Embed Size (px)
Citation preview
ORIGINAL RESEARCH
Ultrasound guidance for central venouscatheter placement in Australasian emergencydepartments: Potential barriers to morewidespread useemm_1347 514..523
Jakub T Matera,1 Diana Egerton-Warburton2 and Robert Meek3
1Peninsula Health, Frankston Hospital, Frankston, 2Southern Health, Monash Medical Centre, Clayton,and 3Southern Health, Dandenong Hospital, Dandenong, Victoria, Australia
Abstract
Objectives: To survey Fellows of the Australasian College for Emergency Medicine (FACEMs) in orderto describe current ultrasound (US) usage during central venous catheter (CVC) placementand to compare practice and opinions between FACEMs routinely using US and those not.
Methods: Descriptive and analytical cross-sectional electronic survey of all FACEMs. Baseline vari-ables including hospital type, US availability, frequency of CVC insertion, US usage andtechnique are presented descriptively. US practice and opinions on usage are comparedbetween routine and non-routine users.
Results: Responses were obtained from 486 (42.4%) of 1146 FACEMs emailed. Whereas 88.5% ofrespondents had US available and 70% had done an US course, only 37% routinely usedUS for CVC placement. Completion of an US course and performance of >11 CVC per yearwere strongly associated with routine US use (odds ratio 10.0 [5.5–18.4] and 2.6 [1.7–3.9],respectively). Common barriers to more frequent US use were not having completed an UScourse (20%) and US-guided CVC placement taking too long (18%). Eighty-five per cent ofFACEMs agreed that there should be ED access to US and US training but only 34%thought its use should be mandatory.
Conclusions: We found that only 37% of FACEM respondents routinely used US to guide placement ofCVCs and a number of barriers to more frequent use are identified. Practices and opinionsregarding US use differed significantly between routine and non-routine users.
Key words: central venous catheter, emergency department, survey, ultrasound.
Correspondence: Dr Jakub T Matera, Emergency Department, Frankston Hospital, PO Box 52, Frankston, Vic. 3199, Australia. Email:[email protected]
Jakub Tomasz Matera, MD, Senior Registrar Emergency Medicine; Diana Egerton-Warburton, MB BS, FACEM, M Clin Epi, Emergency Physician;Robert Meek, MB BS, FACEM, M Clin Epi, Emergency Physician.
doi: 10.1111/j.1742-6723.2010.01347.xEmergency Medicine Australasia (2010) 22, 514–523
© 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

Introduction
Central venous catheters (CVCs) have a number ofimportant uses in both elective and critical care settings.Their uses include: haemodynamic monitoring, con-trolled volume replacement and the delivery of vasoac-tive medications, antibiotics and other medications,which can be associated with significant morbiditywhen administered through peripheral i.v. catheters.Occasionally, a CVC might be the only obtainable formof vascular access. For these reasons the placement ofCVCs is regarded as an essential skill for practitionersin anaesthetics, intensive care and emergency medicine.
Traditionally, placement of CVC has been performedusing well-described techniques based on the sur-rounding surface anatomical landmarks. The needle ispassed ‘blindly’ through the skin in order to puncturethe vein along its anticipated course.1,2 A number ofmechanical complications of CVC placement have beendescribed, including: arterial puncture, excessive bleed-ing, haematoma formation, vessel laceration, nerveinjury, air embolus, catheter malposition, pneumotho-rax, haemothorax and cardiac tamponade.3,4 Complica-tion rates for attempted CVC insertion (successful ornot) have been reported to range between 0.5% and10% but might be as high as 15% in ED patients.4–6 Inone study the incidence of mechanical complicationsafter three or more insertion attempts was reportedto be six times the rate after one attempt.7 Failure tocannulate the vessel might occur in up to 20% ofcases.5,7
The use of Doppler ultrasound to localize the internaljugular vein was first described in 1984 with real-timevisualization prior to catheterization being reported in1986.8,9 Since then, ultrasound assistance in CVC place-ment has been found to reduce the number of attemptsrequired, the time to successful insertion and the com-plication rate.2,10,11 In 1997, the use of two-dimensionalultrasonography-guided internal jugular venous accesswas reported for the first time in the ED setting.12 Overthe last 10 years, the development of ultrasound train-ing courses specifically designed for emergency medi-cine practice has seen the increasing use of ultrasoundby emergency physicians for a number of indicationsincluding vascular access.13–15
Some doubt has remained about the utility of ultra-sound for CVC placement in the subclavian vein,where clinical trials have had mixed results.10,16,17 Thisis thought to be due to the fixed anatomical relation-ship between the subclavian vein and the clavicle,which can make ultrasound technically more difficult
and might render it less reliable than the landmarkmethod.4
The majority of the available literature to date hasfocused on CVC placement for elective patients in anaes-thetics, oncology and radiology.2,10,11,18 Fewer studieshave investigated the utility and efficacy in ED or ICUpatients.12,18–24 But the three randomized controlledED-based trials published to date have consistentlyfound that ultrasound guidance was associated with areduction in the number of attempts required, the timetaken to placement and the complication rate when com-pared with the traditional landmark techniques.22–24
Since 2002 a number of health authorities in the UK,North America and the Australasian College for Emer-gency Medicine (ACEM) have issued guidelines or poli-cies recommending that 2D ultrasound should beconsidered for all CVCs during elective and emergencyplacement.25–27 Despite such recommendations, theextent to which ultrasound has been adopted to assistCVC placement in Australasian EDs is unclear.
We surveyed Fellows of the Australasian College forEmergency Medicine (FACEMs) in order to describecurrent practice in ultrasound usage in the placement ofCVCs and to compare a range of demographic variablesand opinions between FACEMs who routinely use ultra-sound for CVC placement and those who do not. Thepurpose is to describe current practice and provideinformation about potential barriers to ultrasound use,which might be addressed in order to bring about morewidespread usage of ultrasound guidance for CVCplacement in the future.
