Embed Size (px)
Citation preview

NIH EMERGENCY MEDICINE RESEARCH ROUNDTABLES/SPECIAL CONTRIBUTION
Summary of NIH Medical-Surgical Emergency ResearchRoundtable Held on April 30 to May 1, 2009
Amy H. Kaji, MD, PhD, Roger J. Lewis, MD, PhD, Tony Beavers-May, Robert Berg, MD, Eileen Bulger, MD, Charles Cairns, MD,Clifton Callaway, MD, PhD, Carlos A. Camargo, Jr, MD, DrPH, Joseph Carcillo, MD, Roberta DeBiasi, MD, Tania Diaz, MD,Francine Ducharme, MD, Seth Glickman, MD, MBA, Katherine Heilpern, MD, Robert Hickey, MD, Terry Vanden Hoek, MD,
Judd Hollander, MD, Susan Janson, DSc, Gregory Jurkovich, MD, Arthur Kellermann, MD, MPH, Stephen Kingsmore, MD,Jeffrey Kline, MD, Nathan Kuppermann, MD, MPH, Robert Lowe, MD, MPH, David McLario, DO, MS, Larry Nathanson, MD,
Graham Nichol, MD, MPH, Andrew Peitzman, MD, Lynne Richardson, MD, Arthur Sanders, MD, Manish Shah, MD, MPH,Nathan Shapiro, MD, MPH, Robert Silverman, MD, Martin Than, MD, Scott Wilber, MD, MPH, Donald M. Yealy, MD
Roundtable External Participants and Roundtable Steering Committee and Federal Participants*
Study objective: In 2003, the Institute of Medicine Committee on the Future of Emergency Care in the UnitedStates Health System convened and identified a crisis in emergency care in the United States, including a needto enhance the research base for emergency care. As a result, the National Institutes of Health (NIH) formed anNIH Task Force on Research in Emergency Medicine to enhance NIH support for emergency care research.Members of the NIH Task Force and academic leaders in emergency care participated in 3 roundtablediscussions to prioritize current opportunities for enhancing and conducting emergency care research. Theobjectives of these discussions were to identify key research questions essential to advancing the scientificunderpinnings of emergency care and to discuss the barriers and best means to advance research by exploringthe role of research networks and collaboration between the NIH and the emergency care community.
Methods: The Medical-Surgical Research Roundtable was convened on April 30 to May 1, 2009. Before theroundtable, the emergency care domains to be discussed were selected and experts in each of the fields wereinvited to participate in the roundtable. Domain experts were asked to identify research priorities and challengesand separate them into mechanistic, translational, and clinical categories. After the conference, the lists werecirculated among the participants and revised to reach a consensus.
Results: Emergency care research is characterized by focus on the timing, sequence, and time sensitivity of diseaseprocesses and treatment effects. Rapidly identifying the phenotype and genotype of patients manifesting a specificdisease process and the mechanistic reasons for heterogeneity in outcome are important challenges in emergencycare research. Other research priorities include the need to elucidate the timing, sequence, and duration of causalmolecular and cellular events involved in time-critical illnesses and injuries, and the development of treatmentscapable of halting or reversing them; the need for novel animal models; and the need to understand why there areregional differences in outcome for the same disease processes. Important barriers to emergency care researchinclude a limited number of trained investigators and experienced mentors, limited research infrastructure andsupport, and regulatory hurdles. The science of emergency care may be advanced by facilitating the following:(1) training emergency care investigators with research training programs; (2) developing emergency care clinicalresearch networks; (3) integrating emergency care research into Clinical and Translational Science Awards; (4)developing emergency care–specific initiatives within the existing structure of NIH institutes and centers; (5) involvingemergency specialists in grant review and research advisory processes; (6) supporting learn-phase or small, clinicaltrials; and (7) performing research to address ethical and regulatory issues.
Conclusion: Enhancing the research base supporting the care of medical and surgical emergencies will requireprogress in specific mechanistic, translational, and clinical domains; effective collaboration of academicinvestigators across traditional clinical and scientific boundaries; federal support of research in high-priorityareas; and overcoming limitations in available infrastructure, research training, and access to patientpopulations. [Ann Emerg Med. 2010;56:522-537.]
0196-0644/$-see front matterCopyright © 2010 by the American College of Emergency Physicians.doi:10.1016/j.annemergmed.2010.03.014
*All participants are listed in the Appendix.
522 Annals of Emergency Medicine Volume , . : November

Kaji et al NIH Medical-Surgical Emergency Research Roundtable
SEE RELATED ARTICLES AND EDITORIALS,P. 538, 551, 565, 568.
INTRODUCTIONThe Institute of Medicine Committee on the Future of
Emergency Care in the United States Health System wasconvened in 2003 and charged with evaluating the currentemergency care system, creating a vision for the future ofemergency care and recommending strategies for achieving thatvision. Three reports were completed in June 2006,1-3
evaluating the current emergency care system. The Institute ofMedicine reports identify enhancing the emergency careresearch base as a key priority and identify steps to be taken byacademic medical centers, federal agencies, states, and Congressto achieve this. Specifically, the report recommends that “theSecretary of the Department of Health and Human Servicesconduct a study to examine the gaps and opportunities inemergency and trauma care research, and recommend a strategyfor the optimal organization and funding of the researcheffort.”1
In response to the Institute of Medicine report, personnelfrom the National Institutes of Health (NIH) formed an NIHTask Force on Research in Emergency Medicine to enhanceNIH support for emergency care research. Members of the NIHTask Force and academic leaders in emergency care participatedin 3 roundtable discussions to prioritize current opportunitiesfor enhancing and conducting emergency care research: (1)neurological and psychiatric emergencies (December 2008); (2)medical-surgical emergencies (April 2009); and (3) traumaemergencies (June 2009). The objectives of these roundtableswere to identify key research questions essential to advancingthe scientific underpinnings of emergency care and to discussthe barriers and best means to advance research by exploring therole of networks and collaboration between NIH and theemergency care community. Specific goals included facilitatingthe training of the next generation of emergency careresearchers, encouraging emergency care research discussionsduring review and grant processes, and increasing emergencyfunding through Clinical and Translational Science Award andtrans-NIH support.
The following document is a summary of the 2-dayroundtable discussion on medical-surgical emergencies, held onApril 30 to May 1, 2009. The key objectives of the meeting arelisted in Figure 1.
SCOPE OF EMERGENCY CARE ANDEMERGENCY CARE RESEARCH
The scope of emergency care is broad. There are anestimated 120 million patient emergency department (ED)visits per year in the United States, comprising a diversepopulation that includes pediatric, geriatric, medicallyunderserved, and minorities, as well as those with acute illness,exacerbation of chronic illnesses, and injuries. In concert with
the broad range of ED patients, emergency care researchVolume , . : November
domains are broad in scope, covering broad ranges in the timingand scale of the entities being studied (Figure 2).4
Emergency care research spans time-sensitive, emergencycare, as well as chronic care, individual organ systems, wholehealth care systems, and population health. One proposedfundamental hypothesis of emergency care research is that“rapid diagnosis and early intervention in acute illness [andinjury] or acutely decompensated chronic illness improvespatient outcomes.”5 Consistent with this hypothesis, there are anumber of ED interventions that have been shown to reducemortality and improve outcomes for patients with acute, time-sensitive illness or injury (Figure 3).
BARRIERS AND CHALLENGES TO EMERGENCYCARE RESEARCH
The Institute of Medicine also identified the importantbarriers to emergency care research. First, it was observed thatthere is a shortage of adequately trained laboratory, clinical, andhealth services investigators. Few emergency physicians have
1. To define the scope of emergency care and emergencycare research
2. To identify the challenges and gaps broadly inemergency care research
3. To describe the role of research networks in emergencycare research
4. To describe the current level of NIH funding foremergency care research, as well as the barriers tofunding
5. To identify challenges and gaps in selected domains ofthe medical and surgical subfields of emergency careresearch
Figure 1. Key objectives for medical-surgical emergencyroundtable.
Figure 2. Examples of emergency care research domains.
undergone rigorous research training because there are few role
Annals of Emergency Medicine 523

