Embed Size (px)
Citation preview

Biomaterials 25 (2004) 1959–1967
ARTICLE IN PRESS
*Correspondin
8347-203.
E-mail addres
0142-9612/$ - see
doi:10.1016/j.bio
Ultrastructural characterization of the implant/bone interface ofimmediately loaded dental implants
U. Meyera,*, U. Joosa, J. Mythilia, T. Stammb, A. Hohoffb, T. Filliesa,U. Stratmannc, H.P. Wiesmanna
aDepartment of Cranio-Maxillofacial Surgery, University of M .unster, Waldeyerstr. 30, D-48149 M .unster, GermanybDepartment of Orthodontics, University of M .unster, Germany
cDepartment of Anatomy, University of M .unster, Germany
Received 31 March 2003; accepted 11 August 2003
Abstract
Primary stability and an optimized load transfer are assumed to account for an undisturbed osseointegration process of implants.
Immediate loaded newly designed titanium dental implants inserted in the mandible of minipigs were used for the characterization of
the interfacial area between the implant surface and the surrounding bone tissue during the early healing phase. Histological and
electron microscopical studies were performed from implant containing bone specimens. Two different load regimens were applied
to investigate the load related tissue reaction. Histological and electron microscopical analysis revealed a direct bone apposition on
the implant surfaces, as well as the attachment of cells and matrix proteins in the early loading phase. A striking finding of the
ultrastructural immunocytochemical investigations was the synthesis and deposition of bone related proteins (osteonectin,
fibronectin, fibronectin receptor) by osteoblasts from day one of bone/biomaterial interaction. Calcium-phosphate needle-like
crystallites were newly synthesized in a time-related manner directly at the titanium surface. No difference in the ultrastructural
appearance of the interface was found between the two loading groups. Our experimental data suggest that loading of specially
designed implants can be performed immediately after insertion without disturbing the biological osseointegration process.
r 2003 Elsevier Ltd. All rights reserved.
Keywords: Implants; Immediate loading; Interface; Osseointegration
1. Introduction
The use of immediately loaded implants has beenintroduced in clinical routine for many indications.Clinical and experimental studies demonstrate thatosseointegration can be achieved when healing underload is allowed. The bone reaction around loadedimplants has been described by various investigators[1–8] and Szmukler-Moncler et al. have given a literaturereview concerning the timing of loading and the effect ofmicromotion on the bone–implant interface [9]. Moststudies on the interface reaction evaluate the bonereaction on a light microscopical level, whereas limiteddata are available on the reaction of osteoblasts at theinterface on a cellular level. Mineral formation at the
g author. Tel.: +49-251-8347-201; fax: +49-251-
s: [email protected] (U. Meyer).
front matter r 2003 Elsevier Ltd. All rights reserved.
materials.2003.08.070
interface of loaded implants has been investigatedpredominantly by light microscopy (LM), and we knowof no study that has evaluated on the relation betweenmineral deposition and mechanical loading by analyticalultrastructural methods [10,11].It was a long time assumed that premature loading
per-se induces fibrous tissue formation but recentresearch indicates that the extent of micromotionsduring the initial healing phase interferes with theconcomitant bone reaction [9]. When a primarycongruency between the implant and the bone is present,a direct transition of load from the implant to thesurrounding tissue can be assumed. The micromotionat the implant/bone interface can have two principaleffects on the cellular and extracellular components ofbone. First, the micromotion can lead to a disruption ofthe bone–cell/implant contacts and therefore has theability to disturb the cell reaction by a detachment; orsecond the micromotion can lead to a deformation of
ARTICLE IN PRESSU. Meyer et al. / Biomaterials 25 (2004) 1959–19671960
osteoblasts fixed at the surface in a strain-relatedmanner.That peri-implant tissue formation and mineralization
