Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Usefulness of Fetal Three-Dimensional Ultrasonographyfor Detecting of Congenital Heart Defects and AssociatedSyndromes
Nadia Zabadneh • Claudia Santagati •
Elena Reffo • Roberta Biffanti • Alessia Cerutti •
Nicola Maschietto • Ornella Milanesi
Received: 4 October 2010 / Accepted: 22 March 2011 / Published online: 9 April 2011
� Springer Science+Business Media, LLC 2011
Abstract Congenital heart defects (CHDs) occur in 1%
of live-born infants and frequently are associated with
extracardiac malformations. This study aimed to assess the
feasibility and accuracy of three-dimensional ultrasonog-
raphy (3DUS) in fetuses with CHD and to investigate
whether 3DUS can add information about the heart and
general fetal morphology that shows other congenital
malformations or suggests syndromes. For 30 fetuses
affected by CHD, 3DUS was performed using a Sonos
7500 ultrasound machine with a cardiac 3D transducer. In
44% of the exams, 3DUS was completely diagnostic for the
CHD, providing additional information in 28% of the
exams. Furthermore, 3DUS showed 82% of associated
malformations, providing the complete diagnosis in 57% of
the cases and helping with recognition of syndromes in
others. The diagnostic accuracy of 3DUS was superior,
with a higher number of acquisitions per exam. Perfor-
mance was better in fetuses younger than 24 weeks for
general morphologic details and in fetuses older than
24 weeks for the heart morphology.
Keywords Congenital � 3D Echocardiography �Heart defects � Fetus � Prenatal diagnosis � Syndromes
Introduction
Congenital heart defects occur frequently in malformation
syndromes. Approximately 70% of spontaneous aborted
and stillborn fetuses and 25% of infants with a congenital
heart defect (CHD) have associated extracardiac malfor-
mations. Detection of a heart defect should prompt a
detailed search for associated extracardiac malformations.
Parents expect a complete and accurate prenatal diagnosis
and appropriate information regarding the natural history
of the cardiac defect and any associated abnormality [6].
Two-dimensional (2D) ultrasonography imaging is the
principal method for obtaining diagnostic information
about the fetus, but proper interpretation depends on cre-
ating a mental three-dimensional (3D) reconstruction from
the images [4]. The mental process of converting 2D into
3D images depends on the skill, training, and experience of
the operator [20], as evidenced by the wide variability in
diagnostic accuracy for detecting congenital anomalies [12,
19]. In the last few years, 3D imaging techniques have been
applied in fetal ultrasonography with rapid progress [1, 3,
5, 7–11, 14–16, 23, 24, 27, 28], with hope that 3D images
would reduce operator dependency and improve diagnostic
accuracy.
This study aimed to assess the feasibility and accuracy
of 3D ultrasonography in a group of fetuses with a CHD
diagnosed by 2D ultrasonography and to assess the specific
role of the 3D reconstruction in the current practice of fetal
cardiology. Specifically, we aimed to determine whether
3D images added information about the heart and general
fetal morphology that would disclose other congenital
malformations or suggest syndromes, yielding a more
complete diagnosis. To our knowledge, this is the first
report describing this matter from the pediatric cardiology
perspective.
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00246-011-9977-9) contains supplementarymaterial, which is available to authorized users.
N. Zabadneh � C. Santagati � E. Reffo � R. Biffanti �A. Cerutti � N. Maschietto � O. Milanesi (&)
Department of Pediatrics, University of Padova,
Via Giustiniani 3, 35128 Padova, Italy
e-mail: [email protected]
123
Pediatr Cardiol (2011) 32:724–736
DOI 10.1007/s00246-011-9977-9

Materials and Methods
Patients
All fetuses with congenital heart anomalies diagnosed by
2D echocardiography at the Fetal Cardiac Unit of our
Department from October 2008 through February 2009
were eligible for enrollment in the study. Subjects were
enrolled if the parents agreed and gave informed consent.
The 3D ultrasonography study included one or more
real-time or volumetric 3D data sets of the heart, head,
face, limbs, and genitalia. If the patient underwent a fol-
low-up 2D exam, a repeat 3D exam was performed as well
if the parents consented. The outcome of each pregnancy
was determined. For pregnancies that went to term, follow-
up data were obtained from the medical record of the
infant. The fetopsy report was reviewed for all pregnancies
ending in spontaneous or planned termination.
The research protocol was approved by the Hospital
Committee on Clinical Investigation, and the procedures
followed were in accordance with institutional guidelines
for clinical research studies and protection of patient
confidentiality.
Table 1 Cardiac defects in 30 enrolled fetuses with congenital heart
defect (CHD)
Pathologies No. observed in 30
fetuses
%
Ventricular septal defect 11 20.8
Aortic arch hypoplasia 5 9.4
Pulmonary stenosis 4 7.5
Hypoplastic left heart syndrome 3 5.7
Abnormal systemic venous return 2 3.8
Complete atrioventricular septal
defect
2 3.8
Partial atrioventricular septal defect 2 3.8
Univentricular heart 2 3.8
Total anomalous pulmonary venous
return
2 3.8
Cardiac tumors 2 3.8
Heterotaxy 2 3.8
Tetralogy of Fallot 2 3.8
Transposition of the great arteries 2 3.8
Ebstein anomaly 1 1.9
Tricuspid atresia 1 1.9
Pulmonary atresia 1 1.9
Dilated cardiomyopathy 1 1.9
Aortic coarctation 1 1.9
Dextrocardia 1 1.9
Atrial septal defect 1 1.9
Mitral valve regurgitation 1 1.9
Tricuspid valve hypoplasia 1 1.9
Apex malposition 1 1.9
Truncus arteriosus 1 1.9
Left ventricular-aortic tunnel 1 1.9
Total 53 100
Table 2 Morphologic defects in 30 enrolled fetuses with congenital
heart defect (CHD)
Pathologies No. observed
in 30 fetuses
%
Dysmorphic face 4 14.3
Low-set ears 3 10.7
Micrognathia 3 10.7
Cleft lip-palate 2 7.1
Cranial suture diastasis 2 7.1
Mongoloid face 2 7.1
Prognathia 2 7.1
Brachycephaly 1 3.6
Face suggestive of catch 22 1 3.6
Clitoral hypertrophy 1 3.6
Labia majora hypertrophy 1 3.6
Nasal bone hypoplasia 1 3.6
Phalanx agenesia 1 3.6
Prominent occiput 1 3.6
Small feet 1 3.6
Small hands 1 3.6
Ulna’s agenesia 1 3.6
Total 28 100
Table 3 Visualization rate and image quality for each cardiac segment in 42 exams
Cardiotoracic
ratio n (%)
Visceral
atrial situs
n (%)
Cardiac
apex
n (%)
Systemic
veins
n (%)
Pulmonary
veins n (%)
Atrioventricular
connection
n (%)
Ventricular
morphology
n (%)
Septum
n (%)
Outflow
tracts
n (%)
Great
arteries
n (%)
Aortic
arch
n (%)
Visualized 32 (76) 23 (55) 39 (93) 25 (60) 8 (19) 31 (74) 33 (79) 34 (81) 33 (79) 31 (74) 9 (21)
Not visualized 10 (24) 19 (45) 3 (7) 17 (40) 34 (81) 11 (26) 9 (21) 8 (19) 9 (21) 11 (26) 33 (79)
Diagnostic 23 (55) 18 (43) 31 (74) 14 (33) 2 (5) 19 (45) 21 (50) 18 (43) 19 (45) 15 (36) 3 (7)
Not diagnostic 19 (45) 24 (57) 11 (26) 28 (67) 40 (95) 23 (55) 21 (50) 24 (57) 23 (55) 27 (64) 39 (93)
Pediatr Cardiol (2011) 32:724–736 725
123
Instrumentation and Data Acquisition
Each exam was performed transabdominally using a Sonos
7500 ultrasound machine (Philips Medical Systems, Bot-
hell, WA, USA) with a cardiac 2D matrix phased array
2–4 MHz transducer (94, Sonos 7500; Philips Medical
Systems) designed for real-time 3D cardiac imaging.
