Embed Size (px)
Citation preview

Grace E. Dean, PhD, RN
Eman Abu Sabbah, MS, RN
Siritorn Yingrengreung, PhD, RN
Patricia Ziegler, NP, RN
Hongbin Chen, MD, PhD
Lynn M. Steinbrenner, MD
Suzanne S. Dickerson, DNS, RN
Sleeping With the EnemySleep and Quality of Life in Patients With Lung Cancer
K E Y W O R D S
Actigraphy
NonYsmall cell lung cancer
Quality of life
Sleep
Background: Patients with lung cancer have the poorest sleep quality compared
with other patients with cancer and noncancer control subjects. However, few studies
have examined sleep longitudinally. Objective: The objective of this study was to
characterize and correlate sleep quality, daytime sleepiness, sleep-wake actigraphy,
and quality of life (QOL) before, during, and after chemotherapy for nonYsmall cell
lung cancer (NSCLC). Methods: Using a prospective repeated-measures 1-group
design, patients scheduled to receive chemotherapy for NSCLC were recruited.
Pittsburgh Sleep Quality Index, Epworth Sleepiness Scale, Functional Assessment of
Cancer TreatmentYLung (FACT-L), and Motionlogger Actigraph were used for data
collection. Results: Poor nocturnal sleep and QOL were evident among 29 patients
with NSCLC before treatment. The FACT-L subscale scores worsened and then
improved significantly from baseline through 2 rounds of chemotherapy. Objective
sleep duration and sleep efficiency were positively associated with FACT-L scores,
whereas objective sleep latency and wake after sleep onset were negatively associated
with FACT-L scores. Sleepy patients had significantly worse FACT-L scores than did
nonsleepy patients. The FACT-L subscale items that demonstrated significant
worsening and then improvement over time were shortness of breath, weight loss,
coughing, and chest tightness. Lung cancer patients experience early and middle
insomnia before and during treatment. Conclusion: Poor sleep quality is common
in patients receiving treatment for NSCLC and is related to poorer QOL and
respiratory symptoms. Implication for Practice: Patients with NSCLC require
60 n Cancer NursingTM, Vol. 38, No. 1, 2015 Dean et al
Copyright B 2015 Wolters Kluwer Health | Lippincott Williams & Wilkins
Author Affiliations: School of Nursing (Dr Dean, Ms Abu Sabbah, DrDickerson) and School of Medicine (Dr Steinbrenner), University at Buffalo,State University of New York; VA Western New York Health Systems (Ms Ziegler,Dr Steinbrenner); Department of Medicine, Thoracic Oncology, Buffalo (Dr Chen);Boromrajjonnani College of Nursing at Saraburi, Thailand (Dr Yingrengreung).
This work was conducted at and supported by the VA Western New YorkHealthcare System, Buffalo, NY.
Financial support was provided by the Oncology Nursing Society and NationalLung Cancer Partnership Lung Cancer Grant (to Drs Dean and Dickerson).
Mss Abu Sabbah and Ziegler and Drs Chen, Steinbrenner, and Yingrengreunghave no funding or conflicts of interest to disclose.
Correspondence: Grace E. Dean, PhD, RN, School of Nursing, University atBuffalo, 3435 Main St, 208 Wende Hall, Buffalo, NY 14214 ([email protected]).
Accepted for publication December 3, 2013.DOI: 10.1097/NCC.0000000000000128
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

routine screening for sleep disturbances. A positive screen for sleep disturbance
warrants a thorough sleep assessment using practice guidelines and, if necessary,
referral to a sleep specialist for diagnosis and treatment.
Adequate sleep is a fundamental requirement for a healthylifestyle, affecting both biological and psychological func-tioning and overall quality of life (QOL); however, the
impact of insufficient sleep in cancer is relatively uninvestigated.1
Few researchers have examined sleep-wake disturbances in pa-tients with cancer as a primary variable; even still, much of theevidence has emerged from research focusing on symptoms andQOL. Studies that have been conducted have reported that ratesof sleep-wake disturbances in patients with cancer (19%Y40%)are nearly double the rates reported by the general population(10%Y25%).2Y5 Furthermore, sleep-wake disturbances lead topronounced symptom distress: studies in recently diagnosed pa-tients suggest that insomnia, for example, is as significant a causeof distress as pain or nausea6,7 and is one of the most commonreasons patients are seen for a psychological evaluation.8 Despitethis, little is known about the etiology and both short- and long-term consequences of sleep-wake disturbances.9,10
Insomnia is the most common sleep disorder, defined as dif-ficulty falling asleep or early insomnia, difficulty staying asleepor middle insomnia, and early morning wakefulness or lateinsomnia.11 Using polysomnography, the criterion standard ofsleep measurement, the sleep patterns of patients with lung can-cer resembled those of patients with chronic insomnia: poorersleep efficiency, longer sleep latency, and difficulty remainingasleep.12 Long awakenings also interrupted the sleep of lungcancer patients, which included more stage I (light) sleep. Amore recent study of sleep-wake patterns using ambulatorypolysomnography in patients with advanced cancer, which in-cluded 30 patients with lung cancer, reported significantly morestage I sleep and a higher index of awakenings compared withpatients with breast cancer.13
Having a diagnosis of lung cancer is like sleeping with theenemy. For instance, lung cancer patients had the highest fre-quency of being overly fatigued (56%), using sleeping pills (40%),being overly sleepy (39.5%), and sleeping more than usual (34%)compared with other cancer patients with solid tumors.14 Patientswith lung cancer reported that poor sleep was related to worriesabout their state of health, mortality concerns, and stress, bothphysical and psychological.14 In addition, more than 50% ofpatients at diagnosis for primary lung cancer also have chronicobstructive pulmonary disease (COPD).15 It is challenging tosleep when you have difficulty breathing. As such, lung cancer isan excellent diagnostic model for studying sleep-wake distur-bances because of the high prevalence, severity, and impact onQOL. Because the intent of treatment is so often palliative and notcurative, maximizing QOL in this patient population is often asimportant as increasing the length of survival.
Lung cancer patients have significantly different self-reportedsleep quality compared with noncancer control subjects.16Y19
For example, patients with advanced lung cancer (n = 33) hadmuch higher Pittsburgh Sleep Quality Index (PSQI) globalscores (10.6), well above the threshold level of 5 for poor sleep
quality, than a reference group (2.7).19 Similar results have beenreported by others.17,18,20 In addition to sleep quality, differ-ences have been reported for patients with lung cancer in regardto a variety of sleep parameters and daytime consequences thatincluded prolonged sleep latency, shorter sleep duration, lowersleep efficiency, increased wake after sleep onset, and moredaytime sleepiness, compared with healthy adults.18 Gooneratneet al20 used a case-control design to compare lung cancer sur-vivors with noncancer control subjects and reported that lungcancer survivors spent significantly more time in bed and sig-nificantly less time asleep and had significantly lower sleep effi-ciency, but not shorter sleep latency. Because sleep latency didnot differ between the groups, the discrepancies in sleep effi-ciency were due to wakefulness after sleep onset. Surprisingly, thecancer survivors were a mean of 8 years postYcancer treatmentand still had significantly poorer sleep quality and lower sleepefficiency than age- and sex-matched noncancer control subjects.20
Much of the previous research on sleep in patients with lungcancer has focused on self-reported sleep measures. Few studieshave used objective measures to evaluate sleep in lung cancer,and even fewer studies have examined sleep longitudinally. Meth-odological limitations of previous studies also included smallsample sizes, limited valid and reliable measures for sleep-wakedisturbances, cross-sectional research designs, and the absence ofsleep assessment prior to the initiation of therapy. Thus, it isunclear what sleep-wake disturbances preexisted lung cancer treat-ment or whether sleep quality changed as a consequence of therapy.
