Embed Size (px)
Citation preview

S
S2MS
OiSmhil
2
Si9Tti
dtt
fmbrs
sois
sifltthrte
l
S
ports and Performing Arts Medicine
ports and Performing Arts Medicine:. Lower Extremity Injuriesark A. Harrast, MD, Seneca A. Storm, MD, Jonathan T. Finnoff, DO,
tuart Willick, MD, Cedric K. Akau, MD
MmoocdwD
SRlED
JRCD
ShUD
ChoCD
bjective: This self-directed learning module highlights lower limb sports and perform-ng arts injuries. It is part of the study guide on sports and performing arts medicine in theelf-Directed Physiatric Education Program for practitioners and trainees in physicaledicine and rehabilitation. Using a case vignette format, this article specifically focuses onip, knee and ankle pain in athletes and performing artists. The goal of this article is to
nfluence the learner’s existing practice techniques for evaluating and managing commonower limb injuries in these populations.
.1 Clinical Activity: Formulate a diagnostic approach to the identification of apainful, snapping hip in a 28-year-old professional ballet dancer.
napping hip, an audible or palpable ‘snap’ during hip range-of-motion (ROM), hasntra-articular and extra-articular etiologies. The prevalence in ballet dancers approaches0%, with an average onset at age 14-16 years. Eighty percent of cases occur bilaterally [1].he snapping may develop atraumatically or may follow a specific traumatic event like
wisting or falling. Forced hip extension and external rotation is the mechanism for labralnjuries.
Intra-articular causes of hip snapping include loose bodies, labral tears, synovial chon-romatosis, osteochondral fractures, and femoral acetabular impingement (FAI)[1]. Any ofhese diagnoses may lead to clicking with hip rotation. Long-standing labral tears may leado subchondral cysts and premature osteoarthritis [2].
Femoral acetabular impingement is due to abnormal contact between the anterosuperioremoral neck and the anterosuperior acetabulum (Figure 1) [3,4]. There are 2 primary
echanisms for FAI: (1) cam, and (2) pincer. The cam mechanism involves impingementetween a dysmorphic (flattened) superior femoral head-neck junction and the acetabularim, whereas the pincer type is due to a prominent acetabular rim (eg, acetabular retrover-ion). FAI may lead to labral tears and premature osteoarthritis [4].
Extra-articular causes are categorized by medial (internal) or lateral (external) hipnapping. External snapping, the most common type, is caused by the iliotibial band (ITB)r gluteus maximus tendon snapping over the greater trochanter. Internal snapping local-zes over the anterior groin and involves the iliopsoas tendon snapping over deeper osseoustructures (eg, iliopectineal eminence, femoral head, or lesser trochanter) [1,2].
Physical examination of hip snapping should include hip joint ROM and hip girdletrength and flexibility assessments. Having the patient demonstrate the snap may helpdentify the mechanism [1]. Tests that suggest an intra-articular cause include pain with hipexion-abduction-external-rotation (FABER) testing, hip flexion-adduction-internal rota-ion testing, or a positive scour test [4,5]. Labral tears may cause decreased hip propriocep-ion and ROM [2]. Extra-articular internal snapping hip may be reproduced by moving theip from a flexed-abducted-externally rotated position to an extended-adducted-internallyotated position, thus moving the iliopsoas tendon across the anterior osseous hip struc-ures. Hip snapping over the greater trochanteric region that is caused by hip flexion andxtension with the ITB under tension suggests extra-articular external snapping hip [1].
