Embed Size (px)
Citation preview

Tailoring neurophysiological strategies with clinical context enhancesresection and safety and expands indications in gliomas involvingmotor pathways
Lorenzo Bello, Marco Riva, Enrica Fava, Valentina Ferpozzi, Antonella Castellano, Fabio Raneri, Federico Pessina,Alberto Bizzi, Andrea Falini and Gabriella Cerri
Neurosurgical Oncology, Department of Medical Biotechnology and Translational Medicine, Universita degli Studi di Milano, HumanitasClinical and Research Center, Milan, Italy (L.B., M.R., E.F., F.R., F.P.); Laboratory of Motor Control, Department of Medical Biotechnology andTranslational Medicine, University of Milan, Humanitas Clinical and Research Center, Milan, Italy (V.F., G.C.); Scientific Institute andUniversity, Ospedale San Raffaele IRCCS, Neuroradiology, CERMAC, Milan, Italy (A.C., A.F.); Neuroradiology, Humanitas Clinical andResearch Center, Milan, Italy (A.B.)
Corresponding Author: Lorenzo Bello, MD, Neurochirurgia Oncologica, Universita degli Studi di Milano, Department of Medical Biotechnology andTranslational Medicine, Humanitas Clinical and Research Center, Via Manzoni 56, 20089 Rozzano, Milano, Italy ([email protected]).
Background. Resection of motor pathway gliomas requires the intraoperative recognition of essential cortical-subcortical motor struc-tures. The degree of involvement of motor structures is variable, and increases as result of treatments patients are submitted to.Intraoperative neurophysiology offers various stimulation modalities, which efficiency is based on the ability to recognize essentialsites with the highest possible resolution in most clinical conditions. Two stimulation paradigms evolved for intraoperative guidanceof motor tumors removal: the 60 Hz-technique [low frequency (LF)] and the pulse-technique [high frequency-(HF)], delivered by bipolaror monopolar probe respectively. Most surgical teams rely on to either of the 2 techniques. The key point is the integration of the choiceof the stimulation modality with the clinical context.
Methods. In 591 tumors involving the corticospinal tract, the use of HF and LF was tailored to the clinical context defined by patientclinical history and tumor features (by imaging). The effect was evaluated on the feasibility of mapping, the impact on immediate andpermanent morbidity, the extent of resection, and the number of patients treated.
Results. By integrating the choice of the probe and the stimulation protocol with patient clinical history and tumor characteristics, thebest probe-frequency match was identified for the different sets of clinical conditions. This integrative approach allows increasing theextent of resection and patient functional integrity, and greatly expands the number of patients who could benefit from surgery.
Conclusions. The integration of stimulation modalities with clinical context enhances the extent and safety of resection and expandsthe population of patients who could benefit from surgical treatment.
Keywords: brain mapping, extent of resection, gliomas, intraoperative neurophysiology, motor pathways, outcome.
The role of surgery in the treatment of gliomas is crucial for reliev-ing symptoms and determining histological and molecular diag-nosis. The main oncological endpoints for surgery, such asprogression-free survival, overall survival and, in low-grade gli-omas, malignant progression-free survival, greatly depend onthe extent of surgical resection.1 The factors limiting the extentof tumor resection are the highly infiltrative nature of gliomasand their frequent localization in the so-called “eloquent areas,”the areas considered essential in the neural networks underlyingcomplex functions such as sensory-motor, language, or visuo-spatial activities.2 – 4 A lesion of an eloquent area results in a
neurological deficit; therefore, in modern surgery it is mandatorythat maximum tumor resection be accomplished without dam-age to the patient’s functional integrity.3,4 Accordingly, the surgi-cal approach has been changed from the traditional one, whichrelied on anatomical references, to a new one aimed at recogniz-ing the different neural structures based on their functional prop-erties with the aid of intraoperative neurophysiology.4 The mostcritical issue is identifying, with use of the appropriate neuro-physiological techniques during surgery, the eloquent essentialareas to be preserved. To this aim, electrophysiological investiga-tion is supported by preoperative neuroradiological studies to
Received 29 August 2013; accepted 30 November 2013# The Author(s) 2014. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved.For permissions, please e-mail: [email protected].
Neuro-OncologyNeuro-Oncology 16(8), 1110–1128, 2014doi:10.1093/neuonc/not327Advance Access date 4 February 2014
1110
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

provide the surgeon with a high-quality anatomical frame forguiding functional resection.5 This multidisciplinary approachallows the modern neurosurgeon to increase the number ofcases treated by surgery.
Resecting tumors involving the motor pathways is critical, par-ticularly those of the corticospinal system, given their very low de-gree of postoperative plasticity (ie, the ability to transfer theirfunction to another network nearby or distant from the originalnetwork).6 The ability to track functional structures at corticaland subcortical levels, where the surgeon faces systems of fibersof indefinite origin, strictly depends on the protocol of stimulation.Two techniques have been developed to assess the motor path-ways during surgery: the recent “train-of-five” technique (To5)and the traditional 60 Hz technique.7 The To5 technique deliversshort (10–18 millisecond) trains of high-frequency (250–500 Hz)square wave, monophasic pulses with a low-train repetition rate(0.5–2 Hz), while the 60 Hz technique delivers long trains (1–4 s)of biphasic pulses at low frequency (60 Hz). Most surgical teamsrely onto either of the 2 techniques without combining them dur-ing surgery, although an integrative approach may increase theefficiency of mapping. To date, few groups have reported com-parative studies on the different stimulation techniques adoptedfor motor mapping, and no data are available on their clinicalresults.7,8 The key point is integrating the choice of stimulationmodality with the clinical context. Gliomas are highly heteroge-neous tumors, and their degree of heterogeneity increases as aresult of the treatments the patients receive. Regarding tumorswithin the motor pathways, the degree of involvement of the cor-ticospinal tract (CST) is generally quite variable, which determinesthe various spectra of patient clinical history and presentationand influences the level of excitability of the motor pathways atsurgery. This can be predicted by looking at clinical parameterssuch as the history of seizures and their control, the numberand doses of antiepileptic drugs (AEDs), the history of previoustreatments, and the neurological status of the patient. In add-ition, the appearance of the tumor on conventional volumetricfluid-attenuated inversion recovery (FLAIR) images or preopera-tive diffusion tensor imaging (DTI) reconstruction of the CSTmay provide the surgeon with the view of motor pathways in-volvement and represent a useful tool for planning the surgicaland neurophysiological strategy and defining the chance ofresection.5,9
This study reports the data obtained from the combined use ofhigh frequency (HF) and low frequency (LF) for surgical removal ofmany gliomas involving the motor pathways. Our data demon-strate that the combination of the 2 techniques, as tailored tothe clinical context and defined by patient clinical history andtumor features shown by imaging, increases the reliability ofmapping, expands the number of patients who could benefitfrom surgery, optimizes the extent of resection, and decreasespermanent morbidity.
Materials and Methods
Patients
Five-hundred ninety-one patients with gliomas within the motorpathways, operated from 2007 to 2012, were included and gavewritten informed consent for the surgical and mapping proced-ure, which followed the principles outlined in the World Medical
Association Declaration of Helsinki statement on ethical principlesof research involving human subjects. Demographic and clinicalfeatures at admission were documented, and particular attentionwas given to history of seizures (number and duration), numberand doses of AEDs, seizure control, history of previous treatments(surgery, chemotherapy, radiotherapy), and neurological status.Patients underwent preoperative neuropsychological evaluation,baseline MR studies, functional MR imaging (fMRI), and DTI withfiber tractography (DTI-FT). Volumetric scan analysis was used fordefining tumor location and volume.10 Tumor volume was com-puted on volumetric FLAIR MRI scans for low-grade gliomas(LGGs) and on postcontrast T1-weighted MRI scans for high-grade gliomas (HGGs).10 – 12 All patients underwent intraoperativeneurophysiological brain mapping and monitoring. Histology wasclassified according to the WHO brain tumor classification.
Surgical Procedure
A craniotomy, tailored to expose the cortex corresponding to thetumor area and a limited amount of surrounding tissue, was per-formed. Cortical mapping was performed to define the corticalsafe-entry zone. Subcortical brain mapping was then continued,along with tumor resection. For prerolandic tumors located inthe proximity of the CST, resection was started from the posteriorborder where the CST was located and, after its identification, thetract was followed inside the tumor mass. Afterwards, theremaining anterior part of the tumor was removed. Similarly,for parietal tumors, resection was started from the anterior bor-der, following the same principle. For rolandic tumors, the periph-eral functional motor borders were initially located all around thetumor, and then the tumor mass was removed. In all cases, re-section followed the principle of locating the functional motor orlanguage tracts, which represented the limits of resection.
Neurophysiological Brain Monitoring
Neurophysiological monitoring involved simultaneous acquisitionof continuous electroencephalography (EEG), electrocortico-graphy (ECoG), multichannel recording of free-running electro-myographic (EMG) activity, and motor-evoked potentials(MEPs) (Comet-EEG-system, Grass-Astro-Med, ISIS-IOM, andInomedGmbH).
EEG was recorded bilaterally by 2 subdermal needle electrodesin the frontal and postcentral parietal regions of each hemi-sphere, providing 4 bipolar (coupled in 2 longitudinal and 2 trans-versal leads) or/and monopolar (each electrode referred to amidfrontal electrode) derivations. The ongoing EEG signal pro-vided a real-time monitor of the depth of anesthesia and the pos-sible occurrence of seizures involving brain areas distal to thosethat were exposed. EEG was recorded from the beginning of an-esthesia in parallel with ECoG throughout surgery.
ECoG was recorded by a subdural strip electrode with 4–6 con-tacts (Cortical-Strip-Electrode, Integra) in a monopolar array re-ferred to the midfrontal electrode and inserted close to theregion to be mapped. The EcoG signal provided a real-time moni-tor for depth of anesthesia and possible occurrence of after-discharges during stimulation and/or focal seizures throughoutresection. EEG and EcoG signals were filtered (bandpass 1 –100 Hz), displayed with high sensitivity (50– 150 mm/cm and300–500 mm/cm respectively), and recorded.
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1111
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