NIH Medical-Surgical Emergency Research Roundtable Kaji et al
models and departments with substantive trainingopportunities. Most departmental research directors are juniorfaculty, and relatively few have undergone formal fellowshiptraining or have NIH funding.6,7 Second, there is inadequateprotected time for research, poorly defined research-based careertracks, and professional incentives that distract investigatorsfrom research-based careers. Departments of emergencymedicine often have a culture in which clinical care is valuedover research. Emergency medicine departments often lack thenecessary infrastructure (laboratory space, technical supportpersonnel, etc), and few departments of emergency medicineoffer significant protected research time. Third, there are aninadequate number of interdisciplinary research collaborationsand multi-institutional networks. There are also significant gapsin data linkages and standardization of clinical care andinformation systems. For example, there is a need for linkagesand alliances between the care systems of emergency medicalservices (EMS) and specialty services such as critical care,medicine, and surgery. Finally, funding streams are bothinadequate and frequently aligned across disease-specificboundaries that are minimally relevant in the emergency caresetting. Given the nonspecific nature of symptomatic andsyndromic presentations of ED patients, it is often difficult toclassify important, syndrome-based emergency care researchwith the NIH organizational structure, which is disease centered(eg, National Institute of Neurological Disorders and Stroke),organ centered (eg, National Heart, Lung, and Blood Institute),life stage centered (eg, National Institute of Child Health andHuman Development, National Institute on Aging), scientificdiscipline based (eg, National Human Genome ResearchInstitute), or profession based (eg, National Institute of NursingResearch, National Institute of Biomedical Imaging andBioengineering).
Using a mechanistic, translational, and clinical organizational
1. Timely administration of aspirin and fibrinolytictherapy for acute myocardial infarction
2. Percutaneous coronary intervention within 90 min forST-segment elevation myocardial infarction
3. Appropriate empiric antibiotic administration within4-6 h for pneumonia
4. Early goal-directed therapy for sepsis5. Blood pressure management for both ischemic and
hemorrhagic stroke6. Therapeutic hypothermia for adults with ventricular
fibrillation–induced cardiac arrest7. Administration of antibiotics for open fractures8. Administration of antidotes, such as N-acetylcysteine
for acetaminophen poisoning
Figure 3. ED interventions that reduce mortality andimprove outcomes.
framework, the meeting participants identified gaps and
524 Annals of Emergency Medicine
challenges in emergency care and research. Although themeaning and importance of the clinical framework may beobvious, mechanistic research focuses on the timing, sequence,and duration of causal molecular and physiologic events in acuteillness and injury, with the goal of identifying and evaluatingpotential diagnostic methods and therapeutic strategies.Mechanistic research will thus be furthered by developingclinically relevant animal models. In contrast, the first stage oftranslational research focuses on the application of mechanisticknowledge in the clinical environment. This may includeidentifying clinically feasible therapeutic strategies, outliningclear definitions of therapeutic windows, and improving theefficiency, accuracy, and cost-effectiveness of diagnostictechniques in the ED. Challenges in conducting translationalresearch include the need to rapidly phenotype acute carepatients and utilize novel biomarkers and noninvasivemonitoring and imaging techniques and real-time, bedsidemeasurement techniques. Clinical research includes traditionalresearch and health services research.
Substantial regulatory barriers to emergency care researchexist. Although the emergency exception from informed consentfor resuscitation research (21CFR §50.24) was created tofacilitate emergency care research, obtaining communityconsultation is resource and labor intensive. Most localinstitutional review boards do not have experience with theemergency exception from informed consent, and local statelaws (eg, California) may preempt its use. Additionally, theFederalwide Assurance program may discourage nonresearchentities (eg, EMS agencies, community hospitals) fromparticipating in NIH-funded research. Other barriers toemergency care research also exist. Small clinical trials, whichmay be successfully performed in a single or few EDs, often farepoorly in peer review and may be criticized as being only “pilotstudies.” Yet, small trials are critical for hypothesis generation(ie, “learn phase” trials) and are an essential part of an explicit,well-considered, efficient, therapeutic research strategy. Smalltrials also exemplify research that benefits from the use ofinnovative statistical techniques, such as adaptive clinical trialdesign. An adaptive clinical trial design allows one to makeplanned, well-defined changes in key clinical design parametersduring trial execution, according to data from that trial toachieve goals of increased validity, efficiency, and safety.
ROLE OF NETWORKS IN EMERGENCY CARERESEARCH
The purpose of a clinical research network is to provideessential infrastructure and project support for clinical trials andother outcome-oriented research. By capitalizing on thecombined resources of member institutions and by focusing onthe rapid translation of promising scientific knowledge intoclinical advances, networks can efficiently conduct trials ofvariable sizes and duration. With a research infrastructurealready in place, there is improved access to larger and morediverse patient populations and the ability to recruit more
patients in a shorter period, as well as increased efficiencies inVolume , . : November

Kaji et al NIH Medical-Surgical Emergency Research Roundtable
development, review, and implementation. The time from ideaconception to project start is thus decreased. For example, inone emergency care network, the time required for the reviewprocess decreased from approximately 16 months to 7 monthsfor protocols developed within the network compared withthose developed externally. Another benefit of multicenterresearch networks is the increased generalizability of results.
Emergency care clinical research networks have otheradvantages, as well. Many diseases observed in the emergencycare setting have relatively low incidence rates (eg, cervical spineinjuries, serious medication errors), and thus large numbers ofpatients must be screened to obtain sufficient, representativestudy populations. To successfully translate research findingsinto the treatment setting, a well-established infrastructure, suchas a research network, is helpful. Last, research networksimprove research efficiency, reducing the marginal costsassociated with implementing a new study, and funding for aresearch study is easier to obtain if research infrastructure isalready in place. Examples of successful emergency medicineresearch networks are listed in Figure 4.
Developing, maintaining, and utilizing clinical researchnetworks also present challenges. Multicenter research is morecomplex than single-center research. Data transmission betweensites is complicated by security issues. Each site’s institutionalreview board may have different submission requirements andstandards. Furthermore, institutional review boards around theUnited States are generally overburdened and may requireextended periods to review and approve protocols. Onepotential solution to the institutional review board–associatedinefficiencies is to create a central institutional review board formulticenter studies, associated with a particular network.Reviewing only a few protocols per month, the centralinstitutional review board may facilitate brief reviews at the locallevel, allowing the local institutional review boards to decidelocal issues. Large research networks also require greaternumbers of personnel, including investigators, statisticians, andresearch coordinators, and such personnel may be in shortsupply. With large numbers of investigators, it is difficult tobalance the numbers of junior and senior investigators.Maintaining high quality is also difficult, requiring multiple sitemonitors, standardization processes, and uniform training acrosssites. Multicenter studies are also expensive annually, and thereare federal funding caps. After distributing funds to greater than20 sites, there may be very little allocated to each site. It is alsodifficult to track network resources. Each site must ensure thetraining of investigators and staff, have an explicit protocol, andadhere to uniform standards for clinical research and sitemonitoring. With a network, it may be difficult to discern whois actually in charge. Is it the principal investigator, the fundingagency, the steering committee, or the data coordinating center?In publishing studies, because of the number of potentialauthors and investigators, authorship and attribution of credit
are complicated, as well.Volume , . : November
NIH FUNDING OF EMERGENCY CARERESEARCH
The NIH scientific review process involves a dual system forevaluating grant applications. The first level of review occurs atthe Center for Scientific Review or NIH institute and isconducted by the assigned scrientific review group or studysection. The second level of review occurs at the council of theNIH institute or center. When applications appear to beappropriate for more than one institute or center, multipleassignments may be made. Initially, grant applications arereferred to an institute or a center according to a match betweenthe research proposed and the overall mission of the institute orcenter. Each institute or center has established guidelines forreferring specific scientific topics within its mission to reviewgroups or study sections. When the subject matter of theapplication matches the referral guidelines for the study section,the application is sent to a standing Center for Scientific Reviewstudy section. However, when the subject matter does not fit
1. EMERGEncy ID Net: Focus is syndromic surveillanceand research of emerging infections in the UnitedStates, and it comprises 12 geographically diverseurban EDs.
2. Emergency Medicine Network (EMNet): Began as theMulticenter Airway Research Collaboration (MARC),with a focus on respiratory/allergy emergencies, butthen expanded its focus to include health policy, anddiverse public health objectives; it comprises 204medical centers. http://www.emnet-usa.org
3. Neurological Emergency Treatment Trials (NETT):Focus is interventional trials on acute neurologicdisorders, and it is organized around a clinicalcoordinating center with 10 to 20 clinical “hubs.”http://nett.umich.edu/nett/welcome
4. Pediatric Emergency Care Applied Research Network(PECARN): Focus is observational and randomizedtrials for acute illnesses and injuries in children, and itcomprises 4 research “nodes” with 22 participatingsites. http://www.pecarn.org
5. Resuscitation Outcomes Consortium (ROC): Focus ison out-of-hospital research in management ofcardiopulmonary arrest and severe traumatic injurybeing conducted in more than 10 regional centersacross North America. http://roc.uwctc.org/tiki/tiki-index.php
6. US Critical Illness and Injuries Trial Group(USCIITG): Focus is to establish priorities for criticalillness injury research. http://public.wudosis.wustl.edu/USCIITG/default.aspx
Figure 4. Examples of successful emergency researchnetworks.
into any study section or there is a potential conflict of interest,
Annals of Emergency Medicine 525