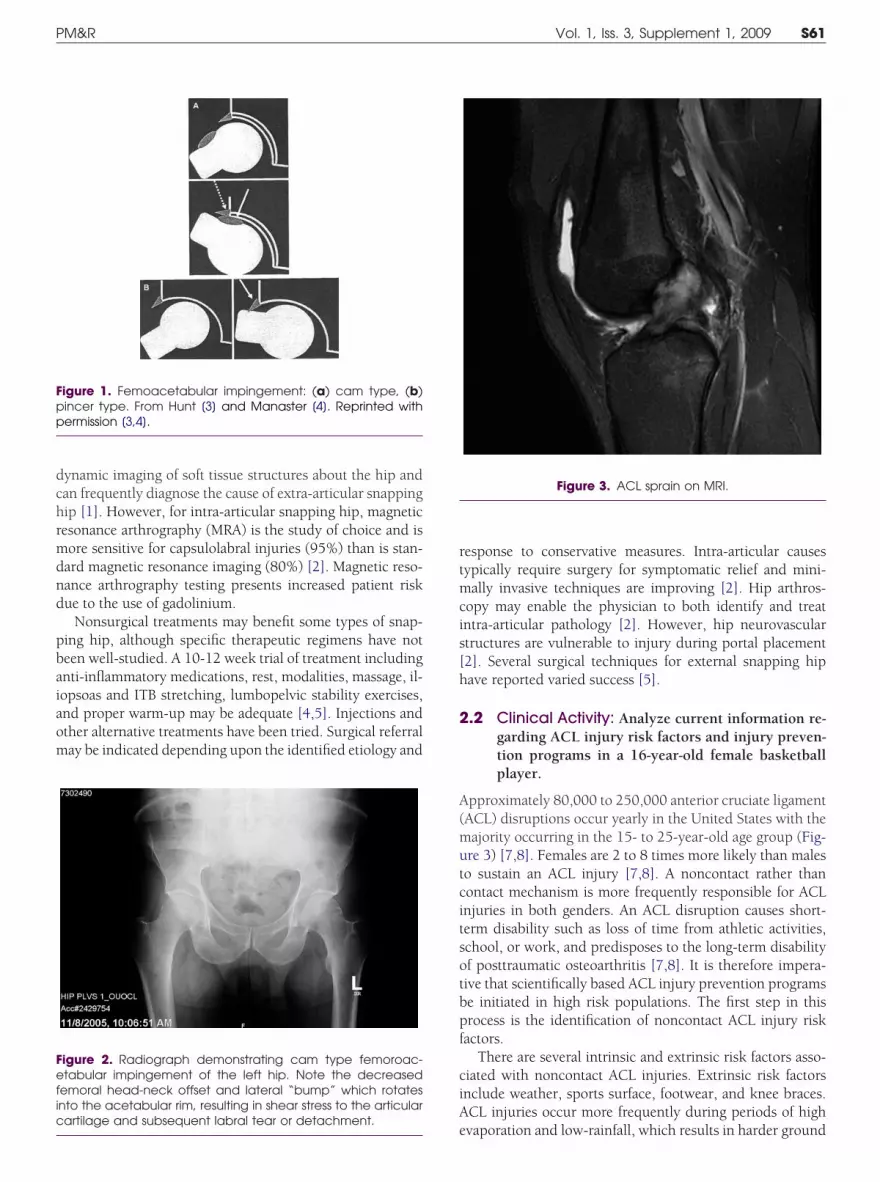
Plain radiographs are typically normal, but occasionally demonstrate osseous injury (eg,
oose body) or findings suggestive of FAI (Figure 2). Real-time ultrasonography providesDC
PM&R © 2009 by the American Academy of P1934-1482/09/$36.00
Printed in U.S.A.60
.A.H. Spine and Sports Fellowship, Depart-ent of Rehabilitation Medicine, Department
f Orthopedics and Sports Medicine, Universityf Washington, Box 356940, 1959 NE Pa-ific, Seattle, WA 98195. Address correspon-ence to: M.A.H.; e-mail: [email protected]: nothing to disclose
.A.S. Department of Physical Medicine &ehabilitation, Michigan State University Col-
ege of Osteopathic Medicine, Lansing Spine &xtremity Rehabilitation, Lansing, MI.isclosure: nothing to disclose
.T.F. Department of Physical Medicine andehabilitation, College of Medicine, Mayolinic, Rochester, MNisclosure: nothing to disclose
.W. Division of Physical Medicine and Re-abilitation, University of Utah, Salt Lake City,Tisclosure: nothing to disclose
.K.A. Division of Physical Medicine and Re-abilitation, University of Hawaii; Departmentf Sports Medicine and Rehabilitation, Straublinic and Hospital, Honolulu, HIisclosure: nothing to disclose
isclosure Key can be found on the Table ofontents and at www.pmrjournal.org
hysical Medicine and RehabilitationSuppl. 1, S60-S66, March 2009
DOI: 10.1016/j.pmrj.2009.02.001
dchrmdnd
pbaiaom
rtmcis[h
2
A(mutcitsotbpf
ciA
Fpp
Fefic
S61PM&R Vol. 1, Iss. 3, Supplement 1, 2009
ynamic imaging of soft tissue structures about the hip andan frequently diagnose the cause of extra-articular snappingip [1]. However, for intra-articular snapping hip, magneticesonance arthrography (MRA) is the study of choice and isore sensitive for capsulolabral injuries (95%) than is stan-ard magnetic resonance imaging (80%) [2]. Magnetic reso-ance arthrography testing presents increased patient riskue to the use of gadolinium.
