Embed Size (px)
Citation preview

Case Report
Successful Percutaneous Transvenous Antegrade MitralValve-in-Valve Implantation
Hector I. Michelena,1 MD, Oluseun Alli,1 MD, Allison K. Cabalka,2 MD,and Charanjit S. Rihal,1* MD
We report a case of transcatheter valve-in-valve therapy performed on an 85-year-oldman with severe mitral bioprosthetic valve dysfunction. He was a high risk candidate forconventional surgery and he underwent placement of the Melody transcatheter heartvalve into the mitral bioprosthesis via the right femoral vein. VC 2012 Wiley Periodicals, Inc.
Key words: valvular heart disease; congestive heart failure; transeptal cath
INTRODUCTION
Transcatheter valve-in-valve implantation for failingbioprosthetic heart valves is rapidly gaining popularityas an alternative treatment approach to surgical valvere-replacement in patients with prohibitive surgical risk.The avoidance of sternotomy and cardiopulmonarybypass in these high risk patients makes this approachparticularly attractive as it leads to a reduction in in-hos-pital morbidity and mortality and a decrease in resourceutilization secondary to quicker recovery period withshorter hospitalization. We report the implantation ofthe Melody valve in a dysfunctional mitral prosthesisusing a percutaneous transvenous approach.
CASE PRESENTATION
An 85-year-old Caucasian male with history of hyper-tension, hyperlipidemia, previous aorto-bi-iliac graft-repair, moderate bilateral renal artery stenoses, and rightpontine stroke, presented for evaluation of NYHA III-IVdyspnea and recurrent heart failure. The patient was apast smoker with significant asbestos exposure. He hadundergone coronary artery bypass grafting (CABG) in1984 and 1991. He had a third CABG procedure withconcomitant mitral valve replacement in 2003 with a27 mm Carpentier Edwards’s bovine bioprosthesis. Sub-sequently, he had developed severe calcific aortic steno-sis which was treated with a percutaneous transfemoralCoreValve (Medtronic Inc Minneapolis MN) aorticreplacement in 2009 (procedure performed in Germany).
At the time of the evaluation, a transthoracic echo-cardiogram revealed normal left and right ventricular
systolic function, a normally functioning CoreValve inthe aortic position with trivial anterior periprostheticregurgitation and mean systolic Doppler gradient of7 mm Hg. The mitral bioprosthesis was well seatedwith mean diastolic Doppler gradient of 15 mm Hg atrest (consistent with severe mitral stenosis) and moder-ate central regurgitation. Pulmonary function testsrevealed a severe restrictive pattern with total lungcapacity of 50% and DLCO of 17%. Serum creatininewas 0.9 mg/dl. His estimated STS mortality for afourth elective sternotomy in light of age and comor-bidities was calculated at 14%. After discussion ofalternatives, risks and benefits, a Melody
VRpercutane-
ous valve (Medtronic, Minneapolis, Minnesota) was
1Division of Cardiovascular Diseases, Mayo Clinic, Rochester,Minnesota2Division of Pediatric Cardiology, Mayo Clinic, Rochester, Min-nesota
Additional Supporting Information may be found in the online
version of this article.
Conflict of interest: Dr. Cabalka is a co-investigator in research pro-
tocols utilizing the MelodyVR
valve. Dr. Cabalka does not receive
monetary compensation in any form from Medtronic.
*Correspondence to: Charanjit S. Rihal, MD, Division of Cardiovas-
cular Diseases, Mayo Clinic, Rochester, MN 55905.
E-mail: [email protected]
Received 5 January 2012; Revision accepted 14 March 2012
DOI 10.1002/ccd.24423
Published online in Wiley Online Library (wiley
onlinelibrary.com)
VC 2012 Wiley Periodicals, Inc.
Catheterization and Cardiovascular Interventions 00:000–000 (2012)

selected for off-label transcatheter mitral valve-in-valveimplantation as the Edwards Sapien or the CoreValvewere not yet approved for use in US at the time of theprocedure.
