Embed Size (px)
Citation preview
ANNALS OF SURGERYVol. 220, No. 5, 691-698© 1994 J. B. Lippincott Company
Timing of Arterialization inLiver TransplantationStefan Post, M.D.,*`t Pablo Palma, M.D.,* Alberto P. Gonzalez, M.D.,*Markus Rentsch,* and Michael D. Menger, M.D.*
From the Institute for Surgical Research,* University of Munich, and the Department of Surgery,tUniversity of Heidelberg, Federal Republic of Germany
ObjectiveThis study analyzed the pathophysiologic sequela of different modes of graft reperfusion in livertransplantation.
Summary Background DataThe grafted liver may be reperfused either immediately after completion of portal anastomosisfollowed by delayed arterial reconstruction or simultaneously by portal and arterial blood if allvascular anastomoses are completed during the anhepatic period.
MethodsDelayed arterialization, that is, arterial reperfusion 8 minutes after portal revascularization (n = 12),was compared with simultaneous arterialization (n = 8) using the model of syngeneic orthotopicliver transplantation in male Lewis rats. After cold storage for 24 hours in University of Wisconsin(UW) solution, intravital fluorescence microscopy was employed 30 to 90 minutes afterreperfusion to assess hepatic microvascular perfusion, leukocyte accumulation, and phagocyticactivity of Kupffer cells.
ResultsCompared with delayed arterialization, the number of both nonperfused acini and nonperfusedsinusoids was reduced after simultaneous reperfusion by 71% (p = 0.008) and 78% (p < 0.001),respectively. Leukocyte accumulation in sinusoids and postsinusoidal venules after simultaneousarterialization decreased by 17% (p = 0.01) and 64% (p < 0.001), respectively. In addition,simultaneous revascularization was able to attenuate Kupffer cell activation, indicated bysignificantly slower adherence of latex beads injected 80 minutes after reperfusion. Improvedhepatocellular excretory function after simultaneous arterialization was demonstrated byincreased bile flow during the observation period of 90 minutes after reperfusion (2.24 ± 0.7 vs.0.95 ± 0.4 mL/100 g liver [mean ± SEM], p < 0.05).
ConclusionsTiming of arterial reperfusion in liver transplantation may be of critical importance in the preventionof various manifestations of reperfusion injury.
Although the first clinical liver transplantation was ac- after the completion of caval and portal anastomoses,2,3complished by reperfusion ofthe graft with arterial blood to minimize the anhepatic period and the period of par-before portal declamping,' many centers prefer to reper- tial rewarming ofthe ischemic organ in the recipient. Ar-fuse the graft before arterial reconstruction, immediately terial anastomosis is usually performed thereafter, lead-
691

692 Post and Others
ing to a variable period of at least 10 minutes, duringwhich the graft is exclusively perfused by portal blood.However, occasional doubts have been expressed aboutthis practice.4 Although improved macroscopic appear-ance ofthe graft was reported after simultaneous arterialand portal reperfusion,5 quantitative data have beenmissing up to now comparing simultaneous with delayedarterialization in clinical or experimental liver transplan-tation.
In the rat model of orthotopic liver transplantation,many authors have regarded arterialization itself as anunnecessary effort in both immunologic and preserva-tion studies,69 despite that in normal and transplantedrats, up to one fourth of total hepatic blood flow mayenter the liver through the hepatic artery.'0 In addition,marked differences have been reported between arterial-ized and nonarterialized rat liver transplants regardingpostoperative weight gain and serum enzymes,"l antigenpresentation, 2 histomorphology,'3 and survival afterprolonged cold storage.'4 Previously, we were able todemonstrate that arterialization of grafted rat liver im-proves blood cell velocities, bile flow, and sinusoidal per-fusion in zone II (without any effects on leukocyte adher-ence) compared with a nonarterialized model.'5 Thesedifferences have provided strong arguments against theomission of arterial reconstruction in the rat. However,although exact timing of arterialization is usually notmentioned, all of these studies used delayed arterializa-tion, and no data on simultaneous reperfusion in ratshave yet been reported.The present study intended to analyze the impact of
timing ofarterialization on various manifestations of he-patic reperfusion injury by application of in vivo fluo-rescence microscopy, which allows direct visualizationand quantitative assessment of microvascular perfusion,leukocyte-endothelium interaction, and activation ofKupffer cells.161'8 Preliminary data of this study werepresented at the Congress of the German Surgical Soci-ety. '9
MATERIALS AND METHODSSurgical Procedure/Experimental Groups
Syngeneic orthotopic liver grafting was performed un-der ether anesthesia in 20 male Lewis rats ( 160 to 265 g;
Supported by grants from Deutsche Forschungsgemeinschaft (DFG He368/7-1, Me 900/1-2), CAPES Brazil, and ForschungsschwerpunktTransplantation Heidelberg.
For this study Dr. Palma was awarded the Banc Sabadell Award forExperimental Surgery by the Real Academia de Medicina de Bar-celona.
Address reprint requests to Priv.-Doz. Dr. med. Stefan Post, Chirur-gische Universitatsklinik, Robert-Koch-Str. 40, 37075 Gottingen,Germany.
Accepted for publication February 9, 1994.
