis i te i s space so tha t a doctor and a t l c a s t a nurse can monitor the cardiac rhythi of the pat ient and il" nccessary administer treatment including cardiac resusci ta t ion. Consequently the ambulance must a l so provide space f o r equipment.
(c) Equipment
Generally speaking the basic equipment required i n a MCCU is the same a s f o r the CCU. The following items a re regarded apl indispensable f o r a MCCU: Oscilloscope with ECG wri ter , portable DC de f ib r i l l a to r , equipment f o r a r t i f i c i a l vent i la t ion, laryngoscope and endotracheal tubes, oxygen, suction apparatus, equipment f o r i n t r a - venous infusion and sampling and a com~le t e s e t of drugs f o r treating cardiovascular pat ients .
(d) Adaitional cquipment
Portable battery-operatcd demand pacemaker with pacing electrodes and portable anaesthesia cquipment.
(e) Staff
The idea l team should comprise a cardiologis t with experience i n CCU, a nurse t rained i n the techniques of coronary care and a techni- cian (or other t ra ined auxi l iary worker) especially t ra ined t o administer shock therapy, record ECGs, e tc . The ambulance dr iver may a l so help i n the carrying of equipment and of thc pat ient .
( f ) General recommendations
A MCCU i s ef fec t ive i n the measure it i s co-ord ik ted and integrated with an e f f i c i e n t hospi tal CCU.
Tne MCCU's team should be always immediately avai lable f o r an emeqgency c a l l . To i%lly u t i l i z e t h i s sk i l l ed s t a f f when there i s under-ut i l izat ion of the coronary component, the MCCU could a l so be used f o r other types of emergency. The development of MCCU should
WHO EImo FN/Card .Vasc ./5 I~M/PRV,~IJ. CARD..VSC .~1S/17. Annex X I V page xi
be adcpted t o l o c a l condit iono : nccdo and rccourocs (manpower, s k i l l , organization and ava i l ab i l i t y of equipment) .
It seems useful topoin t out t ha t thcrc e r e sonc basic rc- qu i s i t e s f o r the establishment of a MCCU. Thesc are: adequate telephone network and mads, and a population re la t ive ly concentrated. A t the same time it i s necessary t o avoid d c l ~ y s i n contacting the mobile coronary care scrvices by proper educatLon of pat ients and poten t ia l pat ients . I t i s generally agreed t h a t pa t ien ts with known coronary a r te ry disease should bc encourz..ged t o obtain the appropr ia te a i d irnmcdiatcly they dovolop symptons suggestive of myocardial in ferc t ion (11).
3.5 Paediatric Cardiovascular Service
(a) Basis f o r t h i s u n i t
Great aavances I n the field US paediatric cardiology have been made during the past three decades. Until re la t ive ly few years ago the exact diagnosis of a congenital hear t disease was a d i f f i c u l t theore t ica l exercise of academic i n t e r e s t only. However, the advent of cardiac surgery and the poss ib i l i ty of surgical ly correcting these congenital anomalies have completcly changed the s i tua t ion i n t o a matter of great prac t ica l importance.
Antibiotics, highly technical laboratory diagnostic procedures, new surgical techniques, cardiac prostheses, and modern anaesthetic r~ethods have a l l played a s ign i f icant ro l c i n thu succcssf i l manage- ment and treatment of hear t diseases i n the pacdiatric age group a s well a s i n adults.
Paediatric cardiology has become a scparntc spec ia l i ty by i t s e l f and it is par t icu lar ly i n t h i s f i e l d t h a t teamwork ~ S ? S p&ved t o be of highest value. Working together closely a s a t e a , the cardio- l o g i s t and surgeon have accordplished many cures f o r cardiac diseases previously considered hopeless (4).
(b) Design
The paediatric ca-rdiovascular service may be a specialized u n i t withinthe aeneral cardiovascular service of a hospi ta l o r a special i - zed separate service i n a chi ldren 's hospi tal o r i n a paediatric service. The paediatric cardiovascular service should be thought of ne i ther as a medical cardiovascular service nor a s a surgical cardiovascular service, but a s both.
A pcediatric cardiovascular service needs t o have those u n i t s already specified for adlilts w i t h the exception o r those f o r coronary

EM/~ard .Vasc ./5 EPI/PRv.MJ . CARD .VSC. D I S / ~ ~ Annex XIV page xii
WHO m o
ccre. Bcsidea, it has +o bc attaohed t o a surgical som%co with i t s operation su i t e vfhich w i l l be analjjzed i n the section below, recovery room and/or 3 special type of intensive care un i t , known as "cardiac surgery uni t" , While paediatric services, i n s p i t e of the need f o r s ingle rooms f o r i so la t ion , could es tab l i sh multiple-bed wards with many advantages, a pncdiatric cardiovascular service c a l l s f o r more single-bed rooms i n which t o care f o r children i n the diagnostic and pre-operative phase of hospi tal izat ion, as well as i n the post-operative phase a f t e r discharge frori~ the cardiac surgery uni t . The rooms should be ample, chce r f i l and have a home- l i l r c atmosphoro, but a t the sams t i m e shoi~ld h ~ v i . a11 the elements t o assure a quick and e f f i c i en t management of the pat ient i n routine and emergency s i tuat ions. Each bed should be provided with i ts own oxygen out le t , suction equipment, bedboard, sockets f o r e l e c t r i c a l equipment, e tc .
According t o the hospi tal ' s resources and policy, the surgical Sector O f the paeulatrlc ci?rdLovasoular sax-vice may have a recovery mom and/or G cardiac surgery u n i t f o r the care of the children during the c r i t i c a l period of the post-operative phase. Because of the potent ial r i sk of cardiorespiratory emergencies during t h i s period, children must never be l e f t unattended and the drugs and equipment s ta ted below should be readily available, a s well a s specialized s t a f f coverage of doctors and nurses based on a 2il-liour , 7-day week. The best choice f o r post-operative control 02 cmldren (as well a s adul t s ) i s the cardiac surgery uni t , a ml t i -bed speelalized ward s imilar t o an intensive care u n i t i n i t s sut-up and f a c i l i t i e s . The number of beds i n these u n i t s w i l l depend on the s i ze of the services, the workload and the policy regarding thc cverage number of days children c r c kept i n {,he uni t .
( c ) Equipment
The d i f fe ren t specialized un i t s comprising the paediatric cardiovascular service (cardiac catheter izat ion 2nd angiocardio- graphy , exercise t e s t s un i t , e t c . ) , require the equipment previously discussed.
The cardiac surgery u n i t f o r the post-oper-?..tive management of cardiac surgical pat ients requires the folloriing equipment (6) :
(i) Equipment f c r the zdministration of oxygen (gauge, mask, t en t o r croupette) ;
(ii) Thoracic suction apparatus with extra bot t les (500 cc s i ze f o r children) ;
(iii) Intravenous stands and tray:

WHO mo EM/Card .Vasc ./5 EDl/pRV.lU . CARD. VSC , D I s / ~ ~ Annex XIV page xiii
(iv) &tr-a L U L L ~ C S of 5 per cent dextrose and water intravenous solutions, and, i f available, a paediatric inl%sion s e t t ha t allows f o r more accurate administration and CaLibration of intravenous f lu ids ;
(v) Sphygmomanometer and stethoscope ;
(vi) Nasogastric suction apparatus with whist le- t ip catheters and a Y connector f o r endotracheal suction and appropriate s i ze Levine tubes;
( v i i ) Graduated container f o r measuring urinary drainage;
( v i i i ) Urinometer and litmus paper;
( i x ) Automatic posi t ive pressure machine with appropriate masks and various-sized endotracheal tubes and laryngoscope;
(x) A cardiac c a r t o r separate items t h a t include:
a. A cardiac a r r e s t t m y with a l l equipment necessary f o r intrathoracic cardiac massage
b. Tracheostomy t ray
c. Thoracentesis s e t
d. Emergency and other drugs such as lanatoside C, digoxin, d ig i toxin, calcium gluconate , epinephrine, phenylephrine, hydrochloride, levcrterenol menadione sodium b i su l f i t e , procaine amido hydroohloridc, aminophyllinc , i suyr-u lerenol, sodium bicarbonate, calciwn chloride, molar sodium l ac t a t e , and heparin sodium. I n addition, sedatives such a s phenobarbital, morphine sulphate, and mepcridine
h ydrochloridc should be readi ly available;
e . Syringes and needles of ~uying s izes including in t r a - cardiac needles;
f . Def ibr i l la tor and pacemaker and equipment f o r placing intra-card? nn clactrodes;
g. Padded tongue depressors.
(xi) Four large Mayo clamps f o r chest tubes;
(x i i ) Equipment (Thennorite mattress, icebags, e t c . ) f o r temperature reducing moasurcc ;

