Embed Size (px)
Citation preview

C
Ud
SCCa
b
a
ARR1A
KIULRAEOSA
1
1
gew
i
U2
m
0d
Resuscitation 83 (2012) 307– 312
Contents lists available at SciVerse ScienceDirect
Resuscitation
jo u rn al hom epage : www.elsev ier .com/ locate / resusc i ta t ion
linical paper
ltrasonographic lung sliding sign in confirming proper endotracheal intubationuring emergency Intubation�
hyh-Shyong Sima,b, Wan-Ching Liena, Hao-Chang Choua, Kah-Meng Chonga,b, Shih-Hung Liua,hih-Hung Wanga, Shey-Yin Chena, Chiung-Yuan Hsua, Zui-Shen Yena, Wei-Tien Changa,hien-Hua Huanga, Matthew Huei-Ming Maa,∗, Shyr-Chyr Chena
Department of Emergency Medicine, National Taiwan University Hospital, Taipei City, TaiwanDepartment of Emergency Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan
r t i c l e i n f o
rticle history:eceived 15 September 2011eceived in revised form0 November 2011ccepted 13 November 2011
eywords:ntubationltrasoundung slidingesuscitationirway managementndobronchial intubationne-lung intubationliding lung sign
a b s t r a c t
Aim of study: Unrecognized one-lung intubations (also known as main-stem intubation) can lead tohypoventilation, atelectasis, barotrauma, and even patient death. Many traditional methods can beemployed to detect one-lung intubation; however, each of these methods has limitations and is notconsistently reliable in emergency settings. This study aimed to assess the accuracy and timeliness ofultrasound to confirm proper endotracheal intubation.Methods: This was a prospective, single-center, observational study conducted at the emergency depart-ment of a national university teaching hospital. Patients received emergency tracheal intubation becauseof respiratory failure or cardiac arrest. After intubation, bedside ultrasound was performed with a trans-ducer placed on the chest bilaterally at the mid-axillary line, to identify lung sliding over the lungsbilaterally during ventilation. Chest radiography was used as the criterion standard for confirmation ofendotracheal tube position.Results: One hundred and fifteen patients needing tracheal intubation were included, and nine (7.8%)had one-lung intubations. The overall accuracy of ultrasound to confirm proper endotracheal intubationwas 88.7% (95% confidence interval (CI): 81.6–93.3%). The positive predictive value was 94.7% (95% CI:
irway87.1–97.9%) in the non-cardiac-arrest group and 100% (95% CI: 87.1–100.0%) in the cardiac-arrest group.The median operating time of ultrasound was 88 s (interquartile range [IQR]: 55.0, 193.0), and of chestradiography was 1349 s (IQR: 879.0, 2221.0) post intubation.Conclusions: In this study, the positive predictive value of bilateral lung sliding in confirming proper endo-tracheal intubation was high, especially among patients with cardiac arrest. Considerable time advantageof ultrasound over chest radiography was demonstrated.
© 2011 Elsevier Ireland Ltd. All rights reserved.
. Introduction
.1. Background
According to the 2010 advanced cardiac life support (ACLS)
uidelines, adequate support of ventilation during resuscitation isssential.1 Currently, endotracheal intubation serves as definite air-ay control during resuscitation; however, it has been associated� A Spanish translated version of the summary of this article appears as Appendixn the final online version at doi:10.1016/j.resuscitation.2011.11.010.∗ Corresponding author at: Department of Emergency Medicine, National Taiwanniversity Hospital, No. 7 Chung-Shan South Road, Taipei 100, Taiwan. Tel.: +886 2312 3456x62831; fax: +886 2 2322 3150.
E-mail addresses: vin [email protected] (S.-S. Sim), [email protected],[email protected] (M.H.-M. Ma).
300-9572/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.resuscitation.2011.11.010
with a 6–25% incidence of unrecognized tube misplacement.2–6
Unrecognized one-lung intubation can lead to hypoventilation,atelectasis, barotrauma, and even patient death. Traditionally, thechest is auscultated bilaterally, but this method is not reliable.In fact, up to 55% of one-lung intubation would be missed byauscultation.7 Chest radiography provides definitive confirmationof tube location, but is time-consuming, and is not available inmany emergency settings, such as the site of in-hospital arrest, orout-of-hospital locations.