Charles River Wiga, Sulzfeld, Germany) as describedpreviously in detail.'5'20'2' Grafts were stored for 24 hoursin UW solution (4 C) and rinsed with cold Ringer's lac-tate immediately before implantation. Arterial recon-struction was accomplished by the cuff technique pro-posed by Steffen et al.,22 with the slight modification thatthe cuff at the recipient hepatic artery was mounted be-fore hepatectomy to minimize the time required for ar-terial anastomosis later on. Suprahepatic vena cava anas-tomosis (hand sutured), infrahepatic vena cava, and por-tal vein reconstruction (cuffs) were performed during theanhepatic period.7 Arterial anastomosis was completedeither during the anhepatic period (simultaneous arteri-alization: SA-group, n = 8) or after portal reperfusion(delayed arterialization, i.e., arterial reperfusion 8 min-utes after portal declamping: DA-group, n = 12). Thecommon bile duct of the graft was cannulated to collectbile excreted after reperfusion. After intravital micros-copy, the animals were killed 90 minutes after reperfu-sion by exsanguination for collection of blood and livertissue. Experiments were performed in accordance withGerman legislation on protection of animals and the"Guide for the Care and Use of Laboratory Animals"(NIH Publication 80-23, revised 1978).
Intravital Fluorescence Microscopy
Thirty to 90 minutes after portal reperfusion, thelower surface of the left liver lobe was exposed to in vivomicroscopy with epi-illumination as previously de-scribed.'5"6'2' Contrast enhancement was accomplishedby intravenous injection of sodium fluorescein and rho-damine 6G (2 to 4 ,umol/kg and 0.1 ,umol/kg respec-tively; Merck AG, Darmstadt, Germany).'8 Phagocyticactivity was assessed by intra-arterial injection of fluo-rescence-labeled latex beads 80 minutes after reperfusion(3 X 108 beads/kg, 1.1 /Mm YG [Yellow/Green] plain;Polysciences, Warrington, PA).'7
Quantitation of microhemodynamics, leukocyte-en-dothelium interaction, and phagocytosis of latex beadswere performed off-line by frame-to-frame analysis ofvideotaped images. Thirty and 90 minutes after reperfu-sion, the left liver lobe was scanned at a lower magnifi-cation (X240), and 50 to 100 acini were graded in threecategories (no, irregular, or good perfusion) according todirect observation of sinusoidal flow behavior and hepa-tocellular uptake of fluorescent dye. An index of acinarperfusion was calculated by the formula
(Ng + 0.5Ni)/Ntwhere Ng represents the number of well-perfused acini,N1 the number of irregularly perfused acini, and N, thetotal number of acini analyzed. This index equals 1 if all
Ann. Surg. * November 1994
Arterialization in Liver Transplantation 693
acini are well perfused and 0 if no acini are perfused atall.'5
Sixty to 80 minutes after reperfusion, 8 to 15 individ-ual acini per animal were randomly selected for videorecording at a higher magnification (X600). The follow-ing parameters were analyzed in each of the experimen-tal groups for a minimum of 75 acini:
Perfusion of sinusoids (percentage ofthe total numberofobserved sinusoids)
Sticking leukocytes, defined as stained cells locatedwithin perfused blood vessels and not moving dur-ing observation for 20 seconds (standardized in si-nusoids per mm2 liver surface, in postsinusoidal ve-nules per endothelial surface area calculated by: 7r Xdiameter X length of vessel segment under observa-tion)
Rolling leukocytes in postsinusoidal venules (cellsmoving with less than 30% of center-line velocity aspercentage of all moving leukocytes).
In addition, analysis of sinusoidal parameters (perfu-sion and leukocyte adherence) was performed separatelyfor zones 1, 2, and 3 ofthe acinus.
Phagocytic activity was analyzed successively duringthe first 5 minutes after injection oflatex beads within 10to 15 randomly selected microscopic fields (405 X 540,um) per experiment (Fig. 1).17 The degree of adherencewas quantified by counting the number ofbeads movingwithin sinusoids as a percentage of all beads visiblewithin the field during an observation period of 10 sec-onds. Beads in pre- or postsinusoidal microvessels werenot counted.
Statistical AnalysisData are presented as mean ± SEM. Differences were
considered significant for p < 0.05. Comparisons be-tween groups were performed by analysis of variance af-ter rank transformation of non-normally distributeddata (depending on the results of the Shapiro-Wilk sta-tistics ofnormality). For all microscopy data with severalmeasurements within each animal, nested-design, two-way analysis of variance was used (group and individualanimals within group). In addition, in repeated measure-ments within the same experiment, effects of the timeofobservation were calculated by multivariate ANOVA.Adherence kinetics of injected latex beads were calcu-lated by a general linear model with log-transformed per-centages of moving beads as the dependent variable. In-dependent variables included in the model were time,time', time', group, time-group interactions, and animalnested within group. Calculations were performed by theSAS procedures UNIVARIATE and GLM (SAS Insti-tute, Cary, NC).