The purpose of this study was to interpret sleep quality,daytime sleepiness, QOL, and 7-day actigraphy data to describepatterns and change over time in sleep-wake disturbances before,during, and after chemotherapy treatment in individuals withnonYsmall cell lung cancer (NSCLC). These time points wereselected to determine if sleep quality and QOL improved ordeclined from baseline levels. If sleep quality and QOL are notreturning to baseline levels before the next treatment, it mayhelp explain the development of chronic sleep disturbances andpoor QOL in some individuals. An improved understandingof sleep-wake disturbances through subjective and objectivemeasures is critical to the development of rational approaches toimprove the sleep and QOL of patients with cancer and improveour fundamental understanding of the relationships amongsleep, cancer, and QOL.
n Methods
Design
A 1-group, prospective, longitudinal design with 4-time repeatedmeasures was used to characterize and compare sleep and QOLbefore, during, and after treatment for lung cancer. The baselinemeasures were obtained 7 days before the first chemotherapy
Sleep in Lung Cancer Cancer NursingTM, Vol. 38, No. 1, 2015 n61
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

treatment. The preYsecond chemotherapy measure was obtained7 days before the second chemotherapy treatment, a time whenrecovery from the first chemotherapy adverse effects would beexpected. The preYthird chemotherapy measure was obtained7 days before the third chemotherapy treatment, a time whenrecovery from the second chemotherapy adverse effects would beexpected. The 6-month measure was obtained 6 months fromthe baseline measure. Because of significant sample attrition at6 months, this time point was not included in the longitudinalanalysis.
Power Analysis
The classic text on power analysis by Cohen21 has power tablesfor a variety of situations, but not paired t test designs. G-Powersoftware for paired t tests, with a medium effect size = 0.50,k = 3, and " = .05, demonstrated that 27 participants were neededfor 0.80 power. Because this was an exploratory pilot study with3 data collection points and a limited budget, our recruitmentgoal was to obtain complete data on 20 participants. Level ofsignificance was adjusted to P G .017 for multiple comparisons.
Participants
Participants were recruited from a Veterans AdministrationMedical Center and a comprehensive cancer center. The studywas approved by the institutional review boards at each hospitaland at the university. All participants provided written informedconsent. Patients eligible for the study were those with a path-ological diagnosis of inoperable NSCLC, scheduled to receivechemotherapy before recruitment, at least 21 years of age, andwith Karnofsky Performance Status of greater than 70% (unable
to carry on normal activities or work, but able to care for self).Patients were excluded if they had known brain metastases anduntreated obstructive sleep apnea.
Theoretical Framework
The theoretical framework that guided this study is the AdaptedTwo-Process Model of Sleep Regulation.18 The Two-ProcessModel of Sleep Regulation, one of the leading theories of sleepregulation, purports that the homeostatic drive to sleep (process S)interacts with the circadian process (process C) to predict thetiming and duration of sleep, structure of sleep, and changes indaytime wakefulness.22,23 With process S, the need to sleepincreases as the amount of prior wakefulness increases. The cir-cadian process communications time of day regulating the op-portunity for sleep. Adaptation of the model for lung cancerincluded a list of potential disease and treatment-related factorsthat may interfere with either process S or process C. For ex-ample, under disease-related factors, the authors suggest that thepresence of pain would produce arousal, affecting the homeo-static process S, whereas the presence of fatigue would reduceactivity, influencing the circadian process C.18
Variables and Measures
A chart review form was used to extract demographic, diagnostic,and treatment information, including age, gender histologic typeof lung cancer, stage, and chemotherapy regimen, from eachpatient’s medical record (Table 1).
Subjective sleep quality was assessed with the PSQI, a 19-item,self-report questionnaire that assesses sleep quality and quantity.24
The PSQI also assesses a range of sleep disturbances including
Table 1 & Summary of Study Instruments
Variable Instrument Scoring Reliability/Validity
Sleep quality PSQI 19 Items with varying response categories, including
forced-choice Likert-type subscales 0Y3,culminating in a global score: G5 (good sleep),95 (poor sleep). Maximum score = 21.
Internal consistency (0.58Y0.81)
Daytime sleepiness ESS 8 Likert-type items, to determine the likelihood of
dozing off or falling asleep in a variety of situations:0 (no chance of dozing) to 3 (high chance ofdozing). Summary scores 910 consistent with
daytime sleepiness. Maximum score = 24.
Internal consistency (0.59Y0.85)
Actigraphy Motion LoggerActigraph
Wrist-worn monitoring of activity used in assessmentof sleep disorders and sleep/wake patterns.
Software used to analyze data contains several sleepalgorithms, with high correlations topolysomnographic (PSG) measurements, for
estimation of sleep quality, quantity, and circadianphasing.
Sensitivity (sleep identification)993%, specificity (wake detection)
966%, and overall agreement withPSG 993%54
Quality of life FACT-L 34 Likert-type items, 0 (not at all) to 4 (very much);higher scores indicate better QOL and are composed
of the 27-item FACT-General (FACT-G) and7-item Lung Cancer Subscale. Maximum score = 136.
Internal consistency (0.79Y0.88)
Abbreviations: ESS, Epworth Sleepiness Scale; FACT-L, Functional Assessment of Cancer TherapyYLung; PSQI, Pittsburgh Sleep Quality Index.
62 n Cancer NursingTM, Vol. 38, No. 1, 2015 Dean et al
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

insomnia, sleep apnea, and limb movement disorders, as well asdaytime consequences of sleep. A global score can be calculated,as well as scores for 7 subscales: subjective sleep quality, sleeplatency, sleep efficiency, sleep duration, sleep disturbances, useof sleep medications, and daytime dysfunction. In addition toglobal sleep quality, the variables of interest for this study weresleep efficiency, sleep-onset latency, and total sleep time. ThePSQI global score ranging from 0 to 21 has been used in clinicaland research settings to distinguish good sleepers (G5) and poorsleepers (95) and is responsive to changes in insomnia.25 Goodmeasures of internal consistency a = 0.77 to 0.83, test-retestreliability r = 0.85 and 0.77, and criterion-related validity havebeen obtained.26,27
Subjective daytime sleepiness was evaluated with the EpworthSleepiness Scale (ESS), an 8-item, self-report questionnaire de-veloped by Johns.28 Epworth Sleepiness Scale is a subjectiverating of ‘‘trait’’ sleepiness that relies on retrospective reports ofdozing behavior in various hypothetical situations to establish anassessment of a patient’s global level of sleepiness. Epworth Sleep-iness Scale scores range from 0 to 24, with scores of more than 10indicating excessive daytime sleepiness. Epworth Sleepiness Scaletotal scores distinguished normal subjects from those with obstruc-tive sleep apnea, narcolepsy, or idiopathic hypersomnia.28 Inter-nal consistency between the 8 items as measured by Cronbach’s "is high, ranging from .73 to .88.29
Objective sleep-wake measures were obtained by using anactigraph. The Motionlogger Actigraph (Ambulatory Monitor-ing, Inc, Ardsley, New York) is a battery-powered wrist-worndevice that records wrist activity counts in 1-minute epochs (in-tervals) using a miniaturized accelerometer (sensitive to Q0.003 g).It is ideally worn on the nondominant wrist. Nocturnal sleep-wake variables of interest were sleep efficiency, sleep-onset latency,total sleep time, and wake after sleep onset. Sleep efficiency is timeasleep divided by time in bed as scored by actigraphy sleepalgorithm. Sleep latency is defined as the time in minutes to thefirst period of persistent inactivity (eg, after 5 minutes of con-tinuous inactivity). Total sleep time and waking after sleep onset(during time in bed) were determined by actigraphy sleep algo-rithm. Sleep diaries were used to determine ‘‘lights off’’ and ‘‘lightson’’ for the Action 3.8 ‘‘auto set down interval.’’ Sleep diaries werecompared with the software selected periods to determine whichepochs were inappropriate for measurement and should be deleted.