Waveform capnography is recommended as the most reliablemethod for confirming and monitoring correct placement of anendotracheal tube6,8–11; however, capnography cannot distinguish
endobronchial from endotracheal placement of the endotrachealtube. Thus, a secondary confirmation tool that balances accuracyand availability is required for confirming proper endotrachealintubation during resuscitation in emergency settings.
3 citatio
1
admic(iscinsse
1
ie
2
2
dRtwta
2
bnatw
2
oteomwbmtius
estls
08 S.-S. Sim et al. / Resus
.2. Importance
Ultrasound is a common tool in emergency departments (EDs)nd intensive care units (ICUs). The utility of ultrasound has beenescribed in various fields in acute care,12 including the confir-ation of endotracheal tube placement.13 Proper endotracheal
ntubation means that the tip of the endotracheal tube is in the tra-hea, without advancement beyond the carina and into a bronchusgenerally known as one-lung intubation). Previous reports, includ-ng cadaver studies and small case series, have described the highensitivity and specificity of ultrasonographic lung sliding sign inonfirmation of endotracheal tube placement.14–16 In addition todentifying tracheal intubation, the absence of lung sliding was alsooticed in some cases of one-lung intubation. Therefore, furthertudy is warranted to validate the utility of ultrasonographic lungliding sign in confirming proper endotracheal intubation duringmergency intubation.14
.3. Goals of this investigation
This study aimed to assess the utility of ultrasound lung slid-ng sign in confirming proper endotracheal tube placement duringmergency intubation.
. Materials and methods
.1. Study design and setting
This was a prospective, single-center, observational study con-ucted between March 2010 and February 2011. The Institutionaleview Board of the National Taiwan University Hospital approvedhe study protocol with a waiver of informed consent. All subjectsere recruited from the ED of National Taiwan University Hospi-
al, which is a 2000-bed, tertiary teaching hospital. The ED has annnual census of over 100,000 patients.
.2. Selection of participants
We enrolled patients who underwent emergency intubationecause of impending respiratory failure or cardiac arrest. Patientsot in cardiac arrest received sedation with or without paralysiss judged by clinical conditions. Patients with penetrating chestrauma or esophageal intubation, and those under 18 years of ageere excluded.
.3. Methods and measurements
This study was parallel to the study reported by Chou et al. fromur group.13 There were 23 overlaps of patient cohort betweenhe two studies. Emergency intubations were performed by seniormergency medicine residents, supervised by attending physiciansn duty. Post-intubation confirmation of endotracheal tube place-ent was checked by auscultation, pulse oximetry and quantitativeaveform capnography. After excluding esophageal intubation,
edside ultrasound was performed by two senior emergencyedicine residents who had completed 2 months of ultrasound
raining course (including abdominal, thoracic ultrasound) dur-ng their clinical rotation. They also completed a two-day certifiedltrasound course with didactic and practicum components spon-ored by the Taiwan Society of Emergency Medicine.
A Toshiba Viamo ultrasound scanner (Toshiba, Tokyo, Japan)quipped with a 3.75 MHz convex transducer was used for ultra-
onography. A transducer was placed on both sides of the chest inhe mid-axillary line around 4th–5th intercostal space, to identifyung sliding bilaterally over the lungs after intubation (Fig. 1A). Thecanning time was restricted so as to make it as short as possible; ton 83 (2012) 307– 312
avoid interruption of chest compression in cardiac arrest patients,we scanned the patients during the pause of chest compression, thescanning time was restricted to 10 s over one side (the scan of theother side had to be done over next pause of compression). For thenon-cardiac arrest patients, the scanning time could be more flex-ible. Images, including thermo-paper hard copies, were stored forlater review. Chest radiography was performed after every emer-gency intubation, which was used as the criterion standard forconfirming proper endotracheal intubation.
