Embed Size (px)
Citation preview
V2.2019
1Guideline for Suspected Cancer Referral in the State of Qatar
GUIDELINE FOR SUSPECTED CANCER REFERRAL
in the State of Qatar
V2.2019
2 Guideline for Suspected Cancer Referral in the State of Qatar
Guideline for Suspected Cancer Referral in the State of Qatar
This document is a best practice guide intended to assist in the timely recognition and appropriate referral of patients with symptoms suggestive of cancer in the State of Qatar. It has been compiled and updated by the Ministry of Public Health (MOPH) and originally based on guidelines from the National Institute for Health and Care Excellence (NICE), Hamad Medical Corporation (HMC), the National Comprehensive Cancer Network (NCCN), and the London Cancer Alliance (LCA) Clinical Network.
This document has been reviewed and updated by clinical experts to assure the quality of referrals and to inform timely decision making.
This guideline is subject to ongoing review on a 24 month basis.
V2.2019
3Guideline for Suspected Cancer Referral in the State of Qatar
Contents
1. Introduction 5
1.1 Purpose of the Guideline 6
2. General Principles of Care 7
2.1 Expectations of compliance with guidelines and process to escalate concerns 9
3. Referral Guidelines and Patient Pathway 10
3.1 Management of Referrals at Hamad Medical Corporation 10
3.2 Management of Referrals at Sidra Medicine 13
3.3 The Patient Referral Pathway in Qatar 15
4. Recommendations Organized by Site of Suspected Cancer 17
4.1 Brain and Central Nervous System Cancers 18
4.2 Breast Cancer 19
4.3 Upper Gastrointestinal Cancers (Oesophageal, Gastric Cancers) 20
4.4 Lower Gastrointestinal Cancers (Colorectal and Anal Cancers) 21
4.5 Gynaecological Cancers 22
4.5.1 Cervical, Uterine, Ovarian, Vulval and Vaginal Cancers 22
4.6 Urological Cancers 24
4.6.1 Bladder and Renal Cancer 24
4.6.2 Testicular Cancer 24
4.6.3 Prostate Cancer 24
4.7 Head and Neck Cancer 25
4.8 Haematological Cancers 26
V2.2019
4 Guideline for Suspected Cancer Referral in the State of Qatar
4.8.1 RED flags for emergency referrals (within 24 hours to the HMC Emergency Room) 26
4.8.2 Leukemia 27
4.8.3 Lymphoma 28
4.8.4 Referral for Multiple Myeloma 29
4.9 Hepatobiliary or Pancreatic Cancer 30
4.10 Lung/Thoracic Cancer 31
4.11 Thyroid Cancer 32
4.12 Sarcoma (Bone and Soft Tissue) 33
4.12.1 Bone Sarcoma 33
4.12.2 Soft Tissue Sarcoma 34
4.13 Skin Cancer 35
4.13.1 Malignant Melanoma of the Skin or Mucosa 35
4.13.2 Squamous Cell Carcinoma and Basal Cell Carcinoma 36
4.13.3 Rare Skin Cancers 37
5 References 38
6 The Guideline Development Group (GDG) 39

V2.2019
5Guideline for Suspected Cancer Referral in the State of Qatar
1. Introduction
Cancer is a leading cause of death globally, with the number of new cases expected to rise by about 70% over the next 2 decades.1-3
The World Health Organization statistics for Qatar in 2018 indicated that the five most common sites of cancer diagnosed in men were colorectum, prostate, leukaemia, lung and non-Hodgkin lymphoma; whilst the breast, colorectum, thyroid, ovarian and non-Hodgkin lymphoma were the five most common sites diagnosed in women.1-2
Cancer has an enormous impact on the people affected by it and also on those close to them. In Qatar, 1466 newly diagnosed cancer cases were reported in 2015.3 The ten most common malignant cancers across all nationalities and genders in 2015 included cancers of the breast, colorectum, prostate, non-Hodgkin lymphoma, leukaemia, thyroid, lung, skin (non-melanoma), liver and brain.3
Each cancer has different presenting features, though they sometimes overlap. Around one third of cancers are associated with the five leading behavioural and dietary risks: high body mass index, low fruit and vegetable intake, lack of physical activity, tobacco use, and alcohol use. Early prevention and detection is known to reduce the risk of mortality with cancers.
Childhood or Paediatric cancers - terms most commonly used to designate cancers that arise in children under the age of 15 years - are rare, representing between 0.5% and 4.6% of all cancers. Overall incidence rates vary between 50 and 200 per million children across the world.1,4 In Qatar, there were 54 newly diagnosed cancer cases in 2015 with the most common cancers including leukemia, brain and non-Hodgkin lymphoma.3

V2.2019
6 Guideline for Suspected Cancer Referral in the State of Qatar
1.1 Purpose of the Guideline
This guideline is intended to aid the recognition of symptom presentation in and/or appropriate timely referral of children, adolescents and adults who may have suspected cancer, by referrers within the primary care, emergency care and private care health services in the State of Qatar.
This guideline is intended as a reference for both public and private healthcare providers to understand what symptoms may suggest a suspected cancer referral in a patient. It is relevant to all healthcare professionals (physicians, nurses, allied health professionals, others) who come into contact with patients with suspected cancer.
It is also expected that this guideline will be of value to those involved in clinical governance across public primary, secondary, tertiary care and private healthcare to help ensure that arrangements are in place to refer and deliver appropriate care to this group of patients.
V2.2019
7Guideline for Suspected Cancer Referral in the State of Qatar
2. General Principles of Care
• Signs and/or symptoms suggestive of cancer require urgent investigation, which may include referral to a specialist team.
• A person presenting with symptoms and/or signs suggestive of cancer should be assessed through a detailed history and examination, irrespective of the presence of risk factors.