Wrist actigraphy has been studied in comparison to poly-somnography (‘‘gold standard’’ sleep studies), and the correlationswith EEG assessment of total sleep time were r = 0.91 (P G .001)for sum activity and r = 0.81 (P G .005) for maximum activity innursing home patients (nursing home patients can have prolongedbed-rest periods, and thus most closely approximate advancedcancer patients in this regard).30 Wrist actigraphy has been lessreliable when discriminating between quiet wakefulness and sleep,where it tends to overestimate sleep.31,32 To aid in the codingof bed time/rise time for actigraphy data, a sleep diary was com-pleted for 7 days in conjunction with actigraphy recordings.
Quality of life including psychological factors and symptomsspecific to lung cancer was measured with the Functional As-sessment of Cancer TherapyYLung (FACT-L) scale.33 A 36-itemself-report instrument, the FACT-L measures multidimensional
QOL by asking patients to rate a series of statements on a 5-pointLikert scale. It is composed of the 27-item FACT-General(FACT-G) and 9-item Lung Cancer Subscale (LCS). The LCSmonitors the severity of 7 lung cancer symptoms (shortness ofbreath, cough, tightness in chest, difficulty breathing, appetiteloss, weight loss, and lack of clear thinking) rated by the patienton a 0- to 4-point Likert scale with a maximum score of 28. Atotal FACT-L score is obtained by summing the FACT-G withthe LCS (2 of the 9 items are not scored). The maximum bestscore obtainable for the FACT-L is 136, with higher scorescorresponding to better QOL. A 2- to 3-point change in theFACT-L lung cancer subscale reflected a minimally importantdifference associated with performance status, weight loss, ob-jective tumor response, and time to progression.34 FunctionalAssessment of Cancer TherapyYLung is widely used in lungcancer clinical trials and provides validated clinically meaning-ful score changes (a +2-point or higher LCS and a +6-point orhigher FACT-L change prospectively define ‘‘improved’’symptom and QOL, respectively, whereas a j2-point or lowerLCS and a j6-point or lower FACT-L change prospectivelydefine ‘‘worsened’’ symptom and QOL, respectively).34,35 Inter-nal consistency of the 5 FACT-L subscales: physical well-being,functional well-being (FWB), social well-being, emotional well-being, and lung cancer symptoms, ranged from 0.56 to 0.89.33
Procedures
Clinical collaborators at the hospitals identified eligible partic-ipants, briefly explained the study, and referred those who agreedto be contacted by the investigator. The principal investigator(PI) then arranged to meet with potential participants at theclinic, determined eligibility, and described the study in moredetail. Following informed consent, each participant was trainedby the PI on completion of the self-report surveys and how/whento wear the actigraph. Participants were provided an oppor-tunity to demonstrate competency for using the sleep diary bycompleting data from the previous night’s bed time and currentday’s rise time. The Motionlogger Actigraph (Ambulatory Mon-itoring, Inc) was placed on the nondominant wrist, and partici-pants were instructed to wear the actigraph for 7 days and to returncompleted data collection materials to the PI on their next clinicappointment. Participants were paid $25 for complete data at eachtime point for a total of $100.
Data Analysis
Descriptive statistics and frequency distributions were com-puted for sample characteristics, PSQI, ESS, and QOL data.Pearson correlation coefficient was used to determine relation-ships among FACT-L subscale and total scores and sleep-wakemeasures. Paired t test was used to detect differences over timefrom baseline through preYthird treatment only, because therewere only 8 subjects at the 6-month data point (Table 2). Meanscores of the different domains of the FACT-L were compared insleepier versus less sleepy patients (ESS 910 vs G10 at any time)using the Mann-Whitney U test. All tests were 2-tailed, andP G .05 was considered statistically significant except for paired
Sleep in Lung Cancer Cancer NursingTM, Vol. 38, No. 1, 2015 n63
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

t tests, which required a value of P G .017 for significance. Ad-justments were not made for missing data. Cases with missingvalues were excluded from the analyses. Analyses were con-ducted with SPSS (version 20; SPSS Inc, Chicago, Illinois).
Action 3.8 analysis software (Ambulatory Monitoring, Inc)was used to score actigraphy data using zero crossing mode, theprimary mode of data collection for sleep estimation.36 The Ac-tion 3.8 sleep scoring algorithm was used to provide summarymeasures of activity during nocturnal time in bed for all pa-tients. Actigraphy recordings were averaged over 7 days.
n Results
Sample Characteristics
The sample included 29 participants. Table 2 provides descrip-tive data for the participants in the study, of whom 17 (59%)were recruited from a comprehensive cancer center, and 12 (41%)were recruited from a veterans hospital. The mean age of thissample was 67 years, with a mean body mass index of 28 (SD,8.3) kg/m2 (range, 18Y55 kg/m2). The majority of the samplewas male (62%), white (83%), married (45%), with at least ahigh school education (77%), and retired (42%) or disabled (27%).There was 1 (3%) who never smoked, 3 (10%) current smokers,23 quitters (79%), and 2 (7%) who refused to answer/missing data.Average number of cigarettes smoked per day was 26 (SD, 15)(range, 6Y70), and the average number of years smoked was38 (SD, 14) (range, 10Y60). The majority of patients were treatedevery 3 weeks (n = 25), with less than half (n = 12) receivingconcurrent radiotherapy.
Sample Attrition
Table 3 includes data on the high rate of attrition over the 6-monthstudy period. Overall, 72% (n = 21) did not complete the study.During the 6-month study period, however, 28% (n = 6) died,and 38% (n = 8) were too ill to continue. Other common reasonsfor not completing the study were loss of patients to follow-upevaluation and withdrawal. The times surrounding a new diag-nosis of cancer and cancer therapy are particularly difficult periodsfor recruitment and retention because patients are grappling withthe consequences of having cancer and undergoing intensivecancer treatment.37 Participants who completed the study were62% male, all white, and with a mean age of 70 years, similar tothe 21 participants who did not complete the study. Compar-isons on baseline FACT-L for those who completed the study(mean, 96.2) to those who did not complete the study (mean,89.1) were not significant (t27 = j1.324, P = .197).
