Embed Size (px)
Citation preview
Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/51392746
Smokingtoself-medicateattentionalandemotionaldysfunctions
ArticleinNicotine&TobaccoResearch·November2007
DOI:10.1080/14622200701685039·Source:PubMed
CITATIONS
79
READS
108
8authors,including:
Jean-G.Gehricke
UniversityofCalifornia,Irvine
28PUBLICATIONS599CITATIONS
SEEPROFILE
StevenGPotkin
UniversityofCalifornia,Irvine
268PUBLICATIONS7,837CITATIONS
SEEPROFILE
JamesFallon
UniversityofCalifornia,Irvine
201PUBLICATIONS12,842CITATIONS
SEEPROFILE
LarryJamner
UniversityofCalifornia,Irvine
66PUBLICATIONS3,475CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyJean-G.Gehrickeon30November2016.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.
Review
Smoking to self-medicate attentional and emotionaldysfunctions
Jean-G. Gehricke, Sandra E. Loughlin, Carol K. Whalen, Steven G. Potkin,James H. Fallon, Larry D. Jamner, James D. Belluzzi, Frances M. Leslie
Received 3 April 2007; accepted 3 August 2007
Individuals with attentional and emotional dysfunctions are most at risk for smoking initiation and subsequentnicotine addiction. This article presents converging findings from human behavioral research, brain imaging, andbasic neuroscience on smoking as self-medication for attentional and emotional dysfunctions. Nicotine and othertobacco constituents have significant effects on neural circuitry underlying the regulation of attention and affect. Age,sex, early environment, and exposure to other drugs have been identified as important factors that moderate both theeffects of nicotine on brain circuitry and behavior and the risk for smoking initiation. Findings also suggest that theeffects of smoking differ depending on whether smoking is used to regulate attention or affect. Individual differencesin the reinforcement processes underlying tobacco use have implications for the development of tailored smokingcessation programs and prevention strategies that include early treatment of attentional and emotional dysfunctions.
Introduction
Smoking prevalence rates in the general population
have shown a steady decline in recent years because
of increased efforts of anti-smoking campaigns and
smoking bans in many states. However, overall
smoking prevalence rates may have reached a
plateau. Some studies suggest that individuals with
attentional and emotional dysfunctions continue to
smoke at high rates and are less successful with
smoking cessation (Acierno et al., 2000; Beckham,
1999; Beckham et al., 1997; Breslau, 1995; Breslau,
Davis, & Schultz, 2003; de Leon, Diaz, Rogers,
Browne, & Dinsmore, 2002; Dierker, Avenevoli,
Merikangas, Flaherty, & Stolar, 2001; Glassman
et al., 1990; Glassman et al., 1988; Kendler et al.,
1993; Kollins, McClernon, & Fuemmeler, 2005;
Marmorstein & Iacono, 2003; O. F. Pomerleau,
Downey, Stelson, & Pomerleau, 1995; Rohde,
Kahler, Lewinsohn, & Brown, 2004; Sonntag,
Wittchen, Hofler, Kessler, & Stein, 2000;
Upadhyaya, Brady, Wharton, & Liao, 2003). With
the majority of smokers beginning to smoke by age
18 (Johnston, O’Malley, & Bachman, 1998), adoles-
cents with attentional and emotional dysfunctions
also have a higher risk for smoking compared with
those without such problems (Stevens, Colwell,
Smith, Robinson, & McMillan, 2005; J. W. Weiss
et al., 2005; Whalen, Jamner, Henker, & Delfino,
2001; Whalen, Jamner, Henker, Delfino, & Lozano,
2002). Adolescents may self-medicate with tobacco
to regulate negative affect associated with attentional
and emotional dysfunctions (Whalen et al., 2001;
Whalen et al., 2002). The notion that individuals with
specific deficits smoke for purposes of self-
medication (Khantzian, 1997; C. S. Pomerleau,
Marks, & Pomerleau, 2000) is supported by evidence
that nicotine treatment can attenuate dysfunction in
depression (Haro & Drucker-Colin, 2004a, 2004b)
ISSN 1462-2203 print/ISSN 1469-994X online # 2007 Society for Research on Nicotine and Tobacco
DOI: 10.1080/14622200701685039
Jean-G. Gehricke, Ph.D., Steven G. Potkin, M.D., Department of
Psychiatry and Human Behavior; Sandra E. Loughlin, Ph.D., Frances
M. Leslie, Ph.D., Department of Pharmacology; James H. Fallon,
Ph.D., Department of Anatomy and Neurobiology; Carol K. Whalen,
Ph.D., Larry D. Jamner, Ph.D., Department of Psychology and Social
Behavior, University of California, Irvine, Irvine, CA.
Correspondence: Jean-G. Gehricke, Ph.D., Department of
Psychiatry and Human Behavior, D402 Medical Sciences I, Irvine,
CA 92697-1675, USA. Tel: +1 (949) 824-1834; Fax: +1 (949) 824-1811;
E-mail: [email protected]
Nicotine & Tobacco Research Volume 9, Supplement 4 (December 2007) S523–S536
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
and attention-deficit/hyperactivity disorder (ADHD;
Levin, Conners, Silva, Canu, & March, 2001).
Individuals with deficits in attention may be
self-medicating with nicotine to improve their atten-
tion (Bekker, Bocker, Van Hunsel, van den Berg, &
Kenemans, 2005; Gehricke, Whalen, Jamner, Wigal,
& Steinhoff, 2006). In contrast, individuals with
affective dysfunctions may be self-medicating to
regulate their emotions (Haro & Drucker-Colin,
2004b).
This review integrates findings from the
Transdisciplinary Tobacco Use Research Center of
the University of California, Irvine (UCI TTURC) in
the context of the existing literature on links between
smoking and attentional and emotional dysfunction.
Attentional and emotional dysfunctions are asso-
ciated with externalizing and internalizing behavior
problems. Externalizing behavior problems include
ADHD, oppositional defiant disorder (ODD), and
conduct disorder (CD). Internalizing behavior pro-
blems, on the other hand, include major depression,
anxiety disorders, and their corresponding subclini-
cal manifestations of negative affect. Externalizing
and internalizing disorders frequently co-occur
(Busch et al., 2002; Jensen et al., 2001; Jensen,
Martin, & Cantwell, 1997; McGough et al., 2005;
Kendall, Brady Verduin, 2001; Kessler et al., 2006),
and such comorbidities may increase the risk for
smoking (Ernst et al., 2006; Marmorstein & Iacono,
2003; Milberger, Biederman, Faraone, Chen, &
Jones, 1997). However, the reinforcing effects of
smoking in externalizing and internalizing disorders
may vary depending on the predominance of atten-
tional or emotional dysfunctions.
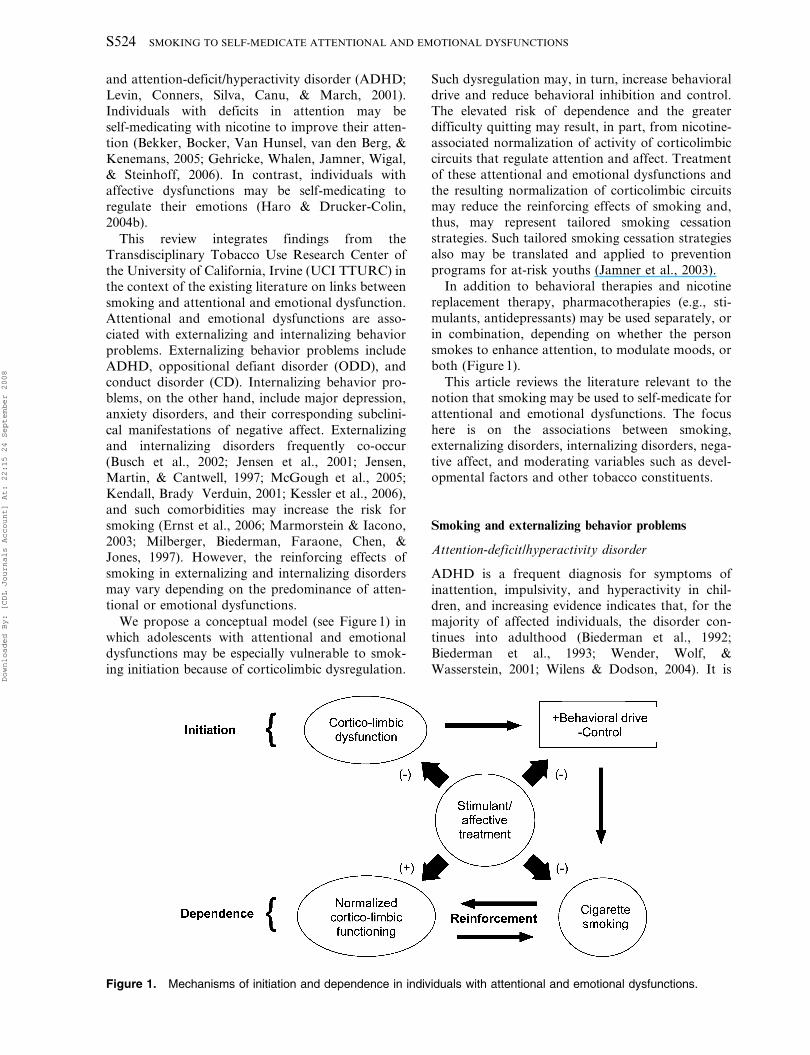
We propose a conceptual model (see Figure 1) in
which adolescents with attentional and emotional
dysfunctions may be especially vulnerable to smok-
ing initiation because of corticolimbic dysregulation.
Such dysregulation may, in turn, increase behavioral
drive and reduce behavioral inhibition and control.
The elevated risk of dependence and the greater
difficulty quitting may result, in part, from nicotine-
associated normalization of activity of corticolimbiccircuits that regulate attention and affect. Treatment
of these attentional and emotional dysfunctions and
the resulting normalization of corticolimbic circuits
may reduce the reinforcing effects of smoking and,
thus, may represent tailored smoking cessation
strategies. Such tailored smoking cessation strategies
also may be translated and applied to prevention
programs for at-risk youths (Jamner et al., 2003).
In addition to behavioral therapies and nicotine
replacement therapy, pharmacotherapies (e.g., sti-
mulants, antidepressants) may be used separately, or
in combination, depending on whether the person
smokes to enhance attention, to modulate moods, or
both (Figure 1).
This article reviews the literature relevant to the
notion that smoking may be used to self-medicate for
attentional and emotional dysfunctions. The focus
here is on the associations between smoking,
externalizing disorders, internalizing disorders, nega-
tive affect, and moderating variables such as devel-opmental factors and other tobacco constituents.
Smoking and externalizing behavior problems
Attention-deficit/hyperactivity disorder
ADHD is a frequent diagnosis for symptoms of
inattention, impulsivity, and hyperactivity in chil-
dren, and increasing evidence indicates that, for themajority of affected individuals, the disorder con-
tinues into adulthood (Biederman et al., 1992;
Biederman et al., 1993; Wender, Wolf, &
Wasserstein, 2001; Wilens & Dodson, 2004). It is
Figure 1. Mechanisms of initiation and dependence in individuals with attentional and emotional dysfunctions.
S524 SMOKING TO SELF-MEDICATE ATTENTIONAL AND EMOTIONAL DYSFUNCTIONS
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
estimated that ADHD affects approximately 7% of
children (Barbaresi et al., 2004; Barbaresi et al., 2002)
and 2%–6% of adults (Kessler et al., 2006; M. Weiss
& Murray, 2003). In a landmark study, O. F.
Pomerleau and colleagues (1995) reported that adults
with ADHD have elevated smoking prevalence (40%)
and reduced quit rates (29%) compared with the
general population (26% and 48.5%, respectively).
