Embed Size (px)
Citation preview

TELEMEDICINE AND E-HEALTH COMMUNICATION SYSTEMS
Ubiquitous wireless telemedicine
H.F. Rashvand, V. Traver Salcedo, E. Monton Sanchez and D. Iliescu
Abstract: A general overview of the emerging wireless and networking technologies and their useto promote the ultimate goal of global health by means of deployment of a telemedicine paradigmis discussed. To achieve this the authors conduct a state-of-the-art study of recent wireless andmedical sensor technologies in conjunction with investigation of continuously growing pressuresfor a better healthcare service throughout the world triggered by the growing age population,social transformations. The study reveals that in spite of available superior technological solutionsthe services are mostly too expensive, mostly inadequate to respond to the growing demand. Then itproposes a flagship solution of making the best use of the next generation of ‘wireless computing’for building a new harmonised healthcare infrastructure for which the authors need to encourageresearchers in the development of an innovative media-independent ubiquitous wireless telemedi-cine system for more cost effective superior quality healthcare services.
1 Introduction
Looking at the known history of mankind’s technologicalinnovation, we see that virtually all significant break-throughs have been irregular and often empowered byspecific windows of opportunity. Considering the fact thatchance does not call upon us repeatedly, we feel that ifwe do not act promptly we may miss an emerging telemedi-cine (TLM)-led superior healthcare opportunity.WHY TLM? TLM is a service-oriented development
process owing its success to two key economy factors of elec-tronic and healthcare industries. However, due to its diversityand complexity, this unique opportunity has been mostlyoverlooked or implemented prematurely. The continuouswandering and changing direction of TLM development indi-cates the roughness of the path leading to solutions. Authorsbelieve there is a need for an update for new, reliable andadvanced TLM solutions empowered by new medicalsensors, collaboration with the medical industries for atimely adventurous development for three main reasons:
The un-stoppable process of the global-village characterisedby a new form of social interconnection through communi-cation is passing through one of its critical phases.There is a need for new potential technological capabilitiesto provide adequate and dependable healthcare services tothe restless world addressing the ever-growing demands.There is a need for a better infrastructure prepared to controlthe ever growing large-scale disease outbreaks. Examples are‘bird flu’, SARS, ‘white plague’ andmany post disaster healthcrises that so often hit populations around the world [1].
# The Institution of Engineering and Technology 2008
doi:10.1049/iet-com:20070361
Paper first received 13th August and in revised form 23rd November 2007
H.F. Rashvand, Adcoms Director, SMIEEE is with the School of Engineering,University of Warwick, Coventry CV4 7AL, UK
V. Traver Salcedo and E. Monton Sanchez are with the ITACA-PolytechnicUniversity of Valencia, Camino de Versa s/n, TSB - Technologies for Healthand Wellbeing, G8 Building, Valencia 46022, Spain
D. lliescu is with the the School of Engineering, University of Warwick, CoventryCV4 7AL, UK
E-mail: [email protected]
IET Commun., 2008, 2, (2), pp. 237–254
WHY UWTM? The ubiquitous wireless (UW) part of thetitle indicates two basic development factors namely:‘dynamics’ and ‘directivity’. The dynamic factor comesfrom ‘ubiquitous’ – the capability of providing a seamlessconnectivity, while the existing solutions lack a universalmedia independence, we won’t be able to remove theobstacles marring existing developments. A harmonisedeffort should enable the directivity. Here, a whole newexciting family of products for wireless medical withbasic features (size, scale, flexibility, quality and compat-ibility) will enable a meaningful deployment. In otherwords, we need a new sustainable TLM development builtupon complementarily of past experience in light of newpotential:Wireless technologies for communication have been
evolving extensively in the last two decades [2, 3],whereas only a few organisations have been able toharness their full potential and fewer made proper use ofthem for the healthcare industry.In spite of their projected potential, today’s healthcare
solutions are far from perfect [4], leaving huge gaps fornew superior products using more effective technologieslike pervasive computing and ubiquitous wirelessconnectivity.
1.1 Definitions
TLM is generally understood as ‘provision of health careover a distance’. ‘Telehealth’(TLH) and ‘telecare’,however, have a broader definition as ‘integration of tele-communications for protecting and promoting health’ [5].E-health, a complementary term, is defined as ‘all formsof electronic healthcare services delivered over the internet’[6], that includes informational, educational and commer-cial aspects of health services. There are some other defi-nitions for e-health such as, ‘a consumer-centred model ofhealthcare where stakeholders collaborate, utilising infor-mation communication technologies (ICTs), includinginternet technologies to manage health, arrange, deliverand account for care and manage the healthcaresystem’[7] as well as other TLM specific definitions [8, 9]:
237
(1) ‘TLM involves the use of modern information technol-ogy, especially two-way interactive audio/video communi-cations, computers and telemetry, to deliver health servicesto remote patients and to facilitate information exchangebetween primary care physicians and specialists located atsome distances from each other’ – lengthy and technologydependent but appropriate for the time.(2) ‘The use of advanced telecommunications technologiesto exchange health information and provide healthcare ser-vices across geographic, time, social and cultural barriers’ –more precisely, this indicates a doubt regarding the ‘exactservices’ and their technologies.(3) ‘If TLH is understood to mean the integration of tele-communications systems into the practice of processingand promoting health, while TLM is the incorporation ofthese systems into curative medicine, then it must beacknowledged that TLH corresponds more closely to theinternational activities of WHO (World HealthOrganisation) in the public health. It covers education forhealth, public and community health, health systems devel-opment and epidemiology, whereas TLM is orientedtowards the clinical aspect’.
As expressed in the media, in order to help TLM to find abetter way, some have considered a change in name fromTLM to TLH but we know without proper supportive tech-nologies a name change won’t make much difference.However, we have recognised that one missing componentcritical to the success of TLM is a solid definition for adistance-independent service interface and associated proto-cols. This requirement is a unique interface, depicted inFig. 1, which should support the integration of all TLMsystems regardless of their location and application.The new definition above may bring the freedom required
enabling a rapid development of a new infrastructure, sothat any suitable TLM capability can be used immediately.This should also enable diverse technologies to developindependently, at their own pace.
1.2 Historical developments
TLM has been recognised as a new technology for manydecades. The original concept, ‘to enhance remote medicalactivities’, was developed some 35 years ago whenmedical applications could be combined with telecom ser-vices using telephone and facsimile at their peaks. In theirearly telecom applications, however, TLM users wereregarded as telecom users. For example, Dowler and Hall[10] considers TLM being started as telediagnostics by psy-chiatrists as early as 1955 using interactive television. Agood source for early developments of TLM is given byMaheu [5] where three phases are identified as ‘the birth’,‘rebirth’ and ‘post 1995’. The ‘birth’ can be traced back topre television era using radio in early 1900 as radio doctor– Fig. 2 shows a front-page image.Since then many experiments set the initial pace includ-
ing the ‘electrical stethoscope’, telepsychiatry, teledermato-log. NASA also tested a wide range of satellite-basedmedical services. NASA interests were limited to disasterrecovery and assisted TLH development. Further
Fig. 1 Technology-independent interface
238
developments in Geo and Leo satellite technologies facili-tated realisation of remote clinics. The ‘rebirth of TLM’,in the early 1990s, begins with recognition of rural health.The compressed digital images and interactive video usingwideband channels removed some barriers for provisionof TLM services. Then use of TLM in the USA increasedby a factor of 8 over 5 years due to some new governmentalinitiatives, such as Joint Working Group on Telemedicine(JWGT) and Office for the Advancement of Telehealth(OAT) in the second half of the 1990s.The early TLM applications were of two distinct cat-
egories. One was mainly gathering and transmission ofinformation for diagnostics such as identification of emer-gencies. The second was for proactive distance medicationsuch as telesurgical operations.
1.3 Bridging opportunity
In order to visualise the complexity of wireless TLM wecould divide the systems processing requirements intofour main inter-related components: wireless, TLM, com-puting and ICT. Fig. 3 shows a general view of today’s com-monly used application map – data rate against bandwidth.Following the hopes to build the TLM upon last century’s
celebrated data superhighways and availability of the internet,wehave seen very fewpotential applications over the last threedecades of fixed telecoms. Nonetheless, we see a spark of newlife on the scene and consequently, a newhope towards a TLMparadigm where we identify two major fields of communi-cation and medical sensors coming closer for first time in
Fig. 2 1924 image of radio doctor – source [11]
Fig. 3 Four main components of wireless TLM
IET Commun., Vol. 2, No. 2, February 2008
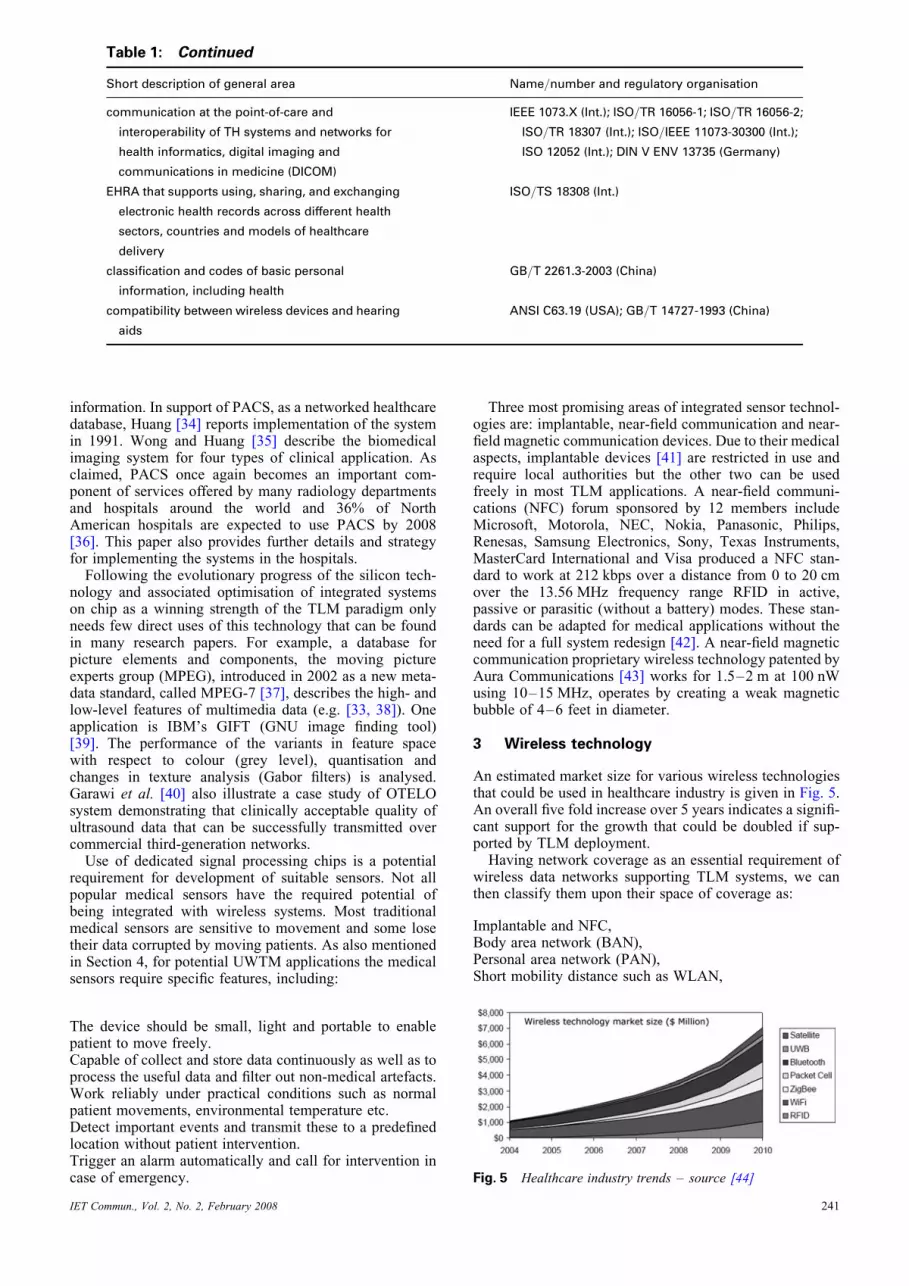
history, ready to close these gaps with minimum cost andefforts. As shown in Fig. 4, if not acted promptly to makethe required connection for TLM to flourish, they maycontinue diverting with further widening gaps.A timely novel wireless bridge, however, should enable
us to cross-connect these two major avenues and establisha long awaited TLM paradigm, a new technological evol-ution. With no doubt the natural mobility advantages ofwireless telecom over the fixed services to help to pavethe required extra mile.
1.4 Standards
An essential consideration is TLM specific standardisation,which has been the centre of controversy and debates.Multimedia was considered once a critical requirementfor TLM. To that effect a challenging view fromChiariglione [12] indicates: ‘the process by which individ-uals recognise the advantage of doing certain things in anagreed way and codify that agreement in a contract.’However, due to the complexities of national laws andhuman aspects of TLM, extensive work and clarificationsare required for a meaningful service deployment [13].Currently, TLM defined standards used by doctors, hospitalsand other healthcare providers are for one-way non-real-time(store and forward technology) or for two-way interactiveteleconferencing style [14]. The first type is used in the trans-fer of radiology or dermatology images. Applications oftwo-way interactive television can be found in manymedical specialties such as cardiology, neurology and gynae-cology [9]. Currently, there are some initiatives betweenhealthcare standardisation organisations such as eHSCG(eHealth Standardisation Coordination Group [15]) andlarge R&D projects such as the Telemedicine AllianceProject, with ITU, WHO and ESA involvement [16].More recent development in standardisation took place
on the ethical and law aspects of medical information. Asindicated by the World Medical Association (WMA) [17]use of genetic engineering and data mining activitiesrequire certain basic principles, mostly compatible withearlier statements in the Lisbon Declaration on the Rightsof the Patient, the Geneva Declaration (International Codeof Medical Ethics) and the Helsinki Declaration(Recommendations Guiding Physicians in BiomedicalResearch Involving Human Subjects).For wireless system engineering, however, technology
enjoys well established and fast moving standards such asIEEE 802.11, 802.15, 802.16, 802.20 and 802.22, Zigbeeetc. In January 2007 the IEEE initiated ten TLH device stan-dards for controlling information exchange to and from per-sonal TLH devices. The ISO/IEEE 802-11073 family ofhealth informatics standards [18], provides definitions ofwhat is needed to implement common communication fea-tures for personal TLH devices.In summary, we can divide TLM standards into three cat-
egories: ‘medical systems’, ‘communications’ and ‘specificdevices’. The first category addresses a set of general rules
Fig. 4 Today’s TLM cross road – wireless bridge opportunity
IET Commun., Vol. 2, No. 2, February 2008
for integrity, safety and effectiveness of medical equipmentand includes standards for electrical safety, EMC, emissionsof radiation from such devices, ESD etc. The second cat-egory is for connectivity. The last category, (wirelessspecific) medical devices addresses implantable medicaldevices, hearing aids, healthcare facilities and healthcaresystem architecture. Table 1 shows these standards andtheir requirements (adapted from FDA [19], NSSN [20],BSI [21], JSA [22], SAC [23], SAL [24], BIS [25] andeHSCG [15]).Having made an attempt to substantiate the need for
UWTM in Section 1, the rest of paper is organised asfollows. Section 2 briefly scans the research and develop-ment activities in three main areas of ICT including infor-mation technology and security (IT), signals and imageprocessing and security. Section 3 analyses progressiveaspects of wireless systems with regards to their suitabilityfor access, processing and communicating medical data.Section 4 looks at the potential trends and requirements ofTLM services with some sample medical solutions includ-ing sensors and wearable systems. Section 5 discusses themain objective and work towards a ubiquitous solutionand its potential to capture future networking solutionsrequired for potential TLM applications. In Section 6, welook at some special applications for analysis and possiblefuture solutions.