Nonsurgical treatments may benefit some types of snap-ing hip, although specific therapeutic regimens have noteen well-studied. A 10-12 week trial of treatment includingnti-inflammatory medications, rest, modalities, massage, il-opsoas and ITB stretching, lumbopelvic stability exercises,nd proper warm-up may be adequate [4,5]. Injections andther alternative treatments have been tried. Surgical referralay be indicated depending upon the identified etiology and
igure 1. Femoacetabular impingement: (a) cam type, (b)incer type. From Hunt [3] and Manaster [4]. Reprinted withermission [3,4].
igure 2. Radiograph demonstrating cam type femoroac-tabular impingement of the left hip. Note the decreased
emoral head-neck offset and lateral “bump” which rotatesnto the acetabular rim, resulting in shear stress to the articular
eartilage and subsequent labral tear or detachment.
esponse to conservative measures. Intra-articular causesypically require surgery for symptomatic relief and mini-ally invasive techniques are improving [2]. Hip arthros-
opy may enable the physician to both identify and treatntra-articular pathology [2]. However, hip neurovasculartructures are vulnerable to injury during portal placement2]. Several surgical techniques for external snapping hipave reported varied success [5].
.2 Clinical Activity: Analyze current information re-garding ACL injury risk factors and injury preven-tion programs in a 16-year-old female basketballplayer.
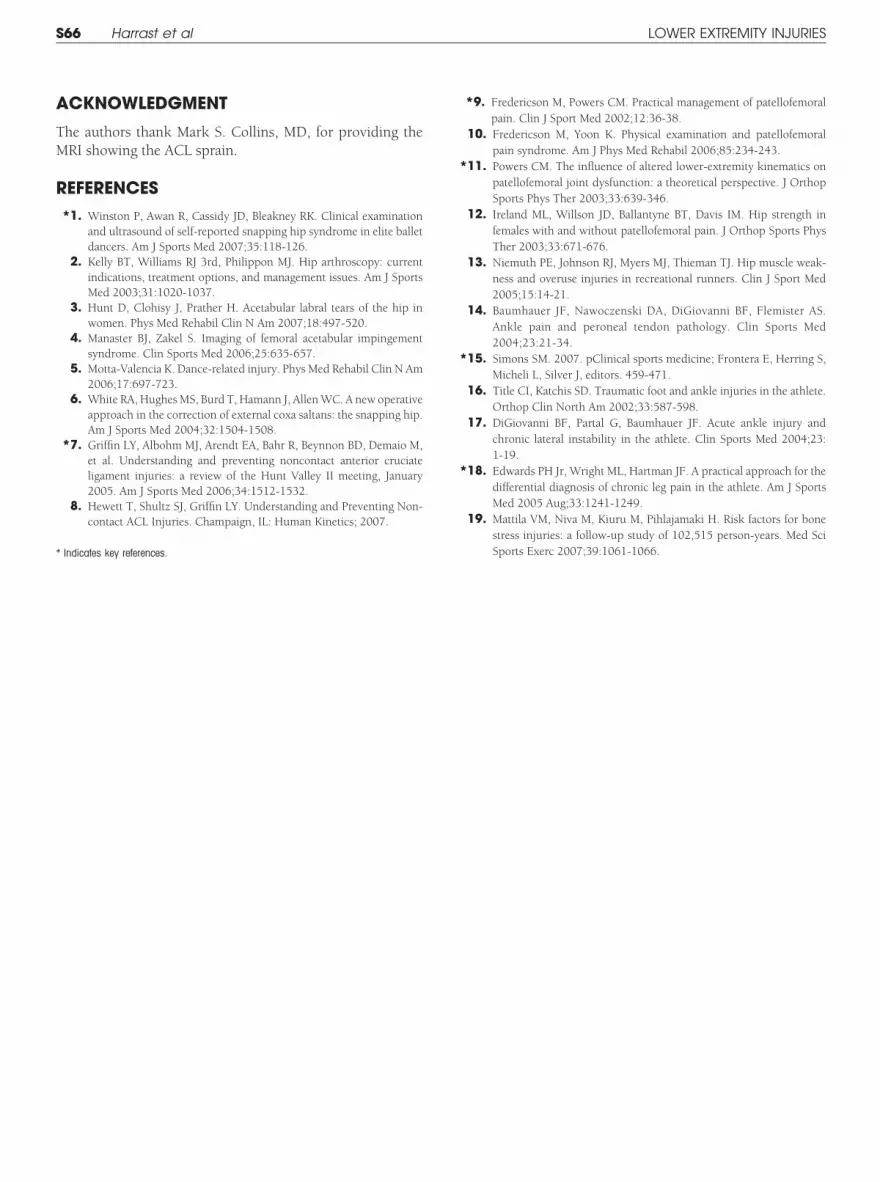
pproximately 80,000 to 250,000 anterior cruciate ligamentACL) disruptions occur yearly in the United States with theajority occurring in the 15- to 25-year-old age group (Fig-re 3) [7,8]. Females are 2 to 8 times more likely than maleso sustain an ACL injury [7,8]. A noncontact rather thanontact mechanism is more frequently responsible for ACLnjuries in both genders. An ACL disruption causes short-erm disability such as loss of time from athletic activities,chool, or work, and predisposes to the long-term disabilityf posttraumatic osteoarthritis [7,8]. It is therefore impera-ive that scientifically based ACL injury prevention programse initiated in high risk populations. The first step in thisrocess is the identification of noncontact ACL injury riskactors.