Sleep Quality
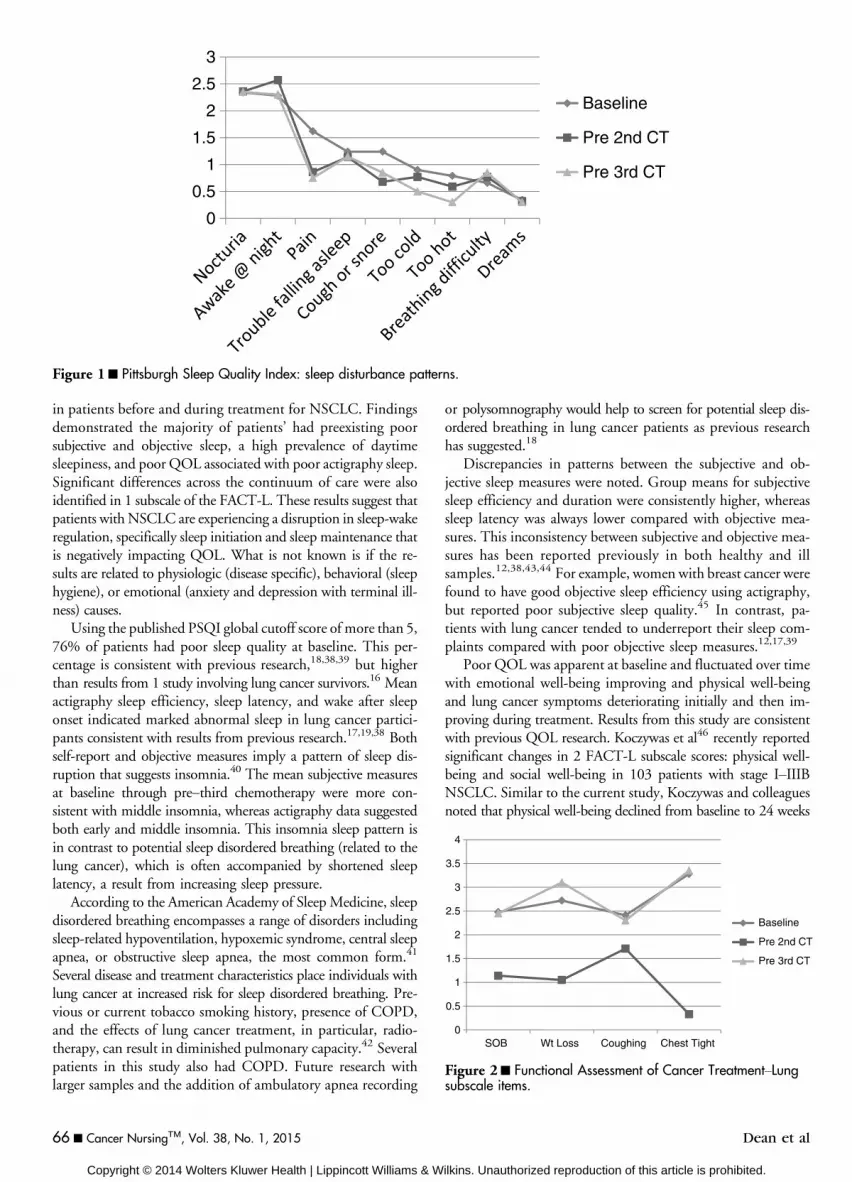
At baseline, nearly all mean PSQI variables suggested poor sleepquality, with 55% sleeping less than 6 hours per night. At preYsecond chemotherapy, all mean PSQI variables improved, butnot significantly, and 41% were sleeping less than 6 hours pernight. At preYthird chemotherapy, mean sleep efficiency andsleep duration were unchanged from preYsecond chemotherapy,whereas sleep latency and global sleep quality continued to de-crease, and 40% were sleeping less than 6 hours per night. Table 4provides descriptive statistics for the PQSI, actigraphy, andQOL. Means for sleep disturbance scores over time are dis-played graphically in Figure 1. Nocturia and sleep interruptionwere the most reported sleep disturbances.
Daytime Sleepiness
Epworth Sleepiness Scale or trait sleepiness scores that aregreater than 10 indicate excessive daytime sleepiness. The per-centage of patients with ESS scores of greater than 10 was 21%
Table 2 & Participant Characteristics (n = 29)
Range, y Mean (SD), y
Age 49Y86 66.6 (9.5)
n (%)
GenderMale 18 (62.1)Female 11 (37.9)
RaceWhite 24 (82.8)Black 5 (17.2)
Marital statusMarried 13 (44.8)Single 1 (3.4)Separated/divorced 11 (37.9)
Widowed 4 (13.8)Cancer stage
IIA 1 (3.4)
IIB 2 (6.9)IIIA 5 (17.2)IIIB 9 (31.0)
IV 12 (41.4)Lung cancer cell type
Adenocarcinoma 18 (62.1)
Squamous 8 (27.6)Large cell 2 (6.9)Mixed cell 1 (3.4)
Radiation therapy
Yes 15 (51.7)No 14 (48.3)
Chemotherapy
Yes 29 (100)No 0 (0)
Chemotherapy regimen
Carboplatin/paclitaxel 17 (58.6)Carboplatin/gemcitabine 2 (6.9)Carboplatin/etoposide 1 (3.4)Cisplatin/etoposide 8 (27.6)
Pemetrexed 1 (3.4)Comorbidities
Chronic obstructive
pulmonary disease
12
Cardiovascular disease 12Arthritis 11
Gastroesophageal refluxdisease
5
64 n Cancer NursingTM, Vol. 38, No. 1, 2015 Dean et al
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

at baseline, 33% at preYsecond chemotherapy, and 35% atpreYthird chemotherapy. Group means for ESS did not sig-nificantly change over time (Table 4).
Actigraphy
At baseline, mean actigraphy results revealed poor sleep (Table 4).All mean sleep measures improved at preYsecond chemotherapy.At preYthird chemotherapy, all mean sleep measures deterio-rated except wake after sleep onset, which was unchanged frompreYsecond chemotherapy. None of the changes were statisti-cally significant. Sleep duration was less than 6 hours in 45%at baseline, 35% at preYsecond chemotherapy, and 37% atpreYthird chemotherapy.
Quality of Life
Mean scores for subscales and total FACT-L indicated poor QOLat baseline (Table 4). The FACT emotional subscale increasedfrom baseline to preYsecond chemotherapy (P = .047), whereasthe FACT physical subscale declined from preYsecond to preYthird chemotherapy (P G .048). Interestingly, the lung cancersubscale deteriorated significantly at preYsecond chemotherapy(P G .001) and then improved significantly above baseline atpreYthird chemotherapy (P G .001). Lung cancer subscale items
that had significant changes over time were shortness of breath,weight loss, cough, and chest tightness (Figure 2).
Correlations
As shown in Table 5, significant negative correlations werefound between both the PSQI and the ESS and the majority ofsubscale and total FACT-L scores across time. Few moderateto large significant correlations among actigraphy sleep-wakeparameters and FACT-L total and subscale scores were evidentat baseline, but gradually increased during treatment. Longeractigraphy sleep duration and higher actigraphy sleep efficiencywere significantly correlated with higher QOL scores. Higheractigraphy sleep latency and more actigraphy wake after sleeponset was significantly correlated with lower QOL scores.
