Embed Size (px)
Citation preview
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 127
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
Stressed Spaces: Mental Health and ArchitectureKathleen Connellan, PhD; Mads Gaardboe, MA; Damien Riggs, PhD; Clemence Due, PhD; Amanda Reinschmidt; and Lauren Mustillo
OBJECTIVE: To present a comprehensive review of the research litera-ture on the effects of the architectural designs of mental health facilities on the users.
BACKGROUND: Using a team of cross-disciplinary researchers, this review builds upon previous reviews on general and geriatric healthcare design in order to focus on research undertaken for mental health care facility design.
METHODS: Sources were gathered in 2010 and 2011. In 2010 a broad search was undertaken across health and architecture; in 2011, using keywords and 13 databases, researchers conducted a systematic search of peer reviewed literature addressing mental health care and architec-tural design published between 2005 to 2012, as well as a systemat-ic search for academic theses for the period 2000 to 2012. Recurrent themes and subthemes were identified and numerical data that emerged from quantitative studies was tabulated.
RESULTS: Key themes that emerged were nursing stations, light, ther-apeutic milieu, security, privacy, designing for the adolescent, forensic facilities, interior detail, patients’ rooms, art, dementia, model of care, gardens, post-occupancy evaluation, and user engagement in design process. Of the 165 articles (including conference proceedings, books, and theses), 25 contained numerical data from empirical studies and 7 were review articles.
CONCLUSIONS: Based on the review results, especially the growing evi-dence of the benefits of therapeutic design on patient and staff well-being and client length of stay, additional research questions are suggested concerning optimal design considerations, designs to be avoided, and the involvement of major stakeholders in the design process.
KEYWORDS: Evidence-based design, hospital, interdisciplinary, litera-ture review, post-occupancy
ABSTRACT
AUTHOR AFFILIATIONS: Kathleen Connellan, PhD, is a Senior Lecturer in the Division of Education, Arts and Social Sciences in the School of Art, Architec-ture and Design at the University of South Australia in Adelaide, South Austra-lia, Australia. Mads Gaardboe, MA, is the Head of School for the School of Art, Architecture and Design at the University of South Australia in Adelaide, South Australia, Australia. Damien Riggs, PhD, is a Senior Lecturer in Social Work and Social Planning in Social and Behavioural Sciences at Flinders University in Adelaide, South Australia, Australia. Clemence Due, PhD, is an Associate Lecturer and Research Associate in the School of Psychology at the University of Adelaide in Adelaide, South Australia, Australia. Amanda Reinschmidt and Lauren Mustillo are Research Assistants at the University of South Australia in Adelaide, South Australia, Australia.
CORRESPONDING AUTHOR: Kathleen Connellan, PhD, Division of Education, Arts and Social Sciences; School of Art, Architecture and Design; University of South Australia, City West Campus, Adelaide, South Australia 5001, Australia; [email protected]; +61 8 830 20355.
PREFERRED CITATION: Connellan, K., Gaardboe, M., Riggs, D., Due, C., Reinschmidt, A., & Mustillo L. (2013). Stressed spaces: Mental health and architecture. Health Environments Research & Design Journal, 6 (4), pp. 127–168

128 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
IntroductionThe research question identified for this literature review was: How does the intersection of mental health care and architecture contribute to positive mental health outcomes? We arrived at this research question because it is sufficiently focused but still broad enough to incorporate important variables such as differ-ent models of care.
The University of South Australia’s Mental Health Research Group was the cata-lyst for the formation of an interdisciplinary team of researchers across architec-ture, design, mental health practice, and psychology. The team, called “Stressed Spaces: Mental Health and Architecture,” won two consecutive university fund-ing grants to conduct research in purpose-built mental health facilities in 2010 and 2011. As part of that collaboration, a survey on the existing literature on the crossover of mental health and architectural research was conducted. The scar-city of research literature dealing with both mental health and architecture along with the specific lack of evidenced-based research was noted, prompting the team to conduct additional research. In the process, the team wrote this review article building upon the most recent literature review publications, from Ulrich et al. (2008) in general healthcare, to Dobrohotoff and Llewellyn-Jones (2010) on geriatric healthcare.
The objective of this article is to present an updated review of the literature across health and architecture, but with a specific focus on mental health care and design in order to make a contribution to this field and assist other researchers, architects, and clinical practitioners in their quest for improved mental health outcomes. The multiple considerations in the complex crossover of architectural design and mental health require multidisciplinary collaboration, as is evidenced by our team of researchers, policy makers, advisors, and partners. The team com-prises two architectural firms that specialize in healthcare design, one based in Australia and the other in the United Kingdom; one experienced architect now heading the School of Art, Architecture and Design at the University of South Australia; two social scientists with backgrounds in psychology; one senior men-tal health nurse; one professor in mental health nursing at the University of South Australia; and one senior lecturer in design theory at the University of South Australia, specializing in design and well-being. Such collaborations have been indicated as an essential aspect of the development of nine more efficacious designs.
The broad socio-economic and political context factors present at the time this article was written included the social context of an aging population in most Western and “developed” countries; the “modern” diseases frequently associated with those countries (such as depression and mental illness, substance abuse, diabetes, obesity, heart disease); the political power held by aging baby boomers (who form a large and comparatively wealthy demographic) to demand compre-hensive health services; the technological impacts of extending life at all costs; the costs of providing the expected standards of healthcare; and the attendant hospital facility construction boom. With these contexts and issues in mind, we observed the emergence of the following themes from the current body of litera-ture: nursing stations, light, therapeutic milieu, security, privacy, designing for

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 129
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
the adolescent, forensic facilities, interior detail, patients’ rooms, art, dementia, model of care, gardens, post-occupancy evaluation, and user engagement in the design process. From these key themes, we learned that only some (25 of the 165) research articles generated evidence-based numerical data. From this data, we also know that the key themes also represent the areas that require more research as they are identified as crucial to improved mental health outcomes. There is no question that the old institutional model of care with its associated asylum-style architectural design is anathema to mental health practice; however, with the construction of new facilities, we question the extent to which seemingly inno-vative designs match contemporary mental health models of care. The gaps in research represent the lack of reliable post-occupancy reviews of facilities. There-fore, this review also questions why that gap exists. Do, for example, ethical pro-tocols and concerns with qualitative methods on vulnerable populations present too much of an obstacle for researchers and hospitals?
Of the 165 research articles, seven were literature review articles, published between 2000 and 2010. The primary reason for writing any literature review is, of course, to share the state of research on a particular subject with the commu-nity. However, this is not the sole reason for doing so, and each of the seven liter-ature review fulfills its own perceived need. Two concentrate upon aged care and design (Day, Carreon, & Stump, 2000; Dobrohotoff & Llewellyn Jones, 2010), and the remaining five center on design with different foci: light and lighting (Anjali, 2006); art (Daykin, Byrne, Soterious, & O’Connor, 2008); safety (Reil-ing, Hughes, & Murphy, 2008); patient rooms and well-being (Lorenz, 2007); and evidenced-based design (Ulrich et al., 2008). Each of the review articles summarizes the recommendations based on previous findings; however, the findings of these predominantly systematic reviews emphasized to us that this area of research runs the risk of losing itself in disparate detail. Consequently, there is a need for more frequent comprehensive reviews of the broad field of mental health and architecture crossovers in the research literature so as to form a platform for other more focused and detailed studies.
MethodologyFor this article we combined comprehensive and systematic reviews of the litera-ture on mental health and architecture. The reason for this lies in the two sepa-rate time periods dedicated to the literature surveys. The first time period (2010) involved a scoping study, which included architecture and health websites and did not set dates or tight exclusions for the searches. In the second time period (2011) we utilized selected databases, set dates, and utilized a defined keyword search criteria (see Table 1). The initial scoping study resulted in 78 articles, of which 19 were annotated according to their mental health focus and empiri-cal/numerical data. On the basis of these findings, we developed a systematic approach to build upon the first literature search, retaining the articles that pre-dated the set start dates for the second literature search.
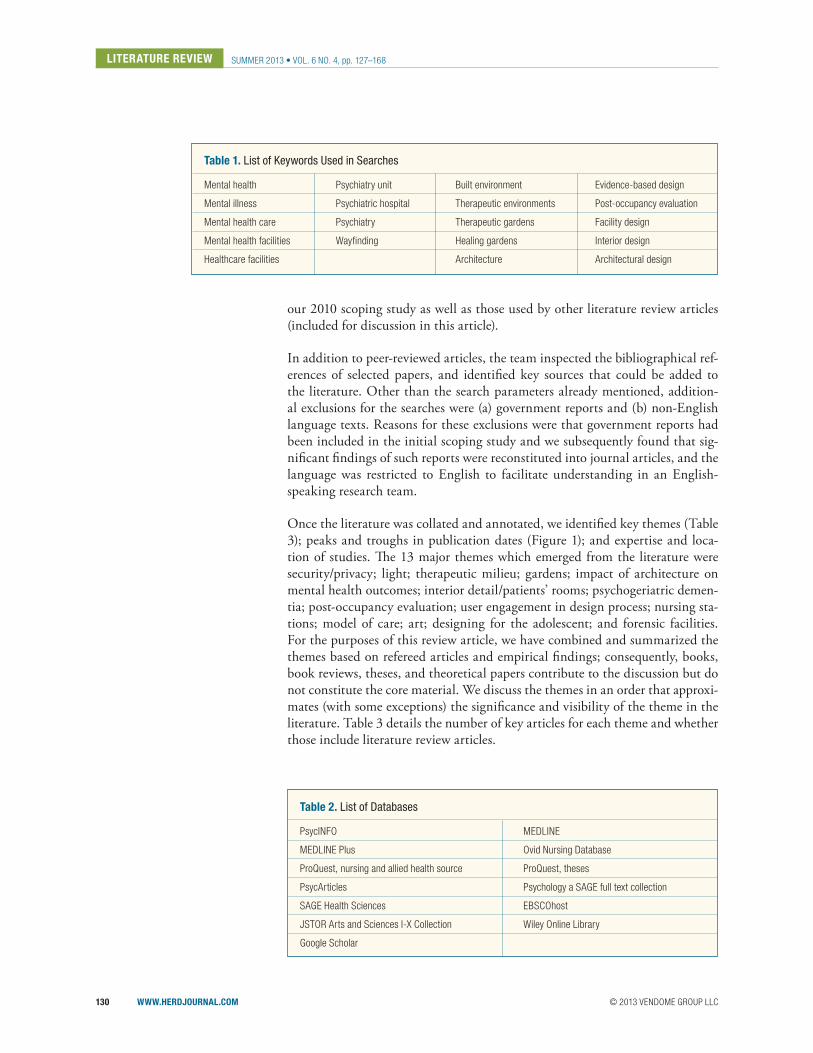
The dates set for searching the literature in the second (systematic stage) were 2000–2011. The keywords used for the searches are listed in Table 1 and the databases searched are listed in Table 2. The keywords were chosen based on
130 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
our 2010 scoping study as well as those used by other literature review articles (included for discussion in this article).
In addition to peer-reviewed articles, the team inspected the bibliographical ref-erences of selected papers, and identified key sources that could be added to the literature. Other than the search parameters already mentioned, addition-al exclusions for the searches were (a) government reports and (b) non-English language texts. Reasons for these exclusions were that government reports had been included in the initial scoping study and we subsequently found that sig-nificant findings of such reports were reconstituted into journal articles, and the language was restricted to English to facilitate understanding in an English-speaking research team.
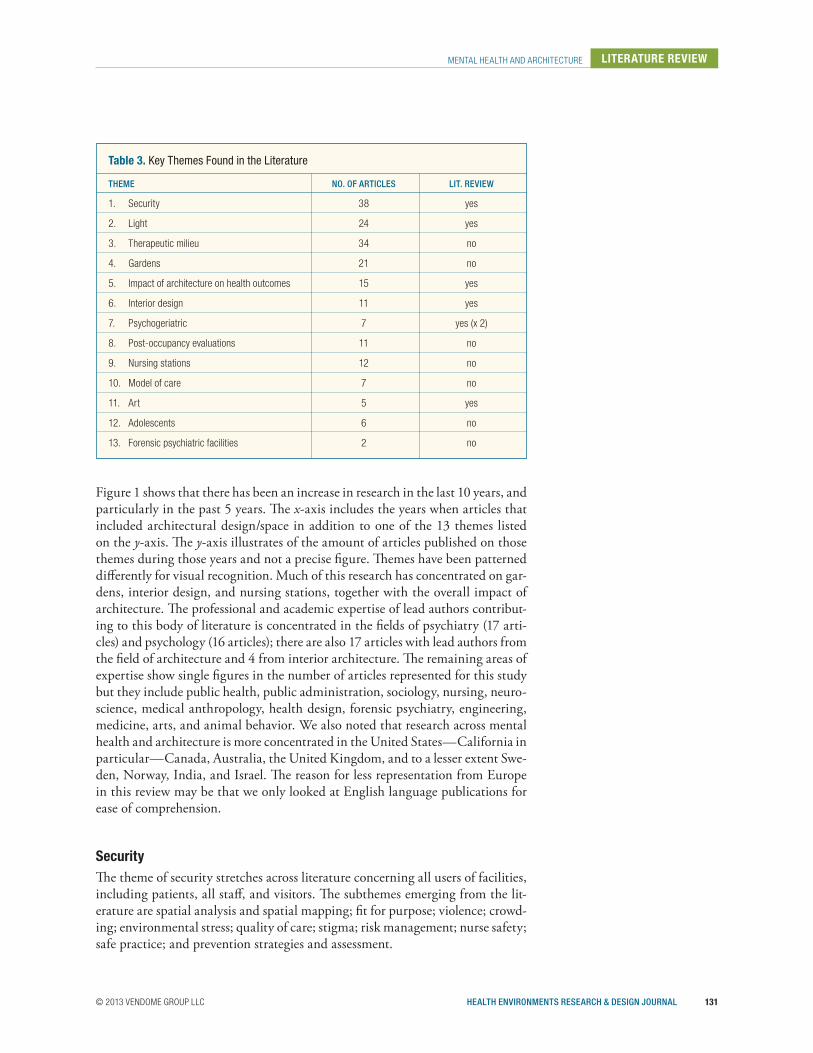
Once the literature was collated and annotated, we identified key themes (Table 3); peaks and troughs in publication dates (Figure 1); and expertise and loca-tion of studies. The 13 major themes which emerged from the literature were security/privacy; light; therapeutic milieu; gardens; impact of architecture on mental health outcomes; interior detail/patients’ rooms; psychogeriatric demen-tia; post-occupancy evaluation; user engagement in design process; nursing sta-tions; model of care; art; designing for the adolescent; and forensic facilities. For the purposes of this review article, we have combined and summarized the themes based on refereed articles and empirical findings; consequently, books, book reviews, theses, and theoretical papers contribute to the discussion but do not constitute the core material. We discuss the themes in an order that approxi-mates (with some exceptions) the significance and visibility of the theme in the literature. Table 3 details the number of key articles for each theme and whether those include literature review articles.
Table 1. List of Keywords Used in Searches
Mental health Psychiatry unit Built environment Evidence-based design
Mental illness Psychiatric hospital Therapeutic environments Post-occupancy evaluation
Mental health care Psychiatry Therapeutic gardens Facility design
Mental health facilities Wayfinding Healing gardens Interior design
Healthcare facilities Architecture Architectural design
Table 2. List of Databases
PsycINFO MEDLINE
MEDLINE Plus Ovid Nursing Database
ProQuest, nursing and allied health source ProQuest, theses
PsycArticles Psychology a SAGE full text collection
SAGE Health Sciences EBSCOhost
JSTOR Arts and Sciences I-X Collection Wiley Online Library
Google Scholar
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 131
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
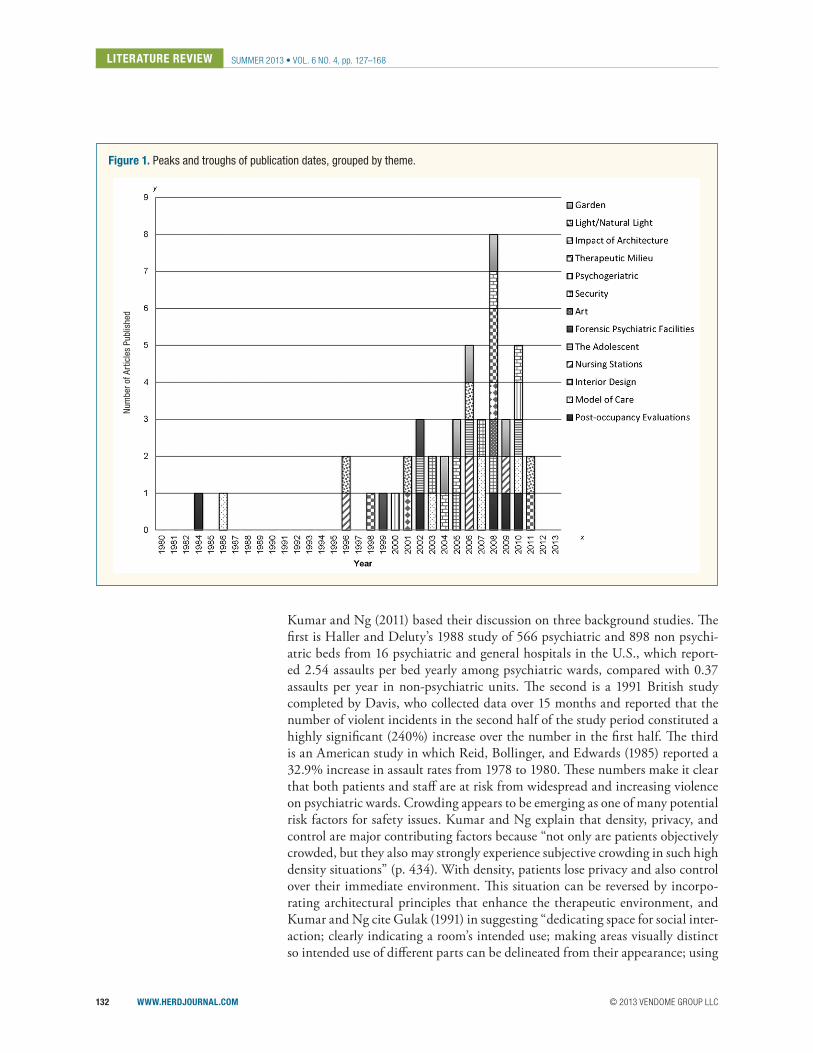
Figure 1 shows that there has been an increase in research in the last 10 years, and particularly in the past 5 years. The x-axis includes the years when articles that included architectural design/space in addition to one of the 13 themes listed on the y-axis. The y-axis illustrates of the amount of articles published on those themes during those years and not a precise figure. Themes have been patterned differently for visual recognition. Much of this research has concentrated on gar-dens, interior design, and nursing stations, together with the overall impact of architecture. The professional and academic expertise of lead authors contribut-ing to this body of literature is concentrated in the fields of psychiatry (17 arti-cles) and psychology (16 articles); there are also 17 articles with lead authors from the field of architecture and 4 from interior architecture. The remaining areas of expertise show single figures in the number of articles represented for this study but they include public health, public administration, sociology, nursing, neuro-science, medical anthropology, health design, forensic psychiatry, engineering, medicine, arts, and animal behavior. We also noted that research across mental health and architecture is more concentrated in the United States—California in particular—Canada, Australia, the United Kingdom, and to a lesser extent Swe-den, Norway, India, and Israel. The reason for less representation from Europe in this review may be that we only looked at English language publications for ease of comprehension.
SecurityThe theme of security stretches across literature concerning all users of facilities, including patients, all staff, and visitors. The subthemes emerging from the lit-erature are spatial analysis and spatial mapping; fit for purpose; violence; crowd-ing; environmental stress; quality of care; stigma; risk management; nurse safety; safe practice; and prevention strategies and assessment.
Table 3. Key Themes Found in the Literature
THEME NO. OF ARTICLES LIT. REVIEW
1. Security 38 yes
2. Light 24 yes
3. Therapeutic milieu 34 no
4. Gardens 21 no
5. Impact of architecture on health outcomes 15 yes
6. Interior design 11 yes
7. Psychogeriatric 7 yes (x 2)
8. Post-occupancy evaluations 11 no
9. Nursing stations 12 no
10. Model of care 7 no
11. Art 5 yes
12. Adolescents 6 no
13. Forensic psychiatric facilities 2 no
132 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
Kumar and Ng (2011) based their discussion on three background studies. The first is Haller and Deluty’s 1988 study of 566 psychiatric and 898 non psychi-atric beds from 16 psychiatric and general hospitals in the U.S., which report-ed 2.54 assaults per bed yearly among psychiatric wards, compared with 0.37 assaults per year in non-psychiatric units. The second is a 1991 British study completed by Davis, who collected data over 15 months and reported that the number of violent incidents in the second half of the study period constituted a highly significant (240%) increase over the number in the first half. The third is an American study in which Reid, Bollinger, and Edwards (1985) reported a 32.9% increase in assault rates from 1978 to 1980. These numbers make it clear that both patients and staff are at risk from widespread and increasing violence on psychiatric wards. Crowding appears to be emerging as one of many potential risk factors for safety issues. Kumar and Ng explain that density, privacy, and control are major contributing factors because “not only are patients objectively crowded, but they also may strongly experience subjective crowding in such high density situations” (p. 434). With density, patients lose privacy and also control over their immediate environment. This situation can be reversed by incorpo-rating architectural principles that enhance the therapeutic environment, and Kumar and Ng cite Gulak (1991) in suggesting “dedicating space for social inter-action; clearly indicating a room’s intended use; making areas visually distinct so intended use of different parts can be delineated from their appearance; using
Figure 1. Peaks and troughs of publication dates, grouped by theme.
Num
ber o
f Art
icle
s Pu
blis
hed
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 133
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
colors to enhance activities and spaces; using various materials to provide different tactile and visual experiences; using light-ing to help define space; and finally, making the spaces that have special meaning to patients stand out” (p. 434).
None of the above elements (or the lack thereof) provide the sole explanation for the violence associated with crowding; possible reasons can only come from combinations and exam-ination of specific sites. Kumar and Ng refer to Nijman and Rector’s 1999 study that found providing additional space on an acute-care psy-chiatric ward lessened episodes of aggression.
Johnstone (2004) notes that people in ward environments occupy 70% less space than did their counterparts of 150 year ago. Johnstone drew his findings from the National Patients Safety Agency’s (NPSA) country pilot audit that revealed that “out of 1,367 [statutory] mental health notifications, 89% relate to unsafe ward environments, [and within that 89%] 438 reports relate to violence and aggression, 300 reports relate to self-harm, 107 reports relate to absconding, and 39 reports relate specifically to the environment” (p. 30). Johnstone does not pro-vide the additional report details but emphasizes that the goals to be achieved to ensure fit for purpose are safety, privacy, dignity, and adequate areas for thera-peutic treatment, and warns that even if a building is “big enough, clean and beautiful to look at” (p. 1), that cannot be seen as an end unto itself. It must be adequate in terms of both therapeutical potential and freedom of movement.
Brickell and McLean (2011) focused on patient security in terms of quality of care, stigma and health outcomes. They built upon existing research by soliciting the help of Canadian, Australian, and American mental health care professionals working in the field of patient health and/or patient safety, which led to inter-views with 72 participants. These interviews revealed a diversity of perspectives on patient safety and mental health but an absence of a clear definition, lead-ing to the confusion over whose safety is covered by the term. One interviewee observed that “when you look at patient safety issues … [it’s] about keeping staff safe from patients, and it’s not about how do we keep the patient safe” (p. 41). Thirty-two percent of those interviewed felt it necessary to balance patient safe-ty with their rights and autonomy. Interviewees also cited such adverse events as slip-and-fall accidents, concerns about medication and substance abuse, the potential for self-harm or sexual assault, the issue of smoking and threat of fire, the risk of leaving the facility without authorization, and harm resulting from restraints as significant concerns.
Security concerns were also implicated in terms of issues around measures taken to protect clients from self-harm. For example, Langan and McDonald (2008) addressed patient dignity via the clothes they are permitted to wear in the units. In an acute psychiatric inpatient setting in the Republic of Ireland, Langan and McDonald used a triangulation research design to investigate the prevalence of attitudes towards the practice of “dressing inpatients in night attire during day-time despite the lack of evidence to support its benefit in reducing absconding or self-harm.” Case note reviews from their study revealed a high prevalence of
Not only are patients objectively crowded, but they also
may strongly experience subjective crowding in such
high density situations.