Methods
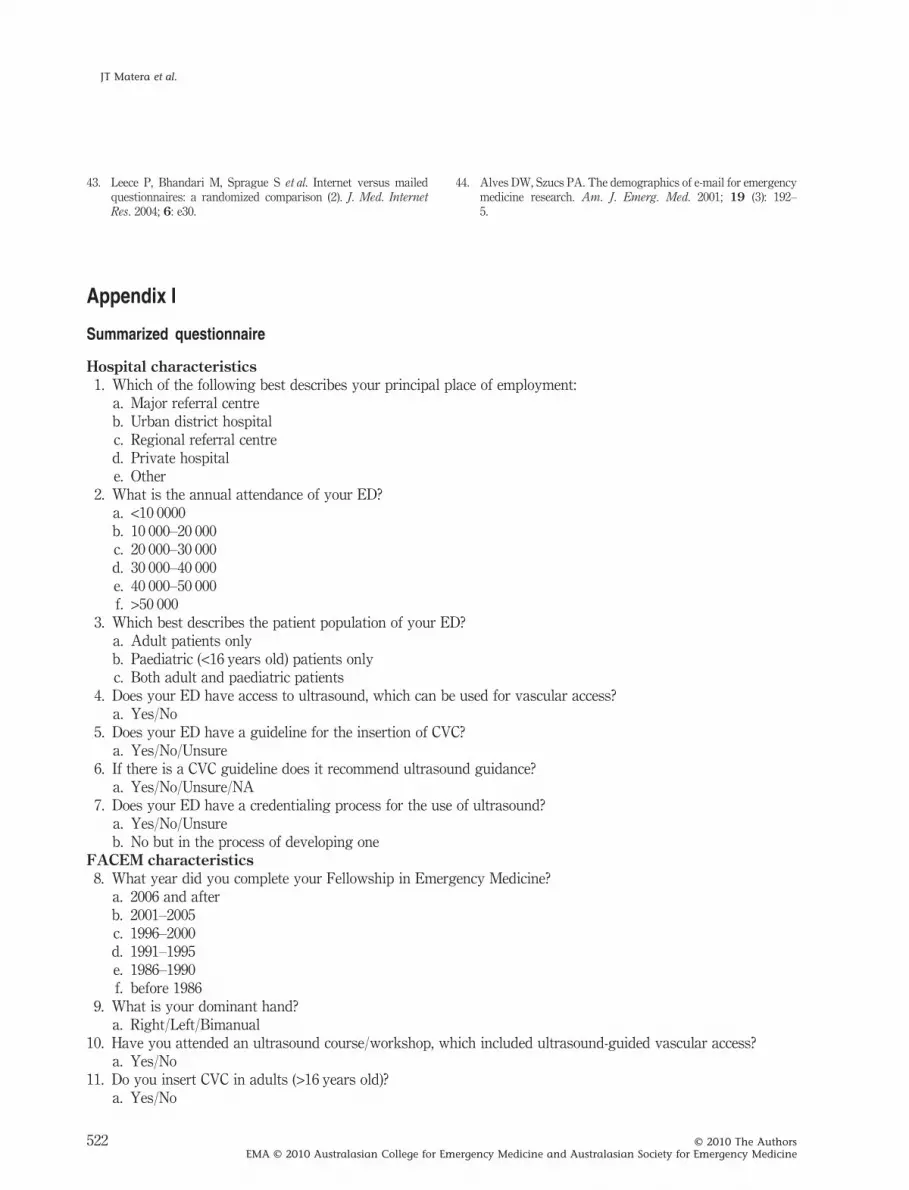
A descriptive and analytical cross-sectional survey wasperformed. The questionnaire was developed by theinvestigators in consultation with the Southern HealthED Ultrasound Group, an expert special interest groupof emergency physicians who advise on local ultra-sound practice. Relevant factors were identified fromthe literature and suggested by the Ultrasound Group.The questionnaire was finalized following focus groupdiscussions and pilot administration on a group of vol-unteer FACEMs and senior registrars.
Baseline information included: type and size of ED,year of FACEM qualification, ultrasound availability,presence of ED ultrasound guidelines and credentialingprocess, personal completion of an ultrasound course,handedness, number of CVCs performed per year, fre-quency of ultrasound use for CVC insertion and confi-
US guidance during CVC insertion in ED
515© 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

dence in landmark and ultrasound-assisted techniques.Information on current ultrasound practice included:machine type, probe/cover type and particulars ofapproach. Opinions were sought on the degree to whichultrasound use and training should be mandated,its relative safety and the presence of particular barriersto personal use. These requested a response to astatement using the adjectival scale: Strongly Agree,Agree, Neither Agree nor Disagree, Disagree, StronglyDisagree.
The study was approved by the Southern HealthEthics Committee and the ACEM Scientific Committee.All FACEMs on the ACEM database who were con-tactable by email were sent invitations to participateby ACEM administrative staff. There were no exclu-sion criteria. The email included a cover letter and aweb link to the SurveyMonkey site, which ensuredconfidentiality.
The questionnaire was distributed in April 2009 withreminders being sent in May 2009 and June 2009. Thetabulated responses were downloaded on to a passwordprotected Microsoft Excel spreadsheet (Microsoft Cor-poration, Redmond, WA, USA). Data were analysedusing the Stata version 8.0 statistical package (StataCorporation, College Station, TX, USA). The categoricaldescriptive data are presented as number and percent-age. Comparisons between ‘routine’ and ‘non-routine’users of ultrasound are presented as odds ratios with95% confidence intervals. ‘Routine users’ were definedas those who responded that ultrasound use was either‘usual’ or ‘always’. The responses to statements arereported descriptively as number and percentage foreach of the five levels of agreement but for the purposeof the comparative analyses these were collapsedto either ‘Agree/Strongly Agree’ versus ‘other’ or‘Disagree/Strongly Disagree’ versus ‘other’ dependingon the wording of the statement being examined.
Results
Responses were received from 486 (42.4%) of the 1146FACEMs who were invited to participate. The majority(78%) of respondents worked in either a major referralor an urban district hospital. There are no currentfigures on FACEM work place distribution but therewere no significant differences between employmentlocation for this sample and that of a cohort of 486FACEM respondents to a survey (56% response rate)conducted for a different purpose by Dent et al. in2008.28 There were also no significant differences in
distribution of year of FACEM attainment between thissample and the whole FACEM population (dataobtained from ACEM).