Comparison of Less Sleepy Versus Sleepier
The ESS was used to compare ‘‘less sleepy’’ defined as an ESSscore of less than 10 and ‘‘sleepier’’ as ESS score of more than 10(Table 6). In sleepier versus less sleepy patients, statistically sig-nificant differences were observed at baseline for emotional well-being (P G .03). This significant finding was also demonstratedat preYsecond chemotherapy for physical well-being (P G .001),FACT-Trial Outcome Index (P G .001), FACT-G (P G .001), andFACT-L (P G .05) and at preYthird chemotherapy for physicalwell-being (P G .02), functional well-being (P G .05), FACT-TrialOutcome Index (P G .03), FACT-G (P G .02), and FACT-L (P G .001).
n Discussion
This study provided prospective longitudinal measures ofsubjective sleep, actigraphy sleep-wake, QOL, and symptoms
Table 3 & Reasons for Attrition
ReasonPreY2ndChemo
PreY3rdChemo 6 mo Total (%)
Died 2 2 2 6 (28)
Declining health 0 1 7 8 (38)Withdrawal 1 0 1 2 (10)Lost to follow-up 3 0 2 5 (24)
Table 4 & Descriptive Data of Sleep and Functional Assessment of Cancer TherapyYLung
VariableBaseline, Mean (SD)
(n = 29)PreY2nd Chemo, Mean (SD)
(n = 23)PreY3rd Chemo, Mean (SD)
(n = 20)
PSQI sleep efficiency, % 84 (13) 85 (13) 85 (15)PSQI sleep duration, h 6.2 (1.2) 6.6 (1.2) 6.6 (1.1)
PSQI sleep latency, min 26 (20) 21 (14) 18 (10)PSQI global 7.3 (3.8) 6.9 (3.3) 6.3 (3.7)ESS 7.7 (3.3) 8.4 (4.9) 8.7 (4.5)
AW sleep efficiency, % 77 (17) 81 (16) 77 (19)AW sleep duration, h 5.9 (2.8) 6.7 (2.0) 5.4 (2.8)AW sleep latency, min 51 (62) 39 (57) 74 (98)
AW WASO, h 1.7 (1.2) 1.5 (1.0) 1.5 (1.2)FACT physical subscale 21 (4.7) 22 (5.4) 21 (6.6)FACT social subscale 22 (4.2) 22 (5.6) 22 (4.5)FACT emotional subscale 18 (4.3) 20 (3.2) 20 (4.3)
FACT functional subscale 17 (5.8) 19 (6.0) 18 (6.0)FACT lung cancer subscale 15 (2.3) 12 (1.7) 18 (3.7)FACT general 78 (13) 82 (15) 81 (15)
FACT-Lung 94 (14) 94 (16) 98 (17)
Abbreviations: AW, actigraphy; ESS, Epworth Sleepiness Scale; FACT, Functional Assessment of Cancer Therapy; PSQI, Pittsburgh Sleep Quality Index;WASO, wake after sleep onset.
Sleep in Lung Cancer Cancer NursingTM, Vol. 38, No. 1, 2015 n65
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
in patients before and during treatment for NSCLC. Findingsdemonstrated the majority of patients’ had preexisting poorsubjective and objective sleep, a high prevalence of daytimesleepiness, and poor QOL associated with poor actigraphy sleep.Significant differences across the continuum of care were alsoidentified in 1 subscale of the FACT-L. These results suggest thatpatients with NSCLC are experiencing a disruption in sleep-wakeregulation, specifically sleep initiation and sleep maintenance thatis negatively impacting QOL. What is not known is if the re-sults are related to physiologic (disease specific), behavioral (sleephygiene), or emotional (anxiety and depression with terminal ill-ness) causes.
Using the published PSQI global cutoff score of more than 5,76% of patients had poor sleep quality at baseline. This per-centage is consistent with previous research,18,38,39 but higherthan results from 1 study involving lung cancer survivors.16 Meanactigraphy sleep efficiency, sleep latency, and wake after sleeponset indicated marked abnormal sleep in lung cancer partici-pants consistent with results from previous research.17,19,38 Bothself-report and objective measures imply a pattern of sleep dis-ruption that suggests insomnia.40 The mean subjective measuresat baseline through preYthird chemotherapy were more con-sistent with middle insomnia, whereas actigraphy data suggestedboth early and middle insomnia. This insomnia sleep pattern isin contrast to potential sleep disordered breathing (related to thelung cancer), which is often accompanied by shortened sleeplatency, a result from increasing sleep pressure.
According to the American Academy of Sleep Medicine, sleepdisordered breathing encompasses a range of disorders includingsleep-related hypoventilation, hypoxemic syndrome, central sleepapnea, or obstructive sleep apnea, the most common form.41
Several disease and treatment characteristics place individuals withlung cancer at increased risk for sleep disordered breathing. Pre-vious or current tobacco smoking history, presence of COPD,and the effects of lung cancer treatment, in particular, radio-therapy, can result in diminished pulmonary capacity.42 Severalpatients in this study also had COPD. Future research withlarger samples and the addition of ambulatory apnea recording
or polysomnography would help to screen for potential sleep dis-ordered breathing in lung cancer patients as previous researchhas suggested.18
Discrepancies in patterns between the subjective and ob-jective sleep measures were noted. Group means for subjectivesleep efficiency and duration were consistently higher, whereassleep latency was always lower compared with objective mea-sures. This inconsistency between subjective and objective mea-sures has been reported previously in both healthy and illsamples.12,38,43,44 For example, women with breast cancer werefound to have good objective sleep efficiency using actigraphy,but reported poor subjective sleep quality.45 In contrast, pa-tients with lung cancer tended to underreport their sleep com-plaints compared with poor objective sleep measures.12,17,39
Poor QOL was apparent at baseline and fluctuated over timewith emotional well-being improving and physical well-beingand lung cancer symptoms deteriorating initially and then im-proving during treatment. Results from this study are consistentwith previous QOL research. Koczywas et al46 recently reportedsignificant changes in 2 FACT-L subscale scores: physical well-being and social well-being in 103 patients with stage IYIIIBNSCLC. Similar to the current study, Koczywas and colleaguesnoted that physical well-being declined from baseline to 24 weeks
Figure 1n Pittsburgh Sleep Quality Index: sleep disturbance patterns.
Figure 2n Functional Assessment of Cancer TreatmentYLungsubscale items.
66 n Cancer NursingTM, Vol. 38, No. 1, 2015 Dean et al
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Table
5&Correlatio
nsAmon
gSleepSe
lf-repo
rt,Actigraph
ySleep-W
ake,
andFunctio
nalA
ssessm
entof
Can
cerTrea
tmen
tYLung
Variable
PSQI1
ESS1
AW
SM1
AW
SE1
AW
SL1
AW
WA1
PSQI2
ESS2
AW
SM2
AW
SE2
AW
SL2
AW
WA2
PSQI3
ESS3
AW
SM3
AW
SE3
AW
SL3
AW
WA3
PW
Bj
0.5
2a
j0
.43
bj
0.4
6b
j0
.43
bj
0.6
7a
j0
.54
b
SWB
0.5
4a
0.5
4b
j0
.44
bj
0.6
1a
00
.63
a0
.61
aj
0.7
4a
EW
Bj
0.4
3b
0.5
3a
j0
.63
a
FW
Bj
0.4
5b
j0
.57
a0
.56
*j
0.6
4a
LC
S0
.40
bj
0.6
9a
FA
CT
-TO
Ij0
.53
aj
0.5
3b
j0
.66
aj
0.6
2a
FA
CT
-Gj
0.5
0b
j0
.56
a0
.62
aj
0.7
2a
FA
CT
-Lj
0.5
1b
j0
.63
a0
.59
bj
0.7
0a
Abbre
viat
ion
s:A
WSE
,ac
tigr
aph
ysl
eep
effi
cien
cy;
AW
SL,
acti
grap
hy
slee
pla
ten
cy;
AW
SM,
acti
grap
hy
slee
pm
inu
tes;
AW
WA
,ac
tigr
aph
yw
ake
afte
rsl
eep
onse
t;E
SS,
Ep
wor
thSl
eep
ines
sSc
ale;
EW
B,
emot
ion
alsu
bsc
ale
ofF
AC
T-L
;F
un
ctio
nal
Ass
essm
ent
ofC
ance
rT
her
apy-
Tri
alO
utc
ome
Ind
ex(F
AC
T-T
OI)
;F
AC
T-G
,su
mof
PW
B,
SWB
,E
WB
,an
dF
WB
;F
AC
T-L
,F
AC
T-G
+L
CS;
FW
B,
fun
ctio
nal
sub
scal
eof
FA
CT
-L;
LC
S,lu
ng
sym
pto
msu
bsc
ale
ofF
AC
T-L
;P
SQI,
Pit
tsb
urg
hSle
epQ
ual
ity
Ind
ex;
PW
B,
ph
ysic
alsu
bsc
ale
ofF
AC
T-L
;SW
B,
soci
alsu
bsc
ale
ofF
AC
T-L
.Su
per
scri
pt
nu
mber
sre
pre
sen
td
ata
collec
tion
tim
ep
oin
t:1
=bas
elin
e,2
=p
re-2
nd
chem
o,3
=p
re-3
rdch
emo.