To monitor the integrity of descending motor pathwaysthroughout the procedure, To5 stimulation was delivered to theprimary motor cortex to elicit MEPs.13,14 To this aim, a 4-contactsubdural strip electrode was placed over the precentral gyrus.Each contact was tested with a vertex reference by stimulationwith trains of 3–5 constant current anodal pulses (pulse duration0.5 –0.8 milliseconds; interstimulus interval [ISI] 2 –4 millise-conds) at 1 Hz. The motor threshold (MT) corresponded to thelowest intensity allowing a reproducible MEP (peak-to-peak amp-litude .0.2 mV) in a distal muscle. The contact showing the low-est MT was chosen for monitoring, and the optimal ISI wasdetermined for every patient. The default pulse duration was0.5 milliseconds, increased to 0.8 milliseconds in patients withhigh MT. The train repetition rate was increased up to 1.5 Hz dur-ing critical phases of surgery (required by the neurosurgeon).MEPs were recorded by pairs of hooked subdermal needle electro-des (Technomed) placed in a muscle-tendon array, and targetmuscles for monitoring were chosen according to cortical expos-ure (in upper limb: extensor digitorum communis, abductor digitiminimi, first dorsal interosseus, abductor pollicis brevis; in lowerlimb: tibialis anterior, triceps surae, flexor hallucis brevis) (for ex-ample see Fig. 2). During surgery, MEPs were continuously moni-tored in asleep and in awake patients and suspended only duringcortical and subcortical mapping to avoid interference. The back-ground muscle activity was also monitored from the very begin-ning of surgery by multiple EMG recordings. Up to 24 muscleswere recorded from the head to the foot contralateral to theoperated brain hemisphere, along with a few recordings on ipsi-lateral muscles. EMG activity was collected, filtered, and displayedby the same equipment used for MEP monitoring (ISIS IOMInomed). Free-running EMG was used to record responses tostimulation and to distinguish between electrical and clinical sei-zures. Electrical seizures are detected on ECoG only; in clinical sei-zures, ECoG alteration is accompanied by ictal muscle activationdetected on free-running EMG.15
Neurophysiological Brain Mapping
Two stimulation techniques were used, low frequency (LF) andhigh frequency (HF), so called according to the frequency ofpulses within the delivered trains.
The LF stimulation consisted in trains lasting from 1 to 4 sec-onds of biphasic square wave pulses (0.5 milliseconds eachphase) at 60 Hz (ISI 16.6 milliseconds) delivered by a constantcurrent stimulator (OSIRIS-NeuroStimulator) integrated into theISIS-System or, in the historical group of patients (Group 2), byan Ojemann-Cortical-Stimulator (Integra) through a bipolarprobe (2 balltips, 2 mm diameter, spaced by 5 mm). For the firsttrial of stimulation in study Group 1, during the mapping at cor-tical level, for the first trial of stimulation, LF was set to an initialintensity of 2 mA, then progressively increased in steps of 0.5 mAuntil a muscle response was clearly detected on the free-runningEMG (cortical Low frequency motor threshold, [cLF-MT]). Duringsubcortical mapping, LF stimulation was either alternated with re-section in a back-and-forth fashion or coupled with resection bykeeping the stimulation probe and instruments used for resectionin the same position. The subcortical stimulation was initially setat the intensity adopted for cortical mapping; in Group 1 only,when a stable motor response was obtained, the intensity wasdecreased to the minimum value needed to evoke an EMG
response (subcortical low frequency motor threshold, [sLF-MT]).LF mapping was considered ineffective in the absence of motorresponse with a stimulus intensity of 15 mA or when electricalor clinical seizures occurred at intensities ,15 mA .
HF stimulation was delivered by a monopolar probe (straighttip, 1.5 mm diameter frontal reference; Inomed) and also by a bi-polar probe in a selected group of patients. HF stimulation wasdelivered according to the same parameters used for the MEPmonitoring procedure (3–5 pulses, pulse duration 0.5–0.8 milli-seconds, ISI 2–4 milliseconds) with anodal polarity for corticalstimulation and cathodal polarity for subcortical stimulation. Atcortical site the current intensity was initially set at the MT usedfor MEPs monitoring, then, during mapping, in each site elicitingmotor responses, the current was adjusted to threshold (MEPpeak-to-peak amplitude ≥ 0.1 mV, cortical high frequencymotor threshold, cHF-MT) in each site eliciting motor responses.This protocol was repeated in all cortical sites of interest. Duringsubcortical mapping, the stimulation -either alternated with re-section or coupled with it- started with the same intensityadopted at cortical level and, when a stable motor responsewas obtained, the intensity was decreased to threshold (subcor-tical high- frequency motor threshold, [sHF-MT]) when a stablemotor response was obtained. In a few patients showing highMTs with anodal stimulation, cathodal polarity allowed a lowerMT for cortical stimulation and was also used for subcorticalmotor mapping. In patients harboring the lesion in the dominanthemisphere, intraoperative language mapping was also per-formed (Supplementary Materials).
Anesthesia
Total intravenous anesthesia was administered with propofol andremifentanil, and no muscle relaxants were employed during sur-gery to permit mapping of motor structures. Close attention waspaid to prevent intraoperative seizures by carefully watching EcoGand free-running EMG. At the first ictal sign, stimulation wasstopped, and cold irrigation was applied, which usually abortedthe seizure. Whenever seizures spread to the whole hemibody,propofol bolus infusion (4 mL on average) was delivered.
Neuroimaging Study
Preoperative MR imaging was performed using a Philips Intera 3Tscanner (Best). Standard MR evaluation for morphological charac-terization of lesions included axial T2-weighted TSE sequence (TR/TE 3000/85 milliseconds; field of view (FOV), 230 mm; 22 slices;section thickness, 5/1-mm gap; matrix, 512×512; SENSE factor,1.5), axial 3D-FLAIR sequence (TR/TE 10 000/110 milliseconds;FOV, 230 mm; 120 slices; section thickness, 1.5/0-mm gap; ma-trix, 224×256; SENSE factor, 2) and postcontrast T1-weighted in-version recovery sequence (TR/TE 2000/10 milliseconds; FOV,230 mm; 22 slices; section thickness, 5/1-mm gap; matrix,400×512; SENSE factor, 1.5). Based on appearance in FLAIRimages, tumor margins were reviewed by 2 experienced neuror-adiologists (A.C. and A.F.) and classified as well defined whensharp borders were visible or diffuse. DTI data were obtained at3T using a single-shot echo planar imaging (EPI) sequence (TR/TE 8986/80 milliseconds; b-value¼ 1 000 s/mm2; 32 diffusiongradients directions; FOV, 240; isotropic acquisition voxel dimen-sions, 2.5×2.5×2.5 mm; acquisition matrix, 96×96; 56 slices, no
Bello et al.: Tailored neurophysiology for motor tumors removal
1112
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

gap; SENSE factor, 2.5). An image set without diffusion weighting,b¼ 0 s/mm2, was also acquired. The data were interpolated inplane to a matrix of 256×256 leading to voxel size of 0.94×0.94×2.5 mm. Two consecutive acquisitions were obtained,and data were realigned and averaged offline to increasesignal-to-noise ratio; thus, total time for DTI was �11 min. Axial3D-FFE T1-weighted imaging (TR 8 milliseconds; TE 4 millise-conds; image resolution equal to DTI) was performed for anatom-ic guidance. Deterministic tractography was performed in allpatients using DTI Studio v2.4.01 software (Jiang H, Mori S, Radi-ology Department, Johns Hopkins University) to obtain maineigenvector and fractional anisotropy (FA) maps. Subcortical con-nections were reconstructed using the fiber assignment by con-tinuous tracking (FACT) method.16– 18 An FA threshold of 0.1 andturning angle .558 were used as criteria to start and stop track-ing.5,9 To reconstruct the component of the CST originating fromM1, a region of interest was placed on an axial section at the levelof subcortical white matter of the precentral gyri; eventual con-taminating fibers were removed. 3D-T1-weighted or 3D-FLAIRimages were coregistered to the mean of all diffusion-weightedimages in order to superimpose white matter tracts on anatom-ical images, allowing comparison of the trajectories of tracts inthe involved hemisphere with those of the contralateral unaffect-ed hemisphere and evaluation of the anatomical relationship be-tween the tract and the tumor mass and the effect exerted by thetumor on the tract of interest. DTI tractography images were sys-tematically reviewed by 2 experienced neuroradiologists (A.C. andA.F.). Tracts were then classified as unchanged, displaced, or infil-trated/disrupted. Unchanged reconstructed tracts showed nor-mal anisotropy, location, and orientation compared withhomologous contralateral tracts. Displaced tracts had normalor only slightly decreased anisotropy and showed abnormal loca-tion or trajectories when compared with those of the contralat-eral unaffected hemisphere. Infiltrated tracts showedsubstantially decreased FA with abnormal hues on directionalcolor maps because infiltrating tumor disrupts the directional or-ganization of fiber tracts and causes altered color patterns on dir-ectional maps. In these cases, DTI tractography reconstructionssuperimposed on morphological series showed that tracts passedthrough the area of altered signal intensity on volumetric
postcontrast T1-weighted or FLAIR images; they may still havea normal location if compared with contralateral unaffectedtracts.5,9 The tractography data were saved in a compatible for-mat (DICOM) using Medx Software (Medical Numerics).5 Allsequences were coregistered offline and made available forintraoperative image guidance through a neuronavigation system(Brainlab). Lesion volumes were computed onto FLAIR volumetricsequences with manual segmentation using I PlanCranial soft-ware suite (BrainLab) by one investigator (M.R.). FLAIR hyperin-tense and T1W-gadolinium-enhanced signal abnormalities wereincluded in the lesion load for LGGs and HGGs, respectively, andwere then reported in cm3.
Postoperative Course
All patients were assessed for motor and language function with-in 1 week and at 1–3 months after surgery to detect acute def-icits (occurring during the first week post surgery) and permanentdeficits (observed at 3 months post surgery). Patients underwentboth an immediate (within 48 h) and a 3-month postoperativeMR scan (volumetric FLAIR and postGdT1-weighted images) toestimate the extent of resection (EOR). EOR corresponded tothe percentage of the volume resected with respect to the pre-operative volume: (preoperative volume-postoperative volume)/preoperative volume.1 The classification was here modified to in-clude in the category of total resections, all the residual signal ab-normalities smaller than 1 cm3 and to account for postoperativeFLAIR changes related to edema and contusion of brain tissuesurrounding the resection cavity due to surgical insult. Therefore,surgical outcome was categorized as (i) total resection (post-operative volume between 0–1 cm3), (ii) subtotal resection (post-operative volume between 1–10 cm3), and (iii) partial resection(postoperative volume .10 cm3).9 Postoperative diffusion-weighted MRI scans were also performed to check for ischemicdamage.
Statistical Analysis
Data were analyzed using Prism 4 for Macintosh (GraphPad Soft-ware). Differences in the extent of resection were studied with the
Table 1. Tumor presentation in the 2 groups
Group 1 (479 patients) Group 2 (112 patients)
Histological diagnosis Low-grade gliomas(348 patients, 72.7%)
174 oligodendrogliomas Low-grade gliomas (75 patients, 67%) 48 oligodendrogliomas/135 astrocytomas 27 astrocytomas39 mixed low-grade gliomas
High-grade gliomasa
(131 patients, 27.3%)67 anaplastic oligodendrogliomas High-grade gliomasa (37 patients, 33%)64 anaplastic astrocytomas
Tumor location 115 rolandic site 32 rolandic site209 precentral site 55 precentral site48 paralimbic site 12 paralimbic site107 postcentral site 13 postcentral site
DTI FT available 389 patients (81.2%) 44 patients (39.3%)
aThese tumors were previously low-grade gliomas that progressed to anaplastic form.Abbreviation: DTI-FT, diffusion tensor imaging with fiber tractography
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1113
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