• The information given to people with suspected cancer and their families and/or carers should cover:
o where the person is being referred to.
o how long they may have to wait for the appointment.
o what to expect from the service the person will be attending.
o what type of tests may be carried out, and what will happen during diagnostic procedures.
o how long it will take to get a diagnosis or test results.
o whether they can take someone with them to the appointment.
o who to contact if they do not receive confirmation of an appointment.
o how to obtain further information about the type of cancer suspected or help before.
o the specialist appointment (check www.ncp.qa).
• Information that is provided should be appropriate for the person in terms of language, ability and culture, recognizing the potential for different cultural meanings associated with the possibility of cancer.
• Information should be available in a variety of formats on both local and national sources of information for people who are being referred with suspected cancer.
• Healthcare professionals should pay careful attention to caregiver
V2.2019
8 Guideline for Suspected Cancer Referral in the State of Qatar
reports of a child or adolescent’s symptoms. When cancer is suspected in a child or adolescent, discuss the referral decision and information with the parents or carers of the child (and the child/ adolescent if appropriate and where consent has been sought and/or given).
• Adult and paediatric healthcare teams should work jointly to provide assessment and services to young people with suspected cancer.
• When referring a person with suspected cancer to a specialist service, their need for continuing support while waiting for their referral appointment should have been assessed. This should include inviting the person to contact their healthcare professional again if they have more concerns or questions before they see a specialist.
• If additional support needs are identified, these should be highlighted as part of the referral information (with the person’s agreement).
• Once the decision to refer has been made, make sure that the referral is made immediately using the agreed referral processes and proformas. It is expected that the suspected cancer referral pathway is followed.
• Include all appropriate contact information in the urgent referral correspondence.
• Local arrangements are in place to identify people who miss their appointments so that they can be followed up.
V2.2019
9Guideline for Suspected Cancer Referral in the State of Qatar
2.1 Expectations of compliance with guidelines
and process to escalate concerns
It is expected that individuals suspected of having a cancer diagnosis be referred and seen in a timely manner by appropriately trained specialists to ensure effective diagnosis and treatment in accordance with this guidance.
If healthcare providers are concerned that process is not being followed, concerns should be escalated in the following way:
• Concerns related to standard compliance should be submitted in writing to the Director of Licensing, Ministry of Public Health.
• Concerns relating to clinical practice or patient care should be submitted in writing to the Fitness to Practice Team, Qatar Council of Healthcare Practitioners, Ministry of Public Health. A decision will be made in collaboration with the Permanent Licensing Committee as to investigation and subsequent action. Please include the following information:
o Patient name and QID number
o Source of referral or location of incident of concern
V2.2019
10 Guideline for Suspected Cancer Referral in the State of Qatar
3. Referral Guidelines and Patient Pathway
Patients are referred to the various cancer specialist teams from the following providers:
• Primary Healthcare Centres (PHCC) by using the electronic Urgent Suspected Cancer (USC) referral order within Cerner or through submitting a routine referral.
• Any other primary healthcare provider – for example Qatar Red Crescent or Qatar Petroleum.
• Internal HMC referrals from other consultants and the emergency department within HMC.
• Other cancer multi-disciplinary teams (MDTs).
• Sidra Medicine.
• Private providers.
• Clinicians whose patients are returning to Qatar following diagnosis or treatment overseas.
Patients referred to the specialist cancer services should be seen in a specialist clinic by a clinician who has been designated as privileged for that specialty.
3.1 Management of Referrals at Hamad Medical
Corporation
Individuals who present with one or a combination of signs or symptoms of a possible cancer, as outlined in this guidance, should be referred urgently to the appropriate specialty service. Those referred with a suspicion of cancer will be seen in a specialist clinic by a clinician who has been privileged within the appropriate specialty.
V2.2019
11Guideline for Suspected Cancer Referral in the State of Qatar
All referrals are managed by the Referral and Booking Management System (RBMS) at HMC.
Referral process for Cerner enabled users
• Urgent Suspected Cancer referrals can be found by searching for individual USC referrals by Tumor group or in the USC referral folder.
• The appropriate Tumor group referral order should be selected.
• Where selecting the referral opens a form, this must be completed and signed prior to the referral order being placed. The system will prevent the referral order from being processed further unless all mandatory fields in a form (where present) are completed.
• Any tests advised in this guidance should be undertaken prior to referral.
Referral process for non-Cerner enabled users
• Complete the Urgent Suspected Cancer form (available at www.ncp.qa).
• Email with referral to [email protected] and the patient will be given an appointment.
• Please refer to the suspected cancer specific pages of this document and complete any advised tests or investigations prior to referral.
Direct referral to Multi-Disciplinary Team (MDT) at HMC
Direct referral to a cancer MDT is appropriate in the following cases:
• Patients who are returning to Qatar following a diagnosis or treatment overseas.
• Patients diagnosed outside HMC (e.g. incidental findings in other providers).
• Incidental findings within HMC (with positive radiology or pathology results).
V2.2019
12 Guideline for Suspected Cancer Referral in the State of Qatar
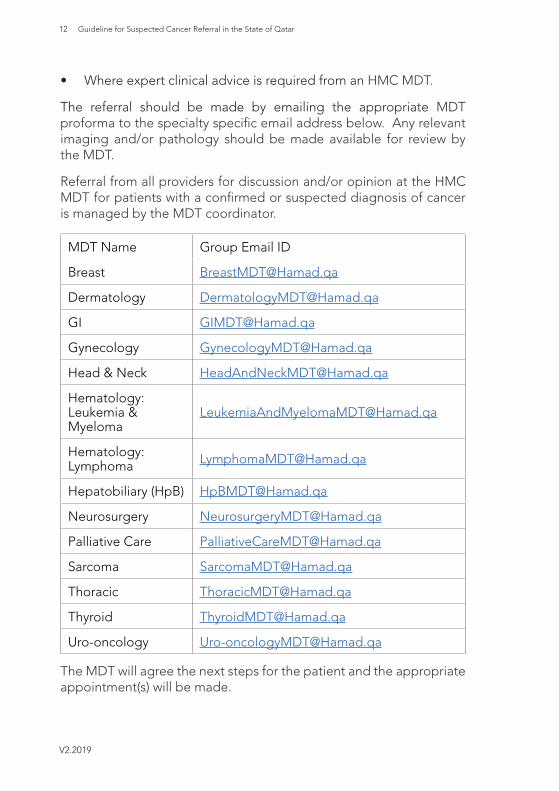
• Where expert clinical advice is required from an HMC MDT.