There are several intrinsic and extrinsic risk factors asso-iated with noncontact ACL injuries. Extrinsic risk factorsnclude weather, sports surface, footwear, and knee braces.CL injuries occur more frequently during periods of high
Figure 3. ACL sprain on MRI.
vaporation and low-rainfall, which results in harder ground

cnsfinfldflkattdl[ri
tm(htapqhAriflp
cwfrwiwthaf
fkmhekaapTk
t[
hcd
ApsipbivcettcAqAt
2
PdcoHsn
cTajeiwttOiaptt
dtlq
S62 Harrast et al LOWER EXTREMITY INJURIES
onditions and increased shoe-surface traction [7,8]. Theew artificial turf installed for American football appears toignificantly reduce noncontact ACL injury rates [7,8]. Arti-cial floors in women’s team handball increase the risk ofoncontact ACL injury when compared to natural woodoors, likely due to the increased shoe-surface traction asocumented by a higher coefficient of friction on artificialoors [7,8]. Previous research has reported a lower risk ofnee injuries in athletes whose shoes had shorter cleats,lthough further research on the role of footwear in noncon-act ACL injury risk is needed [7,8]. One study of intramuralackle football athletes demonstrated a 3 times higher inci-ence of ACL injury in athletes who did not wear a prophy-
actic knee brace when compared to those who wore a brace7,8]. However, other studies have not reproduced theseesults [7,8]. Therefore, the role of prophylactic knee bracingn non-ACL injury prevention remains indeterminate.
Intrinsic risk factors that have been investigated includehe anatomic risks of a wide Q-angle, improper knee align-ent during injury, foot pronation, high body mass index
BMI), and narrow intercondylar notch size. Other risks areormonal factors, familial tendency, and neuromuscular fac-ors. An increased static and dynamic Q-angle has beenssociated with a higher incidence of ACL injury [7,8]. Footronation, as measured by navicular drop, occurs more fre-uently in athletes with ACL injuries when compared toealthy controls, suggesting that pronation may contribute toCL injury [7,8]. Athletes with a higher BMI may be at higherisk for noncontact ACL injury risk, because they tend to landn a more extended knee position and have reduced kneeexion angles [7,8]. A narrow intercondylar notch width mayredispose to noncontact ACL injury [7,8].
Estradiol inhibits fibroblast proliferation and type 1 pro-ollagen synthesis in vitro, and these effects are attenuatedith progesterone [7,8]. Thus, during the estradiol dominant
ollicular phase of the menstrual cycle, it is possible that aelative down regulation of collagen production occurs,hich is reversed during the luteal phase due to the increase
n progesterone. Clinical studies examining ACL laxity inomen have demonstrated the greatest knee laxity occurs in
he early luteal phase [7,8]. Interestingly, it appears that theighest frequency of ACL injury in women occurs in the earlynd late follicular phases, although these findings requireurther study [6-8].
There are a multitude of noncontact ACL injury riskactors in the female population. Women tend to have lessnee and hip flexion during jumping, cutting and pivotinganeuvers when compared to men [7,8]. In addition, they
ave an increase in knee valgus, hip internal rotation, tibialxternal rotation, quadriceps muscle contraction, and lessnee joint stiffness during these activities [7,8]. Fatigue ex-cerbates these abnormal movement patterns [7,8]. Womenlso have a quadriceps dominated thigh muscle contractionattern when performing landing and cutting activities [7,8].his results in an anterior tibial force vector and reduced
nee stiffness [6,7]. Female ACLs are smaller, less elastic, and dear at a lower strain and stress than their male counterparts7,8].
Athletes who sustain an ACL injury are twice as likely toave a relative with an ACL injury when compared withontrols [7,8]. This finding suggests a possible familial pre-isposition to ACL injury.
