Embed Size (px)
Citation preview

Stage-based interventions for smoking cessation (Review)
Cahill K, Lancaster T, Green N
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2010, Issue 11
http://www.thecochranelibrary.com
Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
12DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
25CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
68DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Optimal trial comparisons, Outcome 1 Stage-based vs standard SH materials. . . . . 71
Analysis 1.2. Comparison 1 Optimal trial comparisons, Outcome 2 Stage-based counselling vs standard advice. . . 72
Analysis 2.1. Comparison 2 Abstinence by intervention and comparison, Outcome 1 Expert systems. . . . . . . 72
Analysis 2.2. Comparison 2 Abstinence by intervention and comparison, Outcome 2 Individual counselling. . . . 74
Analysis 2.3. Comparison 2 Abstinence by intervention and comparison, Outcome 3 Interactive computer programme. 75
Analysis 2.4. Comparison 2 Abstinence by intervention and comparison, Outcome 4 Phone quit lines. . . . . . 76
Analysis 2.5. Comparison 2 Abstinence by intervention and comparison, Outcome 5 Training doctors. . . . . . 76
Analysis 2.6. Comparison 2 Abstinence by intervention and comparison, Outcome 6 Training lay supporters. . . . 77
Analysis 2.7. Comparison 2 Abstinence by intervention and comparison, Outcome 7 Staged SH materials. . . . . 77
Analysis 3.1. Comparison 3 Validated abstinence, Outcome 1 Biochemically validated abstinence. . . . . . . . 78
Analysis 3.2. Comparison 3 Validated abstinence, Outcome 2 Self-reported abstinence. . . . . . . . . . . . 79
Analysis 3.3. Comparison 3 Validated abstinence, Outcome 3 ’Bogus pipeline’. . . . . . . . . . . . . . 80
Analysis 4.1. Comparison 4 Missing data testing, Outcome 1 Intervention ITT versus control per protocol. . . . 81
Analysis 4.2. Comparison 4 Missing data testing, Outcome 2 Intervention ITT versus control ITT. . . . . . . 82
Analysis 5.1. Comparison 5 Any stage-based intervention vs control, Outcome 1 Abstinence at longest follow up. . 83
Analysis 5.2. Comparison 5 Any stage-based intervention vs control, Outcome 2 Abstinence by comparison condition. 85
Analysis 6.1. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 1 Expert systems. . . . 87
Analysis 6.2. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 2 Individual counselling. . 88
Analysis 6.3. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 3 Interactive computer
programme. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
Analysis 6.4. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 4 Phone quit lines. . . . 91
Analysis 6.5. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 5 Training doctors. . . . 92
Analysis 6.6. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 6 Training lay supporters. . 92
Analysis 6.7. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 7 Staged SH materials. . . 93
Analysis 7.1. Comparison 7 Per protocol analyses, Outcome 1 Expert systems. . . . . . . . . . . . . . . 93
Analysis 7.2. Comparison 7 Per protocol analyses, Outcome 2 Individual counselling. . . . . . . . . . . . 95
Analysis 7.3. Comparison 7 Per protocol analyses, Outcome 3 Interactive computer programme. . . . . . . . 96
Analysis 7.4. Comparison 7 Per protocol analyses, Outcome 4 Phone quit lines. . . . . . . . . . . . . . 97
Analysis 7.5. Comparison 7 Per protocol analyses, Outcome 5 Training doctors. . . . . . . . . . . . . . 98
Analysis 7.6. Comparison 7 Per protocol analyses, Outcome 6 Training lay supporters. . . . . . . . . . . . 98
Analysis 7.7. Comparison 7 Per protocol analyses, Outcome 7 Staged SH materials. . . . . . . . . . . . . 99
Analysis 8.1. Comparison 8 Cluster randomized trials, Outcome 1 Individual counselling. . . . . . . . . . 99
Analysis 8.2. Comparison 8 Cluster randomized trials, Outcome 2 Interactive computer programme. . . . . . . 101
Analysis 8.3. Comparison 8 Cluster randomized trials, Outcome 3 Training doctors. . . . . . . . . . . . 102
102ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
103APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
105HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iStage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

105CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
106DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
106SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
106DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
106INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiStage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Stage-based interventions for smoking cessation
Kate Cahill1, Tim Lancaster1 , Natasha Green2
1Department of Primary Health Care, University of Oxford, Oxford, UK. 2London, UK
Contact address: Kate Cahill, Department of Primary Health Care, University of Oxford, Rosemary Rue Building, Old Road Campus,
Oxford, OX3 7LF, UK. [email protected].
Editorial group: Cochrane Tobacco Addiction Group.
Publication status and date: New, published in Issue 11, 2010.
Review content assessed as up-to-date: 27 August 2010.
Citation: Cahill K, Lancaster T, Green N. Stage-based interventions for smoking cessation. Cochrane Database of Systematic Reviews2010, Issue 11. Art. No.: CD004492. DOI: 10.1002/14651858.CD004492.pub4.
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
The transtheoretical model is the most widely known of several stage-based theories of behaviour. It proposes that smokers move through
a discrete series of motivational stages before they quit successfully. These are precontemplation (no thoughts of quitting), contemplation(thinking about quitting), preparation (planning to quit in the next 30 days), action (quitting successfully for up to six months), and
maintenance (no smoking for more than six months). According to this influential model, interventions which help people to stop
smoking should be tailored to their stage of readiness to quit, and are designed to move them forward through subsequent stages
to eventual success. People in the preparation and action stages of quitting would require different types of support from those in
precontemplation or contemplation.
Objectives
Our primary objective was to test the effectiveness of stage-based interventions in helping smokers to quit.
Search methods
We searched the Cochrane Tobacco Addiction Group’s specialised register for trials, using the terms (’stage* of change’, ’transtheoretical
model*’, ’trans-theoretical model*, ’precaution adoption model*’, ’health action model’, ’processes of change questionnaire*’, ’readiness
to change’, ’tailor*’) and ’smoking’ in the title or abstract, or as keywords. The latest search was in August 2010.
Selection criteria
We included randomized controlled trials, which compared stage-based interventions with non-stage-based controls, with ’usual care’
or with assessment only. We excluded trials which did not report a minimum follow-up period of six months from start of treatment,
and those which measured stage of change but did not modify their intervention in the light of it.
Data collection and analysis
We extracted data in duplicate on the participants, the dose and duration of intervention, the outcome measures, the randomization
procedure, concealment of allocation, and completeness of follow up.
The main outcome was abstinence from smoking for at least six months. We used the most rigorous definition of abstinence, and
preferred biochemically validated rates where reported. Where appropriate we performed meta-analysis to estimate a pooled risk ratio,
using the Mantel-Haenszel fixed-effect model.
1Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Main results
We found 41 trials (>33,000 participants) which met our inclusion criteria. Four trials, which directly compared the same intervention in
stage-based and standard versions, found no clear advantage for the staging component. Stage-based versus standard self-help materials
(two trials) gave a relative risk (RR) of 0.93 (95% CI 0.62 to 1.39). Stage-based versus standard counselling (two trials) gave a relative
risk of 1.00 (95% CI 0.82 to 1.22). Six trials of stage-based self-help systems versus any standard self-help support demonstrated a
benefit for the staged groups, with an RR of 1.27 (95% CI 1.01 to 1.59). Twelve trials comparing stage-based self help with ’usual care’
or assessment-only gave an RR of 1.32 (95% CI 1.17 to 1.48). Thirteen trials of stage-based individual counselling versus any control
condition gave an RR of 1.24 (95% CI 1.08 to 1.42). These findings are consistent with the proven effectiveness of these interventions
in their non-stage-based versions. The evidence was unclear for telephone counselling, interactive computer programmes or training
of doctors or lay supporters. This uncertainty may be due in part to smaller numbers of trials.
Authors’ conclusions
Based on four trials using direct comparisons, stage-based self-help interventions (expert systems and/or tailored materials) and individual
counselling were neither more nor less effective than their non-stage-based equivalents. Thirty-one trials of stage-based self help or
counselling interventions versus any control condition demonstrated levels of effectiveness which were comparable with their non-
stage-based counterparts. Providing these forms of practical support to those trying to quit appears to be more productive than not
intervening. However, the additional value of adapting the intervention to the smoker’s stage of change is uncertain. The evidence is
not clear for other types of staged intervention, including telephone counselling, interactive computer programmes and training of
physicians or lay supporters. The evidence does not support the restriction of quitting advice and encouragement only to those smokers
perceived to be in the preparation and action stages.
P L A I N L A N G U A G E S U M M A R Y
Are stage-based interventions more effective than non-stage-based ones in helping smokers to quit?
The transtheoretical model is one of several stage-based theories of behaviour change. It suggests that smokers move through a series of
motivational stages before they manage to stop smoking. These are precontemplation (no thoughts of quitting), contemplation (thinking
about quitting), preparation (planning to quit in the next 30 days), action (quitting successfully for up to six months), and maintenance(no smoking for more than six months). According to this widely-known theory, programmes which help people to stop smoking
should be matched to their stage of readiness to quit. They are designed to move them forward through the stages to eventual success.
In this review, we have compared stage-based programmes of smoking cessation with standard (unstaged) programmes, or with ’usual
care’, or with assessment only. We found 41 stage-based trials, covering more than 33,000 smokers, which measured quit rates at least
six months after treatment. Only four of the 41 trials directly compared the same intervention in a standard and a stage-based version.
This showed that the stage-based version was neither more nor less effective than the standard one. Eighteen trials which compared
stage-based self-help programmes with any control condition showed better success rates for the intervention groups. Thirteen trials
of stage-based individual counselling versus any control condition showed a similar benefit for the intervention groups. These findings
confirm the known effectiveness of these interventions, whether staged or unstaged. The evidence was less clear on the effects of stage-
based telephone counselling, interactive computer programmes or training of doctors and helpers. This uncertainty may be due in part
to smaller numbers of trials. We find on the evidence from this review that providing self-help or counselling support to smokers trying
to quit is more effective than ’usual care’ or simple observation. However, the extra value of fitting that support to the smoker’s stage
of change is currently unclear.
B A C K G R O U N D
Almost five million people worldwide die prematurely from smok-
ing each year. If current trends continue, this will rise to 10 mil-
lion within 10 years, with 70% of those deaths occurring within
the developing world (WHO FCTC 2000). It has been estimated
that between 1950 and 2000, 60 million people have died from
tobacco-related diseases (Peto 1994). In the USA alone, smoking
now kills around 512,000 people a year. These premature deaths
2Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

from smoking on average amount to each individual losing 23
years of life (CTSU 2006).
Smokers are also at increased risk of a number of non-lethal ill-
nesses, including cataracts, Crohn’s disease, depression, diabetes
Type 2, impotence, visual impairment, osteoporosis and tuber-
culosis (ACSH 2003). They suffer increased fertility problems,
and aggravated symptoms of asthma, chronic rhinitis, diabetic
retinopathy, Graves’ disease, multiple sclerosis and optic neuri-
tis (ACSH 2003). However, stopping smoking before middle age
avoids more than 90% of the risk attributable to smoking (Peto
2000).
There are a number of established aids to smoking cessation,
including a range of pharmacotherapies (nicotine replacement
therapy (Stead 2008), bupropion (Hughes 2007), varenicline
(Cahill 2008)) and behavioural approaches (group or individ-
ual counselling (Stead 2005; Lancaster 2005a), self-help mate-
rials (Lancaster 2005b)). One widely-used behavioural approach
is the ’stages of change’ or transtheoretical model (TTM), pro-
pounded by Prochaska and colleagues (Prochaska 1985; Prochaska
1991; Prochaska 1997). This approach assumes that smokers pass
through a discrete series of motivational stages (Prochaska 2001):
Precontemplation: the individual does not perceive their smoking
to be a problem and has no intention of quitting in the foreseeable
future (typically over the next six months).
Contemplation: the individual is aware that their smoking is a prob-
lem, and is thinking seriously about overcoming it but has not
committed to a course of action. Contemplators may state that
they are seriously considering changing their behaviour within the
next six months.
Preparation: Individuals intend to take action within the next
month, and have unsuccessfully taken action in the past year (there
is some debate over the appropriateness of previous failure as a
defining feature of this phase; West 2005a).
Action: the person makes overt behavioural changes to stop smok-
ing, and has successfully altered their behaviour for a period of
anything from one day to six months.
Maintenance: the now ex-smoker works to prevent relapse and to
consolidate their abstinence for more than six months.
Termination (not always an explicit component of the model): the
individual has completed the process of change; they have a high
level of confidence across all high-risk situations and no temptation
to relapse.
The model proposes that individuals move sequentially through
the stages, but may revert to earlier stages before finally achieving
complete abstinence. The authors also identify 10 strategies or
’processes of change’, which help an individual to move through
the quitting process, and which vary from stage to stage (Prochaska
1988). Other component variables of the model include decisional
balance (weighing the pros and cons of maintaining current be-
haviour), situational temptations (managing scenarios in which
one might lapse), and self-efficacy (the belief that one will be able
to change one’s behaviour). The theory assumes that an individ-
ual’s stage of change can be accurately defined, so that the ap-
propriate intervention can be offered, and that the stage will fre-
quently be re-assessed and the intervention tailored accordingly. It
also propounds that incremental moves through the stages, inde-
pendently of an active quit attempt, predict higher eventual levels
of abstinence (Prochaska 2004).
The stages of change model has been deployed for a number
of therapeutic purposes. Its application to alcohol abuse (Project
MATCH 1997; Project MATCH 1998), to physical activity
(Blissmer 2002) and to radon testing (Weinstein 1998) have all
been explored elsewhere. Similar models of behaviour change were
hypothesised concurrently with the development of the TTM, in-
cluding the Precaution Adoption model (Weinstein 1988), and the
Health Action model (Tones 1987). The stages of change model
has remained influential in the development of current guide-
lines for clinical practice. It remains standard practice to set a quit
date during supported cessation attempts, on the assumption that
abrupt or spontaneous quit attempts are less likely to succeed (cf.
Larabie 2005; West 2005a; West 2006). However, the conceptual
validity and the practical usefulness of the stages of change model
for smoking cessation have been challenged over recent years, and a
number of systematic reviews of trials based on the model have pro-
duced inconsistent or negative findings (Froelicher 2002; Littell
2002; Spencer 2002; Riemsma 2003; van Sluijs 2004; Bridle 2005;
Webb 2006; Herzog 2008; Herzog 2010). Our review is intended
to contribute to this process of testing the application and value
of the model for smoking cessation.
O B J E C T I V E S
To evaluate the effectiveness of interventions using a stage-based
approach to achieve abstinence from smoking, compared with:
• no intervention (assessment only or usual care)
• a non-stage-based intervention of lower intensity
• a non-stage-based intervention of equal intensity
M E T H O D S
Criteria for considering studies for this review
Types of studies
3Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Randomized or quasi-randomized controlled trials.
Types of participants
Smokers, of any age, race or gender.
Types of interventions
Any intervention using a stage-based design to influence a change
in smoking behaviour. We have attempted to distinguish where
possible, between those studies which substantively modify the
intervention to fit the estimated state of change, and those which
simply assess participants’ stage of change or use the stage-based
model to frame the approach without greatly affecting the content
of the intervention. The latter group have not been treated as
included studies.
The intervention may be compared with a non-stage-based control
(lower or equal intensity), or with a no-intervention control or
usual care group.
Types of outcome measures
The primary outcome is smoking cessation at least six months
after the start of the intervention, and longer wherever the data are
reported. Many of the studies in this review are cessation induction
studies, i.e. aiming to persuade mostly reluctant quitters to try
and stop, and often supporting them as they make a quit attempt.
Assessment of abstinence is therefore made after the period of
cessation induction, where that distinction is reported.
Secondary outcomes include any adverse effects of the interven-
tions. We have not included movement through stages of change
as an outcome of interest, since the primary concern of this re-
view and of the included studies is achievement and maintenance
of smoking cessation (Prochaska 2006). However, we consider
movement through stages of change in the Discussion section, as
a marker of the validity of the model for smoking cessation.
Search methods for identification of studies
We searched the Cochrane Tobacco Addiction Review Group
Specialized Register for trials. This register has been developed
from electronic searching of CENTRAL, MEDLINE, EMBASE
and PsycINFO, together with handsearching of specialist jour-
nals, conference proceedings and reference lists of previous trials
and overviews. We identified potentially relevant records from the
Register by searching for the following phrases in the title, abstract
or keywords; ’stage* of change’, ’transtheoretical model*’, ’trans-
theoretical model*, ’precaution adoption model*’, ’health action
model*’, ’health action process*’, ’health action approach*’ ’pro-
cesses of change’, ’readiness to change’, ’motivational interviewing’
or ’rubicon’). The most recent search of the register was in Au-
gust 2010. See the Tobacco Addiction Group module for Register
search strategies for all databases and dates of searches.
We have also checked the bibliographies of retrieved references
for further relevant publications, and have contacted authors and
experts in the field where necessary. There were no restrictions on
language or publication date.
Data collection and analysis
Two authors (KC and NG) independently assessed the retrieved ti-
tles and abstracts, and obtained full text copies of relevant articles.
They assessed them for possible inclusion against the pre-deter-
mined selection criteria . Each author independently extracted the
relevant data from trials meeting the selection criteria, and then
compared their extraction forms. Any disagreements were resolved
by discussion with the third author, and with the editorial base.
We have recorded the following trial characteristics, where they
were reported:
• Country
• Setting (e.g. community/ hospital/ outpatient clinic/
workplace/school)
• Stage of Change model used (Transtheoretical Model
[TTM]/ Health Action Process/ Precaution Adoption Process/
Rubicon process)
• Method of randomization and allocation concealment (if
used)
• Participant characteristics: number, age, sex, baseline
smoking, stage distribution
• Intervention: method of stage assessment, number and
timing of contacts, total duration
• Comparison group(s)
• Statistical techniques
• Outcomes: Follow-up period (from start of intervention),
definition of quitting (primary outcome), definition of stage of
change. Biochemical validation of self-report (if used)
• Implementation issues, attrition rates, withdrawals/losses to
follow up. Any differential loss to follow up by treatment group
or by stage of change at baseline will be noted.
The primary outcome was the number of quitters at the longest
follow up, and at least six months from the start of the interven-
tion. We preferred, but did not require, biochemically validated
quitting over self report, and measures of continuous or prolonged
abstinence over point prevalence. We treated participants lost to
follow up as continuing to smoke, and included them in an in-
tention-to-treat analysis where possible. However, since many of
the studies were population- rather than clinic-based, we also con-
ducted sensitivity analyses to test different assumptions about the
smoking status of those lost to follow up.
We describe and display results graphically as a risk ratio (RR:
[number of quitters/total number of participants in intervention
group] divided by [number of quitters/total number of partici-
pants in control group]) with 95% confidence intervals.
4Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analyses which included cluster-randomized trials have been con-
ducted with and without adjustment for clustering. Adjustment
for clustering generally delivered slightly wider confidence inter-
vals. Where applicable both versions are reported in the Results
section. The data, the interclass correlation and the design effects
used for these trials are displayed in Additional Table 1.
We have included a brief discussion of secondary outcomes, in-
cluding movement through stages of change.
We have assessed each included trial for methodological quality
and for the quality of the implementation of the intervention,
using the following questions:
• Was the method of randomization (sequence generation)
reported and acceptable?
• Was the method of allocation concealment reported and
acceptable?
• Were the intervention and control groups comparable at
baseline? If not, were analyses adequately adjusted?
• Were rates of attrition (during treatment) and loss to
follow-up (post-treatment) at acceptable levels, and did they
differ between groups ?
• Did all groups get the same treatment apart from the
intervention being tested?
• Was stage of change assessed at baseline?
• Was the stage of change instrument validated?
• Was the intervention tailored to individual stage of change?
• Was the quality and fidelity of the implementation
reported?
• Were the statistical methods appropriate?
• Were details of the training of educators given, where
applicable?
We have performed meta-analysis using the Mantel-Haenszel risk
ratio and fixed-effect method, provided that there was no signifi-
cant heterogeneity between the trials in their interventions, pop-
ulations and design. We assess statistical heterogeneity between
trials using the I² statistic, which describes the percentage of total
variation between studies that is due to heterogeneity rather than
to chance (Higgins 2003). Values over 50% suggest moderate het-
erogeneity, and values over 75% substantial heterogeneity.
We have performed sub-group analyses based primarily on types
of intervention, where such groupings can be made, with pooling
of trials that use the same format for intervention.
We include in this review the Tobacco Addiction Group glossary
of tobacco-specific terms (Appendix 1).
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies; Characteristics of ongoing studies.
We identified 41 trials for inclusion in our review. Full details
of each trial are given in the Characteristics of included studies
table. A further 58 trials did not meet the inclusion criteria for this
review, and are briefly described in the Characteristics of excluded
studies table, with reasons for their exclusion. Seven additional
trials could not be confirmed as meeting our inclusion criteria, and
are listed as excluded because of insufficient information (Hughes
2000; Borrelli 2002; Jones 2003; McDonald 2003; Chan 2005;
Tsoh 2005; Skewes 2007). One included study (Velicer 1999)
did not incorporate a non-stage-based control condition, and has
therefore not contributed to the meta-analyses. Two trials (Cabezas
2009; Prokhorov 2010) have not yet reported their findings, and
are described in the Characteristics of ongoing studies table.
Fifteen of the included studies had more than one intervention
arm. In two cases (Lawrence 2005; Meyer 2008) we have meta-
analysed the data under more than one category, where this could
be done without pooling. For the remainder we have either com-
bined intervention arms versus control or have selected the most
informative comparison for this review. In each case, the selected
comparisons are described in the ’Notes’ field of the Included Stud-
ies table.
The transtheoretical or stages of change model is often used in
conjunction with motivational interviewing (MI). In this review
we have included studies which primarily test stage-based inter-
ventions for smoking cessation, whether or not they deployed
MI techniques. Twelve of the included studies explicitly used
some form of MI-based counselling in the delivery of their stage-
based or control interventions (Lennox 1998; McBride 1999;
Stotts 2002; Mermelstein 2003; Manfredi 2004; Patten 2004;
Hennrikus 2005; Hollis 2005; Prochaska 2008; Prokhorov 2008;
Young 2008; Hannöver 2009). Our review of motivational in-
terviewing for smoking cessation (Lai 2010) covers studies which
concentrate on those interventions. Hennrikus 2005 is an included
study for both reviews; Manfredi 2004 is included in this review
but excluded from the motivational interviewing review, as the
impact of the MI counselling could not be isolated from other
intervention components.
Settings
Twenty-one of the included studies were conducted in the USA.
Five were in the UK, three each in Australia, the Netherlands and
Germany, and one each in Belgium, Canada, Finland, Switzerland,
Taiwan and Japan.
Eleven of the included studies were population-based. Nine were
set in clinics or in out-patient departments, three in antenatal clin-
ics and three on hospital wards. Five were set in family practices.
Six were education-based, including three set in secondary schools,
two in colleges and one accessing the parents of school children.
Two trials were conducted through telephone quitlines, and two
were set in worksites.
5Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Interventions
We have grouped the included studies under six intervention types.
Within these broad categories we have then examined them by the
comparison condition, i.e. generic self-help, ’usual care’, or assess-
ment only. Additionally, four trials which used a non-smoking-
related healthcare intervention as their comparator are treated for
our purposes as assessment only.
1: Tailored, computer-generated or ’expert system’ letters (18 trials):
(Prochaska 1993; Curry 1995; Dijkstra 1998; Dijkstra 1999;
McBride 1999; Velicer 1999; Lennox 2001; Prochaska 2001a;
Stotts 2002; Aveyard 2003; Borland 2003; Borland 2004; Etter
2004; Prochaska 2004; Hollis 2005; Prochaska 2005; Schumann
2006; Meyer 2008 [Int 1]).
These are personalised reports or letters, usually produced elec-
tronically in response to baseline and follow-up questionnaires or
interviews. They are matched to the participant’s perceived stage of
change, and may include self-help materials (tailored or standard)
and/or follow-up phone calls. Stotts 2002 combined individual
MI-based counselling with an expert system letter, but is included
within this group for our review. Five of the studies were struc-
tured incrementally, i.e. augmenting the intervention components
across a number of arms, compared with a non-staged control
group (Prochaska 1993; Curry 1995; Velicer 1999; Aveyard 2003;
Borland 2003). This group of studies is discussed separately in the
’Effects of the Interventions’ section below. Velicer 1999 is not
included in the meta-analyses, as it did not include a non-staged
control group.
2. Individual counselling or brief advice (13 trials):
(Bobo 1998; Pieterse 2001;Mermelstein 2003; Manfredi 2004;
Nakamura 2004; Chouinard 2005; Davies 2005; Hennrikus
2005; Lawrence 2005 [Arm B]; Meyer 2008 [Int 2]; Prokhorov
2008; Hannöver 2009; Meysman 2010). This is usually delivered
by a physician or other healthcare worker, or by a trained counsel-
lor, and often includes one or more follow-up phone calls or letters,
to check progress and to reinforce the advice. The counselling is
tailored to the participant’s perceived stage of change. Mermelstein
2003 gave all participants a seven-week course of group coun-
selling for smoking cessation, and then tested the addition of tai-
lored versus generic phone counselling. Lawrence 2005 compared
usual care (advice from a midwife) with stage-based manuals and
counselling (Arm B), and with the same material presented as an
interactive computer programme (Arm C). We have included each
arm as a separate comparison. Similarly, Meyer 2008 compared
assessment-only controls with stage-based tailored letters (Int 1)
and with stage-based brief advice (Int 2). Each comparison is in-
cluded in the relevant meta-analysis. One trial (Prokhorov 2008)
combined individual counselling with biofeedback (lung function
testing and measurement of exhaled carbon monoxide).
3. Interactive computer programmes (5 trials):
(Aveyard 1999; O’Neill 2000; Escoffery 2004; Lawrence 2005
[Arm C]; Prochaska 2008).
These programmes are usually made available within a fixed time
frame, and are often conducted at the participant’s own pace. They
may be supervised sessions, and generally provide oral or written
feedback. Lawrence 2005 also delivered the material as a stage-
based counselling intervention, and this is treated as a separate
comparison (see Individual Counselling above).
4. Telephone counselling (2 trials):
(Thompson 1993; Young 2008).
Assessments and counselling are conducted entirely by phone, with
advice tailored to the caller’s stage of change.
5. Training in the stages of change model for smoking cessation (3
trials):(Wang 1994; Lennox 1998; Patten 2004).
These trials use rates of abstinence as surrogate markers for the
effectiveness of the training.
(a) Physicians:Two trials tested the training of physicians to deliver smoking ces-
sation advice based on the stages of change model. Other out-
comes included patient movement through stages of change and
number of quit attempts (Lennox 1998), and reduction in daily
cigarette consumption (Wang 1994).
(b) Supporters:Patten 2004 tested stages of change skills training for lay support-
ers of smokers trying to quit. Other outcomes included measures
of supportive behaviour, acceptability of the programme and re-
ceptivity of the smoker to the supporter’s attempts to help.
6. Stage-based self-help materials (1 trial):
Pallonen 1994 provided a manual to participants at six-month
intervals, matched to their stage of change. Many of the trials also
supplied generic or tailored self-help materials to their participants
as part of the intervention programme, or as part of the control
condition.
Comparison
The control or comparison conditions for the trials included
generic self-help materials or services (12 trials), ’usual care’ (13
trials), and assessment only (12 trials). Four trials used a non-
smoking-related healthcare intervention as the control condition.
These were dietary advice (Hollis 2005), advice on diet, hyperten-
sion or stress management (O’Neill 2000), a health risk assessment
(Prochaska 2008), and advice on hypertension or hypercholestero-
laemia (Nakamura 2004). For our analyses, we have combined the
assessment only and the non-smoking-related healthcare interven-
tion groups.
Follow-up assessment
All the included studies followed up their participants for at least
six months. Nine trials followed up for a maximum of 12 months,
nine for between 13 and 18 months, and ten for two years. We
have used the longest available follow-up measurement for our
analyses.
6Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Validation of abstinence
The majority of the trials relied upon self-reported abstinence
rates. Five studies validated their outcomes by salivary cotinine
samples (Bobo 1998; McBride 1999; Lennox 2001; Aveyard 2003;
Hennrikus 2005), one by expired carbon monoxide (Nakamura
2004), and two by combining carbon monoxide with cotinine
testing (Mermelstein 2003; Chouinard 2005). Two further studies
achieved partially validated results, with Curry 1995 and Lawrence
2005 testing at intermediate but not at longest follow ups. Four
trials (Prochaska 1993; Thompson 1993; Dijkstra 1998; Pieterse
2001) used the ’bogus pipeline’ method, i.e. collecting biological
samples for validation but not testing them, and two of these cross-
checked self-report against the testimony of family or friends.
Stages of Change model
The generic five-stage transtheoretical model, with its associated
processes of change, decisional balance and temptation/self-effi-
cacy, is fully described elsewhere (Velicer 1996; Prochaska 1997;
CPRC 1998). This model has been variously applied and adapted
in the studies covered by this review. Although the stages are gen-
erally expressed as discrete steps, the process has also been de-
picted as a spiral (Prochaska 1992; Chouinard 2005), as cyclical
(switching between quitting and relapse; Nakamura 2004), or as a
contemplation ladder (Biener 1991; Patten 2004), to indicate the
likelihood of progression and relapse before achieving behavioural
change.
The concept has been reconfigured as ’perspectives on change’
(Borland 2004), representing the stages as: ’disengaged’ (precon-
templation and contemplation); ’engaged’ (preparation, with a
quit date between 15 and 30 days away); ’committed’ (preparation,
with a quit date set within the next 14 days); ’implementation’ (ac-
tion, during the first one or two weeks of quitting); ’consolidation’
(maintenance, from end of implementation to decline of urges
to smoke or concurrent nicotine replacement therapy (NRT));
’synthesis’ (maintenance or termination, less than daily urges to
smoke and no NRT). Thompson 1993 loosened the parameter
definitions to ’Not even thinking of quitting’ (precontemplation);
’thinking of quitting some time in the near future’ (contempla-
tion); ’set a quit date or made a quit attempt’ (action); ’success-
fully remained smokefree for an extended period (maintenance).
Pieterse 2001 reclassified the stages as low, moderately or highly
motivated to make a quit attempt. Stotts 2002 mapped the stages
to patterns of smoking cessation among pregnant women. Many
of the studies modified the individual stages, while preserving the
conceptual model.
Precontemplation:
The transtheoretical definition for this stage is ’Not thinking about
quitting in the next six months’.
Dijkstra 1998c and Nakamura 2004 both favoured an additional
category, ’immotives’, for those smokers not interested in quitting
or not planning to quit in the foreseeable future. Lennox 1998
subdivided the precontemplators into three groups, based on de-
cisional balance (the pros and cons of change), while Manfredi
2004 subgrouped them as never planning to quit, or planning to
reduce but not quit, or thinking of quitting but not in the next
six months. Meyer 2008 classified the precontemplators into four
groups, based on decisional balance and levels of self-efficacy.
Contemplation:The transtheoretical definition for this stage is ’thinking about
quitting within the next six months, but not in the next month’.
Lennox 2001 subdivided this group, based on positive versus
mixed or negative decisional balance.
Preparation:The transtheoretical definition of this stage is ’having made a 24-
hour quit attempt in the past year and planning to stop within the
next thirty days’.
A number of trials did not require a 24-hour quit attempt as a defin-
ing characteristic of this stage (Curry 1995; Etter 2004). Lennox
2001 subdivided this group on decisional balance. Thompson
1993 did not identify preparation as a separate stage, and de-
fined action as setting a quit date or making a quit attempt. An
earlier transtheoretical model had dropped the preparation stage
(Prochaska 1982; Prochaska 1992), but later reinstated it as an
integral part of the concept.
Risk of bias in included studies
There was considerable variation among the included trials’ at-
tempts to control for risk of bias. Assessment of the quality markers
for the risk of bias in each trial are reported in the Characteristics
of included studies tables, and are displayed in summary form in
Figure 1. A funnel plot (not shown) for all the included studies
did not suggest any significant risk of publication bias.
Randomization procedures, defined as sequence generation and
allocation concealment, were performed and reported adequately
in six trials, and included such techniques as computer-generated
tables of random numbers, minimization, and allocation by sealed
opaque envelopes. Five trials reported methods of sequence gen-
eration or allocation concealment which would be considered in-
adequate, including shuffling of questionnaires (Borland 2003),
assignment by an office assistant (Pieterse 2001), alternate order of
assignment (Escoffery 2004), and ’topping up’ recruitment arms
by extending catchment (Lawrence 2005). Meyer 2008 assigned
participants to study arm by which week they attended over a
three-week recruitment period. Frequent attenders were therefore
more likely to be allocated to the assessment only (control) arm,
or to the tailored letter arm.
The remaining trials either did not report their methods of ran-
domization, or did not describe them in sufficient detail to be as-
sessed.
Blinding of participants to study arm was reported in three trials
(Stotts 2002; Borland 2003; Borland 2004). Blinding of random-
ization staff was reported by one trial (Chouinard 2005), of inter-
7Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

viewers or counsellors by three trials (Mermelstein 2003; Manfredi
2004; Prochaska 2005), of assessors by three trials ( Manfredi
2004; Hollis 2005; Hannöver 2009), and of all study personnel
by Meyer 2008.
Sensitivity analyses excluding trials rated as inadequately random-
ized, allocated or blinded did not demonstrate any significant
change in the point estimates, although the confidence intervals
had widened.
Other events which might have introduced bias included mixing
up questionnaires between the recruitment waves (Aveyard 2003);
an intervention response insufficient to make the three- and six-
month data usable (Borland 2004); a low rate (55%) of inter-
vention delivery (Stotts 2002); disparate drop-out rates between
intervention and control groups (24% vs 8%) (Etter 2004); and
physicians choosing to deliver the intervention to some members
of the control group (Pieterse 2001), with consequent exclusion of
their data from the trial analysis. Four trials which aimed to match
self-help manuals to participants’ stage of change supplied the ap-
propriate manual plus all subsequent manuals in a single delivery,
which may have weakened the specificity of the targeted interven-
tion (Prochaska 1993; Velicer 1999; Prochaska 2001a; Prochaska
2001b). A similar limitation may apply to Curry 1995 (supplying
a composite manual of eight stage-based units) and to Lawrence
2005 (supplying the complete course of six manuals). The degree
of bias introduced in such cases would depend on the accompa-
nying instructions, and on the participants’ level of compliance.