The referral should be made by emailing the appropriate MDT proforma to the specialty specific email address below. Any relevant imaging and/or pathology should be made available for review by the MDT.
Referral from all providers for discussion and/or opinion at the HMC MDT for patients with a confirmed or suspected diagnosis of cancer is managed by the MDT coordinator.
MDT Name Group Email ID
Breast [email protected]
Dermatology [email protected]
Gynecology [email protected]
Head & Neck [email protected]
Hematology: Leukemia & Myeloma
Hematology: Lymphoma [email protected]
Hepatobiliary (HpB) [email protected]
Neurosurgery [email protected]
Palliative Care [email protected]
Sarcoma [email protected]
Thoracic [email protected]
Thyroid [email protected]
Uro-oncology [email protected]
The MDT will agree the next steps for the patient and the appropriate appointment(s) will be made.
V2.2019
13Guideline for Suspected Cancer Referral in the State of Qatar
The patient pathway coordinator will facilitate access to the required service(s). The outcome of the discussion at the MDT will be added to the patient record in Cerner which will enable the referring physician (PHCC or HMC) to review the proposed plan of care.
Feedback to other referring providers will be communicated within a mutually agreed format.
3.2 Management of Referrals at Sidra Medicine
Adolescents and children who present with one or a combination of signs or symptoms of a possible cancer, as outlined in this guidance, should be referred urgently to the oncology service at Sidra Medicine. Those referred with a suspicion of cancer will be seen in a specialist clinic by a clinician who has been privileged within the appropriate specialty.
Sidra Medicine is unable to receive electronic referrals within the Cerner system at this time.
Referral process
Step 1: Download a Sidra Medicine Referral Form. https://www.sidra.org/documents/referral-form-fillable.pdf If necessary to use Hamad Medical Corporation (HMC) referral forms, please mark them ‘For Sidra’, for efficiency.
Step 2: Complete all required fields, including a distinctive Reason for Referral, and a clinically justifiable level of Priority, the patient’s contact details, and the referring doctor’s name, signature and contact details. Please use clearly legible handwriting, and indicate clinical service for referral, and document appropriate clinical history to justify the requested imaging exams.
Step 3: Print three copies; one each for Sidra Medicine, the patient, and the referrer.
Step 4: Sign, stamp, and date the hard copy for Sidra Medicine.
V2.2019
14 Guideline for Suspected Cancer Referral in the State of Qatar
Step 5: Fax copy to +974 4003 6024, and diagnostic imaging referral forms to [email protected]. If necessary, you can e-mail it to [email protected], or courier it to the Barwa Referral Booking Management Office.
Direct referral to Multi-Disciplinary Team (MDT) at Sidra Medicine
Direct referral to a cancer MDT is appropriate in the following cases:
• Patients who are returning to Qatar following a diagnosis or treatment overseas.
• Patients diagnosed outside of Sidra Medicine (e.g. incidental findings in other providers).
• Where expert clinical advice is required from the paediatric MDT.
• The referral should be made by emailing the appropriate MDT proforma to the email address below. Any relevant imaging and/or pathology should be made available for review by the MDT.
• Referral from all providers for discussion and/or opinion at the Sidra MDT for patients with a confirmed or suspected diagnosis of cancer is managed by the MDT coordinator.
MDT Name Group Email ID
Pediatrics [email protected]
Feedback to referring providers will be communicated within a mutually agreed format.
V2.2019
15Guideline for Suspected Cancer Referral in the State of Qatar
3.3 The Patient Referral Pathway in Qatar
Significant Timelines in the Patient Referral Pathway
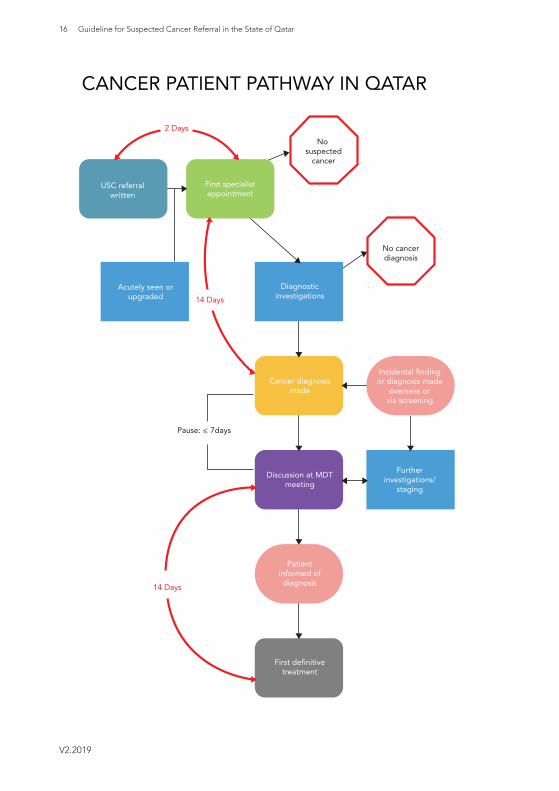
• Referral to Specialist Clinic:
Those referred with an urgent suspected cancer should be seen within 2 working days of the referral being written. This applies to any patient referred with an urgent suspected cancer, regardless of the referral source.
• Time to Definitive Diagnosis:
Once a patient has been seen, a definitive diagnosis should be reached in 14 days using imaging, pathology and/or physical examinations. Every cancer diagnosis must subsequently be discussed at the appropriate multidisciplinary team (MDT) meeting. This applies to any patient seen in a specialist clinic and found to have a diagnosis of cancer, regardless of the referral route.
