Embed Size (px)
Citation preview

Oc
Saa
Rti1dp
Cfi(
AalfdI
rdolb
ameodt
CKMO
2
Specific Language Difficulties and School Achievement in Children Bornat 25 Weeks of Gestation or Less
DIETER WOLKE, PHD, MUTHANNA SAMARA, MSC, MELANIE BRACEWELL, MD, AND NEIL MARLOW, MD,FOR THE EPICURE STUDY GROUP*
bjective To determine whether language and educational problems are specific or due to general cognitive deficits inhildren born at 25 weeks’ gestation or less.
tudy design A national cohort study assessed 241 of 308 (78%) surviving children at a median age of 6 years, 4 monthslong with 160 of these children’s classmates. Formal tests included standard cognitive, language, phonetic, and speechssessments. The children’s school achievement was rated by classroom teachers.
esults Mean cognitive scores for index children were 82 (standard deviation [SD] � 19) compared with 106 (SD � 12) forhe peer group. Extremely preterm children had an increased risk of language problems (odds ratio [OR] � 10; 95% confidencenterval [CI] � 3 to 32), speech problems (OR � 4.4; 95% CI � 3 to 7), and overall school difficulties (OR � 25; 95% CI �2 to 54). Extremely preterm boys were twice as likely to show deficits as extremely preterm girls, but no such sex-basedifferences were apparent in the comparison group. Differences in general cognitive scores explained specific language orhonetic awareness deficits, but not speech ratings or educational difficulties, in the extremely preterm children.
onclusions Language or phonetic difficulties are not specific and indicate general cognitive functional difficulties. Thendings have implications for models of global deviation of brain development in extremely preterm children.J Pediatr 2008;152:256-62)
higher prevalence of cognitive impairments and poorer educational achievement has been repeatedly observed inchildren born preterm or with low birth weight compared with children born at full term.1 Other developmentaldisorders, such as language delays and deficits,2 articulation problems,3 and learning disorders (eg, poor reading, writing,
nd numerical and mathematic skills4,5) also are more common in very low birth weight (VLBW) children. Such language orearning disorders may be associated with general cognitive impairment, or they can be specific and independent of cognitiveunction or environmental disadvantage.2 Specific developmental language impairments or specific learning disorders areiagnosed when there is a clear discrepancy between general intellectual development as measured by, for example, performanceQ and language or learning achievement scores.6,7
Long-term adverse cognitive, language, and psychosocial outcomes have beeneported in children with normal IQ but with specific language impairment.8 Specificeficits may suggest either damage to or inhibition of normal development in specific areasf the brain.9 Few previous studies have evaluated whether these developmental orearning problems truly represent specific developmental disorders or can be accounted fory general cognitive deficits in VLBW children.10
A recent longitudinal analysis of VLBW children suggests that learning difficultiesre not specific, but rather are more likely due to global deficits in cognitive function anday require different interventions than those developed for full-term children.4 How-
ver, the children included in these cohorts were born before the widespread introductionf antenatal corticosteroid and surfactant replacement therapy, which are importanteterminants of the increased survival of extremely preterm infants11 that can be expectedo enhance long-term outcome and also possibly alter patterns of disability. These cohorts
I Confidence interval-ABC Kaufman Assessment Battery for ChildrenPC Mental Processing Composite
PAT Phonological Abilities TestPLS-3 Preschool Language Scale-3SD Standard deviation
From the Department of Psychology andWarwick Medical School, Health SciencesResearch Institute, University of Warwick,Coventry, UK (D.W., M.S.) and the Insti-tute of Neuroscience, University of Not-tingham, Nottingham, UK (M.B., N.M.).
Submitted for publication Mar 30, 2007;last revision received Jun 18, 2007; ac-cepted Jun 28, 2007.
Reprint requests: Dieter Wolke, PhD, Univer-sity of Warwick, Department of Psychologyand Health Sciences Research Institute, War-wick Medical School, Coventry CV4 7AL, UK.E-mail: [email protected].
*A list of EPICURE Study Group membersis available at www.jpeds.com.
0022-3476/$ - see front matter
Copyright © 2008 Mosby Inc. All rightsreserved.
R Odds ratio VLBW Very low birth weight
56
10.1016/j.jpeds.2007.06.043

ihdp
pp2stsw
S
h6dMaAcsappAwbiMc
A
mppPcssi(aciwupsass
wt(
teoANtccwNt
aaita
ratcb
S
foAtbutupcssAsa
C
sMdd[
S
ncluded very few extremely preterm children, whose survivalas increased over the past 15 years and whose high risks ofisability and general cognitive problems have been describedreviously.12
In this report, we describe the results of language, speech,honetic, and educational difficulties during the early school ageeriod in a geographically based sample of children born before6 weeks’ gestation, of whom �60% were exposed to antenatalteroid treatment and 84% received surfactant.13 We investigatehe extent to which the language and learning difficulties ob-erved in this population are specific impairments or are in lineith general cognitive abilities.