EM/~ard . ~ a s c ./5 B/I/PRV . lW . CARD. VS c . DIS/17 Annex XIV pagc x iv
WHO EMRO
( x i i i ) Bladder-drainage equipment
(xiv) a t r a l inen.
(d) S taf f - Among the specialized s t a f f of the various u n i t s comprising
thc paediatric cardiovc?scular service the most important personnel a r e the paediatric cardiologists, c a rd iovascu l~~~r surgeons and spccizlized nurses (the nursing care of in fan ts and children who havc cardiac operations has become a special area of nursing practlcc (6)) . Their number varies according t o workload and s ize of the service.
3.6 Cardiovascular Surgical U n i t
(a) Fksis f o r this u n i t
The same principles a s those which apply t o thc ~ a e d i a t r i c cardiovascular service a r c applied t o the camiiovascular surgical u n i t showing tha t it i s not only i n the f i e l d of congenital heart diseases t h a t cnrdiovascular surgery has progressed. Great advances havc a l so come about i n the surgery of acquired valve lesions, diseases of thc V C G G C ~ E , s u r ~ i a n l . treatment of c o r n n n w pat ients , e tc .
The cardiovascular surgical u n i t may be a specic7.lized u n i t within -he department of surgery o r a separate u n i t attached t o a cardiovascular service.
The ward should preferably comprise s ingle o r double-bed rooms with the f a c i l i t i e s already specified.
For the post-operative care of pat ients , there i s a need f o r a cardiac surgery u n i t which does not d i f f e r from the u h i t already described f o r the surgical u n i t of the paediatric cardiovascular service.
m e operation room f o r t h i s u n i t deserves special comment. The problem of its size io an unanswered question since t h i s is re la ted t o the future progress of cardiovascular surgcry and the s t r ik ing and rapid changes tc?kfng place i n procedures and equipment. Tdhile f o r most purposcs the standard s i ze 02 opemting rooms should bc approximately 25 square metres ( f ive by f ive) t o 76 square metres ( s i x by s i x ) the operating room f o r cardiac surgemj should be a t l e a s t 49 square metres (seven by seven).
WHO Em0 EN/Card.Vasc ./5 EM/PRV. l ' ~ . CARD. VSC . ~ 1 S / 1 7 Anne:: XIV page xv
( c ) Equipment
Among thd spec ia l i zcd instruments f o r cnrdiovascular surgery one very important i tem i s the heart- lung machine uscd i n open h e a r t surgery f o r c i r c u l a t i n g blood extracorporeal ly through f i l t e r s and oxygenntcr. T l i s machine wi th a l l t h c persons i n - volved i n i t s f'unctfcn 2nd the su rg ica l tcam, a r e the f a c t o r s which necess i t a te increascd s i z e of the opc:ixting: room f o r cnrdiovascuLar surgery.
(d) Staff
The number of cardiovascular surgeons, doc-tors, nurses, spec ia l i zed and a u x i l i a r y personnel, and a n c i l l a r y s t a f f , w i l l depend on the s i z e of t h e u n i t and t h e workloed.
7.7 Excrcise Tes t s Unit
Basis f o r this u n i t
The cardiovascular system, wi th t h e lungs and blood, c o n s t i t u t e t h e oxygen t ranspor ta t ion systcm (1) which under normal condi t ions can meet the demand f o r oxygen of t h e m s c l e s under any circumstances. A t rest, the consumption of oxygen of t h e musclcs i s low, increas ing under maximum a c t i v i t y toslOO times t h c r e s t i n g value. I n cases of cardiovascular d i seases t h i s demand cannot bo completely met.
Exercise t e s t s a r c used f o r the purpose of assess ing the f 'unctional e f f i c iency of the cardiovascular system both i n h e a l t h and disease; i n h e a l t h t o t e a t f i t n e s s f o r s p e c i a l types of work o r syorLs; 111 disease tu help i n the diagnooia nnd prognosis of c e r t a i n cardiovascular d i seascs and f o r evaluat ing t h c e f f e c t of preventive, therapeut ic and r e h a b i l i t a t i o n programmes.
I n an Exercise Tes t s Unit of c cardiovascular se rv ice t h e only type of t e s t s used a r c the so-cal lcd "submaximum" t e s t s . The more strenuous ' 'maximum" t c s t s suse?~ on exercise physiology a r e not general ly used i n these u n i t s , Among t h e "submaximumif t e s t s the re a r e two types: t h e "recovery tssts" i n which measurements a r e takcn during the recovery period following exercise , and t h e "efforts tests" in which rncacurorncnt~ are takcn during exercise (1 ) . (b) Design
The room f o r t h e Exercise Tes t s Unit must be of a s i z e t o permit t h e accornmodction of t h e equipment and the s t a f f necessary f o r the exerc i se t e s t s w i t h ample space between the d i f f e r e n t types o f ergometers t o facilitate measurements and coriLi.vl of the p a t i e n t s .
EM/cord,vasc ./5 EIVI/PRV.bLJ. CARD.VSC.DIS/17 Alinex XIV pngc xvi
WHO EMRO
TLle u n i t should bc ideally loca te2 ILU L d i s L a u L r"r4um th; coronary ca re u n i t s ince t h e occurrence of ventricul'r f i b r i l l a - t i o n o r o the r emergencies could. happen during the t e s t s exercises . It should a l s o bc located adjacent t o the Evaluetion Unit of t h e Rehabi l i ta t ion Services wi th which i t shares some f a c i l i t i e s and s t e f f .
(c) E q u i p m e .
rvlethods f o r excrcisc t c s t i n g vary f rom t h e sirnplc procedures o f lmcc- bending, climbing a t o . i r ~ etc., t o s o p h i s t i c a t ~ d techniques f o r which apparatuses r r e used. The most rvidcly u s ~ d types of crgoiiieters f o r exercise t e s t s a re : b icycle crgoi-netcr, s t eps , t r eadmi l l and am1 crank. An ECG and a sphy~7;lornanometer, a r e e s s e n t i a l s ince ECG recording and blood pressurc rncasurements a r e usua l ly an i n t e g r a l p a r t of t h e exercise t c s t s . I.? the u n i t is locc?.ted a t d is tance f'rorn t h e CCU it is necessary t o reckon wi th a d e n D r i l l a t o r a s e t of cardiovascular cmcrgency drugs, as wel l a s wi th a r e s p i r a t o r . Thc u n i t must be equipped wi th a couch where p a t i e n t s may l i e and r e s t .
(d) S t a f f
The i d e a l team should ccrnprise a physician, a nurse and a p h y s i o t h e ~ a p i s t o r technician, wi th bas ic und-erstanfing of exercise physiology and ECG and ab lc t o recognize any abnormality o r impending 5 i i f i c u l t i e s and immediately i n t e r r u p t t h e t e s t and i n i t i a t e emergency therzpy.
3.8 Rehab i l i t a t ion Services f o r C.V. Pa t i en t s
(a) Basis f o r t h i s uniL
U n t i l recent ycars 2. major i ty of t h e ncdic31 profession looked upon r e h a b i l i t r t i o n a s an ex t ra -cur r i cu la r a c t i v i t y of medicine. To-&ay the s i t u a t i o n i s 3 i f f e r e n t and medicine has f u l l y recognized t h c t medical care cannot be considered complctc u n t i l t h e p a t i e n t wi th a physicar d i s a b i l i t y has been t r a i n e d " to l i v e and work with whet he has l e f t " (12). Thc basic philosophy of r e h a b i l i t a t i o n i s t h a t t h e pkysic ian 's r e s p o n s i b i l i t y does not end when the i l l n e s s is ended; i t ends only whcn the ind iv idua l i s m t r d n e d t o l i v e and work wi th the f 2 c u l t i c s he s t i l l possesses through a comprehen- s ive proglmme of physical , psychological, s o c i a l and vocational r e h a b i l i t a t i o n , It i s necessary t o s t r e s s t h a t any programme of r e h a b i l i t a t i o n i s only a s sound a s t h e bas ic medical se rv ice of vrhich it is a par t , and 'chat physical r e h a b i l i t a t i o n should start a s soon as Lhe p a t i e n t ' s c l i n i c a l condit ion allows, t o avoid complications r c s ~ i l t i n g f porn prolonged b u d rest.

WHO m o EM/card .vase ./5 ED.I/PRV.MT. CARD. VSC. ~1S /17 Annex XIV page xv i i
(b) Design
It i s generally agreed t h a t most of cardiovascular pat ients can be rehabi l i ta ted by adequately s ta f fed and equipped cardio- vascular service. Only exceptional cases should be referred t o special rehabi l i ta t ion centres. The rehabi l i tz t ion u n i t should be located adjacent t o thc Exercise Tests Unit since both un i t s a r e m t u z l l y supporting. The Exercise Tests Unit is the place where the l n c t i o n a l effect of a rehabi l i ta t ion programme is evaluated.
The rehabi l i ta t ion u n i t comprises two sub-units: the evaluation un i t and the treatment area.
( i ) Evaluation uni t : Here the general assessnent of the pa t ien t is completed. This i s not only tes t ing of the fknctional eff ic iency of the cardiovascular system nnalyzoci i n the Exercise Tests Unit, but goes fu r the r i n analyzi n g +.he soc i a l s i tua t ion of the pat ient , assessing h i s a b i l i t y and appraising h i s psychological s t ~ t e i n the immediate circwilstances resu l t - ing from h i s cardiac condition, a s comparccl with his previous a t t i t udes and behaviour. The u n i t is only an examining area with cubicles separated by f loo r t o ce i l ing solid par t i t ions f o r confident ial interviewing. The number of cubicles w i l l depend nn the s taff .
Since the Rehabili tation Services a r e a iknctional conti- nuation of the Exercise Tcsts Unit, par t of the f a c i l i t i e s should have n common use. These f a c i l i t i e s arc: a reccpticu arca with comfortable waiting space, an of f ice f o r the pcrformsrnce of administrative and c l e r i c a l dut ics , dressing rooms fur lle staff equlpped with lockers, shower, and a lounge i f possible, and t o i l c t s f o r pat icnts .
( i i ) Treatnlent Area: The establishment of t h i s arca a s a separate u n i t i s ju s t i f i ed only i n very exceptional cascs. For cxamplc, when the cardiovascular services have a very important programme of rehabi l i ta t ion of cardiovascular pa t ien ts covering a big area and with huge attendance. Usually the same t r e a t - ment area of the general rehabi l i ta t ion services of the hospi tal should be used f o r cardiovascular pat ients under the supervision o f cardiovascular scrvices ' persur~rlel. mien the Exercise Tests Unit has a physiotherapist among i t s s t a f f , it i s possible t o perform there some physical rehabi l i ta t ion a c t i v i t i e s .
(c) Equipment
This is usually the same a s f o r a general un i t , t h a t is: equipment f o r ttzermothcrapy, electrotherapy, mechanothempy, therapeutic exercises, e tc .