Ultrasound was available to 88.5% of respondentsand 70% reported having completed an ultrasoundcourse including vascular access. An ultrasound creden-tialing process was present in the ED of 37.7% of therespondents. Presence of CVC insertion guidelines wasinfrequent and less than half recommended ultrasounduse during insertion. Full baseline information is shownin Table 1.
Whereas 447 (92%) of the 486 FACEMs reported thatthey insert CVCs in adults, the frequency varied widelywith 201 (45.0%) inserting <6 per year, 120 (26.8%)inserting 6–11 per year and 126 (28.2%) inserting >11per year. The preferred site was internal jugular for 200(44.7%), subclavian vein for 130 (29.1%) and femoralvein for 117 (26.2%). Of the 447 FACEMs who performCVCs, 380 (86.0%) reported usually or always feelingconfident in applying the landmark technique. Of the274 (61.3%) FACEMs who use ultrasound to assist CVCplacement at least ‘sometimes’ 229 (83.4%) reportedusually or always feeling confident in applying theultrasound-assisted technique. The self-reported fre-quency of ultrasound use to assist with CVC insertion isshown in Table 2.
Of the 332 FACEMs who reported the details of theirultrasound practice, 186 (56.0%) stated they primarilyused the real-time dynamic technique whereas 94(28.3%) used the static technique and 52 (15.7%) onlyused ultrasound as an attempted rescue strategy afterinitial landmark technique failure. Two hundred andforty (71.9%) of 334 reported employing the one-persontechnique with 94 (28.1%) using the two-person tech-nique. Of the 330 who responded to probe type used, 261(79.1%) reported linear probe use whereas 69 (20.9%)reported use of a specific vascular probe. Of the 300 whoresponded to type of probe cover used, 183 (61.0%)reported using a purpose designed sheath, 101 (33.7%)used a sterile glove and 16 (5.3%) used a transparentfilm dressing. Of the 350 who ever use ultrasound, 41(11.7%) reported having used an echotip needle.
The responses of all FACEMs to the statementsregarding ultrasound use, training and credentialing areshown in Table 3. The majority thought that ultrasounduse was beneficial (63%), had advantages over the land-mark technique (88%) and led to fewer complications(67%) but that its use should not be made mandatory(53%). The majority also felt that all ED doctors shouldbe trained in ultrasound (85%) and that there should bea credentialing process for all ED medical staff (67%).
JT Matera et al.
516 © 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
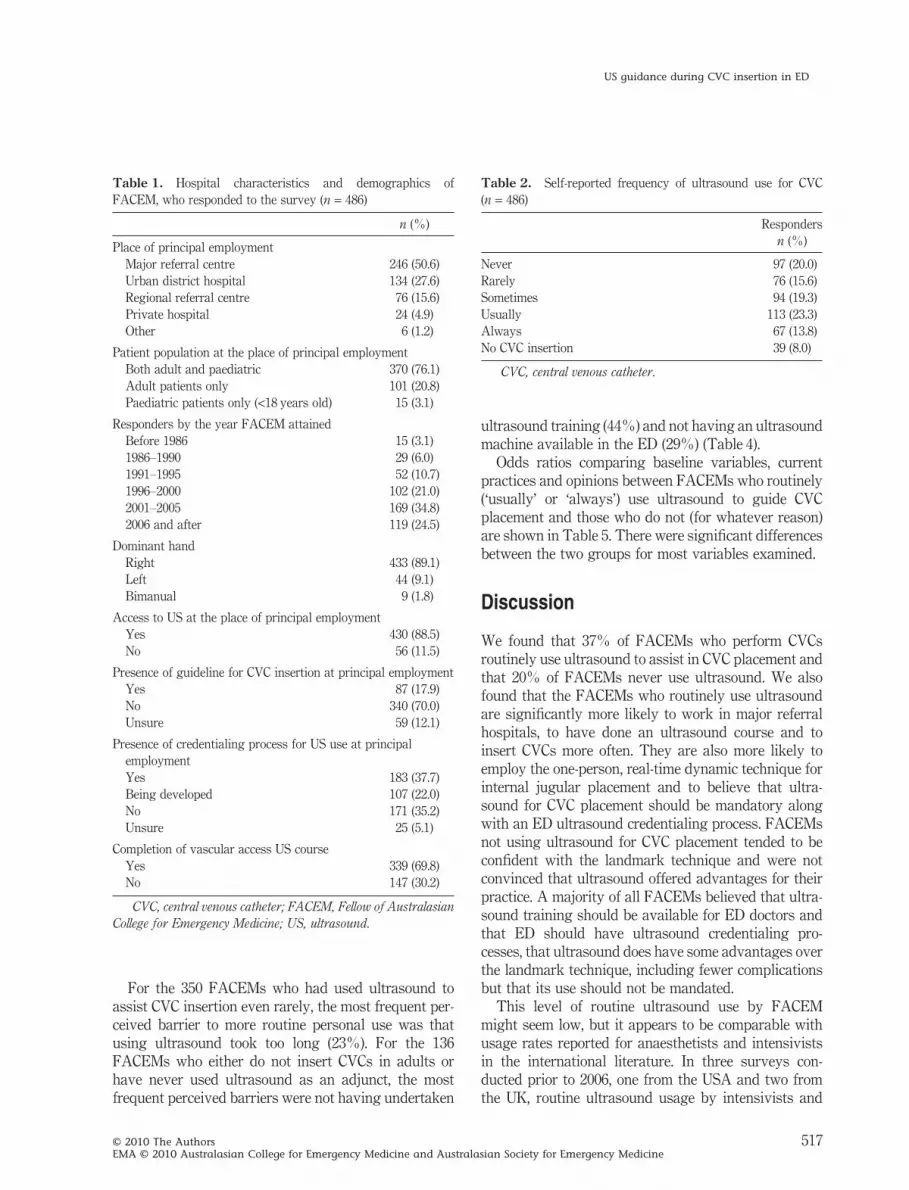
For the 350 FACEMs who had used ultrasound toassist CVC insertion even rarely, the most frequent per-ceived barrier to more routine personal use was thatusing ultrasound took too long (23%). For the 136FACEMs who either do not insert CVCs in adults orhave never used ultrasound as an adjunct, the mostfrequent perceived barriers were not having undertaken
ultrasound training (44%) and not having an ultrasoundmachine available in the ED (29%) (Table 4).