The criteria for identification of the lung sliding in relation to theposition of the endotracheal tube are as follows. When the endotra-cheal tube is in the correct position, the lung inflates and deflateswith ventilations, causing the parietal and visceral pleura to glideover each other (Fig. 1B). If the endotracheal tube were in one of themain bronchi, absence of lung sliding sign would be noted over thecontralateral side during ventilation (Fig. 1D). The presence of lungpulse, a vertical movement of the pleural line synchronous to thecardiac rhythm, could be noted during absence of lung sliding innon-cardiac arrest patients (Fig. 1C). The presence of bilateral lungsliding during ultrasound examination is used as ultrasonographicconfirmation of proper endotracheal intubation.
2.4. Outcome measures
The primary outcome measure was the accuracy of the ultra-sonographic lung sliding sign compared with the criterion standardof chest radiography for confirming proper endotracheal tube posi-tion in emergency intubation. The secondary outcome measurewas the timeliness of ultrasound as compared with that of chestradiography.
2.5. Data collection and processing
The emergency room nurses recorded each enrolled subject’sage, height, weight, body mass index (BMI), underlying medicalconditions, and the time of intubation. The sonographer recordedultrasound operating time and the time when chest radiographwas performed. The sonographer recorded results of ultrasoundinterpretation on separate data collection sheets.
2.6. Primary data analysis
All statistical analyses were performed using SPSS statisticalsoftware, version 18.0 (SPSS Inc., Chicago, IL, USA). Sensitivity,specificity, positive predictive value (PPV), and negative predictivevalue (NPV) were calculated by standard formulas for a binomi-nal proportion. The corresponding 95% confidence intervals (CIs)were calculated by the Wilson interval method.17,18 We calcu-lated sensitivity, specificity, PPV, and NPV for ultrasound againstchest radiography as the criterion standard. The accuracy of atest was determined by dividing the sum of the true positiveand true negative results by the total number of subjects. As thisstudy was designed to show that ultrasound is not inferior tothe criterion standard test (i.e. chest radiography); we specifiedone-sided hypothesis in statistical testing. Any p value <0.05 wasconsidered statistically significant. Comparisons of the test char-acteristics of ultrasound and chest radiography were comparedusing McNemar’s test. Subgroup analysis of the non-cardiac-arrestand cardiac-arrest patients was performed using Fisher’s exacttest. The difference in the mean operating time between non-
cardiac-arrest and cardiac-arrest group were analyzed by using theMann–Whitney U test. Stepwise logistic regression analysis wasconducted to discover the factors associated with the diagnosticaccuracy of ultrasound, as compared with chest radiography.
S.-S. Sim et al. / Resuscitation 83 (2012) 307– 312 309
Fig. 1. Demonstration of lung sliding: (A) longitudinal scan over an intercostal space, pleural lines (arrow), ribs (triangle). (B) Dynamic lung sliding generated sandy patterno ing: (fl g pulst
3
3
ptTd1wtvt
3
Tnssl(
3
pa(uug(o
ver M-mode, generally called a seashore sign. Demonstration of absence of lung sliductuation (heart shape) with heart beat over M-mode, this pattern is called the lunhis pattern is called the stratosphere sign.
. Results
.1. Characteristics of study subjects
A total of 115 patients, 24–94 years of age, were enrolled in thisrospective study (Fig. 2). Their demographics and clinical charac-eristics are listed in Table 1. The mean age was 67.5 ± 17.4 years.he mean BMI was 23.5 ± 5.1 kg/m2. There were 31 cases of car-iac arrest, including 20 out-of-hospital cardiac arrests (OHCA) and1 in-hospital cardiac arrests (IHCA). The remaining 84 patientsere intubated for other medical emergencies. One-lung intuba-
ion occurred more often in the elderly group (mean age 77.6 ± 5.0s. 66.7 ± 17.0, p < 0.001), female (88.9% vs. 39.6%, p = 0.004) and inhe trauma group (22.2% vs. 4.7%, p = 0.036).
.2. Main results
The results of ultrasound identifications are shown in Table 2.here were nine one-lung intubations (7.8%), including seven inon-cardiac-arrest patients and two in cardiac-arrest patients. Theensitivity, specificity, PPV, and NPV of the ultrasonographic lungliding sign, using chest radiography as the criterion standard, areisted in Table 3. The overall accuracy of the ultrasound was 88.7%95% CI: 81.5–93.8%).