EM/~ard.Vasc ./5 EN/PRV.MJ. cARD.VSC. D I S / ~ ~ Annex XIV page x v i i i
WHO m o
(d) S t a f f
The ca rd io log i s t i n charge of t h e Exercise Tes t s Unit may a l s o be responsible f o r t h e Rehabi l i ta t ion Services f o r cardiovascular pa t i en t s . The same a p p l i e s t o t h e nurse. For t h e evaluation u n i t , the se rv ices of a s o c i a l worker, a psychologist , and a vocational counsel lor a r e necessary. For the treatment a rea i f separated from the general r e h a b i l i t a t i o n se rv iccs of t h e hosp i ta l , the se rv ices of physiotherapis ts and occupational t h e r a p i s t s a r e required, t h e i r number according t o the workloac!.
3.9 Out-patient Department of t h e Cardiovascular Service
(a ) Basis f o r t h i s u n i t
The OPD c o n s t i t u t e s an important u n i t i n a cardiovascular scrvice . It should bo phye ioa l ly intoe;ratod with t h o g o n a r d OPD of t h o h o s p i t d , p r ~ v i d i n g - on ambulatory bas i s - t h e following services:
( i ) It serves p a t i e n t s who do not r equ i re h o s p i t a l i z a t i o n by providing them diagnost ic , cu ra t ive and r c h a b i l i t a t i v c services .
( i i ) It provides diagnost ic se rv ices f o r p a t i e n t s requir ing f u r t h e r h u s y l Lal lzu Llur~ Cur* surile s y e c l a l yr-uceilul~us.
( i i i ) It provides follow-up treatment and con t ro l a f t e r p a t i e n t s ' discharge from h o s p i t a l wards.
( i v ) It promotes h e a l t h education and preventive programmes f o r cardiovascular d iseases .
The l a s t point deserves some s p e c i a l comments. A l l t h e a c t i v i t i e s of t h e OPD a r e c r i en ted towards keeping a c l o s e r contact w i t h t h e community served by t h e hosp i ta l . This point p a r t i c u l a r l y s t r e s s e s the need f o r nn a c t i v e i n i t i a t i v e i n a preventive approach t o t h e community.
The preventive aspec t s of h e a l t h ca re cannot be divorced from t h e cura t ive ones and the OPD should be the f o c a l point f o r t h i s in tegra - t ion . Specia l ized teams could perform epidemiological inves t iga t ion t o describe the d l s t r l b u t l o n of cardlovascular cllsoases anQ formulate e t i o l o g i c a l hypotheses aiming a t developing programmes f o r the prevention and con t ro l of cardiovascular d i seases wi th s p e c i a l emphasis on h e a l t h education. This t a sk should be an important a c t i v i t y of the OPD.
An e f f i c i e n t OPD may s u b s t a n t i a l l y reduce t h e demand f o r beds i n t h e cardiovascular szrvices .

WHO m o EN/~ard.Vasc ./5 EM/PRV. M J . CARD .VSC . D I S / ~ ~ Annex XIV page x i x
(b) Design and equipment --------.---
It corresponds t o the design and equipment of t h c OPD of t h e h o s p i t a l concerved-,
( c ) S t a f f
The s t a f f v,dr!;ing i n the cura t ive aspec t s of t h e OPD should i d e a l l y ' e t h e senie as 'chat working i n the wards which f a c i l i t a t e s co-ordinatioc between vards and GPD f o r t h e h o s p i t a l i z a t i o n and follow-up of pa+,ients- Tne s t a f f f o r t h e preventive aspec t s o f the OPD should compriso an epidemiologist , a h e a l t h educator and appro- p r i a t e personnel, f o r the epidemiological surveys and preventive campaigns.
3.10 Home Care Programmes
A very important f a c e t of ambulatory c a r c of cardiovascular p a t i e n t s is hone care. A home ca rc programme makes it possiblc t o extend needed se rv ices t o t h e p a t i e n t a f t e r hc has been discharged from t h e h o s p i t a l and r ~ t u r n e d t o his home.
Pa t i en t s a r e admitted t o a home care programme only a f t e r a s t a y i n t h e hospital and remaln unaor supervlslon of t n e cardlovascular se rv lcc a s long a s they a r e on t h e horn? ca re se rv ice , I m p l i c i t i s t h e idea t h a t home ca re programme i s rnatnly deal ing wi th t h e home card of p a t i e n t s who otherwise would be t r e a t e d i n h o s p i t a l (9).
Decision t o admit a p a t i c n t t o homc ca re sc rv ice comes through thc judgement of t h e c a r d i o l o g i s t i n c lose co l l abora t ion wi th nurses and s o c i a l workers.
When medical atld housing r e q u i s i t e s a r c met, homc ca re has many advantages, among ~ ~ h i c h a r c b c lov~er c o s t and t h c p o s i t i v e emotional inf luencc on t h e pa-lient of remaining i n his own environment. D i f f i c u l t i e s l i e on t h e shortage o f ixanpcvrcr (many people a r e involved i n a home care programme) and t h e re luctance o f doctors t o accept t h e uncer ta in condi t ions they a r e l i k c l y t o encounter during home visits. Howcver, the main l i n k between the h o s p i t a l and liomc i s t h e v i s i t i n g nurse and/or s o c i a l worker viho can supervise t:ic p t i e n t , rcvicw h i s progress and advise, when necessary, h i s readx.ission t o h o s p i t a l .
I n a home ca re programme, a l l se rv ices f o r thc p a t i e n t are arranged f o r and co-ordinated through t h e hosp i ta l . The programme should be managed by a physician ( d i r e c t o r o r co-ordinator of t h e home c a r e programme) for whom an o f f i c e and s e c r e t a r i a t f a c i l i t i e s a r e needed.
EM/~ard.Vasc ./5 EM/PRV.MJ. CARD. VSC . DIS/17 Annex XIV' page xx
WHO m o
There i s a l s o a need f o r part- t ime use of a conference room where t h e d i r e c t o r of t h e programme can meet and d i scuss wi th physicians, nurses, s o c i a l workers and o ther s p e c i e l i s t s , a c t i v i t i e s and problems r e l a t i n g t o t h e programme.
3.11 Co-ordination and C~rcliovascular Services
The Oxford d ic t ionary def ines ffco-ordinates' as t o br ing p a r t s i n t o p r o p r re la t ion . Therefore, co-ordination deals wi th t h e t a sk of blending offorcts in order to onsuro s ~ ~ c c e s s f i ~ l a t t a i n m e n t of nn ohj~rt ivca. It should be pointed out t h a t co-ordination makes poss ible a t o t a l accom- plishment i n excess of the ind iv idua l p a r t s making up t h a t t o t a l . Co- ordinat ion i s so important i n a cardiovascular se rv ice t h a t i t deserves some s p e c i a l comments. It w i l l be analyzed undcr two main headings:
( a ) I n t e r n a l co-ordination
( i ) Teamwork
( i i ) Co-ordination between d i f f e r e n t se rv ices of t h c h o s p i t a l
(b) External co-ordination
(a ) l n t e r n a l co-ordination
( i ) Teamwork. This r e f e r s t o the co-ordination among s t a f f members of the cardiovasculnr sc rv ice i n which the c f f o r t o f each spec ia l i zed doctor, nurse, technician, e t c . should be blended, timed and c a r e f u l l y d i r e c t e d so t h a t t h e team's ac t ions become synchronized a s a u n i t thus maximizing t h e r e s u l t s . Teamwork does not j u s t come i n t o exis tence a s a consequence of people working together. Specif ic measures shoul? be taken by t h e Head of se rv ice t o ensure thls teamwork a t t i t u d e .
( i i ) Co-ordinati on among d i f f e r e n t se rv ices of the hosp i ta l . This r e f e r s t o t h e co-ordinetlon of t h e cardiovascular se rv ice w i t h o t h e r medical departments and se rv ices of t h c hosp i ta l . The f i r s t th ing t o s t r e s s he re i s the need f o r a quick t r a n s f e r from h o s p i t a l recept ion t o coronary ca re u n i t f o r suspacted i n f a r c t i o n p a t i e n t s , The aclministrative fo rmal i t i e s of admission could be completed a f t e r h i s h o s p i t a l i z a t i o n i n thc u n i t . I n respec t of co-ordination wi th o ther medical departments, this i s a must not only f o r t h e e f f i c i e n t running of the cordiovascular se rv ice but f o r t h e whole h o s p i t a l and is t h e b e s t way t o ensure good medical ca re se rv ices f o r a l l those attending t h e hosp i ta l . Here again it i s necessary t o s t r e s s t h e need f o r ensuring quick t r a n s f e r from o ther h o s p i t a l wards t o coronary carc u n i t s i f a p a t i e n t g e t s an i n f a r c t i o n whilc hosp i ta l i zed .
WHO m o EM/~ard .Vasc ./5 EM/PRV. I?J . CARD. VSC . DIS/l7 Annex X I V page xxi
(b) External co-ordinstion
This r e f e r s t o tho co-ordination between the hospi tal cardio- vascular service with cardiovascular services a n d o r other medical services outside the hospitzl .
The co-ordination with cardiovascular services outside the hospi ta l could. be developed a s a type of l'regionalization" i n which the hospi ta l carcliovascular service a c t s a s a centre t o which t o r e f e r gar t icu lar ly d i f f i c u l t or sgecial ly charccterized pa t ien ts who required more sophisticated diagnostic proceclures and/or hospi tal i - zation, a t the same time the hospi ta l cardiovascular service s t a f f can regularly v i s i t tho out-lying medical services and conduct t ra ining meetings, consultations, conferences and tho l i ke . On the other hand the personnel of these services can visit the hospi ta l carciiovascular scrvicc f o r specialized t raining. This is useful not only f o r phyoiciano, but for nurses, laboratory tcchniciana and other specialized personnel. This r e su l t s i n a two-way co-ordination flow.
Special.emphasis should be given t o co-ordination between the c a ~ i o v a s c u l a r service and the school heal th services. Here l i e a l l the complex educational problems posed by childrcn with cardiac Usease. Probably, the maln problem concerns the vocational or ientat ion o f these children. Hcre it is necossary t o s t r e s s once more the need f o r teamwork, since the school physician must co- operate closely with the cardiologist , the t rea t ing physician ard the occupational therapis t , t c make the ch i ld and h i s family understand and accept the ch i ld ' s present and future l imitat ions a s wcl l a s h i s vocational poss ib i l i t i e s .