Odds ratios comparing baseline variables, currentpractices and opinions between FACEMs who routinely(‘usually’ or ‘always’) use ultrasound to guide CVCplacement and those who do not (for whatever reason)are shown in Table 5. There were significant differencesbetween the two groups for most variables examined.
Discussion
We found that 37% of FACEMs who perform CVCsroutinely use ultrasound to assist in CVC placement andthat 20% of FACEMs never use ultrasound. We alsofound that the FACEMs who routinely use ultrasoundare significantly more likely to work in major referralhospitals, to have done an ultrasound course and toinsert CVCs more often. They are also more likely toemploy the one-person, real-time dynamic technique forinternal jugular placement and to believe that ultra-sound for CVC placement should be mandatory alongwith an ED ultrasound credentialing process. FACEMsnot using ultrasound for CVC placement tended to beconfident with the landmark technique and were notconvinced that ultrasound offered advantages for theirpractice. A majority of all FACEMs believed that ultra-sound training should be available for ED doctors andthat ED should have ultrasound credentialing pro-cesses, that ultrasound does have some advantages overthe landmark technique, including fewer complicationsbut that its use should not be mandated.
This level of routine ultrasound use by FACEMmight seem low, but it appears to be comparable withusage rates reported for anaesthetists and intensivistsin the international literature. In three surveys con-ducted prior to 2006, one from the USA and two fromthe UK, routine ultrasound usage by intensivists and
Table 1. Hospital characteristics and demographics ofFACEM, who responded to the survey (n = 486)
n (%)
Place of principal employmentMajor referral centre 246 (50.6)Urban district hospital 134 (27.6)Regional referral centre 76 (15.6)Private hospital 24 (4.9)Other 6 (1.2)
Patient population at the place of principal employmentBoth adult and paediatric 370 (76.1)Adult patients only 101 (20.8)Paediatric patients only (<18 years old) 15 (3.1)
Responders by the year FACEM attainedBefore 1986 15 (3.1)1986–1990 29 (6.0)1991–1995 52 (10.7)1996–2000 102 (21.0)2001–2005 169 (34.8)2006 and after 119 (24.5)
Dominant handRight 433 (89.1)Left 44 (9.1)Bimanual 9 (1.8)
Access to US at the place of principal employmentYes 430 (88.5)No 56 (11.5)
Presence of guideline for CVC insertion at principal employmentYes 87 (17.9)No 340 (70.0)Unsure 59 (12.1)
Presence of credentialing process for US use at principalemploymentYes 183 (37.7)Being developed 107 (22.0)No 171 (35.2)Unsure 25 (5.1)
Completion of vascular access US courseYes 339 (69.8)No 147 (30.2)
CVC, central venous catheter; FACEM, Fellow of AustralasianCollege for Emergency Medicine; US, ultrasound.
Table 2. Self-reported frequency of ultrasound use for CVC(n = 486)
Respondersn (%)
Never 97 (20.0)Rarely 76 (15.6)Sometimes 94 (19.3)Usually 113 (23.3)Always 67 (13.8)No CVC insertion 39 (8.0)
CVC, central venous catheter.
US guidance during CVC insertion in ED
517© 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
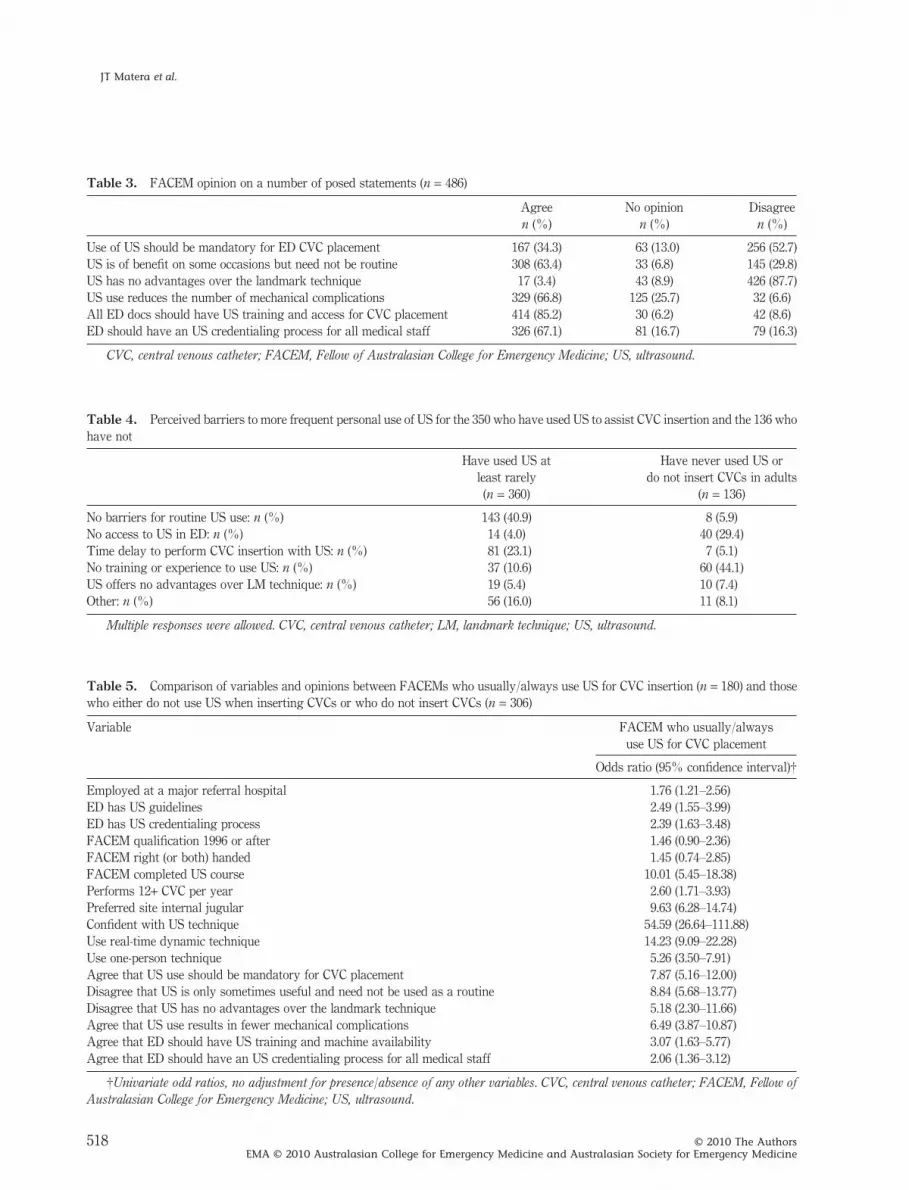
Table 3. FACEM opinion on a number of posed statements (n = 486)
Agree No opinion Disagreen (%) n (%) n (%)
Use of US should be mandatory for ED CVC placement 167 (34.3) 63 (13.0) 256 (52.7)US is of benefit on some occasions but need not be routine 308 (63.4) 33 (6.8) 145 (29.8)US has no advantages over the landmark technique 17 (3.4) 43 (8.9) 426 (87.7)US use reduces the number of mechanical complications 329 (66.8) 125 (25.7) 32 (6.6)All ED docs should have US training and access for CVC placement 414 (85.2) 30 (6.2) 42 (8.6)ED should have an US credentialing process for all medical staff 326 (67.1) 81 (16.7) 79 (16.3)
CVC, central venous catheter; FACEM, Fellow of Australasian College for Emergency Medicine; US, ultrasound.
Table 4. Perceived barriers to more frequent personal use of US for the 350 who have used US to assist CVC insertion and the 136 whohave not
Have used US atleast rarely
Have never used US ordo not insert CVCs in adults