Sensitivity analyses removing these trials made little difference to
the findings.
Figure 1
8Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 1. Risk of bias summary: review authors’ judgements about each risk of bias item for each included
study.
9Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Effects of interventions
Studies varied in the type of staged intervention that they tested,
in the intensity of the intervention, and in the comparison condi-
tions that they used. We have therefore grouped them into their
categories (described above), and then subgrouped each category
by the comparison condition. We have preferred the most rig-
orous definition of abstinence for each trial, and have taken the
longest reported follow-up period. We also analysed the trials for
point prevalence abstinence (PPA) rates where reported, at 6- or12-
month follow up, but found no important differences between the
two sets of analyses.
The most informative comparison for this review is between a
generic or non-stage-based intervention and a similar stage-based
version of comparable intensity. Very few of the included stud-
ies offered such data. For trials of self-help materials (expert sys-
tems, manuals, interactive computer programmes), two studies
(Prochaska 1993; Lennox 2001) included this comparison. The
relative risk (RR) was 0.93 (95% confidence interval (CI) 0.62
to 1.39); analysis 1.1). For trials testing counselling (individual,
with or without supplementary self-help materials), two studies
(Thompson 1993; Mermelstein 2003) contributed to the compar-
ison, returning an RR of 1.00 (95% CI 0.82 to 1.22; analysis 1.2).
These findings demonstrate neither a beneficial nor a detrimental
effect of stage-based over standard approaches.
Type of intervention:
1. Tailored, computer-generated or ’expert system’ letters:Eighteen trials tested stage-based expert systems or tailored self-
help materials against any non-stage-based control group. Velicer
1999 was not included in this analysis, since it did not have a non-
stage-based comparison group, and shared one of its experimen-
tal groups with Prochaska 2001b. We subgrouped these trials on
the comparison condition. The relative risk for stage-based versus
any standard self-help materials was 1.27 (95% CI 1.01 to 1.59;
analysis 2.1.1; PPA at 6 or 12 months: 1.07, 95% CI 0.91 to 1.25;
six trials). This estimate was influenced by the positive findings of
Borland 2004, which had a RR of 1.78 (95% CI 1.20 to 2.63),
and a weighting of 28% in the meta-analysis. A sensitivity analysis
removing this trial returned a RR of 1.07 (095% CI .79 to 1.41)
and reduced the I2 value (estimating heterogeneity) from 28% to
0%. For the ’usual care’ controls the RR was 0.94 (95% CI 0.56
to 1.57; analysis 2.1.2), and for the assessment only controls 1.35
(95% CI 1.19 to 1.52; analysis 2.1.3). Early success for the inter-
vention arm in Etter 2004, the largest trial in analysis 2.1.3, was
not sustained beyond the seven-month assessment; by 24 months
the four-week point prevalence abstinence rates in both groups
were similar (11.1% for the intervention group and 10.5% for the
controls; P = 0.6).
Incremental tailored interventions:Five of the 18 trials compared a non-staged control group with
increasing levels of staged intervention (Prochaska 1993; Curry
1995; Velicer 1999; Aveyard 2003; Borland 2003). A comparison
of the cumulative effects of adding, for example, a counselling
intervention to an expert system to stage-based manuals showed
no clear trend in favour of the additional components, with only
Curry 1995 demonstrating an incremental benefit across the in-
tervention groups (RRs increasing from 0.43 to 1.87, but con-
fidence intervals including 1 in each case [analyses not shown]).
There were no substantive differences between any arms com-
pared with control in Aveyard 2003 or in Borland 2003. Prochaska
1993 demonstrated a benefit at 18 months for the individualized
feedback intervention over standard self-help manuals (RR 2.49,
95% CI 1.18 to 5.24; analysis not shown), but no clear advantage
for stage-based manuals or for additional phone counselling. Al-
though Velicer 1999 is not included in the meta-analyses because
it lacked a non-staged control group, we conducted a separate anal-
ysis of this trial, to assess the effect of adding expert system letters
to stage-based self-help manuals. The RR of 1.33 (95% CI 0.97
to 1.82) favoured the expert system component, while increasing
the number of contacts conferred no additional benefit (analysesnot shown).2. Individual counselling or brief advice:Thirteen trials compared individual counselling (face-to-face or by
phone) with any non-staged control condition. When this group
of studies was subgrouped by comparison condition, only one
of the findings demonstrated a modest advantage for the staged
interventions. The RR for the standard self-help comparator group
(three trials) was 1.33 (95% CI 1.00 to 1.78; analysis 2.2.1), for
the ’usual care’ comparator group (seven trials) 1.19 (95% CI 0.99
to 1.42; analysis 2.2.2), and for the assessment only comparator
group (three trials) 1.28 (95% CI 0.95 to 1.73; analysis 2.2.3).Six of the 13 trials in this group were cluster-randomized, and
the analysis was redone using the generic inverse variance method.
Relative risks on this basis were 1.20 (95% CI 0.92 to 1.55) for
standard self help, 1.24 (95% CI 0.99 to 1.56) for ’usual care’,
and 1.43 (95% CI 0.94 to 2.17) for assessment only (analysis 8).
Key data for the cluster randomized trials are given in Table 1.
3. Interactive computer programmes:Five trials tested stage-based interactive computer programmes, al-
though none used standard interactive programmes as a compara-
tor. Subgrouping by comparison condition detected no conclusive
benefit of this approach versus ’usual care’ (RR 1.14, 95% CI 0.81
to 1.59; analysis 2.3.1 ), and versus assessment only (RR 1.36,
95% CI 0.78 to 2.36; analysis 2.3.2). Two of the five trials were
cluster-randomized, and the analysis was redone using the generic
inverse variance method. The corresponding RRs were 1.14 (95%
CI 0.79 to 1.63) for ’usual care’, and 1.32 (95% CI 0.76 to 2.28)
for assessment only.
4. Telephone counselling:
10Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Two trials comparing staged telephone counselling with a control
condition found no clear benefit for the staged intervention versus
standard self help (RR 1.04, 95% CI 0.59 to 1.82; analysis 2.4.1),
or versus ’usual care’ (RR 1.27, 95% CI 0.56 to 2.89; analysis2.4.2).
5. Training in the stages of change model for smoking cessation:(a) Physicians:Two trials which tested the training of physicians to deliver stage-
based smoking cessation advice against ’usual care’ found no ad-
vantage for the intervention (RR 0.99, 95% CI 0.65 to 1.50; anal-ysis 2.5.1). Lennox 1998 was cluster-randomized, and the data
were reanalysed using the generic inverse variance method. This
returned an adjusted RR of 1.33 (95% CI 0.67 to 2.63), the differ-
ence being mainly attributable to the redistribution of weighting
associated with this statistical method.
(b) Supporters:Patten 2004, testing stages of change skills training for lay sup-
porters of smokers trying to quit, detected a possible benefit of
the training (RR 1.50, 95% CI 0.27 to 8.34; analysis 2.6), but the
small numbers of participants and events (five quitters from 60
participants) meant that chance could not be ruled out.
6. Stage-based self-help materials:Pallonen 1994, testing the provision of staged self-help materials
versus assessment only, found a possible benefit of the interven-
tion (RR 1.31, 95% CI 0.55 to 3.13; analysis 2.7), but could not
exclude the likelihood of this being a chance finding.
Validated outcomes
Relative risks were similar between the studies which relied on self-
reported abstinence (RR 1.25; 95% CI 1.14 to 1.37) and those
which biochemically validated claims of abstinence (RR 1.19; 95%
CI 1.02 to 1.39; analysis 3). However, the quit rates for the vali-
dated studies were predictably lower compared with studies giving
self-reported rates. The median control quit rate in the eight vali-
dated studies, and in the four ’bogus pipeline’ trials, was four per
cent, giving a median intervention quit rate (based on relative risk)
of five per cent. The corresponding rates for the 29 self-reporting
studies were medians of seven per cent for the controls and nine
per cent for the intervention groups.
Use of pharmacotherapy
We excluded five studies which supplied or prescribed NRT, where
appropriate, as part of the intervention (Morgan 1996a; Cornuz
2002a; Pisinger 2005a; Hall 2006; Wilson 2008) .
Seven of the included studies (Mermelstein 2003; Borland 2004;
Chouinard 2005; Davies 2005; Hennrikus 2005; Young 2008;
Meysman 2010) either recommended NRT to all participants or
included a control condition (self-help or usual care) which was
likely to advise the use of pharmacotherapies where appropriate.
Four of the seven trials reported usage: Mermelstein 2003 and
Hennrikus 2005 found no difference in uptake between interven-
tion and control, while Chouinard 2005 and Meysman 2010 both
reported lower usage by controls (6/56 participants and 4/14 quit-
ters respectively) compared with intervention smokers (35/112
participants and 9/28 quitters respectively). Manfredi 2004 left
it to the discretion of each physician whether or not to prescribe
NRT, and reported that fewer than 1% of participants used it.
Pieterse 2001 advised intervention participants to use NRT where
appropriate but left it to control participants to raise it for dis-
cussion with their physician. In that trial, nicotine gum was used
by 9.4% of participants, with no significant differences in usage
between the groups. Etter 2004 reported that, although controls
received no smoking cessation advice, 24.9% of intervention par-
ticipants and 20.8% of controls (P = 0.008) reported having used
NRT by the two-year follow up.
Dose-response effects
Although we have not included Velicer 1999 in the meta-analyses
for this review, it offers evidence that a single staged intervention
can be as effective as two, three or six such contacts, and does
not support a dose-response effect. Borland 2004 found a positive
relationship between quitting and the number of tailored letters
received. Among those smoking at baseline, 6% of the recipients
of one or two letters achieved six-month sustained abstinence,
compared with 45% of those who received seven to ten letters, and
36% of those who received eleven or more letters (P < 0.001). Etter
2004 also observed a linear trend for rates of 4-week abstinence
increasing with the number of counselling letters, from two per
cent for no letter read to 32% for four or more letters read (P =
0.002). However, these observations may be instances of selection
bias, and are examined further in the Discussion section below.
Match-mismatch studies
A few smoking cessation studies have sought to test the robustness
of the transtheoretical model (TTM) by deliberately mismatching
the intervention to the participants’ stage of change.The assump-
tion underpinning this approach is that standard interventions
target people who are ready to make a quit attempt, i.e. those in
preparation or action stages, while contemplators and precontem-
plators need different kinds of support, to move them through the
stages towards action (Prochaska 1997). On this basis, precontem-
plators and contemplators would not be expected to benefit from
standard interventions.
To explore this hypothesis, Aveyard 2009a and Parsons 2009 re-
analysed the Aveyard 2003 data, to compare the efficacy of the
TTM versus standard materials in moving people from one stage
to the next. They found that the combined TTM study arms were
slightly but not significantly more likely to progress through the
stages than the control arm. However, contrary to the TTM hy-
pothesis, those in preparation were slightly more likely to make a
positive change with the TTM interventions than with the stan-
dard materials, and the likelihood of quitting in the TTM arms
compared with the control arm was higher for those in contem-
plation and precontemplation than for those in preparation, al-
though none of these finding reached statistical significance. To
account for these disparities, the authors mapped the content of
the standard materials to the processes of change described by the
TTM, and suggested that the standard manuals were “largely stage
11Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

appropriate”.
The same study group (Lawrence 2005) tested the TTM in an
intervention for smoking cessation in pregnant women, and re-
ported comparable findings. The relative benefits of the stage-
based interventions were not greater for women in precontempla-
tion or contemplation, but proved particularly effective for those
in preparation, for whom they would be considered a mismatch.
This study confirmed that the TTM intervention increased ces-
sation rates, but did not support the appropriateness of the stage-
matched materials to the predicted groups.
Quinlan 2000 (an excluded study) randomized 92 young adult
smokers to receive stage-matched manuals, stage mismatched
manuals or assessment only, and found that the mismatched group
performed better than the other two groups for every outcome.
Fifty-four per cent of the mismatched group progressed through at
least one stage, compared with 30% of the stage-matched group,
and 35% of the assessment only control group. Fourteen per cent
of the mismatched group were abstinent at one month follow up,
compared with three per cent of the matched group, and none in
the assessment-only group. Although the results of this small trial
failed to reach statistical significance, they do not endorse the prac-
tical application of the TTM to smoking cessation programmes.
Two studies by Dijkstra have also tested the plausibility of the
stage-based model. Dijkstra 1998 randomized participants to re-
ceive (i) pros-of-quitting material appropriate to ’immotives’ (i.e.
those with no interest in quitting), or (ii) self-efficacy material ap-
propriate to those preparing to quit, or (iii) both types of material,
suitable for those in precontemplation or contemplation, or (iv)
no intervention (the control group). The group that received both
types of material had significantly more sustained quitters at 14
months than the control group (OR 3.74), leading the authors to
conclude that smokers with varying readiness to quit can benefit
from a combination of information on outcomes of quitting and
of self-efficacy enhancement.
Dijkstra 2006 tested the Social Cognitive Stage Model, which is
inspired by and similar to the transtheoretical model, with forward
stage transition as the primary outcome. Participants were ran-
domized to (i) pros of quitting material (deemed appropriate for
precontemplators), or (ii) reducing the cons of quitting (for con-
templators), or self-efficacy materials (for preparers and ex-smok-
ers). The study confirmed the highest percentage of transitions
in the expected groups for precontemplators, contemplators and
ex-smokers, but not for preparers, for whom the pros and cons
materials proved a better match than the self-efficacy materials.
Overall, matched materials accounted for 44.7% of movement,
and mis-matched for 25.8% (OR 2.78, 95% CI 1.85 to 4.35).
Other trials have reported findings which are inconsistent with
the stages of change model. Curry 1995 reported that 5% of pre-
contemplators in the Phone group had achieved continuous ab-
stinence at 21 months, compared with 2% of the contemplators.
The groups in Prochaska 1993 behaved predictably, apart from
the precontemplator controls (standard manuals), who achieved a
higher quit rate than the contemplators in the same group.
Movement through stages
Movement through the stages of change, without reference to
quitting, was not a primary outcome of interest for this review.
However, we briefly consider it here for the included studies, as a
marker for the validity of the model for behaviour change (Martin
1996). The evidence from the studies in this review was incon-
clusive. Seven studies (O’Neill 2000; Lennox 2001; Stotts 2002;
Patten 2004; Chouinard 2005; Davies 2005; Prokhorov 2008)
confirmed the predicted transitions, although three of them as-
sessed forward movement only. A further five studies did not con-
firm the expected movement through the stages Thompson 1993;
Curry 1995; Aveyard 1999; Schumann 2006; Young 2008). All
five included regression to earlier stages as part of their assessments,
with all except Curry 1995 employing a mean change scoring sys-
tem. Four additional studies detected contradictory or inconsis-
tent patterns of movement through the stages (Pallonen 1994;
Dijkstra 1999; Borland 2004; Lawrence 2005).
D I S C U S S I O N
The most rigorous comparisons that we offer in this review suggest
that stage-based self-help materials (relative risk (RR) 0.93, 95%
confidence interval (CI) 0.62 to 1.39) and stage-based individual
counselling (RR 1.00, 95% CI 0.82 to 1.22) are no more nor less
effective than their generic or non-stage-based equivalents pro-
vided at a similar intensity. These findings are based on four trials
which construct direct comparisons between the two approaches,
involving 3255 participants.
We have also explored other included trials, which test stage-
based interventions against a range of control conditions. Six trials
(5947 participants) of stage-based self-help interventions, includ-
ing manuals and expert systems, compared with generic self-help
materials, demonstrated a modest benefit, with a RR of 1.27 (95%
CI 1.01 to 1.59). Twelve trials (14,446 participants) of stage-based
self-help interventions versus ’usual care’ or assessment only found
a RR of 1.32 (95% CI 1.17 to 1.48; analysis not shown). These esti-
mates are compatible with the Cochrane review of self-help inter-
ventions for smoking cessation (Lancaster 2005b), which demon-
strates a RR of 1.24 (95% CI 1.11 to 1.39) for 19 trials of self-help
materials versus minimal or no self help, and without supportive
contact. However, such comparisons are indirect, and although
they may be suggestive, their significance should not be overstated.
Three trials of stage-based individual counselling (2035 partici-
pants), compared with generic self-help, conferred a marginal ben-
efit, with a RR of 1.33 (95% CI 1.00 to 1.78). Pooling all 13
individual counselling studies, regardless of the control condition,
produced a RR of 1.24 (95% CI 1.08 to 1.42; analysis not shown),
which is somewhat lower than the RR of 1.44 (95% CI 1.25 to
1.65) for 18 trials of counselling versus any control in the Cochrane
12Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

review of individual behavioural counselling (Lancaster 2005a).
Included studies testing stage-based telephone counselling, inter-
active computer programmes or training of physicians and lay sup-
porters were too few to offer meaningful comparisons with the rel-
evant Cochrane reviews. Our findings suggest that established ces-
sation interventions, including self-help materials, both tailored
and standard, and individual counselling, work at the expected
levels of effectiveness when delivered as stage-based interventions.
Evidence for a dose-response effect is currently unclear. Two stud-
ies (Borland 2004 and Etter 2004) support the increased effective-
ness of multiple contacts, while the large study Velicer 1999 found
no differences in outcome between single and multiple contacts.
Etter 2004 cautions against a simplistic interpretation of the ’more
is better’ approach, pointing out that the association between quit-
ting and the number of counselling letters in his trial could be
an instance of selection bias rather than a dose-response effect,
since those with higher motivation to quit were more likely to re-
quest the letters. This may also be true for Borland 2004, since the
provision of the advisory letters was triggered by the participants’
progress through the perspectives on change. The Etter trial also
suffered from differential rates of attrition, with losses of 24% in
the intervention group at six months, compared with 8% of the
controls. Feedback indicated that intervention participants may
have wearied of successive mailings, leading to higher attrition and
potentially to an inverse dose-response effect.
The five studies which cumulated two or three stage-based com-
ponents of increasing intensity to the baseline control condition
did not demonstrate a clear dose-response trend. The first addi-
tional component increased the quit rates compared with controls
in all cases except for Curry 1995, but subsequent increments gen-
erally failed to establish the trend predicted by the model, and in
some cases may have precipitated higher rates of drop-outs than
the less intensive arms (Prochaska 1993; Aveyard 2003; Borland
2003). The evidence from our review lends little support for the
increased effort and resources implicit in this stepped intervention
approach.
The analyses in this review have been conducted on an intention-
to-treat (ITT) basis, wherever the data were available, i.e. includ-
ing all participants randomized in their original groups. We ex-
cluded deaths where reported, but counted drop-outs and those
lost to follow up as continuing smokers. While this approach may
be appropriate for clinic- and counsellor-based intervention trials,
and is recommended by the Russell Standard (West 2005b), its
applicability to population-based studies has been debated (Velicer
1992; Prochaska 1993; Borland 2004). For the 11 population-
based studies eligible for meta-analysis and the two telephone quit-
line studies, we conducted a sensitivity analysis to test the most
conservative assumptions about the smoking status of those with
missing data or lost to follow up. The ITT-based relative risk for
the 13 studies was 1.21 (95% CI 1.09 to 1.36). We then tested the
effect of including all randomized participants in the treatment
groups (ITT analysis) versus only those who had follow-up data
in the control groups (per protocol analysis). This has the effect of
maintaining a conservative quit rate in the treatment group, but a
more optimistic one in the control group. The analysis on this ba-
sis found little difference between the groups, with an RR of 0.88
(95% CI 0.79 to 0.98), marginally favouring the control groups.
It should be emphasised that this approach makes relatively ex-
treme assumptions about differential distribution of missing data
in treatment and control groups, which inevitably reduce the rel-
ative risk.
To further test assumptions about missing data, we repeated all
analyses on a per protocol basis, i.e. including data (where reported)
only for those participants who complete the study. Relative risks
remained similar; stage-based self-help interventions (18 trials, any
control condition) returned a per protocol RR of 1.36 (95% CI 1.23
to 1.51; analysis 7.1), compared with the ITT-based RR of 1.31
(95% CI 1.18 to 1.45). For stage-based individual counselling (13
trials, any control condition), the per protocol RR was 1.26 (95%
CI 1.10 to 1.44; analysis 7.2), compared with the ITT-based RR
of 1.24 (95% CI 1.08 to 1.42).
Although movement through the stages was not a primary out-
come of interest for our review, it is a useful test of the valid-
ity of the transtheoretical model for behaviour change. To judge
the value of the concept solely on numbers achieving abstinence
would misrepresent the process and risk underestimating its ef-
fects. Evidence from the included studies in this review was un-
clear, and depended to some degree on what measures were used
and whether regression to earlier stages was included in the calcu-
lation. Mean change scores were more sensitive to transition than
percentages measured at different points in the study process, and
took account of movement in both directions. The five studies
which used this approach found little evidence for the predictive
strength of the model, and our findings on this question remain
speculative. However, it should be emphasised that the studies in-
cluded in this review were selected for their relevance to smoking
cessation outcomes, and not to test transition between stages.
Disparities noted in the match-mismatch studies are difficult to
square with the theoretical model. Aveyard and colleagues have
speculated that standard self-help materials may be more broadly
applicable than the stages of change model assumes. They also
question the stability of the baseline staging assessments, pointing
out that in their trial (Aveyard 2003; Aveyard 2009a) 24% of the
precontemplators (i.e. with no wish to quit within the next six
months) actually made a quit attempt within three months. They
conclude from their own studies (Aveyard 2003; Lawrence 2005)
that the intensity of the intervention for those ready to try and
change may be more predictive of success than their baseline stage
of change.
The logic of the transtheoretical model is that smokers should be
assessed for their stage of change, and that interventions should
13Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
then be tailored to their stage of readiness to quit. Forward tran-
sition is the primary goal rather than smoking cessation, and mis-
matched interventions are assumed to be a waste of resources and
potentially counterproductive. The evidence from this review does
not unequivocally support this modular and linear view of the
quitting process, with trials frequently showing ’staged’ smokers
behaving unpredictably. A British Marketing Research Bureau sur-
vey in 2005 (West 2006) reported that almost half of the most
recent quit attempts among smokers and ex-smokers had involved
no previous planning. Furthermore, the odds of unplanned quit
attempts being more likely to succeed for at least six months than
planned ones were 2.6 times greater (95% CI 1.9 to 3.6) for at-
tempts made during the previous five years. While the findings
of retrospective surveys may not be wholly reliable, spontaneous
quit attempts such as these, by ’immotives’ or ’precontemplators’,
are at odds with the assumptions underpinning the staged model,
and may raise further questions about its validity and application.
Such discrepancies, together with the findings of the match-mis-
match studies and the movement through stages, may be at-
tributable to a number of factors. These include a flawed be-
havioural model, selective recall by survey participants, inaccurate
stage assessments, or underestimation of the flexibility and fit of
the standard comparators.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice• Direct comparisons between the same intervention in a
standard format or modified by stage of change, with each
intervention delivered at a similar intensity, demonstrate neither
a beneficial nor a detrimental effect of the staged approach.
However, the current evidence base is underpowered, and
precludes robust conclusions.
• Offering practical support to smokers trying to quit delivers
higher success rates than ’usual care’ or assessing their smoking
status, but the additional value of adapting the intervention to
the smoker’s stage of change is unclear.
• Expert systems, tailored self-help materials and individual
counselling, appear to be as effective in a stage-based
intervention as they are in a non-stage-based form.
• The evidence is inconclusive for other types of stage-based
intervention, including telephone counselling, interactive
computer programmes and training of physicians or lay
supporters.
• The evidence does not support the restriction of quitting
advice and encouragement only to those smokers assessed as
being in the preparation and action stages.
Implications for research• Additional trials to test the value of modifying an
intervention by stage of change are unlikely to alter the
conclusions of this review.
• Trials testing the use of the transtheoretical model in stage-
matched self-help manuals should provide only those materials
which match to the participant’s current stage of change.
A C K N O W L E D G E M E N T S
We would like to thank Paul Aveyard, Arie Dijkstra, Rob Riemsma
and Robert West for reading and commenting on drafts of this
review, and Shirley Manknell for consumer input. Thanks also to
Cam Escoffery for additional data. Lindsay Stead (Cochrane To-
bacco Addiction Group) performed literature searches, and Monaz
Mehta (Cochrane Tobacco Addiction Group) double-checked all
data extraction. Rafael Perera gave statistical support.
R E F E R E N C E S
References to studies included in this review
Aveyard 1999 {published data only}
Aveyard P, Cheng KK, Almond J, Sherratt E, Lancashire
R, Lawrence T, et al.Cluster-randomized controlled trial
of expert system based on the transtheoretical (“stages of
change”) model for smoking prevention and cessation in
schools. BMJ 1999;319(7215):948–53.
Aveyard P, Markham WA, Almond J, Lancashire E, Cheng
KK. The risk of smoking in relation to engagement with a
school-based smoking intervention. Social Science Medicine
2003;56(4):869–82.∗ Aveyard P, Sherratt E, Almond J, Lawrence T, Lancashire
R, Griffin C, et al.The change-in-stage and updated
smoking status results from a cluster-randomized trial of
smoking prevention and cessation using the transtheoretical
model among British adolescents. Preventive Medicine
2001;33:313–24.
Guo B, Aveyard P, Fielding A, Sutton S. Do the
Transtheoretical Model processes of change, decisional
balance and temptation predict stage movement? Evidence
from smoking cessation in adolescents. Addiction 2009;
14Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
104:828–38.
Guo B, Aveyard P, Fielding A, Sutton S. The factor structure
and factorial invariance for the decisional balance scale for
adolescent smoking. International Journal of Behavioral
Medicine 2009;16(2):158–63.
Aveyard 2003 {published data only}∗ Aveyard P, Griffin C, Lawrence T, Cheng KK. A controlled
trial of an expert system and self-help manual intervention
based on the stages of change versus standard self-help
materials in smoking cessation. Addiction 2003;98(3):
345–54.
Aveyard P, Massey L, Parsons A, Manaseki S, Griffin C.
The effect of Transtheoretical Model based interventions on
smoking cessation. Social Science and Medicine 2009;68(2):
397–403.
Parsons A, Aveyard P. What is transtheoretical therapy? A
response to Prochaska. Social Science and Medicine 2009;
68:407–9.
Prochaska JO. Flaws in the theory or flaws in the study:
a commentary on “The effect of Transtheoretical Model
based interventions on smoking cessation”. Social Science
and Medicine 2009;68:404–6.
Bobo 1998 {published data only}
Bobo JK, McIlvain HE, Lando HA, Walker RD, Leed
Kelly A. Effect of smoking cessation counseling on recovery
from alcoholism: findings from a randomized community
intervention trial. Addiction 1998;93:877–87.
Borland 2003 {published data only}
Borland R, Balmford J, Segan C, Livingston P, Owen
N. The effectiveness of personalized smoking cessation
strategies for callers to a Quitline service. Addiction 2003;
98(6):837–46.
Borland 2004 {published data only}∗ Borland R, Balmford J, Hunt D. The effectiveness of
personally tailored computer-generated advice letters for
smoking cessation. Addiction 2004;99:369–77.
Borland R, Hunt D, Balmford J. A randomized trial of
a program of computer-generated personalized advice
focussing on relapse prevention [P02 29]. Society for
Research on Nicotine and Tobacco 8th Annual Meeting,
Feb 20th-23rd, Savannah, USA. 2002.
Chouinard 2005 {published data only}
Chouinard MC, Robichaud-Ekstrand S. Predictive value
of the transtheoretical model to smoking cessation in
hospitalized patients with cardiovascular disease. European
Journal of Cardiovascular Prevention and Rehabilitation
2007;14:51–8.∗ Chouinard MC, Robichaud-Ekstrand S. The effectiveness
of a nursing inpatient smoking cessation program in
individuals with cardiovascular disease. Nursing Research
2005;54(4):243–54.
Curry 1995 {published data only}
Britt J, Curry SJ, McBride CM, Grothaus L, Louie D.
Implementation and acceptance of outreach telephone
counselling for smoking cessation with non-volunteer
smokers. Health Education Quarterly 1994;21:55–68.∗ Curry SJ, McBride C, Grothaus LC, Louie D, Wagner
EH. A randomized trial of self-help materials, personalized
feedback, and telephone counseling with nonvolunteer
smokers. Journal of Consulting and Clinical Psychology 1995;
63(6):1005–114.
Davies 2005 {published data only}
Davies SL, Kohler CL, Fish L, Taylor BE, Foster GE,
Annang L. Evaluation of an intervention for hospitalized
African American smokers. American Journal of Health
Behavior 2005;29(3):228–39.
Dijkstra 1998 {published data only}∗ Dijkstra A, De Vries H, Roijackers J. Long-term
effectiveness of computer-generated tailored feedback in
smoking cessation. Health Education Research 1998;13:
207–14.
Dijkstra A, De Vries H, Roijackers J, van Breukelen G.
Tailored interventions to communicate stage-matched
information to smokers in different motivational stages.
Journal of Consulting and Clinical Psychology 1998;66(3):
549–57.
Dijkstra A, De Vries H, Roijackers J, et al.Individualized
interventions in smoking cessation: a field experiment trial.
Gedrag and Gezondheid: Tijdschrift voor Psychologie and
Gezondheid 1996;24:314–22.
Dijkstra 1999 {published data only}∗ Dijkstra A, Devries H, Roijackers J. Targeting smokers
with low readiness to change with tailored and nontailored
self-help materials. Preventive Medicine 1999;28:203–11.
Escoffery 2004 {published data only}
Escoffery C, McCormick L, Bateman K. Development
and process evaluation of a web-based smoking cessation
program for college smokers: innovative tool for education.
Patient Education & Counseling 2004;53(2):217–25.
Etter 2004 {published data only}
Etter JF, Perneger TV. A comparison of cigarette smokers
recruited through the internet or by mail. International
Journal of Epidemiology 2001;30(3):521–5.∗ Etter JF, Perneger TV. Effectiveness of a computer-tailored
smoking cessation program: a randomized trial. Archives of
Internal Medicine 2001;161(21):2596–601.
Etter JF, Perneger TV. Post-intervention effect of a
computer tailored smoking cessation programme. Journal of
Epidemiology and Community Health 2004;58(10):849–51.
Hannöver 2009 {published data only}
Hannöver W, Kelbsch J, Röske K, Thyrian JR, John U,
Hapke U. Smoking cessation and relapse prevention in
women postpartum: Results from a randomized controlled
trial. In: Velicer WF, Keller S editor(s). Research on the
transtheoretical model; Where are we now, where are we going?
. Lengerich: Pabst Science Publishers, 2004:59–61.∗ Hannöver W, Thyrian JR, Röske K, Grempler J, Rumpf
H-J, John U, et al.Smoking cessation and relapse prevention
for postpartum women: results from a randomized
15Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

controlled trial at 6, 12, 18 and 24 months. Addictive
Behaviors 2009;34(1):1–8.
Röske K, Schumann A, Hannöver, Grempler J, Thyrian JR,
Rumpf H-J, et al.Postpartum smoking cessation and relapse
prevention intervention: a structural equation modeling
application to behavioral and non-behavioral outcomes of
a randomized controlled trial. Journal of Health Psychology
2008;13:556–68.
Thyrian JR, Freyer-Adam J, Hannöver W, Röske K,
Mentzel F, Kufeld C, Bischof G, et al.Population-based
smoking cessation in women post partum: adherence to
motivational interviewing in relation to client characteristics
and behavioural outcomes. Midwifery 2010;26(2):202–10.
[DOI: 10.1016/j.midw.2008.04.004]
Thyrian JR, Freyer-Adam J, Hannöver W, Röske K,
Mentzel F, Kufeld C, et al.Adherence to the principles
of Motivational Interviewing, clients’ characteristics and
behavior outcome in a smoking cessation and relapse
prevention trial in women postpartum. Addictive Behaviors
2007;32:2297–303.
Thyrian JR, Hannöver W, Grempler J, Röske K, John U,
Hapke U. An intervention to support postpartum women
to quit smoking or remain smoke-free. Journal of Midwifery
and Women’s Health 2006;51:45–50.
Thyrian JR, Hannöver W, Kelbsch J, Röske K, Hapke U,
John U. smoking cessation and relapse prevention among
women after childbirth. Gesundheitswesen 2004;66(8-9):
567.
Thyrian JR, Hannöver W, Röske K, Rumpf H-J, John
U, Hapke U. Postpartum return to smoking: identifying
different groups to tailor interventions. Addictive Behaviors
2006;31(10):1785–96.
Hennrikus 2005 {published data only}
Hennrikus DJ, Lando HA, McCarty MC, Klevan D, Holtan
N, Huebsch JAet al. The TEAM project: the effectiveness
of smoking cessation interventions with hospital patients.
Preventive Medicine 2005;40:249–58.
Hollis 2005 {published data only}
Hollis JF, Polen MR, Whitlock EP, Lichtenstein E,
Mullooly JP, Velicer WF, et al.Teen Reach: outcomes from a
randomized controlled trial of a tobacco reduction program
for teens seen in primary medical care. Pediatrics 2005;115
(4):981–9.
Lawrence 2005 {published data only}
Aveyard P, Lawrence T, Cheng KK, Griffin C, Croghan
E, Johnson C. A randomized controlled trial of smoking
cessation for pregnant women to test the effect of a
transtheoretical model-based intervention on movement in
stage and interaction with baseline stage. British Journal of
Health Psychology 2006;11(2):263–78.
Aveyard P, Lawrence T, Evans O, Cheng KK. The influence
of in-pregnancy smoking cessation programmes on partner
quitting and women’s social support mobilization: a
randomized controlled trial [ISRCTN89131885]. BMC
Public Health 2005;5:80.∗ Lawrence T, Aveyard P, Cheng KK, Griffin C, Johnson C,
Croghan E. Does stage-based smoking advice in pregnancy
result in long-term quitters? 18-month postpartum follow-
up of a randomized controlled trial. Addiction 2005;100:
107–16.
Lawrence T, Aveyard P, Evans O, Cheng KK. A cluster
randomised controlled trial of smoking cessation in
pregnant women comparing interventions based on the
transtheoretical (stages of change) model to standard care.
Tobacco Control 2003;12(2):168–77.
Lennox 1998 {published data only}
Lennox AS, Bain N, Taylor RJ, McKie L, Donnan PT,
Groves J. Stages of Change training for opportunistic
smoking intervention by the primary health care team.
Part I: randomised controlled trial of the effect of training
on patient smoking outcomes and health professional
behaviour as recalled by patients. Health Education Journal
1998;57(2):140–9.