by osteoblasts are dependent on the local mechanicalenvironment in the interface zone is generally accepted[9,12]. Carter and Giori suggested that proliferation anddifferentiation of the osteoblasts responsible for peri-implant tissue formation are regulated by the localmechanical environment according to the tissue differ-entiation hypothesis proposed by Frost and his collea-gues for callus formation [13,14]. The relationship ofdefined cell deformation and bone remodeling has beendocumented in various in vivo studies. Loading of intactbone after osteotomy, during growth, in fracturehealing, and during distraction osteogenesis resulted instrain-related tissue responses [15,16]. Whereas physio-logical bone loading (500–3000 microstrains) leads tomature bone formation, higher peak strains result inimmature bone mineral formation and fibroblastic cellpattern. Evaluation of the effects of implant loading ontissue ultrastructure in vivo will therefore aid in theunderstanding of the basic mechanisms of the formationof the bone/implant interface.The aims of our investigations were to establish the
features of osteoblast behavior and matrix mineraliza-tion during the early bone/biomaterial interaction andthe reactions that were dependant on implant loading
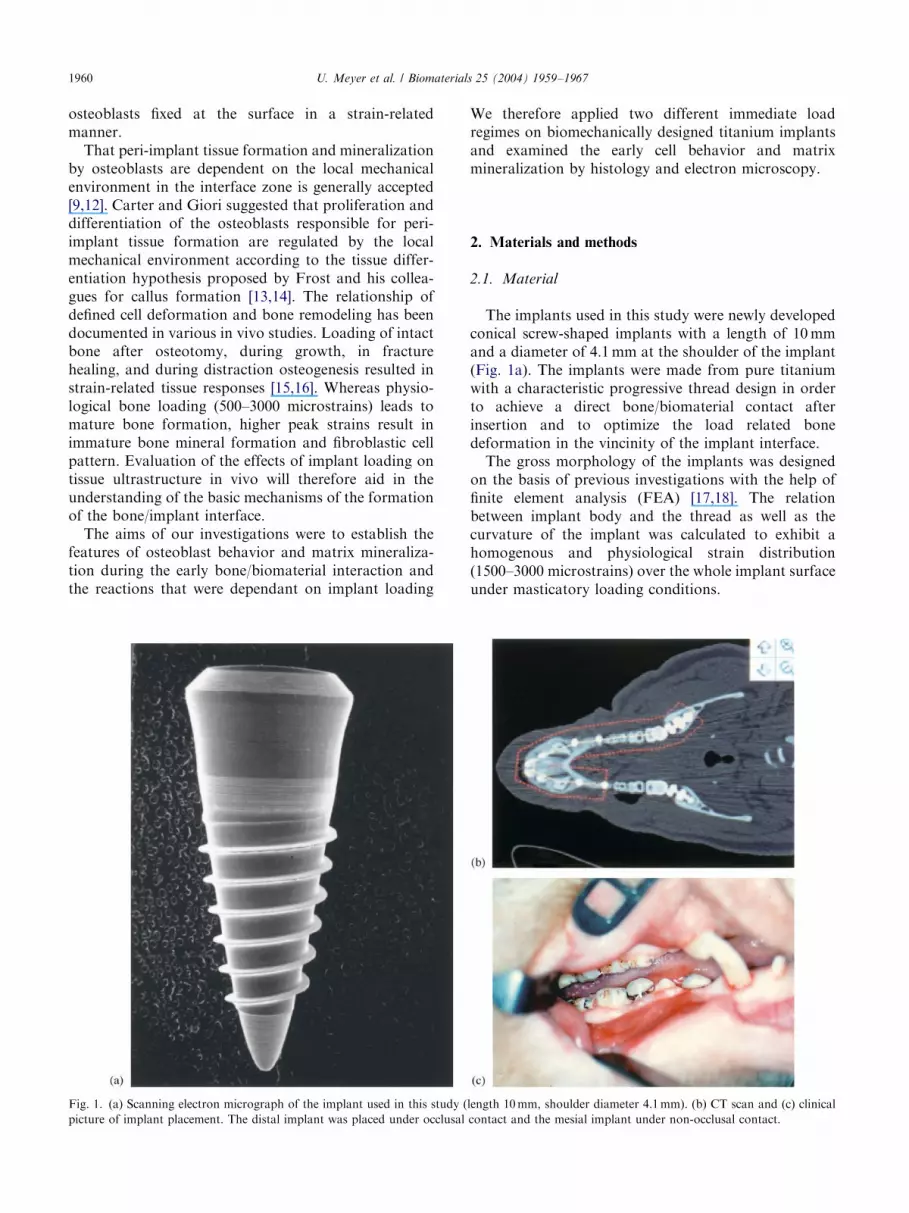
Fig. 1. (a) Scanning electron micrograph of the implant used in this study (
picture of implant placement. The distal implant was placed under occlusal
We therefore applied two different immediate loadregimes on biomechanically designed titanium implantsand examined the early cell behavior and matrixmineralization by histology and electron microscopy.
2. Materials and methods
2.1. Material
The implants used in this study were newly developedconical screw-shaped implants with a length of 10mmand a diameter of 4.1mm at the shoulder of the implant(Fig. 1a). The implants were made from pure titaniumwith a characteristic progressive thread design in orderto achieve a direct bone/biomaterial contact afterinsertion and to optimize the load related bonedeformation in the vincinity of the implant interface.The gross morphology of the implants was designed
on the basis of previous investigations with the help offinite element analysis (FEA) [17,18]. The relationbetween implant body and the thread as well as thecurvature of the implant was calculated to exhibit ahomogenous and physiological strain distribution(1500–3000 microstrains) over the whole implant surfaceunder masticatory loading conditions.
length 10mm, shoulder diameter 4.1mm). (b) CT scan and (c) clinical
contact and the mesial implant under non-occlusal contact.

ARTICLE IN PRESSU. Meyer et al. / Biomaterials 25 (2004) 1959–1967 1961
2.2. Experimental animals
Six male G .ottinger minipigs were used in this study.The experimental study was approved by the AnimalEthics Committee of the University of M .unster underthe reference number G 90/99. Minipigs were selected toensure adequate alveolar ridge size and height forimplant placement [19].The animals were sedated with an intramuscular
injection of ketamine (10mg/kg), atropine (0.06ml/kg),and stresnil (0.03ml/kg). Second premolars of theporcine mandible were extracted bilaterally, and theextraction sites were allowed to heal for 3 months beforeimplant placement (Fig. 1b). A total of 24 implants wereinserted into the mandibles of the minipigs. In accor-dance with our experimental design, two treatmentgroups were tested in each animal: 2 immediately loadedimplants placed in occlusal contact and 2 implantsplaced in a non-occlusal relation (Fig. 1c).
2.3. Surgical procedure
The implants were carefully inserted by manualtapping of the screw-shaped implants until the implantbodies were fully embedded in bone. Single crowns were
Fig. 2. (a) Microscopic view of the mandibular implant. Mature bone cont
Boxes indicate sample positions for TEM (� 10), (b) bone/implant relation a
the implant body (� 20) and (d) cells are present at the surface and in the b
prepared at the day of surgery on a plaster model andwere then inserted to the implants. On days 1, 3, and 14of implant loading two animals each were sacrified andimplant containing block specimens dissected. Oneimplant per study group was embedded in Technovitand subsequent undecalcified histological sections wereprepared to evaluate the gross histology. The otherblock samples containing the implants were divided andthen each sample was further dissected, in order toobtain a sample containing the implant embedded in thealveolar bone and the corresponding bone sampledetached from the implant. Samples containing theimplant were used for scanning electron microscopical(SEM) investigations and immunostaining, whereas thebone sections without implant were prepared fortransmission electron microscopy (TEM) and diffrac-tion analysis.