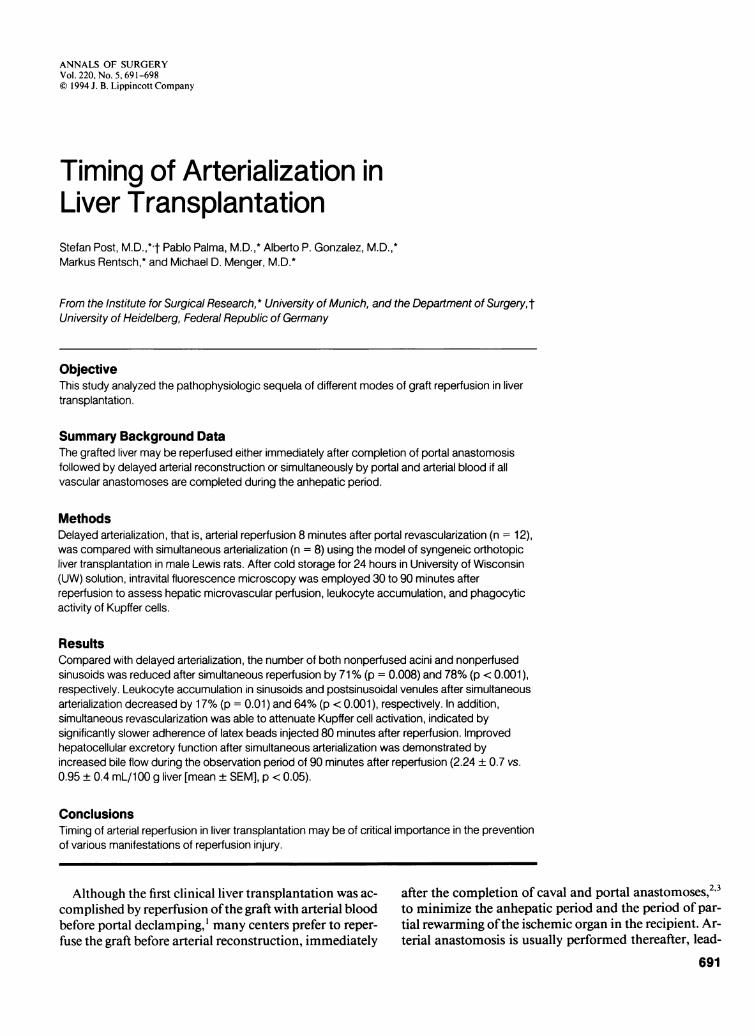
Figure 1. Direct visualization of terminal arterial blood supply. Intravitalfluorescence microscopy of a liver graft 91 min after reperfusion (DA-group). "P" denotes a terminal portal venule, "V" a postsinusoidal venule;arrows indicate direction of blood flow in portal venule; tiny bright whitespots represent phagocytosed fluorescence labeled latex beads. Pho-tograph in (A) was taken a few seconds after intravenous injection of abolus of sodium fluorecein, at the moment when the dye appears in he-patic arterioles (bright white staining) on the surface of the liver but stainingof portal microvessels has not yet occured. (B) shows the identical area14 seconds later, after uptake of the fluorescent compound by hepato-cytes. Note the inhomogeneous supply of arterial blood to the acinus ei-ther by direct arteriosinusoidal twigs (asterisk) or arterioportal anastomosis(arrowhead). Bar = 100 ,um.
RESULTS
General Data
There was no difference between the experimentalgroups regarding actual cold ischemia time and macro-hemodynamic parameters after reperfusion (Table 1).Because of the performance of all four vascular anasto-
Vol. 220 - No. 5
694 Post and Others
C-
-o
._
a)
0.
CL
0
z
20
151
101
51
0
Whole Acini Sinusoids Sinusoidszone 1 zone 2
Sinusoidszone 3
moses during the anhepatic period in the SA-group, thetime of cross-clamping was extended for 3 /2 minutescompared with DA (p = 0.02). However, in no experi-ment of either group did cross-clamping exceed 25 min-utes, which is generally considered to be the limit that iswell tolerated in rats without portosystemic shunting'.Hepatocellular excretory function was markedly im-
a 350
3002 --- ---.----------- .........