134 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
this practice (57%) and its significant association with involuntary admission. Their results also showed that “nursing staff believed that using night attire was effective at reducing absconding and self-harm, and that only voluntary patients should retain the right to choose their clothes. Most patients interviewed were uncomfortable in night clothes and indicated that they should be entitled to choose what to wear.” In fact, the researchers observed that, while it may run counter to the advice of some psychiatrists, it should be noted that “patients may perceive this as undermining their autonomy” and a different approach may be “more acceptable to patients and more respectful of their dignity” (p. 223).
Jayaram and Herzog (2008) conducted a study under the auspices of the Com-mittee on Patient Safety for the American Psychiatric Association in which they reviewed “SAFE MD”:
• S—suicide
• A— aggressive behavior and promotion of the safe use of seclusion and restraints
• F—falls
• E—elopement
• M—complications when dealing with medical co-morbidities
• D—drug/medication errors
In addition, this study focuses on safe practice, prevention strategies, and assess-ment. The results deal with frequency of SAFE MD events applicable to psychi-atric care. In an analysis of 3,548 events in 2005, the authors noted events that included suicide (13.1%), medication errors (10.1%), patient falls (5.3%), death or injury due to the use of restraints (3.9%), and elopement (1.9%).
Commonalities among all publications that relate to safety and security include the acknowledgment of increased crowding and loss of privacy as a risk factor; “violence against patients and staff in psychiatric wards is both prevalent and increasing” (Kumar & Ng, 2001, p. 433); general recommendations are that standardized, single variable-acuity rooms mean that patients do not have to be moved when their condition changes, enhancing a sense of normalcy and con-trolling the spread of infection (where applicable). In addition, visually distinct spaces ensure that the function of the space is clear.
LightThe second distinct theme that emerged as a significant design feature affecting mental health outcomes was that of light and lighting. Although we give light and lighting a separate focus in this review article, it is also the one theme that is common to all others. A major subtheme is that of natural light, which is linked to the following issues in the literature: eating disorders, depression, circadian rhythm, Alzheimer’s disease, sensory stimulation, therapeutic design, and thera-peutic patient rooms.
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 135
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
Joseph’s 2006 review of the available literature focused on the impact of light on outcomes in healthcare settings (without a specific focus on mental health facili-ties) and divided the findings into several categories. The first category was the way in which lighting enables accurate performance of visual tasks, logically, by reducing error. The second was how light affects mood and perception. In that case, it was noted that positive impacts included daylight and proximity to windows; alternately, the negative impact of “glare and thermal discomfort on mood and task performance” were evident. The third category in Joseph’s review focused on the control of the circadian system, which included a number of ben-efits (e.g., substantial increases in the quality of sleep and enhanced rest–activity patterns in patients with dementia). Joseph also mentioned eleven studies that suggested connections between exposure to bright light and depression; symp-toms of seasonal affective disorder (SAD) and the depressive phase of bipolar disorder were diminished through exposures “between 2,500 and 10,000 lux,” with the greatest benefits found in the morning rather than the evening. Further, Joseph cited Beauchim and Hays (1996) as well as Benedetti et al. (2001) as doc-umenting a connection between exposure to light and the length of depressed patients’ stays in the hospital.
Joseph referenced the work of Watch et al. (2005) as to bright versus shaded sides of the hospital in stating that “patients staying on the bright side of a hospital unit were exposed to 46% higher-intensity sunlight on average; it was found that patients exposed to an increased intensity of sunlight experienced less perceived stress, marginally less pain, and had 21% less pain medication costs” (p. 6). The recommendations for adjusting light and lighting to facilitate good health out-comes from Joseph’s review pointed to the following: provide windows for natu-ral light in patient rooms, with provisions for control of glare and temperature; orient patient rooms to maximize early morning sun exposure; provide high lighting for complex visual tasks—reduce errors; provide windows in staff break rooms (p. 9).
In a paper on healing spaces, Schweitzer, Gilpin, and Frampton (2004) noted the different effects of natural versus artificial lighting on patients, specifically in the areas of illuminance, uniformity, diffusion, color, and UV radiation. These, in turn, affect human chronobiology, contributing to, for example, seasonal affective disorder (SAD), sleep disorders, and work disruptions. In addition, the natural circadian rhythm of light regulates melatonin production, influencing biochemical and hormonal body rhythms. On this topic, Basinger’s (2011) thesis says that the body’s circadian rhythms are governed by eating and regulation to natural light cycles; therefore, because eating disorder patients cannot use food to regulate the body, natural light is a key design consideration. Brawley’s 2001 article in Aging & Mental Health asserted that light requirements for older people may be five times higher than that of young people. Older adults take between 5 and 30 minutes to adapt to change when entering space with considerably lower light level, such as entering from outside. Brawley focused on the links between Alzheimer’s, therapeutic design, and sensory stimulants, saying that lighting is important for more than just vision, affecting endocrine systems and producing Vitamin D, as well as other benefits already mentioned. The positive associations of daylight and routine activities outdoors with sensory stimulation

136 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
and interaction with nature was seen to have a beneficial effect on patients suf-fering from Alzheimer’s; however, the problem of controlling indoor glare and flicker were also acknowledged. In a study conducted in a psychiatric hospital in Edmonton, Canada, over a 2-year period in the late 1990s, Beauchemin and Hays (1996) observed that patients in brightly lit rooms stayed on average 16.9 days versus19.5 days for those in dimly lit rooms, a difference of nearly 3 days (2.6 days difference).
Commonalities for all publications related to light include the importance of controlling the circadian system. Natural circadian rhythms regulate melatonin production, which influences biochemical and hormonal body rhythms, which have the following effects upon mental health: reduced depression, decreased length of stay, improved sleep and circadian rhythm, lessened agitation, eased pain, and easier adaptation to night-shift work. The interdisciplinary aspect of light makes it a challenging theme for focused research; for example, Joseph’s 2006 literature review crossed the disciplines of architecture, medicine, psychol-ogy, ergonomics, and lighting design.
Therapeutic MilieuThe therapeutic milieu incorporates a range of thematic features that overlap with other key issues but which we combine into a single theme that encompasses the social and psychological aspects of environmental design. Therapeutic milieu is a term that is also interchangeable with patient-centered design and healing environments. Consequently, the subthemes included here are both numerous and varied; they include rehabilitation, best practice considerations, ambient fea-tures, social features, nursing stations, staff perceptions, program evaluation, the Planetree approach, positive design, multidisciplinary input, architectural change, and psychiatric intensive care units.
Novotna, Urbanoski, and Rush (2011) focused on staff perceptions and program evaluation in client-centered design of residential addiction and mental health care facilities. They discussed the findings of a 3-year series of focus groups, con-ducted both pre- and post-occupancy between 2007 and 2009, using mixed-method evaluation of clinical programs in a large mental health and substance abuse facility in Canada. The main priorities of their research were (a) the impact of the physical design on clients and service delivery; and (b) the impact of physi-cal design on the working environment. Positive outcomes and perceptions from the focus groups made repeated reference to comfort, abundance of natural light, freedom, reduced stigma with new spatial designs that mimicked a “normal” community setting and an enhanced sense of well-being; however, these were partially balanced with negative outcomes and perceptions around limited staff space and the ability to share confidential information, and staff concerns due to reduced sightlines to clients as a result of the changes meant to facilitate greater movement among staff and clients.
Golembiewski (2010) looked at the significance of architectural design in psy-chiatric care facilities and analyzed the architectural elements that may influence mental health. He explored Antonovksy’s salutogenic theory “that better health

