Embed Size (px)
Citation preview
1989 73: 651-661
Merigan and R LevySL Brown, RA Miller, SJ Horning, D Czerwinski, SM Hart, R McElderry, T Basham, RA Warnke, TC combination with alpha interferonTreatment of B-cell lymphomas with anti-idiotype antibodies alone and in
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom

Blood, Vol 73, No 3 (February 15), 1989: pp 651-661 6�1
Treatment of B-Cell Lymphomas With Anti-idiotype Antibodies Alone and inCombination With Alpha Interferon
By Sherri L. Brown, Richard A. Miller, Sandra J. Horning, Debra Czerwinski, Sarah M. Hart, Roxena McElderry,
Teresa Basham, Roger A. Warnke, Thomas C. Merigan, and Ronald Levy
Idiotypes are distinct clonal markers for B-cell lymphomas.
Previously we reported the use of anti-idiotype antibodies
in the therapy of patients with B-cell malignancies.
Because synergy was demonstrated with the addition of
alpha interferon to anti-idiotype antibodies in a murine
lymphoma model, we performed a clinical trial combining
these two agents. Here we provide an update of the
original trial of anti-idiotype antibodies alone and report
the outcome of the new combination trial. In 16 treatment
courses of anti-idiotype antibodies alone there were seven
partial responses and one complete response. In 12
courses of combination anti-idiotype antibody and alpha
interferon there were two complete responses and seven
partial responses. Substantial tumor regressions occurred
J3-CELL LYMPHOMAS represent a special class of
human tumors because they express a cell-surface
immunoglobulin molecule unique for each patient that can
serve as a marker for the tumor.’ Antibodies can be produced
against the idiotype, or variable region of the immunoglobu-
lin molecule, and these anti-idiotype antibodies have been
shown to be exquisitely sensitive in discriminating tumor
cells from normal cells.24
Previously we reported the treatment of 1 1 patients with
B-cell malignancies with monoclonal anti-idiotype antibod-
ies.5 Seven of these patients had tumor regression, including
one complete response and four partial responses. An impor-
tant observation made in this trial was the emergence of
idiotype-negative variant tumor cells upon tumor pro-
gression.6 Subsequent studies showed that idiotype-negative
variant cells exist in the lymphoma cell populations prior to
treatment and that this heterogeneity is due to point muta-
tions in the expressed immunoglobulin-variable region
genes.7 This suggested that treatment with anti-idiotype
antibodies selectively reduced the idiotype-positive lym-
phoma cell population, allowing, in some cases, an idiotype-
negative variant cell to become dominant.
A murine lymphoma model has been developed that
allowed testing of the therapeutic effects of anti-idiotype
� Marked antitumor effects were seen after a
single administration of anti-idiotype antibodies, leading to
cure of up to 80% of mice previously injected with tumor
cells. In this murine model, anti-idiotype antibody therapy
resulted in the selection of idiotype-negative tumor cell
variants similar to those arising in human tumors.9 We have
subsequently used this model to examine the effects of
monoclonal anti-idiotype antibodies in combination with
other biological agents.’#{176}” When interferon, an agent that
has an independent antitumor action, was administered in
combination with monoclonal anti-idiotype antibodies, a
synergistic therapeutic effect was noted.”
In an attempt to address the problem of idiotype-negative
variant cells, we performed a clinical trial combining anti-
idiotype antibodies and alpha interferon, based on the inde-
pendent activities of anti-idiotype antibodies and interferon
in patients with B-cell lymphomas and their synergy when
with minimal toxicity in both trials even in patients refrac-
tory to conventional chemotherapy. Tumor specimens
obtained at the time of disease progression often con-
tamed a preponderance of idiotype-negative lymphoma
cells, suggesting that anti-idiotype antibody treatment
exerted a strong antitumor effect against antigen-positive
cells. Anti-idiotype antibodies have reproducible objective
antitumor activity in B-cell lymphoma. The addition of
alpha inteferon may improve the initial rate of response to
this treatment. Strategies that deal effectively with idio-
type-negative lymphoma cells should improve the extent
and duration of these responses.
S 1989 by Grune & Stratton. Inc.
combined in the murine lymphoma model. Here we provide
an update of the previous trial of anti-idiotype antibodies
alone and report the results of the trial combining anti-
idiotype antibodies and interferon. Both studies confirm the
antitumor effect of anti-idiotype antibodies. In both trials
patients had idiotype-negative cells that persisted after treat-
ment and contributed to regrowth of tumor.
MATERIALS AND METHODS
Patient selection. All patients included in these trials gave
informed consent in accordance with the guidelines established bythe Human Investigation Committee of Stanford University Medi-
cal Center. Eligibility criteria included an initial diagnosis of follicu-lar lymphoma, a peripheral lymph node accessible for biopsy ofgreater than 2 cm in diameter, a projected survival of greater than 1year, and an absence of other major medical problems. Immunophe-notyping of the tumor cells was required to confirm the presence of a
monoclonal surface immunoglobulin. Anti-idiotype antibodies wereproduced (see below) and then each patient was re-evaluated. Beforethe treatment phase patients were required to have measurabledisease and, in the antibody-plus interferon trial, a serum-idiotype
protein level less than SO �tg/mL. (The anti-idiotype antibody alonetrial demonstrated that above SO zg/mL the serum barrier ofidiotype protein makes it difficult to infuse enough antibody to
penetrate tumor tissue.) Prior to the initiation of treatment, a secondlymph-node biopsy was performed to confirm the continued reactiv-ity of the anti-idiotype antibody with the tumor cells. Pretherapy
From the Departments of Medicine and Pathology, Stanford
University School of Medicine, Stanford, CA and IDEC Pharma-
ceuticals Corporation, Mountain View, CA.
Submitted August 2, 1988; accepted October 17, 1988.
Supported by National Institutes of Health Grants CA 33399
and CA 34233.
Address reprint requests to Ronald Levy, MD, Division of
Oncology. M207, Stanford University Medical Center, Stanford,
CA 94305.
The publication costs ofthis article were defrayed in part by page
charge payment. This article must therefore be hereby marked
“advertisement” in accordance with 18 U.S.C. section /734 solely to
indicate this fact.© I 989 by Grune & Stratton, Inc.
0006-4971/89/7303-0008$3.00/0
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom
652 BROWN ET AL
evaluation also included physical examination; CBC; platelet count;general chemistry survey; urinalysis; chest x-ray; lymphangiogram;computed tomography (CT) scan of the chest, abdomen, and pelvis;
and bone marrow biopsy. Patients had not received antitumortherapy for at least 4 weeks before beginning the experimental
treatment. Here we provide an update on the initial group of nineevaluable lymphoma patients treated with anti-idiotype antibodies
alone, along with the results of this trial in five subsequent patients.Additionally the outcomes are reported for 1 1 patients who com-
pleted combined treatment with anti-idiotype antibody and interfer-
on.Anti-idiotype antibodies. Mouse or rat monoclonal anti-idio-
type antibodies were produced by methods previously described indetail.5 Large-scale production of antibodies was accomplishedeither by growing hybridomas as ascites in mice or by in vitrocell-culture techniques.’2”3 In the anti-idiotype antibody alone trial,antibodies for the first nine patients were purified by ammonium
sulfate precipitation. The antibodies for all other patients were
additionally purified by ion exchange chromatography (IDEC Phar-maceutical Corporation, Mountain View, CA). These later prepara-tions were greater than 90% pure IgG as determined by sodiumdodecyl sulfate-palyacrylamide gel electrophoresis (SDS-PAGE).Therapeutic preparations passed general safety, sterility, and endo-
toxin testing and were found to be free of adventitious viruses.’4”5Trial design. Patients received therapy in a hospital setting.