• Time to Treatment:
There must be no more than 14 days between the date of the patient is first discussed at an MDT and the date of first definitive treatment. This applies to any patient who has a confirmed diagnosis of cancer, regardless of the referral route.
The following diagram (Figure 1) presents an overview of how urgent suspected cancer referrals are managed:
V2.2019
16 Guideline for Suspected Cancer Referral in the State of Qatar
CANCER PATIENT PATHWAY IN QATAR
USC referralwritten
First specialistappointment
Acutely seen orupgraded
Diagnosticinvestigations
No suspected
cancer
No cancerdiagnosis
Cancer diagnosismade
Incidental findingor diagnosis made
overseas orvia screening
Furtherinvestigations/
staging
Discussion at MDTmeeting
Patientinformed ofdiagnosis
First definitivetreatment
2 Days
14 Days
14 Days
V2.2019
17Guideline for Suspected Cancer Referral in the State of Qatar
4. Recommendations Organized by Site of Suspected Cancer
The referral recommendations in this guideline have been organised to help healthcare professionals find the relevant information easily. This section includes the recommendations for referral organised by the site of suspected cancer.
People should be referred using the urgent suspected cancer referral pathway (for an appointment with a specialist within 2 working days) if they present with certain signs and symptoms as listed in the cancer sites below.
Criteria for referral within other clinically appropriate timeframes are also listed for some cancer sites.
V2.2019
18 Guideline for Suspected Cancer Referral in the State of Qatar
4.1 Brain and Central Nervous System Cancers
Adults with any of the following:
• Presenting with symptoms related to the CNS
• Progressive neurological deficit weakness of limbs
• New onset of seizures, headaches, mental changes
• Cranial nerve palsy
• Unilateral sensorineural deafness
• Changes in vision without ophthalmological reason
• Presenting with headaches of recent onset accompanied by features suggestive of raised intracranial pressure (vomiting, drowsiness, postural related headache, headache with pulse synchronous tinnitus) or other focal or non-focal neurological symptoms (blackout, change in personality or memory).
Children and Adolescents
• Newly abnormal cerebellar or other central neurological function
• New onset of persistent headaches and/or unexplained persistent vomiting
• Reduced cognitive function
• New onset of seizures, headaches, mental changes
V2.2019
19Guideline for Suspected Cancer Referral in the State of Qatar
4.2 Breast Cancer
• New, discrete lump in the breast or axilla (with or without pain).
• Altered breast contour/dimpling
• Persistent asymmetrical nodularity/ thickening
• Breast abscess/ inflammation not responsive to one course of antibiotics
• Bloodstained, spontaneous nipple discharge
• Recent nipple retraction/ distortion or eczema suspected Paget’s disease
• Abnormal Mammogram (BIRADS 4 or more)
V2.2019
20 Guideline for Suspected Cancer Referral in the State of Qatar
4.3 Upper Gastrointestinal Cancers (Oesophageal, Gastric Cancers
• Persistent dysphagia
• Persistent vomiting
• Epigastric mass
• Progressive unexplained unintentional weight loss
• Chronic gastrointestinal (GI) bleeding.
• Unexplained iron deficiency anaemia*
• Positive occult blood in stool.
• Patients aged over 40 years with unexplained persistent recent onset dyspepsia (> 6-8 weeks).
* Unexplained iron deficiency anaemia means unrelated to other sources of blood loss, for example, heavy menstrual bleeding, non-steroidal anti-inflammatory drug treatment or blood dyscrasia.

V2.2019
21Guideline for Suspected Cancer Referral in the State of Qatar
4.4 Lower Gastrointestinal Cancers (Colorectal and Anal Cancers)
• A man of any age with unexplained iron deficiency anaemia and a haemoglobin level of 11g/dL or below.
• A non-menstruating woman with unexplained iron deficiency anaemia and a haemoglobin level of 10g/dL or below.
• Patients aged 40 years and over with:
� Rectal bleeding and change in bowel habit which is defined as change to loose stools and/or increased or decreased frequency of defecation persisting for 2 weeks or more
� Rectal bleeding persisting 2 weeks or more without change in bowel habit, as defined above, or anal symptoms.
• Change in bowel habit, as defined above, for 2 weeks or more.
• Palpable rectal mass.
• Abdominal mass consistent with involvement of the large bowel.
• Progressive unintentional weight loss.
• Unexplained anal mass or unexplained anal ulceration.
• Strong family history of bowel cancer, one or more 1st degree or two or more 2nd degree relatives.