2.4. Transmission electron microscopy
For TEM, samples were harvested adjacent to theshoulder, the body, and the tip of the implant (Fig. 2a).Tissue samples were fixed in 100mm phosphate buffercontaining 2.5% glutaraldehyde (pH 7.4). Specimenswere dehydrated in a graded series of alcohol and
acts the implant surface. (Specimen: occlusal load, 3 days of loading.)
t the implant threads (� 20), (c) higher magnification of the interface at
one area adjacent to the implant (� 40).
ARTICLE IN PRESSU. Meyer et al. / Biomaterials 25 (2004) 1959–19671962
embedded in Araldite resin. Ultrathin sections werestained for 1 h with 2% uranyl acetate followed byincubation in Reynold’s lead citrat. Sections wereexamined under a Philips CM10 electron microscope.Electron diffraction analysis was carried out on
ultrathin sections with a Philips CM10 TEM. Threepositions from each implant were used to investigate themineral formation.
2.5. Scanning electron microscopy
For SEM, glutaraldehyde fixed specimens werecritical-point dried. Additionally, samples were fixed inliquid nitrogen-cooled propane and cryodried at �80�C.Samples were sputter-coated with gold for histologicalanalysis. Specimens were examined under a fieldemission scanning electron microscope (LEO 1530 VP,Oberkochem, Germany).
2.6. Immunolabeling
After the various time intervals, the probes containingthe implants were fixed with 3% paraformaldehyde,
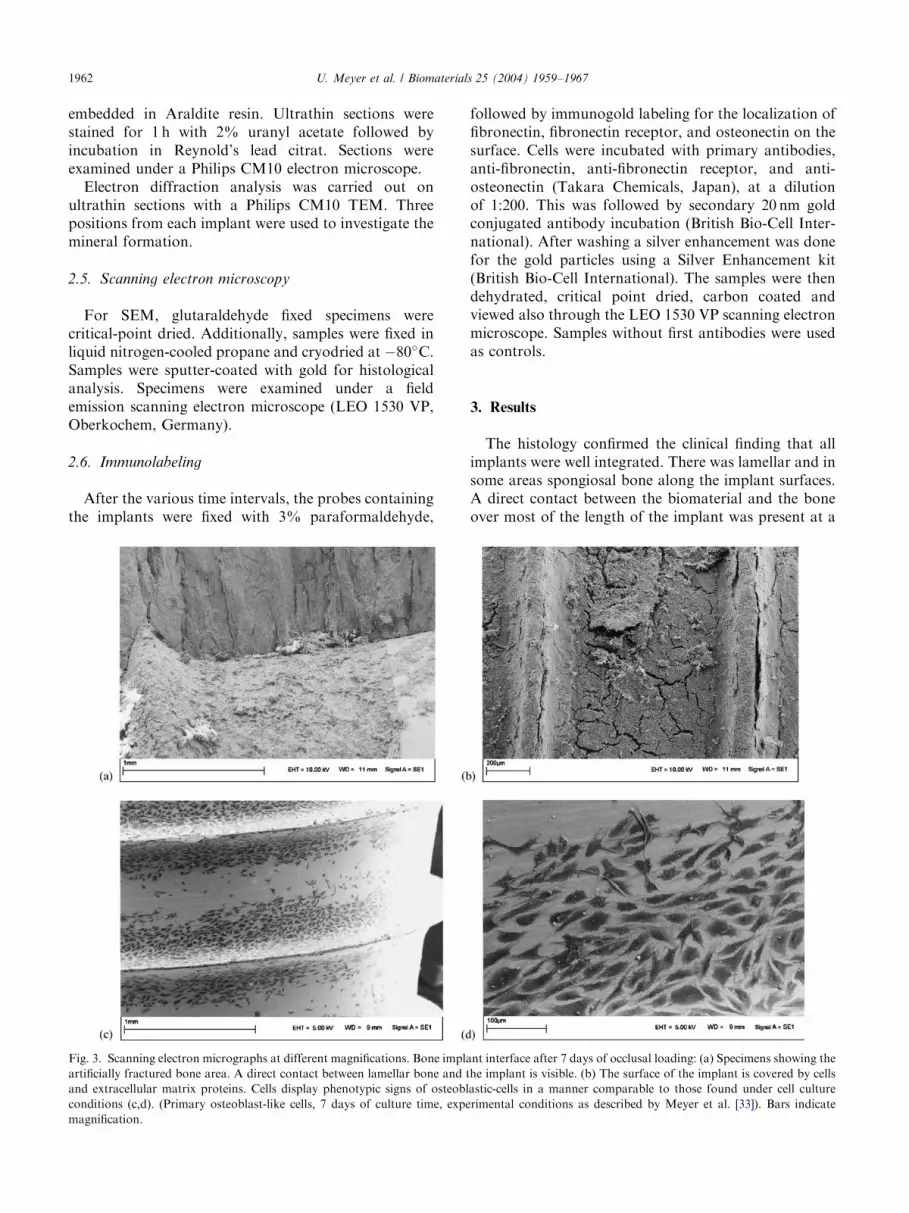
Fig. 3. Scanning electron micrographs at different magnifications. Bone impla
artificially fractured bone area. A direct contact between lamellar bone and t
and extracellular matrix proteins. Cells display phenotypic signs of osteobl
conditions (c,d). (Primary osteoblast-like cells, 7 days of culture time, expe
magnification.