Lennox 2001 {published data only}
Lennox AS, Osman LM, Reiter E, Robertson R, Friend J,
McCann Iet al. Cost effectiveness of computer tailored and
non-tailored smoking cessation letters in general practice:
randomised controlled trial. BMJ 2001;322(7299):1396.
Manfredi 2004 {published data only}
Manfredi C, Crittenden KS, Cho YI, Engler J, Warnecke
R. The effect of a structured smoking cessation program,
independent of exposure to existing interventions. American
Journal of Public Health 2000;90(5):751–6.∗ Manfredi C, Crittenden KS, Cho YI, Gao S. Long-term
effects (up to 18 months) of a smoking cessation program
among women smokers in public health clinics. Preventive
Medicine 2004;38:10–19.
Manfredi C, Crittenden KS, Warnecke R, Engler J, Cho
YI, Shaligram C. Evaluation of a motivational smoking
cessation intervention for women in public health clinics.
Preventive Medicine 1999;28:51–60.
McBride 1999 {published data only}
McBride CM, Scholes D, Grothaus LC, Curry SJ, Ludman
E, Albright J. Evaluation of a minimal self-help smoking
cessation intervention following cervical cancer screening.
Preventive Medicine 1999;29(2):133–8.
Mermelstein 2003 {published data only}
Mermelstein R, Hedeker D, Wong SC. Extended telephone
counseling for smoking cessation: does content matter?
. Journal of Consulting and Clinical Psychology 2003;71(3):
565–74.
Meyer 2008 {published data only}∗ Meyer C, Ulbricht S, Baumeister SE, Schumann A, Rüge
J, Bischof G, et al.Proactive interventions for smoking
cessation in general practice: a quasi-randomized trial
to examine the efficacy of computer-tailored letters and
physician delivered brief advice. Addiction 2008;103(2):
294–304.
Schorr G, Ulbricht S, Schmidt CO, Baumeister S, Rüge
J, Schumann A, et al.Does precontemplation represent
a homogeneous stage category? A latent class analysis
16Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

on German smokers. Journal of Consulting and Clinical
Psychology 2008;76(5):840–51.
Schumann A, John U, Ulbricht S, Rüge J, Bischof G,
Meyer C. Computer-generated tailored feedback letters for
smoking cessation: theoretical and empirical variability of
tailoring. International Journal of Medical informatics 2008;
77:715–22.
Schumann A, John U, Ulbricht S, Rüge J, Bischof G,
Meyer C. variability of tailoring of a smoking cessation
intervention based on the transtheoretical model. Addictive
Behaviors 2007;32:3083–7.
Meysman 2010 {published data only}
Meysman M, Boudrez H, Nackaerts K, Dieriks B, Indemans
R, Vermeire P. Smoking cessation rates after a nurse-
led inpatient smoking cessation intervention. Journal of
Smoking Cessation 2010;5(1):69–76.
Nakamura 2004 {published data only}
Nakamura M, Masui S, Oshima A, Okayama A, Ueshima
H. Effects of stage-matched repeated individual counseling
on smoking cessation: A randomized controlled trial for
the High-risk Strategy by Lifestyle Modification (HISLIM)
study. Environmental Health & Preventive Medicine 2004;9
(4):152–60.
O’Neill 2000 {published data only}
O’Neill HK, Gillispie MA, Slobin K. Stages of change and
smoking cessation: a computer-administered intervention
program for young adults. American Journal of Health
Promotion 2000;15(2):93-6, iii.
Pallonen 1994 {published data only}
Pallonen UE, Fava JL, Salonen JT, Prochaska JO. Readiness
for smoking change among middle-aged Finnish men.
Addictive Behaviors 1992;17:415–23.∗ Pallonen UE, Leskinen L, Prochaska JO, Willey CJ,
Kaariainen R, Salonen JT. A 2-year self-help smoking
cessation manual intervention among middle-aged Finnish
men: an application of the transtheoretical model.
Preventive Medicine 1994;23(4):507–14.
Patten 2004 {published data only}
Patten CA, Offord KP, Hurt RD, et al.Training Support
Persons to Help Smokers Quit: A Pilot Study. American
Journal of Preventive Medicine 2004;26(5):386–90.
Pieterse 2001 {published data only}
Pieterse ME, Seydel ER, Devries H, Mudde AN, Kok
GJ. Effectiveness of a minimal contact smoking cessation
program for Dutch general practitioners: A randomized
controlled trial. Preventive Medicine 2001;32(2):182–90.
Prochaska 1993 {published data only}
DiClemente CC, Prochaska JO, Fairhurst SK, Velicer
WF, Velasquez MM, Rossi JS. The processes of smoking
cessation: an analysis of precontemplation, contemplation,
and preparation stages of change. Journal of Consulting and
Clinical Psychology 1991;59:295–304.
Norman SB, Norman GJ, Rossi JS, Prochaska JO.
Identifying high- and low-success smoking cessation
subgroups using signal detection analysis. Addictive
Behaviors 2006;31(1):31–41.∗ Prochaska JO, Di Clemente CC, Velicer WF, Rossi JS.
Standardized, individualized, interactive, and personalized
self- help programs for smoking cessation. Health Psychology
1993;12(5):399–405.
Velicer WF, Prochaska JO, Bellis JM, DiClemente CC,
Rossi JS, Fava JL, et al.An expert system intervention for
smoking cessation. Addictive Behaviors 1993;18(3):269–90.
Prochaska 2001a {published data only}
Fava JL, Velicer WF, Prochaska JO. Applying the
transtheoretical model to a representative sample of smokers.
Addictive Behaviors 1995;20(2):189–203.∗ Prochaska JO, Velicer WF, Fava JL, Rossi JS, Tsoh JY.
Evaluating a population-based recruitment approach and
a stage-based expert system intervention for smoking
cessation. Addictive Behaviors 2001;26(4):583–602.
Sun X, Prochaska JO, Velicer WF, Laforge RG.
Transhteoretical principles and processes for quitting
smoking: a 24-month comparison of a representative
sample of quitters, relapsers, and non-quitters. Addictive
Behaviors 2007;32(12):2707–26.
Velicer WF, DiClemente CC. Understanding and
intervening with the total population of smokers. Tobacco
Control 1993;2:95–6.
Velicer WF, Fava JL, Prochaska JO, Abrams DB, Emmons
KM, Pierce JP. Distribution of smokers by stage in three
representative samples. Preventive Medicine 1995;24(4):
401–11.
Velicer WF, Prochaska JO. An expert system intervention
for smoking cessation. Patient Education and Counseling
1999;36:119–29.
Velicer WF, Redding CA, Sun X, Prochaska JO.
Demographic variables, smoking variables, and outcome
across five studies. Health Psychology 2007;26(3):278–87.
Prochaska 2001b {published data only}∗ Prochaska JO, Velicer WF, Fava JL, Ruggiero L, Laforge
RG, Rossi JS, et al.Counselor and stimulus control
enhancements of a stage-matched expert system intervention
for smokers in a managed care setting. Preventive Medicine
2001;32(1):23–32.
Prochaska JO, Velicer WF, Guadagnoli E, Rossi JS,
DiClemente CC. Patterns of change: dynamic typology
applied to smoking cessation. Multivariate Behavior Research
1991;26:83–107.
Prochaska JO, Velicer WF, Prochaska JM, Johnson JL.
Size, consistency, and stability of stage effects for smoking
cessation. Addictive Behaviors 2004;29(1):207–13.
Velicer WF, Cumming G, Fava JL, Rossi JS, Prochaska JO,
Johnson J. Theory testing using quantitative predictions
of effect size. Applied Psychology: an International Review
2008;57(4):589–608.
Velicer WF, Prochaska JO, Bellis JM, DiClemente CC,
Rossi JS, Fava JL, et al.An expert system intervention for
smoking cessation. Addictive Behaviors 1993;18:269–90.
Velicer WF, Prochaska JO, Fava JL, Laforge RG, Rossi JS.
Interactive versus noninteractive interventions and dose-
17Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

response relationships for stage-matched smoking cessation
programs in a managed care setting. Health Psychology 1999;
18:21–8.
Velicer WF, Rossi JS, Ruggiero L, Prochaska JO. Minimal
interventions appropriate for an entire population of
smokers. In: Richmond, R editor(s). Interventions for
smokers: an international perspective. Baltimore: Williams &
Wilkins, 1994:69–92.
Prochaska 2004 {published data only}
Prochaska JJ, Velicer WF, Prochaska JO, Delucchi K, Hall
SM. Comparing intervention outcomes in smokers treated
for single versus multiple behavioral risks. Health Psychology
2006;25:380–8.∗ Prochaska JO, Velicer WF, Rossi JS, Redding CA,
Greene GW, Rossi SR, et al.Multiple risk expert systems
interventions: Impact of simultaneous stage-matched expert
system interventions for smoking, high-fat diet, and sun
exposure in a population of parents. Health Psychology 2004;
23(5):503–16.
Velicer WF, Redding CA, Sun X, Prochaska JO.
Demographic variables, smoking variables, and outcome
across five studies. Health Psychology 2007;26(3):278–87.
Prochaska 2005 {published data only}
Blissmer B, Prochaska JO, Velicer WF, Redding CA, Rossi
JS, Greene GW, et al.Common factors predicting long-
term changes in multiple health behaviors. Journal of Health
Psychology 2010;15:205–14.∗ Prochaska JO, Velicer WF, Redding C, Rossi JS, Goldstein
M, DePue J, et al.Stage-based expert systems to guide
a population of primary care patients to quit smoking,
eat healthier, prevent skin cancer, and receive regular
mammograms. Preventive Medicine 2005;41:406–16.
Velicer WF, Redding CA, Sun X, Prochaska JO.
Demographic variables, smoking variables, and outcome
across five studies. Health Psychology 2007;26(3):278–87.
Prochaska 2008 {published data only}
Prochaska JO, Butterworth S, Redding CA, Burden V,
Perrin N, Leo M, et al.Initial efficacy of MI, TTM tailoring
and HRI’s with multiple behaviors for employee health
promotion. Preventive Medicine 2008;46:226–31.
Prokhorov 2008 {published data only}
Prokhorov AV, Fouladi RT, de Moor C, Warneke CL, Luca
M, Mullin-Jones M, et al.Computer-assisted, counselor-
delivered smoking cessation counseling for community
college students: Intervention approach and sample
characteristics. Journal of Child and Adolescent Substance
Abuse 2007;16:35–62.∗ Prokhorov AV, Yost T, Mullin-Jones M, de Moor C, Ford
KH, Marani S, et al.“Look At Your Health”: outcomes
associated with a computer-assisted smoking cessation
counseling intervention for community college students.
Addictive Behaviors 2008;33:757–71.
Schumann 2006 {published data only}∗ Schumann A, John U, Baumeister SE, Ulbricht S, Rumpf
H-J, Meyer C. Computer-tailored smoking cessation
intervention in z general population setting in Germany:
outcome of a randomized controlled trial. Nicotine &
Tobacco Research 2008;10(2):371–9.
Schumann A, John U, Rumpf HJ, Hapke U, Meyer C.
Changes in the ’stages of change’ as outcome measures of a
smoking cessation intervention: A randomized controlled
trial. Preventive Medicine 2006;43(2):101–6.
Schumann A, John U, Ulbricht S, Rüge J, Bischof G,
Meyer C. Computer-generated tailored feedback letters for
smoking cessation: theoretical and empirical variability of
tailoring. International Journal of Medical informatics 2008;
77:715–22.
Schumann A, John U, Ulbricht S, Rüge J, Bischof G,
Meyer C. variability of tailoring of a smoking cessation
intervention based on the transtheoretical model. Addictive
Behaviors 2007;32:3083–7.
Schumann A, Stein JA, Ullman JB, John U, Rumpf H-J,
Meyer C. Patterns and predictors of change in a smoking
intervention study: latent growth analysis of a multivariate
outcome model. Health Psychology 2008;27(3 (Suppl)):
S233–S242.
Stotts 2002 {published data only}
Mullen PD, DiClemente CC, Bartholomew LK. Theory
and context in Project PANDA: a program to help
postpartum women to stay off cigarettes. In: Bartholomew
LK, Parcel GS, Kok G, Gottlieb H editor(s). Intervention
mapping: a process for designing theory- and evidence-
based health promotion programs. Palo Alto, CA: Mayfield
Publishers, 2001:453–77.∗ Stotts AL, DiClemente CC, Dolan-Mullen P. One-to-one:
a motivational intervention for resistant pregnant smokers.
Addictive Behaviors 2002;27:275–92.
Thompson 1993 {published data only}
Kinne S, Thompson B, Wooldridge JA. Response to a
telephone smoking information line. American Journal of
Public Health 1991;5:410–3.∗ Thompson B, Kinne S, Lewis FM, Woolridge JA.
Randomized telephone smoking-intervention trial initially
directed at blue-collar workers. Monographs / National
Cancer Institute 1993;14:105–12.
Velicer 1999 {published data only}
Prochaska JO, Velicer WF, Prochaska JM, Johnson JL.
Size, consistency, and stability of stage effects for smoking
cessation. Addictive Behaviors 2004;29(1):207–13.
Velicer WF, Cumming G, Fava JL, Rossi JS, Prochaska JO,
Johnson J. Theory testing using quantitative predictions
of effect size. Applied Psychology: an International Review
2008;57(4):589–608.
Velicer WF, Fava JL, Prochaska JO, Rossi JS, Laforge
RG. Selecting an appropriate missing data procedure in
proactively recruited clinical trials. Annual Meeting of the
Society for Multivariate Experimental Psychology, Phoenix
AZ. 1997.
Velicer WF, Prochaska JO, Bellis JM, DiClemente CC,
Rossi JS, Fava JL, et al.An expert system intervention for
smoking cessation. Addictive Behaviors 1993;18:269–90.
Velicer WF, Prochaska JO, Fava JL, Laforge RG, Rossi JS.
Interactive versus noninteractive interventions and dose-
18Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

response relationships for stage-matched smoking cessation
programs in a managed care setting. Health Psychology 1999;
18:21–8.
Velicer WF, Redding CA, Sun X, Prochaska JO.
Demographic variables, smoking variables, and outcome
across five studies. Health Psychology 2007;26(3):278–87.
Velicer WF, Rossi JS, Ruggiero L, Prochaska JO. Minimal
interventions appropriate for an entire population of
smokers. In: Richmond, R editor(s). Interventions for
smokers: an international perspective. Baltimore: Williams &
Wilkins, 1994:69–92.
Wang 1994 {published data only}
Wang WD. Feasibility and effectiveness of a stages-of-
change model in cigarette smoking cessation counseling.
Journal of the Formosan Medical Association 1994;93(9):
752–7.
Young 2008 {published data only}
Young JM, Girgis S, Bruce TA, Hobbs M, Ward JE.
Acceptability and effectiveness of opportunistic referral
of smokers to telephone cessation advice from a nurse:
a randomised tiral in Australian general practice. BMC
Family Practice 2008;9:16.
References to studies excluded from this review
Abdullah 2005 {published data only}
Abdullah ASM, Mak YW, Loke AY, Lam TH. Smoking
cessation intervention in parents of young children: a
randomised controlled trial. Addiction 2005;100(11):
1731–40.
Ahluwalia 2007 {published data only}
Ahluwalia JS, Nollen N, Kaur H, James AS, Mayo MS,
Resnicow K. Pathways to health: cluster-randomized trial
to increase fruit and vegetable consumption among smokers
in public housing. Health Psychology 2007;26(2):214–21.
Andersen 2006 {published data only}
Andersen S. Adding addiction to the transtheoretical
model for smoking cessation. Addictive Behaviors 2007;32:
1099–104.
Armitage 2008 {published data only}
Armitage CJ, Arden MA. How useful are the stages of
change for targeting interventions? Randomized test of a
brief intervention. Health Psychology 2008;27:789–98.
Baker 2006 {published data only}
Baker A, Richmond R, Haile M, Lewin TJ, Carr VJ,
Taylor RL, et al.A randomized controlled trial of a smoking
cessation intervention among people with a psychotic
disorder. American Journal of Psychiatry 2006;163(11):
1934–42.
Becona 2001 {published data only}
Becona E, Vazquez FL. Effectiveness of personalized written
feedback through a mail intervention for smoking cessation:
a randomized-controlled trial in Spanish smokers. Journal
of Consulting and Clinical Psychology 2001;69(1):33–40.
Berman 1995 {published data only}
Berman BA, Gritz ER, Braxton Owens H, Nisenbaum R.
Targeting adult smokers through a multi-ethnic public
school system. Journal of Cancer Education 1995;10:
91–101.
Borrelli 2002 {published data only}
Borrelli B, McQuaid EL, Becker B, Hammond K,
Papandonatos G, Fritz G, et al.Motivating parents of kids
with asthma to quit smoking: the PAQS project. Health
Education Research 2002;17(5):659–69.
Campbell 2004 {published data only}
Campbell ANC, Fisher DS, Picciano JF, Orlando MJ,
Stephens RS, Roffman RA. Marketing effectiveness in
reaching the nontreatment-seeking marijuana smoker.
Journal of Social Work Practice in the Addictions 2004;4(1):
39–59.
Carlson 2003 {published data only}
Carlson LE, Taenzer P, Koopmans J, Casebeer A. Predictive
value of aspects of the Transtheoretical Model on smoking
cessation in a community-based, large-group cognitive
behavioral program. Addictive Behaviors 2003;28(4):
725–40.
Chan 2005 {published data only}∗ Chan SC, Lam TH, Lau C-P. The effectiveness of a
nurse-delivered smoking cessation intervention for cardiac
patients: a randomised controlled trial. Nicotine & Tobacco
Research 2005;7(4):692.
Chan SSC, Chan SC, Lam TH, Lau C-P. The effectiveness
of a stage-matched smoking cessation intervention to cardiac
patients: Preliminary results of a randomised controlled trial
[POS3-97]. Society for Research on Nicotine and Tobacco
9th Annual Meeting, February 19th-22nd, New Orleans,
LA. 2003.
Cornuz 2002 {published data only}
Cornuz J, Humair JP, Seematter L, Stoianov R, van Melle
G, Stalder Het al. Efficacy of resident training in smoking
cessation: a randomized, controlled trial of a program
based on application of behavioral theory and practice
with standardized patients.[summary for patients in Ann
Intern Med. 2002 Mar 19;136(6):I31 ]. Annals of Internal
Medicine 2002;136(6):429–37.
Humair JP, Cornuz J. Training physicians in smoking
cessation: Research and education serving public health.
Médecine & Hygiène 2003;61(2451):1809–15.
Humair J-P, Cornuz J. A new curriculum using active
learning methods and standardized patients to train
residents in smoking cessation. Journal of General Internal
Medicine 2003;18:1023–7.
Humair J-P, Cornuz J. Continuing and postgraduate
training of doctors in smoking cessation: description of an
effective programme [Formation postgraduée et continue
des médecins à la désaccoutumance au tabac: description
d’un programme efficace]. Médecine & Hygiène 2003;2451:
1809–15.
Dijkstra 1998b {published data only}
Dijkstra A, Devries H, Roijackers J. Computerized tailored
feedback to change cognitive determinants of smoking: a
Dutch field experiment. Health Education and Research
1998;13:197–206.
19Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Dijkstra 1998c {published data only}
Dijkstra A, De Vries H, Roijackers J, van Breukelen G.
Tailoring information to enhance quitting in smokers with
low motivation to quit: three basic efficacy questions.
Health Psychology 1998;17(6):513–9.
Dijkstra 2006 {published data only}
Dijkstra A, Conijn B, de Vries H. A field experiment
on stages of change for smoking cessation: the effects
of matched and mismatched information. Psychologie &
Gezonheid 2007;35:5–16.∗ Dijkstra A, Conijn B, de Vries H. A match-mismatch test
of a stage model of behaviour change in tobacco smoking.
Addiction 2006;101(7):1035–43.
Drevenhorn 2007 {published data only}
Drevenhorn E, Bengtson A, Allen, JK, Säljö R, Kjellgren K.
Counselling on lifestyle factors in hypertension care after
training on the stages of change model. European Journal of
Cardiovascular Nursing 2007;6(1):46–53.
Erol 2008 {published data only}
Erol S, Erdogan S. Application of a stage based motivational
interviewing approach to adolescent smoking cessation: the
transtheoretical model-based study. Patient Education and
Counseling 2008;72:42–8.
Ershoff 1999 {published data only}
Ershoff DH, Quinn VP, Boyd NR, Stern J, Gregory M,
Wirtschafter D. The Kaiser Permanente prenatal smoking-
cessation trial. When more isn’t better, what is enough?.
American Journal of Preventive Medicine 1999;17(3):161–8.
Etter 2005 {published data only}
Etter JF. Comparing the efficacy of two Internet-based,
computer-tailored smoking cessation programs: a
randomized trial. Journal of Medical Internet Research 2005;
7(1):e2.
Etter 2009 {published data only}
Etter J-F. Comparing computer-tailored, internet-based
smoking cessation counseling reports with generic,
untailored reports: a randomized trial. Journal of Health
Communication 2009;14(7):646–57.
Fang 2006 {published data only}
Fang CY, Ma GX, Miller SM, Tan Y, Su X, Shive S. A brief
smoking cessation intervention for Chinese and Korean
American smokers. Preventive Medicine 2006;43(4):321–4.
Fritz 2008 {published data only}
Fritz DJ, Hardin SB, Gore PA Jr, Bram D. A computerised
smoking cessation intervention for high school smokers.
Pediatric Nursing 2008;34:13–17.
Gritz 1993 {published data only}
Gritz ER, Carr CR, Rapkin D, Abemayor E, Chang LJ,
Wong WKet al. Predictors of long-term smoking cessation
in head and neck cancer patients. Cancer Epidemiology,
Biomarkers & Prevention 1993;2(3):261–70.
Hall 2006 {published data only}
Hall SM, Tsoh JY, Prochaska JJ, Eisendrath S, Rossi JS,
Redding CAet al. Treatment for cigarette smoking among
depressed mental health outpatients: A randomized clinical
trial. American Journal of Public Health 2006;96(10):
1808–14.
Haug 2009 {published data only}
Haug S, Meyer C, Schorr G, Bauer S, John U. Continuous
individual support of smoking cessation using text
messaging: a pilot experimental study. Nicotine & Tobacco
Research 2009;11(8):915–23.
Hoving 2007 {published data only}
Hoving EF. The feasibility of a smoking cessation computer
tailored expert system in Dutch general practice and
community pharmacy setting. http://arno.unimaas.nl/
show.cgi?fid=9388 2007.
Hoving EF, Mudde AN, de Vries H. Smoking and the Ø
pattern; predictors of transitions through the stages of
change. Health Education Research 2006;21(3):305–14.
Smit ES, Hoving C, de Vries H. Does a typical contemplator
exist? Three clusters of smokers in contemplation. Health
Education Research 2010;25(1):61–73.
Huang 2005 {published data only}
Huang M, Hollis J, Polen M, Lapidus J, Austin D. Stages
of smoking acquisition versus susceptibility as predictors of
smoking initiation in adolescents in primary care. Addictive
Behaviors 2005;30(6):1183–94.
Hughes 2000 {published data only}
Hughes EG, Lamont DA, Beecroff ML, Wilson DMC,
Brennan BG, Rice SC. Randomized trial of a “stage-of-
change” oriented smoking cessation intervention in infertile
and pregnant women. Fertility and Sterility 2000;74(3):
498–503.
Hughes 2005 {published data only}
Hughes JR, Keely JP, Fagerstrom KO, Callas PW. Intentions
to quit smoking change over short periods of time. Addictive
Behaviors 2005;30(4):653–62.
Hyman 2007 {published data only}
Hyman DJ, Pavlik VN, Taylor WC. Simultaneous vs
sequential counseling for multiple behaviour change.
Archives of Internal Medicine 2007;167:1152–8.
Jennings 2007 {published data only}
Jennings EG. A randomized clinical trial in a child health
care setting comparing two brief interventions to reduce
environmental tobacco smoke exposure. Dissertation
Abstracts International 2007;Part B: The Sciences and
Engineering(67):pp–B.
Johs 2003 {published data only}
Johs Artisensi JL. The effect of web-based support as
an adjunct to a self-help smoking cessation program.
Dissertation Abstracts International: Section B: The Sciences
and Engineering 2003;63(9-B):4138.
Jones 2003 {published data only}
Jones H, Edwards L, Vallis TM, Ruggiero L, Rossi SR,
Rossi JS, et al.Changes in diabetes self-care behaviors make
a difference in glycemic control: the Diabetes Stages of
Change (DiSC) Study. Diabetes Care 2003;26(3):732–7.
Jones H, Ruggiero L, Edwards L, Vallis TM, Rossi S, Rossi
JS, et al.Diabetes Stages of Change (DiSC): methodlogy
20Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

and study design. Canadian Journal of Diabetes Care 2001;
25:97–107.
Keller 2000 {published data only}
Keller S, Donnerbanzhoff N, Kaluza G, Baum E, Basler
HD. Improving physician-delivered counseling in a primary
care setting: Lessons from a failed attempt. Education for
Health 2000;13(3):387–97.
Kim 2004 {published data only}
Kim S, Nam KA, Seo M, Lee HH. Effectiveness of a
smoking cessation program for adolescents. Taehan Kanho
Hakhoe Chi 2004;34(4):646–54.
Kim 2009 {published data only}
Kim YH, Kim JS, Kim MS. Effectiveness of public health
center smoking cessation counseling program using the
transtheoretical model [Korean]. Journal of Korean Academy
of Nursing 2009;39(4):469–79.
Kohler 2008 {published data only}
Kohler CL, Schoenberger YM, Tseng TS, Ross L. Correlates
of transitions in stage of change for quitting among
adolescent smokers. Addictive Behaviors 2008;33:1615–8.
Lipkus 1999 {published data only}
Lipkus IM, Lyna PR, Rimer BK. Using tailored
interventions to enhance smoking cessation among African-
Americans at a community health center. Nicotine &
Tobacco Research 1999;1(1):77–85.
Rimer BK, Glassman B. Tailored communications for
primary care settings. Methods of Information in Medicine
1998;37:171–8.
Ma 2005 {published data only}
Ma GX, Fang C, Shive SE, Su X, Toubbeh JI, Miller S, et
al.A culturally enhanced smoking cessation study among
Chinese and Korean smokers. International Electronic
Journal of Health Education 2005;8(1):1–10.
McDonald 2003 {unpublished data only}
McDonald PW, Jessup L, Brown KS, Ahmed R, Filsinger
S. Are cessation interventions based on stage of change
really more effective? [POS4-27]. Society for Research on
Nicotine and Tobacco, 9th Annual Meeting, February 19th-
22nd, New Orleanss, LA. 2003:88.
Morgan 1996 {published data only}
Morgan GD, Noll EL, Orleans CT, Rimer BK, Amfoh K,
Bonney G. Reaching midlife and older smokers - tailored
interventions for routine medical care. Preventive Medicine
1996;25:346–54.
Osinubi 2003 {published data only}
Osinubi OY, Moline J, Rovner E, Sinha S, Perez-Lugo
M, Demissie Ket al. A pilot study of telephone-based
smoking cessation intervention in asbestos workers. Journal
of Occupational and Environmental Medicine 2003;45(5):
569–74.
Pallonen 1998 {published data only}
Pallonen UE, Velicer WF, Prochaska JO, Rossi JS, Bellis
JM, Tsoh JYet al. Computer-based smoking cessation
interventions in adolescents: Description, feasibility, and
six-month follow-up findings. Substance Use and Misuse
1998;33(4):935–65.
Pisinger 2005 {published data only}
Jørgensen T, Borch-Johnsen K, Thomsen TF, Ibsen H,
Glümer C, Pisinger C. A randomized non-pharmacological
intervention study for prevention of ischaem,ic heart disease:
baseline results Inter99 (1). Cardiovascular Prevention and
Rehabilitation 2003;10:377–86.
Pisinger C. Smoking cessation and smoking reduction in
a general population. The Inter99 study. A randomised
population-based intervention study. Nordic Journal of
Psychiatry 2006;60(1):67.
Pisinger C, Glümer C, Toft U, von Huth Smith L, Aadahl
M, Borch-Johnsen K, et al.High risk strategy in smoking
cessation is feasible on a population-based level. The
inter99 study. Preventive Medicine 2008;46:579–84.
Pisinger C, Vestbo J, Borch-Johnsen K, Jorgensen T. It is
possible to help smokers in early motivational stages to quit.
The Inter99 study. Preventive Medicine 2005;40(3):278–84.
Pisinger C, Vestbo J, Borch-Johnsen K, Jorgensen T.
Smoking cessation intervention in a large randomised
population-based study. The Inter99 study. Preventive
Medicine 2005;40(3):285–92.
Pisinger C, Vestbo J, Borch-Johnsen K, Thomsen T,
Jørgensen T. Acceptance of the smoking cessation
intervention in a large population-based study: The Inter99
study. Scandinavain Journal of Public Health 2005;33:
138–45.
Pletsch 2002 {published data only}
Pletsch PK. Reduction of primary and secondary smoke
exposure for low-income black pregnant women. Nursing
Clinics of North America 2002;37(2):315-29, viii.
Quinlan 2000 {published data only}
Quinlan KB, McCaul KD. Matched and mismatched
interventions with young adult smokers: Testing a stage
theory. Health Psychology 2000;19(2):165–71.
Reeve 2000 {published data only}
Reeve K, Calabro K, Adams-McNeill J. Tobacco cessation
intervention in a nurse practitioner managed clinic. Journal
of the American Academy of Nurse Practitioners 2000;12(5):
163–9.
Reid 2003 {published data only}
Reid R, Pipe A, Higginson L, Johnson K, D’Angelo MS,
Cooke Det al. Stepped care approach to smoking cessation
in patients hospitalized for coronary artery disease. Journal
of Cardiopulmonary Rehabilitation 2003;23(3):176–82.
Resnicow 1997 {published data only}
Resnicow K, Royce J, Vaughan R, Orlandi MA, Smith M.
Analysis of a multicomponent smoking cessation project:
What worked and why. Preventive Medicine 1997;26:
373–81.
Rissel 2000 {published data only}
Rissel C, Salmon A, Hughes AM. Evaluation of a (pilot)
stage-tailored brief smoking cessation intervention among
hospital patients presenting to a hospital pre-admission
clinic. Australian Health Review 2000;23(3):83–93.
21Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Schneider 1990 {published data only}
Schneider SJ, Walter R, O’Donnell R. Computerised
communication as a medium for behavioral smoking
cessation treatment: Controlled evaluation. Computers in
Human Behavior 1990;6:141–51.
Simon 2003 {published data only}
Simon JA, Carmody TP, Hudes ES, Snyder E, Murray J.
Intensive smoking cessation counseling versus minimal
counseling among hospitalized smokers treated with
transdermal nicotine replacement: a randomized trial.
American Journal of Medicine 2003;114(7):555–62.
Sinclair 1998 {published data only}
Sinclair H, Bond C, Lennox AS, Silcock J, Winfield A. An
evaluation of a training workshop for pharmacists based on
the Stages of Change model of smoking cessation. Health
Education Journal 1997;56:296–312.
Sinclair HK, Bond CM, Lennox AS. The long-term
learning effect of training in stage pf change for smoking
cessation: a three-year follow up of community pharmacy
staff ’s knowledge and attitudes. International Journal of
Pharmacy Practice 1999;7:1–11.∗ Sinclair HK, Bond CM, Lennox AS, Silcock J, Winfield
AJ, Donnan PT. Training pharmacists and pharmcay
assistants in the stage-of-change model of smoking cessation:
a randomised controlled trial in Scotland. Tobacco Control
1998;7:253–61.
Sinclair HK, Silcock J, Bond CM, Lennox AS, Winfield
AJ. The cost-effectiveness of intensive pharmaceutical
intervention in assisting people to stop smoking. Internation
Journal of Pharmacy Practice 1999;7:107–12.
Skewes 2007 {unpublished data only}
Skewes MC. Utep women kick butt! development,
implementation and evaluation of a web-based smoking
cessation intervention targeted to Hispanic female college
students (Texas). Dissertation Abstracts International 2007;
Vol. 67, issue 11–B.
Swanson 2003 {published data only}
Swanson NA, Burroughs CC, Long MA, Lee RW.
Controlled trial for smoking cessation in a Navy shipboard
population using nicotine patch, sustained-release
buproprion, or both. Military Medicine 2003;168(10):
830–4.
Tanaka 2006 {published data only}
Tanaka H, Yamato H, Tanaka T, Kadowaki T, Okamura T,
Nakamura M, et al.Effectiveness of a low-intensity intra-
worksite intervention on smoking cessation in Japanese
employees: a three-year intervention trial. Journal of
Occupational Health 2006;48:175–82.
Tappin 2000 {published data only}
Tappin DM, Lumsden MA, McIntyre D, Mckay C,
Gilmour WH, Webber Ret al. A pilot study to establish
a randomized trial methodology to test the efficacy of a
behavioural intervention. Health Education Research 2000;
15(4):491–502.
Tsoh 2005 {unpublished data only}
Tsoh J, Delucchi K, Benowitz N, Hall S. Cigarette reduction
predicts 12-month smoking cessation in Chinese smokers.
Society for Research on Nicotine and Tobacco, 11th Annual
Meeting, 20th-23rd March, Prague, Czech Republic. 2005.
Valanis 2001 {published data only}
Valanis B, Lichtenstein E, Mullooly JP, Labuhn K, Brody K,
Severson HH, et al.Maternal smoking cessation and relapse
prevention during health care visits. American Journal of
Preventive Medicine 2001;20(1):1–8.
Webb 2005 {published data only}
Webb MS, Simmons VN, Brandon TH. Tailored
interventions for motivating smoking cessation: using
placebo tailoring to examine the influence of expectancies
and personalization. Health Psychol 2005;24(2):179–88.
Wiggers 2005 {published data only}
Wiggers LC, Stalmeier PF, Oort FJ, Smets EM, Legemate
DA, de Haes JC. Do patients’ preferences predict smoking
cessation?. Preventive Medicine 2005;41(2):667–75.
Williams 2006 {published data only}
Williams GC, McGregor HA, Sharp D, Levesque C,
Kouides RW, Ryan RMet al. Testing a Self-Determination
Theory Intervention for Motivating Tobacco Cessation:
Supporting Autonomy and Competence in a Clinical Trial.