METHODS
ubjectsThe derivation and characteristics of this study population
ave been described previously,13,14 as have the details of the-year evaluation.12 The population represents all surviving chil-ren born at 25 weeks, 6 days gestational age or less betweenarch and December 1995. Of the 308 children known to be
live at age 30 months, the parents of 241 consented to the study.total of 204 children were in mainstream education. For each
hild assessed in a mainstream school, we sought an age- andex-matched classmate as a comparison.12 Thus, we were able tossess 160 full-term born children, who form the comparisonopulation. All children were assessed by a pediatrician and asychologist trained in the techniques used for the study (seeppendix; available at www.jpeds.com). All appointmentsere made by the study administrator, and the assessors werelinded to the children’s group status. All parents gave writtennformed consent, and the study was approved by the Trent
ulticentre Research Ethics Committee and the local edu-ation authorities in Scotland.
ssessmentGeneral cognitive ability was assessed using the Kauf-
an Assessment Battery for Children (K-ABC),12,15 com-osed of 2 summative scales: the Mental Processing Com-osite (MPC), comprising Sequential and Simultaneousrocessing subscales, which provides a global measure of thehild’s cognitive ability, and the Achievement Scale, an as-essment of knowledge of facts, language concepts, andchool-related skills. Receptive and expressive language abil-ties were evaluated using the Preschool Language Scale-3UK) (PLS-3), which comprises Auditory Comprehensionnd Expressive Communication scales.16 Articulation diffi-ulties were assessed according to 19 speech sounds in thenitial or final positions of consonant-vowel-consonant words,hich the child is asked to imitate in the PLS assessment. Wesed the Phonological Abilities Test (PAT)17 to assess skillsredictive of reading acquisition.18 The PAT comprises 4ubtests: rhyme detection, phoneme deletion (both beginningnd end sounds), and a test of letter knowledge.17 Quality ofpeech was rated by the psychologists using published
cales;19 phonological disorder (315.39) and stuttering (307) hpecific Language Difficulties and School Achievement in Children Born
ere diagnosed according to criteria specified in the Diagnos-ic and Statistical Manual of Mental Disorders, 4th editionDSM-IV).7
Cognitive impairment or disability precluded the use ofhe K-ABC in 41 index children.12 These children werevaluated using either the Griffiths Scales of Mental Devel-pment20 (in 35 children) or the NEPSY Neuropsychologyssessment21 (in 6 children). The Griffiths quotient or meanEPSY standardized score was used to estimate a score. If
his score was �40 (the lowest score on the K-ABC), then thehild was assigned a score of 39. To give a measure ofognitive function for all of the index children, these valuesere merged with the MPC to give an overall cognitive score.o other substitutions for untestable children were made for
he K-ABC subscales or in reporting other test results.Teachers rated the scholastic performance of the index
nd comparison children against the national expected level ofttainment for a child of the same age in English, mathemat-cs, science, technology, geography, history, and informationechnology. These ratings were combined to yield a totalcademic achievement score.22
Eight experienced developmental psychologists wereecruited to perform the assessments described above. Allttended a course in which they were trained in all aspects ofhe study evaluation. After the training course, every secondhild’s session was videotaped and for random quality checky the senior assessment psychologist.
tatistical AnalysisCategorical outcomes were compared using the �2 test
or trends, as appropriate, or Fisher’s exact test. Continuousutcomes were compared using an independent Student t test.ll statistical tests were 2-sided. Differences in results be-
ween the extremely preterm and comparison children andetween boys and girls (and their interactions) were evaluatedsing a generalized linear model if scales were normally dis-ributed. A priori dichotomized outcomes were determinedsing a cutoff of 2 standard deviations (SDs) or the 10th/90thercentiles as appropriate. The comparison scores served asomparison norms for all tests. Testing for the presence ofpecific learning disabilities was done using multiple regres-ion, with the overall cognitive score (MPC) as a covariate.ll analyses were then repeated after excluding children with
evere physical disability (eg, blindness, hearing loss requiringids, cerebral palsy).
RESULTS
ognitive ScoresThe mean scores for all children and boys and girls
eparately have been reported in detail previously.12 The meanPC score was 105.7 (SD � 1.8) for the comparison chil-
ren and 82.1 (SD � 19.2) for the extremely preterm chil-ren, a difference of 23.6 points (95% confidence intervalCI] � 20.3 to 26.8). In the comparison group, boys and girls
ad similar scores. In contrast, index boys (mean, 77.1 �at 25 Weeks of Gestation or Less 257
1daTp15tp
nhcCth2
L
wcc(hPnrcaca
smt.5CC
tPlamapanme
ta6mim1ctt(
To
T
A
E
A
Ma*†‡
2
9.6) scored lower than index girls (mean, 87.2 � 17.4); theifference in means was 10.1 points (95% CI � 5.4 to 14.8),nd the sex by group interaction was significant (P � .01).hese effects remained after exclusion of children with severehysical disability (mean scores: 81.9 � 15.2) and 90.6 �3.5, respectively; difference of means, 8.7 points; 95% CI �.1 to 12.3; sex by group interaction, P � .01) or when onlyhe children tested using the K-ABC were considered (4.6oints; 95% CI � 1.1 to 8.1).
Compared with the control children (contemporaryorms, 1.3%; n � 2), 98 (40.6%) extremely preterm childrenad a general cognitive ability score (MPC) ��2 SD, indi-ating moderate to severe cognitive impairment (P � .001).12
ompared with extremely preterm girls (32%; n � 38), ex-remely preterm boys (49%; n � 60) were twice as likely toave serious impairment in overall cognitive scores (OR �.1; 95% CI � 1.2 to 3.5; P � .01).