200 -|. ..U)~ ~~~~~- -------
0C1
Sinusoids Sinusoids Sinusoids Postsinus.zone 1 zone 2 zone 3 venules
Cd)
-'
.5
020 =
c._
a)
15 =0.CL0
z
10
5
O
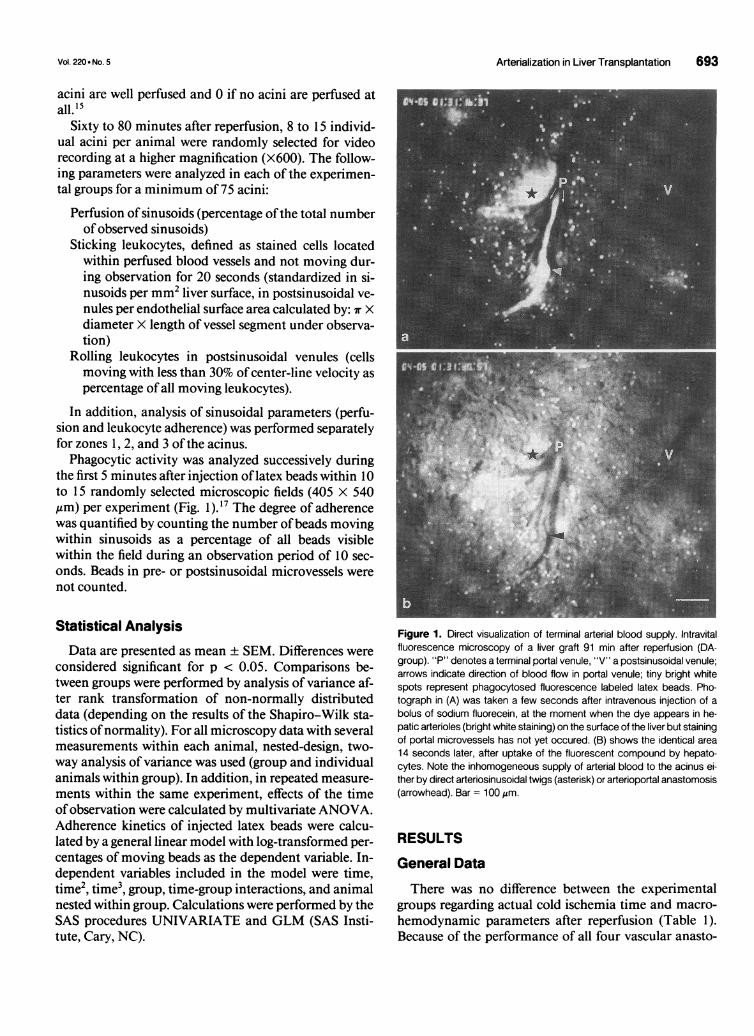
Figure 2. Acinar and sinusoidal per-fusion. Percentage (mean ± SEM) ofnonperfused acini and nonperfusedsinusoids (within perfused acini) afterDA (solid bars) and SA (open bars).There are markedly less microcircu-latory disturbances after SA. *Sig-nificant differences from DA (p <
0.05, nested design two-way AN-OVA).
proved by SA, indicated by total bile flow during the first90 minutes after reperfusion, which was more than twicethe amount secreted after DA (Table 1).
Microvascular PerfusionIn some cases, terminal hepatic arterioles with arterio-
sinusoidal twigs or arterioportal anastomoses could be
700 (D0
600 :'co
0
.0
400 °
E300 E
a)
200
100
0
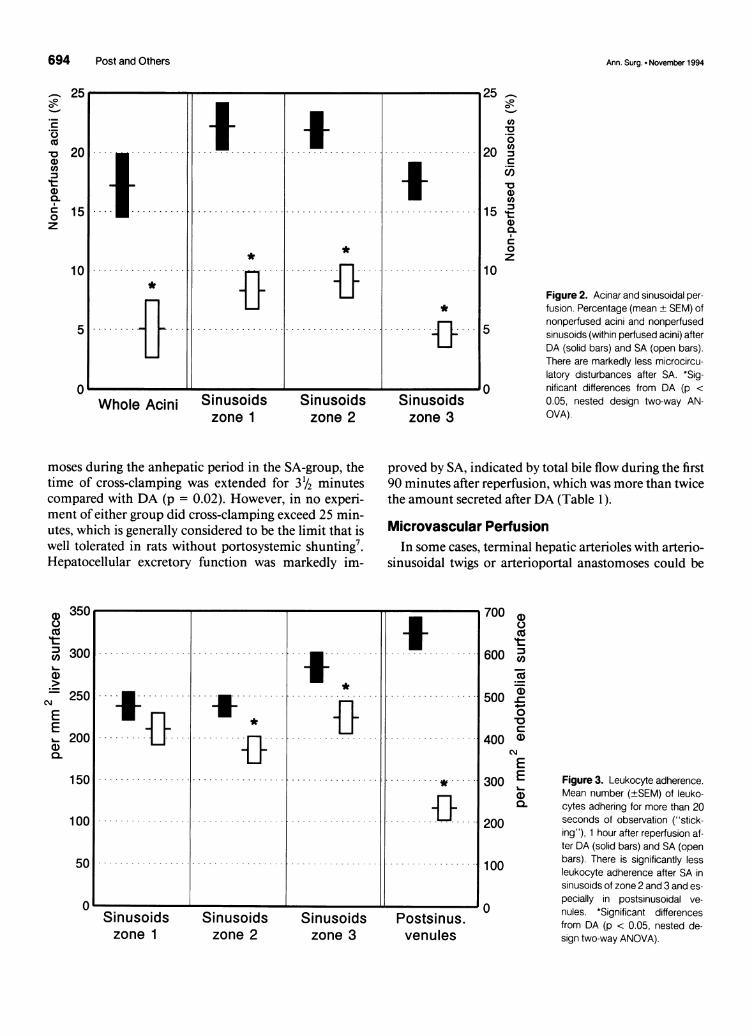
Figure 3. Leukocyte adherence.Mean number (±SEM) of leuko-cytes adhering for more than 20seconds of observation ("stick-ing"), 1 hour after reperfusion af-ter DA (solid bars) and SA (openbars). There is significantly lessleukocyte adherence after SA insinusoids of zone 2 and 3 and es-
pecially in postsinusoidal ve-nules. *Significant differencesfrom DA (p < 0.05, nested de-sign two-way ANOVA).
7r
I1.I.. ..