2 Technology overview
In order to achieve the TLM objectives for a healthcareparadigm the industry needs to build minimum basic capa-bilities in the core disciplines: engineering (ICT), medicaland management. This section with potential for an exten-sive review of ICT in healthcare had to be, however,focused on critical developments. For this reason weaddress very few historical ICT developments.Some consider the 1980s as the main turning point for
ICT. The ICC’84 in Amsterdam briefs the integration ofvoice and data as a true digitisation point [26] realised bytelecom service evolution [27] and local area networking[28].The term ICT is not very old itself. It emerged uponsilicon technology due to two basic trends of broadbandconnectivity (internet [29]) and commonality of the func-tions being used in integrating computing and communi-cations. The term, though technically correct, has affecteddevelopment of the TLM by taking out ‘tele’ part ofTLM – the distance plays a significant role in the view ofthe public and helped to identify the TLM. Some of thepush came from ITU in association with rescue operationsand poverty [30]. At the time considered, the term ICTcould help developing these societies.Three main parts of the ICT, used extensively in TLM,
are IT, signal processing and communication networking.Use of database has already imposed evolutionary
changes to the healthcare systems. Lin et al. [31] proposea remote data access mechanism for home monitoringsystems. Scott [32] investigates the importance of databasein healthcare, hospital records and associated with extra fea-tures including data preservation techniques, filtering, com-patibility and management strategies. In doing this, heseparates the data into two complementary hospital and per-sonal sets of health records. Doeller [33] identifies someproblems with the currently used Database ManagementSystems to fulfil the multimedia requirements: querying,indexing and content modelling. An alternative system ispicture archive and communications systems (PACS) thatintegrates the radiology information systems (RIS), whichin turn supports acquisition and communication of critical
239

240
Table 1: TLM standards, recommendations and their requirements
Short description of general area Name/number and regulatory organisation
Category 1
general risk management of products and
processes
ISO 14971:2000
general safety (including EMC) for general
electronic and medical devices; testing, immunity
and emissions requirements and labelling
regarding them
IEC 60601-1-2: 2001 and:2004; IEC 60601-2-X; IEC
61326 (Int.); 89/336/EEC(Europe); BS EN
55016-1-3:2006 and 61000-4-3:2006 (UK); AAMI
TIR No.18-1997(USA); AS/NZS 3200.1.1(Australia,
NZ); JIS C 1000-4 (Japan); GB 9706 (China)
measurements to establish the immunity of medical
devices to EM radiation and ESD
ANSI ASC C63.18(USA), ANSI/ESD-S20.20-1999
(USA)
safety of products emitting infrared optical radiation
used for data transmission
EN ISO11151 (Int.); IEC 60825-12 (Int.); AS/NZS
2211.7:2002 (Australia New Zealand)
QS requirements for medical devices 21 CFR Part 8xx (USA)
airborne equipment RTCA/DO-160D (USA and Int.)
rules of health monitoring for public places; records
and health information
GB/T 17220-1998(China)
Category 2
general rules regarding allocation of radio
frequency bands
47 CFR Part 2 FCC (USA)
radio equipment and systems; general devices
using radio frequency; low power radio; personal
radio equipment, WMTS
I-ETS 300 220 (Europe); ETSI EN 300 674; 47 CFR Part
15, 18, 95 (USA); AS/NZS 4268:2003/Amdt 1:2005
(Australia New Zealand); IS 10820 (India)
EMC for radio and or specific frequency radio
communication equipment
ETS 300 339, ETS 300 683(Europe); GB 19484.1-2004
SAC (China)
information technology – RFID ISO/IEC 18000-4
interference and EMD for RF equipment CISPR 11(Int.); IS 15598: 2005; 6873: Part 4: 1999
(India)
human exposure to electromagnetic fields from
devices used in EAS, RFID and similar
applications
BS EN 50357:2001(UK)
refers to RF, over-the-air interface between a
wireless client and a base station or between two
wireless clients; coexistence between wireless
local area networks (WLAN) and wireless
personal area networks (WPAN) devices
IEEE 802.11; 802.11.(a, b or g); 802.15.x; (Int.) ISI/
IEEE 11073 X.73-ITU (Int.)
signal transmission using infrared radiation IEC 61603-6 (USA, Int.); IEC 61920 (Int.)
infrared wireless local and metropolitan networks –
WLAN
ISO/IEC 8802-11 (Int.); IEEE 1073.3.2 (Int., USA)
general specification for microwave communication
systems with TDM/FDMA point-to-multipoint
ASTM E2158; DIN EN 12253 (Germany) GB/T
16650-1996(China)
satellite communications; Inter-working between
terrestrial networks and satellite data
transmission systems
ETSI EN 300 and 301 xxx (Europe); COM(95) 529
FINAL (Europe) AS 4080 (Australia); ERC/DEC/
(97) (CEPT); DIN ETS 300xxx (Germany); GB/T
12364, 11443.5, 11444.4 and 12563 (China); X.350
and X.351 (ITU-Int.)
Category 3
general safety requirements of RTTE for medical
devices and systems general
1999/5/EC(Europe)
covers the use of mobile wireless communications
in healthcare facilities
ISO/TR 21730: 2007 (Int.)
covers general safety requirements of active
implantable medical devices (AIMD), including
EMC
90/385/EEC (Europe); ETSI EN 302 195-1 (Europe);
ANSI/AAMI PC69:2000 (USA); ISO 14708 (Int.)
(continued )
IET Commun., Vol. 2, No. 2, February 2008
IET C
Table 1: Continued
Short description of general area Name/number and regulatory organisation
communication at the point-of-care and
interoperability of TH systems and networks for
health informatics, digital imaging and
communications in medicine (DICOM)
IEEE 1073.X (Int.); ISO/TR 16056-1; ISO/TR 16056-2;
ISO/TR 18307 (Int.); ISO/IEEE 11073-30300 (Int.);
ISO 12052 (Int.); DIN V ENV 13735 (Germany)
EHRA that supports using, sharing, and exchanging
electronic health records across different health
sectors, countries and models of healthcare
delivery
ISO/TS 18308 (Int.)
classification and codes of basic personal
information, including health
GB/T 2261.3-2003 (China)
compatibility between wireless devices and hearing
aids
ANSI C63.19 (USA); GB/T 14727-1993 (China)
information. In support of PACS, as a networked healthcaredatabase, Huang [34] reports implementation of the systemin 1991. Wong and Huang [35] describe the biomedicalimaging system for four types of clinical application. Asclaimed, PACS once again becomes an important com-ponent of services offered by many radiology departmentsand hospitals around the world and 36% of NorthAmerican hospitals are expected to use PACS by 2008[36]. This paper also provides further details and strategyfor implementing the systems in the hospitals.Following the evolutionary progress of the silicon tech-
nology and associated optimisation of integrated systemson chip as a winning strength of the TLM paradigm onlyneeds few direct uses of this technology that can be foundin many research papers. For example, a database forpicture elements and components, the moving pictureexperts group (MPEG), introduced in 2002 as a new meta-data standard, called MPEG-7 [37], describes the high- andlow-level features of multimedia data (e.g. [33, 38]). Oneapplication is IBM’s GIFT (GNU image finding tool)[39]. The performance of the variants in feature spacewith respect to colour (grey level), quantisation andchanges in texture analysis (Gabor filters) is analysed.Garawi et al. [40] also illustrate a case study of OTELOsystem demonstrating that clinically acceptable quality ofultrasound data that can be successfully transmitted overcommercial third-generation networks.Use of dedicated signal processing chips is a potential
requirement for development of suitable sensors. Not allpopular medical sensors have the required potential ofbeing integrated with wireless systems. Most traditionalmedical sensors are sensitive to movement and some losetheir data corrupted by moving patients. As also mentionedin Section 4, for potential UWTM applications the medicalsensors require specific features, including:
The device should be small, light and portable to enablepatient to move freely.Capable of collect and store data continuously as well as toprocess the useful data and filter out non-medical artefacts.Work reliably under practical conditions such as normalpatient movements, environmental temperature etc.Detect important events and transmit these to a predefinedlocation without patient intervention.Trigger an alarm automatically and call for intervention incase of emergency.
ommun., Vol. 2, No. 2, February 2008
Three most promising areas of integrated sensor technol-ogies are: implantable, near-field communication and near-field magnetic communication devices. Due to their medicalaspects, implantable devices [41] are restricted in use andrequire local authorities but the other two can be usedfreely in most TLM applications. A near-field communi-cations (NFC) forum sponsored by 12 members includeMicrosoft, Motorola, NEC, Nokia, Panasonic, Philips,Renesas, Samsung Electronics, Sony, Texas Instruments,MasterCard International and Visa produced a NFC stan-dard to work at 212 kbps over a distance from 0 to 20 cmover the 13.56 MHz frequency range RFID in active,passive or parasitic (without a battery) modes. These stan-dards can be adapted for medical applications without theneed for a full system redesign [42]. A near-field magneticcommunication proprietary wireless technology patented byAura Communications [43] works for 1.5–2 m at 100 nWusing 10–15 MHz, operates by creating a weak magneticbubble of 4–6 feet in diameter.
3 Wireless technology
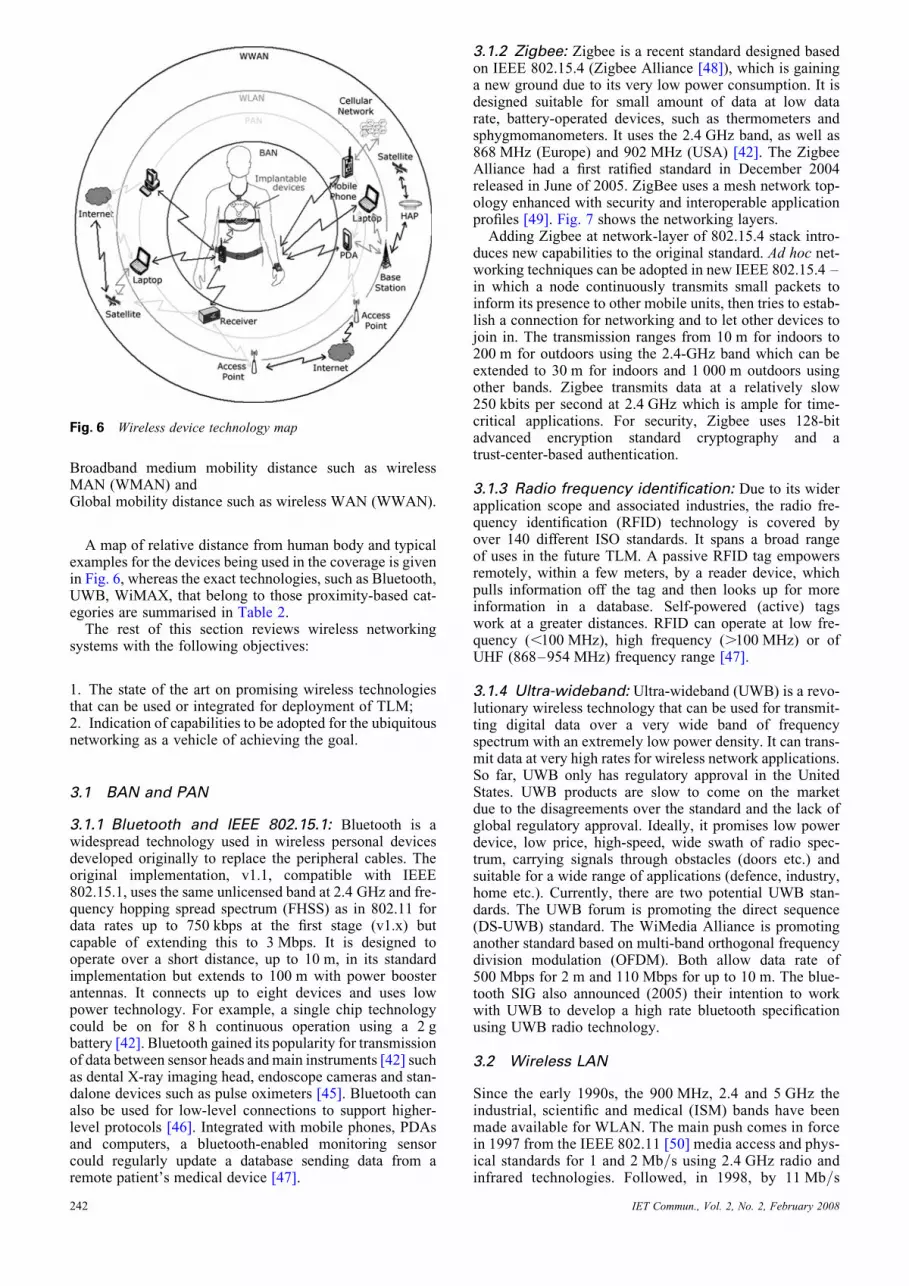
An estimated market size for various wireless technologiesthat could be used in healthcare industry is given in Fig. 5.An overall five fold increase over 5 years indicates a signifi-cant support for the growth that could be doubled if sup-ported by TLM deployment.Having network coverage as an essential requirement of
wireless data networks supporting TLM systems, we canthen classify them upon their space of coverage as:
Implantable and NFC,Body area network (BAN),Personal area network (PAN),Short mobility distance such as WLAN,
Fig. 5 Healthcare industry trends – source [44]
241
Broadband medium mobility distance such as wirelessMAN (WMAN) andGlobal mobility distance such as wireless WAN (WWAN).
A map of relative distance from human body and typicalexamples for the devices being used in the coverage is givenin Fig. 6, whereas the exact technologies, such as Bluetooth,UWB, WiMAX, that belong to those proximity-based cat-egories are summarised in Table 2.The rest of this section reviews wireless networking
systems with the following objectives:
1. The state of the art on promising wireless technologiesthat can be used or integrated for deployment of TLM;2. Indication of capabilities to be adopted for the ubiquitousnetworking as a vehicle of achieving the goal.
3.1 BAN and PAN
3.1.1 Bluetooth and IEEE 802.15.1: Bluetooth is awidespread technology used in wireless personal devicesdeveloped originally to replace the peripheral cables. Theoriginal implementation, v1.1, compatible with IEEE802.15.1, uses the same unlicensed band at 2.4 GHz and fre-quency hopping spread spectrum (FHSS) as in 802.11 fordata rates up to 750 kbps at the first stage (v1.x) butcapable of extending this to 3 Mbps. It is designed tooperate over a short distance, up to 10 m, in its standardimplementation but extends to 100 m with power boosterantennas. It connects up to eight devices and uses lowpower technology. For example, a single chip technologycould be on for 8 h continuous operation using a 2 gbattery [42]. Bluetooth gained its popularity for transmissionof data between sensor heads andmain instruments [42] suchas dental X-ray imaging head, endoscope cameras and stan-dalone devices such as pulse oximeters [45]. Bluetooth canalso be used for low-level connections to support higher-level protocols [46]. Integrated with mobile phones, PDAsand computers, a bluetooth-enabled monitoring sensorcould regularly update a database sending data from aremote patient’s medical device [47].