followed by immunogold labeling for the localization offibronectin, fibronectin receptor, and osteonectin on thesurface. Cells were incubated with primary antibodies,anti-fibronectin, anti-fibronectin receptor, and anti-osteonectin (Takara Chemicals, Japan), at a dilutionof 1:200. This was followed by secondary 20 nm goldconjugated antibody incubation (British Bio-Cell Inter-national). After washing a silver enhancement was donefor the gold particles using a Silver Enhancement kit(British Bio-Cell International). The samples were thendehydrated, critical point dried, carbon coated andviewed also through the LEO 1530 VP scanning electronmicroscope. Samples without first antibodies were usedas controls.
3. Results
The histology confirmed the clinical finding that allimplants were well integrated. There was lamellar and insome areas spongiosal bone along the implant surfaces.A direct contact between the biomaterial and the boneover most of the length of the implant was present at a
nt interface after 7 days of occlusal loading: (a) Specimens showing the
he implant is visible. (b) The surface of the implant is covered by cells
astic-cells in a manner comparable to those found under cell culture
rimental conditions as described by Meyer et al. [33]). Bars indicate

ARTICLE IN PRESSU. Meyer et al. / Biomaterials 25 (2004) 1959–1967 1963
light microscopical level (Fig. 2a). The histologicalpicture of the bone adjacent to the implant surface ofthe occlusal loaded implants resembled that of the non-occlusally loaded implants during the experimentalperiod. Histological analysis of the bone/implant inter-face revealed an intimate contact between the titaniumsurface and the bony implantation bed (Fig. 2b). At thebone–titanium interface, a thin tissue layer stained withToluidine blue was seen in some areas coming into directcontact with the titanium, using LM (Fig. 2c). Highermagnification demonstrated the presence of bonecells directly adjacent to the titanium surface (Fig. 2d)and in the surrounding bone tissue. Application ofocclusal loads did not alter the features of the implant/bone contact with direct contact areas at the implantsurface.SEM probe preparation by fracturing the implant
containing the bone sample indicated that the strengthof the implant/bone bond is comparable to the inter-cellular bond in the bone tissue adjacent to the implant(Fig. 3a). The fractured specimens demonstrated a directbond between osteoblasts and the titanium surface. Astriking feature of the SEM specimens was the cell andmatrix coating of the titanium surface in some areas of
Fig. 4. Scanning electron micrograph of time-related mineralization at the im
directly at the implant surface (a) 3 days, (b) 7 days, (c,d) 14 days. Bars ind
the removed half of the bulky bone. Adhesion of cellsand extracellular matrix proteins was present from dayone of the implant/bone contact and was foundthroughout the experimental period independent onthe kind of load application.Cells displayed at higher magnifications all phenoty-
pic signs of osteoblastic cells. The attachment of cellswas mediated in part by extracellular matrix proteins(Fig. 3b). Flattened cells adhered to the surface in amanner that was also found under cell-culture condi-tions (Fig. 3c and d), indicating a focal contactdependant adhesion. Scanning microscopical observa-tion of the interface matrix revealed a time-dependantmineralization process. Small crystals were found in theprotein layer adjacent to the titanium surface. Over thetime period of 14 days, the minerals coalesced in anattempt to form bone-like nodules (Fig. 4a–c). Electrondense, needle-like structures, regarded as early crystal-lites, were found early after implant insertion. Overtime, crystals grow along newly synthesized collagenfibers and minerals were hardly to distinguish from pre-existing minerals after 14 days of implant loading.Mineral formation was found to be collagen-associated(Fig. 4d).
plant surface. Minerals coalesce over time and form bone-like nodules
icate magnification.