PROCEDURE
Following written, informed consent the patient wasintubated and general anesthesia induced. Real-time 3-Dtransesophageal echocardiogram (TEE) revealed a well-seated mitral bioprosthesis with severely thickened leaf-lets and severe decrease in diastolic excursion (Fig. 1,Supporting information Videos 1 and 2). A 5Fr sheathwas inserted in the right femoral artery and a 7Fr sheathin the ipsilateral vein. Transseptal puncture was per-formed using standard techniques and intravenous hepa-rin was administered. The location of the septal punc-ture was high and posterior (as guided by TEE) therebyallowing more room to manipulate a steerable sheath inthe left atrium and allowing for coaxial orientation ofthe larger valve delivery sheath to the mitral valve oncethe apical rail was established. The inter-atrial septumwas sequentially dilated with 14Fr and 21Fr dilators.Using a steerable 8.5Fr Agilis catheter (St Jude MedicalMinneapolis, MN) and a 0.03500 stiff-angled hydrophilicwire, the stenotic mitral bioprosthesis was crossed (Fig.1 – asterisk, Supporting information Video 1). Becauseof the existing CoreValve aortic prosthesis we elected toavoid crossing this valve to avoid damage to the valve.The alternative option selected was to exteriorize thewire via the left ventricular apex. Left ventricular (LV)apical puncture was performed guided by palpation,transthoracic echocardiogram and fluoroscopy. A 6Frsheath was placed in the LV apex after obtaining access
with an 18 gauge Angiocath (600 Teflon catheter system,Becton-Dickson, San Jose, CA) needle. The stiff-angleguide wire in the left ventricle was snared with a 15 mmAmplatz gooseneck
VRsnare (ev3 Plymouth MN) and
exteriorized via the LV apical sheath thereby creatingan arterio-venous (AV) rail between the LV and theright femoral vein (Figs. 2 and 3). The inner diameter ofthe mitral bioprosthesis was measured at 2 cm and thestrut length at 1.4 cm (Fig. 4), although the reportedinner diameter for this prosthesis by the manufacturer is25 mm. Balloon dilation and sizing of the bioprosthesiswas then performed with a 22 mm Z-Med II balloon(NuMED, Hopkinton, NY). The balloon waist measured18 mm, and a 22 mm Ensemble
VRdelivery system (Med-
tronic, Minneapolis, MN) was selected for implantationof the Melody
VRvalve. The valve was delivered ante-
grade and carefully positioned across the mitral biopros-thesis (Fig. 5, Supporting information Video 3). Thearterio-venous rail created with the exteriorized wirefacilitated successful crossing of the large and relativelystiff delivery system across the interatrial septum andpositioning across the central orifice of the mitral bio-prosthesis with relative ease. The Melody valve prosthe-sis was positioned with a portion of the prosthesis atrialin location, and once we were satisfied with the posi-tioning the valve was deployed with balloon inflation.Fluoroscopy then confirmed a well-seated Melody
VR
valve within the existing mitral bioprosthesis (Fig. 6). 2-D TEE examination revealed no periprosthetic regurgi-tation, trivial central regurgitation (Fig. 7, Supportinginformation Video 4), and diastolic Doppler mean gradi-ent of 2 mm Hg. Real-time 3-D TEE examinationconfirmed a well seated valve-in-valve with normalexcursion of thin leaflets throughout the cardiac cycle
Fig. 1. A: Real-time 3-D TEE diastolic frame from the left atrial (LA) perspective reveals awell seated mitral bioprosthesis (arrowhead 5 sewing ring) with guidewire across theprosthesis (asterisk). Note the severely restricted prosthetic leaflet diastolic excursion.B: Real-time 3-D TEE diastolic frame from the left ventricular (LV) perspective shows severelythickened prosthetic leaflets with restricted diastolic excursion.
2 Michelena et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

(Fig. 8, Supporting information Video 5). The LV apicalpuncture was closed with a 6 mm AVP II plug (AGA,Minneapolis, MN). Total fluoroscopy time was 47 minwith cumulative radiation skin dose of 1611 mGy. Therewere no procedural complications.