t test. Differences in percentage of clinical and electrical seizureand patient immediate and permanent deficits, as well as inthe number of patients submitted for surgical treatment werestudied with the Fisher’ exact test.5
Results
Patients
On the basis of the neurophysiological procedure adopted dur-ing surgery, patients were divided into 2 groups. In Group 1(479 patients) LF and HF were available and combined duringmapping with the aid of complete EEG, ECoG, and To5-MEP mon-itoring. In this group of patients, we used the policy of startingmotor mapping with LF being this stimulation modality the old-est and largely used by the neurosurgical community. In thosecases in which LF was found ineffective (absence of a motor re-sponse with a stimulus intensity of 15 mA or when electrical orclinical seizures occurred at intensities ,15 mA ), HF was appliedfor guiding resection. In Group 2, the historical group of the earli-est 112 patients, only LF stimulation was available, and themonitoring setup included only EEG and EcoG without MEP mon-itoring. Group 2 represents the control group to be compared toGroup 1.
Group 1: 479 patients (283 males males and 196 females,aged 17–58 years, median 37.4 years)
On a total of 479 tumors involving the motor pathways, 348(72.7%) were LGGs, and 131 HGGs, progressed from low-gradegliomas to anaplastic form.
Group 2: 112 patients (55 males and 57 females, aged 19–64 years, median 41 years)
Of a total of 112 tumors, 75 (67%) were LGGs, and 37 HGGs, pro-gressed from LGGs.
The detailed histological analysis and tumor location of bothgroups is shown in Table 1.
Intraoperative Neurophysiological Mapping Results:Correlation with Clinical Data
Various subgroups were identified within Group 1 and Group 2,depending on the stimulating protocol adopted for mappingand the related clinical context (clinical history and imaging fea-tures on conventional MR and available DTI images).
Group 1 (combined HF+LF stimulation)
Within Group 1, two subgroups (subgroups A and B), weredistinguished.
Subgroup A In subgroup A (183 cases), the functional mappingwas performed exclusively with LF stimulation (Table 2), whichwas successful in guiding resection at the cortical and subcorticallevels. HF stimulation was used only to acquire data forcomparison.
Clinical features. Patients belonging to this subgroup were charac-terized by a short history of seizures that were well controlled byadministration of 1–2 AEDs (Table 3). On admission, 177 patientswere neurologically intact, and only 6 showed mild motorimpairment.
Table 2. Subdivision of the experimental (group 1) and control (group 2) groups on the basis of mapping procedure
Group 1 (479 patients) Group 2 (112 patients)
Mappingprocedure
Subgroup A: LF; HF only for comparison Exclusively LFSubgroup BI: HF to remove a significant portion of the tumor and
to partially decompress CST; LF only for recognizing fibersbelonging to the CST
Subgroup BII: HF; LF (with HF) to complete the margin ofresection
Subgroup BIII: HFSubgroup BIV: HF (bipolar and monopolar probes)
Number ofpatients
Subgroup A: 183 patients (38.2%) Subgroup A: 68 patients (60.7%)Subgroup B: 296 patients
(61.8%)Subgroup BI: 150 patients
(50.6%)Subgroup B: 44 patients
(30.3%)Subgroup BI: 36 patients
(32.1%)Subgroup BII: 115 patients
(38.8%)Subgroup BIII: 21 patients
(7.2%)Subgroup BII: 8 patients
(7.2%)Subgroup BIV: 10 patients
(3.4%)Language
mapping183 patients 44 patients
Abbreviations: DTI-FT, diffusion tensor imaging with fiber tractography; HF, high frequency; LF, low frequency
Bello et al.: Tailored neurophysiology for motor tumors removal
1114
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

Radiology. The tumors appeared as well-defined masses withsharp borders in FLAIR-weighted MR images. Tumors were loca-lized at rolandic (32), precentral (79), paralimbic (21), and post-central (51) sites. DTI FT reconstruction of the CST, available in155 cases (84.7%), showed an unaffected tract in 22.4% ofcases, a displacement of the tract’s fibers in 39.9%, and displace-ment and limited infiltration of the tract in 37.7% (Table 3).
Histology. One-hundred twenty-six cases were LGGs, and 57 wereHGGs. In 71 cases (38.8%), the tumor was recurrent (57 LGGs re-curred as HGGs).
Mapping procedure. LF cortical mapping was performed at thresh-old intensities (cLF-MT, Methods) ranging from 3 to 9 mA, alwayseffective over the primary motor area (Fig. 1, Panel-B). Subcorticalresection was continued until a threshold intensity (sLF-MT)
ranging 2 to 3 mA was reached and was successful in all cases(Fig. 1, Panel-C).
Seizures. During the procedure, there were 61 (33.3%) electricalseizures and 31 overt clinical partial seizures (16.9%), whichwere aborted in 3–5 seconds by cold irrigation in most cases.Only 4 cases evolved into convulsive seizure requiring intravenousadministration of propofol.
MEP monitoring. MEP monitoring was available in all patients anddocumented a moderate (,50%) transient reduction of MEP in16% of cases, which did not interfere with subcortical resection.
Subgroup B In subgroup B (296 patients, Table 2) the combineduse of LF and HF stimulation was required for performing and ef-fectively mapping CST during resection.
Table 3. Group 1: Patient clinical characteristics and tumor features defined by imaging
Group 1 (479 patients)
Subgroup A Subgroup B
Clinical history:Previous treatmentsSeizuresAEDsNeurologicaldeficits
171 patients (57.7%) received previoussurgery, chemotherapy, and/orradiotherapy (8 patients radiotherapy only)
3–6 months: 132 patients (72.1%) partialseizures only; 51 patients (27.9%)partial and generalized seizures
Median 6 seizures/month, either partialseizures only or partial seizures evolvinginto generalized seizures
One (82% of patients) or, less frequently, 2 Poorly controlled by the administration of 2 to4 AEDs, although prescribed at high doses
177 (96.7%) intact, 6 (3.3%) mild motorimpairment
54 (18.2%) mild motor impairment(preoperative mild motor deficits inSubgroup BIII)
Tumor characteristics:Tumor localization Well-defined mass with sharp borders Tumor mass appeared diffuse with infiltrative
(261 patients, 88.2%)79 precentral site 130 precentral site21 paralimbic site 27 paralimbic site51 postcentral site 56 postcentral site32 rolandic site 83 rolandic site (harboring tumors in a
rolandic site, located within the CST: 6cases in subgroup BIV)
DTI FT available In 155 patients (84.7%) Unaffected tract in 22.4% In 234patients(79%)
Highly displacedtract in 13.3%
Displacement of the tract’s fibers in 39.9% Highly displaced andinfiltrated tract in86.7%
Displacement and infiltration of the tract in37.7%
Histological diagnosis Low-grade gliomas (126 patients, 68.9%) Low-grade gliomas (222 patients,75%)
High-grade gliomas (57 patients, 31.1%) High-grade gliomas (74 patients,25%)
Abbreviations: AEDs, antiepileptic drugs; DTI-FT, diffusion tensor imaging with fiber tractography
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1115
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