ARTICLE IN PRESS
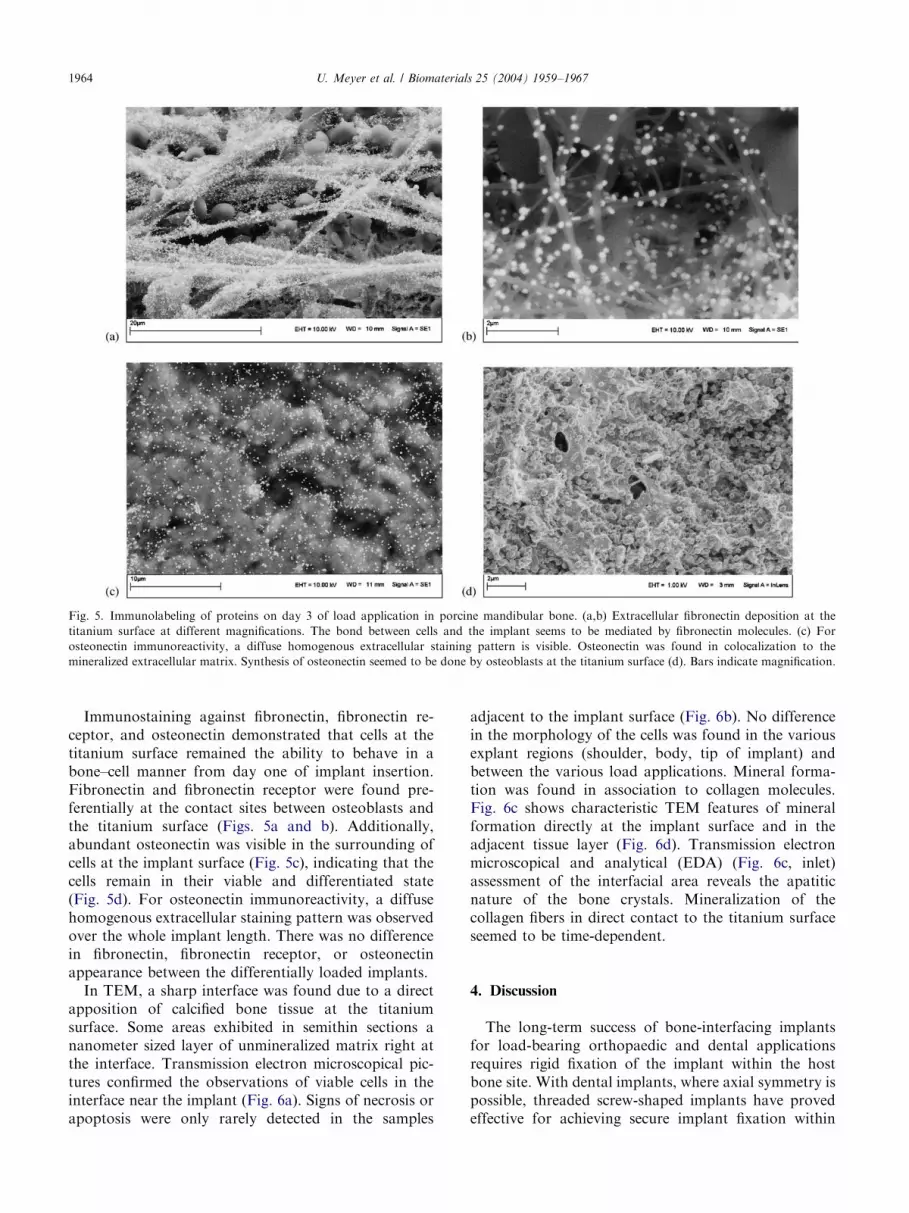
Fig. 5. Immunolabeling of proteins on day 3 of load application in porcine mandibular bone. (a,b) Extracellular fibronectin deposition at the
titanium surface at different magnifications. The bond between cells and the implant seems to be mediated by fibronectin molecules. (c) For
osteonectin immunoreactivity, a diffuse homogenous extracellular staining pattern is visible. Osteonectin was found in colocalization to the
mineralized extracellular matrix. Synthesis of osteonectin seemed to be done by osteoblasts at the titanium surface (d). Bars indicate magnification.
U. Meyer et al. / Biomaterials 25 (2004) 1959–19671964
Immunostaining against fibronectin, fibronectin re-ceptor, and osteonectin demonstrated that cells at thetitanium surface remained the ability to behave in abone–cell manner from day one of implant insertion.Fibronectin and fibronectin receptor were found pre-ferentially at the contact sites between osteoblasts andthe titanium surface (Figs. 5a and b). Additionally,abundant osteonectin was visible in the surrounding ofcells at the implant surface (Fig. 5c), indicating that thecells remain in their viable and differentiated state(Fig. 5d). For osteonectin immunoreactivity, a diffusehomogenous extracellular staining pattern was observedover the whole implant length. There was no differencein fibronectin, fibronectin receptor, or osteonectinappearance between the differentially loaded implants.In TEM, a sharp interface was found due to a direct
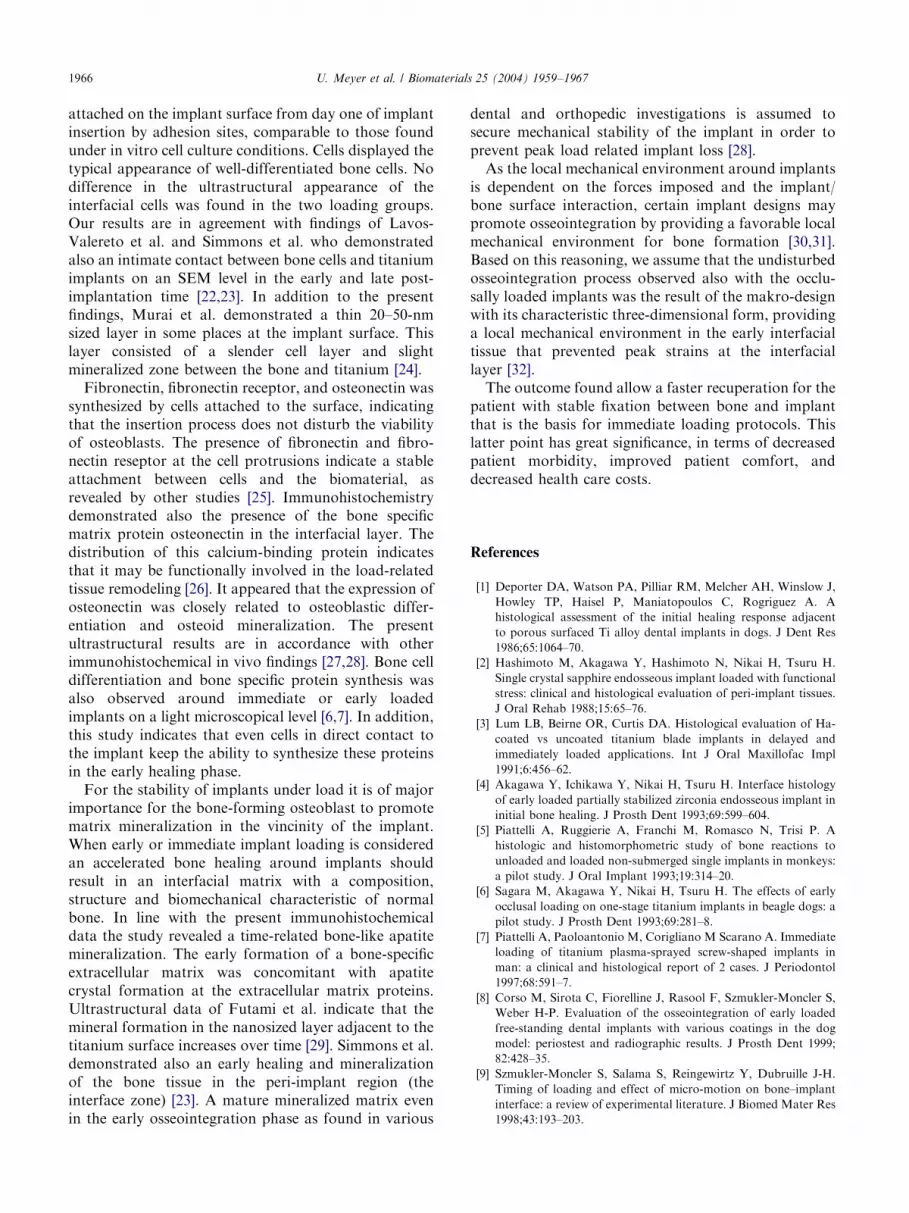
apposition of calcified bone tissue at the titaniumsurface. Some areas exhibited in semithin sections ananometer sized layer of unmineralized matrix right atthe interface. Transmission electron microscopical pic-tures confirmed the observations of viable cells in theinterface near the implant (Fig. 6a). Signs of necrosis orapoptosis were only rarely detected in the samples
adjacent to the implant surface (Fig. 6b). No differencein the morphology of the cells was found in the variousexplant regions (shoulder, body, tip of implant) andbetween the various load applications. Mineral forma-tion was found in association to collagen molecules.Fig. 6c shows characteristic TEM features of mineralformation directly at the implant surface and in theadjacent tissue layer (Fig. 6d). Transmission electronmicroscopical and analytical (EDA) (Fig. 6c, inlet)assessment of the interfacial area reveals the apatiticnature of the bone crystals. Mineralization of thecollagen fibers in direct contact to the titanium surfaceseemed to be time-dependent.
4. Discussion
The long-term success of bone-interfacing implantsfor load-bearing orthopaedic and dental applicationsrequires rigid fixation of the implant within the hostbone site. With dental implants, where axial symmetry ispossible, threaded screw-shaped implants have provedeffective for achieving secure implant fixation within

ARTICLE IN PRESS
Fig. 6. (a) Ultrastructure of viable osteoblast in the layer adjacent to the implant surface (magnification 6300� ). (b) Apoptotic cells were only
seldom present in the bone layer adjacent to the implant (magnification 1500� ). (c) Unstained section of collagen mineralization at the implant (I)
surface (magnification 11000� ) and (d) in the microenvironment of the implant (magnification 6300� ). (c, inlet) Electron diffraction pattern of
mineral formation adjacent to the implant surface.
U. Meyer et al. / Biomaterials 25 (2004) 1959–1967 1965
bone. The threads are representative of macroscopicsurface features that allow mechanical interlocking ofimplant within bone. The results of various studiessuggest that the quality of implant osseointegration andstability is dependent to a large extent on the geometricimplant design. However, the role of implant geometryin affecting early tissue healing and implant stabilitycannot be determined directly from observations madeseveral weeks post-implantation after osseointegrationand bone remodeling have occurred. The issue ofimmediate healing response next to implants and theultrastructural characterization of the tissues formedwithin the implant/bone interface has not yet beenaddressed.Inspection of the bone reaction around oral implants