Fig. 6 Wireless device technology map
242
3.1.2 Zigbee: Zigbee is a recent standard designed basedon IEEE 802.15.4 (Zigbee Alliance [48]), which is gaininga new ground due to its very low power consumption. It isdesigned suitable for small amount of data at low datarate, battery-operated devices, such as thermometers andsphygmomanometers. It uses the 2.4 GHz band, as well as868 MHz (Europe) and 902 MHz (USA) [42]. The ZigbeeAlliance had a first ratified standard in December 2004released in June of 2005. ZigBee uses a mesh network top-ology enhanced with security and interoperable applicationprofiles [49]. Fig. 7 shows the networking layers.Adding Zigbee at network-layer of 802.15.4 stack intro-
duces new capabilities to the original standard. Ad hoc net-working techniques can be adopted in new IEEE 802.15.4 –in which a node continuously transmits small packets toinform its presence to other mobile units, then tries to estab-lish a connection for networking and to let other devices tojoin in. The transmission ranges from 10 m for indoors to200 m for outdoors using the 2.4-GHz band which can beextended to 30 m for indoors and 1 000 m outdoors usingother bands. Zigbee transmits data at a relatively slow250 kbits per second at 2.4 GHz which is ample for time-critical applications. For security, Zigbee uses 128-bitadvanced encryption standard cryptography and atrust-center-based authentication.
3.1.3 Radio frequency identification: Due to its widerapplication scope and associated industries, the radio fre-quency identification (RFID) technology is covered byover 140 different ISO standards. It spans a broad rangeof uses in the future TLM. A passive RFID tag empowersremotely, within a few meters, by a reader device, whichpulls information off the tag and then looks up for moreinformation in a database. Self-powered (active) tagswork at a greater distances. RFID can operate at low fre-quency (,100 MHz), high frequency (.100 MHz) or ofUHF (868–954 MHz) frequency range [47].
3.1.4 Ultra-wideband: Ultra-wideband (UWB) is a revo-lutionary wireless technology that can be used for transmit-ting digital data over a very wide band of frequencyspectrum with an extremely low power density. It can trans-mit data at very high rates for wireless network applications.So far, UWB only has regulatory approval in the UnitedStates. UWB products are slow to come on the marketdue to the disagreements over the standard and the lack ofglobal regulatory approval. Ideally, it promises low powerdevice, low price, high-speed, wide swath of radio spec-trum, carrying signals through obstacles (doors etc.) andsuitable for a wide range of applications (defence, industry,home etc.). Currently, there are two potential UWB stan-dards. The UWB forum is promoting the direct sequence(DS-UWB) standard. The WiMedia Alliance is promotinganother standard based on multi-band orthogonal frequencydivision modulation (OFDM). Both allow data rate of500 Mbps for 2 m and 110 Mbps for up to 10 m. The blue-tooth SIG also announced (2005) their intention to workwith UWB to develop a high rate bluetooth specificationusing UWB radio technology.
3.2 Wireless LAN
Since the early 1990s, the 900 MHz, 2.4 and 5 GHz theindustrial, scientific and medical (ISM) bands have beenmade available for WLAN. The main push comes in forcein 1997 from the IEEE 802.11 [50] media access and phys-ical standards for 1 and 2 Mb/s using 2.4 GHz radio andinfrared technologies. Followed, in 1998, by 11 Mb/s
IET Commun., Vol. 2, No. 2, February 2008

Table 2: Wireless data technologies characteristics (Adopted from [19, 42, 47, 52–55, 62–64])
Name Network Band Bit rate Physical layer Applications
MICS implantable/
BAN ,2 m
402–405 MHz device specific various USA, Ausralia
[65–67]
EN301, TR 101
981
implantable/BAN 9–315 kHz device specific various Europe
EN302, TR 102-
309, 315, 316,
343
implantable/BAN 315–600 kHz,
12.5–20 MHz,
30–37.5 MHz,
402–405 MHz
device specific various Europe
ULP-AMI country specific, see en301-302 and tr101-102 for Europe
RFID (LF, HF,
UHF)
BAN/PAN 125–134.2 kHz,
13.56 MHz,
868–954 MHz
�106 kbps p2p, ook (type a) 10%
ask (type b)
country specific
[68, 69]
NFC implantable/BAN/
PAN
13.56 Mhz 106, 212 or 424 kbit/s RFID compatible
pairing for other
WPAN technologies
Europe [70]
802.15.1 PAN ,10 m 2.4 GHz 721 kbps fully compatible with
bluetooth v1.x
Bluetooth PAN 10–100 m 2.4 GHz 750 kbps (v1.x),2.2Mbps
(EDR)
FHSS v1.x fully
compatible with
802.15.1
[45, 46, 71, 72]
802.15.3 high rate PAN 2.4 GHz (20þ) 11, 22, 33, 44, 55 Mbps OQPSK to be deployed in
near future802.15.3a high rate PAN 2.4 GHz (100þ) Mbps OQPSK
UWB very high rate PAN . 2.4 GHz ,2 Gbps OFDM, DS-CDMA see
802.15.3a
802.15.4 PAN 2.4 GHz,
902 MHz(US)
68 MHz(EU)
20, 40, 260 kbps compatible with
Zigbee
[73]
Zigbee see 802.15.4
DECT PAN 10–50 m 1.88–1.9 GHz 32, 64, 384 kbps FDMA/TDMA/TDD Europe [74]
IrDA PAN ,1 m 850–900 nm
light 308
angle
9.6 kbps–16 Mbps LoS, P2P OOK/PPM [75]
802.11 LAN ,100 m 2.4 GHz 1 or 2 Mbps FHSS or DSSS
802.11 LAN ,10 m 850–950 nm 1 or 2 Mbps LoS and nLoS, OOK/
PPM
802.11a LAN ,100 m 5 GHz 6–54 Mbps OFDM incompatible
with 802.11b
802.11b high rate LAN,100 m 2.4 GHz 11 Mbps (fallback 5.5, 2 or
1 Mbps)
DSSS and CCK
802.11 g LAN 2.4 GHz up to 22 Mbps OFDM compatible
with 802.11b
WiFi see 802.11b and 802.11 g [CareLinkVassar]
802.11n LAN 5 GHz up to 100 (500) Mbps not implemented
yet802.11p LAN 5.9 GHz
802.11s mesh networking on 802.11 networks
WLAN see all 802.11
Hiper-LAN LAN ,150 m 5 GHz 11 Mbps; 54 Mbps OFDM obsolete
802.16, 802.16x MAN ,501 km or
3–52 km
2–111 GHz
10–662 GHz
0.5–30 Mbps1 , 135 Mbps2 PMP and mesh for
nLoS, for LoS,
OFDM, mobile
users , 60 kmph
(continued )
IET Commun., Vol. 2, No. 2, February 2008 243
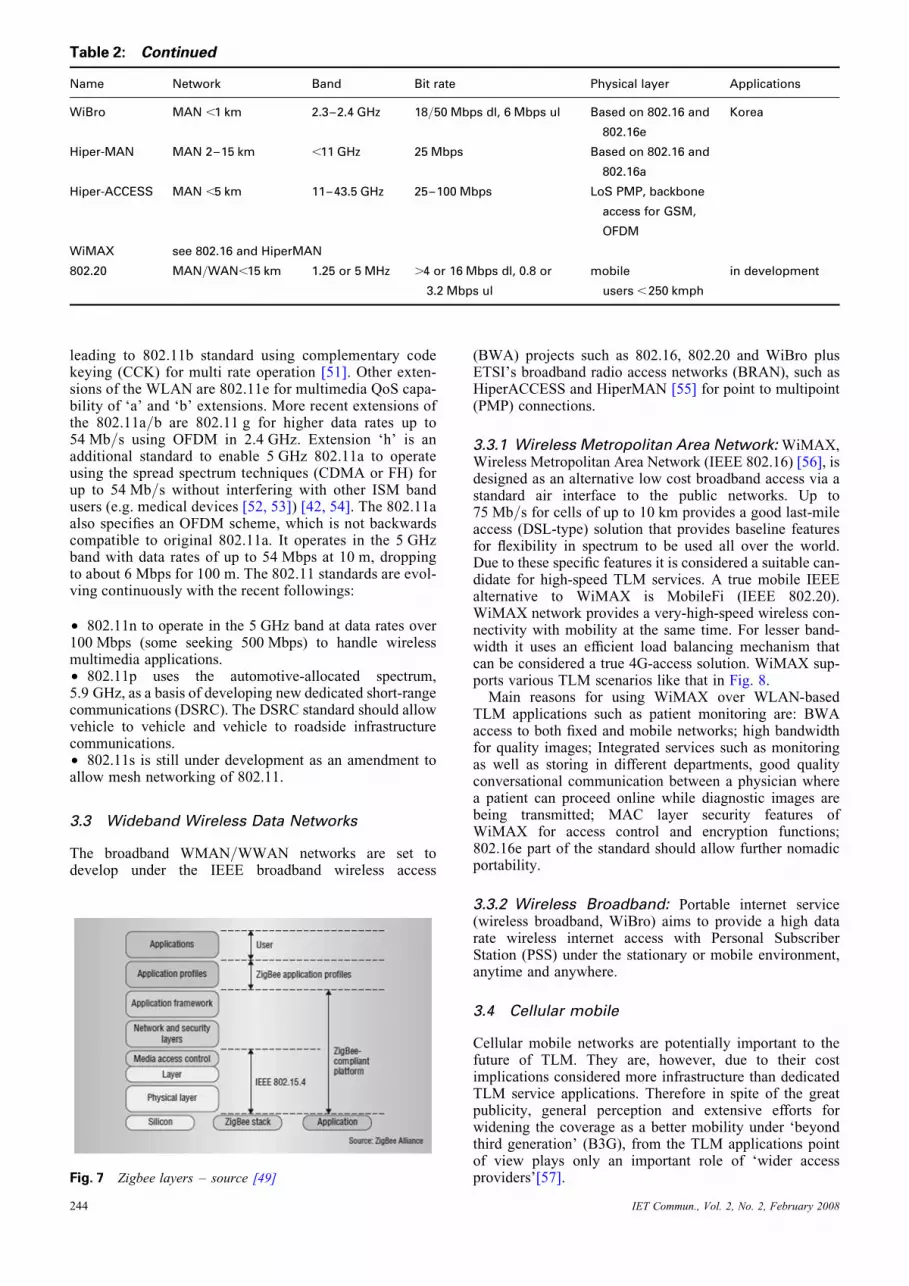
Table 2: Continued
Name Network Band Bit rate Physical layer Applications
WiBro MAN ,1 km 2.3–2.4 GHz 18/50 Mbps dl, 6 Mbps ul Based on 802.16 and
802.16e
Korea
Hiper-MAN MAN 2–15 km ,11 GHz 25 Mbps Based on 802.16 and
802.16a
Hiper-ACCESS MAN ,5 km 11–43.5 GHz 25–100 Mbps LoS PMP, backbone
access for GSM,
OFDM
WiMAX see 802.16 and HiperMAN
802.20 MAN/WAN,15 km 1.25 or 5 MHz .4 or 16 Mbps dl, 0.8 or
3.2 Mbps ul
mobile
users ,250 kmph
in development
leading to 802.11b standard using complementary codekeying (CCK) for multi rate operation [51]. Other exten-sions of the WLAN are 802.11e for multimedia QoS capa-bility of ‘a’ and ‘b’ extensions. More recent extensions ofthe 802.11a/b are 802.11 g for higher data rates up to54 Mb/s using OFDM in 2.4 GHz. Extension ‘h’ is anadditional standard to enable 5 GHz 802.11a to operateusing the spread spectrum techniques (CDMA or FH) forup to 54 Mb/s without interfering with other ISM bandusers (e.g. medical devices [52, 53]) [42, 54]. The 802.11aalso specifies an OFDM scheme, which is not backwardscompatible to original 802.11a. It operates in the 5 GHzband with data rates of up to 54 Mbps at 10 m, droppingto about 6 Mbps for 100 m. The 802.11 standards are evol-ving continuously with the recent followings:
† 802.11n to operate in the 5 GHz band at data rates over100 Mbps (some seeking 500 Mbps) to handle wirelessmultimedia applications.† 802.11p uses the automotive-allocated spectrum,5.9 GHz, as a basis of developing new dedicated short-rangecommunications (DSRC). The DSRC standard should allowvehicle to vehicle and vehicle to roadside infrastructurecommunications.† 802.11s is still under development as an amendment toallow mesh networking of 802.11.
3.3 Wideband Wireless Data Networks
The broadband WMAN/WWAN networks are set todevelop under the IEEE broadband wireless access
Fig. 7 Zigbee layers – source [49]
244
(BWA) projects such as 802.16, 802.20 and WiBro plusETSI’s broadband radio access networks (BRAN), such asHiperACCESS and HiperMAN [55] for point to multipoint(PMP) connections.
3.3.1 Wireless Metropolitan Area Network: WiMAX,Wireless Metropolitan Area Network (IEEE 802.16) [56], isdesigned as an alternative low cost broadband access via astandard air interface to the public networks. Up to75 Mb/s for cells of up to 10 km provides a good last-mileaccess (DSL-type) solution that provides baseline featuresfor flexibility in spectrum to be used all over the world.Due to these specific features it is considered a suitable can-didate for high-speed TLM services. A true mobile IEEEalternative to WiMAX is MobileFi (IEEE 802.20).WiMAX network provides a very-high-speed wireless con-nectivity with mobility at the same time. For lesser band-width it uses an efficient load balancing mechanism thatcan be considered a true 4G-access solution. WiMAX sup-ports various TLM scenarios like that in Fig. 8.Main reasons for using WiMAX over WLAN-based
TLM applications such as patient monitoring are: BWAaccess to both fixed and mobile networks; high bandwidthfor quality images; Integrated services such as monitoringas well as storing in different departments, good qualityconversational communication between a physician wherea patient can proceed online while diagnostic images arebeing transmitted; MAC layer security features ofWiMAX for access control and encryption functions;802.16e part of the standard should allow further nomadicportability.
3.3.2 Wireless Broadband: Portable internet service(wireless broadband, WiBro) aims to provide a high datarate wireless internet access with Personal SubscriberStation (PSS) under the stationary or mobile environment,anytime and anywhere.
3.4 Cellular mobile
Cellular mobile networks are potentially important to thefuture of TLM. They are, however, due to their costimplications considered more infrastructure than dedicatedTLM service applications. Therefore in spite of the greatpublicity, general perception and extensive efforts forwidening the coverage as a better mobility under ‘beyondthird generation’ (B3G), from the TLM applications pointof view plays only an important role of ‘wider accessproviders’[57].