E N / ~ a r d . ~ a s c ./5 EM/PRV.MJ. CARD.VSC.DIS/~~ Annex X I V page xxii
REFERENCES
WHO m o
(1) Andcrsen, K.L., Shephad, R.J., Denolin, H., Varnauskas, E. and Masironi, R. Fundamentals of Exercise Testing, WHO Geneva, 1971
(2) Ceci l and Hoeb: Textbook of Medicine, Vol. 11, 982, Thirteen Edi t ion 1971, W.B. Sauntlcrs Company
(3) Collins, Evans and Clorck: Basic equipment f o r mecucal in tensive- care u n i t s , Lancet, 286, 1972
(4) Cooley, D.A, and Hallman, G.L.: General su rg ica l considerations. Hcart Diseases i n In fan t s , ch i ld ren and adolescents. (Edited by A.J. Moss and F.H. hdams). Baltimore, 1968, t h a W i l l i a m s and Wilkins Co.
( 5 ) G m c c slncl Kcyloum: Thc Coronary Carc Unit, Bclttcrworths, London 1970
(6) Hadley, Betty J. : Nursing Care (Surgery). H e a r t d i seases i n i n f a n t s , ch i ld ren and a d o l o s c ~ n t s (Edited by 1 L . J . Moss and F.H. Ailcams) , Baltimore, 1966. ?he W i l l i a m s and. Wilkins Co .
(7) Laur, Robert J.: Four r e q u i s i t e s f o r tleveloping HMOs. Hospital Prugr,css, Jilrluary 1972
( 8 ) Oliver, M.F. and Ju l i an , D.G.: Manual on In tens ive Coronary Care. WHO Regional Office f o r Europe, Copenhagen, 1970
(9 ) Report of a group study: t h e r e l a t i o n between t h e h o s p i t a l and i t s community. WHO Regional Office f o r Europe, Copenhagen 1958
(10) Report of WHO Expert Conunittee: Hospi ta l Administration. Tech. Rep. Ser., No. 395, 1968
(11) Report on a Working group: The Role of Mobile Coronary Care Unit. WHO Regional Office f o r Europe; Copenhagen 1970
(12) Rusk, H.A. : Rehabi l i t a t ion Medicine. The C.V. Mosby Company, S a i n t Louis, 1964
(13) U.S. Department or Health, Eclucation and welsare: coronary Care Units . Public Health Service Publ icat ion No. 1250, 1964
(14) U.S. Department of Health, Eclucation and Welfare: Proceedings of thc National Conference on Coronary Care Units. Public Health Service Publ icat ion No. 1764, 1968
WHO m o
ANNEX XV
EM/~ard.Vasc ./5 EM/PRV. M J . CARD .VSC . DIS/17 Annex XV page i
PROBLEMS AND CHALLENGES IN REHABILITATION OF PATIENTS WITH ACUTE MYOCARDIAL INFARCTION
D r 7,. Fej far Chief, Cardiovascular Diseases Unit, WKO/Headquarters
Rehabili tation has been recognized f o r a long time a s an in tegra l par t of t o t a l medical care of pat ients . Its aim i s t o restore the pat ient , a s f a r a s possible, t o h i s normal l i f e i n the society i n which he l ives . Adequate rehabi l i ta t ion may, however, do more than ju s t restore the pa t i en t ' s previous capacity. Ischaemic hear t disease usually develops over a number of years, and l i f o habi t s appear important. Thus rehabi l i ta t ion aims t o develop, t o the optimum, physical and mental fbnctions of the pat ient so 2s t o enable him t o have a frui t f 'u l , f'ully act ive l i f e .
This means:
1. t o restore the pat ient t o self-rel iance i n h i s dai ly l i f e ,
2. t o enable h i m t o make such a recovery t h a t he can resume h i s former work act ively,
3 . i f this is not possible, periods of rehabi l i ta t ion should prepare the pat ient f o r othcr full-time employmcnt, which would be compatible with h i s s t a t e of health,
4. i n those who do not recover completely, the rehabi l i ta t ion process should prepare them f o r part-time o r sheltered employment, o r f o r non-remunerative a c t i v i t i e s .g The broad def in i t ion implies t ha t success of rehabi l i ta t ion includes
the patient, his family, the understanding of the heal th team, which i s headed by the physician i n charge of the treatment, and the a t t i t ude of the society in w h i c h the p a t i e n t l i v e s .
'Ell3 PATIENT
Important aspects influencing rehabi l i ta t ion are:
1. severi ty of cardiovascular dysfinc t ion,

EM/Card. Vas c. /5 WPRV. W. CARD. VSC. DIS/l7 Annex XV page ii
WHO mo
2. age a t which the disease develops,
3. personal i ty of t h e p a t i e n t and h i s physical and mental s t a t u s before t h e disease,
4. changes i n behaviour r e s u l t i n g from t h e disease.
I n recent years, ischaemic h e a r t disease, and its most notorious manifestat ion -- acute myocardial infarc t ion, has been made wel l known t o t h e general public. The increas ing frequency, p a r t i c u l a r l y i n younger subjects , increas ing p o s s i b i l i t i e s f o r treatment and prevention of e a r l y l e t h a l complications, and successful r e h a b i l i t a t i o n of t h e majori ty of those who recover, can change t h e atmosphere from f a t a l i s t i c towards, perhaps, a too op t imis t i c a t t i t u d e .
Early treatment and r e h a b i l i t a t i o n depends f i r s t of a l l on e a r l y diagnosis of t h e condition. It is too wel l known and no t necessary t o repeat, t ha t . rnnst. of the l o t h d complications occur within t w o hours a f t e r t h e onset of c l a s s i c a l pain, o r o t h e r symptoms of acute cardio- vascular d iseases .
The s ignif icance of coronary care un i t s , o r mobile coronary care un i t s , depends on l o c a l p o s s i b i l i t i e s f o r reaching t h e p a t i e n t as soon a s possible. Results from published s t u d i e s andfkom t h e ongoing iachaemic heart disease registers' study, cu-uri l ir~erleif by WHO I n elghteen European areas, one i n Aus t ra l i a and one i n I s r a e l , ind ica te t h a t we a r e f a r from t h i s s i t u a t i o n .
I n a community study of acute coronary h e a r t a t t a c k s i n t h e Edinburgh area, 73 p e r cent of a l l deaths which occurred wi thin t h e f i r s t f o u r weeks were outs ide hosp i ta l , and 45 per cent a l ready wi thin an hour of t h e onset of t h e acute at tack.z/ lvlost deaths occurred at home (45.8 per cent of a l l 541 deaths) . 226 were medically unattended; of these 122 occurred a t home, twenty-three a t work and fo r ty - th ree i n t h e s t r e e t . Thirty-seven deaths out of eighty-four of p a t i e n t s seen by t h e doctor, before they died, occurred outs ide of hosp i ta l .
The median time between t h e onset of symptoms and c a l l f o r medical a i d was 1 hour 30 minutes. The median time between t h e c a l l f o r t h e general p r a c t i t i o n e r and h i s a r r i v a l was 44 minutes, and t h e t o t a l time f o r re fe r red p a t i e n t s before t h e onset of symptoms and a r r i v a l a t h o s p i t a l w a s 5 houx-s 23 r i i i r ~ u l e s . The t l m e interval w a s conslaeralsly s2lortened In p a t i e n t s who contacted t h e h o s p i t a l d i r e c t l y (medial time 2 hours 21 minutes f o r s i x t y p a t i e n t s ) . A long delay before t h e onset of symp.Loms and t h e treatment has a l s o been recorded i n t h e WHO study of community ischaemic