Acetaminophen and diphenhydramine were given every four hoursuntil the end of each antibody infusion. Anti-idiotype antibody wasadministered over four hours by intravenous (IV) infusion using a0.22-sm in-line filter. Treatment was given three times per weekuntil all the available antibody had been delivered. This was usuallya duration of three to four weeks. In both trials it was assumed that
the anti-idiotype antibody needed to bind to the tumor cells to havean antitumor effect. In our originial trial with anti-idiotype antibod-ies alone, biopsies of tumor tissue were performed 24 hours afterantibody infusion to document the presence of mouse protein binding
to the target cells.5 Based on this previous experience, antibody was
infused in doses sufficient to overcome circulating serum-idiotypeprotein and to permit penetration of solid-tumor tissue. Because the
antibody treatment, serum-idiotype level, and amount of tumor bulk
were different for each patient, the antibody doses were individual-ized. Recombinant alpha interferon (Roferon, Hoffmann LaRoche,
Nutley, NJ) was given two hours before each antibody infusion at a
dose of 12 x 106 jz/m2 intramuscularly (IM) in the combinationtherapy trial. After the first 3 to 4 weeks of the treatment theinterferon was continued alone at the same dose three times weeklyfor a total duration of eight weeks.
In both trials a general chemistry survey, CBC, and platelet countwere performed prior to each antibody infusion. Serum samples were
collected immediately before, immediately after, two hours after,and 24 hours after each antibody dose. Chest x-ray, lymphography,and CT scans (as appropriate) were performed prior to initiation of
therapy on both protocols. These studies were obtained at the end ofthe three to four weeks of antibody, at the end of the eight weeks ofinterferon in the combination therapy trial, and in follow-up monthlyor bimonthly thereafter in both trials. Bone marrow aspirate andbiopsies were performed at study entry and were repeated if all othermeasurable disease sites responded completely. Repeat lymph-nodebiopsies were performed if the patient had progressive disease
following treatment.Clinical responses were scored according to objective measure-
ment of disease. Since all patients had multiple disease sites, in eachcase several key lesions were designated. A complete response wasdefined as the disappearance of all sites of disease. A partial response
was defined as greater than 50% reduction of the product of the
aggregate perpendicular diameters of the measured key lesions. Aminor response was defined as a reduction of less than 50% of the
product of the aggregate perpendicular diameters of the measuredkey lesions. Responses were required to last at least 1 month with the
observation of response noted on two separate occasions. Freedomfrom progression was scored from the time treatment was initiated
until disease progression occurred.
Serum assays. Enzyme-linked immunosorbent assays were used
to measure serum levels of idiotype protein, mouse immunoglobulin,and human antibody to mouse immunoglobulin as previously
described.5
Immunophenotyping. Single-cell suspensions of tissue samples
were stained with fluorescent antibodies, F(ab’)2 fragments of goat
antihuman immunoglobulin chains and F(ab’)2 fragments of goat
antimouse IgG (Tago, Burlingame, CA) by methods previously
described5 and analyzed by flow cytometry (FACS 440, Becton
Dickinson, Mountain View, CA). An estimate of the total number oftumor cells in each sample was obtained by staining with anti-lambda and anti-kappa antibodies. The number of cells staining with
the light chain not expressed by the tumor was doubled andsubtracted from the total number of cells expressing the tumor’s
heavy chain. In this way small numbers of normal B cells in theanalyzed samples were excluded. Frozen sections of biopsy speci-
mens were stained by the immunoperoxidase method, as previously
Cytocentrifuge preparations were made from lymphocytes from
whole blood or bone marrow following isolation by Ficoll-Hypaque
(FH) sedimentation. Slides were fixed and stained with murinemonoclonal antibodies (MoAbs), followed by enzyme-labeled anti-
bodies. Color was generated with APAAP (Dako, Santa Barbara,
CA) and developed with a naphthol AS-MX phosphate.
RESULTS
Therapeutic trial of anti-idiotype antibody alone. Atotal of 14 evaluable patients with lymphoma have been
treated with anti-idiotype antibodies alone. Nine of these
patients have been reported previously. Two of these have
been treated a second time, and five additional patients are
now evaluated.
Table 1 summarizes the clinical characteristics of the
patients treated with anti-idiotype antibodies alone. Thirteen
of 14 patients had follicular lymphoma at the time of initial
biopsy. Progression to a diffuse histology occurred in the
tumors of three patients prior to antibody treatment. Twelve
patients had previously been treated with chemotherapy.
Eight patients had tumor masses greater than 5 cm.
A summary of the clinical responses is presented in Table
2. In 16 treatment courses there were eight complete or
partial responses with four of these responses lasting 6
months or longer, including one complete response lasting 6
years. The cumulative antibody doses ranged from 500 mg in
patient PK to 1 5,500 mg in patient KC. The importance of
the pretherapy serum-idiotype protein level was demon-
strated by the treatment courses of patients EL and JC. Both
patients were initial nonresponders who had major clinical
responses once the serum-idiotype level was reduced. In five
patients more than one anti-idiotype antibody was used to
achieve comprehensive reactivity with the tumor-cell popula-
tions. Three of these five patients had partial responses
lasting 6 months or greater. Two patients had progressive
disease at 6 and 1 2 months, while patient CC has had
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom

CVP
Bleomycin
Interferon
CC/M/71 FSC
Pretherapy
Id Level
�ig!mL
5.0
.01
Patient
PK
CC
Humana Mouse
Total
Antibody
Dose (mg)
400
6,908
15,500
Tumor
Response
CR
PR
Freedom
fromProgression
6Y
25M+
11,700 -
+ RDPE
CJ
EL(2)
CG
BJ
+ EL(1)CP
TG
JC (1)
PR 12M
PR 6M
- PR 5M
- PR 4M
+ PR 1M
- PR -�
- MR 3M
+ MR 1M
- NR -
+ NR -
+ NR -
- NR -
1.993
3,183
3,079
3,106
3,173
2,492
2,101
3,080
1,775
9,630
Disease Sites
Nodes, liver,
spleen, scalp
nodules
Nodes, bone
marrow
Nodes, bone
marrow
Nodes, femoral
mass, skin
nodules
Supraclavicular
mass, lung
mass, abdomi-
nal mass
Abdominal mass
nodes, bone
marrow
Nodes, liver
Nodes, spleen.
bone marrow
Nodes, liver,
bone marrow
Nodes, liver
Nodes, bone
marrow
Nodes, bone
marrow
Nodes, bone
marrow
Nodes, bone
marrow
9,600 - NR -
3.060 NR
TG/M/36 FSC
EW/M/33 FSC
ANTI-IDIOTYPE ANTIBODY THERAPY 653
Table 2. Anti-idiotype Antibody Therapy: Clinical Responses
Table 1 . Anti-idioty pe Antibody Therapy: Pati ent Characteristics
Patient!Sex/Age Dx Prior Therapy
Tumor
Masses�5 cm
PK/M/67 FSC
DSC
+
KC/M/27 FSC CVP
Chlorambucil
JC/M/44 FSC CVP
DLC Chlorambucil
High-dose
cyclophosphamide
AdriamycinSplenectomy
RD/M/44 DSC CVP
DLC Chlorambucil
MTX
VM 26
Adriamycin
Bleomycin
XRT to abd mass
Interferon
PE/M/38 FSC CVP
Chlorambucil
CJ/M/29 FSC CVP
CMOPP
CHOP
ChlorambucilSplenectomy
EL/F/36 FSC CVP
BVP
Chlorambucil
Adriamycin
Vinblastine
CG/F/53 FM CVP
Interferon
Splenectomy
BJ/F/4O FM CHOP
BVP
CCNU
Splenectomy
CP/M/42 FSC Interferon
CVP
Splenectomy
CVP
BL/F/49 FSC Splenectomy
Abbreviations: FSC, follicular small-cleaved cell lymphoma; DSC,
diffuse small-cleaved cell lymphoma; FM, follicular mixed lymphoma;
DLC. diffuse large-cell lymphoma, CVP, cyclophosphamide, vincristine,
prednisone; BVP, bleomycin, vincristine, prednisone; CHOP, cyclophos-
phamide, Adriamycin, vincristine, prednisone; MTX, methotrexate; XRT,
radiation therapy.
Antibody
Isotype�
IgG2b
lgG2a
IgG2b
lgG 1
KC 12.8 lgG2b
lgG 1
JC (2) 0.8 lgG2a
IgG1
lgG 1
0.10 lgGl
14.50 IgG2b
2.20 IgGi
20.0 IgGi
0.01 IgGi
0.02 lgG2b
243.0 IgGi
0.01 IgGl
3.26 lgG2a
49.4 IgG2a
lgG 1
lgG 1
EW 34.0 IgGi
IgG 1
+ BL 3.0 lgG2blgGl
+
Number in parentheses refers to the fact that the patient has been
treated more than once on this antibody protocol.
tAll antibodies are mouse monoclonals.