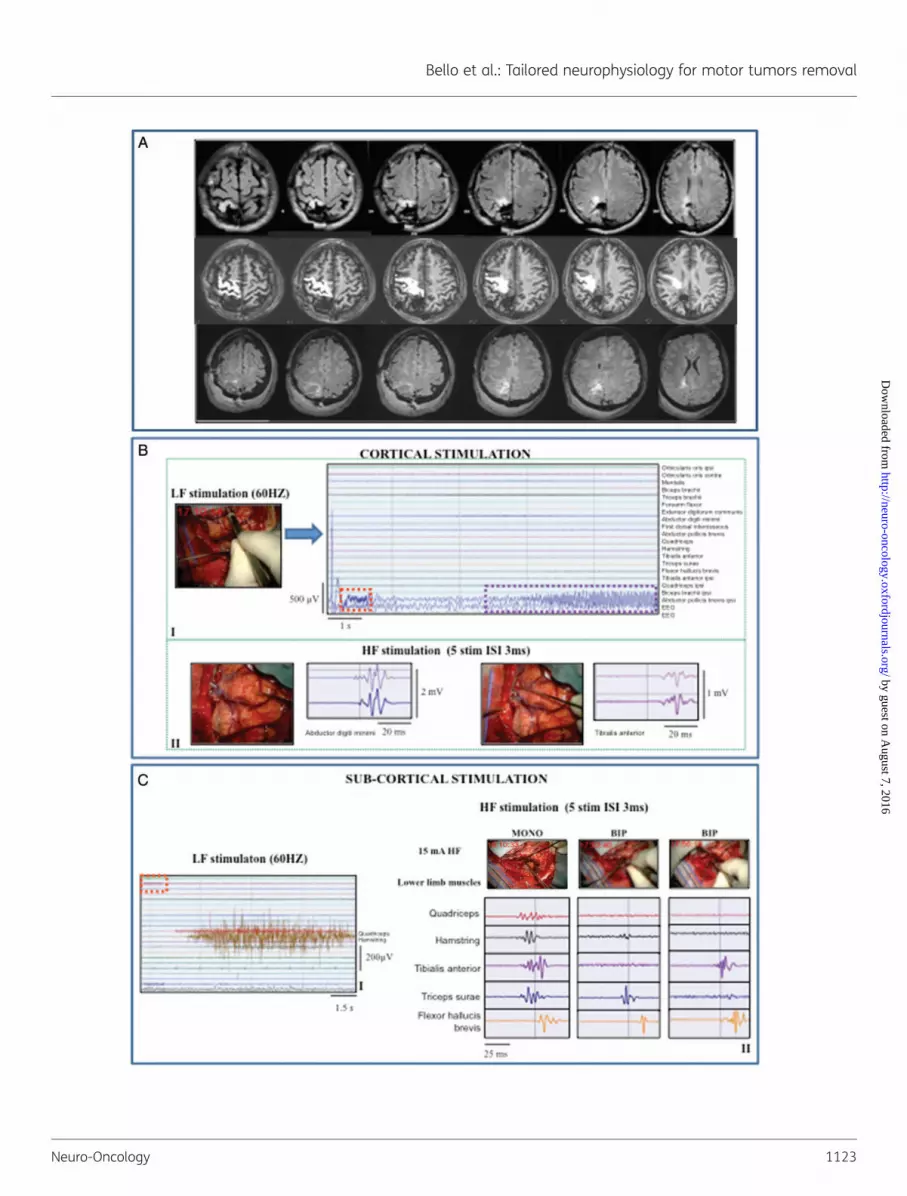
Fig. 1. Low-frequency (LF) stimulation (60 Hz ): tumors with sharp borders (Group 1/subgroup A †and Group 2/subgroup A). Representative case:34-year-old female with a short history of partial seizures (2 episodes of speech arrest), fully controlled by administration of one AED. MR studiesshowed a left (dominant) prerolandic mass resembling a low-grade glioma. She was operated under asleep-awake anesthesia for motor andlanguage mapping. Histology documented a grade II oligodendroglioma, IDH1 mutated, MGMT methylated, codeleted. In the immediatepostoperative course, she experienced transient motor (4/5) deficits, mainly at the upper limb, fully recovered. (A) Preoperative (DTI-FTreconstructions of CST, in white, were superimposed on T1-weighted images) and postoperative (postcontrast T1-weighted) MRI scan (Group 1) ofthe representative case. The CST was mainly displaced and slightly infiltrated. The postoperative MR showed complete resection. (B) LF stimulationof the primary motor cortex with bipolar probe-evoked EMG responses (screen shot) in distal muscles of the contralateral forearm/hand. Stimulusintensity (no stimulus artifact is visible)¼ 2 mA. (C) LF stimulation of the subcortical CST with bipolar probe-evoked EMG responses in differentmuscle groups of upper limb. Stimulation at deeper portion of CST tract (III) also involved the lower limb muscles. †Stimulus intensity¼ 10 mA(I and II); 6 mA (III). Stimulus artifact indicated by dashed red line.
Bello et al.: Tailored neurophysiology for motor tumors removal
1116
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

Fig. 2. Combined low-frequency (LF; 60 Hz)/high-frequency (HF) stimulation: tumor highly displacing and infiltrating the CST (Group 1/1subgroup BI).Representative case: a 38-year-old female with an 8-month history of partial motor seizures, followed in the recent past by some generalized seizurescontrolled by the administration of 2 AEDs. MR studies showed a right (nondominant) prerolandic mass resembling a low-grade glioma. She wasoperated under asleep anesthesia. Histology revealed a grade II oligodendroglioma, IDH1 mutated, MGMT methylated, codeleted. Immediatepostoperative course was characterized by left motor weakness (3/5), lasting 10 days and fully recovered. (A) Preoperative (DTI-FT
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1117
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

Clinical features. One-hundred seventy-one patients (57.7%) hadundergone previous surgeries and chemotherapy and/or radiother-apy. Patients reported frequent seizures (median 6 seizures/month)that were poorly controlled by high doses of 2–4 AEDs, and 54patients showed mild motor impairment on admission (Table 3).
Radiology. In the majority of cases (261 patients), the tumorsappeared diffuse and characterized by infiltrative borders onFLAIR images. DTI FT reconstruction of CST, available in 234cases (79%), showed a highly displaced tract in 31 cases(13.3%) and a highly displaced and markedly infiltrated tract in203 cases (86.7%). Tumors were located at rolandic (83), precen-tral (130), paralimbic (27), and postcentral (56) sites (Table 3).
Histology. Two-hundred twenty-two cases (75%) were LGGs, and74 were HGGs.
Mapping procedure. Four different neurophysiological conditionswere observed intraoperatively, clustering patients into 4 differentsubsets.
(a) In the first subset of patients (1subgroup BI; 150 cases),intraoperative mapping required combined use of LF and HFstimulation. At the beginning, LF stimulation, although athigh intensity, failed to elicit motor responses (Fig. 2,Panel-BI) on prerolandic cortical sites showing motor activa-tion on fMRI and motor fibers on DTI-FT images. When ap-plied over the same sites, the HF stimulation elicitedresponses (cHF-MT intensity: 5–12 mA, Fig. 2, Panel-BII),which allowed cortical mapping. Similarly, at the beginningof the subcortical resection, HF stimulation was required(Fig. 2, Panels-CI/II), while LF was not inducing subcorticallymotor responses. However, when a significant portion ofthe tumor was removed and the CST was decompressed, LFturned out to excite the CST fibers identified by the DTI-FT andalways responsive to HF stimulation (Fig. 2, Panels-CIII/IV).Conclusively, in this subset of patients, HF stimulation was al-ways efficient during resection, while LF stimulation was reli-able only at the final stage of subcortical resection when HFand LF stimulation were delivered at threshold intensity(sHF-MT and sLF-MT) corresponding to 2 mA and 3 mA, re-spectively. Clinically these patients were characterized by along history of seizures, receiving 2 –3 AEDs, and
radiologically by diffuse tumor on FLAIR images and high dis-placement and infiltration of the CST in DTI reconstruction.
(b) In the second subset (1subgroup BII; 115 cases), due to analtered cortical excitability, the LF cortical motor threshold in-tensity (cLF-MT: 2 –6 mA) corresponded to the epilepticthreshold (ie, the minimum current inducing motor responseswith LF also triggered partial or even generalized seizures[rare]), which normally leads to cessation of LF stimulation(Fig. 3, Panel-BI). Conversely, HF stimulation (cHF-MT: 5 –13 mA) allowed safe cortical mapping with no occurrencesof seizures (Fig. 3, Panel-BII). HF stimulation was also neededduring the main portion of subcortical resection when LF wasnot evoking motor responses or inducing seizures. LF elicitedresponses without seizures only at the final stage of resectionwhen the CST had been largely decompressed; HF and LFwere both used at threshold intensity (3 mA for HF and5 mA for LF) to define the resection margins (Fig. 3,Panels-CI/II). Clinically, these patients were characterized bya long history of seizures that were poorly controlled by highdoses of 2–4 AEDs. Radiologically, they presented with dif-fuse tumors on FLAIR images that highly infiltrated and dis-placed the CST in DTI reconstruction.
(c) In the third subset of patients (1subgroup BIII; 21 cases), LFstimulation failed at both cortical and subcortical levels,(Fig. 4, Panels-BI-CI), even at the end of resection when high-current intensity elicited none or inconsistent small-ampli-tude EMG responses. Conversely, HF stimulation was alwaysefficient (cHF-MT: 6–16 mA, sHF-MT: 3 mA), thus represent-ing the unique tool to perform the functional mappingthroughout resection (Fig. 4, Panels-BII-CII). Clinically,patients belonging to this subgroup were characterized by along history of seizures, were taking 2–4 AEDs, and presentedpreoperatively with mild motor deficits. Radiologically theyshowed highly diffuse tumor masses with highly infiltratedCST on DTI images.
(d) The fourth subset included patients (1subgroup BIV; 10cases) with a long history of poorly controlled partial motorseizures who harbored rolandic tumors that were highlyinfiltrating or located within the CST. LF stimulation induceda high percentage of seizures (Fig. 5, Panels-BI/CI) and failedthe mapping at both cortical and subcortical levels, while HFstimulation was always very efficient (Fig. 5, Panels-BII-CII).In this subset, HF was delivered with the monopolar and bipo-lar probes, both equally efficient, with some differences in
reconstructionions of CST, in white, are superimposed on T1-weighted images) and postoperative MRI scan (FLAIR images) (Group 1) of therepresentative case. The CST was displaced and highly infiltrated by the tumor. Postoperative MR (FLAIR) showed complete resection. (B) (I) Failureof LF stimulation (bipolar probe) over the primary motor cortex with intensity up to 7 mA (stimulus artifact indicated by dashed red line). (II) HFstimulation (train of 5 anodal square pulses, 0.5 milliseconds duration, ISI 3 milliseconds, 1 Hz repetition rate) of the primary motor cortex with amonopolar probe evoked a motor response in hand/forearm muscles. MEPs are displayed on the monitor with all the recorded muscles (EMGfree-running modality, upper window) and in a separate monitor in triggered modality (lower window) allowing display of single muscles for moreprecise monitoring. Both LF (I) and HF (II) stimulation were applied over the same site indicated by the intraoperative screen shot (DTI-FTreconstruction of CST, in white, superimposed on T1-weighted images). (III) Continuous MEP monitoring in abductor digiti minimi from the corticalstrip (5 anodal square pulses, 0.5 milliseconds duration, 3 milliseconds ISI, 1 Hz repetition rate). (C) (I) Failure of the LF at initial stage subcorticalresection (8 mA) (the intraoperative picture shows the site of stimulation). Over the same subcortical site, HF (II) successfully evoked response inhand muscle (16 mA monopolar probe). (III) After partial tumor removal, LF stimulation of the CST evoked response in hand/forearm muscles(7 mA). The activated muscles show a sustained clonic motor activity, continuing 1.736 milliseconds beyond the end of the stimulus (verticaldashed green line) and stopped by cold irrigation of the stimulated site. (IV) At the end of resection, LF stimulation evoked an EMG activation inlower limb muscles (4 mA).
Bello et al.: Tailored neurophysiology for motor tumors removal
1118
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