Several other studies have documented relationships
between smoking and ADHD in adolescents
(Barkley et al., 1990; Chilcoat & Breslau, 1999;
Fergusson, Lynskey, & Horwood, 1996; Hartsough
& Lambert, 1987; Lambert & Hartsough, 1998;
Milberger et al., 1997; Riggs, Mikulich, Whitmore,
& Crowley, 1999). These relationships are likely to be
causal because an ADHD diagnosis implies that
some symptoms occur prior to age 7, which means
they always precede the onset of smoking. However,
contradictory findings exist on which aspect of
ADHD (i.e., inattention vs. hyperactivity-
impulsivity) shows stronger relationships with
smoking (Burke, Loeber, & Lahey, 2001; Molina,
Smith, & Pelham, 1999) and whether ADHD subtype
interacts with gender in predicting smoking (Galera,
Fombonne, Chastang, & Bouvard, 2005). A recent
study by Kollins and colleagues (2005), using a
nationally representative sample of young adults,
revealed that the number of retrospectively reported
ADHD symptoms was associated with lifetime
smoking, with each additional ADHD symptom
conferring additional risk for regular smoking.
Hyperactive-impulsive symptoms were found to be
a better predictor of lifetime smoking than were
inattentive symptoms.
Our UCI TTURC used a different approach to
examine links between ADHD and smoking.
Adolescents who were participating in a longitudinal
study of smoking trajectories reported their moods,
contexts, and behaviors (including smoking) twice
each waking hour, across two 4-day recording
intervals. Based on parent ratings, the 153 9th-grade
participants were divided into subgroups with low,
middle, or high levels of ADHD characteristics.
Findings revealed that ADHD characteristics were
associated with an increased risk of smoking and
alcohol consumption as well as elevated rates of
negative affect (Whalen et al., 2002). More specifi-
cally, adolescents with high, in contrast to low,
ADHD symptom levels recorded more negative and
fewer positive moods, lower alertness, and more
tobacco and alcohol use. These findings suggest that,
even at subclinical levels, ADHD characteristics are
associated with behavior patterns and contexts that
may promote unhealthy lifestyle behaviors and
vulnerability to nicotine dependence. A limitation
of the present study was that comorbid ODD and
CD symptoms were not examined.
ADHD comorbidities
Studies have shown that 38%–68% of adolescents
with diagnosed ADHD have comorbid ODD
(Barkley et al., 1991; Barkley et al., 1990;
Biederman, Newcorn, & Sprich, 1991; Fischer et al.,
1990), major depression (Busch et al., 2002; Kessler
et al., 2006), or anxiety disorders (Kessler et al.,
2006). ODD is characterized by a recurrent pattern
of negativism, defiance, disobedience, and hostility to
authority (American Psychiatric Association, 2000).
Although inconsistencies are found across studies,
strong evidence indicates that approximately half of
adolescents with ADHD meet criteria for CD
(Biederman et al., 1991; Jensen et al., 1997), which
is characterized by deceitfulness, rule violations, and
aggressive conduct (American Psychiatric
Association, 2000).
Milberger et al. (1997) examined the role of
comorbidities as predictors of smoking in a study
of 128 children with ADHD and 109 non-ADHD
controls who were assessed at baseline and 4-year
follow-up. Children and adolescents with ADHD
and comorbid mood, conduct, or anxiety disorders
were at higher risk for smoking than were those
without comorbid diagnoses. In particular, CD was
a predictor of smoking independent of ADHD. In
addition, Marmorstein and Iacono (2003) showed
that co-occurrence of CD and major depression in
adolescents was associated with greater nicotine
dependence compared with a single diagnosis of
either CD or major depression. Moreover, in a
longitudinal study (Ernst et al., 2006), aggression was
the strongest predictor of tobacco smoking and
marijuana use in adolescents with and without
ADHD, findings that support Milberger et al.’s
results. Thus negative affect associated with externa-
lizing behavior problems may contribute to an
increased risk for smoking. Unfortunately, little is
known about the reinforcing effects of smoking and
nicotine in ODD and CD. However, some studies
have examined the effects of nicotine on attentional
dysfunctions associated with ADHD.
The effects of nicotine in attentional dysfunctions
A number of research studies have examined the
direct effects of nicotine on ADHD symptoms and
have shown that acute nicotine administration
improves concentration and reduces clinical symp-
toms as well as shortens and homogenizes reaction
times in adult smokers and nonsmokers with ADHD
(Conners et al., 1996; Levin et al., 1996). In one
illustrative study, Levin and colleagues (2001)
randomly assigned adult nonsmokers with ADHD
to one of four 4-week treatment conditions (i.e.,
nicotine patch only, nicotine patch with a fixed dose
of 5-mg/day methylphenidate, methylphenidate only,
NICOTINE & TOBACCO RESEARCH S525
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
and placebo). Acute administration of nicotine
improved clinical symptoms of ADHD and self-
reported depression and also increased consistency
on a continuous performance task, compared with
methylphenidate, nicotine in combination with
methylphenidate, or placebo. In contrast, during
the chronic treatment phase, no differences were
found in clinical symptom ratings, but the antide-
pressant effect of nicotine and the improved con-
sistency on the task were still evident. The authors
speculated that the lack of methylphenidate effects
on clinical symptoms may be attributable to a small
sample size and low methylphenidate doses. Nicotine
also has been found to improve response inhibition,
as indicated in a placebo-controlled pilot study of the
effects of nicotine compared with stimulant medica-
tion on cognitive performance in eight adolescents
with ADHD (Potter & Newhouse, 2004). The
results indicated that nicotine affects cognitive–
behavioral inhibition in a manner comparable with
methylphenidate.
Individuals with ADHD may use cigarettes as a
stimulant drug similar to medications such as
methylphenidate or dextroamphetamine and their
long-acting variants Concerta and Adderall, the
medications most commonly prescribed to treat
ADHD (Conners et al., 1996; Levin et al., 1996).
To examine the effects of nicotine and stimulant
medication on ADHD symptoms and moods in the
daily lives of adult smokers with ADHD, Gehricke
and colleagues (2006) studied 10 adult abstinent
smokers with clinically diagnosed ADHD (5 women,
5 men). Subjects participated in a 262 crossover
design with nicotine and placebo patches in the
presence and absence of stimulant medication. All
participants completed four 2-day sequences, each
time under a different nicotine and stimulant
medication condition. ADHD symptoms, moods,
and behaviors were monitored with an electronic
diary that participants completed approximately
every 30 min during waking hours. In addition, heart
rate and blood pressure as indicators of physiological
arousal and cardiac side effects were recorded with
ambulatory monitors. It was hypothesized that
nicotine and stimulant medication would reduce
ADHD symptoms, improve moods, and increase
cardiovascular arousal.
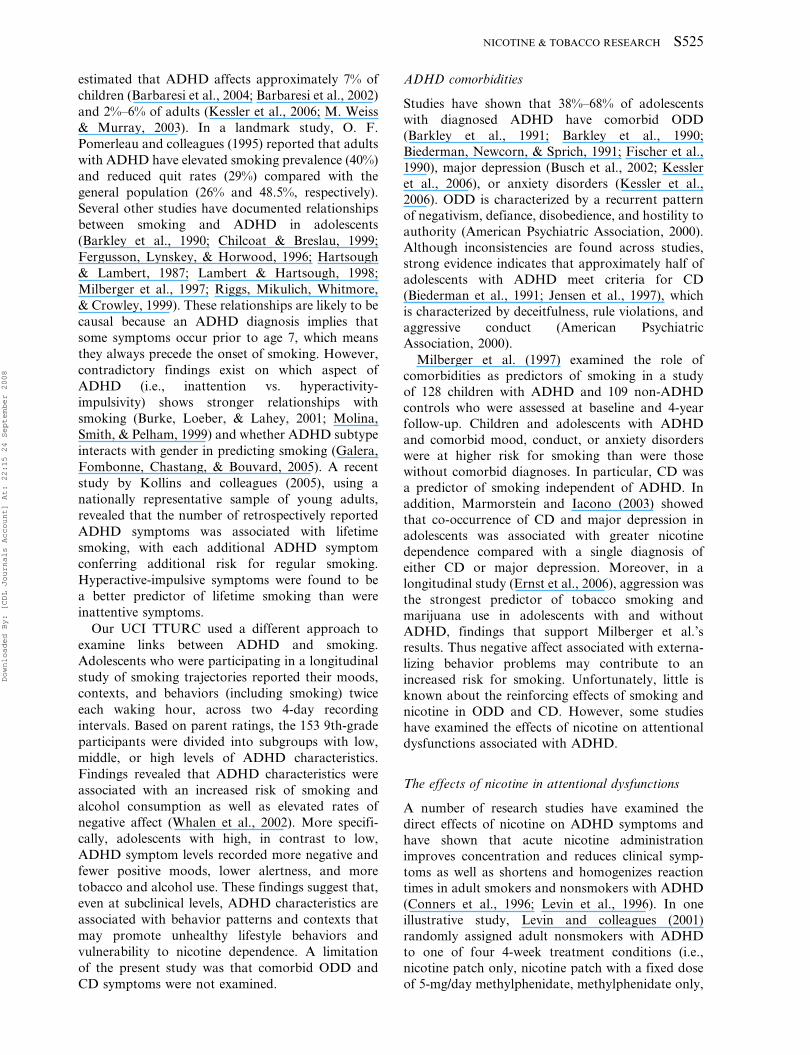
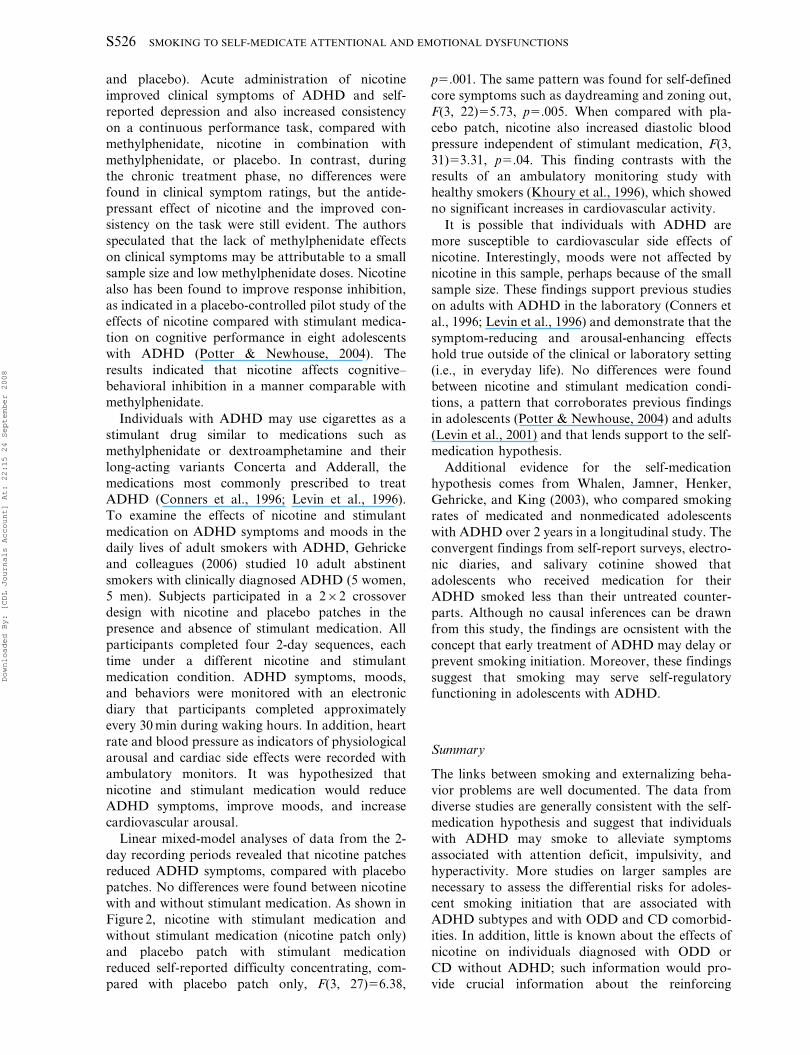
Linear mixed-model analyses of data from the 2-
day recording periods revealed that nicotine patches
reduced ADHD symptoms, compared with placebo
patches. No differences were found between nicotine
with and without stimulant medication. As shown in
Figure 2, nicotine with stimulant medication and
without stimulant medication (nicotine patch only)
and placebo patch with stimulant medication
reduced self-reported difficulty concentrating, com-
pared with placebo patch only, F(3, 27)56.38,
p5.001. The same pattern was found for self-defined
core symptoms such as daydreaming and zoning out,
F(3, 22)55.73, p5.005. When compared with pla-
cebo patch, nicotine also increased diastolic blood
pressure independent of stimulant medication, F(3,
31)53.31, p5.04. This finding contrasts with the
results of an ambulatory monitoring study with
healthy smokers (Khoury et al., 1996), which showed
no significant increases in cardiovascular activity.