�This patient was entered on another treatment protocol after receiv-
ing antibody therapy, and the duration of the PR could not be
determined.
continued tumor regression for over 25 months. Therapy in
patient BL was aborted after five antibody infusions because
of an immune response against horse immunoglobulin, a
minor contaminant, in the antibody preparation. Toxicity
+ was limited to urticaria. Patient EW never achieved circulat-
ing levels of free anti-idiotype antibody in serum because of a
+ relatively high serum-idiotype level and large tumor bulk.Patient PK, the first patient treated with anti-idiotype
antibody, achieved a complete remission. He remained free
ofdisease for 6 years with no additional therapy. At that time
- an erythematous macular skin lesion appeared on the dorsum
of one foot distal to a site of cellulitis. Biopsy of this lesion
- revealed diffuse small-cleaved cell lymphoma. CT scans of
the chest, abdomen, and pelvis; lymphangiogram; bone mar-
- row biopsy; and immunostaining of the bone marrow aspirate
- and peripheral blood lymphocytes were all negative for
disease. Immunoperoxidase staining of the skin lesion
showed this recurrent disease to be idiotype positive.
In the original report of nine patients with B-cell malig-
nancies treated with anti-idiotype antibodies, four patients
developed human antimouse immunoglobulin responses
necessitating cessation of therapy with the murine proteins.
Subsequent patients were treated with purer antibody prepa-
rations, and no further immune responses of this type were
seen in the antibody-alone trial. The only toxicity that was
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom

Table 3. Combination Anti-idiotype Antibody and Interferon
BR/M/45 FSC CVP
Chlorambucil
Vinblastine
Chlorambucil Nodes, bone
marrow, mes-
enteric mass
Stomach ulcer
and associated
mass
Nodes, skin nod-
ules, bone
marrow
Nodes, bone
marrow, mes-
enteric mass
Nodes, bone
marrow
Nodes, neck
mass, skin
nodules
+
+
+
+
RT/M/46 FSC
KB/F/43 FSC
RV/M/55 FSC
Chlorambucil
CVP
654 BROWN ET AL
consistently noted was fever and chills on the first day of
antibody administration. Once circulating idiotype-positive
cells and idiotype protein in the serum were cleared, patients
were able to receive multiple antibody infusions without side
effects.
Therapeutic trial of anti-idiotype antibody and interfer-
on. A summary of the clinical features of the patients
treated with anti-idiotype antibodies and interferon is shown
in Table 3. Eleven patients were entered on this protocol,
including six males and five females. Ages ranged from 32 to
Therapy: Patient Characteristics
TumorPatient! MassesSex/Age Dx Prior Therapy Disease Sites �5 cm
BL/F/49 FSC Splenectomy -
DT/F/44 FSC
MW/F/5 1 FM CVP-B
DLC CMOPP
CHOP
RI
XRT to T spine
mass
XRT to flank
mass
BE/M/32 FSC CVP
FM Chlorambucil
RW/M/47 FM
F + DM
w/DLC
PC/F/46 FSC
Chlorambucil
CVP
BCEPP
CVP
Chlorambucil
JC/M/44 FSC CVP
DLC Chlorambucil
High-dose
cyclophosphamide
Adriamycin
Splenectomy
Nodes, bone
marrow
Nodes, bone
marrow
Nodes, bone
marrow
Nodes, bone
marrow
Nodes, bone
marrow, mes-
enteric mass,
spleen
Abbreviations: FSC, follicular small-cleaved cell lymphoma; FM, fol-
licular mixed lymphoma; DLC. diffuse large-cell lymphoma; F + DM
w/DLC, follicular and diffuse mixed lymphoma with focal areas of diffuse
large-cell lymphoma; CVP, cyclophosphamide, vincristine, prednisone;
C-MOPP, cyclophosphamide. vincristine, prednisone, procarbazine;
CHOP, cyclophosphamide, Adriamycin, vincristine, prednisone; �CEPP,
bleomycin, cyclophosphamide, VP-i 6, prednisone, procarbazine; RI,
total lymphoid radiation; XRT, radiation therapy; T spine, thoracic spine.
55 years. All 1 1 patients had follicular lymphoma at the time
of initial biopsy. However, in three cases a progression in
tumor histology occurred during the period between initial
biopsy and entry into the treatment phase of this study. The
tumors of two patients transformed to diffuse large-cell
lymphoma, and one transformed from a follicular mixed to a
follicular and diffuse mixed with focal areas of diffuse
large-cell lymphoma. Nine patients had been previously
treated with chemotherapy and/or radiotherapy. Two
patients, JC and BL, had previously been treated with
anti-idiotype antibodies. One patient, RT, had no prior
therapy. Nine patients had disease that was progressing prior
to the initiation of therapy, and two patients, RT and BL,
had stable, measurable disease. Ten patients had involve-
ment of five or more lymphoid anatomic sites. The remaining
patient, MW, had diffuse involvement of the gastrointestinal
(GI) tract. Five patients had individual tumor masses of S cm
or greater.
+ Prior to the initiation of therapy, peripheral-blood mono-
nuclear cells were examined as cytocentrifuge preparations.
- Immunostaining with anti-idiotype antibodies allowed the
detection of circulating lymphoma cells in every patient
(manuscript in preparation). These circulating lymphoma
- cells could only rarely be identified by morphology alone
with routine hematologic stains.
Table 4 summarizes the treatments with anti-idiotype
antibodies and interferon. Mouse MoAbs, predominantly of
the IgG 1 class, were used in nine patients, and rat MoAbs
were used in two patients. There were two patients, JC and
BR, who were treated with more than one monoclonal
- anti-idiotype antibody. Patient BR received two separate
courses of treatment. Individual doses of antibody ranged
Table 4. Combination Anti-idiotype Antibody and Inte
Therapy: Antibody and Interferon Treatments
rferon
No. of RXPretherapy Total After
Id Level Antibody Antibody No. of AB Sustained IFN DosePatient �zg!mL lsotype� Dose (mgI RX AB Levels Delivered
BL 7.0 IgGi 4,308 ii 10 80%
BR(i) 4.0 rIgGi 3,800 7 3 75%
(2) 1.0 rIgGi 7,530 11 10
rlgG2a
75%
DT 12.3 IgG1 6.840 12 10 80%
MW 19.8 rlgG2a 4,740 9 8 100%
BE 4.6 IgGi 8,400 12 11 100%
RW 0.1 IgGi 2,930 11 O� 88%
PC 1.7 IgGi 4,440 9 5 76%
JC 1.0 lgG2a 2.500 6 5
lgG 1
lgG 1
46%
RT 4.7 IgGi 2,880 6 4 100%
KB 2.5 IgGi 1,680 6 5 80%
RV 3.5 IgGi 7,440 9 3 45%
‘Number in parentheses refers to the fact that the patient has been
treated more than once on this antibody protocol.
tAll antibodies are mouse monoclonals with the exception of those
with the prefix ‘r,” which are rat monoclonals.
�This patient was treated on a different dosing schedule than other
patients and did not achieve the same peak serum levels.
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom

900 mg
0 2 4 6 8 10 12 14 16 18
DAYS
Fig 1 . Pharmacokinetics of anti-idiotype antibody. The anti-body treatments from the first course of therapy in patient BR areshown. A total of seven treatments were given. The first four
treatments were at a dose of 500 mg. The last three treatmentswere at a dose of 900 mg. Only with the last treatments were peak
serum levels greater than 200 �g/mL and trough levels of freeanti-idiotype antibody in serum sustained.
ANTI-IDIOTYPE ANTIBODY THERAPY 655
from 240 mg to 900 mg. The cumulative antibody dose over
the treatment courses in these patients ranged from 2,500 mg
to 8,400 mg, depending on the availability of antibody.
The initial dose of anti-idiotype antibody was approxi-
mately 500 mg and was adjusted upward in an attempt to
achieve peak serum levels of at least 200 sg/mL and trough
levels that rose with successive treatments. In previous
studies we have demonstrated that tissue penetration occurs
at these serum levels.5 Not all treatment doses resulted in
sustained levels of antibody in serum. For that reason the
number of treatments delivered after levels of free anti-
idiotype were achieved are designated separately in Table 4.