.... ..................... ........ ............... ...............
l
Ann. Surg. * November 1994
Arterialization in Liver Transplantation 695
100 -
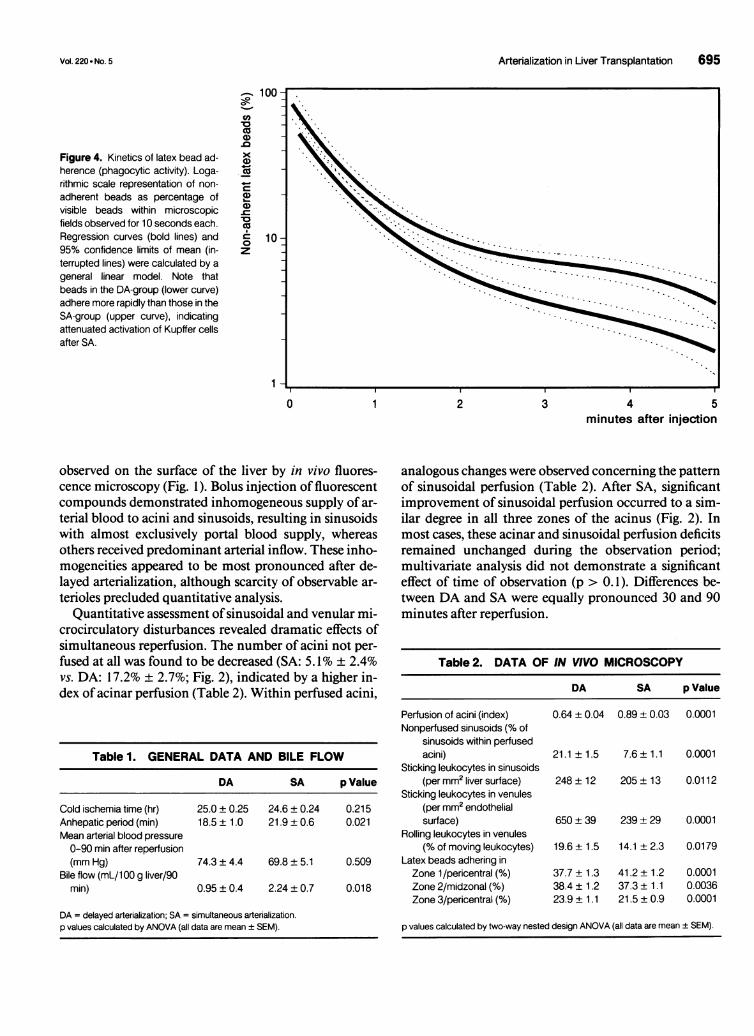
Figure 4. Kinetics of latex bead ad-herence (phagocytic activity). Loga-rithmic scale representation of non-adherent beads as percentage ofvisible beads within microscopicfields observed for 10 seconds each.Regression curves (bold lines) and95% confidence limits of mean (in-terrupted lines) were calculated by ageneral linear model. Note thatbeads in the DA-group (lower curve)adhere more rapidly than those in theSA-group (upper curve), indicatingattenuated activation of Kupffer cellsafter SA.
Cu
a.a10CIO
40.-
co10oz
10 -
1-
4 5minutes after injection
observed on the surface of the liver by in vivo fluores-cence microscopy (Fig. 1). Bolus injection of fluorescentcompounds demonstrated inhomogeneous supply of ar-
terial blood to acini and sinusoids, resulting in sinusoidswith almost exclusively portal blood supply, whereasothers received predominant arterial inflow. These inho-mogeneities appeared to be most pronounced after de-layed arterialization, although scarcity of observable ar-
terioles precluded quantitative analysis.Quantitative assessment ofsinusoidal and venular mi-
crocirculatory disturbances revealed dramatic effects ofsimultaneous reperfusion. The number of acini not per-fused at all was found to be decreased (SA: 5.1% ± 2.4%vs. DA: 17.2% + 2.7%; Fig. 2), indicated by a higher in-dex ofacinar perfusion (Table 2). Within perfused acini,
analogous changes were observed concerning the patternof sinusoidal perfusion (Table 2). After SA, significantimprovement of sinusoidal perfusion occurred to a sim-ilar degree in all three zones of the acinus (Fig. 2). Inmost cases, these acinar and sinusoidal perfusion deficitsremained unchanged during the observation period;multivariate analysis did not demonstrate a significanteffect of time of observation (p > 0. 1). Differences be-tween DA and SA were equally pronounced 30 and 90minutes after reperfusion.
Table 2. DATA OF IN VIVO MICROSCOPY
DA SA p Value
Table 1. GENERAL DATA AND BILE FLOW
DA SA p Value
Cold ischemia time (hr) 25.0 ± 0.25 24.6 ± 0.24 0.215Anhepatic period (min) 18.5 ± 1.0 21.9 ± 0.6 0.021Mean arterial blood pressure0-90 min after reperfusion(mm Hg) 74.3 ± 4.4 69.8 ± 5.1 0.509
Bile flow (mL/1 00 g liver/90min) 0.95 ± 0.4 2.24 ± 0.7 0.018
DA = delayed arterialization; SA = simultaneous arterialization.p values calculated by ANOVA (all data are mean ± SEM).