NIH Medical-Surgical Emergency Research Roundtable Kaji et al
the application is sent to an Ad Hoc Special Emphasis Panel.Emergency care applications are mainly reviewed in 4 studysections: Brain Disorders and Clinical Neurosciences, SurgicalSciences, Biomedical Imaging and Bioengineering, andCardiovascular and Respiratory Sciences.
An analysis of NIH funding of emergency care research wasperformed by NIH personnel to identify NIH-funded studiesthat were directly related, or potentially related, to emergencycare in the following 7 topic areas: sepsis, cardiac, centralnervous system, general emergency care, respiratory, abdominal,and burns. Three fiscal years were selected for analysis: 1999,2004, and 2009. The majority of identified awards fell into thegeneral emergency care subcategory. NIH personnelencountered difficulty in navigating the Computer Retrieval ofInformation on Scientific Projects (CRISP) database, andamong the list of apparent emergency care–related researchfound by using the above search strategy, there were very fewprojects that were actually found to be directly relevant toemergency care. Thus, it is difficult to assess how wellemergency care–related research is funded without an accurateestimate of the numbers of emergency care–related projects.Because of the limitations in the CRISP database, the NIH isshifting away from using it to determine the level of emergencycare–related funding. NIH personnel are continuing to refine asearch strategy for providing a valid estimate of current NIHfunding for emergency care–related research.
MEDICAL AND SURGICAL TOPIC-SPECIFICGAPS AND PRIORITIES IN EMERGENCY CARERESEARCH
The remainder of the conference focused on identifyingmechanistic, translational, and clinical emergency care researchpriorities and challenges in the following topic areas: (1)infection, sepsis, and septic shock; (2) respiratory/allergyemergencies; (3) clinical informatics; (4) health services research;(5) cardiac resuscitation; (6) hypotension and ischemia/reperfusion of the heart; (7) acute chest pain; (8) acuteabdominal pain; and (9) geriatrics. Research priorities that wereidentified as common across all areas are listed in Figure 5.Specific mechanistic, translational, and clinical researchpriorities are briefly summarized below.
Infection, Sepsis and Septic ShockMechanistic: The cellular and subcellular factors that
influence and predict the host response to infection early duringillness warrant better delineation. Describing the responses tointerventions at the organism, cellular, and subcellular level isrequired to yield a better understanding of how and whytherapeutic interventions produce disparate responses amongdifferent hosts. A long-term objective should be to create animalmodels of acute illness that better reflect the full spectrum ofhuman clinical phenotypes, from the very young to the very old,and for those with comorbidities.
Translational: Research is needed to identify early
characteristics of those who have sepsis, those who will develop526 Annals of Emergency Medicine
sepsis, and those who will have adverse outcomes from sepsis,using clinical, biomarker, genetic, or other novel strategies.Because of the time-sensitive nature of these diagnoses,approaches that may yield immediate results at the bedside areneeded. There is also a need for acute “theragnostics”: combinedtherapeutic and diagnostic strategies, allowing clinicians toassess responses to therapy to guide diagnosis and additionaltreatment through feedback loops. Theragnostics also includesthe goal of identifying which patients need which anti-infectives, using targeted approaches that avoid unnecessarydrug adverse effects and the development of antimicrobialresistance.
Clinical: The infection/sepsis phenotypes presenting in theED warrant better characterization, and there is a need forstandardized definitions and clinical research networks focusingon sepsis. Comparative effectiveness studies to determine thebest interventions in routine clinical practice are also needed.After scientific discoveries are made, the most effective methodsof knowledge transfer to the broad medical community need tobe identified and be implemented. Similar to trauma systems ofcare for trauma patients, shock/sepsis systems should beinvestigated as a way to improve the care and outcome of septicpatients. National standards and guidelines to ease consent andenrollment barriers need to be developed because currentwaiver/exemption criteria hinder research in the treatment ofcritically ill patients with sepsis and septic shock.
Respiratory/Allergy EmergenciesMechanistic: Some of the immediate opportunities for
research in this area include identifying major mechanisticcontributors to acute airway obstruction and clarifying thepathophysiology of “poor responders” to emergency treatment.By doing so, the pathophysiology of severe bronchiolitis, acuteasthma, and acute exacerbation of chronic obstructivepulmonary disease will be better understood.
Translational: Biomarkers for the major mechanistic
1. Identify the phenotype and genotype of patientsmanifesting a specific disease process and themechanistic reasons for heterogeneity in outcome. TheED visit should be considered a marker for a high-riskpatient (eg, may benefit from chronic therapy).
2. Develop and test novel animal models to betterunderstand disease processes.
3. Develop biomarkers for point-of-care testing to rapidlyidentify and treat patients in the ED.
4. Understand why there are regional differences inoutcome for the same disease processes.
5. Determine whether there is benefit in regionalizingspecialty centers for care.
Figure 5. Common research gaps and priorities in medical-surgical areas.
contributors to airway obstruction should be identified, and the
Volume , . : November

Kaji et al NIH Medical-Surgical Emergency Research Roundtable
treatment response according to specific triggers (eg, virus versusallergen) and host factors (eg, pharmacogenomics) should alsobe explored. The interaction of environmental factors, triggers,and the host on the treatment response warrants study, as well.Rapid bedside testing tools that identify diverse infectioustriggers would also be helpful, and researchers should explorethe effects of infection (specific versus multiple pathogens) onbronchiolitis, acute asthma, and acute exacerbation of chronicobstructive pulmonary disease.
Clinical: The long-term objective of clinical research in thisarea is to be able to individualize therapy according to theclinical phenotype of the host, the trigger, and the diseaseseverity. Immediate opportunities in the clinical research realmwould be to improve the accuracy of severity assessments forbronchiolitis, asthma, and acute exacerbation of chronicobstructive pulmonary disease. The phenotypes of the differentresponders to treatments should be classified, as well. Criteriafor admission to ward and admission to the ICU also warrantdefinition and validation. Various combinations of treatmentmodalities warrant testing for bronchiolitis, and adjunctivetreatments for asthma should be tested, as well (eg, heliox,intravenous agents). The ED visit should be considered amarker of a high-risk patient (eg, value for chronic treatment),and it would be worthwhile to use adaptive trial designs, asmentioned above, to test novel emergency therapies. Asguidelines are developed, implementation of such guidelinesshould be encouraged and their effectiveness evaluated.
Clinical InformaticsMechanistic: A long-term mechanistic objective is to develop
natural language processing techniques to utilize free-textclinical information for clinical decision support. Toward thatend, research is needed to develop a scientific knowledge baseabout factors (situational awareness, interruption management,distributed cognition) that affect the information needs ofemergency workers. A generalizable infrastructure for electronicdata capture from clinical environments (eg, electronic healthrecords) and patients (eg, patient health records) should beconstructed.
Translational: It will be important to learn the best way toharness real-time data to improve the clinical management ofacute conditions. For example, if monitors and sensors werecoupled with therapies, tight blood pressure control could beachieved for intracranial hemorrhage, vasopressors could beautomatically titrated in sepsis, continuous glucose monitoringcould guide infusions for the management of diabeticketoacidosis, and oximetry and capnometry could be used toadjust ventilator settings. Thus, novel methods ofhuman/computer interaction to better integrate informationtechnology into clinical practice are needed.
Clinical: Broadly speaking, mechanisms to share decisionsupport rules between disparate computing platforms areneeded. Because many information systems are not userfriendly, there is a need for new techniques to visualize and
enhance understanding of complex clinical information whileVolume , . : November
avoiding “alert fatigue.” Unfortunately, lack of attention tohuman factors techniques has made many current EDinformation systems cumbersome to use. Often, poor usabilitydistracts clinicians and slows down clinical care. As the ED isinterconnected with other systems of care, communication linksbetween the ED, public health, and clinics must be improved.Similarly, enhancing out-of-hospital information managementmay improve disaster response.
Health Services ResearchUnlike other topic areas, health services research does not fit
well into the framework of mechanistic, translational, andclinical research because it represents the next “phase” oftranslation of traditional clinical research.
Health Services Access: Emergency medicine data may besystematically used to assess the effect of health care reforminitiatives on access to emergency care and primary care.Barriers to early ED presentation and intervention for time-sensitive conditions (eg, acute coronary syndrome, stroke)should be identified. Toward that end, trials of interventions toreduce delays to early ED care for time-sensitive conditions areneeded. The mechanisms for disparities in access to care shouldbe identified, and trials of patient-, provider-, institutional-,community-, and policy-level interventions to reduce disparitiesin health and inequities in health care should be explored.
Health Services Access and Quality: Outcomes of differentmodels of staffing rural EDs, including the use of telemedicine,should be analyzed. There is a need to establish qualityindicators and benchmarks for ED care of common life-threatening conditions, such as abdominal pain, headache,diabetic emergencies, multiple trauma, and delirium. Otherstudies that are warranted include the examination of outcomesafter regionalization of trauma, acute myocardial infarction,stroke, and pediatric care. To better examine processes of EDcare, systems engineering tools to understand process of EDcare, including work processes, staff communication, andpatient flow, are needed.
Health Services Quality and Cost: An immediate opportunityfor research is the electronic health record for clinical andresearch data sharing. Questions that must be answered includewhat is the optimal electronic health record configuration forED use? What is the optimal health information exchangeapplication for ED data? How will it reduce duplicativediagnostic and therapeutic interventions? Will electronic healthrecords decrease time to definitive treatment? Will electronichealth records improve provider and patient satisfaction? Howwill electronic health records and health information exchangesaffect cost and quality of care in the ED and on post-ED care?Other opportunities for research include developing evidence-based decision rules to guide diagnostic imaging strategies forabdominal pain, back pain, headache, extremity trauma, andother common ED presentations. This will help us develop andimplement care pathways that safely reduce overuse ofdiagnostic imaging. Comparative effectiveness research using
rigorous strategies to adjust for case mix about costs of care andAnnals of Emergency Medicine 527