V2.2019
22 Guideline for Suspected Cancer Referral in the State of Qatar
4.5 Gynaecological Cancers
4.5.1 Cervical, Uterine, Ovarian, Vulval and Vaginal Cancers
Criteria for urgent referral within 5 working days:
• Post-menopausal bleeding
• Biopsy or cytology suggestive of invasive disease
• Radiological findings strongly suspicious of invasive malignancy
• Abnormal Cervix with appearance suspicious for cancer
• Any mass in vulva or vagina that is thought to represent malignancy
• Ovarian mass with risk of malignancy index (RMI) >200 - PLEASE SEE RMI CALCULATOR BELOW
Criteria for referral within 10 working days for further evaluation in the gynaeoncology clinic:
• Abnormal high grade cervical smear such as:
� HSIL (High-grade squamous intraepithelial lesion),
� ASC-H (Atypical Squamous Cells, cannot rule out high-grade
� Squamous Intra-epithelial Lesion
� AGC (atypical glandular cells)
• LSIL (Low-grade squamous intraepithelial lesion)
• Irregular bleeding in a woman on hormone replacement therapy (HRT) or in peri-menopausal patient
• Purulent or bloodstained vaginal discharge in a post menopausal woman
• Women with RMI 100 – 200 (Intermediate risk) - PLEASE SEE RMI CALCULATOR BELOW
V2.2019
23Guideline for Suspected Cancer Referral in the State of Qatar
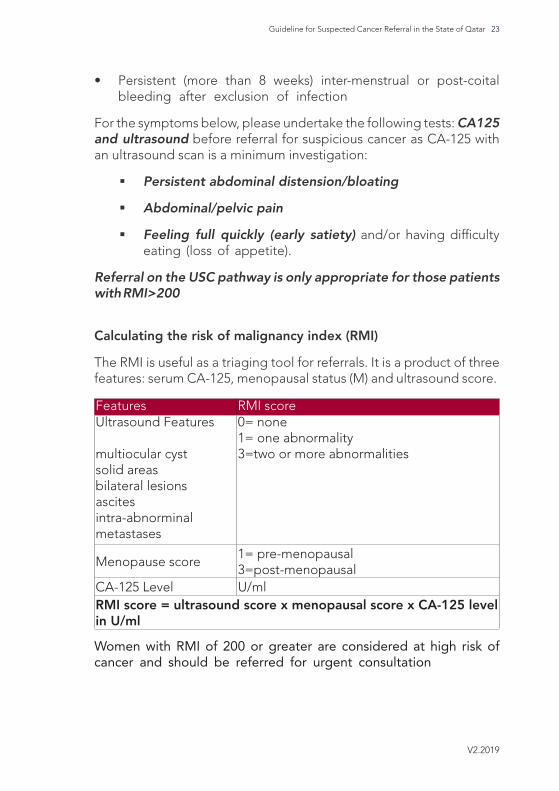
• Persistent (more than 8 weeks) inter-menstrual or post-coital bleeding after exclusion of infection
For the symptoms below, please undertake the following tests: CA125 and ultrasound before referral for suspicious cancer as CA-125 with an ultrasound scan is a minimum investigation:
� Persistent abdominal distension/bloating
� Abdominal/pelvic pain
� Feeling full quickly (early satiety) and/or having difficulty eating (loss of appetite).
Referral on the USC pathway is only appropriate for those patients with RMI>200
Calculating the risk of malignancy index (RMI)
The RMI is useful as a triaging tool for referrals. It is a product of three features: serum CA-125, menopausal status (M) and ultrasound score.
RMI scoreFeatures0= none1= one abnormality3=two or more abnormalities
Ultrasound Features
multiocular cystsolid areasbilateral lesionsascitesintra-abnorminalmetastases
1= pre-menopausal3=post-menopausal
Menopause score
U/mlCA-125 LevelRMI score = ultrasound score x menopausal score x CA-125 level in U/ml
Women with RMI of 200 or greater are considered at high risk of cancer and should be referred for urgent consultation
V2.2019
24 Guideline for Suspected Cancer Referral in the State of Qatar
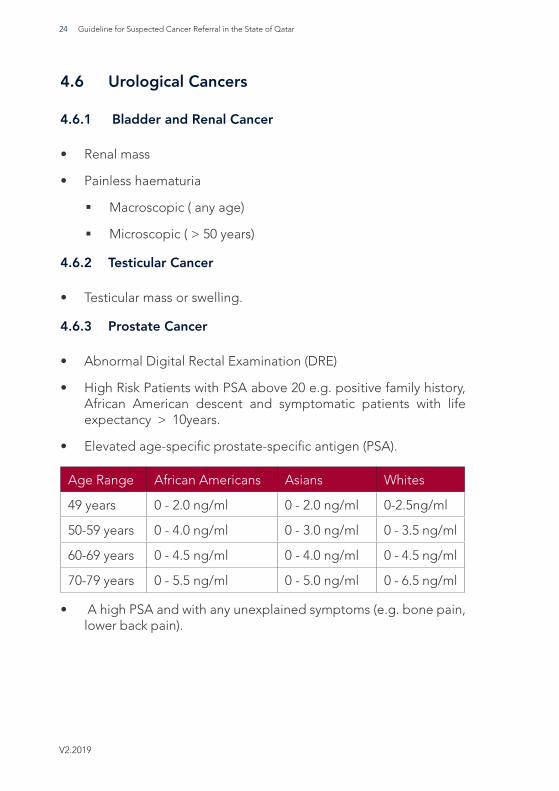
4.6 Urological Cancers
4.6.1 Bladder and Renal Cancer
• Renal mass
• Painless haematuria
� Macroscopic ( any age)
� Microscopic ( > 50 years)
4.6.2 Testicular Cancer
• Testicular mass or swelling.
4.6.3 Prostate Cancer
• Abnormal Digital Rectal Examination (DRE)
• High Risk Patients with PSA above 20 e.g. positive family history, African American descent and symptomatic patients with life expectancy > 10years.
• Elevated age-specific prostate-specific antigen (PSA).
WhitesAsiansAfrican AmericansAge Range
0-2.5ng/ml0 - 2.0 ng/ml0 - 2.0 ng/ml49 years
0 - 3.5 ng/ml0 - 3.0 ng/ml0 - 4.0 ng/ml50-59 years
0 - 4.5 ng/ml0 - 4.0 ng/ml0 - 4.5 ng/ml60-69 years
0 - 6.5 ng/ml0 - 5.0 ng/ml0 - 5.5 ng/ml70-79 years
• A high PSA and with any unexplained symptoms (e.g. bone pain, lower back pain).
V2.2019
25Guideline for Suspected Cancer Referral in the State of Qatar
4.7 Head and Neck Cancer
• Persistent unexplained hoarseness for more than 4 weeks.
• Unexplained ulceration of skin and mucosa of the head and neck persisting for more than 2 weeks.
• Head and neck swellings persisting for more than 2 weeks despite medical treatment.
• All red or white suspicious patches of the oral mucosa persisting for more than 3 weeks.
• Unilateral nasal obstruction, particularly when associated with bloody discharge persisting for more than 3 weeks.
• Dysphagia persisting for more than 3 weeks (not responding to medical treatment).
• Unexplained sensory or motor deficits in the cranial, maxillo-facial domain.
• Orbital extra global masses and lesions.
• Tooth mobility that cannot be otherwise explained persisting for more than 3 weeks.
• Unexplained unilateral hearing loss in an adult.