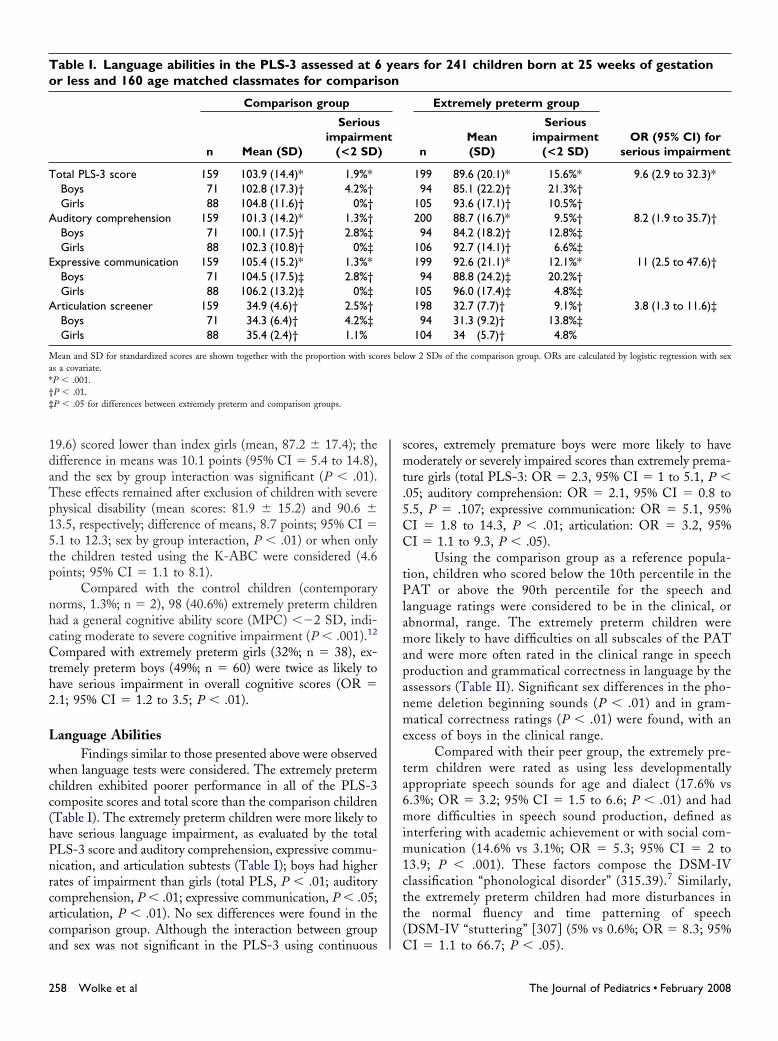
anguage AbilitiesFindings similar to those presented above were observed
hen language tests were considered. The extremely pretermhildren exhibited poorer performance in all of the PLS-3omposite scores and total score than the comparison childrenTable I). The extremely preterm children were more likely toave serious language impairment, as evaluated by the totalLS-3 score and auditory comprehension, expressive commu-ication, and articulation subtests (Table I); boys had higherates of impairment than girls (total PLS, P � .01; auditoryomprehension, P � .01; expressive communication, P � .05;rticulation, P � .01). No sex differences were found in theomparison group. Although the interaction between group
able I. Language abilities in the PLS-3 assessed at 6r less and 160 age matched classmates for comparis
Comparison group
n Mean (SD)
Seriousimpairme
(<2 SD
otal PLS-3 score 159 103.9 (14.4)* 1.9%*Boys 71 102.8 (17.3)† 4.2%†Girls 88 104.8 (11.6)† 0%†
uditory comprehension 159 101.3 (14.2)* 1.3%†Boys 71 100.1 (17.5)† 2.8%‡Girls 88 102.3 (10.8)† 0%‡
xpressive communication 159 105.4 (15.2)* 1.3%*Boys 71 104.5 (17.5)‡ 2.8%†Girls 88 106.2 (13.2)‡ 0%‡
rticulation screener 159 34.9 (4.6)† 2.5%†Boys 71 34.3 (6.4)† 4.2%‡Girls 88 35.4 (2.4)† 1.1%
ean and SD for standardized scores are shown together with the proportion with scos a covariate.P � .001.P � .01.P � .05 for differences between extremely preterm and comparison groups.
nd sex was not significant in the PLS-3 using continuous C
58 Wolke et al
cores, extremely premature boys were more likely to haveoderately or severely impaired scores than extremely prema-
ure girls (total PLS-3: OR � 2.3, 95% CI � 1 to 5.1, P �05; auditory comprehension: OR � 2.1, 95% CI � 0.8 to.5, P � .107; expressive communication: OR � 5.1, 95%I � 1.8 to 14.3, P � .01; articulation: OR � 3.2, 95%I � 1.1 to 9.3, P � .05).