Images were acquired in live 3D mode as a 60� 9 30�pyramid or in full-volume acquisition mode as a 60� 9 60�pyramid [13, 17] . In the latter mode, the data set was
acquired as four 60� 9 15� slices from four different car-
diac cycles and gated to the mother’s electrocardiogram
(ECG).
Images of the heart, head, face, limbs, and genitalia
were obtained at medium- and high-line density, frequency
fusion of 3, gain and compression at midlevel settings,
power output at 0, and time gain compensation (TGC) set
to produce faint intracavitary blood pool echoes.
Offline Processing
Volumetric data sets were stored and evaluated offline by a
pediatric cardiologist with 3D diagnostic imaging experi-
ence. The stored data were manipulated by adjusting gain
and compression, smoothing settings, and using cutting
planes to expose anatomic features.
Data Analysis
The feasibility study investigated the frequency with which
specific cardiac anatomic features and general fetal mor-
phologic features could be displayed in the 3D data set and
the diagnostic quality of the images. First, the fetal cardiac
and overall fetal anatomies were divided into several
domains. For the heart, these included 11 segments:
cardiothoracic ratio, visceral-atrial situs, location of the
cardiac apex, systemic veins, pulmonary veins, atrioven-
tricular connection, ventricles, septum, outflow tracts, great
arteries, and aortic arch. For the general fetal anatomy, we
considered the skull, face, lips, palate, hands, upper limbs,
feet, lower limbs, and genitalia.
Next, the data sets were prospectively examined by a
blinded reviewer (pediatric cardiologist experienced in 3D
fetal imaging) to determine how often the anatomic fea-
tures of each domain were displayed in the 3D data sets
(structure seen or not seen) as well as the diagnostic quality
of the images (seen but not diagnostic). Finally, as com-
plete a diagnosis as possible was formulated from the
review.
The results of the blinded review were compared with
the 2D fetal echocardiogram report to determine what
additional information was provided by the 3D imaging.
The accuracy study involved comparing the diagnoses
based on both the blinded review of the 3D data sets and
the 2D data with the postnatal or fetopsy findings.
Statistical Analysis
Data are presented as raw data and percentages. The sig-
nificance of differences in proportions between groups was
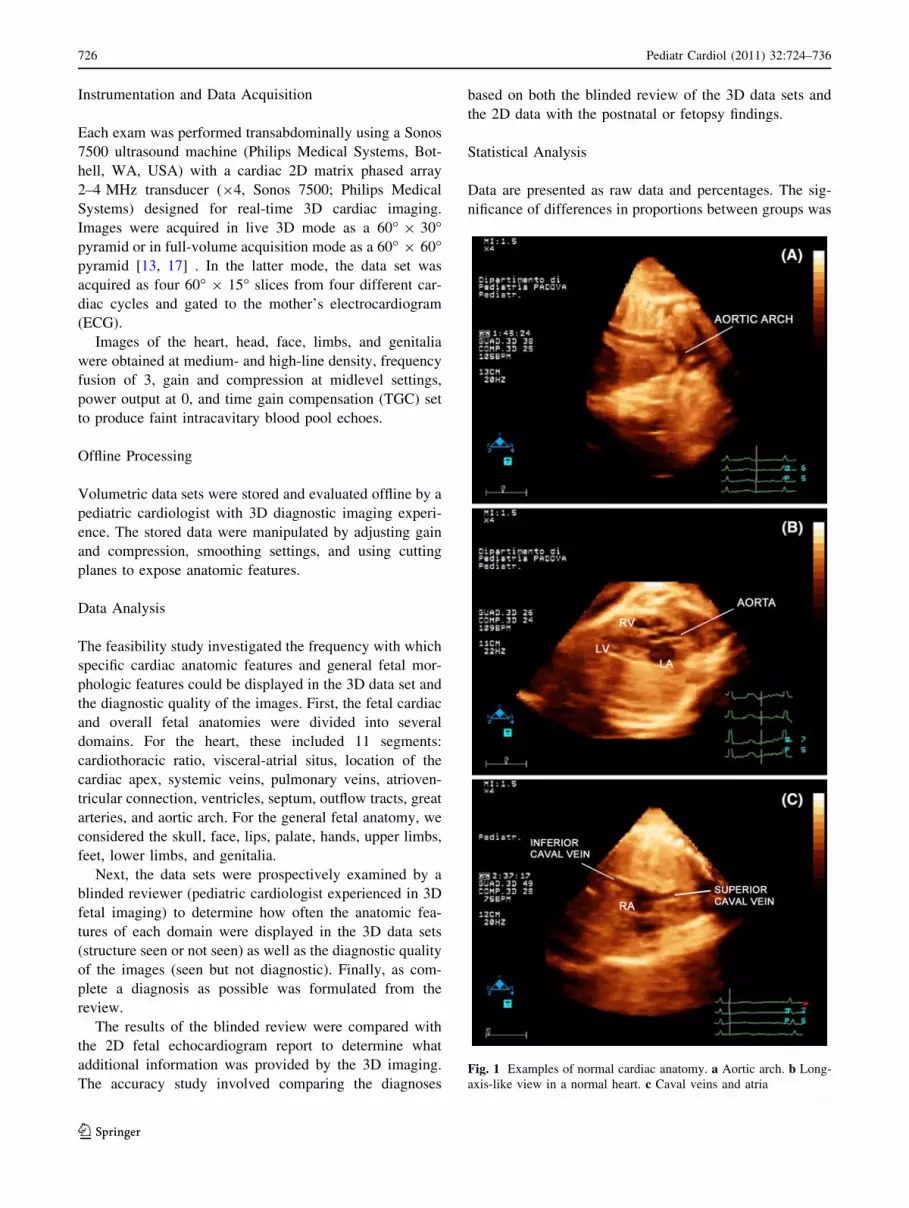
Fig. 1 Examples of normal cardiac anatomy. a Aortic arch. b Long-
axis-like view in a normal heart. c Caval veins and atria
726 Pediatr Cardiol (2011) 32:724–736
123
Ta
ble
4C
om
par
iso
no
fca
rdia
cd
iag
no
ses
infe
tal
thre
e-d
imen
sio
nal
(3D
),fe
tal
2D
,an
dp
ost
nat
al/f
eto
psy
fin
din
gs
No
.o
f
exam
No
.o
f
case
Ges
tati
on
al
wee
k
Dia
gn
ost
icfi
nd
ing
s
3D
Fet
alec
ho
card
iog
rap
hy
2D
Fet
alec
ho
card
iog
rap
hy
Po
stn
atal
/fet
op
sy
Fin
din
gs
11
24
VS
D,
ven
tric
ula
r-ao
rtic
tun
nel
,ao
rtic
atre
sia
VS
D,
ven
tric
ula
r-ao
rtic
tun
nel
VS
D,
ven
tric
ula
r-ao
rtic
tun
nel
,ao
rtic
atre
sia
21
a3
0V
SD
VS
D,
tun
nel
VS
D,
ven
tric
ula
r-ao
rtic
tun
nel
,ao
rtic
atre
sia
32
30
Dis
pro
po
rtio
nao
rta\
pu
lmo
nar
yar
teri
esH
yp
op
last
icao
rtic
arch
Co
arct
atio
n
43
37
Dis
pro
po
rtio
nR
V[
LV
Co
arct
atio
nH
yp
op
last
icao
rtic
arch
54
37
Co
mm
on
AV
SD
and
TO
F,
bal
ance
dv
entr
icle
s,
pu
lmo
nar
yv
alv
est
eno
sis
AV
SD
and
TO
FC
om
mo
nA
VS
Dan
dT
OF
,b
alan
ced
ven
tric
les,
pu
lmo
nar
yv
alv
est
eno
sis
65
21
VS
Dap
ical
,T
OF
,H
yp
op
last
icp
ulm
on
ary
val
ve
TO
FT
OF
,m
ild
pu
lmo
nar
yv
alv
est
eno
sis
75
a2
2N
ET
OF
,m
ild
pu
lmo
nar
yv
alv
est
eno
sis
TO
F,
mil
dp
ulm
on
ary
