Embed Size (px)
Citation preview

THB
TcgpafputpAb
Ka
Aplfy1ccntfbAbAAsfpApuwfC
F
A
R
0d
he Dopamine Transporter and Attention-Deficit/yperactivity Disorder
ertha K. Madras, Gregory M. Miller, and Alan J. Fischman
he high incidence of attention-deficit/hyperactivity disorder (ADHD) and escalating use of ADHD medications present a compellingase for clarifying the pathophysiology of, and developing laboratory or radiologic tests for, ADHD. Currently, the majority of specificenes implicated in ADHD encode components of catecholamine signaling systems. Of these, the dopamine transporter (DAT) is arincipal target of the most widely used antihyperactivity medications (amphetamine and methylphenidate); the DAT gene isssociated with ADHD, and some studies have detected abnormal levels of the DAT in brain striatum of ADHD subjects. Medicationsor ADHD interfere with dopamine transport by brain-region- and drug-specific mechanisms, indirectly activating dopamine- andossibly norepinephrine-receptor subtypes that are implicated in enhancing attention and experiential salience. The most commonlysed DAT-selective ADHD medications raise extracellular dopamine levels in DAT-rich brain regions. In brain regions expressing both
he DAT and the norepinephrine transporter (NET), the relative contributions of dopamine and norepinephrine to ADHDathophysiology and therapeutic response are obfuscated by the capacity of the NET to clear dopamine as well as norepinephrine. Thus,DHD medications targeting DAT or NET might disperse dopamine widely and consign dopamine storage and release to regulationy noradrenergic, as well as dopaminergic neurons.
ey Words: Methylphenidate, atomoxetine, amphetamine, mono-mine transporters, brain imaging, norepinephrine transporter
ttention-deficit/hyperactivity disorder (ADHD) is the mostcommonly diagnosed neuropsychiatric disorder in child-hood. Although ADHD wanes with age, symptoms can
ersist into adolescence and adulthood. Estimates of the preva-ence of ADHD vary widely, with incidence in children rangingrom 3% to �5% (Biederman 1998) but community studiesielding a prevalence range from 1.7% to 16% (Goldman et al998). The diagnosis of ADHD is currently based on DSM-IVriteria, structured interviews or a structured questionnaire. Theore symptoms—impulsivity, inattention, and motor restless-ess—are either reported by patients and/or observed by con-acts of ADHD subjects. Because attentional difficulties arerequently encountered with other psychiatric disorders andrain diseases, under- or overdiagnosis is possible. Accordingly,DHD is diagnosed by exclusion only if social behaviors cannote accounted for by other causes. The inconsistent prevalence ofDHD channels into treatment controversies: particularly, whetherDHD is over- or undertreated. The past decade has seen aignificant increase in prescribed stimulants to treat ADHD,ueled by rising awareness of the disorder, recognition of itsersistence into adulthood, and growing acceptance of anti-DHD medications. Increased prescribing rates magnify theotential for inappropriate prescriptions and diversion for illicitse. Notwithstanding these concerns, ADHD can be comorbidith substance abuse disorders, and treatment reduces the risk
or continued use of illicit substances (Biederman et al 1997;lure et al 1999; Lambert and Hartsough 1998; Wilens 2004).
rom the Department of Psychiatry (BKM, GMM), Harvard Medical School,New England Primate Research Center, Southborough; and the Depart-ment of Radiology (AJF), Massachusetts General Hospital, Boston,Massachusetts.
ddress reprint requests to Correspondence to: Bertha K. Madras, Ph.D.,Chair, Division of Neurochemistry, New England Primate Research Cen-ter, Harvard Medical School, 1 Pine Hill Drive, Southborough, MA 01772-9102; E-mail: [email protected].
eceived July 22, 2004; revised September 29, 2004; accepted October 25,
2004.006-3223/05/$30.00oi:10.1016/j.biopsych.2004.10.011
These considerations provide strong incentives to clarify thepathophysiology of ADHD, associated substance abuse, anddevelop biologically based criteria for diagnosis and treatment.
Biological Basis of ADHD
The biological origins of ADHD are complicated by heterog-enous clinical symptoms, comorbidity (approximately 65%) withother disorders (conduct, mood, bipolar and anxiety disorders,Tourette’s), and exacerbation by adverse environments andpsychosocial events (for overview of ADHD, see Solanto et al2001). Nonetheless, assembled neuroanatomic, genetic, and neu-rophysiologic evidence strongly support a pathophysiologicbasis for ADHD. Abnormal morphology and function of ADHDbrains, detected primarily by magnetic resonance imaging, con-verge on the catecholamine-rich frontal cortex and subcorticalneural networks (Durston 2003; Sowell et al 2003). From adop-tion and twin studies, genetics is estimated to account for morethan 70% of the prevalence (Biederman and Faraone 2002;Faraone, in press). At present, a majority of specific genesimplicated in ADHD encode components of catecholaminesignaling systems and include the dopamine transporter (DAT),norepinephrine transporter (NET), D4 and D5 dopamine recep-tors, dopamine �-hydroxylase, and synaptosomal-associatedprotein-25 (SNAP-25), which facilitates neurotransmitter release(Figure 1), (Faraone, in press; Yang et al 2004). The positivecorrelation of levels of homovanillic acid, a dopamine metabolitein cerebrospinal fluid (CSF), and ADHD symptoms supports theview that excess dopamine in brain might contribute to hyper-activity (Castellanos et al 1996). At a cellular level, catecholamineneurotransmission is implicated in the etiology and therapeuticefficacy of ADHD, with the dopamine and norepinephrinetransporters functioning as principal targets of anti-ADHD drugs.Unfortunately, a survey of all candidate genes in individualADHD subjects has not been conducted systematically, therebyimpeding the development of an integrated model of how thedifferent components might interact. On the basis of the follow-ing lines of evidence, the DAT is one of several lead candidatesfor investigating the pathophysiology of ADHD and anti-ADHDdrug mechanisms: 1) dopamine transport inhibitors indirectlyactivate dopamine receptor subtypes; D4 and D5 dopamine
receptors are implicated in ADHD, and dopamine receptorBIOL PSYCHIATRY 2005;57:1397–1409© 2005 Society of Biological Psychiatry

adtaAb
D
M
cEp(rbtpowmmccidrcpA
T
pffNeaairDsDe(mn
Fa
1398 BIOL PSYCHIATRY 2005;57:1397–1409 B.K. Madras et al
w
ctivity enhances attention and experiential salience and engen-ers stimulation; 2) the DAT is a selective and principal target ofhe most widely used antihyperactivity medications (amphet-mine and methylphenidate); 3) the DAT gene is associated withDHD; and 4) in some studies, abnormal levels of the DAT haveeen detected in brains of ADHD subjects.
This review focuses on the DAT and its relevance to ADHD.
opamine Transporter Function and ADHD
onoamine Neurotransmitter TransportersEffective neuronal communication in the brain requires pre-
ise and dynamic regulation of neurotransmitter concentrations.xtracellular neurotransmitter concentrations are regulated, inart, by monoamine transporters that sequester dopamineDAT), serotonin (SERT), and norepinephrine (NET) into neu-ons. The critical role of monoamine transporters for normalrain function is underscored by the wide range of drugs thatarget monoamine transporters, including medications for de-ression, ADHD, smoking addiction, obsessive-compulsive dis-rder, and sleep disorders. The majority of these drugs interfereith transporter-mediated clearance of extracellular neurotrans-itters. An ensuing surge of extracellular monoamines activatesonoamine receptors and triggers a cascade of molecular and
ellular events to produce therapeutic benefit. Repeated use ofertain transport inhibitors, such as cocaine, can eventually resultn compulsive drug-seeking behavior. All current anti-ADHDrugs modulate dopamine and norepinephrine levels in brainegions expressing DAT and NET, suggesting that aberrantatecholamine signaling might play a significant role in theathophysiology of ADHD and therapeutic response to anti-DHD medications.
he Dopamine Transporter (DAT)At the molecular level, the 12-membrane–spanning DAT
rotein contains a large extracellular loop, with consensus sitesor glycosylation (Figure 2) that function to regulate DAT traf-icking and stability (Li et al 2004). Similarly, glycosylation of theET controls stability, trafficking, and transport activity (Melikiant al 1996). Potential phosphorylation sites (serine, threonine,nd tyrosine) might also acutely modulate DAT trafficking andctivity (for review, see Mortensen and Amara 2003). Dopamines released from both dendrites and axons and might activateeceptors locally or remotely through volume transmission. TheAT limits the duration of synaptic activity and diffusion by
equestering dopamine into neurons (Cragg and Rice 2004). TheAT is present on cell bodies, dendrites, and axons but appar-ntly is not localized in the immediate active zone of the synapseHersch et al 1997; Nirenberg et al 1996). Accordingly, the DATight reduce dopamine overflow into perisynaptic regions but
igure 1. DAT is one of several genes implicated in attention-deficit/hyper-ctivity disorder.
ot robustly sequester dopamine within the synapse.
ww.sobp.org/journal
The DAT is expressed selectively in all dopamine neurons,including those originating in the substantia nigra and ventraltegmental area (Ciliax et al 1995), with neuronal projections tothe striatum, nucleus accumbens, prefrontal cortex, and hypo-thalamus. High densities of DAT-immunoreactive axons wererecently detected in posterior parietal cortex and dentate gyrus ofthe hippocampus, regions not previously thought to receive asubstantial dopamine input (Lewis et al 2001). The relativeconcentrations of dopamine, DAT, and dopamine receptor den-sities are not consistent in all brain regions. In the caudate–putamen, nucleus accumbens, and substantia nigra, the ratio ofthese three components of dopamine signaling are similar, andthe DAT is likely to be a major contributor to dopamine signalingstrength and duration. In other brain regions, the ratio of DAT todopamine receptor expression levels (e.g., prefrontal cortex DATand D4 dopamine receptors) is lower, and this mismatch mightpermit dopamine clearance by metabolism, diffusion, or byanother transporter (De La Garza and Madras 2000). Accordingly,DAT control of dopamine signaling is contingent on its density,activity and regulation, and anatomic juxtaposition to dopaminerelease sites and dopamine receptors, as well as the capacity ofother transporters to sequester dopamine.
The critical and brain-region–specific role of the DAT in regulat-ing dopamine neurotransmission and presynaptic homeostasis isstrikingly borne out by targeted deletion of the DAT gene in mice.In comparison with their wild-type controls, DAT mutant micepresent with significant phenotypic transformations, including hy-peractivity, small size, skeletal abnormalities, pituitary hypoplasia,impaired care by females for their offspring, cognitive and sensori-motor gating deficits, and sleep dysregulation. The striatum of themutant mice adapts by reducing the dopamine-synthesizing en-zyme tyrosine hydroxylase, vesicular dopamine stores, stimulateddopamine release, and D1 and D2 (but not D3) dopamine receptordensities and function (for review, see Gainetdinov and Caron2003). The extreme changes in dopamine-signaling systems of thestriatum are not replicated in the frontal cortex, and indeed, thisbrain region retains normal dopamine systems. In normal brain, thefrontal cortex expresses much lower levels of the DAT and dopa-mine autoreceptors, stores less dopamine, and relies more ondopamine synthesis than on vesicular recycling for dopaminerelease. These contrasting cortical and striatal dopamine regulatoryprocesses have implications for ADHD; in particular, dopamine-signaling parameters (e.g., DAT) in striatum cannot be liberallyextrapolated to frontal cortex.