Health Psychology 2006;25(1):91–101.
Wilson 2008 {published data only}
Wilson JS, Fitzsimons D, Bradbury I, Elborn JS. Does
additional support by nurses enahnce the effect of a brief
smoking cessation intervention in people with moderate to
severe chronic obstructive pulmonary disease? a randomised
controlled trial. International Journal of Nursing Studies
2008;45:508–17.
Wu 2009 {published data only}
Wu D, Ma GX, Zhou K, Zhou D, Liu A, Poon AN. The
effect of a culturally tailored smoking cessation for Chinese
American smokers. Nicoitne & Tobacco Research 2009;11
(12):1448–57.
Young 2002 {published data only}
Young JM, Ward J. Can distance learning improve smoking
cessation advice in family practice? A randomized trial.
Journal of Continuing Education in the Health Professions
2002;22(2):84–93.
References to ongoing studies
Cabezas 2009 {published data only}
Cabezas C, Martin C, Granollers S, Morera C, Ballve
JL, Zarza E, et al.Effectiveness of a stepped primary care
smoking cessation intervention (ISTAPS study): design of a
cluster randomised trial. BMC Public Health 2009;9:48–59.
[: clinicaltrials ID: NCT00125905]
Prokhorov 2010 {published data only}
Prokhorov AV, Kelder SH, Shegog R, Conroy JL, Murray N,
Peters R, et al.Project ASPIRE: an interactive, multimedia
smoking prevention and cessation curriculum for culturally
22Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
diverse high school students. Substance Use & Misuse 2010;
45:983–1006.
Additional references
ACSH 2003
Ross GL, Schneider KL, Whelan EM (eds). Cigarettes: what
the warning label doesn’t tell you. 2nd Edition. New York:
American Council on Science and Health, 2003.
Aveyard 2009a
Aveyard P, Massey L, Parsons A, Manaseki S, Griffin C.
The effect of Transtheoretical Model based interventions on
smoking cessation. Social Science and Medicine 2009;68(2):
397–403.
Biener 1991
Biener L, Abrams DB. The Contemplation Ladder:
validation of a measure of readiness to consider smoking
cessation. Health Psychology 1991;10(5):360–5.
Blissmer 2002
Blissmer B, McAuley E. Testing the requirements of
stages of physical activity among adults: the comparative
effectiveness of stage-matched, mismatched, standard care,
and control interventions. Annals of Behavioral Medicine
2002;24:181–9.
Bridle 2005
Bridle C, Riemsma RP, Pattenden J, Sowden AJ, Mather L,
Watt IS, et al.Systematic review of the effectiveness of health
behavior interventions based on the transtheoretical model.
Psychology and Health 2005;20(3):283–301.
Cahill 2008
Cahill K, Stead LF, Lancaster T. Nicotine receptor partial
agonists for smoking cessation. Cochrane Database
of Systematic Reviews 2008, Issue 3. [DOI: 10.1002/
14651858.pub3]
CPRC 1998
Cancer Prevention Research Center. Transtheoretical Model.
http://www.uri.edu/research/cprc/transtheoretical.htm
(accessed 18th September 2009) 1998.
CTSU 2006
Clinical Trials service Unit and Epidemiological Studies
Unit. http://www.deathsfromsmoking.net/countries.html
(accessed 14th February 2007). Oxford: CTSU, 2006.
Froelicher 2002
Froelicher ES, Kozuki Y. Theoretical applications of
smoking cessation interventions to individuals with medical
conditions: women’s initiative for nonsmoking (WINS) -
Part III. International Journal of Nursing Studies 2002;39(1):
1–15.
Grimshaw 2006
Grimshaw G, Stanton A. Tobacco cessation intervetnions for
young people. Cochrane Database of Systematic Reviews 2006,
Issue 4. [DOI: 10.1002/14651858.CD003289.pub4]
Herzog 2008
Herzog TA. Analyzing the transtheoretical model using the
framework of Weinstein, Rothman, and Sutton (1998):
The example of smoking cessation. Health Psychology 2008;
27(5):548–56.
Herzog 2010
Herzog TA. A welcomed and overdue debate. Health
Psychology 2010;29:102–3.
Higgins 2003
Higgins JP, Thompson SG, Deeks JJ, Altman DG.
Measuring inconsistency in meta-analyses. BMJ 2003;
7414:557–60.
Hughes 2007
Hughes JR, Stead LF, Lancaster T. Antidepressants for
smoking cessation. Cochrane Database of Systematic Reviews
2007, Issue 1. [DOI: 10.1002/14651858.CD000031.pub3]
Lai 2010
Lai DTC, Cahill K, Qin Y, Tang J-L. Motivational
interviewing for smoking cessation. Cochrane Database
of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/
14651858]
Lancaster 2005a
Lancaster T, Stead LF. Individual behavioural
counselling for smoking cessation. Cochrane Database
of Systematic Reviews 2005, Issue 2. [DOI: 10.1002/
14651858.CD001292.pub2]
Lancaster 2005b
Lancaster T, Stead LF. Self-help interventions for smoking
cessation. Cochrane Database of Systematic Reviews 2005,
Issue 3. [DOI: 10.1002/14651858.CD001118.pub2]
Larabie 2005
Larabie LC. To what extent do smokers plan quit attempts?.
Tobacco Control 2005;14:425–8.
Littell 2002
Littell JH, Girvin H. Stages of change: a critique. Behavior
Modification 2002;26(2):223–73.
Martin 1996
Martin RA, Velicer WF, Fava JL. Latent transitional analysis
to the stages of change for smoking cessation. Addictive
Behaviors 1996;21:67–80.
Parsons 2009
Parsons A, Aveyard P. What is transtheoretical therapy? A
response to Prochaska. Social Science and Medicine 2009;
68:407–9.
Peto 1994
Peto R, Lopez AD, Boreham J, Thun M, Heath Jr C.
Mortality from smoking in developed countries 1950-2000.
Oxford: Oxford University Press, 1994.
Peto 2000
Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R.
Smoking, smoking cessation and lung cancer in the UK
since 1950: combination of national statistics with two
case-control studies. BMJ 2000;321:323–9.
Prochaska 1982
Prochaska JO, DiClemente CC. Transtheoretical therapy:
toward a more integrative model of change. Psychotherapy:
Theory,Research and Practice 1982;20:161–73.
23Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prochaska 1985
Prochaska JO, DiClemente CC, Velicer WF, Ginpil S,
Norcross JC. Predicting change in smoking status for self-
changers. Addictive Behaviors 1985;10(4):396–406.
Prochaska 1988
Prochaska JO, Velicer WF, DiClemente CC, Fava J.
Measuring processes of change: applications to the cessation
of smoking. Journal of Consulting and Clinical Psychology
1988;56(4):520–8.
Prochaska 1991
Prochaska JO, Goldstein MG. Process of smoking cessation:
implications for clinicians. Clinical Chest Medicine 1991;
12:727–35.
Prochaska 1992
Prochaska JO, DiClemente CC, Norcross JC. In search of
how people change: applications to addictive behaviors.
American Psychologist 1992;47(9):1102–14.
Prochaska 1997
Prochaska JO, Velicer WF. The transtheoretical model
of health behavior change. American Journal of Health
Promotion 1997;12:38–48.
Prochaska 2001
Prochaska JO, Norcross JC. Stages of change. Psychotherapy
2001;38(4):443–8.
Prochaska 2004
Prochaska JO, Velicer WF, Prochaska JM, Johnson JL.
Size, consistency, and stability of stage effects for smoking
cessation. Addictive Behaviors 2004;29:207–13.
Prochaska 2006
Prochaska JO. Further commentaries on West (2005).
Addiction 2006;101:768–78.
Project MATCH 1997
Project MATCH Research Group. Project MATCH
secondary a priori hypotheses. Addiction 1997;92:1671–98.
Project MATCH 1998
Project MATCH Research Group. Matching alcohol
treatments to client heterogeneity: Project MATCH
three year drinking outcomes. Alcoholism, Clinical and
Experimental Research 1998;22:1300–11.
Riemsma 2003
Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L,
Watt IS, et al.Systematic review of the effectiveness of stage
based interventions to promote smoking cessation. BMJ
2003;326(7400):1175–7.
Spencer 2002
Spencer L, Pagell F, Hallion ME, Adams TB. Applying the
transtheoretical model to tobacco cessation and prevention:
a review of literature. American Journal of Health Promotion
2002;17(1):7–71.
Stead 2005
Stead LF, Lancaster T. Group behavioural therapy for
smoking cessation. Cochrane Database of Systematic Reviews
2005, Issue 2. [DOI: 10.1002/14651858.CD001007.pub2]
Stead 2008
Stead LF, Perera R, Bullen C, Mant D, Lancaster T. Nicotine
replacement therapy for smoking cessation. Cochrane
Database of Systematic Reviews 2008, Issue 1. [DOI:
10.1002/14651858.CD000146.pub3]
Tones 1987
Tones K. Devising strategies for preventing drug misuse: the
role of the Health Action Model. Health Education Research
1987;2(4):305–17.
van Sluijs 2004
van Sluijs EMF, van Poppel MNM, van Mechelen W. Stage-
based lifestyle interventions in primary care - are they
effective?. American Journal of Preventive Medicine 2004;26
(4):330–43.
Velicer 1992
Velicer WF, Prochaska JO, Rossi JS, Snow MG. Assessing
outcome in smoking cessation studies. Psychological Bulletin
1992;111:23–41.
Velicer 1996
Velicer WF, Rossi JS, DiClemente CC, Prochaska JO. A
criterion measurement model for health behavior change.
Addictive Behaviors 1996;21:555–84.
Webb 2006
Webb TL, Sheeran P. Does changing behavioral intentions
engender behavior change? a meta-analysis of the
experimental evidence. Psychological Bulletin 2006;132(2):
249–68.
Weinstein 1988
Weinstein ND. The precaution adoption process. Health
Psychology 1988;7(4):355–86.
Weinstein 1998
Weinstein ND, Lyon JE, Sandman PM, Cuite CL.
Experimental evidence for stages of health behaviour
change: the precaution adoption process model applied to
home radon testing. Health Psychology 1998;17:445–53.
West 2005a
West R. Time for a change: putting the Transtheoretical
(Stages of Change) Model to rest [editorial]. Addiction
2005;100:1036–9.
West 2005b
West R, Hajek P, Stead LF, Stapleton J. Outcome criteria in
smoking cessation trials: proposal for a common standard.
Addiction 2005;100:299–303.
West 2006
West R, Sohal T. “Catastrophic” pathways to smoking
cessation: findings from national survey. BMJ 2006;332:
458–60.
WHO FCTC 2000
World Health Organization. Framework Convention on
Tobacco Control: Tobacco factsheet. 11th Conference on
Tobacco or Health. 2000.∗ Indicates the major publication for the study
24Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Aveyard 1999
Methods Setting: 52 schools, West Midlands, UK.
Study Design: Cluster-randomized controlled trial
Recruitment: Year 9 classes of students; 52 schools agreed / 89 schools approached
SoC model: Standard TTM (10 processes of change, decisional balance, self-efficacy,
temptations to smoke)
Participants Students aged 13-14; Int (4125), controls (4227). Ethnicity 86% W; gender 50% M.
Smoking prevalence: Int: 13.3% current (547), 7.6% ex, 26.5% tried, 51.8% never.
Control: 12.8% current (543), 8.5% ex, 23.2% tried, 54.8% never.
Only children smoking at baseline included in the analysis
Interventions Intervention: 1 computer session and 1 class lesson per term (=6 sessions). Computer
sessions were interactive expert system, questionnaire + visual and oral feedback. 2nd
and 3rd sessions included feedback from previous sessions; included tailored video clips
of other students.
Lesson was 1hr with their own teacher, to explore SoC and pros and cons of smoking
Control: Usual care, i.e. standard English curriculum on smoking i.e. smoking quizzes
and advice on persuading people to quit
Outcomes Prevalence of weekly and daily smoking at 1yr and 2yrs.
Biochem validation: None
2 year 30-day PPA supplied by author.
Notes Type of intervention: Interactive computer expert system
Interclass correlation of 0.008.
Funded by West Midlands Health Authorities (NHS)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer-generated block randomiza-
tion, balanced by class size
Allocation concealment? Yes Computerised and anonymised
Blinding?
All outcomes
Unclear N/A
Incomplete outcome data addressed?
All outcomes
Yes Analyses tested all models of losses to follow
up (Table 3)
25Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Aveyard 1999 (Continued)
Free of other bias? Unclear Fidelity of implementation for controls un-
clear
Aveyard 2003
Methods Setting: 65 general practices, West Midlands, UK
Study design: Randomized controlled trial
Recruitment: Inviting randomly selected smokers within practices to participate; 3 waves
of recruitment, with 3rd wave practices non-randomly selected.
SoC Model: TTM, Pro-Change programme
Participants Manual Group (683), Phone Group (685), Nurse Group (413), Controls (690). Gender
42% M; ethnicity 96% W; mean CPD 20;
Motivation to quit not required.
Interventions Int 1. Manual: TTM-based Pro-Change programme for a healthier lifestyle + 6-8 pp expert
system letter based on Q responses; Qs at 3m and 6m, to generate 2 more tailored letters.
Int 2. Phone: As 1, + phone calls at baseline, 3m and 6m, structured as reminders rather
than motivational.
Int 3. Nurse: As 1, + nurse appointment to explain and motivate.
Control: (i) Stopping smoking made easier booklet
(ii) The Quit guide to stopping smoking manual
(iii) ’Credit card’ with bulleted quit tips
(iv) ’credit card’ with pros and cons of smoking.
(i) - (iii) all included quitline phone number
Outcomes PPA and sustained abstinence at 12m.
Biochem validation: Salivary cotinine, face-to-face or postal sample. >14.2ng/ml=smok-
ing
Notes Type of intervention: Tailored self help; expert system; telephone counselling; individual
counselling.
We have compared Int 1 (TTM manuals) with Control (standard SH manuals) for our
MAs in this review.
Uptake on nurse arm very low, so abandoned for wave 3 recruitment. Analyses performed
as 3-way and 4-way comparisons.
Funded by West Midlands Health Authorities (NHS)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Minimization, balancing SoC, FTND and
SES; Qs read optically into ACCESS
database
Allocation concealment? Yes Computerised
26Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Aveyard 2003 (Continued)
Blinding?
All outcomes
Unclear Not reported
Incomplete outcome data addressed?
All outcomes
Yes Complete case and ITT analyses per-
formed. Control lost 24%, Int 1 31%, Int
2 31%, Int 3 29%
Free of other bias? No Wave 3 practices were targeted, not ran-
domly selected; some practices mixed Qs
between waves 1 and 2, leading to some
oversampling in wave 1
Bobo 1998
Methods Setting: 12 alcohol drug treatment centres, Iowa, Kansas and Nebraska, USA.
Study design: Cluster-randomized controlled trial, six matched pairs, each pair 50+ miles
apart
Recruitment: By study staff, with scripts and a/v aids, enrolled 50 per site. All smokers
eligible.
SoC Model: TTM;
Participants Int (288), Control (287); 67% M, mean age 33, 33% “ethnic minority”. Mean CPD
20.
Motivation to quit not required, but conts encouraged to think about quitting.
Interventions All completed baseline and follow-up Qs.
Int: 1 x face-to-face session in treatment centre, delivered by centre staff, + 3 follow-
up phone calls, at 8w, 12w and 16w. All sessions 10-15 mins. Follow up delivered by
counsellors trained in psychology, health education or social work.
Control: ’usual care with respect to tobacco use’.
Outcomes 7-day PPA at 1, 6 and 12m.
Validation: 70% of quitters supplied saliva cotinine; also by collateral informants for
30% of respondents
Notes Type of intervention: individual counselling, follow-up telephone support.
Supported by National Institute on Alcohol Abuse and Alcoholism
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “randomly determined by coin toss”
Allocation concealment? Unclear Not reported
27Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bobo 1998 (Continued)
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes Response rates at 1m 86%, 6m 82%, 12m
78%
Free of other bias? Unclear Not stated
Borland 2003
Methods Setting: smokers calling a quitline in Victoria, Australia
Study Design: Randomized controlled trial
Recruitment: Invited to participate after consent and baseline assessment.
SoC Model: TTM, adapted for Australian users; all received stage-based support, but int
groups were interactive and tailored
Participants Int 1: Tailored letters (523); Int 2: Callback (528); Int 3: Control (527). Gender 46%
M; mean CPD 23; No sig diffs in baseline SoC between groups. 56% had made quit
attempt in previous 12m.
Motivation to quit implicit in contact call, but not required
Interventions Control: Quit pack: 30pp Can Quit Book, using SoC; leaflets promoting callback service
and Fresh Start smoking cessation courses; ’business card’ with strategies for craving
reduction. [Callers who requested callback were excluded]
Int 1: As control, + 2-3pp computer-generated letters based on responses at baseline, 3m
and 6m. Feedback and tailored advice on cons of smoking, up to 6 processes of change
and temptations to smoke
Int 2: As Int 1, + callback, i.e. a series of CBT-based stage-based calls around quit attempts
or relative to letters; calls lasted 10-15 mins
Outcomes 9m sustained at 12m, 3m sustained at 6m, 12m PPA.
Biochem validation: None
Notes Type of intervention: self help; expert system; telephone counselling.
We have compared Int 1 (SH manuals + ES letters) with Control (SH manuals) for our
MAs in this review.
Funded by NHMRC, The Cancer Council Victoria, and Quit Victoria
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? No “by shuffling questionnaires”
Allocation concealment? Unclear “no opportunity for interviewers to influ-
ence the choice of condition”
28Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Borland 2003 (Continued)
Blinding?
All outcomes
Yes Pts only informed of their assigned condi-
tion, not of other options
Incomplete outcome data addressed?
All outcomes
Yes Complete case and ITT analyses; 23.4%
dropped out by 12m, with a trend for
higher losses in more intensive int groups
Free of other bias? Unclear Of 528 callback pts, only 358 received any
calls (129 refused, 41 not reached)
Borland 2004
Methods Setting: Telephone quitline in Victoria, Australia
Study Design: Randomized controlled trial
Recruitment: Invited adult smokers or recent quitters calling quitline and requesting S-
H materials only.
SoC Model: Modified TTM, adapted to ’perspectives on change’, i.e. six levels. ’Steps to
Stop’ programme
Participants Int 521, Control 537, mix of current and former smokers. Int smokers refusing tailored
advice (34) remained in Int group and followed up.
Baseline smokers only are included in our analyses (Int 382, Control 390).
46% M, mean age 47, mean CPD 19. 27% already quit at baseline.
Motivation to quit implicit in contact call, but not required
Interventions Int: Series of assessments followed by computerised letter, tailored to SoC, quitting
history, level of addiction, need for NRT, lapses, age, gender. Also standard S-H info
sent as needed. Schedule varied by progress. Mean 5.7 letters received
Control: Standard ’quit pack’, i.e. A5 SoC booklet, details of callback service and group-
based counselling
Outcomes Assessments at 3, 6 and 12m
Self-reported 6m sustained abstinence at 12m
PPA at 12m
Validation: None
Notes Type of intervention: Written S-H materials; tailored advice letters.
Funded by NHMRC.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “computer-generated ID numbers, with
even numbers allocated to the intervention
group”
29Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
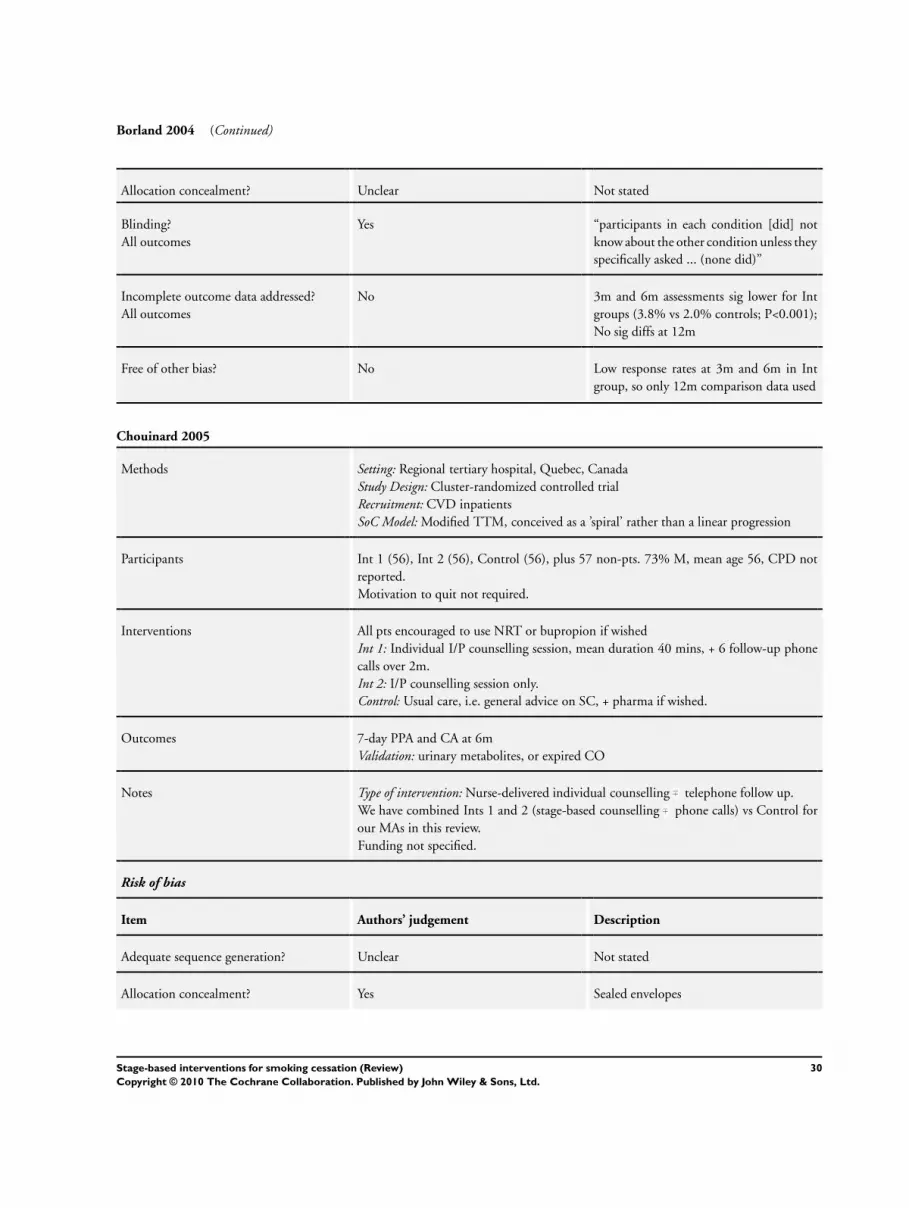
Borland 2004 (Continued)
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Yes “participants in each condition [did] not
know about the other condition unless they
specifically asked ... (none did)”
Incomplete outcome data addressed?
All outcomes
No 3m and 6m assessments sig lower for Int
groups (3.8% vs 2.0% controls; P<0.001);
No sig diffs at 12m
Free of other bias? No Low response rates at 3m and 6m in Int
group, so only 12m comparison data used
Chouinard 2005
Methods Setting: Regional tertiary hospital, Quebec, Canada
Study Design: Cluster-randomized controlled trial
Recruitment: CVD inpatients
SoC Model: Modified TTM, conceived as a ’spiral’ rather than a linear progression
Participants Int 1 (56), Int 2 (56), Control (56), plus 57 non-pts. 73% M, mean age 56, CPD not
reported.
Motivation to quit not required.
Interventions All pts encouraged to use NRT or bupropion if wished
Int 1: Individual I/P counselling session, mean duration 40 mins, + 6 follow-up phone
calls over 2m.
Int 2: I/P counselling session only.
Control: Usual care, i.e. general advice on SC, + pharma if wished.
Outcomes 7-day PPA and CA at 6m
Validation: urinary metabolites, or expired CO
Notes Type of intervention: Nurse-delivered individual counselling telephone follow up.
We have combined Ints 1 and 2 (stage-based counselling phone calls) vs Control for
our MAs in this review.
Funding not specified.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Not stated
Allocation concealment? Yes Sealed envelopes
30Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chouinard 2005 (Continued)
Blinding?
All outcomes
Yes “Individuals not familiar with the study
were in charge of the randomization pro-
cedure”
Incomplete outcome data addressed?
All outcomes
Yes At 6m, Ints 1 and 2 each lost 3, and controls
lost 1. 25% of Int 1 pts did not receive all
6 calls
Free of other bias? Unclear Not stated
Curry 1995
Methods Setting: HMO in Puget Sound, WA, USA
Study Design: randomized controlled trial
Recruitment: non-volunteer population-based sample of HMO members
SoC Model: Modified TTM; no previous quit attempt required for conts
Participants Int 1 (330), Int 2 (329), Int 3 (150), Control (328). 47% M, mean age 41, mean CPD
17.
Motivation to quit not required.
Interventions Incremental programmes:
Int 1: Manual: Breaking Away S-H programme booklet, 8 units covering all stages of
change.
Int 2: as 1, + personalized feedback: computer-generated from baseline Q data, tailored
to SoC.
Int 3: as 2, + phone calls tailored to SoC at 2w, 6w, 10w.
Control: No materials or intervention
Outcomes 24-hr quit; 7-day PPA; CA between follow-up points.
Validation: Salivary cotinine at 12m only
Notes Type of intervention: S-H, tailored feedback, phone support
Resources limited number randomized to phone intervention.
We have compared Int 2 (TTM manual + feedback) vs Control (assessment) for our
MAs in this review.
Funded by National Institute on Drug Abuse
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Not stated
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
31Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Curry 1995 (Continued)
Incomplete outcome data addressed?
All outcomes
Yes 24% dropped out by 21m; 88% provided
data at 3m and 12m, 67% at 3m, 12m and
21m
Free of other bias? Unclear S-H manual included all stages, so not truly
tailored.
Davies 2005
Methods Setting: Public indigent-care hospital, Birmingham, AL, USA
Study Design: randomized pretest post-test trial
Recruitment: low-income African-American in-patient smokers
Study: HOPE intervention
SoC Model: Transtheoretical Model of Change (TCM)
Participants Int (127), Control (121); 67% M, mean age 47, mean CPD 16. Ns not reported but
extrapolated from results section.
Motivation to quit not required
Interventions Int: (i) brief stage-matched physician advice, recommending NRT if appropriate; (ii)
1x 20-30 min tailored, stage-matched counselling session; (iii) S-H manual Pathways toFreedom (iv) post-discharge phone call at 2w; same counsellor.
Control: usual care
Outcomes PPA at 6m
Validation: None
Notes Significant losses to follow up (114/248 completed at 6m post-discharge); only used
follow-up data collected 6-9m after intervention; Int 50, Control 46.
Type of intervention: Physician advice, individual counselling, S-H, follow-up phone
support.
Funded by National Cancer Institute.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear randomization by hospital room
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Unclear Major losses to follow up (152/248), but
no significant differences between lost and
retained, other than mean age (43 vs 47)
32Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Davies 2005 (Continued)
Free of other bias? Unclear Not stated; population was difficult to re-
cruit and to retain
Dijkstra 1998
Methods Setting: Population-based, Netherlands
Study Design: randomized controlled trial
Recruitment: any cigarette smokers
SoC Model: modified TTM, with new category ’immotives’, i.e. no plans for any change
at any time
Participants 1540 Qs returned from 1733 registrants. Int 1: OC (384), Int 2: SE (385), Int 3: BO
(386), Control (385). 41% M, mean age 40, mean CPD 20.
Motivation to quit not required
Interventions Int 1. OC: computer-generated tailored letter on outcomes of smoking and quitting.
Int 2. SE: computer-generated tailored letter on self-efficacy, active skills to quit, boosting
confidence, coping skills.
Int 3. BO: computer-generated tailored letter stressing both types of info.
Control: Letter confirming no S-H info would be sent
Outcomes 7-day PPA at 10w and 14m
Validation: None; ’bogus pipeline’ used.
Notes Type of intervention: computer-generated tailored mailed S-H materials.
We have compared Ints 1+2+3 (stage-based letters) vs Control (assessment only) for our
MAs in this review.
Study funded by the Dutch Cancer Society
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “smokers were randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes 36% at 14m; no diffs between groups re-
ported. Analyses repeated with ITT [not
quite sure what the 36% is, isn’t it 61% lost
to follow up - 152/248?]
Free of other bias? Unclear Not stated
33Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Dijkstra 1999
Methods Setting: Population-based, Netherlands
Study Design: randomized controlled trial
Recruitment: nation-wide local newspaper advertising
SoC Model: modified TTM, with new category ’immotives’, i.e. no plans for any change
at any time
Participants 843, assigned to Int 1: MT (214), Int 2: ST (206), Int 3: SHG (215), Control (208).
63% F, mean age 42, mean CPD 21.5
Pts selected for low or no motivation to quit
Interventions Int 1: MT: 3 computer-generated tailored letters, at 2wks, 7wks and 12wks; 2nd and
3rd modified by 10 min phone interviews.
Int 2: ST: single computer-generated tailored letter at 2wks.
Int 3: SHG: 46pp S-H Guide
Control: CO: no materials sent
Outcomes 7-day PPA at 6m
Validation: None
Notes Type of intervention: computer-generated tailored letter(s), S-H manual.
We have compared Ints 1+ 2 (stage-based letters) vs Int 3 (SH Guide) for our MAs in
this review.
Study supported by the Dutch Cancer Society
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “smokers were randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes 11% at 6m (MT 12.6%, ST 12.2% [I get
12.6%], SHG 6.9% [6.5%], CO 12.5%).
Analyses repeated as ITT
Free of other bias? Unclear Not stated
34Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Escoffery 2004
Methods Setting: College, Atlanta, GA, USA
Study Design: randomized controlled trial
Recruitment: ads, fliers, posters, mailings; recruitment incentives
Study: Kick It! Programme
SoC Model: TTM
Participants 70 college student smokers, Int (35), Control (35). Int: 43% M, mean age 21, mean
CPD 9.
Motivation to quit not required.
Interventions Int: 4 x web-based sessions, 2-7 screens of SC information, tailored and interactive, over
2wks. Stage assessment, stage-matched messages, approaches to managing temptation,
alternatives to smoking. Feedback online and by email, + links to related websites.
Control: No intervention, assessment only
Outcomes PPA at 6m
Validation: None
Notes Type of intervention: Interactive web-based S-H
Additional data supplied by the author.
Funded by National Institute of Drug Abuse
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? No “simple randomization through drawings
and alternate assignment”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes 46% lost at post-test, 35% at 6m
Free of other bias? Unclear Not stated
Etter 2004
Methods Setting: Population-based, francophone Switzerland
Study design: Randomized controlled trial
Recruitment: 20,000 invitations to random addresses in population register.
SoC Model: TTM, (no previous quit attempt required for conts), + theory of planned
behaviour, theories of RP and tobacco dependence, AHCP recommendations
35Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
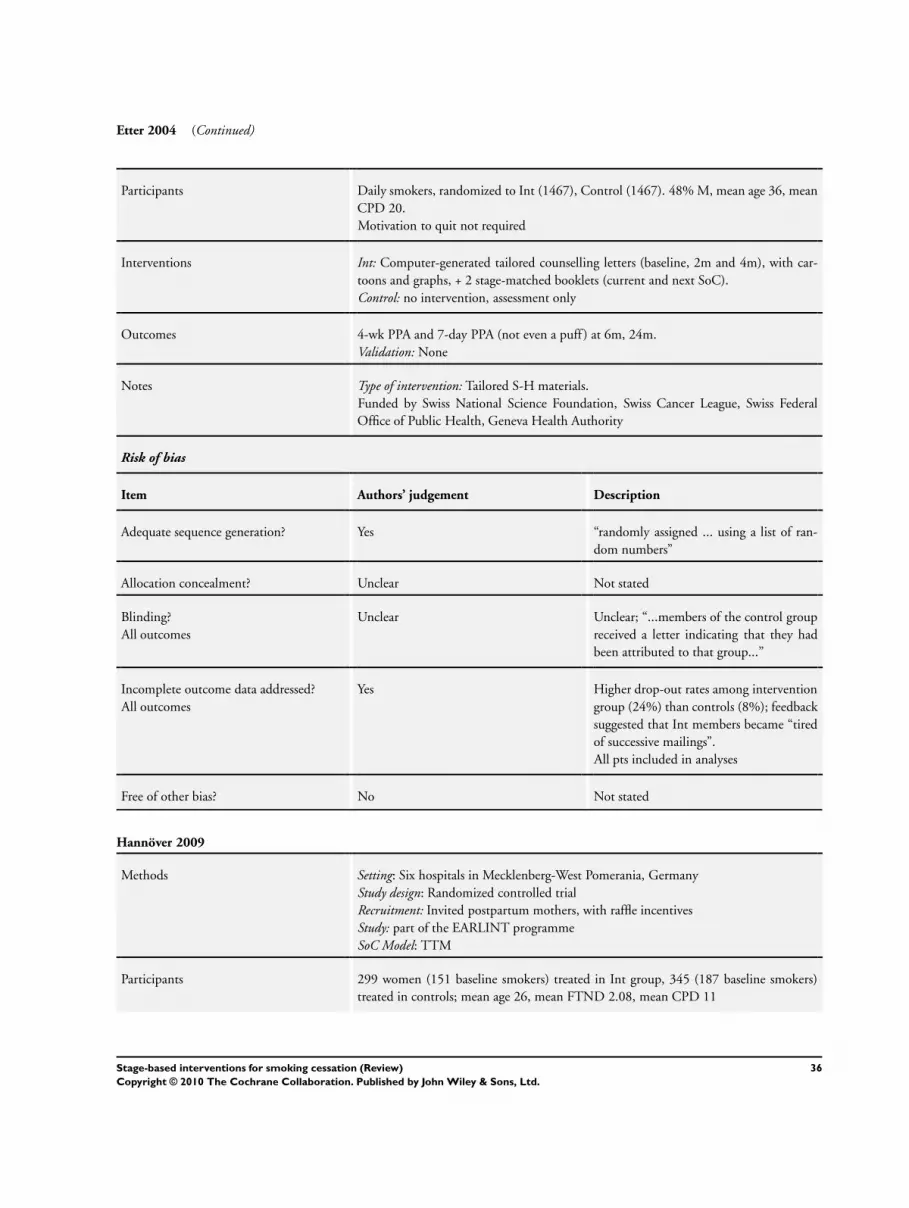
Etter 2004 (Continued)
Participants Daily smokers, randomized to Int (1467), Control (1467). 48% M, mean age 36, mean
CPD 20.