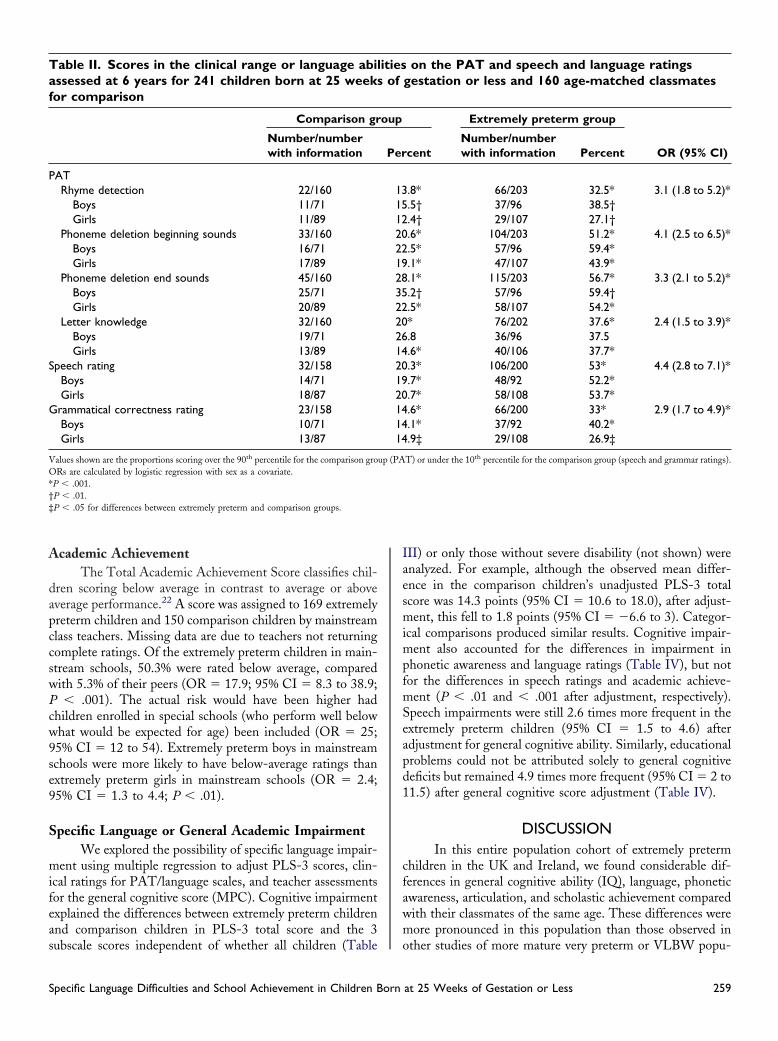
Using the comparison group as a reference popula-ion, children who scored below the 10th percentile in theAT or above the 90th percentile for the speech and
anguage ratings were considered to be in the clinical, orbnormal, range. The extremely preterm children wereore likely to have difficulties on all subscales of the PAT
nd were more often rated in the clinical range in speechroduction and grammatical correctness in language by thessessors (Table II). Significant sex differences in the pho-eme deletion beginning sounds (P � .01) and in gram-atical correctness ratings (P � .01) were found, with an
xcess of boys in the clinical range.Compared with their peer group, the extremely pre-
erm children were rated as using less developmentallyppropriate speech sounds for age and dialect (17.6% vs.3%; OR � 3.2; 95% CI � 1.5 to 6.6; P � .01) and hadore difficulties in speech sound production, defined as
nterfering with academic achievement or with social com-unication (14.6% vs 3.1%; OR � 5.3; 95% CI � 2 to
3.9; P � .001). These factors compose the DSM-IVlassification “phonological disorder” (315.39).7 Similarly,he extremely preterm children had more disturbances inhe normal fluency and time patterning of speechDSM-IV “stuttering” [307] (5% vs 0.6%; OR � 8.3; 95%
rs for 241 children born at 25 weeks of gestation
Extremely preterm group
OR (95% CI) forserious impairmentn
Mean(SD)
Seriousimpairment
(<2 SD)
199 89.6 (20.1)* 15.6%* 9.6 (2.9 to 32.3)*94 85.1 (22.2)† 21.3%†
105 93.6 (17.1)† 10.5%†200 88.7 (16.7)* 9.5%† 8.2 (1.9 to 35.7)†94 84.2 (18.2)† 12.8%‡
106 92.7 (14.1)† 6.6%‡199 92.6 (21.1)* 12.1%* 11 (2.5 to 47.6)†94 88.8 (24.2)‡ 20.2%†
105 96.0 (17.4)‡ 4.8%‡198 32.7 (7.7)† 9.1%† 3.8 (1.3 to 11.6)‡94 31.3 (9.2)† 13.8%‡
104 34 (5.7)† 4.8%
ow 2 SDs of the comparison group. ORs are calculated by logistic regression with sex
yeaon
nt)
res bel
I � 1.1 to 66.7; P � .05).
The Journal of Pediatrics • February 2008
A
dapccswPcw9se9
S
mifeas
IaesmimpfmSeapd1
cfawm
Taf
P
S
G
VO*†‡
S
cademic AchievementThe Total Academic Achievement Score classifies chil-
ren scoring below average in contrast to average or aboveverage performance.22 A score was assigned to 169 extremelyreterm children and 150 comparison children by mainstreamlass teachers. Missing data are due to teachers not returningomplete ratings. Of the extremely preterm children in main-tream schools, 50.3% were rated below average, comparedith 5.3% of their peers (OR � 17.9; 95% CI � 8.3 to 38.9;� .001). The actual risk would have been higher had
hildren enrolled in special schools (who perform well belowhat would be expected for age) been included (OR � 25;5% CI � 12 to 54). Extremely preterm boys in mainstreamchools were more likely to have below-average ratings thanxtremely preterm girls in mainstream schools (OR � 2.4;5% CI � 1.3 to 4.4; P � .01).