As an example of how dosage adjustments were made, Fig 1
shows the pharmacokinetics of MoAb in patient BR during
the first course of treatment. Four infusions were given at the
500-mg dose level. When the dose was then raised to 900 mg,
peak serum levels greater than 200 �g/mL were achieved
and trough levels of free anti-idiotype rose progressively.
All patients experienced some toxicity attributable to the
interferon. Fever and rigors were invariably noted on the first
day of interferon administration. Fever was less frequent on
subsequent days. Seven patients developed neutropenia
(WBC <2,500), four patients developed thrombocytopenia
(platelet count < 100,000), and/or three patients developed
GI distress. Because of these side effects, only three of 1 1
patients could tolerate the full interferon dose. No toxicity
could be related to the antibody administration, although it
could have contributed to the fever and chills observed on the
first day of each patient’s therapy. Two patients (RT and
KB) in this trial made an immune response against mouse
immunoglobulin. Interestingly this included the single
patient who had no prior therapy for lymphoma (RT) and a
patient treated only in the past with limited amounts of pulse
chlorambucil (KB). Symptomatic arthralgias necessitated
discontinuation of antibody therapy in patient RT on day 10.
400
350
300
.� 250
� 200
� 150
100
50
0
500mg
Q Q ,c� v�
In patient KB difficulty swallowing without respiratory
compromise necessitated discontinuation of antibody ther-
apyonday 14.
During the first week of antibody therapy, several patients
developed swelling in one or more lymph node sites that
subsided within 2 weeks. All tumor sites that showed this
reaction had major regressions following treatment.
Eleven patients and 12 treatment courses were evaluable
for tumor response (Table 5). Ten of the 1 1 patients had
objective evidence of tumor regression. In 1 2 treatment
courses there were two complete responses, seven partial, and
two minor responses. Response durations ranged from 2
months for patient JC to greater than 24 months for patient
BL. The median response time was 7 months, with a mean
that is yet to be determined since two patients are still
responding at 21 and 24 months. Tumor regressions were
first noted between ten days to 3 weeks after initiation of
treatment. In many cases tumors continued to regress slowly
for weeks to months after the discontinuation of therapy.
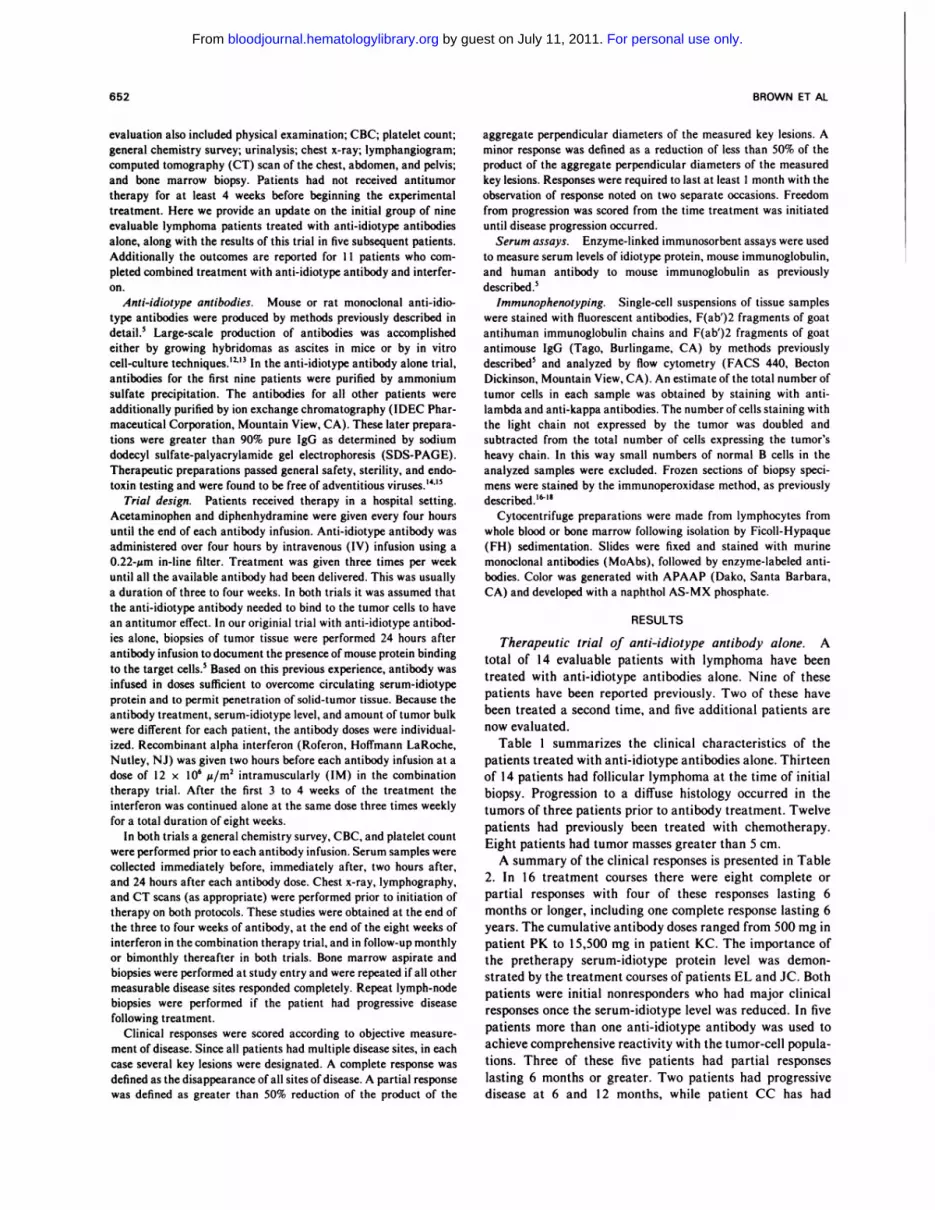
Details ofseveral cases are shown in Figs 2 through S. The
course of Patient BR was particularly interesting. Immedi-
ately prior to inclusion on this trial he had rapidly progressive
disease after failing chemotherapy. All nodal sites and bone
marrow were involved, including large tumor masses in the
mediastinum and iliac nodes. Two weeks after the initiation
of anti-idiotype antibody and interferon treatment an objec-
tive tumor response was noted. With each evaluation over the
next 3 months the tumor mass continued to decrease (Fig 2).
In the pelvis, however, the initial tumor response occurred
mostly in the right iliac lymph nodes, while the nodes on the
left responded to a lesser degree (Fig 3A and B). Three and
one-half months after the initiation of treatment, the left
iliac lymph nodes began to regrow (Fig 3C). The patient
received a second course of treatment, this time with two
anti-idiotype antibodies (anti-BR 1 and anti-BR 2). Ten days
after the reinitiation of treatment a second tumor response
was detected. The left iliac lymph nodes responded (Fig 3D).
The tumor continued to regress over the subsequent 8 months
until no radiographic evidence of disease was apparent. Bone
Table 5. Combination Anti-idiotype Antibody and Interferon
Therapy: Clinical Responses
Freedom
PatientHuman
a MouseTumor
Responsefrom
Progression
BL - CR 24M+
BR(2) - CR 21M+
DT - PR i3M
MW - PR 9M
BE - PR 7M
RW - PR SM
BR(i) - PR 3M
PC - PR 3M
Jc - PR 2M
RT + MR 6M
KB + MR SM
RV - NR -
#{149}Numberin parentheses refers to the fact that the patient has been
treated more than once on this antibody protocol.
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom
656 BROWN ET AL
Fig 2. Chest CT scans of
patient BR. A and C prior totreatment and B and D follow-ing the first course of combina-tion anti-idiotype and inter-
feron treatment. Shown is areduction in the prevascular.
paratracheal, and pericardial
adenopathy.
marrow biopsy and aspirate at that time showed no lympho- treatment was initiated. In each case a pretherapy biopsy
matous involvement, and the patient remains in a complete confirmed that the lymphoma cells continued to express
remission. idiotype. All three of these patients achieved objective tumor
Three patients, JC, MW, and RW, had histologic trans- responses. Patient JC had regression of a neck mass that
formation to a predominantly large-cell pattern by the time extended from the mandible to the thoracic inlet; MW had
Fig 3. Pelvic CT scans ofpatient BR. Prior to treatment
(A) enlarged lymph nodes areevident bilaterally in the iliacchains, but only the lymphnodes on the left were opaci-fled by lymphangiogram dye.After the first course of ther-apy (B) the lymph nodes in the
right iliac chain underwent amarked regression. Lymphnodes in the left iliac chain alsoregressed but not completely.Prior to the second course oftreatment (C) lymph nodes inthe left iliac chain grew. Lymphnodes in the right iliac chain re-
mained stably regressed. Afterthe second course of treatment(D) the lymph nodes in the leftiliac chain completely re-
greased.