EN/card. Vasc . /5 B~/PRV. NJ . CARD. VSC. DIS/l7 Annex XV page iii
hear t d isease reg i s te r s , which a r e done i n d i f f e r e n t cu l t u r a l s e t t i n g s and i n soc i e t i a s which do vary g rea t ly i n the organization of hea l th services . In a l l however, the longest delay is the time before t he pa t ien t recognizes t h a t he should c a l l f o r help; obviously b e t t e r heal-th education is needed t o explain f rankly t he disease symptoms, treatment and prognosis, but i n a w a y so a s not t o sca re the pa t ien t .
Apart from the ignorance of s ignif icance of the symptoms, the re may be a var ie ty of reasons why the pa t ien t does not c a l l f o r medical a id . Snme of them may he related to the fear of l o d n g the job, too negative o r pess imis t ic a t t i t u d e of t he soc ie ty towards cardiovascular diseases, f e a r of economic loss , f e a r of dying, of t h e hospi ta l , e tc .
PHASES OF RMABILITATION
I f one accepts t h a t r ehab i l i t a t i on is a par t of treatment, one should consider when t o start it, w h a t it means, and wlio shuuld do it.
The methods used i n r ehab i l i t a t i on of pa t i en t s who have had acute myocardial i n f a r c t i on are, in essence, s im i l a r t o those used f o r pa t i en t s with o ther diseases. A l l aim t o r e in t eg ra t e t he pa t ien t i n due time i n t o h i s environment. The d iv i s ion i n to t h e psychological aspects, physical t r a i n ing and vocational measures, i s meant only t o stress the various aspects o r t he r ehab i l i t a t i on process. 'I'he t h r ee of course a r e i n t e r r e l a t ed s ince t he onset of r ehab i l i t a t i on and individualized wifh varying emphasis on one o r the o the r at d i f f e r en t phases of t he r ehab i l i t a - t ion.
For p r ac t i c a l purposes of r ehab i l i t a t i on of pa t i en t s with acute myocardial infarct ion, t he !LW working group, which met i n Freiburg i n 1967, divided the programme in to th ree phases:
Phase I - Acute phase, o f ten hosp i ta l i za t ion - l a s t i n g on average th ree weeks i f the re a re no complications
Phase I1 - Convalescence - on average of e igh t weeks' durat ion
Phase I11 - Post convalescence - of uniimited period - which i n e f f e c t should continue f o r years o r even f o r t he r e s t of t he p a t i e n t ' s l i f e .
Acute Phase
Psychological aspects are i n t he foreground and the a t t i t u d e of t he physician who f i r s t comes, i n answer t o t he ca l l , may be decis ive f o r t he

EM/~ard.Vasc ./5 EM/PRV.MJ .cAI~.VSC.DIS/~~ Annex XV page i v
WHO EMRO
whole fu tu re . Rapid diagnosis, onset of treatment, and explanation of the ser iousness of the i l l n e s s wi th t h e calm assurance of what a r e t h e present p o s s i b i l i t i e s , o f t e n apply more t o tlie family than t o the p a t i e n t . Equally t h i s continues at the place where the p a t i e n t i s t rea ted . I f i n hosp i ta l , and i n a coronary car? u n i t dur5ng t h e rirst few days, t h e con- t i n u i t y of contact wi th t h e family physician i n one cu l tu re , o r t h e d i s t r i c t h e a l t h o f f i c e r i n another , i s very important. Other members of t h e h e a l t h team a l s o play an important r o l e .
Psychological problems a r e not necessar i ly due t o t h e behaviour type of t h e p a t i e n t o r h i s a t t i t u d e s tc,,rsrds sudden l i f e threatening disease . They may or ig ina te from the z t t i t u d e , remarks, s i l ence o r l ack of communica- t i o n wi th members of the h e a l t h team.
Permanent monitoring wi th su rve i l l ance i n a coronary ca re u n i t may be a reassur ing protect ion. I n a number of ins tances , however, the p a t i e n t may f e e l l o s t among t h e wires. Resusci ta t ion procedures of cardiac a r r e s t again may f r i g h t e n o r reassure the neighbours.
Advantages f o r having an understanding c l i n i c a l psychologist a r e without doubt. However the l ack of them and t h e g rea t number of p a t i e n t s c a l l s u rgen t ly f o r more in tens ive t r a i n i n g of physicians i n psychology. It must be re-emphasized t h a t even a t t h e acute s t age a r e a l i s t i c but o p t i - mistio approach i s encouraging for the patient and his Family, and develops t h e i r a c t i v e p a r t i c i p a t i o n i n the r e h a b i l i t a t i o n progmme. The physician, who was and/or w i l l be responsible f o r the p a t i e n t a f t e r recovery, is tremendously valuable as pa r t of t h e team of s p e c i a l i s t s . I n my opinion, i n the major i ty o f cases, he i s b e s t q u a l i f i e d t o solve t h e personal problems facing t h e p a t i e n t i n future , while the psychologist, and p s y c h i a t r i s t , a r e needed f o r s p e c i a l cases and s i t u a t i o n s , and f o r t r a i n i n g of s tuden t s and physicians.
The f u t u r e organization o f l i f e may be discussed wi th the p a t i e n t and family a l ready a t t h i s stage, depending on the p a t i e n t ' s pe r sona l i ty and on t h e s e v e r i t y of a t t ack .
Taking i n t o considerat ion the l i m i t a t i o n of movement caused by t h e s e v e r i t y of the acute d i s c a ~ e and, of course c l i n i c a l s t a t 2 of t h e pa t i en t , t h e gradual, super-dsed mouemonts, r e sp i ra to ry exercises , and movement of ex t remi t i es he lp t o overcame the unwanted e f f e c t s of complete immobiliza- tion, and provide important psychological stimulus to the patient, indicating t h e onset of r e c o v e v . Examples of how t o proceed were out l ined i n a number of publ icat ions and w i l l be dZscussed by D r Broustet .5 %
An important aspect worth re-emphasizing i s t h a t r e h a b i l i t a t i o n begins wi th the reassurance t h a t it should concern every member of the h e a l t h team
WHO EMRO EM/~ard .Vasc ./5 E M / ~ V .W . Ct'iFD .VSC . ~ 1 S / 1 7 Annex XV page v
who p a r t i c i p a t e i n t h e care of t h e pa t i en t , and thk physician of f i r s t contact wi th t h e patlen'c may Dc 'in6 most lmportarlt person. f ~ l s o included is the family and p a r t i c u l a r l y the wife.
Another important s t e p f o r t h e recovering p a t i e n t i s t h e time when he i s allowed, f o r the l irst timc, t o leave h i s bed and proceed from s i t t i n g i n a c h a i r t o s-canding and walking. 14onitoring t h e h e a r t a c t i v i t y and t h e neasurcntent of bloocl pressure e r e u s e f i l a i d s t o c l i n i c a l observation, undcr which t h e p a t i e n t begins h i s convalescence.
Twenty years ago we attempted t o measure c i r c u l a t o r y adapta t ion i n twenty-sewn convc?lescu:;is ( t w u ~ l t ~ -f ive riierl, twu w U I I I ~ I ~ ) f r u ~ i i acu Le myocardial i n f a r c t i o n . ti11 were exposed t o t h e o r t h o s t a t i c t e s t of t en minutes ' duration, Curing which ECGs and blood pressure were measured. 6/ Reaction vzr ied among incl iv i lual p a t i e n t s , but on average t h e o r t h o s t a t i c t e s t becane normal wi thin t e n clays of f i r s t stan::ing up. Some pa t i en t s , p a r t i c u l a r l y t h e o lder ones, reacted very l i t t l e indeed, while on t h e o ther hand, a f i f t y - s i x year olcl nervous, anxious pa t i cn t , wi th only s l i g h t ischacmic changes i n ECG, showed g r e a t e levet ion of t h e h e a r t r a t e during the f i r s t minute a f t a r standing up, which d id not improve even cn t h c seventeenth day from t h c onset of convalescence. H i s ECG, however, never cletcriorated.
The ECGs showed a dirninishei! nega t iv i ty of inver ted T waves and t h e e leva t ion of ST s e m e n t i n the ches t l eads i n sub.iects wi th a n t e r i o r i n f a r c t i o n . I n p a t i e n t s wi th p o s t e r i o r i n f a r c t i o n decrease of the amplitude of pos i t ive T waves, together wi th t h e ST cleprcssion, was observed. Al te ra t ion of t h ~ T wave were found i n 95 per cent of sub jec t s ( t a b l e 1 & 2) . A l l charges appeared iLmeJiately a f t e r standing up (even wi thin two seconds), were more marked i n p a t i d n t s wi th nervous l a b i l i t y , and. were a l s o influznccd by resp i ra t ion . The changes were ~xplninsd as being of ixtra cardiac origin. Tho alteration i n the repo la r iza t ion phase of ECG Curing convalescence the re fore requ i res caution, when considered alone i n the c l i n i c a l dizgnosis.T/
During the phzse of convalescknce, t h e p a t i e n t is t r c i n e d t o increase his physical a c t i v i t y , so t h a t hc can resumc h i s previous l i f e . Equally, t h e psychological s ide of t h e problem i s t o prevent and t r e a t emotional clisturbanccs r e l a t e d t o t h e coming back home and i d e n t i f i c a t i o n o f problems associa ted wi th re tu rn t o wcrk. L number of l e c t u r c s tocay dea l wi th a very important aspect of physical t r a i n i n g during convalescence. Physical condit ioning w i l l a lso assist i n ovcrcomjng the f e a r and am3 c?ty p r i o r t o s t a r t i n g work, and make him ab lc t o come back t o h i s previous a c t i d t i e s and be again a u s e f u l member of the socie ty .
The guidance of t h e physician i n charge i s of g r e a t importance here. The physical t r a i n i n g and psychological a d j u s t ~ e n t shoulc! go hand i n
Er/I/Card .Vasc ./5 E;M/PRV,MJ. C A ~ .. mc: . ~1s/17 Annex XV pegc v i
WHO EMRO
hand wi th t h c p o s s i o i l i t i e s i n t:ic socie ty f o r re turning t o a f r u i t m l l i f c . Thc spec i f i c c?.ctxons must be -tailorec1 for pn i n l l i v i d ~ ~ a l pationt, clepending on thc sevcvrity c - tht cardiac Jayage, s i t u a t i o n of the family, previous l i f e n c ~ j - v ~ i L c s , anG p o s s i b i l i t i e s i n a givcn c u l t u r e o r soc ie ty s t r u c r , u M ~ ( q 3 , L t t a i l ~ > by ~ellerstein181') .
Tho increc?si_t7g ~~u? lbcr o f p a t i e n t s and need f o r spec ia l i zed se rv ices i n Giagnosis , t r ca ~mer, t xi. r c h a b i l l t a t i o n , r equ i res t h a t r e h a b i l i t a t i o n programmes should k,: 2 : n ~ b 7 r zhc. team which inc luJus a t l c a s t a physio- t h e r a p i s t , psychologist ,13rt from a physician traine?. i n r e h a b i l i t a t i o n . This nucleus, : ~ h i c ! ~ i s ihc r;i~niiiium f o r any community cen t re , can e a s i l y Sc p a r t of t i c usual- s c r ~ i c c s i n the hosp i ta l . ii condi t ion qup- nnn i s close contact wi th the bas ic per ipheral h e a l t h ccn t re o r &enera1 p r a c t i t i o n e r .
It was a co'isenms of opinion of the WHO group of exper ts i n 1963, t h a t t h e maJor5ty of cardiova-sculzr p a t i a n t s can be taken ca re of by adequately staffcc! 2nd equipnec dep~?.rtmcnt of medicinc o r cardiology. However " d i f f i c u l t casts" ; , T , ~ tv 1 7 ~ r c f r l r r o d tc spacial a l i n i ce o r assessment cect res .r"ci. ?O.I:TJ~-O~:PS~VL s tud les , physical and recondit ioning, vocational t ra i f i ipg a n 3 ?et.-.sinirI3.ll/ The various sc rv iccs and f a c i l i - t i c s a r e i l l u s t r a t e d i n f i g u r e 1.
Nevcrthcless, the re a r c a number of s i t u a t i o n s where a simple commonsense approach by the physician towar2,s an i n t e l l i g e n t and under- standing rat . iont m a y be rcrra13fiLngr
Two examples may be i/ lua t ra t iv i :
I n 1948, 1 t r e a t e d a pa t i en t , aged about M f t y years, f o r a severe i n f a r c t i o n t r i th nccrosis c11 over the ches t l eads who, a f t e r c g r e a t emotional u p s e t , ha1 ~2 re:inf 21 c t i o n f o u r weeks a f t z r t h e f i r s t one. His prcccding l i f e vdns very Mcctlc, He was a professor of theology a t the un ivers i ty , dean of L c f a c u l t y and head of t h e church. The r e h a b i l i t a - t i o n programme consis ted od- explanation of thc f u t u r e organization of h i s whole l i f e an6 gca.?~1~1 :2-i:isicnl condit ioning. The p a t i c n t gave up two of h i s th ree funct ions and was ab le t o follow-up exact ly t h e medical advice, c.g, s ta rk ing t o work kr':o o r th rce hours da i ly , and accepting o t h e r engagements only a f t e r consul ta t ion wi th h i s physician. He a l s o kep t very s t r i c t l y t o +,lie FxSramme of gradual physical condit ioning. Eight years l a t e r , v~lien t h c qaest ion c f r e -e lec t ion of head of t h e church arose, he ria:: I n such a goo?, physical and mental condi t ion t h a t ho was able to ncccpt the 1 - ~ s p u ~ 1 s l b l l i t y (agaln ar tcp consul ta t ion and examination by h i s physic isn) ,
Another pn t ien t (s ix ty-four years old), a highly i n t e l l i g e n t physician, suffe?ed from acute myoca~Jia1 i n f a r c t i o n t e n ycars ago. A t t h a t time,