NIH Medical-Surgical Emergency Research Roundtable Kaji et al
outcomes for various ED presentations are also warranted. Itwill be important to optimize the cost-effectiveness of caredelivery processes for high-volume ED presentations.
Access, Quality, Cost, and Outcomes: Finally, there is a needfor supplemental funding to train emergency care providers inhealth services research.
Cardiac ResuscitationSudden cardiac arrest is a leading cause of death in North
America. Despite this fact, survival varies between regions, andonly 3 interventions used today have high-level supportingevidence: cardiopulmonary resuscitation (CPR), electricalcountershock for ventricular fibrillation, and hypothermia aftercardiac arrest. Most mortality results from irreversible cardiacfailure or brain injury.
Mechanistic: Important basic science issues were identifiedrelevant to emergency cardiac resuscitation. To restore normalcardiac electrical activity, there is a need to identify optimalwaveforms for electrical defibrillators, the role of drug therapy,and the optimal timing of defibrillation in relation to chestcompressions. For restoration of mechanical cardiac activity,research is required on the best timing and character for chestcompressions, the role of intrathoracic pressure changes, the roleof vasoactive drug therapy, and the mechanisms of postischemicstunning and electromechanical uncoupling. Brain injury afterglobal ischemia-reperfusion is still incompletely understood andhas only been responsive to therapeutic hypothermia. Betterunderstanding of the timing and sequence of events thatcontribute to pathobiology during global cerebral ischemia andreperfusion is needed. Mechanisms of how hypothermia maywork should be better delineated, whereas efforts continue tounderstand the mechanisms of ischemic neuronal death.Restorative therapies (stem cells, rehabilitation), long-termneuronal changes, and the significance of systemic inflammatoryresponse after resuscitation also require study.
Translational: Successful cardiac resuscitation requires time-sensitive, multiple interventions affecting multiple organsystems. Therefore, organ-specific research is difficult totranslate into clinical practice, and important translationalefforts must not be criticized as lacking specific focus or beinginsufficiently innovative. Specific areas to study include thedevelopment of devices to achieve hypothermia, to augmentCPR, and to monitor resuscitation progress. There is a need forclinical phenotyping, including biomarkers or surrogate markersto follow the time course and severity of organ injury, guidetherapeutic interventions, and predict survival. The effects ofcardiac resuscitation on other organ systems—kidney, liver, andlung—are largely unknown. Finally, drug kinetics and drugactions may be altered after ischemia-reperfusion, and thiswarrants investigation.
Clinical: Most drugs, devices, and clinical practices currentlyused in resuscitation lack rigorous clinical testing foreffectiveness. Yet clear differences in successful outcome ratesvary greatly among institutions and care systems. Thus, bundles
of care may be more important than individual interventions,528 Annals of Emergency Medicine
and these pathways of care should begin in the out-of-hospitalsetting, with EMS as an integral part of the research team.Challenges in clinical cardiac resuscitation research include theroutine need for an exception from informed consent. Thisprocess is equally difficult and expensive for a large trial and fora small pilot study, which is a deterrent to the conduct ofimportant hypothesis-generating clinical research. The lowbaseline survival rate from cardiac arrest also demands largersample sizes for adequate power, further increasing expense.Adaptive research designs should be used to increase studyefficiency.
Pediatric: Children are developmentally different, the causesfor adult and pediatric cardiac arrest differ, and fewer childrenthan adults are available for studies. Thus, studies sensitive todevelopmental differences are needed to define the optimalpediatric CPR method (rate, depth, and timing) andappropriate defibrillation doses for children and to validate allother practices at different developmental stages. Finally,patient-oriented outcome measures for cardiac arrest have notbeen rigorously validated (eg, Cerebral Performance Categoryscore), and consensus is needed on an appropriatedevelopmentally specific outcome measure after pediatriccardiac arrest.
Hypotension and Ischemia-ReperfusionMechanistic: Basic science models of global/focal heart
ischemia/reperfusion injury and cardioprotection should bedeveloped and tested. Animal models may help define thecorrect timing of medication administration and when toinstitute hypothermia. The complex effect of whole-bodyischemia and the potential role of induced hibernation in organand whole-body protection warrant investigation. Researchersneed to better describe mechanisms of reperfusion injury causedby oxidation, inflammation, mitochondrial dysfunction,modulation of the contractile apparatus and ion channels,microvascular dysfunction, coagulopathy, and the relationshipwith autoimmune disorders. The processes of secondaryreperfusion damage during CPR and after return ofspontaneous circulation, involving focal and global ischemia-reperfusion, should be better described. To better understandwhy some patients achieve return of spontaneous circulationwhereas others do not, the phenotypes of cardiac arrest patientsassociated with molecular/genetic markers should be delineated.Questions that should be answered include, are there certaingenes that are associated with return of spontaneous circulation?Are there markers that can be tested that correlate with thephenotype that survives cardiac arrest?
Translational: The association of genomic and proteomicpatterns, as well as the effect of timing and sequenceof reperfusion therapies on neurologic outcome and endothelialresponse, should be investigated. Tools and strategies torecognize impending arrest are needed. Important questionsremaining to be answered are the following: How does high-quality CPR work and how does it affect return of spontaneous
circulation and survival? How does therapeutic hypothermiaVolume , . : November
Kaji et al NIH Medical-Surgical Emergency Research Roundtable
work? What is the optimal timing of percutaneous coronaryintervention?
Clinical: Barriers to implementation of known effectiveresuscitation strategies in clinical practice should be identified.Multidisciplinary approaches to measure and improve recoveryshould be evaluated. The effectiveness of interventions targetedto physiologic phases of resuscitation, includingpostresuscitation care (eg, optimizing oxygenation,hemodynamics, nutrition, revascularization, other supportivetherapies) should be tested. Tools for the stratification ofpopulations with contemporary imaging, outcome instruments,and biomarkers for guiding therapy and predicting recoveryshould be validated. Approaches to reducing the gap betweendata/discovery and new lifesaving devices and treatments shouldbe minimized.
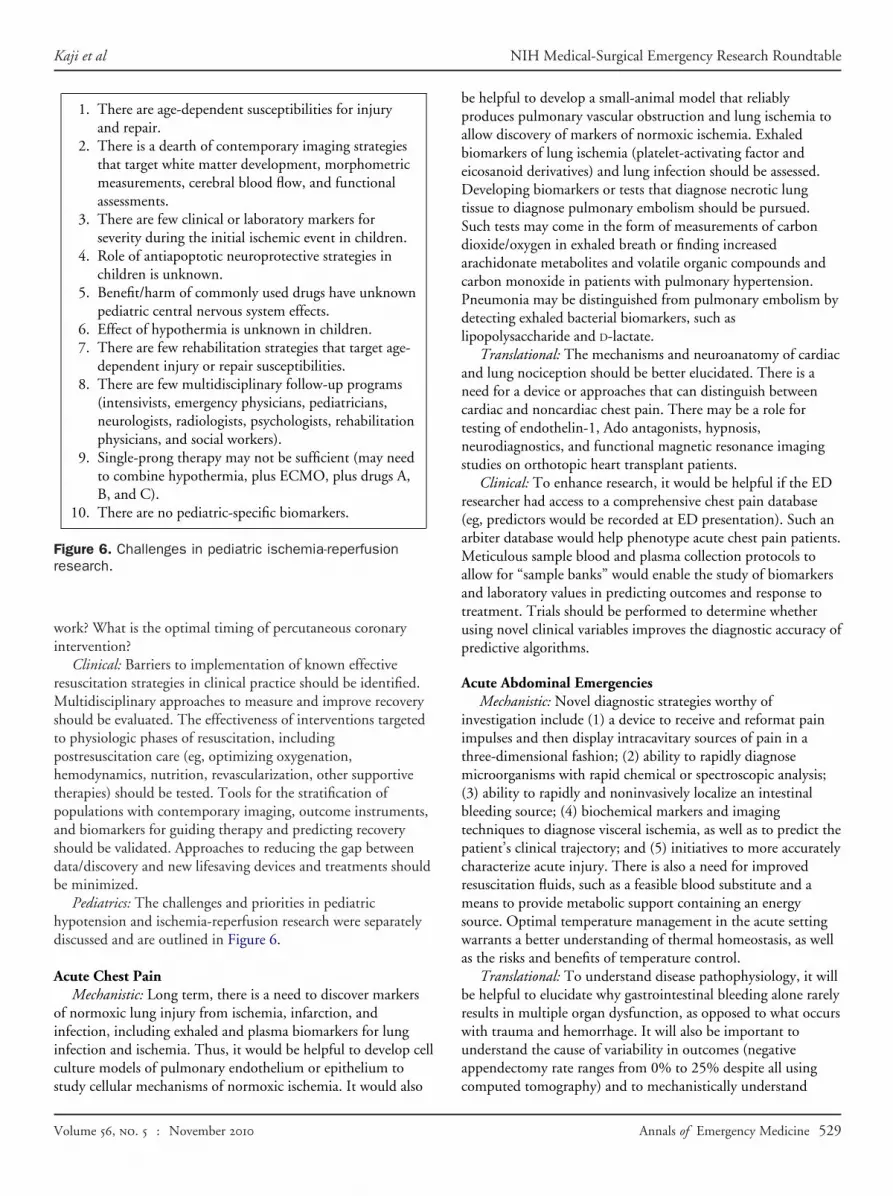
Pediatrics: The challenges and priorities in pediatrichypotension and ischemia-reperfusion research were separatelydiscussed and are outlined in Figure 6.
Acute Chest PainMechanistic: Long term, there is a need to discover markers
of normoxic lung injury from ischemia, infarction, andinfection, including exhaled and plasma biomarkers for lunginfection and ischemia. Thus, it would be helpful to develop cellculture models of pulmonary endothelium or epithelium to
1. There are age-dependent susceptibilities for injuryand repair.
2. There is a dearth of contemporary imaging strategiesthat target white matter development, morphometricmeasurements, cerebral blood flow, and functionalassessments.
3. There are few clinical or laboratory markers forseverity during the initial ischemic event in children.
4. Role of antiapoptotic neuroprotective strategies inchildren is unknown.
5. Benefit/harm of commonly used drugs have unknownpediatric central nervous system effects.
6. Effect of hypothermia is unknown in children.7. There are few rehabilitation strategies that target age-
dependent injury or repair susceptibilities.8. There are few multidisciplinary follow-up programs
(intensivists, emergency physicians, pediatricians,neurologists, radiologists, psychologists, rehabilitationphysicians, and social workers).
9. Single-prong therapy may not be sufficient (may needto combine hypothermia, plus ECMO, plus drugs A,B, and C).
10. There are no pediatric-specific biomarkers.
Figure 6. Challenges in pediatric ischemia-reperfusionresearch.
study cellular mechanisms of normoxic ischemia. It would also
Volume , . : November
be helpful to develop a small-animal model that reliablyproduces pulmonary vascular obstruction and lung ischemia toallow discovery of markers of normoxic ischemia. Exhaledbiomarkers of lung ischemia (platelet-activating factor andeicosanoid derivatives) and lung infection should be assessed.Developing biomarkers or tests that diagnose necrotic lungtissue to diagnose pulmonary embolism should be pursued.Such tests may come in the form of measurements of carbondioxide/oxygen in exhaled breath or finding increasedarachidonate metabolites and volatile organic compounds andcarbon monoxide in patients with pulmonary hypertension.Pneumonia may be distinguished from pulmonary embolism bydetecting exhaled bacterial biomarkers, such aslipopolysaccharide and D-lactate.
Translational: The mechanisms and neuroanatomy of cardiacand lung nociception should be better elucidated. There is aneed for a device or approaches that can distinguish betweencardiac and noncardiac chest pain. There may be a role fortesting of endothelin-1, Ado antagonists, hypnosis,neurodiagnostics, and functional magnetic resonance imagingstudies on orthotopic heart transplant patients.
Clinical: To enhance research, it would be helpful if the EDresearcher had access to a comprehensive chest pain database(eg, predictors would be recorded at ED presentation). Such anarbiter database would help phenotype acute chest pain patients.Meticulous sample blood and plasma collection protocols toallow for “sample banks” would enable the study of biomarkersand laboratory values in predicting outcomes and response totreatment. Trials should be performed to determine whetherusing novel clinical variables improves the diagnostic accuracy ofpredictive algorithms.
Acute Abdominal EmergenciesMechanistic: Novel diagnostic strategies worthy of
investigation include (1) a device to receive and reformat painimpulses and then display intracavitary sources of pain in athree-dimensional fashion; (2) ability to rapidly diagnosemicroorganisms with rapid chemical or spectroscopic analysis;(3) ability to rapidly and noninvasively localize an intestinalbleeding source; (4) biochemical markers and imagingtechniques to diagnose visceral ischemia, as well as to predict thepatient’s clinical trajectory; and (5) initiatives to more accuratelycharacterize acute injury. There is also a need for improvedresuscitation fluids, such as a feasible blood substitute and ameans to provide metabolic support containing an energysource. Optimal temperature management in the acute settingwarrants a better understanding of thermal homeostasis, as wellas the risks and benefits of temperature control.
Translational: To understand disease pathophysiology, it willbe helpful to elucidate why gastrointestinal bleeding alone rarelyresults in multiple organ dysfunction, as opposed to what occurswith trauma and hemorrhage. It will also be important tounderstand the cause of variability in outcomes (negativeappendectomy rate ranges from 0% to 25% despite all using
computed tomography) and to mechanistically understandAnnals of Emergency Medicine 529