V2.2019
26 Guideline for Suspected Cancer Referral in the State of Qatar
4.8 Haematological Cancers
Suspected haematological cancers in adults should be referred to the Emergency department of HMC.
Suspected haematological cancers in children and adolescents should be referred to Sidra Medicine.
Any patient with haematological disease should have the following tests done immediately before referral to either HMC or Sidra Medicine:
• Complete blood count (CBC)
• Peripheral smear
• +/- Chest X-ray (if any respiratory symptoms)
4.8.1 RED flags for emergency referrals (within 24 hours to the HMC / Sidra Emergency Room)
• New suspected Acute Leukaemia (based on blood film report).
• Neurologic symptoms with abnormal CBC (polycythemia, severe anaemia <8 grams/ dL).
• Wide mediastinum by chest X-ray.
• Hypercalcemia with increased total protein.
• Patients with multiple myeloma with suspected spinal cord compression.
• Patients with platelets <20 x 109/L or active bleeding with thrombocytopenia.
• Neutrophils < 0.5 x 109/L (significant risk of serious infection).
• Leucoerythroblastic anaemia (based on blood film report).
• New suspected chronic myeloid leukaemia (based on blood film report).
V2.2019
27Guideline for Suspected Cancer Referral in the State of Qatar
• Thrombocytosis associated with recent arterial or venous thrombosis and/or bleeding.
• Polycythaemia in association with recent arterial or venous thrombosis and/or bleeding.
Patients who do not present with the red flag symptoms can be referred to NCCCR / Sidra Haematological clinic within 2 weeks.
4.8.2 Leukemia
Request urgent blood count (within 24 hours) with peripheral smear to assess for leukaemia in children, adolescents and adults with any of the following:
• Pallor
• Persistent fatigue
• Unexplained fever
• Unexplained persistent infection
• Generalised lymphadenopathy
• Persistent or unexplained bone pain
• Unexplained bruising
• Unexplained bleeding
Refer if there is:
• Abnormal Full Blood Count / Blood Film suggestive of leukaemia.
• Unexplained persistent or recurrent infections.
• Unexplained bruising, bleeding or petechiae.
V2.2019
28 Guideline for Suspected Cancer Referral in the State of Qatar
4.8.3 Lymphoma
Consider a suspected cancer pathway referral (for an appointment within 48 hours) for lymphoma in children, adolescent and adults presenting with:
• Unexplained lymphadenopathy or splenomegaly.
• Lymphadenopathy which persists for more than 6 weeks or where lymph nodes are larger than 2cm or are increasing in size.
• Associated symptoms include:
� Fever
� Night sweats
� Pruritus
� Shortness of breath
� Weight loss
Lymphadenopathy should be managed at the corresponding surgical specialty (cervical lymph node to head and neck surgery; axillary lymph node to general surgery and etc.) for biopsy before referring to haematology even if radiology suggests lymphomas.
NOTE: If CBC or peripheral smear is abnormal in a patient with lymphadenopathy, inform the haematology patient pathway coordinator.
4.8.4 Referral for Multiple Myeloma
• People aged 40 and over with any of the following:
� Persistent bone pain*
� Back pain associated with red flags symptoms (Spinal cord compression)
� Unexplained fracture**
V2.2019
29Guideline for Suspected Cancer Referral in the State of Qatar
*Persistent bone pain is an unexplained extreme tenderness or aching in one or more bones that persists beyond six weeks.
**An Unexplained or pathological fracture usually occurs with normal routine activities and is unexplained by osteoporosis or trauma.
• Offer a full blood count, calcium and total serum protein.
• Urgent protein electrophoresis and a Bence Jones protein urine test (to be performed within 48 hours) to assess for myeloma in people:
� Aged 40 and over with
� Hypercalcemia
� Leucopoenia
� A presentation consistent with possible myeloma
Refer to National Centre for Cancer Care and Research (NCCCR) unless red flag which needs referral to the Emergency Department in HMC:
• Protein electrophoresis suggestive of myeloma
• Urine Bence-Jones protein / electrophoresis suggestive of myeloma
V2.2019
30 Guideline for Suspected Cancer Referral in the State of Qatar
4.9 Hepatobiliary or Pancreatic Cancer
• Progressive jaundice without viral hepatitis
• Progressive jaundice with viral hepatitis
• Painless progressive jaundice with rapid weight loss
• Radiological findings suggestive of either:
o liver lesions or
o pancreatic mass or
o gall bladder mass or
o biliary dilatation or mass.
V2.2019
31Guideline for Suspected Cancer Referral in the State of Qatar
4.10 Lung/Thoracic Cancer
Patients should ONLY be referred using the Urgent Suspected Cancer referral once a chest x-ray has been done which identifies the following:
� Lung nodule
� Mass
� Pleural effusion
� Hilar adenopathy
� Consolidation
Please consider the increased risk of lung cancer in the following circumstances and in the context of an abnormal x-ray. Please highlight any relevant information in your referral:
• Previous exposure to radiation therapy to the chest for other cancer
• Family history of lung cancer or any other malignancies
• The patient has lived in area with high levels of arsenic in drinking water (some areas in southeast Asia or South America)
• Smokers who are taking beta carotene supplements
• Chronic smokers or chronic exposure to second hand smoke (passive smokers)
V2.2019
32 Guideline for Suspected Cancer Referral in the State of Qatar
4.11 Thyroid Cancer
Thyroid carcinoma can occur in any thyroid nodule that has suspicious features radiologically and/or clinically. Patients or clinicians discover most of these nodules during routine palpation of the neck.
Emergency/ Urgent Referrals:
Refer immediately to the Emergency Department if there are acute pressure symptoms; stridor, tracheal compression, breathing difficulties.