IET Commun., Vol. 2, No. 2, February 2008
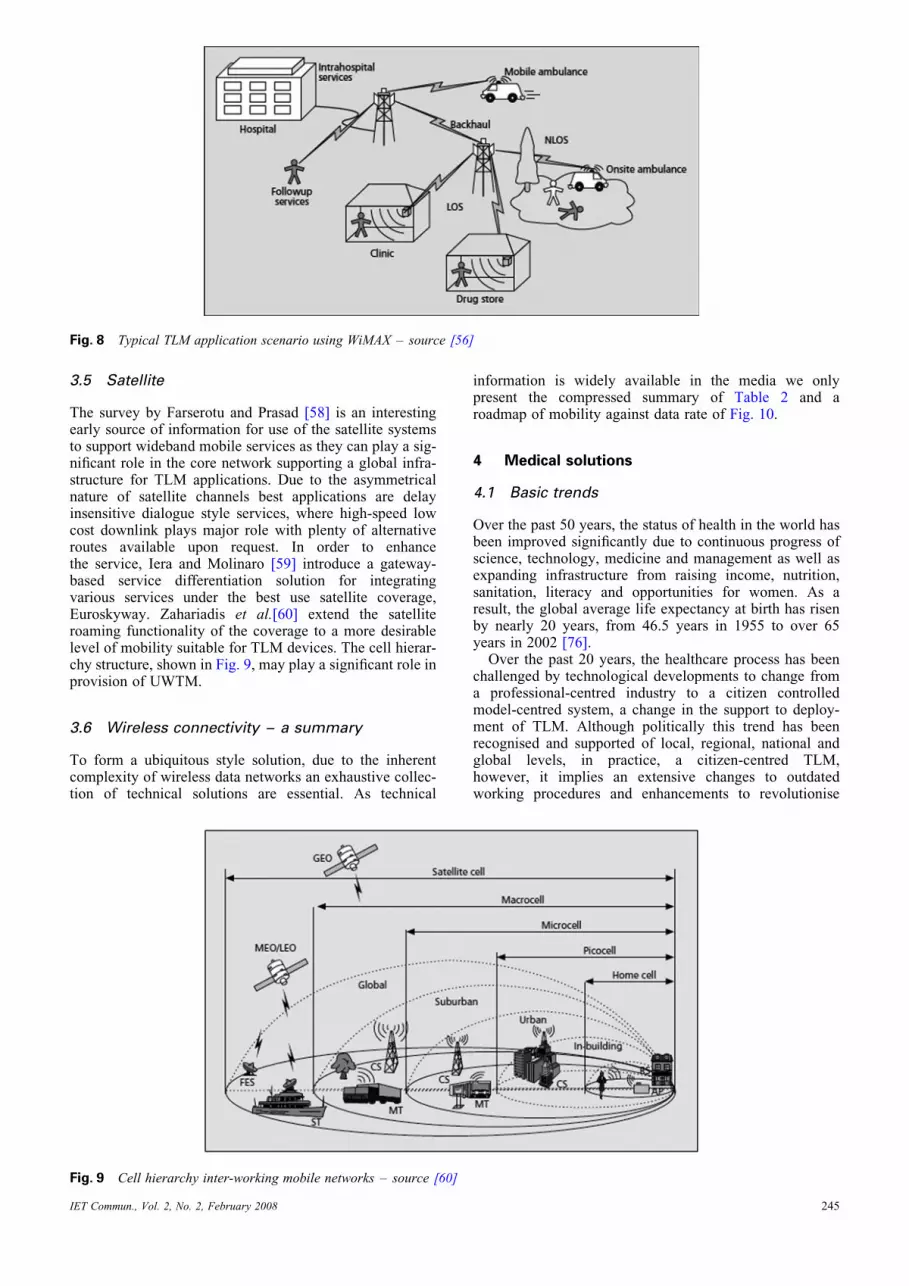
Fig. 8 Typical TLM application scenario using WiMAX – source [56]
3.5 Satellite
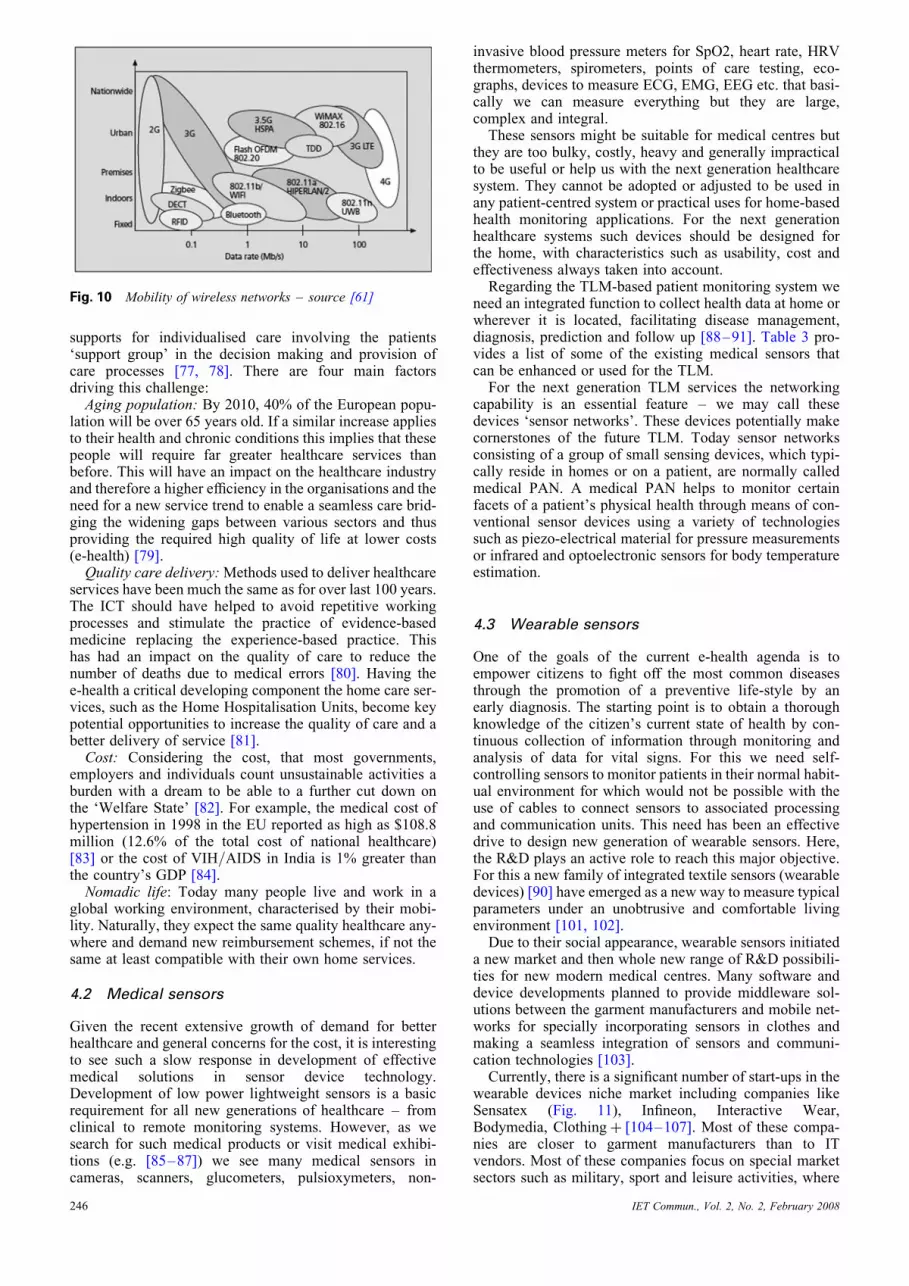
The survey by Farserotu and Prasad [58] is an interestingearly source of information for use of the satellite systemsto support wideband mobile services as they can play a sig-nificant role in the core network supporting a global infra-structure for TLM applications. Due to the asymmetricalnature of satellite channels best applications are delayinsensitive dialogue style services, where high-speed lowcost downlink plays major role with plenty of alternativeroutes available upon request. In order to enhancethe service, Iera and Molinaro [59] introduce a gateway-based service differentiation solution for integratingvarious services under the best use satellite coverage,Euroskyway. Zahariadis et al.[60] extend the satelliteroaming functionality of the coverage to a more desirablelevel of mobility suitable for TLM devices. The cell hierar-chy structure, shown in Fig. 9, may play a significant role inprovision of UWTM.
3.6 Wireless connectivity – a summary
To form a ubiquitous style solution, due to the inherentcomplexity of wireless data networks an exhaustive collec-tion of technical solutions are essential. As technical
IET Commun., Vol. 2, No. 2, February 2008
information is widely available in the media we onlypresent the compressed summary of Table 2 and aroadmap of mobility against data rate of Fig. 10.
4 Medical solutions
4.1 Basic trends
Over the past 50 years, the status of health in the world hasbeen improved significantly due to continuous progress ofscience, technology, medicine and management as well asexpanding infrastructure from raising income, nutrition,sanitation, literacy and opportunities for women. As aresult, the global average life expectancy at birth has risenby nearly 20 years, from 46.5 years in 1955 to over 65years in 2002 [76].Over the past 20 years, the healthcare process has been
challenged by technological developments to change froma professional-centred industry to a citizen controlledmodel-centred system, a change in the support to deploy-ment of TLM. Although politically this trend has beenrecognised and supported of local, regional, national andglobal levels, in practice, a citizen-centred TLM,however, it implies an extensive changes to outdatedworking procedures and enhancements to revolutionise
Fig. 9 Cell hierarchy inter-working mobile networks – source [60]
245
supports for individualised care involving the patients‘support group’ in the decision making and provision ofcare processes [77, 78]. There are four main factorsdriving this challenge:Aging population: By 2010, 40% of the European popu-
lation will be over 65 years old. If a similar increase appliesto their health and chronic conditions this implies that thesepeople will require far greater healthcare services thanbefore. This will have an impact on the healthcare industryand therefore a higher efficiency in the organisations and theneed for a new service trend to enable a seamless care brid-ging the widening gaps between various sectors and thusproviding the required high quality of life at lower costs(e-health) [79].Quality care delivery:Methods used to deliver healthcare
services have been much the same as for over last 100 years.The ICT should have helped to avoid repetitive workingprocesses and stimulate the practice of evidence-basedmedicine replacing the experience-based practice. Thishas had an impact on the quality of care to reduce thenumber of deaths due to medical errors [80]. Having thee-health a critical developing component the home care ser-vices, such as the Home Hospitalisation Units, become keypotential opportunities to increase the quality of care and abetter delivery of service [81].Cost: Considering the cost, that most governments,
employers and individuals count unsustainable activities aburden with a dream to be able to a further cut down onthe ‘Welfare State’ [82]. For example, the medical cost ofhypertension in 1998 in the EU reported as high as $108.8million (12.6% of the total cost of national healthcare)[83] or the cost of VIH/AIDS in India is 1% greater thanthe country’s GDP [84].Nomadic life: Today many people live and work in a
global working environment, characterised by their mobi-lity. Naturally, they expect the same quality healthcare any-where and demand new reimbursement schemes, if not thesame at least compatible with their own home services.
4.2 Medical sensors
Given the recent extensive growth of demand for betterhealthcare and general concerns for the cost, it is interestingto see such a slow response in development of effectivemedical solutions in sensor device technology.Development of low power lightweight sensors is a basicrequirement for all new generations of healthcare – fromclinical to remote monitoring systems. However, as wesearch for such medical products or visit medical exhibi-tions (e.g. [85–87]) we see many medical sensors incameras, scanners, glucometers, pulsioxymeters, non-
Fig. 10 Mobility of wireless networks – source [61]
246
invasive blood pressure meters for SpO2, heart rate, HRVthermometers, spirometers, points of care testing, eco-graphs, devices to measure ECG, EMG, EEG etc. that basi-cally we can measure everything but they are large,complex and integral.These sensors might be suitable for medical centres but
they are too bulky, costly, heavy and generally impracticalto be useful or help us with the next generation healthcaresystem. They cannot be adopted or adjusted to be used inany patient-centred system or practical uses for home-basedhealth monitoring applications. For the next generationhealthcare systems such devices should be designed forthe home, with characteristics such as usability, cost andeffectiveness always taken into account.Regarding the TLM-based patient monitoring system we
need an integrated function to collect health data at home orwherever it is located, facilitating disease management,diagnosis, prediction and follow up [88–91]. Table 3 pro-vides a list of some of the existing medical sensors thatcan be enhanced or used for the TLM.For the next generation TLM services the networking
capability is an essential feature – we may call thesedevices ‘sensor networks’. These devices potentially makecornerstones of the future TLM. Today sensor networksconsisting of a group of small sensing devices, which typi-cally reside in homes or on a patient, are normally calledmedical PAN. A medical PAN helps to monitor certainfacets of a patient’s physical health through means of con-ventional sensor devices using a variety of technologiessuch as piezo-electrical material for pressure measurementsor infrared and optoelectronic sensors for body temperatureestimation.