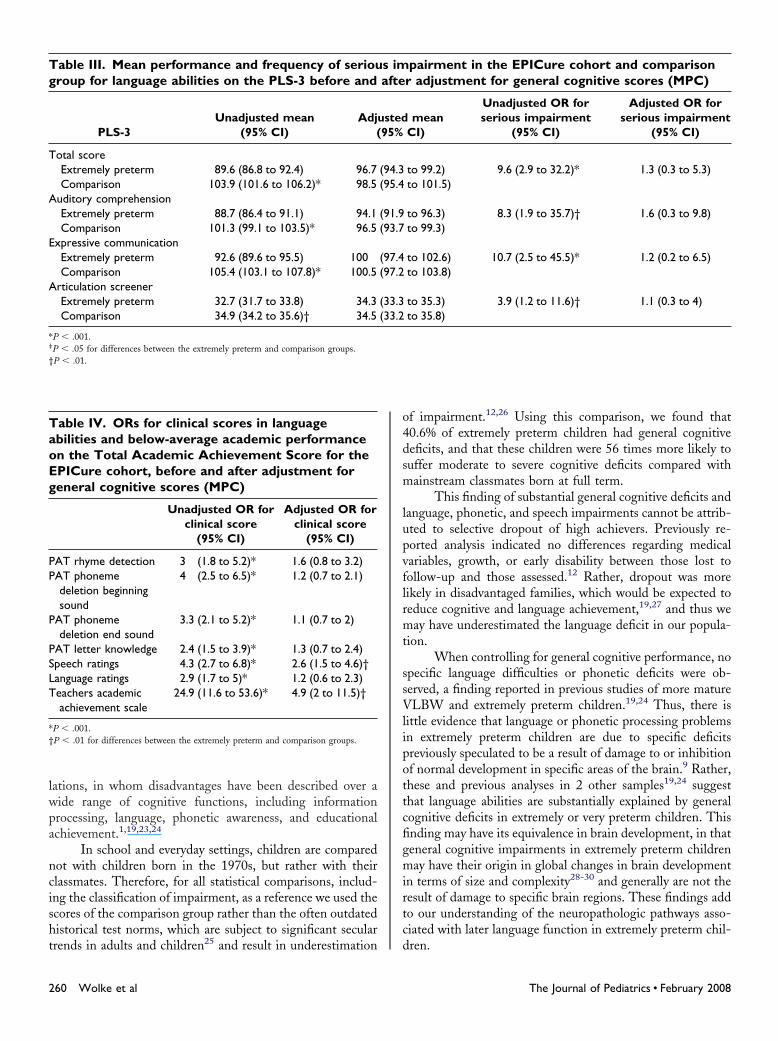
pecific Language or General Academic ImpairmentWe explored the possibility of specific language impair-
ent using multiple regression to adjust PLS-3 scores, clin-cal ratings for PAT/language scales, and teacher assessmentsor the general cognitive score (MPC). Cognitive impairmentxplained the differences between extremely preterm childrennd comparison children in PLS-3 total score and the 3
able II. Scores in the clinical range or language abilssessed at 6 years for 241 children born at 25 weeksor comparison
Comparison gr
Number/numberwith information
ATRhyme detection 22/160
Boys 11/71Girls 11/89
Phoneme deletion beginning sounds 33/160Boys 16/71Girls 17/89
Phoneme deletion end sounds 45/160Boys 25/71Girls 20/89
Letter knowledge 32/160Boys 19/71Girls 13/89
peech rating 32/158Boys 14/71Girls 18/87rammatical correctness rating 23/158Boys 10/71Girls 13/87
alues shown are the proportions scoring over the 90th percentile for the comparison groRs are calculated by logistic regression with sex as a covariate.
P � .001.P � .01.P � .05 for differences between extremely preterm and comparison groups.
ubscale scores independent of whether all children (Table o
pecific Language Difficulties and School Achievement in Children Born
II) or only those without severe disability (not shown) werenalyzed. For example, although the observed mean differ-nce in the comparison children’s unadjusted PLS-3 totalcore was 14.3 points (95% CI � 10.6 to 18.0), after adjust-ent, this fell to 1.8 points (95% CI � �6.6 to 3). Categor-
cal comparisons produced similar results. Cognitive impair-ent also accounted for the differences in impairment in
honetic awareness and language ratings (Table IV), but notor the differences in speech ratings and academic achieve-ent (P � .01 and � .001 after adjustment, respectively).
peech impairments were still 2.6 times more frequent in thextremely preterm children (95% CI � 1.5 to 4.6) afterdjustment for general cognitive ability. Similarly, educationalroblems could not be attributed solely to general cognitiveeficits but remained 4.9 times more frequent (95% CI � 2 to1.5) after general cognitive score adjustment (Table IV).
DISCUSSIONIn this entire population cohort of extremely preterm
hildren in the UK and Ireland, we found considerable dif-erences in general cognitive ability (IQ), language, phoneticwareness, articulation, and scholastic achievement comparedith their classmates of the same age. These differences wereore pronounced in this population than those observed in
on the PAT and speech and language ratingsgestation or less and 160 age-matched classmates
Extremely preterm group
OR (95% CI)centNumber/numberwith information Percent
.8* 66/203 32.5* 3.1 (1.8 to 5.2)*
.5† 37/96 38.5†
.4† 29/107 27.1†
.6* 104/203 51.2* 4.1 (2.5 to 6.5)*
.5* 57/96 59.4*
.1* 47/107 43.9*
.1* 115/203 56.7* 3.3 (2.1 to 5.2)*
.2† 57/96 59.4†
.5* 58/107 54.2** 76/202 37.6* 2.4 (1.5 to 3.9)*.8 36/96 37.5.6* 40/106 37.7*.3* 106/200 53* 4.4 (2.8 to 7.1)*.7* 48/92 52.2*.7* 58/108 53.7*.6* 66/200 33* 2.9 (1.7 to 4.9)*.1* 37/92 40.2*.9‡ 29/108 26.9‡
T) or under the 10th percentile for the comparison group (speech and grammar ratings).