is conventionally performed and histomorphometricallyevaluated either on ground sections of methyl-metacry-late-embedded materials or at the cellular level byhistologic analysis of the peri-implant tissue by LM.Alternatively, the architecture of the tissue/implantinterface is visualized by electron microscopy (SEM/TEM). The two approaches exclude each other because
of the sample preparation. Therefore, a combined probesampling and preparation was done in this study to givea better insight into the morphological and functionalfeatures of interfacial tissue formation.The histological overview of the bone/implant rela-
tion in the present study demonstrates a congruencybetween the implant and the surrounding bone tissue. Adirect contact between titanium and bone was visibleover the whole surface area of the implant directly afterinsertion and during the experimental period. Excellentadaptation of the host bone to titanium surfaces wasobserved on an ultrastructural level in a comparablemanner as reported after insertion of self-tapping screwsin calvaria bone by Sowden and Schmitz [20]. It wasdemonstrated that when self-tapping screws were placedin loading or non-loading positions the long-termhistology showed that the bone tissue around theimplants was maintained in both situations [21].SEM observations demonstrate that not only miner-
alized bone tissue contacts the surface but thatosteoblast are also attached firmly to the titaniumsurface. The ultrastructural data indicate that cells are
ARTICLE IN PRESSU. Meyer et al. / Biomaterials 25 (2004) 1959–19671966
attached on the implant surface from day one of implantinsertion by adhesion sites, comparable to those foundunder in vitro cell culture conditions. Cells displayed thetypical appearance of well-differentiated bone cells. Nodifference in the ultrastructural appearance of theinterfacial cells was found in the two loading groups.Our results are in agreement with findings of Lavos-Valereto et al. and Simmons et al. who demonstratedalso an intimate contact between bone cells and titaniumimplants on an SEM level in the early and late post-implantation time [22,23]. In addition to the presentfindings, Murai et al. demonstrated a thin 20–50-nmsized layer in some places at the implant surface. Thislayer consisted of a slender cell layer and slightmineralized zone between the bone and titanium [24].Fibronectin, fibronectin receptor, and osteonectin was
synthesized by cells attached to the surface, indicatingthat the insertion process does not disturb the viabilityof osteoblasts. The presence of fibronectin and fibro-nectin reseptor at the cell protrusions indicate a stableattachment between cells and the biomaterial, asrevealed by other studies [25]. Immunohistochemistrydemonstrated also the presence of the bone specificmatrix protein osteonectin in the interfacial layer. Thedistribution of this calcium-binding protein indicatesthat it may be functionally involved in the load-relatedtissue remodeling [26]. It appeared that the expression ofosteonectin was closely related to osteoblastic differ-entiation and osteoid mineralization. The presentultrastructural results are in accordance with otherimmunohistochemical in vivo findings [27,28]. Bone celldifferentiation and bone specific protein synthesis wasalso observed around immediate or early loadedimplants on a light microscopical level [6,7]. In addition,this study indicates that even cells in direct contact tothe implant keep the ability to synthesize these proteinsin the early healing phase.For the stability of implants under load it is of major