It is possible that individuals with ADHD are
more susceptible to cardiovascular side effects of
nicotine. Interestingly, moods were not affected by
nicotine in this sample, perhaps because of the small
sample size. These findings support previous studies
on adults with ADHD in the laboratory (Conners et
al., 1996; Levin et al., 1996) and demonstrate that the
symptom-reducing and arousal-enhancing effects
hold true outside of the clinical or laboratory setting
(i.e., in everyday life). No differences were found
between nicotine and stimulant medication condi-
tions, a pattern that corroborates previous findings
in adolescents (Potter & Newhouse, 2004) and adults
(Levin et al., 2001) and that lends support to the self-
medication hypothesis.
Additional evidence for the self-medication
hypothesis comes from Whalen, Jamner, Henker,
Gehricke, and King (2003), who compared smoking
rates of medicated and nonmedicated adolescents
with ADHD over 2 years in a longitudinal study. The
convergent findings from self-report surveys, electro-
nic diaries, and salivary cotinine showed that
adolescents who received medication for their
ADHD smoked less than their untreated counter-
parts. Although no causal inferences can be drawn
from this study, the findings are ocnsistent with the
concept that early treatment of ADHD may delay or
prevent smoking initiation. Moreover, these findings
suggest that smoking may serve self-regulatory
functioning in adolescents with ADHD.
Summary
The links between smoking and externalizing beha-
vior problems are well documented. The data from
diverse studies are generally consistent with the self-
medication hypothesis and suggest that individuals
with ADHD may smoke to alleviate symptoms
associated with attention deficit, impulsivity, and
hyperactivity. More studies on larger samples are
necessary to assess the differential risks for adoles-
cent smoking initiation that are associated with
ADHD subtypes and with ODD and CD comorbid-
ities. In addition, little is known about the effects of
nicotine on individuals diagnosed with ODD or
CD without ADHD; such information would pro-
vide crucial information about the reinforcing
S526 SMOKING TO SELF-MEDICATE ATTENTIONAL AND EMOTIONAL DYSFUNCTIONS
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
mechanisms of nicotine in these populations. More
specifically, it still needs to be determined if
individuals diagnosed during childhood or adoles-
cence with ODD or CD smoke to reduce emotional
dysfunctions such as excessive feelings of anger,
resentment, and hostility.
Smoking and internalizing behavior problems
Major depression
Relationships between smoking and depression
became more prominent when the overall smoking
prevalence rates declined (Murphy et al., 2003).
Several studies have documented a relationship
between smoking and major depression in adults
(Breslau, Kilbey, & Andreski, 1991; de Leon et al.,
2002; Glassman et al., 1990; Kendler et al., 1993) and
adolescents (Brown, Lewinsohn, Seeley, & Wagner,
1996; Fergusson et al., 1996; Marmorstein & Iacono,
2003). Interestingly, a longitudinal study by Dierker
and colleagues (2001), found associations between
reports of tobacco use and mood and anxiety
disorders but not ADHD. Upadhyaya and collea-
gues (2003) found similar results: associations
between smoking and mood disorders and no
associations between smoking and ADHD.
Other longitudinal studies revealed reciprocal
associations between smoking and major depression
in that a history of smoking increased the risk for
major depression and vice versa (Breslau, Peterson,
Schultz, Chilcoat, & Andreski, 1998; Hanna &
Grant, 1999). However, a 21-year longitudinal study
of a birth cohort showed that major depression was
associated with increased rates of smoking and
nicotine dependence but that reciprocal influences
were inconsistent across time (Fergusson, Goodwin,
& Horwood, 2003). The findings of associations
between smoking and major depression suggest that
the neural substrates of smoking and antidepressant
medication may overlap (Quattrocki, Baird,
& Yurgelun-Todd, 2000). Furthermore, tricyclic
antidepressants (Rana et al., 1993; Schofield,
Witkop, Warnick, & Albuquerque, 1981), seroto-
nin-reuptake inhibitors (Fryer & Lukas, 1999a), and
atypical antidepressants such as bupropion (Fryer &
Lukas, 1999b) all have been shown to be noncompe-
titive antagonists of nicotinic receptors. Recent
preclinical findings suggest that nicotinic receptor
inactivation may be essential to the antidepressant
effects of some of these drugs (Caldarone et al.,
2004). Although nicotine does have antidepressant
effects, these may result from agonist-induced
receptor desensitization.
Figure 2. Difficulty concentrating in adult smokers with ADHD under nicotine and stimulant medication conditions.
NICOTINE & TOBACCO RESEARCH S527
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008

Some studies have shown that nicotine reduces
depression in smokers and nonsmokers with major
depression, a finding that supports the self-
medication hypothesis (Covey, Glassman, & Stetner,
1990, 1997; Cox et al., 2003; Glassman, Covey,
Stetner, & Rivelli, 2001; Haro & Drucker-Colin,
2004b; McClernon, Hiott, Westman, Rose, & Levin,
2006). Thus antidepressant therapy in combination
with nicotine replacement therapy may be a tailored
smoking cessation strategy for smokers with major
depression.
Anxiety disorders
As with the relationship between smoking and
depression, nicotine can have both anxiolytic and
anxiogenic effects (Picciotto, Brunzell, & Caldarone,
2002), depending perhaps on the type and time
course of anxiety disorder and whether nicotine is
administered acutely or chronically. Smoking initia-
tion and prevalence rates are increased in individuals
with post-traumatic stress disorder (PTSD; Acierno
et al., 2000; Beckham, 1999; Beckham et al., 1997;
Breslau et al., 2003), which indicates that nicotine
may act as an anxiolytic in response to developing
PTSD. Supporting evidence for this notion comes
from a study on smoking topography in trauma
survivors with and without PTSD (McClernon et al.,
2005). Most notably, puff volumes were higher in the
PTSD group than in the non-PTSD group.
Similar relationships between smoking and social
phobia have been found in adolescents and young
adults (Sonntag et al., 2000). In contrast, a long-
itudinal study on smoking and psychiatric disorders
found that heavy smoking in adolescence increased
the risk for agoraphobia, generalized anxiety dis-
order, and panic disorder during early adulthood
(Johnson et al., 2000). Thus the anxiogenic effects of
smoking may be caused by chronic exposure to
nicotine. Indirect support for this notion comes from
research using animal models to show that nicotine
exposure in adolescent rats leads to increased
anxiety-like behavior in adulthood (Slawecki,
Gilder, Roth, & Ehlers, 2003). The study’s authors
also proposed that increased anxiety associated with
smoking abstinence may play a role in continued
adolescent tobacco use.
In a review of the animal literature on the effects of
nicotine and nicotinic receptors on anxiety and
depression, Picciotto and colleagues (2002) suggested
that the paradoxical effects of nicotine on anxiety
and depression may be related to the broad expres-
sion of nicotinic acetylcholine receptors (nAChRs)
across many brain areas, the large number of nAChR
subtypes, and the ability of nicotine to activate and
desensitize nAChRs simultaneously. However, direct
support for the self-medication hypothesis for
anxiety was provided by Salin-Pascual and
Basanez-Villa (2003), who showed that transdermal
nicotine administration reduced anxiety in nonsmo-
kers with obsessive–compulsive disorder (OCD).
Although little is known about the relationship
between smoking and OCD, the results indicate that
smoking may serve as a self-medication for those
with elevated levels of anxiety.
Internalizing and externalizing behavior comorbidities
The underlying mechanisms for smoking to self-
medicate externalizing and internalizing behaviors
may involve nicotine-induced regulation of emo-
tional dysfunctions. Studies have shown an associa-
tion between smoking and negative affect such as
depressive or anxious mood (Goodman & Capitman,
2000; Hawkins, Hawkins, & Seeley, 1992; Kandel &
Davies, 1986; Upadhyaya, Deas, Brady, & Kruesi,
2002; Wu & Anthony, 1999). In addition, negative
affect frequently co-occurs with ADHD (Costello,
Mustillo, Erkanli, Keeler, & Angold, 2003; Palacio
et al., 2004; Pliszka, McCracken, & Maas, 1996;
Whalen et al., 2002; Wilens & Dodson, 2004), so that
some individuals with attentional dysfunctions may
smoke to regulate emotion.
Additional evidence of an association between
depressive, anxious, and aggressive dispositions and
smoking in adolescents comes from studies within the
UCI TTURC that used experience sampling methods
to assess smoking in the daily lives of adolescents
with emotional dysfunctions. Whalen and colleagues
(2001) used surveys and electronic diaries to assess
how depressive and aggressive dispositions relate to
smoking and daily moods in 170 adolescents.
Overall, cigarette and alcohol intake were elevated
in adolescents with depressive or aggressive disposi-
tions. Depression in boys, however, appeared to
reduce the risk for smoking associated with externa-
lizing behaviors. Moreover, depression combined
with aggression was associated with diary reports
of anxiety, stress, and fatigue in girls but not in boys.