Beyond functioning as a carrier for dopamine, DAT mediates
Figure 2. Model of DAT protein. The trans-membrane (TM)-spanning hydro-phobic domains are shown as blue cylinders, linked by amino acid chains.Conserved TMs across DAT, NET, and SERT are shown as textured cylinders
(1, 2, 8). DAT, dopamine; NET, norepinephrine; SERT, serotonin.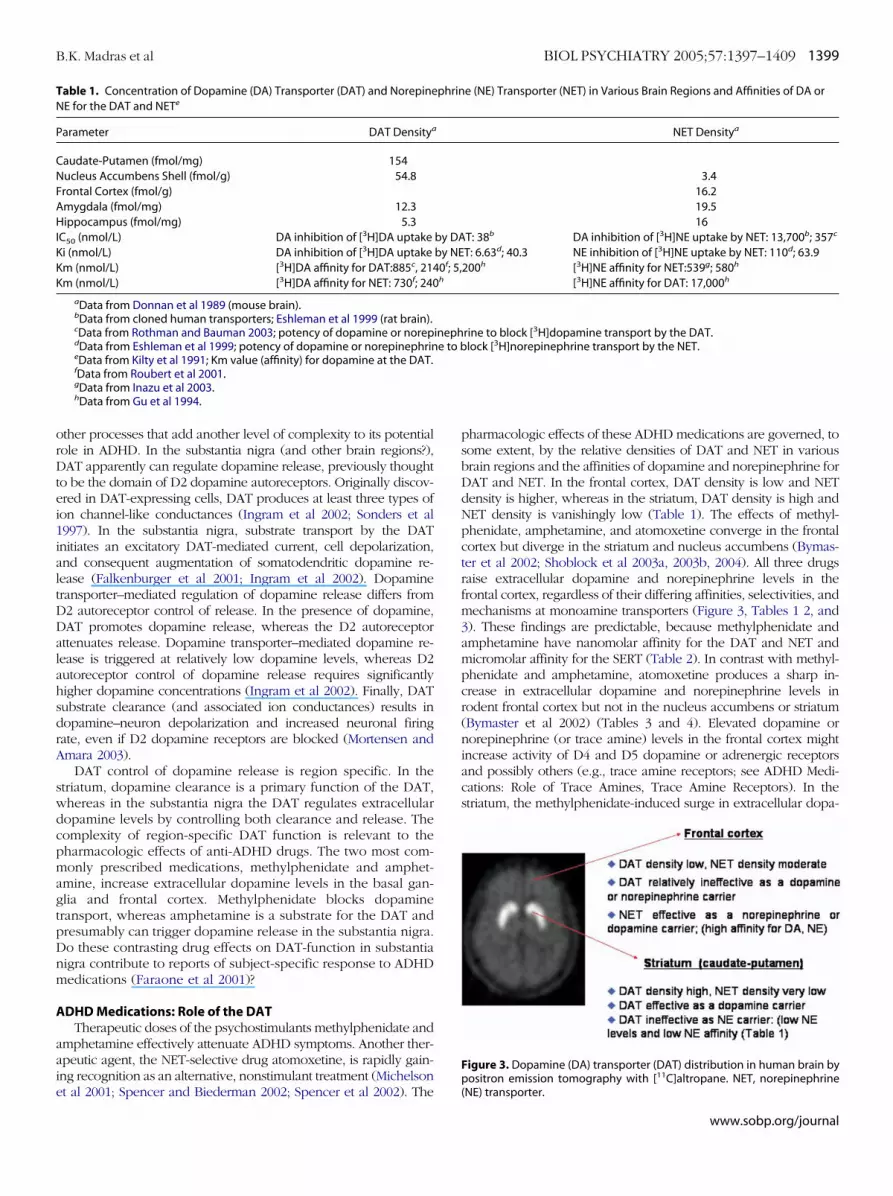
orDtei1ialtDDalahsdrA
swdcpmagtpDnm
A
aaie
TN
P
CNFAHIKKK
B.K. Madras et al BIOL PSYCHIATRY 2005;57:1397–1409 1399
ther processes that add another level of complexity to its potentialole in ADHD. In the substantia nigra (and other brain regions?),AT apparently can regulate dopamine release, previously thought
o be the domain of D2 dopamine autoreceptors. Originally discov-red in DAT-expressing cells, DAT produces at least three types ofon channel-like conductances (Ingram et al 2002; Sonders et al997). In the substantia nigra, substrate transport by the DATnitiates an excitatory DAT-mediated current, cell depolarization,nd consequent augmentation of somatodendritic dopamine re-ease (Falkenburger et al 2001; Ingram et al 2002). Dopamineransporter–mediated regulation of dopamine release differs from2 autoreceptor control of release. In the presence of dopamine,AT promotes dopamine release, whereas the D2 autoreceptorttenuates release. Dopamine transporter–mediated dopamine re-ease is triggered at relatively low dopamine levels, whereas D2utoreceptor control of dopamine release requires significantlyigher dopamine concentrations (Ingram et al 2002). Finally, DATubstrate clearance (and associated ion conductances) results inopamine–neuron depolarization and increased neuronal firingate, even if D2 dopamine receptors are blocked (Mortensen andmara 2003).
DAT control of dopamine release is region specific. In thetriatum, dopamine clearance is a primary function of the DAT,hereas in the substantia nigra the DAT regulates extracellularopamine levels by controlling both clearance and release. Theomplexity of region-specific DAT function is relevant to theharmacologic effects of anti-ADHD drugs. The two most com-only prescribed medications, methylphenidate and amphet-
mine, increase extracellular dopamine levels in the basal gan-lia and frontal cortex. Methylphenidate blocks dopamineransport, whereas amphetamine is a substrate for the DAT andresumably can trigger dopamine release in the substantia nigra.o these contrasting drug effects on DAT-function in substantiaigra contribute to reports of subject-specific response to ADHDedications (Faraone et al 2001)?
DHD Medications: Role of the DATTherapeutic doses of the psychostimulants methylphenidate and
mphetamine effectively attenuate ADHD symptoms. Another ther-peutic agent, the NET-selective drug atomoxetine, is rapidly gain-ng recognition as an alternative, nonstimulant treatment (Michelson
able 1. Concentration of Dopamine (DA) Transporter (DAT) and NorepineE for the DAT and NETe
arameter DAT Densitya
audate-Putamen (fmol/mg) 154ucleus Accumbens Shell (fmol/g) 54.8rontal Cortex (fmol/g)mygdala (fmol/mg) 12.3ippocampus (fmol/mg) 5.3
C50 (nmol/L) DA inhibition of [3H]DA uptakei (nmol/L) DA inhibition of [3H]DA uptakem (nmol/L) [3H]DA affinity for DAT:885c, 214m (nmol/L) [3H]DA affinity for NET: 730f; 240
aData from Donnan et al 1989 (mouse brain).bData from cloned human transporters; Eshleman et al 1999 (rat brain).cData from Rothman and Bauman 2003; potency of dopamine or norepdData from Eshleman et al 1999; potency of dopamine or norepinephrineData from Kilty et al 1991; Km value (affinity) for dopamine at the DAT.fData from Roubert et al 2001.gData from Inazu et al 2003.hData from Gu et al 1994.
t al 2001; Spencer and Biederman 2002; Spencer et al 2002). The
pharmacologic effects of these ADHD medications are governed, tosome extent, by the relative densities of DAT and NET in variousbrain regions and the affinities of dopamine and norepinephrine forDAT and NET. In the frontal cortex, DAT density is low and NETdensity is higher, whereas in the striatum, DAT density is high andNET density is vanishingly low (Table 1). The effects of methyl-phenidate, amphetamine, and atomoxetine converge in the frontalcortex but diverge in the striatum and nucleus accumbens (Bymas-ter et al 2002; Shoblock et al 2003a, 2003b, 2004). All three drugsraise extracellular dopamine and norepinephrine levels in thefrontal cortex, regardless of their differing affinities, selectivities, andmechanisms at monoamine transporters (Figure 3, Tables 1 2, and3). These findings are predictable, because methylphenidate andamphetamine have nanomolar affinity for the DAT and NET andmicromolar affinity for the SERT (Table 2). In contrast with methyl-phenidate and amphetamine, atomoxetine produces a sharp in-crease in extracellular dopamine and norepinephrine levels inrodent frontal cortex but not in the nucleus accumbens or striatum(Bymaster et al 2002) (Tables 3 and 4). Elevated dopamine ornorepinephrine (or trace amine) levels in the frontal cortex mightincrease activity of D4 and D5 dopamine or adrenergic receptorsand possibly others (e.g., trace amine receptors; see ADHD Medi-cations: Role of Trace Amines, Trace Amine Receptors). In thestriatum, the methylphenidate-induced surge in extracellular dopa-
e (NE) Transporter (NET) in Various Brain Regions and Affinities of DA or
NET Densitya
3.416.219.516
T: 38b DA inhibition of [3H]NE uptake by NET: 13,700b; 357c
T: 6.63d; 40.3 NE inhibition of [3H]NE uptake by NET: 110d; 63.9200h [3H]NE affinity for NET:539g; 580h
[3H]NE affinity for DAT: 17,000h
rine to block [3H]dopamine transport by the DAT.lock [3H]norepinephrine transport by the NET.
Figure 3. Dopamine (DA) transporter (DAT) distribution in human brain bypositron emission tomography with [11C]altropane. NET, norepinephrine
phrin
by DAby NE0f; 5,h
inephe to b
(NE) transporter.
www.sobp.org/journal

mpO6abwts
ecarrw2ty
DDteepf2
T
AM
M
dl
A
tieS
1400 BIOL PSYCHIATRY 2005;57:1397–1409 B.K. Madras et al
w
ine levels has been confirmed in living human brain striatum withositron emission tomography (PET) (Volkow et al 2002a, 2002b).ral methylphenidate achieves peak concentrations in the brain0–90 min after administration, blocks more than 50% of the DAT,nd significantly enhances extracellular dopamine levels in theasal ganglia (Volkow et al 2002b). Comparable and essential dataith atomoxetine in human brain have not been reported, reflecting
he need for creative noninvasive imaging approaches to verify thisignificant observation.
On the basis of region-specific differences in pharmacologicffects, ADHD medications that modulate DAT would raise extra-ellular levels of dopamine several-fold, activating autoreceptorsnd possibly reducing catecholamine transmission. The relativelyeduced amplitude of impulse-associated dopamine release couldesult in diminished activation of postsynaptic dopamine receptors,hich drives psychomotor activity (Seeman and Madras 1998,002). The hypothesis is not sustained by electrophysiologic activityhat demonstrates no autoreceptor-preferring dose range of meth-lphenidate or amphetamine (Ruskin et al 2001).
At the cellular level, methylphenidate (100 nmol/L) blocks theAT and increases DAT density 21% after 24-hour exposure in aAT-N2A cell line (Little et al 2002). Although not described in
his report, methylphenidate might also increase cell-surfacexpression of the DAT, in parallel with cocaine under thesexperimental conditions. Because peak blood levels of methyl-henidate range from 18 to 74 nmol/L (low to high doses) andall back to normal within 4–6 hours (Swanson and Volkow003), the in vitro findings might be more relevant to the
Table 3. Methylphenidate, Amphetamine, and AtomoxDopamine or Norepinephrine Levels in Various Regions
Brain Region Neurotransmitter Me
Striatum DopamineNorepinephrine
Prefrontal Cortex DopamineNorepinephrine
Nucleus Accumbens DopamineNorepinephrine
aData from Bymaster et al 2002.
able 2. Affinities of ADHD Medications for DAT, NET, and SERT
DHDedication
DATKi or IC50
(nmol/L)
NETKi or IC50
(nmol/L)
SERTKi or IC50
(nmol/L)
ethylphenidate 1 34a 339a �10,000a
2 200b
-Amphetamine 2 34c; 41d 38.9c; 23.2d 3830c; 11,000d
-Amphetamine 2 138d 30.1d 57,000d
1 1451a 5a 77a
tomoxetine 2 1600e 2.6f 48f
ADHD, attention-deficit/hyperactivity disorder; DAT, dopamine (DA)ransporter; NET, norepinephrine (NE) transporter; SERT, serotonin; 1, bind-ng affinities: DAT: [3H] WIN 35,428; NET: [3H]nisoxetine; SERT: [3H]parox-tine; 2, transport affinities: DAT: [3H]dopamine; NET[3H]norepinephrine;ERT: [3H]serotonin.
aData from Bymaster et al 2002 (human).bData from Hyttel 1978 (rodent).cData from Rothman and Bauman 2003 (rodent).dData from Eshleman et al 1999 (human).eData from Wong et al 1982.fData from Gehlert et al 1995.
bData from Shoblock et al 2003a, 2003b, 2004.
ww.sobp.org/journal
development of tolerance to high and continuous doses, ratherthan to standard doses/dosing regimens. In vivo, DAT imagingdoes not reveal parallel increases in DAT density shortly aftermethylphenidate administration, either because methylpheni-date occupies DAT sites to prevent ligand binding or because ashort burst of methylphenidate exposure at clinically relevantdoses does not lead to DAT upregulation.