importance for the bone-forming osteoblast to promotematrix mineralization in the vincinity of the implant.When early or immediate implant loading is consideredan accelerated bone healing around implants shouldresult in an interfacial matrix with a composition,structure and biomechanical characteristic of normalbone. In line with the present immunohistochemicaldata the study revealed a time-related bone-like apatitemineralization. The early formation of a bone-specificextracellular matrix was concomitant with apatitecrystal formation at the extracellular matrix proteins.Ultrastructural data of Futami et al. indicate that themineral formation in the nanosized layer adjacent to thetitanium surface increases over time [29]. Simmons et al.demonstrated also an early healing and mineralizationof the bone tissue in the peri-implant region (theinterface zone) [23]. A mature mineralized matrix evenin the early osseointegration phase as found in various
dental and orthopedic investigations is assumed tosecure mechanical stability of the implant in order toprevent peak load related implant loss [28].As the local mechanical environment around implants
is dependent on the forces imposed and the implant/bone surface interaction, certain implant designs maypromote osseointegration by providing a favorable localmechanical environment for bone formation [30,31].Based on this reasoning, we assume that the undisturbedosseointegration process observed also with the occlu-sally loaded implants was the result of the makro-designwith its characteristic three-dimensional form, providinga local mechanical environment in the early interfacialtissue that prevented peak strains at the interfaciallayer [32].The outcome found allow a faster recuperation for the
patient with stable fixation between bone and implantthat is the basis for immediate loading protocols. Thislatter point has great significance, in terms of decreasedpatient morbidity, improved patient comfort, anddecreased health care costs.
References
[1] Deporter DA, Watson PA, Pilliar RM, Melcher AH, Winslow J,
Howley TP, Haisel P, Maniatopoulos C, Rogriguez A. A
histological assessment of the initial healing response adjacent
to porous surfaced Ti alloy dental implants in dogs. J Dent Res
1986;65:1064–70.
[2] Hashimoto M, Akagawa Y, Hashimoto N, Nikai H, Tsuru H.
Single crystal sapphire endosseous implant loaded with functional
stress: clinical and histological evaluation of peri-implant tissues.
J Oral Rehab 1988;15:65–76.
[3] Lum LB, Beirne OR, Curtis DA. Histological evaluation of Ha-
coated vs uncoated titanium blade implants in delayed and
immediately loaded applications. Int J Oral Maxillofac Impl
1991;6:456–62.
[4] Akagawa Y, Ichikawa Y, Nikai H, Tsuru H. Interface histology
of early loaded partially stabilized zirconia endosseous implant in
initial bone healing. J Prosth Dent 1993;69:599–604.
[5] Piattelli A, Ruggierie A, Franchi M, Romasco N, Trisi P. A
histologic and histomorphometric study of bone reactions to
unloaded and loaded non-submerged single implants in monkeys:
a pilot study. J Oral Implant 1993;19:314–20.
[6] Sagara M, Akagawa Y, Nikai H, Tsuru H. The effects of early
occlusal loading on one-stage titanium implants in beagle dogs: a
pilot study. J Prosth Dent 1993;69:281–8.
[7] Piattelli A, Paoloantonio M, Corigliano M Scarano A. Immediate
loading of titanium plasma-sprayed screw-shaped implants in
man: a clinical and histological report of 2 cases. J Periodontol
1997;68:591–7.
[8] Corso M, Sirota C, Fiorelline J, Rasool F, Szmukler-Moncler S,
Weber H-P. Evaluation of the osseointegration of early loaded
free-standing dental implants with various coatings in the dog
model: periostest and radiographic results. J Prosth Dent 1999;
82:428–35.
[9] Szmukler-Moncler S, Salama S, Reingewirtz Y, Dubruille J-H.
Timing of loading and effect of micro-motion on bone–implant
interface: a review of experimental literature. J Biomed Mater Res
1998;43:193–203.
ARTICLE IN PRESSU. Meyer et al. / Biomaterials 25 (2004) 1959–1967 1967
[10] H .ohling HJ, Barckhaus RH, Krefting ER, Althoff J, Quint P.