a Cor
rela
tion
issi
gnif
ican
tat
the
.01
leve
l.bC
orre
lati
onis
sign
ific
ant
atth
e.0
5le
vel.
Table
6&Qua
lityof
Life
inSleepier
andLess
Sleepy
Individu
alsDetermined
bytheEp
worth
Sleepine
ssScale(ESS
)at
Baseline
FACT-LSu
bscales(93Times
Point)Group
s(Based
onES
SScore)
Baseline
PreY2nd
Che
mo
PreY3rd
Che
mo
ESS910
ESSe10
ESS910
ESSe10
ESS910
ESSe10
Ph
ysic
al,
n(m
ean
ran
k),P
(2-t
aile
d)
14
(12
.79
)1
5(1
7.0
7),
.17
31
2(7
.08
)1
0(1
6.8
0),
.00
01
0(7
.20
)1
0(1
3.8
0),
.01
2So
cial
,n
(mea
nra
nk)
,P
(2-t
aile
d)
14
(13
.68
)1
5(1
6.2
3),
.41
71
2(9
.96
)1
0(1
3.3
5),
.22
01
0(9
.75
)1
0(1
1.2
5),
.56
9E
mot
ion
al,
n(m
ean
ran
k),P
(2-t
aile
d)
14
(11
.21
)1
5(1
8.5
3),
.02
01
2(9
.17
)1
0(1
4.3
0),
.06
21
0(8
.30
)1
0(1
2.7
0),
.09
3F
un
ctio
nal
,n
(mea
nra
nk)
,P
(2-t
aile
d)
14
(13
.82
)1
5(1
6.1
0),
.47
01
2(9
.33
)1
0(1
4.1
0),
.08
41
0(7
.90
)1
0(1
3.1
0),
.04
9
Lu
ng
can
cer
sub
scal
e,n
(mea
nra
nk)
,P
(2-t
aile
d)
14
(15
.18
)1
5(1
4.8
3),
.91
11
2(1
0.8
3)
10
(12
.30
),.5
90
10
(7.9
5)
10
(13
.05
),.0
52
Tri
alO
utc
ome
Ind
ex,
n(m
ean
ran
k),P
(2-t
aile
d)
14
(13
.25
)1
5(1
6.6
3),
.28
41
2(7
.88
)1
0(1
5.8
5),
.00
41
0(7
.45
)1
0(1
3.5
5),
.02
1F
AC
T-G
ener
al,
n(m
ean
ran
k),P
(2-t
aile
d)
14
(12
.04
)1
5(1
7.7
7),
.07
01
2(8
.21
)1
0(1
5.4
5),
.00
91
0(7
.25
)1
0(1
3.7
5),
.01
4
FA
CT
-L,
n(m
ean
ran
k),P
(2-t
aile
d)
14
(12
.04
)1
5(1
7.7
7),
.07
01
2(8
.33
)1
0(1
5.3
0),
.01
21
0(7
.05
)1
0(1
3.9
5),
.00
9
Abbre
viat
ion
:F
AC
T-L
,F
un
ctio
nal
Ass
essm
ent
ofC
ance
rT
her
apyY
Lu
ng.
Sleep in Lung Cancer Cancer NursingTM, Vol. 38, No. 1, 2015 n67
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

and then improved over time to surpass baseline at 36 and52 weeks. Other investigators have reported similar variations inQOL and symptoms in patients with NSCLC throughout treat-ment.47Y50 Understanding individual patient patterns of changein symptoms and QOL is also important when planning forassessment and management.
The addition of actigraphy measures added new perspectives.Significant associations among objective sleep-wake parametersand FACT-L total and subscale scores were evident. In addition,few studies have explored the relationship between sleep andQOL in patients with lung cancer. Similar to our study, Chenet al51 found that sleep disturbance was significantly associatedwith poorer functional status in 115 patients receiving a fourthcycle of chemotherapy for lung cancer. Gooneratne et al16 re-ported that QOL in lung cancer survivors was not significantlydifferent from noncancer control subjects, but lung cancer sur-vivors with poorer sleep quality had significantly worse QOLthan those with good sleep quality, similar to our study. Thesestudies suggest that patients with newly diagnosed lung cancerand patients receiving treatment for lung cancer have increasedsymptoms and significantly worse QOL compared with controlsubjects. Later on, survivors with poor quality sleep continue to havesignificantly worse QOL than those with good sleep quality. Soperhaps improving sleep quality may be a key to improving QOL.
The FACT-LCS subscale items that changed significantlyover time were shortness of breath, cough, chest tightness, andweight loss. Three of these items (eg, shortness of breath, cough,and chest tightness) were identified as the most important symp-toms reported by patients with NSCLC and a core set of rel-evant pulmonary symptoms that may be used to meaningfullyassess patients’ pulmonary status.52 Similarly, dyspnea was fre-quently reported as a cause of poor sleep in patients receivingtreatment and in lung cancer survivors.14,18,20 Although the lackof support for a robust relationship between sleep disturbancesand respiratory symptoms in the current study rests mainly withthe small sample size, the impact of respiratory symptoms onarousal and resulting insomnia in patients with lung cancer war-rants further exploration. Assessment and management of pul-monary symptoms may improve outcomes for these patientsboth during and after treatment.
Significant differences in FACT-L scores were identified whennonsleepy patients were compared with sleepy patients using pub-lished ESS score cut-points. Although several FACT-L total andsubscale scores were statistically significant when comparing these2 groups of sleepers in this study, previous research has dem-onstrated that differences greater than 2 to 3 points are consideredclinically important for the FACT-G physical and functionalsubscales and greater than 2 points for the FACT-G emotionalsubscale.53 Mean subscale and total FACT-L scores were morethan 10 points lower in poor sleepers before the second and thirdchemotherapy treatments in the current study, thus indicating theclinical significance of sleepiness on their QOL. For those withpoor sleep, sleep is indeed the enemy that affects their QOLbefore and during treatment. Future investigation into the role ofpoor sleep in symptom distress and the potential influence ofsleep interventions, such as for insomnia treatment, in moderat-ing the distress are warranted.