4.3 Wearable sensors
One of the goals of the current e-health agenda is toempower citizens to fight off the most common diseasesthrough the promotion of a preventive life-style by anearly diagnosis. The starting point is to obtain a thoroughknowledge of the citizen’s current state of health by con-tinuous collection of information through monitoring andanalysis of data for vital signs. For this we need self-controlling sensors to monitor patients in their normal habit-ual environment for which would not be possible with theuse of cables to connect sensors to associated processingand communication units. This need has been an effectivedrive to design new generation of wearable sensors. Here,the R&D plays an active role to reach this major objective.For this a new family of integrated textile sensors (wearabledevices) [90] have emerged as a new way to measure typicalparameters under an unobtrusive and comfortable livingenvironment [101, 102].Due to their social appearance, wearable sensors initiated
a new market and then whole new range of R&D possibili-ties for new modern medical centres. Many software anddevice developments planned to provide middleware sol-utions between the garment manufacturers and mobile net-works for specially incorporating sensors in clothes andmaking a seamless integration of sensors and communi-cation technologies [103].Currently, there is a significant number of start-ups in the
wearable devices niche market including companies likeSensatex (Fig. 11), Infineon, Interactive Wear,Bodymedia, Clothingþ [104–107]. Most of these compa-nies are closer to garment manufacturers than to ITvendors. Most of these companies focus on special marketsectors such as military, sport and leisure activities, where
IET Commun., Vol. 2, No. 2, February 2008
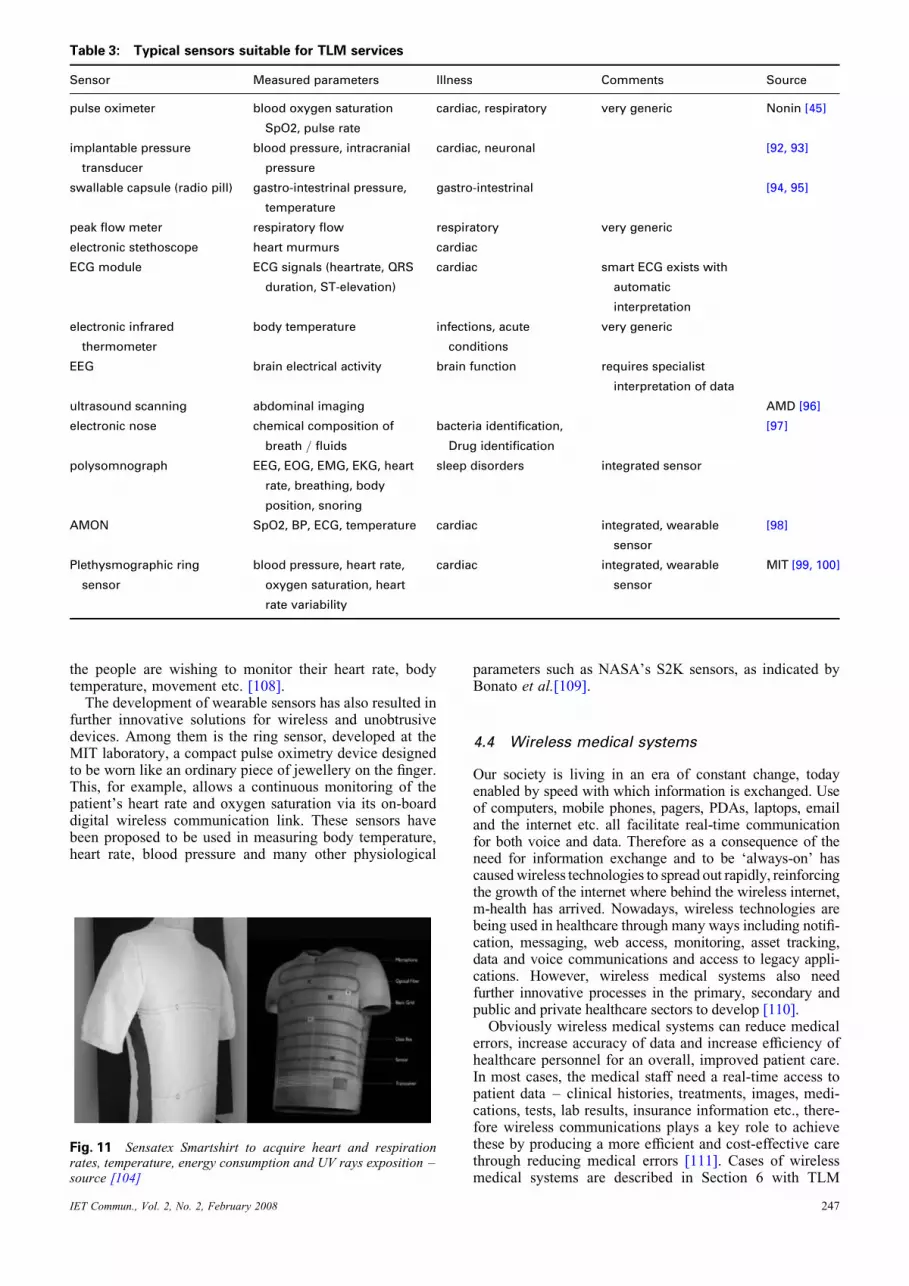
Table 3: Typical sensors suitable for TLM services
Sensor Measured parameters Illness Comments Source
pulse oximeter blood oxygen saturation
SpO2, pulse rate
cardiac, respiratory very generic Nonin [45]
implantable pressure
transducer
blood pressure, intracranial
pressure
cardiac, neuronal [92, 93]
swallable capsule (radio pill) gastro-intestrinal pressure,
temperature
gastro-intestrinal [94, 95]
peak flow meter respiratory flow respiratory very generic
electronic stethoscope heart murmurs cardiac
ECG module ECG signals (heartrate, QRS
duration, ST-elevation)
cardiac smart ECG exists with
automatic
interpretation
electronic infrared
thermometer
body temperature infections, acute
conditions
very generic
EEG brain electrical activity brain function requires specialist
interpretation of data
ultrasound scanning abdominal imaging AMD [96]
electronic nose chemical composition of
breath / fluids
bacteria identification,
Drug identification
[97]
polysomnograph EEG, EOG, EMG, EKG, heart
rate, breathing, body
position, snoring
sleep disorders integrated sensor
AMON SpO2, BP, ECG, temperature cardiac integrated, wearable
sensor
[98]
Plethysmographic ring
sensor
blood pressure, heart rate,
oxygen saturation, heart
rate variability
cardiac integrated, wearable
sensor
MIT [99, 100]
the people are wishing to monitor their heart rate, bodytemperature, movement etc. [108].The development of wearable sensors has also resulted in
further innovative solutions for wireless and unobtrusivedevices. Among them is the ring sensor, developed at theMIT laboratory, a compact pulse oximetry device designedto be worn like an ordinary piece of jewellery on the finger.This, for example, allows a continuous monitoring of thepatient’s heart rate and oxygen saturation via its on-boarddigital wireless communication link. These sensors havebeen proposed to be used in measuring body temperature,heart rate, blood pressure and many other physiological
Fig. 11 Sensatex Smartshirt to acquire heart and respirationrates, temperature, energy consumption and UV rays exposition –source [104]
IET Commun., Vol. 2, No. 2, February 2008
parameters such as NASA’s S2K sensors, as indicated byBonato et al.[109].
4.4 Wireless medical systems
Our society is living in an era of constant change, todayenabled by speed with which information is exchanged. Useof computers, mobile phones, pagers, PDAs, laptops, emailand the internet etc. all facilitate real-time communicationfor both voice and data. Therefore as a consequence of theneed for information exchange and to be ‘always-on’ hascausedwireless technologies to spread out rapidly, reinforcingthe growth of the internet where behind the wireless internet,m-health has arrived. Nowadays, wireless technologies arebeing used in healthcare through many ways including notifi-cation, messaging, web access, monitoring, asset tracking,data and voice communications and access to legacy appli-cations. However, wireless medical systems also needfurther innovative processes in the primary, secondary andpublic and private healthcare sectors to develop [110].Obviously wireless medical systems can reduce medical
errors, increase accuracy of data and increase efficiency ofhealthcare personnel for an overall, improved patient care.In most cases, the medical staff need a real-time access topatient data – clinical histories, treatments, images, medi-cations, tests, lab results, insurance information etc., there-fore wireless communications plays a key role to achievethese by producing a more efficient and cost-effective carethrough reducing medical errors [111]. Cases of wirelessmedical systems are described in Section 6 with TLM
247

services [112], teletrauma [113], telemonitoring [114, 115]and ambulatory major surgery [116].As an opportunity at our fingertips, TLM could also
enable investigation for many rare diseases and difficultcases using various new and special inventive medicaldevices by integrating the traditional systems with completenew solutions based on the vast amount of information thatcan be made available to cure diseases such as cancer andheart failure that we never had the chance to handlebefore. As an example, we can consider the Loop-TissueInteraction of a Circular Loop Antenna study of Curto andAmmann [117] with a potential for skin medical diseaseor cancer applications. Fig. 12 shows a sample result ofthe specific absorption rate (SAR) in the muscle tissue.Similarly, we have a UWB model of human skin [118]and use of hyperthermia for cancer treatment [119].
5 Ubiquitous solution
Here, we propose starting deployment of the TLM basedupon the best use of existing intelligent connectivityunder ubiquity of unbeatable wireless networking com-ponents integrated with light weight multifunctionalmedical sensors as the most desirable evolutionary inno-vation of the time – UWTM.The rest of this section examines the ways ahead, poten-
tial issues, bottlenecks of the existing solutions and identify-ing huge scope for a whole new set of research anddevelopment objectives.
5.1 UWTM
One way to define this new family of products is to considerUWTM applies of ambient intelligence concept [120, 121]to the ‘traditional’ TLM, allowing a ubiquitous and continu-ous access to the patient’s state of health. This shouldprovide virtually all information and healthcare servicesto both the patient and medical staff when and where isrequired. This UWTM solution, when implemented,should provide a powerful tool for treating patients remo-tely. This not only applies to people with long-term andchronic diseases but also applies to those at risk as well ashealthy people who wish to keep themselves in their beststate of health by simply determining certain critical datato be monitored for timely information and decision forthe services that may be required for an individual.
5.2 Implementation
Considering deployment of a TLM paradigm under a newfamily of innovative products supported by UWTM requiresa globally harmonised move and a whole new set of projectssupported by governments, academia, health organisations,telecom operators and many other influential organisations;our solution here is just a predictive brief of technological
248
possibility for the communication end – a simple yet witha potential to play an upmost critical role.To this end, in order to push the UWTM concept closer to
a reality, it is necessary to address some technologic chal-lenges dealing with the communications [122, 123]. Letus examine some four basic requirements of such a device:
(a) One basic requirement of medical devices as a datasource is a continuous monitoring of patients’ biologicaland health info. Ideally they should operate at comfortand should be free from any obtrusions, so that patientscan have their normal daily-life. Existing medical sensorsvary extensively from being in touch with an organ tobeing implanted inside the body. This imposes limitationsto an integrated UWTM device especially if the monitoringsystem is to be integrated. This integration could be desir-able if the same monitoring system could provide infor-mation or alert the patient as it performs the basic dataprocessing. Further capabilities may come from beingable to send the data (raw data or more significant infor-mation, depending on the capacity of processing of thesystem) to a server at a health centre, where a morethorough analysis can be performed, both automaticallyby means of extensive data processing or via the medicalstaff in charge of the health of the patient [124, 125].(b) Networking requirement of the UWTM to provide thepossibility of sending information to the users in a ‘push’way. In order to be able to send urgent information, alerts,advices etc., upon the necessities of the user, this connec-tivity should be independent from time and place of theuser being located [126].(c) All users, patients and medical staff, should have accessto the device and the health information at any place, anytime, any way and independently [127].(d) In order to offer a timely service and using the meansmost suitable for the user, the user location identificationpresents an important challenge.
If we regard complexity as an obstacle to the diffusion ofradical innovative systems then seamlessness property of aUWTM system, that hides the integration complexity fromusers, plays a critical role in the success.So far, most of existing access technologies cannot be
integrated seamlessly therefore they are integrated at theapplication level. Monitoring sensors can be integrated inthe body using the wireless BAN technologies [128](Zigbee, Bluetooth etc.) or possibility of using wirelessmesh networks in a particular environment (Zigbee). Thisintegration then allows the acquisition of monitoring databeing transmitted to the information systems in the healthcentres using WLAN and WWAN access networks (WiFi,WIMAX, GPRS/UMTS etc.). The TCP/IP networkingcould be used at the background technology for a seamlesstransmission of the data in a suitable way for integratingdifferent networks between the users and the health
Fig. 12 Skin cancer patient monitoring – source [117]
IET Commun., Vol. 2, No. 2, February 2008
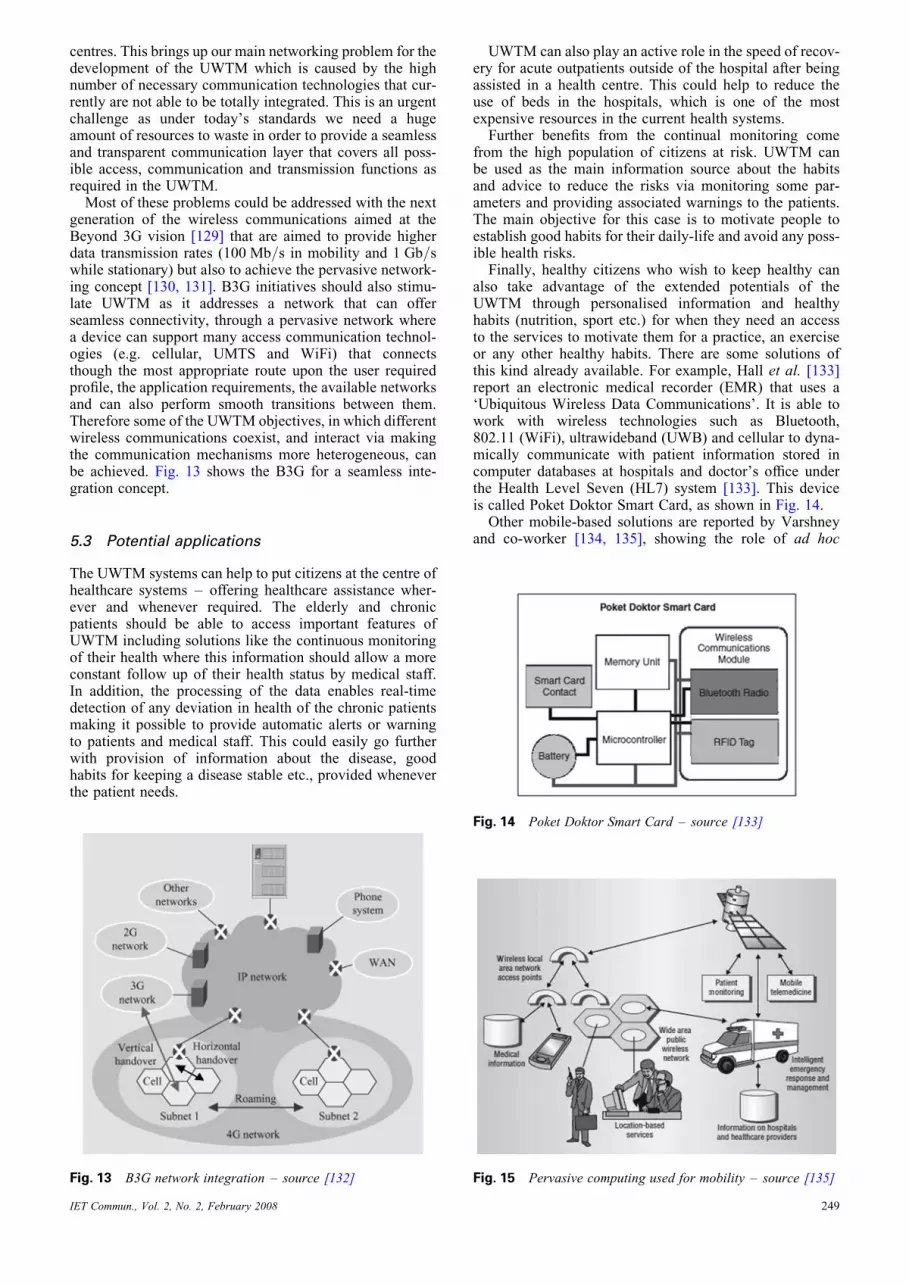
centres. This brings up our main networking problem for thedevelopment of the UWTM which is caused by the highnumber of necessary communication technologies that cur-rently are not able to be totally integrated. This is an urgentchallenge as under today’s standards we need a hugeamount of resources to waste in order to provide a seamlessand transparent communication layer that covers all poss-ible access, communication and transmission functions asrequired in the UWTM.Most of these problems could be addressed with the next
generation of the wireless communications aimed at theBeyond 3G vision [129] that are aimed to provide higherdata transmission rates (100 Mb/s in mobility and 1 Gb/swhile stationary) but also to achieve the pervasive network-ing concept [130, 131]. B3G initiatives should also stimu-late UWTM as it addresses a network that can offerseamless connectivity, through a pervasive network wherea device can support many access communication technol-ogies (e.g. cellular, UMTS and WiFi) that connectsthough the most appropriate route upon the user requiredprofile, the application requirements, the available networksand can also perform smooth transitions between them.Therefore some of the UWTM objectives, in which differentwireless communications coexist, and interact via makingthe communication mechanisms more heterogeneous, canbe achieved. Fig. 13 shows the B3G for a seamless inte-gration concept.