.3. Subgroup analysis
The diagnostic value of ultrasound lung sliding in confirmingroper endotracheal intubation was better among cardiac-rrest patients, when compared with non-cardiac-arrest patientsTable 3). The comparison of the required operating time betweenltrasound detection and chest radiography is shown in Table 4. The
ltrasound detection took significantly less time than chest radio-raphy in both the non-cardiac arrest and cardiac arrest groupsp < 0.001). In a logistic regression model, the diagnostic accuracyf ultrasound against chest radiography is not influenced by age,C) absence of lung sliding produced succession of horizontal lines with intermittente. (D) Absence of lung sliding produced succession of horizontal lines over M-mode,
gender, BMI, the length of intubation time, the length of ultrasoundoperating time, daytime vs. nighttime, or individual sonographers.
4. Discussion
This study was designed to assess the accuracy of the ultra-sound lung sliding in identifying endotracheal tube position afteremergency intubation, as compared with chest radiography. Theoverall results of this study demonstrated that ultrasound was notequivalent to chest radiography in identifying endotracheal tubeposition; however, among patients with cardiac arrest, the posi-tive predictive value of bilateral lung sliding for confirming properendotracheal intubation was very high. During emergency intuba-tion, using ultrasound to confirm proper endotracheal intubationis feasible and timely, with a satisfactory predictive value amongpatients with cardiac arrest.
Ultrasonographic ‘lung sliding sign’ indicates the gliding of pari-etal pleura and visceral pleura as the lung inflates and deflates withrespiration, with intact anatomy. The absence of the lung slidingsuggests that either the pleura are not normally apposed (as hap-pens in a pneumothorax), or that the lung is not moving as it should.Currently, the lung sliding is commonly acknowledged as a sign toexclude pneumothorax.19
Unilateral absence of lung sliding alone after intubation is inad-equate to confirm one-lung intubation. Other causes of unilaterallung sliding despite proper intubation (false negative) includesunderlying pulmonary malignancies, pneumothorax, pleural effu-sion, or other factors that lead to unilateral inadequate ventilation.On the other hand, a false-positive test, i.e. bilateral lung slid-ing observed during one-lung intubation, might occur when thereis spontaneous breathing. This may explain the lower positivepredictive value of ultrasound lung sliding in identifying properintubation among the non-cardiac arrest vs. the cardiac arrest
group.Accidental one-lung intubation occurs in about 5% of patientsin intensive care, 28% of those with a cardiac arrest, and10% of out-of-hospital endotracheal intubations.20–22 Currently

310 S.-S. Sim et al. / Resuscitation 83 (2012) 307– 312
y flow
wmecp
pestt
Fig. 2. Stud
aveform capnography is recommended as the most reliableethod of confirming and monitoring correct placement of an
ndotracheal tube1; however, the implementation of waveformapnography cannot distinguish endobronchial from endotracheallacement of the endotracheal tube.
The assessments of physical examination are often unreliable inrehospital and emergency room settings, even in well-controlled
nvironment as operating room. A recently published studyhowed that 55% of one-lung intubation was missed by auscul-ation. In the study, Sitzwohl et al. proposed that the best wayo rule out one-lung intubation is by using the combination ofdiagram.