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 137
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
results from a state of mind which has a fortified sense of coherence” (p. 100) from an architectural perspective. From a psychiatric point of view, the saluto-genic perspective is that the relationship between a patient and environment is understood as being transactional and not fixed. Generally salutogenic now indi-cates a focus upon holistic human wellbeing rather than disease cause and effect. In this way, Golembiewski notes the environment should ensure that perceptual cues are present to assist perceptual processes; clear textures, objects and lines should prevent the possibility of perceptual distortion and ambiguity. Object comprehension is manufactured through filters of memory, culture and epis-temology; therefore, the environment should be familiar to psychotic patients as this helps stabilize both comprehension and delusions. Such an environment should mimic a safe and cozy home where noise is kept to a minimum; echoes, as well as repetitive sounds, should be eliminated as much as possible as this exacerbates delusional “voices.” In terms of control and meaningfulness, the salutogenic approach should encourage day to day “outside” domestic tasks (cooking, washing) and limit the number of people in shared spaces. The outside world should not be sepa-rated from the patient. For that reason, access to nature, pets, and supported communication with family and friends is essential to rehabilitation. To this end, environmental stimu-lation should provide sensory gratification.
Stichler’s (2008) article, “Healing by Design,” reviews the Planetree approach to architectural design. This is not dissimilar to Golembiewski’s (2010) inter-pretation of the salutogenic model; however, Stichler’s work does not focus on mental health as such. She states that architectural aspects of healing environ-ments include those elements that create an optimally restful patient environ-ment. These components include views to the outside or, if that is not possible, at least images of nature; adequately sized bathrooms; extra seating provided as an alternative to the bed; reduced noise levels; a variety of lighting options; comfortable room temperatures; and close attention paid to aesthetics. And for “staff, designs should address: the work flow process of caregiving to minimize the steps necessary to secure supplies and equipment; safety features that reduce employee injuries resulting from repetitive movement, patient lifting, mobiliza-tion, and transfers; visual access of patients from nursing stations or documenta-tion alcoves; security designs to enhance protection of staff from hostile visitors; and staff stress reduction with the design of respite rooms (quiet, meditative envi-ronments)” (Stichler 2008, p. 507). These features incorporate some of the nine Planetree elements of patient-centered care, which are:
1. Human interaction
2. Consumer and patient education
3. Healing partnerships with the patients’ family and friends
4. Nurturing through food and nutrition
5. Spirituality
6. Human touch
7. Healing arts and visual therapy
[B]etter health results from a state of mind which has a
fortified sense of coherence.

138 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
8. Integration of complementary therapies
9. Healing environments created in the architecture and design of the healthcare setting (p. 504)
The Planetree elements and the salutogenic model are commensurate with the aims of The Center for Healthcare Design’s Pebble Project (http://www.health-design.org/pebble) as well as models for “new residentialism” and “critical region-alism,” as explained in Verderber and Fine (2000). All of these approaches strive to move away from both the bureaucratization locked into some of the architec-tural language of modernism (Verderber & Fine, 2000) and to depart completely from conservatism of the institution.
Karlin and Zeiss (2006) reviewed environmental and therapeutic issues in psy-chiatric hospital design over the 50 years prior to their article and noted several considerations for best practice, including patient-centered design; ambient fea-tures; architectural features (physical plan, layout, size and shape of units); social features; and nursing station design and placement. These authors recommended the enhanced privacy associated with single rooms and private visiting areas that facilitate intimacy but noted that unit design should also encourage family par-ticipation and group activities. They mentioned that gardens and views of nature serve as positive distractions. In terms of interior design, furnishings should be such that they have minimal institutional connotations, and they observed that while the studies of the optimum choices for wall color show inconsistent results, blue tones can be calming and bland color schemes and trendy palettes should be avoided. They also suggested that it is important to incorporate spatial flexibility into design and that social features are also applicable to staff, who require loung-es and/or a garden to promote their own communication and job satisfaction.
The theme of the therapeutic milieu in healthcare design, particularly mental health care design, is even more dependent upon multidisciplinary expertise than other themes. This is not a recent realization, and papers from the late 1990s include research findings regarding multidisciplinary input to design, architectural change and positive outcomes that have remained relevant. For example, Gross, Sasson, Zarhy, and Zohar (1998) review empirical studies and, in particular, one case study of a psychiatric hospital in Israel where design and execution was conducted by a multidisciplinary team of architects, psychiatrists, and other mental health professionals and administrators. The major design goal was for the “humane, efficient containment and reduction of severe psychopa-thology. Here it was the role of psychiatrists and other mental health workers to redirect the focus of ward design to the patients and their families” (p. 108). As a result, design elements included no overcrowding so that patients were not forced to interact with too many people; provision of a variety of spaces that supported social interaction; an abundance of “classical” daylight and fresh air; openness of design to encourage staff to leave the nursing station and spend more time in the day room; meticulous care of buildings and grounds to reduce van-dalism; easy observation of patients; and segregation of staff work and rest areas. Dix and Williams (1996) made recommendations for the design of psychiatric intensive care units, suggesting that the sites/wards should be on the ground

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 139
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
floor with access to enclosed gardens with standard fencing or hedges; that they should have a separate entrance, and corridors should be wide enough to accom-modate four abreast; there should be a good-sized quiet recreation room away from the day room and that numerous corners and corridors should be avoided. They recommended disturbance buttons, louver-type observation panels in bed-room doors that are operable from outside, and vandal-proof light fittings, but also advocated fixtures and fittings that provide a homely environment.
Mazuch and Stephen (2005) explained how the London-based architectural firm, Nightingale Associates, combined psychotherapeutic methods with tra-ditional architectural methods to create healing healthcare environments. The authors dubbed this “humanistic architecture,” which “draws on international research in the fields of psychology and sociology, biology and physiology into the effects of the environment on health” (p. 48). These architects used emotion-al mapping based, in general, on all the senses but also on colors associated with the predominant emotional response aroused in particular areas. For example, they noted that blues have been indicated to subdue aggressive individuals and “visual monotony can contribute to physiological and emotional stress” (p. 50). In terms of touch, Mazuch and Stephen noted the important role this can have in the recovery of patients, as surfaces help to “re-engage with the materiality of the world” (p. 50). They emphasized that perceptual confusion should be avoided (e.g., a wood-grain finish on a metal door would give inaccurate sen-sory information because a metal door will be heavier and colder than would be expected with a real wooden door). As to sound, excessive noise has implications for increased heart rate, blood pressure, respiration, and blood cholesterol; they stressed that hard materials absorb less noise. The architects noted that smell can relax muscles and aid concentration; pleasant smells help produce endorphins and can decrease heart rate. Further, they noted the hypothesis that pleasant smells can reduce the amount of anesthetic administered during surgery (p. 50). In the areas of light and nature, Mazuch and Stephen observed that a lack of windows and connection to the outside world can heighten stress and depression.
To reiterate, the commonalities across the literature on providing a therapeutic milieu through the design of facilities for mental health care focus on the ele-ments of light; adequate personal, communal, and work space; home-like com-fort; and access to gardens.
GardensThe theme of gardens includes open spaces within the precincts of the hospital. Subthemes include therapeutic gardens, Alzheimer’s facility, historical perspec-tive, moral therapy, landscapes, therapeutic relationships, natural environments, directed attention, attention restoration theory, restorative experience, stress, nurses, evidenced-based design, and environments for renewal/stress relief. The theme of gardens is not confined to mental health care design per se because the healing garden is emerging as a topic for mental health in the context of general healthcare as well. It is therefore a holistic theme that, due to its very nature, is highly relevant to mental health care.

140 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
Hartig and Marcus (2006) recognize that the concept of healing is not synony-mous with cure; clearly, gardens are not curative and misconceptions concern-ing this notion should be avoided. However, they note that “healing gardens … are allied with a broad conception of health, one that recognizes that a person can move between greater and lesser degrees of health along diverse physical, mental and social continua” (p. S36). They offer several recommendations as to the structure of such healing gardens—there should be an absence of harsh noises and unwanted demands, landscape architects with knowledge of heal-ing plants should be employed to translate medical approaches. Unfortunately, as the authors note, “sadly, many opportunities to make gardens available have been wasted” (p. S37). This is something that Connellan et al. (2011b) also found in their ethnographic observations of a purpose built mental health unit in Aus-tralia. The upkeep and expense of gardens are mentioned as deterrents for their wider use.
In the subthemes of nurses, evidence-based design, and envi-ronments for renewal/stress relief, Naderi and Shin’s (2008) study offers useful information concerning the benefits of outside spaces in a medical environment. They conducted a two-part nursing staff survey in the United States based on a landscape design project at a healthcare center in Texas. The
results of Naderi and Shin’s survey showed that the availability of an outside space was important to those nurses surveyed; 88% said it was important to get outside during their workday and nearly all of the participants felt it was import-ant for their co-workers to get outside. Favorite activities included sitting (25%), walking (21%), and eating (10%). Nine percent expressed the need to be close to nature and get some sunshine and fresh air, while others went out to be social, with 18% going outside to talk to friends and 3% to engage in people watching. However, the survey found that 52% of nurses went outside to be alone and if nurses did go out in a group, it was with one (26%) or two (20%) other people. The need for some improvements in existing outdoor spaces was noted: 54% didn’t use the courtyard when it rained; 44% didn’t use it when it was too hot or sunny; 23% didn’t use it due to lack of seating; 16% because the entrance was sometimes blocked; and 11% because they felt privacy was compromised. As a result of the survey, two courtyard garden designs were proposed and, incorpo-rating nurses’ responses to the proposals, landscape architects designed a court-yard garden primarily for their use.
In terms of the specific needs of psychiatric patients, the writings of Clare Hick-man (2005, 2009) provide a particular perspective based on moral therapy and historic associations with landscapes and gardens. In the 2009 article, Hick-man draws upon English Romantic poetry, landscape painting, and the Pre-Raphaelite art movement in the 19th century to develop her arguments on the important relationship between mental health and nature. She refers to poets’ and artists’ beliefs in the “morality” of the landscape and the potential of natural environments for the prevention of what was considered to be “immoral” behav-ior. Hickman discusses in detail themes such as the Garden of Eden and being in nature as providing a closeness to God, a rural work ethic, and the romantic notion of man in and of the landscape. She refers to Louis James’s “Lines Com-
“[S]adly, many opportunities to make gardens available
have been wasted.”

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 141
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
posed a Few Miles above Tintern Abbey” regarding civilization and industrial-ization bringing about insanity because of the exodus from the rural idyll. Her 2005 article refers specifically to the large old parks and gardens of the 18th and 19th century asylums. The moral therapy that was part of those asylums’ treat-ment protocol was focused on the placement of a patient in a carefully designed environment and seeking to minimize physical restraints. It was believed that viewing the landscape had positive effects on the patients and therefore buildings were designed so the landscape could be viewed from inside the building as well. Design features included verandas, conservatories, airing courts, ornate aviaries, pagodas, and even a Chinese gallery; however the cost of creating complex land-scapes restricted such designs to institutions accommodating a wealthy clientele.
The presence of the gardens can be one of the most positive aspects of psychiatric treatment. Curtis, Gesler, Priebe, and Hickman (2009) noted that in the post-asylum age of mental health care, long-term patients were known to return to the asylums in which they were housed in order to walk in the gardens because of an attachment to and their positive associations with the therapeutic benefits of such places (citing Parr, Philo, & Burns, 2003).
In one article that emerged from the initial scoping study, “the restorative bene-fits of nature” are discussed in terms of developing an integrated framework that concentrates on directed attention, attention restoration theory, and restorative experiences for health outcomes (Kaplan, 1995). Kaplan included three com-ponents that are necessary for the restorative experience: “being away,” which implies not merely entering a new setting, but instead a change that “involves a conceptual rather than a physical transformation” (p. 173); an environment that is rich but that maintains coherence; and compatibility between the envi-ronment and one’s own goals. In reference to attention restoration theory and the natural environment, and drawing upon further empirical evidence to sup-port nature as a restorative element, Kaplan noted that being in nature requires less effort than being in a “civilized” environment; that intervention measures suggest that the use of nature as a restorative method have longer term benefits and participants were more likely to, for example, start new initiatives after the intervention.
The area of mental health aged care and gardens has a growing body of evi-denced-based research but Heath’s (2004) research is particularly useful for the design of Alzheimer’s facilities. Heath looked at post-occupancy studies that had been done to evaluate the therapeutic qualities of gardens and gardening in an Alzheimer’s facility. It is a multilevel care facility in British Columbia, Can-ada, which opened in 1995 and has eight courtyard gardens. The interview data revealed that 75% of visitors reported feeling more relaxed and calmer and 25% felt refreshed. The gardens were designed with five major goals:
1. To provide a safe outdoor environment;
2. To provide a place for reflection;
3. To provide a place for relaxation;
4. To provide a place for socialization; and