Fig. 3. Combined low-frequency (LF; 60 Hz)/high-frequency (HF) stimulation: tumor highly displacing and infiltrating the CSTand long history of seizures,poorly controlled by AEDs (Group 1/1subgroup BII). Representative case: a 41 year old male, with a 2 year history of motor partial seizures, increasing infrequency to 3–4 a week, associated in the recent past with several generalized seizures, poorly controlled by the administration of 4 AEDs at highdosage. MR studies showed a right (nondominant) postrolandic mass resembling a low-grade glioma. He was operated under asleep anesthesia.Histology revealed a grade II oligoastrocytoma, IDH1 wild-type, MGMT methylated, non-codeleted. Postoperative course was characterized by mild(4/5) motor weakness, recovered in 2 weeks. Seizures disappeared, and the number of AEDs reduced to one at 3 months post surgery.
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1119
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

spatial resolution (Fig. 5, Panel-CII). Specifically, the bipolarprobe was used at the end of resection, because of its higherspatial resolution, to get closer to the CST and better definethe margins of resection.
Seizures. In subgroup B, 156 patients (52.7%) showed electricalseizures, specifically all patients in subgroup BII, 20 (13.2%) insubgroup BI, and 15 and 6 patients in subgroups BIII and BIV, re-spectively. Seizures occurred with LF stimulation, which triggeredpartial seizures in 39 paticipants (11%, mostly in subgroup BII).Only 6 patients (2%) developed clinical seizures during HF stimu-lation. The interruption of stimulation and use of cold irrigationcontrolled partial seizures. Only 3 cases (1%) spread to thewhole hemibody and required infusion of propofol.
MEP monitoring. MEP monitoring was available for all patients anddocumented moderate (,50%) transient reduction of MEP in37.8% and severe transient reduction (.50%) in 7%. Moderatereduction of MEP did not interfere with subcortical resection,which was briefly interrupted or continued in distant areas ofthe surgical cavity and resumed after MEP normalization incases of severe MEP reduction. Transient MEP loss was observedin only 2 cases. In those cases, MEP trace was recovered by in-creasing the current intensity (+2 mA) and increasing the levelof blood pressure.
Group 2 (sole LF stimulation)
Two subgroups (subgroups A and B) were identified in the historicalgroup (112 patients; Table 2) according to the neurophysiologicalfindings observed intraoperatively and related clinical context.
Subgroup A In the first subgroup (2Subgroup A; 68 cases), LF suc-cessfully allowed mapping in all cases at both the cortical andsubcortical levels. The motor threshold intensity (cortical andsubcortical LF-MT) was not assessed, and the same range of cur-rent intensity (3–8 mA) was used at the cortical and subcorticallevels for guiding resection. Clinically, tumors were mostly LGGs,and patients free from neurological deficits reported a short his-tory of seizures that were well controlled with one AED. Radio-logically, patients presented with tumors with sharp margins inFLAIR images and DTI, when available, showed a displaced CTSwith limited infiltration (Table 4). Twenty-five percent of thepatients experienced intraoperative seizures.
Subgroup B In subgroup B, LF stimulation was partially or totallyinefficient at the cortical and/or subcortical level in 44 patients.
Two subsets were identified according to the clinical and radio-logical scenario and associated intraoperative neurophysiologicalfindings (Table 4).
(a) In the first subset (2Subgroup BI; 36 cases), patientsreported a long history of seizures, controlled with 2 –3AEDs, and 5 patients had preoperative mild to moderatemotor impairment. Radiologically, these patients had tumorswith diffuse margins or edema in FLAIR images and highlyinfiltrated CST in DTI images. Intraoperatively, the high inten-sity needed for LF at the cortical level (range 10–18 mA) toinduce motor responses led to a significant occurrence of sei-zures (18 cases, 50%), generalized in 3 cases (8.3%). The sub-cortical mapping was performed by applying LF at currentintensities higher (beginning) or equal (end of resection) tothose applied over the cortex and occasionally led to seizures(4 cases, 11.1% partial).
(b) The second subset (2Subgroup BII; 8 cases) clusteredpatients with large tumors and considerable edema dislocat-ing/infiltrating the CST. Seven patients showed preoperativemild motor deficits. LF stimulation, despite the high intensity(average 20 mA), produced negative results while mappingover cortical areas reporting fMRI motor activation and/orDTI CST reconstruction. In these cases, resection was startedin an area of tumor distant from the fMRI/DTI-positive sites.After a partial tumor removal, LF turned out to work, al-though with a high intensity (mean 15 mA), which was asso-ciated in 4 patients (50%) to partial seizures.
Impact of the Different Mapping Protocolson EOR and the Occurrence of Transientand Permanent Motor Deficits
The extent of resection (EOR) and the occurrence of transient andpermanent deficits were assessed in all patients.
Group 1
Subgroup A (LF efficient, HF for comparison; LF-MT current use-d)In a total of 183 procedures, EOR was estimated as total in 154cases (84.2%), subtotal in 20 cases (10.9%), and partial in 9 (4.9%).
Acute motor deficits occurred in 109 patients (59.5%), fullyrecovered in all patients.
Subgroup B (LF–HF Combined; LF-MT and HF-MT Current Used)1Subgroup BI (150 patients. HF used; LF inefficient and used atthe end of resection).
(A) Preoperative (DTI-FT reconstructions of CST, in white, are superimposed on T1-weighted images) and postoperative MRI scan (FLAIR images) (Group1) of the representative case. The CST was highly infiltrated by tumor. Postoperative MR (FLAIR) showed a subtotal resection with the persistence ofFLAIR abnormalities at the site of CST. (B) (I) LF stimulation (.10 mA, bipolar probe) over primary motor cortex evoked tiny response in forearm andhand muscles, but a seizure ensued starting from the muscles barely responding to stimulation and progressed to involve the whole upper limb.Stimulus artifact is indicated by red dashed line. The intraoperative screenshot (DTI-FT reconstruction of CST, in white, superimposed onT1-weighted images) indicates the site of stimulation. (II) Stimulation of the same site (screen shot) with HF stimulation (3–4 cathodal squarepulses, 0.5 milliseconds duration, 3 milliseconds ISI, 1 Hz repetition rate, monopolar probe) at high intensity (21 mA) evoked MEPs in hand andlower limb muscles. (C) (I) At the end of surgery, a response in lower limb muscles was obtained by LF stimulation (4 mA). (II) In the final part ofthe resection, the motor threshold to HF stimulation was reduced to 8 mA. The intraoperative screenshot (DTI-FT reconstruction of CST, in white,superimposed on T1-weighted images) indicates the site of stimulation.
Bello et al.: Tailored neurophysiology for motor tumors removal
1120
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

Fig. 4. Combined low-frequency (LF; 60 Hz)/high-frequency (HF) stimulation: highly diffuse tumor mass, highly infiltrated CST, and preoperative mildmotor deficits (Group 1/1subgroup BIII). Representative case: a 49-year-old-male with a 2-year history of motor partial seizures in the recent pastand poorly controlled by administration of 4 AEDs. MR studies showed a right (nondominant) pre and postrolandic mass resembling a low-gradeglioma and associated with ventricular enlargement (the patient had a previous history of intracerebral meningitis at birth). He was operated underasleep anesthesia. Histology revealed a grade II oligoastrocytoma, IDH1 nonmutated, MGMT methylated, non-codeleted. Immediate postoperative
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1121
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

EOR was total in 105 cases (70%) and subtotal in 45 (30%).Acute motor deficits were observed in 103 patients (68.7%, in-
cluding those with preoperative deficits) and permanent deficitsin 4 patients (2.7%, including 2 patients with previous deficits).
1Subgroup BII (115 patients; HF used; LF induced seizures andwas used at the end of resection). EOR was total in 67 cases(58.3%), subtotal in 41 (35.7%), and partial in 7 (6%).
Acute motor deficits occurred in 64 patients (55.6%) includingthose with preoperative deficits, and permanent deficits occurredin 2 patients (1.7%).
1Subgroup BIII (21 patients. HF used; LF totally inefficient).EOR was subtotal in 12 (57.2%) cases and partial in 9 cases
(42.8%).Acute motor deficits occurred in 18 (85.7%) patients (including
16 with preoperative deficits), and permanent deficits occurred in2 patients (9.5%).
1Subgroup BIV (10 patients. HF used, both probes tested; LFtotally inefficient)
EOR was total in 6 (60%) cases and subtotal in 4 (40%).Acute motor deficits occurred in 1 patient, who recovered fully.
Group 2
Subgroup A (LF Efficient. No LF-MT Current Assessed)In 68 pro-cedures, EOR was total in 49 (72.1%) cases and subtotal in 19(27.9%).
Acute motor deficits occurred in 42 (61.8%) patients, whorecovered fully.
Subgroup B (LF Partially or Not Successful)2Subgroup BI (36 patients; LF induced seizures)
EOR was total in 21 (58.4%) cases, subtotal in 12 (33.3%)cases, and partial in 3 cases (8.3%).
Acute motor deficits occurred in 34 patients (94.4%, includingthose with preoperative deficits). Four (11.1%) patients had per-manent deficits.
2Subgroup BII (8 patients. LF totally inefficient)EOR was total in 5 (62.5%) cases and subtotal in 3 (37.5%)
cases.All (100%) patients showed acute motor deficits, and 6 (75%)
had permanent deficits.
Clinical Remarks
By looking at the mapping procedures adopted during surgery,the patients’ related clinical and imaging features, and the clinicalresults, patients harboring a tumor involving the motor pathwayscan be clustered into 2 main groups (Fig. 6). The first group
(low-risk motor tumors) comprises patients with a short historyof seizures that are well controlled by one or a maximum of 2AEDs, harbor tumors with well-demarcated (sharp) borders inFLAIR images, and have mostly displaced and minimally infil-trated CST in DTI images. In this setting, LF is efficient and,when delivered at threshold intensity (Group 1, subgroup A),allows better EOR (total resections: 84% in group1 vs 72% inGroup 2; P¼ .05) and reduces the occurrence of intraoperativeseizures (25% in Group 2: vs 16% in Group 1; P , .001). The se-cond group (high-risk motor tumors) comprises patients with along history of seizures who take high doses of several AEDsand is characterized by eventual poor seizure control, previoustreatment, the appearance of diffuse and poorly demarcatedtumor borders in FLAIR images, and highly displaced and infil-trated CST in DTI images. When LF is used in this high-riskgroup, it is usually not efficient and is associated with a highrate of permanent deficits (22.7% in Group 2 subgroups BI andBII) and a high occurrence of intraoperative seizures. The percent-age of clinical seizures was indeed higher (50%) in Group 2 (sub-group B, only LF available and requiring high intensity) than inGroup 1 (11% subgroup B) because HF was rapidly substitutedwhen LF was found to be inefficient in this group. In this high-riskpatient group, HF allows reliable mapping in all conditions withlow permanent morbidity (2.7%) and low occurrence of intrao-perative seizures (2%). In addition, subdividing the high-riskgroup into 4 subsets, according to their clinical and radiologicalfeatures, allowed identification of each subgroup and determin-ation of the best cortical and subcortical stimulation modalitiesand current intensities and the most appropriate probe (monopo-lar vs bipolar) choices to optimize mapping at the cortical andsubcortical levels and reduce the occurrence of permanent defi-cits. Moreover, tailoring the use of LF and HF to clinical conditionshas increased the percentage of high-risk patients who weretaken to surgery, from 39.3% when only LF was available to63% when both LF and HF were used (P , .001). Notably, theincreased number of treated patients was associated with a sig-nificant reduction in permanent morbidity (from 22.7% in Group 2to 2.7% in Group 1), a reduced incidence of intraoperative seizures(from 50% to 2%; P , .001), and a high rate of EOR (total resec-tion .60%).
Neurophysiological Remarks: Intraoperative Use of LFand HF Stimulation Mapping
The use of LF and HF, as proposed here, requires technical nuan-ces and careful interpretation by an in-house experienced neuro-physiologist. The principal aspects are highlighted here (seeSupplementary Materials for more details and Figs 7, 8, 9 in
course was characterized by a mild motor weakness at the arm (4/5), recovered in one week. Seizures disappeared after surgery. (A) Preoperative(DTI-FT reconstruction of CST, in white, are superimposed on T1-weighted images) (Group 1) of the representative case. The CST was displaced andinfiltrated by the tumor. Postoperative MR (T1) showed a partial resection, with the persistence of T1 abnormalities at the level of prerolandic andinsular sites. (B) (I) Failure of LF stimulation over the primary motor cortex (8 mA, bipolar probe). Stimulus artifact is indicated by red dashed line.(II) HF stimulation (0.5 milliseconds duration, 4 milliseconds ISI, 1 Hz repetition rate, monopolar probe) evoked clear MEPs in the hand muscles(8 mA).The intraoperative screenshots (DTI-FT reconstructions of CST, in white, are superimposed on T1-weighted images) indicated the site ofstimulation. (C) (I) Failure of LF stimulation at subcortical level (10 mA, bipolar probe). (II) HF stimulation (5 cathodal square pulses, 0.5 millisecondsduration, 4 milliseconds ISI, 1 Hz repetition rate, monopolar probe) evoked MEPs from the hand and the forearm muscles. The intraoperativescreenshots (DTI-FT reconstructions of CST, in white, superimposed on T1-weighted images) indicated the site of stimulation.
Bello et al.: Tailored neurophysiology for motor tumors removal
1122
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1123
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