itiesof
oup
Per
131512202219283522202614201920141414
up (PA
ther studies of more mature very preterm or VLBW popu-
at 25 Weeks of Gestation or Less 259
lwpa
ncisht
o4dsm
lupvflrmt
ssVlipottcfigmirtc
Tg
T
A
E
A
*‡
†
TaoEg
PP
P
PSLT
*†
2
ations, in whom disadvantages have been described over aide range of cognitive functions, including informationrocessing, language, phonetic awareness, and educationalchievement.1,19,23,24
In school and everyday settings, children are comparedot with children born in the 1970s, but rather with theirlassmates. Therefore, for all statistical comparisons, includ-ng the classification of impairment, as a reference we used thecores of the comparison group rather than the often outdatedistorical test norms, which are subject to significant secular
able III. Mean performance and frequency of seriouroup for language abilities on the PLS-3 before and
PLS-3Unadjusted mean
(95% CI)Adju
(
otal scoreExtremely preterm 89.6 (86.8 to 92.4) 96.7Comparison 103.9 (101.6 to 106.2)* 98.5
uditory comprehensionExtremely preterm 88.7 (86.4 to 91.1) 94.1Comparison 101.3 (99.1 to 103.5)* 96.5
xpressive communicationExtremely preterm 92.6 (89.6 to 95.5) 100Comparison 105.4 (103.1 to 107.8)* 100.5
rticulation screenerExtremely preterm 32.7 (31.7 to 33.8) 34.3Comparison 34.9 (34.2 to 35.6)† 34.5
P � .001.P � .05 for differences between the extremely preterm and comparison groups.P � .01.
able IV. ORs for clinical scores in languagebilities and below-average academic performancen the Total Academic Achievement Score for thePICure cohort, before and after adjustment foreneral cognitive scores (MPC)
Unadjusted OR forclinical score
(95% CI)
Adjusted OR forclinical score
(95% CI)
AT rhyme detection 3 (1.8 to 5.2)* 1.6 (0.8 to 3.2)AT phonemedeletion beginningsound
4 (2.5 to 6.5)* 1.2 (0.7 to 2.1)
AT phonemedeletion end sound
3.3 (2.1 to 5.2)* 1.1 (0.7 to 2)
AT letter knowledge 2.4 (1.5 to 3.9)* 1.3 (0.7 to 2.4)peech ratings 4.3 (2.7 to 6.8)* 2.6 (1.5 to 4.6)†anguage ratings 2.9 (1.7 to 5)* 1.2 (0.6 to 2.3)eachers academicachievement scale
24.9 (11.6 to 53.6)* 4.9 (2 to 11.5)†
P � .001.P � .01 for differences between the extremely preterm and comparison groups.
rends in adults and children25 and result in underestimation d
60 Wolke et al
f impairment.12,26 Using this comparison, we found that0.6% of extremely preterm children had general cognitiveeficits, and that these children were 56 times more likely touffer moderate to severe cognitive deficits compared withainstream classmates born at full term.
This finding of substantial general cognitive deficits andanguage, phonetic, and speech impairments cannot be attrib-ted to selective dropout of high achievers. Previously re-orted analysis indicated no differences regarding medicalariables, growth, or early disability between those lost toollow-up and those assessed.12 Rather, dropout was moreikely in disadvantaged families, which would be expected toeduce cognitive and language achievement,19,27 and thus weay have underestimated the language deficit in our popula-
ion.When controlling for general cognitive performance, no
pecific language difficulties or phonetic deficits were ob-erved, a finding reported in previous studies of more matureLBW and extremely preterm children.19,24 Thus, there is
ittle evidence that language or phonetic processing problemsn extremely preterm children are due to specific deficitsreviously speculated to be a result of damage to or inhibitionf normal development in specific areas of the brain.9 Rather,hese and previous analyses in 2 other samples19,24 suggesthat language abilities are substantially explained by generalognitive deficits in extremely or very preterm children. Thisnding may have its equivalence in brain development, in thateneral cognitive impairments in extremely preterm childrenay have their origin in global changes in brain development
n terms of size and complexity28-30 and generally are not theesult of damage to specific brain regions. These findings addo our understanding of the neuropathologic pathways asso-iated with later language function in extremely preterm chil-
pairment in the EPICure cohort and comparisonr adjustment for general cognitive scores (MPC)
meanCI)
Unadjusted OR forserious impairment
(95% CI)
Adjusted OR forserious impairment
(95% CI)
to 99.2) 9.6 (2.9 to 32.2)* 1.3 (0.3 to 5.3)to 101.5)
to 96.3) 8.3 (1.9 to 35.7)† 1.6 (0.3 to 9.8)to 99.3)
to 102.6) 10.7 (2.5 to 45.5)* 1.2 (0.2 to 6.5)to 103.8)
to 35.3) 3.9 (1.2 to 11.6)† 1.1 (0.3 to 4)to 35.8)
s imafte
sted95%
(94.3(95.4
(91.9(93.7
(97.4(97.2
(33.3(33.2
ren.
The Journal of Pediatrics • February 2008

eIcmcObarpaWsrtgsemmeFtptdTpe
ipshftttniipamls
tccoaldc
ttactmm
cmmmetosfiriaagv
1Si2i3pa4m5b6c47D8fP9b1sc1c21d1SP1N21M1A
S
In contrast, speech problems and a global rating ofducational difficulties could not be explained solely by lowerQ, a finding replicating the results reported for VLBWhildren in Germany.19 Speech difficulties often involve oralotor problems31 and may be significantly affected by spe-
ific motor problems and controlled by specific brain areas.ral motor problems, such as in eating difficulties, have long
een suspected to be associated with later speech problems32
nd warrant further exploration. Furthermore, our findingsegarding educational problems are consistent with those re-orted by Taylor et al,24 who found specific mathematicalchievement deficits in children with birth weight �750 g.
olke and Meyer19 found that numerical abilities were notolely accounted for by IQ in a German VLBW sample. Aecent longitudinal study comparing extremely and very pre-erm children and full-term control children showed thateneral cognitive impairment had a strong initial impact onpecific abilities (phonetic accuracy, letter and number knowl-dge) that are prerequisites for learning reading, writing, andathematical skills. However, attained reading, writing, andathematical abilities are the mediating link to longer-term
ducational success in both full-term and preterm children.4
urthermore, other factors, such as working memory,33 at-ention deficit and peer relationship problems,1,34 motorroblems,35 and family socioeconomic factors,4,24 also con-ribute to educational problems in extremely premature chil-ren and need to be further explored in longitudinal analysis.his is relevant, because motor or behavioral managementrograms may be able to increase educational performance inxtremely preterm children.