NIH Medical-Surgical Emergency Research Roundtable Kaji et al
heterogeneity of outcomes (why one patient dies from aperforated viscus, whereas another patient does well).
Clinical: The cost-effectiveness and consequences ofregionalization should be assessed. How many regional centersare needed? What is the cost of transport versus the cost ofsaving life? What are the unexpected consequences ofregionalization? Pilot projects on the regionalization of acuteabdominal emergencies should be funded, and outcomemeasures other than mortality should be defined and assessed.
GeriatricsMechanistic: The long-term objective is to identify
physiologic and bioenergetic changes associated with aging thatcontribute to the greater predisposition to worse outcomes afteracute events.
Translational: It will be important to define the modifiablefactors (such as components of frailty, nutrition, inflammation)that predispose older patients to functional decline anddependence after acute injury or illness. There is thus a need todelineate the genomic, proteomic, metabolomic phenotype forbetter risk stratification, tailored therapy, and prediction oftreatment response.
Clinical: There is a need for diagnostic tools to improve theED recognition and diagnosis of delirium, and it would beimportant to determine whether ED recognition andmanagement of delirium and other cognitive abnormalitiesresults in reduced morbidity/mortality. Because the elderly aresusceptible to medication interactions and adverse effects, thereshould be greater efforts toward prevention of such adverseeffects. Elderly pain management is also a challenge because oftheir predisposition to medication adverse effects, and thusclinical trials are needed to delineate optimal dosing of differentanalgesics. Out-of-hospital care providers are a potentialunderused source for assessing and referring patients who are atrisk for falls, functional decline, substance abuse, and elderabuse. We must develop practical methods of incorporatingfunctional assessments into the evaluation of the elderly patient.
CONCLUSIONSThis medical-surgical roundtable discussion highlighted
numerous opportunities for emergency care research:● In vitro and in vivo studies to elucidate the timing, sequence,
and duration of causal molecular and cellular events involvedin time-critical illnesses and injuries, and the development oftreatments capable of halting or reversing them.
● The innovation, translation, and application of biomedicaldiscoveries to enhance early diagnosis and definition of life-threatening conditions (in both out-of-hospital andinhospital settings).
● Clinical studies to evaluate promising treatments, andbundles of treatments, to treat the most critically ill patientsand patients whose underlying disease processes may be ill-
defined, at least at the outset.530 Annals of Emergency Medicine
● The optimal design of systems—information processing, caremanagement, environmental design, materials andmethods—to improve care and promote patient safety.
● The adaptive, innovative clinical trial designs and use ofemergency care research networks to efficiently conductpromising, clinical research.We believe that the science of emergency care may thus be
advanced by facilitating the following: (1) training newinvestigators with dedicated emergency care research trainingprograms (eg, national K12, T32 programs within the existingNIH structure, and enhanced K02/K08/K23 support); (2)developing new emergency care clinical research networks; (3)integrating emergency care research into existing Clinical andTranslational Science Award programs; (4) developingemergency care-specific initiatives within the existing structureof NIH Institutes and Centers; (5) involving emergencyspecialists in grant review and research advisory processes; (6)supporting learn-phase or small clinical trials; and (7)performing research to address ethical and regulatory issues(emergency consent, use of central institutional review boards,and data linkages and privacy).
Supervising editors: Donald M. Yealy, MD; Michael L.Callaham, MD
Dr. Yealy was the supervising editor on this article but he didnot participate in the decision to publish this article.
Funding and support: By Annals policy, all authors are requiredto disclose any and all commercial, financial, and otherrelationships in any way related to the subject of this articlethat might create any potential conflict of interest. The authorshave stated that no such relationships exist. See theManuscript Submission Agreement in this issue for examplesof specific conflicts covered by this statement.
Publication dates: Received for publication February 4, 2010.Accepted for publication March 4, 2010.
Reprints not available from the authors.
Address for correspondence: Amy H. Kaji, MD, PhD,Department of Emergency Medicine, Harbor-UCLA MedicalCenter, 1000 W. Carson Street, Box 21, Torrance, CA 90509-2910; 310-222-3500, fax 310-782-1763; [email protected].
REFERENCES1. Committee on the Future of Emergency Care in the United States
Health System. Future of Emergency Care—Hospital-BasedEmergency Care at the Breaking Point. Washington, DC: NationalAcademies Press; 2007.
2. Committee on the Future of Emergency Care in the United StatesHealth System. Future of Emergency Care—Emergency MedicalServices at the Crossroads. Washington, DC: National AcademiesPress; 2007.
3. Committee on the Future of Emergency Care in the United StatesHealth System. Future of Emergency Care—Emergency Care forChildren, Growing Pains. Washington, DC: National Academies
Press; 2007.Volume , . : November