Supplementary Materials). High-sensitivity display of EMG allowsdetection of the earliest signs of muscle response to stimulationand thus prevents further increase of current intensity to gener-ate evident movement of the body segment. This current limita-tion certainly helps reduce intraoperative seizures. In addition,multichannel EMG equipment can detect activity from multiplemuscles, either induced by brain stimulation or by ictal activation,including less evident muscles such as the orofacial muscles. De-tection of the earliest EMG signs of seizures, together with ECoGdetection of AD, prompts interruption of stimulation and actionsthat usually succeed in aborting seizure activity.
At the cortical level, LF stimulation generates progressivemotor unit recruitment with different features when comparedwith voluntary activation (Fig. 7B in Supplementary Materials).At the subcortical level, the time course of EMG activation,showed a progressive EMG recruitment only when stimulatingCST fibers at the superficial (proximal to the cortex) loosing thisfeature when stimulating at deeper level (Fig. 7E in Supplemen-tary Materials). HF stimulation requires EMG for visualization. HFstimulation generates MEPs, (ie, time-locked EMG responses todiscrete stimulation) and shows similar morphology at any levelof CST stimulation. Generally in HGGs, large tumors, previous sur-geries/radiation, it is sometimes necessary to change polarity ofstimulation to obtain responses at cortical level. For both LF andHF, the recruitment of cephalic (head-neck) and lower limb mus-cles generally requires higher current intensity (mean increment2 mA) compared with upper limb muscles. Using an ultrasonic as-pirator during LF stimulation at the subcortical level abolishes theresponses19 but does not affect HF responses. At the subcorticallevel, assessment of the threshold current is crucial to estimatingthe minimal distance between the probe and the fibers and hasto be adjusted according to clinical and radiological conditions(Fig. 6, high risk patients, 4 subgroups). In patients with well-demarcated tumors and history of well-controlled seizures,(Group 1, subgroup A), the LF threshold intensity (sLF-MT) corre-sponded to about 2 mA. In large tumors with edema and poorlycontrolled seizures, the sLF-MT increased about 2–4 mA (Group 1,subgroup B) and sometimes triggered seizures even before orwithout motor responses. With HF stimulation, the threshold
intensity (sHF-MT, on average 2–3 mA) allowed mapping in allclinical contexts. When delivered by monopolar probe at the cor-tical level, HF generates responses from the primary motor andoccasionally from somatosensory cortex, possibly due to a cur-rent spread. In these cases, the use of a bipolar probe evokedmore focused responses (single or small groups of muscles)and no responses from the somatosensory cortex, but higher in-tensity is needed (range 4–7 mA). Subcortical stimulation with amonopolar probe at sHF-MT (3 mA) elicited multiple muscleresponses even in distant body segments (eg, forearm and leg),suggesting a low spatial resolution of the stimulus. The bipolarprobe, despite requiring higher intensity is more focal, allowingto extend the dissection closer to the CST (Fig. 5, 1Subgroup BIV).
The intensity of stimulation current must also be adjusted tothe anesthesiological setting, being higher in asleep patientsthan in awake patients.
DiscussionThis study reports the data obtained with the combined use of LFand HF stimulation for surgical removal of gliomas involvingmotor pathways. The analysis was performed on a large seriesof cases with a wide spectrum of clinical conditions. We adoptedthe strategy of applying the more effective stimulation protocolaccording to the conditions encountered at surgery. The success-ful neurophysiological protocols used at surgery were thenrelated to the clinical context, defined by patient clinical historyand tumor features, identified by tumor appearance on FLAIRconventional images and CST involvement on DTI images, andto clinical results, defined by occurrence of intraoperative sei-zures, EOR and percentage of permanent deficits. This allowedclustering patients with motor gliomas in clinical subgroups, de-fining for each the most effective neurophysiological protocol forguiding resection. Our data demonstrate that the integration ofLF with HF stimulation tailored to the clinical context increasesthe number of patients who would benefit from surgery andsignificantly increases the EOR, while decreasing permanentmorbidity and the occurrence of intraoperative seizures.
Fig. 5. Combined low-frequency (LF; 60 Hz)/high-frequency (HF) stimulation: tumor highly infiltrating or located within the CSTand long history of poorlycontrolled partial motor seizures (Group 1/1subgroup BIV). Representative case: a 39-year-old male with a previous history of right postrolandic grade IIoligodedroglioma, treated by surgery and followed by observation. Patient started to experience several partial sensory-motor seizures in the last 8months, poorly controlled by AEDs (which were progressively increased in number and dosage). He was submitted to neuroradiological follow-upthat showed a progressive increase of FLAIR abnormalities anterior to the previous surgical cavity within the CST, consistent with recurrence of thetumor. He was operated under asleep anesthesia. Histology showed a grade II oligodendroglioma, IDH1 mutated, MGMT methylated, codeleted.Immediate postoperative course was characterized by mild (4/5) weakness at the lower limb, fully recovered in one week. (A) Preoperative (FLAIR,upper), preoperative reconstruction of CST by DTI FT (white) superimposed on T1-weighted images (middle), and postoperative (FLAIR, lower) MRIscan of the representative case. Postoperative MR showed a subtotal resection with a little persistence (1,1 mL) of FLAIR abnormalities close to thelateral ventricle. (B) (I) LF stimulation of primary motor cortex (2 mA, bipolar probe) failed to evoke muscular responses (stimulus artifact indicatedby red dashed square) while inducing electrical seizure on EcoG (violet dashed line). The intraoperative picture of the surgical field indicates the siteof stimulation with the bipolar probe. (II) Over the same site, HF stimulation (5 anodal square pulses, 0.5 milliseconds duration, ISI 3 milliseconds, 1 Hzrepetition rate, monopolar probe) induced MEPs without occurrence of seizures. The intraoperative picture of the surgical field indicated the site ofstimulation with the monopolar probe. (C) (I) LF stimulation at subcortical level at the end of resection (7 mA, bipolar probe) failed to evokemuscular responses but triggered a focal seizure involving the lower limb muscles, which lasted 10.5 seconds and was interrupted by coldirrigation. (II) Subcortical mapping of the motor fibers with HF during surgical dissection. HF stimulation (cathodal square pulses, 0.5 millisecondsduration, ISI 3 milliseconds, 1 Hz repetition rate, 15 mA) was applied through monopolar and bipolar probes. Monopolar probe: activation ofmultiple muscles at the same site. Bipolar probe: focal responses of few muscles, which differed when the probe position was changed. Theintraoperative picture of the surgical field indicated the site of stimulation with the monopolar or bipolar probes. MONO, monopolar probe; BIP,bipolar probe.
Bello et al.: Tailored neurophysiology for motor tumors removal
1124
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