Attrition was a major issue in this study. The most commonreasons for attrition were declining health (38%) and death(28%), both reasons highlighted by others with similar pop-ulations.37,54 Higher rates of retention have been reported whenstudy designs require fewer data collection points.55 The challengefor recruiting and retaining vulnerable populations, such as pa-tients receiving treatment for NSCLC, is the ability to balancelow patient burden against the need to record the patient ex-perience and related needs at the end of life.55
Limitations
Our study has several limitations. First, this small cohort withattrition was collected with restrictive eligibility criteria (Karnofsky970%) and selectivity of clinicians who referred patients versussystematic screening for eligibility from a Veterans Affairs oncologyclinic and comprehensive cancer center lung cancer clinic. Second,our data collection period with the actigraph and sleep diary wasfor 7 days. Although longer observation periods, such as 2 weeks,have been used, we felt that a 7-day period provided a reasonableand complete picture of an individual’s sleep. Longer recordingperiods would increase subject burden and could result in anincreased chance of data loss due to subjects forgetting/neglectingto complete daily sleep diaries. The subjects in the current studywere in the advanced stages of their disease and were particularlyvulnerable to these additional study burdens. Third, while wenoted large sleep latencies with actigraphy, these findings should beinterpreted with caution. Sleep latency assessment by actigraphy isgenerally considered to be one of the least accurate actigraphic sleepparameters. Whereas actigraphy can provide useful informationregarding sleep and wakefulness, polysomnography is requiredto determine stages of sleep and is used for diagnosing a variety ofsleep disorders. Inclusion of polysomnography in future researchwould permit assessment of other causes of sleep-wake disturbances,including periodic limb movements and sleep apnea. Patients werenot screened at enrollment for sleep apnea, periodic limb move-ments, or restless leg syndrome due to study budgetary constraints.
Implications for Practice
Although this study is limited by sample size and attrition, sev-eral insights are provided for clinical practice. Given that themajority of patients receiving treatment for lung cancer reportedpoor sleep, routine sleep assessment at diagnosis is essential.18 Inaddition, poor sleepers had lower QOL, particularly related toshortness of breath, cough, and chest tightness. Improving lungcancer symptoms such as dyspnea may improve sleep. Resourceguides for the clinical assessment and management of sleep anddyspnea include the Oncology Nursing Society’s putting evidenceinto practice and the National Comprehensive Cancer Network’sPractice Guidelines for Supportive Care, Palliative Care, andSurvivorship.56,57
n Conclusion
In conclusion, the findings from this study demonstrate that poorsleep quality is common in patients before receiving treatment for
68 n Cancer NursingTM, Vol. 38, No. 1, 2015 Dean et al
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

NSCLC and that poor sleep is related to QOL and respiratorysymptoms. Future research using larger samples and prospectivemethods will help to elucidate their clinical significance.
ACKNOWLEDGMENTS
The authors thank the Oncology Nursing Society and NationalLung Cancer Partnership Lung Cancer Grant for financial supportof the study (to Drs Dean and Dickerson). The authors also thankMary Ann Jezewski, PhD, FAAN, and Yow-Wu B. Wu, PhD,for their thoughtful review of earlier versions of this manuscript.
References
1. Ancoli-Israel S. Sleep and fatigue in cancer patients. In: Kryper MH,
Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 4th ed.
Philadelphia, PA: Elsevier Saunders; 2005:1218Y1224.
2. Lee K, Cho M, Miaskowski C, Dodd M. Impaired sleep and rhythms in
persons with cancer. Sleep Med Rev. 2004;8(3):199Y212.
3. Fiorentino L, Ancoli-Israel S. Insomnia and its treatment in women with
breast cancer. Sleep Med Rev. 2006;10(6):419Y429.
4. Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and
psychiatric disorders. An opportunity for prevention? JAMA. 1989;262(11):
1479Y1484.
5. Ohayon M. Epidemiological study on insomnia in the general pop-
ulation. Sleep. 1996;19(Suppl 3):S7YS15.
6. Munro AJ, Potter S. A quantitative approach to the distress caused by
symptoms in patients treated with radical radiotherapy. Br J Cancer. 1996;
74(4):640Y647.
7. Degner LF, Sloan JA. Symptom distress in newly diagnosed ambulatory
cancer patients and as a predictor of survival in lung cancer. J Pain SymptomManage. 1995;10(6):423Y431.
8. Akechi T, Nakano T, Okamura H, et al. Psychiatric disorders in cancer
patients: descriptive analysis of 1721 psychiatric referrals at two Japanese
cancer center hospitals. Jpn J Clin Oncol. 2001;31(5):188Y194.
9. Savard J, Morin CM. Insomnia in the context of cancer: a review of a
neglected problem. J Clin Oncol. 2001;19(3):895Y908.
10. Barton-Burke M. Cancer-related fatigue and sleep disturbances. Further
research on the prevalence of these two symptoms in long-term cancer
survivors can inform education, policy, and clinical practice. Am J Nurs.2006;106(Suppl 3):72Y77.
11. Pigeon WR, Caine ED. Insomnia and the risk for suicide: does sleep
medicine have interventions that can make a difference? Sleep Med.
2010;11(9):816Y817.
12. Silberfarb PM, Hauri PJ, Oxman TE, Schnurr P. Assessment of sleep in
patients with lung cancer and breast cancer. J Clin Oncol. 1993;11(5):
997Y1004.
13. Parker KP, Bliwise DL, Ribeiro M, et al. Sleep/Wake patterns of individuals
with advanced cancer measured by ambulatory polysomnography. J ClinOncol. 2008;26(15):2464Y2472.
14. Davidson JR, MacLean AW, Brundage MD, Schulze K. Sleep distur-
bance in cancer patients. Soc Sci Med. 2002;54(9):1309Y1321.
15. Loganathan RS, Stover DE, Shi W, Venkatraman E. Prevalence of COPD
in women compared to men around the time of diagnosis of primary lung
cancer. Chest. 2006;129(5):1305Y1312.
16. Gooneratne NS, Dean GE, Rogers AE, Nkwuo JE, Coyne JC, Kaiser LR.
Sleep and quality of life in long-term lung cancer survivors. Lung Cancer.2007;58(3):403Y410.
17. Le Guen Y, Gagnadoux F, Hureaux J, et al. Sleep disturbances and impaired
daytime functioning in outpatients with newly diagnosed lung cancer. LungCancer. 2007;58(1):139Y143.
18. Vena C, Parker K, Allen R, Bliwise D, Jain S, Kimble L. Sleep-wake dis-
turbances and quality of life in patients with advanced lung cancer. OncolNurs Forum. 2006;33(4):761Y769.
19. Levin RD, Daehler MA, Grutsch JF, et al. Circadian function in pa-
tients with advanced non-small-cell lung cancer. Br J Cancer. 2005;93(11):
1202Y1208.
20. Gooneratne NS, Dean GE, Rogers AE, Nkwuo JE, Coyne JC, Kaiser LR.
Sleep and quality of life in long-term lung cancer survivors. Lung Cancer.2007;58(3):403Y410.
21. Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York:
Academic Press; 1977.
22. Borbely AA. A two process model of sleep regulation. Hum Neurobiol.1982;1(3):195Y204.
23. Borbely AA, Achermann P. Sleep Homeostasis and Models of Sleep Regulation.Principles and Practice of Sleep Medicine. 4th ed. Philadelphia, PA: Elsevier
Saunders; 2005:405Y417.