OUTCOME
The patient was transferred to the intensive care unitintubated due to post-procedure pulmonary edema. Thepatient was extubated 24 hr after to BIPAP and wasaggressively diuresed for both pulmonary edema andsuspected ARDS. His initial antiplatelet regimenincluded dual antiplatelet therapy with aspirin and Clo-pidogrel. The patient developed thrombocytopenia andhemoptysis with clinical suspicion of disseminatedintravascular coagulation and was treated accordingly.Clopidogrel was discontinued due to thrombocytopeniaand he was not placed on warfarin. The patient pro-gressed satisfactorily and was discharged 17 days after
admission. At 3-month outpatient follow-up, the patientwas tolerating decubitus with resolution of night symp-toms and stable NYHA class II dyspnea.
DISCUSSION
We report successful performance of a percutaneousantegrade mitral valve-in-valve implantation with aMelody
VRvalve in a patient with concomitant aortic
valve prosthesis (CoreValve). Previous-in-human trans-septal anterograde attempts at mitral valve-in-valve(Cribier-Edwards and SAPIEN expandable valves,Edward Life sciences, Irvine, Calif) implantation wereinitially unsuccessful due to extreme difficulty withcrossing the mitral valve and ensuring coaxial place-ment of the new prosthesis across the existing mitralprosthesis [1]. Non-coaxial or too ventricular position-ing of a balloon expandable valve can result in post-deployment embolization [2]. Moreover, open surgical
Fig. 3. Exteriorized glide wire through LV puncture site.
Fig. 2. A: Glide wire snared in the LV (arrow). B: Glide wire exteriorized via the LV apicalsheath (arrow). CV, core valve; MV, mitral bioprosthesis.
Fig. 4. 2-D TEE still frame at 66� shows end-systolic meas-urements of the inner mitral bioprosthetic diameter and strutlength. LA, left atrium; LV, left ventricle.
Transcatheter Valve-in-Valve Implantation 3
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

transatrial approach has also failed to achieve stablecannulation and coaxial positioning within the mitralprosthesis [2]. This has resulted in transapical valvedelivery being the only prior successful technique [1,2]for mitral valve-in-valve implantation. Recently, therehave been reports of successful percutaneous antegradetranscatheter valve-in-valve implantation [3]. This wasachieved in patients with native aortic valves in which
the guide wire was advanced antegrade across the mi-tral and aortic valves, snared in the aorta and exterior-ized via the femoral artery [3]. This case demonstratesfeasibility of the transseptal antegrade approach inwhich passage and exteriorization of the guide wire viathe aortic valve was inadvisable due to existing aorticprosthesis. The LV apical exteriorization of the guide-wire was crucial to achieving success as it provided analternative to passage of the guide wire via the aorticvalve allowing us to deliver the large valve ensemble.It also provided a stable/maneuverable platform thatensured delivery of the large valve apparatus allowingcoaxial positioning of the expandable valve within themitral prosthesis. Exteriorization of the guide wireallows and provides better coaxial alignment for therelatively stiff delivery system than passage of theguide wire via the aortic valve. With the transseptalwire exteriorized there is a more gradual curve throughthe mitral valve that the larger 22Fr delivery systemwill track nicely, rather than a tighter, U-shaped, path-way typically produced with the guide wire passedthrough the aortic valve. Rapid ventricular pacing wasnot used in our case as initial inflation of the inner bal-loon showed that the valve-in-valve position was verystable, but this may be of utility in stabilizing the valveif needed [3].
Fig. 5. A: MelodyVR
valve co-axially positioned across the mitral bioprosthesis (arrow).B: MelodyV
R
valve deployed (arrow). C: MelodyVR
valve post deployment LAO view (arrow).D: MelodyV
R
valve post deployment LAO caudal view (arrow).
Fig. 6. A: 2-D TEE systolic still frame at 69� depicts normallycoapting, thin, Melody valve leaflets. B: Systolic color-flowDoppler shows trivial central regurgitation and no evidence ofperiprosthetic leaks. LA, left atrium; LV, left ventricle.
4 Michelena et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).
It should be noted that LV apical puncture as usedin this case is not an entirely benign procedure. Thereis a learning curve associated with adequate perform-ance of this procedure and it should only be performedby interventionalists proficient and familiar with thetechnique. Complication rates reported in literaturehave ranged from 8 to 40% [4] and known complica-tions of this procedure includes development of peri-cardial or pleural effusions, coronary artery laceration,access site bleeding, and death [4].