(n = 360) (n = 136)
No barriers for routine US use: n (%) 143 (40.9) 8 (5.9)No access to US in ED: n (%) 14 (4.0) 40 (29.4)Time delay to perform CVC insertion with US: n (%) 81 (23.1) 7 (5.1)No training or experience to use US: n (%) 37 (10.6) 60 (44.1)US offers no advantages over LM technique: n (%) 19 (5.4) 10 (7.4)Other: n (%) 56 (16.0) 11 (8.1)
Multiple responses were allowed. CVC, central venous catheter; LM, landmark technique; US, ultrasound.
Table 5. Comparison of variables and opinions between FACEMs who usually/always use US for CVC insertion (n = 180) and thosewho either do not use US when inserting CVCs or who do not insert CVCs (n = 306)
Variable FACEM who usually/alwaysuse US for CVC placement
Odds ratio (95% confidence interval)†
Employed at a major referral hospital 1.76 (1.21–2.56)ED has US guidelines 2.49 (1.55–3.99)ED has US credentialing process 2.39 (1.63–3.48)FACEM qualification 1996 or after 1.46 (0.90–2.36)FACEM right (or both) handed 1.45 (0.74–2.85)FACEM completed US course 10.01 (5.45–18.38)Performs 12+ CVC per year 2.60 (1.71–3.93)Preferred site internal jugular 9.63 (6.28–14.74)Confident with US technique 54.59 (26.64–111.88)Use real-time dynamic technique 14.23 (9.09–22.28)Use one-person technique 5.26 (3.50–7.91)Agree that US use should be mandatory for CVC placement 7.87 (5.16–12.00)Disagree that US is only sometimes useful and need not be used as a routine 8.84 (5.68–13.77)Disagree that US has no advantages over the landmark technique 5.18 (2.30–11.66)Agree that US use results in fewer mechanical complications 6.49 (3.87–10.87)Agree that ED should have US training and machine availability 3.07 (1.63–5.77)Agree that ED should have an US credentialing process for all medical staff 2.06 (1.36–3.12)
†Univariate odd ratios, no adjustment for presence/absence of any other variables. CVC, central venous catheter; FACEM, Fellow ofAustralasian College for Emergency Medicine; US, ultrasound.
JT Matera et al.
518 © 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

other hospital specialists was reported to be in the rangeof 11–15%.29–31 More recent international surveys fromthe USA, the UK and Germany have reported increasedroutine ultrasound usage rates of 18–30% by groups ofintensivists, paediatric and cardiac anaesthetists,32–35
with most of these studies also citing lack of ultrasoundavailability, training and a reluctance for ultrasound useto be made mandatory as significant barriers to morewidespread use.29,31,32,34 No current information on ultra-sound usage rates by emergency physicians in othercountries, or by Australasian intensivists or anaesthe-tists could be located.
The type of practice and opinions of the FACEMswho routinely use ultrasound for CVCs is consistentwith the published best practice recommendations of anumber of health bodies, including the ACEM.25–27
These bodies advocate the routine use of ultrasound forCVC placement in the belief that the evidence supportsits advantages in reducing attempt numbers, increasingsuccess rate, reducing time to insertion and reduction ofcomplications but published opinion is not entirelyunanimous. Some maintain that there is little evidenceto support the apparent advantages in critically illpatients, especially in the ED, that many of the compli-cations, which are avoided, are minor and that many ofthe improvements pertain to the internal jugular siterather than the femoral or subclavian veins where thelandmark technique can be more straightforward.36
Ultrasound to assist CVC placement in the ED wasonly first described in 1997 and ED use of ultrasoundfor this purpose, along with assessment of blood loss intrauma and the evaluation of the abdominal aorta hasonly steadily increased over the past 10 years.13–15,37
Given that an ultrasound in the ED is relatively new, itis not surprising that 30% of our respondents had notcompleted an ultrasound training course but this is notentirely ‘generational’ as the percentage of routine ultra-sound users was not significantly higher among thosewho had attained Fellowship after 1996.