val
ve
sten
osi
s
86
32
NE
Ao
rtic
val
ve
sten
osi
sH
yp
op
last
icao
rtic
arch
97
31
Co
mp
lete
TG
AC
om
ple
teT
GA
and
larg
eV
SD
Co
mp
lete
TG
Aan
dla
rge
VS
D
10
82
3N
EM
usc
ula
rV
SD
Mu
scu
lar
VS
D
11
8a
30
Mu
scu
lar
VS
DM
usc
ula
rV
SD
Mu
scu
lar
VS
D
12
92
1H
LH
S,
VS
DH
LH
S,
VS
DH
LH
S,
VS
D
13
10
22
NE
HL
HS
No
tav
aila
ble
14
11
23
NE
Rig
ht-
sid
edst
om
ach
,A
VS
D,
RV
giv
ing
rise
on
lyto
aort
icar
ch,
pu
lmo
nar
yat
resi
a
Het
ero
tax
y,
lev
oca
rdia
,b
ilat
eral
SC
Vs,
com
mo
n
AV
val
ve,
2p
ost
erio
rV
SD
can
alty
pe,
pu
lmo
nar
yat
resi
a
15
11
a3
0B
ilat
eral
SC
Vs,
AV
SD
,R
Vg
ivin
gri
seo
nly
to
aort
icar
ch,
pu
lmo
nar
yat
resi
a,
Sit
us
inv
ersu
s,A
VS
D,
RV
giv
ing
rise
on
lyto
aort
icar
ch,
pu
lmo
nar
yat
resi
a
Het
ero
tax
y,
lev
oca
rdia
,b
ilat
eral
SC
Vs,
Co
mm
on
AV
val
ve,
2p
ost
erio
rV
SD
can
alty
pe,
pu
lmo
nar
yat
resi
a
16
12
32
Rh
abd
om
yo
mas
,in
flo
w-o
utfl
ow
no
to
bst
ruct
edR
hab
do
my
om
as,
infl
ow
-ou
tflo
wn
ot
ob
stru
cted
Rh
abd
om
yo
mas
,in
flo
w-o
utfl
ow
no
to
bst
ruct
ed
17
12
a3
7R
hab
do
my
om
as,
infl
ow
-ou
tflo
wn
ot
ob
stru
cted
Rh
abd
om
yo
mas
,in
flo
w-o
utfl
ow
no
to
bst
ruct
edR
hab
do
my
om
as,
infl
ow
-ou
tflo
wn
ot
ob
stru
cted
18
13
20
Sin
gle
ven
tric
leh
eart
Sin
gle
ven
tric
leh
eart
,su
bp
ulm
on
ary
sten
osi
sN
ot
avai
lab
le
19
14
24
HL
HS
,sm
all
aort
icar
ch,
pu
lmo
nar
yv
ein
sn
ot
seen
Hy
po
pla
stic
mit
ral
val
ve,
HL
HS
,h
yp
op
last
ic
asce
nd
ing
aort
icar
ch.
TP
AV
C
HL
HS
,ao
rtic
val
ve
atre
sia,
hy
po
pla
stic
asce
nd
ing
aort
icar
ch
20
14
a3
0H
LH
S,
smal
lao
rtic
arch
,p
ulm
on
ary
vei
ns
no
t
seen
Hy
po
pla
stic
mit
ral
val
ve,
HL
HS
,h
yp
op
last
ic
asce
nd
ing
aort
icar
chT
PA
VC
HL
HS
,ao
rtic
val
ve
atre
sia,
hy
po
pla
stic
asce
nd
ing
aort
icar
ch
21
15
19
TG
A,
VS
DH
yp
op
last
icm
itra
lv
alv
e,h
yp
op
last
icL
V,
TG
A,
VS
D
Hy
po
pla
stic
LV
,T
GA
,V
SD
22
16
24
Ap
exm
alp
osi
tio
nA
pex
mal
po
siti
on
No
tav
aila
ble
23
17
20
Sm
all
VS
DS
mal
lV
SD
Sm
all
VS
D
24
18
20
VS
DE
bst
ein
ano
mal
yE
bst
ein
ano
mal
y
25
18
a2
7M
ild
Eb
stei
nan
om
aly
,n
oV
SD
Eb
stei
nan
om
aly
Mil
dE
bst
ein
ano
mal
y
26
19
32
AV
SD
par
tial
/in
term
ediu
m,
2d
iffe
ren
tv
alv
e
AV
,p
rob
able
mit
ral-
clef
t,A
SD
pri
mu
m
AV
SD
par
tial
AV
SD
par
tial
/in
term
ediu
m,
2d
iffe
ren
tv
alv
e
AV
,p
rob
able
mit
ral-
clef
t,A
SD
pri
mu
m
Pediatr Cardiol (2011) 32:724–736 727
123

Ta
ble
4co
nti
nu
ed
No
.o
f
exam
No
.o
f
case
Ges
tati
on
al
wee
k
Dia
gn
ost
icfi
nd
ing
s
3D
Fet
alec
ho
card
iog
rap
hy
2D
Fet
alec
ho
card
iog
rap
hy
Po
stn
atal
/fet
op
sy
Fin
din
gs
27
20
16
Dex
tro
card
iaH
yp
op
last
icao
rta
and
LV
,H
yp
op
last
icm
itra
l
val
ve
Dex
tro
card
ia,
inte
rru
pte
dIC
V,
pat
ent
left
SC
V,
abse
nt
rig
ht
VC
S,
TP
AV
C,
AV
SD
,d
ysp
last
ic
pu
lmo
nar
yv
alv
e,ap
ical
VS
D
28
20
a2
9D
extr
oca
rdia
,p
aten
tle
ftS
CV
,A
VS
DS
itu
sso
litu
s/am
big
uo
us,
inte
rru
pte
dIC
V,
Par
tial
AV
PC
,ri
gh
td
om
inan
tA
VS
D,
dy
spla
stic
pu
lmo
nar
yv
alv
e
Dex
tro
card
ia,
inte
rru
pte
dIC
V,
pat
ent
left
SC
V,
abse
nt
rig
ht
VC
S,
TP
AV
C,
AV
SD
,d
ysp
last
ic
pu
lmo
nar
yv
alv
e,ap
ical
VS
D
29
21
26
Inte
rru
pte
dao
rtic
arch
Hy
po
pla
stic
aort
icar
ch,
VS
DH
yp
op
last
icao
rtic
arch
,la
rge
VS
D
30
22
23
NE
Sm
all
VS
D,
hy
po
pla
stic
aort
icar
ch/c
oar
ctat
ion
TP
AV
C,
hy
po
pla
stic
tran
sver
seao
rtic
arch
31
22
a2
8N
E,
sug
ges
tiv
eo
fT
PA
VC
Sm
all
VS
D,
hy
po
pla
stic
aort
icar
ch/c
oar
ctat
ion
TP
AV
C,
hy
po
pla
stic
tran
sver
seao
rtic
arch
32
23
26
Po
ster
ior
VS
D,
can
alty
pe
Po
ster
ior
VS
D,
can
alty
pe
Po
ster
ior
VS
D,
can
alty
pe
33
23
a3
4P
ost
erio
rV
SD
,ca
nal
typ
eP
ost
erio
rV
SD
,ca
nal
typ
eP
ost
erio