Motivation to quit not required
Interventions Int: Computer-generated tailored counselling letters (baseline, 2m and 4m), with car-
toons and graphs, + 2 stage-matched booklets (current and next SoC).
Control: no intervention, assessment only
Outcomes 4-wk PPA and 7-day PPA (not even a puff ) at 6m, 24m.
Validation: None
Notes Type of intervention: Tailored S-H materials.
Funded by Swiss National Science Foundation, Swiss Cancer League, Swiss Federal
Office of Public Health, Geneva Health Authority
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “randomly assigned ... using a list of ran-
dom numbers”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Unclear; “...members of the control group
received a letter indicating that they had
been attributed to that group...”
Incomplete outcome data addressed?
All outcomes
Yes Higher drop-out rates among intervention
group (24%) than controls (8%); feedback
suggested that Int members became “tired
of successive mailings”.
All pts included in analyses
Free of other bias? No Not stated
Hannöver 2009
Methods Setting: Six hospitals in Mecklenberg-West Pomerania, Germany
Study design: Randomized controlled trial
Recruitment: Invited postpartum mothers, with raffle incentives
Study: part of the EARLINT programme
SoC Model: TTM
Participants 299 women (151 baseline smokers) treated in Int group, 345 (187 baseline smokers)
treated in controls; mean age 26, mean FTND 2.08, mean CPD 11
36Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hannöver 2009 (Continued)
Interventions Int: Home-based MI + RP counselling session, + 2 booster phone calls at 4 and 12wks.
Covered harms, ETS, decisional balance, self-efficacy, temptations to smoke, RP strate-
gies.
Control: Usual care, + 2 x S-H brochures, targeting women smokers and partners’ ETS
Outcomes 4-wk PPA, sustained abstinence at 6, 12, 18 and 24m.
Validation: None
Notes Type of intervention: MI, follow-up phone calls, S-H booklets.
Funded by German Federal Ministry of Education and Research, the Social Ministry
of the Federal State of Mecklenburg-West Pomerania, and the Krupp von Bohlen and
Halbach Foundation
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “allocating women... alternating in the or-
der on the screening forms. Whether the al-
location sequence would begin with treat-
ment or control condition was decided ad
hoc”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Yes “impossible”, but assessors “were blind to
the women’s group membership”
Incomplete outcome data addressed?
All outcomes
Yes 12% at 6m, 18% at 12m, 24% at 18m,
25% at 24m
Free of other bias? Unclear Not stated
Hennrikus 2005
Methods Setting: Four hospitals, MN, USA
Study design: Randomized controlled trial
Recruitment: Newly admitted eligible patients invited by research staff
Study: the TEAM [Teachable Moment] Project
SoC Model: TTM
Participants Inpatients, smoked 1+ cigs in wk before admission, assigned to Int 1: Advice (703), Int
2; Advice + Counselling (696) or Control: Usual care (696). 47% M, mean age 47, 78%
W, mean CPD not stated.
Motivation to quit not required
Interventions Control: Usual care: 2 x SC manuals + directory of local SC services
Int 1: A: As Control, + brief (60-sec) advice from nurse or physician, and post-discharge
37Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hennrikus 2005 (Continued)
letter + pamphlets confirming SC benefits.
Int 2: A+C: As 1, + longer bedside MI and RP counselling, post-discharge letter, + 3-6
post-discharge phone calls over 6m.
NRT/bupropion encouraged but not supplied.
Outcomes 7-day PPA at 12m
Validation: saliva cotinine at 12m
Notes Type of intervention: MI counselling, brief advice, S-H materials.
We have compared Int 2 (stage-based counselling + phone calls) vs Control (UC SH
materials) + Int 1 (brief advice + UC) for our MAs in this review.
Funded by National Institutes of Health
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “the next available group assignment on a
list on which the three conditions were ran-
domly ordered within blocks of 30 assign-
ments”
Allocation concealment? Yes As above
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes Losses at 12m: UC 21%, A 23%, A+C
28%; losses not significantly related to
study condition
Free of other bias? Unclear Not stated
Hollis 2005
Methods Setting: Seven HMO medical centres in OR and WA, USA
Study design: Randomized controlled trial
Recruitment: Invited during routine visits
Study: the Teen Reach Study
SoC Model: Pathways to Change (included TTM)
Participants Teenagers (14-17), smokers and non-smokers, randomized to Int (1254) or Control
(1270). 41% M, 78% W, smoking prevalence 22.4% in both groups.
Baseline smokers or exsmokers: Int: 281, Control 284 (from SoC in Table 1)
Interventions Int: (i) Written prompt to clinician to give 30-60s message against smoking, and advice
to consult health counsellor (ii) 10-12 min computer session, to assess SoC and give
tailored feedback.
(iii) 3-5 min MI counselling. Also tailored S-H material + quit kits.
38Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hollis 2005 (Continued)
2 booster sessions over 11m, face-to-face or by phone.
Control: 3-5 mins dietary advice (5-a-day fruit and veg).
Outcomes 30-day no-smoking status at 1 and 2yr follow up.
Validation: None
Notes Type of intervention: Expert system, tailored S-H materials, MI counselling, brief advice,
quit kits.
Only baseline smokers and exsmokers (448) used for this review. Denominators taken
from Grimshaw 2006.
Funded by National Cancer Institute
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “blocked over time and stratified accord-
ing to medical center and 30-day cigarette
smoking status”
Allocation concealment? Yes Assignment printed on index cards in
sealed envelopes
Blinding?
All outcomes
Yes Assessor blinded
Incomplete outcome data addressed?
All outcomes
Yes Six types of analyses to model missing data.
Free of other bias? Unclear Not stated
Lawrence 2005
Methods Setting: 100 general practices in W Midlands, UK
Study design: Cluster-randomized controlled trial
Recruitment: by midwives in routine antenatal appointments
SoC Model: TTM, Pro-Change system
Participants 918 pregnant smokers, allocated to Arm A (control: 289), Arm B (305) or Arm C (324)
. Mean age 26, 89% W, CPD 70% 5-20.
Motivation to quit not required
Interventions Control: Arm A: standard care, i.e. advice + leaflet Thinking about StoppingInt 1: Arm B: 6 x 30pp stage-based manuals (1 per stage + RP) Pro-Change programmefor a healthy pregnancy. Assessed and guided (15 mins) at <20wks, 23-25 wks, 28-30wks,
by midwife
Int 2: Arm C: As B, + computer session at each assessment, with audio and on-screen
feedback on SoC, progress, decisional balance, temptations, processes of change. Feed-
39Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lawrence 2005 (Continued)
back print-out supplied after each visit
Outcomes 24hr PPA and sustained abstinence (10 wks+) at 28-30 wks, 10 days post-natal and
18m.
Validation: Urinary cotinine≤1.5µg/l at 10-day post-natal only
Notes Type of interventions: S-H materials, nurse counselling, expert system.
We have compared (a) Int 1 (stage-based counselling) and (b) Int 2 (interactive computer)
vs Control (advice/SH Guide) for our MAs in this review.
Funded by the West Midlands Regional Levies Board
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “computerised minimisation programme”
allocating practices, minimising by
Townsend score, urban/rural, birth rate
Allocation concealment? No 17 top-up practices added to Arm A af-
ter 9m slow recruitment, + 12 midwives to
Arm B
Blinding?
All outcomes
Unclear Midwives aware of allocation
Incomplete outcome data addressed?
All outcomes
Yes Higher losses to follow up in SArm A (36%)
than B (28%) or C (23%) at 10 days p/n.
At 18m, 41% lost from A, 43% from B and
47% from C
Free of other bias? Unclear Not stated
Lennox 1998
Methods Setting: 16 general practices in Aberdeen, UK
Study design: Cluster-randomized controlled trial
Recruitment: invited by post, with 2 reminders
SoC Model: TTM
Participants 2588 smokers, 1381 in 8 Int practices and 1207 in 8 control practices. ”No significant
difference ... in age, sex, addiction score,or readiness to change.
Motivation to quit not required
Interventions Int: All or most GPs and all practice nurses and health visitors workshop-trained to
deliver stage-based SC advice, MI-based techniques
Control: no special training
40Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lennox 1998 (Continued)
Outcomes 24hr PPA at 8 and 14m; CA from 8 to 14m
Validation: none used
Notes Type of intervention: Practitioner training in SC
Funded by Chief Scientist Office, Scottish Office Department of Health
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “pair-matched by list size, staff numbers
and social deprivation and randomly and
blindly allocated”
+ computer-generated random sample of
1 in 6 patients using Community Health
Index number, done centrally by Grampian
Health Board
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear “blindly allocated to control or interven-
tion”
Incomplete outcome data addressed?
All outcomes
Yes Losses similar across groups: 8m: Int 32%,
Control 28%; 14m: Int 35%, Control
34%. Analyses per protocol
Free of other bias? Unclear Not stated
Lennox 2001
Methods Setting: 6 general practices in Aberdeen, UK
Study design: Randomized controlled trial
Recruitment: invited by post, with 2 reminders
SoC Model: modified TTM, with preconts subdivided into 3 groups, conts into 2 groups,
preps into 2 groups
Participants 2553 smokers, randomized to Int 1 (870), Int 2 (869) or control (871). No demographic
info reported, but % of heavy smokers significantly higher in Int 1 (tailored letter) group
than in Int 2 (standard letter) group.
Motivation to quit not required.
Interventions Int 1: TL: computer-generated letter, tailored for SoC, age and sex.
Int 2: SL: computer-generated standard letter
Control: NL: letter of thanks and promise to send SC material at study end
Outcomes 7-day PPA at 6m
Validation: salivary cotinine
41Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lennox 2001 (Continued)
Notes Type of intervention: tailored letter, S-H materials
Analysis did not control for general practice.
We have compared Int 1 (stage-based letter) vs Int 2 (standard letter) for our MAs in
this review.
Funded by Chief Scientist Office, Scottish Executive Health Department, and Engineer-
ing and Physical Sciences Research Council
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “computer generated random numbers”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes Withdrawals at 6m were 13 (TL), 23 (SL)
, 21 (C), excluded from analyses; dropouts
included as continuing smokers (200; 213;
145)
Free of other bias? Unclear Not stated
Manfredi 2004
Methods Setting: 12 clinics, pre-natal, family planning and paediatric, Ill, USA
Study design: Cluster-randomized controlled trial
Recruitment: by invitation at clinic
Study: The ’IT’S TIME’ Programme
SoC Model: modified TTM, i.e. 6 ’stages of readiness’
Participants 1063 women smokers allocated to Int (516), Control (547); mean age 29, mean CPD
11; more Afro-Americans in Int than control (86% vs 70%).
Motivation to quit not required.
Interventions Int: At clinic: video, posters, brief advice, S-H booklet, agreement form to set quit date.
After clinic: reminder letter from provider, 15min MI phone call if wished.
Control: Measurement only.
Outcomes PPA at 2, 6, 12 and 18m.
Validation: None
Notes Type of intervention: Videos, posters, MI, brief advice, S-H materials, NRT if wished
(<1%).
Denominators inconsistent between reports.
Funded by National Cancer Institute and Centers for Disease Control
42Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Manfredi 2004 (Continued)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear clinics “randomly assigned within pairs
to intervention and control conditions”,
matched on clinic type, location, ethnic
mix
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Yes assessed by non-clinic staff; interviews con-
ducted by market researchers
Incomplete outcome data addressed?
All outcomes
Yes Losses at 6m 24% (I), 14% (C); at 12m
43% (I), 34% (C); at 18m 56% (I), 48%
(C); Prenatal smokers under-represented,
and well-child smoking mothers over-rep-
resented
Free of other bias? Unclear Not stated
McBride 1999
Methods Setting: HMO in Puget Sound, WA, USA
Study design: Randomized controlled trial
Recruitment: 15% sample of all cervical screening clinic results; all class 3 & 4 + random
sample of normal and class 2 invited.
SoC Model: TTM
Participants 580 women smokers, allocated to Int (288) or Control (292). Mean age 36, 84% W,
mean CPD 13.
Motivation to quit not required.
Interventions Int: SC kit, i.e. personalised computer-generated cover letter, S-H guide Clearing the
Air, cervical cancer info card, tea bags, bath salts. MI counselling phone calls at 2wks,
6wks, 10wks.
Control: Usual care
Outcomes PPA at 6 and 15m
Validation: saliva cotinine at 15m
Notes Type of intervention: S-H, telephone counselling
Funded by National Cancer Insititute, and National Heart, Lung and Blood Institute
Risk of bias
Item Authors’ judgement Description
43Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

McBride 1999 (Continued)
Adequate sequence generation? Unclear “stratified on Pap test ... and randomized
to one of two groups”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Unclear 12% lost at 6m, 19% at 15m.
Free of other bias? Unclear Not stated
Mermelstein 2003
Methods Setting: USA
Study design: Cluster-randomized controlled trial
Recruitment: paid ads, media coverage, fliers, referrals
SoC Model: TTM
Participants 771 smokers completing group SC programme, allocated to Int (381) or control (375).
34% M, mean age 43, 63% W, mean CPD 22.
Motivation to quit not required
Interventions All pts completed 7wk group SC programme. Then 6 x 15-min counsellor calls over
10wks.
Int: Enhanced: If still smoking at end of group programme, given a video, Yes you can.If relapsed, given a video, It’s Time. Calls tailored to pt’s smoking status, following MI
principles. Mood management skills,self-efficacy, S-H manual.
Control: Basic: 5-20 mins per call. Generic encouragement, no specific guidance, “sup-
portive but nonspecific”
Outcomes 7-day PPA at 3, 6, 9, 12 and 15m
Validation: CO≤8ppm or cotinine <10ng/ml
Notes Type of intervention: telephone counselling, S-H manuals, videos.
Funded by National Cancer Institute, and National Heart, Lung and Blood Institute
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “Groups were randomly assigned to condi-
tion”
Allocation concealment? Unclear Not stated
44Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Mermelstein 2003 (Continued)
Blinding?
All outcomes
Yes “Counselors were kept blind to condition
until the last group meeting”
Incomplete outcome data addressed?
All outcomes
Yes 4% lost to follow up; “Attrition was min-
imal during the follow-up, and there were
no
differences in attrition by condition.”
Free of other bias? Unclear Not stated
Meyer 2008
Methods Setting: 34 family practices in Vorpommern, Germany
Study design: Randomized controlled trial
Recruitment: all smokers invited by practice during routine visits
Study: part of the Pro GP project
SoC Model: modified TTM
Participants 1499 pts, randomized by week of attendance to Control (609), Int 1(488) or Int 2 (402)
; 52% M, mean age 34, mean CPD 16.
Motivation to quit not required.
Interventions Int 1: Letters: 3 computer-generated letters, tailored to SoC, scores on decisional balance,
self-efficacy, processes of change. Letters went at 1 wk, 3m and 6m from baseline visit.
Pts also given relevant S-H manuals
Int 2: Brief advice (10 mins), tailored to SoC, plus same manuals as Int 1.
Control: Assessment only, no intervention
Outcomes 24hr and 7-day PPA at 6, 12, 18 and 24 m.
6m PA at 6, 12, 18 and 24m.
18m PA at 24m.
Validation: None
Notes Type of intervention: Expert system, brief advice, S-H manuals.
We have compared (a) Int 1 (ES) and (b) Int 2 (brief counselling) vs Control in our MAs
for this review.
Funded by German Ministry of Research and Education, the Social Ministry of Meck-
lenburg-Vorpommern, and the German Research Foundation
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? No (i) “44 of 149 practices were selected ran-
domly”
(ii) All pts in 1st week allocated to assess-
ment only, 2nd week letters, 3rd week brief
advice
45Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Meyer 2008 (Continued)
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Yes Practice team, practitioner and follow-up
interviewers all blinded
Incomplete outcome data addressed?
All outcomes
Yes 8.8% lost at 6m, 3.7% at 24m.
Free of other bias? No “patients attending the practice frequently
... had a lower probability of inclusion in
the later study groups”
Meysman 2010
Methods Setting: Surgical wards in 4 Flemish hospitals
Study design: Randomized controlled trial
Recruitment: inpatient smokers
SoC Model: modified TTM
Participants 358 adult smokers admitted for surgery; randomized to experimental (178) or control
(180) groups. 63% M, mean age 43.2, 39% smoked >20 CPD, 61% 10-20 CPD.
Motivation to quit not required.
Interventions Int: Brief nurse-led counselling session; SoC assessed, and appropriate advice given, i.e.
precontemplators got risks of smoking and health gains after cessation, contemplators got
barriers and pitfalls to quitting, + raising self-efficacy, and preparers were either referred
to a SC counsellor of agreed a SC plan with the nurse.
Control: a standard booklet on smoking cessation.
Outcomes Self-reported continuous abstinence on discharge and at 6m post-discharge.
Validation: None
Notes Type of intervention: Brief counselling from a nurse.
Funded by a grant from Pfizer.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “a web-base stage of change calculation was
done and patients were randomised to two
treatment groups”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
46Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Meysman 2010 (Continued)
Incomplete outcome data addressed?
All outcomes
Unclear Losses at 6m not reported
Nakamura 2004
Methods Setting: 72 sites (26 communities and 46 worksites), Osaka, Japan
Study design: Multisite randomized controlled trial
Recruitment: 20 subjects with two risk factors from each site by health care providers,
Study: HISLIM Study
SoC Model: modified TTM: includes immotives
Participants 977 smokers (from 1386 pts); 332 in smoking/hypertension (SHT) group, 645 in smok-
ing/hypercholesterolaemia (SHC) group. SHT group allocated Int: 173, Control 159;
SHC allocated to Int 327, Control 318. 98% M, mean age 44, mean CPD 25.
Motivation to quit not required.
Interventions Int: 1 x 40-min individual counselling session + 4 x 20-30 min follow-up sessions at 1,
2, 4 and 6m. If quit date set, 1 extra phone session or letter. S-H guide. Counsellors were
nurses, physicians, nutritionists, medical technologists.
Control: Interventions for hypertension or hypercholesterolaemia
Outcomes PPA at 6m, CA at 2 and 6m, and at 1, 2, 4 and 6m.
Validation: CO≤8ppm
Notes Type of intervention: Physician advice, S-H materials.
Funded by Japanese Ministry of Health and Welfare
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “stratified by study site and randomly as-
signed”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes Losses at 6m 4.8% (I) and 6.3% (C).
Free of other bias? Unclear Not stated
47Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

O’Neill 2000
Methods Setting: North Dakota State University, ND, USA
Study design: Randomized controlled trial
Recruitment: invitation to all lower-level psychology undergraduates
SoC Model: TTM
Participants 65 undergraduate daily smokers, allocated to int (31), Control (34). 37% M, mean age
19, 48% smoked 10-20 CPD.
Motivation to quit not required.
Interventions Int: 4 x computer sessions over 6wks, adapted from Smoke Mall programme. 6 x modules
tailored to SoC.
Control: 3 x computer modules related to other health behaviours, i.e. diet, hypertension,
stress management
Outcomes Primary outcome was movement through SoC, not cessation.
PPA and CA at 7m
Validation: None
Notes Type of intervention: computerized experts system.
Funding not reported.
Possible conflict of interest: the intervention being tested was developed by one of the
authors
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “randomly assigned to a condition”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes 6% lost at 3m, 14% at 7m
Free of other bias? Unclear Not stated
Pallonen 1994
Methods Setting: Eastern Finland
Study design: Randomized controlled trial within longitudinal CV risk factor study
Recruitment: Invited as part of ongoing surveillance study
SoC Model: TTM
Participants 482 male moderate smokers (10+ CPD) assigned 2:1 to intervention or control. Prepar-
ers in intervention group were offered SC course (62 accepted). Precontemplators, con-
templators and preparers refusing SC (N=263) received stage-matched manual. Control
48Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
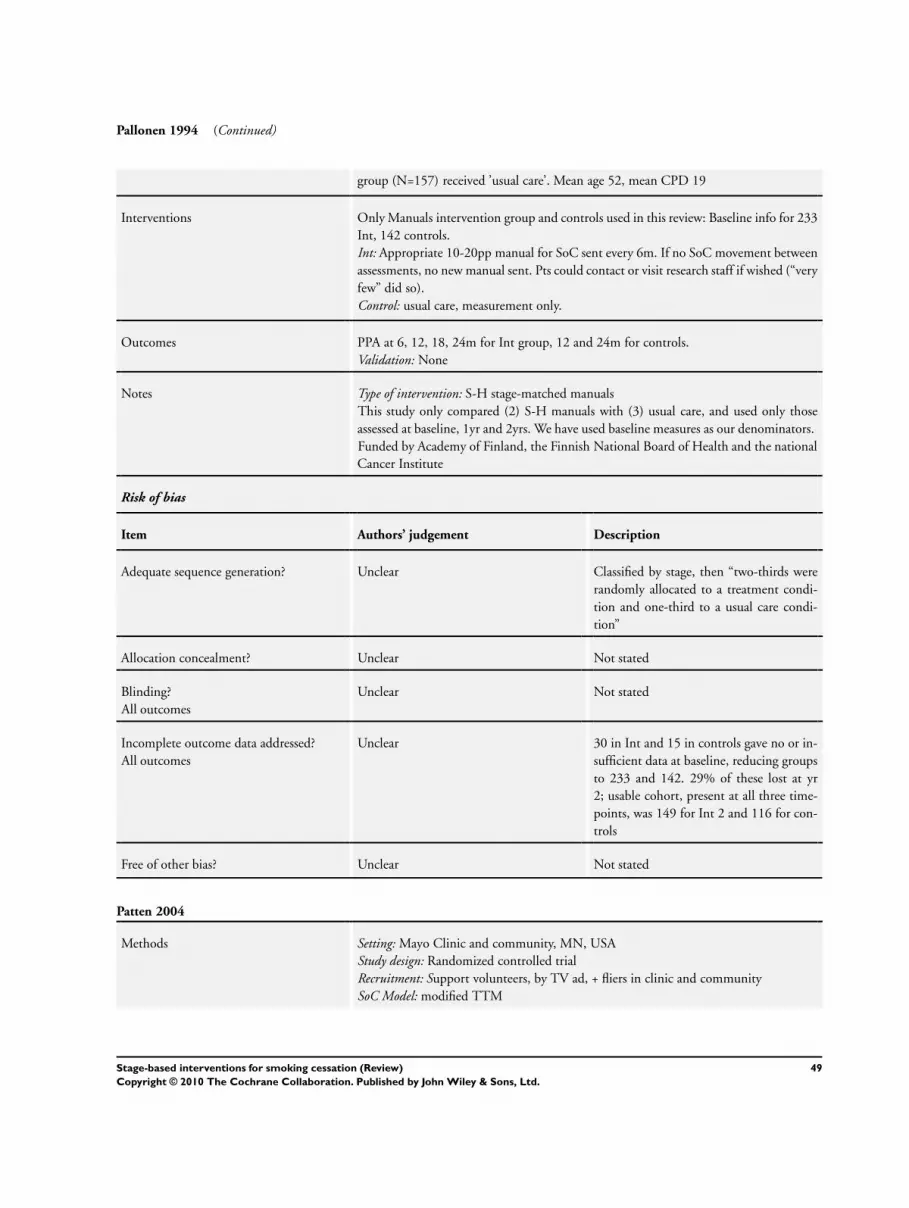
Pallonen 1994 (Continued)
group (N=157) received ’usual care’. Mean age 52, mean CPD 19
Interventions Only Manuals intervention group and controls used in this review: Baseline info for 233
Int, 142 controls.
Int: Appropriate 10-20pp manual for SoC sent every 6m. If no SoC movement between
assessments, no new manual sent. Pts could contact or visit research staff if wished (“very
few” did so).
Control: usual care, measurement only.
Outcomes PPA at 6, 12, 18, 24m for Int group, 12 and 24m for controls.
Validation: None
Notes Type of intervention: S-H stage-matched manuals
This study only compared (2) S-H manuals with (3) usual care, and used only those
assessed at baseline, 1yr and 2yrs. We have used baseline measures as our denominators.
Funded by Academy of Finland, the Finnish National Board of Health and the national
Cancer Institute
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Classified by stage, then “two-thirds were
randomly allocated to a treatment condi-
tion and one-third to a usual care condi-
tion”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Unclear 30 in Int and 15 in controls gave no or in-
sufficient data at baseline, reducing groups
to 233 and 142. 29% of these lost at yr
2; usable cohort, present at all three time-
points, was 149 for Int 2 and 116 for con-
trols
Free of other bias? Unclear Not stated
Patten 2004
Methods Setting: Mayo Clinic and community, MN, USA
Study design: Randomized controlled trial
Recruitment: Support volunteers, by TV ad, + fliers in clinic and community
SoC Model: modified TTM
49Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Patten 2004 (Continued)
Participants 60 volunteers willing to help a smoker to quit. Mean age 47, 100% W, 50% married/
living with smoking spouse/partner
Interventions Int: (i) S-H manual Because you care: information for those wanting to help someone stopsmoking. Stressed MI techniques, tailoring to SoC; (ii) 5 x weekly 90 min group sessions,
average 4 people, to support volunteers.
Control: One-page leaflet of generic support strategies
Outcomes 7-day PPA at 6m
Validation: None
Notes Type of intervention: S-H materials + group support sessions (training supporters, not
smokers).
Funded by Mayo Clinic Cancer Center and National Cancer Institute
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “people were randomized”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Yes “Study assistants who were not involved in
the intervention conducted all follow-up
assessments”
Incomplete outcome data addressed?
All outcomes
Yes 10% lost in each group at 6m
Free of other bias? Unclear Not stated
Pieterse 2001
Methods Setting: 18 general practices, Netherlands
Study design: Randomized controlled trial
Recruitment: poster in waiting room, proactive invitations by practice assistants
SoC Model: modified TTM, i.e. low, moderate or high motivation to quit
Participants 530 smokers, allocated to Int (269) and Control (261). 40% M, mean age 35, 70% (Int) and 68%
(Control) smoked 11-24 CPD.
Motivation to quit not required, but some GPs felt it a waste of time to counsel unmotivated
smokers
Interventions Int: Brief physician advice, mean 10 mins, tailored to SoC, S-H manual, NRT gum recommended
if appropriate.
Control: usual care (smoking discussed only if raised by patient).
50Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pieterse 2001 (Continued)
Outcomes PPA and CA at 6 and 12m
Validation: None; ’bogus pipeline’ at 1m
Notes Type of intervention: Brief physician advice, S-H materials
Funded by Dutch Cancer Society
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? No “subjects were assigned ... by the office assistant”,
but GPs were allowed to give the intervention to
some control patients, who were later excluded
from analyses
Allocation concealment? Yes Prestructured allocation lists.
Blinding?
All outcomes
Unclear Not stated
Free of other bias? No Disparities in baseline characteristics in CPD
and motivation to quit suggest selection bias.
Follow up period ’contaminated’ by intensive
mass media anti-smoking campaign
Prochaska 1993
Methods Setting: Houston, TX, and Rhode Island, USA
Study design: Randomized controlled trial
Recruitment: Mass media ads + incentives
SoC Model: TTM
Participants 1466 smokers randomized by SoC: Preconts: 166 [93 in RI] (not seriously considering
quitting within next 6m); Conts 794 [435 in RI] (seriously considering quitting in next
6m, but not in next 30 days and/or had not made a 24-hr quit attempt in previous yr)
; Preps 506 [228 in RI] (planning to quit in next 30 days and had made previous 24-hr
quit attempt).
37% M, mean age 42, 86% W (TX), 98% W (RI), mean CPD 27.
Motivation to quit not required
Interventions Int 1: TTT manuals, matched to current SoC + all subsequent manuals.
Int 2: As 1, + computerised feedback tailored to baseline, post-test and 6m Qs.
Int 3: As 2, + 4 personalised stage-matched counsellor phone calls (≃ 15 mins) at pretest,
1, 3 and 6m.
Control: 3 standardized ALA manuals + cover letter advising on best fit for each stage.
Reactive hot line available to all pts, but hardly used.
51Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prochaska 1993 (Continued)
Outcomes Pts from both sites assessed at baseline, 1m, 6m, but only RI pts at 12 and 18m
24-hr PPA and PA (abstinent at 2 points).
Validation: None, but ’bogus pipeline’ of confirmation by ’significant other’
Notes Type of intervention: S-H, expert system, phone counselling.
We have compared Int 1 (stage-based manuals) with Controls (standard S-H manuals)
for our MAs.
RI cohort used for our analyses; denominators by treatment groups not reported.
Funded by National Cancer Institute
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “randomly assigned, stratified by stage”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Unclear Not stated
Free of other bias? No Pts received stage-matched manual + all
subsequent manuals in one delivery
Prochaska 2001a
Methods Setting: Houston, Rhode Island, USA
Study design: Randomized controlled trial
Recruitment: Random digit dialling
SoC Model: TTM
Participants 4144 smokers assigned to Int (1358) or control (2786). 44% M, mean age 41, ethnicity
96% W, mean CPD 20.
Motivation to quit not required
Interventions Int: Expert System (ES): Baseline feedback report + stage-matched S-H manuals; Qs at
3 and 6m, with computerised tailored feedback.
Control: Assessment Only (AS): proactively assessed at 6m intervals
Outcomes 24-hr PPA and 30 day and 6m PA at 6, 12, 18 and 24m.
Validation: None
Notes Type of intervention: S-H manuals, expert system.
Funded by National Cancer Institute
52Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prochaska 2001a (Continued)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “Subjects were randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes By 24m 39.8% Int group and 35.6% Cont
group lost or refused.
Free of other bias? No Pts received stage-matched manual + all
subsequent manuals in one delivery
Prochaska 2001b
Methods Setting: SE Massachusetts and Rhode Island, USA
Study design: Randomized controlled trial
Recruitment: Smokers identified and invited from managed care system
SoC Model: TTM
Participants 1452 smokers randomized to ES (368), ES+CO (359), ES+SC (366) and AS (359).
Shares the ES group with Velicer 1999, but denominator discrepant by 6.
44% M, mean age 38, mean CPD 20.
Motivation to quit not required.
Interventions Int 1: Expert System (ES): S-H manual, matched to SoC + all subsequent manuals +
computerised tailored feedback reports.
Int 2: ES + Counselling (ES+CO): As 1, + 3 proactive tailored counselling calls at baseline,
3 and 6m.
Int 3: ES+Stimulus Control (ES+SC): As 1, + Conts and preps were sent Lifesign hand-
held computer (nicotine fading) + materials. Preconts who moved to Cont within dura-
tion of trial were sent the computer.
Control: Assessment only (AS):
Outcomes 24-hr, 7-day PPA and 30-day and 6m PA at 6, 12 and 18m
Validation: None
Notes Type of intervention: S-H materials, expert system, nicotine fading.
Study reports 1447 randomized, but group totals come to 1452.
We have compared Int 1 (ES letters + manuals) vs Control (Assessment) for our MAs in
this review.
Funded by National Cancer Institute
Risk of bias
53Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prochaska 2001b (Continued)
Item Authors’ judgement Description
Adequate sequence generation? Unclear “random assignment was employed”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes Five models of “missingness” tested
Free of other bias? No Pts received stage-matched manual + all
subsequent manuals in one delivery
Prochaska 2004
Methods Setting: Rhode Island schools, USA
Study design: Randomized controlled trial
Recruitment: Parents of 9th grade teenagers
SoC Model: TTM
Participants 711 smokers, from 2460 parents with at least 1 risk factor (sun, smoking, high fat).
Randomized to Int (349) or Control (362). Across whole cohort, 25% M, mean age 42,
mean CPD 18.
Motivation to quit not required
Interventions Int: Expert System (ES): S-H materials, + 3 computer-generated tailored reports at
baseline, 6 and 12m, based on phone follow up.
Control: Assessment only at 6 and 12m
Outcomes 24-hr and 7-day PPA, + 6m PA at 12 and 24m.
Notes Type of intervention: S-H manuals, expert system
4 died before assessment, but distribution NK.
Funded by National Cancer Institute
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “subjects were randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
54Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prochaska 2004 (Continued)
Incomplete outcome data addressed?
All outcomes
Yes At 12m 36% and at 24m 42% of smokers
were lost or refused.
Free of other bias? Unclear Not stated
Prochaska 2005
Methods Setting: 79 primary care practices within an HMO, USA
Study design: Randomized controlled trial
Recruitment: by phone, for pts registered with the practices
SoC Model: TTM
Participants 1211 smokers, from 5407 pts with at least 1 cancer risk factor (smoking, diet, sun
exposure, mammography). Smoker allocation to int and control not reported. 30% M,
mean age 45, mean CPD 17
Interventions Int: Home-based ES: 3 x computer reports at baseline, 6 and 12m.
Control: assessment only at 12 and 24m.
Outcomes 24-hr and 7-day PPA at 6m (int only), 12 and 24m, + 6m PA at 12 and 24m
Validation: None
Notes Type of intervention: expert system
ITT denominators not known.
Funded by National Cancer Institute
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “patients were randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Yes “Telephone surveyors were blind to assign-
ment”
Incomplete outcome data addressed?
All outcomes
Unclear By 24m, 35% of smokers were lost to follow
up or refused (distribution not stated)
Free of other bias? Unclear Not stated
55Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prochaska 2008
Methods Setting: Medical University, OR, USA
Study design: Randomized controlled trial
Recruitment: Randomized to mail/email only, mail/email + incentive, or mail + incentive + phone
prompt.
SoC Model: TTM
Participants 1400 employees, randomized to health risk assessment intervention (HRI: 464; 48 smokers), HRI +
MI counselling (433; 40 smokers) or HRI + interactive TTM programme (TTM: 503; 48 smokers)
. Study targeted 4 risk-reduction programmes: stress, exercise, weight control and smoking. 11%
M, mean age 41, mean CPD N/S
Interventions Control: Health risk assessment (HRA) only. SoC assessed for each risk, and identified single best
step to remedy.
Int 1: MI: HRA + 3 x phone or face-to-face MI sessions, to move along SoC and reduce risky
behaviour.
Int 2: TTM: HRA + online TTM programme (Pro-Change Lifestyle Management Program); 4
programmes over 6m; recommended 3 sessions of each course
Outcomes ’Reaching criterion’ at 6m, i.e. PPA (no longer at risk) for smokers.
We have compared Int 2 (TTM computer programme) vs Control (HRA) for our MAs in this
review.