142 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
5. To provide a place for people to maintain the hobby of gardening (2004, p. 239).
The results of the post-occupancy evaluation showed that of the respondents, 83% visited the gardens and 96.5% of those liked them. Additional information from this study included that 80% of respondents said the aims of the gardens were met, except for providing a place for people to maintain a gardening hobby, as the gardens were already fully planted with no free space; and more family members used the gardens than did patients or staff, with suggested reasons being that some patients are not independently mobile, staff lacked the time to do so, or family members found the gardens a relaxing way to relieve the stress of ailing family members. There were also recommendations for improvements, such as the use of signs, maps, and automatic doors to increase access and aware-ness; further education of both staff and volunteers; the need for lawns where families could gather rather than areas dominated by paths and garden beds; leaving space for residents to create their own gardens; a lack of spontaneity in the plantings; and a lack of flexible, multi-use spaces.
Common points of discussion across the literature include the use of the various uses of gardens, access issues, retreats for staff, and specifically designed gardens.
The Impact of Architecture on Health OutcomesThe fifth theme is another general category and although it would be ideal to have each theme discreet and separate, as was the case with “therapeutic milieu,” there were too many articles that centered on one issue and merely mentioned others. Therefore, while this theme does overlap with others, its focus is largely on the impact of architecture on health outcomes. Among other issues, this category of publications addresses aesthetics and sensory stimulation as well as spatial design. The subthemes include mental health services, psychiatric care, salutogenic theory, sense sensitivities, emotional mapping, physiological respons-es, psychological responses, design models, evidenced-based healthcare design, and healthcare quality outcomes.
By far, the most extensive and influential research on the impact of architecture upon health outcomes is that of Ulrich and his colleagues, specifically, their 2008 comprehensive review of the research literature on evidence-based (gen-eral) healthcare design published in this journal, Health Environments Research & Design Journal (HERD). This review by Ulrich et al. expanded on a previous (2004) review, especially in relation to the scale of hospital-acquired infections. The keywords in Ulrich’s 2008 review were “evidence-based design, hospital design, healthcare design, healthcare quality, outcomes, patient safety, staff safe-ty, infection, hand washing, medical errors, falls, pain, sleep, stress, depression, confidentiality, social support, satisfaction, single rooms, noise, nature, and day light.” The three main areas of focus were patient safety, other patient outcomes, and staff outcomes. Although this review was on general health, we regarded it as a strong foundation for the work that needs to be done in the area of men-tal health care. Ulrich et al. tabulated their findings (p. 148), showing where empirical studies have revealed relationships between particular design factors
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 143
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
and healthcare outcomes. Ulrich’s table also indicates where “is especially strong evidence (converging findings from multiple rigorous studies) indicating that a design intervention improves a healthcare outcome” (p. 148). Single bed rooms, natural and appropriate lighting, and nature views are the three most significant design factors that contribute to positive health outcomes. For example Ulrich et al. showed that patient privacy and confidentiality as well as communication improves with single bed rooms; day and appropriate lighting contributed posi-tively to 14 of the 16 health outcomes listed; and nature views contributes signifi-cantly to reduced pain and stress and also to five other health outcomes (p. 148).
Ulrich et al. (2008) used a two-step approach to their review, and one upon which, to some extent, we modeled our own review. For the Ulrich study, the first step was a 32-keyword search across the literature and then a cross- referenced search using Ebsco Host, which enabled the search of multiple data-bases. This was supplemented with searches through ISI Web of Knowledge and Google Scholar to obtain additional sources from reference lists. Their second step or stage involved screening all identified references using two criteria: that the study “should be empirically based and examine the influence of environ-mental characteristics on patient, family, or staff outcomes;” and, “that the qual-ity of each study was evaluated in terms of its research design and methods and whether the journal was peer-reviewed” (p. 102). Their report was organized according to three types of outcomes:
1. Patient safety issues, such as infections, medical errors, and falls.
2. Other patient outcomes, such as pain, sleep, stress, depression, length of stay, spatial orientation, privacy, communication, social support, and overall patient satisfaction.
3. Scientific research relevant to staff outcomes, such as injuries, stress, work effectiveness, and satisfaction (p. 103).
The authors noted the increasing number of rigorous studies across design and healthcare but also observed that, despite this, “it is also important to address the limitations of the quality of existing evidence [because] in medical fields, a randomized controlled trial or experiment is considered the strongest research design for generating sound and credible empirical evidence [but Ulrich et al.’s review] found relatively few randomized controlled trials linking specific design features or interventions directly to impacts on healthcare outcomes” (p. 103).
Dennard’s (1997) review of David Halpern’s book, More Than Bricks and Mor-tar? Mental Health and the Built Environment, although written some time ago, highlights the publication of a book that is rare in this cross disciplinary field. Dennard reviewed Halpern’s approach of cause-and-effect associations of the built environment according to the following four categories: as a source of stress; as an influence over social networks and support; through symbolic effects and social labeling; and through the action of the (building) planning process itself. Creative conflict often arises in finding a balance between what is best for the patients, how the community perceives the design, and health and building regulations and policies. The perfect patient facility may not be feasible due to conflicts between the these factors.

144 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
Golembiewski’s previously mentioned (2010) theoretical study on salutogenics in architectural design for psychiatric care used Antonovsky’s Salutogenic perspective, and specifi-cally that the patient and environment are understood as being transactional, to inform his analyses. Golembiewski acknowl-edged that salutogenics do not replace evidence-based studies
but said that in the absence of evidence-based design for mental health facilities, applying salutogenics “in a methodological way” can provide a useful framework for informing architects regarding the functionality of facilities and improving mental health outcomes (p. 100). Acknowledging that unwell people do not nec-essarily adapt easily, Golembiewski suggested that “the salutogenic model seems an appropriate broad framework in which to locate the stress model because it supports the stress model with much needed substance; effectively filling the causation gap between action and effect” (p. 103). Therefore, although patients might not always adjust well to innovations, if the environment can be designed to change for and with the patient’s sensory and perceptual abilities, positive out-comes could result. Golembiewski drew upon Hall (1975) in that “perception is a complex neuro-chemical process that is highly reactive to the surrounding environment and yet it is the only channel for receiving new information of any sort” (p. 103). With this in mind, the author explained the comprehensibility of the salutogenic model as providing perceptual cues to assist the perceptual processes and providing an environment that is ubiquitous and desirable and is understood through the familiar and which can help stabilize comprehension and delusions. In terms of manageability of the model, it is important to allow patients to control their environment though meaningfulness. This goal can be attained by “enriching the environment with complexity, order and aesthetic considerations” (p. 114); allowing pets and personal items on the premises; and providing a stimulating milieu.
In their assessment of the role of environment on behaviors, actions, and inter-actions, Schweitzer, Gilpin, and Frampton (2004) focused on physiological and psychological responses. The authors hypothesized “a hierarchy of effect of envi-ronmental elements ranging from simply nontoxic to safe (both physically and psychologically) to ‘providing a positive context’ to being actively salutogenic” (p. S71). This article, published in The Journal of Alternative Medicine, advocat-ed design to facilitate intention and awareness; wholeness and energy; healing relationships; health promotion; and collaborative treatments. Schweitzer et al. presented the existing research in terms of physical parameters, and as includ-ing the following preferences in a healthcare setting: smells, noise, temperature, environmental complexity, fresh air and ventilation, color, nature, art/aesthetics and entertainment, and nursing stations.
In terms of personal space, there is a preference for single rooms; patient satisfac-tion is related to perceived pleasantness of décor, cleanliness, courtesy of house-keepers, temperature and noise, and (citing Kaldenberg, 1999) “how well things work” (p. S73). As with Mazuch and Stephen (2005), Schweitzer et al. noted that existing literature reveals the importance of the sensory environment in terms of smells, saying that pleasing aromas may reduce blood pressure, slow respira-tion, and lower pain perception levels, while unpleasant odors stimulate anxiety,
It is important to allow patients to control their environment
through meaningfulness.

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 145
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
fear, and stress. There was also some evidence that (a) excessive noise increases patients’ length of stay as well as causing interruption of sleep and increased stress; (b) environments with greater complexity correlate with greater cognitive functioning and beneficial physical activity in the elderly; and (c) sensory varia-tion in ambient conditions between spaces and over time is preferred by building occupants. The authors’ comments on light are covered in the “Light” section of this article, above.
The viewing of nature was dealt with separately from the experiencing of nature. Regarding the former, Schweitzer et al. noted Ulrich’s (2008) points concern-ing the lack of a window, which may have a negative effect by reducing positive stimulation and aggravating the negative effects of sensory deprivation; access to views of nature with gardens, through windows and in artwork, can reduce stress; and patients residing in units without windows developed more symptoms of depression. In terms of actually experiencing nature, the literature reported evidence of “lowered stress and muscle tension” (Schwetizer et al. 2004, p. S76) and fewer incidences of violence. Indoor plants were also shown to be beneficial. As to the last theme, Schweitzer et al.’s literature review included a section related to arts, aesthetics, and entertainment. Here, a preference was shown for visual art encompassing nature images, positive facial expressions, and depiction of caring relationships, whereas ambiguous or abstract imagery was shown to have nega-tive outcomes. Schweitzer et al. also pointed to research that demonstrates the positive effect of music on health and also positive distractions such as humor and entertainment, which may lead to greater optimism, socialization, coopera-tion, and decreased dependence on medication. These authors also covered nurs-ing stations (see “Nursing Stations,” below).
Commonalities in the literature on the impact of architecture on mental health outcomes include:
• Perceptual cues assist the perceptual processes, help avoid confusion.
• Enriching the environment with complexity, order, and aesthetic consid-erations is beneficial.
• Access to nature can have positive mental health outcomes and add com-plexity and stimulation.
• There is a general preference for single rooms.
• Smells: pleasing aromas may reduce blood pressure, slow respiration, and lower pain perception levels; unpleasant odors stimulate anxiety, fear, and stress.
• Access to views of nature with gardens, through windows and in artwork, can reduce stress.
Interior DesignThis theme relates specifically to interiors; subthemes of varying importance include interior design and furnishings, interior design and color, wayfinding, cognitive mapping, spatial organization, and type of patient room (multi-occu-

146 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
pancy, semi-private, and private). Lorenz’s (2007) integrative research review, “The Potential of the Patient Room to Promote Healing and Well-Being in Patients and Nurses,” addressed the issue of multi- and single-occupancy patient bedrooms in general healthcare. Within this study, Lorenz synthesized empiri-cal and chiefly quantitative studies on patients’ rooms in the acute care hospital in terms of “promotion, maintenance or restoration of healing and well-being for patients” (p. 263). Lorenz also focused on patient outcomes and the ability of nurses to provide optimal care. Studies deemed relevant fell into three general categories related to the patient room type:
1. Clinical outcomes
2. Patient perceptions
3. Staff perceptions
Outcomes were generally measured in length of stay, utilization of narcotics, and physiological and behavioral responses. Lorenz concluded that the gaps in the literature related to room type and impact on patient falls and medication errors; and how room type relates to specific patient populations and impacts on their clinical outcomes. She also noted that further study is required to expand the study of room type to include the design of the patient care unit.
Vaaler, Morken, and Linaker (2005) conducted a carefully controlled study in the acute care Østmarka Norwegian psychiatric hospital between 2000 and 2001. Vaaler et al. wrote that in the 140,000 catchment area of the city of Trond-heim, “600 patients above 18 years suffering from acute psychiatric conditions are admitted each year” (p. 20). The researchers conducted the study in a unit that had been refurbished 4 years prior; the traditional interior design consist-ed of grey colors, no window curtains, a single lamp in 4-meter-high ceilings and tubular metal beds and chairs. In close collaboration with architects, one of the wings was redecorated and refurnished to make it look like a standard Norwegian home, with the goal of allowing a comparison between the symp-toms, behaviors, treatment, and relative satisfaction of the patients staying in the traditional area as opposed to those housed in the redecorated wing. This involved “colorful wallpaper and paintings on the walls, lowering the ceilings and installing multiple lighting spots, tastefully curtaining the windows, putting wardrobes, chairs, flowers and personal items in the patient rooms and Italian ceramic tile covered the entire bathroom” (p. 21), while the other wing was left unchanged. The findings included “no negative effects of changing to a more pleasant and home-like environment” (p. 22); non-significant tendency toward symptom amelioration in the traditional wing; creating a pleasant environment does not generally increase length of patient stay; and there was a “complete lack of vandalism” (p. 23) on the new side. The authors concluded that “interior and furnishing like an ordinary home … created an environment with comparable treatment outcomes to the traditional dismal interior, and had positive effects on many patients’ well-being, at least among the women” (p. 19). And although the outcomes were not markedly different, the researchers emphasized that they “… find little to justify the often-dismal interiors of wards used to seclude severe-

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 147
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
ly mentally ill patients. This practice should be abandoned unless there are very specific reasons to introduce it for special cases” (p. 24).
Salmi’s (2008) comments on wayfinding for people with disabilities, although not focused on the hospital environment or mental disabilities specifically, threw light on universal applications for developing better wayfinding in interior design. She concentrated on spatial organization—architectural features, destination zones, spatial overview opportunities and overall layout—advocating landmarks that are distinct in shape and color and with appropriate signage. For example, signage should be properly designed and well-placed. It should be perpendicu-lar to the line of travel and at eye level for wheelchair users; the readability must be legible, incorporating large text and high contrast with the background; it should designed mindful of glare and paired with a graphic image. Color should reinforce links with the environment; directories should cluster information, be accompanied by graphics, use simple color coding, and be placed in relation to the specific floor. Maps should be less cluttered—“You Are Here” designations are of the greatest importance.
The most telling studies are possibly those that have been able to map behavior through pre- and post-renovation data. Devlin (1992) reported on such a study involving four psychiatric wards in New England in the late 1980s; changes were made to interior decorating including color schemes/painting, indoor plants, new furniture, bathroom renovations, and similar minor works. The method was primarily an environmental design survey that involved staff rating design fea-tures; these ratings were analyzed and combined with observations and behavior mapping. Devlin emphasized patient population and seasonal variation (warm weather) as a determining factor in understanding reactions and movements in a spatially altered and renovated area; however, there was sufficient data to indi-cate a decrease in stereotypic behavior among patients and improved staff morale after elements such as wallpaper, live plants, increased light, colored walls, and upholstered furniture replaced the previous spaces that had green and gray walls and “mismatched vinyl-covered chairs” (p. 71).
PsychogeriatricResearch literature on aged care is growing with the worldwide concern about a huge aged population in the coming decades, one which will put pressure on both the social and economic infrastructures. It is therefore not surprising that the impact of facility design in psychogeriatrics is an area that has seen two literature review articles within the last decade, those of Dobrohotoff and Llewellyn-Jones (2010) and Day, Carreon, and Stump (2000). Subthemes that emerged from both include psychiatry, violence, design, dementia, and ther-apeutic design. Dobrohotoff and Llewellyn-Jones focused more on psychiatry and violence in psychogeriatric units (PGUs), noting the historically deleteri-ous effect of hospital environments on psychiatric patients, where depressing environments convey regression and loss of control and present as intimidating for patients and families. They searched the databases of Medline (1950–2010), psycINFO (1806–2009), EMBASE (1980–2009), and CINAHL (1982–2009) for literature concerning PGU design, from which they reviewed 200 papers,

148 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
including some government reports and non–peer-reviewed articles. They note that “there are few good quality studies to guide the design of acute PGUs and much of the existing literature is based on opinion and anecdote or, at best, based on observational studies. Randomized controlled studies comparing different designs and assessing outcomes are virtually non-existent” (p. 1). With regard to violence, these authors show that in the literature they reviewed, 18% of demen-tia patients were violent during admission, specific factors relating to prevalence of violence were not well-studied, and staff working in noisy conditions with poor lighting were more likely to be assaulted (citing Soares, Lawoko, & Nolan, 2000). As to trauma, 34% of post-discharge patients “felt frightened, unsafe, a sense of intrusion and lack of privacy, disgust and embarrassment, powerlessness, and feeling undermined at some time during their hospital stay” (p. 3). There had been no systematic research into the effect of various ward environments on patients’ experiences; the loss of self-esteem, patients’ sense of self-worth, inten-sified psychiatric symptoms, and a reduction in patient’s participation in their care may be caused by “sanctuary harm” (citing Robins et al., 2005). Dohrohot-off and Llewellyn Jones make the following recommendations for designing the optimal physical environment:
• Optimize patient and staff safety, manage patients’ physical health, design a productive ward environment.
• Ensure access to a psychiatric intensive care unit (PICU) or high depen-dency unit (HDU).
• Provide space—a garden, a quiet area, a seclusion suite, an activity and games room.
• Include separate bedrooms with louver-type observation panels, doors that open two ways, vandal-proof dimmer light fittings, and safe fixtures and duress alarms.
• Design an environment that is secure, structured, with minimal stimula-tion, non-intrusive, and supportive.
• Create a design that facilitates patient observation as well as high nurse-to-patient ratios.
• Facilitate limited use of restraints and seclusion.
• Make it possible for cognitively impaired patients to be segregated from those who are not cognitively impaired.
• Create separate male and female sections.
• Provide direct access to usable outdoor space.
• Have clear indications for the intended use of each area or room.
• Optimize the location of nurses’ station to enable direct line of sight to as much area as possible.
• Ensure locked doors on secure wards.
• If possible create good external visibility and access to public transportation.
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 149
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
In addition, design should incorporate deinstitutionalizing features such as:
• Separate living and treatment areas.
• The elimination of long echoing corridors and highly reverberant spaces.
• Residential features such as a laundry and galley kitchens.
• Reduced psychopathology among younger patients facilitated by design solutions that encouraged social interactions: ward kitchen, an open nursing station, and a dayroom module for crafts and other occupational therapy activities.
The second, earlier literature review (Day et al. 2000) on psychogeriatrics focused specifically on therapeutic design and dementia. These authors commented on the problem of small sample sizes in studies on design and dementia, noting that more than 30% of the studies reviewed used samples of fewer than 30 par-ticipants (p. 398), with many including fewer than 10. With respect to this fac-tor, it should be noted that the majority of studies Day et al. looked at in their 600-paper review article were qualitative, where small sample sizes are accept-able. Despite this, they mentioned the increased rate of research on design and dementia, from 6 research reports from 1981 to 1985, to 17 research reports from 1986 to 1990, to 26 research reports from 1991 to 1995, and 21 research reports already published since 1996 (p. 398). Day et al. provided a useful table that lists all the papers reviewed with summaries for each. Sections include:
1. Concept and focus of study;
2. Research design;
3. Sample information;
4. Outcome measures of well-being;
5. Physical environment features; and
6. Major findings of environmental impacts on well-being.
The authors’ method for collecting papers to review stipulated empirical findings as one of the criteria. Their findings can be summarized as the benefits of group living for patients with dementia; the disorienting problems with changes to their environment; the benefit of reduced use of psychotropic drugs and a decline in behavioral disturbance in Secure Care Unit (SCU) design that showed clearly colored wayfinding, names on doors, photos of family, separate activity areas, secure exits and closets, visual tapes across glass, and appropriate sound proof-ing; other aspects such as the benefits of nature and natural light, recreational activities and personal as well as gendered spaces were shown to be beneficial to both staff and patients.
Commonalities across both of the Dobrohotoff and Llwellyn Jones (2010) arti-cles and the research of Day et al. (2000) included security issues, gender sepa-ration, and gardens.