Perfusion of acini (index)Nonperfused sinusoids (% of
sinusoids within perfusedacini)
Sticking leukocytes in sinusoids(per mm2 liver surface)
Sticking leukocytes in venules(per mm2 endothelialsurface)
Rolling leukocytes in venules(% of moving leukocytes)
Latex beads adhering inZone 1 /pericentral (%)
Zone 2/midzonal (%)Zone 3/pericentral (%)
0.64 ± 0.04 0.89 ± 0.03 0.0001
21.1 ± 1.5 7.6 ± 1.1 0.0001
248 ± 12 205 ± 13 0.0112
650 ± 39 239 ± 29 0.0001
19.6 ± 1.5 14.1 ± 2.3 0.0179
37.7 ± 1.338.4 ± 1.223.9 ± 1.1
41.2 ± 1.237.3± 1.121.5 ± 0.9
0.00010.00360.0001
p values calculated by two-way nested design ANOVA (all data are mean ± SEM).
0 1 2 3
Vol. 220 - No. 5

696 Post and Others
Leukocyte Adherence
In both experimental groups, considerable accumula-tion of leukocytes was observed within sinusoids of allthree acinar zones and in postsinusoidal venules. Simul-taneous arterialization resulted in a marked decrease ofthe number ofleukocytes adhering for more than 20 sec-onds ("sticking") in postsinusoidal venules 1 hour afterreperfusion. Alterations in sinusoids were less pro-nounced: no change in zone 1 and moderately reducedsticking in zones 2 and 3 (Table 2, Fig. 3). Temporaryinteractions between circulating leukocytes and micro-vascular endothelium were quantified by counting thenumber of rolling white blood cells in postsinusoidal ve-nules as a percentage of all moving leukocytes. Again,this phenomenon was found to be dependent on the tim-ing of arterialization: SA significantly decreased thenumber of rolling cells after 1 hour of reperfusion(Table 2).
Phagocytic Activity
As described previously, 17 rapid intrasinusoidal adher-ence of fluorescence-labeled latex particles was observedafter delayed arterialization (Fig. 4). This adherence wasmarkedly slower after SA, resembling the pattern ob-served previously in normal livers. In addition, SA wasable to change the zonal pattern of adherence of latexbeads (Table 2) toward the steep portocentral intra-aci-nar gradient known from normal, untransplantedorgans. 17
DISCUSSION
These results provide evidence that simple technicalmodifications such as changing the time of arterializa-tion may have profound effects on various manifesta-tions of reperfusion injury in liver transplantation. Eightminutes of exclusively portal reperfusion may be suffi-cient to induce prolonged deterioration of graft micro-circulation and hepatocellular excretory function, ac-companied by enhanced activation of Kupffer cells andadherence of circulating leukocytes. Although the mag-nitude of observed differences may be surprising, it is inaccordance with previous results on the key role of thefirst few minutes ofgraft reperfusion: One and 5 minutesafter reperfusion, a massive intrahepatic release ofpotentmediators may be observed,23 accompanied by morpho-logic signs ofKupffer cell activation as early as 6 minutesafter reperfusion.24 Pharmacologic interventions, such asapplication of rinse solutions (which are rapidly washedout during the first minutes after revascularization) im-mediately before reperfusion, may induce prolonged at-tenuation of reperfusion injury.20'2'25
Interestingly, unlike Carolina rinse, which selectivelyblocks sticking ofleukocytes but not rolling,20'2' simulta-neous arterialization was able to inhibit both rolling andsticking, thus interacting with the first and second step ofleukocyte-endothelial cell interaction.26 Rolling, consid-ered a necessary step before sticking occurs, is mediatedby selectins expressed on activated endothelial cells and/or leukocytes.27 The minor effects ofsimultaneous reper-fusion on adherence in sinusoids, together with markedalterations in postsinusoidal venules, are in accordancewith recent data on differential intrahepatic patterns ofexpression of adhesion molecules.28 Further studies arerequired to elucidate the initial stimuli of leukocyte-en-dothelium activation and their contribution to hepato-cellular injury.2930The present data do not allow definite conclusions on
the primary mechanisms involved in the action ofsimul-taneous arterialization. Interference with Kupffer cell ac-tivation and/or direct microcirculatory effects suggestspossible explanations for the present results. As men-tioned above, Kupffer cell activation with release of va-soactive mediators is observed during the first minutesafter reperfusion.2324 Migrating Kupffer cells may blocksinusoidal flow,3 1activated Kupffer cells are the predom-inant source of reactive oxygen intermediates during theinitial reperfusion period,32 phagocytic Kupffer cell ac-tivity shows an inverse correlation with hepatocellularexcretory function after cold storage,'7 and blockade ofKupffer cells by methyl palmitate improves survival inrat liver transplantation.33 Because phagocytic activity ofKupffer cells was found to be significantly decreased bysimultaneous reperfusion, it may be speculated that indelayed arterialization, decreased oxygenation, or dete-rioration of sinusoidal flow during the period of exclu-sively portal reperfusion induces enhanced activation ofKupffer cells. This may be accompanied by increased ox-idant stress and mediator release, which eventually resultin impaired microcirculation, depressed hepatocellularfunction, and pronounced leukocyte adherence.