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom
ANTI-IDIOTYPE ANTIBODY THERAPY 657
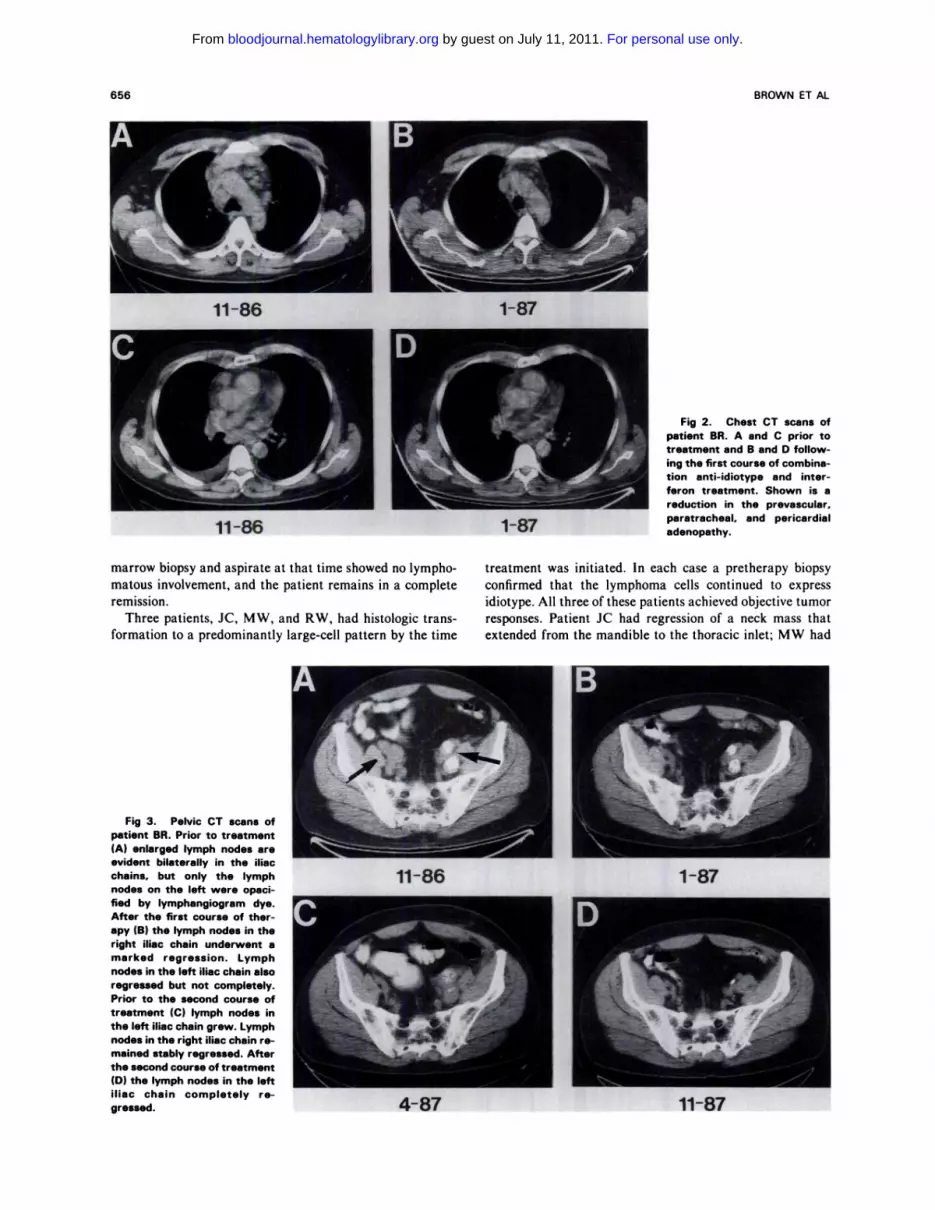
Fig 4. Lymphangiogram of patient BE before and after treat-ment with anti-idiotype antibody and interferon. Patient BE hadslowly progressive disease despite chemotherapy. Sites ofinvolvement included bone marrow. multiple skin nodules scat-
tered across the trunk and face. and enlarged para-aortic and leftiliac nodes. Tumor regression was noted 3 weeks after theinitiation of treatment and continued for 5 months before stabiliz-ing. Opacified nodes (see left iliac region) on lymphangiogramwere decreased in size. and multiple skin lesions resolved. Someskin lesions became smaller. less indurated. and less erythema-tous without disappearing completely. These skin lesions pro-greased at 71/2 months. and several new peripheral nodesdeveloped. The regression in the nodal disease visualized onlymphangiogram was maintained.
endoscopically proven regression of an ulcerating gastric
mass; and RW had regression of bulky peripheral disease
and a mesenteric mass.
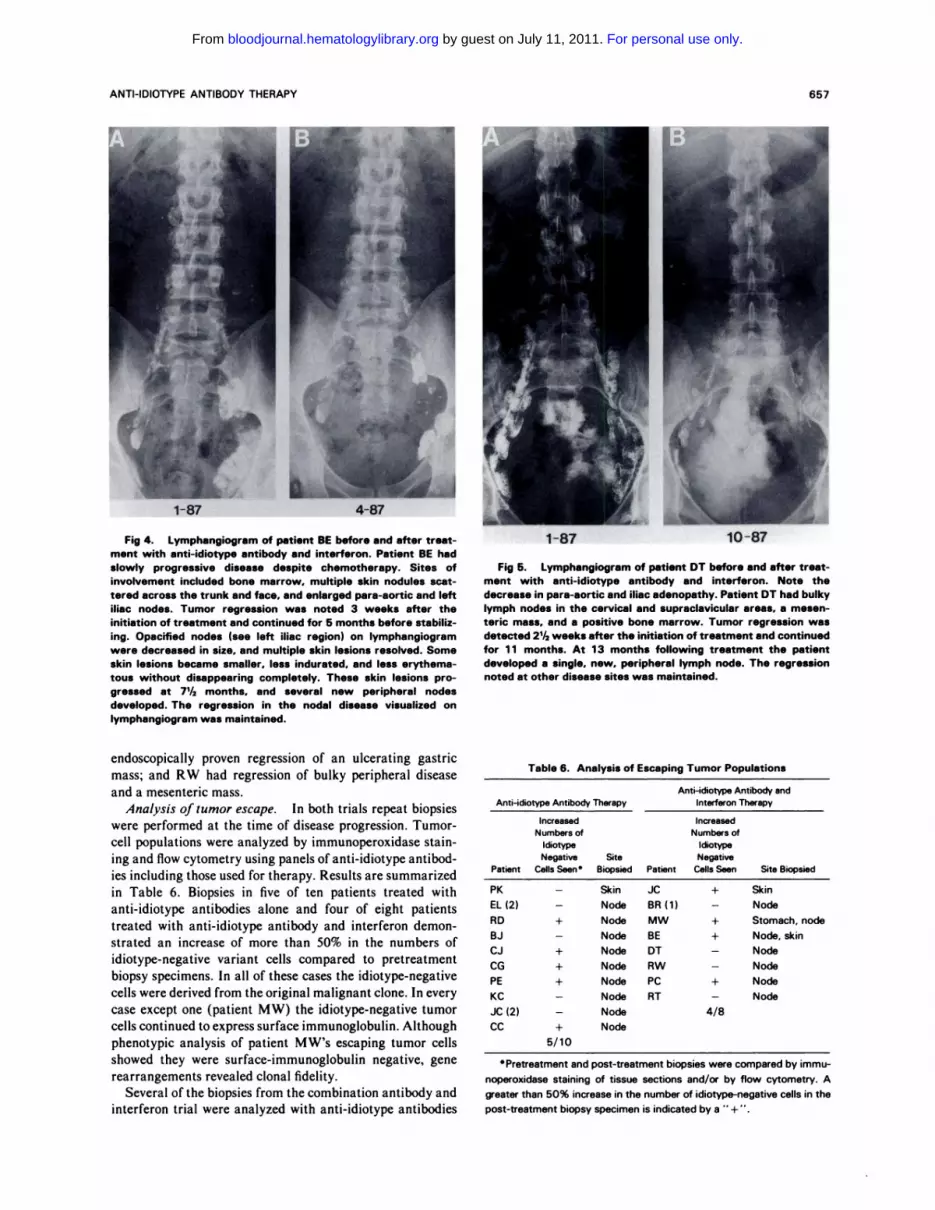
Analysis oftumor escape. In both trials repeat biopsies
were performed at the time of disease progression. Tumor-
cell populations were analyzed by immunoperoxidase stain-
ing and flow cytometry using panels of anti-idiotype antibod-
ies including those used for therapy. Results are summarized
in Table 6. Biopsies in five of ten patients treated with
anti-idiotype antibodies alone and four of eight patients
treated with anti-idiotype antibody and interferon demon-
strated an increase of more than 50% in the numbers of
idiotype-negative variant cells compared to pretreatment
biopsy specimens. In all of these cases the idiotype-negative
cells were derived from the original malignant clone. In every
case except one (patient MW) the idiotype-negative tumor
cells continued to express surface immunoglobulin. Although
phenotypic analysis of patient MW’s escaping tumor cells
showed they were surface-immunoglobulin negative, gene
rearrangements revealed clonal fidelity.