To date, 10 successful programs to prevent noncontactCL injury have been developed [7,8]. These successfulrograms feature many different exercise and behavioraltrategies to correct modifiable risk factors. The programsnclude improving the athlete’s coordination and movementatterns by means of proprioception exercises on wobbleoards, increasing knee and hip flexion angles during land-
ng by means of “soft landing” drills, reducing dynamic kneealgus through cutting and jumping technique drills, in-reasing hamstring strength via hamstring strengthening ex-rcises, and improving understanding of noninjury risk fac-ors through risk awareness education [7,8]. The success ofhese programs suggests that correcting the modifiable non-ontact ACL injury risk factors can reduce the incidence ofCL injury. While further research on this subject is re-uired, initiating a program aimed at preventing noncontactCL injury in high risk populations should be considered at
his time.
.3 Clinical Activity: Develop a diagnostic and manage-ment strategy for patellofemoral pain in a triathlete.
atellofemoral pain (PFP) is one of the most common kneeisorders evaluated by sports medicine practitioners. It isonsidered a syndrome because it consists of a constellationf symptoms that are not explained by an isolated etiology.owever, the most commonly accepted source of pain is the
ubchondral bone of the patellofemoral joint, since there areo nerve endings in the overlying articular cartilage.
Athletes with PFP typically describe retropatellar and oc-asionally medial or lateral patellar retinacular aching [8,9].he pain is frequently exacerbated by hills, stairs, squatting,nd prolonged sitting, all of which increase patellofemoraloint compressive forces. For triathletes, the event that exac-rbates their pain (ie, running and/or biking) should bedentified. The knee examination should include inspectionith close attention paid to lower limb alignment and patellar
racking. It should also include palpation, range-of-motionests, neurologic evaluation, and PFP provocative testing.ther causes of knee pain, such as meniscal or ligamentous
njuries, should be ruled out. Strength and flexibility imbal-nces should be identified. Particular attention should beaid to ITB tightness since it may lead to lateral patellarilting, excessive lateral patellar pressure, and decreased pa-ellar mobility [10].
While the focused knee examination is helpful to detectiagnoses other than patellofemoral pain (eg, mensical tears),he most important portion of the examination for patel-ofemoral pain is the kinetic chain evaluation. The hip fre-uently plays an important role in PFP. Dynamic MRI has
emonstrated lateral patellar displacement due to excessive
fsfnaptj
sgmpdmks(iafpp
etm
tisnbroad
mifljaretEwmlpicisn
2
Tartm
aq[mmml(aetlLtcr[yattt[a
1l[ewmTfmn5am
jwlins
S63PM&R Vol. 1, Iss. 3, Supplement 1, 2009
emoral adduction and internal rotation during knee exten-ion in PFP subjects [11]. In addition, several studies haveound hip abduction and external rotation weakness in run-ers with knee injuries, including PFP [12,13]. The foot andnkle may also contribute to PFP. Excessive subtalar jointronation can lead to tibial internal rotation and compensa-ory femoral internal rotation, thus increasing patellofemoraloint stress.
The kinetic chain evaluation should begin with a statictanding evaluation of the athlete for femoral anteversion,enu valgum, and pes planus, the hip, knee, ankle, and foototion should be inspected during gait for signs of increasedatellofemoral joint stress. A double leg squat can be used toetect dysfunctional lower limb movement patterns. Thisaneuver will also reveal restrictions in functional hip and
nee flexion, and in ankle dorsiflexion motion. The single legquat is a great test of functional hip strength, femoral controlie, presence or absence of excessive femoral adduction andnternal rotation), and ankle-foot motion (ie, presence orbsence of excessive pronation). For triathletes with PFProm running, video running technique analysis should beerformed. If their pain is due to cycling, their bicycle fit andedaling technique should be evaluated.
Radiologic imaging is rarely helpful during the initial PFPvaluation. Radiographs may detect bony lesions or osteoar-hritis of the patellofemoral joint. An MRI can evaluate theenisci, ligaments, and articular cartilage.Historically, PFP treatment focused on correction of pa-
ellar malalignment and tracking abnormalities. It typicallyncluded strengthening of the medial thigh (vastus medialis),tretching of the lateral structure (ITB), patellar taping tech-iques (eg, McConnell taping), patellar bracing, patellar mo-ilizations, and surgical procedures such as lateral patellaretinacular releases and realignment procedures. While somef these treatments may still be employed, current treatmentsre more functional and focus on correcting kinetic chaineficits.