150 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
Post-Occupancy EvaluationsPost-occupancy evaluations (POEs) are rarely carried out, yet it is known that architectural designs for mental health care contribute to mental health out-comes; therefore, in order for these results to be positive for both the patients and the community, it seems strange that evaluations are not routinely carried out and the results disseminated. Carthey (2006), in conjunction with the Uni-versity of New South Wales (UNSW) and the New South Wales (NSW) health department in Australia, conducted research into the reasons for the lack of POEs and worked toward establishing a standardized model for post-occupancy evaluations across healthcare. Carthey offered three different types of evalua-tions, which might sometimes be confused:
1. Post-occupancy evaluations (POEs)—The process of examining and evaluating the functioning of a building in a systematic way after com-pletion and occupation (from 12 months to 2 years) (p. 58).
2. Post-implementation review (PIR)—“The last step in the process,” which includes closure of the “feedback loop” that takes lessons from previous projects (p. 59).
3. Post-completion review (PCR)—A systematic comparison of original brief and objects with the actual outcomes (p. 62).
Although Carthey does not state this specifically, “POE” is the most commonly used term encompassing all three.
The complexity and variables present in healthcare design evaluations give rise to subthemes across the literature reviewed for this article: interdisciplinary research; evidenced-based design; environment and behavior; occupant’s feed-back/users’ needs; psychiatric unit; serious game; service planning; and ser-vice users. Some of the publications concentrated on suitable methodologies for conducting evaluations, and all agreed that interdisciplinary research and input is essential (Marmot, 2002; Veitch, 2008; Vischer, 2009; Whitehead, Pol-sky, Crookshank, & Fik, 1984). However, Veitch notes that interdisciplinary research presents barriers such as different disciplinary cultures and professional “languages” and that parties are required to challenge institutional policies that may hinder collaboration such as the choice of journals in which to publish results, academic publication rates, the ability to write for peer reviewed journals, and promotion opportunities.
Marmot (2002) noted that the relative scarcity of evaluative research on build-ings may be related to cost, fear of negative outcomes, perceived uniqueness of buildings—lessons learned in one location for particular set of consumers may not be applicable elsewhere—,and determining what conclusions to draw amid many variables and influencing factors. Therefore, Marmot said that assertions of design briefs are rarely tested properly.
The title of Liddell’s 2010 article in Health Estate, “Good Data Critical to a Suc-cessful Outcome,” speaks for itself. Liddell examined what to look for in devel-oping a POE process for large hospital environments, what is actually required to

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 151
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
perform a rigorous POE, and what can be expected from the process. The goals of Liddell’s project on post-occupancy strategies to arrive at the best process for critique involved documenting generic project information to enable compari-son of similar sized projects; reviewing the planning and construction phases of the project; reviewing the operation of the facility and the communications strategy; and providing comment on the current NSW POE Guidelines. Liddell detailed the reasons that POEs are not pursued more effectively, observing that “the Government even has a manual on the subject … which itself notes that there are a number of reasons why post-implementation review is not pursued more effectively” (p. 26). These include the temporary nature of teams involved; 3- to 5-year timeframes between feasibility and occupancy; the changeabili-ty of factors such as service delivery, budgets, political climate, the economy, unwillingness to criticize participants, budget shortfalls; and the inability of the asset management to engage in effective critical examina-tion and evaluation. Liddell’s recommendations included the active involvement of key staff and stakeholders throughout the planning process and continuing through every stage of the project, implementing document management systems and initiating POEs before the project team disbands.
Vischer’s (2009) review article on designing intelligently and designing intelli-gent buildings stated that when POE studies are conducted, the “voluminous amount of research findings lie unread on desks or are published in academic journals that practitioners seldom read” (p. 240), also that designers frequently go to new sites, measure in accordance with number of users, and therefore resort to reinventing the wheel. While Vischer did not discount the usefulness of tradi-tional POEs that ascertain the effectiveness of a building by gathering informa-tion from users and testing hypotheses, she emphasized that “in the real world” the newer focus on evidence-based design (EBD) is a better option. She there-fore compared the POE process with EBD, using healthcare design as one of her two areas of focus. Vischer cited her own 2008 research, noting that an inherent deficit of the POE approach is that this form of measurement measures “people’s preferences and perceived needs rather than the effectiveness of building design and operation decisions” (p. 242); further, she argues that the traditional POE accumulates building users’ subjective likes and dislikes, information that is not helpful to designers who need to know exactly how aspects of the building func-tion. In contrast, “evidence based design has evolved out of the precedent set by evidence-based medicine” (p. 242). Therefore, if both the methods and results of EBDs are targeted, their uptake by both designers and healthcare professionals is more purposeful and the outcomes are arguably more accurate.
In an older study (but one directed specifically at a 30-bed psychiatric unit), Whitehead, Polsky, Crookshank, and Fik (1984) considered the “Objective and Subjective Evaluation of Psychiatric Ward Redesign.” They posited four psy-choenvironmental hypotheses for evaluation:
1. Environmental alteration correlates with changes in social behavior.
2. Environmental alteration correlates with altered spatial distribution of behavior.
Evidence-based design has evolved out of the precedent
set by evidence-based medicine.

152 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
3. Environmental alteration correlates with reduced psychopathology.
4. Social organizers may be used to focus the alterations in therapeutic and socializing ways.
These authors assessed a unit that had been redesigned in accordance with psy-choenvironmental principles as they aimed to ascertain the effectiveness of such an approach. Using behavioral mapping derived from ethological studies among psychiatric patients, the researchers mapped and recorded the movements and behavior of patients in particular parts of the wards and whether they presented pathology. The observation was detailed and noted the following behaviors in areas such as hallways, sitting rooms, etc.: head even, looking at person, oriented toward neighbor, sitting quietly, talking, or no pathology. Their conclusions were positive in terms of clinical outcomes but limited; the authors noted that length of stay was not reduced substantially by the redesign and that the results would have been more informative if patients could be returned to the older designed units and observed there.
A recurring theme through the literature on post-occupancy evaluations is that of the patient/user engagement in process of design. While users have been engaged, this happens to varying extents, and there are fluctuations in the degree to which their recommendations are applied. Fitzgerald, Kirk, and Bris-tow (2011) described and evaluated “serious game intervention to engage low secure service users with serious mental illness in the design and refurbishment of their environment” (p. 316). The advantages of a serious game (defined as a game that has a useful purpose or models real life situations) “lie in the famil-iarity of its format, its non-threatening facilitation of communication and the creative and fun approach to serious issues” (citing Lamey & Bristow, 2007). This self-selecting process of engagement resulted in 25 of 30 service users par-ticipating in the game. Feedback from participants was overwhelmingly posi-tive. The use of the serious game format has potential for mental health services to successfully engage service users in collaborative dialogue such as treatment planning, illness education and recovery. “The game begins, similar to the ‘Go’ square in ‘Monopoly’ and as in real life on the ward, at the airlock square. Instead of streets, as in Monopoly there were themes that were grouped in accordance to questions and issues submitted by staff, architects, management, estates and builders” (p. 318). Simple questions such as “what would you like in a dining room” and “how would you like your medication dispensed” were some of the questions used in the game, with prizes as is the case with most board games. Fitzgerald et al. wrote that these service users had not been part of the original design decisions and management wanted to know what was working or how it could be improved; previously, the meeting and consultation style of communi-cation to obtain feedback from users had not proved successful and the resulting information from the game was better. The authors said that the game removed barriers present in the meeting style consultation and recommended that these games be used earlier and specifically in the design conceptualization stage of projects.

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 153
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
Nursing StationsIn terms of physical spatial design, nursing stations (also often called “duty stations”) emerge as the single most significant factor in mental health facility design. Issues in nursing station design overlap with security and models of care; therefore, the subthemes include nurse-patient relationships, staff safety, space and control, and function and work environment.
Andes and Shattell (2006) explored “the meanings of space and place in acute psychiatric settings, to discuss how these meanings affect human relationships, nurses’ work environment and patients’ perception of care, and to present how the design and use of nursing stations affects therapeutic relationships” (p. 699). These authors concluded that the generally positive features of nursing stations and space control include the fact that nurse-only and patient-only spaces are beneficial to both groups and positive nurse-patient interactions “increased dra-matically” after redesigns that “include more private areas for nurses” (p. 702). And in terms of negative design outcomes of nursing station design and space control, Andes and Shattell determined that, in the minds of both patients and nurses, psychiatric patients cannot and will not respect the nursing station as a work area. The physical barriers used in the design of nursing stations rein-force the idea that they are off-limits to patients and impede the development of interactions. Andes and Shattell affirmed that psychiatric nurses had few meaningful interactions with patients because of interpersonal barriers (e.g., an impoverished view of person-al efficacy) and organizational barriers (e.g., short lengths of hospitalization and high patient acuity). These authors stressed the “hospital should be designed in such a way as not only to serve as a temporary home [for psychiatric patients], but its environment should aid recovery” (citing Shrivastava, Kumar, & Jacobson, 1999, p. 703).
Brown (2009) noted that, while the objectives of the nursing station is to make staff feel safe, open areas are essential to “encourage interactions between patients and staff” but that “staff must have a private space where they can retreat and conduct administrative tasks” (p. 22). This reiterates Connellan, Due, and Riggs’ (2011b) note that, in an ethnographic observational study of a recently complet-ed purpose built mental health unit, the design of the nursing station combined intense administrative activity with patient interaction with the result inade-quate patient-staff communication. Brown identified that the optimal design of the nursing station needed to incorporate appropriate seating, stimulants, acoustics, and size to suit the intended function of the space and to place thera-py spaces close to nurse stations. A sense of boundary to the patient is necessary but there still needs to be high visibility.
Karlin and Zeiss (2006) noted that open nursing stations have been recommend-ed by several sources; they refer to Edwards and Hutts (1970) findings of “sig-nificant positive psychological, behavioral, and social effects after the removal of glass partitions from psychiatric unit nursing stations. Patient requests of nurs-es at nursing stations were dramatically reduced, as were the negative beliefs of those patients, and improvements in ward milieu and patient-staff communica-
They found significant positive psychological, behavioral, and social effects after the removal
of glass partitions from psychiatric unit nursing stations.

154 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
tion were also noted” (p. 1378). Karlin and Zeiss wrote that “available reports of experiences with open nursing stations do not support concerns of patient abuse of increased access to nurses, although additional empirical research on this issue is needed. Contiguous, secure, closed to patients, is recommended to maintain confidentiality of patient records” (p. 1378). These authors observed that, prior to the dawn of effective psychoactive medications, closed nursing stations were the norm, but they fostered a perception that the staff members were inaccessible and welcomed neither patients nor visitors to their environs.
Schweitzer, Gilpin, and Frampton (2004) reported that large centralized nursing stations separated from patients by half-walls or glass partitions that are located some distance from the rooms of the patients “clearly distance staff members from patients, sending the message that they are busy and inaccessible” (p. S78). These authors stated that “a decentralized nursing work station that is small, open and located outside clusters of 4–6 patient rooms, with the main nursing station completely open to patients, suggest[s] that healing is a collaborative pro-cess and not something exclusively under the purview of ‘professionals’” (p. S78). The above research, published in the last 6 years, differs from some of the ear-lier studies, which did not use ethnographic observational studies or include the views of the patients and their families. For example, a study that came out of our original scoping of the literature asserted that the positioning of the nursing sta-tion should allow observation of all patients, use one-way mirrors, and surround the nursing station with Plexiglas. In that study, a survey of nurses’ attitudes pro-posed strengthening of windows for the station and improved sound-proofing of quiet rooms (Dix & Williams, 1996).
The commonalities for all publications which relate to nursing stations include the need for discreet and separate spaces for nurses and other staff to relax and also for spaces away from patients where they can attend to administrative tasks. In addition, open areas are necessary to encourage interactions between patients and staff because closed nursing stations often convey an image of staff inacces-sibility and are not welcoming to patients and visitors.
Model of CareThe literature shows that the numerous types of models of care are one of the chief reasons for the complexity in designing for mental health care (Cleary, Hunt, O’Connor, & Snars, 2010; Costello, 2007; Killpsy, Ritchie, Grerr, & Robinson, 2004). Subthemes emerging from the literature include phase of ill-ness model of care, therapeutic space, inpatient care, bio-psycho-social approach, built environment, length of stay, homelessness, and engagement.
Cleary, Hunt, O’Connor, and Snars (2010) shared their findings on the Concord Centre for Mental Health’s new “phase of illness” model of care, asking wheth-er this is the direction in which we should be moving. The professionals at the Centre had come to question their traditional approach to mental health treat-ment, “rehabilitation and acute psychiatry were perceived as dichotomous … [i]npatient rehabilitation was something to which a person was referred … after all other avenues had been exhausted” (p. 247). Their main points included attempts