A range of adverse perinatal outcomes has been describedn males, ranging from death,36 perinatal brain injury,37 cerebralalsy, and delayed lung maturation38 to preterm birth andtillbirth. Significant sex differences in cognitive functioningave been reported in some cohorts38 but not in others.19 Weound a substantial and clinically relevant increase in cogni-ive, language, and educational difficulties in extremely pre-erm boys compared with extremely preterm girls. This is inhe context of the lower survival and greater frequency ofeonatal problems13 and higher rates of disability14 in males
n this population. It may be speculated that sex differences inntrauterine development may make the male fetus/extremelyreterm infant particularly vulnerable to perinatal adversitynd may have important consequences for later develop-ent.39 The gestational age at which male vulnerability is no
onger demonstrable remains to be determined, but it wouldeem to be particularly evident at very low gestational age.
The present study has some limitations. We requiredhe cooperation of the children’s teachers to obtain parentalonsent to communicate the contact details of the controlhildren to the investigators. Lack of teacher cooperation orf parental consent was the major reason why we did not haveclass control for all target children. We found no pattern or
ack of cooperation according to regional variation or socialeprivation in the area that the school was serving; thus, we
onsider any bias to be minimal. All assessors were unaware of1P
pecific Language Difficulties and School Achievement in Children Born
he children’s group status and family background; however,otal blinding throughout the assessment may not have beenchieved in all cases, considering that the extremely pretermhildren were on average smaller, more often required correc-ion for sight, and more often had a motor disability. Thisay have provided clues to the assessors regarding groupembership.
In conclusion, our findings demonstrate that adverseognitive, language, phonetic, and educational sequelae areore frequent in extremely premature children than in moreature preterm populations and that the cognitive impair-ent is general rather than specific. Cognitive impairments
xplain only part of the educational difficulties experienced byhese children, and future analysis needs to take into accountther areas of function, including behavioral, motor, andocial difficulties. Our findings of patterns of functional dif-culties may have important implications for brain imagingesearch.40 Extremely preterm birth and very early extrauter-ne development may alter the pattern of brain developmentcross a range of brain regions, including all areas of the cortexnd deeper brain structures,28 and may be responsible for thelobal deficits in neuropsychological function seen in thisulnerable population.
REFERENCES. Saigal S, denOuden L, Wolke D, Hoult L, Paneth N, Streiner DL, et al.chool-age outcomes in children who were extremely low birth weight from four
nternational population-based cohorts. Pediatrics 2003;112:943-50.. Wolke D. Language problems in neonatal at risk children: towards an understand-ng of developmental mechanisms. Acta Paediatr 1999;88:488-90.. Largo RH, Molinari L, Kundu S, Duc G. Intellectual outcome, speech and schoolerformance in high-risk preterm children with birth weight appropriate for gestationalge. Eur J Pediatr 1990;149:845-50.. Schneider W, Wolke D, Schlagmüller M, Meyer R. Pathways to school achieve-ent in very preterm and full-term children. Eur J Psychol Educ 2004;19:385-406.
. Taylor HG, Minich N, Klein N, Hack M. Longitudinal outcomes of very lowirth weight: neuropsychological findings. J Int Neuropsychol Soc 2004;10:149-63.. Dyck MJ, Hay D, Anderson M, Smith LM, Piek J, Hallmayer J. Is the discrepancyriterion for defining developmental disorders valid? J Child Psychol Psychiatry 2004;5:979-95.. Diagnostic and Statistical Manual of Mental Disorders. 4th edition. Washington,C: American Psychiatric Association; 1994.
. Clegg J, Hollis C, Mawhood L, Rutter M. Developmental language disorders: aollow-up in later adult life. Cognitive, language and psychosocial outcomes. J Childsychol Psychiatry 2005;46:128-49.. Mutch L, Leyland A, McGee A. Patterns of neuropsychological function in a lowirth weight population. Dev Med Child Neurol 1993;35:943-56.0. Saigal S, Szatmarl P, Rosenbaum P, Campbell D, King S. Cognitive abilities andchool performance of extremely low birth weight children and matched term controlhildren at age 8 years: a regional study. J Pediatr 1991;118:751-60.1. Fanaroff AA, Hack M, Walsh MC. The NICHD neonatal research network:hanges in practice and outcomes during the first 15 years. Semin Perinatol 2003;7:281-7.2. Marlow N, Wolke D, Bracewell MA, Samara M. Neurologic and developmentalisability at 6 years of age after extremely preterm birth. N Engl J Med 2005;352:9-19.3. Costeloe K, Hennessy E, Gibson AT, Marlow N, Wilkinson AR. The EPIcuretudy: outcomes to discharge from hospital for infants born at the threshold of viability.ediatrics 2000;106:659-71.4. Wood NS, Marlow N, Costeloe K, Gibson AT, Wilkinson AR, Group ES.eurologic and developmental disability after extremely preterm birth. N Engl J Med
000;343:378-84.5. Kaufman A, Kaufman N. Kaufman Assessment Battery for Children. Circle Pines,N: American Guidance Service, 1983.