It seems intuitive that those who have done an ultra-sound course and use it routinely for CVC insertionshould report having a high degree of confidence with theultrasound technique but it was also the case that routineultrasound users insert CVCs much more frequently thanothers. This raises the issue of the association betweenperforming a critical number of procedures, competenceand confidence. It is unclear if these FACEMs learnt theultrasound technique and became confident using itbecause they were already frequently inserting CVCs orif the learning of the ultrasound technique led to someFACEMs becoming more confident and hence attempt-
ing more CVCs. This issue warrants further explorationbecause it might be that FACEMs whose clinical loadcurrently involves little need for CVCs feel less inclined tolearn the ultrasound technique because skill mainte-nance might be difficult. This was raised by someFACEMs in the free text section and might be reflected inthe fact that those who reported using ultrasound rarelyor never tended to have not done a training course. Itwould be interesting to know if these FACEMs thoughtthey would use ultrasound frequently when, or if, theydid complete a training course. This might be supportedby the finding that the majority of all respondents didbelieve ultrasound had advantages and that training anda subsequent credentialing process should be available.
It was also of interest that 23% of ultrasound usersfelt that ultrasound taking too long was a barrier tomore routine use when the literature suggests that thisis not the case.22–24 This might stem from lack of unifor-mity in study methodology where most researchersreport ‘skin to blood’ time and neglect time taken for thepositioning and preparation of the machine, assemblingthe related equipment and preparatory scanning of theanatomy.38
A recurring free text theme from infrequent users ofultrasound was that they had been successfully employ-ing the landmark technique for years, so had no reasonto change and would be concerned if the advent ofultrasound was associated with a decline in teaching ofthe landmark technique to emergency medicine train-ees. Part of this concern was that the functional pres-ence of the technology could not always be guaranteed.
The present study has a number of limitations, whichwarrant discussion. Non-response bias might be signifi-cant as those who did not respond might have markedlydifferent practices and opinions to those who did. It ispossible that FACEMs who use and support ultrasoundwere more motivated to respond, in which case thepercentage of routine users in the present study wouldbe higher than in the total FACEM population.
The response rate of 42% might be falsely low,because the FACEMs on the ACEM database who areeither no longer practicing at all or are working in areasother than emergency or critical care medicine mighthave been less likely to respond. There was also no wayof knowing if all email addresses on the ACEM databasewere currently active. Survey response rates amonghealth professionals have been reported to be decliningover time.39 The emerging literature suggests that elec-tronic survey response rates might not match those ofhard copy mail-outs.40,41 However, this might be out-weighed by other reported advantages including low
US guidance during CVC insertion in ED
519© 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

costs and reliable information transfer.42,43 Our responserate is at least consistent with previous studies usingunsolicited electronic surveys of emergency physi-cians.44
The validity of newly created questionnaires cannever be proven. Expert focus group input was soughtand pilot trials conducted after which face and contentvalidity seemed reasonable. Elements of this question-naire were also similar to those used in surveys ofpaediatric anaesthetists by Bosman and Kavanagh andcardiovascular anaesthesiologists by Bailey et al., whichsupports construct validity but it still might be that thequestionnaire was not structured in the best way toaccurately deliver the desired information.31,34 Weattempted to limit interviewer bias through the devel-opment stages by attention to wording in order toprevent leading responses. Respondents still mightwish to give answers that they perceive to be ‘correct’and this can also bias results but we would hope thatthe guarantee of confidentiality would minimize thisbias. The descriptors: ‘never’, ‘rarely’, ‘sometimes’,‘usually’ and ‘always’, which were used to describe fre-quency of ultrasound use, are open to individual inter-pretation and the defining of the ‘usual’ and ‘always’respondents as ‘routine’ users is also somewhat arbi-trary. This was felt to be both practical and easier forrespondents as defining quantitative responses, such asultrasound being used 41–60% of the time etc., is stillprone to individual interpretation and recalls bias. Pre-sumably for this reason the published surveys of inten-sivists and anaesthetists in other countries have alsotended to use the same type of adjectival scales.
Conclusion
We found that only 37% of FACEM respondents rou-tinely used ultrasound to guide placement of CVCs in amanner consistent with published best practiceguidelines.25–27 The characteristics, practices and opin-ions of FACEM respondents who routinely use ultra-sound differs significantly from those who do not. Itappears that lack of completion of an ultrasound train-ing course and low exposure to patients requiring CVCsmight be significant barriers to more routine use of theultrasound technique. It is difficult to suggest strategiesthat might improve uptake of ultrasound for CVC inser-tion without further focused research to explore reasonsfor not training in ultrasound and the role that likelyexposure to a ‘critical number’ of CVCs might play inboth motivation and ongoing skill maintenance.
Acknowledgements
The authors would like to thank all emergency physi-cians who responded to this survey and the administra-tive staff of ACEM for their help with distribution of thequestionnaire.
Author contributions
JM, major role in literature search, formulation of studyquestion, questionnaire design and manuscript prepara-tion. DEW, major role in formulation of study question,significant assistance in literature search, questionnairedesign and manuscript preparation. RM, major role instatistical analysis, significant assistance in formulationof study question and manuscript preparation.
Competing interests
None declared.
Accepted 28 July 2010
References
1. Roberts JR, Hedges JR, Chanmugam AS et al. Clinical Proceduresin Emergency Medicine 2004, 4th edn. Philadelphia: WBSaunders.
2. Hind D, Calvert N, McWilliams R et al. Ultrasonic locatingdevices for central venous cannulation: meta-analysis. BMJ 2003;327: 361.
3. Merrer J, De Jonghe B, Golliot F et al. Complications of femoraland subclavian venous catheterization in critically ill patients: arandomized controlled trial. JAMA 2001; 286: 700–7.
4. McGee D, Gould M. Current concepts: preventing complicationsof central venous catheterization. N. Engl. J. Med. 2003; 348:1123–33.
5. Sznajder JI, Zveibil FR, Bitterman H, Weiner P, Bursztein S.Central vein catheterization: failure and complication rates bythree percutaneous approaches. Arch. Intern. Med. 1986; 146:259–61.