Similarly, anxiety in adolescents increased the risk of
both smoking urges and tobacco use (Henker,
Whalen, Jamner, & Delfino, 2002). Recent findings
from the longitudinal studies conducted by Jamner
and colleagues on over 330 high school students
confirmed that trait hostility (Cook & Medley, 1954)
is a significant vector of vulnerability for tobacco
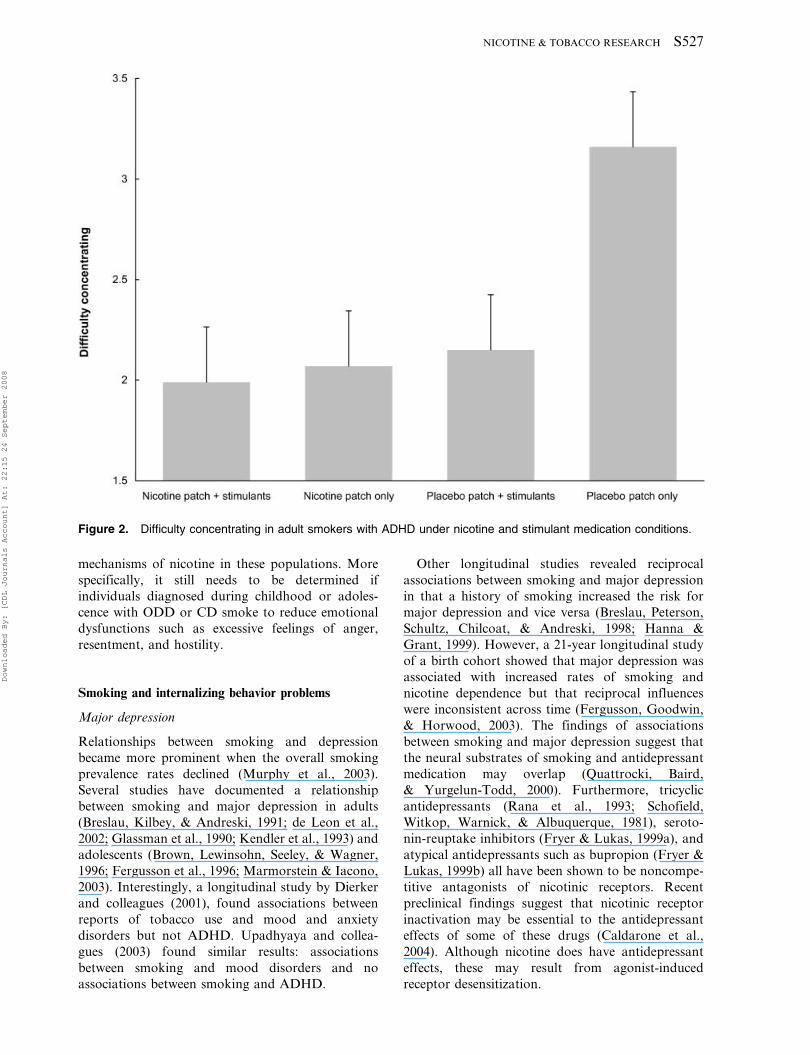
uptake in adolescents (Figure 3). Changes in salivary
cotinine levels (4-day mean) between the start of 9th
grade and the end of 11th grade were prospectively
examined in high (n5155) compared with low
(n5172) trait hostile adolescents. Although the two
groups had similar cotinine levels upon enrollment
into the study, the cotinine levels of high-hostile
youth increased significantly over time: 9th gra-
S528 SMOKING TO SELF-MEDICATE ATTENTIONAL AND EMOTIONAL DYSFUNCTIONS
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
de53.8¡3.5 ng/ml versus 11th grade521.5¡
8.6 ng/ml. In contrast, cotinine levels among low-
hostile adolescents did not change across this 3-year
period: 9th grade57.4¡3.5 ng/l versus 11th grade5
8.3¡8.5ng/ml; hostility6grade interaction, F(1,
320)510.65; p5.009.
Such associations between smoking and mood
suggest that the addictive properties of nicotine may
stem in part from its potential to enhance mood in
individuals with dysfunctions in emotional regulation
(Jamner, Shapiro, & Jarvik, 1999; Whalen et al.,
2001). Consistent with this notion, it has been
proposed that tobacco may be acting as an anti-
depressant through monoamino oxidase inhibition,
which in turn reduces catabolism of catecholamines
(i.e., serotonin, norepinephrine, and dopamine; see
animal studies discussed later). Such mood-enhan-
cing properties of tobacco may make smoking
particularly rewarding for adolescents with primarily
emotional dysfunctions. Self-medication to reduce
negative affect may be a critical factor that leads to
the initiation of cigarette smoking in adolescents and
maintenance of smoking during adulthood.
Effects of nicotine on emotional dysfunction
Studies that support the self-medication hypothesis
have shown that nicotine reduces depression in
depressive smokers and nonsmokers (Covey et al.,
1990, 1997; Glassman et al., 2001; Haro & Drucker-
Colin, 2004b), anger in high-hostile smokers and
nonsmokers (Jamner et al., 1999), and anxiety in
obsessive–compulsive nonsmokers (Salin-Pascual &
Basanez-Villa, 2003). Further insights into the
underlying brain circuitry of nicotine administration
in emotional dysfunctions come from a brain
imaging study conducted at the UCI TTURC
(Fallon, Keator, Mbogori, & Potkin, 2004). Fluoro
deoxy-glucose positron emission topography (FDG-
PET) was used to measure brain glucose metabolism
in response to nicotine and placebo patches during a
sustained attention task (continuous performance
task [CPT]), which assessed attentional performance
(Conners et al., 1996; Levin et al., 2001; Levin et al.,
1996; Walker, Shores, Trollor, Lee, & Sachdev, 2000),
and a modified anger provocation task (Bushman,
1995). A total of 86 participants were divided into
high- and low-hostility subgroups based on their scores
on the Cook–Medley Hostility Scale (Cook & Medley,
1954). Findings indicated that nicotine reduced global
brain metabolism in high-hostile smokers during anger
provocation, whereas high-hostile nonsmokers showed
the reverse effect. In contrast, nicotine had no
significant effects on brain metabolism in low-hostile
smokers or nonsmokers. These metabolic changes
were not observed when subjects performed the CPT.
These findings suggest that nicotine may have the
strongest effects on brain metabolism in individuals
with dysfunctions in affect regulation (i.e., hostile and
aggressive individuals). However, the central nervous
system effects of nicotine also were shown to differ
between men and women.
Sex differences have been established in smoking
topography, response rates to nicotine replacement
therapies, and sensitivity to nicotine and smoking
cues (Centers for Disease Control and Prevention,
2003; Delfino, Jamner, & Whalen, 2001; National
Institute on Drug Abuse, 2000). The UCI TTURC
(Fallon, Keator, Mbogori, Taylor, & Potkin, 2005)
examined gender differences in brain metabolism in
response to different levels of transdermal nicotine
compared with placebo in 42 women and 77 men
during a CPT and an anger provocation task. More
specifically, 54 nonsmokers received a placebo and a
3.5-mg nicotine patch; 55 smokers received a
placebo, a 3.5-mg nicotine patch, and a 21-mg patch.
Findings suggested that brain metabolism, as mea-
sured by FDG-PET, in response to nicotine com-
pared with placebo, was a function of gender, type of
task, and smoking status. Gender differences were
most apparent under placebo: Compared with males,
female smokers during the CPT and female non-
smokers during anger provocation showed consis-
tently higher brain glucose metabolism in the
prefrontal system, mid and anterior temporal lobe,
language cortices, and related subcortical systems.
These brain regions are primarily responsible for
attention, short-term memory, executive function,
affect regulation, and language. Sex differences were
not observed in brain metabolism patterns in subjects
treated with a nicotine patch. Such findings suggest
that nicotine may decrease gender differences asso-
ciated with task-specific brain metabolism.
Summary
The relationships between smoking and internalizing
behavior problems appear to be dependent on the
Figure 3. Smoking trajectories in high- versus low-hostile adolescents.
NICOTINE & TOBACCO RESEARCH S529
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
type of emotional dysfunction (depressed, anxious)
and the stage of smoking trajectory (i.e., initiation vs.
dependence). The findings suggest that individuals
start smoking because of problems with emotional
regulation underlying depression, anxiety, and
aggression. However, evidence indicates that smok-
ing also increases the risk for major depression and
anxiety disorders, which seems to suggest that
nicotine, the major psychoactive ingredient in
tobacco smoke, may initially alleviate symptoms
and moods associated with depression and anxiety
but then increase the risk of negative affectivity as the
individual becomes addicted to nicotine. The
increased negative affectivity in dependent smokers
may result in part from nicotine withdrawal experi-
enced between cigarettes. Between-study differences
in the pattern of associations between smoking,
internalizing, and externalizing behaviors may be
related to methods of assessing smoking (e.g., the use
of retrospective self-report measures rather than
salivary cotinine levels).
Our human behavioral and brain imaging studies
used salivary and serum levels to determine nicotine
intake and showed that trait hostility is a significant
vector of vulnerability for tobacco uptake and
susceptibility. In addition, interactions emerged
between type of emotional dysfunction and gender
in the risk for smoking initiation and in brain
metabolic responses to nicotine, findings that require
replication. Finally, to increase understanding of the
complex and paradoxical effects of nicotine in
relation to internalizing problems, studies are needed
on the receptor-activating and -desensitizing effects
of nicotine.
Developmental factors that contribute to the
association between smoking and attentional and
emotional dysfunctions: Evidence from animal studies
Adolescence has been identified as a critical period
for the initiation of alcohol and tobacco use (Chen &
Kandel, 1995; Kandel & Logan, 1984) and is also a
time of active neural remodeling (Huttenlocher,
1990; Pechmann, Levine, Loughlin, & Leslie, 2005).
Among adolescents, those with emotional and
attentional dysfunctions are most likely to start
smoking (Stevens et al., 2005; J. W. Weiss et al.,
2005; Whalen et al., 2001; Whalen et al., 2002) and
also develop psychiatric disorders as they grow older
(Dryman & Eaton, 1991; Erlenmeyer-Kimling &
Cornblatt, 1992; Gosden, Kramp, Gabrielsen,
Andersen, & Sestoft, 2005; Hofstra, van der Ende,
& Verhulst, 2002; Pine, Cohen, Cohen, & Brook,
1999; Wilcox & Anthony, 2004). It has been unclear
whether smoking initiation during adolescence
reflects social influences or an increased biological
sensitivity to the addictive effects of tobacco.
Whereas this question cannot be addressed easily
in human studies, the use of rodents permits a direct
experimental examination of the effects of nicotine
and other tobacco constituents on behavior and the
developing brain. Leslie and colleagues at the UCI
TTURC have used this model to provide evidence
supporting the concept that adolescence is a time of
unique sensitivity to the biological effects of nicotine
(Belluzzi, Lee, Oliff, & Leslie, 2004; Belluzzi, Wang,
& Leslie, 2005; Cao et al., 2007; Leslie et al., 2004;
McQuown, Belluzzi, & Leslie, 2007). In particular,
nicotine has been shown to be more rewarding and
less aversive during early adolescence compared with
adulthood (Vastola, Douglas, Varlinskaya, & Spear,
2002; Adriani & Laviola, 2004; Belluzzi et al., 2004;
Belluzzi et al., 2005; Shram, Funk, Li, & Le, 2006).
This age difference in behavioral response to nicotine
may result, in part, from differential activation of
both central and peripheral stress pathways (Cao
et al., 2007). Two critical domains of the stress
response pathway, the paraventricular nuclei of the
hypothalamus and thalamus, are differentially acti-
vated by nicotine in adolescents and adults. Whereas
the hypothalamic paraventricular nucleus regulates
peripheral stress response (Herman & Cullinan,
1997), the thalamic paraventricular nucleus projects
to the medial prefrontal cortex (Bubster & Deutsch,
1998; Moga, Weis, & Moore, 1995) and regulates
attention and emotion (Cardinal, Parkinson, Hall, &
Everitt, 2002; Chirstakou, Ribbins, & Everitt, 2004).
Thus, nicotine has significant, age-dependent effects
on neural circuitry that is critical to the regulation of
attention and emotion.
We also have shown that early exposure to
environmental stressors may lead to alterations in
central stress responses which, in turn, may influence
subsequent tobacco use. Neonatal handling (i.e.,
mild early environment stress) of rats significantly
reduces stress-induced corticosterone levels and
anxiety in male adolescents, but not in females
(Park, Hoang, Belluzzi, & Leslie, 2003).
Furthermore, nicotine was shown to reduce anxiety
only in males that were not handled at birth and that
showed a high degree of fearfulness when placed in a
novel environment (Park, Belluzzi, Han, Cao, &
Leslie, 2007). Thus, these studies powerfully demon-
strate that the effects of nicotine on emotional
response are dependent on the baseline state of
anxiety and stress responsiveness, and that these may
be influenced by environmental conditions.