rV
SD
,ca
nal
typ
e
34
24
28
Su
bp
ulm
on
ary
VS
DS
ub
pu
lmo
nar
yV
SD
Su
bp
ulm
on
ary
VS
D
35
25
22
Tri
cusp
idat
resi
aT
ricu
spid
atre
sia
Tri
cusp
idat
resi
a
36
25
a3
2T
ricu
spid
atre
sia,
bu
lbo
ven
tric
ula
rfo
ram
en,
seco
nd
ary
cham
ber
Tri
cusp
idat
resi
aT
ricu
spid
atre
sia
37
26
21
Sin
gle
ven
tric
leh
eart
,h
yp
op
last
ictr
icu
spid
val
ve
Tri
cusp
idat
resi
aS
ing
lev
entr
icle
hea
rt,
hy
po
pla
stic
tric
usp
id
val
ve
38
26
a3
0S
ing
lev
entr
icle
hea
rt,
hy
po
pla
stic
tric
usp
id
val
ve
Sin
gle
ven
tric
leh
eart
,h
yp
op
last
ictr
icu
spid
val
ve
Sin
gle
ven
tric
leh
eart
,h
yp
op
last
ictr
icu
spid
val
ve
39
27
30
VS
Ds
Mit
ral
val
ve
reg
urg
itat
ion
,p
ulm
on
ary
val
ve
sten
osi
s
Mit
ral
val
ve
reg
urg
itat
ion
,p
ulm
on
ary
val
ve
sten
osi
s
40
28
32
Car
dio
meg
aly
Car
dio
meg
aly
Car
dio
meg
aly
41
29
21
Tru
ncu
sar
teri
osu
sty
pe
1T
run
cus
arte
rio
sus
Tru
ncu
sar
teri
osu
sty
pe
I
42
30
32
Rh
abd
om
yo
mas
Rh
abd
om
yo
mas
,in
flo
w-o
utfl
ow
trac
tn
ot
ob
stru
cted
Rh
abd
om
yo
mas
,in
flo
w-o
utfl
ow
trac
tn
ot
ob
stru
cted
VS
Dv
entr
icu
lar
sep
tal
def
ect,
LV
left
ven
tric
le,
RV
rig
ht
ven
tric
le,
AV
SD
atri
ov
entr
icu
lar
sep
tal
def
ect,
TO
Fte
tral
og
yo
fF
allo
t,N
Ed
iag
no
stic
hy
po
thes
isn
ot
exp
ress
ible
,T
GA
tran
spo
siti
on
of
the
gre
atar
teri
es,
HL
HS
hy
po
pla
stic
left
hea
rtsy
nd
rom
e,S
CV
sup
erio
rca
val
vei
n,
TP
AV
Cto
tal
pu
lmo
nar
yan
om
alo
us
vei
nco
llec
t,A
SD
atri
alse
pta
ld
efec
t,IC
Vin
feri
or
cav
alv
ein
aF
oll
ow
-up
exam
inat
ion
728 Pediatr Cardiol (2011) 32:724–736
123

tested using the chi-square test or Fisher’s test. A p value
less than 0.05 was considered statistically significant.
Results
Patients
Of the 230 fetuses scanned between October 2008 and
February 2009, 35 (15%) had a CHD diagnosed by 2D fetal
echocardiography. The gestational ages ranged from 16 to
38 weeks (mean, 24.4 weeks; median, 23 weeks). Of the
35 parents, 30 gave consent for the 3D ultrasonography
evaluation and were enrolled in the study. We performed
12 follow-up exams, for a total of 42 examinations in 30
fetuses. The number of acquisitions ranged from 1 to 6
(average, 2.5; median, 2) for the cardiac domains and from
1 to 15 (average, 5; median, 5) for the fetal morphologic
domains. The 3D acquisitions required an average of 4 min
(range, 3–6 min), whereas the postprocessing and analysis
required a longer time, 20–55 min (average, 35 min).
The outcome of the pregnancies was 24 live-born infants
and six voluntary terminations of pregnancy. Postnatal or
fetopsy data were available for 23 of the 24 neonates and
for four of the six abortions. These data showed a wide
spectrum of cardiac defects, with some fetuses having more
than one defect (Table 1). Nine fetuses had a total of 28
extracardiac abnormalities, suggesting a syndrome in eight
fetuses (Table 2).
Heart Segments
The rate for visualization of the 11 cardiac segments was
highly variable, ranging from 19 to 93% (Table 3). Fig-
ure 1 presents examples of normal cardiac anatomy. The
aortic arch (21%) and the pulmonary veins (19%) were the
least consistently imaged, whereas the atrioventricular
canal, ventricles, outflows, and great arteries were imaged
in 74–93% of cases. Diagnostic quality images were
obtained in fewer segments (5–55%) (Table 3), but the rate
of obtaining diagnostic images was higher if at least three
acquisitions were performed during the exam (p \ 0.01;
p value, 0.000008). Images were more likely to be diag-
nostic after 24 weeks of gestation (p \ 0.01; p value,
0.00007) due to the intrinsic resolution of the 3D matrix
probe and the smaller dimension of the heart in younger
fetuses.