6. Zimmermann IL, Steiner VG, Pond RE. Preschool Language Scale-3. Sanntonio, TX: Harcourt Brace Jovanovich; 1992.
7. Muter V, Hulme C, Snowling M. Phonological Abilities Test (PAT). London:sychological Testing Corp; 1997.
at 25 Weeks of Gestation or Less 261

1rP16M2M2N12i2M2s212pm2sA2s2
m23c3Cl3iE3eJ3BL3M3233l34d
2
8. Bryant P, Nunes T, Bindman M. Awareness of language in children who haveeading difficulties: historical comparisons in a longitudinal study. J Child Psycholsychiatry 1998;39:501-10.9. Wolke D, Meyer R. Cognitive status, language attainment and prereading skills of-year-old very preterm children and their peers: the Bavarian Longitudinal Study. Deved Child Neurol 1999;41:94-109.
0. Griffiths R. Abilities of Young Children: A Comprehensive System of Mentaleasurement for the First 8 Years of Life. Somerset, UK: Young and Son; 1970.
1. Korkman M, Kirk U, Kemp S. Manual for the NEPSY: A Developmentaleuropsychological Assessment. San Antonio, TX: Harcourt Brace Jovanovich;
998.2. Wolke D, Rizzo P, Woods S. Persistent infant crying and hyperactivity problemsn middle childhood. Pediatrics 2002;109:1054-60.3. Aylward GP. Cognitive and neuropsychological outcomes: More than IQ scores.ent Retard Dev Disabil Res Rev 2002;8:234-40.
4. Taylor HG, Burant CJ, Holding PA, Klein N, Hack M. Sources of variability inequelae of very low birth weight. Child Neuropsychol 2002;8:163-78.5. Flynn JR. Searching for justice: the discovery of IQ gains over time. Am Psychol999;54:5-20.6. Wolke D, Ratschinski G, Ohrt B, Riegel K. The cognitive outcome of veryreterm infants may be poorer than often reported: an empirical investigation of howethodological issues make a big difference. Eur J Pediatr 1994;153:906-15.
7. Laucht M, Esser G, Baving L, Gerhold M, Hoesch I, Ihle W, et al. Behavioralequelae of perinatal insults and early family adversity at 8 years of age. J Am Acad Childdolesc Psychiatry 2000;39:1229-37.
8. Inder TE, Warfield SK, Wang H, Huppi PS, Volpe JJ. Abnormal cerebral
tructure is present at term in premature infants. Pediatrics 2005;115:286-94.9. Kesler SR, Ment LR, Vohr B, Pajot SK, Schneider KC, Katz KH, et al. Volu- 262 Wolke et al
etric analysis of regional cerebral development in preterm children. Pediatr Neurol004;31:318-25.0. MacKendrick W. Understanding neurodevelopment in premature infants: appliedhaos theory. J Pediatr 2006;148:427-9.1. Rejno-Habte Selassie G, Jennische M, Kyllerman M, Viggedal G, Hartelius L.omorbidity in severe developmental language disorders: neuropediatric and psycho-
ogical considerations. Acta Paediatr 2005;94:471-8.2. Reilly S, Skuse D, Wolke D. The nature and consequences of feeding problems innfancy. In: Cooper PJ, Stein A, editors. Childhood Feeding Problems and Adolescentating Disorders. London: Routledge; 2006. p 7-40.3. Sansavini A, Guarini A, Alessandroni R, Faldella G, Giovanelli G, Salvioli G. Arearly grammatical and phonological working memory abilities affected by preterm birth?Commun Disord 2007;40:239–56.4. Hille ETM, den Ouden AL, Saigal S, Wolke D, Lambert M, Whitaker A, et al.ehavioural problems in children who weigh 1000 g or less at birth in four countries.ancet 2001;357:1641-3.5. Bracewell M, Marlow N. Patterns of motor disability in very preterm children.ent Retard Dev Disabil Res Rev 2002;8:241-8.
6. Mizuno R. The male/female ratio of fetal deaths and births in Japan. Lancet000;357:738-9.7. Edwards D. Brain protection for girls and boys. J Pediatr 2004;145:723-4.8. Brothwood M, Wolke D, Gamsu H, Benson J, Cooper D. Prognosis of the veryow birth weight baby in relation to sex. Arch Dis Child 1986;61:559-64.9. Kraemer S. The fragile male. BMJ 2000;321:1609-12.0. Woodward LJ, Edgin JO, Thompson D, Inder TE. Object working memoryeficits predicted by early brain injury and development in the preterm infant. Brain
005;128:2578-87.The Journal of Pediatrics • February 2008

(dDgHrMM
a(
ccaoo
S
APPENDIXThe EPICure Investigator Group: K Costeloe
London), AT Gibson (Sheffield), EM Hennessy (Lon-on), N Marlow (Nottingham), AR Wilkinson (Oxford),
Wolke (Warwick). Developmental Panel: Psycholo-ists: Emma Luck, Catherine Bamford, Helen Betteridge,anne Bruhn, Sandra Johnson, Iliana Magiati, Maria Mo-
ahan, Isabel Tsverik. Paediatricians: Melanie Bracewell,ichele Cruwys, Ruth MacGregor, Lesley McDonald,
argaret Morton, Margaret Morris, Sue Thomas. Muth- lpecific Language Difficulties and School Achievement in Children Born
nna Samara (Psychological data analysis), Heather PalmerStudy Administrator).
Funding: BLISS, PPP Foundation and WellBeing.The EPICure Study Group comprises the paediatri-
ians in 276 maternity units across the UK and Ireland whoontributed data to the study, whose invaluable help wecknowledge. The investigator group was responsible for theriginal study cohort identification and studies up to 2.5 yearsf age and the developmental panel performed the data col-
ection and validation.at 25 Weeks of Gestation or Less 262.e1





