Amphetamine modulates dopamine levels with greater com-plexity than methylphenidate. In parallel with methylphenidate,amphetamine robustly raises extracellular dopamine levels in thestriatum, nucleus accumbens, and both dopamine and norepineph-rine in the frontal cortex (Shoblock et al 2003b, 2004) (Table 3). Apotent DAT substrate, amphetamine competes with dopamine forDAT transport and raises extracellular dopamine concentrations byattenuating dopamine transport (Heikkila et al 1975). It also acutelypromotes internalization of the DAT (at comparatively high doses),rendering the DAT inactive in the face of continued dopamineaccumulation (Fleckenstein et al 1999; Saunders et al 2000). Uponentry into neurons via the DAT (or via diffusion), amphetamine issequestered into synaptic vesicles by the vesicular monoaminetransporter (or via diffusion) and promotes release of dopaminefrom vesicles into the cytoplasm (Sulzer and Rayport 1990). Cyto-plasmic dopamine is also increased by amphetamine-mediatedinhibition of monoamine oxidase (Green and el Hait 1978). Thesurge of cytoplasmic dopamine leads to dopamine release viareverse DAT transport (Raiteri et al 1979). Amphetamine alsostimulates release of dopamine by increasing DAT-mediated Ca��influx and ion conductances and promoting dopamine neuronexcitability (Gnegy et al 2004; Ingram et al 2002). Accordingly,amphetamine can raise extracellular dopamine levels by at least sixmechanisms, whereas methylphenidate blocks dopamine transport,can increase DAT density and cell-surface expression with contin-uous exposure, and facilitates sequestration of dopamine by thevesicular monoamine transporter (see ADHD Medications: Role ofthe Vesicular Monoamine Transporter). The contrasting effects ofmethylphenidate and amphetamine are underscored in mice withnull mutations of the DAT. Both methylphenidate and amphet-amine are ineffective in raising dopamine levels in these mice, butthe vesicle-depleting effect of amphetamine is retained (Gainetdi-nov and Caron 2003). Another intriguing distinction between thetwo drugs is their potential influence on the endogenous traceamine system (see ADHD Medications: Role of Trace Amines, TraceAmine Receptors). Amphetamine, but not methylphenidate, acti-vates trace amine receptors, and these divergent responses are ofunknown significance.
ADHD Medications: Role of the NETThe noradrenergic system modulates attention, alertness,
arousal, and vigilance. For the past three decades, proponentshave postulated that dysregulation of noradrenergic systems was
Have Distinct Effects on Extracellular Levels oft Brain, as Measured by Microdialysis
henidatea Amphetamineb Atomoxetinea
rease Increase No effectNo effect
rease Increase Increaserease Increase Increaserease Increase No effect
etineof Ra
thylp
Inc
IncIncInc

ca1aa(pBefn(NmcedDDthtGboTmdrppfdDs
iicDp(omApbst
azabiexo-e
B.K. Madras et al BIOL PSYCHIATRY 2005;57:1397–1409 1401
ritical to the pathophysiology of ADHD and/or mechanisms ofnti-ADHD drugs (Biederman and Spencer 1999; Kornetsky970; Shekim et al 1982; Zametkin and Rappaport 1987). Thedvent of the effective therapeutic drug atomoxetine, with anpproximately 300-fold selectivity for the NET over the DATTable 2), again catapulted NET and noradrenergic systems intorominence for ADHD (Bymaster et al 2002; Spencer andiederman 2002). To complicate the “either-dopamine-or-nor-pinephrine” paradigm, atomoxetine, which has very low affinityor the DAT, raises extracellular dopamine as well as norepi-ephrine levels in rodent frontal cortex (Bymaster et al 2002)Table 3). (Atomoxetine effects are not unique, because theET-selective antidepressant and ADHD medication desipra-ine also raises extracellular dopamine levels in the frontal
ortex [Biederman and Spencer 1999; Carboni et al 1990; Moront al 2002].) Because DAT density in the frontal cortex is low andopamine (DA) uptake proceeds normally in frontal cortex ofAT knockout mice (Table 1), it is unlikely that blockade of theAT is a significant contributor to elevated dopamine levels in
he prefrontal cortex; however, dopamine affinity for the NET isigher compared with its affinity for the DAT, and NET density inhis brain region is higher than DAT density (Eshleman et al 1999;iros et al 1994; Horn 1973; Moron et al 2002) (Table 1). Bylocking the NET, atomoxetine most likely blocks sequestrationf dopamine into norepinephrine neurons (Bymaster et al 2002).o underscore the NET as a dopamine carrier in frontal cortex,ice with null mutations of the NET do not effectively clearopamine in frontal cortex (Moron et al 2002), and amphetamineeportedly releases dopamine from noradrenergic neurons in therefrontal cortex (Shoblock et al 2004). Because the NET isoorly expressed in the striatum and robustly expressed in therontal cortex (Table 1), a selective NET inhibitor can raiseopamine levels in frontal cortex, but not in the striatum. Thus,AT/NET ratios in discrete brain regions are likely to govern
elective drug effects on catecholamine transport.Accordingly, transporter-selective inhibitors are not necessar-
ly transmitter-selective inhibitors, and selectivity of transportnhibitors for blocking transport of a single neurotransmitterannot be predicted solely on the basis of their affinities forA/DAT or norepinephrine (NE)/NET. When viewed from theerspective of promiscuous neurotransmitters and parsimoniousselective) drugs, nonselective transport of catecholamines (orther monoamines?) by monoamine transporters might be aore critical determinant of therapeutic benefit than selectivity ofDHD medications for monoamine transporters. Overall, theharmacologic properties of transport inhibitors are influencedy expression levels of transporters in various brain regions,ubstrate affinities for transporters, as well as localized produc-
Table 4. Dopamin Transporter Imaging in Human SubjCompared with Matched Control Subjects
Study ADHD Subjects
Dougherty et al 1999 6 adults
Barkley 2001 Adult Dresel et al 2000 17 adults
Cheon et al 2003 9 children van Dyck et al 2002 9 adults
TRODAT-1: [2-[[2-[[[3-(4-chlorophenyl)-8-methyl-8-ethy] amino]ethanethiolato-(3-)N2,N2=,S2,S2=] oxo-[1R-(
ion and release of transporter substrates and their diffusion
distance. Accordingly, the relative contributions of dopamine ornorepinephrine to the pathophysiology of ADHD should beconsidered from the perspective of common therapeutic effectsof ADHD medications.
From this vantage, different biochemical scenarios elicited byADHD medications might be necessary or sufficient to alleviateADHD symptoms: 1) increased extracellular dopamine levels inthe frontal cortex, via NET- and/or DAT-modulation are essential,whereas increased norepinephrine levels are superfluous; 2)increased norepinephrine levels in the frontal cortex are essen-tial, whereas increased dopamine levels are superfluous; 3)elevation of both dopamine and norepinephrine levels areessential to activate, in their respective fields, dopaminergic andnoradrenergic receptors; and 4) ADHD medications might reor-ganize dopamine distribution in frontal cortex and other brainregions that express DAT and NET. Clearance of excess dopa-mine by the NET would insert it into noradrenergic neurons;subsequent dopamine release by noradrenergic neurons couldfall under the rubric of noradrenergic regulation. If so, dopamineand norepinephrine might be co-released from noradrenergicneurons (Devoto et al 2004; Shoblock et al 2004) and cross-activate dopamine and noradrenergic receptor subtypes in fron-tal cortical areas. Of relevance to ADHD medications, the NET-selective atomoxetine effectively raises extracellular dopaminelevels in the frontal cortex by blocking the NET, which transportsdopamine efficiently. In the striatum, NET expression levels arevanishingly small, rendering atomoxetine ineffective in this brainregion. Although highly speculative, all current ADHD medica-tions might disperse dopamine throughout the frontal cortex (orother NET-rich regions, such as thalamus, hypothalamus, amgy-dala, mammillary nuclei), eventually leading to dopamine se-questration nonselectively into catecholamine neurons. Underthese conditions, ADHD medications targeting DAT or NETmight disperse dopamine widely and consign dopamine storageand release to regulation by noradrenergic, as well as dopami-nergic neurons, particularly because medications do not fullysaturate transporters. The consequent reorganization of dopa-mine distribution and regulation might be relevant to ADHDpathophysiology and therapeutic effect. For example, will dopa-mine dispersion via the NET permit higher dopamine levels to bein proximity to D4 or D5 dopamine or adrenergic receptors? Totest this hypothesis, it is necessary to compare the therapeuticpotential of compounds that are highly DAT- but not NET-selective with DAT-NET or NET-selective compounds. Neverthe-less, it is premature to craft a comprehensive model of therapeu-tic mechanisms until a systematic study of the effects of ADHDmedications on extracellular monoamine levels in multiple brain
ith Attention-Deficit/Hyperactivity Disorder (ADHD),
Probe Results
[123I]altropane 70% increasep � .001
[123I]altropane 30% increase[99mTc]TRODAT 17% increase
p � .001[123I]IPT �40%–51% increase[123I]CIT No difference
cyclo [3.2.1]oct-2-yl]methyl](2-mercaptoethyl)amino]-xo)]- [99mTc]technetium,[99mTc].
ects w
regions is completed and detailed comparisons are made be-
www.sobp.org/journal

tt
AepphlttsA
AT
isiasiVIad2prTa
AR
(feacdPeEpvci(tUtp(ievmmmu
1402 BIOL PSYCHIATRY 2005;57:1397–1409 B.K. Madras et al
w
ween therapeutic responses elicited by the three major drugherapies.
Drugs acting at the DAT and NET are highly effective inDHD, as summarized by a comprehensive review of thefficacy of ADHD medications (Wilens 2003). Dopamine trans-orter–selective (methylphenidate), DAT/NET-selective (am-hetamine), or NET-selective (atomoxetine) ADHD medicationsave one pharmacologic effect in common: to elevate extracel-ular dopamine and norepinephrine levels in the frontal cortex. Ishis mechanism necessary and sufficient to account for therapeu-ic response, or can other transporters or other DAT and NETubstrates contribute to the pathophysiology of ADHD andDHD therapeutic effects?
DHD Medications: Role of the Vesicular Monoamineransporter
The vesicular monoamine transporter-2 (VMAT-2), located onntracellular vesicular membranes of monoaminergic neurons,equesters cytoplasmic dopamine and norepinephrine into ves-cles, and controls their storage and release. Methylphenidatend amphetamine differentially modulate VMAT-2 function. Aingle administration of methylphenidate rapidly and reversiblyncreases vesicular dopamine transport by the VMAT-2 and raisesMAT-2 densities associated with vesicles (Sandoval et al 2002).n contrast, methamphetamine, a close analogue of amphet-mine, rapidly and reversibly decreases vesicular uptake ofopamine and promotes loss of VMAT-2 function (Brown et al001; Johnson-Davis et al 2004). To summarize, methylphenidateromotes sequestration of dopamine into vesicles for futureelease, whereas amphetamine interferes with dopamine storage.he implications of these contrasting effects of methylphenidatend amphetamine in ADHD are unknown.
DHD Medications: Role of Trace Amines, Trace Amineeceptors
Trace amines are substrates for monoamine transportersMadras et al, unpublished data) and activate a newly clonedamily of trace amine receptors. For more than 20 years, endog-nous trace amines have been implicated in ADHD. The tracemine �-phenethylamine (PEA) is significantly lower in urines ofhildren with ADHD, whereas amphetamine and methylpheni-ate normalize, or boost above normal, concentrations of urinaryEA in boys diagnosed with ADHD, or only in responders (Bakert al 1991; Kusaga et al 2002; Zametkin et al 1983, 1984).ndogenous trace amines are synthesized from amino acidrecursors, stored with biogenic amines in neurons (but not inesicles), released quantally, and affect transport or release ofatecholamines (Branchek and Blackburn 2003). With the clon-ng of trace amine receptor subtypes from human brainBorowsky et al 2001), the barriers to elucidating the relevance ofrace amines and trace amine receptors to ADHD are fading.nexpectedly, amphetamine acts as an agonist in stimulating rat
race amine receptor-1–mediated cyclic adenosine monophos-hate formation at pharmacologically relevant concentrationsBunzow et al 2001; Madras et al, unpublished data). A tantaliz-ng conjecture is that amphetamine might exert therapeuticffects, in part, by activating trace amine receptors. Geneticsariants of these receptors warrant investigation. In contrast,ethylphenidate does not activate the trace amine receptor-1 butight do so indirectly by blocking trace amine transport byonoamine transporters or orphan transporters (Madras et al,
npublished data).ww.sobp.org/journal
ADHD Medications: Comparison of Therapeutic ResponseThe transport inhibitors methylphenidate and atomoxetine
and the transport substrate amphetamine all raise extracellulardopamine and norepinephrine levels in frontal cortex but mightelicit different biochemical responses at monoamine transportersand receptors. Do the two drug categories produce differenttherapeutic outcomes? In an earlier study of 48 boys with ADHD,d-amphetamine, methylphenidate, and placebo were comparedin a double-blind crossover study. Both drugs were highly andequally efficacious for the group as a whole, but frequently onedrug or the other was superior for an individual child, or adverseeffects occurred with only one of the stimulants (Elia et al 1990,1991), highlighting the critical need to incorporate discretecase-by-case drug response and pharmacogenetic data into theanalysis. In a more recent study of methylphenidate, amphet-amine, and placebo to address differences in efficacy of medi-cations, Faraone et al (2001) reported that the efficacy ofamphetamine to improve functioning was seen throughout thefull range of improvement scores, whereas methylphenidateshowed a substantial effect for “mildly” and “much improved”but not for “very much improved.” Both drugs prevented wors-ening of symptoms. Is this reported higher efficacy of amphet-amine attributable to its more complex effects on amine trans-porters than that of methylphenidate? Do pharmacogeneticscontribute to different therapeutic responses? As the clinicaltherapeutic data on atomoxetine matures, will it reveal subtle orsignificant differences compared with more conventional medi-cations? Is high NET-selectivity critical for nonstimulant ADHDmedications, or will a nonselective DAT-NET inhibitor be as ormore effective?