Sizing of the bioprosthesis is based on knowledge ofthe manufacturer’s dimension which includes the innerand outer diameters and the height of the prosthesis.The inner diameter is the most important dimension toaccurately evaluate when planning for a valve-in-valveprocedure. The existing bioprosthetic valve innerdiameter is initially evaluated using transesophagealechocardiography, but compliant balloon sizing isabsolutely critical to be certain that the valve innerdiameter is not too large to safely seat the Melody
VR
bioprosthesis. Though not used in this case multislicecomputed tomographic scan may also be of value inassessing the dimensions of the bioprosthesis.
The MelodyVR
valve was chosen because it was theonly available transcatheter valve in the US at the timeof the procedure. The valve is made of bovine jugularvein sutured within a platinum-iridium stent [5]. Origi-nally developed for placement in the low-pressure dys-functional right ventricular outflow tract (RVOT) con-duits marked by either stenosis or regurgitation [5].There have been few cases in which this valve hasbeen used in a high-pressure circulation with placementin aortic and mitral valves or dysfunctional RVOT con-duits with associated significant pulmonary hyperten-
sion [6]. Short-term performance of the MelodyVRvalve
prosthesis in this high-pressure circulation, has beenencouraging. One of the patients followed for 2 yearspost implant had excellent function of the Melody
VR
valve prosthesis which had been placed in the mitralposition [6]. Nonetheless the use of the Melody
VRvalve
in the aortic or mitral position is off label and longterm durability of the valve in this situation remains tobe determined. The recent approval and availability ofthe Edward Sapien valve in the US would provide analternative valve to be used in lieu of the Melody valvein these situations.
CONCLUSION
We report an alternative and innovative approach topercutaneous transvenous antegrade delivery and per-formance of mitral valve-in-valve procedure in apatient with an existing aortic prosthetic valve. Thisapproach may be beneficial in patients with existingaortic prosthesis or patients in whom delivery of thevalve apparatus with an antegrade wire passed via theaortic valve is difficult.