Several of the biopsies from the combination antibody and
interferon trial were analyzed with anti-idiotype antibodies
Fig 5. Lymphangiogram of patient DT before and after treat-ment with anti-idiotype antibody and interferon. Note the
decrease in para-aortic and iliac adenopathy. Patient DT had bulkylymph nodes in the cervical and supraclavicular areas. a mesen-teric mass, and a positive bone marrow. Tumor regression wasdetected 21/2 weeks after the initiation of treatment and continuedfor 1 1 months. At 1 3 months following treatment the patientdeveloped a single, new, peripheral lymph node. The regressionnoted at other disease sites was maintained.
Table 6. Analysis of Escaping Tumor Populations
Anti-idiotype Antibody andAnti-idiotype Antibody Therapy Interferon Therapy
Increased IncreasedNumbersof Numbers of
Idiotype ldiotype
Negative Site NegativePatient Cells Seen Biopsied Patient Cells Seen Site Biopsied
PK - Skin JC + Skin
EL(2) - Node BR(1) - Node
RD + Node MW + Stomach, node
BJ - Node BE + Node, skin
CJ + Node DT - Node
CG + Node RW - Node
PE + Node PC + Node
KC - Node RT - Node
Jc (2) - Node 4/8
CC + Node
5/10
Pretreatment and post-treatment biopsies were compared by immu-
noperoxidase staining of tissue sections and/or by flow cytometry. A
greater than 50% increase in the number of idiotype-negative cells in the
post-treatment biopsy specimen is indicated by a “ +“.
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom

658 BROWN ET AL
Table 7. Analy sis of Escaping Tumor-C elI Populations: Patient BE
AnalysisPretreatment Biopsy
% ld+ CellsPost-treatment Biopsy
% ld+ Cells
a-BE 1
a-BE 2
a-BE 3
85
90
88
0.5
25
84
C Numbers represent the percent of the tumor population that reacted
with each anti-idiotype antibody. Total tumor population was estimated
by staining with antikappa and antilambda antibodies.
specific for the patient’s idiotype that were not used for
treatment. An example of this is shown in Table 7. Patient
BE had a biopsy of a progressing skin lesion that showed the
tumor cells retained reactivity with anti-BE 1, the antibody
used for therapy. A lymph-node biopsy at the same time,
however, contained almost exclusively anti-BE 1 idiotype-
negative cells. Analysis with other anti-idiotype antibodies,
anti-BE 2 and anti-BE 3, was revealing. (These antibodies
were not available in amounts large enough for inclusion in
the treatment program.) The determinant (idiotope) recog-
nized by anti-BE 2 was expressed by 90% of the tumor cells
in a pretreatment biopsy but by only 25% of the tumor cells
in the biopsy at the time of progressive disease. This example
demonstrates the strong selective pressure anti-idiotype anti-
bodies exert against antigen-positive cells and also shows that
coselection against a related idiotope can occur. An idiotope
defined by the third anti-idiotype, antibody anti-BE 3, was
expressed by 88% of the tumor cells pretreatment and 84% of
the tumor cells post-treatment and was not selected against
by the treatment antibody.
A more subtle selective pressure was revealed by analysis
of tissue samples from patient BR. In those samples flow
cytometry analysis with the two anti-idiotype antibodies
showed three distinct populations of lymphoma cells (Fig 6).
One population reacted with anti-BR 1 alone, one population
reacted with anti-BR 1 and anti-BR 2, and one population
reacted with anti-BR 2 alone. During’the time between the
intake and pretreatment biopsies the total number of tumor
cells staining with anti-BR 1 (the number of cells that stain
with anti-BR 1 alone plus the number of cells that stain with
both antibodies) remained fairly constant and was 96% or
greater. However, heterogeneity that can exist in lymphoma
cell populations from site to site and in different points in
time was demonstrated by the change in the number of cells
reacting with both anti-idiotype antibodies. The pretreat-
ment lymph node showed comprehensive reactivity with
anti-BR 1 and was biopsied from a chain of lymph nodes that
underwent a major tumor regression in response to treatment
with that antibody (Fig 3B). At the time of disease
progression a biopsy from a left pelvic lymph node chain that
responded incompletely to therapy showed a population of
cells (approximately 9.5%) reacting with anti-BR 2 but not
with anti-BR 1. These cells were not effectively eliminated
until the patient received infusions of both anti-BR 1 and
anti-BR 2 (Fig 3D).
DISCUSSION
The current results confirm that treatment with anti-
idiotype antibodies produce significant tumor regressions in
B-cell lymphoma. In 16 courses of therapy there were eight
complete or partial responses with anti-idiotype antibodies
alone. This compares to nine complete or partial responses in
12 courses of therapy with combination anti-idiotype anti-
bodies and interferon. In both trials tumor responses
occurred in patients who had failed multiple conventional
forms of treatment and in patients who had histologic
conversion to intermediate-grade lymphoma. Because of its
lack of toxicity, therapy with anti-idiotype antibodies was
well tolerated, even in patients who had been heavily
pretreated with other therapies.
The dose and scheduling of anti-idiotype antibodies are
both important issues. In the current trials the dose of
antibody was individualized for each patient with the goal of
penetrating tumor tissue. This pharmacologic concept led to
cumulative doses greater than 2 g for most patients. It is
possible that lower doses would be equally effective. For
instance, the patient with the longest remission, PK, received
only 500 mg of antibody. By analogy to chemotherapy
models, antibody treatment may also be improved by
changes in the schedule of administration. For instance,
multiple cycles of antibody may be preferable. The timing of
such cycles would need to be chosen according to a better
understanding of the way in which antibodies act.
The mechanism of action of anti-idiotype antibodies has
not been elucidated in man, although antibody-dependent
cellular cytotoxicity (ADCC) plays a role in the murine
lymphoma model.’ In the clinical trials, antibody affinity
and isotype do not seem to have discernible impact on
treatment results.’9 The presence of a tumor response, or the
magnitude of that response, could not be correlated in either
trial with the subclass of the antibody, since major clinical
responses were induced by antibodies of IgG 1 as well as
IgG2a and IgG2b subclasses. Anti-idiotype antibodies are
more active in B-cell malignancies than antibodies that react
with nonimmunoglobulin differentiation antigens.2#{176}’23 This
could be related to the greater specificity of the anti-idiotype
antibodies or to their inherent biological activity, since
anti-idiotypes have regulatory functions in the immune sys-
tem.2�26 In both trials it was common to see tumor regression
continuing months after the treatment phase was complete,
suggesting that passive infusion of anti-idiotype antibodies
may have an antitumor effect by altering the idiotype-
anti-idiotype network that plays a role in the regulation of
B-cell clones.