Treatment begins with pain reduction through activityodification and judicious use of physical modalities, med-
cations (eg, acetaminophen and/or -nonsteroidal anti-in-ammatory drugs), McConnell taping, and patellofemoral
oint bracing. Examples of activity modifications for runningthletes include deep water running, elliptical machines, andunning on softer surfaces. If the proximal kinetic chainvaluation revealed weak hip abductors and external rota-ors, strengthening of this musculature should take place.xcessive femoral adduction and internal rotation duringeight bearing activities can be corrected through neuro-uscular reeducation and strengthening of the dynamic
umbopelvic stabilizing muscles. Excessive subtalar jointronation can be corrected through strengthening of the foot
ntrinsic muscles and ankle support muscles, stretching thealf, and utilizing orthotics. In addition to calf tightness,nflexibility of the hip flexors, quadriceps, ITBs and ham-trings should be corrected. Running and bicycling tech-
ique and bicycle fit abnormalities should be corrected. e.4 Educational Activity: Describe the various etiol-ogies of ankle pain following a traumatic ankleinjury sustained by a 35-year-old man while he wasplaying basketball.
he ankle is the most frequently injured joint in athletes,ccounting for 20% to 35% of total time lost to injury inunning and jumping sports [14]. Thus, it is important forhe physiatrist to understand the various etiologies of trau-atic ankle injuries.Sprains are the most common ankle injury, comprising
bout 40% of all sports-related injuries [15]. The most fre-uent mechanism of injury is plantarflexion and inversion16]. In this position, the bony constraints of the ankleortise around the talus are reduced and the lateral liga-ents are susceptible to injury. The anterior talofibular liga-ent (ATFL) is injured first, followed by the calcaneofibular
igament (CFL), and finally the posterior talofibular ligamentPTFL) [15]. The patient’s history should include the mech-nism of injury, history of previous ankle sprains, the pres-nce of a “pop” at the time of the injury, pain intensity, abilityo immediately weight-bear, neurological symptoms, and theength of time postinjury until the onset of swelling [15].ocalized tenderness over the ankle ligaments assist in iden-ifying the presence of a tear [15]. Laxity of the ATFL and CFLan be detected by the anterior drawer and talar tilt tests,espectively, with the contralateral ankle serving as a control16]. The Ottawa Ankle Rules for patients ages 18-55ears recommend radiographs only when there is ankle painnd 1 of the following findings: bone tenderness at the base ofhe fifth metatarsal, inability to bear weight immediately afterhe injury or for 4 steps in the emergency room, or boneenderness at the tip or posterior edge of either malleolus17]. Subtle physeal injuries can also occur in pediatricthletes [15].
Syndesmotic or “high” ankle sprains account for only0%-20% of all ankle sprains. However, they result in more
ost playing time and disability than lateral ankle sprains16]. The usual mechanism of injury is dorsiflexion andxternal rotation [15,16]. Athletes present with difficulty ineight-bearing and pain in the region of the distal syndes-osis. They are tender to palpation over the anterior ankle.heir pain is exacerbated by passive external rotation of the
oot with the ankle in a neutral position or by squeezing theid tibia and fibula (Figure 4) [14,15]. Radiographs areecessary to evaluate for ankle mortise widening. More thanmm of mortise widening on radiographs of plantar flexion
nd external rotation views is deemed abnormal [14]. MRIay be helpful if radiographs are normal [15].Achilles tendon rupture usually occurs during a sudden
ump or push off. It is most common in 30-year-old men,ith 75% of the ruptures occurring during an athletic activity
ike basketball and soccer [16]. The tendon usually rupturesn a hypovascular zone located 2-6cm proximal to the calca-eal insertion [16]. The athlete usually feels a pop andudden pain, and is unable to continue activity. Physical
xamination frequently reveals a palpable tendon gap, posi-
tsm
top
ttMaflir
TsteMoassc
oaklnd
2
Tce
utmiacipgcip
mlsatfcocm
Ff
S64 Harrast et al LOWER EXTREMITY INJURIES
ive Thompson test (Figure 5), and inability to perform aingle heel raise [16]. In equivocal cases, ultrasound or MRIay be useful in making the diagnosis [16].In athletes with chronic ankle pain and mechanical symp-
oms, particularly adolescent athletes, osteochondral lesionsf the talus should be considered. Symptoms may include
igure 4. External rotation stress test (a) and Squeeze test (b)or syndesmotic ankle sprains.
ain, swelling, instability, catching, or locking [14,15]. Os- u
eochondral lesions occur on the lateral talar dome 43% ofhe time and often develop following ankle trauma [14,15].
edial lesions are less commonly associated with trauma andre often difficult to see on standard radiographs. Plantar-exed oblique views of the ankle mortise facilitate lesion
dentification, and MRI can provide additional informationequired for appropriate treatment recommendations [15].
Subluxing peroneal tendons can cause lateral ankle pain.he acute clinical presentation includes a history of a pop ornap followed by pain, swelling, and tenderness posterior tohe lateral malleolus. Provocative testing consists of resistingversion with the ankle dorsiflexed [15]. In equivocal cases,RI or ultrasound is helpful [15]. Peroneal tendons can
ccasionally tear following lateral ankle sprains in youngthletes [15]. The presentation includes tenderness andwelling posterior to the distal fibula with no evidence ofubluxation. Magnetic resonance imaging or ultrasound canonfirm the diagnosis [15].