Fig. 6. Motor pathways tumor patient group stratification. Patients with tumors involving motor pathways can be stratified into 2 main groups (low-riskand high-risk) according to clinical variables and tumor features defined by imaging. The most appropriate stimulation modality for each group isindicated. The high-risk group is further subdivided into 4 subgroups according to clinical and imaging parameters and the most appropriateneurophysiological strategy to be used intraoperatively. Abbreviations: LF, low-frequency stimulation (60 Hz); HF, high-frequency stimulation; sMT,subcortical motor threshold; sLF MT, subcortical motor threshold with LF; sHF MT, subcortical motor threshold with HF. The current intensity of sMTis indicated in milliamperes.
Table 4. Group 2: Patients clinical characteristics and tumor features defined by imaging
Group 2 (112 patients)
2Subgroup A 2Subgroup BI 2Subgroup BII68 patients (60.7%) 36 patients (32.1%) 8 patients (7.2%)
Clinical historyPrevious treatments 16 (23.5%) 19 (52.7%) 2 (25%)Seizures Short history of seizures Several seizures Short history of seizuresAEDs 1 2–3 1–2Neurological deficits Free 5 mild (13.9%) 7 mild (87.5%)
Tumor characteristics Sharp margins Diffuse margins and edema Large tumors with edemaDTI FT available 22 patients (32.3%) displaced CTS and
with a limited infiltration17 patients (47.2%) displaced
and highly infiltrated CST5 patients (62.5%) Significantly dislocating
and infiltrating the motor area and tractHistological diagnosis 54 LGG (79.4%) and 14 HGG (20.6%) 20 LGG (55.6%) and 16 HGG (44.4%) 8 HGG (progressive LGG)
Abbreviations: AEDs, antiepileptic drugs; DTI-FT, diffusion tensor imaging with fiber tractography; HGG, high-grade glioma; LGG, low-grade glioma
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1125
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

Historical Background
During surgery, it is crucial to distinguish the eloquent essentialareas to be preserved from those that can be safely removed.The electrical stimulation of an eloquent area produces responses(positive site) consistent with its function (eg, muscular activationduring motor cortex stimulation).4,20 Therefore, resection mustpreserve the positive sites.12 The challenge is finding the appropri-ate stimulating protocol to identify the different structures withdifferent properties in the largest number of clinical conditionsand reduce the bias of false-positive or false-negative sites.With regard to the motor system, the main issue is preservingthe corticospinal system. Two stimulation paradigms evolvedfor intraoperative guidance: the 60 Hz technique (low frequency)and the “train-of-five” technique. At present, LF stimulation, intro-duced by Penfield, is widely used. The To5, which delivers shorttrains of pulses at high frequency, was originally conceived as aconstant monitor for functional integrity of the descendingmotor pathways13 rather than a tool for mapping. Most surgicalteams rely on either of these 2 techniques. In addition, there is avery strict association between the stimulating protocol and theprobe (LF: bipolar probe; HF: monopolar probe),12,20 – 28 and fewdata are available on the comparison between HF and LF.7,8,29
No data are available on integrating the choice of stimulation mo-dality with the clinical context. Gliomas are, in fact, highly hetero-geneous tumors, and their degree of heterogeneity increases as aresult of the treatments the patients receive. With regard totumors within the motor pathways, the degree of involvementof the corticospinal tract is generally quite variable, determiningthe various spectra of patients’ clinical history and presentationand impacting the level of excitability of the motor pathways atsurgery. Clinical features, such as seizure history, number anddoses of AEDs, seizure control, and previous treatments, are theclinical parameters that offer indication for the level of CST excit-ability that may be found intraoperatively. In addition, preopera-tive MR studies, such as the appearance of tumor on volumetricFLAIR images or DTI reconstruction, may provide the surgeonwith a view of CST involvement and represents a useful tool forplanning intraoperative surgical and neurophysiological strategy,9
This study compared HF with LF by investigating their clinicalfield of application, the advantages, the disadvantages, and theoverlapping features. The probe was analyzed independently ofthe stimulating protocol to determine the best probe-frequencymatch for different clinical conditions (patient clinical historyand tumor appearance on imaging) and evaluated in terms ofclinical outcome (percentage of intraoperative seizures, rate ofpermanent morbidity, EOR) and the number of patients whounderwent successful surgery.
The analysis of the data suggests 2 levels of discussion: amethodological level, in which the technical aspect of the stimu-lation is discussed, and a clinical level, in which the advantages interms of clinical feasibility and outcome are discussed.
Analysis of the Frequency of Stimulationand Probes
Subdividing the 2 groups into different subsets allowed assess-ment of the advantages and disadvantages of HF and LF forthe different clinical conditions related to patient clinical historyand tumor. Both the frequency of stimulation and the probe
emerged as crucial parameters for the mapping procedure. Intumors with sharp borders on FLAIR images, no or little CST infil-tration in DTI images, and stable cortical excitability, as sug-gested by short seizure history, optimal seizure control by oneor few AEDs, LF stimulation is maximally efficient (Group 1/Subgroup A; Group 2/Subgroup A), and optimized by using thethreshold current (total EOR Group 1. Group 2) Group 1/subgroupB shows 4 different subsets corresponding to the different clinicalsettings (history of several seizures, edema, infiltrative behavior ofthe tumor at imaging, and altered cortical excitability) in which LFstimulation failed at mapping the cortical or subcortical level,while HF was conversely very efficient. In tumors with diffusemargins and high CST infiltration, HF allowed resection after con-siderable decompression until LF resumed its efficacy. A questionarises on whether the efficiency of HF was optimized by using themonopolar probe, which presumably stimulated a larger areathan the bipolar probe and reached fibers with tumor infiltrationand edema that were far from the electrode. In fact, the samefibers became responsive to LF after decompression. LF stimula-tion was efficient but ictogenic in patients with altered excitability(Group 1/subgroup BII, long seizure history and poor seizure con-trol), while HF stimulation was optimal; this may have been due tothe frequency. Short trains at high frequency (250–500 Hz) arevery effective for exciting the motor structures, while LF (60 Hz)needs long trains (1–4 s), at high risk of seizures over a tissuewith aberrant excitability. In the last 2 subsets (Group 1/subgroupBIII-IV) of high-risk patients (highly diffuse tumor, edema, highlyinfiltrated CST, seizures, motor deficits), LF completely failed map-ping, while HF was efficient. Finally, the last subset (Group 1/sub-group BIV) highlighted the advantages of delivering HF with amore focal stimulus (bipolar probe). Overall, these data suggestthat HF stimulation is an efficient tool for testing the motor path-ways in all clinical settings, with selection of the cortical and sub-cortical MT and probe (monopolar vs bipolar) being based onclinical conditions. The use of LF should be restricted to patientswith a short history of seizures and tumor with limited CST infil-tration. In these cases, LF has the advantage of delivering thestimulus focally with a bipolar probe.
Clinical Impact
The clinical impact of combining HF and LF stimulation needs tobe evaluated for feasibility of mapping (number of cases in whichreliable mapping is obtained) and clinical outcome (EOR and rateof permanent morbidity).
Generally, resection is continued until positive sites areencountered. The concept that resection can be safely performedin areas not responsive to electrical stimulation (negative foci)assumed that the absence of response accounted for the ab-sence of a neurological function.4 However, the occurrence ofpermanent post-operative deficits, leads to consider the possibleinadequacy of the stimulating procedure has yielded to the occur-rence of “false negative foci”. In our experience, in fact, where LFstimulation failed, thus reporting a false negative site (in high riskpatients, 63% of Group 1), HF stimulation was conversely efficient.In 89% of these patients (Group 1-BI and Group 1-BII) LF stimu-lation resumed after decompression of the motor pathways. Hadthe negative-site approach been used in these cases, permanentdeficits could have occurred. The presumable occurrence of LFfalse-negative sites at the beginning of surgery should be
Bello et al.: Tailored neurophysiology for motor tumors removal
1126
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from