In addition, direct microhemodynanic consequencesofdelayed arterialization may contribute to the observeddifferences: The lack of vis a tergo34 during initial reper-fusion, when sinusoids have to be cleared ofhepatocellu-lar blebs and endothelial cells detached during cold stor-age,2435 may be responsible for acinar and subacinar no-
reflow phenomenon,36 particularly in areas receivingpredominantly arterial inflow (Fig. 1). It may be hypoth-esized that because of ensuing local stasis, warm isch-emia, and secondary activation of sinusoidal lining cells,some of these microcirculatory disturbances are nolonger reversible when arterial inflow is restored 8 min-utes later.The continuing controversy on whether to perform ar-
terial anastomosis at all in rats9 may (at least in part) be
Ann. Surg. * November 1994
Vol. 220 - No. 5
explained by unnoticed differences in timing of arterial-ization, which are usually not reported, quantified, orstandardized. The differences observed earlier by ourgroup between delayed arterialization and no arterializa-tion after 17 hours ofcold storage' 5 were less pronouncedthan those found in the present study between delayedand simultaneous arterialization after 24 hours of pres-ervation. In preservation/reperfusion studies, prolongedperiods of exclusively portal reperfusion (>20 minutes)that occur in the case ofhand-sutured arterial anastomo-ses37,38 may abrogate many ofthe advantages ofdual vas-cularization in the rodent model. Because ofthe limit of25 minutes of cross clamping,7 simultaneous arterializa-tion in the rat should be impossible using hand-suturedanastomoses. Steffen's technique of cuff anastomosis,22preferably our modification, or, alternatively, the stenttechnique recently proposed by Gao et al.,'4 may be usedinstead.The present observations were limited to the early re-
perfusion period. Although none of the differences be-tween the experimental groups diminished during theobservation period 30 to 90 minutes after revasculariza-tion, no data are yet available on the long term outcome.Further studies are required to clarify the impact of si-multaneous arterialization versus that of delayed arteri-alization on the prognosis ofthe recipient and graft func-tion days later. However, because early microcirculatorydisturbances are known to be of prognostic signifi-cance,39 it may be advantageous in clinical liver trans-plantation to reperfuse the graft only after completion ofall vascular anastomoses.
References
1. Starzl TE, Marchioro TL, von Kaulla KH, et al. Homotransplan-tation ofthe liver in humans. Surg Gynecol Obstet 1963; 117:659-676.
2. Caine RY. Recipient operation. In Calne RY, ed. Liver Transplan-tation. 2nd ed. London and Orlando: Grune & Stratton, 1987, pp221-246.
3. Stieber AC, Makowka L, Starzl TE. Orthotopic liver transplanta-tion. In Starzl TE, Shapiro R, Simmons RL, eds. Atlas of OrganTransplantation. New York and London: Gower Medical Pub,1992, pp 7.1-7.51.
4. Kakizoe S, Yanaga K, Starzl TE, Demetris AJ. Evaluation of pro-tocol before transplantation and after reperfusion biopsies fromhuman orthotopic liver allografts: considerations of preservationand early immunological injury. Hepatology 1990; 11:932-941.
5. Neuhaus P, Brolsch CE, Ringe B, Pichlmayr R. Experimental livertransplantation. In Gips CH, Krom RAF, eds. Progress in LiverTransplantation. Boston: Martinus NijhoffPub, 1985, pp 13-22.
6. Zimmermann FA, Butcher GW, Davies HS, et al. Techniques oforthotopic liver-transplantation in the rat and some studies of theimmunologic response to fully allogeneic liver grafts. TransplantProc 1979; 11:571-582.
7. Kamada N, Calne RY. A surgical experience with five hundredthirty liver transplants in the rat. Surgery 1983; 93:64-69.
Arterialization in Liver Transplantation 697
8. Yu W, Coddington D, Bitter-Suermann H. Rat liver preservation.I. the components ofUW solution that are essential to its success.Transplantation 1990; 49:1060-1066.
9. Kamada N, Sumimoto R, Kaneda K. The value of hepatic arteryreconstruction as a technique in rat liver transplantation. Surgery1992; 111: 195-200.
10. Chaland P, Braillon A, Gaudin C, et al. Orthotopic liver transplan-tation with hepatic artery anastomoses: hemodynamics and re-sponse to hemorrhage in conscious rats. Transplantation 1990; 49:675-678.
11. Zhao D, Wheatley AM. Orthotopic liver transplantation in the rat:comparison of models with and without rearterialization of thegraft. Eur Surg Res 1993; 25:294-302.
12. Engemann R, Ulrichs K, Thiede A, et al. Value of a physiologicalliver transplant model in rats. Transplantation 1982; 33:566-568.
13. Zhao D, Zimmermann A, Wheatley AM. Morphometry of theliver after liver transplantation in the rat: significance of an intactarterial supply. Hepatology 1993; 17:310-317.
14. Gao W, Lemasters JJ, Thurman RG. Development of a newmethod for hepatic rearterialization in rat orthotopic liver trans-plantation. Transplantation 1993; 56:19-24.
15. Post S, Menger MD, Rentsch M, et al. The impact ofarterializationon hepatic microcirculation and leukocyte accumulation afterliver transplantation in the rat. Transplantation 1992; 54:789-794.
16. Menger MD, Marzi I, Messmer K. In vivo fluorescence microscopyfor quantitative analysis of the hepatic microcirculation in ham-sters and rats. Eur Surg Res 1991; 23:158-169.