Validation: None
Notes Denominators by group not reported for 6m follow up, but 35/136 did not supply 6m follow-up
data. We have applied 6m % quit rates to baseline denominators for our MAs in this review.
Funded by US Centers for Disease Control and Prevention
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Free of other bias? Unclear Not stated
Prokhorov 2008
Methods Setting: 15 Community colleges, Houston, TX, USA
Study design: Cluster-randomized controlled trial
Recruitment: by instructors, newspapers, newsletters, fliers, sign-up booths, promo items
Study: “Look At Your Health”
SoC Model: TTM + Health Belief Model
56Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prokhorov 2008 (Continued)
Participants 426 students, assigned by college to Int (219) or control (207). 46% M (SC), 27% M
(LAYH); mean age 23; mean CPD 13.
Motivation to quit not required.
Interventions Int: Look At Your Health: MI counselling + lung function and CO test feedback; Coun-
selling modified by expert system software, tailoring for nicotine dependence, decisional
balance, temptations to smoke, SoC. Each pt given a brief individualised newsletter of
their data.
Control: Standard Care: brief MI counselling + S-H manual Clearing the Air.Follow ups at 2, 4 and 10m, to support, answer questions, assess
Outcomes 7-day PPA at 10m.
Validation: salivary cotinine ≤5 g/mL at baseline and 10m.
Notes Type of intervention: expert system, biofeedback, S-H manuals.
“phenomenal” discrepancies between self-reported and validated quit rates: LAYH: 28.
5 vs 16.6; SC 24.4 vs 10.1.
Funded by National Cancer Institute
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “campuses were pair-matched by size and
then randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Unclear By 10m, SC had lost 19%, LAYH 28%
Free of other bias? Unclear 1 campus dropped out and was replaced
Schumann 2006
Methods Setting: 3 cities in W Pomerania, Germany
Study design: Randomized controlled trial
Recruitment: Identified smokers invited to take part.
Study: SHIP study
SoC Model: TTM
Participants 485 daily smokers, assigned to Int (240) or control (245). 52% M, mean age 44, mean
CPD 15.
Motivation to quit not required.
57Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Schumann 2006 (Continued)
Interventions Int: 3 x computer-generated expert system letters + tailored S-H materials.
Control: Assessment only
Outcomes PPA at 3m (int only), 6, 12, 18 and 24m
Validation: None
Notes Type of intervention: expert system, S-H material
2008 data includes ex-smokers in denominator, but our comparison uses baseline smok-
ers only.
Funded by German Federal Ministry of Education and Research, and Social Ministry of
mecklenburg-West Pomerania
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “Each subject was assigned a unique com-
puter-generated random number”
Allocation concealment? Yes “subject data file was sorted by ascending
random numbers, and then subjects were
consecutively assigned to the three study
conditions”
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes At 12m 27.4% and at 24m 30.5% lost or
refused
Free of other bias? Unclear Not stated
Stotts 2002
Methods Setting: 21 satellite locations of 3 large clinics in Houston and Dallas, TX, USA
Study design: Pilot randomized controlled trial
Recruitment: phone invitation at 28 wks
Study: One-to-One Study
SoC Model: modified TTM
Participants 269 late-pregnancy smokers (28 wks+) who had already tried and failed to quit, allocated
to Int (134) or control (135). Mean age 28, 79% W, mean CPD not stated
Interventions Int: 1 x 20-30 min tailored counselling call, SoC-based personalised letter + follow-up
phone call, + postpartum newsletters and video
Control: Usual care, i.e. brief counselling and S-H booklets, received by all participants
58Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Stotts 2002 (Continued)
Outcomes PPA or ’not smoking most of the time’ at 6m postpartum
Validation: 175 anonymized cotinine samples at 34 wks (41% of Int, 39% of control)
Notes Type of intervention: Tailored expert system letter, phone-based MI counselling, video.
Funded by National Cancer Institute.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “computer-generated random number list”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Yes Pts blinded to purpose of follow-up survey
Incomplete outcome data addressed?
All outcomes
Yes 45% of Int group did not receive full inter-
vention
Free of other bias? No Only 55% of Int group received full inter-
vention
Thompson 1993
Methods Setting: Free Cancer Information Service hotline throughout USA
Study design: Randomized controlled trial
Recruitment: Invitation to callers, + ads, posters, fliers
SoC Model: modified TTM
Participants 4 worksites + “other sources”, i.e. callers to a free SC hotline. 382 callers allocated to Int
(197) or control (185). Int 43% M, Control 35% M, mean age 40, mean CPD 22
Interventions Callers to ’hotline’ did not include any in precontemplation.
Int: Tailored responses, to move caller along cessation continuum; Mean duration of call
34 mins
Control: Reactive ’general information’ + standard S-H materials. Mean duration of call
20 mins
Outcomes PPA at 6 and 12m (subset)
Validation: mailed saliva samples as ’bogus pipeline’; surrogates contacted
Notes Study targeted blue-collar workers, but recruited only 24% in cohort.
Type of intervention: telephone counselling.
Funded by National Cancer Institute.
Risk of bias
59Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
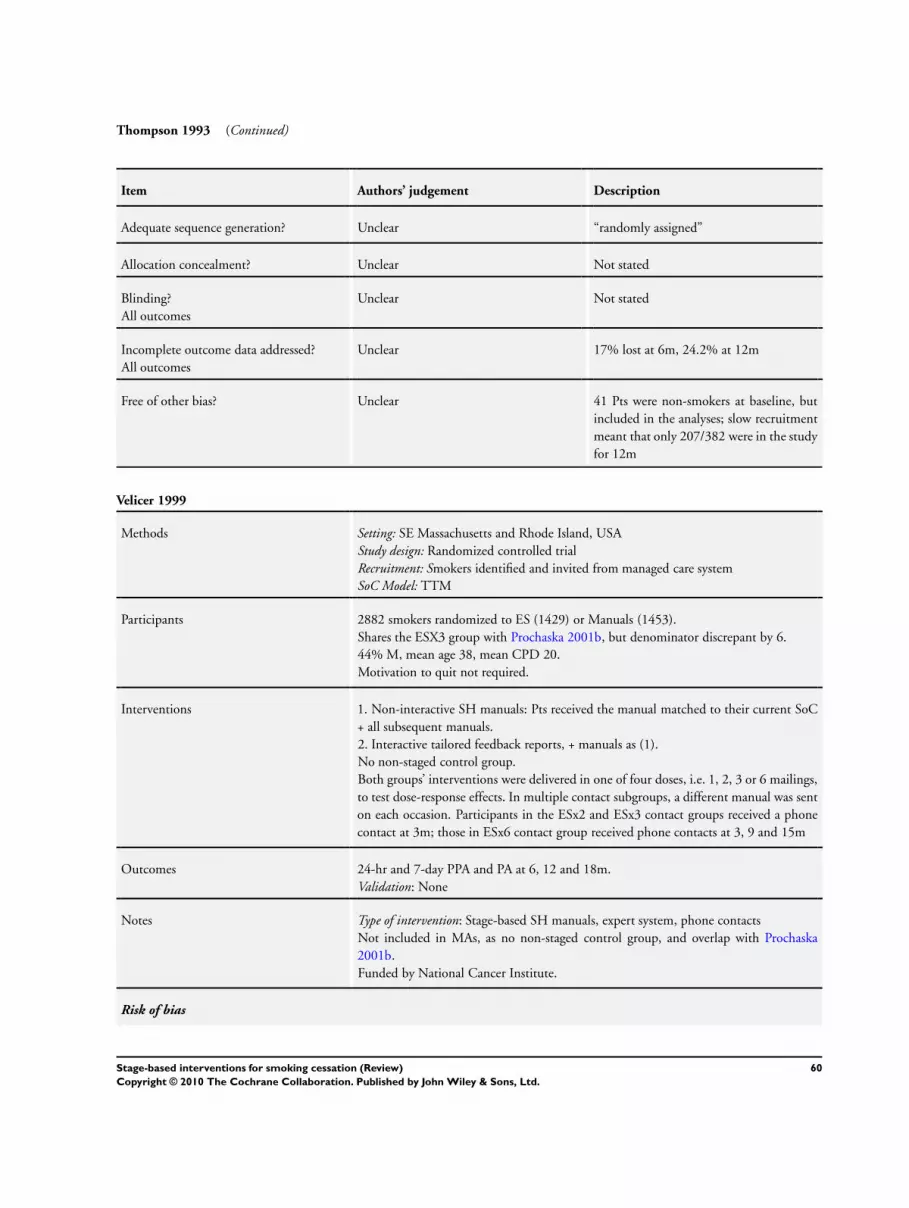
Thompson 1993 (Continued)
Item Authors’ judgement Description
Adequate sequence generation? Unclear “randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Unclear 17% lost at 6m, 24.2% at 12m
Free of other bias? Unclear 41 Pts were non-smokers at baseline, but
included in the analyses; slow recruitment
meant that only 207/382 were in the study
for 12m
Velicer 1999
Methods Setting: SE Massachusetts and Rhode Island, USA
Study design: Randomized controlled trial
Recruitment: Smokers identified and invited from managed care system
SoC Model: TTM
Participants 2882 smokers randomized to ES (1429) or Manuals (1453).
Shares the ESX3 group with Prochaska 2001b, but denominator discrepant by 6.
44% M, mean age 38, mean CPD 20.
Motivation to quit not required.
Interventions 1. Non-interactive SH manuals: Pts received the manual matched to their current SoC
+ all subsequent manuals.
2. Interactive tailored feedback reports, + manuals as (1).
No non-staged control group.
Both groups’ interventions were delivered in one of four doses, i.e. 1, 2, 3 or 6 mailings,
to test dose-response effects. In multiple contact subgroups, a different manual was sent
on each occasion. Participants in the ESx2 and ESx3 contact groups received a phone
contact at 3m; those in ESx6 contact group received phone contacts at 3, 9 and 15m
Outcomes 24-hr and 7-day PPA and PA at 6, 12 and 18m.
Validation: None
Notes Type of intervention: Stage-based SH manuals, expert system, phone contacts
Not included in MAs, as no non-staged control group, and overlap with Prochaska
2001b.
Funded by National Cancer Institute.
Risk of bias
60Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Velicer 1999 (Continued)
Item Authors’ judgement Description
Adequate sequence generation? Unclear “2882 were randomly assigned”
Allocation concealment? Unclear Not stated
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes Full details of attrition and refusals
Free of other bias? Unclear Pts received relevant + all subsequent stage
manuals.
Wang 1994
Methods Setting: Outpatient clinics in Taiwanese Hospital
Study design: Randomized controlled trial
Recruitment: Physicians within Dept Family Medicine
SoC Model: modified TTM
Participants 93 smoker patients of physicians allocated to SoC training (39 pts), to reminder (26 pts)
or to usual care (28 pts). 95% M
Interventions Int 1: 2 x lessons on SoC model and counselling for SC
Int 2: Reminder poster placed in clinic room to encourage standard SC advice.
Control: Usual care (may or may not include reference to SC)
Outcomes PPA at 6m
Validation: None
Notes Type of intervention: training physicians in SoC SC techniques.
We have compared Int 1 (stage-based physician advice) vs Int 2+Control (minimal or
usual care) for our MAs in this review.
Supported by Taiwanese Department of Health
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear “All physicians were numbered and ran-
domly assigned to one of three groups by
number of years in practice”
Allocation concealment? Unclear Not stated
61Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wang 1994 (Continued)
Blinding?
All outcomes
Unclear Not stated
Incomplete outcome data addressed?
All outcomes
Yes 12% at 6m
Free of other bias? Unclear Not stated
Young 2008
Methods Setting: 30 general practices, Sydney, Australia
Study design: Randomized controlled trial
Recruitment: All patients assessed over 3wk period, and smokers invited
SoC Model: TTM
Participants 318 smokers, randomized to Int (169) or control (149); 46% M, mean age 38; 73%
smoked ≥20 CPD
Interventions Int: 4 x counselling phone calls, delivered by trained nurse, based on 5As, MI, 5Rs.
Those not ready to make a quit attempt received a motivational intervention to move
them through the stages. Quit-attempters were sent quit pack, encouraged to use NRT;
Calls made on TQD, +1wk and +3wks.
Control: Usual care, including free quit kits
Outcomes PPA at 6, 12m
Validation: None
Notes Type of intervention: telephone counselling.
Only 76 of 169 intervention smokers agreed to participate in the counselling phase.
Funded by National Heart Foundation of Australia
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes “prerandomized questionnaires”
Allocation concealment? Yes Before consultation
Blinding?
All outcomes
Unclear phone follow-up “blind to ... group alloca-
tion”
Incomplete outcome data addressed?
All outcomes
Yes 21% (I) and 26% (C) lost at 6m; 31% (I)
and 41% (C) at 12m
Free of other bias? Unclear 5 control pts received intervention in error;
analysed as controls (ITT).
Only 55 smokers completed all 4 calls.
62Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
4As: Ask-Advise-Assist-Arrange follow up
a/v: audio-visual
AHCP: Agency for Health Care Policy
APA: American Psychiatric Association
CA: continuous abstinence
CO: carbon monoxide
Cont: contemplator
CPD: cigarettes per day
FTND: Fagerström Test for Nicotine Dependence
M: male
m: month(s)
MA: meta-analysis
MI: motivational interviewing
PA: prolonged abstinence
PPA: point prevalence abstinence
Precont: precontemplators
Prep: in preparation
Pt: participant
Q: questionnaire
SC: smoking cessation
SES: socio-economic status
SoC: stage of change
TTM: Transtheoretical Model
W: white
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Abdullah 2005 Both groups received staged materials; tested intervention was additional telephone counselling
Ahluwalia 2007 Main outcome was fruit and vegetable consumption among smokers; smoking behaviour was not a reported
outcome
Andersen 2006 Outcomes were effect of support on smoking and movement through stages; Only 5 weeks follow up
Armitage 2008 Only 2 months follow up.
Baker 2006 Intervention was mainly MI and CBT; Stage of change was measured but not used in intervention
Becona 2001 Participants were classified by stage of change, but it did not modify the intervention
Berman 1995 Stage of change was measured but not integrated into the intervention
Borrelli 2002 PAQS Study: Insufficient information to treat as an included study (results not reported)
Campbell 2004 Report of recruitment; participants were marijuana users.
63Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Carlson 2003 Uncontrolled cohort study, follow up only to 3 months.
Chan 2005 Insufficient information to treat as an included study (details of intervention not available)
Cornuz 2002 Prescribed NRT as part of the intervention where appropriate
Dijkstra 1998b Outcomes were attitudes and movement through stages, not smoking behaviour change
Dijkstra 1998c Only 4 months follow up.
Dijkstra 2006 Outcome was movement through the stages of change, not smoking cessation
Drevenhorn 2007 Outcome was consultation skills, not smoking behaviour change
Erol 2008 Main outcome was movement through stages of change, and main intervention was MI. Smoking rates were
reported as an incidental outcome
Ershoff 1999 All pts received SoC-based interventions. Study tested addition of phone counselling and MI
Etter 2005 Only 10 weeks follow up.
Etter 2009 Short-term (48-hour) effects of tailored vs generic advice to quit
Fang 2006 Only 3 months follow up.
Fritz 2008 Only 1 month follow up.
Gritz 1993 Stage of change was recorded, but not used in tailoring the intervention
Hall 2006 Supplied NRT or bupropion as appropriate as part of the intervention
Haug 2009 Three group trial of text messaging support. Final assessment was at 3m
Hoving 2007 Stage of change was measured to determine eligibility, but did not significantly modify the intervention
Huang 2005 Outcome was prevention rather than cessation.
Hughes 2000 Insufficient information to treat as an included study (quit rates for intervention and control groups not reported
separately)
Hughes 2005 Outcome was intention to quit over 30 days, not cessation.
Hyman 2007 Stage of change was reported, but intervention was timing.
Jennings 2007 Stage of change was measured but not integrated with intervention
64Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Johs 2003 Only 3 months follow up.
Jones 2003 Insufficient information to treat as an included study (disparities in denominators for intervention and control
groups)
Keller 2000 Movement through stages of change was main outcome, not cessation
Kim 2004 Intervention was not tailored to stage of change.
Kim 2009 Non-randomized study. Outcomes included movement through stages and scores on processes of change, but
not abstinence achieved
Kohler 2008 Motivation and movement through stages were main outcomes; only 10 weeks follow up
Lipkus 1999 All participants received stage-based support, and heavier smokers were given a coupon for free NRT, which
could have confounded the results
Ma 2005 Follow up was to 3m.
McDonald 2003 Insufficient information to treat as an included study (results and denominators not available)
Morgan 1996 Provided NRT gum where appropriate as part of the intervention
Osinubi 2003 Stage of change was measured but did not modify intervention
Pallonen 1998 Quit rates for each group not reported separately.
Pisinger 2005 Both intervention arms were given free samples of NRT if wished
Pletsch 2002 Outcome was movement through stages of change, not cessation
Quinlan 2000 Only 1 month follow up.
Reeve 2000 Only 3 months follow up.
Reid 2003 Stage of change was measured, but not integrated into intervention
Resnicow 1997 Stage of change advice not separable from other components.
Rissel 2000 Only 3 months follow up.
Schneider 1990 Tailored intervention not modified by stage of change.
Simon 2003 Impact of stage of change could not be isolated from other components
Sinclair 1998 Tailoring was not modified by stage of change.
65Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Skewes 2007 Insufficient information to treat as an included study
Swanson 2003 Main outcome was comparison of NRT and/or bupropion versus counselling. Stage of change was measured
but did not modify the intervention
Tanaka 2006 Intervention was not modified by stage of change.
Tappin 2000 Quit rates were assessed at 14 weeks and in late pregnancy; intervention was more MI than stage of change
Tsoh 2005 Insufficient information to treat as an included study (18m results not yet available)
Valanis 2001 Quasi-experimental prospective cohort study, not randomized, with historical and interim controls
Webb 2005 Changes in smoking behaviour were not an outcome of interest
Wiggers 2005 Only 8 weeks follow up.
Williams 2006 Main theoretical model was self-determination theory, not stages of change
Wilson 2008 Both intervention groups were given free NRT if wished.
Wu 2009 Stage of change measured, but primarily a trial of MI techniques + NRT
Young 2002 Outcome was changes in competencies among family doctors using distance learning, not smoking cessation
CBT: cognitive behavioural therapy
MI: motivational interviewing
Characteristics of ongoing studies [ordered by study ID]
Cabezas 2009
Trial name or title ISTAPS Study
Methods Cluster-randomized trial, in 82 primary care centres (PCCs) in Spain
Participants 3024 teenage and adult smokers attending PCC
Interventions MI counselling, brief advice, NRT, vs usual care
Outcomes PPA at 6m, 1 yr,2 yrs, CO-validated.
Starting date 2003
66Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Cabezas 2009 (Continued)
Contact information [email protected]
Notes Supported by grants from Carlos III Health Institute
Prokhorov 2010
Trial name or title Project ASPIRE
Methods Nested-cohort group-randomized trial of students from 16 schools in Houston, Texas
Participants school students, smoking and non-smoking
Interventions CD-ROM-based interactive programme of five sessions + 2 booster sessions
Outcomes Rates of uptake among baseline non-smokers, and cessation among baseline smokers
Starting date
Contact information [email protected]
Notes Supported by a grant from National Cancer institute
67Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Optimal trial comparisons
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Stage-based vs standard SH
materials
2 2117 Risk Ratio (M-H, Fixed, 95% CI) 0.93 [0.62, 1.39]
2 Stage-based counselling vs
standard advice
2 1138 Risk Ratio (M-H, Fixed, 95% CI) 1.00 [0.82, 1.22]
Comparison 2. Abstinence by intervention and comparison
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Expert systems 18 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
1.1 Standard self help 6 5947 Risk Ratio (M-H, Fixed, 95% CI) 1.27 [1.01, 1.59]
1.2 Usual care 2 849 Risk Ratio (M-H, Fixed, 95% CI) 0.94 [0.56, 1.57]
1.3 Assessment only 10 13597 Risk Ratio (M-H, Fixed, 95% CI) 1.35 [1.19, 1.52]
2 Individual counselling 13 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
2.1 Standard self help 3 2035 Risk Ratio (M-H, Fixed, 95% CI) 1.33 [1.00, 1.78]
2.2 Usual care 7 3293 Risk Ratio (M-H, Fixed, 95% CI) 1.19 [0.99, 1.42]
2.3 Assessment only 3 3056 Risk Ratio (M-H, Fixed, 95% CI) 1.28 [0.95, 1.73]
3 Interactive computer programme 5 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
3.1 Usual care 2 1702 Risk Ratio (M-H, Fixed, 95% CI) 1.14 [0.81, 1.59]
3.2 Assessment only 3 231 Risk Ratio (M-H, Fixed, 95% CI) 1.36 [0.78, 2.36]
4 Phone quit lines 2 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
4.1 Standard self help 1 207 Risk Ratio (M-H, Fixed, 95% CI) 1.04 [0.59, 1.82]
4.2 Usual care 1 318 Risk Ratio (M-H, Fixed, 95% CI) 1.27 [0.56, 2.89]
5 Training doctors 2 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
5.1 Usual care 2 2681 Risk Ratio (M-H, Fixed, 95% CI) 0.99 [0.65, 1.50]
6 Training lay supporters 1 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
6.1 Standard self help 1 60 Risk Ratio (M-H, Fixed, 95% CI) 1.5 [0.27, 8.34]
7 Staged SH materials 1 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
7.1 Assessment only 1 375 Risk Ratio (M-H, Fixed, 95% CI) 1.31 [0.55, 3.13]
68Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 3. Validated abstinence
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Biochemically validated
abstinence
8 7603 Risk Ratio (M-H, Fixed, 95% CI) 1.19 [1.02, 1.39]
2 Self-reported abstinence 28 23334 Risk Ratio (M-H, Fixed, 95% CI) 1.25 [1.14, 1.37]
3 ’Bogus pipeline’ 4 3033 Risk Ratio (M-H, Fixed, 95% CI) 1.72 [1.20, 2.46]
Comparison 4. Missing data testing
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Intervention ITT versus control
per protocol
13 12715 Risk Ratio (M-H, Fixed, 95% CI) 0.88 [0.79, 0.98]
2 Intervention ITT versus control
ITT
13 14832 Risk Ratio (M-H, Fixed, 95% CI) 1.21 [1.09, 1.36]
Comparison 5. Any stage-based intervention vs control
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Abstinence at longest follow up 40 33446 Risk Ratio (M-H, Fixed, 95% CI) 1.25 [1.16, 1.35]
2 Abstinence by comparison
condition
40 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
2.1 Standard self-help
materials
12 9383 Risk Ratio (M-H, Fixed, 95% CI) 1.19 [1.04, 1.37]
2.2 Usual care 12 7569 Risk Ratio (M-H, Fixed, 95% CI) 1.23 [1.02, 1.48]
2.3 Assessment only 16 16650 Risk Ratio (M-H, Fixed, 95% CI) 1.33 [1.19, 1.48]
Comparison 6. PPA at 6 or 12 m by intervention and comparison
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Expert systems 18 20472 Risk Ratio (M-H, Fixed, 95% CI) 1.14 [1.05, 1.24]
1.1 Standard self help 6 5947 Risk Ratio (M-H, Fixed, 95% CI) 1.07 [0.91, 1.25]
1.2 Usual care 2 849 Risk Ratio (M-H, Fixed, 95% CI) 0.75 [0.51, 1.10]
1.3 Assessment only 10 13676 Risk Ratio (M-H, Fixed, 95% CI) 1.20 [1.09, 1.33]
2 Individual counselling 12 8026 Risk Ratio (M-H, Fixed, 95% CI) 1.33 [1.18, 1.51]
2.1 Standard self help 2 1677 Risk Ratio (M-H, Fixed, 95% CI) 1.23 [0.90, 1.67]
69Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2.2 Usual care 7 3293 Risk Ratio (M-H, Fixed, 95% CI) 1.19 [1.01, 1.41]
2.3 Assessment only 3 3056 Risk Ratio (M-H, Fixed, 95% CI) 1.70 [1.34, 2.14]
3 Interactive computer programme 5 1933 Risk Ratio (M-H, Fixed, 95% CI) 1.24 [0.96, 1.59]
3.1 Usual care 2 1702 Risk Ratio (M-H, Fixed, 95% CI) 1.25 [0.93, 1.67]
3.2 Assessment only 3 231 Risk Ratio (M-H, Fixed, 95% CI) 1.21 [0.74, 1.98]
4 Phone quit lines 2 525 Risk Ratio (M-H, Fixed, 95% CI) 1.12 [0.70, 1.78]
4.1 Standard self help 1 207 Risk Ratio (M-H, Fixed, 95% CI) 1.04 [0.59, 1.82]
4.2 Usual care 1 318 Risk Ratio (M-H, Fixed, 95% CI) 1.27 [0.56, 2.89]
5 Training doctors 2 2681 Risk Ratio (M-H, Fixed, 95% CI) 1.03 [0.79, 1.34]
5.1 Usual care 2 2681 Risk Ratio (M-H, Fixed, 95% CI) 1.03 [0.79, 1.34]
6 Training lay supporters 1 60 Risk Ratio (M-H, Fixed, 95% CI) 1.5 [0.27, 8.34]
6.1 Standard self help 1 60 Risk Ratio (M-H, Fixed, 95% CI) 1.5 [0.27, 8.34]
7 Staged SH materials 1 375 Risk Ratio (M-H, Fixed, 95% CI) 1.45 [0.65, 3.22]
7.1 Assessment only 1 375 Risk Ratio (M-H, Fixed, 95% CI) 1.45 [0.65, 3.22]
Comparison 7. Per protocol analyses
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Expert systems 18 15504 Risk Ratio (M-H, Fixed, 95% CI) 1.36 [1.23, 1.51]
1.1 Standard self help 6 4947 Risk Ratio (M-H, Fixed, 95% CI) 1.35 [1.08, 1.70]
1.2 Usual care 2 724 Risk Ratio (M-H, Fixed, 95% CI) 0.92 [0.55, 1.53]
1.3 Assessment only 10 9833 Risk Ratio (M-H, Fixed, 95% CI) 1.39 [1.24, 1.57]
2 Individual counselling 13 6329 Risk Ratio (M-H, Fixed, 95% CI) 1.29 [1.13, 1.48]
2.1 Standard self help 3 1748 Risk Ratio (M-H, Fixed, 95% CI) 1.42 [1.07, 1.89]
2.2 Usual care 7 2314 Risk Ratio (M-H, Fixed, 95% CI) 1.19 [1.00, 1.42]
2.3 Assessment only 3 2267 Risk Ratio (M-H, Fixed, 95% CI) 1.44 [1.10, 1.89]
3 Interactive computer programme 5 1554 Risk Ratio (M-H, Fixed, 95% CI) 1.21 [0.91, 1.61]
3.1 Usual care 2 1347 Risk Ratio (M-H, Fixed, 95% CI) 1.16 [0.83, 1.61]
3.2 Assessment only 3 207 Risk Ratio (M-H, Fixed, 95% CI) 1.41 [0.82, 2.42]
4 Phone quit lines 2 412 Risk Ratio (M-H, Fixed, 95% CI) 1.05 [0.66, 1.67]
4.1 Standard self help 1 207 Risk Ratio (M-H, Fixed, 95% CI) 1.04 [0.59, 1.82]
4.2 Usual care 1 205 Risk Ratio (M-H, Fixed, 95% CI) 1.09 [0.49, 2.43]
5 Training doctors 2 1738 Risk Ratio (M-H, Fixed, 95% CI) 1.00 [0.66, 1.51]
5.1 Usual care 2 1738 Risk Ratio (M-H, Fixed, 95% CI) 1.00 [0.66, 1.51]
6 Training lay supporters 1 54 Risk Ratio (M-H, Fixed, 95% CI) 1.5 [0.27, 8.28]
6.1 Standard self help 1 54 Risk Ratio (M-H, Fixed, 95% CI) 1.5 [0.27, 8.28]
7 Staged SH materials 1 265 Risk Ratio (M-H, Fixed, 95% CI) 1.67 [0.70, 3.96]
7.1 Assessment only 1 265 Risk Ratio (M-H, Fixed, 95% CI) 1.67 [0.70, 3.96]
70Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 8. Cluster randomized trials
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Individual counselling 13 Risk Ratio (Fixed, 95% CI) 1.25 [1.07, 1.46]
1.1 Standard Self help 3 Risk Ratio (Fixed, 95% CI) 1.20 [0.92, 1.55]
1.2 Usual care 7 Risk Ratio (Fixed, 95% CI) 1.24 [0.99, 1.56]
1.3 Assessment only 3 Risk Ratio (Fixed, 95% CI) 1.43 [0.94, 2.17]
2 Interactive computer programme 5 Risk Ratio (Fixed, 95% CI) 1.19 [0.88, 1.61]
2.1 Usual care 2 Risk Ratio (Fixed, 95% CI) 1.14 [0.79, 1.63]
2.2 Assessment only 3 Risk Ratio (Fixed, 95% CI) 1.32 [0.76, 2.28]
3 Training doctors 2 Risk Ratio (Fixed, 95% CI) 1.33 [0.67, 2.63]
3.1 Usual care 2 Risk Ratio (Fixed, 95% CI) 1.33 [0.67, 2.63]
Analysis 1.1. Comparison 1 Optimal trial comparisons, Outcome 1 Stage-based vs standard SH materials.
Review: Stage-based interventions for smoking cessation
Comparison: 1 Optimal trial comparisons
Outcome: 1 Stage-based vs standard SH materials
Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Lennox 2001 30/870 37/869 80.2 % 0.81 [ 0.51, 1.30 ]
Prochaska 1993 13/192 9/186 19.8 % 1.40 [ 0.61, 3.20 ]
Total (95% CI) 1062 1055 100.0 % 0.93 [ 0.62, 1.39 ]
Total events: 43 (Experimental), 46 (Control)
Heterogeneity: Chi?? = 1.27, df = 1 (P = 0.26); I?? =21%
Test for overall effect: Z = 0.37 (P = 0.71)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
71Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 Optimal trial comparisons, Outcome 2 Stage-based counselling vs standard
advice.
Review: Stage-based interventions for smoking cessation
Comparison: 1 Optimal trial comparisons
Outcome: 2 Stage-based counselling vs standard advice
Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Mermelstein 2003 106/381 108/375 75.6 % 0.97 [ 0.77, 1.21 ]
Thompson 1993 40/197 34/185 24.4 % 1.10 [ 0.73, 1.67 ]
Total (95% CI) 578 560 100.0 % 1.00 [ 0.82, 1.22 ]
Total events: 146 (Experimental), 142 (Control)
Heterogeneity: Chi?? = 0.32, df = 1 (P = 0.57); I?? =0.0%
Test for overall effect: Z = 0.00 (P = 1.0)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
Analysis 2.1. Comparison 2 Abstinence by intervention and comparison, Outcome 1 Expert systems.
Review: Stage-based interventions for smoking cessation
Comparison: 2 Abstinence by intervention and comparison
Outcome: 1 Expert systems
Study or subgroup Expert system Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Aveyard 2003 15/683 10/690 8.2 % 1.52 [ 0.69, 3.35 ]
Borland 2003 24/523 21/527 17.3 % 1.15 [ 0.65, 2.04 ]
Borland 2004 61/382 35/390 28.6 % 1.78 [ 1.20, 2.63 ]
Dijkstra 1999 14/420 7/215 7.7 % 1.02 [ 0.42, 2.50 ]
Lennox 2001 30/870 37/869 30.6 % 0.81 [ 0.51, 1.30 ]
Prochaska 1993 13/192 9/186 7.6 % 1.40 [ 0.61, 3.20 ]
Subtotal (95% CI) 3070 2877 100.0 % 1.27 [ 1.01, 1.59 ]
0.1 0.2 0.5 1 2 5 10
Favours control Favours intervention
(Continued . . . )
72Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Expert system Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Total events: 157 (Expert system), 119 (Control)
Heterogeneity: Chi?? = 6.93, df = 5 (P = 0.23); I?? =28%
Test for overall effect: Z = 2.00 (P = 0.045)
2 Usual care
McBride 1999 16/288 14/292 49.9 % 1.16 [ 0.58, 2.33 ]
Stotts 2002 10/134 14/135 50.1 % 0.72 [ 0.33, 1.56 ]
Subtotal (95% CI) 422 427 100.0 % 0.94 [ 0.56, 1.57 ]
Total events: 26 (Expert system), 28 (Control)
Heterogeneity: Chi?? = 0.80, df = 1 (P = 0.37); I?? =0.0%
Test for overall effect: Z = 0.24 (P = 0.81)
3 Assessment only
Curry 1995 7/329 7/328 1.7 % 1.00 [ 0.35, 2.81 ]
Dijkstra 1998 26/1155 4/385 1.5 % 2.17 [ 0.76, 6.17 ]
Etter 2004 163/1467 154/1467 37.8 % 1.06 [ 0.86, 1.30 ]
Hollis 2005 54/281 25/284 6.1 % 2.18 [ 1.40, 3.41 ]
Meyer 2008 14/488 5/609 1.1 % 3.49 [ 1.27, 9.63 ]
Prochaska 2001a 96/1346 136/2761 21.9 % 1.45 [ 1.12, 1.86 ]
Prochaska 2001b 28/362 16/350 4.0 % 1.69 [ 0.93, 3.07 ]
Prochaska 2004 29/349 18/362 4.3 % 1.67 [ 0.95, 2.95 ]
Prochaska 2005 85/352 81/437 17.7 % 1.30 [ 0.99, 1.71 ]
Schumann 2006 15/240 16/245 3.9 % 0.96 [ 0.48, 1.89 ]
Subtotal (95% CI) 6369 7228 100.0 % 1.35 [ 1.19, 1.52 ]
Total events: 517 (Expert system), 462 (Control)
Heterogeneity: Chi?? = 16.65, df = 9 (P = 0.05); I?? =46%
Test for overall effect: Z = 4.83 (P < 0.00001)
0.1 0.2 0.5 1 2 5 10
Favours control Favours intervention
73Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.2. Comparison 2 Abstinence by intervention and comparison, Outcome 2 Individual counselling.