The addition of interferon to the treatment program was
based on both its known independent activity in follicular
non-Hodgkin’s lymphoma and its synergistic activity with
anti-idiotype antibodies in a murine lymphoma model. The
interferon dose chosen in this study, 12 x 106 z/m2 three
times weekly for 8 weeks, was based on the results of an
Eastern Cooperative Oncology Group pilot trial.27 In that
study seven of 16 patients with previously untreated follicu-
lar lymphoma had objective tumor responses, including one
complete response and six partial responses. Responding
patients on that study continued to receive maintenance
doses of interferon; however, no additional responses were
noted after the first 8-week treatment block. For this reason
we chose to limit the time of treatment with interferon to 8
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom

BIOPSY
98%�
BIOPSY
2.6% 12%� 75.5%
�-1
L �
I-z
0.1% 9.5%
ANTI-IDIOTYPE ANTIBODY THERAPY 659
There was a trend toward a higher rate of tumor response
INTAKE PRE TREATMENT POST TREATMENT
BIOPSY
ANTI-BR 2
ANTI-HUMAN KAPPA
Fig 6. Distinct tumor cell populations in patient BR. Two-color flow cytometry analysis was performed on cell suspensions from biopsyspecimens. The percentages of the total tumor population staining with each antibody alone and with both antibodies are indicated. Thetotal tumor population. as measured by those cells staining with antihuman kappa, remains constant. Intake biopsies from right and leftinguinal lymph nodes showed a population of cells staining with anti-BR 1 and a population doubly stained with anti-BR 1 and anti-BR 2.Biopsy immediately prior to treatment. a right iliac lymph node. showed that anti-BR 1 stained virtually all of the B cells. Biopsy from a leftiliac lymph node after the first course of combination anti-idiotype antibody and interferon treatment showed an increasing population ofcells staining exclusively with anti-BR 2. Additionally the population of cells doubly stained with anti-BR I and anti-BR 2 had increased.
weeks. In other studies response rates to alpha interferon
have ranged from 1 6% to 54% in low-grade lymphoma.2834
The dose of interferon was chosen for its antitumor effect,
but this may not have been the optimal dose and schedule to
provide a synergistic biological effect with the anti-idiotype
antibodies. The addition of interferon did not prevent the
emergence of idiotype-negative clones in this study. Indeed,
in recent animal experiments the addition of interferon” or
interleukin-2 (IL-2)’#{176}to MoAb therapy has enhanced the
action of antibody against idiotype-positive disease, resulting
in more efficient selection for antigen-negative variant tumor
cells.
in patients receiving the combination of antibody and inter-
feron. However, the antitumor contribution of interferon was
difficult to assess because of the small number of patients on
both trials. Furthermore, the trials were not identical in
several respects. Although an attempt was made to select
patients with similar clinical characteristics in both trials,
this was difficult to assure. The purity of the antibody
preparations was improved after the first nine patients were
treated on the antibody-alone trial and for the combination
trial. There was a lower rate of antimouse immunoglobulin
responses in these later patients. When the patients who
made antimouse immune responses are excluded from analy-
sis, the response rates are more comparable between the two
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom
REFERENCES
660 BROWN ET AL
12. Evans TL, Hart SM, Nguyen HT, Coulter C, Quentin J,
trials. Interferon was added with the expectation that its
antilymphoma action would equally affect idiotype-positive
and idiotype-negative variant cells, yet selection for idiotype-
negative variants still occurred. Thus the current results
suggest a stronger antitumor effect by the antibodies than by
the interferon.
In previous clinical trials with MoAbs, the development of
a human antimouse immunoglobulin response has been a
significant obstacle to therapy. In our first report of nine
patients with B-cell lymphoma treated with murine anti-
idiotype antibodies, four immune responses to mouse immu-
noglobulins were seen. With the more highly purified anti-
bodies used in the current studies, two immune responses to
mouse immunoglobulin were seen. One immune response
occurred in a patient who had received no prior chemothera-
py; the other occurred in a patient who had received minimal
prior chemotherapy. Additionally, the low rate of antimouse
immunoglobulin responses in B-cell malignancies is in stark
contrast to other diseases where treatment with murine
antibodies is almost universally associated with the develop-
ment of an immune response, even in patients heavily
pretreated with chemotherapy.3�#{176} Thus patients with B-cell
malignancies may be specially suited to treatment with
xenogeneic antibodies because of immunosuppression asso-
ciated with a decreased ability to mount a humoral immune
response’#{176}
Detailed analysis of escaping tumor cell populations with
multiple anti-idiotype antibodies revealed subtle differences
in the idiotypes expressed. This was seen, for example, in the
cells of patient BE, in whom coselection against a second
idiotope could be demonstrated following treatment with an
anti-idiotype antibody while the expression of a third idio-
tope was unaffected by the antibody exposure. On the other
hand, the ability to recapture the clinical responsiveness of
patient BR to anti-idiotype antibodies with an additional
antibody was noteworthy. Mixtures, or cocktails, of anti-
idiotypes for each patient may increase the therapeutic
efficacy of this treatment. Although somatic mutation of the
variable region of the immunoglobulin genes can produce
1. Levy R, Warnke R, Dorfman RF, Haimovich J: The mono-
clonality of human B cell lymphoma. J Exp Med 145:1014, 19772. Stevenson GT, Elliot EV, Stevenson FK: Idiotypic determi-
nants on the surface immunoglobulin of neoplastic lymphocytes: Atherapeutic target. Fed Proc 36:2268, 1977
3. Houghton G, Lanier LL, Babcock GF, Lynes MA: Antigen-induced murine B cell lymphomas. II. Exploitation of the surfaceidiotype as tumor specific antigen. J Immunol 121:2358, 1978
4. Brown 5, Dilley J, Levy R: Immunoglobulin secretion bymouse v human hybridomas: An approach for the production ofanti-idiotype reagents useful in monitoring patients with B cell
lymphoma. J Immunol 125:1037, 19805. Meeker TC, Lowder J, Maloney DG, Miller R, Thielemans K,
Warnke R, Levy R: A clinical trial ofanti-idiotype therapy for B cell
malignancy. Blood 65:1349, 1985
6. Meeker T, Lowder J, Cleary ML, Stewart 5, Warnke R, SklarJ, Levy R: Emergence of idiotype variants during treatment of B-cell
lymphomas with anti-idiotype antibodies. N Engl J Med 3 12:1658,1985
idiotype variants, it should be possible to target idiotypic
determinants that are either less susceptible to change or are
maintained in the tumor population due to selective forces
within the host.4’
The problem of tumor-cell heterogeneity may also be
addressed by combining anti-idiotype antibodies with cyto-
toxic agents. Tumor-cell populations may be rendered espe-
cially sensitive to cycle-active drugs by anti-idiotype antibod-
ies. Idiotype-negative variant cells, which pre-exist in the
lymphoma cell population in small numbers, may be
recruited into cycling to account for their increased propor-
tion in the escaping tumor cell population. If recruitment of
idiotype-negative variant cells following exposure to anti-
idiotype antibodies could be demonstrated, properly timed
cytotoxic drugs may improve future clinical results.
Anti-idiotype antibodies have reproducible antitumor
activity in B-cell malignancies, even in patients with disease
progression following standard therapies. They offer a novel
approach to lymphoma management. In this trial the addi-
tion of alpha interferon may have improved the response rate
but did not prevent the emergence of idiotype-negative
variant clones. This is an important problem that must still
be addressed. The optimal integration of this new treatment
modality with more conventional forms of treatment will
require further trials. Improvements in the dosing and sched-
uling of antibodies, the use of multiple anti-idiotype antibod-
ies, and combining anti-idiotype antibodies with cytotoxic
therapies and/or biological response modifiers should
improve the extent and duration of the clinical responses.
ACKNOWLEDGMENT
The authors wish to acknowledge the laboratories of Dr JeffreySklar for the gene rearrangement studies and Dr Joanne Cornbleetfor the immunophenotyping of the cytocentrifuge preparations. The
authors also wish to thank Carol Doss and Virginia Rojas for help inprocessing tissue samples and the nurses of the Cancer Research
Center B, Stanford University Hospital, for excellent patient care.Expert secretarial assistance was provided by Phyllis Bussey and
Cheryl Joo.