DAT Regulation and Adaptation
Regulation of DAT density and function is of core interest tothe pathophysiology of ADHD and anti-ADHD drug mechanismsand is of potential diagnostic value. Physiologic turnover of theDAT protein in rodent brain is approximately 2–3 days (Kimmelet al 2000), but the DAT is also dynamically regulated. Iongradients, phosphorylation activity, and other agents can modifyDAT activity transiently or for extended periods, even after theagents are cleared from DAT (Gulley and Zahniser 2003;Mortensen and Amara 2003). Adaptive changes are reflected indensity, activity, and cellular localization.
DAT Regulation: Transient EffectsThe DAT can be regulated acutely by a range of physiologic,
pharmacologic, and activity-dependent mechanisms. Under nor-mal conditions, the DAT is trafficked constitutively from the cellmembrane to the intracellular milieu and then degraded orrecycled to the cell surface (Daniels and Amara 1999; Loder andMelikian 2003). Activation of protein kinase C pathways byphorbal esters reduces dopamine transport capacity and thenumber of binding sites on the cell surface (for reviews, seeGulley and Zahniser 2003; Mortensen and Amara 2003). Acuteexposure to substrates or inhibitors can also rapidly and revers-ibly modify DAT function. Of relevance to ADHD medications,amphetamine acutely reduces dopamine transport capacity inrodent brain or cultured cells within 1 hour of administration bypromoting DAT trafficking to the cell interior and internalization(Fleckenstein et al 1999; Saunders et al 2000). Whether thisprocess subsequently alters DAT function is not known, but itmight constitute an important mechanism for raising extracellulardopamine levels. In contrast, the DAT-inhibitor cocaine pro-
duces the opposite effect by promoting upregulation of DAT
ditcN
iD2maa1
ofaItarpmpaseilrtctcp
D
et1lqaki
brpsfdBtdmhoamb
B.K. Madras et al BIOL PSYCHIATRY 2005;57:1397–1409 1403
ensity, function, mobilization of the DAT to the cell surface andncreased cell-surface expression in DAT cell lines, as well as inhe striatum (Daws et al 2002; Little et al 2002). Whether thisocaine–DAT interaction extends to methylphenidate, or to theET, is unknown.Dopamine itself regulates the DAT, directly by downregulat-
ng surface expression, or indirectly by upregulating the DAT via2 dopamine autoreceptors (for review, see Gulley and Zahniser003). If excess extracellular dopamine levels persist after ADHDedications clear, dopamine-mediated DAT regulation could be
mplified. Dopamine transporter function is also regulated byrachidonic acid, ethanol, and nitric oxide (Lonart and Johnson994; Mayfield et al 2001; Zhang and Reith 1996).
The DAT can act as a single unit, self-associate, or bind tother proteins. Oligomers of the DAT exist, but again, theirunctional significance is not known (Sorkina et al 2003; Torres etl 2003). Certain intracellular proteins (PICK1 [Protein1 thatnteracts with C-kinase], �-synuclein) also interact with the DATo stabilize its cell-surface expression (Sidhu et al 2004; Torres etl 2001). In the context of ADHD, the relevance of acute DATegulation by association with substrates, drugs, and otherroteins is unknown. The development of tolerance to ADHDedications is controversial. Intermittently administered methyl-henidate reportedly produces no significant tolerance (Safernd Allen 1989), but tolerance can develop with high doses,teady blood levels, or in individuals (Ross et al 2002; Swansont al 1999, 2003). The development of tolerance to performancen response to a single, high daily dose compared with two,ower daily doses of amphetamine was also postulated in aecent study, but in the absence of a placebo control or subjec-ive reports, the investigators were unwilling to draw firmonclusions (Greenhill et al 2003). Overall, the development ofolerance is likely to depend on dose and whether plasma drugoncentrations are maintained at constant levels over longeriods of time.
AT Regulation: Repeated Exposure to ADHD MedicationsMore than 150 studies have documented the safety and
fficacy of stimulant medications for ADHD, which have beenhe mainstay of treatment for at least 50 years (Spencer et al996). The medications are prescribed for years, yet there isimited information on the neurochemical and behavioral conse-uences of long-term exposure during development. Concernsbout the use of stimulant drugs need to be balanced by theirnown efficacy and the associated social, functional, and behav-oral risks of not treating ADHD.
Do anti-ADHD medications promote neuroadaptation inrain dopamine systems, with consequences to behavior, oresponse to other drugs? Rats chronically exposed to methyl-henidate have altered brain dopamine systems, enhanced sen-itivity to stressful stimuli, decreased response to natural rein-orcers, decreased threshold for helplessness, and increased orecreased cocaine-induced reinforcement (Bolanos et al 2003;randon and Steiner 2003; Carlezon et al 2003). Extrapolation of
hese data to ADHD subjects is limited by differences in dose andosing regimen, the use of normal animals, the context andethod of drug administration, and contradictory findings inuman subjects with ADHD (e.g., Wilens et al 2003), amongther reasons. Investigation of these changes in a naturalistic,lbeit tentative, model of ADHD in nonhuman primates might beore clinically relevant (Goulet et al 2000). Although restricted
y interpretational challenges, preclinical research can providesome guidance for developing clinical research protocols inADHD.
Neuroadaptation in response to drugs can occur at multiplelevels of organization in brain. In cell lines transfected with theDAT or NET, methylphenidate and amphetamine induce expres-sion of the immediate early gene c-fos, implicated in neuroad-aptation (Yatin et al 2002). It is conceivable that DAT regulatesgene expression by triggering a cascade of biochemical events orby enabling access of dopamine to an intracellular receptorsignaling system. A similar, possibly indirect, c-fos response iselicited in rodent striatum after acute exposure to methylpheni-date but declines with repeated dosing (Brandon and Steiner2003; Chase et al 2003). Methylphenidate also directly promotesDAT density downregulation in rodent striatum but not in thenucleus accumbens or substantia nigra (Izenwasser et al 1999;Moll et al 2001). The mechanism underlying the persistent DATdownregulation is unknown but might represent an adaptivedecrease in carrier function to compensate for reduced dopa-mine release. The contrasting adaptive responses in striatum,nucleus accumbens, and substantia nigra might reflect differ-ences in DAT function or regulation in these brain regions: in thestriatum DAT primarily transports dopamine, whereas in thesubstantia nigra DAT promotes dopamine release as well (In-gram et al 2002). Before drawing further inferences from thesefindings, it is necessary to replicate these findings, conductcomparable studies in the nucleus accumbens and prefrontalcortex, and above all, determine whether downregulation occursin human brain.
The ability of therapeutic doses of methylphenidate to pro-duce a sustained decrease in DAT density, even after drugcessation, has not been adequately studied in human subjects.Brain imaging of the DAT in adult striatum after repeatedmethylphenidate administration revealed a decline in DAT den-sity; however, because imaging was conducted 90 min after thelast of three daily doses, it is impossible to distinguish betweenmethylphenidate-mediated DAT occupancy and DAT downregu-lation (Krause et al 2000). In another study, 3–4 months ofmethylphenidate treatment in boys with ADHD resulted in a27%–75% decrease in DAT binding potential (a measure ofdensity). It is unclear whether methylphenidate was withdrawnfor any period before the imaging study, and the apparentreduction might again reflect competition between methylpheni-date and the radioligand probe for DAT binding sites (Vles et al2003). On the basis of these studies, it is not clear whethermethylphenidate changes DAT density in human subjects afterwithdrawal from the drug, and if so, how much time is requiredfor reversal. The effects of repeated, therapeutic doses of am-phetamine on DAT density in living human brain are unknown.
From a clinical vantage, ADHD medications do not seem toinduce neuroadaptative changes that are reflected by robustnontherapeutic behavioral or pharmacologic responses or with-drawal symptoms, except with higher-than-usual doses (Ross et al2002). In contrast to the days or weeks required for antidepres-sant or antipsychotic drug response, methylphenidate has a rapidonset, and the effects are short-lived. ADHD symptoms returnquickly when the drug is cleared and discontinued, and nosignificant tolerance or sensitization is evident in the majority ofsubjects, if given in 2–3 daily doses over extended periods.
DAT Regulation: Brain Imaging of DAT in ADHDIt is important to inquire whether DAT, a principal target of
anti-ADHD drugs in brain, is normal in brains of ADHD subjects.
If not, do abnormal levels reflect a state or trait of the disorder? Itwww.sobp.org/journal

ira(aMei
ApsKaawplpelcth(vTw2tmS1pi
vt1acN2
ctetded
F
1404 BIOL PSYCHIATRY 2005;57:1397–1409 B.K. Madras et al
w
s feasible to visualize and quantify the DAT in living brain byadioligand probes that actively bind the transporter. All currentgents for PET or single-photon emission computed tomographySPECT) imaging of the DAT are based on a phenyltropanenalogue of cocaine (Canfield et al 1990; Fischman et al 2001;adras et al 1989). Although discovered fortuitously, more thanight compounds in this chemical class have been introducednto clinical studies of the DAT (Madras 1998).
In the first study of DAT density in brains of adults withDHD, Dougherty et al (1999) reported increased DAT bindingotential, an index of DAT density (Table 4). The study wasubsequently confirmed in ADHD adults (Dresel et al 2000;rause et al 2000) and ADHD children (Cheon et al 2003), withn important exception (van Dyck et al 2002). Each center useddifferent phenyltropane analogue probe for imaging. Probesith different lipophilic properties might measure different DATopulations if a portion of DAT sites are nonfunctional and
ocalized internally. Divergent results might also reflect differentopulation samples and other experimental parameters. It isssential to verify this potentially significant finding in a mucharger cohort, in multiple centers using similar techniques, and inombination with detailed documentation of presenting symp-oms. Increased DAT densities might not be unique to ADHD;igher densities were reported in a population with depressionBrunswick et al 2003), in normal subjects with higher scores oferbal memory (Mozley et al 2001), and possibly in subjects withourette’s disorder, of which approximately 50% also presentith ADHD symptoms (Malison et al 1995; Muller-Vahl et al000; Singer et al 1991; Stamenkovic et al 2001). Notwithstandinghese unconfirmed reports, DAT density is depleted in theajority of pathologic states examined thus far with PET or
PECT imaging of brain (e.g., Parkinson’s disease; Fischman et al998). If elevated DAT densities in ADHD are confirmed in largeropulations, DAT will present a unique molecular target for
nvestigating the pathophysiology of ADHD.Brain imaging of the NET is also warranted. The long-standing
iew that norepinephrine contributes to ADHD pathology andherapeutic benefit (Biederman and Spencer 1999; Pliszka et al996) was sustained by the discovery of a NET-selective drug,tomoxetine, as an effective medication for ADHD. Atomoxetinelears norepinephrine and dopamine in the frontal cortex via theET (Bymaster et al 2002; Michelson et al 2001; Spencer et al002).