optimal endotracheal tube insertion depths and physical exami-nation, including auscultation and observation of the symmetry ofchest movements.7
Previous studies demonstrated the high sensitivity of theultrasound lung sliding in identifying proper endotrachealintubation.14–16 For example, Weaver et al. conducted cadaverstudies, showing that lung sliding is accurate for confirmation
of endotracheal tube placement.14 In 2004, Chun et al. revealedthat the lung sliding correlated well with endotracheal tubeplacement16; however, the number of cases was very small, andthe final confirmation was by auscultation by an anaesthesiologist,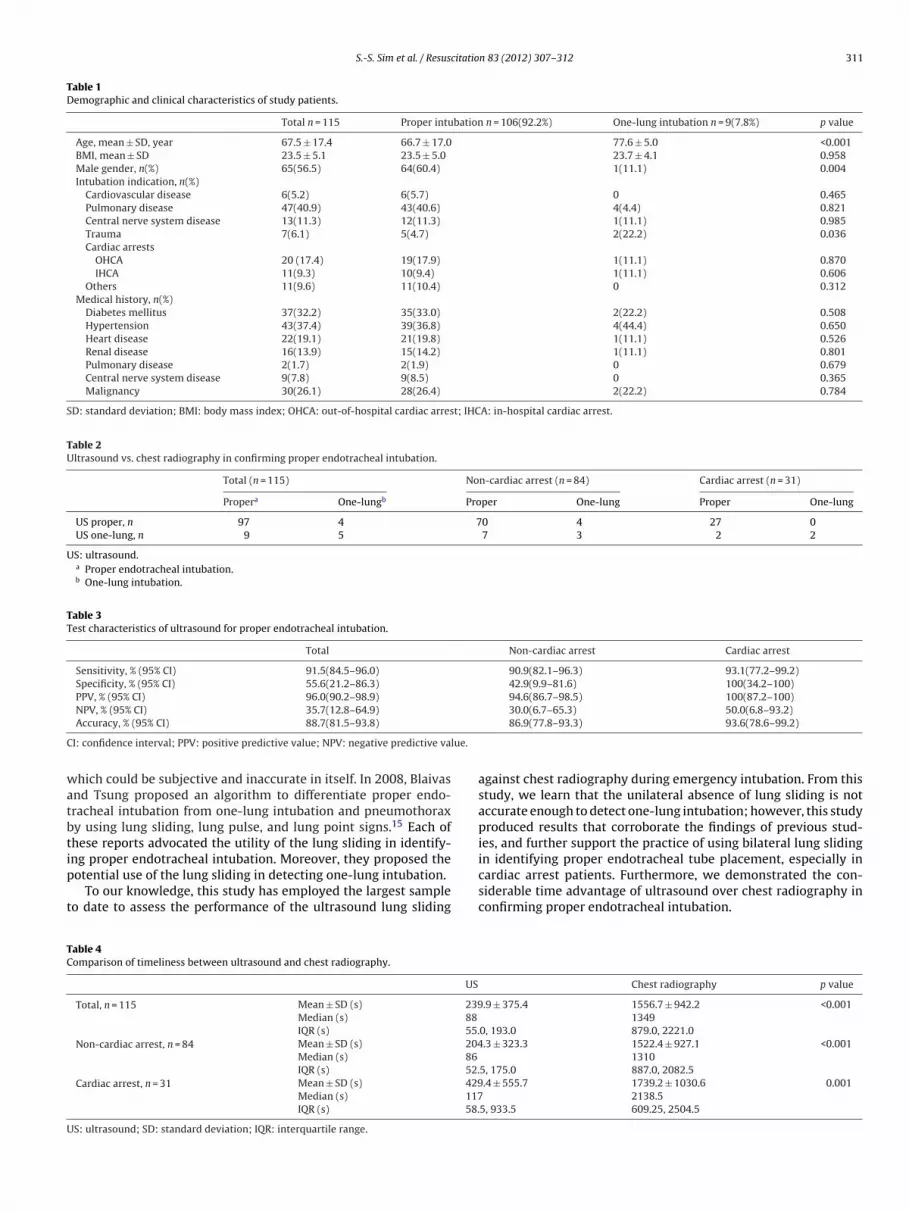
S.-S. Sim et al. / Resuscitation 83 (2012) 307– 312 311
Table 1Demographic and clinical characteristics of study patients.
Total n = 115 Proper intubation n = 106(92.2%) One-lung intubation n = 9(7.8%) p value
Age, mean ± SD, year 67.5 ± 17.4 66.7 ± 17.0 77.6 ± 5.0 <0.001BMI, mean ± SD 23.5 ± 5.1 23.5 ± 5.0 23.7 ± 4.1 0.958Male gender, n(%) 65(56.5) 64(60.4) 1(11.1) 0.004Intubation indication, n(%)
Cardiovascular disease 6(5.2) 6(5.7) 0 0.465Pulmonary disease 47(40.9) 43(40.6) 4(4.4) 0.821Central nerve system disease 13(11.3) 12(11.3) 1(11.1) 0.985Trauma 7(6.1) 5(4.7) 2(22.2) 0.036Cardiac arrests
OHCA 20 (17.4) 19(17.9) 1(11.1) 0.870IHCA 11(9.3) 10(9.4) 1(11.1) 0.606
Others 11(9.6) 11(10.4) 0 0.312Medical history, n(%)
Diabetes mellitus 37(32.2) 35(33.0) 2(22.2) 0.508Hypertension 43(37.4) 39(36.8) 4(44.4) 0.650Heart disease 22(19.1) 21(19.8) 1(11.1) 0.526Renal disease 16(13.9) 15(14.2) 1(11.1) 0.801Pulmonary disease 2(1.7) 2(1.9) 0 0.679Central nerve system disease 9(7.8) 9(8.5) 0 0.365Malignancy 30(26.1) 28(26.4) 2(22.2) 0.784
SD: standard deviation; BMI: body mass index; OHCA: out-of-hospital cardiac arrest; IHCA: in-hospital cardiac arrest.