5.3 Potential applications
The UWTM systems can help to put citizens at the centre ofhealthcare systems – offering healthcare assistance wher-ever and whenever required. The elderly and chronicpatients should be able to access important features ofUWTM including solutions like the continuous monitoringof their health where this information should allow a moreconstant follow up of their health status by medical staff.In addition, the processing of the data enables real-timedetection of any deviation in health of the chronic patientsmaking it possible to provide automatic alerts or warningto patients and medical staff. This could easily go furtherwith provision of information about the disease, goodhabits for keeping a disease stable etc., provided wheneverthe patient needs.
Fig. 13 B3G network integration – source [132]
IET Commun., Vol. 2, No. 2, February 2008
UWTM can also play an active role in the speed of recov-ery for acute outpatients outside of the hospital after beingassisted in a health centre. This could help to reduce theuse of beds in the hospitals, which is one of the mostexpensive resources in the current health systems.Further benefits from the continual monitoring come
from the high population of citizens at risk. UWTM canbe used as the main information source about the habitsand advice to reduce the risks via monitoring some par-ameters and providing associated warnings to the patients.The main objective for this case is to motivate people toestablish good habits for their daily-life and avoid any poss-ible health risks.Finally, healthy citizens who wish to keep healthy can
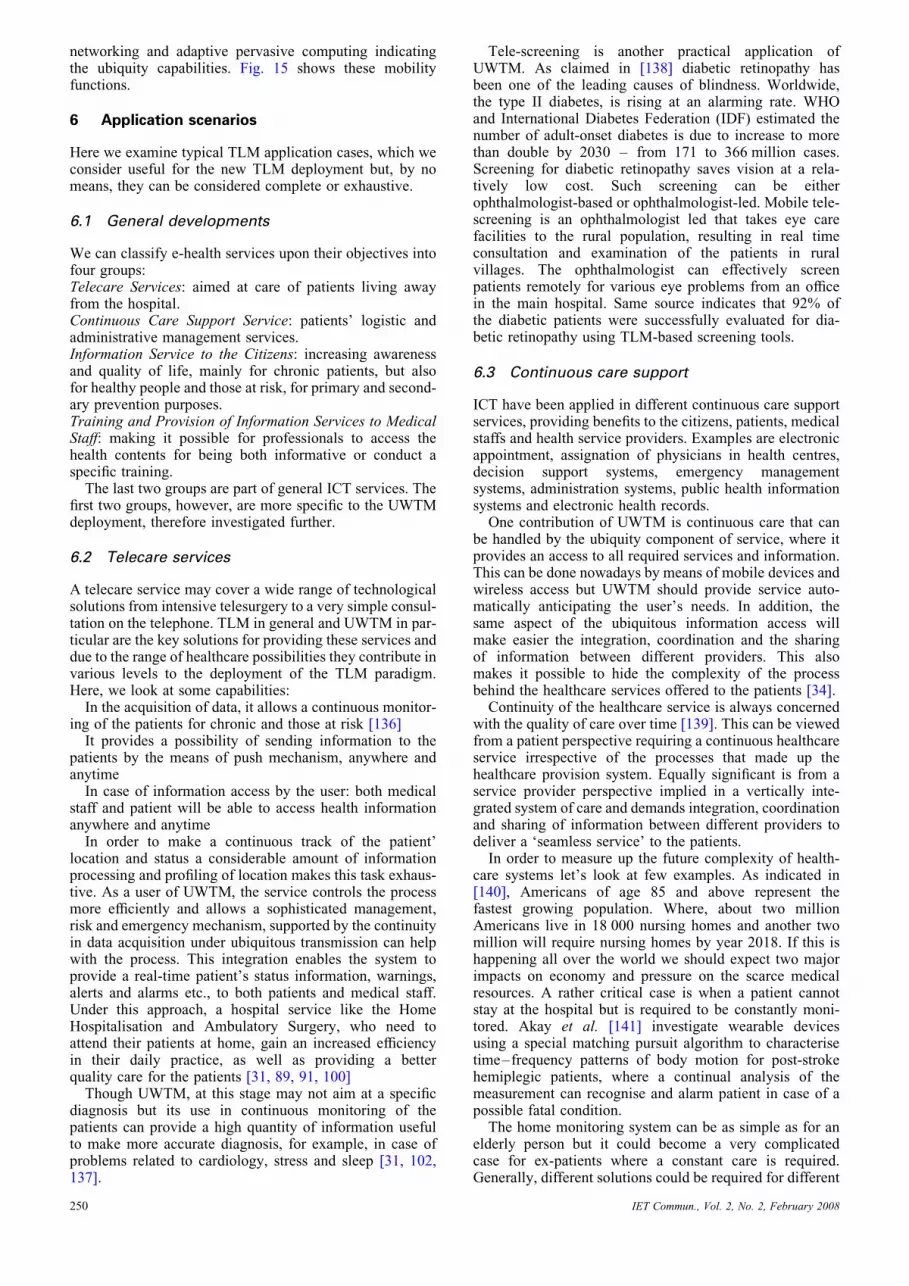
also take advantage of the extended potentials of theUWTM through personalised information and healthyhabits (nutrition, sport etc.) for when they need an accessto the services to motivate them for a practice, an exerciseor any other healthy habits. There are some solutions ofthis kind already available. For example, Hall et al. [133]report an electronic medical recorder (EMR) that uses a‘Ubiquitous Wireless Data Communications’. It is able towork with wireless technologies such as Bluetooth,802.11 (WiFi), ultrawideband (UWB) and cellular to dyna-mically communicate with patient information stored incomputer databases at hospitals and doctor’s office underthe Health Level Seven (HL7) system [133]. This deviceis called Poket Doktor Smart Card, as shown in Fig. 14.Other mobile-based solutions are reported by Varshney
and co-worker [134, 135], showing the role of ad hoc
Fig. 14 Poket Doktor Smart Card – source [133]
Fig. 15 Pervasive computing used for mobility – source [135]
249
networking and adaptive pervasive computing indicatingthe ubiquity capabilities. Fig. 15 shows these mobilityfunctions.
6 Application scenarios
Here we examine typical TLM application cases, which weconsider useful for the new TLM deployment but, by nomeans, they can be considered complete or exhaustive.
6.1 General developments
We can classify e-health services upon their objectives intofour groups:Telecare Services: aimed at care of patients living awayfrom the hospital.Continuous Care Support Service: patients’ logistic andadministrative management services.Information Service to the Citizens: increasing awarenessand quality of life, mainly for chronic patients, but alsofor healthy people and those at risk, for primary and second-ary prevention purposes.Training and Provision of Information Services to MedicalStaff: making it possible for professionals to access thehealth contents for being both informative or conduct aspecific training.The last two groups are part of general ICT services. The
first two groups, however, are more specific to the UWTMdeployment, therefore investigated further.
6.2 Telecare services
A telecare service may cover a wide range of technologicalsolutions from intensive telesurgery to a very simple consul-tation on the telephone. TLM in general and UWTM in par-ticular are the key solutions for providing these services anddue to the range of healthcare possibilities they contribute invarious levels to the deployment of the TLM paradigm.Here, we look at some capabilities:In the acquisition of data, it allows a continuous monitor-
ing of the patients for chronic and those at risk [136]It provides a possibility of sending information to the
patients by the means of push mechanism, anywhere andanytimeIn case of information access by the user: both medical
staff and patient will be able to access health informationanywhere and anytimeIn order to make a continuous track of the patient’
location and status a considerable amount of informationprocessing and profiling of location makes this task exhaus-tive. As a user of UWTM, the service controls the processmore efficiently and allows a sophisticated management,risk and emergency mechanism, supported by the continuityin data acquisition under ubiquitous transmission can helpwith the process. This integration enables the system toprovide a real-time patient’s status information, warnings,alerts and alarms etc., to both patients and medical staff.Under this approach, a hospital service like the HomeHospitalisation and Ambulatory Surgery, who need toattend their patients at home, gain an increased efficiencyin their daily practice, as well as providing a betterquality care for the patients [31, 89, 91, 100]Though UWTM, at this stage may not aim at a specific
diagnosis but its use in continuous monitoring of thepatients can provide a high quantity of information usefulto make more accurate diagnosis, for example, in case ofproblems related to cardiology, stress and sleep [31, 102,137].
250
Tele-screening is another practical application ofUWTM. As claimed in [138] diabetic retinopathy hasbeen one of the leading causes of blindness. Worldwide,the type II diabetes, is rising at an alarming rate. WHOand International Diabetes Federation (IDF) estimated thenumber of adult-onset diabetes is due to increase to morethan double by 2030 – from 171 to 366 million cases.Screening for diabetic retinopathy saves vision at a rela-tively low cost. Such screening can be eitherophthalmologist-based or ophthalmologist-led. Mobile tele-screening is an ophthalmologist led that takes eye carefacilities to the rural population, resulting in real timeconsultation and examination of the patients in ruralvillages. The ophthalmologist can effectively screenpatients remotely for various eye problems from an officein the main hospital. Same source indicates that 92% ofthe diabetic patients were successfully evaluated for dia-betic retinopathy using TLM-based screening tools.
6.3 Continuous care support
ICT have been applied in different continuous care supportservices, providing benefits to the citizens, patients, medicalstaffs and health service providers. Examples are electronicappointment, assignation of physicians in health centres,decision support systems, emergency managementsystems, administration systems, public health informationsystems and electronic health records.One contribution of UWTM is continuous care that can
be handled by the ubiquity component of service, where itprovides an access to all required services and information.This can be done nowadays by means of mobile devices andwireless access but UWTM should provide service auto-matically anticipating the user’s needs. In addition, thesame aspect of the ubiquitous information access willmake easier the integration, coordination and the sharingof information between different providers. This alsomakes it possible to hide the complexity of the processbehind the healthcare services offered to the patients [34].Continuity of the healthcare service is always concerned
with the quality of care over time [139]. This can be viewedfrom a patient perspective requiring a continuous healthcareservice irrespective of the processes that made up thehealthcare provision system. Equally significant is from aservice provider perspective implied in a vertically inte-grated system of care and demands integration, coordinationand sharing of information between different providers todeliver a ‘seamless service’ to the patients.In order to measure up the future complexity of health-
care systems let’s look at few examples. As indicated in[140], Americans of age 85 and above represent thefastest growing population. Where, about two millionAmericans live in 18 000 nursing homes and another twomillion will require nursing homes by year 2018. If this ishappening all over the world we should expect two majorimpacts on economy and pressure on the scarce medicalresources. A rather critical case is when a patient cannotstay at the hospital but is required to be constantly moni-tored. Akay et al. [141] investigate wearable devicesusing a special matching pursuit algorithm to characterisetime–frequency patterns of body motion for post-strokehemiplegic patients, where a continual analysis of themeasurement can recognise and alarm patient in case of apossible fatal condition.The home monitoring system can be as simple as for an
elderly person but it could become a very complicatedcase for ex-patients where a constant care is required.Generally, different solutions could be required for different
IET Commun., Vol. 2, No. 2, February 2008

Fig. 16 Mobile TLM architecture – source [142]
patients. In most cases a set of low power sensor tag systemscan constantly transfer data from the required parts of thebody or surrounding environment to a centralised monitor-ing system where it automatically informs experts of anyurgent deterioration of the patient conditions. Fig. 16shows an example for these cases [142].Tele-monitoring devices have been developed in a variety
of shapes. One is the MobiHealth [143] solution, that consistsof a body area network (BAN) part, a small box with sensorsthat register and transmit physiological data. The data sent byBluetooth to a handheld computer that delivers the data to ahospital or a primary care centre where the data are reviewedonline by the medical staff.
6.4 Communitity tele-health
The WHO e-health strategy includes ‘Policy’, ‘Equitableaccess’ and ‘Best use’. According to WHO, the use ofICTs in health is not merely about technology but a‘means to reach the desired outcome’. In connection withthe international initiatives to fight against issues such asglobal poverty, digital divide and health, the importanceof TLM/H shows to be able to implement these programsmost effectively. One requirement of the ICT that hasbeen exercised and implemented in many programs is toimprove the public health in all parts of the globe withspecial emphasise on less developed societies. There aretoo many extensive reports on these. Let us look at acouple. One is the infoDev framework paper, edited byChetley [30] under ‘the role of ICTs in the health sectorof developing countries, where some pilot projects demon-strate significant improvements indicated by a 50%reduction in mortality and 25–50% increase in productivitywithin the healthcare systems [144].Wireless internet has shown its potential to provide more
effective low-cost connectivity to the underserved andremote areas [145]. Leapfrogging the wired infrastructureby moving to wireless or radio is attractive for developingcountries [146]. Wireless technologies may be deployedrapidly to enable delivery of e-health applications. Use ofthe wireless technology [147] and strategy for conversionof community telecentres to TLH centres [148] may countas a step towards the UWTM goal for the populations insevere need of a basic healthcare, where harmonisation ofinternational organisations with telecom operators mayoffer more effective outcomes.
IET Commun., Vol. 2, No. 2, February 2008
7 Conclusions
Following an overview of TLM development, this paperinvestigates the new available wireless technological capa-bilities to identify the key opportunities to remove the criti-cal pitfalls dealing with e-health and TLM. The ‘ubiquitouswireless’ function is then considered as a key component offuture TLM that can manage access, information and com-munication processing of medical data that can make use ofrecent potential sensors and wearable systems for continu-ous healthcare support services. The proposed solution ofUWTM is for developing a ubiquitous e-health platform-based solution that can help with deployment of our goal,TLM paradigm: ‘Any Content, Any Service Anytime,Anywhere, on any Device.’Finally, as a start, we recommend further research and
development under two topics: (i) short range communi-cation technologies (Zigbee, Bluetooth and the furthernew ones) to cope with biosensors and wearable devicesand (ii) innovative media-independent UWTM systems forthe provision of continuous care services.
8 Acknowledgment
This work is proposed and supported by ‘AdvancedCommunication Systems Limited’.