Kaji et al NIH Medical-Surgical Emergency Research Roundtable
4. Lewis, RJ, Cone DC, Biros MH. Enhancing emergency careresearch. Background paper prepared for the IoM Committee onthe Future of Emergency Care [Internal Document], 2006.
5. Neumar RW. The Zerhouni challenge: defining the fundamentalhypothesis of emergency care research. Ann Emerg Med.2007;49:696-697.
6. Blanda M, Gerson LW, Dunn K. Emergency medicine researchrequirements and director characteristics. Acad Emerg Med. 1999;6:286-291.
7. Karras DJ, Kruus LK, Baumann BM, et al. Emergency medicineresearch directors and research programs: characteristics andfactors associated with productivity. Acad Emerg Med. 2006;13:637-644.
APPENDIXContributing Authors (External Participants)
Amy H. Kaji, MD, PhDDepartment of Emergency MedicineHarbor-UCLA Medical Center1000 W Carson Street, #21Torrance, CA 90509Telephone: 310-222-3500E-mail [email protected]
Roger J. Lewis, MD, PhDDepartment of Emergency MedicineHarbor-UCLA Medical CenterBuilding D91000 W Carson Street, Box 21Torrance, CA 90509Telephone: 310-222-6741E-mail [email protected]
Toni Beavers-MayMicrobiology LaboratoryArkansas Children’s Hospital3 Children’s WayLittle Rock, AR 72202Telephone: 501-364-1931E-mail [email protected]
Robert Berg, MDDivision of Critical Care MedicineDepartment of Anesthesiology and Critical Care MedicineChildren’s Hospital of Philadelphia34th Street and Civic Center BoulevardPhiladelphia, PA 19104Telephone: 267-426-3014E-mail [email protected]
Jeremy Brown, MDDepartment of Emergency MedicineThe George Washington University2150 Pennsylvania Avenue, NW, Suite 2B-410
Washington, DC 20037Volume , . : November
Telephone: 202-741-2902E-mail [email protected]
Eileen Bulger, MDDepartment of SurgeryUniversity of WashingtonHarborview Medical Center, Box 359796325 9th AvenueSeattle, WA 98104Telephone: 206-744-6448E-mail [email protected]
Charles Cairns, MDDepartment of Emergency MedicineUniversity of North Carolina at Chapel HillCB #7594170 Manning DriveChapel Hill, NC 27599-7594Telephone: 919-843-3045E-mail [email protected]
Clifton Callaway, MD, PhDDepartment of Emergency MedicineUniversity of Pittsburgh3600 Forbes AvenuePittsburgh, PA 15261Telephone: 412-647-9047E-mail [email protected]
Carlos A. Camargo, Jr, MD, DrPHDepartment of Emergency MedicineMassachusetts General Hospital326 Cambridge St, Suite 410Boston, MA 02114Telephone: 617-726-5276E-mail [email protected]
Joseph Carcillo, MDDepartment of Critical Care MedicineUniversity of Pittsburgh3550 Terrace StreetPittsburgh, PA 15261Telephone: 412-647-3136E-mail [email protected]
Roberta DeBiasi, MDPediatric Infectious Diseases Training ProgramChildren’s National Medical Center111 Michigan Avenue, NWWashington, DC 20010Telephone: 202-329-9629E-mail [email protected]
Tania Diaz, MD
4221 29th StreetAnnals of Emergency Medicine 531