Other tobacco constituents
Although nicotine is the major psychoactive ingre-
dient of tobacco smoke, other tobacco constituents
such as acetaldehyde (Belluzzi et al., 2005; Park,
Belluzzi, Han, Cao, & Leslie, 2007) and monoamine
S530 SMOKING TO SELF-MEDICATE ATTENTIONAL AND EMOTIONAL DYSFUNCTIONS
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
oxidase inhibitors (MAOIs; Berlin, Said, Spreux-
Varoquaux, Launay et al., 1995; Berlin, Said,
Spreux-Varoquaux, Olivares et al., 1995; Fowler,
Volkow, Wang, Pappas, Logan, MacGregor et al.,
1996; Fowler, Volkow, Wang, Pappas, Logan, Shea
et al., 1996) also may play an important role in
facilitating and potentiating the rewarding actions of
nicotine. MAOIs have been used for the treatment of
ADHD (Akhonzadeh, Tavakolian, Davari-Ashtiani,
Arabgol, & Amini, 2003; Rubinstein, Malone,
Roberts, & Logan, 2006) and depression
(Amsterdam & Chopra, 2001; Robinson, 2002) and
act synergistically with nicotine to enhance its
reinforcing effects (Villegier, Lotfipour, McQuown,
Belluzzi, & Leslie, 2007; Villegier et al., 2006).
However, in contrast to acetaldehyde (Belluzzi et
al., 2005; Park et al., 2007), there are no age
differences in this synergistic interaction. Both
adolescent and adult rats treated with MAOIs
respond with increased and robust self-administra-
tion of nicotine. Taken together, these findings
indicate that the use of nicotine alone to study the
addictive and reinforcing effects of tobacco on
attention and affect regulation may be too restrictive.
Furthermore, other components of tobacco smoke,
such as MAOIs that are known to have antidepres-
sant effects, may contribute to the self-medicating
effects of smoking.
Summary
Animal studies support and complement findings
from studies of human adolescents and adults.
Findings have shown that adolescence represents
a critical period for an increased biological
sensitivity to the addictive effects of tobacco.
Nicotine, the major psychoactive ingredient in
tobacco, regulates neural circuits via specific
nicotinic receptors in the brain that are associated
with the regulation of attention and affect. Other
tobacco constituents, such as acetaldehyde and
MAOIs, facilitate the rewarding actions of nicotine
and may contribute to the self-medicating effects of
nicotine. Early exposure to environmental stressors
may influence central nervous system responses,
which may predispose individuals to subsequent
tobacco use and addiction. More research is needed
on how early environment, along with age, sex, and
tobacco constituents, may influence responses to
nicotine in individuals with attentional and emo-
tional dysfunctions.
Conclusion: Translation of findings for tailored
smoking prevention and cessation strategies
The UCI TTURC’s contribution to the understand-
ing of the relationship between smoking and
attentional and emotional dysfunctions is unique in
that it presents converging evidence from various
disciplines and integrates basic neuroscience, human
behavioral research, human brain imaging, and
public policy. Researchers in marketing, education,
and social ecology also participated in the process of
developing unifying theoretical constructs and the-
ories. Such theoretical constructs served as a basis to
explore the varying responses to tobacco across
developmental stages and to identify characteristics
that put people at risk for smoking. Within this
framework, we examined the linkage between smok-
ing, attention, and affect with an emphasis on
integrating human findings from behavioral studies
and those from brain imaging and animal studies.
The findings on dispositional risk factors (i.e.,
ADHD, hostility, depression, aggression), age, and
gender in the human behavioral and brain imaging
studies along with animal models suggest that
attentional and emotional dysfunctions elevate the
risk for smoking initiation and uptake in adolescents.
This increased risk for smoking initiation and
subsequent nicotine addiction in individuals with
attentional and emotional dysfunctions may be
mediated in part by genetic polymorphisms.
Genetic variations in the dopamine pathway asso-
ciated with nicotine abuse and addiction (e.g.,
Audrain-McGovern, Lerman, Wileyto, Rodriguez,
& Shields, 2004) also may coregulate the expression
of attentional dysfunction (e.g., Waldman et al.,
1998). In addition, interactions have been found
between smoking, emotional dysfunctions, and
serotonin transporter genes (Hu et al., 2000;
Lerman et al., 2000). Research has shown that the
serotonin transporter short allele is associated with
reduced prefrontal cortex activation during emo-
tional challenge, which may result in decreased
inhibitory regulation of the amygdala (Heinz et al.,
2005; Pezawas et al., 2005). People with such
genotypes and corticolimbic dysfunctions may ben-
efit the most from tailored smoking prevention and
cessation strategies that aim to improve attention
and affect regulation.
The notion that some people may use smoking as a
stimulant drug, whereas others may use smoking to
regulate their affect, has important implications for
smoking cessation strategies, suggesting the need to
tailor interventions to subgroups for whom smoking
serves different functions and may be maintained by
different reinforcing mechanisms. Tailored interven-
tions may need to be adjusted depending on where the
individual is on the smoking trajectory. Early affect
management interventions with adolescents who have
emotional dysfunctions may prevent smoking uptake.
However, adolescents with both emotional dysfunc-
tions and high rates of smoking (i.e., 10 cigarettes/day
or more) may need to learn strategies for overcoming
NICOTINE & TOBACCO RESEARCH S531
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008

nicotine withdrawal symptoms such as inability to
concentrate and elevated levels of negative affect. For
such individuals, affective regulation training plus
nicotine replacement may be the most potent smoking
cessation strategy. Similarly, adolescents with atten-
tional dysfunctions may need pharmacotherapy such
as stimulant medication to prevent or delay smoking
initiation and nicotine replacement therapy when
tobacco dependent.
Although the negative health consequences from
smoking are indisputable, the effects of nicotine and
other tobacco constituents may delay and alter the
onset and course of some diseases. In fact, the self-
medication hypothesis has found its strongest sup-
port in nicotine therapies that aim to treat cognitive
and affective impairments such as those character-
istic of Alzheimer’s disease (Newhouse, Potter,
Kelton, & Corwin, 2001; Sahakian, Jones, Levy,
Gray, & Warburton, 1989; White & Levin, 1999;
Wilson et al., 1995), Parkinson’s disease (Kelton,
Kahn, Conrath, & Newhouse, 2000), ADHD (Levin
et al., 2001; Potter & Newhouse, 2004), depression
(Haro & Drucker-Colin, 2004a, 2004b), and anxiety
(Salin-Pascual & Basanez-Villa, 2003). However,
findings documenting beneficial effects of nicotine
are not always replicated, and more research needs to
be done on well-defined patient groups with close
monitoring of clinical symptoms and characteriza-
tion of side effects and potential drug interactions.
The potential benefits of nicotine have to be weighed
against its addictive and health-threatening proper-
ties. An important consideration to emerge from the
UCI TTURC research is the interaction of nicotine
with other tobacco constituents such as acetaldehyde
and MAOIs (Belluzzi et al., 2005; Park et al., 2007;
Villegier et al., 2006). Animal studies show that the
effects of nicotine are modulated by other compo-
nents of tobacco smoke. Further research is needed
to characterize these interactions and their under-
lying mechanisms. Such studies may lead to the
development of novel therapeutic strategies for the
treatment of tobacco addiction.
Acknowledgments
This research was supported by the U.S. Public Health Services
(DA13332, DA018752, DA19138, DA21267, CA80301) and the
California Tobacco-Related Disease Research Program (14RT-0147
and 10RT-0255). The authors thank the members of the UCI TTURC
and the dedicated staff and students whose contributions made this
work possible.
References
Acierno, R., Kilpatrick, D. G., Resnick, H., Saunders, B., De
Arellano, M., & Best, C. (2000). Assault, PTSD, family substance
use, and depression as risk factors for cigarette use in youth:
findings from the National Survey of Adolescents. Journal of
Traumatic Stress, 13(3), 381–396.
Adriani, W., & Laviola, G. (2004). Windows of vulnerability to
psychopathology and therapeutic strategy in the adolescent rodent
model. Behavioural Pharmacology, 15(5–6), 341–352.
American Psychiatric Association. (2000). Diagnostic and statistical
manual of mental disorders. (4th ed., text revision). Washington, DC:
Author.
Amsterdam, J. D., & Chopra, M. (2001). Monoamine oxidase
inhibitors revisited. Psychiatry Annals, 31, 361–370.
Akhonsadeh, S., Tavakolian, R., Davari-Ashtiani, R., Arabgol, F., &
Amini, H. (2003). Selegeline in the treatment of attention deficit
hyperactivity disorder in children: A double-blind randomized trial.
Progress in Neuro-Psychopharmacology and Biological Psychiatry,
27, 841–845.
Audrain-McGovern, J., Lerman, C., Wileyto, E. P., Rodriguez, D., &
Shields, P. G. (2004). Interacting effects of genetic predisposition
and depression on adolescent smoking progression. American
Journal of Psychiatry, 161(7), 1224–1230.
Barbaresi, W. J., Katusic, S., Colligan, R., Weaver, A., Pankratz, V.,
Mrazek, D., & Jacobsen, S. (2004). How common is attention-
deficit/hyperactivity disorder? Towards resolution of the contro-
versy: Results from a population-based study. Acta Paediatrica,
Supplement, 93(445), 55–59.
Barbaresi, W. J., Katusic, S. K., Colligan, R. C., Pankratz, V. S.,
Weaver, A. L., Weber, K. J., Mrazek, D. A., & Jacobsen, S. J.
(2002). How common is attention-deficit/hyperactivity disorder?
Incidence in a population-based birth cohort in Rochester, Minn.
Archives of Pediatrics and Adolescent Medicine, 156(3), 217–224.
Barkley, R. A., Anastopoulos, A. D., Guevremont, D. C., &
Fletcher, K. E. (1991). Adolescents with ADHD: Patterns of
behavioral adjustment, academic functioning, and treatment utiliza-
tion. Journal of the American Academy of Child and Adolescent
Psychiatry, 30(5), 752–761.
Barkley, R. A., Fischer, M., Edelbrock, C. S., & Smallish, L. (1990).
The adolescent outcome of hyperactive children diagnosed by
research criteria: I. An 8-year prospective follow-up study. Journal
of the American Academy of Child and Adolescent Psychiatry, 29(4),
546–557.
Beckham, J. C. (1999). Smoking and anxiety in combat veterans with
chronic posttraumatic stress disorder: A review. The Journal of
Psychoactive Drugs, 31(2), 103–110.
Beckham, J. C., Kirby, A. C., Feldman, M. E., Hertzberg, M. A.,
Moore, S. D., Crawford, A. L., Davidson, J. R. T., & Fairbank, J.
A. (1997). Prevalence and correlates of heavy smoking in Vietnam
veterans with chronic posttraumatic stress disorder. Addictive
Behaviors, 22(5), 637–647.
Bekker, E. M., Bocker, K. B., Van Hunsel, F., van den Berg, C. M., &
Kenemans, J. L. (2005). Acute effects of nicotine on attention and
response inhibition. Pharmacology, Biochemistry, and Behavior,
82(3), 539–548.
Belluzzi, J. D., Lee, A. G., Oliff, H. S., & Leslie, F. M. (2004).
Age-dependent effects of nicotine on locomotor activity and
conditioned place preference in rats. Psychopharmacology, 174(3),
389–395.
Belluzzi, J. D., Wang, R., & Leslie, F. M. (2005). Acetaldehyde
enhances acquisition of nicotine self-administration in adolescent
rats. Neuropsychopharmacology, 30(4), 705–712.
Berlin, I., Said, S., Spreux-Varoquaux, O., Launay, J. M., Olivares, R.,
Millet, V., Lecrubier, Y., & Puech, A. J. (1995). A reversible
monoamine oxidase A inhibitor (moclobemide) facilitates smoking
cessation and abstinence in heavy, dependent smokers. Clinical
Pharmacology and Therapeutics, 58(4), 444–452.
Berlin, I., Said, S., Spreux-Varoquaux, O., Olivares, R., Launay, J. M.,
& Puech, A. J. (1995). Monoamine oxidase A and B activities in
heavy smokers. Biological Psychiatry, 38(11), 756–761.