6. Steele R, Irwin CB. Central line mechanical complication rate inemergency medicine patients. Acad. Emerg. Med. 2001; 8: 204–7.
7. Mansfield PF, Hohn DC, Fornage BD et al. Complications andfailures of subclavian-vein catheterization. N. Engl. J. Med. 1994;331: 1735–8.
8. Legler D, Nugent M. Doppler localization of the internal jugularvein facilitates central venous catheterization. Anesthesiology1984; 60: 481–2.
JT Matera et al.
520 © 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

9. Yonei A, Nonoue T, Sari A. Real-time ultrasonic guidance forpercutaneous puncture of the internal jugular vein. Anesthesiol-ogy 1986; 64: 830–1.
10. Randolph AG, Cook DJ, Gonzales CA et al. Ultrasound guidancefor placement of central venous catheters: a meta-analysis of theliterature. Crit. Care Med. 1996; 24: 2053–8.
11. Keenan SP. Use of ultrasound to place central lines. J. Crit. Care2002; 17: 126–37.
12. Hudson PA, Rose JS. Real-time ultrasound guided internaljugular vein catheterization in the emergency department. Am. J.Emerg. Med. 1997; 15: 79–82.
13. Brenchley J, Sloan JP, Thompson PK. Echoes of things to come.Ultrasound in UK emergency medicine practice. J. Accid. Emerg.Med. 2000; 17: 170–5.
14. McLaughlin RE, Lee A, Clenaghan S, McGovern S, Martyn C,Bowra J. Survey of attitudes of senior emergency physicianstowards the introduction of emergency department ultrasound.Emerg. Med. J. 2005; 22: 553–5.
15. Fluman KR, Theodoro DL, Adhikari S. Emergency physicianattitudes regarding ultrasound-guided central venous cannula-tion. Ann. Emerg. Med. 2008; 51: 545.
16. Lefrant JY, Cuvillon P, Benezet JF et al. Pulsed Doppler ultra-sonography guidance for catheterization of the subclavian vein: arandomized study. Anesthesiology 1998; 88: 1195–201.
17. Bold RJ, Winchester DJ, Madary AR, Gregurich MA, MansfieldPF. Prospective, randomized trial of Doppler-assisted subclavianvein catheterization. Arch. Surg. 1998; 133: 1089–93.
18. Atkinson P, Boyle A, Robinson S, Campbell-Hewson G. Shouldultrasound guidance be used for central venous catheterisation inthe emergency department? Emerg. Med. J. 2005; 22: 158–64.
19. Milling T, Rose J, Briggs W. Randomized, controlled clinical trialof point-of-care limited ultrasonography assistance of centralvenous cannulation: The Third Sonography Outcomes Assess-ment Program (SOAP-3) Trial. Crit. Care Med. 2005; 33: 1764–9.
20. Dunning J, James Williamson J. Ultrasonic guidance and thecomplications of central line placement in the emergency depart-ment. Emerg. Med. J. 2003; 20: 551–2.
21. Hrics P, Wilber S, Blanda MP. Ultrasound assisted internaljugular vein catheterization in the ED. Am. J. Emerg. Med. 1998;16: 401–3.
22. Hilty W, Hudson P, Levitt AM. Real-time ultrasound guidedfemoral vein catheterization during cardiopulmonary resuscita-tion. Ann. Emerg. Med. 1997; 29: 331–6.
23. Miller AH, Roth BA, Mills TJ et al. Ultrasound guidance versusthe landmark technique for the placement of central venous cath-eters in the emergency department. Acad. Emerg. Med. 2002; 9:800–5.
24. Leung J, Finckh A, Duffy M. Real-time ultrasonography-guidedinternal jugular vein catheterization in the emergency depart-ment increases success rates and reduces complications: a ran-domized, prospective study. Ann. Emerg. Med. 2006; 48: 540–7.
25. NHS National Institute for Clinical Excellence. Guidance on theuse of ultrasound locating devices for placing central venous cath-eters. [policy guideline]. September 2002. [Cited 15 May 2009.]Available from URL: http://www.nice.org.uk/nicemedia/pdf/Ultrasound_49_GUIDANCE.pdf
26. American College of Emergency Physicians. American College ofEmergency Physicians Policy Statement: Emergency UltrasoundGuidelines. Dallas: American College of Emergency Physicians,Approved October 2008. [Cited 15 May 2009.] Availablefrom URL: http://www.acep.org/workarea/downloadasset.aspx?id=32878
27. Australasian College for Emergency Medicine Policy Document– Use of bedside ultrasound by emergency physicians. Adoptedby Council July 1999, Reviewed March 2006. [Cited 15 May 2009.]Available from URL: http://www.acem.org.au/media/policies_and_guidelines/P21_Policy_on_Use_of_Bedside_Ultrasound.pdf
28. Dent AW, Asadpour A, Weiland TJ, Paltridge D. Australasianemergency physicians: a learning and educational needs analy-sis. Part One. Emerg. Med. Australas. 2008; 20: 51–7.
29. Jefferson P, Ogbue MN, Hamilton KE, Ball DR. A survey of theuse of partable ultrasound for central vein cannulation on criticalcare units in the UK. Anaesthesia 2002; 57: 365–8.
30. Girard TD, Schectman JM. Ultrasound guidance during centralvenous catheterization: a survey of use by house staff physicians.J. Crit. Care 2005; 20: 224–9.
31. Bosman M, Kavanagh RJ. Two dimensional ultrasound guidancein central venous catheter placement: a postal survey of thepractice and opinions of consultant pediatric anesthetists in theUnited Kingdom. Paediatr. Anaesth. 2006; 16: 530–7.
32. Schummer W, Sakka SG, Huttemann E, Reinhart K, SchummerC. Ultrasound guidance for placement control of central venouscatheterization. Survey of 802 anesthesia departments for 2007 inGermany. Anaesthetist 2009; 58: 677–85.