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 155
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
to integrate “early intervention” approaches into the philosophy of a large insti-tution to provide services responsive to the different phases of a patient’s illness; the need to combine management of risk and vulnerability with an emphasis on the patient’s experience and “journey” to recovery; to acknowledge the prevalent levels and ranges of disability; and to discount the perception “that ‘rehabilita-tion’ should be targeted at only those with severe levels of disability” (p. 247).
Costello’s (2007) thesis advocated for an architecture that balances supervision, treatment, freedom, and community integration, and noted the problems with current models of mental health care facilities, hospitals, independent living situ-ations, and group homes include being insufficient as a continuum of care model for mentally ill patients; hospitals disregard therapeutic qualities of long-term care centers (focus on stabilizing and releasing); other options such as living alone or in a group home eliminate medical stability and enhance patient inde-pendence, but without sufficient connection to therapy; and group homes can be problematic as they can act as small isolated islands within the community.
Key design principles recommended were:
• Balance between connection with the community and retreat.
• Retail as a buffer between life in the facility and life in the larger community.
• Integrated building form (fits into the existing urban landscape).
• Interactive wayfinding.
• Facility design should support multiple levels of interaction.
Fitzpatrick’s (2007) study addressed mental health care from a bio-psycho-social perspective, one that aims to treat the patient holistically, using psychological therapy including individual therapy and spirituality as well as social network-ing, and which includes group and family therapy in a community. Fitzpatrick noted that personal visual elements may ground a person’s sense of self, and a sense of self can add to the experience of space. In addition, being able to with-draw is important as well as aiding a person with self discovery.
Length of stay in healthcare is a significant factor in terms of demand for beds and economic factors but short lengths of stay do not necessarily equate with recovery or a stable condition, and this is particularly significant in mental health care. Frank and Lave (1986) provided an analysis that showed that the treat-ment of psychiatric patients and their length of stay responds strongly to finan-cial incentives. Their analysis focused on the U.S. Medicaid program, a federally supported, state-administered program that pays for medical care provided to eligible low-income individuals and families.
Aligned to economic issues and length of stay in mental health care is that of homelessness, Killapsy, Ritchie, Grerr, and Robinson’s article was aimed at the assessment of “whether admission to a designated ward for the homeless men-tally ill improves outcomes 12 months after discharge in terms of housing sta-bility and engagement with services” (2004, p. 593). They found that, although

156 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
the idea of a designated ward seemed the best alternative for a population that was both mobile and resistant to services, those admitted were no more likely to be discharged or to move on to or remain in stable housing than were those in the control group, although this might be explained by the patients’ compara-tive degree of ingrained homelessness. However, there was an improvement seen in engagement with services for those who were admitted as well as diminished issues with medication non-compliance.
ArtThis theme includes a systematic literature review article by Daykin, Byrne, Sote-rious and O’Connor (2008) on the impact of art, design and the environment on mental health care. Daykin et al. reviewed over 600 papers published between 1985 and 2005, including discussions of contextual and policy literature, as well as 19 reports of quantitative and qualitative studies. Their inclusion criteria were international papers on arts, architecture or design initiatives in healthcare; papers on participatory arts in healthcare; artists in residence; and intervention studies. Exclusion criteria were not relevant to arts or design initiatives in health-care; not relevant to participatory arts in healthcare; art forms (music, drama, play, dance); art therapy where art was a purely diagnostic intervention; patient arts; not English language; and pre-1985.
The authors revealed that there are few studies that directly examine arts inter-ventions and a notable absence of evidence-based studies. Of these studies, two are reviews, one does include art therapy but specifically its effect upon schizo-phrenia; Daykin et al. explained that the “methodological challenges of evaluat-ing the clinical effects of art, design and environment are illustrated in a report [that of Ruddy and Miles, 2005] of a systematic review of art therapy for schizo-phrenia” (p. 87). The other review mentioned is that of White and Angus (2003), “Arts and Adult Mental Health Literature Review.” They also noted small sample sizes, which make it difficult to detect significant results. However, a key finding of one empirical study by Staricoff and Loppert (2003), who measured psychoso-cial effects after art interventions, was that “depression and anxiety were respec-tively 34% and 20% lower where intervention had taken place than with groups not exposed to arts” (p. 88). Eight studies examined the impact of environmental conditions, sometimes taking into account aesthetics as well as functional con-siderations; two studies used structured assessment tools to evaluate healthcare facilities (Daykin et al. 2008, p. 88).
The authors pointed out the issue of differing perspectives regarding art among the various stakeholders in mental health care, stating the “[w]hile there is some convergence of agendas, the growth of the arts for health agenda has raised chal-lenges. First, there is a need to identify the respective contributions of the var-ied disciplines involved in arts for health. As well as art therapists, an increasing number of stakeholders are involved in projects, such as arts agencies, artists, community arts workers and designers. These groups may draw on different perspectives when it comes to artworks and environments in healthcare” (p. 86). These authors acknowledged the limitations of their own study, notwith-

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 157
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
standing their efforts to make the selection transparent through software such as REFworks.
Nanda, Eisen, Zadeh, and Owen (2011) published a paper focusing on the “Effect of Visual Art on Patient Anxiety and Agitation in a Mental Health Facil-ity and Implications for the Business Case,” which was aimed at investigating “the impact of different visual art conditions on agitation and anxiety levels of patients by measuring the rate of pro re nata (PRN) incidents and collecting nurse feedback” (p. 386). The results did indeed show a substantial effect of the nature of the displayed art work on the amount of PRN medication dispensed for anxiety and agitation, being significantly higher when abstract art was featured than when the patients viewed a realistic landscape. These results were comple-mentary to those of a 2008 study conducted by Nanda, Eisen, and Baladan-dayuthapani at St. Luke’s Episcopal Hospital in Houston, Texas, in which “[i]mages selected covered a wide range: pure, contemporary abstract with non-representational graphic forms; classic works of art from grandmasters such as Van Gogh, Chagall, and Klimt, which used representational forms; and final-ly, stylized nature images. Only one of the seven images was a realistic image of nature” (p. 276). Patients were encouraged to comment on their subjective experience of the art works rather than judge them. Two questions were asked: “How does this painting make you feel?” and “Would you hang this picture in your room?” (p. 285), with answers on a Likert scale. “Hospital in-patients con-sistently preferred images of realistic art with nature content over images that were stylized or abstract” (p. 295), as opposed to the students from a neighbor-ing university who rated stylized and abstract images highly. Patients rated the autumn waterfall image as their highest preference overall.
The subthemes coming out of all the literature are art in a healthcare setting, design, environment, visual art, and nature. Commonalities across the literature relate to the therapeutic benefits of visual art in healthcare environments.
The AdolescentMany mental health and other health facilities focus on a specific population, usually children, adults, or the aged. Therefore, the needs of young people who are subject to extreme bodily changes in their bodies and their lives during their adolescent period are a crucial category for study, particularly in terms of treat-ment for mental illness.
Subthemes emerging from the literature include hospital design, family-centered care, visual preferences, and evidenced based design.
In his 2010 article in Behavioral Healthcare, Huffcut asks if design can actually promote healing, and then answers that question through the use of research in evidence-based design (EBD) and how its principles can be utilized to “sculpt the space within long-term facilities to better meet the needs of adolescents” (p. 33). Huffcut cites surveys of adolescent inpatients conducted by an architec-ture design team concerning their preferences in the design of the facility. Their suggestions, which included “calm down” spaces with in-depth, lifelike imagery;

158 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
the use of cool colors (blue and purple); increased daylight; and varied seating options (with males in favor of seating placed around the television), coincided with features suggested by previous EBD research.
In Blumberg and Devlin’s (2006) study, they observed that the needs of a sick child are quite different from those of adults, and to meet those needs, “the design of pediatric therapeutic settings differs greatly from those in adult or general care facilities” (p. 296). They too made use of a survey to ascertain the preferences of adolescents, should they require hospitalization. According to the majority of the young participants, access to a television (97%), music (96%), and a telephone (95%) was of utmost importance. To explain these choices, the authors cited the research of Brown, O’Keeffe, Sanders, and Baker (1986), which demonstrated that, for young people, the most common coping measure in stressful situations is attention distraction, which can be provided easily by television, music, and conversations with friends.
In terms of spaces beyond their rooms, Blumberg and Devlin’s research revealed that an area in which to visit with friends was of a high priority; “a gym or exer-cise room to work out in was selected by 82% of participants, and an accessible kitchen was selected by 79% of participants” (p. 310). They also addressed ado-lescent need for privacy, stating that [t]he specific developmental traits of ado-lescents seem to call for distinct amenities, such as private bathrooms, single rooms, and comfortable full-coverage pajamas, to provide for the expression of identity” (p. 315).
In the thesis, “View Out of a Window: Visual Preferences of Dually Diagnosed Adolescents Residing in Group Homes,” Boggavarapu (2002) observed that the adolescents surveyed had very distinct preferences in terms of what they saw every day from the windows of the facility in which they resided: medium veg-etation was preferred over dense or sparse vegetation; they wanted variety— plants, trees, bushes, shrubs, vegetation with fruits, flowers, vegetables, and greens; some form of body of water was a favorite, with a pool the most preferred choice; “houses” were the most preferred kind of building, beating stores, play-grounds, schools, roads, and offices. Almost two-thirds (62.2%) of participants wanted equal proportions of vegetation and buildings. Research from previous studies showed nature was always preferred over man-made; this study indicated they were desired equally.
It should be kept in mind that it is possible that results of this study are not consistent with earlier studies. There are two plausible reasons for this: first, the earlier studies were conducted on mentally normal people and this sample of population would not be considered “mentally normal.” Second, familiarity and preference can be both positive and negative, depending on the context. It’s pos-sible that dually diagnosed adolescents whose group homes are generally built away from residential communities may prefer man-made settings.
Commonalities for all publications relating to designing for adolescents relate to the need for connection with the outside world.

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 159
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
Forensic Psychiatric FacilitiesThe last key theme in this literature review is that of designing for forensic psy-chiatric facilities. Key themes emerging here are architectural design, safety, pri-vacy, and escapes. Commonalities for all publications relating to the designing of forensic psychiatric facilities include a comfortable domestic scale and ambi-ence; security; a pleasant, domestic atmosphere that is well-lit by natural light; and ample space for the patients.
In their study, Dvoskin et al. (2002) addressed the requirement for a secure forensic psychiatric hospital as derived from the preferences of professionals in that field. According to those surveyed, design considerations should include ambience and a comfortable domestic scale, the use of good lighting, bright colors and subdivided spaces, and a safe environment that promotes both pri-vacy and observability and fosters the acquisition of skills. In addition, designers should be mindful of the fact that one of the most significant stressors in prisons or psychiatric hospitals is the virtually constant level of noise; anything that can be done to buffer excessive noise would be very helpful. In terms of organization of space, the best design would offer “a compromise between staff efficiency and a reasonable therapeutic milieu;” it was believed that this could be “achieved with relatively smaller social units” that afforded a reasonable degree of freedom to the patients (p. 490).
Enser and MacInnes (1999) examined a serious issue concerning secure facili-ties: the link between building designs and escape. Their research revealed that the primary areas mentioned when discussing escapes are perimeter fencing, roofs, and internal and external windows. They found that security breaches and building design correlated, in that units with design problems are units that experience a greater number of escapes, and escapes becomes much less likely the higher the garden fence. Design features that add security without compromis-ing patient care include secure bedrooms overlooking an inner courtyard, any covering of that courtyard modified by a feature that cannot be climbed, fencing with a double overhand, the installation of closed circuit television, airlocks and alarms on exit doors, and new and secure window fittings.
ConclusionThe research question that led us to review the literature was, How does the intersection of mental health care and architecture contribute to positive mental health outcomes? Our combined comprehensive and systematic review of the literature revealed 13 major themes. In order of prevalence these are (1) security/privacy; (2) light; (3) therapeutic milieu; (4) gardens; (5) impact of architecture on mental health outcomes; (6) interior design; (7) psychogeriatric; (8) post-oc-cupancy evaluation,; (9) nursing stations; (10) model of care; (11) art; (12) design-ing for the adolescent; and (13) forensic psychiatric facilities.
The themes overlap and some statistics apply to several themes. However, for the purpose of some clarity, we will summarize according to themes. The first theme comprises security, violence, privacy, and overcrowding, showing that people in ward environments occupy 70% less space than their counterparts of 150 years
160 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
ago (Johnstone, 2004). Violence against patients and staff in psychiatric wards is widely prevalent and increasing (Kumar et al., 2011). This has important impli-cations for the architectural design of psychiatric units, including the impor-tance of demarcated spaces for particular activities and extra space provided where possible.
The second theme, light, includes natural light and artificial lighting. The pri-mary findings here were the importance of light for controlling the circadian system thus reducing depression, agitation, sleep, eating patterns and also easing pain in some instances. Patients in brightly lit rooms stay on average 2.6 days less in hospital than those in dimly lit rooms (Beauchemin and Hays, 1996). Signifi-cant differences were found between natural and artificial lighting including for both staff and patients, for example, a lack of natural lighting can cause seasonal affective disorder (SAD), changes to hormonal body rhythms, glare and flicker, work disruptions, increased staff stress, and decreased staff satisfaction (Ulrich et al., 2008; Schweitzer et al., 2004).
The third theme of the therapeutic milieu includes therapeutic design and environments; patient-centered design; healing environments, especially the Planetree approach, and positive design (Stichler, 2008); and the need for a mul-tidisciplinary approach to healing. This theme overlapped extensively with the fourht theme, regarding gardens and contact with nature. The fourth theme of gardens is revealed as extremely important for both patients and staff for renew-al/restoration of attention, stress relief, and for its social aspects, with evidenced-based research showing high percentages to support this (Naderi & Shin, 2008).
The fifth theme, the impact of architecture on health outcomes, also overlaps with other themes but the literature shows that architecture can enrich the envi-ronment with complexity, order, and aesthetic considerations offering perceptual cues to assist and avoid confusion. Access to nature and sensory/salutogenic con-siderations (Golembiewski, 2010) are important themes within this literature as is the need for privacy and a preference of single bedrooms.
The sixth theme of interior design, which includes the subthemes of furnishings, color, wayfinding, cognitive mapping, spatial organization, and type of patient room, shows the need for clear visual communication balanced with a home-like environment (Lorenz, 2007).
The seventh theme is that of psychogeriatric considerations, which include dementia, violence, and trauma as major subthemes that highlight the need for quiet spaces and gardens, with an emphasis on deinstitutionalizing design fea-tures to encourage social interactions (Dobrohotoff & Llewellyn-Jones, 2010; Day, Carreon, & Stump, 2000).
The eighth theme of post-occupancy evaluations (POEs) deals with the lack of effective evaluations in health architecture generally and mental health partic-ularly. The literature calls for an interdisciplinary approach to POEs, using evi-dence-based design including building performance factors but also with the specific need for occupants’ feedback (Carthey, 2006; Liddell, 2010).

© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 161
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
The ninth theme is that of nursing (duty) stations. The effectiveness of the nurs-ing station is addressed by the literature, with nurse-only and patient-only spaces found to be beneficial to both groups. Closed nursing stations often convey an image of staff inaccessibility to patients and visitors (Andes & Shattell, 2006).
The tenth theme, model of care, incorporates several subthemes such as the bio-psycho-social approach that deals with the patient holistically, length of stay, personal visual elements in the environment, and homelessness. The literature shows the need for a balance between drug-therapy, environmental context and psychological and social therapy and interactions (Cleary, Hunt, O’Connor, & Snars, 2010).
The eleventh theme is the role and importance of art, not only as an activity but also as an aesthetic therapy. Daykin et al. (2008) note that few studies directly examine arts interventions, however a key finding is that depression and anxiety were 34% and 20% lower, respectively, in contexts where patients were exposed to arts.
The twelfth theme, of designing for the adolescent mental health patient, is one that highlights the need for maintaining connectedness to the outside world, including family-centered care; the role of visual preferences, including medi-um density gardens with water; as well as the need to keep personal items, have access to movies, and have private bathrooms (Huffcut, 2010).
The thirteenth theme is forensic psychiatric facility design. Here the subthemes include safety, privacy, and escapes. The literature emphasizes a pleasant domes-tic atmosphere that is well-lit with natural light and provides ample space for patients (Dvoskin et al. (2002).
Finally, the literature shows that there is a need for more research concerning evidence-based design, and for user input into design across all themes. Despite the noted difficulties with post-occupancy evaluations there is a need to have an evidence base in terms of design for mental health units.
ReferencesAnderson, S. E., Good, L.R., & Hurtig, W. E. (1976). Designing a mental health center to replace
a county hospital. Hospital & Community Psychiatry, 27(11), 807–813.
Andes, M., & Shattell, M. M. (2006). An exploration of the meanings of space and place in acute psy-chiatric care. Issues in Mental Health Nursing, 27(6), 699–707. doi:10.1080/01612840600643057
Applebaum, D., Fowler, S., & Fiedler, N. (2010).The impact of environmental factors on nursing stress, job satisfaction & turnover intention. The Journal of Nursing Administration, 40(7-8), 323–328.
Arneill, B. P. (1959). Award winning design for mental health center. Psychiatric Services, 10(6), 37–39.
Au, D. H., McDonell, M. B., Martin, D. C., & Fihn, S. D. (2001) Regional variations in health status, Medical Care, 39(8), 879–888.
Baker, A., Davies, R. L., & Sivadon, P. (1959). Psychiatric services and architecture. Geneva, Switzerland: World Health Organization.

162 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
Barkkume, A. (2007). Innovative building skins: Double glass wall ventilated façade. (Unpub-lished research paper). New Jersey School of Architecture, Newark, NJ.
Basinger, S. B. (2011). Spatial parameters in therapeutic spaces: Design of a residential treat-ment facility for eating disorder patients. (Unpublished master’s thesis). Virginia Common-wealth University, Richmond, VA.
Beauchemin, K. M. & Hays, P. (1996). Sunny hospital rooms expedite recovery from severe and refractory depressions. Journal of Affective Disorders, 40(1), 49–51. doi:10.1016/0165-0327(96)00040-7
Bennington, L., Cummane, J., & Conn, P. (2000). Customer satisfaction and call centres: An Aus-tralian study. International Journal of Service Industry Management, 11(2), 162–173.
Blumberg, R., & Devlin, A. S. (2006). Design issues in hospitals: The adolescent client. Environ-ment and Behavior, 38(3), 293–317. doi:10.1177/0013916505281575
Brawley, E. C. (2001). Environmental design for Alzheimer’s disease: A quality of life issue. Aging & Mental Health, 5(1), S79–S83. doi:10.1080/13607860120044846
Bremner, A. G. (2003). “Some imperial institute”: Architecture, symbolism, and the ideal of empire in late Victorian Britain, 1887-93. Journal of the Society of Architectural Historians, 62(1), 50–73.
Brickell, T. A., & McLean, C. (2001). Emerging issues and challenges for improving patient safety in mental health: A qualitative analysis of expert perspectives. Journal of Patient Safety, 7(1), 39–44. Retrieved from http://www.patientsafetyinstitute.ca/English/research/commissione-dResearch/mentalHealthAndPatientSafety/Documents/Deliverables/A%20Canadian%20Perspective%20of%20Patient%20Safety%20in%20Mental%20Health%20(Handout).pdf
Brown, D. (2009). Designing an effective nurses’ station. Behavioral Healthcare, 29(10), 22–25. Retrieved from http://www.behavioral.net/article/designing-effective-nurses-station/
Brunton, W. (2003). The origins of deinstitutionalization in New Zealand, Health & History: Jour-nal of the Australian & New Zealand Society for the History of Medicine, 5(2), 75–103.
Butera, F. M. (2005, May). Glass architecture: Is it sustainable? Paper presented at Passive and Low Energy Cooling for the Built Environment, Santorini, Greece.
Butler, J., & Ciarrochi, J. (2007). Psychological acceptance and the quality of life in the elderly. Quality of Life Research, 16(4), 607–615.
Caine, R .M. (2003). Psychological influences in critical care: Perspectives from psychoneuroim-munology. Critical Care Nurse, 23(2), 60–70.
Cameron, D. (1959). New frontiers in the mental health effort, Psychiatric Services, 10(2), 66–69.
Carr, R. F. (2011). Psychiatric facility. In Design Guidance. Retrieved from http://www.wbdg.org/design/psychiatric.php/
Carter, M. M. (2008). Physical landscape/mental landscape: Mental health, architecture and the city. (Doctoral dissertation). Retrieved from ProQuest Dissertations and Theses. (Accession Order No. 304406160)
Carthey, J. (2006). Post occupancy evaluation: Development of a standardized methodology for Australian health projects. International Journal of Construction Management, 38(5), 57–74.
Caspari, S. (2011). The importance of aesthetic surroundings: A study interviewing experts within different aesthetic fields. Scandinavian Journal of Caring Science, 25, 134–142. doi:10.1111/j.1471-6712.2010.00803.x
Chaudhry, K., & Pereira, S. M. (2009). A comparison of NHS and private psychiatric intensive care units: Unit and patient characteristics. Journal of Psychiatric Intensive Care, 5(1), 5–13.
Chen, T. S., & Sanoff, H. (1988). The patients’ view of their domain. Design Studies, 9(1). 40–55.
Cleary, M., Hunt, G., O’Connor, N., & Snars, J. (2010). The Concord Centre for Mental Health’s new ‘phase of illness’ model of care: Are we on the right track? Australasian Psychiatry, 18(3), 246–49. doi:10.3109/10398561003686755
Cohen-Mansfield, J., & Werner, P. (1998). The effects of an enhanced environment on nursing home residents who pace. The Gerontologist, 38(2), 199–208.
Connellan, K., Due C., & Riggs, D. (2011a, May). Light lies: How does glass communicate in a men-tal health unit? Paper presented at the Australia and New Zealand Communication Association (ANZCA) Annual Conference. Retrieved from http://unisa.academia.edu/KathleenConnellan/Papers/1419825/Light_Lies_how_does_glass_communicate_in_a_mental_health_unit/
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 163
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
Connellan, K., Due, C., & Riggs, D. (2011b, October). Gardens of the mind: Nature, power and design for mental health. Paper presented at IASDR Diversity and Unity, the 4th World Con-ference on Design Research. Retrieved from http://unisa.academia.edu/KathleenConnellan/Papers/1419818/GARDENS_OF_THE_MIND_nature_power_and_design_for_mental_health/
Cooper-Marcus, C., & Barnes, M. (1995). Gardens in healthcare facilities: Uses, therapeutic ben-efits, and design recommendations. Concord, CA: The Center for Health Design.
Costello, B. (2007). Integrated treatment facility: An alternative care setting for adult patients with mental illness. Clemson, SC: Clemson University.
Curtis, S., Gesler, W., Priebe, S., & Francis, S. (2009). New spaces of inpatient care for peo-ple with mental illness: A complex ‘rebirth’ of the clinic? Health & Place, 15(1), 340–348. doi:10.1016/j.healthplace.2008.06.007
Day, K, Carreon, D., & Stump, C. (2000). The therapeutic design of environments for people with dementia. The Gerontologist, 40(4), 397. doi:10.1093/geront/40.4.397
Daykin, N., Byrne E., Soteriou, T., & O’Connor, S. (2008). The impact of art, design and environ-ment in mental health care: A systematic review of the literature. Journal of the Royal Society for the Promotion of Health, 128(2), 85–94.
Dennard, L. (1997). Review of the book More than bricks and mortar? Mental health and the built environment. Human Relations, 50(4), 451–460. doi:10.1177/001872679705000407
Desai, S. (2010) Violence and surveillance: Some unintended consequences of CCTV monitoring within mental health hospital wards. Surveillance & Society 8(1), 85–92.
Detweiler, M. B., Murphy, P. F., Myers, L. C., & Kim, K. Y. (2008). Does a wander garden influence inappropriate behaviors in dementia residents? American Journal of Alzheimer’s Disease & Other Dementias, 23(1), 31–45, doi:10.1177/1533317507309799
Devlin, A. S. (1992). Psychiatric ward renovation: Staff perception and patient behavior. Environ-ment and Behavior, 24(1), 66–84. doi: 10.1177/0013916592241003
Devlin, A. S., & Arneil, A. B. (2003). Health care environments and patient outcomes: A review of the literature, Environment and Behavior, 35(5), 665–694. doi: 10.1177/0013916503255102
Dijkstra K., Pieterse M., & Pruyn, A. (2006). Physical environmental stimuli that turn healthcare facilities into healing environments through psychologically mediated effects: systematic review. Journal of Advanced Nursing, 56(2), 166–181.
Dix, R., & Williams, K. (1996). Psychiatric intensive care units, a design for living. Psychiatric Bul-letin, 20(9), 527–529. doi:10.1192/pb.20.9.527
Dobrohotoff, J. T., & Llewellyn-Jones, R. H. (2010). Psychogeriatric inpatient unit design: A litera-ture review. International Psychogeriatrics, 23(2), 174–189. doi:10.1017/S1041610210002097
Doherty, J., & Sell, J. E. (2011). Deinstitutionalizing design: Strategies to design a more residen-tial environment for psychiatric patients. Behavioral Healthcare, 31(1), 30–33.
Douglas, J. F. (2011). It all starts with a story. Behavioral Healthcare. Retrieved from http://www.behavioral.net/article/it-all-starts-story
Due, C., & Riggs, D. W. (2010). Playing at the edges: Use of playground spaces in South Aus-tralian primary schools with new arrivals programs. Social Geography, 5, 25–37. doi:10.5194/sg-5-25-2010
Dyer, S. (2003). Designing “community” in the Cherry Hill Mall: The social production of a con-sumer space. Perspectives in Vernacular Architecture, 9, 263–275.
Dvoskin, J. A., Radomski, S. J., Bennett, C., Olin, J. A., Hawkins, R. L., Dotson, L. A., & Drewnicky, I. N. (2002). Architectural design of a secure forensic state psychiatric hospital. Behavioral Sciences & the Law, 20(5), 481–493. doi:10.1002/bsl.506
Ecoff, L., & Brown, C. E. (2010). Evidence-based architectural and design supports Magnet® empirical outcomes. The Journal of Nursing Administration, 40(12), 505–508. doi:10.1097/NNA.0b013e3181fc1a4b
Edge, K. J. (2003). Wall color of patient’s room: Effects on recovery. (Master’s thesis). Retrieved from http://etd.fcla.edu/UF/UFE0000857/edge_k.pdf
Edgerton, E., Ritchie, L., & McKechnie, J. (2010). Objective and subjective evaluation of a rede-signed corridor environment in a psychiatric hospital. Issues in Mental Health Nursing, 31(5), 306–214.
Edginton, B. (2003). The design of moral architecture at the York retreat. Journal of Design His-tory, 16(2), 103–117.