Biederman, J., Faraone, S. V., Keenan, K., Benjamin, J., Krifcher, B.,
Moore, C., Sprich-Buckminster, S., Ugaglia, K., Jellinek, M. S., &
Steingard, R., et al. (1992). Further evidence for family-genetic risk
factors in attention deficit hyperactivity disorder. Patterns of
comorbidity in probands and relatives psychiatrically and pediatri-
cally referred samples. Archives of General Psychiatry, 49(9),
728–738.
Biederman, J., Faraone, S. V., Spencer, T., Wilens, T., Norman, D.,
Lapey, K. A., Mick, E., Lehman, B. K., & Doyle, A. (1993).
Patterns of psychiatric comorbidity, cognition, and psychosocial
functioning in adults with attention deficit hyperactivity disorder.
American Journal of Psychiatry, 150(12), 1792–1798.
S532 SMOKING TO SELF-MEDICATE ATTENTIONAL AND EMOTIONAL DYSFUNCTIONS
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
Biederman, J., Newcorn, J., & Sprich, S. (1991). Comorbidity of
attention deficit hyperactivity disorder with conduct, depressive,
anxiety, and other disorders. American Journal of Psychiatry, 148(5),
564–577.
Breslau, N. (1995). Psychiatric comorbidity of smoking and nicotine
dependence. Behavior Genetics, 25(2), 95–101.
Breslau, N., Davis, G. C., & Schultz, L. R. (2003). Posttraumatic stress
disorder and the incidence of nicotine, alcohol, and other drug
disorders in persons who have experienced trauma. Archives of
General Psychiatry, 60(3), 289–294.
Breslau, N., Kilbey, M., & Andreski, P. (1991). Nicotine dependence,
major depression, and anxiety in young adults. Archives of General
Psychiatry, 48(12), 1069–1074.
Breslau, N., Peterson, E. L., Schultz, L. R., Chilcoat, H. D., &
Andreski, P. (1998). Major depression and stages of smoking. A
longitudinal investigation. Archives of General Psychiatry, 55(2),
161–166.
Brown, R. A., Lewinsohn, P. M., Seeley, J. R., & Wagner, E. F. (1996).
Cigarette smoking, major depression, and other psychiatric dis-
orders among adolescents. Journal of the American Academy of
Child and Adolescent Psychiatry, 35(12), 1602–1610.
Bubser, M., & Deutsch, A. Y. (1998). Thalamic paraventricular
nucleus neurons collateralize to innervate the prefrontal cortex and
nucleus accumbens. Brain Research, 787, 304–310.
Burke, J. D., Loeber, R., & Lahey, B. B. (2001). Which aspects of
ADHD are associated with tobacco use in early adolescence? The
Journal of Child Psychology and Psychiatry and Allied Disciplines,
42(4), 493–502.
Busch, B., Biederman, J., Cohen, L. G., Sayer, J. M., Monuteaux, M.
C., Mick, E., Zallen, B., & Faraone, S. (2002). Correlates of ADHD
among children in pediatric and psychiatric clinics. Psychiatric
Services, 53(9), 1103–1111.
Bushman, B. J. (1995). Moderating role of trait aggressiveness in the
effects of violent media on aggression. Journal of Personality and
Social Psychology, 69(5), 950–960.
Caldarone, B. J., Harrist, A., Cleary, M. A., Beech, R. D., King, S. L.,
& Picciotto, M. R. (2004). High-affinity nicotinic acetylcholine
receptors are required for antidepressant effects of amitriptyline on
behavior and hippocampal cell proliferation. Biological Psychiatry,
56(9), 657–664.
Cao, J., Belluzzi, J. D., Loughlin, S. E., Keyler, D. E., Pentel, P. R., &
Leslie, F. M. (2007). Acetaldehyde, a major constituent of tobacco
smoke, enhances behavioral, endocrine, and neuronal responses to
nicotine in adolescent and adult rats. Neuropsychopharmacology, 32,
2025–2035.
Centers for Disease Control and Prevention. (2003). Cigarette smoking
among adults—United States, 2001. Morbidity and Mortality
Weekly Report, 52, 953–956. [Erratum: 52, 1025–1025.]
Cardinal, R. N., Parkinson, J. A., Hall, J., & Everitt, B. J. (2002).
Emotion and motivation: the role of the amygdala, ventral striatum,
and prefrontal cortex. Neuroscience and Biobehavioral Reviews, 26,
321–352.
Chen, K., & Kandel, D. B. (1995). The natural history of drug use from
adolescence to the mid-thirties in a general population sample.
American Journal of Public Health, 85(1), 41–47.
Chilcoat, H. D., & Breslau, N. (1999). Pathways from ADHD to early
drug use. Journal of the American Academy of Child and Adolescent
Psychiatry, 38(11), 1347–1354.
Christakou, A., Robbins, T. W., & Everitt, B. J. (2004). Prefrontal
cortical-ventral striatal interactions involved in affective modulation
of attentional performance: implications for corticostriatal circuit
function. Journal of Neuroscience, 24, 773–780.
Conners, C. K., Levin, E. D., Sparrow, E., Hinton, S. C., Erhardt, D.,
Meck, W. H., Rose, J. E., & March, J. (1996). Nicotine and
attention in adult attention deficit hyperactivity disorder (ADHD).
Psychopharmacology Bulletin, 32(1), 67–73.
Cook, W. W., & Medley, D. M. (1954). Proposed hostility and
pharisaic-virtue scales for the MMPI. Journal of Applied
Psychology, 38, 414–418.
Costello, E. J., Mustillo, S., Erkanli, A., Keeler, G., & Angold, A.
(2003). Prevalence and development of psychiatric disorders in
childhood and adolescence. Archives of General Psychiatry, 60(8),
837–844.
Covey, L. S., Glassman, A. H., & Stetner, F. (1990). Depression and
depressive symptoms in smoking cessation. Comprehensive
Psychiatry, 31(4), 350–354.
Covey, L. S., Glassman, A. H., & Stetner, F. (1997). Major depression
following smoking cessation. American Journal of Psychiatry,
154(2), 263–265.
Cox, L. S., Patten, C. A., Krahn, L. E., Hurt, R. D., Croghan, I. T.,
Wolter, T. D., Schroeder, D. R., Tri, D., & Offord, K. P. (2003).
The effect of nicotine patch therapy on depression in nonsmokers: A
preliminary study. Journal of Addictive Diseases, 22(4), 75–85.
de Leon, J., Diaz, F. J., Rogers, T., Browne, D., & Dinsmore, L.
(2002). Initiation of daily smoking and nicotine dependence in
schizophrenia and mood disorders. Schizophrenia Research, 56(1–2),
47–54.
Delfino, R. J., Jamner, L. D., & Whalen, C. K. (2001). Temporal
analysis of the relationship of smoking behavior and urges to mood
states in men versus women. Nicotine & Tobacco Research, 3(3),
235–248.
Dierker, L. C., Avenevoli, S., Merikangas, K. R., Flaherty, B. P., &
Stolar, M. (2001). Association between psychiatric disorders and the
progression of tobacco use behaviors. Journal of the American
Academy of Child and Adolescent Psychiatry, 40(10), 1159–1167.
Dryman, A., & Eaton, W. W. (1991). Affective symptoms associated
with the onset of major depression in the community: Findings from
the US National Institute of Mental Health Epidemiologic
Catchment Area Program. Acta Psychiatrica Scandinavica, 84(1),
1–5.
Erlenmeyer-Kimling, L., & Cornblatt, B. A. (1992). A summary of
attentional findings in the New York High-Risk Project. Journal of
Psychiatric Research, 26(4), 405–426.
Ernst, M., Luckenbaugh, D. A., Moolchan, E. T., Leff, M. K.,
Allen, R., Eshel, N., Edythe, D. L., & Kimes, A. (2006). Behavioral
predictors of substance-use initiation in adolescents with and
without attention-deficit/hyperactivity disorder. Pediatrics, 117(6),
2030–2039.
Fallon, J. H., Keator, D. B., Mbogori, J., & Potkin, S. G. (2004).
Hostility differentiates the brain metabolic effects of nicotine. Brain
Research. Cognitive Brain Research, 18(2), 142–148.
Fallon, J. H., Keator, D. B., Mbogori, J., Taylor, D., & Potkin, S. G.
(2005). Gender: A major determinant of brain response to
nicotine. International Journal of Neuropsychopharmacology, 8(1),
17–26.
Fergusson, D. M., Goodwin, R. D., & Horwood, L. J. (2003). Major
depression and cigarette smoking: Results of a 21-year longitudinal
study. Psychological Medicine, 33(8), 1357–1367.
Fergusson, D. M., Lynskey, M. T., & Horwood, L. J. (1996).
Comorbidity between depressive disorders and nicotine dependence
in a cohort of 16-year-olds. Archives of General Psychiatry, 53(11),
1043–1047.
Fischer, M., Barkley, R. A., Edelbrock, C. S., & Smallish, L. (1990).
The adolescent outcome of hyperactive children diagnosed by
research criteria: II. Academic, attentional, and neuropsychological
status. Journal of Consulting and Clinical Psychology, 58(5),
580–588.
Fowler, J. S., Volkow, N. D., Wang, G. J., Pappas, N., Logan, J.,
MacGregor, R., Alexoff, D., Shea, C., Schlyer, D., Wolf, D.,
Zezulkova, I., & Cilento, R. (1996). Inhibition of monoamine
oxidase B in the brains of smokers. Nature, 379(6567), 733–736.
Fowler, J. S., Volkow, N. D., Wang, G. J., Pappas, N., Logan, J.,
Shea, C., Alexoff, D., MacGregor, R., Schlyer, D., Zezulkova, I., &
Wolf, A. (1996). Brain monoamine oxidase A inhibition in cigarette
smokers. Proceedings of the National Academy of Sciences of the
United States of America, 93(24), 14065–14069.
Fryer, J. D., & Lukas, R. J. (1999a). Antidepressants noncompetitively
inhibit nicotinic acetylcholine receptor function. Journal of
Neurochemistry, 72(3), 1117–1124.
Fryer, J. D., & Lukas, R. J. (1999b). Noncompetitive functional
inhibition at diverse, human nicotinic acetylcholine receptor
subtypes by bupropion, phencyclidine, and ibogaine. Journal of
Pharmacology and Experimental Therapeutics, 288(1), 88–92.
Galera, C., Fombonne, E., Chastang, J. F., & Bouvard, M. (2005).
Childhood hyperactivity-inattention symptoms and smoking in
adolescence. Drug and Alcohol Dependence, 78(1), 101–108.
Gehricke, J.-G., Whalen, C. K., Jamner, L. D., Wigal, T. L., &
Steinhoff, K. (2006). The reinforcing effects of nicotine and
stimulant medication in the everyday lives of adult smokers with
ADHD: A preliminary examination. Nicotine & Tobacco Research,
8(1), 37–47.
NICOTINE & TOBACCO RESEARCH S533
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008

Glassman, A. H., Covey, L. S., Stetner, F., & Rivelli, S. (2001).
Smoking cessation and the course of major depression: A follow-up
study. Lancet, 357(9272), 1929–1932.
Glassman, A. H., Helzer, J. E., Covey, L. S., Cottler, L. B., Stetner, F.,
Tipp, J. E., & Johnson, J. (1990). Smoking, smoking cessation, and
major depression. The Journal of the American Medical Association,
264(12), 1546–1549.
Glassman, A. H., Stetner, F., Walsh, B. T., Raizman, P. S., Fleiss, J.