Review: Stage-based interventions for smoking cessation
Comparison: 2 Abstinence by intervention and comparison
Outcome: 2 Individual counselling
Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Hann??ver 2009 2/151 0/187 0.6 % 6.18 [ 0.30, 127.85 ]
Hennrikus 2005 66/666 59/673 80.3 % 1.13 [ 0.81, 1.58 ]
Meysman 2010 28/178 14/180 19.1 % 2.02 [ 1.10, 3.71 ]
Subtotal (95% CI) 995 1040 100.0 % 1.33 [ 1.00, 1.78 ]
Total events: 96 (Experimental), 73 (Control)
Heterogeneity: Chi?? = 3.73, df = 2 (P = 0.15); I?? =46%
Test for overall effect: Z = 1.94 (P = 0.052)
2 Usual care
Bobo 1998 20/288 16/287 8.9 % 1.25 [ 0.66, 2.35 ]
Chouinard 2005 26/108 7/56 5.1 % 1.93 [ 0.89, 4.16 ]
Davies 2005 10/127 7/121 4.0 % 1.36 [ 0.54, 3.46 ]
Lawrence 2005 14/305 12/289 6.9 % 1.11 [ 0.52, 2.35 ]
Mermelstein 2003 106/381 108/375 60.7 % 0.97 [ 0.77, 1.21 ]
Pieterse 2001 22/269 8/261 4.5 % 2.67 [ 1.21, 5.89 ]
Prokhorov 2008 26/219 17/207 9.8 % 1.45 [ 0.81, 2.58 ]
Subtotal (95% CI) 1697 1596 100.0 % 1.19 [ 0.99, 1.42 ]
Total events: 224 (Experimental), 175 (Control)
Heterogeneity: Chi?? = 9.31, df = 6 (P = 0.16); I?? =36%
Test for overall effect: Z = 1.90 (P = 0.058)
3 Assessment only
Manfredi 2004 57/527 61/541 88.2 % 0.96 [ 0.68, 1.35 ]
Meyer 2008 10/402 5/609 5.8 % 3.03 [ 1.04, 8.80 ]
Nakamura 2004 18/500 4/477 6.0 % 4.29 [ 1.46, 12.59 ]
Subtotal (95% CI) 1429 1627 100.0 % 1.28 [ 0.95, 1.73 ]
Total events: 85 (Experimental), 70 (Control)
Heterogeneity: Chi?? = 10.12, df = 2 (P = 0.01); I?? =80%
Test for overall effect: Z = 1.61 (P = 0.11)
0.5 0.7 1 1.5 2
Favours control Favours intervention
74Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.3. Comparison 2 Abstinence by intervention and comparison, Outcome 3 Interactive computer
programme.
Review: Stage-based interventions for smoking cessation
Comparison: 2 Abstinence by intervention and comparison
Outcome: 3 Interactive computer programme
Study or subgroup Programme Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Usual care
Aveyard 1999 53/547 46/542 78.5 % 1.14 [ 0.78, 1.66 ]
Lawrence 2005 15/324 12/289 21.5 % 1.11 [ 0.53, 2.34 ]
Subtotal (95% CI) 871 831 100.0 % 1.14 [ 0.81, 1.59 ]
Total events: 68 (Programme), 58 (Control)
Heterogeneity: Chi?? = 0.00, df = 1 (P = 0.96); I?? =0.0%
Test for overall effect: Z = 0.74 (P = 0.46)
2 Assessment only
Escoffery 2004 9/35 6/35 33.7 % 1.50 [ 0.60, 3.77 ]
O’Neill 2000 5/31 4/34 21.4 % 1.37 [ 0.40, 4.65 ]
Prochaska 2008 10/48 8/48 44.9 % 1.25 [ 0.54, 2.89 ]
Subtotal (95% CI) 114 117 100.0 % 1.36 [ 0.78, 2.36 ]
Total events: 24 (Programme), 18 (Control)
Heterogeneity: Chi?? = 0.08, df = 2 (P = 0.96); I?? =0.0%
Test for overall effect: Z = 1.09 (P = 0.28)
0.01 0.1 1 10 100
Favours control Favours intervention
75Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
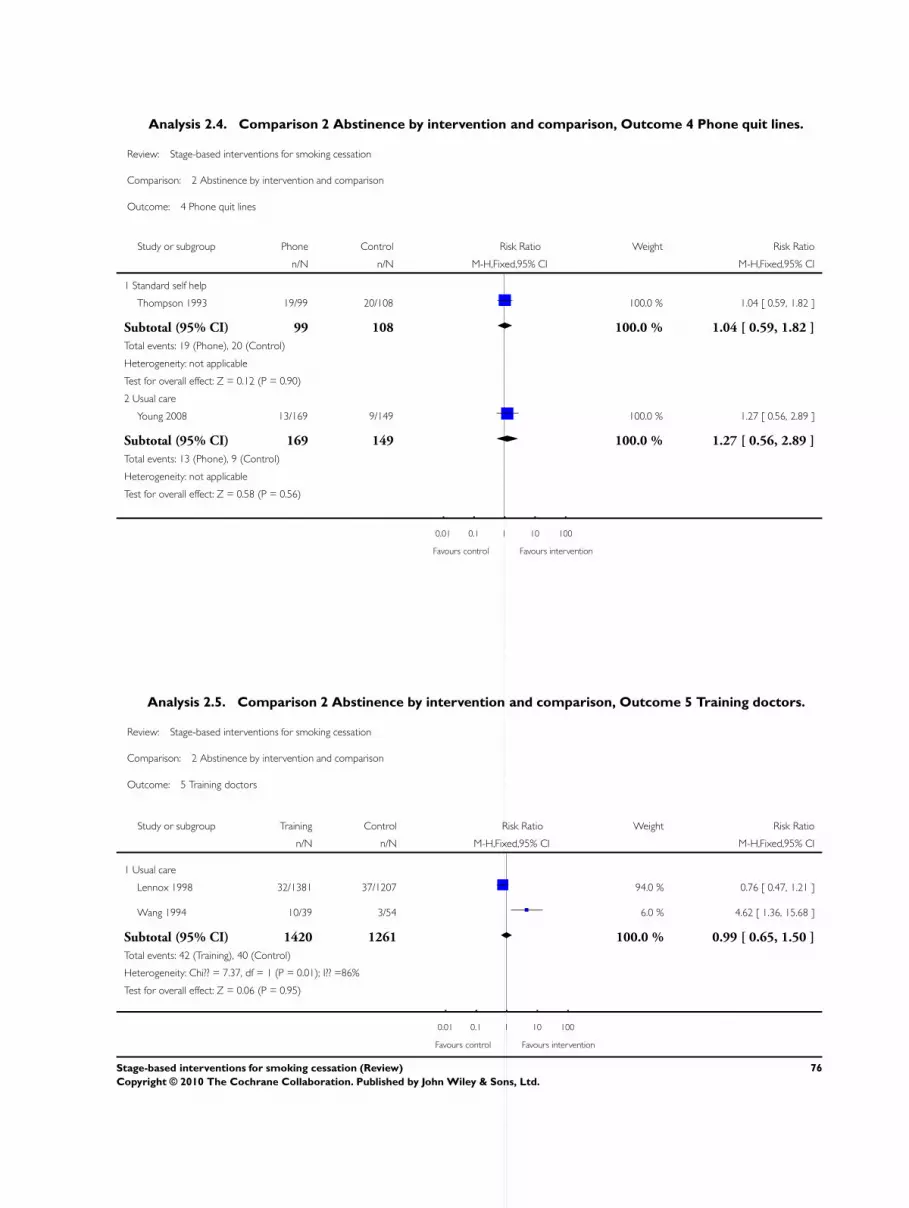
Analysis 2.4. Comparison 2 Abstinence by intervention and comparison, Outcome 4 Phone quit lines.
Review: Stage-based interventions for smoking cessation
Comparison: 2 Abstinence by intervention and comparison
Outcome: 4 Phone quit lines
Study or subgroup Phone Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Thompson 1993 19/99 20/108 100.0 % 1.04 [ 0.59, 1.82 ]
Subtotal (95% CI) 99 108 100.0 % 1.04 [ 0.59, 1.82 ]
Total events: 19 (Phone), 20 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.12 (P = 0.90)
2 Usual care
Young 2008 13/169 9/149 100.0 % 1.27 [ 0.56, 2.89 ]
Subtotal (95% CI) 169 149 100.0 % 1.27 [ 0.56, 2.89 ]
Total events: 13 (Phone), 9 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.58 (P = 0.56)
0.01 0.1 1 10 100
Favours control Favours intervention
Analysis 2.5. Comparison 2 Abstinence by intervention and comparison, Outcome 5 Training doctors.
Review: Stage-based interventions for smoking cessation
Comparison: 2 Abstinence by intervention and comparison
Outcome: 5 Training doctors
Study or subgroup Training Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Usual care
Lennox 1998 32/1381 37/1207 94.0 % 0.76 [ 0.47, 1.21 ]
Wang 1994 10/39 3/54 6.0 % 4.62 [ 1.36, 15.68 ]
Subtotal (95% CI) 1420 1261 100.0 % 0.99 [ 0.65, 1.50 ]
Total events: 42 (Training), 40 (Control)
Heterogeneity: Chi?? = 7.37, df = 1 (P = 0.01); I?? =86%
Test for overall effect: Z = 0.06 (P = 0.95)
0.01 0.1 1 10 100
Favours control Favours intervention
76Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.6. Comparison 2 Abstinence by intervention and comparison, Outcome 6 Training lay supporters.
Review: Stage-based interventions for smoking cessation
Comparison: 2 Abstinence by intervention and comparison
Outcome: 6 Training lay supporters
Study or subgroup training Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Patten 2004 3/30 2/30 100.0 % 1.50 [ 0.27, 8.34 ]
Subtotal (95% CI) 30 30 100.0 % 1.50 [ 0.27, 8.34 ]
Total events: 3 (training), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.46 (P = 0.64)
0.01 0.1 1 10 100
Favours control Favours intervention
Analysis 2.7. Comparison 2 Abstinence by intervention and comparison, Outcome 7 Staged SH materials.
Review: Stage-based interventions for smoking cessation
Comparison: 2 Abstinence by intervention and comparison
Outcome: 7 Staged SH materials
Study or subgroup SH materials Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Assessment only
Pallonen 1994 15/233 7/142 100.0 % 1.31 [ 0.55, 3.13 ]
Subtotal (95% CI) 233 142 100.0 % 1.31 [ 0.55, 3.13 ]
Total events: 15 (SH materials), 7 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.60 (P = 0.55)
0.01 0.1 1 10 100
Favours control Favours intervention
77Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.1. Comparison 3 Validated abstinence, Outcome 1 Biochemically validated abstinence.
Review: Stage-based interventions for smoking cessation
Comparison: 3 Validated abstinence
Outcome: 1 Biochemically validated abstinence
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Aveyard 2003 15/683 10/690 3.9 % 1.52 [ 0.69, 3.35 ]
Bobo 1998 20/288 16/287 6.3 % 1.25 [ 0.66, 2.35 ]
Chouinard 2005 26/108 7/156 2.3 % 5.37 [ 2.42, 11.91 ]
Hennrikus 2005 66/666 59/673 23.2 % 1.13 [ 0.81, 1.58 ]
Lennox 2001 30/870 37/869 14.6 % 0.81 [ 0.51, 1.30 ]
McBride 1999 16/288 13/292 5.1 % 1.25 [ 0.61, 2.55 ]
Mermelstein 2003 106/381 108/375 43.0 % 0.97 [ 0.77, 1.21 ]
Nakamura 2004 18/500 4/477 1.6 % 4.29 [ 1.46, 12.59 ]
Total (95% CI) 3784 3819 100.0 % 1.19 [ 1.02, 1.39 ]
Total events: 297 (Intervention), 254 (Control)
Heterogeneity: Chi?? = 25.41, df = 7 (P = 0.00064); I?? =72%
Test for overall effect: Z = 2.20 (P = 0.028)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours controll Favours intervention
78Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Validated abstinence, Outcome 2 Self-reported abstinence.
Review: Stage-based interventions for smoking cessation
Comparison: 3 Validated abstinence
Outcome: 2 Self-reported abstinence
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Aveyard 1999 53/683 46/452 7.5 % 0.76 [ 0.52, 1.11 ]
Borland 2003 24/523 21/527 2.8 % 1.15 [ 0.65, 2.04 ]
Borland 2004 61/382 35/390 4.7 % 1.78 [ 1.20, 2.63 ]
Curry 1995 7/329 7/328 1.0 % 1.00 [ 0.35, 2.81 ]
Davies 2005 10/127 7/121 1.0 % 1.36 [ 0.54, 3.46 ]
Dijkstra 1999 14/420 10/208 1.8 % 0.69 [ 0.31, 1.53 ]
Escoffery 2004 9/35 6/35 0.8 % 1.50 [ 0.60, 3.77 ]
Etter 2004 163/1467 154/1467 20.9 % 1.06 [ 0.86, 1.30 ]
Hann??ver 2009 2/151 0/187 0.1 % 6.18 [ 0.30, 127.85 ]
Hollis 2005 54/281 25/284 3.4 % 2.18 [ 1.40, 3.41 ]
Lawrence 2005 29/629 12/289 2.2 % 1.11 [ 0.57, 2.14 ]
Lennox 1998 32/1381 37/1207 5.4 % 0.76 [ 0.47, 1.21 ]
Manfredi 2004 57/527 61/541 8.2 % 0.96 [ 0.68, 1.35 ]
Meyer 2008 24/890 5/609 0.8 % 3.28 [ 1.26, 8.56 ]
Meysman 2010 28/178 14/180 1.9 % 2.02 [ 1.10, 3.71 ]
O’Neill 2000 5/31 4/34 0.5 % 1.37 [ 0.40, 4.65 ]
Pallonen 1994 15/233 7/142 1.2 % 1.31 [ 0.55, 3.13 ]
Patten 2004 3/30 2/30 0.3 % 1.50 [ 0.27, 8.34 ]
Prochaska 2001a 96/1346 136/2761 12.1 % 1.45 [ 1.12, 1.86 ]
Prochaska 2001b 28/362 16/350 2.2 % 1.69 [ 0.93, 3.07 ]
Prochaska 2004 29/349 18/362 2.4 % 1.67 [ 0.95, 2.95 ]
Prochaska 2005 85/352 81/437 9.8 % 1.30 [ 0.99, 1.71 ]
Prochaska 2008 10/48 8/48 1.1 % 1.25 [ 0.54, 2.89 ]
Prokhorov 2008 26/219 17/207 2.4 % 1.45 [ 0.81, 2.58 ]
Schumann 2006 15/240 16/245 2.1 % 0.96 [ 0.48, 1.89 ]
Stotts 2002 10/134 14/135 1.9 % 0.72 [ 0.33, 1.56 ]
0.01 0.1 1 10 100
Favours control Favours intervention
(Continued . . . )
79Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wang 1994 10/39 3/54 0.3 % 4.62 [ 1.36, 15.68 ]
Young 2008 13/169 9/149 1.3 % 1.27 [ 0.56, 2.89 ]
Total (95% CI) 11555 11779 100.0 % 1.25 [ 1.14, 1.37 ]
Total events: 912 (Intervention), 771 (Control)
Heterogeneity: Chi?? = 45.72, df = 27 (P = 0.01); I?? =41%
Test for overall effect: Z = 4.77 (P < 0.00001)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
Analysis 3.3. Comparison 3 Validated abstinence, Outcome 3 ’Bogus pipeline’.
Review: Stage-based interventions for smoking cessation
Comparison: 3 Validated abstinence
Outcome: 3 ’Bogus pipeline’
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Dijkstra 1998 26/1155 4/385 12.8 % 2.17 [ 0.76, 6.17 ]
Pieterse 2001 22/269 8/261 17.3 % 2.67 [ 1.21, 5.89 ]
Prochaska 1993 53/570 9/186 29.0 % 1.92 [ 0.97, 3.82 ]
Thompson 1993 19/99 20/108 40.9 % 1.04 [ 0.59, 1.82 ]
Total (95% CI) 2093 940 100.0 % 1.72 [ 1.20, 2.46 ]
Total events: 120 (Intervention), 41 (Control)
Heterogeneity: Chi?? = 4.55, df = 3 (P = 0.21); I?? =34%
Test for overall effect: Z = 2.97 (P = 0.0030)
0.01 0.1 1 10 100
Favours control Favours intervention
80Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.1. Comparison 4 Missing data testing, Outcome 1 Intervention ITT versus control per protocol.
Review: Stage-based interventions for smoking cessation
Comparison: 4 Missing data testing
Outcome: 1 Intervention ITT versus control per protocol
Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Borland 2003 24/523 21/416 3.9 % 0.91 [ 0.51, 1.61 ]
Borland 2004 61/382 83/278 16.1 % 0.53 [ 0.40, 0.72 ]
Curry 1995 7/329 7/324 1.2 % 0.98 [ 0.35, 2.78 ]
Dijkstra 1998 26/1155 4/250 1.1 % 1.41 [ 0.50, 4.00 ]
Dijkstra 1999 14/420 10/182 2.3 % 0.61 [ 0.27, 1.34 ]
Etter 2004 163/1467 154/1346 27.0 % 0.97 [ 0.79, 1.20 ]
Mermelstein 2003 106/381 108/354 18.8 % 0.91 [ 0.73, 1.14 ]
Pallonen 1994 15/233 7/116 1.6 % 1.07 [ 0.45, 2.54 ]
Patten 2004 3/30 2/27 0.4 % 1.35 [ 0.24, 7.48 ]
Prochaska 1993 13/192 9/166 1.6 % 1.25 [ 0.55, 2.85 ]
Prochaska 2001a 96/1346 136/1769 19.7 % 0.93 [ 0.72, 1.19 ]
Prochaska 2001b 28/362 16/252 3.2 % 1.22 [ 0.67, 2.20 ]
Schumann 2006 15/240 16/175 3.1 % 0.68 [ 0.35, 1.35 ]
Total (95% CI) 7060 5655 100.0 % 0.88 [ 0.79, 0.98 ]
Total events: 571 (Experimental), 573 (Control)
Heterogeneity: Chi?? = 16.79, df = 12 (P = 0.16); I?? =29%
Test for overall effect: Z = 2.28 (P = 0.022)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
81Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.2. Comparison 4 Missing data testing, Outcome 2 Intervention ITT versus control ITT.
Review: Stage-based interventions for smoking cessation
Comparison: 4 Missing data testing
Outcome: 2 Intervention ITT versus control ITT
Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Borland 2003 24/523 21/527 4.3 % 1.15 [ 0.65, 2.04 ]
Borland 2004 61/382 35/390 7.1 % 1.78 [ 1.20, 2.63 ]
Curry 1995 7/329 7/328 1.4 % 1.00 [ 0.35, 2.81 ]
Dijkstra 1998 26/1155 4/385 1.2 % 2.17 [ 0.76, 6.17 ]
Dijkstra 1999 14/420 10/208 2.7 % 0.69 [ 0.31, 1.53 ]
Etter 2004 163/1467 154/1467 31.4 % 1.06 [ 0.86, 1.30 ]
Mermelstein 2003 106/381 108/375 22.2 % 0.97 [ 0.77, 1.21 ]
Pallonen 1994 15/233 7/142 1.8 % 1.31 [ 0.55, 3.13 ]
Patten 2004 3/30 2/30 0.4 % 1.50 [ 0.27, 8.34 ]
Prochaska 1993 53/570 9/186 2.8 % 1.92 [ 0.97, 3.82 ]
Prochaska 2001a 96/1346 136/2761 18.2 % 1.45 [ 1.12, 1.86 ]
Prochaska 2001b 28/362 16/350 3.3 % 1.69 [ 0.93, 3.07 ]
Schumann 2006 15/240 16/245 3.2 % 0.96 [ 0.48, 1.89 ]
Total (95% CI) 7438 7394 100.0 % 1.21 [ 1.09, 1.36 ]
Total events: 611 (Experimental), 525 (Control)
Heterogeneity: Chi?? = 17.82, df = 12 (P = 0.12); I?? =33%
Test for overall effect: Z = 3.40 (P = 0.00067)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
82Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.1. Comparison 5 Any stage-based intervention vs control, Outcome 1 Abstinence at longest
follow up.
Review: Stage-based interventions for smoking cessation
Comparison: 5 Any stage-based intervention vs control
Outcome: 1 Abstinence at longest follow up
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Aveyard 1999 53/547 46/542 4.5 % 1.14 [ 0.78, 1.66 ]
Aveyard 2003 15/683 10/690 1.0 % 1.52 [ 0.69, 3.35 ]
Bobo 1998 20/288 16/287 1.6 % 1.25 [ 0.66, 2.35 ]
Borland 2003 24/523 21/527 2.0 % 1.15 [ 0.65, 2.04 ]
Borland 2004 61/382 35/390 3.4 % 1.78 [ 1.20, 2.63 ]
Chouinard 2005 26/108 7/56 0.9 % 1.93 [ 0.89, 4.16 ]
Curry 1995 7/329 7/328 0.7 % 1.00 [ 0.35, 2.81 ]
Davies 2005 10/127 7/121 0.7 % 1.36 [ 0.54, 3.46 ]
Dijkstra 1998 26/1155 4/385 0.6 % 2.17 [ 0.76, 6.17 ]
Dijkstra 1999 14/420 10/208 1.3 % 0.69 [ 0.31, 1.53 ]
Escoffery 2004 9/35 6/35 0.6 % 1.50 [ 0.60, 3.77 ]
Etter 2004 163/1467 154/1467 15.0 % 1.06 [ 0.86, 1.30 ]
Hann??ver 2009 2/151 0/187 0.0 % 6.18 [ 0.30, 127.85 ]
Hennrikus 2005 66/666 59/673 5.7 % 1.13 [ 0.81, 1.58 ]
Hollis 2005 54/281 25/284 2.4 % 2.18 [ 1.40, 3.41 ]
Lawrence 2005 29/629 12/289 1.6 % 1.11 [ 0.57, 2.14 ]
Lennox 1998 32/1381 37/1207 3.8 % 0.76 [ 0.47, 1.21 ]
Lennox 2001 30/870 37/869 3.6 % 0.81 [ 0.51, 1.30 ]
Manfredi 2004 57/527 61/541 5.9 % 0.96 [ 0.68, 1.35 ]
McBride 1999 16/288 13/292 1.3 % 1.25 [ 0.61, 2.55 ]
Mermelstein 2003 106/381 108/375 10.6 % 0.97 [ 0.77, 1.21 ]
Meyer 2008 24/890 5/609 0.6 % 3.28 [ 1.26, 8.56 ]
Meysman 2010 28/178 14/180 1.4 % 2.02 [ 1.10, 3.71 ]
Nakamura 2004 18/500 4/477 0.4 % 4.29 [ 1.46, 12.59 ]
O’Neill 2000 5/31 4/34 0.4 % 1.37 [ 0.40, 4.65 ]
0.01 0.1 1 10 100
Favours control Favours intervention
(Continued . . . )
83Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Pallonen 1994 15/233 7/142 0.8 % 1.31 [ 0.55, 3.13 ]
Patten 2004 3/30 2/30 0.2 % 1.50 [ 0.27, 8.34 ]
Pieterse 2001 22/269 8/261 0.8 % 2.67 [ 1.21, 5.89 ]
Prochaska 1993 13/192 9/186 0.9 % 1.40 [ 0.61, 3.20 ]
Prochaska 2001a 96/1346 136/2761 8.7 % 1.45 [ 1.12, 1.86 ]
Prochaska 2001b 28/362 16/350 1.6 % 1.69 [ 0.93, 3.07 ]
Prochaska 2004 29/349 18/362 1.7 % 1.67 [ 0.95, 2.95 ]
Prochaska 2005 85/352 81/437 7.0 % 1.30 [ 0.99, 1.71 ]
Prochaska 2008 10/48 8/48 0.8 % 1.25 [ 0.54, 2.89 ]
Prokhorov 2008 26/219 17/207 1.7 % 1.45 [ 0.81, 2.58 ]
Schumann 2006 15/240 16/245 1.5 % 0.96 [ 0.48, 1.89 ]
Stotts 2002 10/134 14/135 1.4 % 0.72 [ 0.33, 1.56 ]
Thompson 1993 19/99 20/108 1.9 % 1.04 [ 0.59, 1.82 ]
Wang 1994 10/39 3/54 0.2 % 4.62 [ 1.36, 15.68 ]
Young 2008 13/169 9/149 0.9 % 1.27 [ 0.56, 2.89 ]
Total (95% CI) 16918 16528 100.0 % 1.25 [ 1.16, 1.35 ]
Total events: 1289 (Intervention), 1066 (Control)
Heterogeneity: Chi?? = 59.49, df = 39 (P = 0.02); I?? =34%
Test for overall effect: Z = 5.72 (P < 0.00001)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
84Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.2. Comparison 5 Any stage-based intervention vs control, Outcome 2 Abstinence by comparison
condition.
Review: Stage-based interventions for smoking cessation
Comparison: 5 Any stage-based intervention vs control
Outcome: 2 Abstinence by comparison condition
Study or subgroup Intervention Control Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self-help materials
Aveyard 2003 15/683 10/690 1.52 [ 0.69, 3.35 ]
Borland 2003 24/523 21/527 1.15 [ 0.65, 2.04 ]
Borland 2004 61/382 35/390 1.78 [ 1.20, 2.63 ]
Dijkstra 1999 14/420 7/215 1.02 [ 0.42, 2.50 ]
Hann??ver 2009 2/151 0/187 6.18 [ 0.30, 127.85 ]
Hennrikus 2005 66/666 59/673 1.13 [ 0.81, 1.58 ]
Lennox 2001 30/870 37/869 0.81 [ 0.51, 1.30 ]
Mermelstein 2003 106/381 108/375 0.97 [ 0.77, 1.21 ]
Meysman 2010 28/178 14/180 2.02 [ 1.10, 3.71 ]
Patten 2004 3/30 2/30 1.50 [ 0.27, 8.34 ]
Prochaska 1993 53/570 9/186 1.92 [ 0.97, 3.82 ]
Thompson 1993 19/99 20/108 1.04 [ 0.59, 1.82 ]
Subtotal (95% CI) 4953 4430 1.19 [ 1.04, 1.37 ]
Total events: 421 (Intervention), 322 (Control)
Heterogeneity: Chi?? = 16.69, df = 11 (P = 0.12); I?? =34%
Test for overall effect: Z = 2.53 (P = 0.011)
2 Usual care
Aveyard 1999 53/547 46/542 1.14 [ 0.78, 1.66 ]
Bobo 1998 20/288 16/287 1.25 [ 0.66, 2.35 ]
Chouinard 2005 26/108 7/56 1.93 [ 0.89, 4.16 ]
Davies 2005 10/127 7/121 1.36 [ 0.54, 3.46 ]
Lawrence 2005 29/629 12/289 1.11 [ 0.57, 2.14 ]
Lennox 1998 32/1381 37/1207 0.76 [ 0.47, 1.21 ]
McBride 1999 16/288 13/292 1.25 [ 0.61, 2.55 ]
Pieterse 2001 22/269 8/261 2.67 [ 1.21, 5.89 ]
Prokhorov 2008 26/219 17/207 1.45 [ 0.81, 2.58 ]
0.01 0.1 1 10 100
Favours control Favours intervention
(Continued . . . )
85Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Intervention Control Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Stotts 2002 10/134 14/135 0.72 [ 0.33, 1.56 ]
Wang 1994 10/39 3/54 4.62 [ 1.36, 15.68 ]
Young 2008 0/55 0/34 0.0 [ 0.0, 0.0 ]
Subtotal (95% CI) 4084 3485 1.23 [ 1.02, 1.48 ]
Total events: 254 (Intervention), 180 (Control)
Heterogeneity: Chi?? = 16.08, df = 10 (P = 0.10); I?? =38%
Test for overall effect: Z = 2.19 (P = 0.029)
3 Assessment only
Curry 1995 7/329 7/328 1.00 [ 0.35, 2.81 ]
Dijkstra 1998 26/1155 4/385 2.17 [ 0.76, 6.17 ]
Escoffery 2004 9/35 6/35 1.50 [ 0.60, 3.77 ]
Etter 2004 163/1467 154/1467 1.06 [ 0.86, 1.30 ]
Hollis 2005 54/281 25/284 2.18 [ 1.40, 3.41 ]
Manfredi 2004 57/527 61/541 0.96 [ 0.68, 1.35 ]
Meyer 2008 24/890 5/609 3.28 [ 1.26, 8.56 ]
Nakamura 2004 18/500 4/477 4.29 [ 1.46, 12.59 ]
O’Neill 2000 5/31 4/34 1.37 [ 0.40, 4.65 ]
Pallonen 1994 15/233 7/142 1.31 [ 0.55, 3.13 ]
Prochaska 2001a 96/1346 136/2761 1.45 [ 1.12, 1.86 ]
Prochaska 2001b 28/362 16/350 1.69 [ 0.93, 3.07 ]
Prochaska 2004 29/349 18/362 1.67 [ 0.95, 2.95 ]
Prochaska 2005 85/352 81/437 1.30 [ 0.99, 1.71 ]
Prochaska 2008 10/48 8/48 1.25 [ 0.54, 2.89 ]
Schumann 2006 15/240 16/245 0.96 [ 0.48, 1.89 ]
Subtotal (95% CI) 8145 8505 1.33 [ 1.19, 1.48 ]
Total events: 641 (Intervention), 552 (Control)
Heterogeneity: Chi?? = 24.71, df = 15 (P = 0.05); I?? =39%
Test for overall effect: Z = 5.07 (P < 0.00001)
0.01 0.1 1 10 100
Favours control Favours intervention
86Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.1. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 1 Expert systems.
Review: Stage-based interventions for smoking cessation
Comparison: 6 PPA at 6 or 12 m by intervention and comparison
Outcome: 1 Expert systems
Study or subgroup Expert system Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Aveyard 2003 23/683 15/690 1.6 % 1.55 [ 0.82, 2.94 ]
Borland 2003 91/523 92/527 10.1 % 1.00 [ 0.77, 1.30 ]
Borland 2004 84/382 82/390 8.9 % 1.05 [ 0.80, 1.37 ]
Dijkstra 1999 14/420 7/215 1.0 % 1.02 [ 0.42, 2.50 ]
Lennox 2001 30/870 37/869 4.1 % 0.81 [ 0.51, 1.30 ]
Prochaska 1993 31/192 18/186 2.0 % 1.67 [ 0.97, 2.88 ]
Subtotal (95% CI) 3070 2877 27.8 % 1.07 [ 0.91, 1.25 ]
Total events: 273 (Expert system), 251 (Control)
Heterogeneity: Chi?? = 5.48, df = 5 (P = 0.36); I?? =9%
Test for overall effect: Z = 0.81 (P = 0.42)
2 Usual care
McBride 1999 30/288 40/292 4.4 % 0.76 [ 0.49, 1.19 ]
Stotts 2002 10/134 14/135 1.5 % 0.72 [ 0.33, 1.56 ]
Subtotal (95% CI) 422 427 5.9 % 0.75 [ 0.51, 1.10 ]
Total events: 40 (Expert system), 54 (Control)
Heterogeneity: Chi?? = 0.01, df = 1 (P = 0.90); I?? =0.0%
Test for overall effect: Z = 1.46 (P = 0.14)
3 Assessment only
Curry 1995 30/329 36/328 4.0 % 0.83 [ 0.52, 1.32 ]
Dijkstra 1998 77/1155 28/385 4.6 % 0.92 [ 0.60, 1.39 ]
Etter 2004 163/1467 154/1467 17.0 % 1.06 [ 0.86, 1.30 ]
Hollis 2005 64/281 31/284 3.4 % 2.09 [ 1.40, 3.10 ]
Meyer 2008 44/488 38/609 3.7 % 1.44 [ 0.95, 2.19 ]
Prochaska 2001a 154/1349 284/2774 20.5 % 1.12 [ 0.93, 1.34 ]
Prochaska 2001b 55/362 37/350 4.1 % 1.44 [ 0.97, 2.12 ]
Prochaska 2004 31/349 22/362 2.4 % 1.46 [ 0.86, 2.47 ]
Prochaska 2005 64/379 51/473 5.0 % 1.57 [ 1.11, 2.21 ]
Schumann 2006 16/240 15/245 1.6 % 1.09 [ 0.55, 2.15 ]
0.1 0.2 0.5 1 2 5 10
Favours control Favours intervention
(Continued . . . )
87Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Expert system Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Subtotal (95% CI) 6399 7277 66.3 % 1.20 [ 1.09, 1.33 ]
Total events: 698 (Expert system), 696 (Control)
Heterogeneity: Chi?? = 18.09, df = 9 (P = 0.03); I?? =50%
Test for overall effect: Z = 3.58 (P = 0.00034)
Total (95% CI) 9891 10581 100.0 % 1.14 [ 1.05, 1.24 ]
Total events: 1011 (Expert system), 1001 (Control)
Heterogeneity: Chi?? = 29.90, df = 17 (P = 0.03); I?? =43%
Test for overall effect: Z = 3.06 (P = 0.0022)
0.1 0.2 0.5 1 2 5 10
Favours control Favours intervention
Analysis 6.2. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 2 Individual
counselling.