Fractures of the ankle should always be suspected in casesf significant trauma [15]. Further, overuse injuries of thenkle such as anterior tibiotalar impingement, posterior an-le impingement, posterior tibial tendinopathy, medial mal-
eolus stress fractures, chronic lateral ankle instability anderve entrapment syndromes should be considered in theifferential diagnosis of ankle pain [14-17].
.5 Educational Activity: Discuss the causes of lowerleg pain in a 33-year-old marathon runner.
he differential diagnosis of leg pain in a marathoner in-ludes muscle/tendon overload, bone overload, chronic ex-rtional compartment syndrome, and vascular causes [18].
Muscle/tendon overload can occur in any muscle/tendonnit. Muscle/tendon overload is often caused by errors inraining technique and/or biomechanical problems. Theost common training error that leads to tissue overload is
ncreasing running volume too fast. Hard running surfacesnd incorrect running shoes can also play a role. Biomechani-al issues associated with muscle/tendon overload in runnersnclude pes planus, rigid pes cavus, toe running, and im-aired function of the larger, stronger hip muscles, includingluteus medius and the hip external rotators. Impaired ec-entric control of the hip external rotators allows the femur tonternally rotate after heel strike, which promotes hyper-ronation and overload of tibialis posterior.
Muscle/tendon overload in the leg of endurance runners isost commonly seen in the posterior compartments of the
eg. Overload of tibialis posterior and the gastrocnemius/oleus/Achilles complex is commonly seen in hill runnersnd toe runners, who place excessive concentric and eccen-ric loads on these structures. Achilles tendon pain is oftenelt between 2 and 6 centimeters above the insertion ontoalcaneus, but can also be felt at the insertion itself. Overloadf tibialis posterior can be appreciated anywhere along theourse of the muscle and tendon. Often, it is felt along theedial tibia. The term “shin splints”---although commonly
sed for anterior and medial leg pain in runners---is nonspe-
csitphsm
apat
ccbusmtre
stocsiscw
oons
wqlemptdTctim
raapbmTaiacv
Ft g the
S65PM&R Vol. 1, Iss. 3, Supplement 1, 2009
ific and is discouraged. The preferred term, “medial tibialtress syndrome” refers to a continuum of overload pathologynvolving tibialis posterior, medial soleus, the tibial perios-eum and the tibia itself. Early on, symptoms are oftenresent at the beginning of a run and then may improve as theeel cord loosens up. As the condition worsens, symptomstart earlier in the run and do not improve. Later, symptomsay be present even with walking.Runners who have a sudden increase in downhill running
re at risk for eccentric overload of the anterior leg muscles,rincipally tibialis anterior. Pain is usually of insidious onsetnd can be present anywhere along the course of the muscle/endon unit.
The peroneal muscles can become strained when trying toontrol a sudden inversion ankle sprain. They can also be-ome chronically overloaded, and longitudinal split tears cane seen in the peroneal tendons on MRI. If the lateral retinac-lum of the ankle is incompetent, the peroneal tendon canublux over the lateral malleolus. Occasionally a peronealuscle can herniate through a defect in the lateral fascia of
he leg. Peroneal muscle pain can be reliably diagnosed byeproducing concordant pain with resistance testing of footversion.
Bone overload is also common in endurance runners. Thepectrum of bone overload includes periostitis, stress reac-ion, and stress fracture. High volume running can causeverload of normal bone. Low and medium volume runningan cause overload of bone with abnormal mineralization,tructure or metabolism. Risk factors for stress fracturesnclude high volume running, improper training techniqueuch as increasing running volume too quickly, inadequatealoric and protein intake and hormonal imbalance, as seen
igure 5. Thompson test for Achilles tendon rupture. Upon squest result is negative). A lack of plantar flexion upon squeezin
ith amenorrhea in the female athlete triad [19]. Symptoms a
f bone stress can be difficult to distinguish from symptomsf tendinopathy on clinical grounds alone. Magnetic reso-ance imaging is the criterion standard for diagnosing bonetress.