EM/~ard. .Vasc ./5 EM/PRV.. M J . CARD. VSC . DIS/17 Annex XV page v i i
the concept of e a r l y physical r e t r a i n i n g was not so accepted a s it i s to-day. The convalescence period progressed slowly and t h e p a t i e n t f e l t f r u s t r a t e d .
When seen by a consult ing physician, s t i l l a t ttc- convalescent home, he had no s igns of cardiac f a i l u r e . While walking, he used t o s t o p a f t e r 30-50 metres and always seemed a l i t t l e breathless . From time t o time however, when he had seen mushrooms of which he was very fond, he bent, picked them and forgot t o s top. Then a Pew minutes l a t e r , when he remembered, he paused again a s beforc, a f - i e r a brief walk of 30-50 metres. Onc hour walking wi th him, and 5 rninutes of explanation of t h e above was a l l t h a t was needed t o r e h a b i l i t a t e him. H i s condit ion, up t o the present time, has remained unchanged.
These examples serve only t o show t h a t t h e psychological a spec t s i n r d a - t i o n t o p a r t i c u l a r f u t u r e a c t i v i t i e s and Lo pos i t ion i n t h e soc ie ty may be tho dominant feature, and that the commonocnac approach of a p r a c t i t i o n e r , o r of a consul t ing physicians may s u f f i c e t o f u l l y r e i n t e g r a t e the pa t i en t i n t o the soc ie ty . There a r e obviously a varying number of problem cases f o r wkLch one needs mul t id i sc ip l ine co-operation of the physician, psychologist , s p e c i a l i s t i n r e h a b i l i t a t i o n and a vocational counsellor.
The place a i d dm-n t iu i l uf Lhe oorlvulesoerice phase; var lzs . Ttlls depends on t h e c l i n i c a l condi t ion of t h e p a t i e n t , on Lhc concept of r e h a b i l i t a t i o n by the medical profession, and a l s o on t h e age and socio- economic condi t ion of t h e p a t i e n t and on t h e community i n which he l i v e s .
I n one c u l t u r e i n Europe, f o r exmple , p a t i e n t s ppefer t o be a t home within t h e c i r c l e of t h e i r family. I n another cu l tu re , most, i f not al.1 p a t i e n t s who recover from acu te myocardial i n f a r c t i o n are rehabi- l i t a t e d i n s p e c i a l c o n v a l e s c ~ n t homes and the expenses incurred a r e covered by the na t iona l o r p r iva te h e a l t h insurance. RegaTdless of the place, where t h e p a t i e n t i s recovering, t h e p r inc ip le aims and problems a r e s i m i l a r - how t o prepare physical ly and mentally t h e p a t i e n t s t r i c k e n wi th acute myocardial i n f a r c t i o n i n t o an a c t i v e l i f e .
An important aspect of t h i s period is the education of the family and the p a t i e n t on t h e o r ig in , n a t u r a l h i s t o r y and p o s s i b i l i t i e s f o r con t ro l of ischaemic h e a r t d isease . Again, t h i s w i l l be individual ized uucording t o the c l l n l c a l s t a t e a t present, psycMologlca1 make up, age and benaviour of the pa t i en t . The education includes explanation .bT heal thy l i f e hab i t s , t h e importance of adequate d i e t , withdrawal df smoking ( i f app l icab le ) , education of the p a t i e n t on how t o match h i s ambition wi th h i s ap t i tudes , and how t o adapt t o s t r a i n s of d a i l y l i f e .
Vocational cousel l ing i s very important. The problem of employing p a t i e n t s who have recovered from ischaemic h e a r t d isease concerns t h e