Notwithstanding the need to replicate the findings in a largerohort, the increased levels of the transporter might constitute arait or state of ADHD. If the increase reflects a “trait” of ADHD,levated DAT density might represent “hypertrophy” of dendriticrees or dopaminergic neurons, a result of inadequate pruninguring neurodevelopment. This possibility was raised by Singert al (1991) to account for elevated DAT levels in Tourette’s
igure 4. DAT gene variants.
isorder.
ww.sobp.org/journal
DAT Regulation and Density: The DAT GeneDopamine transporter density might also be altered by genetic
abnormalities, but currently there are no candidate polymorphismsthat correlate with DAT density. The 3=-untranslated region of theDAT gene has a fixed length–repeat sequence, which varies bynumber of repeats from 3 to 11 (Vandenbergh et al 1992) (Figure 4).Although the 10-repeat sequence is the most common form of thegene, inheritance of this repeat length in both alleles is associatedwith ADHD in some studies but accounts for less than 4% of thevariance (Cook et al 1995; Faraone, in press; Madras et al 2002;Waldman et al 1998;). The repeat number in this region of the geneis not clearly associated with DAT density. One study demonstrateda higher DAT density with the 10/10 repeat genotype (Heinz et al2000), another study found a lower density in the 10/10 than in the9/10 repeat (Jacobsen et al 2000), and a third study found nodifference in DAT density (Martinez et al 2001). The variablenumber of tandem repeats (VNTR) region of the DAT gene hasbeen associated with ADHD and methylphenidate response insome studies (Cook et al 1995; Chen et al 2003; Daly et al 1999;Gill et al 1997; Kirley et al 2003; Loo et al 2003; Oh et al 2003; Romanet al 2002; Waldman et al 1998; Winsberg and Comings 1999) butnot in others (Holmes et al 2000; Kahn et al 2003; Palmer et al 1999;Qian et al 2003; Roman et al 2001; Todd et al 2001); Curran et al(2001) reported both association and no association. The polygenicnature of ADHD (Comings et al 1996; reviewed in DiMaio et al 2003;Galili-Weisstub and Segman 2003) suggests that the contribution ofthe DAT gene is limited and might be of greater or lesser influencedepending on the constellation of alleles of other contributinggenes. Whereas discrepancies between association studies mightrelate to the statistical power of individual samples, there is evi-dence that multiple haplotypes of the DAT gene might contain10-repeat VNTR alleles (Barr et al 2001; Miller and Madras 2002;Rubie et al 2001). Because the diversity of DAT alleles might extendbeyond the length of the VNTR region, specific DAT haplotypesmight have differential contributions. A number of studies havedemonstrated that variation of length or of sequence in the 3=-untranslated region of the DAT gene might affect DAT expression(Fuke et al 2001; Inoue-Murayama et al 2002; Michelhaugh et al2001; Mill et al 2002; Miller et al 2002; Miller et al 2001). Becauseparticular alleles of the DAT gene might differentially contribute toaltered levels of DAT protein, it is important to further define andanalyze the function of specific DAT haplotypes and to recognizethat the functional consequence of a particular polymorphism iscontext dependent. Intragenic allelic interactions might distinguishhaplotype functional diversity, and association studies might inad-vertently group haplotypes of different function together on thebasis of VNTR length. Accordingly, there is a need to definehaplotypes on a functional level and group together those haplo-types that share similar function, to clarify the validity of associationstudies and progress toward a fuller understanding of the contribu-tion of the DAT gene to ADHD. Aside from potential mechanisms,overexpression of the DAT might lead to compensatory increases indopamine release, a reduction in extracellular dopamine levels, oraltered cellular distribution of the DAT.
DAT Density Regulation: NeuroadaptationElevated DAT expression might reflect a state, not a trait, of
ADHD and arise from neuroadaptive processes that compensatefor increased (or decreased) neurotransmission mediated bydopamine or other transmitters in brain. One variable notconsidered in the majority of imaging studies was the potentialinfluence of smoking on DAT density. In a comparison of
nonmedicated smoking patients with ADHD with nonsmoking
bps(pf
tlSmobmdttaam
ccrmcderdp
O
Diamt
tandpFprddcrmrIbt
sdmm
B.K. Madras et al BIOL PSYCHIATRY 2005;57:1397–1409 1405
ut medication-naïve adults with ADHD, the smokers subgroupresented with higher clinical scores, yet DAT densities wereignificantly lower than those of the nonsmoking ADHD cohortKrause et al 2003). Notwithstanding these intriguing findings,ostmortem analysis of DAT density in smokers and nonsmokersailed to reveal an association (Court et al 1998).
Elevated DAT density might also reflect an adaptive responseo increased clearance of excess dopamine, mediated by highevels of production and release, altered synaptic activity (e.g.,NAP-25), vesicular storage, or flawed activity of D1–D5 dopa-ine receptor subtypes, or receptor–effector coupling. Severalf these hypotheses are amenable to investigation in living brainy PET imaging (Madras et al 2002). If confirmed in a largeulticenter trial in adults, it is reasonable to investigate DATensity in a broader age range. Childhood ADHD might progresshrough adolescence into adulthood, and the presenting symp-oms, although context dependent, are similar in children anddults. If consistent across studies and ages, this discovery offerslead to investigate the pathophysiology of ADHD and theechanism of anti-ADHD drugs.Elevated DAT density in the striatum might promote excessive
learance of dopamine in this brain region and in the frontalortex (DAT or NET), leading to hypodopaminergic (and norad-energic) tone. Introduction of DAT/NET inhibitors would nor-alize basal dopamine (and noradrenergic) tone in the frontal
ortex to compensate for increased dopamine clearance. Hyper-opaminergic tone in the unmedicated striatum is also a possibletiologic cause of hyperactivity. Testing these postulates willequire monitoring DAT and NET densities and extracellularopamine and norepinephrine levels with greater anatomicrecision than has been done previously.
verview
At present, the most effective medications for ADHD affectAT and NET. From the vantage of medications and pathophys-
ology of ADHD, a unifying mechanism of methylphenidate,mphetamine, and atomoxetine that raises extracellular dopa-ine and norepinephrine in frontal cortex, has broad implica-
ions:First, drug screening procedures should focus not only on
ransporter selectivity and affinity of a candidate therapeutic butlso on the potency of a compound to block transport of variouseurotransmitters by transporters (Madras et al, unpublishedata), with a parallel approach applied to screening of com-ounds at receptors activated by dopamine and norepinephrine.or example, norepinephrine, dopamine, and the trace aminehenylethylamine are effective substrates for the NET, yet theirelative contributions to therapeutic benefit are unknown (Ma-ras et al, unpublished data). Nevertheless, transporter affinityata will not be fully predictive of pharmacologic effects, be-ause brain region–specific transporter expression levels andatios contribute significantly to carrier capacity. For example,ethylphenidate has modest affinity at the NET but effectively
aises dopamine levels in NET-rich and DAT-poor frontal cortex.t is equally important to verify data from rodent brain in primaterain because their relative transporter densities, neurotransmit-er levels, neural projections, and anatomy differ.
Second, the relative advantages of NET-, DAT-, or DAT–NET-elective compounds are not fully understood. Is the surge inopamine in the basal ganglia, mediated by amphetamine andethylphenidate, essential for overall therapeutic efficacy? Ato-
oxetine’s selective blockade of dopamine transport in thefrontal cortex and not in striatum or nucleus accumbens supportsthe need to fully assess ADHD medications with variable activi-ties at the DAT or NET. Is selective DAT blockade essential oraffinity for NET (or SERT) necessary? Reduced potency at theDAT in the basal ganglia could diminish associated stimulanteffects and potential abuse liability. More research is needed withother drugs, with a broad range of pharmacologic effects atmonoamine transporters (e.g., highly selective DAT inhibitors,nonselective DAT and NET inhibitors).
Third, methylphenidate, amphetamine, and atomoxetine allelevate extracellular dopamine and norepinephrine levels in thefrontal cortex but not in striatum or nucleus accumbens. Accord-ingly, for therapeutic response, rectification of catecholaminetone might be more critical in the frontal cortex than in thestriatum. This view is tempered by limited clinical comparisonsof atomoxetine with methylphenidate or amphetamine and ourimperfect knowledge of how the frontal cortex and other brainregions process dopamine and norepinephrine (and possiblytrace amines) in ADHD and subsequent to ADHD medications.
Fourth, in the frontal cortex, the relative contributions ofdopamine and norepinephrine (or their respective transport-ers) to therapeutic response is not known. Atomoxetine orother NET-selective compounds increase extracellular levelsof both norepinephrine and dopamine, indicating that dopa-mine diffuses into the vicinity of noradrenergic neurons atsufficiently high levels to register, by microdialysis, NET-mediated dopamine transport blockade. Because dopaminecan be incorporated into norepinephrine neurons in thefrontal cortex, co-release of both dopamine and norepineph-rine is possible. Although highly speculative, blockade of theNET and DAT by ADHD medications might disperse dopa-mine widely throughout the cortex, activating a range ofcatecholamine receptors for which dopamine has relativelyhigh affinity. Blockade of dopamine transport by DAT andNET might also seed noradrenergic neurons with dopamine asthe transport inhibitor levels decline. Upon release fromnoradrenergic neurons, dopamine could activate both dopa-mine and norepinephrine receptors. Accordingly, dopaminemight function in noradrenergic circuits, at �-adrenergic re-ceptors, and dopamine release in the frontal cortex might beregulated by noradrenergic neuron signaling in the locuscoeruleus, as well as dopaminergic neurons in the ventraltegmental area. It is intriguing to speculate whether dopaminestorage, release, and activation within noradrenergic signalingsystems produces effects divergent from those elicited bynorepinephrine and whether these differences contribute totherapeutic response. Equally interesting is whether dopa-mine tone is deficient in brain regions expressing D4 and D5dopamine receptors and whether these regions are juxtaposedto the NET.
Fifth, differences in the pharmacology of ADHD medica-tions in a region-specific manner might also be relevant totherapeutic response. Comparison of ADHD medication ef-fects in striatum with effects in substantia nigra (or ventraltegmental area, locus coeruleus, hippocampus, amygdala, orother brain regions?) are warranted. In the substantia nigra,amphetamine triggers a different presynaptic physiologic cas-cade than it does in the striatum, whereas there is no evidencethat methylphenidate affects each brain region differently.This difference should be explored in the context of variabletherapeutic response to the two classes of medications.
Sixth, trace amines and their receptors are implicated in
ADHD. It is of fundamental interest: to develop selective com-www.sobp.org/journal

ptrtArts
ib
opsmbbcopiega
ND
biBpL
vBStc
B
B
B
B
B
B
B
B
1406 BIOL PSYCHIATRY 2005;57:1397–1409 B.K. Madras et al
w
ounds for assessing trace amine receptor function; to assess theherapeutic potential of compounds that act at trace amineeceptors and trace amine transporters in models of ADHD; ando genotype trace amine receptor (or transporter) subtypes inDHD subjects. By virtue of the intronless nature of trace amineeceptor genes, receptor structure in brain is likely to be rela-ively constant compared with proteins generated by exonplicing.
Seventh, the DAT interacts with several regulatory proteins,ncluding �-synuclein and PICK, and this association shoulde explored in the context of ADHD and drug response.
In summary, the high incidence of ADHD and escalating usef ADHD medications provide a compelling case to clarify theathophysiology of ADHD and anti-ADHD mechanisms. Thetrong genetic component, proven effectiveness of anti-ADHDedications, morphologic and functional anomalies observed inrains of ADHD subjects are strong indicators that ADHD has aiological basis. The hunt for pathologic processes is compli-ated by the heterogenous clinical symptoms, comorbidity withther disorders, and influence of adverse environments andsychosocial events. Nevertheless, comorbidity and heterogene-
ty in symptoms and response to ADHD medications should bexploited as leads for pathophysiologic mechanisms, pharmaco-enetics, pathophysiogenetics, and drug discovery. (Spencer etl., 1999)
This work was supported by National Institutes of Health–ational Institute on Drug Abuse grants DA06303 (BKM),A15305 (BKM), DA11558 (BKM), and RR00168 (NEPRC).
Boston Life Sciences (Boston) has licensed Altropane forrain imaging of the dopamine transporter. BKM et al have anssued patent on Altropane for dopamine transporter imaging.KM and AJF have a patent application for dopamine trans-orter imaging in ADHD. Both patents are licensed by Bostonife Sciences.