Chronic exertional compartment syndrome (CECS),hile less common than tendinopathies, is nonetheless fre-uently encountered in running clinics. Although the under-
ying pathophysiology of CECS has not yet been clarified, thend result is increased pressure during exercise within 1 orore of the 4 compartments of the leg. The increased com-artment pressure can cause pain, impaired function, andemporary ischemia to muscles and nerves. The CECS isiagnosed by intramuscular compartment pressure testing.he most commonly involved compartment is the anteriorompartment, followed by the posterior compartments. In-ramuscular pressures that are diagnostic for CECS are: rest-ng � 15 mm Hg; 1 minute postexercise � 30 mm Hg; 5
inutes postexercise � 20 mm Hg.Vascular causes of leg pain are far less common in younger
unners. One clinical entity of note, however, is poplitealrtery entrapment syndrome. This relatively rare conditionffects women more than men. Causes include a hypertro-hied medial gastrocnemius muscle and abnormal tissueands associated with plantaris, popliteus and gastrocne-ius, which can potentially compromise the popliteal artery.wo physical examination maneuvers that suggest poplitealrtery entrapment if symptoms are reproduced are (1) repet-tive activation of the plantar flexors with the knee extendednd (2) prolonged passive stretch of the hamstring and heelord. More definitive diagnosis is usually made by dynamicascular ultrasound or arteriogram with and without the
a healthy calf, the foot will passively plantar flex (arrow) (ie,calf is indicative of a positive test.
eezing
ppropriate provocative maneuvers.
A
TM
R*
*
*
*
S66 Harrast et al LOWER EXTREMITY INJURIES
CKNOWLEDGMENT
he authors thank Mark S. Collins, MD, for providing theRI showing the ACL sprain.
EFERENCES*1. Winston P, Awan R, Cassidy JD, Bleakney RK. Clinical examination
and ultrasound of self-reported snapping hip syndrome in elite balletdancers. Am J Sports Med 2007;35:118-126.
2. Kelly BT, Williams RJ 3rd, Philippon MJ. Hip arthroscopy: currentindications, treatment options, and management issues. Am J SportsMed 2003;31:1020-1037.
3. Hunt D, Clohisy J, Prather H. Acetabular labral tears of the hip inwomen. Phys Med Rehabil Clin N Am 2007;18:497-520.
4. Manaster BJ, Zakel S. Imaging of femoral acetabular impingementsyndrome. Clin Sports Med 2006;25:635-657.
5. Motta-Valencia K. Dance-related injury. Phys Med Rehabil Clin N Am2006;17:697-723.
6. White RA, Hughes MS, Burd T, Hamann J, Allen WC. A new operativeapproach in the correction of external coxa saltans: the snapping hip.Am J Sports Med 2004;32:1504-1508.
*7. Griffin LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD, Demaio M,et al. Understanding and preventing noncontact anterior cruciateligament injuries: a review of the Hunt Valley II meeting, January2005. Am J Sports Med 2006;34:1512-1532.
8. Hewett T, Shultz SJ, Griffin LY. Understanding and Preventing Non-contact ACL Injuries. Champaign, IL: Human Kinetics; 2007.
Indicates key references.
*9. Fredericson M, Powers CM. Practical management of patellofemoralpain. Clin J Sport Med 2002;12:36-38.
10. Fredericson M, Yoon K. Physical examination and patellofemoralpain syndrome. Am J Phys Med Rehabil 2006;85:234-243.
11. Powers CM. The influence of altered lower-extremity kinematics onpatellofemoral joint dysfunction: a theoretical perspective. J OrthopSports Phys Ther 2003;33:639-346.
12. Ireland ML, Willson JD, Ballantyne BT, Davis IM. Hip strength infemales with and without patellofemoral pain. J Orthop Sports PhysTher 2003;33:671-676.
13. Niemuth PE, Johnson RJ, Myers MJ, Thieman TJ. Hip muscle weak-ness and overuse injuries in recreational runners. Clin J Sport Med2005;15:14-21.
14. Baumhauer JF, Nawoczenski DA, DiGiovanni BF, Flemister AS.Ankle pain and peroneal tendon pathology. Clin Sports Med2004;23:21-34.
15. Simons SM. 2007. pClinical sports medicine; Frontera E, Herring S,Micheli L, Silver J, editors. 459-471.
16. Title CI, Katchis SD. Traumatic foot and ankle injuries in the athlete.Orthop Clin North Am 2002;33:587-598.
17. DiGiovanni BF, Partal G, Baumhauer JF. Acute ankle injury andchronic lateral instability in the athlete. Clin Sports Med 2004;23:1-19.
18. Edwards PH Jr, Wright ML, Hartman JF. A practical approach for thedifferential diagnosis of chronic leg pain in the athlete. Am J SportsMed 2005 Aug;33:1241-1249.
19. Mattila VM, Niva M, Kiuru M, Pihlajamaki H. Risk factors for bonestress injuries: a follow-up study of 102,515 person-years. Med Sci
Sports Exerc 2007;39:1061-1066.




