L., Cooper, T. B., & Covey, L. S. (1988). Heavy smokers, smoking
cessation, and clonidine. Results of a double-blind, randomized
trial. The Journal of the American Medical Association, 259(19),
2863–2866.
Goodman, E., & Capitman, J. (2000). Depressive symptoms and
cigarette smoking among teens. Pediatrics, 106(4), 748–755.
Gosden, N. P., Kramp, P., Gabrielsen, G., Andersen, T. F., &
Sestoft, D. (2005). Violence of young criminals predicts schizo-
phrenia: A 9-year register-based follow up of 15- to 19-year-old
criminals. Schizophrenia Bulletin, 31(3), 759–768.
Hanna, E. Z., & Grant, B. F. (1999). Parallels to early onset alcohol
use in the relationship of early onset smoking with drug use and
DSM-IV drug and depressive disorders: Findings from the National
Longitudinal Epidemiologic Survey. Alcoholism: Clinical and
Experimental Research, 23(3), 513–522.
Haro, R., & Drucker-Colin, R. (2004a). Effects of long-term
administration of nicotine and fluoxetine on sleep in depressed
patients. Archives of Medical Research, 35(6), 499–506.
Haro, R., & Drucker-Colin, R. (2004b). A two-year study on the
effects of nicotine and its withdrawal on mood and sleep.
Pharmacopsychiatry, 37(5), 221–227.
Hartsough, C. S., & Lambert, N. M. (1987). Pattern and progression of
drug use among hyperactives and controls: A prospective short-term
longitudinal study. Journal of Child Psychology and Psychiatry,
28(4), 543–553.
Hawkins, W. E., Hawkins, M. J., & Seeley, J. (1992). Stress, health-
related behavior and quality of life on depressive symptomatology
in a sample of adolescents. Psychological Reports, 71(1), 183–186.
Heinz, A., Braus, D. F., Smolka, M. N., Wrase, J., Puls, I.,
Hermann, D., Klein, S., Grusser, S. M., Flor, H., Schumann, G.,
Mann, K., & Buchel, C. (2005). Amygdala-prefrontal coupling
depends on a genetic variation of the serotonin transporter. Nature
Neuroscience, 8(1), 20–21.
Henker, B., Whalen, C. K., Jamner, L. D., & Delfino, R. J. (2002).
Anxiety, affect, and activity in teenagers: Monitoring daily life with
electronic diaries. Journal of the American Academy of Child and
Adolescent Psychiatry, 41(6), 660–670.
Herman, J. P., & Cullinan, W. E. (1997). Neurocircuitry of stress:
central control of the hypothalamo-pituitary-adrenocortical axis.
Trends in Neuroscience, 20(2), 78–84.
Hofstra, M. B., van der Ende, J., & Verhulst, F. C. (2002). Child and
adolescent problems predict DSM-IV disorders in adulthood: A 14-
year follow-up of a Dutch epidemiological sample. Journal of the
American Academy of Child and Adolescent Psychiatry, 41(2),
182–189.
Hu, S., Brody, C. L., Fisher, C., Gunzerath, L., Nelson, M. L.,
Sabol, S. Z., Sirota, L. A., Marcus, S. F., Greenberg, B. D.,
Murphy, D. L., & Hamer, D. H. (2000). Interaction between the
serotonin transporter gene and neuroticism in cigarette smoking
behavior. Molecular Psychiatry, 5(2), 181–188.
Huttenlocher, P. R. (1990). Morphometric study of human cerebral
cortex development. Neuropsychologia, 28(6), 517–527.
Jamner, L. D., Shapiro, D., & Jarvik, M. E. (1999). Nicotine reduces
the frequency of anger reports in smokers and nonsmokers with
high but not low hostility: An ambulatory study. Experimental and
Clinical Psychopharmacology, 7(4), 454–463.
Jamner, L. D., Whalen, C. K., Loughlin, S., Mermelstein, R., Audrain-
McGovern, J., Krishnan-Sarin, S., Worden, J., & Leslie, F. (2003).
Tobacco use across the formative years: A road map to develop-
mental vulnerabilities. Nicotine & Tobacco Research, 5(Suppl. 1),
S71–S87.
Jensen, P. S., Hinshaw, S. P., Kraemer, H. C., Lenora, N., Newcorn, J.
H., Abikoff, H. B., March, J. S., Arnold, L. E., Cantwell, D. P.,
Conners, C. K., Elliott, G. R., Greenhill, L. L., Hechtman, L.,
Hoza, B., Pelham, W. E., Severe, J. B., Swanson, J. M., Wells, K.
C., Wigal, T., & Vitiello, B. (2001). ADHD comorbidity findings
from the MTA study: comparing comorbid groups. Journal of the
American Academy of Child and Adolescent Psychiatry, 40(2),
147–158.
Jensen, P. S., Martin, D., & Cantwell, D. P. (1997). Comorbidity in
ADHD: Implications for research, practice, and DSM-V. Journal of
the American Academy of Child and Adolescent Psychiatry, 36(8),
1065–1079.
Johnson, J. G., Cohen, P., Pine, D. S., Klein, D. F., Kasen, S., &
Brook, J. S. (2000). Association between cigarette smoking and
anxiety disorders during adolescence and early adulthood. The
Journal of the American Medical Association, 284(18), 2348–2351.
Johnston, L., O’Malley, P., & Bachman, J. (1998). National survey
results on drug use from Monitoring the Future Study, 1975–1997.
Washington, DC: National Institute on Drug Abuse.
Kandel, D. B., & Davies, M. (1986). Adult sequelae of adolescent
depressive symptoms. Archives of General Psychiatry, 43(3),
255–262.
Kandel, D. B., & Logan, J. A. (1984). Patterns of drug use from
adolescence to young adulthood: I. Periods of risk for initiation,
continued use, and discontinuation. American Journal of Public
Health, 74(7), 660–666.
Kelton, M. C., Kahn, H. J., Conrath, C. L., & Newhouse, P. A. (2000).
The effects of nicotine on Parkinson’s disease. Brain and Cognition,
43(1–3), 274–282.
Kendall, P. C., Brady, E. U., & Verduin, T. L. (2001). Comorbidity in
childhood anxiety disorders and treatment outcome. Journal of the
American Academy of Child and Adolescent Psychiatry, 40(7),
787–794.
Kendler, K. S., Neale, M. C., MacLean, C. J., Heath, A. C., Eaves, L.
J., & Kessler, R. C. (1993). Smoking and major depression. A causal
analysis. Archives of General Psychiatry, 50(1), 36–43.
Kessler, R. C., Adler, L., Barkley, R., Biederman, J., Conners, C. K.,
Demler, O., Faraone, S. V., Greenhill, L. L., Howes, M. J.,
Secnik, K., Spencer, T., Ustun, B., Walter, E., & Zaslavsky, A.
(2006). The prevalence and correlates of adult ADHD in the United
States: Results from the National Comorbidity Survey Replication.
American Journal of Psychiatry, 163(4), 716–723.
Khantzian, E. J. (1997). The self-medication hypothesis of substance
use disorders: A reconsideration and recent applications. Harvard
Review of Psychiatry, 4(5), 231–244.
Khoury, Z., Comans, P., Keren, A., Lerer, T., Gavish, A., &
Tzivoni, D. (1996). Effects of transdermal nicotine patches on
ambulatory ECG monitoring findings: A double-blind study in
healthy smokers. Cardiovascular Drugs and Therapy, 10(2), 179–184.
Kollins, S. H., McClernon, F. J., & Fuemmeler, B. F. (2005).
Association between smoking and attention-deficit/hyperactivity
disorder symptoms in a population-based sample of young adults.
Archives of General Psychiatry, 62(10), 1142–1147.
Lambert, N. M., & Hartsough, C. S. (1998). Prospective study of
tobacco smoking and substance dependencies among samples of
ADHD and non-ADHD participants. Journal of Learning
Disabilities, 31(6), 533–544.
Lerman, C., Caporaso, N. E., Audrain, J., Main, D., Boyd, N. R., &
Shields, P. G. (2000). Interacting effects of the serotonin transporter
gene and neuroticism in smoking practices and nicotine dependence.
Molecular Psychiatry, 5(2), 189–192.
Leslie, F. M., Loughlin, S. E., Wang, R., Perez, L., Lotfipour, S., &
Belluzzi, J. D. (2004). Adolescent development of forebrain
stimulant responsiveness: Insights from animal studies. Annals of
the New York Academy of Sciences, 1021, 148–159.
Levin, E. D., Conners, C. K., Silva, D., Canu, W., & March, J. (2001).
Effects of chronic nicotine and methylphenidate in adults with
attention deficit/hyperactivity disorder. Experimental and Clinical
Psychopharmacology, 9(1), 83–90.
Levin, E. D., Conners, C. K., Sparrow, E., Hinton, S. C., Erhardt, D.,
Meck, W. H., Rose, J., & March, J. (1996). Nicotine effects on adults
with attention-deficit/hyperactivity disorder. Psychopharmacology,
123(1), 55–63.
Marmorstein, N. R., & Iacono, W. G. (2003). Major depression and
conduct disorder in a twin sample: gender, functioning, and risk for
future psychopathology. Journal of the American Academy of Child
and Adolescent Psychiatry, 42(2), 225–233.
McClernon, F. J., Beckham, J. C., Mozley, S. L., Feldman, M. E.,
Vrana, S. R., & Rose, J. E. (2005). The effects of trauma recall on
smoking topography in posttraumatic stress disorder and non-
posttraumatic stress disorder trauma survivors. Addictive Behaviors,
30(2), 247–257.
McClernon, F. J., Hiott, F. B., Westman, E. C., Rose, J. E., & Levin, E.
D. (2006). Transdermal nicotine attenuates depression symptoms
S534 SMOKING TO SELF-MEDICATE ATTENTIONAL AND EMOTIONAL DYSFUNCTIONS
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008
in nonsmokers: A double-blind, placebo-controlled trial.
Psychopharmacology, 189(1), 125–133.
McGough, J. J., Smalley, S. L., McCracken, J. T., Yang, M.,
Del’Homme, M., Lynn, D. E., & Loo, S. (2005). Psychiatric
comorbidity in adult attention deficit hyperactivity disorder:
findings from multiplex families. American Journal of Psychiatry,
162(9), 1621–1627.
McQuown, S. C., Belluzzi, J. D., & Leslie, F. M. (2007). Low dose
nicotine treatment during early adolescence increases subsequent
cocaine reward. Neurotoxicology and Teratology, 29(1), 66–73.
Milberger, S., Biederman, J., Faraone, S. V., Chen, L., & Jones, J.
(1997). ADHD is associated with early initiation of cigarette
smoking in children and adolescents. Journal of the American
Academy of Child and Adolescent Psychiatry, 36(1), 37–44.
Moga, M. M., Weis, R. P., & Moore, R. Y. (1995). Efferent projections
of the paraventricular thalamic nucleus in the rat. Journal of
Comparative Neurology, 359, 221–238.
Molina, B. S. G., Smith, B. H., & Pelham, W. E. (1999). Interactive
effects of attention deficit hyperactivity disorder and conduct
disorder on early adolescent substance use. Psychology of
Addictive Behaviors, 13(4), 348–358.
Murphy, J. M., Horton, N. J., Monson, R. R., Laird, N. M., Sobol, A.
M., & Leighton, A. H. (2003). Cigarette smoking in relation to
depression: Historical trends from the Stirling County Study.
American Journal of Psychiatry, 160(9), 1663–1669.
Newhouse, P. A., Potter, A., Kelton, M., & Corwin, J. (2001).
Nicotinic treatment of Alzheimer’s disease. Biological Psychiatry,
49(3), 268–278.
National Institute on Drug Abuse. (2000). Update on nicotine
addiction and tobacco research. NIDA Notes, 15(5).