24. Buysse DJ, Reynolds CF 3rd, Monk TH, Hoch CC, Yeager AL, Kupfer DJ.
Quantification of subjective sleep quality in healthy elderly men and
women using the Pittsburgh Sleep Quality Index (PSQI). Sleep. 1991;14(4):
331Y338.
25. Dolberg OT, Hirschmann S, Grunhaus L. Melatonin for the treatment
of sleep disturbances in major depressive disorder. Am J Psychiatry. 1998;
155(8):1119Y1121.
26. Beck SL, Schwartz AL, Towsley G, Dudley W, Barsevick A. Psychometric
evaluation of the Pittsburgh Sleep Quality Index in cancer patients. J PainSymptom Manage. 2004;27(2):140Y148.
27. Gentili A, Weiner DK, Kuchibhatla M, Edinger JD. Test-retest reliability of
the Pittsburgh sleep quality index in nursing home residents. J Am GeriatrSoc. 1995;43(11):1317Y1318.
28. Johns MW. A new method for measuring daytime sleepiness: the Epworth
Sleepiness Scale. Sleep. 1991;14(6):540Y545.
29. Johns MW. Reliability and factor analysis of the Epworth Sleepiness
Scale. Sleep. 1992;15(4):376Y381.
30. Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP.
The role of actigraphy in the study of sleep and circadian rhythms. Sleep.
2003;26(3):342Y392.
31. Hauri PJ, Wisbey J. Wrist actigraphy in insomnia. Sleep. 1992;15(4):
293Y301.
32. Buysse DJ, Ancoli-Israel S, Edinger JD, Lichstein KL, Morin CM. Recom-
mendations for a standard research assessment of insomnia. Sleep. 2006;
29(9):1155Y1173.
33. Butt Z, Webster K, Eisenstein AR, et al. Quality of life in lung cancer:
the validity and cross-cultural applicability of the Functional Assessment
of Cancer TherapyYLung scale. Hematol Oncol Clin North Am. 2005;
19(2):389Y420, viii.
34. Cella D, Eton DT, Fairclough DL, et al. What is a clinically meaningful
change on the Functional Assessment of Cancer TherapyYLung (FACT-L)
Questionnaire? Results from Eastern Cooperative Oncology Group
(ECOG) study 5592. J Clin Epidemiol. 2002;55(3):285Y295.
35. Cella DF, Tulsky DS, Gray G, et al. The Functional Assessment of Cancer
Therapy scale: development and validation of the general measure. J ClinOncol. 1993;11(3):570Y579.
36. Berger AM, Wielgus KK, Young-McCaughan S, Fischer P, Farr L, Lee KA.
Methodological challenges when using actigraphy in research. J PainSymptom Manage. 2008;36(2):191Y199.
37. Cooley ME, Sarna L, Brown JK, et al. Challenges of recruitment and
retention in multisite clinical research. Cancer Nurs. 2003;26(5):376Y384;
quiz 376Y385.
38. Wang SY, Chang HJ, Lin CC. Sleep disturbances among patients with
nonYsmall cell lung cancer in Taiwan: congruence between sleep log and
actigraphy. Cancer Nurs. 2010;33(1):E11YE17.
39. Dean GE, Finnell DS, Scribner M, Wang YJ, Steinbrenner LM, Gooneratne NS.
Sleep in lung cancer: the role of anxiety, alcohol and tobacco. J Addict Nurs.2010;21:130Y138.
40. Pigeon WR. Diagnosis, prevalence, pathways, consequences & treatment
of insomnia. Indian J Med Res. 2010;131:321Y332.
41. Medicine AAoS. The international classification of sleep disorders. 2nd ed.
Westchester, IL: American Academy of Sleep Medicine; 2005.
42. Parish JM. Sleep-related problems in common medical conditions. Chest.2009;135(2):563Y572.
43. Rumble ME, Keefe FJ, Edinger JD, Porter LS, Garst JL. A pilot study
investigating the utility of the cognitive-behavioral model of insomnia in
early-stage lung cancer patients. J Pain Symptom Manage. 2005;30(2):
160Y169.
Sleep in Lung Cancer Cancer NursingTM, Vol. 38, No. 1, 2015 n69
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

44. Vitiello MV, Larsen LH, Moe KE. Age-related sleep change: gender and
estrogen effects on the subjective-objective sleep quality relationships of
healthy, noncomplaining older men and women. J Psychosom Res. 2004;56(5):
503Y510.
45. Enderlin CA, Coleman EA, Cole C, et al. Subjective sleep quality, ob-
jective sleep characteristics, insomnia symptom severity, and daytime
sleepiness in women aged 50 and older with nonmetastatic breast cancer.
Oncol Nurs Forum. 2011;38(4):E314YE325.
46. Koczywas M, Williams AC, Cristea M, et al. Longitudinal changes in
function, symptom burden, and quality of life in patients with early-stage
lung cancer. Ann Surg Oncol. 2013;20(6):1788Y1797.
47. Akin S, Can G, Aydiner A, Ozdilli K, Durna Z. Quality of life, symptom
experience and distress of lung cancer patients undergoing chemotherapy.
Eur J Oncol Nurs. 2010;14(5):400Y409.
48. Lee LJ, Chung CW, Chang YY, et al. Comparison of the quality of life
between patients with nonYsmall-cell lung cancer and healthy controls.
Qual Life Res. 2011;20(3):415Y423.
49. Lovgren M, Tishelman C, Sprangers M, Koyi H, Hamberg K. Symp-
toms and problems with functioning among women and men with
inoperable lung cancerVa longitudinal study. Lung Cancer. 2008;60(1):
113Y124.
50. Matsuda A, Yamaoka K, Tango T. Quality of life in advanced nonYsmall
cell lung cancer patients receiving palliative chemotherapy: a meta-analysis
of randomized controlled trials. Exp Ther Med. 2012;3(1):134Y140.
51. Chen ML, Yu CT, Yang CH. Sleep disturbances and quality of life in lung
cancer patients undergoing chemotherapy. Lung Cancer. 2008;62(3):391Y400.
52. Salminen EK, Silvoniemi M, Syrj.nen K, Kaasa S, Kloke M, Klepstad P.
Opioids in pain management of mesothelioma and lung cancer patients.
Acta Oncol. 2013;52(1):30Y37.
53. Webster K, Cella D, Yost K. The Functional Assessment of Chronic
Illness Therapy (FACIT) measurement system: properties, applications,
and interpretation. Health Qual Life Outcomes. 2003;1:79.
54. Cleeland CS, Wang XS, Shi Q, et al. Automated symptom alerts reduce
postoperative symptom severity after cancer surgery: a randomized con-
trolled clinical trial. J Clin Oncol. 2011;29(8):994Y1000.
55. Steinhauser KE, Clipp EC, Hays JC, et al. Identifying, recruiting, and
retaining seriously-ill patients and their caregivers in longitudinal re-
search. Palliat Med. 2006;20(8):745Y754.
56. NCCN. Clinical Practice Survivorship Guidelines. National Comprehen-
sive Cancer Network. March 13, 2013. http://www.nccn.org/professionals/
physician_gls/f_guidelines.asp#survivorship. Accessed August 30, 2013.
57. Page MS, Berger AM, Johnson LB. Putting evidence into practice:
evidence-based interventions for sleep-wake disturbances. Clin J OncolNurs. 2006;10(6):753Y767.
70 n Cancer NursingTM, Vol. 38, No. 1, 2015 Dean et al
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.





