9 References
1 WHO: ‘New global disease’, 20072 Boukerche, E.A.: ‘Handbook of algorithms for wireless networking
and mobile computing’ (Chapman & Hall/CRC, 2006)3 Sikora, A.: ‘Wireless personal and local area networks’ (John Wiley,
2003)4 Rigby, M., Roberts, R., and Thick, M. (ed.): ‘Taking health
telematics into the 2lst century’ (Radcliffe Medical Press Ltd, 2000)5 Maheu, M.M.: ‘E-health, telehealth and telemedicine: a guide to
start-up and success’ (Jossy-Bass, 2001)6 Mclendon, K.: ‘E-commerce and HIM: ready or not, here it comes’,
AHIMA, 2000, 71, (1), pp. 22–237 Alvarez, R.C.: ‘Review: the promise of e-health – a Canadian
perspective’, eHealth Int., 2002, 1, pp. 1–6, available at: http://www.ehealthinternational.net/content/1/1/4, accessed on 1 May2007
8 Darkins, A.W., and Cary, M.A.: ‘Telemedicine and telehealth:principles, policies, performance and pitfalls’ (Free Association,2000)
9 Choi, Y.B., Krause, J.S., Capitan, K.E., and Chung, K.:‘Telemedicine in the USA: standardization through informationmanagement and technical applications’, IEEE Commun. Mag.,2006, 44, pp. 41–48
251

10 Dowler, N., and Hall, C.J.: ‘Safety issues in telesurgery – summary’.IEE Colloquium on ‘Towards Telesugery’ (IEE, 1995)
11 Radio_News_1924: ‘Front page’, available at: http://www.boingboing.net/images/radio_news_1924.jpg, accessed on 18February 2008
12 Chiariglione, L.: ‘The challenge of multimedia standardization’,IEEE Mutltimedia, 1997, 4, pp. 79–83
13 Eyers, D.M., Bacon, J., and Moody, K.: ‘OASIS role-based accesscontrol for electronic health records’, IEE Proc., Softw., 2006, 153,pp. 16–23
14 ISO: ‘TR 16056-1: health informatics: interoperability of telehealthsystems and networks’ (ISO Press, 2006)
15 WHO: ‘eHSCG standards’, available at: http://www.who.int/ehscg/resources/en/ehscg_standards_list.pdf, accessed on 18 February2008
16 ESA: ‘http://www.esa.int/SPECIALS/Telemedicine_Alliance/ESAM428708D_0.html’, accessed on 18 February 2008
17 Snaedal, J.: ‘Commentary: the ethics of health sector databases’,eHealth Int., 2002, 1, p. 6
18 Mccabe, K.: ‘http://standards.ieee.org/’, accessed on 18 February2008
19 Fda, : ‘Draft guidance for industry and FDA staff: radio-frequencywireless technology in medical devices’ (Food and DrugAdministration, USA, 2007), available at: www.fda.gov/cdrh/osel/guidance/1618.pdf
20 NSSN: ‘Search engine for standards’, available at: http://www.nssn.org/,accessed on 18 February 2008
21 BSI: ‘British Standards Institute’, available at: http://www.bsi-global.com/en/Standards-and-Publications/, accessed on 18February 2008
22 JSA: ‘Japanese Standards Association, standards and publications’,available at: http://www.webstore.jsa.or.jp/webstore/Top/indexEn.jsp,accessed on 18 February 2008
23 SAC: ‘Standardization Administration of China, English home’,available at: http://www.sac.gov.cn/templet/english, accessed on 18February 2008
24 SAL: ‘Standards Australia Limited’, available at: http://www.standards.org.au/, accessed on 18 February 2008
25 BIS: ‘Bureau of Indian Standards, BIS on-line catalogue’, availableat: http://www.bis.org.in/bis/start.htm, accessed on 18 February 2008
26 IEEE: ‘Special section: evolution of integrated access’, Commun.Mag., 1984, 22, (4), pp. 6–23
27 IEEE: ‘Users’ views of telecommunications needs’, Commun. Mag.,1984, 22, (7), pp. 7–31
28 IEEE: ‘Architectures of local area networks (LAN)’, Commun. Mag.,1984, 22, (8), pp. 7–56
29 Al_shahi, R., Sadler, M., Rees, G., and Bateman, D.: ‘The internet’,J Neurol. Neurosurg. Psychiatry, 2002, 73, pp. 619–628
30 Davies, J., Trude, B., McConnell, H., Ramirez, R., Shields, T., Drury,P., Kumekawa, J., Louw, J., Fereday, G., Nyamai-Kisia, C., et al.:‘Improving health, connecting people: the role of ICTs in thehealth sector of developing countries’, in Chetley, A. (Ed.),InfoDev Framework Paper, p. 65, infoDev program Grant no.1254, 31 May 2006 by Healthlink Worldwide Website, availableat: www.healthlink.org.uk, accessed September 2007.
31 Lin, C.H., Young, S.T., and Kuo, T.S.: ‘A remote data accessarchitecture for home-monitoring health-care applications’, Med.Eng. Phys., 2007, 29, pp. 199–204
32 Scott, R.E.: ‘e-records in health – preserving our future’, Int. J. Med.Inform., 2007, 76, pp. 427–431
33 Doeller, M.: ‘MPEG-7 meets multimedia database systems’,J. Universal Knowl. Manag., 2006, 1, pp. 18–25
34 Huang, H.K.: ‘Multimedia Applications in Health Care’, IEEEMutltimedia, 1997, 4, p. 23
35 Wong, S.T.C., and Huang, H.K.: ‘Networked multimedia for medicalimaging’, IEEE Mutltimedia, 1997, 4, pp. 25–35
36 Pare, G., and Trudel, M.C.: ‘Knowledge barriers to PACS adoption andimplementation in hospitals’, Int. J. Med. Inform., 2007, 76, pp. 22–33
37 MARTINEZ: ‘MPEG-7 Overview’, 2003: available at: http://www.chiariglione.org/mpeg/standards/mpeg-7/mpeg-7.htm, accessed on18 February 2008
38 Rashvand, H.: ‘Lecture notes – multimedia communications’ (Cov& Magdeburg, 2003)
39 Muller, H., Rosset, A., Vallee, J.-P., and Geissbuhler, A.:‘Comparing feature sets for content-based image retrieval in amedical case database’, SPIE Medical Imaging, SPIE Proc. Vol.5371, San Diego, CA, USA, February 2004
40 Garawi, S.A., Istepanian, R.S.H., andAbu-Rgheff,M.A.: ‘Perorrmanceanalysis of a compact robotic tele-echography e-health system overterrestrail and mobile communication links’, IEE, 2004, pp. 118–122
41 BSI: ‘Active implantable medical devices directive (AIMDD)’,available at: http://www.bsi-global.com/en/ProductServices/Medical/,(BSI_MEDICAL, Ed.), accessed on 18 February 2008
252
42 Varshney, U.: ‘Using wireless technologies in healthcare’, Int. J.Mobile Commun., 2006, 4, (3), pp. 354–368
43 AURA: ‘Near-field magnetic communication technology’, availableat: http://www.auracomm.com/site/content/technology.asp, AuraCommunications, accessed on 18 February 2008
44 Williams, J.C.: ‘Wireless inhealthcare: a study tracking the useofRFID,wireless sensor solutions, and telemetry by medical devicemanufacturers, system integrators and adopters’, in ‘The FocalPointGroup Website Publication’, 2004, available at: http://www.thefpgroup.com/Healthcare2004-brochure.pdf, accessed 18 June 2007
45 NOMIN: ‘Nonin Model 4100 digital pulse oximeter containingBluetoothw Technology Specifications’, Nomin Medical,Document Website, available at: http://www.nonin.com/documents/4100%20Specifications.pdf, accessed 18 February 2008
46 Yao, J., and Warren, S.: ‘Applying the ISO/IEEE 11073 standard towearable home health monitoring system’, J. Clin. Monit. Comput.,2005, 19, pp. 427–436
47 BLUETOOTH: ‘Compare with other technologies’, available at:http://www.bluetooth.com/Bluetooth/Technology/Works/Compare/,(SIG, Ed.), accessed on 18 February 2008
48 ZIGBEE ALLIANCE: available at: http://www.zigbee.org/,accessed on 18 February 2008
49 Geer, D.: ‘Users make a beeline for Zigbee sensor technology’, IEEEComput., 2005, 38, pp. 16–19
50 ‘IEEE wireless standards zone, overview (802.11)’, available at:http://standards.ieee.org/wireless/overview.html#802.11, accessedon 18 June 2007
51 Vannee, R., Awater, G., Morikura, M., Takanashi, H., Webster, M.,and Halford, K.W.: ‘Indoor geolocation science and technology’,IEEE Commun. Mag., 1999, 37, pp. 82–88
52 Campbell, R.J., and Durigon, L.: ‘Wireless communications inhealthcare: who will win the right to send data where no data hasgone before?’, Health Care Manag., 2003, 22, pp. 233–240
53 ISO: ‘TR 21730:Health Informatics – Use of mobilewireless communications and computing technology in Healthcarefacilities – Recommendations for the management of unintentionalelectromagnetic interference with medical devices’ (ISO, Ed.) 2007
54 Carruthers, J.B.: ‘Wireless Infrared communications’, in ‘WileyEncyclopedia of Telecommunications’, 2006
55 Kuran, M.S., and Tugcu, T.: ‘A survey on emerging broadbandwireless access technologies’, Comput. Netw., 2007, 51,pp. 3013–3046
56 Niyato, D., Hossain, E., and Diamond, J.: ‘IEEE 802.16/WiMAX-based broadband wireless access and its application fortelemedicine/e-health services’, IEEE Commun. Mag., 2007, 14,pp. 72–83
57 Rashvand, H.: ‘Lecture notes – wireless mobile communications’(Warwick University, 2006)
58 Farserotu, J., and Prasad, R.: ‘A survey of future broadbandmultimedia satellite systems, issues and trends’, IEEE Commun.Mag., 2000, 38, pp. 128–133
59 Iera,A., andMolinaro,A.: ‘Designing the interworkingof terrestrial andsatellite IP-based networks’, IEEE Commun. Mag., 2002, 40,pp. 136–144
60 Zahariadis, T.B., Vaxevanakis, K.G., Tsantilas, C.P., Zervos, N.A.,and Nikolaou, N.A.: ‘Global roaming in next-generation networks’,IEEE Commun. Mag., 2002, 40, pp. 144–151
61 Stuckmann, P., and Zimmermann, R.: ‘Toward ubiquitous andunlimited-capacity communication networks: European research inframework programme 7’, IEEE Commun. Mag., 2007, 45, p. 148
62 Pandya, R.: ‘Mobile and personal communication systems andservices’ (IEEE Press, 2000)
63 ETSI: ‘Medical devices’, available at: http://portal.etsi.org/radio/MedicalDevices/MedicalDevices.asp, accessed 1 June 2007
64 ATMEL: ‘Understanding the requirements of ISO/IEC 14443 forType B proximity contactless identification cards’, available at:http://www.atmel.com/dyn/resources/prod_documents/doc2056.pdf,accessed on 18 February 2008
65 INNERWIRELESS: ‘The university of chicago comer childrenhospital installs a medical-grade wireless utility to enhance itshealing power’, available at: http://www.integratedsolutionsmag.com/index.php?option=com_docman&task=doc_view&gid=65,accessed on 18 February 2008
66 MEDTRONIC: ‘Radio frequency considerations for the use ofwireless telemetry with the medtronic carelinkw programmer andimplanted medical devices’, available at: http://www.medtronic.com/physician/hf/RadioFreqWirelessTelemetryWhitePaper.pdf,accessed on 18 February 2008
67 Bradley, P.D.: ‘Implantable ultralow-power radio chip facilitates in-body communications’, available at: http://rfdesign.com/next_generation_wireless/short_range_wireless/706RFDF1.pdf, RFDesign (online magazine), available at: http://rfdesign.com/, Issue20070601, accessed 1 June 2007
IET Commun., Vol. 2, No. 2, February 2008

68 PHILIPS: ‘Item-level visibility in the pharmaceutical supply chain:a comparison of HF and UHF RFID technologies, integratedsolutions’, available at: http://www.integratedsolutionsmag.com/index.php?option=com_docman&task=doc_view&gid=13,accessed on 18 February 2008
69 INNERWIRELESS: ‘Vassar brothers medical center goes wireless toimprove productivity and patient care, integrated solutions’,available at: http://www.integratedsolutionsmag.com/index.php?option=com_docman&task=doc_view&gid=64, accessedon 18 February 2008
70 Bacheldor, B.: ‘Diabetic Device Uses RFID to Administer Insulin’,available at: http://www.rfidjournal.com/article/articleview/2617/1/1/ in RFID Journal (online magazine), available at: http://www.rfidjournal.com/ accessed 28 May 2007
71 Bluetooth: Corscience GMBH, 12-chennal Bluetooth ECG –BT12, available at: http://shop.corscience.de/product_info.php?info¼p1_12-channel-Bluetooth-ECG—BT12.html, accessed 18February 2008
72 VIVO: ‘Vivometrics Life Shirt’, available at: http://www.vivometrics.com, accessed on 18 February 2008
73 Zigbee: Corscience GMBH, available at: http://www.corscience.de/en/medical-engineering/company/expertise/wireless-telemetry/zigbee.html, accessed 18 February 2008
74 DECT: ‘DECT applications & case studies’, available at: http://www.dectweb.com/Introduction/applications.htm, accessed on 28May 2007
75 Rodriguez, F.: ‘Employing infrared wireless communications’,medical device Technology magazine, 2006, January/February2006, also on http://www.devicelink.com/mdt/archive/06/01/005.html, accessed 18 February 2008