Palacio, J. D., Castellanos, F. X., Pineda, D. A., Lopera, F., Arcos-
Burgos, M., Quiroz, Y. T., Henao, G., Puerta, C. I., Ramirez, D. L.,
Rapoport, J. L., Bailey-Wilson, J., Berg, K., & Mueneke, M. (2004).
Attention-deficit/hyperactivity disorder and comorbidities in 18
Paisa Colombian multigenerational families. Journal of the
American Academy of Child and Adolescent Psychiatry, 43(12),
1506–1515.
Park, M. K., Belluzzi, J. D., Han, S. H., Cao, J., & Leslie, F. M. (2007).
Age, sex and early environment contribute to individual differences
in nicotine/acetaldehyde-induced behavioral and endocrine
responses in rats. Pharmacology, Biochemistry, and Behavior,
86(2), 297–305.
Park, M. K., Hoang, T. A., Belluzzi, J. D., & Leslie, F. M. (2003).
Gender specific effect of neonatal handling on stress reactivity of
adolescent rats. Journal of Neuroendocrinology, 15(3), 289–295.
Pechmann, C., Levine, L., Loughlin, S., & Leslie, F. (2005). Impulsive
and self-conscious: Adolescents’ vulnerability to advertising and
promotion. Journal of Public Policy and Marketing, 24(2), 203–221.
Pezawas, L., Meyer-Lindenberg, A., Drabant, E. M., Verchinski, B.
A., Munoz, K. E., Kolachana, B. S., Egan, M. F., Mattay, V. S.,
Hairiri, A. R., & Weinberger, D. R. (2005). 5-HTTLPR poly-
morphism impacts human cingulate-amygdala interactions: A
genetic susceptibility mechanism for depression. Nature
Neuroscience, 8(6), 828–834.
Picciotto, M. R., Brunzell, D. H., & Caldarone, B. J. (2002). Effect of
nicotine and nicotinic receptors on anxiety and depression.
Neuroreport, 13(9), 1097–1106.
Pine, D. S., Cohen, E., Cohen, P., & Brook, J. (1999). Adolescent
depressive symptoms as predictors of adult depression: moodiness
or mood disorder? American Journal of Psychiatry, 156(1), 133–135.
Pliszka, S. R., McCracken, J. T., & Maas, J. W. (1996).
Catecholamines in attention-deficit hyperactivity disorder: Current
perspectives. Journal of the American Academy of Child and
Adolescent Psychiatry, 35(3), 264–272.
Pomerleau, C. S., Marks, J. L., & Pomerleau, O. F. (2000). Who gets
what symptom? Effects of psychiatric cofactors and nicotine
dependence on patterns of smoking withdrawal symptomatology.
Nicotine & Tobacco Research, 2(3), 275–280.
Pomerleau, O. F., Downey, K. K., Stelson, F. W., & Pomerleau, C. S.
(1995). Cigarette smoking in adult patients diagnosed with attention
deficit hyperactivity disorder. Journal of Substance Abuse, 7(3),
373–378.
Potter, A. S., & Newhouse, P. A. (2004). Effects of acute nicotine
administration on behavioral inhibition in adolescents with atten-
tion-deficit/hyperactivity disorder. Psychopharmacology, 176(2),
182–194.
Quattrocki, E., Baird, A., & Yurgelun-Todd, D. (2000). Biological
aspects of the link between smoking and depression. Harvard
Review of Psychiatry, 8(3), 99–110.
Rana, B., McMorn, S. O., Reeve, H. L., Wyatt, C. N., Vaughan, P. F.,
& Peers, C. (1993). Inhibition of neuronal nicotinic acetylcholine
receptors by imipramine and desipramine. European Journal of
Pharmacology, 250(2), 247–251.
Riggs, P. D., Mikulich, S. K., Whitmore, E. A., & Crowley, T. J.
(1999). Relationship of ADHD, depression, and non-tobacco
substance use disorders to nicotine dependence in substance-
dependent delinquents. Drug and Alcohol Dependence, 54(3),
195–205.
Robinson, D. S. (2002). Monoamine oxidase inhibitors: a new
generation. Psychopharmacology Bulletin, 36, 124–138.
Rohde, P., Kahler, C. W., Lewinsohn, P. M., & Brown, R. A. (2004).
Psychiatric disorders, family factors, and cigarette smoking: III.
Associations with cessation by young adulthood among daily
smokers. Nicotine and Tobacco Research, 6(3), 509–522.
Rubinstein, S., Malone, M. A., Roberts, W., & Logan, W. J. (2006).
Placebo-controlled study examining effects of selegiline in children
with attention-deficit/hyperactivity disorder. Journal of Child and
Adolescent Psychopharmacology, 16, 404–415.
Sahakian, B., Jones, G., Levy, R., Gray, J., & Warburton, D. (1989).
The effects of nicotine on attention, information processing, and
short-term memory in patients with dementia of the Alzheimer type.
British Journal of Psychiatry, 154, 797–800.
Salin-Pascual, R. J., & Basanez-Villa, E. (2003). Changes in compul-
sion and anxiety symptoms with nicotine transdermal patches in
non-smoking obsessive–compulsive disorder patients. Revista de
Investigacion Clınica, 55(6), 650–654.
Schofield, G. G., Witkop, B., Warnick, J. E., & Albuquerque, E. X.
(1981). Differentiation of the open and closed states of the ionic
channels of nicotinic acetylcholine receptors by tricyclic antidepres-
sants. Proceedings of the National Academy of Sciences of the United
States of America, 78(8), 5240–5244.
Shram, M. J., Funk, D., Li, Z., & Le, A. D. (2006). Periadolescent and
adult rats respond differently in tests measuring the rewarding and
aversive effects of nicotine. Psychopharmacology (Berl), 186(2),
201–208.
Slawecki, C. J., Gilder, A., Roth, J., & Ehlers, C. L. (2003).
Increased anxiety-like behavior in adult rats exposed to nicotine
as adolescents. Pharmacology, Biochemistry, and Behavior, 75(2),
355–361.
Sonntag, H., Wittchen, H. U., Hofler, M., Kessler, R. C., & Stein, M.
B. (2000). Are social fears and DSM-IV social anxiety disorder
associated with smoking and nicotine dependence in adolescents and
young adults? European Psychiatry, 15(1), 67–74.
Stevens, S. L., Colwell, B., Smith, D. W., Robinson, J., & McMillan, C.
(2005). An exploration of self-reported negative affect by
adolescents as a reason for smoking: Implications for tobacco
prevention and intervention programs. Preventive Medicine, 41(2),
589–596.
Upadhyaya, H. P., Brady, K. T., Wharton, M., & Liao, J. (2003).
Psychiatric disorders and cigarette smoking among child and
adolescent psychiatry inpatients. The American Journal on
Addictions, 12(2), 144–152.
Upadhyaya, H. P., Deas, D., Brady, K. T., & Kruesi, M. (2002).
Cigarette smoking and psychiatric comorbidity in children and
adolescents. Journal of the American Academy of Child and
Adolescent Psychiatry, 41(11), 1294–1305.
Vastola, B. J., Douglas, L. A., Varlinskaya, E. I., & Spear, L. P. (2002).
Nicotine-induced conditioned place preference in adolescent and
adult rats. Physiology & Behavior, 77(1), 107–114.
Villegier, A. S., Lotfipour, S., McQuown, S. C., Belluzzi, J. D., &
Leslie, F. M. (2007). Tranylcypromine enhancement of nicotine self-
administration. Neuropharmacology, 52(6), 1415–1425.
Villegier, A. S., Salomon, L., Granon, S., Changeux, J. P., Belluzzi, J.
D., Leslie, F. M., & Tassin, J. (2006). Monoamine oxidase inhibitors
allow locomotor and rewarding responses to nicotine.
Neuropsychopharmacology, 31(8), 1704–1713.
Waldman, I. D., Rowe, D. C., Abramowitz, A., Kozel, S. T., Mohr, J.
H., Sherman, S. L., Cleveland, H. H., Sanders, M. L., Gard, J. M.,
& Stever, C. (1998). Association and linkage of the dopamine
transporter gene and attention-deficit hyperactivity disorder in
children: Heterogeneity owing to diagnostic subtype and severity.
American Journal of Human Genetics, 63(6), 1767–1776.
NICOTINE & TOBACCO RESEARCH S535
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008

Walker, A. J., Shores, E. A., Trollor, J. N., Lee, T., & Sachdev, P. S.
(2000). Neuropsychological functioning of adults with attention
deficit hyperactivity disorder. Journal of Clinical and Experimental
Neuropsychology, 22(1), 115–124.
Weiss, J. W., Mouttapa, M., Chou, C. P., Nezami, E., Anderson
Johnson, C., Palmer, P. H., Cen, S., Gallaher, P., Ritt-Olson, A.,
Azen, S., & Unger, J. B. (2005). Hostility, depressive symptoms,
and smoking in early adolescence. Journal of Adolescence, 28(1),
49–62.
Weiss, M., & Murray, C. (2003). Assessment and management of
attention-deficit hyperactivity disorder in adults. Canadian Medical
Association Journal, 168(6), 715–722.
Wender, P. H., Wolf, L. E., & Wasserstein, J. (2001).
Adults with ADHD: An overview. In: J. Wasserstein, L. Wolf, &
F. F. Lefever (Eds.), Adult attention deficit disorder: Brain
mechanisms and life outcomes. New York: New York Academy of
Sciences.
Whalen, C. K., Jamner, L. D., Henker, B., & Delfino, R. J. (2001).
Smoking and moods in adolescents with depressive and aggressive
dispositions: Evidence from surveys and electronic diaries. Health
Psychology, 20(2), 99–111.
Whalen, C. K., Jamner, L. D., Henker, B., Delfino, R. J., & Lozano, J.
(2002). The ADHD spectrum and everyday life: Experience
sampling of adolescent moods, activities, smoking, and drinking.
Child Development, 73, 209–227.
Whalen, C. K., Jamner, L. D., Henker, B., Gehricke, J.-G., & King, P.
S. (2003). Is there a link between adolescent cigarette smoking and
pharmacotherapy for ADHD? Psychology of Addictive Behaviors,
17(4), 332–335.
White, H. K., & Levin, E. D. (1999). Four-week nicotine skin patch
treatment effects on cognitive performance in Alzheimer’s disease.
Psychopharmacology, 143(2), 158–165.
Wilcox, H. C., & Anthony, J. C. (2004). Child and adolescent clinical
features as forerunners of adult-onset major depressive disorder:
Retrospective evidence from an epidemiological sample. Journal of
Affective Disorders, 82(1), 9–20.
Wilens, T. E., & Dodson, W. (2004). A clinical perspective of attention-
deficit/hyperactivity disorder into adulthood. Journal of Clinical
Psychiatry, 65(10), 1301–1313.
Wilson, A. L., Langley, L. K., Monley, J., Bauer, T., Rottunda, S.,
McFalls, E., Kovera, C., & McCarten, J. R. (1995). Nicotine patches
in Alzheimer’s disease: Pilot study on learning, memory, and safety.
Pharmacology, Biochemistry, and Behavior, 51(2–3), 509–514.
Wu, L. T., & Anthony, J. C. (1999). Tobacco smoking and depressed
mood in late childhood and early adolescence. American Journal of
Public Health, 89(12), 1837–1840.
S536 SMOKING TO SELF-MEDICATE ATTENTIONAL AND EMOTIONAL DYSFUNCTIONS
Downloaded By: [CDL Journals Account] At: 22:15 24 September 2008























![[The genetics of smoking]](https://img.dokumen.tips/doc/110x75/6335cc3402a8c1a4ec01ecad/the-genetics-of-smoking.jpg)