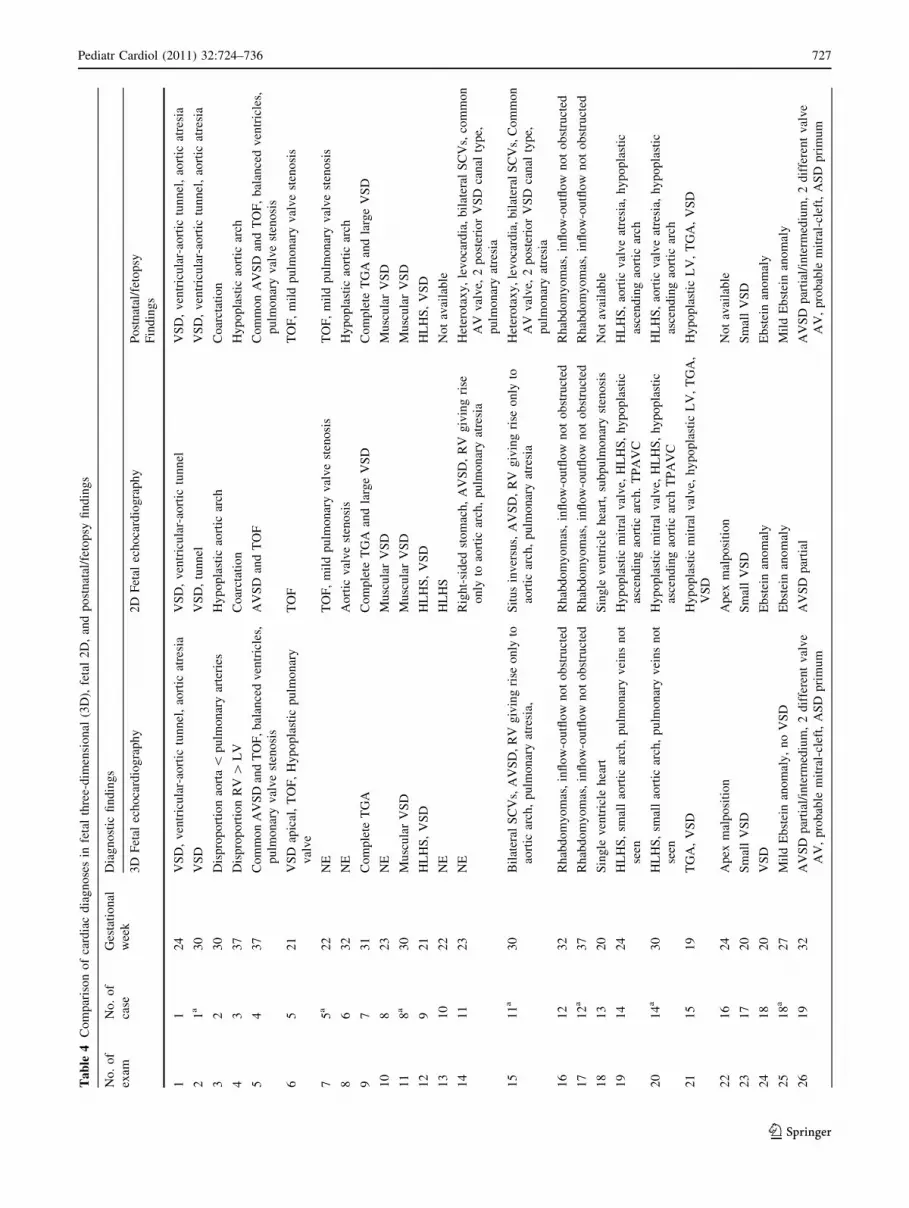
Compared with postnatal or fetopsy findings, the 3D
echo was completely diagnostic in 17 exams (44%), par-
tially diagnostic in 14 exams (36%), and not diagnostic in 8
exams (20%). As analyzed by patient, combining all the
exams performed for a single patient, the 3D exam was
completely diagnostic in 52%, partially diagnostic in 37%,
and nondiagnostic in 11% of cases (see Table 4 compari-
son of 2D and 3D postnatal findings). Compared with the
2D ultrasonography, the 3D exam provided additional
information about the cardiac defects in 28% of cases.
Fetal Morphology
Again, substantial variability was noted among the fetal
morphology domains for visualization, ranging from 25%
for the feet to 86% for the face (Table 5). See the examples
of normal morphologic features in Fig. 2. Diagnostic
images were obtained in slightly fewer domains: 18% for
the feet to 60% for the skull (Table 5). In general, the face,
lip, palate, and skull were more often imaged than the
limbs and genitalia, and the images were more often
diagnostic, probably due to the lower number of specific
acquisitions for these latter structures. More acquisitions
per exam and gestational age younger than 24 weeks were
associated with a higher likelihood of obtaining diagnostic
images (p value, 0.000015 for gestational weeks fewer than
24; p value, 0.000035 for more than 4 acquisitions). In
contrast to the heart, the somatic anatomy was better
imaged in younger fetuses, whose bodies were more
completely enclosed in the 3D sector.
The postnatal or fetopsy findings disclosed 28 extra-
cardiac malformations in nine infants or aborted fetuses
(Table 2). The 3D images suggested that multiple malfor-
mations were present in eight fetuses of the nine cases and
that a syndrome likely was present in seven cases (in
Table 6 see comparison of 2D and 3D postnatal findings).
Images of the malformation were obtained for 23 (82%) of
Table 5 Visualization rate and image quality for each morphologic segment in 42 exams
Skull
n (%)
Face
n (%)
Lips and
palate n (%)
Hands
n (%)
Superior limbs
n (%)
Feet
n (%)
Inferior limbs
n (%)
Genitalia
n (%)
Visualized 29 (69) 36 (86) 34 (81) 22.5 (54) 17.5 (42) 10.5 (25) 17.5 (42) 22 (52)
Not visualized 13 (31) 6 (14) 8 (19) 19.5 (46) 24.5 (58) 31.5 (75) 24.5 (58) 20 (48)
Diagnostic 25 (60) 22 (52) 28 (67) 11.5 (27) 15 (36) 7.5 (18) 14.5 (35) 20 (48)
Not diagnostic 17 (40) 20 (48) 14 (33) 30.5 (73) 27 (64) 34.5 (82) 27.5 (65) 22 (52)
a Considering limbs, feet and hands, we counted 0.5 for each single segment
Pediatr Cardiol (2011) 32:724–736 729
123

the 28 anomalies present. A complete diagnosis was pos-
sible for 16 malformations (57%), a partial diagnosis for
seven malformations (25%), and no diagnosis in three
cases (11%). Two anomalies (7%) were misdiagnosed: a
fetus with hypertrophy of the labia majora was diagnosed
as normal, and clinodactyly was incorrectly diagnosed in a
fetus with small hands at birth. In general, skull anomalies
(micrognathia, prognathia, brachycephaly, cranial suture
diastase), facial anomalies (low-set ears, dysmorphic face),
and cleft lips and palate were more readily detected than
abnormalities of the limbs or genitalia. Figure 3 shows a
cleft lip diagnosed with 3D examination. More examples of
diagnostic findings are discussed later.