76 WHO: ‘Connecting for health global vision, local insight report forthe world summit on the information society’ (WHO, 2005)
77 TMA project: ‘Telemedicine 2010: visions for a personalmedical network. Final report roadmap’, available at: http://www.esa.int/esaMI/Telemedicine_Alliance/index.html, accessed on 28May 2007
78 Rubel, P., Fayn, J., Simon-Chautemps, L., and Atoui, H., et al.: ‘Newparadigms in telemedicine: ambient intelligence, wearable, pervasiveand personalized’, in ‘Wearable eHealth Systems for PersonalisedHealth Management: State of the Art and Future Challenges’, Stud.Health Technol. Inform., 2004, 108, pp. 123–132
79 WHO: ‘Life in the 21st century – a vision for all – fifty facts fromthe world health report’ (WHO, 1998)
80 Kohn, L.: ‘To err is human: building a safer health system’ (NationalAcademy Press, 2000)
81 Committee on Quality of Health Cave in America: ‘Crossing thequality chasm: a new health system for the 21st century’ (Instituteof Medicine, 2001)
82 Paho: ‘Innovative care for chronic health conditions’, PanAm. J. Public Health, 2002, 12, pp. 71–74
83 Hodgson, T., and Cai, L.: ‘Medical care expenditures forhypertension, its complications, and its comorbidities’, Med Care,2001, 39, pp. 599–615
84 Anand, K., Pandav, C.S., andNath, L.M.: ‘Impact of HIV/AIDS on thenational economy of India’, Health Policy, 1999, 47, pp. 195–205
85 MEDICA: ‘Medica fair website’, available at: http://www.medica.de/cipp/md_medica/custom/pub/content,lang,2/oid,155/ticket,g_u_e_s_t/~/MEDICA.html’, accessed on 18 February2008
86 ATA: ‘American Telemedicine Association fair website’, availableat: http://www.atmeda.org/conf/2008/concurrents.htm, accessedon 28 May 2007
87 MED-E-TEL: ‘The international educational and networking forumfor ehealth, telemedicine and health ICT’, available at: http://www.medetel.lu/index.php, accessed 18th February 2008
88 HEALTHHERO: ‘Health buddy’, available at: http://www.healthhero.com/, accessed on 18 February 2008
89 Traver, V., Monton, E., Bayo, J.L., Garcia, J.M., Hernandez, J.,and Guillen, S.: ‘Multiagent home telecare platform for patientswith cardiac diseases’, Computers in Cardiology, 2003, 1,pp. 117–120
90 EUPROJECTS: ‘My heart project’, available at: http://www.hitech-projects.com/euprojects/myheart/home.html, accessed on 18February 2008
91 CSCI: ‘Time to care’: Available at: http://www.csci.org.uk/about_csci/publications/time_to_care.aspx, (Commission for Social CareInspection, 2006)
92 Lindstrom, L.H.: ‘Miniaturised pressure transducer intendedfor intravascular use’, IEEE Trans. Biomed. Eng., 1970, BME-17,p. 207
93 Schnakenberg, U., Kruger, C., and Pfeffer, J.G., et al.: ‘Transpondersystem for non-invasive measurement of intravascular pressure’,Biomed. Tech., 2002, 47, p. 191
IET Commun., Vol. 2, No. 2, February 2008
94 Farrar, J., Zworykin, V.K., and Baum, J.: ‘Pressure sensitivetelemetering capsue for study of gastrointestinal motility’, Science,1957, 126, p. 975
95 Nordin, M., Elfstrom, G., and Dahlquist, P.: ‘Intra-abdominalpressure measurements using a wireless radio pressure pill and twowire connected pressure transducers: a comparison’,Scand. J. Rehabil. Med., 1984, 16, pp. 139–146
96 Description of the AMD Telemedicine Company, available at: http://www.amdtelemedicine.com, accessed on 28 May 2007
97 Kress-Rogers, E.: ‘Handbook of biosensors and electronic noses:medicine, food and the environment’ (CRC Press Inc, 1996)
98 Lukowicz, P., Anlinker, U., Ward, J., Troster, G., Hirt, E. andNeufelt, C.: ‘AMON: a wearable medical computer for high riskpatients. Wearable Computers, 2002. (ISWC 2002)’. Proc. SixthInt. Symp. 2002, pp. 133–134
99 The ring sensor project description, available at: http://shaltis.com/www/research.html, accessed on 28 May 2007
100 Asada, H.H., Shaltis, P., Reisner, A., Rhee, S., and Hucthinson, R.C.:‘Mobile monitoring with wearable photoplethysmographicbiosensors’, IEEE Eng. Med. Biol. Mag., 2003, 22, (3), pp. 28–40
101 EUPROJECTS: ‘Sensation project’, available at: http://www.sensation-eu.org/, accessed on 18 February 2008
102 Benny, P.L., Thiemjarus, S., King, R., and Yang, G.: ‘Body sensornetwork – a wireless sensor platform for pervasive healthcaremonitoring’, Department of Computing, Imperial College ofScience, Technology and Medicine, UK
103 Kruger, P.: ‘Wireless healthcare’, Wireless architecture, Ed, 2004104 ‘Sensatex’, available at: http://www.sensatex.com/smartshirt.html,
accessed February 2008105 ‘Wearable electronics website’, available at: http://www.interactive-
wear.de/cms/front_content.php, accessed on 18 February 2008106 ‘Bodymedia website’, available at: http://www.bodymedia.com,
accessed on 18 February 2008107 ‘Clothing plus website’, available at: http://www.clothingplus.fi,
accessed on 18 February 2008108 Binkley, P.F., Frontera, W., Standaert, D.G., and Stein, J.:
‘Predicting the potential of wearable technology’, IEEE Eng. Med.Biol. Mag., 2003, 22, pp. 23–27
109 Bonato, P., Mork, P.J., Sherrill, D.M., and Westgaard, R.H.: ‘Datamining of motor patterns recorded with wearable technology’,IEEE Eng. Med. Biol. Mag., 2003, 22, pp. 110–119
110 DAOU SYSTEMS: ‘Going mobile: from ehealth to mhealth’,available at: http://www.daou.com, accessed on 18 February 2008
111 Wachter, G.: ‘Hospitals unplugged: the wireless revolution reacheshealthcare; telemedicine technology topicstelemedicine informationexchange’, available at: http://tie.telemedicine.org, accessed on 1May 2007
112 Woodward, B., Istepanian, R.S.H., and Richards, C.I.: ‘Design of atelemedicine system using a mobile telephone’, IEEE Trans. Inf.Technol. Biomed., 2001, 5, pp. 13–15
113 Chu, Y., and Ganz, A.: ‘A mobile teletrauma system using3G networks’, IEEE Trans. Inf. Technol. Biomed., 2004, 8,pp. 456–462
114 Konstantas, D., Halteren, A.V., Bults, R., Wac, K., Jones, V., andWidya, I.: ‘MobiHealth: ambulant patient monitoring over publicwireless networks’. Mediterranean Conf. Medical and BiologicalEngineering, MEDICON, 2004
115 Moron, M.J., Casilari, E., Luque, R., and Gazquez, J.A.: ‘A wirelessmonitoring system for pulse-oximetry sensors’, Syst. Commun.,2005, 1, pp. 79–84
116 Perez, F., Monton, F., Nodal, M.J., Vinoles, J., Guillen, S., and Traver,V.: ‘Evaluation of a mobile health system for supporting postoperativepatients following day surgery’, J. Telemed. Telecare, 2006, 12,pp. 41–43
117 Curto, S., and Ammann, M.J.: ‘Circular loop antenna operating at434 MHz for medical applications: loop-tissue interaction’, in‘ISSC 2006’ (Dublin Institute of Technology, 2006)
118 O’Halloran, M.G., and Jones, E.: ‘Frequency-dependent modeling ofultra-wideband pulses in human tissue for biomedical applications’,in ‘ISSC 2006’ (Dublin Institute of Technology, 2006)
119 Jacobsen, S., and Stauffer, P.R.: ‘Is single band radiometry adequatefor temperature monitoring and control of superficial hyperthermiatreatments?’. IET Conf., 2006, vol. 64
120 Aarts, E.: ‘Ambient intelligence: a multimedia perspective’, IEEEMultimedia, 2004, 11, pp. 12–19
121 Ducatel, K., Bogdanowicz, M., Scapolo, F., Leijten, J., andBurgelman, J.-C.: ‘Scenarios for ambient intelligence 2010, ISTAGreport, european commission, institute for prospectivetechnological studies’, available at: ftp://ftp.cordis.lu/pub/ist/docs/istagscenarios2010.pdf
122 Kyriacou, E., Voskarides, S., and Istepanian, R.: ‘Wirelesstelemedicine systems: a brief overview’. Proc. Healthcom 2002,Nancy, France, 2002
253
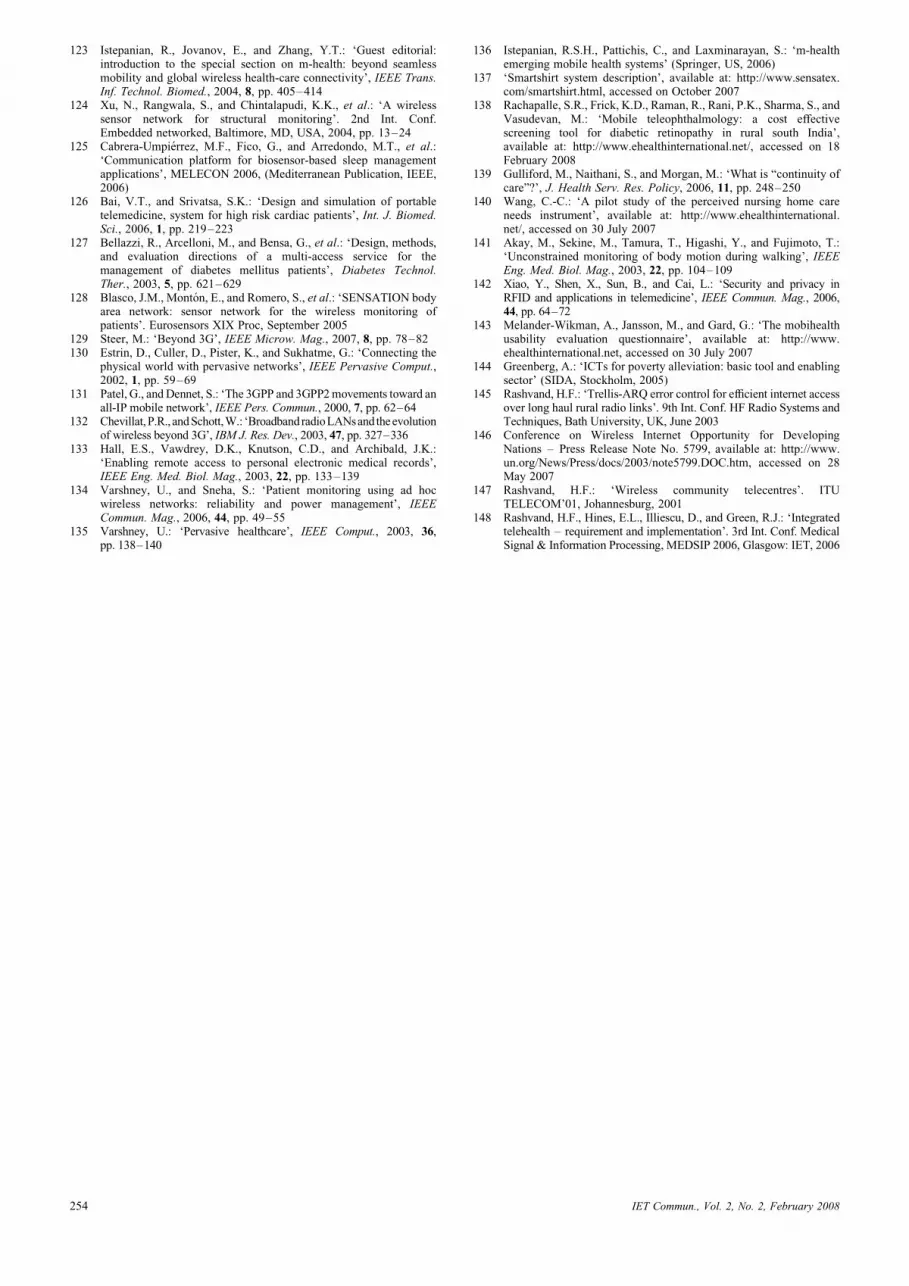
123 Istepanian, R., Jovanov, E., and Zhang, Y.T.: ‘Guest editorial:introduction to the special section on m-health: beyond seamlessmobility and global wireless health-care connectivity’, IEEE Trans.Inf. Technol. Biomed., 2004, 8, pp. 405–414
124 Xu, N., Rangwala, S., and Chintalapudi, K.K., et al.: ‘A wirelesssensor network for structural monitoring’. 2nd Int. Conf.Embedded networked, Baltimore, MD, USA, 2004, pp. 13–24
125 Cabrera-Umpierrez, M.F., Fico, G., and Arredondo, M.T., et al.:‘Communication platform for biosensor-based sleep managementapplications’, MELECON 2006, (Mediterranean Publication, IEEE,2006)
126 Bai, V.T., and Srivatsa, S.K.: ‘Design and simulation of portabletelemedicine, system for high risk cardiac patients’, Int. J. Biomed.Sci., 2006, 1, pp. 219–223
127 Bellazzi, R., Arcelloni, M., and Bensa, G., et al.: ‘Design, methods,and evaluation directions of a multi-access service for themanagement of diabetes mellitus patients’, Diabetes Technol.Ther., 2003, 5, pp. 621–629
128 Blasco, J.M., Monton, E., and Romero, S., et al.: ‘SENSATION bodyarea network: sensor network for the wireless monitoring ofpatients’. Eurosensors XIX Proc, September 2005
129 Steer, M.: ‘Beyond 3G’, IEEE Microw. Mag., 2007, 8, pp. 78–82130 Estrin, D., Culler, D., Pister, K., and Sukhatme, G.: ‘Connecting the
physical world with pervasive networks’, IEEE Pervasive Comput.,2002, 1, pp. 59–69
131 Patel, G., and Dennet, S.: ‘The 3GPP and 3GPP2movements toward anall-IP mobile network’, IEEE Pers. Commun., 2000, 7, pp. 62–64
132 Chevillat,P.R., andSchott,W.: ‘BroadbandradioLANsand theevolutionof wireless beyond 3G’, IBM J. Res. Dev., 2003, 47, pp. 327–336
133 Hall, E.S., Vawdrey, D.K., Knutson, C.D., and Archibald, J.K.:‘Enabling remote access to personal electronic medical records’,IEEE Eng. Med. Biol. Mag., 2003, 22, pp. 133–139
134 Varshney, U., and Sneha, S.: ‘Patient monitoring using ad hocwireless networks: reliability and power management’, IEEECommun. Mag., 2006, 44, pp. 49–55
135 Varshney, U.: ‘Pervasive healthcare’, IEEE Comput., 2003, 36,pp. 138–140
254
136 Istepanian, R.S.H., Pattichis, C., and Laxminarayan, S.: ‘m-healthemerging mobile health systems’ (Springer, US, 2006)
137 ‘Smartshirt system description’, available at: http://www.sensatex.com/smartshirt.html, accessed on October 2007
138 Rachapalle, S.R., Frick, K.D., Raman, R., Rani, P.K., Sharma, S., andVasudevan, M.: ‘Mobile teleophthalmology: a cost effectivescreening tool for diabetic retinopathy in rural south India’,available at: http://www.ehealthinternational.net/, accessed on 18February 2008
139 Gulliford, M., Naithani, S., and Morgan, M.: ‘What is “continuity ofcare”?’, J. Health Serv. Res. Policy, 2006, 11, pp. 248–250
140 Wang, C.-C.: ‘A pilot study of the perceived nursing home careneeds instrument’, available at: http://www.ehealthinternational.net/, accessed on 30 July 2007
141 Akay, M., Sekine, M., Tamura, T., Higashi, Y., and Fujimoto, T.:‘Unconstrained monitoring of body motion during walking’, IEEEEng. Med. Biol. Mag., 2003, 22, pp. 104–109
142 Xiao, Y., Shen, X., Sun, B., and Cai, L.: ‘Security and privacy inRFID and applications in telemedicine’, IEEE Commun. Mag., 2006,44, pp. 64–72
143 Melander-Wikman, A., Jansson, M., and Gard, G.: ‘The mobihealthusability evaluation questionnaire’, available at: http://www.ehealthinternational.net, accessed on 30 July 2007
144 Greenberg, A.: ‘ICTs for poverty alleviation: basic tool and enablingsector’ (SIDA, Stockholm, 2005)
145 Rashvand, H.F.: ‘Trellis-ARQ error control for efficient internet accessover long haul rural radio links’. 9th Int. Conf. HF Radio Systems andTechniques, Bath University, UK, June 2003
146 Conference on Wireless Internet Opportunity for DevelopingNations – Press Release Note No. 5799, available at: http://www.un.org/News/Press/docs/2003/note5799.DOC.htm, accessed on 28May 2007
147 Rashvand, H.F.: ‘Wireless community telecentres’. ITUTELECOM’01, Johannesburg, 2001
148 Rashvand, H.F., Hines, E.L., Illiescu, D., and Green, R.J.: ‘Integratedtelehealth – requirement and implementation’. 3rd Int. Conf. MedicalSignal & Information Processing, MEDSIP 2006, Glasgow: IET, 2006
IET Commun., Vol. 2, No. 2, February 2008





