Collagen mineralization: Aspects of the structural relationships
between collagen and the apatitic crystallites. In: Bonucci E,
Motta PM, editors. Ultrastructure of Skeletal Tissues. New York:
Academic Press; 1990. p. 41–62.
[11] Landis WJ. Mineral characterization in calcifying tissues: atomic,
molecular and macromolecular perspectives. Connect Tissue Res
1996;34:239–46.
[12] Pilliar RM. Quantitative evaluation of the effect of movement at a
porous coated implant–bone interface. In: Davies JE, editor. The
bone–biomaterial interface. Toronto: University of Toronto
Press; 1991. p. 380.
[13] Carter DR, Giori NJ. Effect of mechanical stress on tissue
differentiation in the bony implant bed. In: Davies JE, editor. The
bone–biomaterial interface. Toronto: University of Toronto
Press; 1991. p. 367.
[14] Frost H, Joos U, Meyer U, Jensen OT. Distraction osteogenesis
based on the utah paradigm. In: Jensen OT, editor. Alveolar
Distraction Osteogenesis. Illionois, USA: Quintessence Publisher.
[15] Cheal EJ, Mansmann KA, DiGioia III AM, Hayes WC, Perren
SM. Role of interfragmentary strain in fracture healing: ovine
model of a healing osteotomy. J Orthop Res 1991;9:131–42.
[16] Meyer U, Wiesmann HP, Kruse-L .osler B, Handschel J, Strat-
mann U, Joos U. Strain related bone remodeling in distraction
osteogenesis of the mandible. Plast Reconstr Surg 1999;103:
800–7.
[17] Meyer U, Vollmer D, Bourauel C, Joos U. Sensitivity analysis of
bone geometries around oral implants upon bone loading using
finite element method. Comp Methods Biomech Biomed Eng
2001;3:553–9.
[18] Joos U, Vollmer D, Kleinheinz J. Effect of implant geometry on
strain distribution in peri-implant bone. Mund Kiefer Ge-
sichtschir 2000;4:143–7.
[19] Buser D, Nydegger T, Hirt HP, Cochran DL, Nolte LP. Removal
torque values of titanium implants in the maxilla of miniature
pigs. Int J Oral Maxillofac Implants 1998;13:611–9.
[20] Sowden D, Schmitz JP. AO self-drilling and self-tapping screws in
rat calvarial bone: an ultrastructural study of the implant
interface. J Oral Maxillofac Surg 2002;60:294–9.
[21] Akin-Nergiz N, Nergiz I, Schulz A, Arpak N, Niedermeier W.
Reactions of peri-implant tissues to continuous loading of
osseointegrated implants. Am J Orthodont Dent Orthop
1998;114:292–8.
[22] Lavos-Valereto IC, Wolynec S, Deboni MC, Konig Jr B. In vitro
and in vivo biocompatibility testing of Ti–6AI–7Nb alloy with
and without plasma-sprayed hydroxyapatite coating. J Biomed
Mater Res 2001;58:727–33.
[23] Simmons CA, Valiquette N, Pilliar RM. Osseointegration of
sintered porous-surfaced and plasma-spray coated implants: an
animal model study of early post-implantation healing response
and mechanical stability. J Biomed Mater Res 1999;47:127–38.
[24] Murai K, Takeshita F, Ayukawa Y, Kiyoshima T, Suetsugu T,
Tanaka T. Light and electron microscopic studies of bone–
titanium interface in the tibiae of young and mature rats.
J Biomed Mater Res 1996;30:523–33.
[25] Rosengren A, Johansson BR, Danielsen N, Thomsen P, Ericson
LE. Immunohistochemical studies on the distribution of albumin,
fibrinogen, fibronectin, IgG and collagen around PTFE and
titanium implants. Biomaterials 1996;17:1779–86.
[26] Roach HI. Why does bone matrix contain non-collagenous
proteins? The possible roles of osteocalcin, osteonectin, osteo-
pontin and bone sialoprotein in bone mineralisation and
resorption. Cell Biol Int 1994;18:617–28.
[27] Johansson CB, Roser K, Bolind P, Donath K, Albrektsson T.
Bone–tissue formation and integration of titanium implants: an
evaluation with newly developed enzyme and immunohistochem-
ical techniques. Clin Implant Dent Relat Res 1999;1:33–40.
[28] R .oser K, Johansson CB, Donath K, Albrektsson T. A new
approach to demonstrate cellular activity in bone formation
adjacent to implants. J Biomed Mater Res 2000;51:280–91.
[29] Futami T, Fujii N, Ohnishi H, Taguchi N, Kusakari H, Ohshima
H, Maeda T. Tissue response to titanium implants in the rat
maxilla: ultrastructural and histochemical observations of the
bone–titanium interface. J Periodontol 2000;71:287–98.
[30] Misch CE, Bidez MW, Sharawy M. A bioengineered implant for a
predetermined bone cellular response to loading forces A
literature review and case report. J Periodontol 2001;72:1276–86.
[31] Simmons CA, Meguid SA, Pilliar RM. Mechanical regulation of
localized and appositional bone formation around bone–interfa-
cing implants. J Biomed Mater Res 2001;55:63–71.
[32] Simmons CA, Meguid SA, Pilliar RM. Differences in osseointe-
gration rate due to implant surface geometry can be explained by
local tissue strains. J Orthop Res 2001;19:187–94.
[33] Meyer U, Szulczewski DH, Barckhaus RH, Atkinson M, Jones
DB. Biological evaluation of an ionomeric bone cement by
osteoblast cell culture methods. Biomaterials 1993;14:917–24.





