Discussion and Conclusions
This study demonstrated that 3D ultrasonography can
diagnose many cardiac defects, and in nearly one-third
Fig. 2 Normal fetal
morphology visualized with
three-dimensional
ultrasonography (3DUS).
a, b Face. c Hands. d Female
genitalia. e Male genitalia
730 Pediatr Cardiol (2011) 32:724–736
123

Ta
ble
6C
om
par
ing
extr
acar
dia
cd
iag
no
ses
infe
tal
thre
e-d
imen
sio
nal
(3D
)an
dp
ost
nat
al/p
ost
abo
rtio
nfi
nd
ing
s
No
.o
f
exam
No
.o
f
case
Ges
tati
on
al
wee
k
Mal
form
ed
fetu
s
Dia
gn
ost
icfi
nd
ing
s
Ind
icat
ion
tofe
tal
ech
oca
rdio
gra
ph
y3
DF
etal
dia
gn
osi
sP
ost
nat
al/p
ost
abo
rtio
n
54
37
1S
usp
ect
CH
DN
EM
on
go
loid
face
,n
uch
alfo
ld,
AS
D,
TO
F:
Do
wn
syn
dro
me
6,
75
21
,2
22
Su
spec
tC
HD
Fac
esu
gg
esti
ve
of
mic
rod
elet
ion
22
q1
1F
ace
sug
ges
tiv
eo
fm
icro
del
etio
n2
2q
11
,T
OF
10
,1
18
23
–3
03
Su
spec
tC
HD
,m
icro
gn
ath
ia,
nu
chal
cyst
ich
yg
rom
a,IU
GR
Mic
rog
nat
hia
,d
iast
atic
sag
itta
lsu
ture
,
clin
od
acty
ly
Mic
rog
nat
hia
,d
iast
atic
sag
itta
lan
dm
eto
pic
sutu
re,
mic
roce
ph
aly
,sy
no
ph
rys,
hy
per
tric
ho
sis,
low
-set
ear,
smal
lfe
etan
d
han
ds,
VS
D:
Co
rnel
iad
eL
ang
esy
nd
rom
e
12
92
14
Su
spec
tC
HD
Pro
gn
ath
ia,
flat
nas
alro
ot,
lon
gan
dth
in
no
sefi
lter
,lo
w-s
etea
rs
Dy
smo
rph
icfa
ce,
low
-set
ears
,T
GA
,V
SD
21
15
19
5S
usp
ect
CH
D,m
icro
gn
ath
ia,ag
enes
iao
fa
fore
arm
seg
men
t
Mic
rog
nat
hia
,ag
enes
iao
fa
fore
arm
seg
men
t,an
om
alo
us
han
d
Mic
rog
nat
hia
,lo
w-s
etea
rs,
agen
esia
of
1
ph
alan
xo
fle
fth
and
,ag
enes
iao
fle
ftu
lna,
hy
po
pla
sia
of
left
rad
ius,
hy
po
pla
sia
LV
,T
GA
,
VS
D
23
17
20
?3
6:N
T3
,37
,si
ng
leu
mb
ilic
alar
tery
,
sto
mac
hn
ot
vis
ual
ized
Mic
rog
nat
hia
,b
rach
yce
ph
aly
,p
rom
inen
t
occ
ipu
t,d
iast
atic
sag
itta
lsu
ture
,cl
eft
lip
Dy
smo
rph
icsk
ull
and
face
,cl
eft
lip
,
hy
po
telo
rism
,re
nal
ano
mal
ies,
VS
D:
Ed
war
ds
syn
dro
me
30
,3
12
22
3–
28
7S
usp
ect
CH
DD
ysm
orp
hic
face
,p
rog
nat
hia
,an
om
alo
us
gen
ital
ia
Mic
rop
hth
alm
ia,
sun
ken
eyes
,h
yp
ertr
ich
osi
s,
pro
gn
ath
ia,
hy
per
tro
ph
yo
fth
ecl
ito
ris,
TP
AV
C:
Tra
nsl
oca
tio
nt(
4:1
5)
32
,3
32
32
6–
34
8S
usp
ect
CH
DH
yp
op
last
icn
asal
bo
ne,
up
war
dsl
ant
to
the
eye,
epic
anth
icfo
ldo
fth
eey
elid
,
ten
t-sh
aped
lip
s
Mo
ng
olo
idfa
ce,
lab
iam
ajo
ra,
hy
per
tro
ph
y,
VS
D:
Do
wn
syn
dro
me
35
,3
62
52
2–
32
9S
usp
ect
CH
DC
left
lip
,cl
eft
pal
ate
Cle
ftli
p,
clef
tp
alat
e,tr
icu
spid
atre
sia
CH
Dco
ng
enit
alh
eard
def
ect,
NE
dia
gn
ost
ich
yp
oth
esis
no
tex
pre
ssib
le,
AV
SD
atri
ov
entr
icu
lar
sep
tal
def
ect,
TO
Fte
tral
og
yo
fF
allo
t,IU
GR
intr
aute
rin
eg
row
thre
stri
ctio
n,
TG
Atr
ansp
osi
tio
n
of
the
gre
atar
teri
es,
VS
Dv
entr
icu
lar
sep
tal
def
ect,
LV
left
ven
tric
le,
TP
AV
Cto
tal
pu
lmo
nar
yan
om
alo
us
vei
nco
llec
t
Pediatr Cardiol (2011) 32:724–736 731
123

of cases adds significant information to that obtained by
2D imaging. Furthermore, 3D ultrasonography can
detect extracardiac defects in the majority of patients
and can suggest the presence of malformation syn-
dromes. Image acquisition is rapid, minimally prolong-
ing the exam. Processing and analysis of the images
require more time and expertise, but the yield is pro-
portionally greater.
Although a number of reports [2, 18, 21, 22, 25, 26, 29]
have indicated advantages for 3D fetal imaging over 2D
imaging similar to those described in this report, a clear
role for 3D fetal imaging has yet to be established. Our
experience gives us the impression that 3D imaging is one
step closer to a direct physical examination of the fetus.
Just as the physical exam cannot always diagnose the
specific syndrome and must be confirmed by other means
such as karyotyping, so too, 3D ultrasonography requires
confirmation. In fact, a syndrome was suspected in eight of
nine fetuses, and a specific diagnosis was suggested in two
fetuses.
Examples of Syndromes Detected by 3D
Ultrasonography
Example 1 (Case 23 in Table 6)
A 3D exam performed at 23 gestational weeks because of
suspected CHD (and no other anomalous finding on 2D
examination) showed a hypoplastic nasal bone, upward
slant to the eyes, epicanthal folds of the eyelids, and an
anomalous oral fissure (tent-shaped lips), suggesting tri-
somy 21, which was confirmed at birth (Fig. 4).
Example 2 (Case 17 in Table 6)
A 3D examination of a 20-week-old fetus for high nuchal
translucency and single umbilical artery showed brachy-
cephaly, micrognathia, prominent occiput, diastatic sagittal
suture, and cleft lip. These findings suggested Edwards
syndrome (Fig. 5), which was confirmed by amniocentesis
and fetopsy.