Table 2Ultrasound vs. chest radiography in confirming proper endotracheal intubation.
Total (n = 115) Non-cardiac arrest (n = 84) Cardiac arrest (n = 31)
Propera One-lungb Proper One-lung Proper One-lung
US proper, n 97 4 70 4 27 0US one-lung, n 9 5 7 3 2 2
US: ultrasound.a Proper endotracheal intubation.b One-lung intubation.
Table 3Test characteristics of ultrasound for proper endotracheal intubation.
Total Non-cardiac arrest Cardiac arrest
Sensitivity, % (95% CI) 91.5(84.5–96.0) 90.9(82.1–96.3) 93.1(77.2–99.2)Specificity, % (95% CI) 55.6(21.2–86.3) 42.9(9.9–81.6) 100(34.2–100)PPV, % (95% CI) 96.0(90.2–98.9) 94.6(86.7–98.5) 100(87.2–100)NPV, % (95% CI) 35.7(12.8–64.9) 30.0(6.7–65.3) 50.0(6.8–93.2)
C lue.
watbtip
t
TC
U
Accuracy, % (95% CI) 88.7(81.5–93.8)
I: confidence interval; PPV: positive predictive value; NPV: negative predictive va
hich could be subjective and inaccurate in itself. In 2008, Blaivasnd Tsung proposed an algorithm to differentiate proper endo-racheal intubation from one-lung intubation and pneumothoraxy using lung sliding, lung pulse, and lung point signs.15 Each ofhese reports advocated the utility of the lung sliding in identify-
ng proper endotracheal intubation. Moreover, they proposed theotential use of the lung sliding in detecting one-lung intubation.To our knowledge, this study has employed the largest sampleo date to assess the performance of the ultrasound lung sliding
able 4omparison of timeliness between ultrasound and chest radiography.
US
Total, n = 115 Mean ± SD (s) 239Median (s) 88
IQR (s) 55.Non-cardiac arrest, n = 84 Mean ± SD (s) 204
Median (s) 86
IQR (s) 52.Cardiac arrest, n = 31 Mean ± SD (s) 429
Median (s) 117IQR (s) 58.
S: ultrasound; SD: standard deviation; IQR: interquartile range.
86.9(77.8–93.3) 93.6(78.6–99.2)
against chest radiography during emergency intubation. From thisstudy, we learn that the unilateral absence of lung sliding is notaccurate enough to detect one-lung intubation; however, this studyproduced results that corroborate the findings of previous stud-ies, and further support the practice of using bilateral lung sliding
in identifying proper endotracheal tube placement, especially incardiac arrest patients. Furthermore, we demonstrated the con-siderable time advantage of ultrasound over chest radiography inconfirming proper endotracheal intubation.Chest radiography p value
.9 ± 375.4 1556.7 ± 942.2 <0.0011349
0, 193.0 879.0, 2221.0.3 ± 323.3 1522.4 ± 927.1 <0.001
13105, 175.0 887.0, 2082.5.4 ± 555.7 1739.2 ± 1030.6 0.001
2138.55, 933.5 609.25, 2504.5

3 citatio
icotptsbtue
(iaocei
pgcidt
atitceccbbti
ruocst
mnaoTs
5
fico
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
12 S.-S. Sim et al. / Resus
Another ultrasound sign that deserved discussion in the settings lung pulse, which is a vertical movement of the pleural line syn-hronous to the cardiac rhythm. It is more prominent in the absencef lung sliding, and could be used to confirm complete atelectasis oro exclude pneumothorax.23,24 In the absence of lung sliding, lungulse could mimic lung sliding. The sonographer should be aware ofhis possibility, although it would not occur in cardiac arrest. In thistudy, some of the observed false positive cases (i.e. one lung intu-ation with bilateral lung sliding) could actually be lung pulse. Ifhese cases were differentiated more properly, the diagnostic val-es of lung sliding in determining one lung intubation would beven higher.