NIH Medical-Surgical Emergency Research Roundtable Kaji et al
Mount Rainier, MD 20712Telephone: 301-927-4240E-mail [email protected]
Francine Ducharme, MDDepartment of PediatricsCHU Sainte-Justine Research CenterUniversity of Montreal3175 Cote-Sainte-Catherine, Room 7939Montreal, QC H3T 1C5, CanadaTelephone: 514-345-4931, ext 4398E-mail [email protected]
Seth Glickman, MD, MBADepartment of Emergency MedicineUniversity of North Carolina at Chapel HillPhysicians Office Building170 Manning Drive, CB #7594Chapel Hill, NC 27599-7594Telephone: 919-264-4612E-mail [email protected]
Katherine Heilpern, MDDepartment of Emergency MedicineEmory University531 Asbury Circle-Annex, Suite N340Atlanta, GA 30322Telephone: 404-778-5975E-mail [email protected]
Robert Hickey, MDDivision of Pediatric Emergency MedicineChildren’s Hospital of PittsburghAdministrative Office Building, Second FloorChildren’s Hospital DrivePittsburgh, PA 15201Telephone: 412-692-7692E-mail [email protected]
Terry Vanden Hoek, MDSection of Emergency MedicineDepartment of MedicineThe University of Chicago5841 S Maryland AvenueChicago, IL 60637Telephone: 773-702-0895E-mail [email protected]
Judd Hollander, MDDepartment of Emergency MedicineUniversity of PennsylvaniaGround Ravdin3400 Spruce Street
Philadelphia, PA 19104532 Annals of Emergency Medicine
Telephone: 215-662-2767E-mail [email protected]
Susan Janson, DScCommunity Health SystemsUniversity of California, San FranciscoN505, Fifth Floor2 Koret Way, Box 0608San Francisco, CA 94143-0608Telephone: 415-476-5282E-mail [email protected]
Gregory Jurkovich, MDDepartment of SurgeryHarborview Medical CenterUniversity of Washington325 Ninth AvenueSeattle, WA 98104Telephone: 206-744-8485E-mail [email protected]
Arthur Kellermann, MD, MPHDepartment of Emergency MedicineEmory University School of MedicineSchool of Medicine Building1648 Pierce Drive, NE, Suite 445Atlanta, GA 30322Telephone: 404-558-5136E-mail [email protected]
Stephen Kingsmore, MDNational Center for Genome Resources2935 Rodeo Park Drive EastSanta Fe, NM 87505Telephone: 505-995-4466E-mail [email protected]
Jeffrey Kline, MDDepartment of Emergency MedicineCarolinas Medical CenterMEB, Third Floor1000 Blythe Boulevard, Room 306Charlotte, NC 28203Telephone: 704-355-7092E-mail [email protected]
Nathan Kuppermann, MD, MPHDepartment of Emergency MedicineSchool of MedicineUniversity of California, DavisPSSB, Suite 21002315 Stockton Boulevard
Sacramento, CA 95817Volume , . : November

Kaji et al NIH Medical-Surgical Emergency Research Roundtable
Telephone: 916-734-1535E-mail [email protected]
Robert Lowe, MD, MPHDepartment of Emergency MedicineOregon Health & Science University3181 SW Sam Jackson Park Road, MC CR114Portland, OR 97239Telephone: 503-494-7134E-mail [email protected]
David McLario, DO, MSEmergency Department Quality ImprovementSection of Emergency MedicineDepartment of PediatricsArkansas Children’s HospitalUniversity of Arkansas for Medical SciencesOne Children’s Way, Slot 512-16Little Rock, AR 72202Telephone: 501-364-1598E-mail [email protected]
Larry Nathanson, MDEmergency Medicine InformaticsDepartment of Emergency MedicineBeth Israel Deaconess Medical CenterOne Deaconess Road, W-CC2Boston, MA 02215Telephone: 617-754-2389E-mail [email protected]
Graham Nichol, MD, MPHCenter for Prehospital Emergency CareDepartment of MedicineUniversity of Washington Harborview Medical Center325 9th Avenue, Box 359727Seattle, WA 98104Telephone: 206-521-1728E-mail [email protected]
Andrew Peitzman, MDDepartment of SurgeryUniversity of Pittsburgh School of MedicineF1281 Presbyterian University Hospital200 Lothrop StreetPittsburgh, PA 15213Telephone: 412-647-0635E-mail [email protected]
Lynne Richardson, MDAcademic, Research, and Community ProgramsDepartment of Emergency MedicineMount Sinai School of Medicine
One Gustave L. Levy Place, Box 1620Volume , . : November
New York, NY 10029Telephone: 212-659-1653E-mail [email protected]
Arthur Sanders, MDDepartment of Emergency MedicineUniversity of ArizonaP.O. Box 2450571609 N Warren Avenue, Room 104Tucson, AZ 85724-5057Telephone: 520-626-5032E-mail [email protected]
Manish Shah, MD, MPHDepartment of Emergency MedicineUniversity of Rochester Medical Center601 Elmwood Avenue, Box 655Rochester, NY 14642Telephone: 585-463-2920E-mail [email protected]
Nathan Shapiro, MD, MPHDepartment of Emergency MedicineBeth Israel Deaconess Medical CenterOne Deaconess Road, CC2-WBoston, MA 02215Telephone: 617-754-2343E-mail [email protected]
Robert Silverman, MDDepartment of Emergency MedicineLong Island Jewish Medical CenterNorth Shore–Long Island Jewish Health System270-05 76th AvenueQueens, NY 11040Telephone: 718-470-7501E-mail [email protected]
Martin Than, MDEmergency DepartmentChristchurch Public HospitalPrivate Bag 4710Christ Church 4710New ZealandTelephone: 64-33640270E-mail [email protected]
Scott Wilber, MD, MPHDepartment of Emergency MedicineSumma Health SystemNortheastern Ohio Universities Colleges of Medicine andPharmacy41 Arch Street, Room 519
Akron, OH 44309Annals of Emergency Medicine 533

NIH Medical-Surgical Emergency Research Roundtable Kaji et al
Telephone: 330-375-7530E-mail [email protected]
Donald Yealy, MDDepartment of Emergency MedicineUniversity of Pittsburgh10028 Forbes Tower3600 Forbes AvenuePittsburgh, PA 15241Telephone: 412-647-8295E-mail [email protected]
NIH and Federal Roundtable Participants
Nahid AkhyaniStrategic Planning and Evaluation BranchNational Institute of Allergy and Infectious DiseasesNational Institutes of HealthBuilding 6610, Room 11086610 Rockledge DriveBethesda, MD 20892Telephone: 301-443-9339E-mail [email protected]
Guy Arcuri, MPHNational Institute of Allergy and Infectious DiseasesBuilding 6610, Room 2100A6610 Rockledge Drive, MSC 6620Bethesda, MD 20892-6620Telephone: 301-385-4729E-mail [email protected]
Hugh Auchincloss, MDNational Institute of Allergy and Infectious DiseasesNational Institutes of HealthBuilding 31, Room 7A-0331 Center Drive, MSC 2520Bethesda, MD 20892-2520Telephone: 301-496-9677E-mail [email protected]
Sarah Dunsmore, PhDDivision of Pharmacology, Physiology, and BiologicalChemistryNational Institute of General Medical SciencesNational Institutes of HealthBuilding 45, Room 2AS49C45 Center Drive, MSC 6200Bethesda, MD 20892-6200Telephone: 301-594-3827E-mail [email protected]
Basil Eldadah, MD, PhDDivision of Geriatrics and Clinical Gerontology
National Institute on Aging534 Annals of Emergency Medicine
National Institutes of HealthGateway Building, Room 3C3077201 Wisconsin Avenue, MSC 9205Bethesda, MD 20892-9205Telephone: 301-496-6761E-mail [email protected]
Rosemarie Filart, MDDivision of Clinical Research ResourcesNational Center for Research ResourcesNational Institutes of HealthOne Democracy Plaza, Room 9186701 Democracy Boulevard, MSC 4874Bethesda, MD 20892-4874Telephone: 301-435-0178E-mail [email protected]
Giovanna Guerrero, PhDOffice of Science Policy and PlanningNational Institute of Neurological Disorders and StrokeNational Institutes of HealthBuilding 31, Room 8A0331 Center Drive, MSC 2540Bethesda, MD 20892-2540Telephone: 301-402-9296E-mail [email protected]
Michael Handrigan, MDEmergency Care Coordination CenterOffice of the Assistant Secretary for Preparedness and ResponseUS Department of Health and Human Services330 C Street, SWWashington, DC 20024Telephone: 202-245-0715E-mail [email protected]
Steven Hirschfeld, MD, PhDEunice Kennedy Shriver National Institute of Child Health andHuman DevelopmentNational Institutes of HealthBuilding 31, Room 2A0331 Center Drive, MSC 2425Bethesda, MD 20892-2425Telephone: 301-496-0044E-mail [email protected]
Van Hubbard, MD, PhDDivision of Nutrition Research CoordinationNational Institute of Diabetes and Digestive and KidneyDiseasesNational Institutes of HealthTwo Democracy Plaza, Room 6316707 Democracy Boulevard, MSC 5461
Bethesda, MD 20892-5461Volume , . : November