Other Referrals
The following can be referred to be seen within a two week timeframe:
• Rapid nodular growth in euthyroid
• Newly discovered thyroid nodule in the following patients:
� Patients older than 60 years and in patients younger than 30 years
• Hard and fixed nodules
• Family history of endocrine tumour (e.g. thyroid, pancreas and parathyroid)
• Unexplained voice changes
• Cervical lymphadenopathy combined with thyroid nodules
• History of neck radiotherapy
V2.2019
33Guideline for Suspected Cancer Referral in the State of Qatar
4.12 Sarcoma (Bone and Soft Tissue)
Suspected sarcomas in children, adolescents and adults should be referred to the Bone and Joint Centre within HMC.
4.12.1 Bone Sarcoma
• Unexplained bone swelling and/or tenderness
• X-ray that is suspicious and showing one or more of the following features:
� Bone lesion (hole in the bone)
� Bone destruction
� Spontaneous (pathological) fracture
� Periosteal elevation
� New bone formation
� Soft tissue swelling
• Normal or equivocal x-ray but high clinical suspicion of bone sarcoma
• Bone pain (including night pain and pain not responding to simple analgesics especially in children).
V2.2019
34 Guideline for Suspected Cancer Referral in the State of Qatar
4.12.2 Soft Tissue Sarcoma
• Unexplained soft tissue mass (lump) with one or more of the following:
� Greater than 5cm in size
� Deep to fascia
� Painful
� Increasing in size
� Fixed ( immobile)
• Abnormal x-ray findings suggestive of sarcoma
� Abnormal soft tissue shadow on x-ray
� Abnormal soft tissue calcification on x-ray
• Unplanned excision of soft tissue sarcoma (Please describe)
• Recurrence following excision (Please describe)
V2.2019
35Guideline for Suspected Cancer Referral in the State of Qatar
4.13 Skin Cancer
The following para neoplastic signs could be signs for internal malignancy and not skin malignancy:
• Persistent pruritus not responding to treatment.
• Acanthosis nigricans of abnormal onset and abnormal distribution.
• Sudden erruptive seborrhoeic keratosis.
4.13.1 Malignant Melanoma of the Skin or Mucosa
• Refer people with a suspicious pigmented or non-pigmented skin lesion with a weighted 7-point checklist score of 3 or more.
• Refer people with a suspicious pigmented or non-pigmented skin lesion and/or when dermoscopy is suggestive of melanoma of the skin or mucosa.
Both the ABCDE rule and the seven point checklist are suitable for use in clinical assessment. (See tables 1 and 2 below).
Table 1 ABCDE of melanoma
A Asymmetry
B Border irregularity
C Colour variation (Note: black is not essential and may not be present in some melanomas, i.e. nodular or amelanotic melanoma)
D Diameter greater than 6mm. However, melanoma can be diagnosed when less than this in diameter
E Evolution and/or elevation e.g. lesions may enlarge and a flat lesion may become raised in a matter of a few weeks
Source: Suspected cancer in primary care. New Zealand Guidelines Group. 2009.
V2.2019
36 Guideline for Suspected Cancer Referral in the State of Qatar
4.13.2 Squamous Cell Carcinoma and Basal Cell Carcinoma
Consider urgent referral for a person presenting with:
• A skin lesion that raises the suspicion of squamous cell carcinoma. Skin lesions suggestive of squamous cell carcinoma are non-healing, keratinizing or crusted lesions with significant induration on palpation, a documented expansion over 8 weeks and are typically on sun exposed skin and may include:
� Lesion with hyperkeratotic warty surface and induration.
� Ulcers arising on previous scar or old burn (Marjolin’s ulcer)
� Bowen’s (SCC in situ) red scaly patch could be itchy in older individuals and may turn into SCC if not treated.
• A skin lesion that raises the suspicion of a basal cell carcinoma if there is particular concern that a delay may have a significant impact, because of factors such as lesion site or size. Basal cell carcinomas are slow growing, usually without significant expansion
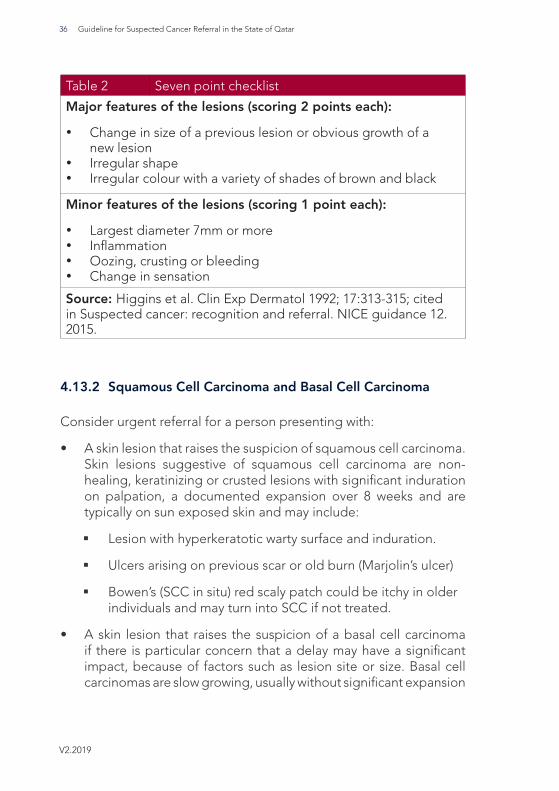
Table 2 Seven point checklist
Major features of the lesions (scoring 2 points each):
· Change in size of a previous lesion or obvious growth of a new lesion
· Irregular shape· Irregular colour with a variety of shades of brown and black
Minor features of the lesions (scoring 1 point each):
· Largest diameter 7mm or more· Inflammation· Oozing, crusting or bleeding· Change in sensation
Source: Higgins et al. Clin Exp Dermatol 1992; 17:313-315; cited in Suspected cancer: recognition and referral. NICE guidance 12. 2015.
V2.2019
37Guideline for Suspected Cancer Referral in the State of Qatar
over 8 weeks. Typical features of basal cell carcinoma include:
� An ulcer with a raised rolled edge;
� Prominent fine blood vessels around a lesion; or
� A nodule on the skin (particularly pearly or waxy nodules)
� Never healing sore or ulcer
� Scar like or morphoeic like telangiectatic patch with vague border
� Pigmented slow growing nodule.