A recent published protocol, the tracheal rapid ultrasound examTRUE), was proposed as a confirmation tool after emergencyntubation.13 The TRUE showed high accuracy with significant timedvantage. The combination of TRUE with immediate observationf lung sliding potentially provides us a new protocol for moreomprehensive confirmation of endotracheal tube placement aftermergency intubation,25 especially in cardiac arrest, while minimalnterruption of chest compression is anticipated.
To date, there is no single method or rule that can reliablyrevent or detect one-lung intubation completely during emer-ency intubation; however, we believe that one-lung intubationan be prevented maximally by practicing the combination of clin-cal assessment, respecting optimal endotracheal tube insertionepths, and ultrasound examination. Further studies, which takehese variables into account, will need to be undertaken.
There were several limitations in our study. First, cases of cardiacrrest were fewer than those of non-cardiac-arrest; there were onlywo cases of one-lung intubation in the cardiac-arrest group. Dur-ng cardiac arrest, chest radiography is usually not obtained unlesshe resuscitation succeeds in achieving return of spontaneous cir-ulation; the utility of bedside ultrasound during resuscitation withmergency intubation is particularly practical. More cardiac arrestases will be needed to validate the agreement of ultrasound withhest radiography. Second, we did not specify whether the patienteing intubated had been paralyzed. It is possible for lung sliding toe present in patients of one-lung intubation with preserved spon-aneous breathing. These may account for the false positive casesn the non-cardiac-arrest group.
Third, the sonographers in our study were emergency medicineesidents who underwent standardized education in emergencyltrasound during residency. The ultrasound examination dependsn the performer’s skill and experience. Although the learningurve of ultrasound lung sliding has not been evaluated, we believetrongly that more-experienced sonographers would produce bet-er agreement with chest radiography.
Fourth, we didn’t include the lung pulse and diaphragmaticovement into our study design as we aimed to assess the diag-
ostic value of lung sliding. Scanning diaphragmatic movement isnother ultrasound examination that previously proposed as a sec-ndary confirmation tool of proper endotracheal intubation.26,27
he potential implication of these additional ultrasonographicigns should be addressed in future ultrasound protocol.
. Conclusions
The positive predictive value of bilateral lung sliding in con-rming proper endotracheal intubation was high, especially amongardiac-arrest patients. In addition, a considerable time advantagef ultrasound over chest radiography was demonstrated.
2
2
n 83 (2012) 307– 312
Conflict of interest statement
The authors have no commercial associations or sources of sup-port that might pose a conflict of interest.
References
1. Neumar RW, Otto CW, Link MS. Part 8: adult advanced cardiovascular lifesupport: 2010 American Heart Association Guidelines for CardiopulmonaryResuscitation and Emergency Cardiovascular Care. Part 8.1: adjuncts for airwaycontrol and ventilation. Circulation 2010;122:S729–35.
2. Jones JH, Murphy MP, Dickson RL, Somerville GG, Brizendine EJ. Emergencyphysician-verified out-of-hospital intubation: miss rates by paramedics. AcadEmerg Med 2004;11:707–9.
3. Sayre MR, Sakles JC, Mistler AF, Evans JL, Kramer AT, Pancioli AM. Field trial ofendotracheal intubation by basic EMTs. Ann Emerg Med 1998;31:228–33.
4. Katz SH, Falk JL. Misplaced endotracheal tubes by paramedics in an urban emer-gency medical services system. Ann Emerg Med 2001;37:32–7.
5. Jemmett ME, Kendal KM, Fourre MW, Burton JH. Unrecognized mis-placementof endotracheal tubes in a mixed urban to rural emergency medical servicessetting. Acad Emerg Med 2003;10:961–5.