Aspects of this work were presented at the conference “Ad-ancing the Neuroscience of ADHD,” February 28, 2004 inoston, Massachusetts.The conference was sponsored by theociety of Biological Psychiatry through an unrestricted educa-ional grant from McNeil Consumer & Specialty Pharmaceuti-als.
aker GB, Bornstein RA, Rouget AC, Ashton SE, van Muyden JC, Coutts RT(1991): Phenylethylaminergic mechanisms in attention-deficit disorder.Biol Psychiatry 29:15–22.
arkley RA (2001): The ADHD Report Non-archival Newsletter; vol. 9. New York:Guilford Publications.
arr CL, Xu C, Kroft J, Feng Y, Wigg K, Zai G, et al (2001): Haplotype study ofthree polymorphisms at the dopamine transporter locus confirm link-age to attention-deficit/hyperactivity disorder. Biol Psychiatry 49:333–339.
iederman J (1998): Attention-deficit/hyperactivity disorder: A life-span per-spective. J Clin Psychiatry 59(suppl 7):4 –16.
iederman J, Faraone SV (2002): Current concepts on the neurobiology ofAttention-Deficit/Hyperactivity Disorder. J Atten Disord 6(suppl 1):S7–S16.
iederman J, Spencer T (1999): Attention-deficit/hyperactivity disorder(ADHD) as a noradrenergic disorder. Biol Psychiatry 46:1234 –1242.
iederman J, Wilens T, Mick E, Faraone SV, Weber W, Curtis S, et al (1997): IsADHD a risk factor for psychoactive substance use disorders? Findingsfrom a four-year prospective follow-up study. J Am Acad Child AdolescPsychiatry 36:21–29.
olanos CA, Barrot M, Berton O, Wallace-Black D, Nestler EJ (2003): Methyl-phenidate treatment during pre- and periadolescence alters behavioralresponses to emotional stimuli at adulthood. Biol Psychiatry 54:1317–
1329.ww.sobp.org/journal
Borowsky B, Adham N, Jones KA, Raddatz R, Artymyshyn R, Ogozalek KL, et al(2001): Trace amines: Identification of a family of mammalian G protein-coupled receptors. Proc Natl Acad Sci USA 98:8966 – 8971.
Branchek TA, Blackburn TP (2003): Trace amine receptors as targets for noveltherapeutics: Legend, myth and fact. Curr Opin Pharmacol 3:90 –97.
Brandon CL, Steiner H (2003): Repeated methylphenidate treatment in ad-olescent rats alters gene regulation in the striatum. Eur J Neurosci 18:1584 –1592.
Brown JM, Hanson GR, Fleckenstein AE (2001): Regulation of the vesicularmonoamine transporter-2: A novel mechanism for cocaine and otherpsychostimulants. J Pharmacol Exp Ther 296:762–767.
Brunswick DJ, Amsterdam JD, Mozley PD, Newberg A (2003): Greater avail-ability of brain dopamine transporters in major depression shown by[99m c]TRODAT-1 SPECT imaging [erratum in Am J Psychiatry. 2004;161:384]. Am J Psychiatry 160:1836 –1841.
Bunzow JR, Sonders MS, Arttamangkul S, Harrison LM, Zhang G, Quigley DI,et al (2001): Amphetamine, 3,4-methylenedioxymethamphetamine, ly-sergic acid diethylamide, and metabolites of the catecholamine neuro-transmitters are agonists of a rat trace amine receptor. Mol Pharmacol60:1181–1188.
Bymaster FP, Katner JS, Nelson DL, Hemrick-Luecke SK, Threlkeld PG, Heili-genstein JH, et al (2002): Atomoxetine increases extracellular levels ofnorepinephrine and dopamine in prefrontal cortex of rat: A potentialmechanism for efficacy in attention deficit/hyperactivity disorder. Neu-ropsychopharmacology 27:699 –711.
Canfield DR, Spealman RD, Kaufman MJ, Madras BK (1990): Autoradio-graphic localization of cocaine receptors by [3H]CFT in monkey brain.Synapse 5:189 –195.
Carboni E, Tanda GL, Frau R, Di Chiara G (1990): Blockade of the noradrena-line carrier increases extracellular dopamine concentrations in the pre-frontal cortex: Evidence that dopamine is taken up in vivo by noradren-ergic terminals. J Neurochem 55:1067–1070.
Carlezon WA Jr, Mague SD, Andersen SL (2003): Enduring behavioral effectsof early exposure to methylphenidate in rats. Biol Psychiatry 54:1330 –1337.
Castellanos FX, Elia J, Kruesi MJ, Marsh WL, Gulotta CS, Potter WZ, et al (1996):Cerebrospinal fluid homovanillic acid predicts behavioral response tostimulants in 45 boys with attention deficit/hyperactivity disorder. Neu-ropsychopharmacology 14:125–137.
Chase TD, Brown RE, Carrey N, Wilkinson M (2003): Daily methylphenidateadministration attenuates c-fos expression in the striatum of prepuber-tal rats. Neuroreport 14:769 –772.
Chen CK, Chen SL, Mill J, Huang YS, Lin SK, Curran S, et al (2003): Thedopamine transporter gene is associated with attention deficit hyperac-tivity disorder in a Taiwanese sample. Mol Psychiatry 8:393–396.
Cheon KA, Ryu YH, Kim YK, Namkoong K, Kim CH, Lee JD (2003): Dopaminetransporter density in the basal ganglia assessed with [123I]IPT SPET inchildren with attention deficit hyperactivity disorder. Eur J Nucl Med MolImaging 30:306 –311.
Ciliax BJ, Heilman C, Demchyshyn LL, Pristupa ZB, Ince E, Hersch SM, et al(1995): The dopamine transporter: Immunochemical characterizationand localization in brain. J Neurosci 15:1714 –1723.
Clure C, Brady KT, Saladin ME, Johnson D, Waid R, Rittenbury M (1999):Attention-deficit/hyperactivity disorder and substance use: Symptompattern and drug choice. Am J Drug Alcohol Abuse 25:441– 448.
Comings DE, Wu S, Chiu C, Ring RH, Gade R, Ahn C, et al (1996): Polygenicinheritance of Tourette syndrome, stuttering, attention deficit hyperac-tivity, conduct, and oppositional defiant disorder: The additive and sub-tractive effect of the three dopaminergic genes—DRD2, D beta H, andDAT1. Am J Med Genet 67:264 –288.
Cook EH Jr, Stein MA, Krasowski MD, Cox NJ, Olkon DM, Kieffer JE, LeventhalBL (1995): Association of attention-deficit disorder and the dopaminetransporter gene. Am J Hum Genet 56:993–998.
Court JA, Lloyd S, Thomas N, Piggott MA, Marshall EF, Morris CM, et al (1998):Dopamine and nicotinic receptor binding and the levels of dopamineand homovanillic acid in human brain related to tobacco use. Neuro-science 87:63–78.
Cragg SJ, Rice ME (2004): DAncing past the DAT at a DA synapse. TrendsNeurosci 27:270 –277.
Curran S, Mill J, Tahir E, Kent L, Richards S, Gould A, et al (2001): Associationstudy of a dopamine transporter polymorphism and attention deficithyperactivity disorder in UK and Turkish samples. Mol Psychiatry 6:425–
428.
D
D
D
D
D
D
D
D
D
D
E
E
E
F
F
F
F
F
F
G
G
G
B.K. Madras et al BIOL PSYCHIATRY 2005;57:1397–1409 1407
aly G, Hawi Z, Fitzgerald M, Gill M (1999): Mapping susceptibility loci inattention deficit hyperactivity disorder: Preferential transmission of pa-rental alleles at DAT1, DBH and DRD5 to affected children. Mol Psychiatry4:192–196.
aniels GM, Amara SG (1999): Regulated trafficking of the human dopa-mine transporter. Clathrin-mediated internalization and lysosomaldegradation in response to phorbol esters. J Biol Chem 274:35794 –35801.
aws LC, Callaghan PD, Moron JA, Kahlig KM, Shippenberg TS, Javitch JA,Galli A (2002): Cocaine increases dopamine uptake and cell surface ex-pression of dopamine transporters. Biochem Biophys Res Commun 290:1545–1550.
e La Garza R II, Madras BK (2000): [(3)H]PNU-101958, a D(4) dopaminereceptor probe, accumulates in prefrontal cortex and hippocampus ofnon-human primate brain. Synapse 37:232–244.
evoto P, Flore G, Pira L, Longu G, Gessa GL (2004): Alpha2-adrenoceptormediated co-release of dopamine and noradrenaline from noradrener-gic neurons in the cerebral cortex. J Neurochem 88:1003–1009.
iMaio S, Grizenko N, Joober R (2003): Dopamine genes and attention-deficit hyperactivity disorder: A review. J Psychiatry Neurosci 28:27–38.
onnan GA, Kaczmarczyk SJ, McKenzie JS, Kalnins RM, Chilco PJ, Mendel-sohn FA (1989): Catecholamine uptake sites in mouse brain: Distributiondetermined by quantitative [3H]mazindol autoradiography. Brain Res504:64 –71.
ougherty DD, Bonab AA, Spencer TJ, Rauch SL, Madras BK, Fischman AJ(1999): Dopamine transporter density in patients with attention deficithyperactivity disorder. Lancet 354:2132–2133.
resel S, Krause J, Krause KH, LaFougere C, Brinkbaumer K, Kung HF, et al(2000): Attention deficit hyperactivity disorder: Binding of [99mTc]TRO-DAT-1 to the dopamine transporter before and after methylphenidatetreatment. Eur J Nucl Med 27:1518 –1524.
urston S (2003): A review of the biological bases of ADHD: What have welearned from imaging studies? Ment Retard Dev Disabil Res Rev 9:184 –195.
lia J, Borcherding BG, Potter WZ, Mefford IN, Rapoport JL, Keysor CS (1990):Stimulant drug treatment of hyperactivity: Biochemical correlates. ClinPharmacol Ther 48:57– 66.
lia J, Borcherding BG, Rapoport JL, Keysor CS (1991): Methylphenidate anddextroamphetamine treatments of hyperactivity: Are there true nonre-sponders? Psychiatry Research. 36:141–155.
shleman AJ, Carmolli M, Cumbay M, Martens CR, Neve KA, Janowsky A(1999): Characteristics of drug interactions with recombinant biogenicamine transporters expressed in the same cell type. J Pharmacol Exp Ther289:877– 885.
alkenburger BH, Barstow KL, Mintz IM (2001): Dendrodendritic inhibitionthrough reversal of dopamine transport. Science 293:2465–2470.
araone SV, Pliszka SR, Olvera RL, Skolnik R, Biederman J (2001): Efficacy ofAdderall and methylphenidate in attention deficit hyperactivity disor-der: A reanalysis using drug-placebo and drug-drug response curvemethodology. J Child Adolesc Psychopharmacol 11:171–180.
ischman AJ, Bonab AA, Babich JW, Livni E, Alpert NM, Meltzer PC, Madras BK(2001): [11C, 127I]Altropane: A highly selective ligand for PET imaging ofdopamine transporter sites. Synapse 39:332–342.
ischman AJ, Bonab AA, Babich JW, Palmer EP, Alpert NM, Elmaleh DR, et al(1998): Rapid detection of Parkinson’s disease by SPECT with altropane:A selective ligand for dopamine transporters. Synapse 29:128 –141.
leckenstein AE, Haughey HM, Metzger RR, Kokoshka JM, Riddle EL, HansonJE, et al (1999): Differential effects of psychostimulants and relatedagents on dopaminergic and serotonergic transporter function. EurJ Pharmacol 382:45– 49.
uke S, Suo S, Takahashi N, Koike H, Sasagawa N, Ishiura S (2001): The VNTRpolymorphism of the human dopamine transporter (DAT1) gene affectsgene expression. Pharmacogenomics J 1:152–156.
ainetdinov RR, Caron MG (2003): Monoamine transporters: From genes tobehavior. Annu Rev Pharmacol Toxicol 43:261–284.
alili-Weisstub E, Segman RH (2003): Attention deficit and hyperactivitydisorder: Review of genetic association studies. Isr J Psychiatry Relat Sci40:57– 66.
ehlert DR, Schober DA, Hemrick-Luecke SK, Krushinski J, Howbert JJ,Robertson DW, et al (1995): Novel halogenated analogs of tomoxetinethat are potent and selective inhibitors of norepinephrine uptake in
brain. Neurochem Int 26:47–52.Gill M, Daly G, Heron S, Hawi Z, Fitzgerald M (1997): Confirmation of associ-ation between attention deficit hyperactivity disorder and a dopaminetransporter polymorphism. Mol Psychiatry 2:311–313.
Giros B, Wang YM, Suter S, McLeskey SB, Pifl C, Caron MG (1994): Delineationof discrete domains for substrate, cocaine, and tricyclic antidepressantinteractions using chimeric dopamine-norepinephrine transporters.J Biol Chem 269:15985–15988.