Review: Stage-based interventions for smoking cessation
Comparison: 6 PPA at 6 or 12 m by intervention and comparison
Outcome: 2 Individual counselling
Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Hann??ver 2009 13/151 8/187 1.9 % 2.01 [ 0.86, 4.73 ]
Hennrikus 2005 66/666 59/673 15.9 % 1.13 [ 0.81, 1.58 ]
Subtotal (95% CI) 817 860 17.8 % 1.23 [ 0.90, 1.67 ]
Total events: 79 (Experimental), 67 (Control)
Heterogeneity: Chi?? = 1.52, df = 1 (P = 0.22); I?? =34%
Test for overall effect: Z = 1.29 (P = 0.20)
2 Usual care
Bobo 1998 20/288 16/287 4.3 % 1.25 [ 0.66, 2.35 ]
Chouinard 2005 38/108 11/56 3.9 % 1.79 [ 0.99, 3.23 ]
Davies 2005 10/127 7/121 1.9 % 1.36 [ 0.54, 3.46 ]
Lawrence 2005 14/305 10/289 2.8 % 1.33 [ 0.60, 2.94 ]
Mermelstein 2003 112/381 117/375 31.9 % 0.94 [ 0.76, 1.17 ]
0.005 0.1 1 10 200
Favours control Favours intervention
(Continued . . . )
88Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Pieterse 2001 36/269 19/261 5.2 % 1.84 [ 1.08, 3.12 ]
Prokhorov 2008 26/219 17/207 4.7 % 1.45 [ 0.81, 2.58 ]
Subtotal (95% CI) 1697 1596 54.9 % 1.19 [ 1.01, 1.41 ]
Total events: 256 (Experimental), 197 (Control)
Heterogeneity: Chi?? = 9.53, df = 6 (P = 0.15); I?? =37%
Test for overall effect: Z = 2.04 (P = 0.041)
3 Assessment only
Manfredi 2004 59/527 59/541 15.8 % 1.03 [ 0.73, 1.44 ]
Meyer 2008 37/402 38/609 8.2 % 1.48 [ 0.95, 2.28 ]
Nakamura 2004 68/500 12/477 3.3 % 5.41 [ 2.96, 9.86 ]
Subtotal (95% CI) 1429 1627 27.3 % 1.70 [ 1.34, 2.14 ]
Total events: 164 (Experimental), 109 (Control)
Heterogeneity: Chi?? = 23.05, df = 2 (P<0.00001); I?? =91%
Test for overall effect: Z = 4.40 (P = 0.000011)
Total (95% CI) 3943 4083 100.0 % 1.33 [ 1.18, 1.51 ]
Total events: 499 (Experimental), 373 (Control)
Heterogeneity: Chi?? = 37.58, df = 11 (P = 0.00009); I?? =71%
Test for overall effect: Z = 4.53 (P < 0.00001)
Test for subgroup differences: Chi?? = 0.0, df = 2 (P = 0.0), I?? =0.0%
0.005 0.1 1 10 200
Favours control Favours intervention
89Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
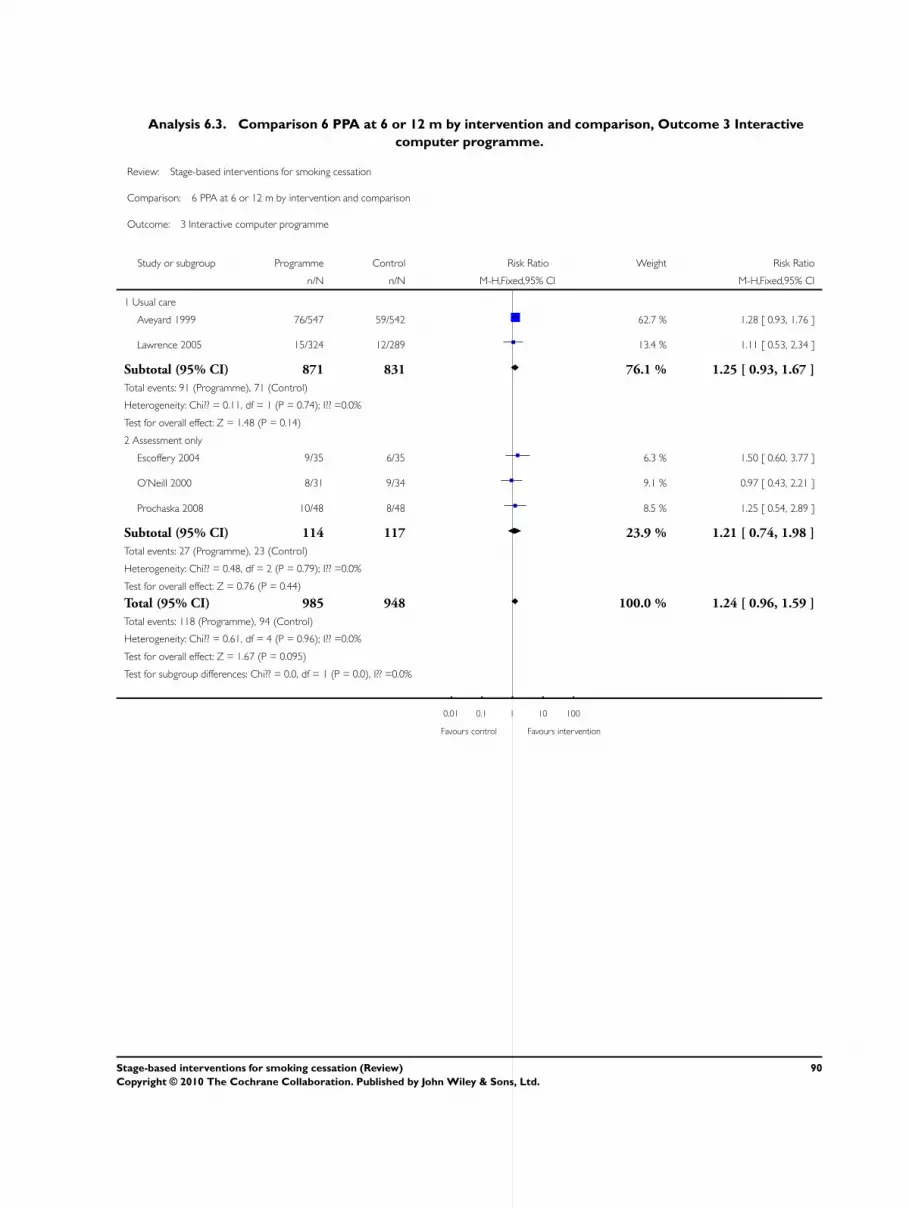
Analysis 6.3. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 3 Interactive
computer programme.
Review: Stage-based interventions for smoking cessation
Comparison: 6 PPA at 6 or 12 m by intervention and comparison
Outcome: 3 Interactive computer programme
Study or subgroup Programme Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Usual care
Aveyard 1999 76/547 59/542 62.7 % 1.28 [ 0.93, 1.76 ]
Lawrence 2005 15/324 12/289 13.4 % 1.11 [ 0.53, 2.34 ]
Subtotal (95% CI) 871 831 76.1 % 1.25 [ 0.93, 1.67 ]
Total events: 91 (Programme), 71 (Control)
Heterogeneity: Chi?? = 0.11, df = 1 (P = 0.74); I?? =0.0%
Test for overall effect: Z = 1.48 (P = 0.14)
2 Assessment only
Escoffery 2004 9/35 6/35 6.3 % 1.50 [ 0.60, 3.77 ]
O’Neill 2000 8/31 9/34 9.1 % 0.97 [ 0.43, 2.21 ]
Prochaska 2008 10/48 8/48 8.5 % 1.25 [ 0.54, 2.89 ]
Subtotal (95% CI) 114 117 23.9 % 1.21 [ 0.74, 1.98 ]
Total events: 27 (Programme), 23 (Control)
Heterogeneity: Chi?? = 0.48, df = 2 (P = 0.79); I?? =0.0%
Test for overall effect: Z = 0.76 (P = 0.44)
Total (95% CI) 985 948 100.0 % 1.24 [ 0.96, 1.59 ]
Total events: 118 (Programme), 94 (Control)
Heterogeneity: Chi?? = 0.61, df = 4 (P = 0.96); I?? =0.0%
Test for overall effect: Z = 1.67 (P = 0.095)
Test for subgroup differences: Chi?? = 0.0, df = 1 (P = 0.0), I?? =0.0%
0.01 0.1 1 10 100
Favours control Favours intervention
90Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.4. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 4 Phone quit lines.
Review: Stage-based interventions for smoking cessation
Comparison: 6 PPA at 6 or 12 m by intervention and comparison
Outcome: 4 Phone quit lines
Study or subgroup Phone Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Thompson 1993 19/99 20/108 66.7 % 1.04 [ 0.59, 1.82 ]
Subtotal (95% CI) 99 108 66.7 % 1.04 [ 0.59, 1.82 ]
Total events: 19 (Phone), 20 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.12 (P = 0.90)
2 Usual care
Young 2008 13/169 9/149 33.3 % 1.27 [ 0.56, 2.89 ]
Subtotal (95% CI) 169 149 33.3 % 1.27 [ 0.56, 2.89 ]
Total events: 13 (Phone), 9 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.58 (P = 0.56)
Total (95% CI) 268 257 100.0 % 1.12 [ 0.70, 1.78 ]
Total events: 32 (Phone), 29 (Control)
Heterogeneity: Chi?? = 0.17, df = 1 (P = 0.68); I?? =0.0%
Test for overall effect: Z = 0.46 (P = 0.65)
Test for subgroup differences: Chi?? = 0.0, df = 1 (P = 0.0), I?? =0.0%
0.01 0.1 1 10 100
Favours control Favours intervention
91Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.5. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 5 Training doctors.
Review: Stage-based interventions for smoking cessation
Comparison: 6 PPA at 6 or 12 m by intervention and comparison
Outcome: 5 Training doctors
Study or subgroup Training Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Usual care
Lennox 1998 100/1381 93/1207 97.5 % 0.94 [ 0.72, 1.23 ]
Wang 1994 10/39 3/54 2.5 % 4.62 [ 1.36, 15.68 ]
Total (95% CI) 1420 1261 100.0 % 1.03 [ 0.79, 1.34 ]
Total events: 110 (Training), 96 (Control)
Heterogeneity: Chi?? = 6.22, df = 1 (P = 0.01); I?? =84%
Test for overall effect: Z = 0.23 (P = 0.82)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
Analysis 6.6. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 6 Training lay
supporters.
Review: Stage-based interventions for smoking cessation
Comparison: 6 PPA at 6 or 12 m by intervention and comparison
Outcome: 6 Training lay supporters
Study or subgroup training Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Patten 2004 3/30 2/30 100.0 % 1.50 [ 0.27, 8.34 ]
Total (95% CI) 30 30 100.0 % 1.50 [ 0.27, 8.34 ]
Total events: 3 (training), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.46 (P = 0.64)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
92Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.7. Comparison 6 PPA at 6 or 12 m by intervention and comparison, Outcome 7 Staged SH
materials.
Review: Stage-based interventions for smoking cessation
Comparison: 6 PPA at 6 or 12 m by intervention and comparison
Outcome: 7 Staged SH materials
Study or subgroup SH materials Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Assessment only
Pallonen 1994 19/233 8/142 100.0 % 1.45 [ 0.65, 3.22 ]
Total (95% CI) 233 142 100.0 % 1.45 [ 0.65, 3.22 ]
Total events: 19 (SH materials), 8 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.91 (P = 0.36)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
Analysis 7.1. Comparison 7 Per protocol analyses, Outcome 1 Expert systems.
Review: Stage-based interventions for smoking cessation
Comparison: 7 Per protocol analyses
Outcome: 1 Expert systems
Study or subgroup Expert system Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Aveyard 2003 15/471 10/524 1.7 % 1.67 [ 0.76, 3.68 ]
Borland 2003 24/402 21/416 3.8 % 1.18 [ 0.67, 2.09 ]
Borland 2004 61/244 33/278 5.7 % 2.11 [ 1.43, 3.10 ]
Dijkstra 1999 14/367 7/201 1.7 % 1.10 [ 0.45, 2.67 ]
Lennox 2001 30/857 37/846 6.8 % 0.80 [ 0.50, 1.28 ]
Prochaska 1993 13/175 9/166 1.7 % 1.37 [ 0.60, 3.12 ]
Subtotal (95% CI) 2516 2431 21.4 % 1.35 [ 1.08, 1.70 ]
0.1 0.2 0.5 1 2 5 10
Favours control Favours intervention
(Continued . . . )
93Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Expert system Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Total events: 157 (Expert system), 117 (Control)
Heterogeneity: Chi?? = 10.47, df = 5 (P = 0.06); I?? =52%
Test for overall effect: Z = 2.60 (P = 0.0094)
2 Usual care
McBride 1999 16/283 14/277 2.6 % 1.12 [ 0.56, 2.25 ]
Stotts 2002 10/82 14/82 2.6 % 0.71 [ 0.34, 1.51 ]
Subtotal (95% CI) 365 359 5.2 % 0.92 [ 0.55, 1.53 ]
Total events: 26 (Expert system), 28 (Control)
Heterogeneity: Chi?? = 0.74, df = 1 (P = 0.39); I?? =0.0%
Test for overall effect: Z = 0.33 (P = 0.74)
3 Assessment only
Curry 1995 7/323 7/328 1.3 % 1.02 [ 0.36, 2.86 ]
Dijkstra 1998 26/740 4/250 1.1 % 2.20 [ 0.77, 6.23 ]
Etter 2004 163/1261 154/1310 27.8 % 1.10 [ 0.89, 1.35 ]
Hollis 2005 54/226 25/222 4.6 % 2.12 [ 1.37, 3.28 ]
Meyer 2008 14/232 5/341 0.7 % 4.12 [ 1.50, 11.27 ]
Prochaska 2001a 96/802 136/1769 15.6 % 1.56 [ 1.22, 1.99 ]
Prochaska 2001b 28/251 16/252 2.9 % 1.76 [ 0.98, 3.17 ]
Prochaska 2004 29/191 18/218 3.1 % 1.84 [ 1.06, 3.20 ]
Prochaska 2005 85/352 81/437 13.3 % 1.30 [ 0.99, 1.71 ]
Schumann 2006 16/175 15/153 2.9 % 0.93 [ 0.48, 1.82 ]
Subtotal (95% CI) 4553 5280 73.4 % 1.39 [ 1.24, 1.57 ]
Total events: 518 (Expert system), 461 (Control)
Heterogeneity: Chi?? = 18.11, df = 9 (P = 0.03); I?? =50%
Test for overall effect: Z = 5.48 (P < 0.00001)
Total (95% CI) 7434 8070 100.0 % 1.36 [ 1.23, 1.51 ]
Total events: 701 (Expert system), 606 (Control)
Heterogeneity: Chi?? = 31.74, df = 17 (P = 0.02); I?? =46%
Test for overall effect: Z = 5.86 (P < 0.00001)
0.1 0.2 0.5 1 2 5 10
Favours control Favours intervention
94Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.2. Comparison 7 Per protocol analyses, Outcome 2 Individual counselling.
Review: Stage-based interventions for smoking cessation
Comparison: 7 Per protocol analyses
Outcome: 2 Individual counselling
Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Hann??ver 2009 2/151 0/187 0.1 % 6.18 [ 0.30, 127.85 ]
Hennrikus 2005 66/501 59/551 17.7 % 1.23 [ 0.88, 1.71 ]
Meysman 2010 28/178 14/180 4.4 % 2.02 [ 1.10, 3.71 ]
Subtotal (95% CI) 830 918 22.2 % 1.42 [ 1.07, 1.89 ]
Total events: 96 (Experimental), 73 (Control)
Heterogeneity: Chi?? = 2.93, df = 2 (P = 0.23); I?? =32%
Test for overall effect: Z = 2.39 (P = 0.017)
2 Usual care
Bobo 1998 20/218 16/226 4.9 % 1.30 [ 0.69, 2.43 ]
Chouinard 2005 26/106 7/55 2.9 % 1.93 [ 0.89, 4.16 ]
Davies 2005 10/50 7/46 2.3 % 1.31 [ 0.55, 3.17 ]
Lawrence 2005 14/139 12/127 3.9 % 1.07 [ 0.51, 2.22 ]
Mermelstein 2003 106/372 108/354 34.8 % 0.93 [ 0.75, 1.17 ]
Pieterse 2001 22/144 8/151 2.5 % 2.88 [ 1.33, 6.27 ]
Prokhorov 2008 26/158 17/168 5.2 % 1.63 [ 0.92, 2.88 ]
Subtotal (95% CI) 1187 1127 56.5 % 1.19 [ 1.00, 1.42 ]
Total events: 224 (Experimental), 175 (Control)
Heterogeneity: Chi?? = 12.31, df = 6 (P = 0.06); I?? =51%
Test for overall effect: Z = 1.93 (P = 0.054)
3 Assessment only
Manfredi 2004 59/226 69/285 19.2 % 1.08 [ 0.80, 1.46 ]
Meyer 2008 10/224 5/609 0.8 % 5.44 [ 1.88, 15.73 ]
Nakamura 2004 18/476 4/447 1.3 % 4.23 [ 1.44, 12.39 ]
Subtotal (95% CI) 926 1341 21.3 % 1.44 [ 1.10, 1.89 ]
Total events: 87 (Experimental), 78 (Control)
Heterogeneity: Chi?? = 13.43, df = 2 (P = 0.001); I?? =85%
Test for overall effect: Z = 2.64 (P = 0.0082)
Total (95% CI) 2943 3386 100.0 % 1.29 [ 1.13, 1.48 ]
Total events: 407 (Experimental), 326 (Control)
Heterogeneity: Chi?? = 30.35, df = 12 (P = 0.002); I?? =60%
Test for overall effect: Z = 3.84 (P = 0.00012)
Test for subgroup differences: Chi?? = 0.0, df = 2 (P = 0.0), I?? =0.0%
0.005 0.1 1 10 200
Favours control Favours intervention
95Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.3. Comparison 7 Per protocol analyses, Outcome 3 Interactive computer programme.
Review: Stage-based interventions for smoking cessation
Comparison: 7 Per protocol analyses
Outcome: 3 Interactive computer programme
Study or subgroup Programme Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Usual care
Aveyard 1999 53/547 46/542 60.9 % 1.14 [ 0.78, 1.66 ]
Lawrence 2005 15/131 12/127 16.0 % 1.21 [ 0.59, 2.49 ]
Subtotal (95% CI) 678 669 76.9 % 1.16 [ 0.83, 1.61 ]
Total events: 68 (Programme), 58 (Control)
Heterogeneity: Chi?? = 0.02, df = 1 (P = 0.89); I?? =0.0%
Test for overall effect: Z = 0.85 (P = 0.39)
2 Assessment only
Escoffery 2004 9/26 6/29 7.5 % 1.67 [ 0.69, 4.06 ]
O’Neill 2000 5/27 4/29 5.1 % 1.34 [ 0.40, 4.48 ]
Prochaska 2008 10/48 8/48 10.5 % 1.25 [ 0.54, 2.89 ]
Subtotal (95% CI) 101 106 23.1 % 1.41 [ 0.82, 2.42 ]
Total events: 24 (Programme), 18 (Control)
Heterogeneity: Chi?? = 0.23, df = 2 (P = 0.89); I?? =0.0%
Test for overall effect: Z = 1.23 (P = 0.22)
Total (95% CI) 779 775 100.0 % 1.21 [ 0.91, 1.61 ]
Total events: 92 (Programme), 76 (Control)
Heterogeneity: Chi?? = 0.64, df = 4 (P = 0.96); I?? =0.0%
Test for overall effect: Z = 1.34 (P = 0.18)
Test for subgroup differences: Chi?? = 0.0, df = 1 (P = 0.0), I?? =0.0%
0.01 0.1 1 10 100
Favours control Favours intervention
96Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.4. Comparison 7 Per protocol analyses, Outcome 4 Phone quit lines.
Review: Stage-based interventions for smoking cessation
Comparison: 7 Per protocol analyses
Outcome: 4 Phone quit lines
Study or subgroup Phone Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Thompson 1993 19/99 20/108 65.1 % 1.04 [ 0.59, 1.82 ]
Subtotal (95% CI) 99 108 65.1 % 1.04 [ 0.59, 1.82 ]
Total events: 19 (Phone), 20 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.12 (P = 0.90)
2 Usual care
Young 2008 13/117 9/88 34.9 % 1.09 [ 0.49, 2.43 ]
Subtotal (95% CI) 117 88 34.9 % 1.09 [ 0.49, 2.43 ]
Total events: 13 (Phone), 9 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.20 (P = 0.84)
Total (95% CI) 216 196 100.0 % 1.05 [ 0.66, 1.67 ]
Total events: 32 (Phone), 29 (Control)
Heterogeneity: Chi?? = 0.01, df = 1 (P = 0.92); I?? =0.0%
Test for overall effect: Z = 0.22 (P = 0.82)
Test for subgroup differences: Chi?? = 0.0, df = 1 (P = 0.0), I?? =0.0%
0.01 0.1 1 10 100
Favours control Favours intervention
97Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.5. Comparison 7 Per protocol analyses, Outcome 5 Training doctors.
Review: Stage-based interventions for smoking cessation
Comparison: 7 Per protocol analyses
Outcome: 5 Training doctors
Study or subgroup Training Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Usual care
Lennox 1998 32/877 37/779 93.9 % 0.77 [ 0.48, 1.22 ]
Wang 1994 10/35 3/47 6.1 % 4.48 [ 1.33, 15.07 ]
Total (95% CI) 912 826 100.0 % 1.00 [ 0.66, 1.51 ]
Total events: 42 (Training), 40 (Control)
Heterogeneity: Chi?? = 7.10, df = 1 (P = 0.01); I?? =86%
Test for overall effect: Z = 0.02 (P = 0.98)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
Analysis 7.6. Comparison 7 Per protocol analyses, Outcome 6 Training lay supporters.
Review: Stage-based interventions for smoking cessation
Comparison: 7 Per protocol analyses
Outcome: 6 Training lay supporters
Study or subgroup training Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Standard self help
Patten 2004 3/27 2/27 100.0 % 1.50 [ 0.27, 8.28 ]
Total (95% CI) 27 27 100.0 % 1.50 [ 0.27, 8.28 ]
Total events: 3 (training), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.47 (P = 0.64)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
98Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.7. Comparison 7 Per protocol analyses, Outcome 7 Staged SH materials.
Review: Stage-based interventions for smoking cessation
Comparison: 7 Per protocol analyses
Outcome: 7 Staged SH materials
Study or subgroup SH materials Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Assessment only
Pallonen 1994 15/149 7/116 100.0 % 1.67 [ 0.70, 3.96 ]
Total (95% CI) 149 116 100.0 % 1.67 [ 0.70, 3.96 ]
Total events: 15 (SH materials), 7 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.16 (P = 0.25)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours control Favours intervention
Analysis 8.1. Comparison 8 Cluster randomized trials, Outcome 1 Individual counselling.
Review: Stage-based interventions for smoking cessation
Comparison: 8 Cluster randomized trials
Outcome: 1 Individual counselling
Study or subgroup log [Risk Ratio] Risk Ratio Weight Risk Ratio
(SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Standard Self help
Hann??ver 2009 1.821318 (1.5446) 0.3 % 6.18 [ 0.30, 127.57 ]
Hennrikus 2005 0.04879 (0.145968) 30.5 % 1.05 [ 0.79, 1.40 ]
Meysman 2010 0.703098 (0.310133) 6.8 % 2.02 [ 1.10, 3.71 ]
Subtotal (95% CI) 37.5 % 1.20 [ 0.92, 1.55 ]
Heterogeneity: Chi?? = 4.78, df = 2 (P = 0.09); I?? =58%
Test for overall effect: Z = 1.36 (P = 0.17)
2 Usual care
Bobo 1998 0.219665 (0.344366) 5.5 % 1.25 [ 0.63, 2.45 ]
Chouinard 2005 0.655407 (0.416246) 3.8 % 1.93 [ 0.85, 4.35 ]
0.01 0.1 1 10 100
Favours experimental Favours control
(Continued . . . )
99Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup log [Risk Ratio] Risk Ratio Weight Risk Ratio
(SE) IV,Fixed,95% CI IV,Fixed,95% CI
Davies 2005 0.307485 (0.47384) 2.9 % 1.36 [ 0.54, 3.44 ]
Lawrence 2005 0.100266 (0.401153) 4.0 % 1.11 [ 0.50, 2.43 ]
Mermelstein 2003 -0.03457 (0.172319) 21.9 % 0.97 [ 0.69, 1.35 ]
Pieterse 2001 0.982078 (0.403734) 4.0 % 2.67 [ 1.21, 5.89 ]
Prokhorov 2008 0.36853 (0.32769) 6.1 % 1.45 [ 0.76, 2.75 ]
Subtotal (95% CI) 48.1 % 1.24 [ 0.99, 1.56 ]
Heterogeneity: Chi?? = 7.17, df = 6 (P = 0.31); I?? =16%
Test for overall effect: Z = 1.85 (P = 0.064)
3 Assessment only
Manfredi 2004 -0.0416 (0.254389) 10.0 % 0.96 [ 0.58, 1.58 ]
Meyer 2008 1.108563 (0.544778) 2.2 % 3.03 [ 1.04, 8.81 ]
Nakamura 2004 1.456287 (0.549609) 2.2 % 4.29 [ 1.46, 12.60 ]
Subtotal (95% CI) 14.4 % 1.43 [ 0.94, 2.17 ]
Heterogeneity: Chi?? = 8.36, df = 2 (P = 0.02); I?? =76%
Test for overall effect: Z = 1.68 (P = 0.093)
Total (95% CI) 100.0 % 1.25 [ 1.07, 1.46 ]
Heterogeneity: Chi?? = 20.82, df = 12 (P = 0.05); I?? =42%
Test for overall effect: Z = 2.76 (P = 0.0058)
Test for subgroup differences: Chi?? = 0.51, df = 2 (P = 0.77), I?? =0.0%
0.01 0.1 1 10 100
Favours experimental Favours control
100Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 8.2. Comparison 8 Cluster randomized trials, Outcome 2 Interactive computer programme.
Review: Stage-based interventions for smoking cessation
Comparison: 8 Cluster randomized trials
Outcome: 2 Interactive computer programme
Study or subgroup log [Risk Ratio] Risk Ratio Weight Risk Ratio
(SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Usual care
Aveyard 1999 0.132468 (0.20694) 55.3 % 1.14 [ 0.76, 1.71 ]
Lawrence 2005 0.108827 (0.400688) 14.8 % 1.11 [ 0.51, 2.45 ]
Subtotal (95% CI) 70.1 % 1.14 [ 0.79, 1.63 ]
Heterogeneity: Chi?? = 0.00, df = 1 (P = 0.96); I?? =0.0%
Test for overall effect: Z = 0.69 (P = 0.49)
2 Assessment only
Escoffery 2004 0.405465 (0.468852) 10.8 % 1.50 [ 0.60, 3.76 ]
O’Neill 2000 0.157004 (0.616954) 6.2 % 1.17 [ 0.35, 3.92 ]
Prochaska 2008 0.223144 (0.427919) 12.9 % 1.25 [ 0.54, 2.89 ]
Subtotal (95% CI) 29.9 % 1.32 [ 0.76, 2.28 ]
Heterogeneity: Chi?? = 0.13, df = 2 (P = 0.94); I?? =0.0%
Test for overall effect: Z = 0.98 (P = 0.33)
Total (95% CI) 100.0 % 1.19 [ 0.88, 1.61 ]
Heterogeneity: Chi?? = 0.32, df = 4 (P = 0.99); I?? =0.0%
Test for overall effect: Z = 1.12 (P = 0.26)
Test for subgroup differences: Chi?? = 0.19, df = 1 (P = 0.66), I?? =0.0%
0.01 0.1 1 10 100
Favours experimental Favours control
101Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 8.3. Comparison 8 Cluster randomized trials, Outcome 3 Training doctors.
Review: Stage-based interventions for smoking cessation
Comparison: 8 Cluster randomized trials
Outcome: 3 Training doctors
Study or subgroup log [Risk Ratio] Risk Ratio Weight Risk Ratio
(SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Usual care
Lennox 1998 -0.27985 (0.419376) 68.9 % 0.76 [ 0.33, 1.72 ]
Wang 1994 1.530395 (0.623699) 31.1 % 4.62 [ 1.36, 15.69 ]
Total (95% CI) 100.0 % 1.33 [ 0.67, 2.63 ]
Heterogeneity: Chi?? = 5.80, df = 1 (P = 0.02); I?? =83%
Test for overall effect: Z = 0.82 (P = 0.41)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours experimental Favours control
A D D I T I O N A L T A B L E S
Table 1. Cluster randomized trials data
Study Events (I) N (I) Clusters (I) Events (C) N (C) Clusters (C) ICC Design effect (I) Design effect (C)
Bobo 1998 20 288 6 16 287 6 1.123595506 1.123595506
Chouinard
2005
26 108 18 7 56 9.33333 1.123595506 1.123595506
Lawrence
2005
(Coun-
selling)
14 305 36 12 289 41 0.013 1.097138889 1.078634146
Lawrence
2005
(Com-
puter)
15 324 23 12 289 41 0.013 1.170130435 1.078634146
Lennox
1998
32 1381 8 37 1207 8 0.013 3.231125 2.948375
Manfredi
2004
57 527 6 61 541 6 0.013 2.128833333 2.159166667
102Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Cluster randomized trials data (Continued)
Prokhorov
2008
26 219 8 17 207 7 0.008 1.211 1.228571429
Aveyard
1999
53 547 26 46 542 26 0.008 1.160307692 1.158769231
Mermel-
stein 2003
106 381 4 108 375 4 0.013 2.22525 2.20575
A P P E N D I C E S
Appendix 1. Glossary of tobacco-related terms
Term Definition
Abstinence A period of being quit, i.e. stopping the use of cigarettes or other tobacco products,
May be defined in various ways; see also:
point prevalence abstinence; prolonged abstinence; continuous/sustained abstinence
Biochemical verification Also called ’biochemical validation’ or ’biochemical confirmation’:
A procedure for checking a tobacco user’s report that he or she has not smoked or used
tobacco. It can be measured by testing levels of nicotine or cotinine or other chemicals
in blood, urine, or saliva, or by measuring levels of carbon monoxide in exhaled breath
or in blood
Bupropion A pharmaceutical drug originally developed as an antidepressant, but now also licensed
for smoking cessation; trade names Zyban, Wellbutrin (when prescribed as an antide-
pressant)
Carbon monoxide (CO) A colourless, odourless highly poisonous gas found in tobacco smoke and in the lungs
of people who have recently smoked, or (in smaller amounts) in people who have been
exposed to tobacco smoke. May be used for biochemical verification of abstinence
Cessation Also called ’quitting’
The goal of treatment to help people achieve abstinence from smoking or other tobacco
use, also used to describe the process of changing the behaviour
Continuous abstinence Also called ’sustained abstinence’
A measure of cessation often used in clinical trials involving avoidance of all tobacco
use since the quit day until the time the assessment is made. The definition occasionally
allows for lapses. This is the most rigorous measure of abstinence
103Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
’Cold Turkey’ Quitting abruptly, and/or quitting without behavioural or pharmaceutical support
Craving A very intense urge or desire [to smoke].
See: Shiffman et al ’Recommendations for the assessment of tobacco craving and with-
drawal in smoking cessation trials’
Nicotine & Tobacco Research 2004: 6(4): 599-614
Dopamine A neurotransmitter in the brain which regulates mood, attention, pleasure, reward,
motivation and movement
Efficacy Also called ’treatment effect’ or ’effect size’:
The difference in outcome between the experimental and control groups
Harm reduction Strategies to reduce harm caused by continued tobacco/nicotine use, such as reducing
the number of cigarettes smoked, or switching to different brands or products, e.g.
potentially reduced exposure products (PREPs), smokeless tobacco
Lapse/slip Terms sometimes used for a return to tobacco use after a period of abstinence. A
lapse or slip might be defined as a puff or two on a cigarette. This may proceed to
relapse, or abstinence may be regained. Some definitions of continuous, sustained or
prolonged abstinence require complete abstinence, but some allow for a limited number
or duration of slips. People who lapse are very likely to relapse, but some treatments
may have their effect by helping people recover from a lapse
nAChR [neural nicotinic acetylcholine receptors]: Areas in the brain which are thought to
respond to nicotine, forming the basis of nicotine addiction by stimulating the overflow
of dopamine
Nicotine An alkaloid derived from tobacco, responsible for the psychoactive and addictive effects
of smoking
Nicotine Replacement Therapy (NRT) A smoking cessation treatment in which nicotine from tobacco is replaced for a limited
period by pharmaceutical nicotine. This reduces the craving and withdrawal experi-
enced during the initial period of abstinence while users are learning to be tobacco-free
The nicotine dose can be taken through the skin, using patches, by inhaling a spray, or
by mouth using gum or lozenges
Outcome Often used to describe the result being measured in trials that is of relevance to the
review. For example smoking cessation is the outcome used in reviews of ways to help
smokers quit. The exact outcome in terms of the definition of abstinence and the length
of time that has elapsed since the quit attempt was made may vary from trial to trial
Pharmacotherapy A treatment using pharmaceutical drugs, e.g. NRT, bupropion
Point prevalence abstinence (PPA) A measure of cessation based on behaviour at a particular point in time, or during a
relatively brief specified period, e.g. 24 hours, 7 days. It may include a mixture of recent
and long-term quitters. cf. prolonged abstinence, continuous abstinence
104Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Prolonged abstinence A measure of cessation which typically allows a ’grace period’ following the quit date
(usually of about two weeks), to allow for slips/lapses during the first few days when
the effect of treatment may still be emerging.
See: Hughes et al ’Measures of abstinence in clinical trials: issues and recommendations’;
Nicotine & Tobacco Research, 2003: 5 (1); 13-25
Relapse A return to regular smoking after a period of abstinence
Secondhand smoke Also called passive smoking or environmental tobacco smoke [ETS]
A mixture of smoke exhaled by smokers and smoke released from smouldering
cigarettes, cigars, pipes, bidis, etc. The smoke mixture contains gases and particulates,
including nicotine, carcinogens and toxins
Self-efficacy The belief that one will be able to change one’s behaviour, e.g. to quit smoking
SPC [Summary of Product Characteristics] Advice from the manufacturers of a drug, agreed with the relevant licensing authority,
to enable health professionals to prescribe and use the treatment safely and effectively
Tapering A gradual decrease in dose at the end of treatment, as an alternative to abruptly stopping
treatment
Titration A technique of dosing at low levels at the beginning of treatment, and gradually in-
creasing to full dose over a few days, to allow the body to get used to the drug. It is
designed to limit side effects
Withdrawal A variety of behavioural, affective, cognitive and physiological symptoms, usually tran-
sient, which occur after use of an addictive drug is reduced or stopped.
See: Shiffman et al ’Recommendations for the assessment of tobacco craving and with-
drawal in smoking cessation trials’
Nicotine & Tobacco Research 2004: 6(4): 599-614
H I S T O R Y
Protocol first published: Issue 3, 2007
Review first published: Issue 11, 2010
105Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C O N T R I B U T I O N S O F A U T H O R S
KC and NG selected studies and extracted data. TL checked data extraction. KC wrote the review, with contributions from all authors.
D E C L A R A T I O N S O F I N T E R E S T
None known
S O U R C E S O F S U P P O R T
Internal sources
• Department of Primary Health Care, Oxford University, UK.
External sources
• No sources of support supplied
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
We have added sections on matched-mismatched studies and on movement through stages of change, to test the robustness and validity
of the transtheoretical model.
I N D E X T E R M S
Medical Subject Headings (MeSH)
∗Motivation; Program Evaluation; Randomized Controlled Trials as Topic; Smoking [∗psychology; therapy]; Smoking Cessation
[∗methods; psychology]
MeSH check words
Humans
106Stage-based interventions for smoking cessation (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.





