4.13.3 Rare Skin Cancers
• Merkel Cell Carcinoma:
� Firm, shiny, flesh-coloured or bluish-red mass which is asymptomatic (no pain and no tenderness).
� Rapidly growing on sun exposed skin.
• Paget’s disease:
� Mammary pagets involving the nipples and areola
� Extra mammary involving the genital, groin, perianal and appears as red oozing crusting plaque not responding to topical therapy.
• Dermatofibrosarcoma protuberans:
� Soft tissue sarcoma that develops in deep layers of skin.
� Slow growing small, firm patch, nodule; may be purplish, reddish or flesh coloured with high tendency of recurrence after removal. May resemble keloid.
V2.2019
38 Guideline for Suspected Cancer Referral in the State of Qatar
5. References1. The Global Cancer Observatory 2018. Lyon, France: International Agency for Research on Cancer.
2. Qatar National Cancer Registry. Annual Report 2015. Available at [email protected]
3. National Institute for Health and Care Excellence. Suspected Cancer: Recognition and Referral. NG12. June 2015. Available at: www.nice.org.uk/guidance/ng12
4. National Cancer Program. Guidelines for Management of Breast cancer in the State of Qatar. Ministry of Public Health. August 2015. Available at: www.ncp.qa
5. National Cancer Program. Guidelines for Management of Bladder cancer in the State of Qatar. Ministry of Public Health. August 2015. Available at: www.ncp.qa
6. National Cancer Program. Guidelines for Management of Prostate cancer in the State of Qatar. Ministry of Public Health. August 2015. Available at: www.ncp.qa
7. National Cancer Program. Guidelines for Management of Renal cancer in the State of Qatar. Ministry of Public Health. August 2015. Available at: www.ncp.qa
8. National Cancer Program. Guidelines for Management of Testicular cancer in the State of Qatar. Ministry of Public Health. August 2015. Available at: www.ncp.qa
9. National Cancer Program. Guidelines for Management of Upper Gastrointestinal cancer in the State of Qatar. Ministry of Public Health. August 2015. Available at: www.ncp.qa
10. National Cancer Program. Guidelines for Management of Colorectal cancer in the state of Qatar. Ministry of Public Health. August 2015. Available at: www.ncp.qa
11. National Cancer Program. Guidelines for Management of Cervical cancer in the State of Qatar. Ministry of Public Health. December 2015. Available at: www.ncp.qa
12. National Cancer Program. Guidelines for Management of Endometrial cancer in the State of Qatar. Ministry of Public Health. December 2015. Available at: www.ncp.qa
13. National Cancer Program. Guidelines for Management of Ovarian cancer in the State of Qatar. Ministry of Public Health. December 2015. Available at: www.ncp.qa
14. National Cancer Program. Guidelines for Management of Head and Neck cancers in the State of Qatar. Ministry of Public Health. March 2016. Available at: www.ncp.qa
15. Higgins E.M., Hall P.,Todd P., Murthi R. and Du Vivier A.W.P. The application of the seven-point check-list in the assessment of benign pigmented lesions. Clin Exp Dermatol 1992; 17: 313–315. DOI: 10.1111/j.1365-2230.1992.tb00218.x
16. http://www.nice.org.uk/guidance/ng35/chapter/Recommendations#laboratory-investigations
17. https://www.myhealth.london.nhs.uk/nhsrefer/formlinks/guides/Pan%20London%20Suspected%20Cancer%20Referral%20Guide%20Haematology.pdf
18. http://www.londoncancer.org/media/86514/haemguidelines.pdf
19. http://www.southend.nhs.uk/media/22256/referralguidelineshaematology.pdf
20. https://healthygc.com.au/MedicareLocal/media/Site-Pages-Content/GP%20Resources/Haematology/Haematology-GP-Referral-Guidelines-Sept-2015.pdf
21. https://www.moph.gov.qa/health-strategies/Documents/Guidelines/Acute%20Myeloid%20leukemia.pdf
22. Suspected cancer in primary care. New Zealand Guidelines Group. 2009.
V2.2019
39Guideline for Suspected Cancer Referral in the State of Qatar
6. The Guideline Development Group (GDG)
The suspected cancer referral guidelines have been produced with the assistance of the national clinical advisory groups (NCAGs) - a multidisciplinary group of clinicians – who have provided a comprehensive overview of the suspected cancer patient’s journey from referral to timely diagnosis and treatment.
The NCAGs are made up of staff from the following organizations including the Hamad Medical Corporation (HMC), Primary Health Care Corporation (PHCC), and Ministry of Public Health (MOPH). The criteria for each cancer was reviewed, updated and approved by the NCAG of the corresponding cancer. The compiled draft document was subsequently forwarded to all stakeholders for consultation.
Following the consultation period, staff from MOPH finalized the recommendations with support from the Quality and Patient Safety, Fitness to Practice and Facility Licensing and Accreditation teams. The final document approval is granted by the National Cancer Committee (NCC), prior to dissemination across all healthcare providers.
Updating the Guideline
Two years after publication of the guideline, the guideline development group will review the guideline to determine whether the evidence base has progressed significantly to alter the guideline recommendations and warrant an early update.
Disclaimer
The GDG assumes that healthcare professionals will use clinical judgment, knowledge and expertise when deciding whether it is appropriate to apply these guidelines. The recommendations cited here are a guide and may not be appropriate for use in all situations. The decision to adopt any of the recommendations cited here must be made by the practitioner in light of individual patient circumstances, the wishes of the patient and clinical expertise.
The MOPH disclaims any responsibility for damages arising out of the use or non-use of these guidelines and the literature used in support of these guidelines.
V2.2019
40 Guideline for Suspected Cancer Referral in the State of Qatar
في دولــــة قطـر
الدليـــــل ا�رشـــــادي �حــــــالةحاالت ا�شــــتباه بالســــرطان





