card .Vase ./5 EX/PRV. PU . CARD. VSC. DIS/1'( Annex XV page v i i i
WHO EMRO
physician a s we l l a s t h e employer. P r iva te o r na t iona l e n t e r p r i s e s may sometimes p r e f e r t o pay t h e d i s a b i l i t y remuneration than t o employ them. And, not uncommonly, physicians a r e not w i l l i n g t o take c l e a r c u t r e s p o n s i b i l i t y fo' ind ica t ing t h a t t h e convalescent p a t i e n t can resume his previous work. The proSlem i s more and more urgent because o f t h e increas ing number of younger sub jec t s wi th acu te myocai-dial i n f a r c t i o n a t t h e height of t h e i r physical and mental a b i l i t i e s , and a l s o because most o f t h e jobs i n modern i n d u s t r i a l e n t e r p r i s e s do not r equ i re much more physical e f f o r t than ordinary l i f e a t home.
It is d i f f i c u l t t o advise t h e p a t i e n t t o r e f r a i n from smoking i f t h e physician himself smokes. Equally an obese physician w i l l o f t en race questions if he advises t h e p a t i e n t t o l o s e surp1v.s weight.
Post convalescence - Maintenance Period .- - This goes on f o r years and should oontinue for the r e s t o f the l i f e
of t h e pa t i en t , wi th t h e aim t o keep him f i t physical ly and mentally f o r a s long as possible.
?"ne main f e a t u r e is a permanent contact between t h e doc to r and t h e pa t i en t . Sometimes on individual bas i s , o t h e r times a t regu la r sess ions organized a t t h e ou tpa t i en t c l i n i c s f o r groups of pa t i en t s . Experience fr.0111 Gii LaLur.g: has sliowrl Lt~a L these a r e very important because the pa t i e n t s themselves pos i t ive ly p a r t i c i p a t e i n physical condit ioning and i n so lv in t h e various problems of d a i l y l i f e under t h e guidance of t h e physician. 1%
The physical t r a i n i n g aims t o maintain physical r i t n e s s and, i n p a r t i c u l a r , t o s t r e s s the c i r c u l a t o r y system. I n t e r m i t t e n t ( i n t e r v a l ) t r a i n i n g o r prolonged physical a c t i v i t y once o r twice a week, aim t o reach a t peak l e v e l s t h e submaximal h e a r t r a t e . Non-competitive s p o r t s and. p a r t i c u l a r l y walking i n the h i l l s wi th varying speed, a r e more n a t u r a l than indoor exercise on s teps , o r b icyc le ergometer. The type of exerc i se should be t h a t which t h e p a t i e n t p re fe r s , un less the re would be any p a r t i c u l a r reasons aga ins t it.
A few minutes 02 d a i l y exerc i se becomes a f t e r severa l weeks of s t rugg le wi th s e l f and rou t ine something which w i l l be appreciated by the p a t i e n t a i t e r months and years.
Iri s o m e countr ies , p a t l e n t s who have recovered from myocardial i n f a r c t i o n e s t a b l i s h myocardial i n f a r c t i o n clubs. Their aims d i f f e r and they may he lp t o improve l i f e h a b i t s , exchange information on common s o c i a l and vocational problems, OF even defend t h e i n t e r e s t o r t h e p a t i e n t s v i s - &-vis the socie ty .
An important f ea tu re of whatever type of follow-up, i s t h e regu la r contact wi th t h e p a t i e n t and an attempt t o l i v e i n accordance wi th t h e present knowledge on secondary prevention o r on promotion of b e t t e r heal th .

~ . ! / c ; ~ F ~ . V E ~ E C . /5 EN/PRV.~~Z. CAIID.VSC . D I S / ~ ~ Annex XV page i x
A l t h o u ~ h the prognostic importance of recognized coronary 13isk f a c t o r s seel:ls J i r f e r e l ~ L i l l Lht! pa Lie11 L s 2 s compared wi th heal thy subjects , It is nevertheless an es taQ i she6 common prac t i ce t o r e s t r a i n p a t i e n t s S from c i g a r e t t e smoking,. t o advise on d i e t moderate i n c a l o r i e s and with reduced animal f a t , arid con-trol and t r e a t adequua-tzly hypertension, ?lyperlipidaemia, d iabetes and o ther abnormalit ies associa ted wi th t h e progress of a the rosc le ros i s .
Other consideration
Systematic r e h a b i l i t a t i o n programmes f o r p a t i e n t s with acute myocardial i n f a r c t i o n have not had a l u n g traditiul-1 i n Eui-.opt.. Even now t h e med-ical profession i n sorne countr ies does not prac"cic, as a rout ine , a c t i v e r e h a b i l i t a t i o n programmes, and p a t i e n t s kept i n bed f o r too long need more time f o r f u l l recovery.
A s e r i e s of questions a r e o f ten r a i s e d - Pmat a r e tt?e aangers or t h e r a t n e r heavy physical - training i n un-
accustomed pa t i en t s? How d-oes physical r e h a b i l i t a t i o n a l t e r the prognosis f o r l i f e and f o r reoccurrence of acute myocardial in fa rc t ion? How of ten do t h e important s ide e f f e c t s require cessat ion of t h e r e h a b i l i - t a t i o n programme? Is t h e e f f e c t of physical t r a i n i n g r e a l l y more psychological than r e a l , and how f a r should one s t r e s s the programme f o r e l d e r l y subjects?
There a r e no c l e a r c u t answers t o most of these questions, al though they have been discussed a t severa l i n t e r n a t i o n a l meetings.
One accepts general ly t h a t a c t i v e e a r l y mobilization of t h e p a t i e n t done under medical supervision i s not dangerous, and does not r e s u l t i n increased frequency of complications. On the contrary the b e n e f i c i a l e f f e c t of it is seen when the p a t i e n t proves t o himsclf t h a t he can l ead t h e usua l a c t i v e l i f e .
There is , however, not enough evidence from long-telm follow-up s t u d i e s t o show how much physical t r a i n i n g i t s e l f , o r i n combination with o ther r i s k f a c t o r s , would a l t e r the prognosis o r pa.-tients wi th myocardial in fa rc t ion .
Information on a p a r t i c u l a r group followed-up f o r severa l years CS presented by Dr . ~e l l e lmann .g / A preliminary s-tudv Irom Gijteborg myocardial i n f a r c t i o n c l i n i c s i n d i c a t e s that p a t i e n t s r c s l a r l y seen a t t h e pos t - in fa rc t ion c l i n i c s have considerably lower mor ta l i ty than matched conti-01 subjects .
The WHO working group, wi th p a r t i c i p a n t s fror!~ severa l European coun t r i es have discussed t h i s problem severa l t i n c s . A t -the l a s t
Eil/card .Vasc ./5 EP.l/PKV. FIT. CARD. VSC . DIS/17 Annex XV page x
WHO m o
meeting i n October 1971 i n Prague, two types of s t u d i e s were proposed and agreed rlgon.5/ Vorkers i n some countr ies w i s h t o prove how e f feo t ive a r e comprehensive r e h a b i l i t a t i o n programmes during chc- phase I1 (convalescence) f o r f u l r i l l i n g the alms of r e h a b i l i t a t i o n a s compared wi th t h e a t present convctltionnl eszablished methods. Yl is study, of only s e v e r a l months' duur~tion, e i n s t o provide information oil a community bas i s , and the end points , i.e. the goal, a r e d a i l y l i f e a c t i v i t i e s .
Thc study on prognosis hzs, f o r i t s aim, t o discover whether a long- term programme of pi?;rslcal condit ioning w i l l have a s i g n i f i c a n t e f f e c t on mor ta l i ty and morbidity. It is , i n e f f e c t , a secondaly prevention study, i n which a randomly se lec ted groug of pa t i en t s , a l l with classical r i s k fac to rs , w i l l be t r ea ted ; t h e "experimental" group w i l l d i f f e r f r o the "control" group by having progressive physical t r a i n i n g programmes. 57
An important challenge Is t o assess t h e h a b i t u a l physical a c t i v i t y and i t s r e l a t i o n s h i p t o coronary h e a r t d isease . There a re , of course, means how t o measure d i r e c t l y t h e l e v e l s of energy expenditure, t h e acrobic component from oxyzen con~umption, the anaerobic Irom blood lactate l e v e l s f o r ins tance. Eowever these methods cannot be used commonly and i n l a r g e r groups. Ammg t h e i n d i r e c t methods, which a r e l e s s p rec i se but more acceptable, a r e a c t i v i t y r e c a l l quest ionnaires , pedometers o r accelero- meters f o r measuring the movement o f l a r g e ,muscle groups, d i e t a r y surveys, measurement of deep body temperature and continuous rccorciing of t h e h e a r t r a t e . Questionnaires and h e a r t :-ate recording appeaiq a t present most suilablc: Tor' Ll-le assessment o l hab l tua l physlcal ac t lv l ' iy oI popul t i o n groups, including sub jec t s recovering from myocardi-1 i n h r c t i o n . 17
There i s a lack of personnel t r a ined i n r e h a b i l i t a t i o n of cardiac pa t i en t s , and t h e number o f c l i n i c a l psychologists , s o c i a l workers and vocational adv i se r s i s equally inadequate f o r tha increas ing demands. The overburdened physician a l s o does not have ,?nou:sh Lime t o devote t o every p a t i e n t whenever enere i s a need f o r it.
I f the re i s s t i l l a considerable number of physicians who p r e f e r " to go slowly" and t o keep the p a t i e n t from a c t i v e l i f e f o r a long time, t h e o ther extreme a l s o e x i s t s : 'illere a r e some who a r e persuaded t h a t r e h a b i l i t a t i o n can be wel l and e r f i c i e n t l y done only i n spec ia l i zed cen t res and by s p e c i a l i s t s i n r e h a b i l i t a t i o n .
I n my personal opinion, t h e most important i s team approach f o r the whole complex of treatment of ischaemic h e a r t d isease , of '~hich r e h a b i l i t a - t i o n 1s a p a r t . It has t o be understood t h a t one physician should be cont inual ly responsible f o r the p a t i e n t o who co-operates c lose ly with a number of s p e c i a l i s t s i n the ve.riatls phases of the n a t u r a l h i s t o r y o f t h e disease . Ultimately, i n the broadest sense, the r e h a b i l i t a t i o n of p a t i e n t s should a l s o increase h i s knowledge of h i s d isease and i ts control . General preventive measures wi th appropr ia te l i f e h a b i t s a r e an obvious p a r t i n t h i s chain of ac t ions .