33. Tovey G, Stokes M. A survey of the use of 2D ultrasoundguidance for insertion of central venous catheters by UK con-sultant paediatric anaesthetists. Eur. J. Anaesth. 2007; 24: 71–5.
34. Bailey PL, Glance LG, Eaton MP, Parshall B, McIntosh S. Asurvey of the use of ultrasound during central venous catheter-ization. Anesth. Analg. 2007; 104: 491–7.
35. McGratten T, Duffty J, Green JS, O’Donnell N. A survey of the useof ultrasound guidance in internal jugular venous cannulation.Anaesthesia 2008; 63: 1222–5.
36. Chikungwa M, Lim M. Ultrasound guidance for central venouscatheter insertion. Emerg. Med. J. 2005; 22: 608–9.
37. McLaughlin R, Collum N, McGovern S, Martyn C, Bowra J. Emer-gency department ultrasound (EDU): clinical adjunct or play-thing? Emerg. Med. J. 2005; 22 (3): 333–5.
38. Sabbaj A, Hedges JR. Ultrasonographic guidance for internaljugular vein cannulation: an educational imperative, a desirablepractice alternative. Ann. Emerg. Med. 2006; 48: 548–50.
39. Kellerman SE, Herold J. Physician response to surveys: a reviewof the literature. Am. J. Prev. Med. 2001; 20: 61–7.
40. Seguin R, Godwin M, MacDonald S, McCall M. E-mail or snailmail? Randomized controlled trial on which works better forsurveys. Can. Fam. Physician 2004; 50: 414–19.
41. VanDenKerkhof EG, Parlow JL, Goldstein DH, Milne B. InCanada, anesthesiologists are less likely to respond to an elec-tronic, compared to a paper questionnaire. Can. J. Anaesth. 2004;51: 449–54.
42. Braithwaite D, Emery J, De Lusignan S, Sutton S. Using theInternet to conduct surveys of health professionals: a valid alter-native? Fam. Pract. 2003; 20: 545–51.
US guidance during CVC insertion in ED
521© 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
43. Leece P, Bhandari M, Sprague S et al. Internet versus mailedquestionnaires: a randomized comparison (2). J. Med. InternetRes. 2004; 6: e30.
44. Alves DW, Szucs PA. The demographics of e-mail for emergencymedicine research. Am. J. Emerg. Med. 2001; 19 (3): 192–5.
Appendix I
Summarized questionnaire
Hospital characteristics1. Which of the following best describes your principal place of employment:
a. Major referral centreb. Urban district hospitalc. Regional referral centred. Private hospitale. Other
2. What is the annual attendance of your ED?a. <10 0000b. 10 000–20 000c. 20 000–30 000d. 30 000–40 000e. 40 000–50 000f. >50 000
3. Which best describes the patient population of your ED?a. Adult patients onlyb. Paediatric (<16 years old) patients onlyc. Both adult and paediatric patients
4. Does your ED have access to ultrasound, which can be used for vascular access?a. Yes/No
5. Does your ED have a guideline for the insertion of CVC?a. Yes/No/Unsure
6. If there is a CVC guideline does it recommend ultrasound guidance?a. Yes/No/Unsure/NA
7. Does your ED have a credentialing process for the use of ultrasound?a. Yes/No/Unsureb. No but in the process of developing one
FACEM characteristics8. What year did you complete your Fellowship in Emergency Medicine?
a. 2006 and afterb. 2001–2005c. 1996–2000d. 1991–1995e. 1986–1990f. before 1986
9. What is your dominant hand?a. Right/Left/Bimanual
10. Have you attended an ultrasound course/workshop, which included ultrasound-guided vascular access?a. Yes/No
11. Do you insert CVC in adults (>16 years old)?a. Yes/No
JT Matera et al.
522 © 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
FACEM work practice12. Approximately how many CVC do you insert in adults per year?
a. 1–5b. 6–11c. 12–24d. 25–42e. >42
13. What is your preferred vessel for CVC placement?a. Femoralb. Internal jugularc. SubclavianResponse to questions 14, 15 and 16 used the adjectival scale: Never, Rarely, Sometimes, Usually,
Always (without further qualification)14. How often do you feel confident using the landmark technique for CVC placement?15. How often do you use ultrasound to assist CVC insertion?16. How often do you feel confident using ultrasound to guide CVC insertion?17. Which statement best describes your use of ultrasound for CVC insertion?
a. Don’t use ultrasound for CVC placementb. Dynamic (real-time) ultrasound guidance during the CVC insertionc. Static ultrasound to screen vessel anatomy and mark puncture sited. Rescue use only after failure using landmark techniquee. Other
Technical questions18. What type of ultrasound machine is available in your ED?
a. Free text description19. Do you use one- or two-person technique for ultrasound-guided CVC placement?
a. One/Two20. What type of probe do you use?
a. Linear/Dedicated vascular/Other21. What type of probe cover do you use?
a. Dedicated sterile sheath/Large opsite/Sterile glove/Other22. Do you use ‘Echo tip’ needle?
a. Yes/NoFACEM opinions: Response to questions 23–29 used the adjectival scale of Strongly Agree, Agree, No opinion,Disagree, Strongly Disagree23. Use of ultrasound should be mandatory for CVC insertion in the ED24. Ultrasound is of benefit in some circumstances but use needn’t be routine25. Ultrasound has no advantages over the landmark technique26. Ultrasound guidance for CVC reduces the mechanical complications27. All ED doctors should train in ultrasound use for CVC insertion28. ED should have a credentialing process for ultrasound use by junior medical staff for CVC insertion29. ED should have a credentialing process for ultrasound use by ALL medical staff for CVC insertion30. Why might you not use ultrasound routinely for CVC insertion?
a. N/A – Do use ultrasound routinelyb. Don’t have access to ultrasound in the EDc. Don’t have appropriate training/experience for ultrasound used. Ultrasound use involves time delay for CVC insertione. In my clinical practice, ultrasound offers no advantage for CVC insertionf. Other – free text
US guidance during CVC insertion in ED
523© 2010 The AuthorsEMA © 2010 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine





