6. Silvestri S, Ralls GA, Krauss B, et al. The effectiveness of out-of-hospital use ofcontinuous end-tidal carbon dioxide monitoring on the rate of unrecognizedmisplaced intubation within a regional emergency medical services system. AnnEmerg Med 2005;45:497–503.
7. Sitzwohl C, Langheinrich A, Schober A, et al. Endobronchial intubation detectedby insertion depth of endotracheal tube, bilateral auscultation, or observationof chest movements: randomised trial. BMJ 2010;341:c5943.
8. Grmec S. Comparison of three different methods to confirm tracheal tube place-ment in emergency intubation. Intensive Care Med 2002;28:701–4.
9. Ko FY, Hsieh KS, Yu CK. Detection of airway CO2 partial pressure to avoidesophageal intubation. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi1993;34:91–7.
0. Linko K, Paloheimo M, Tammisto T. Capnography for detection of accidentaloesophageal intubation. Acta Anaesthesiol Scand 1983;27:199–202.
1. Williamson JA, Webb RK, Cockings J, Morgan C. The Australian Incident Moni-toring Study. The capnograph: applications and limitations—an analysis of 2000incident reports. Anaesth Intensive Care 1993;21:551–7.
2. Xirouchaki N, Magkanas E, Vaporidi K, et al. Lung ultrasound in criticallyill patients: comparison with bedside chest radiography. Intensive Care Med2011;37:1488–93.
3. Chou HC, Tseng WP, Wang CH, et al. Tracheal rapid ultrasound exam (T.R.U.E.) forconfirming endotracheal tube placement during emergency intubation. Resus-citation 2011;82:1279–84.
4. Weaver B, Lyon M, Blaivas M. Confirmation of endotracheal tube placementafter intubation using the ultrasound sliding lung sign. Acad Emerg Med2006;13:239–44.
5. Blaivas M, Tsung JW. Point-of-care sonographic detection of left endobronchialmain stem intubation and obstruction versus endotracheal intubation. J Ultra-sound Med 2008;27:785–9.
6. Chun R, Kirkpatrick AW, Sirois M, et al. Where’s the tube? Evaluation ofhand-held ultrasound in confirming endotracheal tube placement. PrehospitalDisaster Med 2004;19:366–9.
7. Agresti A, Coull BA. Approximate is better than “exact” for interval estimationof binomial proportions. Am Stat 1998;52:119–26.
8. Newcombe RG. Two-sided confidence intervals for the single proportion: com-parison of seven methods. Stat Med 1998;17:857–72.
9. Razzaq QM. Use of the ‘sliding lung sign’ in emergency bedside ultrasound. EurJ Emerg Med 2008;15:238–41.
0. Brunel W, Coleman DL, Schwartz DE, Peper E, Cohen NH. Assessment of routinechest roentgenograms and the physical examination to confirm endotrachealtube position. Chest 1989;96:1043–5.
1. Dronen S, Chadwick O, Nowak R. Endotracheal tip position in the arrestedpatient. Ann Emerg Med 1982;11:116–7.
2. Timmermann A, Russo SG, Eich C, et al. The out-of-hospital esophageal andendobronchial intubations performed by emergency physicians. Anesth Analg2007;104:619–23.
3. Lichtenstein DA, Lascols N, Prin S, Meziere G. The “lung pulse”: an early ultra-sound sign of complete atelectasis. Intensive Care Med 2003;29:2187–92.
4. Volpicelli G. Sonographic diagnosis of pneumothorax. Intensive Care Med2011;37:224–32.
5. Zechner PM, Breitkreutz R. Ultrasound instead of capnometry for confirmingtracheal tube placement in an emergency? Resuscitation 2011;82:1259–61.
6. Kerrey BT, Geis GL, Quinn AM, et al. A prospective comparison of diaphragmaticultrasound and chest radiography to determine endotracheal tube position in apediatric emergency department. Pediatrics 2009;123:e1039–44.
7. Hsieh KS, Lee CL, Lin CC, et al. Secondary confirmation of endotracheal tubeposition by ultrasound image. Crit Care Med 2004;329 (Suppl.):S374–7.





