REFERENCES
1. Cheung AW, Gurvitch R, Ye J, Wood D, Lichtenstein SV,
Thompson C, Webb JG. Transcatheter transapical mitral valve-
in-valve implantations for a failed bioprosthesis: A case series.
J Thorac Cardiovasc Surg 2011;141:711–715.
2. Webb JG, Wood DA, Ye J, Gurvitch R, Masson JB, Rodes-
Cabau J, Osten M, Horlick E, Wendler O, Dumont E. Transcath-
eter valve-in-valve implantation for failed bioprosthetic heart
valves. Circulation 2010;121:1848–1857.
3. Montorfano M, Latib A, Chieffo A, Moshiri S, Franco A,
Grimaldi A, Alfieri O, Colombo A. Successful percutaneous
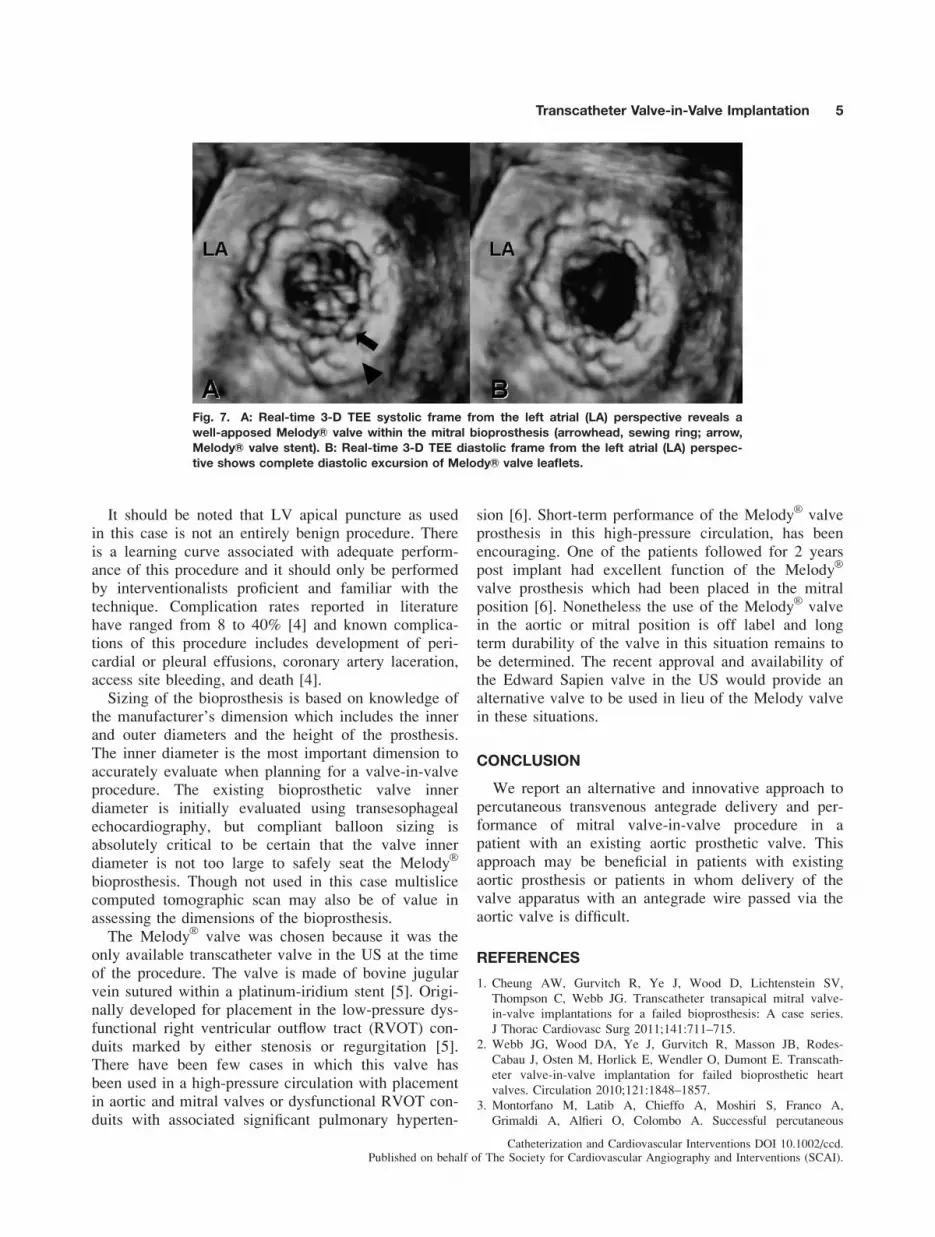
Fig. 7. A: Real-time 3-D TEE systolic frame from the left atrial (LA) perspective reveals awell-apposed MelodyVR valve within the mitral bioprosthesis (arrowhead, sewing ring; arrow,MelodyVR valve stent). B: Real-time 3-D TEE diastolic frame from the left atrial (LA) perspec-tive shows complete diastolic excursion of MelodyVR valve leaflets.
Transcatheter Valve-in-Valve Implantation 5
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

anterograde transcatheter valve-in-valve implantation in the
mitral position. JACC. Cardiovasc Interv 2011;4:1246–
1247.
4. Pitta SR, Cabalka AK, Rihal CS. Complications associated with
left ventricular puncture. Catheter Cardiovasc Interv: Off J Soc
Cardiac Angiography Interv 2010;76:993–997.
5. Bonhoeffer P, Boudjemline Y, Saliba Z, Merckx J, Aggoun Y,
Bonnet D, Acar P, Le Bidois J, Sidi D, Kachaner J. Percutaneous
replacement of pulmonary valve in a right-ventricle to pulmo-
nary-artery prosthetic conduit with valve dysfunction. Lancet
2000;356:1403–1405.
6. Hasan BS, McElhinney DB, Brown DW, Cheatham JP, Vincent
JA, Hellenbrand WE, Jones TK, Zahn EM, Lock JE. Short-term
performance of the transcatheter melody valve in high-pressure
hemodynamic environments in the pulmonary and systemic circu-
lations. Circ Cardiovasc Interv 2011;4:615–620.
6 Michelena et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).





