164 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
Enser, J., & MacInnes, D. (1999). The relationship between building design and escapes from secure units. Journal of the Royal Society for the Promotion of Health, 119(3), 170–174. doi:10.1177/146642409911900307
Evans, G. W. (2003). The built environment and mental health. Journal of Urban Health, 80(4), 536–555.
Evans, G. W., Lepore, S. J., & Schroeder, A. (1996). The role of interior design elements in human responses to crowding. Journal of Personality and Social Psychology, 70(1), 41–46.
Finnane, M. (2009). Australian asylums and their histories: Introduction. Health and History, 11(1), 6–8.
Fitzgerald, M. M., Kirk, D. G., & Bristow, C. A. (2011). Description and evaluation of a seri-ous game intervention to engage low secure service users with serious mental illness in the design and refurbishment of their environment. Journal of Psychiatric and Mental Health Nursing, 18(4), 316–322.
Fitzpatrick, H. C. (2007). Supportive housing for mental health recovery: A bio-psycho-social approach. (Master’s thesis). University of Waterloo, Waterloo, Ontario, Canada. Retrieved from http://uwspace.uwaterloo.ca/bitstream/10012/2719/1/OGS_Resub.pdf
Foley, A.R., & Lacy, B.N. (1967). On the need for interprofessional collaboration: Psychiatry and architecture, American Journal of Psychiatry, 123(8).
Folkins, C., O’Reilly, C., Roberts, K., & Miller, S. Physical. (1977). Physical environment and job satisfaction in a community mental health center. Community Mental Health Journal, 13(1), 24–30.
Fottler, M. D., Ford, R. C., Roberts, V. Ford, E. Q., & Spears, J. D. (2000). Creating a healing environment: The importance of the service setting in the new consumer-oriented healthcare system. Journal of Healthcare Management, 42(2), 91–106.
Fox, C. (2003). Debating deinstitutionalization: The fire at Kew Cottages in 1996 and the idea of community. Health and History, 5(2), 37–59.
Frampton, S., Guastello, S., Brady, C., Hale, M., Horowitz, S., Bennett-Smith, S., & Stone, S. (2008). Patient-centered care improvement guide, Derby, CT: Planetree, Inc.
Frank, R. G., & Lave, J. R. (1986). The effect of benefit design on the length of stay of Medicaid psychiatric patients. The Journal of Human Resources, 21(3), 321–337. doi:10.2307/145966
Freeman, H. (1978). Mental health and the environment. The British Journal of Psychiatry, 132, 113–124. doi:10.1192/bjp.132.2.113
Frumkin, H. (1974). Urban sprawl and public health. Public Health Reports, 117(3), 201–217.
Gesler, W., Bell, M., Curtis, S., Hubbard, P., & Francis, S. (2004). Therapy by design: Evaluating the UK hospital building program. Health & Place, 10(2), 117–128.
Golaszewski, T., & Fisher, B. (2002). Heart check: The development and evolution of an orga-nizational heart health assessment. American Journal of Health Promotion, 17(2), 132–153.
Golembiewski, J. A. (2010). Start making sense: Applying a salutogenic model to architecture design for psychiatric care. Facilities, 28(3/4), 100–117. doi:10.1108/02632771011023096
Griffin, W. V., Mauritzen, J. H., & Kasmar, J. V. (1969). The psychological aspects of the architec-tural environment: A review. American Journal of Psychiatry, 125(8), 1057–1062.
Gross, R., Sasson, Y, Zarhy, M., & Zohar, J. (1998). Healing environment in psychiatric hospital design. General Hospital Psychiatry, 20(2), 108–114.
Gulak, M. B. (1991). Architectural guidelines for state psychiatric hospitals. Hospital & Commu-nity Psychiatry, 42(7), 705–707.
Gutkowski, S., Ginath, Y., & Guttmann, F. (1992). Improving psychiatric environments through minimal architectural change. Hospital & Community Psychiatry, 43(9), 920–923.
Hall, E. T. (1973). Mental health research and out-of-awareness cultural systems. In L. Nader & T. W. Maretzki (Eds.), Cultural Illness and Health: Essay in Human Adaption (pp. 97–103). Wash-ington, DC: American Anthropological Association.
Hartig, T., & Marcus, C. C. (2006). Essay: Healing gardens—places for nature in health care. The Lancet, 368, S36–S37. doi:10.1016/S0140-6736(06)69920-0
Heath, Y. (2004). Evaluating the effects of therapeutic gardens. American Journal of Alzheimer’s Disease and Other Dementias, 19(4), 239–242. doi:10.1177/153331750401900410
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 165
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
Hickman, C. (2009). Cheerful prospects and tranquil restoration: The visual experience of land-scape as part of the therapeutic regime of the British asylum, 1800–60. History of Psychiatry, 20(4), 425–441. doi:10.1177/0957154X08338335
Hickman, C. (2005). The picturesque at Brislington House, Bristol: The role of landscape in rela-tion to the treatment of mental illness in the early nineteenth-century asylum. Garden History, 33(1), 47–60.
Holohan, C. J. (1976). Environmental change in a psychiatric setting: A social systems analysis. Human Relations, 29(2), 153–166. doi:10.1177/001872677602900205
Holahan, C. J., & Dobrowolny, M. B. (1978). Cognitive and behavioral correlates of the spa-tial environment: An interactional analysis. Environment and Behavior, 10(3), 317–333. doi:10.1177/0013916578103003
Huffcut, Jamie C. (2010). Can design promote healing? Behavioral Healthcare, 30(9), 33–35. Retrieved from http://www.behavioral.net/article/can-design-promote-healing/
Izumi, K. (1976). Perceptual factors in the design of environments for the mentally ill. Hospital & Community Psychiatry, 27(11), 802–806.
Jackson, L. E. (2003).The relationship of urban design to human health and condition, Land-scape and Urban Planning, 64(4), 191–200.
Jayaram, G., & Herzog, A. (Eds.). (2009). SAFE MD: Practical applications and approaches to safe psychiatric practice. Arlington, VA: APA Committee on Patient Safety.
Johansson, I. M., Skarsater, I., & Danielson, E. (2006). The health-care environment on a locked psychiatric ward: An ethnographic study. International Journal of Mental Health Nursing, 15(4), 242–250.
Joseph, A. (2006). The impact of light on outcomes in healthcare settings. Concord, CA: The Center for Health Design. Retrieved from http://www.healthdesign.org/chd/research/impact-light-outcomes-healthcare-settings/
Kantrowitz, M. (1993). Design evaluation of six primary care facilities for the purpose of informing future design decisions. Concord, CA: The Center for Health Design.
Kaplan, S. (1996). The restorative benefits of nature: Toward an integrative framework. Journal of Environmental Psychology, 15(3), 169–182. doi:10.1016/0272-4944(95)90001-2
Karlin, B. E., & Zeiss, R. A. (2006). Environmental and therapeutic issues in psychiatric hospi-tal design: Toward best practices. Psychiatric Services, 57(10), 1376–1378. doi:10.1176/appi.ps.57.10.1376
Killaspy, H., Ritchie, C. W., Greer, E., & Robertson, M. (2004). Treating the homeless mentally ill: Does a designated inpatient facility improve outcome? Journal of Mental Health, 13(6), 593–599. doi:10.1080/09638230400017038
Korpella, K., & Hartig, T. (1996). Restorative qualities of favorite places. Journal of Environmental Psychology, 16, 221–233. doi:10.1006/jevp.1996.0018
Korpella, K., Hartig, T., Kaiser, F.G., & Fuhrer, U. (2001). Restorative experience and self-regulation in favorite places. Environment and Behavior, 33(4), 572–589. doi:10.1177/00139160121973133
Korpella, K.M., & Ylén, M. (2007). Perceived health is associated with visiting natural favorite places in the vicinity. Health & Place, 13(1), 138–151.
Kumar, S., & Ng, B. (2001). Crowding and violence on psychiatric wards: Explanatory models. The Canadian Journal of Psychiatry, 46(5), 433–447. Retrieved from http://ww1.cpa-apc.org/French_Site/publications/Archives/CJP/2001/June/PDF/crowding.pdf
Laffey, P. (2003). Antipsychiatry in Australia: Sources for a social and intellectual history. Health and History, 5(2), 17–36.
Lawton, M. P. (2001). The physical environment of the person with Alzheimer’s disease. Aging and Mental Health, 5(Suppl 1), S56–S64.
Langan, C., & McDonald, C. (2008). Daytime night attire as a therapeutic intervention in an acute adult psychiatric in-patient unit. The Psychiatrist, 32(6), 221–224. doi:10.1192/pb.bp.107.017491
Levin, A. (2007). Psychiatric hospital design reflects treatment trends. Psychiatric News, 42(2), 9.
Levin, A. (2005). Rational buildings designed to “calm the disorderly mind.” Psychiatric News, 40(17), 24.
Liddell, K. (2010). Good data critical to a successful outcome. Health Estate Journal, 64(5) 23–27. Retrieved from http://www.healthestatejournal.com/Story.aspx?Story=6687
166 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
London, P. (2006). Toward a holistic paradigm in art education. Baltimore, MD: Center for Art Education, Maryland Institute College of Art. Retrieved from http://www.mica.edu/Docu-ments/Art%20Education/HolisticMonograph.pdf
Lorenz, S. G. (2007). The potential of the patient room to promote healing and well-being in patients and nurses. Holistic Nursing Practice, 21(5), 263–277.
Lyubomirsky, S., Sheldon, K. M., Schkade, D. (2005). Pursuing happiness: The architecture of sustainable change. Review of General Psychology, 9(2) 111–131.
MacKinnon, D. (2009). Divine service, music, sport, and recreation as medicinal in Australian asylums 1860s–1945. Health and History, 11(1), 128–148.
Magowan, R. (2010). Self-portrait in a rock garden. Southwest Review, 95(1-2), 255–263.
Main, S., McBride, A. B., & Austin, J. K. (1991). Patient and staff perceptions of a psychiatric ward environment. Issues in Mental Health Nursing, 12(2), 149–157.
Malcom, E. (2009). Australian asylum architecture through German eyes. Health and History, 11(1), 46–64.
Marcus, C. C., & Barnes, M. (1995). Gardens in healthcare facilities: Uses, therapeutic benefits, and design recommendations. Concord, CA: The Center for Health Design.
Marmot, A. (2002). Architectural determinism: Does design change behavior? The British Jour-nal of General Practice, 52(476), 252–253.
Mays, J. B. (2007). Mind over matter. The Canadian Architect. Retrieved from http://www.cana-dianarchitect.com/news/mind-over-matter/1000215070/
Mazuch, R., & Stephen, R. (2005). Creating healing environments: Humanistic architecture and ther-apeutic design. Journal of Public Mental Health, 4(4), 48–52. doi:10.1108/17465729200500031
McGuire, M. T., Fairbanks, L. A., Cole, S. R., Sbordone, R., Silvers, F. M., Richards, M., & Akers. J. (1977). The ethological study of four psychiatric wards: Behavior changes asso-ciated with new staff and new patients. Journal of Psychiatry, 13(4), 211–236. doi:10.1016/S0022-3956(77)90017-6
Moon, G. (2000). Risk and protection: The discourse of confinement in contemporary mental health policy. Health & Place, 6(3), 239–250.
Morrall, P., & Hazelton, M. (2000). Architecture signifying social control: The restoration of asy-lumdom in mental health care? Australian and New Zealand Journal of Mental Health Nursing, 9(2), 89–96. doi:10.1046/j.1440-0979.2000.00166.x
Munt, D., & Hargreaves, J. (2009). Aesthetic, emotion and empathetic imagination: Beyond inno-vation to creativity in the health and social care workforce. Health Care Analysis, 17(4), 285–295. doi:10.1007/s10728-009-0131-2
Murdoch, M., Hodges, J., Cowper, D., Fortier, L., & van Ryn, M. (2003). Racial disparities in VA service connection for posttraumatic stress disorder disability. Medical Care, 41(4), 536–549.
Naderi, J. R., & Shin, W.-H. (2008). Humane design for hospital landscapes: A case study in land-scape architecture of a healing garden for nurses. Health Environments Research & Design Journal, 2(1), 82–119.
Nanda, U., Eisen, S. L., & Baladandayuthapani, V. (2008). Undertaking an art survey to com-pare patient versus student art preferences. Environment & Behavior, 40(2), 269–301. doi:10.1177/0013916507311552
Novotná, G., Urbanoski, K. A., & Rush, B. R. (2011). Client-centered design of residential addic-tion and mental health care facilities: Staff perceptions of their work environment. Quality Health Research, 21(11), 1527–1538.
Osborn, L. A. (1952). Functional design of psychiatric hospitals. American Journal of Psychiatry, 109(2), 139–142.
Osmond, H. (1957). Function as the basis of psychiatric ward design. Mental Hospitals, 8(4), 23–29.
Pagan, J. D., Cunningham, S. D. and Higgs, P. L.(2008). Getting creative in healthcare: The contribution of creative activities to Australian healthcare. Brisbane, Australia: ARC Centre of Excellence for Creative Industries and Innovation. Retrieved from http://eprints.qut.edu.au/14757/1/14757.pdf
Pelikan, J. M., Krajic, K., & Dietscher, C. (2001). The health promoting hospital (HPH): Concept and development. Patient Education and Counseling, 45(4), 239–243.
© 2013 VENDOME GROUP LLC HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 167
MENTAL HEALTH AND ARCHITECTURE LITERATURE REVIEW
Philo, C. (1997). Across the water: Reviewing geographical studies of asylums and other mental health facilities, Health & Place, 3(2), 73–89.
Piddock, S. (2004). Possibilities and realities: South Australia’s asylums in the 19th century. Aus-tralasian Psychiatry, 12(2), 172–175.
Pressly, P. K., & Heesacker, M. (2001). The physical environment and counseling: A review of theory and research. Journal of Counseling & Development, 79(2), 148–160. doi:10.1002/j.1556-6676.2001.tb01954.x
Prior, L. (1988). The architecture of the hospital: A study of spatial organization and medical knowledge. The British Journal of Sociology, 39(1), 86–113.
Prior, L. (1993). The social organization of mental illness. London, England: Sage Publications.
Rawcliffe, C. (2008). Delectable sights and fragrant smells: Gardens and health in late mediaeval and early modern England. Garden History, 36(1), 3–21.
Reiling, J., Hughes, R. G., & Murphy, M. R. (2008). The impact of facility design on patient safety. In R. G. Hughes (Ed.), Patient safety and quality: An evidence-based handbook for nurses. Rockville, MD: Agency for Healthcare Research and Quality. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK2633/
Rosenthal, M. (2008). London versus Sydney, 1815–1823: The politics of colonial architecture. Journal of Historical Geography, 34(2), 191–219.
Rubin, H. R., Owens, A. J., & Golden, G. (1998). Investigation to determine whether the built environment affects patients’ medical outcomes. Concord, CA: The Center for Health Design. Retrieved from http://www.healthdesign.org/chd/research/investigation -determine-whether-built-environment-affects-patients-medical-outcomes
Rynor, B. (2010). Beautifying hospitals: A tough sell. Canadian Medical Association Journal, 182(13), E633–E634. doi:10.1503/cmaj.109-3320
Sadar, J. (2008). The healthful ambience of Vitaglass: Light, glass and the curative environment. Architectural Research Quarterly, 12(3-4), 269–281. doi:10.1017/S1359135508001206.
Salmi, P. (2008). Wayfinding design: Hidden barriers to universal access. InformeDesign, 5(8). Retrieved from http://www.informedesign.org/_news/aug_v05r-p.pdf
Savage, J. (2000). Ethnography and health care. British Medical Journal, 321(7273), 1400–1402.
Schofield, P. (2003). A pilot study into the use of a multisensory environment (Snoezelen) within a palliative day-care setting. International Journal of Palliative Nursing, 9(3), 124–129.
Schweitzer, M., Gilpin, L., & Frampton, S. (2004). Healing spaces: Elements of environmental design that make an impact on health. Journal of Alternative and Complementary Medicine, 10(Suppl 1), S71–S83. doi:10.1089/1075553042245953
Staricoff, R., & Loppert, S. (2003). Integrating the arts into health care: Can we affect clinical outcomes? In D. Kirklin & R. Richardson (Eds.), The healing environment: Without and within (pp. 63–80). London, England: Royal College of Physicians.
Stichler, J. F. (2008). Healing by design. Journal of Nursing Administration, 38(12), 505–509. doi:10.1097/NNA.0b013e31818ebfa6
Thibaud, J.-P. (2001). Frames of visibility in public places. Places,14(1), 42–47. Retrieved from http://www.escholarship.org/uc/item/59r5834p
Ulrich, R. S. (1991). Effects of interior design on wellness: Theory and recent scientific research. Journal of Health Care Interior Design, 3, 97–109. Retrieved from http://www.majorhospital-foundation.org/pdfs/Effects%20of%20Interior%20Design%20on%20Wellness.pdf
Ulrich, R. S. (2001). Effects of healthcare environmental design on medical outcomes. In A. Dilani (Ed.), Design and health: The therapeutic benefits of design (pp. 49–59). Stockholm, Swe-den: AB Svensk Byggtjanst. Retrieved from http://treebenefits.terrasummit.com/Documents/Health/Effects%20of%20Healthcare%20environments.pdf
Ulrich, R. S. (2000). Evidence-based environmental design for improving medical outcomes. Paper presented at Healing by Design: Building for Healthcare in the 21st Century, Montreal, Quebec, Canada.
Ulrich, R., Zimring, C., Zhu X., DuBose, J., Seo, H.-B., Choi, Y.-S., ... Joseph A. (2008). A review of the research literature on evidence-based healthcare design. Health Environments Research & Design Journal, 1(3), 61–125. Retrieved from https://www.herdjournal.com/article/review-research-literature-evidence-based-healthcare-design-part-i

168 WWW.HERDJOURNAL.COM © 2013 VENDOME GROUP LLC
SUMMER 2013 • VOL. 6 NO. 4, pp. 127–168LITERATURE REVIEW
Vaaler, A. E., Morken, G., & Linaker, O. M. (2005). Effects of different interior decorations in the seclusion area of a psychiatric acute ward. Nordic Journal of Psychiatry, 59(1), 19–24. doi:10.1080/08039480510018887
Vanoni-De La Garza, L. (2007). Inside psychiatric architecture: Metaphor applied to a case study of the San Antonio State hospital. (Unpublished master’s thesis). University of Texas at San Antonio, San Antonio, TX.
Verderber, S., & Fine, D. J. (2000). Healthcare architecture in an era of radical transformation. New Haven, CT: Yale University Press.
Vischer, J. C. (2009). Applying knowledge on building performance: From evidence to intelli-gence. Intelligent Buildings International, 1(4)239–248. doi:10.3763/inbi.2009.SI02
Ware, N. C., Tugenberg, T., Dickey, B., & McHorney, C. A. (1999). An ethnographic study of the meaning of continuity of care in mental health services. Psychiatric Services, 50(3), 395–400.
Weich, S., Blanchard, M., Prince, M., Burton, E., Erens, B., & Sproston, K. (2002). Mental health and the built environment: Cross-sectional survey of individual and contextual risk factors for depression. The British Journal of Psychiatry, 180, 428–433.
Wessling, R. (2009). On the threshold of hope. Behavioral Healthcare, 29(5), 30–32. Retrieved from http://www.behavioral.net/article/threshold-hope
Whitehead, C. C., Polsky, R. H., Crookshank, C., & Fik, E. (1984).Objective and subjective evalu-ation of psychiatric ward redesign. American Journal of Psychiatry, 141(5), 639–644.
Worpole, K. (2009). Modern hospice design: The architecture of palliative care. New York, NY: Routledge.
Yanni, C. (2003). The linear plan for insane asylums in the United States before 1866. Journal of the Society of Architectural Historians, 62(1), 24–49.
Zborowsky, T., & Kreitzer, M. J. (2008). Creating optimal healing environments in a health care setting. Minnesota Medicine, 91(3), 35–38.
Zeiger, M. (2006). Mind matters: London students analyze the architecture of mental illness. Architecture, 95(9), 62–65.
Copyright of Health Environments Research & Design Journal (HERD) is the property ofVendome Group LLC and its content may not be copied or emailed to multiple sites or postedto a listserv without the copyright holder's express written permission. However, users mayprint, download, or email articles for individual use.





