WHO EMRO EM/~ard . ~ a s c ./5 EM/PRV .PU. CARD. VSC . ~ 1 S / 1 7 Annex XV page x i
COIJCLUSIONS
1. The aim of r e h a b i l i t a t i o n i s t o re tu rn t h e p a t i e n t , i n as f a r a s poss ible t o h i s previous l i f e a c t i v i t i e s .
2. The r e h a b i l i t a t i o n programme has psychological, physical , s o c i a l and vocational a spec t s . It involves t h e pa t i en t , his family and t h e s o c i a l environment.
- . The r e h a b i l i t a t i o n programme is b e s t c a r r i e d out by a team of t r a ined h e a l t h workers, headed by t h e physician. The procedures vary according t o the s e v c r i t y of the disease , a t t i t u d e of t h e p a t i e n t a s we l l a s l o c a l t r a d i t i o n s . The various problems r e l a t e d t o acute phase, t o convalusccnce and post-convalescence per iods have been described.
4. There is an urgc~nt . need t.n ~ v a l i i a t . ~ t n w h a t e v t ~ n t progressive physical t r a i n i n g a l t e r s tile prognosis of cardiac p a t i e n t s . A secondary prevention prografime of t h a t nature has been suggested by a WHO co-operative group.
5. Ear ly mobilization and r e t u r n of a p a t i e n t t o an a c t i v e l i f e i s of ten impeded by t h e lack of' knowledge of r e h a b i l i t a t i o n procedures and by lack of trained personnel. --
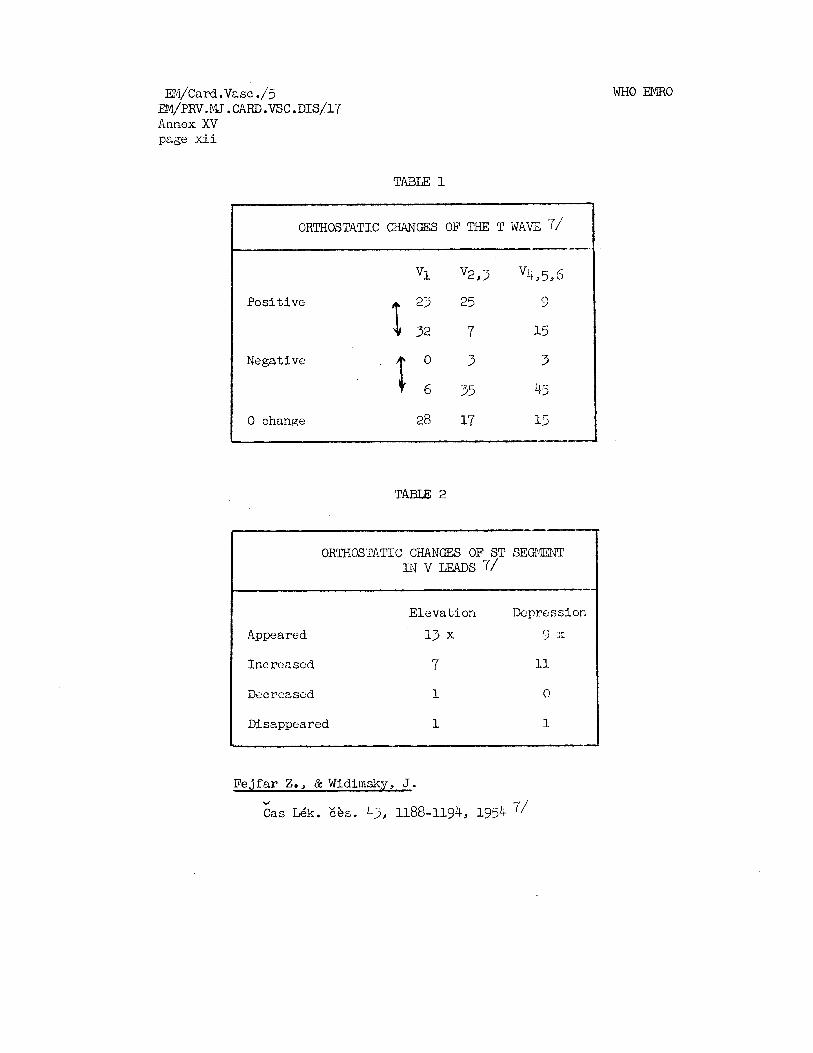
EM/~ard.Vasc ./ j EM/pRV. M J . CARD. VSC . DIS/17 Annex XV page x i i
WHO EMRO
TABLE 1
ORTHOSTATIC C?JANGES OF THE T WAVE 7/
Positive
Negative
0 change
ORTHOSTATIC CHANGES OF ST SEGMENT I N v LEADS 71
-- Elevation Depression
Appeared 13 x 3 x
Increased 7 11
Decreased 1 0
Disappeared 1 1
1
Fejfar Z., & Widimsky, J. Y
Cas Gk. Fhr . 4 j, 1188-1194, 1954 7/

WIIO EMno EN/~ai-d. Va s c . /5 EM/PRV.ZVLJ. c~m.vsc .~1s/17 Annex XV page x i i i
1. Assessment of h a b i t u a l physical a c t i v i t y : Report of a meeting of WHO advisers , Prague,, 1971. Available on r c q ~ l z s t .
2. A-mstrong, A., Duncan, Barbara, Oliver, M.F., J?&,ian, D.G., Donald, K.W., f i l t o n , Mary, Lutz, W., Morrison, S.L. - ITatural h i s t o r y of acute coronary h e a r t a t t acks : A community study, B r i t i s h Heart Journal , 2, 67-80, 1972
3. Blackburn, H., Canner, P., Krol l , W., Tominaga, S. and Stamler, J. The coronary drug pro iec t . Presented a t t h e Symposium organized by thi? Council on Epidemiology and Prevention of t h e ~ n t e r n a t i o n a l Socie ty of yardiology, a t Skovdc (Sweden), 1971
4. Broustet , J.P. - Prograilliles de mobi l isa t ion dans l a plz,?.sc aiguz, Schvi. med. Wsch. ( i n press)
5. Evaluation of r e h a b i l i t a t i o n programcs f o r p a t i e n t s vrith myocardial in-iarction: Report of. a 4030 Working Group. Prn~uc , 4-7 October 1971. EURO 8206 (6) . Available on request .
6 . Fcj fa r , Z., Linhar t , J., Pk.rovsky, I. and Widimslr?, J. - Zm"ey or thos ta t i ck6 reakcc u rekonvalescent6 po i n h r k t u myokardu . &s, Lkk. & s . 43, 495-432, 195b
7. FC j f a r , Z., Wid imsk'j, J. - 0rthostatick"yektrokardiogram u rckonvclescent6 po in fnrk tu nTgokardu. a s , L6k. cas. 43, 1188-1194,
8. He l le r s te in , H.K. - Convalescent phase t r a in ing . Schw. med. wsch. (in prcoc)
9, Kellermann, J . J. - Physical condit ioning i n p a t i e n t s a f t e r myocardial i n f a r c t i o n (comparative study - 9 years ' follow-up) . Schvr. med. Wchsch. ( i n press)
10. A programme f o r the physical r e h a b i l i t a t i o n of p a t i e n t s wi th acute rnyo- c a r d i a l i n f a r c t i o n : Report 02 a WHO Working Group, Freiburgim-Breisgau, 4-6 March 1968. EURO 5030 ( 1 ) . Available on request
11. Rehabilitation of patients with cardiovascular diseases: Roport ol
a WHO exper t Committee. Wld. Hlth. Org. Teclin. Rep. Ser. 270, 1964
2 Vedin, A. and Wilhelmsson, C. (1972) - Personal coniiirunication ( i n press)

m/Card. va.s c . /5 EM/PKv.MJ. CARD.VSC .DIS/l7 Annex XV pa.ge xiv
WHO EMRO
- Periodic evaluation of the pa t ien t ' s physical working capacity throughout
HOSPITAL (S)
Trea b e n t : Convalescence
- HOME 3
<- I
1
1 I
I I
I
I I
I
r- ----I I
t I
I
I I I
1 I I
>
VOCATIONAL REHABILITATION c m m
Advice and guidance: Employment agencies :
Training : Retraining: Education
WORK Original
L- Modified She1 terpd





