Example 3 (Case 15 in Table 6)
The 3D images of a skeletal malformation in a 19-week-old
fetus with the 2D diagnosis of suspected CHD, microgna-
thia, and agenesia demonstrated micrognathia and an
anomalous left arm (Fig. 6a, b). A lateral view of the left
arm showed absence of the ulna (Fig. 6c, d).
Example 4 (Case 8 in Table 6)
The 3D examination of skull malformation in a 23-week-old
fetus detected micrognathia, diastatic sagittal suture, and
low-set ears (Fig. 7). Cornelia de Lange syndrome was
diagnosed postnatally, characterized by microcephaly,
micrognathia, small feet and hands, low-set ears, sagittal and
metopic diastatic suture, synophrys, and hypertrichosis.
The only fetus in which a syndrome was not detected
presented at 37 gestational weeks when adequate images of
the head and face could not be obtained. The most diag-
nostic images for general fetal morphology were obtained
in younger fetuses, generally before 24 gestational weeks
when termination of pregnancy still was an option.
In contrast to fetal morphology imaging, the cardiac
diagnostic definition was better for older fetuses, after 24
gestational weeks. This temporal limitation somehow
decreases the impact of 3D ultrasonography on the defi-
nition of the fetal cardiac anatomy. Three-dimensional
cardiac imaging was most useful for atrioventricular valves
and outflows.
Fig. 3 a Cleft lip well highlighted with three-dimensional ultraso-
nography (3DUS). b Postnatal comparison
732 Pediatr Cardiol (2011) 32:724–736
123

Examples of important new findings from the 3D exam
not present on the 2D ultrasonogram include a patent but
hypoplastic tricuspid valve in a fetus with a diagnosis of
tricuspid atresia by 2D ultrasonography (case 26 in
Table 4, Fig. 8, video 1 in supplementary material), dex-
trocardia in a fetus at 16 weeks of gestational age not
detected by 2D (case 20 in Table 4, Fig. 9, video 2 in
supplementary material), and aortic valve atresia in a
patient with aorto left ventricular tunnel (case 1 in Table 4,
Fig. 10, video 3 in supplementary material).
Adequate images of the aortic arch and the pulmonary
veins were rarely obtained, in part due to the lack of
dedicate acquisitions. A false image of a ventricular septal
defect (Fig. 11) occurred for one fetus, indicating a limi-
tation of this technique.
Despite the relative low surplus value of 3D versus 2D
ultrasonography with regard to the cardiac anatomy, we
think that what parents want to know above all is whether
their child will live a normal life. Therefore, the capability
of 3D imaging to detect features suggestive of genetic and
chromosomal syndromes is not of secondary importance.
Considering the high rate of such syndromes in fetuses
affected by CHD, we believe that a thorough 3D study
would be advisable for all the fetuses with a diagnosis of
CHD.
Even if the new generation of real-time 3D echocardi-
ography equipment allows a quicker reconstruction of the
image, we believe that 2D study will remain the first-line
approach for pediatric cardiologists studying the fetal heart,
whereas 3D ultrasonography should be reserved for all
cases in which a cardiac anomaly is detected.
In conclusion, our findings indicate that 3D fetal ultra-
sonography is a valuable tool for comprehensive evaluation
of the fetus. Besides providing information on the heart
anatomy using the three planes of space not obtainable with
2D echocardiography, it allows important features of the
somatic anatomy to be depicted in most cases. It thus
identifies those fetuses in whom a syndromic setting is
more likely present, allowing parents to receive more
Fig. 4 Down syndrome. b A three-dimensional (3D) exam of a
23-week-old fetus with suspected congenital heart defect (CHD)
showing hypoplastic nasal bone, upward slant to the eyes, epicanthal
folds of the eyelids, and an anomalous oral fissure (tent-shaped lips).
These findings suggest trisomy 21, which was confirmed at birth.
Note the normal nasal bone (a) compared with hypoplastic nasal bone
(b), and the postnatal view of the same patient (c)
Fig. 5 Edwards syndrome. A three-dimensional (3D) exam per-
formed at 20 gestational weeks (GW) because of high nuchal
translucency and a single umbilical artery shows brachicephaly,
micrognathia, prominent occiput, diastatic sagittal suture, and cleft
lip, suggesting Edwards syndrome, which was confirmed by amnio-
centesis and fetopsy
Pediatr Cardiol (2011) 32:724–736 733
123

Fig. 6 A 19-week-old fetus
with a two-dimensional (2D)
diagnosis of suspected
congenital heart defect (CHD),
micrognathia, and agenesia of
the ulna. The 3D images
demonstrate micrognathia
(a) and anomalous left arm (b).
The lateral view of the left arm
shows absence of the ulna (c, d)
Fig. 7 Cornelia de Lange
syndrome. a A three-
dimensional (3D) exam
performed at 23 gestational
weeks (GW) showing
micrognathia, diastatic sagittal
suture, and low-set ears.
Cornelia de Lange syndrome
was diagnosed postnatally,
characterized by microcephaly,
micrognathia, small feet and
hands, low-set ears, sagittal and
metopic diastatic suture,
synophrys, and hypertrichosis.
b Postnatal comparison
Fig. 8 Tricuspid hypoplasia in
a fetus (32 weeks gestational
age) affected by a univentricular
heart. The two-dimensional
(2D) image suggests tricuspid
atresia, whereas the 3D study at
the valvular plane demonstrated
that this valve was hypoplastic
but patent (refer video 1)
734 Pediatr Cardiol (2011) 32:724–736
123

comprehensive prenatal counseling, including the manda-
tory necessity of karyotyping in these specific cases. It is
useful to remember that the malformative syndrome rate is
very high for patients affected by CHD, accounting for
almost 25% of live-borns, and 70% of spontaneous abor-
tions and stillborns.
Fig. 9 Dextrocardia in a
16-week-old fetus clearly
showing the head, chest, and
heart (refer video 2)
Fig. 10 Valvular plane in a
24-week-old fetus affected by
aorto left ventricular tunnel,
ventricular septal defect, and
aortic atresia. a, b, c,
d Pulmonary valve (PA)
opening and closing according
to the cardiac cycle. The tunnel
is recognizable as a small
opening next to the aortic valve,
which is seen always closed and
firm. A clear view of this detail
was obtained only
retrospectively during a blind
review of the pediatric
cardiologist expert on three-
dimensional (3D) echo. The
atresia of the aortic valve was
not recognized on 2D
echocardiography but
discovered at the operating
table, with important clinical
implication. The understanding
of this defect would have
changed the surgical approach,
consequently improving the
outcome (refer video 3)
Fig. 11 False image of
ventricular septal defect (VSD).
a Labeled view of a false image
of apical VSD, referring to a
fetus of 21 gestational weeks
(GW) affected by tetralogy of
Fallot. Two apparent VSDs
seem well detectable, but only
one really exists. b Same image,
not labeled
Pediatr Cardiol (2011) 32:724–736 735
123

To our knowledge, this is the first study to outline the
role of 3D ultrasonography in a pediatric cardiology fetal
unit. With its specific limitations kept in mind, 3D ultra-
sonography should became a routine tool in the arma-
mentarium of the pediatric cardiologist, together with other
methods for fetal diagnosis.