Gnegy ME, Khoshbouei H, Berg KA, Javitch JA, Clarke WP, Zhang M, Galli A(2004): Intracellular Ca2� regulates amphetamine-induced dopamineefflux and currents mediated by the human dopamine transporter. MolPharmacol 66:137–143.
Goldman LS, Genel M, Bezman RJ, Slanetz PJ (1998): Diagnosis and treat-ment of attention-deficit/hyperactivity disorder in children and adoles-cents. Council on Scientific Affairs, American Medical Association. JAMA279:1100 –1107.
Goulet M, Mathews P, Madras BK (2000): Chronic methylphenidate treat-ment suppresses activity in more active juvenile monkeys and inducessleep disturbances. Soc Neurosci Abstracts 26:2177.
Green AL, el Hait MA (1978): Inhibition of mouse brain monoamine oxidaseby (�)-amphetamine in vivo. J Pharm Pharmacol 30:262–263.
Greenhill LL, Swanson JM, Steinhoff K, Fried J, Posner K, Lerner M, et al (2003):A pharmacokinetic/pharmacodynamic study comparing a single morn-ing dose of Adderall to twice-daily dosing in children with ADHD. J AmAcad Child Adolesc Psychiatry 42:1234 –1241.
Gu H, Wall SC, Rudnick G (1994): Stable expression of biogenic amine trans-porters reveals differences in inhibitor sensitivity, kinetics, and ion de-pendence. J Biol Chem 269:7124 –7130.
Gulley JM, Zahniser NR (2003): Rapid regulation of dopamine transporterfunction by substrates, blockers and presynaptic receptor ligands. EurJ Pharmacol 479:139 –152.
Heikkila RE, Orlansky H, Cohen G (1975): Studies on the distinction betweenuptake inhibition and release of (3H)dopamine in rat brain tissue slices.Biochem Pharmacol 24:847– 852.
Heinz A, Goldman D, Jones DW, Palmour R, Hommer D, Gorey JG, et al (2000):Genotype influences in vivo dopamine transporter availability in humanstriatum. Neuropsychopharmacology 22:133–139.
Hersch SM, Yi H, Heilman CJ, Edwards RH, Levey AI (1997): Subcellular local-ization and molecular topology of the dopamine transporter in thestriatum and substantia nigra. J Comp Neurol 388:211–227.
Holmes J, Payton A, Barrett JH, Hever T, Fitzpatrick H, Trumper AL, et al(2000): A family-based and case-control association study of the dopa-mine D4 receptor gene and dopamine transporter gene in attentiondeficit hyperactivity disorder. Mol Psychiatr 5:523–530.
Horn AS (1973): Structure-activity relations for the inhibition of catechol-amine uptake into synaptosomes from noradrenaline and dopaminer-gic neurones in rat brain homogenates. Br J Pharmacol 47:332–338.
Hyttel J (1978): Inhibition of [3H]dopamine accumulation in rat striatalsynaptosomes by psychotropic drugs. Biochem Pharmacol 27:1063–1078.
Inazu M, Takeda H, Matsumiya T (2003): Functional expression of the norepi-nephrine transporter in cultured rat astrocytes. J Neurochem 84:136 –144.
Ingram SL, Prasad BM, Amara SG (2002): Dopamine transporter-mediatedconductances increase excitability of midbrain dopamine neurons. NatNeurosci 5:971–978.
Inoue-Murayama M, Adachi S, Mishima N, Mitani H, Takenaka O, Terao K, et al(2002): Variation of variable number of tandem repeat sequences in the3’-untranslated region of primate dopamine transporter genes that af-fects reporter gene expression. Neurosci Lett 334:206 –210.
Izenwasser S, Coy AE, Ladenheim B, Loeloff RJ, Cadet JL, French D (1999):Chronic methylphenidate alters locomotor activity and dopamine trans-porters differently from cocaine. Eur J Pharmacol 373:187–193.
Jacobsen LK, Staley JK, Zoghbi SS, Seibyl JP, Kosten TR, Innis RB, Gelernter J(2000): Prediction of dopamine transporter binding availability by geno-type: A preliminary report. Am J Psychiatry 157:1700 –1703.
Johnson-Davis KL, Truong JG, Fleckenstein AE, Wilkins DG (2004): Alter-ations in vesicular dopamine uptake contribute to tolerance to the neu-rotoxic effects of methamphetamine. J Pharmacol Exp Ther 309:578 –586.
Kahn RS, Khoury J, Nichols WC, Lanphear BP (2003): Role of dopaminetransporter genotype and maternal prenatal smoking in childhood hy-peractive-impulsive, inattentive, and oppositional behaviors. J Pediatr
143:104 –110.www.sobp.org/journal

K
K
K
K
K
K
K
L
L
L
L
L
L
L
M
M
M
M
M
M
M
M
M
1408 BIOL PSYCHIATRY 2005;57:1397–1409 B.K. Madras et al
w
ilty JE, Lorang D, Amara SG (1991): Cloning and expression of a cocaine-sensitive rat dopamine transporter. Science 254:578 –579.
immel HL, Carroll FI, Kuhar MJ (2000): Dopamine transporter synthesis anddegradation rate in rat striatum and nucleus accumbens using RTI-76.Neuropharmacology 39:578 –585.
irley A, Lowe N, Hawi Z, Mullins C, Daly G, Waldman I, et al (2003): Associa-tion of the 480 bp DAT1 allele with methylphenidate response in asample of Irish children with ADHD. Am J Med Genet 121B:50 –54.
ornetsky C (1970): Psychoactive drugs in the immature organism. Psycho-pharmacologia 17:105–136.
rause KH, Dresel SH, Krause J, Kung HF, Tatsch K (2000): Increased striataldopamine transporter in adult patients with attention deficit hyperac-tivity disorder: Effects of methylphenidate as measured by single pho-ton emission computed tomography. Neurosci Lett 285:107–110.
rause KH, Dresel SH, Krause J, la Fougere C, Ackenheil M (2003): The dopa-mine transporter and neuroimaging in attention deficit hyperactivitydisorder. Neurosci Biobehav Rev 27:605– 613.
usaga A, Yamashita Y, Koeda T, Hiratani M, Kaneko M, Yamada S, MatsuishiT (2002): Increased urine phenylethylamine after methylphenidatetreatment in children with ADHD. Ann Neurol 52:372–374.
ambert NM, Hartsough CS (1998): Prospective study of tobacco smokingand substance dependence among samples of ADHD and non-ADHDsubjects. J Learn Disability 31:533–544.
ewis DA, Melchitzky DS, Sesack SR, Whitehead RE, Auh S, Sampson A (2001):Dopamine transporter immunoreactivity in monkey cerebral cortex: Re-gional, laminar, and ultrastructural localization. J Comp Neurol 432:119 –136.
i LB, Chen N, Ramamoorthy S, Chi L, Cui XN, Wang LC, Reith ME (2004): Therole of N-glycosylation in function and surface trafficking of the humandopamine transporter. J Biol Chem 279:21012–21020.
ittle KY, Elmer LW, Zhong H, Scheys JO, Zhang L (2002): Cocaine inductionof dopamine transporter trafficking to the plasma membrane. Mol Phar-macol 61:436 – 445.
oder MK, Melikian HE (2003): The dopamine transporter constitutivelyinternalizes and recycles in a protein kinase C-regulated manner in sta-bly transfected PC12 cell lines. J Biol Chem 278:22168 –22174.
onart G, Johnson KM (1994): Inhibitory effects of nitric oxide on the uptakeof [3H]dopamine and [3H]glutamate by striatal synaptosomes. J Neuro-chem 63:2108 –2117.
oo SK, Specter E, Smolen A, Hopfer C, Teale PD, Reite ML (2003): Functionaleffects of the DAT1 polymorphism on EEG measures in ADHD. J Am AcadChild Adolesc Psychiatry 42:986 –993.
adras, BK (1998): Imaging the dopamine transporter: A window on dopa-mine neurons. In: Marwah J, Teitelbaum H, editors. Advances in Neurode-generative Disorders, volume 1. Scottsdale, Arizona: Prominent Press,229 –253.
adras BK, Miller GM, Fischman AJ (2002): The dopamine transporter: Rele-vance to attention deficit hyperactivity disorder (ADHD). Behav Brain Res130:57– 63.
adras BK, Spealman RD, Fahey MA, Neumeyer JL, Saha JK, Milius RA (1989):Cocaine receptors labeled by [3H]2�-carbomethoxy-3�-(4-fluorophe-nyl)tropane. Mol Pharmacol 36:518 –524.
alison RT, McDougle CJ, van Dyck CH, Scahill L, Baldwin RM, Seibyl JP, et al(1995): [123I]beta-CIT SPECT imaging of striatal dopamine transporterbinding in Tourette’s disorder. Am J Psychiatry 152:1359 –1361.
artinez D, Gelernter J, Abi-Dargham A, van Dyck CH, Kegeles L, Innis RB,Laruelle M (2001): The variable number of tandem repeats polymor-phism of the dopamine transporter gene is not associated with signifi-cant change in dopamine transporter phenotype in humans. Neuropsy-chopharmacology 24:553–560.
ayfield RD, Maiya R, Keller D, Zahniser NR (2001): Ethanol potentiates thefunction of the human dopamine transporter expressed in Xenopusoocytes. J Neurochem 79:1070 –1079.
elikian HE, Ramamoorthy S, Tate CG, Blakely RD (1996): Inability to N-glycosylate the human norepinephrine transporter reduces protein sta-bility, surface trafficking, and transport activity but not ligand recogni-tion. Mol Pharmacol 50:266 –276.
ichelhaugh SK, Fiskerstrand C, Lovejoy E, Bannon MJ, Quinn JP (2001): Thedopamine transporter gene (SLC6A3) variable number of tandem re-peats domain enhances transcription in dopamine neurons. J Neuro-chem 79:1033–1038.
ichelson D, Faries D, Wernicke J, Kelsey D, Kendrick K, Sallee FR, Spencer T
(2001): Atomoxetine ADHD Study Group. Atomoxetine in the treatmentww.sobp.org/journal
of children and adolescents with attention-deficit/hyperactivitydisorder: A randomized, placebo-controlled, dose-response study. Pedi-atrics 108:E83.
Mill J, Asherson P, Browes C, D’Souza U, Craig I (2002); Expression of thedopamine transporter gene is regulated by the 3’ UTR VNTR: Evidencefrom brain and lymphocytes using quantitative RT-PCR. Am J Med Genet114:975–979.
Miller GM, De La Garza RD, Novak MA, Madras BK (2001): Single nucleotidepolymorphisms distinguish multiple dopamine transporter alleles inprimates: Implications for association with attention deficit hyperactiv-ity disorder and other neuropsychiatric disorders. Mol Psychiatry 6:50 –58.
Miller GM, Madras BK (2002): Polymorphisms in the 3’-untranslated region ofhuman and monkey dopamine transporter genes affect reporter geneexpression. Mol Psychiatry 7:44 –55.
Moll GH, Hause S, Ruther E, Rothenberger A, Huether G (2001): Early meth-ylphenidate administration to young rats causes a persistent reductionin the density of striatal dopamine transporters. J Child Adolesc Psycho-pharmacol 11:15–24.
Moron JA, Brockington A, Wise RA, Rocha BA, Hope BT (2002): Dopamineuptake through the norepinephrine transporter in brain regions withlow levels of the dopamine transporter: Evidence from knock-out mouselines. J Neurosci 22:389 –395.
Mortensen OV, Amara SG (2003): Dynamic regulation of the dopaminetransporter. Eur J Pharmacol 479:159 –170.
Mozley LH, Gur RC, Mozley PD, Gur RE (2001): Striatal dopamine transportersand cognitive functioning in healthy men and women. Am J Psychiatry158:1492–1499.
Muller-Vahl KR, Berding G, Brucke T, Kolb H, Meyer GJ, Hundeshagen H, et al(2000): Dopamine transporter binding in Gilles de la Tourette syndrome,J Neurol 247 514 –520.
Nirenberg MJ, Vaughan RA, Uhl GR, Kuhar MJ, Pickel VM (1996): The dopa-mine transporter is localized to dendritic and axonal plasma membranesof nigrostriatal dopaminergic neurons. J Neurosci 16:436 – 447.
Oh KS, Shin DW, Oh GT, Noh KS (2003): Dopamine transporter genotypeinfluences the attention deficit in Korean boys with ADHD. Yonsei Med J44:787–792.
Palmer CG, Bailey JN, Ramsey C, Cantwell D, Sinsheimer JS, Del’HommeM, et al (1999): No evidence of linkage or linkage disequilibrium betweenDAT1 and attention deficit hyperactivity disorder in a large sample.Psychiatr Genet 9:157–160.