suspected in cases with altered CST excitability and may be pre-dicted by looking at both clinical parameters (eg, long history ofseizures, poor seizure control, large number of AEDs, or previoustreatment) and tumor features (eg, diffuse infiltration on FLAIRimages and high CST involvement on DTI images). In these con-ditions, which defined the high-risk motor group patients, the useof LF is not the first choice because of its association with highpermanent morbidity (22.7%) and high occurrence of intraopera-tive seizures (50%). In this setting, HF should be considered thefirst choice because it is efficient in all conditions, with low per-manent morbidity (2.7%) and low incidence of intraoperative sei-zures (2%). As stated in the previous paragraph, in this setting, theefficiency of HF may be due either to the use of the monopolarprobe, presumably stimulating a larger area with respect to thebipolar probe, reaching fibers suffering by tumor infiltration andedema and distant to the electrode (subgroup BI-I); alternatively,in tumors with altered cortical exitability (subgroup BI-II) may bedue to due to its frequency (short trains), which is highly efficientin exciting motor structures and is less ictogenic. Notably, withthe combined use of LF and HF, the percentage of high riskpatients who were successfully mapped and benefit from surgeryincreased from 39% of the historical group (only LF available) to63% (both HF and LF available).
This study clearly demonstrates that the search for the thresh-old current, suggesting the minimal distance from the essentialfibers,30 – 35 is mandatory for increasing EOR and decreasing per-manent morbidity. Total resection was in fact accomplished withLF in 72% of sharp tumors (Group 2/subgroup A) and increased to84.1% when LF-threshold current was used (Group 1/subgroupA). The use of HF and LF stimulation at threshold current intensityincreased the rate of total resection in infiltrative tumors (from 60to 70%), decreasing permanent deficits (from 9% Group 2 Sub-group B, to 2.1% Group 1).
Procedures guided by subcortical mapping are associated withoccurrence of transient deficits (from 10.4% to 49.6% in differentstudies).1,12,31,36 – 38 The finding of positive subcortical sites is gen-erally associated with a higher rate of permanent deficits (from7.4% to 15.1% according to various series). Our data show thatit is possible to further decrease this percentage to 1.8%, evenin high risk cases, by using stimulation either alternated withresection or coupled with it and using threshold current withthe appropriate probe.
Clinical Constraints
The combined use of LF and HF protocols adopted in the presentseries showed the advantage of tailoring the stimulation protocolto clinical conditions, enhancing motor pathways identification atboth cortical and subcortical levels, and targeting resection to theMT to further extend the margin of resection. The use of MT EMGresponses, by decreasing the current intensity needed to evoke aresponse, significantly reduces the incidence of intraoperative sei-zures. However, there are 2 limitations: the need for complexequipment provided with wide EMG recording to detect evokedresponses during surgery and the need for an inhouse, experi-enced neurophysiologist to carefully interpret the responses.EMG recording is necessary for distinguishing induced movementfrom voluntary movement, to monitor the superficial or deeplevel of stimulation, to record MEPs induced by HF simultaneously
in different muscles, and to recognize different muscle recruit-ment when changing probe.
The intensity of current should be adjusted to the anesthesiasetting (higher in asleep conditions) and to the muscular district(cephalic, upper or lower limb) to be tested. Using the appropriatefrequency and probe is suggested when mapping nonprimarymotor or sensory areas to avoid current spread and to relateresponses to the correct area.
Conclusions
Our data suggest that the combined use of LF-HF stimulation,when tailored to the clinical conditions identified by patient clin-ical history and tumor features as shown by imaging, increasesthe feasibility of mapping and the number of patients whowould be candidates for surgery. The frequency of stimulationand the choice of probe must be considered independently. Thechoice of the appropriate stimulation and probe depends uponthe clinical context and may change within the same surgeryaccording to ongoing modifications during the procedure. Intumors involving motor pathways, it seems reasonable to sug-gest HF as the best frequency paradigm to stimulate the motorsystem.39 In conclusion, being the chance to identify the “posi-tive” sites strictly related to the stimulation paradigm, it is man-datory that both the surgeon and the clinical neurophysiologistknow the advantages and limitations of each stimulation modal-ity and probe for various clinical conditions.
Supplementary MaterialSupplementary material is available at Neuro-Oncology Journalonline (http://neuro-oncology.oxfordjournals.org/).
FundingThe work was supported by grants from the Italian Ministry of Health,Ricerca Finalizzata RF-2009-1530888 (to AF and LB), 2010 (to LB, GC,AF); Associazione Italiana Ricerca sul Cancro (to LB); Fondazione Berlucchi(to LB); Fondazione Italo Monzino (to LB).
Conflict of interest statement. None declared.
References1. Smith JS, Chang EF, Lamborn KP, et al. Role of extent of resection in
the longterm outcome of low grade hemispheric gliomas. J ClinOncol. 2008;10:1338–1345.
2. Bello L, Fava E, Carrabba G, Papagno C, Gaini SM. Present day’sstandards in microsurgery of low-grade gliomas. Adv Tech StandNeurosurg. 2010;35:113–157.
3. Duffau H. Introduction. Surgery of gliomas in eloquent areas: frombrain hodotopy and plasticity to functional neurooncology.Neurosurg Focus. 2010;28(2):Intro.
4. Sanai N, Berger MS. Intraoperative stimulation techniques forfunctional pathway preservation and glioma resection. NeurosurgFocus. 2010;28(2):E1.
5. Bello L, Gambini A, Castellano A, et al. Motor and language DTI FiberTracking combined with intraoperative subcortical mapping forsurgical removal of gliomas. Neuroimage. 2008;39(1):369–382.
Bello et al.: Tailored neurophysiology for motor tumors removal
Neuro-Oncology 1127
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from
6. Robles SG, Gatignol P, Lehericy S, Duffau H. Long-term brain plasticityallowing a multistage surgical approach to World HealthOrganization Grade II gliomas in eloquent areas. J Neurosurg.2008;109(4):615–624.
7. Szelenyi A, Senft C, Jardan M, et al. Intra-operative subcorticalelectrical stimulation: a comparison of two methods. ClinNeurophysiol. 2011;122(7):1470–1475.
8. Kombos T, Suess O, Kern BC, et al. Comparison between monopolarand bipolar electrical stimulation of the motor cortex. Acta Neurochir(Wien). 1999;141(12):1295–1301.
9. Castellano A, Bello L, Michelozzi C, et al. Role of diffusion tensormagnetic resonance tractography in predicting the extent ofresection in glioma surgery. NeuroOncol. 2012;14(2):192–202.
10. Bello L, Gallucci M, Fava M, et al. Intraoperative subcortical languagetract mapping guides surgical removal of gliomas involving speechareas. Neurosurgery. 2007;60(1):67–80; comments: 80–82.
11. Duffau H, Capelle L, Sichez N, et al. Intraoperative mapping ofsubcortical language pathways using direct stimulation: ananatomo-functional study. Brain. 2002;125:199–214.
12. Keles GE, Lundin DA, Lamborn KR, Chang EF, Ojemann G, Berger MS.Intraoperative subcortical stimulation mapping for hemisphericalperirolandic gliomas located within or adjacent to the descendingmotor pathways: evaluation of morbidity and assessment offunctional outcome in 294 patients. J Neurosurg. 2004;100(3):369–375.
13. Taniguchi M, Nadstawek J, Langenbach U, Bremer F, Schramm J.Effects of four intravenous anesthetic agents on motor evokedpotentials elicited by magnetic transcranial stimulation.Neurosurgery. 1993;33(3):407–415.
14. Szelenyi A, Hattingen E, Weidauer S, Seifert V, Ziemann U.Intraoperative motor evoked potential alteration in intracranialtumor surgery and its relation to signal alteration in postoperativemagnetic resonance imaging. Neurosurgery. 2010;67(2):302–313.
15. Proposal for Revised Clinical and ElectroencephalographicClassification of Epileptic Seizures. Epilepsia. 1981;22:489–501.
16. Mori S, Crain BJ, Chacko VP, van Zijl PC. Three-dimensional tracking ofaxonal projections in the brain by magnetic resonance imaging. AnnNeurol. 1999;45(2):265–269.
17. Mori S, Frederiksen K, van Zijl PC, Stieltjes B, Kraut MA, Solaiyappan M.Brain white matter anatomy of tumor patients evaluated withdiffusion tensor imaging. Ann Neurol. 2002;51(3):377–380.
18. Xue R, van Zijl PC, Crain BJ, Solaiyappan M, Mori S. In vivothree-dimensional reconstruction of rat brain axonal projections bydiffusion tensor imaging. Magn Reson Med. 1999;42(6):1123–1127.
19. Carrabba G, Mandonnet E, Fava E, et al. Transient inhibition of motorfunction induced by the Cavitron ultrasonic surgical aspirator duringbrain mapping. Neurosurgery. 2008;63(1):E178–E179; comments:E179.
20. Szelenyi A, Bello L, Duffau H, et al. Intraoperative electricalstimulation in awake craniotomy: methodological aspects ofcurrent practice. Neurosurg Focus. 2010;28(2):E7.
21. Chacko AG, Thomas SG, Babu KS, et al. Awake craniotomy andelectrophysiological mapping for eloquent area tumours. ClinNeurol Neurosurg. 2013;115(3):329–334.
22. Krieg SM, Schnurbus L, Shiban E, et al. Surgery of highly eloquentgliomas primarily assessed as non-resectable: risks and benefits ina cohort study. BMC Cancer. 2013;2:13–51.
23. Prabhu SS, Gasco J, Tummala S, Weinberg JS, Rao G. Intraoperativemagnetic resonance imaging-guided tractography with integrated
monopolar subcortical functional mapping for resection of braintumors. Clinical article. J Neurosurg. 2011;114(3):719–726.
24. Suess O, Suess S, Brock M, Kombos T. Intraoperative electrocorticalstimulation of Brodman area 4: a 10-year analysis of 255 cases.Head Face Med. 2006;3:2–20.
25. Schucht P, Moritz-Gasser S, Herbet G, Raabe A, Duffau H. Subcorticalelectrostimulation to identify network subserving motor control.Hum Brain Mapp. 2013;34(11):3023–3030.
26. Talacchi A, Turazzi S, Locatelli F, et al. Surgical treatment ofhigh-grade gliomas in motor areas. The impact of differentsupportive technologies: a 171-patient series. J Neurooncol. 2010;100(3):417–426.
27. Yamaguchi F, Takahashi H, Teramoto A. Intra-operative detection ofmotor pathways using a simple electrode provides safe brain tumorsurgery. J Clin Neurosci. 2007;14(11):1106–1110.
28. Yamaguchi F, Takahashi H, Teramoto A. Navigation-assistedsubcortical mapping: intraoperative motor tract detection bybipolar needle electrode in combination with neuronavigationsystem. J Neurooncol. 2009;93(1):121–125.
29. Kombos T, Suess O, Funk T, Kern BC, Brock M. Intra-operativemapping of the motor cortex during surgery in and around themotor cortex. Acta Neurochir (Wien). 2000;142(3):263–268.
30. Bello L, Fava E, Casaceli G, et al. Intraoperative mapping for tumorresection. Neuroimaging Clin N Am. 2009;19(4):597–614.
31. Bello L, Castellano A, Fava E, et al. Intraoperative use of diffusiontensor imaging fibertractography and subcortical mapping forresection of gliomas: technical considerations. Neurosurg Focus.2010;28(2):E6.
32. Bertani G, Fava E, Casaceli G, et al. Intraoperative mapping andmonitoring of brain functions for the resection of low-gradegliomas: technical considerations. Neurosurg Focus. 2009;27(4):E4.
33. Nossek E, Korn A, Shahar T, et al. Intraoperative mapping andmonitoring of the corticospinal tracts with neurophysiologicalassessment and 3-dimensional ultrasonography-based navigation.Clinical article. J Neurosurg. 2011;114(3):738–746.
34. Ohue S, Kohno S, Inoue A, et al. Accuracy of diffusion tensormagnetic resonance imaging-based tractography for surgery ofgliomas near the pyramidal tract: a significant correlation betweensubcortical electrical stimulation and postoperative tractography.Neurosurgery. 2012;70(2):283–293.
35. Seidel K, Beck J, Stieglitz L, Schucht P, Raabe A. The warning-signhierarchy between quantitative subcortical motor mapping andcontinuous motor evoked potential monitoring during resection ofsupratentorial brain tumors. J Neurosurg. 2013;118(2):287–296.
36. Carrabba G, Fava E, Giussani C, et al. Cortical and subcortical motormapping in rolandic and perirolandic glioma surgery: impact onpostoperative morbidity and extent of resection. J Neurosurg Sci.2007;51(2):45–51.
37. Talacchi A, Turazzi S, Locatelli F, et al. Surgical treatment ofhigh-grade gliomas in motor areas. The impact of differentsupportive technologies: a 171-patient series. J Neurooncol. 2010;100(3):417–426.
38. Wilden JA, Voorhies J, Mosier KM, O’Neill DP, Cohen-Gadol AA.Strategies to maximize resection of complex, or high surgical risk,low-grade gliomas. Neurosurg Focus. 2013;34(2):E5.
39. Deletis V, Sala F. Subcortical stimulation (mapping) of thecorticospinal tract. Clin Neurophysiol. 2011;122(7):1275–1276.
Bello et al.: Tailored neurophysiology for motor tumors removal
1128
by guest on August 7, 2016
http://neuro-oncology.oxfordjournals.org/D
ownloaded from




