Acknowledgment The authors gratefully acknowledge professor
Stephen P. Sanders for his valuable assistance in reviewing the
manuscript.
References
1. Baba K, Satoh K, Sakamoto S, Okai T, Ishii S (1989) Develop-
ment of an ultrasonic system for three-dimensional reconstruction
of the fetus. J Perinat Med 17:19–24
2. Bega G, Kuhlman K, Lev-Toaff A, Kurtz A, Wapner R (2001)
Application of three-dimensional ultraultrasonography in the
evaluation of the fetal heart. J Ultrasound Med 20:307–313
3. Bega G, Lev-Toaff A, Kuhlman K, Kurtz A, Goldberg B, Wapner
R (2001) Three-dimensional ultrasonographic imaging in
obstetrics: present and future applications. J Ultrasound Med 20:
391–408
4. Benacerraf BR (2002) Three-dimensional fetal ultrasonography:
use and misuse. J Ultrasound Med 21:1063–1067
5. Chaoui R, Kalache KD, Hartung J (2001) Application of three-
dimensional power Doppler ultrasound in prenatal diagnosis.
Ultrasound Obstet Gynecol 17:22–29
6. De Luca I (1999) Ecocardiografia fetale. In: Nicolosi GL (ed)
Trattato di ecocardiografia clinica 1999, vol 3. Piccin Publ,
Padova, pp 1983–2033
7. Deng J, Birkett AG, Kalache KD, Hanson MA, Peebles DM,
Linney AD et al (2001) Conversion of umbilical arterial Doppler
waveforms to cardiac cycle triggering signals: a preparatory study
for online motion-gated three-dimensional fetal echocardiogra-
phy. Ultrasound Med Biol 27:51–59
8. Deng J, Sullivan ID, Yates R, Vogel M, Mcdonald D, Linney AD
et al (2002) Real-time three-dimensional fetal echocardiography:
optimal imaging windows. Ultrasound Med Biol 28:1099–1105
9. DeVore GR, Falkensammer P, Sklansky MS, Platt LD (2003)
Spatiotemporal image correlation (STIC): a new technology for
evaluation of the fetal heart. Ultrasound Obstet Gynecol 22:380–
387
10. DeVore GR (2005) Three-dimensional and four-dimensional fetal
echocardiography: a new frontier. Curr Opin Pediatr 17:592–604
11. Espinoza J, Goncalves LF, Lee W, Mazor M, Romero R (2005) A
novel method to improve prenatal diagnosis of abnormal systemic
venous connections using three- and four-dimensional ultraultr-
asonography and ‘‘inversion mode’’. Ultrasound Obstet Gynecol
25:428–434
12. Ewigman BG, Crane JP, Frigoletto FD, LeFevre ML, Bain RP,
McNellis D (1993) Effect of prenatal ultrasound screening on
perinatal outcome. RADIUS study group. N Engl J Med 329:
821–827
13. Goncalves LF, Espinoza J, Kusanovic JP, Lee W, Nien JK,
Santolaya-Forgas J et al (2006) Applications of 2D matrix array
for 3D and 4D examination of the fetus: a pictorial essay.
J Ultrasound Med 25:745–755
14. Goncalves LF, Espinoza J, Lee W, Mazor M, Romero R (2004)
Three- and four-dimensional reconstruction of the aortic and
ductal arches using inversion mode: a new rendering algorithm
for visualization of fluid-filled anatomical structures. Ultrasound
Obstet Gynecol 24:696–698
15. Goncalves LF, Romero R, Espinoza J, Lee W, Treadwell M,
Chintala K et al (2004) Four-dimensional ultrasonography of the
fetal heart using color Doppler spatiotemporal image correlation.
J Ultrasound Med 23:473–481
16. Herberg U, Goldberg H, Breuer J (2003) Dynamic free-hand
three-dimensional fetal echocardiography gated by cardiotocog-
raphy. Ultrasound Obstet Gynecol 22:493–502
17. Houck RC, Cooke JE, Gill EA (2006) Live 3D echocardiography:
a replacement for traditional 2D echocardiography? AJR Am J
Roentgenol 187:1092–1106
18. Levental M, Pretorius DH, Sklansky MS, Budorick NE, Nelson
TR, Lou K (1998) Three-dimensional ultrasonography of normal
fetal heart: comparison with two-dimensional imaging. J Ultra-
sound Med 17:341–348
19. Levi S (2002) Ultrasound in prenatal diagnosis: polemics around
routine ultrasound screening for second trimester fetal malfor-
mations. Prenat Diagn 22:285–295
20. Linney AD, Deng J (1999) Three-dimensional morphometry in
ultrasound. Proc Inst Mech Eng H 213:235–245
21. Meyer-Wittkopf M, Cook A, McLennan A, Summers P, Sharland
GK, Maxwell DJ (1996) Evaluation of three-dimensional ultra-
sonography and magnetic resonance imaging in assessment of
congenital heart anomalies in fetal cardiac specimens. Ultrasound
Obstet Gynecol 8:303–308
22. Meyer-Wittkopf M, Rappe N, Sierra F, Barth H, Schmidt S
(2000) Three-dimensional (3D) ultrasonography for obtaining the
four and five-chamber view: comparison with cross-sectional
(2D) fetal sonographic screening. Ultrasound Obstet Gynecol
15:397–402
23. Nelson TR, Pretorius DH, Sklansky M, Hagen-Ansert S (1996)
Three-dimensional echocardiographic evaluation of fetal heart
anatomy and function: acquisition, analysis, and display. J Ultra-
sound Med 15:1–9
24. Scharf A, Geka F, Steinborn A, Frey H, Schlemmer A, Sohn C
(2000) 3D real-time imaging of the fetal heart. Fetal Diagn Ther
15:267–274
25. Sklansky MS, Nelson TR, Pretorius DH (1998) Three-dimen-
sional fetal echocardiography: gated versus non gated techniques.
J Ultrasound Med 17:451–457
26. Sklansky MS, Nelson TR, Pretorius DH (1997) Usefulness of
gated three-dimensional fetal echocardiography to reconstruct
and display structures not visualized with two-dimensional
imaging. Am J Cardiol 80:665–668
27. Tutschek B, David JS (2007) Three-dimensional echocardiogra-
phy for studies of the fetal heart: present status and future per-
spectives. Cardiol Clin 25:341–355
28. Yagel S, Cohen SM, Shapiro I, Valsky DV (2007) 3D and 4D
ultrasound in fetal cardiac scanning: a new look at the fetal heart.
Ultrasound Obstet Gynecol 29:81–95
29. Zosmer N, Jurkovic D, Jauniaux E, Gruboeck K, Lees C,
Campbell S (1996) Selection and identification of standard car-
diac views from three-dimensional volume scans of the fetal
thorax. J Ultrasound Med 15:25–32
736 Pediatr Cardiol (2011) 32:724–736
123




















![[I Brazilian consensus of endoscopic ultrasonography]](https://img.dokumen.tips/doc/110x75/634ac5bce2b881b8bf0189bc/i-brazilian-consensus-of-endoscopic-ultrasonography.jpg)