7. Cleary ML, Meeker TC, Levy 5, Lee E, Trela M, Sklar J,Levy R: Clustering of extensive somatic mutations in the variableregion of an immunoglobulin heavy chain gene from a human B cell
lymphoma. Cell 44:97, 19868. Kaminski MS. Kitamura K, Maloney DG, Campbell Mi, Levy
R: Importance of antibody isotype in monoclonal anti-idiotypetherapy of a murine B cell lymphoma. A study of hybridoma classswitch variants. J Immunol 136:1 123, 1986
9. Starnes CO. Carroll WL, Campbell MJ, Houston LL, Apell G,
Levy R: Heterogeneity of a murine B cell lymphoma: Isolation andcharacterization of idiotypic variants. J Immunol 141:333, 1988
10. Berinstein N, Levy R: Treatment of a murine B celllymphoma with monoclonal antibodies and IL 2. J Immunol
139:971, 1987
1 1. Basham TY, Kaminski MS, Kitamura K, Levy R, MeriganTC: Synergistic antitumor effect of interferon and anti-idiotype
monoclonal antibody in murine lymphoma. J Immunol 137:3019,
1986
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom

ANTI-IDIOTYPE ANTIBODY THERAPY 661
Miller RA, Fleig GE: Large scale production of monoclonal antibod-ies using hollow fiber bioreactors with specific molecular weight
cutoffs. IV Decennial TCA Review Conference, September 198613. Posillico EG: Microencapsulation technology for large scale
antibody production. Bio Tech 4:1 14, 1986
14. Collins Mi, Parker JC: Murine virus contaminants of leuke-
mia viruses and transplantable tumors. J Natl Cancer Inst 49:1 139,
1972
I 5. Peebles PT: An in vitro focus induction assay for xenotropic
murine leukemia virus, feline leukemia virus C, and the feline-
primate viruses RD-I l4/CCC/M-7. Virol 67:128, 1975
16. Warnke R, Levy R: Detection of T and B cell antigens withhybridoma monoclonal antibodies. A biotin-avidin-horseradish per-
oxidase method. J Histochem Cytochem 28:771, 198017. Wood GS, Warnke RA: The immunologic phenotyping of
bone marrow biopsies and aspirates: Frozen section techniques.Blood 59:913, 1982
18. Meeker TC, Miller RA, Link MP, Bindl J, Warnke R, Levy
R: A unique human B lymphocyte antigen defined by a monoclonal
antibody. Hybridoma 3:305, 198419. Lowder JN, Meeker TC, Campbell M, Garcia C, Gralow J,
Miller R, Warnke R, Levy R: Studies on B lymphoid tumors treatedwith monoclonal anti-idiotype antibodies: Correlation with clinical
responses. Blood 69:199, 198720. Foon KA, Schroff RW, Bunn PA, Mayer D, Abrams PG. Fer
M, Ochs J, Bottino GC, Sherwin SA, Carlo DJ, Herberman RB,
Oldham RK: Effects of monoclonal antibody therapy in patientswith chronic lymphocytic leukemia. Blood 64:1085, 1984
21. Dillman RO, Beauregard J, Shawler DL, Halpern SE, Mark-
man M, Ryan KP, Baird SM, Clutter M: Continuous infusion ofTIOl monoclonal antibody in chronic lymphocytic leukemia and
cutaneous T-cell lymphoma. J Biol Response Mod 5:394, 1986
22. Dillman RO, Shawler DL, Dillman JB, Royston I: Therapy ofchronic lymphocytic leukemia and cutaneous T-cell lymphoma with
TiOl monoclonal antibody: J Clin Oncol 2:881, 1984
23. Press OW, Appelbaum F, Ledbetter JA, Martin P, Zarling J,Kidd P. Thomas ED: Monoclonal antibody lF5 (anti-CD2O) sero-therapy of human B cell lymphomas. Blood 69:584, 1987
24. Jerne NK: Towards a network theory of the immune system.
Ann Immunol 125C:373, 1974
25. Geha RS: Regulation of the immune response by idiotype-
anti-idiotype interactions. New Engl J Med 305:25, 1981
26. Kearney JF, Vakil M: Idiotype-directed interactions duringontogeny play a major role in the establishment of the adult B cellrepertoire. Immunol Rev 94:39, 1986
27. O’Connell MJ, Colgan JP, Oken MM, Ritts RE Jr, Kay NE,Itri LM: Clinical trial of recombinant leukocyte A interferon as
initial therapy for favorable histology non-Hodgkin’s lymphomas
and chronic lymphocytic leukemia: An Eastern Cooperative Oncol-
ogy Group pilot study. J Clin Onc 4:128, 1986
28. Goldstein D, Laszlo J: Interferon therapy in cancer: Fromimaginon to interferon. Cancer Res 46:4315, 1986
29. Louie AC, Gallagher JG, Sikora K, Levy R, Rosenberg SA,Merigan TC: Follow-up observations on the effect of human leuko-
cyte interferon in non-Hodgkin’s lymphoma. Blood 58:712, 198130. Quesada JR, Hawkins M, Horning S, Alexanian R, Borden
E, Merigan 1, Adams F, Gutterman JV: Collaborative Phase I-Ilstudy of recombinant DNA-produced leukocyte interferon (clone A)in metastatic breast cancer, malignant lymphoma and multiple
myeloma. Am J Med 77:427, 198431. Gams R, Gordon D, Guaspani A: Phase II trial of human
polyclonal lymphoblastoid interferon in the management of malig-nant lymphomas. Proc Am Soc Clin Oncol 3:65, 1984
32. Horning Si, Merigan TL, Krown SE, Gutterman JU, LowieA, Gallagher J, McCravey J, Abramson J, Cabarrillas F, Oettger H,
Rosenberg SA: Human interferon a in malignant lymphoma and
Hodgkin’s disease. Cancer 56:1305, 198533. Foon KA, Sherwin SA, Abrams PG: Treatment of advanced
non-Hodgkin’s lymphoma with recombinant leukocyte A interferon.N EnglJ Med3ll:ll48, 1984
34. Leavitt RD, Ratanatharathorn V, Ozer H, Ultmann JE,Portlock C, Myers JW, Kisner D, Norred S, Spiegel Ri, Bonnem
EM: Alfa-2b interferon in the treatment of Hodgkin’s disease andnon-Hodgkin’s lymphoma. Semin Oncol 14 (2 Suppl 2):18, 1987
35. Houghton AN, Mintzer D, Cordon-Cardo C, Welt S, FliegelB, Vadham S, Carswell E, Melaned M, Oettgen AF, Oh Li: Mousemonoclonal IgG3 antibody detecting GD3 ganglioside: A phase I
trial in patients with malignant melanoma. Proc Natl Aced Sci USA82:1242, 1985
36. Oldham RK, Foon KA, Morgan AC: Monoclonal antibody
therapy of malignant melanoma: In vivo localization in cutaneousmetastasis after intravenous administration. J Clin Oncol 2:1235,
198437. Foon KA, Schroff RW, Mayer D, Sherwink SA, Oldham
RK, Burns PA, Hsu SM: Monoclonal antibody therapy of chroniclymphocytic leukemia and cutaneous T cell lymphoma: Preliminary
observations, in Boss BD, Langman RE, Trowbridge IS (eds):Monoclonal Antibodies and Cancer. Orlando, Academic, 1983, p39
38. Sears HF, Mattis i, Herlyn D, Hayry P, Atkinson B, Ernst C,Steplewski Z, Koprowski H: Phase I clinical trial with monoclonalantibody treatment of gastrointestinal tumors. Lancet 1:762, 1982
39. Sears HF, Herlyn D, Steplewski Z, Koprowski H: Phase IIclinical trial of a murine monoclonal antibody cytotoxic for gastroin-testinal adenocarcinoma. Cancer Res 45:5910, 1985
40. Shawler DL, Bartholomew RM, Smith LM, Dillman RO:
Human immune response to multiple injections of murine mono-clonal IgG. J Immunol 135:1530, 1985
41 . Kon 5, Levy 5, Levy R: Retention of an idiotypic determinantin a human B-cell lymphoma undergoing immunoglobulin variable-
region mutation. Proc Natl Acad Sci USA 84:5053, 1987
For personal use only. by guest on July 11, 2011. bloodjournal.hematologylibrary.orgFrom





