Pliszka SR, McCracken JT, Maas JW (1996): Catecholamines in attention-deficit hyperactivity disorder: Current perspectives. J Am Acad Child Ado-lesc Psychiatry 35:264 –272.
Qian Q, Wang Y, Li J, Yang L, Wang B, Zhou R (2003): Association studies ofdopamine D4 receptor gene and dopamine transporter gene polymor-phisms in Han Chinese patients with attention deficit hyperactivity dis-order. Beijing Da Xue Xue Bao 35:412– 418.
Raiteri M, Cerrito F, Cervoni AM, Levi G (1979): Dopamine can be released bytwo mechanisms differentially affected by the dopamine transport in-hibitor nomifensine. J Pharmacol Exp Ther 208:195–202.
Roman T, Schmitz M, Polanczyk G, Eizirik M, Rohde LA, Hutz MH (2001):Attention-deficit hyperactivity disorder: A study of association with boththe dopamine transporter gene and the dopamine D4 receptor gene.Am J Med Genet 105:471– 478.
Roman T, Szobot C, Martins S, Biederman J, Rohde LA, Hutz MH (2002):Dopamine transporter gene and response to methylphenidatein attention-deficit/hyperactivity disorder. Pharmacogenetics 12:497– 499.
Ross DC, Fischhoff J, Davenport B (2002): Treatment of ADHD when toler-ance to methylphenidate develops. Psychiatric Services 53:102.
Rothman RB, Bauman MH (2003): Monoamine transporters and psycho-stimulant drugs. Eur J Pharmacol 479:23–30.
Roubert C, Cox PJ, Bruss M, Hamon M, Bonisch H, Giros B (2001): Determina-tion of residues in the norepinephrine transporter that are critical fortricyclic antidepressant affinity. J Biol Chem 276:8254 – 8260.
Rubie C, Schmidt F, Knapp M, Sprandel J, Wiegand C, Meyer J, et al (2001):The human dopamine transporter gene: The 5’-flanking region revealsfive diallelic polymorphic sites in a Caucasian population sample. Neuro-sci Lett 297:125–128.
Ruskin DN, Bergstrom DA, Shenker A, Freeman LE, Baek D, Walters JR (2001):
Drugs used in the treatment of attention-deficit/hyperactivity disorder
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
B.K. Madras et al BIOL PSYCHIATRY 2005;57:1397–1409 1409
affect postsynaptic firing rate and oscillation without preferentialdopamine autoreceptor action. Biol Psychiatry 49:340 –350.
afer DJ, Allen RP (1989): Absence of tolerance to the behavioral effects ofmethylphenidate in hyperactive and inattentive children. J Pediatr 115:1003–1008.
andoval V, Riddle EL, Hanson GR, Fleckenstein AE (2002): Methylphenidateredistributes vesicular monoamine transporter-2: Role of dopamine re-ceptors. J Neurosci 22:8705– 8710.
aunders C, Ferrer JV, Shi L, Chen J, Merrill G, Lamb ME, et al (2000): Amphet-amine-induced loss of human dopamine transporter activity: An inter-nalization-dependent and cocaine-sensitive mechanism. Proc Natl AcadSci U S A 97:6850 – 6855.
eeman P, Madras B (2002): Methylphenidate elevates resting dopaminewhich lowers the impulse-triggered release of dopamine: A hypothesis.Behav Brain Res 130:79 – 83.
eeman P, Madras BK (1998): Anti-hyperactivity medication: Methylpheni-date and amphetamine. Mol Psychiatry 3:386 –396.
hekim WO, Javaid J, Dekirmenjian H, Chapel JL, Davis JM (1982): Effects ofd-amphetamine on urinary metabolites of dopamine and norepineph-rine in hyperactive boys. Am J Psychiatry 139:485– 488.
hoblock JR, Maisonneuve IM, Glick SD (2003a): Differences betweend-methamphetamine and d-amphetamine in rats: Working memory,tolerance, and extinction. Psychopharmacology (Berl) 170:150 –156.
hoblock JR, Maisonneuve IM, Glick SD (2004): Differential interactions ofdesipramine with amphetamine and methamphetamine: Evidence thatamphetamine releases dopamine from noradrenergic neurons in themedial prefrontal cortex. Neurochem Res 29:1437–1442.
hoblock JR, Sullivan EB, Maisonneuve IM, Glick SD (2003b): Neurochemicaland behavioral differences between d-methamphetamine and d-am-phetamine in rats. Psychopharmacology (Berl) 165:359 –369.
idhu A, Wersinger C, Vernier P (2004): alpha-Synuclein regulation of thedopaminergic transporter: A possible role in the pathogenesis of Parkin-son’s disease. FEBS Lett 565:1–5.
inger HS, Hahn IH, Moran TH (1991): Abnormal dopamine uptake sites inpostmortem striatum from patients with Tourette’s syndrome. Ann Neu-rol 30:558 –562.
olanto MV, Arnsten FT, Castellanos X (2001): Stimulant Drugs and ADHD,Basic and Clinical Neuroscience. New York: Oxford University Press.
onders MS, Zhu SJ, Zahniser NR, Kavanaugh MP, Amara SG (1997): Multipleionic conductances of the human dopamine transporter: The actions ofdopamine and psychostimulants. J Neurosci 17:960 –974.
orkina T, Doolen S, Galperin E, Zahniser NR, Sorkin A (2003 ): Oligomeriza-tion of dopamine transporters visualized in living cells by fluorescenceresonance energy transfer microscopy. J Biol Chem 278:28274 –28283.
owell ER, Thompson PM, Welcome SE, Henkenius AL, Toga AW, Peterson BS(2003): Cortical abnormalities in children and adolescents with atten-tion-deficit hyperactivity disorder. Lancet 362:1699 –1707.
pencer T, Biederman J (2002): Non-stimulant treatment for Attention-deficit/Hyperactivity Disorder. J Atten Disord 6(suppl 1):S109 –S119.
pencer T, Biederman J, Wilens T (1999): Attention-deficit/hyperactivity dis-order and comorbidity. Pediatr Clin North Am 46:915–927.
pencer T, Biederman J, Wilens T, Harding M, O’Donnell D, Griffin S (1996):Pharmacotherapy of attention-deficit hyperactivity disorder across thelife cycle. J Am Acad Child Adolesc Psychiatry 35:409 – 432.
pencer TJ, Biederman J, Wilens TE, Faraone SV (2002): Novel treatments forattention-deficit/hyperactivity disorder in children. J Clin Psychiatry63(suppl 12):16 –22.
tamenkovic M, Schindler SD, Asenbaum S, Neumeister A, Willeit M,Willinger U, et al (2001): No change in striatal dopamine re-uptake sitedensity in psychotropic drug naive and in currently treated Tourette’sdisorder patients: A [(123)I]-beta-CIT SPECT study. Eur Neuropsychophar-macol 11:69 –74.
ulzer D, Rayport S (1990): Amphetamine and other psychostimulants re-duce pH gradients in midbrain dopaminergic neurons and chromaffingranules: A mechanism of action. Neuron 5:797– 808.
wanson J, Gupta S, Guinta D, Flynn D, Alger D, Lerner M, et al (1999): Acutetolerance to methylphenidate in the treatment of attention deficit hy-peractivity disorder in children. Clin Pharmacol Ther 66:295–305.
wanson J, Gupta S, Lam A, Guinta D, Shoulson I, Lerner M, et al (2003):Development of a new once-a-day formulation of methylphenidate
for the treatment of attention-deficit/hyperactivity disorder: Proof-of-concept and proof-of-product. Arch Gen Psychiatry 60:204 –211.Swanson JM, Volkow ND (2003): Serum and brain concentrations of meth-ylphenidate: Implications for use and abuse. Neurosci Biobehav Reviews27:615– 621.
Todd RD, Jong YJ, Lobos EA, Reich W, Heath AC, Neuman RJ (2001): Noassociation of the dopamine transporter gene 3’ VNTR polymorphismwith ADHD subtypes in a population sample of twins. Am J Med Genet105:745–748.
Torres GE, Carneiro A, Seamans K, Fiorentini C, Sweeney A, Yao WD, CaronMG (2003): Oligomerization and trafficking of the human dopaminetransporter. Mutational analysis identifies critical domains importantfor the functional expression of the transporter. J Biol Chem 278:2731–2739.
Torres GE, Yao WD, Mohn AR, Quan H, Kim KM, Levey AI, et al (2001):Functional interaction between monoamine plasma membrane trans-porters and the synaptic PDZ domain-containing protein PICK1. Neuron30:121–134.
Vandenbergh DJ, Persico AM, Uhl GR (1992): A human dopamine trans-porter cDNA predicts reduced glycosylation, displays a novel repetitiveelement and provides racially-dimorphic TaqI RFLPs. Brain Res Mol BrainRes 15:161–166.
van Dyck CH, Quinlan DM, Cretella LM, Staley JK, Malison RT, Baldwin RM, et al(2002): Unaltered dopamine transporter availability in adult attention defi-cit hyperactivity disorder. Am J Psychiatry 159:309–312.
Vles JS, Feron FJ, Hendriksen JG, Jolles J, van Kroonenburgh MJ, Weber WE(2003): Methylphenidate down-regulates the dopamine receptor andtransporter system in children with attention deficit hyperkinetic disor-der (ADHD). Neuropediatrics 34:77– 80.
Volkow ND, Fowler JS, Wang G, Ding Y, Gatley SJ (2002b): Mechanism ofaction of methylphenidate: Insights from PET imaging studies. J AttenDisord 6(suppl 1):S31–S43.
Volkow ND, Wang GJ, Fowler JS, Logan J, Franceschi D, Maynard L, et al(2002a): Relationship between blockade of dopamine transporters byoral methylphenidate and the increases in extracellular dopamine: Ther-apeutic implications. Synapse 43:181–187.
Waldman ID, Rowe DC, Abramowitz A, Kozel ST, Mohr JH, Sherman SL, etal (1998): Association and linkage of the dopamine transporter geneand attention-deficit hyperactivity disorder in children: Heterogene-ity owing to diagnostic subtype and severity. Am J Hum Genet 63:1767–1776.
Wilens TE (2003): Drug therapy for adults with attention-deficit hyperactivitydisorder. Drugs 63:2395–2411.
Wilens TE (2004): Attention-deficit/hyperactivity disorder and the substanceuse disorders: The nature of the relationship, subtypes at risk, and treat-ment issues. Psychiatr Clin North Am 27:283–301.
Wilens TE, Faraone SV, Biederman J, Gunawardene S (2003): Does stimulanttherapy of attention-deficit/hyperactivity disorder beget later substanceabuse? A meta-analytic review of the literature. Pediatrics 111:179–185.
Winsberg BG, Comings DE (1999): Association of the dopamine transportergene (DAT1) with poor methylphenidate response. J Am Acad ChildAdolesc Psychiatry 38:1474 –1477.
Wong DT, Threlkeld PG, Best KL, Bymaster FP (1982): A new inhibitor ofnorepinephrine uptake devoid of affinity for receptors in rat brain.J Pharmacol Exp Ther 222:61–5.
Yang L, Wang, Y-U, Li J, Faraone SV (2004): Association of norepinephrinetransporter gene with methylphenidate response. J Am Acad Child Ado-lesc Psychiatry 43:1154 –1158.
Yatin SM, Miller GM, Norton C, Madras BK (2002): Dopamine transporter-dependent induction of C-Fos in HEK cells. Synapse 45:52– 65.
Zametkin AJ, Brown GL, Karoum F, Rapoport JL, Langer DH, Chuang LW,Wyatt RJ (1983): Urinary phenethylamine response to d-amphetamine in12 boys with attention deficit disorder. Am J Psychiatry 141:1055–1058.
Zametkin AJ, Karoum F, Rapoport JL, Brown GL, Wyatt RJ (1984): Phenyleth-ylamine excretion in attention deficit disorder. J Am Acad Child Psychiatry23:310 –314.
Zametkin AJ, Rapoport JL (1987): Neurobiology of attention deficit disorderwith hyperactivity: Where have we come in 50 years? J Am Acad ChildAdolesc Psychiatry 26:676 – 686.
Zhang L, Reith ME (1996): Regulation of the functional activity of the humandopamine transporter by the arachidonic acid pathway. Eur J Pharmacol
315:345–354.www.sobp.org/journal





