Kaji et al NIH Medical-Surgical Emergency Research Roundtable
Telephone: 301-594-8827E-mail [email protected]
Richard Hunt, MDDivision of Injury ResponseNational Center for Injury Prevention and ControlCenters for Disease Control and Prevention1600 Clifton RoadAtlanta, GA 30333Telephone: 770-488-4031E-mail [email protected]
Karen Huss, PhDNational Institute of Nursing ResearchNational Institutes of HealthOne Democracy Plaza, Suite 7106701 Democracy Boulevard, MSC 4870Bethesda, MD 20892-4870Telephone: 301-594-5970E-mail [email protected]
Daniel Kavanaugh, MSWEmergency Medical Services for Children ProgramHealth Resources and Services AdministrationUS Department of Health and Human Services5600 Fishers Lane, Room 18A-38Rockville, MD 21114Telephone: 301-443-1321E-mail [email protected]
Paul Kimmel, MDAcute Kidney Injury ProgramDivision of Kidney, Urologic, and Hematologic DiseasesNational Institute of Diabetes and Digestive and KidneyDiseasesNational Institutes of HealthTwo Democracy Plaza, Room 6126707 Democracy Boulevard, MSC 5462Bethesda, MD 20892-5462Telephone: 301-594-7717E-mail [email protected]
Cheryl Kitt, PhDCenter for Scientific ReviewNational Institutes of HealthTwo Rockledge Center, Room 30306701 Rockledge Drive, MSC 7760Bethesda, MD 20892-7760Telephone: 301-435-1112E-mail [email protected]
Jeffrey Kopp, MDNational Institute of Diabetes and Digestive and KidneyDiseases
National Institutes of HealthVolume , . : November
Building 10, Room 3N11610 Center Drive, MSC 1268Bethesda, MD 20892-1268Telephone: 301-594-3403E-mail [email protected]
Jukka Korpela, MDBacterial and Mycology BranchNational Institute of Allergy and Infectious DiseasesNational Institutes of HealthBuilding 6610, Room 42086610 Rockledge Drive, MSC 6604Bethesda, MD 20892-6604Telephone: 301-402-9522E-mail [email protected]
Alice Mascette, MDHeart Failure and Arrhythmias BranchDivision of Cardiovascular DiseasesNational Heart, Lung, and Blood InstituteTwo Rockledge Center, Room 81706701 Rockledge Drive, MSC 7956Bethesda, MD 20892-7956Telephone: 301-435-0504E-mail [email protected]
Clement McDonald, MDNational Library of MedicineLister Hill Center for Biomedical CommunicationsBuilding 38, Room 7N7079000 Rockville Pike, MSC 3828Bethesda, MD 20892-3828Telephone: 301-496-4441E-mail [email protected]
Sarah Miers, JDPolicy, Legislation, and Communication SectionNational Institute of Allergy and Infectious DiseasesNational Institutes of HealthBuilding 6610, Room 41136610 Rockledge Drive, MSC 6603Bethesda, MD 20892-6603Telephone: 301-402-8407E-mail [email protected]
Ryan Mutter, PhDCenter for Delivery, Organization, and MarketsAgency for Healthcare Research and Quality540 Gaither RoadRockville, MD 20851Telephone: 301-427-1415E-mail [email protected]
Jane Scott, ScD, MSN
Office of Research Training and Career DevelopmentAnnals of Emergency Medicine 535

NIH Medical-Surgical Emergency Research Roundtable Kaji et al
National Heart, Lung, and Blood InstituteNational Institutes of HealthTwo Rockledge Center, Room 81386701 Rockledge Drive, MSC 7940Bethesda, MD 20892-7940Telephone: 301-435-0535E-mail [email protected]
Scott Somers, PhDDivision of Pharmacology, Physiology, and BiologicalChemistryNational Institute of General Medical SciencesNational Institutes of HealthBuilding 45, Room 2AS49B45 Center Drive, MSC 6200Bethesda, MD 20892-6200Telephone: 301-594-3827E-mail [email protected]
George Sopko, MDDivision of Cardiovascular DiseasesNational Heart, Lung, and Blood InstituteTwo Rockledge Center, Room 81686701 Rockledge Drive, MSC 7956Bethesda, MD 20892-7956Telephone: 301-435-0504E-mail [email protected]
Betty Tai, PhDClinical Trials NetworkNational Institute on Drug AbuseNational Institutes of HealthNeuroscience Center, Room 31206001 Executive Boulevard, MSC 9557Bethesda, MD 20892-9557Telephone: 301-443-2397E-mail [email protected]
Alkis Togias, MDAsthma and InflammationDivision of Allergy, Immunology, and TransplantationNational Institute of Allergy and Infectious DiseasesNational Institutes of HealthBuilding 6610, Room 30656610 Rockledge Drive, MSC 6601Bethesda, MD 20892-6601Telephone: 301-451-3104E-mail [email protected]
Kishena Wadhwani, PhDDivision of Scientific ReviewOffice of Extramural Research, Education and PriorityPopulationAgency for Healthcare Research and Quality
540 Gaither Road, Room 2032536 Annals of Emergency Medicine
Rockville, MD 20850Telephone: 301-427-1556E-mail [email protected]
Kevin Wright, MPAEvaluation SectionStrategic Planning and Evaluation BranchNational Institute of Allergy and Infectious DiseasesNational Institutes of HealthBuilding 6610, Room 21176610 Rockledge Drive, MSC 6620Rockville, MD 20892-6620Telephone: 301-402-3574E-mail [email protected]
Planning Group RosterExternal Members
Charles Cairns, MDUniversity of North Carolina at Chapel HillE-mail [email protected]
Carlos A. Camargo, Jr, MD, DrPHMassachusetts General HospitalE-mail [email protected]
Gregory Jurkovich, MDHarborview Medical CenterUniversity of WashingtonE-mail [email protected]
Arthur Kellermann, MD, MPHEmory University School of MedicineE-mail [email protected]
Nathan Kuppermann, MD, MPHUniversity of California, DavisE-mail [email protected]
Roger J. Lewis, MD, PhDHarbor-UCLA Medical CenterE-mail [email protected]
Arthur Sanders, MDUniversity of ArizonaE-mail [email protected]
Nathan Shapiro, MD, MPHBeth Israel Deaconess Medical CenterE-mail [email protected]
NIH Members
Hugh Auchincloss, MDVolume , . : November

Kaji et al NIH Medical-Surgical Emergency Research Roundtable
National Institute of Allergy and Infectious DiseasesE-mail [email protected]
Sarah Dunsmore, PhDDivision of Pharmacology, Physiology, and BiologicalChemistryNational Institute of General Medical SciencesE-mail [email protected]
Debra Egan, MSc, MPHNational Heart, Lung, and Blood InstituteE-mail [email protected]
Basil Eldadah, MD, PhDDivision of Geriatrics and Clinical GerontologyNational Institute on AgingE-mail [email protected]
Michael Handrigan, MDEmergency Care Coordination CenterOffice of the Assistant Secretary for Preparedness and ResponseUS Department of Health and Human ServicesE-mail [email protected]
Richard Hunt, MDDivision of Injury ResponseNational Center for Injury Prevention and ControlCenters for Disease Control and PreventionE-mail [email protected]
Karen Huss, PhDNational Institute of Nursing ResearchE-mail [email protected]
Daniel Kavanaugh, MSW
Emergency Medical Services for Children ProgramVolume , . : November
Health Resources and Services AdministrationUS Department of Health and Human ServicesE-mail [email protected]
Jeffrey Kopp, MDNational Institute of Diabetes and Digestive and KidneyDiseasesE-mail [email protected]
Jukka Korpela, MDBacterial and Mycology BranchNational Institute of Allergy and Infectious DiseasesE-mail [email protected]
Alice Mascette, MDHeart Failure and Arrhythmias BranchDivision of Cardiovascular DiseasesNational Heart, Lung, and Blood InstituteE-mail [email protected]
Ryan Mutter, PhDCenter for Delivery, Organization, and MarketsAgency for Healthcare Research and QualityE-mail [email protected]
Scott Somers, PhDDivision of Pharmacology, Physiology, and BiologicalChemistryNational Institute of General Medical SciencesE-mail [email protected]
George Sopko, MDDivision of Cardiovascular DiseasesNational Heart, Lung, and Blood Institute
E-mail [email protected]Annals of Emergency Medicine 537





