17. Post S, Gonzalez AP, Palma P, et al. Assessment of hepatic phago-cytic activity by in vivo microscopy after liver transplantation inthe rat. Hepatology 1992; 16:803-809.
18. Post S, Palma P, Rentsch M, et al. Hepatic reperfusion injury fol-lowing cold ischemia in the rat: potentials of quantitative analysisby in vivo fluorescence microscopy. Prog Appl Microcirc 1993; 19:152-166.
19. Palma P, Gonzalez AP, Rentsch M, et al. Bedeutung der simulta-nen arteriellen und portalen reperfusion bei der lebertransplanta-tion. Langenbecks Arch Chir (Suppl Chir Forum) 1993: 249-252.
20. Post S, Rentsch M, Gonzalez AP, et al. Effects of Carolina rinseand adenosine rinse on microvascular perfusion and intrahepaticleukocyte-endothelium interaction after liver transplantation inthe rat. Transplantation 1993; 55:972-977.
21. Post S, Palma P, Rentsch M, et al. Differential impact of Carolinarinse and University of Wisconsin solutions on microcirculation,leukocyte adhesion, Kupffer cell activity, and biliary excretion af-ter liver transplantation. Hepatology 1993; 18:1490-1497.
22. Steffen R, Ferguson DM, Krom RAF. A new method for or-thotopic rat liver transplantation with arterial cuff anastomosis tothe recepient common hepatic artery. Transplantation 1989; 48:166-168.
23. Post S, Goerig M, Otto G, et al. Prostanoid release in experimentalliver transplantation. Transplantation 1990; 49:490-494.
24. Caldwell-Kenkel JC, Currin RT, Tanaka Y, et al. Kupffer cell acti-vation and endothelial cell damage after storage of rat livers: effectsof reperfusion. Hepatology 1991; 13:83-95.
25. Gao W, Takei Y, Marzi I, et al. Carolina rinse solution-a newstrategy to increase survival time after orthotopic liver transplanta-tion in the rat. Transplantation 1991; 52:417-424.
26. Butcher EC. Leukocyte-endothelial cell recognition: three (ormore) steps to specificity and diversity. Cell 1991; 67:1033-1036.
27. Von Andrian UH, Hansell P, Chambers JD, et al. L-selectin func-tion is required for beta 2-integrin-mediated neutrophil adhesionat physiological shear rates in vivo. Am J Physiol 1992; 263:H 1034-H 1044.
28. SteinhoffG, Behrend M, Schrader B, et al. Expression patterns of

698 Post and Others
leukocyte adhesion ligand molecules on human liver endothelia:lack of ELAM-1 and CD62 inducibility on sinusoidal endotheliaand distinct distribution of VCAM-1, ICAM-1, ICAM-2, andLFA-3. Am J Pathol 1993; 142:481-488.
29. Jaeschke H, Bautista AP, Spolarics Z, Spitzer JJ. Superoxide gen-eration by Kupffer cells and priming of neutrophils during reper-fusion after hepatic ischemia. Free Radic Res Commun 1991; 15:277-284.
30. Otto G, Hofheinz H, Hofmann WJ, Manner M. Questionable roleof leukocyte sticking in the pathogenesis of preservation damage.Transplant Proc 1991; 23:85-86.
31. MacPhee PJ, Schmidt EE, Groom AC. Organization and flow inthe liver microcirculation. Prog Appl Microcirc 1993; 19:52-73.
32. Jaeschke H, Farhood A. Neutrophil and Kupffer cell-induced oxi-dant stress and ischemia-reperfusion injury in rat liver. Am J Phys-iol 1991; 260:G355-G362.
33. Marzi I, Cowper K, Takei Y, et al. Methyl palmitate preventsKupffer cell activation and improves survival after orthotopic livertransplantation in the rat. Transpl Int 1991; 4:215-220.
Ann. Surg. * November 1994
34. Rappaport AM, Schneiderman JH. The function of the hepaticartery. Rev Physiol Biochem Pharmacol 1976; 76:129-175.
35. Fratte S, Gendrault JL, Steffan AM, Kirn A. Comparative ultra-structural study of rat livers preserved in Euro-Collins or Univer-sity ofWisconsin solution. Hepatology 1991; 13:1173-1180.
36. Menger MD, Steiner D, Messmer K. Microvascular ischemia-re-perfusion injury in striated muscle: significance of"no reflow". AmJ Physiol 1992; 263:H 1892-H 1900.
37. Lee S, Charters AC III, Chandler JG, Orloff MJ. A technique fororthotopic transplantation in the rat. Transplantation 1973; 16:664-667.
38. Hanisch E, Lemperle S, Jakobi R, et al. Die orthotope Lebertrans-plantation mit arteriellem Wiederanschluss bei der Ratte - eine de-taillierte Beschreibung der Technik und Analyse von Fehlerquel-len. Langenbecks Arch Chir 1993; 378:73-81.
39. Manner M, Schult W, Senninger N, et al. Evaluation of preserva-tion damage after porcine liver transplantation by assessment ofhepatic microcirculation. Transplantation 1990; 50:940-943.





























